Submitted:
20 February 2025
Posted:
20 February 2025
You are already at the latest version
Abstract
Background: The emergency of carbapenem-resistant Enterobacterales is prevalent and poses a significant threat to health systems worldwide. This study aimed to conduct a molecular analysis of tigecycline resistance in 100 CRE in hospital isolates from Mthatha and surrounding hospitals. Methods: A retrospective study among patients who attended Nelson Mandela Academic Hospital (NMAH) and Mthatha Regional Hospital (MRH), Eastern Cape, South Africa. Enterobacterales isolates were identified using the Vitek2® system (bioMérieux), E-test was performed in 100 CRE hospital isolates according to manufacturer’s instructions, A multiplex SYBR green-based PCR assay for rapid detection of tet(X) and its variants, including tet(X1), tet(X2), and high-level tigecycline resistance genes tet(X3), tet(X4), and tet(X5) were developed. Results: The results show a notable high prevalence of CRE infections in neonatal, male surgical, and maternal and pediatric wards, predominantly driven by Klebsiella spp. (53.4%), followed by Enterobacter spp. (20.5 %), then Escherichia coli (6.7%), 7.2% of CRE were resistant to Tigecycline (E-TEST), Tet(X) genes were Not responsible for tigecycline resistance in this setting. The risk factors associated with tigecycline resistance in CRE include age, pre-exposure to antibiotics, prolonged hospitalization, and undergoing invasive procedures indicated by strong r2 =0.9501. Conclusion: CRE gradually evolves, posing a significant threat to patients of all ages; early detection of carbapenemase production in clinical infections, carriage states, or both is essential to prevent hospital-based outbreaks.
Keywords:
Tigecycline resistance
; E-test
; CRE infections
; PCR
; Tigecycline resistance risk factors
; Tet(X) genes and Carbapenamase genes
1. Introduction
The emergency of carbapenem-resistant Enterobacterales is prevalent and poses a significant threat to health systems worldwide [52]. There is an increment of about 50-60% of mortality rate in patients with CRE bloodstream infections reported by European Centers for Diseases Control and Prevention [100]. The most common CRE that are responsible for a wide range of infections (Urinary tract, Pneumonia, soft tissue bloodstream infection, wound infection, meningitis, septicaemia, endocarditis, severe intra-abdominal infections, and lower respiratory tract infection in clinical settings are Escherichia coli, Klebsiella pneumoniae, Salmonella spp., Serratia marcescens, Enterobacter spp., and other gram-negative bacteria [39]. The first CRE case was reported in 2011 in Gauteng province with Klebsiella pneumoniae carbapenem (KPC) and New Delhi metallolactamase-β-1 (NDM-1) as carbapenem resistant genes, followed by many others in 2012 [13]. A study conducted by Thamma et al. (2017) reported a mortality of about 32% in patients with CRE bloodstream infections within 14 days, even higher in critically ill patients, cancer, and immuno-compromised patients [30]. Prolonged unnecessary stays at hospitals, higher mortality rates, and higher morbidity rates have increased worldwide and are caused by nosocomial carbapenem-resistant Enterobacterales (CRE) outbreaks [100]. Carbapenems were a last resort to treat CRE infections but due to misuse, overuse and other resistance mechanisms acquired by CRE, drug of choice had to be changed. There are two ways in which CRE acquire resistant mechanism (intrinsic and acquired), both play a significant role in drastic rise on CRE resistance. On intrinsic mechanism there is a development of carbapenemases from class A serine carbapenemases while in acquired mechanism the main the development of efflux pumps mostly reported on Enterobacter cloacae, Serratia marcescens, and Klebsiella spp., [58]. Most of the acquired mechanism are mediated by plasmid and associated with horizontal gene transfer. Common carbapenemases are linked to acquired mechanisms with New Delhi metallo-lactamase (NDM) reported as the most dominating now in clinical isolates [24]. KPC is one of the most common genes in clinical isolates and has caused multiple nosocomial outbreaks worldwide [67]. CRE have developed resistant strains to almost all classes of antibiotics available which makes it difficult for clinicians to select an appropriate and effective drug to treat and reduce infections and outbreaks caused by CRE [49]. Fosfomycin, clindamycin and cotrimoxazole were successfully used to treat CRE infections, after some time limitation such as nephrotoxicity to patients with renal complications were reported and new, effective/ appropriate drug options to treat CRE infections had to be revised [57].In 2010, Colistin and Tigecycline became the last resort treatment option for CRE and made available in clinical practice depending on the country and its antibiotic guidelines for instance in South Africa both antibiotics are reserved for specific clinical cases [14]. Tigecycline is one of the antibiotics developed to treat MDR infections including infections caused by CRE, it belongs to tetracycline class [78,96]. Tetracycline class has significant properties that allow them to effectively treat CRE infections and it has perfect anti-bacterial activities. Over a decade tetracycline has been used to successfully treat infections on both animal and humans. However, only 25% of tetracycline is absorbable after intake and 75% is excreted as metabolite according to [50]. Due to these limitations the contact time between pathogen and drug was limited resulting in tetracycline class being not completely effective. Scientists structurally modified tetracycline and produced tigecycline, a drug with perfect anti-bacterial properties that enables it to treat MDR infection successfully. The first member of the glycylcycline class of antibiotics to display vital properties in vitro activity against MDR including CRE is tigecycline, some of these properties are its ability to overcome typical resistance mechanism that confers bacteria resistance to tetracycline class, it has different binding orientation which allows it to bind high affinity to bacterial ribosomes, it prevents protein synthesis of bacteria by interfering with aminoacyl-tRNA that usually binds with ribosomes allowing the bacteria to multiple. Eventually, bacterial growth is inhibited by binding to the bacterial 30S ribosome [32,51,91]. Another name for tigecycline is GAR-936 (third generation of tetracycline class of antibiotics because it was derived from the addition of 9-tert-butyl-glycylamido to minocycline. Tigecycline overcomes standard resistant mechanisms of CRE such as efflux pumps, ribosomal protection mechanism [94]. FAD- approved tigecycline for treating patients with complicated skin and skin structure infections (cSSTI), complicated intra-abdominal infections (cIAI), and community-acquired bacterial pneumonia, but recommended it not to be used in patients with a diabetic foot infection in 2005 [91]. All infections caused by Clostridium difficile are successfully treated using tigecycline. Due to its broad spectrum of most pathogens that are resistant to first-line antibiotics, clinicians now use it off-label to treat ventilator-associated pneumonia (VAP), hospital-acquired pneumonia (HAP), and bloodstream infections (BSI) caused by pathogens, particularly carbapenem-resistant (CR) bacteria [51]. Pathogens have developed resistance mechanisms against tigecycline, even though it is a last resort for treating infections caused by MRD or XDR and tigecycline resistance has been reported globally (Yaghoubi et al., 2022). Tigecycline resistance in CRE is associated with increased mortality and morbidity [105]. Antimicrobial sales are predicted to increase by 11.5% from 2017 to 104,079 tons globally in 2030 [84]. Tigecycline resistance is not only a health care system burden but also an economic burden that needs the world’s immediate intervention [24,49]. This study aimed to conduct a molecular analysis of tigecycline resistance in 100 CRE in hospital isolates from Mthatha and surrounding hospitals
2. Materials and Methods
2.1. Study Area
Nelson Mandela Academic Hospital is a large Provincial government-funded hospital in central Mthatha in South Africa in the Eastern Cape. It is a tertiary teaching hospital and part of the Mthatha Hospital Complex. The study was conducted in this hospital and surrounding hospitals such as NMAH Mthatha Regional Hospital and surrounding hospitals (Zithulele Hospital, St. Elizabeth Hospital, Malizo Phehle Hospital, Madzikane Hospital, etc.).
