Submitted:
24 February 2025
Posted:
25 February 2025
Read the latest preprint version here
Abstract
Organ transplantation is an indispensable therapeutic approach for patients experiencing end-stage organ failure. Despite ongoing advancements and refinements in immunosuppressive therapies aimed at mitigating graft rejection and enhancing graft longevity, environmental influences including particulate matter 2.5 (PM2.5) have emerged as significant determinants of post-transplant health. PM2.5, a prevalent environmental contaminant, is particularly concerning due to its widespread presence and detrimental biological effects. Notably, the living environment of transplant recipients further exacerbates the complexity of post-transplant outcomes. Evaluating findings from recent investigations, this review delves into the influence of PM2.5 exposure on the immune system. The findings identify its capacity to provoke systemic inflammation, disrupt cytokine profiles, and compromise immune tolerance mechanisms. Such immune dysfunction poses direct risks to graft integrity, with potential implications for both graft health and the prospects of achieving long-term graft survival in affected patients.
Keywords:
particulate matter 2.5
; immunosuppressive therapy
; environmental pollution
; chronic rejection
; systemic inflammation
; macrophages
; immune tolerance
Introduction
Air pollution represents a significant global health challenge, contributing to a multitude of serious medical conditions and diminished life expectancy. Key pollutants include carbon monoxide (CO), sulfur oxides (SO₂), nitrogen oxides (NO₂), ozone (O₃), and airborne particulate matter (PM) [1]. Among these, PM2.5, defined as particulate matter with an aerodynamic diameter of 2.5 microns or less, is particularly detrimental. It is associated with various adverse health outcomes, including cerebrovascular, cardiovascular, pulmonary, hepatic, renal diseases, malignancy, graft complications, and increased mortality [2]. The World Health Organization (WHO) attributes over seven million premature deaths annually to air pollution, with PM2.5 being especially hazardous due to its ability to penetrate deep into the respiratory system, traverse the alveolar barrier, and subsequently enter systemic circulation, thereby affecting multiple organ systems [3]. The health complications of PM2.5 exposure are extensive, encompassing respiratory and cardiovascular diseases, neurological disorders, graft complications, and carcinogenesis. Epidemiological research has indisputably demonstrated a strong correlation between PM2.5 exposure and elevated rates of morbidity and mortality worldwide, particularly in urban and industrial settings characterized by high pollution levels. The deleterious effects on health can largely be attributed to the small size and aerodynamic properties of PM2.5, which facilitate its evasion of the body’s innate defense mechanisms and allow for deep lung penetration. Upon inhalation, these particles incite localized inflammatory responses, which can rapidly escalate to systemic inflammation [4]. PM2.5 comprises various toxic constituents, including heavy metals, polycyclic aromatic hydrocarbons, and organic compounds [5-7]. Research indicates that these particles not only provoke inflammation and oxidative stress in the lungs but also adversely affect endothelial function and promote vascular inflammation, critical mechanisms in the pathogenesis of cardiovascular disease [8,9]. Moreover, PM2.5 exposure is implicated in the initiation and progression of conditions such as atherosclerosis, hypertension, and myocardial infarction, establishing it as a notable risk factor for cardiovascular morbidity and mortality [9]. Beyond cardiovascular implications, PM2.5 exposure has been linked to adverse outcomes in the liver, pancreas, kidneys, and central nervous system [10].Studies reveal that PM2.5 particles can cross the blood-brain barrier, fostering neuroinflammation and potentially contributing to the onset of neurodegenerative diseases such as Alzheimer's and Parkinson's [11]. Therefore, the toxicological attributes of PM2.5 underscore its capacity to induce oxidative stress and trigger immune dysregulation across various organ systems, emphasizing its role as a systemic health hazard [5,6,12].
For individuals undergoing organ transplantation, the environmental health risks posed by PM2.5 are markedly intensified. Transplant recipients, who rely on lifelong immunosuppressive therapy to mitigate graft rejection, constitute a particularly susceptible population in terms of the effects of environmental pollutants [13]. While immunosuppressive agents are critical to maintaining graft tolerance by inhibiting immune responses, they simultaneously elevate the risk of infections, malignancies, and adverse responses to environmental stressors, including air pollution [13,14]. Notably, PM2.5 exposure has been shown to trigger immune reactions, resulting in the release of pro-inflammatory cytokines, such as interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and interleukin-1 beta (IL-1β) [15]. This inflammatory response, commonly referred to as a "cytokine storm," poses threats to immunosuppressed patients, potentially accelerating graft rejection and complicating long-term post-transplant outcomes [16]. The risk of infections among transplant recipients is further exacerbated by PM2.5 exposure, which compromises respiratory defenses and impairs immune cell functionality, thereby increasing vulnerability [17]. Research indicates that PM2.5 can diminish the effectiveness of alveolar macrophages and hinder mucociliary clearance, resulting in augmented susceptibility to both bacterial and viral infections [18,19]. For transplant patients, such infections can rapidly escalate to severe complications, including graft rejection and sepsis, underscoring the imperative for diligent air quality management in post-transplant care [20,21]. Despite the considerable health risks associated with PM2.5, there is a substantial deficiency in research examining its impact specifically on transplant recipients. To date, most studies have concentrated on the effects of PM2.5 within the general population, leaving a significant gap regarding its specific implications for individuals with compromised immune systems. This gap in knowledge highlights the urgent need for focused research to clarify the mechanisms through which PM2.5 influences graft survival and patient outcomes among transplant recipients. It is essential to standardize pollution measurement techniques and establish uniform criteria for assessing exposure, as these steps are vital for advancing research in this area. Furthermore, investigating the long-term consequences of PM2.5 exposure on transplant populations could provide crucial insights into the ways environmental factors contribute to chronic rejection and other post-transplant complications.
Considering these risks, it is imperative to integrate air quality considerations into clinical guidelines for transplant patients. Implementing practical interventions such as the installation of in-home air filtration systems, the use of protective masks in areas with high pollution levels, and regular monitoring of air quality indices could significantly reduce exposure to PM2.5. Additionally, public health policies aimed at improving urban air quality would greatly benefit vulnerable groups, including transplant recipients, whose long-term health is contingent upon a stable environment and functioning immune system. This review seeks to synthesize the existing literature on PM2.5 exposure and its effects on organ transplant recipients, particularly focusing on immune dysregulation and graft survival. By identifying gaps in current research and recommending pathways for future investigations, this work aspires to enhance understanding of the environmental challenges facing transplant patients, emphasizing the critical need to address air quality in the post-transplant care continuum.
To gather relevant studies from 2014 to 2024, searches were conducted in PubMed, Google Scholar, Scopus, and Web of Science databases. Only peer-reviewed studies that directly connect air pollution to transplant outcomes in human populations were selected. Due to a scarcity of human data, supplementary systematic reviews and animal studies were utilized. In situations where human data was lacking, animal models as well as systematic reviews and meta-analyses were employed to ensure a comprehensive synthesis. This review highlights the effects of PM2.5 exposure on immune dysregulation, cardiovascular events, and long-term graft outcomes following transplantation.
