Submitted:
19 February 2025
Posted:
20 February 2025
You are already at the latest version
Abstract
(1) Background: In Manitoba, most people get the HPV vaccine in the publicly-funded school-based program. If they miss the school-based program, they remain eligible for the free HPV immunization program. This study explored whether invitation and reminder letters would increase HPV vaccine uptake among adult women who remained eligible for the publicly-funded program. (2) Methods: Eligible individuals were randomized into three groups of 4,650 women. Intervention groups I and II were mailed an information package inviting them to be vaccinated. Six weeks later, intervention group II received a reminder letter if they remained unvaccinated. Vaccination status, defined as at least one dose of an approved HPV vaccine, was calculated six months after the packages were mailed. (3) Results: 4.0% of individuals in intervention group II (invitation/reminder) and 2.5% of individuals in intervention group I (invitation) received one dose of the HPV vaccine. Compared to the control group, sending invitation/reminder and invitation packages increased the likelihood of getting at least one dose of the HPV vaccine by 4.9 times (3.4 - 6.9) and 3.0 (2.1 - 4.4) times, respectively. (4) Conclusion: Sending invitation and reminder letters to unvaccinated women may be an effective and low-cost way to increase HPV vaccination coverage among adults who are eligible for the publicly-funded immunization program.
Keywords:
human papillomavirus
; HPV vaccine
; vaccine uptake
; elimination of cervical cancer
; vaccine interventions
1. Introduction
The HPV (human papillomavirus) vaccine is one of the most effective ways to prevent cancer. Not only can the vaccine prevent over 90% of cervical cancers, it can also reduce rates of vulvar, vaginal, anal, oropharyngeal, and penile cancers [1], as well as non-cancerous genital warts. In 2015, it was estimated that 3,829 cases of cancer in Canada were caused by HPV [2].
Manitoba is a province in central Canada with a population of about 1.34 million people. The low population density of 2.5 people per km2 [3] makes it challenging for everyone in the population to access health services. In 2008, Manitoba introduced a publicly-funded HPV vaccine program for girls born in 1997 or later. Immunizations are primarily offered in grade six (approximate age: 10-11 years) through a school-based program, though families can also access vaccines from their healthcare providers. In 2016, the HPV vaccine program became available to boys born in 2002 or later and is also primarily delivered in grade six through a school-based program [4].
Females born in 1997 and later are eligible to receive the HPV vaccine free of charge. Most girls receive the vaccine in the school-based program. However, since Manitoba maintains a once-eligible, always-eligible policy, individuals can be vaccinated even if they missed the school-based program or were opted out of the program by their parents [5]. This policy is uncommon in Canada; most jurisdictions have an age cut-off for HPV vaccine eligibility [6]. The Manitoba policy therefore provides an opportunity to reach eligible individuals once they become adults.
In 2022, Manitoba’s HPV vaccination coverage rate among females at age 17 was 70% [7]. This rate remains below the national target of 90% [8] and varies by region. Among vaccine-eligible adult women (born 1997-2002), approximately 29% have had zero doses of the HPV vaccine [9]. The initial vaccination decisions were made by parents. Now that some of the vaccine-eligible cohort has reached adulthood, they could be informed of their eligibility and access options and make an informed decision about vaccination for themselves.
Invitation letters have been demonstrated to be effective in the use of other health services, such as cancer screening [10,11,12,13,14,15] and immunization [16,17] uptake. However, to our knowledge, invitation letters have not been used to remind adults of their continued eligibility for a childhood vaccine. This project investigated the association between mailed invitation and reminder letters with subsequent HPV vaccination among eligible adult women who were unvaccinated.
2. Materials and Methods
This study targeted adult women who had received zero doses of the HPV vaccine but were still eligible for the publicly-funded HPV immunization program. This included women aged 20 years and older, who were born in 1997 or later.
2.1. Study Group Selection
The potential study sample was generated from data contained within the CervixCheck registry. CervixCheck is the population-based cervical screening program in Manitoba. Its database registry includes the names and addresses of all adult females in the province, as well as their health histories related to cervical cancer screening and follow-up, HPV vaccination, hysterectomy, and cervical cancer.