2.2. Study Design
The present study was a retrospective study focusing on CRE bacterial isolates. The aim was to conduct a molecular analysis of tigecycline resistance in CRE in hospital isolates from Mthatha and surrounding hospitals. This is a sub-study of the study; “Genes responsible for Carbapenem-Resistant. Enterobacterales (CRE) in Mthatha and correlating predisposing factors.” which was conducted by Vasaikar, et al. (2019). No direct intervention or interaction with any participant occurred as previously non-identified records of CRE data were used. From the previous main study, written informed consent was obtained from all adult cases and controls and while parental consent was obtained for child cases and controls. Participants were interviewed by a medical practitioner and research assistant. A clinical research form (CRF) questionnaire was completed upon obtaining a patient’s consent. Factors associated with a clinical sample positive for CRE and CSE in participants who received medical care in NMAH and MRH were studied using a case-control study. Participants prospectively identified by National Health Laboratory Service (NHLS) microbiological laboratory (Mthatha branch) of each participating hospital with a clinical sample yielding CRE or CSE were eligible for the study and were selected from the laboratory register of the same hospital.
2.3. Study Setting
The main study was carried out from April 2019 to December 2024 in South Africa in the Eastern Cape province, Mthatha region on bacterial isolates of participants who received medical care at NMAH and MRH during the study period. The data used was retrospective and was sought from NHLS in Mthatha.
2.4. Study Population and Sampling Method
The population criteria for the study were all hospitalized or clinically based patients who attended Nelson Mandela Academic Hospital (NMAH) and Mthatha Regional Hospital (MRH) during the period April 2019 to October 2024.The study population for this study male and female patients who had routine laboratory microbiological investigations for bacterial infections (culture and sensitivity) during the study period. Exclusion criteria: Missing critical data and isolates with mixed colonies suggestive of sample contamination. All the CRE isolates were without tigecycline phenotypic resistance, and non-CRE isolates were like Acinetobacter baumannii. Inclusion criteria: All CRE isolates with tigecycline phenotypic resistance. A case of CRE was defined as a clinical culture with organisms of the Enterobacterales family exhibiting phenotypic resistance (determined using Pure Mercy VITEK-tool (Automated) for the performance of the Antibiotic Sensitivity Test) to carbapenems (imipenem, meropenem or ertapenem). An initial literature review identified members of the Enterobacteriaceae family to be included in the study: Klebsiella pneumoniae, Klebsiella oxytoca, Escherichia coli, Proteus mirabilis, Enterobacter spp., Morganella morganii, and Providencia spp. (Alon et al., 2021). All CRE isolates were taken from NHLS, where all the isolates from different hospitals were referred to for microbiology testing by the original study principal investigator. Sample size: The study is a retrospective study of genes responsible for Carbapenem-Resistant Enterobacterales (CRE) in Mthatha and correlating predisposing factors conducted by Prof Vasaikar.
2.5. Data Treatment and Analysis
All variables from the questionnaires and laboratory investigation were captured and coded in Microsoft Excel and exported to SPSS version 20 for analysis. The validity and reliability of the questionnaire data were determined using SPSS version 20. Numerical variables were explored using the Shapiro-Wilk test, histogram, and box-and-whisker plot. The median and interquartile range (IQR) were used to summarise data that was not normally distributed. The chi-squared test and Fisher’s exact test were used to compare the association of two categorical variables depending on the value of expected frequencies, where if 20% or more of the cells have expected frequencies of <5 or any cell has expected frequencies of “0” the Fisher’s exact test was used. Descriptive statistics and logistical regressions were used to estimate the crude ratios with a 95% confidence interval (CI) for the variables. The significance level was 5%; a p-value of less or equal to 0.05 was considered significant.
2.6. Ethical Considerations
An ethical clearance certificate was obtained from the Faculty of Medicine & Health Science Ethics Committee with ethical number 026/2024. Hospital approval was obtained through the Department of Health. No consent was required from participants as this was a retrospective study. Ethical consideration followed the non-identification principle. Identifiers’ names and surnames (Personal information including the patient’s identity number) were removed, and files were created so that any researcher could access them without violating confidentiality. Study IDs were made and used instead. Collected data was stored in a Microsoft Office spreadsheet, which was stored in a password-protected folder on a password-protected laptop. The only individuals with access to this were the researcher and research supervisor. This research is aligned with research objective number 3 of a study conducted by Prof. Vasaikar, who was the principal investigator of the research. Ethics certificate 080/2017 and the letter extension were issued on 21 July 2023. Prof. Vasaikar obtained and provided the gatekeeper with a permission letter.
2.7. Methodological Design
2.7.1. Antibiotic Susceptibility Testing (E-Test)
Phenotypic resistance of tigecycline in 100 CRE isolates was detected using the semi-automated microbial identification and drug susceptibility method, Vitek2 COMPACT (bioMérieux, France), using the AST-GN16 card, confirmation of tigecycline resistance was performed using Epsilometer (E-test) (bioMérieux, France), The strains were grown in 0.5 McF bacterial suspension using normal saline. The bacterial suspension was applied to the Mueller–Hinton agar surface with a sterile cotton swab, and the E-test strip of 0.016 to 256 mg/l gradient (was placed onto the agar surface. E. coli ATCC 25922 was used for Quality control. The culture plates and agar plates were incubated at 35°C ± 2°C for 16–20 hours. An elliptical zone of inhibition was produced surrounding the strip, and the MIC was determined. All tests were performed according to CLSI 2020 recommendations. Antimicrobial susceptibility results were interpreted according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) recommendations (2023).
2.7.2. DNA Extraction
About three to four colonies of broth were grown overnight, and suspended in small, capped vials. The 10 mls of ZYMO Quick-DNATM Bacterial Miniprep Kit bacteria lysis butter were added to the vails, then vortexed briefly for 10 seconds to mix thoroughly. They were heated at 95 degrees for 10 minutes in a heat block to burst open and lyse the cells and centrifuged for about 10 minutes at 13000g so as the pellet. The supernatant was pipetted into sample tubes and loaded into the ZYMO Quick-DNATM nucleic acid isolation kit following the manufacturer’s instructions.
2.7.3. Tet x gene detection using PCR
A multiplex SYBR green-based PCR assay was developed for rapid, sensitive, and specific detection of five tet(X) variant genes from different samples, including tet(X1) GenBank accession no. AJ311171), tet(X2) (GenBank accession no. AJ311171), tet(X3) (GenBank accession no. MK134375), tet(X4) (GenBank accession no. MK134376) and tet(X5) (GenBank accession no. CP040912.1) which were also used as positive controls for each gene . Primer Premier 5.0 (PRIMIER Biosoft International, Palo Alto, CA, USA) was used to design specific primers for tet(X1), tet(X2), tet(X3), and tet(X4), as well as a universal tet(X5) primer set (Table 1.).
To guarantee the specificity, the designed primers were checked using Primer-BLAST (https://www.ncbi.nlm.nih.gov/tools/primer-blast/). Preliminary specificity verification of the designed primers was conducted by conventional simplex PCR analysis and agarose gel electrophoresis. Further specificity verification was then performed using the QuantStudio 5 Flex real-time PCR, Applied Biosystems, Foster City, CA, USA) with the following conditions: 50°C for 2 min, 95°C for 3 min, and 40 cycles, with one cycle consisting of 95°C for 30 s, 60°C for 30 s, and 72°C for 30 s, following by a melt curve stage. PCR assays were conducted in 20-l reaction volumes containing 10 l of 2 PowerUp SYBR green master mix (Thermo Fisher Scientific, Waltham, MA, USA), 0.8 l of each primer (10 mol/liter), 6.4 l of nuclease-free water, and 2 l of DNA template. Three technical replicates were conducted for each sample. Five Escherichia coli DH5 strains containing the tet(X1), tet(X2), tet(X3), tet(X4), or tet(X5) gene were used as positive controls, while E. coli DH5 was used as the negative control to confirm the assay’s specificity.
3. Results
3.1. Carbapenem Resistant Enterobacterales Species
The first objective was to determine carbapenem-resistant Enterobacterales’ prevalence in Mthatha and surrounding hospitals. The CRE prevalence graph charts were obtained using SPSS version 2.0 Figure 1. It was produced from descriptive analysis (frequency) because a categorical variable (Organism) against frequency was investigated, from SPSS, a chart builder, Figure 2. It was created. A boxplot chart was made because a relationship between two categorical variables (Sex and CRE organism) and one continuous variable (age) was explored. The bar chart represents the distribution of CRE (Carbapenem-Resistant Enterobacterales) infections in different wards of Mthatha Hospital, with various organisms identified using different colors. The pathogens identified include Klebsiella pneumoniae, Escherichia coli, Enterobacter spp., Citrobacter spp.
