Submitted:
23 February 2025
Posted:
24 February 2025
You are already at the latest version
Abstract
Congestion is a key clinical feature of heart failure (HF), contributing to hospitalizations, disease progression, and poor outcomes. While traditionally considered a hemodynamic issue, congestion is now recognized as a systemic process affecting multiple organs. Renal dysfunction arises from impaired perfusion and sodium retention, leading to maladaptive left ventricular remodeling. Hepatic congestion contributes to cholestatic liver injury, while metabolic disturbances drive anemia, muscle wasting, and systemic inflammation. Additionally, congestion disrupts the intestinal barrier and immune function, exacerbating HF progression. Given its widespread impact, effective congestion management requires a shift from a cardiovascular-centered approach to a comprehensive, multidisciplinary strategy. Targeted decongestive therapy, metabolic and nutritional optimization, and immune modulation are crucial in mitigating congestion-related organ dysfunction. Early recognition and intervention are essential to slow disease progression, preserve functional capacity, and improve survival. Addressing HF congestion through personalized, evidence-based strategies is vital for optimizing long-term care and advancing treatment paradigms.
Keywords:
heart failure
; congestion
; pathophysiology
1. Introduction
Heart failure (HF) is a complex syndrome in which congestion plays a central role in disease progression and clinical outcomes. Characterized by extracellular fluid accumulation, congestion is the leading cause of hospitalizations and readmissions, affecting patients across various HF phenotypes, from de novo HF to acute decompensation and advanced HF [1,2,3].
The etiology of HF is diverse, with ischemic heart disease as the most common cause, often linked to prior myocardial infarction [4,5]. Non-ischemic factors such as hypertension, diabetes, obesity, chronic lung disease, systemic inflammation, and cardiotoxic agents also contribute, frequently interacting with arrhythmias, infections, and comorbidities, leading to varied clinical presentations [6,7]. Clinically, HF presents in various forms, from acute pulmonary edema and hypertensive HF to severe cases like cardiogenic shock and decompensated chronic HF. Prognosis varies, with hypertension-related HF showing better outcomes, while cardiogenic shock remains the most fatal presentation [6,9].
While HF originates in the heart, persistent congestion and impaired perfusion impact multiple organ systems, including the kidneys, liver, lungs, gastrointestinal tract, and nervous system. This systemic involvement, driven by congestion, inflammation, and neurohormonal activation, worsens morbidity and mortality, complicating management [8]. Recognizing the multi-organ impact of HF-related congestion is essential for optimizing treatment and improving patient outcomes.
2.1. Congestion Is a Distinctive Mark of Heart Failure
2.1.1. Clinical Profile of Patients and Symptomatology
Heart failure (HF) classification has evolved, yet defining distinct patient groups remains challenging (Table 1). One widely accepted system categorizes HF into four progressive stages. Stage A includes individuals at risk but without structural heart disease, while Stage B, or pre-HF, involves structural abnormalities without symptoms. Stage C marks the onset of symptomatic HF, and Stage D represents advanced disease with persistent symptoms despite optimal treatment [6,10].
Ejection fraction remains central to HF classification, distinguishing between preserved (HFpEF), mildly reduced (HFmrEF), and reduced ejection fraction (HFrEF). The NYHA functional classification further assesses severity based on physical limitations, ranging from asymptomatic (Class I) to severe symptoms even at rest (Class IV) [11].
The clinical presentation of HF varies depending on which side of the heart is affected. Left-sided HF leads to pulmonary congestion, causing breathlessness, fatigue, and cough. In contrast, right-sided HF results in systemic congestion, often manifesting as peripheral edema, hepatomegaly, and jugular vein distension. While right HF can develop as a consequence of left HF, it may also arise from pulmonary diseases or congenital heart defects, further complicating disease progression [12,13,14].

Table 1.
Comprehensive Heart Failure Classification Table.
| Classification System | Criteria and Categories | Clinical Implications |
|---|---|---|
| Universal Classification |
Stage A: At risk (no structural disease or symptoms) Stage B: Pre-HF (structural disease, abnormal function, elevated biomarkers, no symptoms) Stage C: Symptomatic HF (structural/functional abnormality with past or current symptoms) Stage D: Advanced HF (persistent symptoms despite optimal treatment, requiring specialized care) |
Identifies patients at risk and guides early intervention strategies to prevent progression. |
| ACC/AHA Stages |
Stage A:
At risk for HF Stage B: Pre-HF (structural disease, no symptoms) Stage C: Symptomatic HF Stage D: Advanced HF (persistent symptoms despite optimal therapy) |
Provides a framework for staging HF, aiding in risk stratification and treatment escalation. |
| NYHA Functional Classification |
Class I:
No limitation on physical activity Class II: Mild symptoms with ordinary activity Class III: Marked limitation in daily activities Class IV: Symptoms present at rest and worsened by any activity |
Assesses functional impairment, guiding therapy intensity, and predicting prognosis. |
2.2. Pathophysiology of Congestion in HF
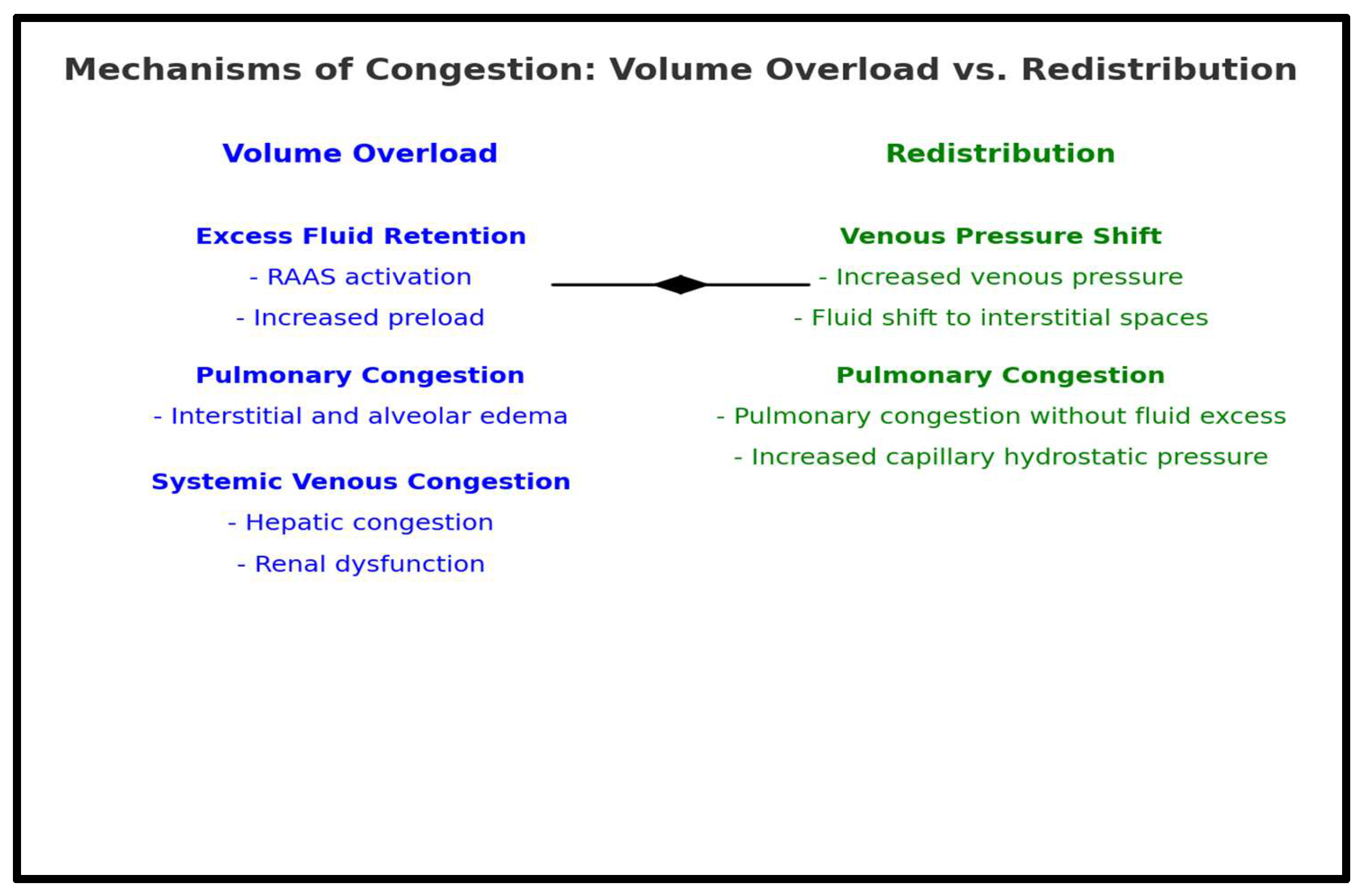
Congestion is a primary contributor to acute heart failure (AHF) hospitalizations, often outweighing symptoms related to reduced cardiac output [15]. It develops through two distinct mechanisms: volume overload and redistribution, each with unique pathophysiological implications.