A sample size calculation was completed to determine group sizes. To obtain 80% power, a sample size of 1200 individuals, evenly distributed across the three groups, would be needed to detect a difference at a 5% level of significance. However, bigger group sizes were selected to increase the potential HPV vaccine uptake rate.
Approximately 14,000 women who met the study inclusion criteria were randomized into three study groups. Intervention group I included 4,650 women who were mailed an invitation letter. Intervention group II included 4,650 women who were mailed an invitation letter, and if needed, a reminder letter. The control group included 4,650 women who received no correspondence related to HPV vaccination. The protocol is shown in Figure 1.
People were included in the potential study sample if they met the following inclusion criteria:
- Have had zero doses of an approved HPV vaccine
- At least 20 years old and born in 1997 or later
- Female sex, as identified on their Manitoba Health card
- Valid Manitoba health insurance coverage and a complete Manitoba mailing address
People were excluded from the potential study sample if they met the following exclusion criteria:
- Have received one or more doses of an approved HPV vaccine
- Have had cervical cancer
- Have had a hysterectomy
- In active colposcopy treatment
The sample groups were derived using random allocation. First, the population of women in the registry who met the study inclusion and exclusion criteria were identified. Then, women were assigned to a study arm using restricted randomization to achieve the desired sample sizes. Random selection was done using SAS version 9.4 (SAS Institute Inc., Cary, NC).
2.2. Mail-Outs
In May 2023, invitation packages were mailed to women in Intervention Groups I & II. In June 2023, reminder packages were sent to women in Intervention Group II who had not yet been vaccinated. The packages, including their content, design, and branding, were developed in consultation with public advisors via in-person discussion and online survey. They included a bilingual (English and French) invitation letter and an educational insert in the form of frequently asked questions. The reminder package included a bilingual reminder letter.
The initial groups included 4,650 women each (13,950 total). However, subsequent analyses revealed that several people were included in the groups inappropriately due to delayed data entry or becoming ineligible within the 6-month study period. Final group sizes and reasons for exclusion are shown in Figure 2.
2.3. Assessing Intervention Response
To determine whether the invitation letters increased vaccine uptake among adult women, vaccination status was measured six months after the information packages were mailed. The six-month timeframe was selected to limit when the behaviour could potentially be attributed to the invitation. Women who received at least one dose of an approved HPV vaccine within six months of the invitation were counted as having been vaccinated. Given limited access to primary care throughout Manitoba, a subsequent analysis was done extending the follow-up timeframe to twelve months.
A chi-square test of homogeneity was performed to determine whether HPV vaccination uptake differed across the three study groups and logistic regression was used to assess the strength of the relationship between the dependent variable (vaccine uptake) and the independent variable (study arm). Analyses were done using SAS version 9.4 (SAS Institute Inc., Cary, NC).
This study was approved by the University of Manitoba’s Health Research Ethics Board (HS25709, H2022:325) and CancerCare Manitoba’s Research Review Impact Committee (2022-028).
3. Results
3.1. Cohort Demographics
Group demographics are shown in Table 1. There were no differences between the groups with respect to age, geography, or cervical cancer screening status.
3.2. Six-Month HPV Vaccine Uptake
Table 2 shows the results of vaccine uptake within six months of the invitation mailing date. Of the individuals who received an invitation and reminder letter, 4.0% received at least one dose of the HPV vaccine. Of the individuals who only received the invitation letter, 2.5% received had at least one dose of the HPV vaccine, compared to only 0.9% of the control group. The difference between the groups was statistically significant at a 5% level of significance (X2 = 91.1, p < 0.001).
Logistic regression was completed to determine the effect size (see Table 3). Compared to the control group, sending an invitation package increased the likelihood of getting at least one dose of HPV vaccine by 3.0 times. Compared to the control group, sending invitation and reminder packages increased the likelihood of getting the vaccine by 4.9 times.