There is a notable high prevalence of CRE infections in Neonatal wards, Male Surgical Ward, Maternity and Pediatric Wards, predominantly driven by Klebsiella spp. (53.4%), followed by Enterobacter spp. (20.5 %), then Escherichia coli (6.7%). Klebsiella spp. (light purple) is the most common organism across multiple wards, indicating its dominance in causing infections. Enterobacter spp. and Escherichia coli were present in several wards but at significantly lower frequencies. Accident Emergency, Adult Care Ward, and Outpatient departments exhibit relatively low occurrences of CRE infections.
The boxplot chart shows age distribution by gender, categorized by different CRE organisms in a clustered format.
No gender and age difference in CRE distribution was observed for females; most organisms have a relatively compact age distribution, except for a few outliers. KLEPP (purple) was reported more on the comprehensive age range for both genders, with a few exceptions in younger individuals. CITFR (light blue) is present primarily in older age groups, particularly for females; ENTCX (teal) has a relatively younger distribution for males and females, with a narrow range. There were exceptional cases observed in both genders, indicating that some patients fall outside the usual age ranges affected by specific pathogens.
A RESIST-4 OKNV test was used to detect the positive carbapenemase gene found on Mthatha CRE. The table below demonstrates the summary of prevalent carbapenemase genes accordingly. There were no KPC and VIM genes detected (0%) on our CRE; the most prevalent carbapenemase was NDM (54.2%), most detected on Klebsiella spp. and E. coli, followed by OXA-48 (30.6 %) mostly detected E. coli and Klebsiella spp. Also, about 15.2% of CRE were negative (no gene detected).

Table 3.
Distribution of positive carbapenemase gene loci according to bacterial species.
| Species | VIM | KPC | NDM | OXA-48 | Not detected |
|---|---|---|---|---|---|
| Citrobacter spp. | 0 | 0 | 50% | 25% | 25% |
| Enterobacter spp. | 0 | 0 | 45.6% | 27.8% | 27.% |
| Escherichia coli | 0 | 0 | 60% | 40% | 0 |
| Klebsiella pneumoniae | 0 | 0 | 60.2% | 29.1% | 11.3% |
Table 4.
Showing Species of carbapenem-resistant Enterobacterales according to the specimen type.
| Specimen | Type | ||||||
|---|---|---|---|---|---|---|---|
| Species | Abscess | Blood culture | Pus swab | Sputum | Urine | Tissue | Other |
| Citrobacter spp. | 0 | 0 | 8.3% | 14.3% | 5.9% | 0 | 0 |
| Enterobacter spp. | 0 | 13% | 33.3% | 33.3% | 41.2% | 0 | 80% |
| Escherichia coli | 0 | 4.35% | 50% | 14.3% | 5.9% | 0 | 0 |
| Klebsiella pneumoniae | 100% | 86.9 % | 41.7 | 71.4% | 41.2% | 100% | 20% |
3.2. Tigecycline Susceptibility Using E-Test
Tigecycline susceptibility was determined using an E-test (Etest, bioMérieux, France), Bar graph chart was produced from SPSS. Version 20. to represent the results obtained. Since a relationship between one dependent categorical variable (Tigecycline susceptibility) and one continuous independent variable (age) was explored, a descriptive analysis (frequency) was an appropriate tool to use. The chart shows tigecycline susceptibility in different age groups, categorized into three susceptibility levels: S (susceptible), R (resistant), and I (intermediate). The data is represented as bars, with error bars indicating each measurement’s 95% confidence interval.
Figure 3.
Showing tigecycline susceptibility in different age groups of Mthatha and surrounding hospitals.
Figure 3.
Showing tigecycline susceptibility in different age groups of Mthatha and surrounding hospitals.
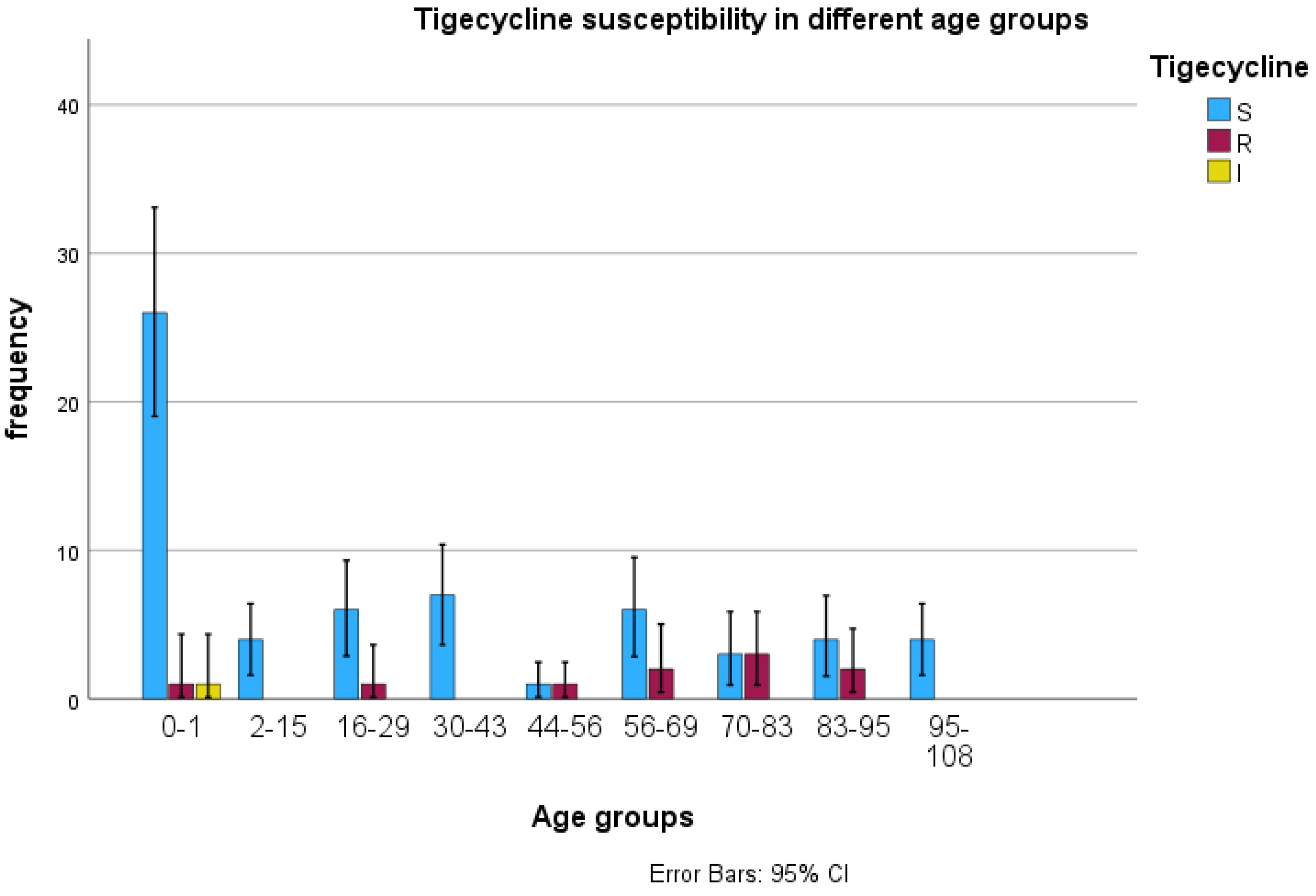
From the graph, tigecycline resistance increases with age, except in a few cases with no resistance. The E-test showed a tigecycline susceptibility of 92.8 %, a resistance of 5.8 %, and 1.5% intermediate resistance. Age group 0-1 shows a high level of tigecycline susceptibility (S) compared to other age groups; there is relatively low tigecycline resistance (R) and Intermediate resistance (I). Age Groups 2-15, 16-29, 30-43, and onwards: In these groups, susceptibility frequency decreases notably compared to the 0-1 age group.