Volume overload occurs gradually over days or weeks as reduced cardiac output activates neurohormonal compensatory mechanisms, including RAAS and SNS activation, leading to vasoconstriction, sodium and water retention, and increased preload and afterload [16,17,18,19]. Initially, congestion is hemodynamic, characterized by rising venous pressures. As fluid accumulates in the lungs and liver, it progresses to clinical congestion, presenting with overt symptoms [19].
Volume redistribution, in contrast, is a rapid shift of fluid from the splanchnic venous system to the central circulation, often triggered by hypertension, myocardial ischemia, renal dysfunction, or neurohormonal activation [16,17]. This process elevates central venous and pulmonary pressures, leading to acute pulmonary congestion without significant weight gain [17,21,22]. In such cases, vasodilator therapy is often more effective than diuretics in symptom management [17].
Recognizing these mechanisms is essential for optimizing therapeutic strategies, as targeted interventions can improve clinical outcomes in patients with HF.
Figure 1.
Mechanism of congestion in heart failure: Volume overload vs Redistribution.
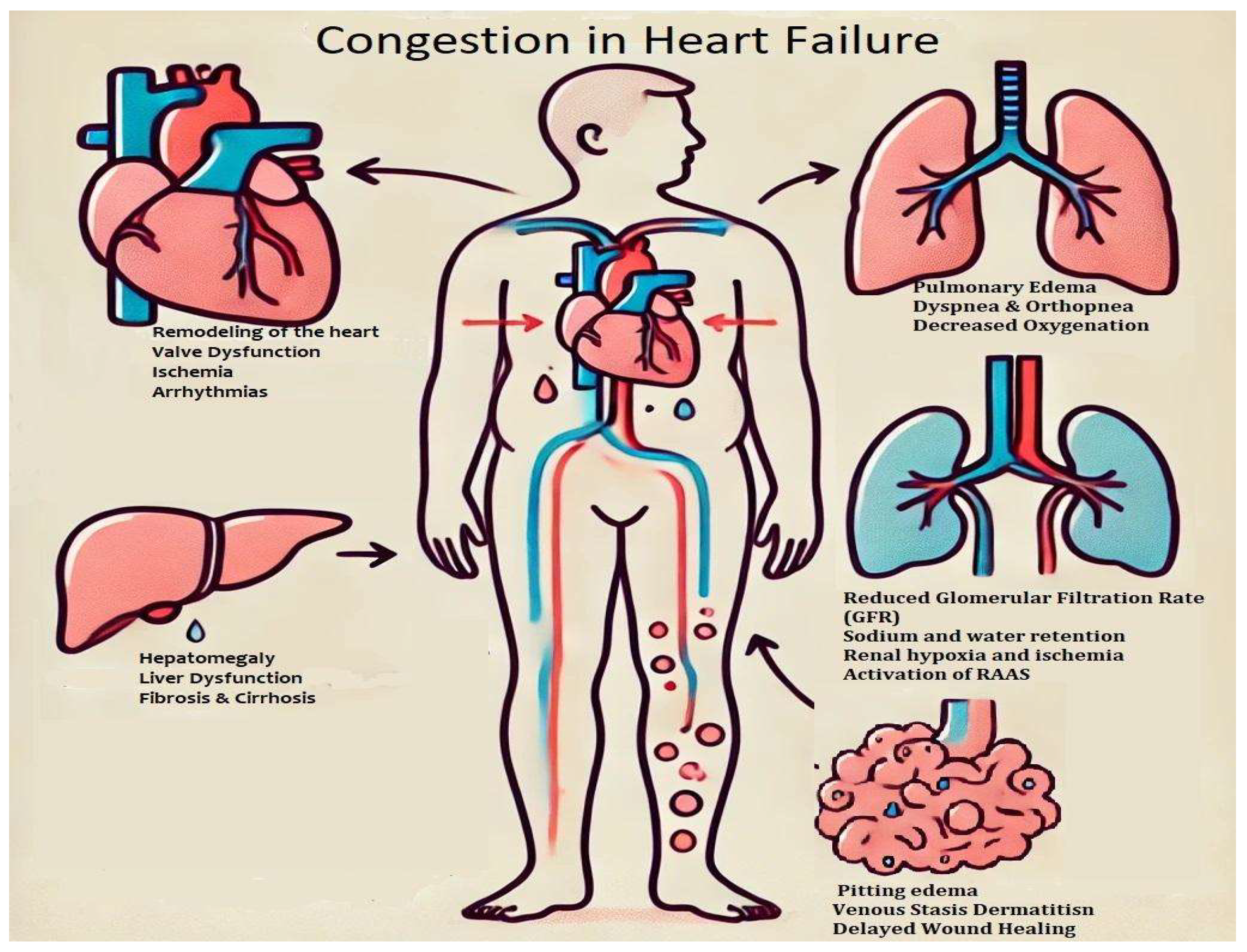
3. Congestion and Organ Response
Congestive heart failure is considered a systemic condition, affecting not only the heart but also contributing to renal dysfunction due to reduced perfusion pressure, sodium retention, and subsequent subendocardial ischemia, which leads to left ventricular remodeling [23]. Additionally, it can cause cholestatic liver injury, anemia, muscle damage due to metabolic disturbances, and various other complications [24].
Figure 2.
Congestion in heart failure. This schematic illustration depicts venous congestion in heart failure and its systemic consequences.
Figure 2.
Congestion in heart failure. This schematic illustration depicts venous congestion in heart failure and its systemic consequences.
3.1. Effects of Congestion on the Heart
3.1.1. Congestion and Heart Remodeling
As venous congestion increases in heart failure (HF), the heart faces higher preload, leading to greater ventricular wall stress. Initially, the heart compensates by stretching its chambers and thickening its walls to maintain output [13,15,25,26]. Natriuretic peptides are released to help manage the overload, but this relief is temporary. Over time, what starts as an adaptation turns into a pathway toward heart failure [19].
The left ventricle undergoes significant changes, enlarging and becoming more spherical, a sign of worsening HF. These changes are part of various patterns of left ventricular (LV) remodeling, including concentric and eccentric hypertrophy, which often precede dysfunction and dilation. As remodeling progresses, myocytes hypertrophy, but persistent congestion leads to myocardial apoptosis, fibrosis, and loss of contractility, worsening LV dysfunction [19,27].
In a four-year study by Wolfgang Lieb, similar remodeling patterns were observed in patients with obesity and hypertension [28]. Ciampi and Villari classified heart failure into several phenotypes, including:
- The Weak Heart: Systolic dysfunction with LV dilation and reduced ejection fraction (HFrEF).
- The Big Heart: Remodeling from hypertension or cardiomyopathies with LV dilation and mitral regurgitation.
- The Noisy Heart: Mitral regurgitation due to LV distortion in dilated or ischemic cardiomyopathy.
- The Stiff Heart: Diastolic dysfunction with elevated filling pressures.
- The Wet Heart: Pulmonary congestion and edema, visible on imaging [29].
3.1.2. Valves Disfunction
As the heart chambers enlarge, the mitral and tricuspid valves struggle to function properly. Geometric distortion from remodeling prevents proper valve coaptation, causing functional mitral and tricuspid regurgitation. This allows blood to flow backward, worsening congestion and creating a cycle of volume overload [15]. What started as minor distortion leads to significant valvular insufficiency, making it harder for the heart to generate forward flow and exacerbating pulmonary and systemic congestion [30].
3.1.3. Ischemia and Arrhythmias
A congested heart is oxygen-starved, as rising ventricular pressures compress the coronary microcirculation, limiting oxygen delivery to the myocardium. This causes subendocardial ischemia, leading to fibrosis, scarring, and impaired contractility [19]. Congestion also disrupts electrical stability, with ischemia and fibrosis increasing the risk of arrhythmias, especially atrial fibrillation (AF). The dilated left atrium increases AF risk, reducing atrial contraction and worsening congestion. Elevated ventricular rates worsen left ventricular function, creating a cycle of heart failure and arrhythmia. Arrhythmias are common in HF, with 20-80% of patients experiencing non-sustained ventricular tachycardia (VT), which can lead to palpitations, syncope, or sudden cardiac death [19].
3.1.4. The Right Ventricle Dysfunction
While left heart failure receives much attention, the right ventricle (RV) often fails quietly [31]. Pulmonary congestion increases pulmonary artery pressures, placing an afterload burden on the thin-walled RV. Initially, the RV compensates with hypertrophy, but as congestion worsens, it dilates, weakens, and ultimately fails [15,32]. Right-sided heart failure causes systemic venous congestion, leading to hepatic congestion, ascites, and worsening peripheral edema, spreading the effects of congestion to multiple organ systems [19,33]
3.1.5. The Need for Early Intervention and Treatment
Congestion fuels the progression of heart failure, accelerating cardiac remodeling, dilation, and ischemia. Recognizing it early is crucial to breaking the cycle. Echocardiographic markers and advanced techniques like speckle-tracking can identify early dysfunction before symptoms worsen [13,34]. However, imaging alone isn’t enough. Proactive treatment with decongestive therapy, volume control, and neurohormonal blockade is essential to preserve heart function and prevent further damage [15].