3.3. Twelve-Month HPV Vaccine Uptake
The vaccine uptake pattern observed over six months was the same as what was observed over 12 months: individuals who received the invitation and reminder letters were most likely to get an HPV vaccine, followed by individuals who only received an invitation letter, and then those in the control group. All groups had higher proportions of HPV uptake over 12 months compared to six months (see Table 4). The differences between the intervention and control groups remained statistically significant at a 5% level of significance (X2 = 78.9, p < 0.001).
Logistic regression was completed to determine the effect size within 12 months (see Table 5). Compared to the control group, sending an invitation package increased the likelihood of getting at least one dose of HPV vaccine by 2.3 times. Compared to the control group, sending invitation and reminder packages increased the likelihood of getting the vaccine by 3.2 times.
4. Discussion
The World Health Organization has called for the elimination cervical cancer through improvements in three key areas: HPV vaccination, cervical cancer screening, and treatment [18]. This project explored whether invitation and reminder letters to unvaccinated adult women could impact the first area by increasing HPV vaccine uptake.
Unvaccinated individuals, those who were not vaccinated in the publicly-funded school-based program, were targeted for the study. The reason for their vaccination status is not known; it could have been the result of an intentional decision by their parents/guardians (e.g., based on their values or preferences about immunization), or an unintentional decision (e.g., the result of a practical or structural barrier). Additionally, they could have moved into the province at a later age, thereby missing the school-based program. Regardless of their initial reason, this project sought to determine whether reminding unvaccinated adult women of their ongoing eligibility for the publicly-funded program could increase HPV vaccination coverage.
4.1. Main Findings
While this study found a relatively low HPV vaccine uptake among the groups (4.0% among people who received invitation and reminder letters and 2.5% among people who only received the invitation letters), a significant difference was observed between the groups. Compared to the control group, the invitation/reminder group was 4.9 times as likely to receive at least one dose of an HPV vaccine within six months and the invitation group was 3.0 times as likely. This demonstrates that a relatively simple and low-cost intervention can be effective at increasing HPV vaccine rates among unvaccinated adult women.
The cost of sending letters is very small compared to the potential long-term impact of a well-vaccinated population. The HPV vaccine is highly effective at preventing HPV-related cancers. With good population coverage, the need for follow-up and treatment for cancer and pre-cancerous lesions could be significantly reduced, eventually decreasing morbidity and mortality from HPV cancers.
4.2. Strengths and Limitations
One of the key strengths of this study is the robust cervical cancer screening registry in Manitoba. Having access to the population-based registry allowed us to determine vaccine status and eligibility for the publicly-funded program, and allow targeted invitation and reminder letters to be sent.
Even though registry data is updated frequently, it was necessary to adjust for late data entry. Several health records were updated after the study groups were identified. That was accounted for by removing from analysis the individuals who became eligible for the study. Additionally, over 500 information packages were returned due to incorrect addresses, which might relate to increased address mobility among the age cohort.
Additionally, while the odds ratios were quite large (people in the intervention groups were 4.9 and 3.0 times as likely to get an HPV vaccine compared to the control group), the net uptake in each group was small (4.0% and 2.5% increases). The large study sample size may have exaggerated the small differences and found them to be statistically significant. Regardless, the small increases observed in this study were expected, given that the cohort had likely rejected a vaccine offer on at least one previous occasion.
Finally, there was no controlling for potential confounding variables in this study, such as proximity to healthcare services, rurality, or past healthcare use. Further study may be required to determine whether the vaccine invitation strategy should differ based on demographic, geographic, or other factors.
4.3. Future Directions
Due to its relative low-cost and low-effort, it is likely that invitation and reminder letters for unvaccinated women will be incorporated into routine operations in Manitoba. However, more research is needed to determine the optimal timing of the letters (e.g., age at which they should be mailed), how many letters/reminders to send, and the content of the invitation packages. It would also be valuable to consider the impact of sending invitation/reminder letters to under-vaccinated people who remain eligible for the publicly-funded program.
Additionally, further research is needed to investigate the different impact of letters among different geographic regions in the province. For example, it was observed that vaccination uptake was highest in the most urban health region and among individuals living in urban postal codes. This might be due to improved vaccine access in urban areas or different values and preferences among people in those areas. Different interventions might be needed to improve HPV vaccine uptake in different areas of the province.