The frequency of resistance (R) and intermediate (I) levels become more noticeable, although still lower than tigecycline susceptibility. In Older Age Groups (44-56 and beyond): There is a trend of lower tigecycline susceptibility rates with some variability across different age groups. Resistance (R) and intermediate (I) levels appear relatively consistent but remain lower than in susceptible cases of tigecycline.
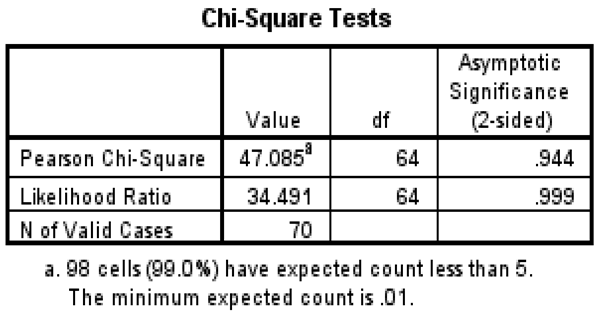
SPSS version 20. was deployed to explore the association between tigecycline resistance (categorial variable) and age (categorical variable, age was grouped) to evaluate the statistical significance. Tigecycline resistance is present in children (neonates) and adult patients, with slightly more in adults than children. The difference in tigecycline resistance between age groups is statistically insignificant, as indicated by a p-value of 0.944. Based on this sample, there is no evidence that tigecycline resistance is associated with age, even though it is mostly seen in adult patients.
Table 1.
A chi-square table showing tigecycline resistance by age group of Mthatha and surrounding hospitals.
Table 1.
A chi-square table showing tigecycline resistance by age group of Mthatha and surrounding hospitals.
3.3. Detection of tet(X) Genes Using PCR
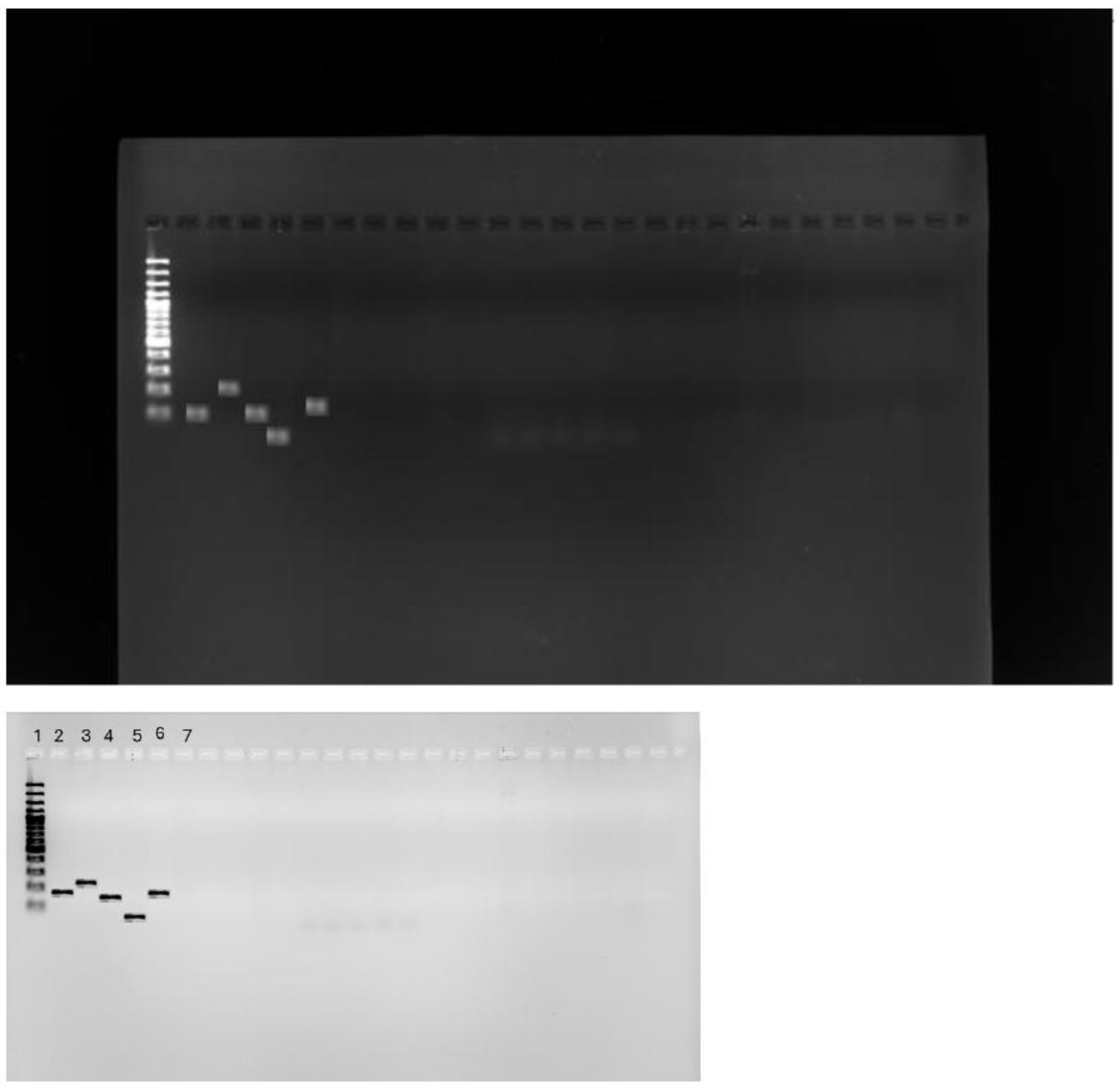
A multiplex SYBR green-based PCR assay was developed for the specific detection of five tet(X) genes from other samples, including tet(X) (GenBank accession no. GU014535.1), tet(X1) GenBank accession no. AJ311171), tet(X2) (GenBank accession no. AJ311171), tet(X3) (GenBank accession no. MK134375), tet(X4) (GenBank accession no. MK134376), and tet(X5) (GenBank accession no. CP040912.1) . The Light cycler device and the intercalating fluorescent dye SYBR Green (I) could monitor the accumulation of amplicons in reaction over time. SYBR Green (I) eliminates the requirement for analyzing PCR results on time-consuming agarose gels. After PCR amplification, the Light Cycler monitors the fluorescence decrease caused by SYBR Green (I) release during DNA melting point analysis by gradually increasing the temperature. Target genes were identified based on certain amplicons’ melting peak form and Tm. Of the 100 CRE clinical isolates studied there was no tet (X) gene detected that was responsible for tigecycline resistance. This was expected since both phenotypic methods used showed lower tigecycline resistance < 15%. The DNA extracts were NANODROPPED determined the concentration of each extract, and isolates with <1.81 concentration were qualified until the required DNA concentration were met. Following is the Agarose Gel result viewed from UV light machine.
Figure 4.
Agarose gel electrophoresis picture of Tigecycline Tet(X) genes, DNA ladder on lane 1, with positive control of each gene, tet (X1) with 141 base pairs (lane 2), with tet (X2) with 227 base pairs (lane 3), tet (X3) with 125 base pairs (lane 4), tet (X4) with 93 base (lane 5) pairs and tet (X5) with 161 base pairs (lane 6).
Figure 4.
Agarose gel electrophoresis picture of Tigecycline Tet(X) genes, DNA ladder on lane 1, with positive control of each gene, tet (X1) with 141 base pairs (lane 2), with tet (X2) with 227 base pairs (lane 3), tet (X3) with 125 base pairs (lane 4), tet (X4) with 93 base (lane 5) pairs and tet (X5) with 161 base pairs (lane 6).
3.4. Risk Factors Associated with Tigecycline Resistance
To determine the risk factors associated with tigecycline resistance in CRE of Mthatha and surrounding hospitals, GraphPad Prism 8.0.1 (Multiple linear regression) was used to determine p-values and R-values, as shown in Table 2 below. The R-value could not be determined for other risk factors, such as Pre-exposure to antibiotics, invasive procedures, and hospitalization duration. The correlation between tigecycline resistance and wards was weak, indicated by r=0.4182, and the p-value of 0.1631 suggested that the association was not statistically significant; in Age, a statistically significant p-value of 0.001 suggests a strong relationship between tigecycline resistance and age groups. The r= value of 0.9501 indicates a very strong correlation. There was a positive correlation between tigecycline resistance and pre-exposure to antibiotics, as indicated by a statistically significant p-value of 0.0478. Undergoing specific invasive procedures might contribute to tigecycline resistance, as indicated by a statistically significant p-value of 0.0478. A non-significant p-value of 0.3679 was found between the length of hospitalization and tigecycline resistance.