3.2. Effects of Congestion in the Lungs
Pulmonary congestion in heart failure (HF) results from elevated left atrial pressure, leading to fluid leakage into the interstitial and alveolar spaces. This disrupts gas exchange, causing dyspnea and respiratory symptoms [13,15,35].
Increased left ventricular filling pressures heighten pulmonary capillary permeability, exacerbated by mitral regurgitation, leading to alveolar edema and pleural effusion when lymphatic drainage is overwhelmed [15,36]. Persistent congestion disrupts Starling forces, contributing to cardiopulmonary remodeling, endothelial dysfunction, and fibrosis, impairing alveolar diffusion and promoting pulmonary vasoconstriction [37,38]. Over time, these changes result in pulmonary hypertension and restrictive lung dysfunction, further worsening respiratory capacity and HF progression.
Beyond fluid accumulation and impaired gas exchange, pulmonary congestion in heart failure (HF) leads to further complications that accelerate disease progression.
- Respiratory Complication: Pulmonary congestion reduces lung compliance, increasing breathing effort and causing hypoxemia and respiratory distress [39]. Impaired mucociliary clearance heightens pneumonia risk, while ventilation-perfusion mismatch worsens oxygen exchange, triggering compensatory mechanisms such as increased respiratory rate and sympathetic activation [26,40,41]. Many HF patients also experience sleep-disordered breathing, including Cheyne-Stokes respiration and central sleep apnea, contributing to nocturnal hypoxia, fatigue, and cognitive decline [39].
- Right Heart Strain and Pulmonary Hypertension: Persistent pulmonary congestion raises pulmonary vascular resistance, increasing right ventricular workload and leading to hypertrophy and eventual right-sided heart failure. In severe cases, pulmonary hypertension develops, further impairing gas exchange and reducing exercise tolerance [37,38,42].
3.2.4. Diagnostic and Therapeutic Approaches
Pulmonary congestion is identified through imaging techniques such as chest X-rays (detecting pulmonary edema and Kerley B lines), lung ultrasound (revealing B-lines), and echocardiography (assessing left atrial and pulmonary artery pressures) [15,42]. Persistent congestion increases morbidity and mortality, necessitating early intervention.
3.3. Interdependence Between Renal Function and Heart Failure
3.3.1. Kidney and Congestion
The interplay between the heart and kidneys is fundamental to fluid balance and circulatory homeostasis. Any dysfunction in one organ inevitably influences the other, forming a pathophysiological cycle that exacerbates cardiorenal syndrome. Heart failure frequently coexists with chronic kidney disease (CKD), with nearly 49% of HF patients exhibiting some degree of renal impairment [44,45]. Persistent congestion in this setting contributes to diuretic resistance, electrolyte imbalances, hypotension, and systemic inflammation, all of which worsen outcomes [46,47,48].
Renal congestion in heart failure is a multifaceted problem. Primary kidney disease, such as glomerulonephritis or diabetic nephropathy, reduces the glomerular filtration rate (GFR), impairing the excretion of sodium and water. In response, the RAAS is activated, leading to sodium retention, volume overload, and hypertension. Proteinuria, common in CKD, further lowers oncotic pressure, allowing fluid to shift into the interstitial space, worsening edema and congestion [23]. On the other hand, chronic heart failure (CHF) leads to progressive renal dysfunction due to declining cardiac output and rising central venous pressure (CVP). Increased renal venous congestion diminishes glomerular perfusion, disrupting the pressure gradient between afferent and efferent arterioles. This results in impaired sodium handling, water retention, and worsening congestion, setting off a vicious cycle of progressive kidney and heart dysfunction [49,50].
The decline in GFR is a well-established marker of poor prognosis in HF [52]. Left ventricular dysfunction impairs renal perfusion, activating RAAS and the SNS, further vasoconstricting afferent arterioles, and reducing GFR [53,54,55]. Right ventricular failure, in contrast, leads to elevated CVP, increasing renal interstitial pressure and causing tubular compression, which exacerbates sodium and water retention, ultimately worsening systemic congestion [51].
Chronic renal congestion in heart failure (HF) contributes to acute kidney injury (AKI) due to medullary hypoxia and tubular necrosis, often worsened by aggressive diuresis or hypotension [26]. Persistent venous hypertension promotes inflammation, fibrosis, and oxidative stress, leading to renal dysfunction [52,56]. Impaired clearance increases drug toxicity risks, while electrolyte imbalances and systemic inflammation accelerate endothelial dysfunction and myocardial remodeling [57]. Reduced erythropoietin (EPO) production leads to anemia, exacerbating fatigue, hypoxia, and cardiac strain, further worsening HF outcomes [24,57]. All these effects of chronic congestion are summarized in Table 2.
3.3.2. Assessing and Managing Renal Congestion in Heart Failure
Renal congestion assessment requires hemodynamic and imaging techniques. While CVP monitoring is useful, it may not accurately reflect intrarenal congestion. Intrarenal Doppler ultrasonography, particularly intrarenal venous flow (IRVF) analysis, correlates with right atrial pressure and predicts prognosis. Abnormal IRVF patterns are linked to higher 1-year mortality in HF patients. Contrast-enhanced ultrasonography (CEUS) offers direct visualization of renal microvascular perfusion, with studies showing improved renal outcomes following decongestive therapy [58,59].
3.4. Effects of Congestion on the Digestive System
3.4.2. Liver and Congestion
One of the most prominent consequences of congestion is hepatic involvement, commonly referred to as congestive hepatopathy. The liver becomes engorged due to elevated central venous pressure, which is transmitted to the sinusoidal capillaries. Because the hepatic venous system lacks valves, venous pressure is directly transmitted, causing sinusoidal congestion, peri-sinusoidal edema, and hepatocyte hypoxia. This process reduces oxygen diffusion to hepatocytes, impairing liver metabolism and detoxification functions [60,61,62]. Laboratory markers often show elevated alkaline phosphatase, bilirubin, and γ-glutamyltransferase (GGT) due to cholestasis and hepatocyte stress. Over time, chronic congestion may result in fibrosis and progression to cardiac cirrhosis. Although liver dysfunction in HF is often asymptomatic, routine biochemical testing frequently reveals elevations in right atrial pressure, severe tricuspid regurgitation, and serum natriuretic peptides, all of which correlate with worsening hepatic congestion.
Chronic passive congestion may also impair hepatic synthetic function, leading to prolonged prothrombin time and hypoalbuminemia, further contributing to edema formation [63].
3.4.3. Intestinal and Congestion
In heart failure (HF), intestinal function is significantly impacted by splanchnic venous congestion, low cardiac output, and ischemia, leading to symptoms like nausea, bloating, and anorexia, often worsened by HF medications [64,65]. Impaired circulation causes malabsorption, exacerbating malnutrition and weight loss. Additionally, changes in gut microbiota play a critical role in HF progression. Weakened intestinal barriers allow bacteria and endotoxins to enter the bloodstream, triggering systemic inflammation and worsening cardiac and renal function [54,66]. This "leaky gut" effect, along with microbial dysbiosis, contributes to increased inflammation and metabolic dysfunction, accelerating HF and cachexia development [61,67]. The malabsorption of key nutrients worsens weight loss and instability, and cardiac cachexia, marked by muscle wasting and metabolic decline, remains a strong predictor of poor outcomes in HF [60,67].
These interconnected issues highlight the need for targeted interventions to manage both gastrointestinal and systemic complications in HF patients.
3.4.4. Assessment and Management of Digestive Congestion in HF
Gastrointestinal involvement in heart failure (HF) is often overlooked. While liver dysfunction can be assessed through hepatic enzyme tests and imaging, intestinal impairment remains challenging to evaluate [60,68,69].
Treatment focuses on relieving congestion while preserving gut and liver function. Diuretics aid in managing hepatic and splanchnic congestion, though excessive use may worsen ischemia and malabsorption [68]. Nutritional strategies, including micronutrient supplementation and gut microbiome modulation, are essential for preventing cachexia. Probiotics and prebiotics are emerging as potential therapies to restore microbial balance and reduce inflammation [69].
3.5. Effects of Congestion in Heart Failure on the Neurovascular System
Congestion in heart failure (HF) significantly impacts the neurovascular system, affecting both central and peripheral circulation. The interplay of elevated venous pressure, endothelial dysfunction, cerebral hypoperfusion, and autonomic dysregulation contributes to neurological decline and vascular complications, worsening disease severity [70,71].
Reduced cerebral perfusion due to impaired cardiac output disrupts blood flow regulation, increasing the risk of cognitive impairment, white matter lesions, and stroke. Chronic hypoxia and neuroinflammation further accelerate neurodegeneration, leading to deficits in memory, executive function, and processing speed, resembling vascular dementia [72]. Advanced HF and atrial fibrillation further elevate stroke risk [71,72].
HF-associated autonomic imbalance enhances sympathetic activity while weakening parasympathetic control, resulting in baroreflex impairment, vascular resistance elevation, and unstable blood pressure regulation. Increased angiotensin II and norepinephrine levels exacerbate vasoconstriction, hypertension, and endothelial dysfunction, contributing to arrhythmias and sudden cardiac death [16,73,74].