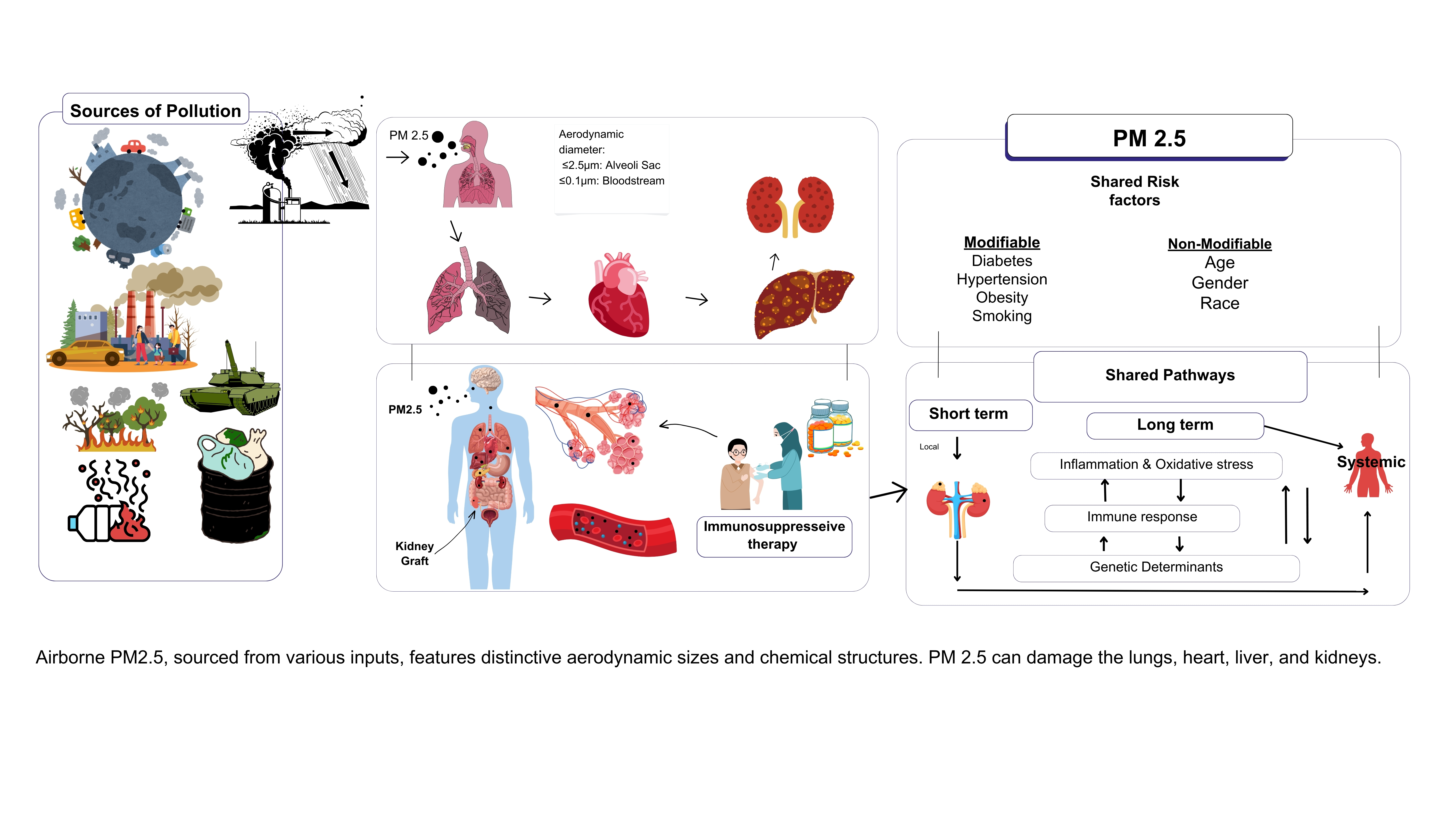
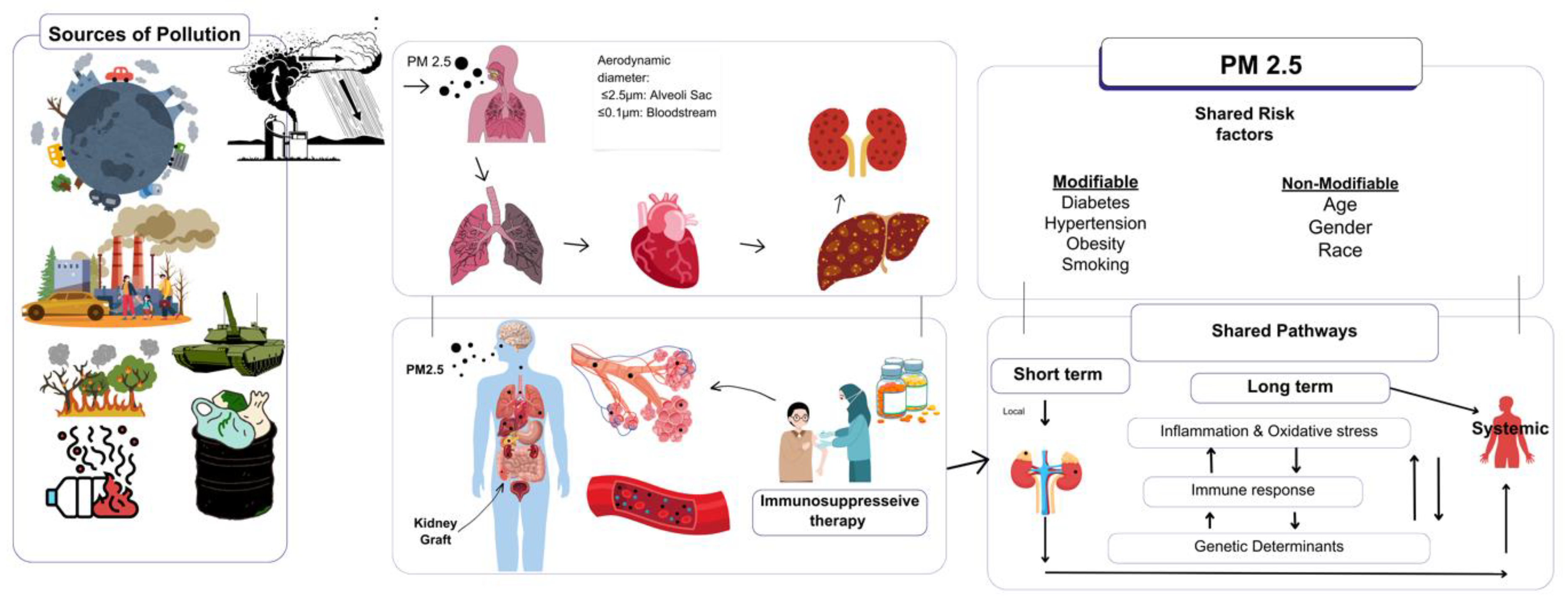
Figure 1.
Airborne PM2.5, sourced from various inputs, features distinctive aerodynamic sizes and chemical structures can damage the lungs, heart, liver, and kidneys.
Figure 1.
Airborne PM2.5, sourced from various inputs, features distinctive aerodynamic sizes and chemical structures can damage the lungs, heart, liver, and kidneys.
1. (PM2.5): A Critical Health Threat
PM2.5 is an airborne contaminant primarily produced by traffic emissions, industrial activities, and the combustion of residential fuels. Its minute size allows it to bypass the body's defense mechanisms, reaching the alveolar sacs and ultimately entering the systemic circulation. Worldwide, exposure to PM2.5 has been linked to an increased risk of respiratory and cardiovascular health issues in the general population; however, these effects are particularly detrimental for transplant recipients due to their existing immunosuppression and vulnerability of their organs [4] .
2. PM2.5 and Immune Modulation in Transplant Recipients
For transplant recipients, the use of immunosuppressive medications is essential for maintaining graft acceptance and minimizing infection risk. Nonetheless, exposure to PM2.5 complicates this balance [4,22]. Research indicates that PM2.5 can stimulate the production of pro-inflammatory cytokines, including interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α), which have the potential to intensify immune responses that might otherwise remain regulated [22,23].
Multiple studies have found that transplant patients who are exposed to elevated levels of PM2.5 face an increased risk of acute graft rejection, suggesting that air pollution aggravates the immune system's reaction to the transplanted organ [24,25]. Additionally, PM2.5 exposure is associated with dysregulation of immune cells, specifically T lymphocytes and dendritic cells, which are vital for achieving transplant tolerance. Such immunological imbalances may threaten the long-term success of a transplant by leading to both acute and chronic rejection.
2.1. Organ-Specific Effects of PM2.5 on Transplant Recipients
2.1.1. Respiratory Complications in Transplant Recipients
Transplant recipients who are immunosuppressed face a heightened risk of respiratory infections following exposure to PM2.5, primarily due to compromised lung function, reduced muco-ciliary clearance, and increased vulnerability [2]. Respiratory complications are among the most immediate and significant consequences of PM2.5 exposure in transplant patients, particularly for those who have undergone lung transplants, as respiratory issues frequently contribute to morbidity [26]. PM2.5 exposure stimulates alveolar macrophages, leading to the release of pro-inflammatory cytokines such as IL-6, TNF-α, and IL-1β. This cytokine release enhances neutrophil recruitment and triggers oxidative stress, which can damage ciliated epithelial cells and impair the lungs' ability to clear pathogens and particulates effectively. By disrupting alveolar macrophage function, PM2.5 diminishes the lungs' primary defense mechanism, increasing susceptibility to opportunistic infections and resulting in chronic pathogen colonization. Consequently, this raises the risk of bacterial and viral infections, including pneumonia, chronic obstructive pulmonary disease (COPD), and lung fibrosis. Transplant recipients residing in areas with high PM2.5 levels are more likely to experience infections like pneumonia, which is notably the leading cause of death among these individuals [26,27]. These respiratory infections can severely compromise graft function and negatively impact patient survival [27]. Research has shown that respiratory infections, particularly pneumonia, are more common in transplant recipients exposed to significant air pollution [28,29] . The impairment of macrophage function due to PM2.5 presents a substantial threat to immune defenses, leaving transplant patients at an elevated risk for opportunistic infections from environmental pollutants. Such infections can lead to serious complications, including graft dysfunction or failure [30] .
2.1.2. Cardiovascular Complications in Transplant Recipients
Cardiovascular diseases represent the leading cause of death among graft recipients [3]. The complications arising from PM2.5 exposure extend beyond just heart transplant recipients to include patients with other types of grafts, primarily due to systemic oxidative stress and endothelial dysfunction. Long-term exposure to PM2.5 is correlated with increased incidences of hypertension, atherosclerosis, and myocardial infarction within the general population, underscoring its association with cardiovascular morbidity [31,32]. Research indicates that residing in areas with elevated PM2.5 levels amplifies cardiovascular risks such as heart attacks and strokes in transplant recipients [33,34]. PM2.5 acts as an immunosuppressive agent that significantly deteriorates cardiovascular health by promoting oxidative stress and endothelial dysfunction. It contributes to the generation of reactive oxygen species (ROS), decreases nitric oxide (NO) bioavailability, and disrupts vasodilation, which increases arterial stiffness and ischemic risks. Moreover, elevated cytokine levels (e.g., IL-6, TNF-α) enhance platelet activation, fostering a pro-thrombotic environment that predisposes patients to vascular occlusion, resulting in increased morbidity and mortality. The detrimental impact of PM2.5 is exacerbated when combined with immunosuppressive medications [2]. Chronic low-grade inflammation driven by PM2.5 exposure accelerates the progression of atherosclerosis, leading to complications such as cardiac allograft vasculopathy (CAV), further worsening outcomes in transplant recipients across all organ types.