4. Discussion
4.1. To Determine the CRE Species
Carbapenem-resistant Enterobacterales (CRE) is a global public health concern affecting community and healthcare facilities. The worldwide increase in CRE infections is alarming, given its association with high mortality and mortality rates and its substantial economic burden on clinical settings (Park et al., 2020). The acquisition of CRE infections is linked to prolonged ICU stays, the use of medical devices such as mechanical ventilation and catheters, and the performance of invasive surgical procedures (Varma et al., 2018). Carbapenem resistance among Enterobacterales in South Africa has historically been relatively low and stable. However, the recent emergence of the CRE resistance mechanism, which includes overexpression of efflux pumps, development of tet(X) genes, and overuse and misuse of carbapenems, has raised concerns. The overuse and misuse of these antibiotics can lead to resistance, making infections more challenging to treat and posing a significant threat to public health (Korczak et al., 2024). This study explored the Prevalence of CRE infections in Mthatha and surrounding hospitals. The study involved a comprehensive review of patient records and laboratory data to identify cases of CRE infection. The prevalence was then represented in a graph chart using SPSS. The results show a notable high prevalence of CRE infections in neonatal, male surgical, and maternal and pediatric wards, predominantly driven by Klebsiella spp. (53.4%), followed by Enterobacter spp. (20.5 %), then Escherichia coli (6.7%).These findings are in agreement with findings obtained in previous studies conducted in community hospitals in Bahrain (87%), Taiwan, and Nigeria (91%) (Korczak et al., 2024; Saeed et al., 2019; Alraddadi et al., 2022). This is because K. pneumoniae has been reported worldwide as a dominant species; hence, a carbapenem-resistant K. pneumoniae (CRKP) gene is reported. The dominance of Klebsiella spp. in causing infections is significant as it indicates the need for targeted interventions to control the spread of CRE. This shows that neonatal wards are significantly affected by CRE infections because neonates have weak immune systems to fight off CRE infections. Male surgical and maternity wards have a broad diversity of CRE infections; hence, multiple organisms were detected. This might be because of the high number of immunocompromised patients in these wards. Usually, these wards have a population pre-exposed to tetracycline antibiotics and undergone different surgeries, which are risk factors for acquiring CRE infection (Jiang et al., 2022). Klebsiella spp. is the most common organism across multiple wards, indicating its dominance in causing infections—Enterobacter spp. Escherichia coli is present in several wards but at significantly lower frequencies. Accident Emergency, Adult Care Ward, and Outpatient departments exhibit relatively low occurrences of CRE infections. These findings are significant in South Africa’s healthcare system as they highlight the urgent need for targeted interventions and increased surveillance to control the spread of CRE infections. In this study, the age distribution was skewed toward old patients when CRE infections were analyzed—Klebsiella spp. was prevalent in a comprehensive age range for both genders, with some exceptional cases in younger individuals; Citrobacter spp. is primarily present in older age groups, particularly for females; Enterobacter spp. has a relatively younger age distribution for both males and females, with a narrow range. As age increases, the variety of CRE organisms also increases; this might be because older patients are affected by more than one CRE acquisition risk factor, leading to the high prevalence of CRE in wards occupied by older people (Zhang et al., 2022). The outcome of this study shows that the prevalence of this CRE infection in Mthatha Hospital and surrounding hospitals is 30%. This estimate is lower than the estimates reported in the literature of other countries, such as the United States (32%) and India (28%) (Paveenkittiporn et al., 2021). Still, higher estimates were reported in Tunisia (15.8%), and other countries such as China and Nigeria reported varying numbers of CRE infection prevalence (Adesanya et al., 2020). This could be because the population size of the study was different, and study sites are in other regions of the world with different economic statuses and clinical settings. Three central resistant genes of carbapenems have been reported in clinical isolates worldwide, namely KPC, NDM, and OXA-48, with KPC being the most prevalent (Rizzo et al., 2019). This study’s most identified class A genes are NDM (56.9%) and OXA-48 (31.9%); 11.1% were negative. These findings are consistent with the outcome reported by Park et al. (2020), where the prevalence of CRE was investigated in clinical isolates, and NDM (5.1%) was reported, followed by Oxa-48 (26.8%). The outcomes of this study differ from those of Lee et al. (2021), where CRE prevalent genes were evaluated in clinical isolates, and VIM (80%) was the most prevalent gene. This may be due to the different years of reporting; sometimes, specific genes are prevalent in that particular year because of the reported outbreaks. CRE gradually evolves, posing a significant threat to patients of all ages; early detection of carbapenemase production in clinical infections, carriage states, or both is essential to prevent hospital-based outbreaks (Aslam et al., 2020). This shows the need for further research to understand and combat the rise of CRE infections in South Africa. More research is needed to explore the specific factors contributing to the increase of CRE infections, the effectiveness of current control measures, and the development of new strategies to prevent and manage these infections. This suggests that further research is crucial to inform evidence-based interventions and policies to control the spread of CRE in South Africa.
4.2. Tigecycline Susceptibility Using E-Test
The emergency of multi-drug-resistant bacteria in hospitals significantly limits the therapeutic options to treat life-threatening infections and forces clinicians to use the last resort antibiotics, including tigecycline (Babaei et al., 2021). Since CRE infections are prevalent and are associated with increased mortality and morbidity worldwide, WHO, FDA, and EUCAST recommend clinicians to use colistin and tigecycline to treat these infections (Chen et al., 2021). This study focuses more on tigecycline and its effectiveness in CRE. Tigecycline is the first member of the glycylcycline class of antibiotics that has displayed important properties in vitro activity against CRE and is a last resort of treatment options for CRE; hence it is crucial to study its antibiotic susceptibility (Jenner et al., 2013, Wang et al., 2020, Li et al., 2020). Several methods are used to perform tigecycline antibiotic susceptibility tests (AST), but the most reliable and accurate ones include disk diffusion and E-test (Wilson et al., 2023). Though many factors affect TGC susceptibility, such as unavailability of predictive breakpoints to interpret results for some pathogens on CLSI, US FDA was used as an alternative. The present study performed tigecycline AST using an E-test on 100 CRE hospital isolates in South Africa, Mthatha, and surrounding hospitals. 