Congestion also affects peripheral circulation, leading to endothelial dysfunction, vascular stiffness, and reduced blood flow, causing symptoms like claudication, fatigue, and neuropathy [75]. Retinal microvascular changes, including venous dilation and hypertensive retinopathy, serve as markers of systemic vascular damage and HF severity [72,76].
Managing neurovascular dysfunction in HF requires optimizing cardiac output, reducing congestion, and correcting neurohormonal imbalances. Beta-blockers, ACE inhibitors, and aldosterone antagonists help regulate sympathetic overactivity and improve vascular function. Routine cognitive assessments, neuroimaging, and autonomic function testing enable early detection and intervention [13,71].
3.6. Anemia as a Consequence of Congestion in Heart Failure
Anemia is a common complication of chronic congestion in heart failure (HF), with prevalence increasing as HF severity progresses [77,78]. The underlying mechanisms involve hemodilution, renal dysfunction, hepatic impairment, systemic inflammation, and malabsorption, all of which contribute to worsening anemia [79].
Hemodilution due to fluid retention reduces hemoglobin concentration, particularly in advanced HF, affecting up to 50-60% of patients. Hepatic congestion elevates hepcidin levels, restricting iron release and absorption, while inflammatory cytokines suppress erythropoietin (EPO) production, further impairing erythropoiesis [80]. Congestion-induced renal hypoxia exacerbates anemia, particularly in patients with coexisting chronic kidney disease (CKD), which leads to decreased EPO synthesis and increased hepcidin levels [81]. Gastrointestinal congestion and inflammation further hinder iron absorption, compounding iron deficiency and anemia in HF patients [82].
Anemia significantly worsens HF by increasing myocardial hypoxia, left ventricular hypertrophy, and myocardial fibrosis. Additionally, anemia-induced neurohormonal activation (SNS and RAAS) contributes to vasodilation, fluid retention, and renal dysfunction, accelerating HF and CKD progression [82]. In cardiac cachexia, nutritional deficiencies further exacerbate anemia, creating a cycle of worsening HF symptoms [80].
3.7. Musculoskeletal System and Skeletal Muscle Dysfunction
Chronic congestion in heart failure (HF) leads to muscle atrophy, weakness, and reduced endurance due to impaired circulation, which limits oxygen and nutrient supply to muscles, causing mitochondrial dysfunction and oxidative stress [84,85]. Sarcopenia, muscle loss, and strength reduction result from poor perfusion, inflammation, and hormonal imbalances, worsening mobility [86]. Autonomic dysfunction and reduced cardiac output further disrupt stability, increasing fall and fracture risk, especially in older adults [87]. Cardiac cachexia, driven by inflammation, hormonal dysregulation, and poor nutrition, accelerates muscle breakdown, decreases exercise tolerance, and causes fatigue. Fluid retention worsens discomfort, while muscle hypoxia and metabolic dysfunction reduce energy utilization, further impairing function. This cycle of inflammation and physical decline highlights the need for targeted interventions to address musculoskeletal complications in HF patients.
3.8. Endocrine System and Metabolic Dysregulation
Heart failure (HF) is associated with significant endocrine disturbances, including insulin resistance, thyroid dysfunction, and adrenal insufficiency. Chronic inflammation and hepatic impairment contribute to insulin resistance, increasing the risk of type 2 diabetes mellitus and worsening cardiovascular complications [88,89].
Thyroid dysfunction, particularly low T3 syndrome, is prevalent in HF due to impaired T4-to-T3 conversion, resulting in reduced cardiac output and exercise intolerance, further exacerbating disease progression [88]. Additionally, severe congestion may impair adrenal perfusion, leading to dysregulated cortisol and aldosterone secretion, which contributes to fluid retention, electrolyte imbalances, and hemodynamic instability [90].
Dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis leads to elevated cortisol levels, promoting insulin resistance and metabolic dysfunction, which negatively impact HF prognosis [91]. Furthermore, activation of the renin-angiotensin-aldosterone system (RAAS) increases aldosterone secretion, exacerbating sodium retention and fluid overload, thereby worsening HF symptoms [92].
Sex hormone imbalances, particularly low testosterone levels in men, have been linked to muscle wasting, reduced exercise capacity, and increased morbidity and mortality in HF patients [93,94]. Additionally, HF-related metabolic dysregulation results in reduced insulin sensitivity and impaired glucose tolerance, resembling a starvation state that promotes cachexia and muscle wasting, further accelerating disease progression [91].
3.9. Immune System and Chronic Inflammation
Congestion in heart failure (HF) weakens the immune system, increasing vulnerability to infections, sepsis, and delayed wound healing. Persistent venous congestion and tissue hypoxia raise pro-inflammatory cytokines like TNF-α, IL-6, and CRP, leading to endothelial dysfunction, muscle wasting, and cardiac remodeling [18,84,95,96,97,98]. These cytokines are released by immune cells such as macrophages and T lymphocytes in response to congestion and injury, while Angiotensin-converting enzyme inhibitors reduce IL-6 levels and improve HF outcomes [98,99,100]. The renin-angiotensin-aldosterone system (RAAS) worsens inflammation and metabolic disturbances, including insulin resistance, promoting cachexia, worsening H F, and complicating disease management [101,102].
3.10. Skin and Peripheral Edema
Congestion and capillary leakage in heart failure (HF) lead to chronic skin changes like venous stasis dermatitis, tissue edema, and ulcers [13,36]. Elevated hydrostatic pressure causes skin discoloration and thickening and increases infection risk, while impaired microvascular perfusion hinders wound healing, making patients prone to pressure ulcers [67,103]. Peripheral edema, common in HF, swells the lower extremities, weakening skin integrity and increasing the risk of cellulitis and other dermatological issues [17,104]. The skin may also show pallor or cyanosis from poor perfusion and become cool and clammy as the body compensates for reduced cardiac output [105].
3.10. Hepatosplenic and Lymphatic System Dysfunction
Chronic venous congestion affects both the spleen and lymphatic system, leading to splenomegaly and hematologic abnormalities. Spleen dysfunction disrupts platelet sequestration, increasing the risk of bleeding disorders and pancytopenia [106]. Additionally, congestion impairs lymphatic drainage, contributing to fluid retention and exacerbating peripheral edema [107]. The accumulation of stagnant lymphatic fluid promotes immune cell and cytokine buildup in interstitial spaces, intensifying the inflammatory response [107].
Lymphatic congestion further disrupts interstitial fluid drainage, leading to widespread edema, ascites, and persistent volume overload. The complex interaction between lymphatic dysfunction, venous congestion, and inflammation exacerbates systemic congestion, accelerating HF progression [108].
4. Conclusion
Congestion in heart failure (HF) extends far beyond a simple hemodynamic disturbance, representing a complex, multisystem pathology that impacts nearly every organ system. The pathophysiological interactions between renal dysfunction, hepatic congestion, intestinal permeability, immune dysregulation, and musculoskeletal deterioration highlight the extensive and deleterious effects of congestion in HF. These systemic consequences contribute to a progressive worsening of the disease, increasing morbidity, exacerbating functional impairment, and significantly reducing patient quality of life [25,36].
Renal congestion in HF diminishes renal perfusion and impairs sodium and water handling, further exacerbating fluid retention. Hepatic congestion contributes to a cascade of metabolic dysfunction, including reduced detoxification and compromised protein synthesis. Impaired intestinal integrity, coupled with congestion-induced ischemia, promotes inflammation and nutrient malabsorption, further undermining nutritional status and systemic homeostasis. Concurrently, musculoskeletal atrophy, driven by prolonged fluid retention and inflammation, contributes to cachexia, muscle wasting, and frailty. Collectively, these organ-specific disruptions perpetuate the cycle of congestion, exacerbating both the cardiac and systemic manifestations of heart failure [23,49,50].
The multifaceted nature of congestion in HF underscores its critical role in disease progression. It is not solely the heart that suffers but rather the entire body, as the effects of congestion propagate across organ systems. Acknowledging and understanding the systemic repercussions of congestion is essential to developing more effective therapeutic strategies and improving patient outcomes in heart failure management [2,15,84].