2.1.3. Hepatic Complications in Transplant Recipients
The liver's crucial role in metabolism and detoxification renders it particularly susceptible to systemic effects induced by PM2.5, impacting liver grafts and overall hepatic health in transplant recipients. PM2.5 exerts notable immunomodulatory effects on liver transplant recipients [35]. Any compromise to liver function can increase the risk of immune-mediated graft rejection [2] . PM2.5 exposure results in the production of pro-inflammatory cytokines and activates immune pathways within liver grafts, potentially impairing their immunological tolerance. The exposure stimulates liver-resident macrophages to release pro-inflammatory cytokines such as TNF-α and IL-6, perpetuating liver inflammation and hepatocellular damage. Persistent activation of TGF-β can induce stellate cell differentiation, leading to increased collagen deposition and eventual graft fibrosis. While direct studies linking PM2.5 exposure to acute liver transplant rejection are sparse, broader research into air pollution suggests a significant association between high PM2.5 levels and such rejections. PM2.5 exposure may heighten the immune response against the transplanted liver, leading to an increased risk of rejection. Furthermore, liver transplant recipients are at risk of disrupted cytochrome P450 enzyme activity due to PM2.5, complicating the metabolism of immunosuppressive medications and raising the potential for toxicity or graft rejection [32,34,36]. Those patients are also at an elevated risk for respiratory infections upon exposure to PM2.5, which can cause graft rejection or other complications, heightening the overall risk. Patients in high pollution areas may experience increased rates of infections and hospitalizations, adversely impacting both graft and patient survival [36,37]. Chronic exposure to PM2.5 is linked to the long-term deterioration of liver grafts [38] . The systemic inflammation and oxidative stress caused by PM2.5 can accelerate liver fibrosis, a significant contributor to chronic graft dysfunction [39,40]. Although limited research has specifically focused on PM2.5's impact on liver graft survival, studies on chronic liver disease indicate that air pollution exacerbates hepatic inflammation and fibrosis, thereby affecting transplanted livers [40]. High PM2.5 exposure is associated with accelerated liver graft fibrosis in transplant recipients, leading to decreased function and potential graft failure [7,40]. The long-term effects of air pollution on liver graft survival necessitate further investigation, particularly regarding preventive measures.
2.1.4. Renal Complications in Transplant Recipients
Kidney transplant recipients face considerable risks from PM2.5 due to its inflammatory and fibrotic properties, which undermine renal graft function and overall survival. PM2.5 exposure threatens kidney transplantation success by disrupting the delicate balance between immunosuppression and general health through systemic inflammation and altered immune responses [3] . Specifically, PM2.5 exposure incites the release of inflammatory cytokines, such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α), that can have detrimental effects on the kidney's functionality and the longevity of the graft. This continued inflammation exacerbates graft dysfunction and the risk of chronic rejection [41]. Persistent inflammation activates TGF-β, driving fibroblast proliferation and extracellular matrix accumulation, ultimately resulting in tubular atrophy and interstitial fibrosis. Oxidative stress further compromises renal blood flow and filtration capabilities, intensifying ischemic damage. The inflammatory response during kidney transplantation can significantly elevate the likelihood of both acute and chronic rejection episodes [42]. Living in regions with elevated PM2.5 concentrations correlates with an increased incidence of acute rejection and diminished graft survival for kidney transplant patients [37,43]. Exposure to PM2.5 disrupts key immune cells essential for maintaining graft tolerance, notably regulatory T cells, and dendritic cells [43]. This disruption can amplify the immune response toward the transplanted kidney, increasing the risks of both early and late rejection [44]. Consequently, immune dysregulation may lead to heightened early rejection episodes and chronic loss of graft function. Extended PM2.5 exposure is associated with accelerated declines in renal function, underscoring the necessity for proactive intervention strategies. In such circumstances, chronic graft survival is seriously threatened by ongoing low-grade inflammation stemming from prolonged immune dysregulation, culminating in fibrosis and potential graft failure [45].
Immunosuppressive therapies, vital for preventing kidney graft rejection, inadvertently increase the susceptibility of transplant recipients to opportunistic infections [46]. Ensuring the survival and functionality of transplants remains a primary concern for kidney transplant recipients. Exposure to PM2.5 heightens the likelihood of graft rejection while simultaneously compromising immune defenses, which in turn fosters infections [47,48] . Patients in high-pollution areas bear an elevated risk of hospitalization due to respiratory infections, adversely affecting post-transplant care and graft outcomes a significant concern for healthcare systems [2,43]. Long-term exposure to PM2.5 has detrimental effects on kidney graft performance [4,48]. Research indicates that PM2.5 is implicated in the development of chronic allograft nephropathy, a leading contributor to late graft failure among kidney transplant recipients [49] . Inflammatory processes induced by PM2.5 can instigate progressive fibrosis in the kidney, impairing its filtration capacity and electrolyte homeostasis, which are critical for renal function [2]. Data suggest that kidney transplant recipients exposed to higher levels of PM2.5 show a more pronounced decline in estimated glomerular filtration rate (eGFR) over time [50,51] . Emphasizing the significance of environmental influences like PM2.5 in the long-term management of kidney transplant patients can markedly improve graft survival rates [3,43] . Furthermore, PM2.5 exposure correlates with increased risks of respiratory infections, leading to substantial morbidity and mortality among kidney transplant patients [7,49].
2.1.5. Long-Term Graft Survival and Environmental Exposures
Sustained exposure to PM2.5 poses diverse threats to human health, notably hindering long-term graft survival [54]. Research has established associations between long-term PM2.5 exposure and the onset of conditions such as chronic allograft vasculopathy, characterized by progressive arterial thickening that compromises blood flow and leads to graft failure [3]
Comprehensive analyses indicate that elevated PM2.5 concentrations are linked to significantly diminished graft survival rates among transplant recipients. It is critical to afford equal consideration to environmental factors alongside clinical interventions when overseeing long-term transplant outcomes [52] . Implementing air filtration systems within the homes of transplant patients and advocating for improved urban air quality could potentially enhance long-term health outcomes [48,52].
2.1.6. Shared Pathophysiological Effects Across Organs
PM2.5 exposure triggers common pathological mechanisms that adversely affect graft function across all transplant recipients. Cytokine dysregulation, characterized by elevated levels of IL-6, TNF-α, and TGF-β, perpetuates inflammatory responses, fibrosis, and vascular injury. The dysfunction of regulatory T cells and macrophages exacerbates immune-mediated graft rejection. Significantly, PM2.5-related activation of TGF-β signaling promotes fibrosis in the lungs, liver, and kidneys, diminishing graft longevity [31] .
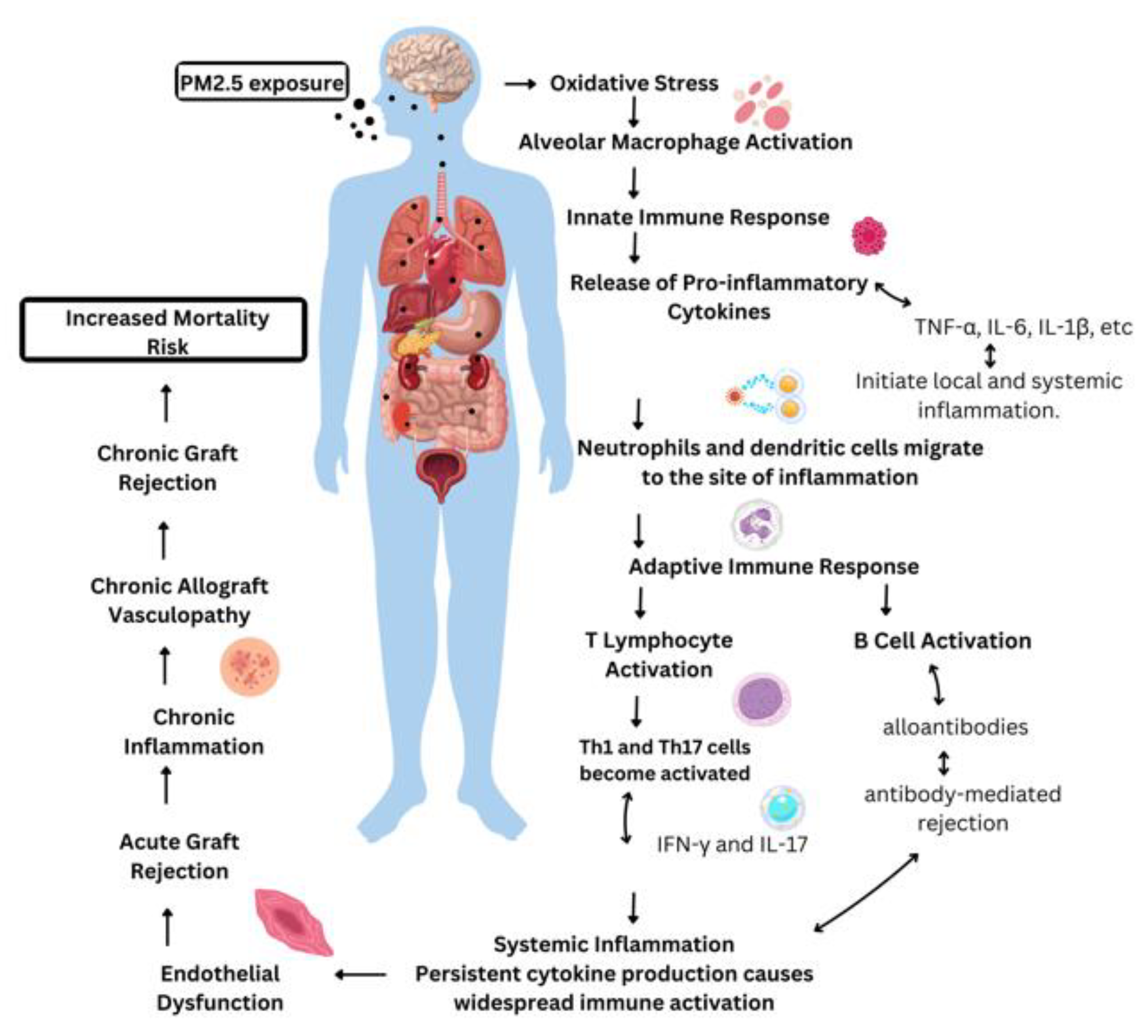
Figure 2.