92.8% CRE was susceptible to tigecycline, 1.5% intermediate resistant to tigecycline, and 5.8 % resistant to tigecycline. Tigecycline resistance is present in children (neonates) and adult patients, with slightly more in adults than children. The difference in tigecycline resistance between age groups is statistically insignificant, as indicated by a p-value of 0.944. Based on this sample, there is no evidence that tigecycline resistance is associated with age, even though it is mainly seen in adult patients. Age group 0-1 shows a high level of tigecycline susceptibility (S) compared to other age groups; there is relatively low tigecycline resistance (R) and Intermediate resistance (I). Age Groups 2-15, 16-29, 30-43, and onwards: In these groups, susceptibility frequency decreases notably compared to the 0-1 age group. As age increases, tigecycline resistance also increases; this is justified by the fact that as people use health facilities, use antibiotics (especially tetracyclines), undergo surgeries, others who are admitted to ICU, have underlying health conditions that are prime risk factors for tigecycline resistance (Korczak et al., 2024, Sun et al., 2023, Heidary et al., 2024, Su et al., 2024). These outcomes were consistent with outcomes reported by Wilson et al. (2023), where 75.3% tigecycline susceptibility was obtained on CRE hospital isolates using the E-test method; the study was conducted in India. Li et al. (2021) conducted a similar study in China, where tigecycline AST was performed on CRE, and 82% tigecycline susceptibility was reported using KB diffusion. Yu et al. (2020) conducted an AST on CRE and reported 80-90% tigecycline sensitivity in critically ill patients. Lower tigecycline resistance in other countries may be because tigecycline is a reserved drug; WHO recommends the use of this drug on certain specifications and prevents the overuse and misuse of this tigecycline that could lead to increased resistance. The outcomes of this study are not aligned with the study conducted by Sah et al. (2022), where Tigecycline AST was performed using the disc diffusion method on 51 CRE hospital isolates, and 30 (58%) were resistant to tigecycline. This significant difference might be because of the difference in sample size and different screening methods employed to perform AST. The suggested dose of TG for patients is 100 mg on the first day, followed by 50 mg every 12 hours on subsequent days. The systemic clearance of TG is 0.2 to 0.3 L/h/Kg, with a half-life of 37 to 67 hours. This antibiotic’s most common side effects include nausea and vomiting (Heidary et al., 2023).TG is used to treat surgical wound infections caused by MRSA, Enterobacterales, Streptococci, and anaerobic bacteria. Additionally, it is being tested for treating skin infections caused by MRSA and Gram-negative bacteria. According to Viechtbauer et al. (2010), TG is equivalent to imipenem in abdominal and intra-abdominal infections and to a combination of aztreonam and vancomycin in skin and skin structures. Reasons for substituting TG with equivalent drugs include: 1) TG possesses an extensive range of action against bacteria, including oxygen-requiring and oxygen-averse types and Gram-negative and Gram-positive varieties. 2) It is potent against severe infections like those resistant to vancomycin among Enterococcus species (VRE), Methicillin-resistant Staphylococcus aureus (MRSA), antibiotic-resistant Streptococcus pneumoniae, and Gram-negative respiratory pathogens. 3) It is effective in treating a variety of diseases caused by pathogens. 4) TG shows efficacy against less common bacterial infections, such as those caused by Mycoplasma pneumonia. 5) It is safe for use in patients with renal and hepatic insufficiency and the elderly without the need to adjust the dose (Bajaj et al., 2020). Other studies reported ribosome protection, drug-degrading enzymes, cell membrane pore channel protein modification, and efflux pump mechanisms as the primary mechanisms of bacterial resistance to tigecycline (Zhang et al., 2022). Tigecycline is derived from minocycline by adding a 9-tert-butyl-glycylamido side chain to the D ring at the ninth position. This side chain aids in overcoming the ribosomal protection proteins and efflux pumps, which confer resistance to other tetracyclines. Tigecycline remains a promising treatment option for CRE. Still, clinicians are urged not to use it as a monotherapy because of its bacteriostatic activity and low steady-state concentration, especially when treating severe multidrug-resistant Gram-negative infections. For neonates, the recommended combination therapy is tigecycline and amikacin.
4.3. PCR for Tet (X) Genes
Tigecycline resistance has been detected in hospital isolates worldwide, including South Africa, Eastern Cape Mthatha, and surrounding hospitals (5.8 %). There is an urgent need to develop an effective, fast, yet specific method to detect tigecycline-resistant genes; real time PCR technology has allowed the development of a quick and reliable alternative to traditional hybridization for the detection of tetracycline-resistant determinants. PCR-based techniques are commonly used in the diagnostic laboratory (Heidary et al., 2023). This fluorescence-based real-time assay can identify target genes independently and allows for multiple PCR reactions in one tube by employing the unique melting curve analysis following DNA amplification. According to recent research, real-time PCR can detect and quantify tet genes. The real-time PCR assay is commonly used in molecular diagnosis to detect environmental diseases and pathogens. It is most advanced compared to previously used approaches regarding sensitivity, reliability, precision, and time efficiency (Zou et al., 2024). Yu et al. (2023) developed a multiplex test for three groups of tet genes using universal primers. The majority of the tet genes studied encoded ribosome protection proteins. Due to their high sequence divergence, the researchers targeted three classes of efflux tet genes with only two pairs of primers. In this study, tet(X) genes and their variants in different types of samples, a multiplex SYBR green-based real-time PCR assay was developed for specific detection of five tet(X) genes from other samples, including tet(X) (GenBank accession no. GU014535.1), tet(X1) GenBank accession no. AJ311171), tet(X2) (GenBank accession no. AJ311171), tet(X3) (GenBank accession no. MK134375), tet(X4) (GenBank accession no. MK134376), and tet(X5) (GenBank accession no. CP040912.1) (Fu et al., 2020). With the Lightcycler device and the intercalating fluorescent dye SYBR Green, I can monitor the accumulation of amplicons in reaction over time. SYBR Green (I) eliminates the requirement for analyzing PCR results on time-consuming agarose gels. After PCR amplification, the LightCycler monitors the fluorescence decrease caused by SYBR Green I release during DNA melting point analysis by gradually increasing the temperature. Target genes can be identified based on certain amplicons’ melting peak form and Tm. Except for tet(X1) (65.2%), all other tet(X) (tet(X1), tet(X2), tet(X3), tet(X4)) gene composition is like tet(X) about 85.1% to 99.8%. Though each gene has its pair of primers, the high level of similarity on the tet(X) variant does give a challenge to design specific primers, especially tet(X2) and tet(X), since they are the same except for two nucleotides (Ji et al., 2020). Of the 100 CRE clinical isolates studied 0 (%) yielded 0 (tet(X1)), tet(X2), tet(X3), tet(X4) and tet(X5) using PCR. There were no tet(X) genes responsible for tigecycline resistance in CRE detected from this sample, even though tigecycline resistance is notable high from the sample of this study, it is still lower than 15%, this means that there is other resistance mechanism that confers tigecycline resistance such as efflux pumps and Mutations in genes like ramR, acrR, adeS, rrf, and rpoB. These findings align with a study conducted by Li et al. (2020), where real-time PCR was performed to detect tet(X) genes in hospital isolates. The justification for similar results might be that other countries reserve tigecycline drugs, and it is used in exceptional cases, as is South Africa and China. The results of this study are contrary to the study obtained by et al., 2023, where tet(X) genes were detected in hospital isolates. The difference is about %; this could be the difference in CLSI guidelines on tigecycline. In conclusion, we developed a multiplex SYBR green-based real-time PCR assay for the rapid screening and quantification of various tet(X) variants, including tet(X), tet(X1), tet(X2), tet(X3), tet(X4), and tet(X5). It is susceptible and specific for detecting tet(X) and its variants from hospital samples. The prevalence of tet(X) in hospital isolates in South Africa has been increasing since 2020; more methods to detect tet(X) are recommended.