Author Contributions
D.M., F.C.R., and R.I.L. took the lead in writing the manuscript and planning its conception. I.G., R.S. and M.P. provided support and advice regarding the design of the manuscript. D.M. and F.C.R. wrote the manuscript. All authors contributed to editorial changes in the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of open access journals |
| HF | Heart failure |
References
- Gheorghiade, M.; Vaduganathan, M.; Fonarow, G.C.; Bonow, R.O. Rehospitalization for Heart Failure. J. Am. Coll. Cardiol. 2013, 61, 391–403. [Google Scholar] [CrossRef]
- Ambrosy, A.P.; Fonarow, G.C.; Butler, J.; Chioncel, O.; Greene, S.J.; Vaduganathan, M.; Nodari, S.; Lam, C.S.P.; Sato, N.; Shah, A.N.; Gheorghiade, M. The Global Health and Economic Burden of Hospitalizations for Heart Failure. J. Am. Coll. Cardiol. 2014, 63, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Hummel, A.; Empen, K.; Dörr, M.; Felix, S.B. De Novo Acute Heart Failure and Acutely Decompensated Chronic Heart Failure. Dtsch. Ärztebl. Int. 2015. [Google Scholar] [CrossRef] [PubMed]
- Mosterd, A.; Hoes, A.W. Clinical Epidemiology of Heart Failure. Heart 2007, 93, 1137–1146. [Google Scholar] [CrossRef] [PubMed]
- Rogler, G.; Rosano, G. The Heart and the Gut. Eur. Heart J. 2014, 35, 426–430. [Google Scholar] [CrossRef]
- Bozkurt, B.; Coats, A.J.; Tsutsui, H.; Abdelhamid, M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Böhm, M.; Butler, J.; Drazner, M.H.; Felker, G.M.; Filippatos, G.; Fonarow, G.C.; Fiuzat, M.; Gomez-Mesa, J.; Heidenreich, P.; Imamura, T.; Januzzi, J.; Jankowska, E.A.; Khazanie, P.; Kinugawa, K.; Lam, C.S.P.; Matsue, Y.; Metra, M.; Ohtani, T.; Francesco Piepoli, M.; Ponikowski, P.; Rosano, G.M.C.; Sakata, Y.; SeferoviĆ, P.; Starling, R.C.; Teerlink, J.R.; Vardeny, O.; Yamamoto, K.; Yancy, C.; Zhang, J.; Zieroth, S. Universal Definition and Classification of Heart Failure. J. Card. Fail. 2021, 27, 387–413. [Google Scholar] [CrossRef]
- Nieminen, M.S.; Brutsaert, D.; Dickstein, K.; Drexler, H.; Follath, F.; Harjola, V.-P.; Hochadel, M.; Komajda, M.; Lassus, J.; Lopez-Sendon, J.L.; Ponikowski, P.; Tavazzi, L.; on behalf of the EuroHeart Survey Investigators. EuroHeart Failure Survey II (EHFS II): A Survey on Hospitalized Acute Heart Failure Patients: Description of Population. Eur. Heart J. 2006, 27, 2725–2736. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; Jessup, M.; Linde, C.; Nihoyannopoulos, P.; Parissis, J.T.; Pieske, B.; Riley, J.P.; Rosano, G.M.C.; Ruilope, L.M.; Ruschitzka, F.; Rutten, F.H.; Van Der Meer, P. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC)Developed with the Special Contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Harjola, V.; Follath, F.; Nieminen, M.S.; Brutsaert, D.; Dickstein, K.; Drexler, H.; Hochadel, M.; Komajda, M.; Lopez-Sendon, J.L.; Ponikowski, P.; Tavazzi, L. Characteristics, Outcomes, and Predictors of Mortality at 3 Months and 1 Year in Patients Hospitalized for Acute Heart Failure. Eur. J. Heart Fail. 2010, 12, 239–248. [Google Scholar] [CrossRef]
- Ammar, K.A.; Jacobsen, S.J.; Mahoney, D.W.; Kors, J.A.; Redfield, M.M.; Burnett, J.C.; Rodeheffer, R.J. Prevalence and Prognostic Significance of Heart Failure Stages: Application of the American College of Cardiology/American Heart Association Heart Failure Staging Criteria in the Community. Circulation 2007, 115, 1563–1570. [Google Scholar] [CrossRef]
- Lam, C.S.P.; Solomon, S.D. Classification of Heart Failure According to Ejection Fraction. J. Am. Coll. Cardiol. 2021, 77, 3217–3225. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; Fang, J.C.; Fedson, S.E.; Fonarow, G.C.; Hayek, S.S.; Hernandez, A.F.; Khazanie, P.; Kittleson, M.M.; Lee, C.S.; Link, M.S.; Milano, C.A.; Nnacheta, L.C.; Sandhu, A.T.; Stevenson, L.W.; Vardeny, O.; Vest, A.R.; Yancy, C.W. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145. [Google Scholar] [CrossRef] [PubMed]
- Martens, P.; Mullens, W. How to Tackle Congestion in Acute Heart Failure. Korean J. Intern. Med. 2018, 33, 462–473. [Google Scholar] [CrossRef] [PubMed]
- Christersson, M.; Gustafsson, S.; Lampa, E.; Almstedt, M.; Cars, T.; Bodegård, J.; Arefalk, G.; Sundström, J. Usefulness of Heart Failure Categories Based on Left Ventricular Ejection Fraction. J. Am. Heart Assoc. 2024, 13, e032257. [Google Scholar] [CrossRef] [PubMed]
- Mocan, D.; Lala, R.I.; Puschita, M.; Pilat, L.; Darabantiu, D.A.; Pop-Moldovan, A. The Congestion “Pandemic” in Acute Heart Failure Patients. Biomedicines 2024, 12, 951. [Google Scholar] [CrossRef]
- Fallick, C.; Sobotka, P.A.; Dunlap, M.E. Sympathetically Mediated Changes in Capacitance: Redistribution of the Venous Reservoir as a Cause of Decompensation. Circ. Heart Fail. 2011, 4, 669–675. [Google Scholar] [CrossRef]
- Fudim, M.; Hernandez, A.F.; Felker, G.M. Role of Volume Redistribution in the Congestion of Heart Failure. J. Am. Heart Assoc. 2017, 6, e006817. [Google Scholar] [CrossRef]
- Mullens, W.; Verbrugge, F.H.; Nijst, P.; Tang, W.H.W. Renal Sodium Avidity in Heart Failure: From Pathophysiology to Treatment Strategies. Eur. Heart J. 2017, 38, 1872–1882. [Google Scholar] [CrossRef]
- Kumric, M.; Kurir, T.T.; Bozic, J.; Slujo, A.B.; Glavas, D.; Miric, D.; Lozo, M.; Zanchi, J.; Borovac, J.A. Pathophysiology of Congestion in Heart Failure: A Contemporary Review. Card. Fail. Rev. 2024, 10, e13. [Google Scholar] [CrossRef]
- Cotter, G.; Metra, M.; Milo-Cotter, O.; Dittrich, H.C.; Gheorghiade, M. Fluid Overload in Acute Heart Failure — Re-distribution and Other Mechanisms beyond Fluid Accumulation. Eur. J. Heart Fail. 2008, 10, 165–169. [Google Scholar] [CrossRef]
- Miller, W.L. Fluid Volume Overload and Congestion in Heart Failure: Time to Reconsider Pathophysiology and How Volume Is Assessed. Circ. Heart Fail. 2016, 9. [Google Scholar] [CrossRef] [PubMed]
- Colombo, P.C.; Jorde, U.P. The Active Role of Venous Congestion in the Pathophysiology of Acute Decompensated Heart Failure. Rev. Esp. Cardiol. Engl. Ed. 2010, 63, 5–8. [Google Scholar] [CrossRef]
- Udani, S.M.; Koyner, J.L. The Effects of Heart Failure on Renal Function. Cardiol. Clin. 2010, 28, 453–465. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.-D.; Katz, S.D. Anemia in Chronic Heart Failure: Prevalence, Etiology, Clinical Correlates, and Treatment Options. Circulation 2006, 113, 2454–2461. [Google Scholar] [CrossRef]
- Dupont, M.; Mullens, W.; Tang, W.H.W. Impact of Systemic Venous Congestion in Heart Failure. Curr. Heart Fail. Rep. 2011, 8, 233–241. [Google Scholar] [CrossRef]
- Boorsma, E.M.; Ter Maaten, J.M.; Damman, K.; Dinh, W.; Gustafsson, F.; Goldsmith, S.; Burkhoff, D.; Zannad, F.; Udelson, J.E.; Voors, A.A. Congestion in Heart Failure: A Contemporary Look at Physiology, Diagnosis and Treatment. Nat. Rev. Cardiol. 2020, 17, 641–655. [Google Scholar] [CrossRef]
- Verma, A.; Meris, A.; Skali, H.; Ghali, J.K.; Arnold, J.M.O.; Bourgoun, M.; Velazquez, E.J.; McMurray, J.J.V.; Kober, L.; Pfeffer, M.A.; Califf, R.M.; Solomon, S.D. Prognostic Implications of Left Ventricular Mass and Geometry Following Myocardial Infarction. JACC Cardiovasc. Imaging 2008, 1, 582–591. [Google Scholar] [CrossRef]
- Lieb, W.; Gona, P.; Larson, M.G.; Aragam, J.; Zile, M.R.; Cheng, S.; Benjamin, E.J.; Vasan, R.S. The Natural History of Left Ventricular Geometry in the Community. JACC Cardiovasc. Imaging 2014, 7, 870–878. [Google Scholar] [CrossRef]