Immune Response Pathways Involving PM2.5 in Organ Transplant Rejection.
3. The impact of PM2.5 on transplant immunity
3.1. Innate Immune System and PM2.5 in Transplantation
3.1.1. Alloantigen Recognition and Immune Activation
The immune response to transplanted organs, known as allografts, initiates through the recognition of foreign antigens presented by donor cells, termed alloantigen recognition [53]. This process engages both innate and adaptive immune systems [54]. Dendritic cells (DCs) play a pivotal role in this mechanism; they capture donor antigens and migrate to lymphoid tissues to present these antigens to T cells. This antigen presentation activates T cells, prompting their differentiation into effector T cells that target the graft, facilitating rejection. Environmental factors, notably pollutants such as PM2.5, modulate this immune activation. Table 1 summarizes the effects of PM2.5 on Immunity in transplant patients [55].
PM2.5 exposure has been documented to enhance the expression of toll-like receptors (TLRs) on various immune cells, including DCs, macrophages, and neutrophils. TLRs are instrumental in detecting pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs). Their activation by PM2.5 amplifies immune surveillance and inflammatory responses, thereby promoting T-cell priming and expediting graft rejection [59].
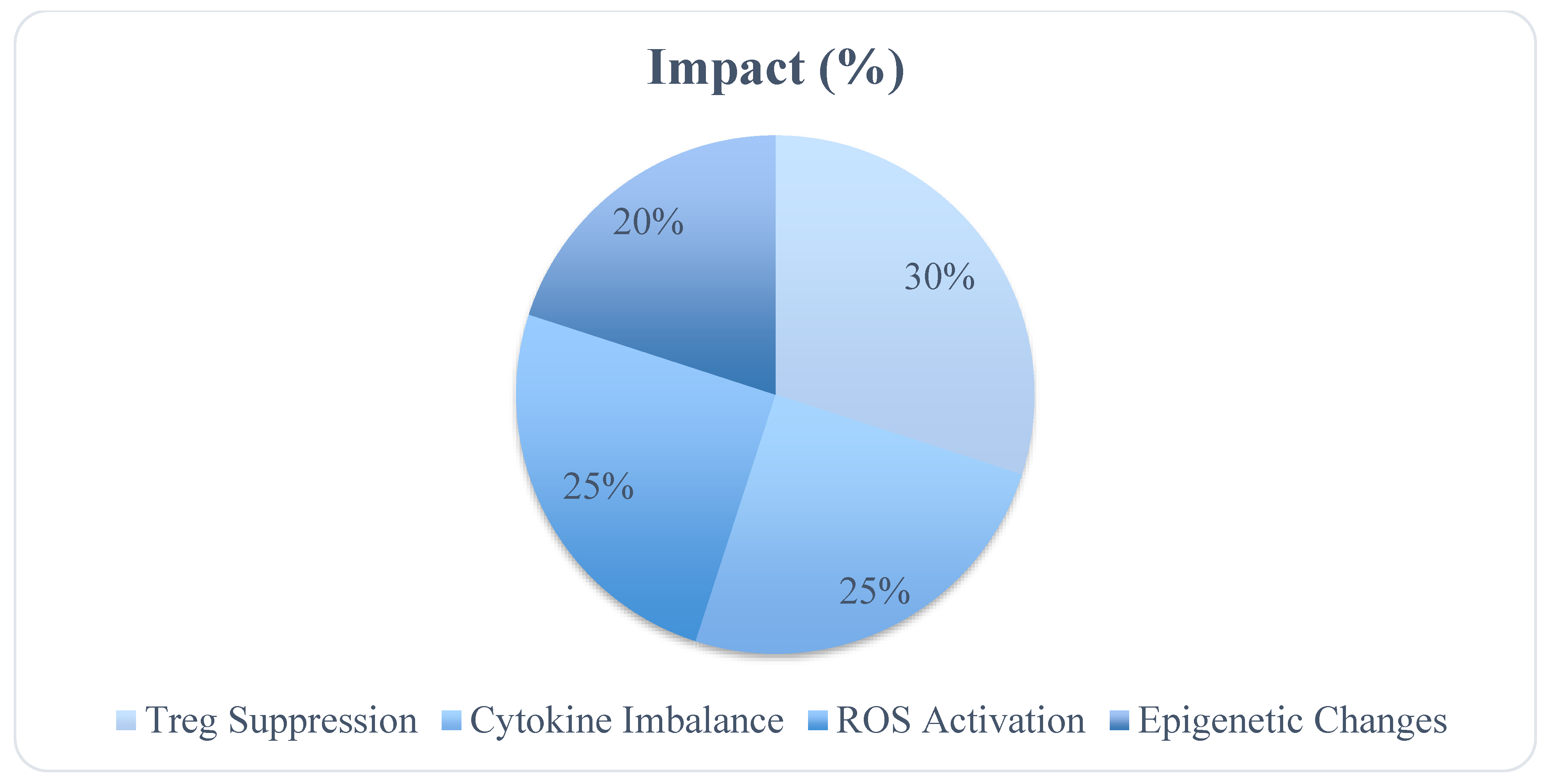
Figure 3.
Immune Pathways Affected by PM2.5.
3.1.2. Cytokine Storm and Inflammation
Cytokines, which are small signaling molecules released by immune cells, play a crucial role in orchestrating inflammation and immune responses [57]. Within the transplantation context, pro-inflammatory cytokines such as interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and interleukin-1 beta (IL-1β) serve as key mediators of graft rejection. PM2.5 exposure triggers a "cytokine storm," characterized by excessive cytokine release that leads to dysregulated inflammation [58]. Increased levels of IL-6 and TNF-α activate immune cell populations, including neutrophils, macrophages, and T cells, facilitating both acute and chronic rejection processes [59] . Specifically, IL-6 promotes the differentiation of naïve T cells into Th17 cells, which produce interleukin-17 (IL-17), a significant recruiter of neutrophils. The hyperactivation of Th17 cells and overproduction of IL-17 contributes to acute rejection and chronic damage across diverse organs such as kidneys, lungs, and hearts [58] . TNF-α further drives tissue destruction and fibrosis, adversely affecting graft function [60,61]
3.1.3. T-Cell Activation and Graft Rejection
T cells are instrumental in graft rejection as they identify donor antigens and initiate immune responses [62]. Activation of T cells occurs via two primary pathways: the direct and indirect pathways. In the direct pathway, recipient T cells directly recognize donor MHC molecules on graft cells [63]. Conversely, in the indirect pathway, recipient antigen-presenting cells (APCs) process and present donor-derived peptides to T cells. Both pathways culminate in the activation of cytotoxic T lymphocytes (CTLs), which target graft tissue, resulting in rejection [63,64] . PM2.5 enhances T-cell activation by upregulating co-stimulatory molecules and cytokines that support T-cell proliferation and differentiation [65]. Research demonstrates that PM2.5 exposure amplifies Th1 and Th17 responses, resulting in elevated interferon-gamma (IFN-γ) and IL-17 levels, both critical mediators of graft rejection [17,66] . IFN-γ activates macrophages, promoting graft cell destruction, while IL-17 is instrumental in neutrophil recruitment, exacerbating graft inflammation [67] .
3.2. Adaptive Immune System and PM2.5 in Transplantation
3.2.1. Macrophage Activation and Tissue Damage
Macrophages are fundamental to the innate and adaptive immune responses, fulfilling a dual role in transplant immunity [68]. They can adopt two predominant phenotypes, M1 Macrophages, these pro-inflammatory cells secrete cytokines such as TNF-α and IL-6. While they initiate immune responses, their activity can escalate inflammation, causing tissue damage in transplanted organs. M2 Macrophages, these anti-inflammatory cells are crucial for tissue repair and fostering immune tolerance essential for graft survival [69-71] . PM2.5 exposure shifts the balance towards M1 macrophage polarization, resulting in the release of pro-inflammatory cytokines, reactive oxygen species (ROS), and nitric oxide (NO), all of which exacerbate graft injury [69] . For example, in the pulmonary context, PM2.5-stimulated alveolar macrophages produce excessive ROS and TNF-α, promoting chronic inflammation and fibrosis, which can ultimately result in chronic lung allograft dysfunction (CLAD) [72,73].