4.4. Risk Factors Associated with Tigecycline
Few studies have assessed the risk factors associated with tigecycline resistance in CRE among hospital isolates. According to the Literature available, tigecycline resistance may be conferred by many factors, including prior exposure to antibiotics, the use of different drugs (particularly tetracycline) can confer tigecycline resistance in patients, and being in ICU where you might be exposed to a variety of resistant organisms (Jiang et al., 2022).Multivariable analysis indicated that nasal catheter and exposure to antibiotics such as penicillin and fluoroquinolones were independent predictors for acquiring TCREC (Yuansu et al., 2022).This study aimed to determine the risk factors associated with tigecycline resistance in CRE using patient history and demographic characteristics. The correlation between tigecycline resistance and wards was weak, indicated by r=0.4182, and the p-value of 0.1631 indicated that the association was not statistically significant. This suggests that being admitted to clinical wards does not necessarily mean that patients would be resistant to tigecycline, even though patients admitted to ICU (25.1%) showed an increased resistance than those admitted to other wards. Most patients admitted to the ICU are more vulnerable to MDR pathogens, which confer resistance to tigecycline. Another study reported that patients with urinary catheterization admitted to the Intensive care unit (ICU) had increased tigecycline-resistant infections (Heidary et al., 2024; Jiang et al., 2019). In Age, a statistically significant p-value of 0.001 suggests a strong relationship between tigecycline resistance and age groups. The r= value of 0.9501 indicates a strong correlation. There was a notable tigecycline resistance in older patients than neonates; as people grow, they tend to use different antibiotics; most older patients are immunocompromised and are vulnerable to many pathogens with resistant strains. This suggests that age is a critical factor in tigecycline resistance. One of the most prevalent tigecycline risk factors is the demographic age of the patient; elderly patients are at a higher risk of acquiring tigecycline resistance due to their weakened immune systems and higher likelihood of various comorbidities (Saraci et al., 2023; Curcio et al., 2007).There was a positive correlation between tigecycline resistance and pre-exposure to antibiotics, as indicated by a statistically significant p-value of 0.0478. Undergoing specific invasive procedures might contribute to tigecycline resistance, as indicated by a statistically significant p-value of 0.0478. Invasive medical procedures also significantly increase the risk of tigecycline resistance. Patients having central venous catheterization, mechanical ventilation, or urine catheterization are more vulnerable. These procedures may bring pathogens into sterile conditions, facilitating the acquisition of MDR organisms (Heidary et al., 2024). A non-significant p-value of 0.3679 was found between the length of hospitalization and tigecycline resistance. This suggests that hospitalization duration might not be a direct risk factor for tigecycline resistance, even though patients with prolonged, unnecessary stays might acquire tigecycline resistance more than patients with standardized hospitalization (Zhou et al., 2023). Jiang et al. (2019) discovered that using nasal catheters and exposure to medications such as penicillin and fluoroquinolones were independent predictors of tigecycline resistance. The prevalence of tigecycline resistance in this study was 97.1%, higher than that of Jiang in China, where He evaluated tigecycline resistance in CRE. It is recommended that tigecycline resistance be reduced by practicing reasonable antibiotic use and minimizing invasive procedures. Underlying health conditions such as HIV, cancer, etc., might be a risk factor for tigecycline because the use of immunosuppressive drugs increases vulnerability to resistant organisms (Zhou et al., 2023). Social-economic factors also play a crucial role in infection rates and resistance; poor living conditions are associated with high tigecycline resistance in CRE isolates. This is likely due to age-related changes in pharmacokinetics and pharmacodynamics and the higher prevalence of underlying conditions in the elderly population. Healthcare professionals should exercise vigilance when prescribing tigecycline to older patients and closely monitor adverse events like thrombocytopenia, particularly those with three or more risk factors.
5. Conclusions
CRE gradually evolves, posing a significant threat to patients of all ages; early detection of carbapenemase production in clinical infections, carriage states, or both is essential to prevent hospital-based outbreaks. More research is needed to explore the specific factors contributing to the rise of CRE infections, the effectiveness of current control measures, and the development of new strategies to prevent and manage these infections. As using Tigecycline is the last line of treatment of the CRE infection, the high rate of tigecycline resistance in this study is alarming for the healthcare system in South Africa, Eastern Cape Mthatha and surrounding hospitals, tigecycline combination therapy is recommended when treating critically ill patients and also it should be better that clinicians do not use broad-spectrum antibiotics easily, especially in experimental treatment to minimize tigecycline resistance in CRE. Tet (X) genes are not responsible for tigecycline resistance in sample of this study. The risk factors associated with tigecycline resistance in CRE include age, pre-exposure to antibiotics, pro-longed hospitalization and undergoing invasive procedures.
Author Contributions
Luyolo Vumba drafted the original work and conducted laboratory work, Sandeep Vasaikar and Ravesh Singh, supervisor and proof-read the work provid-ing all necessities and supervision. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Informed Consent Statement
No consent statement.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Al-Qadheeb, N.S., Althawadi, S., Alkhalaf, A., Hosaini, S. and Alrajhi, A.A., 2010. Evolution of tigecycline resistance in Klebsiella pneumoniae in a single patient. Annals of Saudi Medicine, 30(5), pp.404-407.
- Alraddadi, B.M., Heaphy, E.L., Aljishi, Y., Ahmed, W., Eljaaly, K., Al-Turkistani, H.H., Alshukairi, A.N., Qutub, M.O., Alodini, K., Alosaimi, R. and Hassan, W., 2022. Molecular epidemiology and outcome of carbapenem-resistant Enterobacterales in Saudi Arabia. BMC Infectious Diseases, 22(1), p.542. [CrossRef]
- Araj, G.F. and Ibrahim, G.Y., 2008. Tigecycline in vitro activity against commonly encountered multidrug-resistant Gram-negative pathogens in a Middle Eastern country. Diagnostic microbiology and infectious disease, 62(4), pp.411-415. [CrossRef]
- Aslam, B., Rasool, M., Muzammil, S., Siddique, A.B., Nawaz, Z., Shafique, M., Zahoor, M.A., Binyamin, R., Waseem, M., Khurshid, M. and Arshad, M.I., 2020. Carbapenem resistance: Mechanisms and drivers of global menace. Pathog Bact, pp.1-11.
- Babaei, S. and Haeili, M., 2021. Evaluating the performance characteristics of different antimicrobial susceptibility testing methodologies for testing susceptibility of gram-negative bacteria to tigecycline. BMC Infectious Diseases, 21, pp.1-8Adesanya, O.A. and Igwe, H.A., 2020. Carbapenem-resistant Enterobacteriaceae (CRE) and gram-negative bacterial infections in south-west Nigeria: a retrospective epidemiological surveillance study. AIMS Public Health, 7(4), p.804.
- Bajaj, A., Mishra, B., Loomba, P.S., Thakur, A., Sharma, A., Rathod, P.G., Das, M. and Bhasin, A., 2020. Tigecycline Susceptibility of Carbapenem Resistant Enterobacteriaceae and Acinetobacter spp. isolates from Respiratory Tract: A Tertiary Care Centre Study. Journal of Krishna Institute of Medical Sciences (JKIMSU), 9(1).
- Bankan, N., Koka, F., Vijayaraghavan, R., Basireddy, S.R. and Jayaraman, S., 2021. Overexpression of the adeB efflux pump gene in tigecycline-resistant Acinetobacter baumannii clinical isolates and its inhibition by (+) usnic acid as an adjuvant. Antibiotics, 10(9), p.1037. [CrossRef]
- Baron, S.A., Cassir, N., Hamel, M., Hadjadj, L., Saidani, N., Dubourg, G. and Rolain, J.M., 2021. Risk factors for acquisition of colistin-resistant Klebsiella pneumoniae and expansion of a colistin-resistant ST307 epidemic clone in hospitals in Marseille, France, 2014 to 2017. Eurosurveillance, 26(21), p.2000022. [CrossRef]
- Bender, J.K., Klare, I., Fleige, C. and Werner, G., 2020. A nosocomial cluster of tigecycline-and vancomycin-resistant Enterococcus faecium Isolates and the Impact of rpsJ and tet (M) mutations on tigecycline resistance. Microbial Drug Resistance, 26(6), pp.576-582. [CrossRef]
- Bilal, H., Khan, M.N., Rehman, T., Hameed, M.F. and Yang, X., 2021. Antibiotic resistance in Pakistan: a systematic review of the past decade. BMC Infectious Diseases, 21, pp.1-19. [CrossRef]
- Brink, A.J., Coetzee, J., Corcoran, C., Clay, C.G., Hari-Makkan, D., Jacobson, R.K., Richards, G.A., Feldman, C., Nutt, L., van Greune, J. and Deetlefs, J.D., 2013. Emergence of OXA-48 and OXA-181 carbapenemases among Enterobacteriaceae in South Africa and evidence of in vivo selection of colistin resistance as a consequence of selective decontamination of the gastrointestinal tract. Journal of clinical microbiology, 51(1), pp.369-372. [CrossRef]
- Bush, K. and Bradford, P.A., 2020. Epidemiology of β-lactamase-producing pathogens. Clinical microbiology reviews, 33(2), pp.10-1128. [CrossRef]
- Campany-Herrero, D., Larrosa-Garcia, M., Lalueza-Broto, P., Rivera-Sánchez, L., Espinosa-Pereiro, J., Mestre-Torres, J. and Pigrau-Serrallach, C., 2020. Tigecycline-associated hypofibrinogenemia in a real-world setting. International Journal of Clinical Pharmacy, 42, pp.1184-1189. [CrossRef]
- Cassir, N., Rolain, J.M. and Brouqui, P., 2014. A new strategy to fight antimicrobial resistance: the revival of old antibiotics. Frontiers in microbiology, 5, p.109581.