Finally, there were anecdotal reports of people being unable to access HPV vaccines from their healthcare providers. Additional efforts are needed to ensure knowledge among health care providers about the vaccine program, and in particular, the once eligible, always eligible policy.
5. Conclusions
Sending invitation and reminder letters to unvaccinated women may be an effective and low-cost way to increase HPV vaccination coverage among the population eligible for the publicly-funded immunization program. More research is needed to refine the invitation packages and determine the optimal timing and frequency of the letters and whether the invitation strategy should differ based on demographic, geographic, or other factors.
Author Contributions
Conceptualization, KB, DT, LC; methodology, KB and LC; formal analysis, CJ, CK, AH; writing—original draft preparation, KB; writing—review and editing, LC, DT, CJ, CK, AH; supervision, DT; project administration, LC; funding acquisition, KB. All authors have read and agreed to the published version of the manuscript.
Funding
This work was partially funded by the CancerCare Manitoba Foundation.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the University of Manitoba Health Research Ethics Board (ethics #: HS25709, H2022:325, November 14, 2022). The CancerCare Manitoba Research Review Impact Committee approved this study (RRIC #: 2022-28, December 12, 2022). Ethical review and approval were waived by the Provincial Health Research Privacy Committee because, as a trustee of the cancer screening registries, CancerCare Manitoba can use the information in the registries as authorized under the Personal Health Information Act.
Informed Consent Statement
Patient consent was waived because mailing educational information fits within CervixCheck’s usual activities and is done in accordance with Manitoba Regulation 31/2009 of the Public Health Act. Per usual operations, individuals can decline to receive correspondence from CervixCheck by contacting the program. If participants chose to obtain the HPV vaccine, immunization consent occurred according to usual processes between the healthcare provider (physician, nurse, or pharmacist) and the participant.
Data Availability Statement
The data associated with this study are not publicly available. This ensures the privacy and confidentiality of personal health information, in accordance with Manitoba’s Personal Health Information Act. The data may be made available to health researchers following guidelines established by CancerCare Manitoba’s Research and Resource Impact Committee (https://www.cancercare.mb.ca/Research/research-office/research-impact-commitee) and/or Manitoba Health’s Provincial Health Research Privacy Committee (https://www.rithim.ca/phrpc-overview).
Acknowledgments
We thank CancerCare Manitoba staff, including CervixCheck staff, who helped coordinate administrative study activities; the Prevention & Screening Education team, who helped develop public resources; and Epidemiology, who reviewed the study results and interpretation.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- National Advisory Committee on Immunization. Updated Recommendations on Human Papillomavirus (HPV) Vaccines: 9-valent HPV vaccine and clarification of minimum intervals between doses in the HPV immunization schedule. Public Health Agency of Canada: Ottawa, Canada, 2017.
- Canadian Cancer Society. Compare Study. The attributable risk of cancer in Canada. Available online: https://prevent.cancer.ca/ (accessed July 2024).
- Statistics Canada. Manitoba Population and dwelling counts. Focus on Geography Series, 2021 Census of Population. Available online: https://www12.statcan.gc.ca/census-recensement/2021/as-sa/fogs-spg/index.cfm (accessed July 2024).
- Manitoba Health and Seniors Care. Manitoba's School Immunization Program: Questions & Answers for Health Care Providers. Government of Manitoba. Accessed online: https://www.gov.mb.ca/health/publichealth/factsheets/mb_school_imms.pdf (accessed July 2024).
- Province of Manitoba. Manitoba's Immunization Program: Vaccines Offered Free-of-Charge. Available online: https://www.gov.mb.ca/health/publichealth/cdc/vaccineeligibility.html (accessed July 2024).
- Canadian Partnership Against Cancer. Eliminating cervical cancer in Canada: Improving HPV vaccination rates. Canadian Partnership Against Cancer. Available online: https://www.partnershipagainstcancer.ca/topics/eliminating-cervical-cancer/hpv-vaccination/ (accessed July 2024).