3.2.2. Dendritic Cell Activation and Antigen Presentation
Dendritic cells (DCs) are the foremost antigen-presenting cells (APCs) within the immune system, essential in triggering immune responses against transplanted organs [74] . Exposure to PM2.5 amplifies the maturation and activation of dendritic cells, enhancing their capacity to present donor antigens to T cells [64,74] . This increased antigen presentation expedites the activation of effector T cells, specifically Th1 and Th17 subsets, which play pivotal roles in mediating graft rejection [75]. In transplant recipients, PM2.5-induced DC activation results in elevated levels of IL-12, a cytokine that facilitates Th1 differentiation and stimulates the production of IFN-γ [76,77]. Enhanced IFN-γ levels promote macrophage activation and exacerbate graft damage, contributing to both acute and chronic rejection processes [78]. Similar mechanisms are evident across various organ transplant recipients, whereby dendritic cell-mediated T cell activation drives immune rejection [79].
3.2.3. Regulatory T-Cell Dysfunction
Regulatory T cells (Tregs) are instrumental in sustaining immune tolerance toward transplanted organs [80] . They play a pivotal role in suppressing effector T cell activation and curtailing excessive immune responses that could precipitate graft rejection [81]. PM2.5 exposure compromises Treg functionality by elevating oxidative stress and enhancing pro-inflammatory cytokine production. This disturbance in Treg activity creates an imbalance between effector and regulatory T cells, tilting the response toward increased immune activation and consequent rejection [88]. In the context of lung and liver transplantation, dysfunctional Tregs have been linked to higher instances of chronic rejection and diminished graft survival rates [82] . By dampening Treg function, PM2.5 exposure further amplifies Th1 and Th17 cell activation, intensifying the inflammatory milieu and advancing graft dysfunction [83] . Table 2 shows the key molecules and their mechanism affecting immune system.
4. PM2.5 and Chronic Inflammatory Processes in Transplantation
4.1. Oxidative Stress and Endothelial Dysfunction
Oxidative stress serves as a principal mechanism driving chronic inflammation and tissue impairment in transplantation [84] . Exposure to PM2.5 leads to the generation of reactive oxygen species (ROS), which inflict oxidative damage on endothelial cells that constitute the vasculature of transplanted organs. The ensuing endothelial dysfunction is a critical feature of chronic allograft rejection, fostering vascular inflammation, smooth muscle cell hypertrophy, and fibrosis [85-88] . PM2.5 initiates macrophage activation through toll-like receptors (TLRs), which identify particulate pollutants as damage-associated molecular patterns (DAMPs). As a result, oxidative stress exacerbates damage to endothelial cells and graft tissues. Increased concentrations of pro-inflammatory cytokines such as TNF-α and IL-6 further compound systemic inflammation, elevating the likelihood of acute rejection episodes. Additionally, in kidney and liver transplantation, oxidative stress is instrumental in promoting fibrosis and chronic allograft nephropathy or hepatopathy, contributing to long-term graft dysfunction [87].
4.2. Fibrosis and Chronic Graft Dysfunction
Persistent exposure to PM2.5 facilitates the development of fibrosis, characterized by the excessive accumulation of extracellular matrix components, leading to tissue scarring and impaired organ functionality [88]]. Fibrosis is a common feature of chronic rejection in all transplanted organs, including the lungs (bronchiolitis obliterans), liver (hepatic fibrosis), and kidneys (interstitial fibrosis and tubular atrophy) [89]. Chronically elevated PM2.5 levels intensify pro-fibrotic mechanisms mediated by TGF-β (transforming growth factor-beta), a cytokine that stimulates fibroblast differentiation into myofibroblasts, responsible for collagen and extracellular matrix secretion [88] . The upregulation of TGF-β occurs in response to PM2.5-induced oxidative stress and inflammation, culminating in progressive fibrosis and chronic graft dysfunction [88,90]. Furthermore, TGF-β production by macrophages contributes to fibroblast activation, resulting in enhanced collagen deposition, a hallmark of chronic rejection. While macrophages typically engage with regulatory T cells (Tregs) to uphold immune tolerance and mitigate graft rejection, PM2.5 exposure disrupts this interaction by favoring a pro-inflammatory macrophage phenotype, compromising Treg-mediated suppression. This shift accelerates effector T cell activation and potentiates the risk of graft rejection. The key determinants of adverse post-transplant outcomes include the impacts of PM2.5 exposure, which give rise to immune system dysregulation, cardiovascular issues, and dysfunction across respiratory, renal, and hepatic systems, alongside an increased risk of infections, these complex interaction between PM2.5-induced immune responses and the outcomes of multi-organ transplantation [91]. PM2.5 also incites immune dysregulation through several pathways, such as the elevation of pro-inflammatory cytokines, T-cell activation, macrophage polarization, and impairment of Treg function [92,93]. These phenomena are integral to both acute and chronic graft rejection, contributing to long-term complications like fibrosis and vascular dysfunction [94,95]. The inconsistencies in pollution measurement methods, along with inadequate long-term cohort studies, present obstacles to understanding the relationship between PM2.5 exposure and transplant complications. Nonetheless, the observed correlations warrant the integration of air quality considerations into clinical guidelines, advocating for protective strategies, including in-home air filtration systems. Such measures not only benefit transplant recipients but also improve overall health outcomes for individuals residing in high-pollution regions [37,96]. This review underscores the multifaceted influences of PM2.5 on organ transplant recipients, highlighting acute and chronic immunological reactions, alongside complications pertaining to respiratory, cardiovascular, hepatic, and renal systems, with a significant risk of long-term graft rejection. The establishment of standardized exposure metrics will enhance pollution monitoring efficacy and elucidate the causal relationships between PM2.5 and transplant outcomes. Considering the systemic effects of PM2.5 emphasizes the importance of incorporating air quality measures within clinical guidelines for transplant recipients, promoting protective interventions such as air filtration systems and urban air quality improvements to enhance patient outcomes and mitigate long-term complications [97]. Recent clinical studies have investigated the impact of PM2.5 exposure on cytokine modulation and its subsequent effects on organ transplantation outcomes. A cohort study examined the association between ambient air pollution exposure and outcomes in lung transplant recipients. Exposure to PM2.5 was linked to increased inflammatory cell infiltration in the lungs and elevated levels of pro-inflammatory mediators. These inflammatory responses were associated with higher rates of graft failure and mortality among lung transplant patients [17]. Another Research focused on the effects of long-term exposure to airborne particulate matter on kidney transplant recipients. Chronic exposure to PM2.5 was associated with increased levels of pro-inflammatory cytokines, such as IL-6 and TNF-α. This cytokine imbalance correlated with a higher incidence of graft rejection and reduced graft survival in kidney transplant patients [7]. Furthermore, Exposure to air pollution, particularly PM2.5, post-transplantation was linked to increased risks of organ rejection, cardiovascular complications, and infection-related mortality. The study highlighted the role of pollution-induced cytokine modulation in these adverse outcomes [17,26].
5. Clinical Implications and Recommendations
In clinical settings, transplant recipients residing in areas with elevated PM2.5 levels may benefit from individualized risk assessments that incorporate air quality metrics into their post-operative care plans. Future clinical guidelines ought to emphasize environmental health considerations, advising the implementation of regular air quality monitoring protocols. Additionally, the identification of specific biomarkers that indicate macrophage activity is crucial for the early detection of inflammatory responses. Strategies should also focus on the development of interventions to reduce reactive oxygen species (ROS) production and to fine-tune macrophage polarization to mitigate excessive M1-driven inflammatory processes. Enhancing the functionality of regulatory T cells (Tregs) is vital for sustaining immune tolerance, thereby facilitating appropriate responses to preserve graft integrity. Patient education serves as a cornerstone of general clinical practices, with particular attention to the risks associated with PM2.5 exposure and tailored strategies for cardiovascular and infection prevention. Furthermore, adopting protective strategies such as in-home air purification systems, community initiatives aimed at improving urban air quality, and comprehensive policies to reduce PM2.5 emissions will likely yield significant benefits in graft longevity and overall health outcomes for transplant recipients. Educational campaigns on these topics can further enhance awareness and encourage proactive behavior among individuals living in high-pollution environments.
6. Conclusion
The outcomes of organ transplantation are profoundly influenced by the often-neglected risks associated with PM2.5 exposure. PM2.5 can impair innate immune functions, particularly the activity of alveolar macrophages, rendering transplant recipients more susceptible to opportunistic infections. Chronic exposure to PM2.5 adversely impacts transplant immunity by provoking pro-inflammatory cytokine responses, which elevate the likelihood of acute rejection events, even in the context of existing immunosuppression protocols. This underscores the necessity for customized immunosuppressive therapy strategies aimed at mitigating PM2.5-induced immune dysregulation. Furthermore, prolonged PM2.5 exposure contributes to the acceleration of chronic allograft vasculopathy through the induction of endothelial dysfunction, leading to vascular inflammation and fibrosis. The continuum from acute immune activation to chronic tissue damage ultimately reduces graft longevity and predisposes recipients to organ transplant failure. Hence, addressing PM2.5 exposure is critical in optimizing transplant outcomes.
Authors Contribution
Conceptualization, Editing and Writing: Muhammad Adil Malik; Supervision: Quan Zhuang.
Acknowledgment
The author extends his sincere gratitude to Quan Zhuang for his kind supervision and guidance throughout.
Declaration
The authors declare no conflict of interest.