- Ciampi, Q.; Villari, B. Role of Echocardiography in Diagnosis and Risk Stratification in Heart Failure with Left Ventricular Systolic Dysfunction. Cardiovasc. Ultrasound 2007, 5, 34. [Google Scholar] [CrossRef]
- Cammalleri, V.; Antonelli, G.; De Luca, V.M.; Carpenito, M.; Nusca, A.; Bono, M.C.; Mega, S.; Ussia, G.P.; Grigioni, F. Functional Mitral and Tricuspid Regurgitation across the Whole Spectrum of Left Ventricular Ejection Fraction: Recognizing the Elephant in the Room of Heart Failure. J. Clin. Med. 2023, 12, 3316. [Google Scholar] [CrossRef]
- Dietz, M.F.; Prihadi, E.A.; Van Der Bijl, P.; Goedemans, L.; Mertens, B.J.A.; Gursoy, E.; Van Genderen, O.S.; Ajmone Marsan, N.; Delgado, V.; Bax, J.J. Prognostic Implications of Right Ventricular Remodeling and Function in Patients With Significant Secondary Tricuspid Regurgitation. Circulation 2019, 140, 836–845. [Google Scholar] [CrossRef] [PubMed]
- Ghio, S.; Guazzi, M.; Scardovi, A.B.; Klersy, C.; Clemenza, F.; Carluccio, E.; Temporelli, P.L.; Rossi, A.; Faggiano, P.; Traversi, E.; Vriz, O.; Dini, F.L.; on behalf of all investigators. Different Correlates but Similar Prognostic Implications for Right Ventricular Dysfunction in Heart Failure Patients with Reduced or Preserved Ejection Fraction. Eur. J. Heart Fail. 2017, 19, 873–879. [Google Scholar] [CrossRef]
- Kobayashi, M.; Gargani, L.; Palazzuoli, A.; Ambrosio, G.; Bayés-Genis, A.; Lupon, J.; Pellicori, P.; Pugliese, N.R.; Reddy, Y.N.V.; Ruocco, G.; Duarte, K.; Huttin, O.; Rossignol, P.; Coiro, S.; Girerd, N. Association between Right-Sided Cardiac Function and Ultrasound-Based Pulmonary Congestion on Acutely Decompensated Heart Failure: Findings from a Pooled Analysis of Four Cohort Studies. Clin. Res. Cardiol. 2021, 110, 1181–1192. [Google Scholar] [CrossRef] [PubMed]
- Marwick, T.H. The Role of Echocardiography in Heart Failure. J. Nucl. Med. 2015, 56 (Supplement 4), 31S–38S. [Google Scholar] [CrossRef] [PubMed]
- Fromm, R.E.; Varon, J.; Gibbs, L.R. Congestive Heart Failure and Pulmonary Edema for the Emergency Physician. J. Emerg. Med. 1995, 13, 71–87. [Google Scholar] [CrossRef]
- Girerd, N.; Seronde, M.-F.; Coiro, S.; Chouihed, T.; Bilbault, P.; Braun, F.; Kenizou, D.; Maillier, B.; Nazeyrollas, P.; Roul, G.; Fillieux, L.; Abraham, W.T.; Januzzi, J.; Sebbag, L.; Zannad, F.; Mebazaa, A.; Rossignol, P. Integrative Assessment of Congestion in Heart Failure Throughout the Patient Journey. JACC Heart Fail. 2018, 6, 273–285. [Google Scholar] [CrossRef]
- Pirrotta, F.; Mazza, B.; Gennari, L.; Palazzuoli, A. Pulmonary Congestion Assessment in Heart Failure: Traditional and New Tools. Diagnostics 2021, 11, 1306. [Google Scholar] [CrossRef]
- Rosenkranz, S.; Howard, L.S.; Gomberg-Maitland, M.; Hoeper, M.M. Systemic Consequences of Pulmonary Hypertension and Right-Sided Heart Failure. Circulation 2020, 141, 678–693. [Google Scholar] [CrossRef]
- Valika, A.; Advocate Medical Group – Midwest Heart Specialists, Advocate Heart Institute, Oak Brook, IL, USA; Costanzo, M.R.; Advocate Medical Group – Midwest Heart Specialists, Advocate Heart Institute, Oak Brook, IL, USA. Sleep-Disordered Breathing During Congestive Heart Failure: To Intervene or Not to Intervene? Card. Fail. Rev. 2017, 3, 134. [Google Scholar] [CrossRef]
- Waldman, S.; Pelner, L. The Relationship of Upper Respiratory Infections to Congestive Heart-Failure in Patients With Heart Disease. Postgrad. Med. 1956, 19, 451–458. [Google Scholar] [CrossRef]
- Melenovsky, V.; Andersen, M.J.; Andress, K.; Reddy, Y.N.; Borlaug, B.A. Lung Congestion in Chronic Heart Failure: Haemodynamic, Clinical, and Prognostic Implications. Eur. J. Heart Fail. 2015, 17, 1161–1171. [Google Scholar] [CrossRef] [PubMed]
- Berthelot, E.; Bauer, F.; Eicher, J.; Flécher, E.; Gellen, B.; Guihaire, J.; Guijarro, D.; Roul, G.; Salvat, M.; Tribouilloy, C.; Zores, F.; Lamblin, N.; De Groote, P.; Damy, T. Pulmonary Hypertension in Chronic Heart Failure: Definitions, Advances, and Unanswered Issues. ESC Heart Fail. 2018, 5, 755–763. [Google Scholar] [CrossRef]
- Kobayashi, M.; Bercker, M.; Huttin, O.; Pierre, S.; Sadoul, N.; Bozec, E.; Chouihed, T.; Ferreira, J.P.; Zannad, F.; Rossignol, P.; Girerd, N. Chest X-Ray Quantification of Admission Lung Congestion as a Prognostic Factor in Patients Admitted for Worsening Heart Failure from the ICALOR Cohort Study. Int. J. Cardiol. 2020, 299, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.; Brito, D.; Vaqar, S.; Chhabra, L.; Doerr, C. Congestive Heart Failure (Nursing). In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar] [PubMed]
- Damman, K.; Valente, M.A.E.; Voors, A.A.; O’Connor, C.M.; Van Veldhuisen, D.J.; Hillege, H.L. Renal Impairment, Worsening Renal Function, and Outcome in Patients with Heart Failure: An Updated Meta-Analysis. Eur. Heart J. 2014, 35, 455–469. [Google Scholar] [CrossRef]
- Pugliese, N.R.; Fabiani, I.; Conte, L.; Nesti, L.; Masi, S.; Natali, A.; Colombo, P.C.; Pedrinelli, R.; Dini, F.L. Persistent Congestion, Renal Dysfunction and Inflammatory Cytokines in Acute Heart Failure: A Prognosis Study. J. Cardiovasc. Med. 2020, 21, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Rossignol, P.; Coats, A.J.; Chioncel, O.; Spoletini, I.; Rosano, G. Renal Function, Electrolytes, and Congestion Monitoring in Heart Failure. Eur. Heart J. Suppl. 2019, 21 (Supplement_M), M25–M31. [Google Scholar] [CrossRef]
- Rubio-Gracia, J.; Demissei, B.G.; Ter Maaten, J.M.; Cleland, J.G.; O’Connor, C.M.; Metra, M.; Ponikowski, P.; Teerlink, J.R.; Cotter, G.; Davison, B.A.; Givertz, M.M.; Bloomfield, D.M.; Dittrich, H.; Damman, K.; Pérez-Calvo, J.I.; Voors, A.A. Prevalence, Predictors and Clinical Outcome of Residual Congestion in Acute Decompensated Heart Failure. Int. J. Cardiol. 2018, 258, 185–191. [Google Scholar] [CrossRef]
- Clark, A.L.; Kalra, P.R.; Petrie, M.C.; Mark, P.B.; Tomlinson, L.A.; Tomson, C.R. Change in Renal Function Associated with Drug Treatment in Heart Failure: National Guidance. Heart 2019, 105, 904–910. [Google Scholar] [CrossRef]
- Al-Naher, A.; Wright, D.; Devonald, M.A.J.; Pirmohamed, M. Renal Function Monitoring in Heart Failure – What Is the Optimal Frequency? A Narrative Review. Br. J. Clin. Pharmacol. 2018, 84, 5–17. [Google Scholar] [CrossRef]
- Hillege, H.L.; Nitsch, D.; Pfeffer, M.A.; Swedberg, K.; McMurray, J.J.V.; Yusuf, S.; Granger, C.B.; Michelson, E.L.; Östergren, J.; Cornel, J.H.; De Zeeuw, D.; Pocock, S.; Van Veldhuisen, D.J. Renal Function as a Predictor of Outcome in a Broad Spectrum of Patients With Heart Failure. Circulation 2006, 113, 671–678. [Google Scholar] [CrossRef]
- Szlagor, M.; Dybiec, J.; Młynarska, E.; Rysz, J.; Franczyk, B. Chronic Kidney Disease as a Comorbidity in Heart Failure. Int. J. Mol. Sci. 2023, 24, 2988. [Google Scholar] [CrossRef]
- Blankstein, R.; Bakris, G.L. Renal Hemodynamic Changes in Heart Failure. Heart Fail. Clin. 2008, 4, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Afsar, B.; Ortiz, A.; Covic, A.; Solak, Y.; Goldsmith, D.; Kanbay, M. Focus on Renal Congestion in Heart Failure. Clin. Kidney J. 2016, 9, 39–47. [Google Scholar] [CrossRef]