- Manitoba Health. Annual Report of Immunization Surveillance: Public Health Information Management System. Manitoba. Available online: https://www.gov.mb.ca/health/publichealth/surveillance/immunization/index.html (accessed July 2024).
- CancerCare Manitoba. HPV vaccine data in CervixCheck registry. Winnipeg, Canada: unpublished data, 2022.
- Bonfill X, Marzo M, Pladevall M, Martí J, Emparanza JI. Strategies for increasing women participation in community breast cancer screening. Cochrane Database Systematic Reviews January 2001. CD002943.
- E. Ferroni, L. Camilloni, B. Jimenez, G. Furnari, P. Borgia, G. Guasticchi, P. Giorgi Rossi. How to increase uptake in oncologic screening: A systematic review of studies comparing population-based screening programs and spontaneous access. Preventive Medicine, 2012, Vol. 55, pp. 587-596. [CrossRef]
- Jager M, Demb J, Asghar A, Selby K, Marquez Mello E, Heskett KM, Lieverman AJ, geng Z, Bharti B, Singh S, Gupta S. Mailed Outreach Is Superior to Usual Care Alone for Colorectal Cancer Screening in the USA: A Systematic Review and Meta-analysis. Dig Dis Sci, March 2019, Vol. 64, pp. 2489-2496. [CrossRef]
- Staley, Helen, et al. Interventions targeted at women to encourage the uptake of cervical screening. Cochrane Database of Systematic Reviews 2021 1465-1858.
- Dougherty MK, Brenner AT, Crockett SD, Gupta S, Wheeler SB, Coker-Schwimmer M, Cubillos L, Malo T, Reuland DS. Evaluation of Interventions Intended to Increase Colorectal Cancer Screening Rates in the United States: A Systematic Review and Meta-analysis. JAMA Intern Med 2018, 178, 1645–1658. [CrossRef] [PubMed]
- Camilloni L, Ferroni E, Cendales BJ, Pezzarossi A, Furnari G, Borgia P, Guasticchi G, Giorgi Rossi P and Methods to increase participation Working Group. Methods to increase participation in organised screening programs: a systematic review. BMC Public Health, 2013, Vol. 13. [CrossRef]
- Jacobson Vann JC, Jacobson RM, Coyne-Beasley T, Asafu-Adjei JK, Szilagyi PG. Patient reminder and recall interventions to improve immunization rates. Cochrane Database of Systematic Reviews, January 2018. [CrossRef]
- Szilagyi PG, Bordley C, Vann JC, Chelminski MD, Kraus RM, Margolis PA, Rodewald, LE. Effect of Patient Reminder/Recall Interventions on Immunization Rates: A Review. JAMA, 2000, Vol. 284, pp. 1820-1827. [CrossRef]
- World Health Organization. Cervical Cancer Elimination Initiative. World Health Organization. Available online: https://www.who.int/initiatives/cervical-cancer-elimination-initiative (accessed July 2024).
Figure 1.
Study protocol.