Abbreviations
ED (Erectile Dysfunction), ESRD (end-stage renal disease),
KT (kidney transplantation), CKD (chronic kidney disease)
| Abbreviation | Meaning |
| PM2.5 | Particulate Matter 2.5 |
| O₃ | Ozone |
| CO | Carbon monoxide |
| SO₂ | Sulfur oxides |
| NO₂ | Nitrogen oxides |
| WHO | World Health Organization |
| IL-6 | Interleukin-6 |
| IFN-γ | Interferon-gamma |
| TNF-α | Tumor necrosis factor-alpha |
| COPD | Chronic obstructive pulmonary disease |
| ROS | Reactive oxygen species |
| CAV | Cardiac allograft vasculopathy |
| eGFR | Estimated glomerular filtration rate |
| DCs | Dendritic cells |
| TLRs | Toll-like receptors |
| PAMPs | Pathogen-associated molecular patterns |
| DAMPs | Damage-associated molecular patterns |
| APCs | Antigen-presenting cells |
| CTLs | Cytotoxic T lymphocytes |
References
- Baklanov, A.; Molina, L.T.; Gauss, M. Megacities, air quality and climate. Atmospheric Environment 2016, 126, 235–249. [Google Scholar]
- Supphapipat, K.; Leurcharusmee, P.; Chattipakorn, N.; Chattipakorn, S.C. Impact of air pollution on postoperative outcomes following organ transplantation: Evidence from clinical investigations. Clinical Transplantation 2024, 38, e15180. [Google Scholar] [PubMed]
- Dehom, S.; Knutsen, S.; Shavlik, D.; Bahjri, K.; Ali, H.; Pompe, L.; Spencer-Hwang, R. Long-term exposure to fine particulate matter (PM2. 5) and cardiovascular disease mortality among renal transplant recipients. OBM Transplantation 2019, 3, 1–22. [Google Scholar]
- Perico, N.; Casiraghi, F.; Cortinovis, M.; Remuzzi, G. A Modern View of Transplant Immunology and Immunosuppression. In Contemporary Lung Transplantation; Springer: 2024; pp. 81-110.
- Xu, J.; Hu, W.; Liang, D.; Gao, P. Photochemical impacts on the toxicity of PM2.5. Critical Reviews in Environmental Science and Technology 2022, 52, 130–156. [Google Scholar]
- Thangavel, P.; Park, D.; Lee, Y.-C. Recent insights into particulate matter (PM2. 5)-mediated toxicity in humans: an overview. International journal of environmental research and public health 2022, 19, 7511. [Google Scholar]
- Nozza, E.; Valentini, S.; Melzi, G.; Vecchi, R.; Corsini, E. Advances on the immunotoxicity of outdoor particulate matter: A focus on physical and chemical properties and respiratory defence mechanisms. Science of The Total Environment 2021, 780, 146391. [Google Scholar]
- Rao, X.; Zhong, J.; Brook, R.D.; Rajagopalan, S. Effect of particulate matter air pollution on cardiovascular oxidative stress pathways. Antioxidants & redox signaling 2018, 28, 797–818. [Google Scholar]
- Kelly, F.J.; Fussell, J.C. Role of oxidative stress in cardiovascular disease outcomes following exposure to ambient air pollution. Free Radical Biology and Medicine 2017, 110, 345–367. [Google Scholar]
- Chen, R.; Hu, B.; Liu, Y.; Xu, J.; Yang, G.; Xu, D.; Chen, C. Beyond PM2. 5: The role of ultrafine particles on adverse health effects of air pollution. Biochimica et Biophysica Acta (BBA)-General Subjects 2016, 1860, 2844–2855. [Google Scholar] [CrossRef]
- Calderón-Garcidueñas, L.; Hernández-Luna, J.; Aiello-Mora, M.; Brito-Aguilar, R.; Evelson, P.A.; Villarreal-Ríos, R.; Torres-Jardón, R.; Ayala, A.; Mukherjee, P.S. APOE peripheral and brain impact: APOE4 carriers accelerate their Alzheimer continuum and have a high risk of suicide in PM2. 5 polluted cities. Biomolecules 2023, 13, 927. [Google Scholar]
- Gangwar, R.S.; Bevan, G.H.; Palanivel, R.; Das, L.; Rajagopalan, S. Oxidative stress pathways of air pollution mediated toxicity: Recent insights. Redox biology 2020, 34, 101545. [Google Scholar]
- Dhir, A.; Suphathamwit, A. Transplant patients. In Anesthesia and Perioperative Care of the High-Risk Patient, Third Edition; Cambridge University Press: 2014; pp. 444-461.
- Perico, N.; Casiraghi, F.; Cortinovis, M.; Remuzzi, G. A Modern View of Transplant Immunology and Immunosuppression. In Contemporary Lung Transplantation; Springer: 2024; pp. 1-30.
- Arias-Pérez, R.D.; Taborda, N.A.; Gómez, D.M.; Narvaez, J.F.; Porras, J.; Hernandez, J.C. Inflammatory effects of particulate matter air pollution. Environmental Science and Pollution Research 2020, 27, 42390–42404. [Google Scholar] [PubMed]
- Hill, G.R.; Betts, B.C.; Tkachev, V.; Kean, L.S.; Blazar, B.R. Current concepts and advances in graft-versus-host disease immunology. Annual review of immunology 2021, 39, 19–49. [Google Scholar]
- Feng, Y.; Jones, M.R.; Ahn, J.B.; Garonzik-Wang, J.M.; Segev, D.L.; McAdams-DeMarco, M. Ambient air pollution and posttransplant outcomes among kidney transplant recipients. American Journal of Transplantation 2021, 21, 3333–3345. [Google Scholar]
- Ma, J.; Chiu, Y.-F.; Kao, C.-C.; Chuang, C.-N.; Chen, C.-Y.; Lai, C.-H.; Kuo, M.-L. Fine particulate matter manipulates immune response to exacerbate microbial pathogenesis in the respiratory tract. European Respiratory Review 2024, 33. [Google Scholar]
- Zaręba, Ł.; Piszczatowska, K.; Dżaman, K.; Soroczynska, K.; Motamedi, P.; Szczepański, M.J.; Ludwig, N. The relationship between fine particle matter (PM2. 5) exposure and upper respiratory tract diseases. Journal of Personalized Medicine 2024, 14, 98. [Google Scholar] [PubMed]
- Elalouf, A.; Yaniv-Rosenfeld, A.; Maoz, H. Immune response against bacterial infection in organ transplant recipients. Transplant Immunology 2024, 102102. [Google Scholar]
- Allen, U.D.; Preiksaitis, J.K.; Practice, A.I.D.C.o. Post-transplant lymphoproliferative disorders, Epstein-Barr virus infection, and disease in solid organ transplantation: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clinical transplantation 2019, 33, e13652. [Google Scholar]
- Moore, E.A. Autoimmune diseases and their environmental triggers; McFarland: 2015.
- Mpakosi, A.; Cholevas, V.; Tzouvelekis, I.; Passos, I.; Kaliouli-Antonopoulou, C.; Mironidou-Tzouveleki, M. Autoimmune diseases following environmental disasters: a narrative review of the literature. In Proceedings of the Healthcare; 2024; p. 1767. [Google Scholar]
- Ibironke, O. Air Pollution Particulate Matter Effects on Adaptive Human Antimycobacterial Immunity. Rutgers The State University of New Jersey, School of Graduate Studies, 2019.
- Slepicka, P.F.; Yazdanifar, M.; Bertaina, A. Harnessing mechanisms of immune tolerance to improve outcomes in solid organ transplantation: a review. Frontiers in Immunology 2021, 12, 688460. [Google Scholar]
- Han, F.; Yang, X.; Xu, D.; Wang, Q.; Xu, D. Association between outdoor PM2. 5 and prevalence of COPD: A systematic review and meta-analysis. Postgraduate Medical Journal 2019, 95, 612–618. [Google Scholar]
- Amubieya, O.; Weigt, S.; Shino, M.Y.; Jackson, N.J.; Belperio, J.; Ong, M.K.; Norris, K. Ambient air pollution exposure and outcomes in patients receiving lung transplant. JAMA Network Open 2024, 7, e2437148–e2437148. [Google Scholar] [PubMed]
- Dizdar, O.S. Pneumonia after kidney transplant: incidence, risk factors, and mortality. 2014.
- Giannella, M.; Muñoz, P.; Alarcón, J.; Mularoni, A.; Grossi, P.; Bouza, E.; Group, P.S. Pneumonia in solid organ transplant recipients: a prospective multicenter study. Transplant Infectious Disease 2014, 16, 232–241. [Google Scholar] [CrossRef]
- Pompilio, A.; Di Bonaventura, G. Ambient air pollution and respiratory bacterial infections, a troubling association: epidemiology, underlying mechanisms, and future challenges. Critical Reviews in Microbiology 2020, 46, 600–630. [Google Scholar] [CrossRef]
- Lippmann, M. Toxicological and epidemiological studies of cardiovascular effects of ambient air fine particulate matter (PM2. 5) and its chemical components: coherence and public health implications. Critical reviews in toxicology 2014, 44, 299–347. [Google Scholar] [PubMed]
- Di Maira, T.; Little, E.C.; Berenguer, M. Immunosuppression in liver transplant. Best Practice & Research Clinical Gastroenterology 2020, 46, 101681. [Google Scholar]
- Pope, C.A.; Bhatnagar, A. Does air pollution increase risk of mortality after cardiac transplantation? 2019, 74, 3036-3038.