- Aronson, D. The Interstitial Compartment as a Therapeutic Target in Heart Failure. Front. Cardiovasc. Med. 2022, 9, 933384. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, D.; Ali, M.A.; Wang, A.Y.-M.; Jha, V. Acute Kidney Injury in Acute Heart Failure–When to Worry and When Not to Worry? Nephrol. Dial. Transplant. 2024, 40, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Rangaswami, J.; Bhalla, V.; Blair, J.E.A.; Chang, T.I.; Costa, S.; Lentine, K.L.; Lerma, E.V.; Mezue, K.; Molitch, M.; Mullens, W.; Ronco, C.; Tang, W.H.W.; McCullough, P.A.; on behalf of the American Heart Association Council on the Kidney in Cardiovascular Disease and Council on Clinical Cardiology. Cardiorenal Syndrome: Classification, Pathophysiology, Diagnosis, and Treatment Strategies: A Scientific Statement From the American Heart Association. Circulation 2019, 139. [Google Scholar] [CrossRef]
- Pellicori, P.; Kallvikbacka-Bennett, A.; Dierckx, R.; Zhang, J.; Putzu, P.; Cuthbert, J.; Boyalla, V.; Shoaib, A.; Clark, A.L.; Cleland, J.G.F. Prognostic Significance of Ultrasound-Assessed Jugular Vein Distensibility in Heart Failure. Heart 2015, 101, 1149–1158. [Google Scholar] [CrossRef]
- Nijst, P.; Verbrugge, F.H.; Grieten, L.; Dupont, M.; Steels, P.; Tang, W.H.W.; Mullens, W. The Pathophysiological Role of Interstitial Sodium in Heart Failure. J. Am. Coll. Cardiol. 2015, 65, 378–388. [Google Scholar] [CrossRef]
- Sundaram, V.; Fang, J.C. Gastrointestinal and Liver Issues in Heart Failure. Circulation 2016, 133, 1696–1703. [Google Scholar] [CrossRef]
- Møller, S.; Bernardi, M. Interactions of the Heart and the Liver. Eur. Heart J. 2013, 34, 2804–2811. [Google Scholar] [CrossRef]
- Auer, J. What Does the Liver Tell Us about the Failing Heart? Eur. Heart J. 2013, 34, 711–714. [Google Scholar] [CrossRef] [PubMed]
- Van Deursen, V.M.; Damman, K.; Hillege, H.L.; Van Beek, A.P.; Van Veldhuisen, D.J.; Voors, A.A. Abnormal Liver Function in Relation to Hemodynamic Profile in Heart Failure Patients. J. Card. Fail. 2010, 16, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Harjola, V.; Mullens, W.; Banaszewski, M.; Bauersachs, J.; Brunner-La Rocca, H.; Chioncel, O.; Collins, S.P.; Doehner, W.; Filippatos, G.S.; Flammer, A.J.; Fuhrmann, V.; Lainscak, M.; Lassus, J.; Legrand, M.; Masip, J.; Mueller, C.; Papp, Z.; Parissis, J.; Platz, E.; Rudiger, A.; Ruschitzka, F.; Schäfer, A.; Seferovic, P.M.; Skouri, H.; Yilmaz, M.B.; Mebazaa, A. Organ Dysfunction, Injury and Failure in Acute Heart Failure: From Pathophysiology to Diagnosis and Management. A Review on Behalf of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2017, 19, 821–836. [Google Scholar] [CrossRef]
- Myers, R.P.; Cerini, R.; Sayegh, R.; Moreau, R.; Degott, C.; Lebrec, D.; Lee, S.S. Cardiac Hepatopathy: Clinical, Hemodynamic, and Histologic Characteristics and Correlations. Hepatology 2003, 37, 393–400. [Google Scholar] [CrossRef]
- Krack, A.; Sharma, R.; Figulla, H.R.; Anker, S.D. The Importance of the Gastrointestinal System in the Pathogenesis of Heart Failure. Eur. Heart J. 2005, 26, 2368–2374. [Google Scholar] [CrossRef]
- Sandek, A.; Bauditz, J.; Swidsinski, A.; Buhner, S.; Weber-Eibel, J.; Von Haehling, S.; Schroedl, W.; Karhausen, T.; Doehner, W.; Rauchhaus, M.; Poole-Wilson, P.; Volk, H.-D.; Lochs, H.; Anker, S.D. Altered Intestinal Function in Patients With Chronic Heart Failure. J. Am. Coll. Cardiol. 2007, 50, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- Gallo, A.; Macerola, N.; Favuzzi, A.M.; Nicolazzi, M.A.; Gasbarrini, A.; Montalto, M. The Gut in Heart Failure: Current Knowledge and Novel Frontiers. Med. Princ. Pract. 2022, 31, 203–214. [Google Scholar] [CrossRef]
- Aspromonte, N.; Fumarulo, I.; Petrucci, L.; Biferali, B.; Liguori, A.; Gasbarrini, A.; Massetti, M.; Miele, L. The Liver in Heart Failure: From Biomarkers to Clinical Risk. Int. J. Mol. Sci. 2023, 24, 15665. [Google Scholar] [CrossRef]
- Rajeev, V.; Chai, Y.L.; Poh, L.; Selvaraji, S.; Fann, D.Y.; Jo, D.-G.; De Silva, T.M.; Drummond, G.R.; Sobey, C.G.; Arumugam, T.V.; Chen, C.P.; Lai, M.K.P. Chronic Cerebral Hypoperfusion: A Critical Feature in Unravelling the Etiology of Vascular Cognitive Impairment. Acta Neuropathol. Commun. 2023, 11, 93. [Google Scholar] [CrossRef]
- Goyal, P.; Didomenico, R.J.; Pressler, S.J.; Ibeh, C.; White-Williams, C.; Allen, L.A.; Gorodeski, E.Z.; Albert, N.; Fudim, M.; Lekavich, C.; Watson, K.; Gulati, S.; Kalogeropoulos, A.; Lewsey, S. Cognitive Impairment in Heart Failure: A Heart Failure Society of America Scientific Statement. J. Card. Fail. 2024, 30, 488–504. [Google Scholar] [CrossRef]
- Ovsenik, A.; Podbregar, M.; Fabjan, A. Cerebral Blood Flow Impairment and Cognitive Decline in Heart Failure. Brain Behav. 2021, 11, e02176. [Google Scholar] [CrossRef] [PubMed]
- Florea, V.G.; Cohn, J.N. The Autonomic Nervous System and Heart Failure. Circ. Res. 2014, 114, 1815–1826. [Google Scholar] [CrossRef]
- Rowell, L.B. Reflex Control of Regional Circulations in Humans. J. Auton. Nerv. Syst. 1984, 11, 101–114. [Google Scholar] [CrossRef] [PubMed]
- Maiuolo, J.; Gliozzi, M.; Musolino, V.; Carresi, C.; Nucera, S.; Macrì, R.; Scicchitano, M.; Bosco, F.; Scarano, F.; Ruga, S.; Zito, M.C.; Oppedisano, F.; Mollace, R.; Paone, S.; Palma, E.; Muscoli, C.; Mollace, V. The Role of Endothelial Dysfunction in Peripheral Blood Nerve Barrier: Molecular Mechanisms and Pathophysiological Implications. Int. J. Mol. Sci. 2019, 20, 3022. [Google Scholar] [CrossRef]
- Nägele, M.P.; Barthelmes, J.; Ludovici, V.; Cantatore, S.; Von Eckardstein, A.; Enseleit, F.; Lüscher, T.F.; Ruschitzka, F.; Sudano, I.; Flammer, A.J. Retinal Microvascular Dysfunction in Heart Failure. Eur. Heart J. 2018, 39, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Szlagor, M.; Dybiec, J.; Młynarska, E.; Rysz, J.; Franczyk, B. Chronic Kidney Disease as a Comorbidity in Heart Failure. Int. J. Mol. Sci. 2023, 24, 2988. [Google Scholar] [CrossRef]
- Silverberg, D.S.; Wexler, D.; Blum, M.; Keren, G.; Sheps, D.; Leibovitch, E.; Brosh, D.; Laniado, S.; Schwartz, D.; Yachnin, T.; Shapira, I.; Gavish, D.; Baruch, R.; Koifman, B.; Kaplan, C.; Steinbruch, S.; Iaina, A. The Use of Subcutaneous Erythropoietin and Intravenous Iron for the Treatment of the Anemia of Severe, Resistant Congestive Heart Failure Improves Cardiac and Renal Function and Functional Cardiac Class, and Markedly Reduces Hospitalizations. J. Am. Coll. Cardiol. 2000, 35, 1737–1744. [Google Scholar] [CrossRef]
- Esteves, A.F.; Gonçalves, S.; Duarte, T.; Ferreira, J.; Coelho, R.; Quintal, J.; Pohle, C.; Fonseca, N.; Caria, R. Iron Deficiency in Acute Coronary Syndromes: Prevalence and Prognostic Impact. Porto Biomed. J. 2025, 10. [Google Scholar] [CrossRef]
- McCullough, P.A. Anemia of Cardiorenal Syndrome. Kidney Int. Suppl. 2021, 11, 35–45. [Google Scholar] [CrossRef]
- Palazzuoli, A.; Gallotta, M.; Iovine, F.; Nuti, R.; Silverberg, D.S. Anaemia in Heart Failure: A Common Interaction with Renal Insufficiency Called the Cardio-Renal Anaemia Syndrome: Anaemia and Heart Failure. Int. J. Clin. Pract. 2007, 62, 281–286. [Google Scholar] [CrossRef]
- Kumar, U.; Wettersten, N.; Garimella, P.S. Cardiorenal Syndrome. Cardiol. Clin. 2019, 37, 251–265. [Google Scholar] [CrossRef]