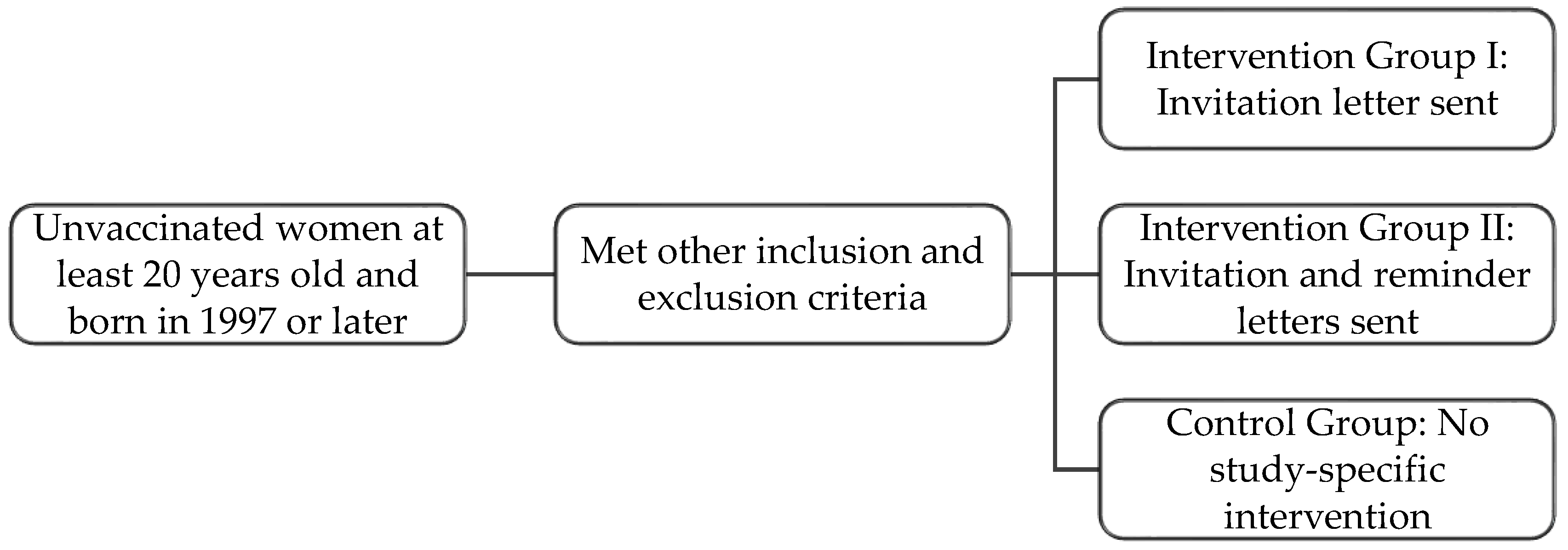
Figure 2.
Study group sizes and reasons for exclusion post-randomization.
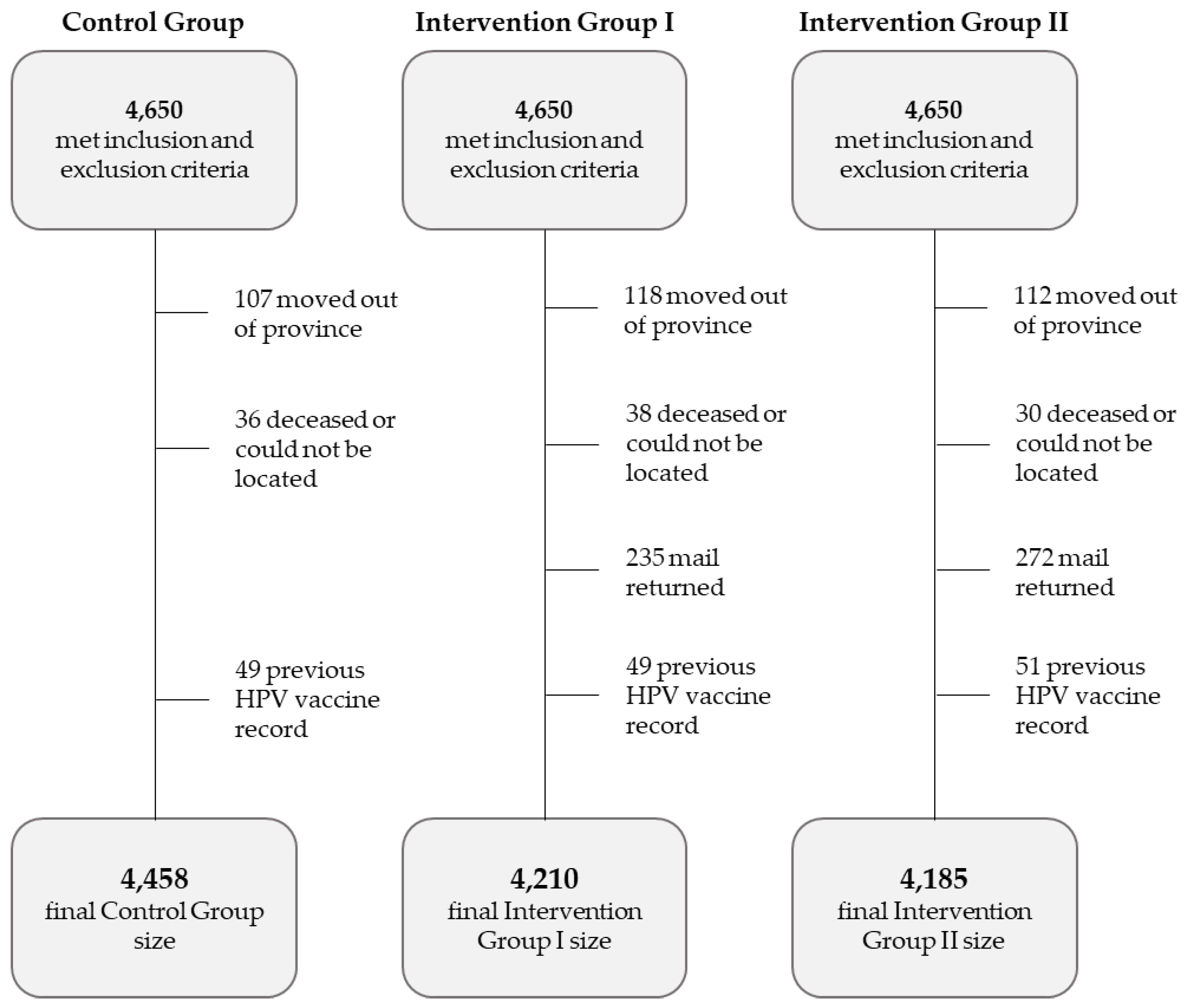

Table 1.
Cohort demographics.
| Control Group (No Study-Specific Letters) |
Intervention Group I: Invitation Letter |
Intervention Group II: Invitation Letter and Reminder Letter |
|
| Average age Age range |
23.1 years 20-26 years |
23.1 years 20-26 years |
23.2 years 20-26 years |
| Living in a rural region of the province | 23.4 % | 24.4% | 25.5% |
| Unscreened for cervical cancer* | 72.8% | 74.3% | 72.7% |
* Unscreened is defined as having no record of ever having had a Pap test.
Table 2.
HPV vaccine uptake among the control and intervention groups within six months of invitation.
Table 2.
HPV vaccine uptake among the control and intervention groups within six months of invitation.
| Control Group (No Study-Specific Letters) |
Intervention Group I: Invitation Letter |
Intervention Group II: Invitation Letter and Reminder Letter |
|
| Group size (met inclusion and exclusion criteria over six months of follow-up) | 4,458 | 4,210 | 4,185 |
| Received at least one dose of the HPV vaccine within six months of invitation sent date | 38 (0.9%) |
107 (2.5%) |
168 (4.0%) |
Table 3.