- Dhanasekaran, R. Management of immunosuppression in liver transplantation. Clinics in liver disease 2017, 21, 337–353. [Google Scholar] [CrossRef]
- Deng, H.; Eckel, S.P.; Liu, L.; Lurmann, F.W.; Cockburn, M.G.; Gilliland, F.D. Particulate matter air pollution and liver cancer survival. International journal of cancer 2017, 141, 744–749. [Google Scholar]
- Yang, L.; Li, C.; Tang, X. The impact of PM2. 5 on the host defense of respiratory system. Frontiers in cell and developmental biology 2020, 8, 91. [Google Scholar]
- Shahbaz, M.A.; Martikainen, M.-V.; Rönkkö, T.J.; Komppula, M.; Jalava, P.I.; Roponen, M. Urban air PM modifies differently immune defense responses against bacterial and viral infections in vitro. Environmental Research 2021, 192, 110244. [Google Scholar]
- Xin, S.; Qu, J.; Xu, N.; Xu, B. PM2. 5 inhalation aggravates inflammation, oxidative stress, and apoptosis in nonalcoholic fatty liver disease. Environmental Disease 2019, 4, 62–68. [Google Scholar]
- Ge, C.; Tan, J.; Zhong, S.; Lai, L.; Chen, G.; Zhao, J.; Yi, C.; Wang, L.; Zhou, L.; Tang, T. Nrf2 mitigates prolonged PM2. 5 exposure-triggered liver inflammation by positively regulating SIKE activity: Protection by Juglanin. Redox biology 2020, 36, 101645. [Google Scholar]
- Yue, D.; Zhang, Q.; Zhang, J.; Liu, W.; Chen, L.; Wang, M.; Li, R.; Qin, S.; Song, X.; Ji, Y. Diesel exhaust PM2. 5 greatly deteriorates fibrosis process in pre-existing pulmonary fibrosis via ferroptosis. Environment international 2023, 171, 107706. [Google Scholar]
- Ghezzi, P.; Floridi, L.; Boraschi, D.; Cuadrado, A.; Manda, G.; Levic, S.; D'Acquisto, F.; Hamilton, A.; Athersuch, T.J.; Selley, L. Oxidative stress and inflammation induced by environmental and psychological stressors: a biomarker perspective. Antioxidants & redox signaling 2018, 28, 852–872. [Google Scholar]
- Ravindranath, M.H.; El Hilali, F.; Filippone, E.J. The impact of inflammation on the immune responses to transplantation: tolerance or rejection? Frontiers in Immunology 2021, 12, 667834. [Google Scholar]
- Chang, S.-H.; Merzkani, M.; Murad, H.; Wang, M.; Bowe, B.; Lentine, K.L.; Al-Aly, Z.; Alhamad, T. Association of ambient fine particulate matter air pollution with kidney transplant outcomes. JAMA network Open 2021, 4, e2128190–e2128190. [Google Scholar]
- Salvadori, M.; Rosso, G.; Bertoni, E. Update on ischemia-reperfusion injury in kidney transplantation: Pathogenesis and treatment. World journal of transplantation 2015, 5, 52. [Google Scholar]
- Franzin, R.; Stasi, A.; Fiorentino, M.; Stallone, G.; Cantaluppi, V.; Gesualdo, L.; Castellano, G. Inflammaging and complement system: a link between acute kidney injury and chronic graft damage. Frontiers in immunology 2020, 11, 734. [Google Scholar]
- Marroquin, C.E. Patient selection for kidney transplant. Surgical Clinics 2019, 99, 1–35. [Google Scholar] [PubMed]
- Wang, M.; Yang, J.; Fang, X.; Lin, W.; Yang, Y. Membranous nephropathy: pathogenesis and treatments. MedComm 2024, 5, e614. [Google Scholar]
- Yi, J.; Kim, S.H.; Lee, H.; Chin, H.J.; Park, J.Y.; Jung, J.; Song, J.; Kwak, N.; Ryu, J.; Kim, S. Air quality and kidney health: Assessing the effects of PM10, PM2. 5, CO, and NO2 on renal function in primary glomerulonephritis. Ecotoxicology and Environmental Safety 2024, 281, 116593. [Google Scholar]
- Zhang, Y.; Liu, D.; Liu, Z. Fine particulate matter (PM2. 5) and chronic kidney disease. Reviews of Environmental Contamination and Toxicology Volume 254 2021, 183-215.
- An, Y.; Liu, Z.-H. Air pollution and kidney diseases: PM2. 5 as an emerging culprit. Nephrology and Public Health Worldwide 2021, 199, 274–284. [Google Scholar]
- Chen, Y.; Cao, F.; Xiao, J.-P.; Fang, X.-Y.; Wang, X.-R.; Ding, L.-H.; Wang, D.-G.; Pan, H.-F. Emerging role of air pollution in chronic kidney disease. Environmental Science and Pollution Research 2021, 28, 52610–52624. [Google Scholar] [PubMed]
- Neuberger, J.M.; Bechstein, W.O.; Kuypers, D.R.; Burra, P.; Citterio, F.; De Geest, S.; Duvoux, C.; Jardine, A.G.; Kamar, N.; Krämer, B.K. Practical recommendations for long-term management of modifiable risks in kidney and liver transplant recipients: a guidance report and clinical checklist by the consensus on managing modifiable risk in transplantation (COMMIT) group. Transplantation 2017, 101, S1–S56. [Google Scholar]
- Li, Q.; Lan, P. Activation of immune signals during organ transplantation. Signal transduction and targeted therapy 2023, 8, 110. [Google Scholar] [PubMed]
- Phillips, B.L.; Callaghan, C. The immunology of organ transplantation. Surgery (Oxford) 2017, 35, 333–340. [Google Scholar]
- Peruzzi, L.; Cocchi, E. Transplant Immunobiology. In Pediatric Solid Organ Transplantation: A Practical Handbook; Springer: 2023; pp. 19-44.
- Fu, H.; Liu, X.; Li, W.; Zu, Y.; Zhou, F.; Shou, Q.; Ding, Z. PM2. 5 exposure induces inflammatory response in macrophages via the TLR4/COX-2/NF-κB pathway. Inflammation 2020, 43, 1948–1958. [Google Scholar]
- Turner, M.D.; Nedjai, B.; Hurst, T.; Pennington, D.J. Cytokines and chemokines: At the crossroads of cell signalling and inflammatory disease. Biochimica et Biophysica Acta (BBA)-Molecular Cell Research 2014, 1843, 2563–2582. [Google Scholar]
- de Morales, J.M.G.R.; Puig, L.; Daudén, E.; Cañete, J.D.; Pablos, J.L.; Martín, A.O.; Juanatey, C.G.; Adán, A.; Montalbán, X.; Borruel, N. Critical role of interleukin (IL)-17 in inflammatory and immune disorders: An updated review of the evidence focusing in controversies. Autoimmunity reviews 2020, 19, 102429. [Google Scholar]
- Veldhoen, M. Interleukin 17 is a chief orchestrator of immunity. Nature immunology 2017, 18, 612–621. [Google Scholar]
- Ponticelli, C.; Campise, M.R. The inflammatory state is a risk factor for cardiovascular disease and graft fibrosis in kidney transplantation. Kidney International 2021, 100, 536–545. [Google Scholar] [PubMed]
- Steen, E.H.; Wang, X.; Balaji, S.; Butte, M.J.; Bollyky, P.L.; Keswani, S.G. The role of the anti-inflammatory cytokine interleukin-10 in tissue fibrosis. Advances in wound care 2020, 9, 184–198. [Google Scholar] [CrossRef]
- Marino, J.; Paster, J.; Benichou, G. Allorecognition by T lymphocytes and allograft rejection. Frontiers in immunology 2016, 7, 582. [Google Scholar] [CrossRef] [PubMed]
- Duneton, C.; Winterberg, P.D.; Ford, M.L. Activation and regulation of alloreactive T cell immunity in solid organ transplantation. Nature Reviews Nephrology 2022, 18, 663–676. [Google Scholar] [PubMed]
- Zhuang, Q.; Liu, Q.; Divito, S.J.; Zeng, Q.; Yatim, K.M.; Hughes, A.D.; Rojas-Canales, D.M.; Nakao, A.; Shufesky, W.J.; Williams, A.L. Graft-infiltrating host dendritic cells play a key role in organ transplant rejection. Nature communications 2016, 7, 12623. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Gong, C.; Ying, L.; Fu, W.; Liu, S.; Dai, J.; Fu, Z. PM 2.5 affects establishment of immune tolerance in newborn mice by reducing PD-L1 expression. Journal of biosciences 2019, 44, 1–8. [Google Scholar]
- Wang, C.; Wang, J.; Zheng, X.; Zhang, J.; Zhang, J.; Qiao, G.; Liu, H.; Zhao, H.; Bai, J.; Zhang, H. Epigenetic regulation is involved in traffic-related PM2. 5 aggravating allergic airway inflammation in rats. Clinical Immunology 2022, 234, 108914. [Google Scholar] [CrossRef]
- Venosa, A. Senescence in pulmonary fibrosis: between aging and exposure. Frontiers in medicine 2020, 7, 606462. [Google Scholar]
- Vannella, K.M.; Wynn, T.A. Mechanisms of organ injury and repair by macrophages. Annual review of physiology 2017, 79, 593–617. [Google Scholar] [CrossRef]
- Oishi, Y.; Manabe, I. Macrophages in inflammation, repair and regeneration. International immunology 2018, 30, 511–528. [Google Scholar]