- Jelani, Q.; Katz, S.D. Treatment of Anemia in Heart Failure: Potential Risks and Benefits of Intravenous Iron Therapy in Cardiovascular Disease. Cardiol. Rev. 2010, 18, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Arrigo, M.; Parissis, J.T.; Akiyama, E.; Mebazaa, A. Understanding Acute Heart Failure: Pathophysiology and Diagnosis. Eur. Heart J. Suppl. 2016, 18 (suppl G), G11–G18. [Google Scholar] [CrossRef]
- Lena, A.; Anker, M.S.; Springer, J. Muscle Wasting and Sarcopenia in Heart Failure—The Current State of Science. Int. J. Mol. Sci. 2020, 21, 6549. [Google Scholar] [CrossRef] [PubMed]
- He, N.; Zhang, Y.; Zhang, L.; Zhang, S.; Ye, H. Relationship Between Sarcopenia and Cardiovascular Diseases in the Elderly: An Overview. Front. Cardiovasc. Med. 2021, 8, 743710. [Google Scholar] [CrossRef]
- Denfeld, Q.E.; Turrise, S.; MacLaughlin, E.J.; Chang, P.-S.; Clair, W.K.; Lewis, E.F.; Forman, D.E.; Goodlin, S.J.; on behalf of the American Heart Association Cardiovascular Disease in Older Populations Committee of the Council on Clinical Cardiology and Council on Cardiovascular and Stroke Nursing; Council on Lifestyle and Cardiometabolic Health; Stroke Council. Preventing and Managing Falls in Adults With Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circ. Cardiovasc. Qual. Outcomes 2022, 15. [Google Scholar] [CrossRef] [PubMed]
- Binu, A.; Cherian, K.; Kapoor, N.; Chacko, S.; George, O.; Paul, T. The Heart of the Matter: Cardiac Manifestations of Endocrine Disease. Indian J. Endocrinol. Metab. 2017, 21, 919. [Google Scholar] [CrossRef]
- Aroor, A.R.; Mandavia, C.H.; Sowers, J.R. Insulin Resistance and Heart Failure. Heart Fail. Clin. 2012, 8, 609–617. [Google Scholar] [CrossRef]
- Lisco, G.; Giagulli, V.A.; Iovino, M.; Zupo, R.; Guastamacchia, E.; De Pergola, G.; Iacoviello, M.; Triggiani, V. Endocrine System Dysfunction and Chronic Heart Failure: A Clinical Perspective. Endocrine 2022, 75, 360–376. [Google Scholar] [CrossRef]
- Kopkan, L.; Hosková, L.; Melenovský, V.; Husková, Z.; Cervenka, L. Abstract P421: The Effects of Dual Angiotensin Receptor and Neprilysin Inhibitor on Organoprotection in Experimental Model of Chronic Heart Failure. Hypertension 2017, 70 (suppl_1), AP421. [Google Scholar] [CrossRef]
- Perrone-Filardi, P.; Paolillo, S.; Agostoni, P.; Basile, C.; Basso, C.; Barilla, F.; Correale, M.; Curcio, A.; Mancone, M.; Merlo, M.; Metra, M. Renin-angiotensin-aldosterone system inhibition in patients affected by heart failure: efficacy, mechanistic effects and practical use of sacubitril/valsartan. Position Paper of the Italian Society of Cardiology. European Journal of Internal Medicine 2022, 102, 8–16. [Google Scholar] [CrossRef]
- Di Lodovico, E.; Facondo, P.; Delbarba, A.; Pezzaioli, L.C.; Maffezzoni, F.; Cappelli, C.; Ferlin, A. Testosterone, hypogonadism, and heart failure. Circulation: Heart Failure 2022, 15, e008755. [Google Scholar] [CrossRef] [PubMed]
- Martucci, G.; Pappalardo, F.; Subramanian, H.; Ingoglia, G.; Conoscenti, E.; Arcadipane, A. Endocrine Challenges in Patients with Continuous-Flow Left Ventricular Assist Devices. Nutrients 2021, 13, 861. [Google Scholar] [CrossRef]
- Alevroudis, I.; Kotoulas, S.-C.; Tzikas, S.; Vassilikos, V. Congestion in Heart Failure: From the Secret of a Mummy to Today’s Novel Diagnostic and Therapeutic Approaches: A Comprehensive Review. J. Clin. Med. 2023, 13, 12. [Google Scholar] [CrossRef] [PubMed]
- Fudim, M.; Felker, G.M. Biomarkers of Congestion. JACC Heart Fail. 2020, 8, 398–400. [Google Scholar] [CrossRef]
- Van Linthout, S.; Tschöpe, C. Inflammation – Cause or Consequence of Heart Failure or Both? Curr. Heart Fail. Rep. 2017, 14, 251–265. [Google Scholar] [CrossRef]
- Hofmann, U.; Frantz, S. How can we cure a heart "in flame"? A translational view on inflammation in heart failure. Basic Res Cardiol. 2013, 108, 356. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wrigley, B.J.; Shantsila, E.; Tapp, L.D.; Lip, G.Y.H. CD 14++ CD 16+ Monocytes in Patients with Acute Ischaemic Heart Failure. Eur. J. Clin. Invest. 2013, 43, 121–130. [Google Scholar] [CrossRef]
- Kologrivova, I.; Shtatolkina, M.; Suslova, T.; Ryabov, V. Cells of the Immune System in Cardiac Remodeling: Main Players in Resolution of Inflammation and Repair After Myocardial Infarction. Front Immunol. 2021, 12, 664457. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Howerton, E.; Tarzami, S.T. Tumor Necrosis Factor-Alpha and Inflammation-Mediated Cardiac Injury. J Cell Sci Ther 2017, 8, 268. [Google Scholar] [CrossRef]
- Prokopidis, K.; Irlik, K.; Hendel, M.; Piaśnik, J.; Lip, G.Y.H.; Nabrdalik, K. Prognostic Impact and Prevalence of Cachexia in Patients With Heart Failure: A Systematic Review and Meta-Analysis. J Cachexia Sarcopenia Muscle 2024, 15, 2536–2543. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yosipovitch, G.; Nedorost, S.T.; Silverberg, J.I.; Friedman, A.J.; Canosa, J.M.; Cha, A. Stasis Dermatitis: An Overview of Its Clinical Presentation, Pathogenesis, and Management. Am. J. Clin. Dermatol. 2023, 24, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Cooper, K.L. Care of the lower extremities in patients with acute decompensated heart failure. Crit Care Nurse 2011, 31, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Boehmer, J.P.; Blaha, C.; Lucking, R.; Kunselman, A.R.; Sinoway, L.I. Chronic heart failure does not attenuate the total activity of sympathetic outflow to skin during whole-body heating. Circ Heart Fail. 2013, 6, 271–278. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hiraiwa, H.; Okumura, T.; Murohara, T. The Cardiosplenic Axis: The Prognostic Role of the Spleen in Heart Failure. Heart Fail. Rev. 2022, 27, 2005–2015. [Google Scholar] [CrossRef]
- Verbrugge, F.H.; Dupont, M.; Steels, P.; Grieten, L.; Malbrain, M.; Tang, W.H.; Mullens, W. Abdominal contributions to cardiorenal dysfunction in congestive heart failure. J Am Coll Cardiol. 2013, 62, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.; Iwakiri, Y. The Lymphatic Vascular System in Liver Diseases: Its Role in Ascites Formation. Clin. Mol. Hepatol. 2013, 19, 99. [Google Scholar] [CrossRef]
Table 2.
Summary of Renal Congestion Effects on long term.
| Effect | Description |
|---|---|
| Acute Kidney Injury (AKI) | Chronic congestion reduces renal perfusion, making the renal medulla hypoxic and predisposing it to acute tubular necrosis (ATN). |
| Fibrosis and Chronic Kidney Disease (CKD) | Persistent renal venous hypertension promotes inflammation, oxidative stress, and tubulointerstitial fibrosis, progressively leading to structural nephron loss and worsening renal function. |
| Altered Drug Metabolism and Toxicity | Decreased renal clearance in congested kidneys impairs the excretion of medications such as loop diuretics, ACE inhibitors/ARBs, and Digoxin. |
| Electrolyte and Acid-Base Imbalances |
Hyperkalemia due to impaired potassium excretion, exacerbated by RAAS inhibitors; Hyponatremia Metabolic acidosis |
| Systemic Inflammation and Endothelial Dysfunction |
Release of pro-inflammatory cytokines (TNF-α, IL-6), contributing to vascular endothelial dysfunction. Accumulation of uremic toxins promotes vascular calcification, oxidative stress, and worsening myocardial remodeling. |
| Anemia and Erythropoietin Deficiency | Impaired erythropoietin (EPO) production in congested kidneys leads to anemia of chronic disease, exacerbating fatigue, hypoxia, and cardiac strain. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