Odds ratios with 95% confidence limits.
| Control group vs. intervention group I: Invitation letter | Control group vs. intervention group II: Invitation and reminder letters | |
| Odds ratio estimates | 3.0 | 4.9 |
| 95% Wald confidence limits | 2.1 - 4.4 | 3.4 - 6.9 |
| P-value | <0.001 | <0.001 |
Table 4.
HPV vaccine uptake among the control and intervention groups within 12 months of invitation.
Table 4.
HPV vaccine uptake among the control and intervention groups within 12 months of invitation.
| Control Group (No Study-Specific Letters) |
Intervention Group I: Invitation Letter |
Intervention Group II: Invitation Letter and Reminder Letter |
|
| Group size (met inclusion and exclusion criteria) over 12 months of follow-up | 4,430 | 4,191 | 4,167 |
| Received at least one dose of the HPV vaccine within twelve months of invitation sent date | 74 (1.7%) |
157 (3.7%) |
215 (5.2%) |
Table 5.
Odds ratios with 95% confidence limits.
| Control group vs. intervention group I: Invitation letter | Control group vs. intervention group II: Invitation and reminder letters | |
| Odds ratio estimates | 2.3 | 3.2 |
| 95% Wald confidence limits | 1.7 - 3.0 | 2.5 - 4.2 |
| P-value | <0.001 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