- Yunna, C.; Mengru, H.; Lei, W.; Weidong, C. Macrophage M1/M2 polarization. European journal of pharmacology 2020, 877, 173090. [Google Scholar]
- Alvarez, M.M.; Liu, J.C.; Trujillo-de Santiago, G.; Cha, B.-H.; Vishwakarma, A.; Ghaemmaghami, A.M.; Khademhosseini, A. Delivery strategies to control inflammatory response: Modulating M1–M2 polarization in tissue engineering applications. Journal of Controlled Release 2016, 240, 349–363. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, S.; Al-Kindi, S.G.; Brook, R.D. Air pollution and cardiovascular disease: JACC state-of-the-art review. Journal of the American College of Cardiology 2018, 72, 2054–2070. [Google Scholar] [CrossRef] [PubMed]
- Tanwar, V.; Gorr, M.W.; Velten, M.; Eichenseer, C.M.; Long III, V.P.; Bonilla, I.M.; Shettigar, V.; Ziolo, M.T.; Davis, J.P.; Baine, S.H. In utero particulate matter exposure produces heart failure, electrical remodeling, and epigenetic changes at adulthood. Journal of the American heart association 2017, 6, e005796. [Google Scholar] [CrossRef] [PubMed]
- Ochando, J.; Ordikhani, F.; Jordan, S.; Boros, P.; Thomson, A.W. Tolerogenic dendritic cells in organ transplantation. Transplant International 2020, 33, 113–127. [Google Scholar] [CrossRef]
- Li, H.; Shi, B. Tolerogenic dendritic cells and their applications in transplantation. Cellular & molecular immunology 2015, 12, 24–30. [Google Scholar]
- Zhuang, Q.; Lakkis, F.G. Dendritic cells and innate immunity in kidney transplantation. Kidney international 2015, 87, 712–718. [Google Scholar] [CrossRef]
- Moya-Guzmán, M.J.; de Solminihac, J.; Padilla, C.; Rojas, C.; Pinto, C.; Himmel, T.; Pino-Lagos, K. Extracellular vesicles from immune cells: A biomedical perspective. International Journal of Molecular Sciences 2023, 24, 13775. [Google Scholar] [CrossRef]
- Yu, S.; Lu, J. Macrophages in transplant rejection. Transplant Immunology 2022, 71, 101536. [Google Scholar] [CrossRef]
- Hakim, F.T.; Memon, S.; Jin, P.; Imanguli, M.M.; Wang, H.; Rehman, N.; Yan, X.-Y.; Rose, J.; Mays, J.W.; Dhamala, S. Upregulation of IFN-inducible and damage-response pathways in chronic graft-versus-host disease. The Journal of Immunology 2016, 197, 3490–3503. [Google Scholar] [CrossRef]
- Safinia, N.; Scotta, C.; Vaikunthanathan, T.; Lechler, R.I.; Lombardi, G. Regulatory T cells: serious contenders in the promise for immunological tolerance in transplantation. Frontiers in immunology 2015, 6, 438. [Google Scholar] [CrossRef]
- Lee, C.-F.; Lo, Y.-C.; Cheng, C.-H.; Furtmüller, G.J.; Oh, B.; Andrade-Oliveira, V.; Thomas, A.G.; Bowman, C.E.; Slusher, B.S.; Wolfgang, M.J. Preventing allograft rejection by targeting immune metabolism. Cell reports 2015, 13, 760–770. [Google Scholar]
- Tang, Q.; Vincenti, F. Transplant trials with Tregs: perils and promises. The Journal of clinical investigation 2017, 127, 2505–2512. [Google Scholar] [PubMed]
- Huang, D.-L.; He, Y.-R.; Liu, Y.-J.; He, H.-Y.; Gu, Z.-Y.; Liu, Y.-M.; Liu, W.-J.; Luo, Z.; Ju, M.-J. The immunomodulation role of Th17 and Treg in renal transplantation. Frontiers in immunology 2023, 14, 1113560. [Google Scholar] [PubMed]
- Tejchman, K.; Kotfis, K.; Sieńko, J. Biomarkers and mechanisms of oxidative stress—last 20 years of research with an emphasis on kidney damage and renal transplantation. International journal of molecular sciences 2021, 22, 8010. [Google Scholar]
- Matyas, C.; Haskó, G.; Liaudet, L.; Trojnar, E.; Pacher, P. Interplay of cardiovascular mediators, oxidative stress and inflammation in liver disease and its complications. Nature Reviews Cardiology 2021, 18, 117–135. [Google Scholar]
- Liu, H.; Lai, W.; Nie, H.; Shi, Y.; Zhu, L.; Yang, L.; Tian, L.; Li, K.; Bian, L.; Xi, Z. PM2. 5 triggers autophagic degradation of Caveolin-1 via endoplasmic reticulum stress (ERS) to enhance the TGF-β1/Smad3 axis promoting pulmonary fibrosis. Environment international 2023, 181, 108290. [Google Scholar] [PubMed]
- Xu, M.-X.; Ge, C.-X.; Qin, Y.-T.; Gu, T.-T.; Lou, D.-S.; Li, Q.; Hu, L.-F.; Feng, J.; Huang, P.; Tan, J. Prolonged PM2. 5 exposure elevates risk of oxidative stress-driven nonalcoholic fatty liver disease by triggering increase of dyslipidemia. Free Radical Biology and Medicine 2019, 130, 542–556. [Google Scholar]
- Xu, Z.; Li, Z.; Liao, Z.; Gao, S.; Hua, L.; Ye, X.; Wang, Y.; Jiang, S.; Wang, N.; Zhou, D. PM2. 5 induced pulmonary fibrosis in vivo and in vitro. Ecotoxicology and environmental safety 2019, 171, 112–121. [Google Scholar]
- Angelico, R.; Sensi, B.; Manzia, T.M.; Tisone, G.; Grassi, G.; Signorello, A.; Milana, M.; Lenci, I.; Baiocchi, L. Chronic rejection after liver transplantation: Opening the Pandora’s box. World journal of gastroenterology 2021, 27, 7771. [Google Scholar] [CrossRef]
- Wu, H.; Wang, D.; Shi, H.; Liu, N.; Wang, C.; Tian, J.; Wang, X.; Zhang, Z. PM2. 5 and water-soluble components induce airway fibrosis through TGF-β1/Smad3 signaling pathway in asthmatic rats. Molecular Immunology 2021, 137, 1–10. [Google Scholar]
- Pryor, J.T.; Cowley, L.O.; Simonds, S.E. The physiological effects of air pollution: particulate matter, physiology and disease. Frontiers in Public Health 2022, 10, 882569. [Google Scholar] [CrossRef]
- Li, R.; Zhou, R.; Zhang, J. Function of PM2. 5 in the pathogenesis of lung cancer and chronic airway inflammatory diseases. Oncology letters 2018, 15, 7506–7514. [Google Scholar] [PubMed]
- Marín-Palma, D.; Fernandez, G.J.; Ruiz-Saenz, J.; Taborda, N.A.; Rugeles, M.T.; Hernandez, J.C. Particulate matter impairs immune system function by up-regulating inflammatory pathways and decreasing pathogen response gene expression. Scientific Reports 2023, 13, 12773. [Google Scholar] [CrossRef] [PubMed]
- Boor, P.; Floege, J. Renal allograft fibrosis: biology and therapeutic targets. American journal of transplantation 2015, 15, 863–886. [Google Scholar] [PubMed]
- Bhattarai, G.; Shrestha, S.K.; Sim, H.-J.; Lee, J.-C.; Kook, S.-H. Effects of fine particulate matter on bone marrow-conserved hematopoietic and mesenchymal stem cells: a systematic review. Experimental & Molecular Medicine 2024, 56, 118–128. [Google Scholar]
- Rajagopalan, S.; Brauer, M.; Bhatnagar, A.; Bhatt, D.L.; Brook, J.R.; Huang, W.; Münzel, T.; Newby, D.; Siegel, J.; Brook, R.D. Personal-level protective actions against particulate matter air pollution exposure: a scientific statement from the American Heart Association. Circulation 2020, 142, e411–e431. [Google Scholar]
- Zafar, S.; Fatima, S.; Asad, F.; Nazir, M.M.; Batool, S.; Ashraf, A. Combating Lead (Pb) Contamination: Integrating Biomonitoring, Advanced Detection, and Remediation for Environmental and Public Health. Water, Air, & Soil Pollution 2025, 236, 8. [Google Scholar]

| Immune Component | Effect of PM2.5 |
|---|---|
| Regulatory T Cells (Tregs) | Suppressed, reducing immune tolerance |
| Pro-inflammatory Cytokines | Elevated TNF-α, IL-6, IL-1β |
| Oxidative Stress Markers | Increased ROS production leading to DNA damage |
| Epigenetic Changes | Histone modifications affecting immune gene expression |
Table 2.
Key Molecules and their Mechanisms affecting Immune System.
| Mechanism | Description | Key Molecule(s) | Impact on Immune System |
|---|---|---|---|
| PM2.5-induced Treg Dysfunction | Disruption of regulatory T cell function | TGF-β, FoxP3 | Reduced immune tolerance |
| Dendritic Cell Dysfunction | Impaired antigen presentation and activation of T-cells | IL-10, IL-12 | Altered immune response |
| Oxidative Stress | Elevated reactive oxygen species (ROS) impairs immune function | ROS, NF-κB | Chronic inflammation |
| Cytokine Imbalance | Overproduction of pro-inflammatory cytokines | TNF-α, IL-6 | Immune dysregulation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