- Cattoir, V., Isnard, C., Cosquer, T., Odhiambo, A., Bucquet, F., Guérin, F. and Giard, J.C., 2015. Genomic analysis of reduced susceptibility to tigecycline in Enterococcus faecium. Antimicrobial agents and chemotherapy, 59(1), pp.239-244. [CrossRef]
- Chen, H.L., Jiang, Y., Li, M.M., Sun, Y., Cao, J.M., Zhou, C., Zhang, X.X., Qu, Y. and Zhou, T.L., 2021. Acquisition of Tigecycline Resistance by carbapenem-resistant Klebsiella pneumoniae confers collateral hypersensitivity to aminoglycosides. Frontiers in Microbiology, 12, p.674502. [CrossRef]
- Cheng, Q., Cheung, Y., Liu, C., Chan, E.W.C., Wong, K.Y., Zhang, R. and Chen, S., 2022. Functional and phylogenetic analysis of TetX variants to design a new classification system. Communications Biology, 5(1), p.522. [CrossRef]
- Cui, C.Y., He, Q., Jia, Q.L., Li, C., Chen, C., Wu, X.T., Zhang, X.J., Lin, Z.Y., Zheng, Z.J., Liao, X.P. and Kreiswirth, B.N., 2021. The evolutionary trajectory of the Tet (X) family: critical residue changes towards high-level tigecycline resistance. Msystems, 6(3), pp.10-1128. [CrossRef]
- Curcio, D., Fernández, F. and Duret, F., 2007. Tigecycline use in critically ill older patients: case reports and critical analysis. Journal of the American Geriatrics Society, 55(2), pp.312-313. [CrossRef]
- Fang, L.X., Chen, C., Cui, C.Y., Li, X.P., Zhang, Y., Liao, X.P., Sun, J. and Liu, Y.H., 2020. Emerging high-level tigecycline resistance: novel tetracycline destructases spread via the mobile Tet (X)—Bioessays, 42(8), p.2000014.
- Fu, Y., Chen, Y., Liu, D., Yang, D., Liu, Z., Wang, Y., Wang, J., Wang, X., Xu, X., Li, X. and He, J., 2021. Abundance of tigecycline resistance genes and association with antibiotic residues in Chinese livestock farms. Journal of Hazardous Materials, 409, p.124921. [CrossRef]
- Fu, Y., Liu, D., Song, H., Liu, Z., Jiang, H. and Wang, Y., 2020. Development of a multiplex real-time PCR assay to rapidly detect tigecycline resistance gene tet (X) variants from bacterial, fecal, and environmental samples. Antimicrobial Agents and Chemotherapy, 64(4), pp.10-1128.
- Gajic, I., Ranin, L., Kekic, D., Opavski, N., Smitran, A., Mijac, V., Jovanovic, S., Hadnadjev, M., Travar, M. and Mijovic, G., 2020. Tigecycline susceptibility of multidrug-resistant Acinetobacter baumannii from intensive care units in the western Balkans. Acta Microbiologica et Immunologica Hungarica, 67(3), pp.176-181. [CrossRef]
- Gao, Y., Chen, M., Cai, M., Liu, K., Wang, Y., Zhou, C., Chang, Z., Zou, Q., Xiao, S., Cao, Y. and Wang, W., 2022. An analysis of risk factors for carbapenem-resistant Enterobacteriaceae infection. Journal of Global Antimicrobial Resistance, 30, pp.191-198. [CrossRef]
- Ghosh, S., Sadowsky, M.J., Roberts, M.C., Gralnick, J.A. and LaPara, T.M., 2009. Sphingobacterium sp. strain PM2-P1-29 harbors a functional tet (X) gene encoding for the degradation of tetracycline. Journal of Applied Microbiology, 106(4), pp.1336-1342.
- Gomis, P.F., Jean-Pierre, H., Rousseau-Didelot, M.N., Compan, B., Michon, A.L. and Godreuil, S., 2013. Tigécycline: CMI 50/90 vis-à-vis de 1766 bacilles à Gram-négatif (entérobactéries résistantes aux céphalosporines de troisième génération), Acinetobacter baumannii et Bacteroides du groupe fragilis, CHU–Montpellier, 2008–2011. Pathologie Biologie, 61(6), pp.282-285.
- Han, X., Shi, Q., Mao, Y., Quan, J., Zhang, P., Lan, P., Jiang, Y., Zhao, D., Wu, X., Hua, X. and Yu, Y., 2021. The emergence of ceftazidime/avibactam and tigecycline resistance in carbapenem-resistant Klebsiella pneumoniae due to in-host microevolution. Frontiers in Cellular and Infection Microbiology, 11, p.757470. [CrossRef]
- Heidary, M., Sholeh, M., Asadi, A., Khah, S.M., Kheirabadi, F., Saeidi, P., Darbandi, A., Taheri, B. and Ghanavati, R., 2024. Prevalence of tigecycline resistance in methicillin-resistant Staphylococcus aureus: a systematic review and meta-analysis. Diagnostic Microbiology and Infectious Disease, 108(1), p.116088. [CrossRef]
- Heidary, M., Sholeh, M., Asadi, A., Khah, S.M., Kheirabadi, F., Saeidi, P., Darbandi, A., Taheri, B. and Ghanavati, R., 2023. Prevalence of Tigecycline Resistance in Methicillin-resistant Staphylococcus aureus: A systematic review and meta-analysis. Diagnostic Microbiology and Infectious Disease, p.116088. [CrossRef]
- Hovan, M.R., Narayanan, N., Cedarbaum, V., Bhowmick, T. and Kirn, T.J., 2021. Comparing mortality in patients with carbapenemase-producing carbapenem resistant Enterobacterales and non-carbapenemase-producing carbapenem resistant Enterobacterales bacteremia. Diagnostic Microbiology and Infectious Disease, 101(4), p.115505. [CrossRef]
- Hua, X., He, J., Wang, J., Zhang, L., Zhang, L., Xu, Q., Shi, K., Leptihn, S., Shi, Y., Fu, X. and Zhu, P., 2021. Novel tigecycline resistance mechanisms in Acinetobacter baumannii are mediated by mutations in adeS, rpoB, and rrf. Emerging Microbes & Infections, 10(1), pp.1404-1417.
- Jenner, L., Starosta, A.L., Terry, D.S., Mikolajka, A., Filonava, L., Yusupov, M., Blanchard, S.C., Wilson, D.N. and Yusupova, G., 2013. Structural basis for potent inhibitory activity of the antibiotic tigecycline during protein synthesis. Proceedings of the National Academy of Sciences, 110(10), pp.3812-3816. [CrossRef]
- Ji, K., Xu, Y., Sun, J., Huang, M., Jia, X., Jiang, C. and Feng, Y., 2020. Harnessing efficient multiplex PCR methods to detect the expanding Tet (X) family of tigecycline resistance genes. Virulence, 11(1), pp.49-56. [CrossRef]
- Jiang, Y., Jia, X. and Xia, Y., 2019. Risk factors with the development of infection with tigecycline-and carbapenem-resistant Enterobacter cloacae. Infection and drug resistance, pp.667-674.
- Jiang, Y., Yang, S., Deng, S., Lu, W., Huang, Q. and Xia, Y., 2022. Epidemiology and resistance mechanisms of tigecycline-and carbapenem-resistant Enterobacter cloacae in Southwest China: a 5-year retrospective study. Journal of Global Antimicrobial Resistance, 28, pp.161-167. [CrossRef]
- Juan, C.H., Huang, Y.W., Lin, Y.T., Yang, T.C. and Wang, F.D., 2016. Risk factors, outcomes, and mechanisms of tigecycline-nonsusceptible Klebsiella pneumoniae bacteremia. Antimicrobial agents and chemotherapy, 60(12), pp.7357-7363.
- Karami-Zarandi, M., Rahdar, H.A., Esmaeili, H. and Ranjbar, R., 2023. Klebsiella pneumoniae: an update on antibiotic resistance mechanisms. Future Microbiology, 18(1), pp.65-81.
- Karlowsky, J.A., Kazmierczak, K.M., Young, K., Motyl, M.R. and Sahm, D.F., 2020. In vitro activity of ceftolozane/tazobactam against phenotypically defined extended-spectrum β-lactamase (ESBL)-positive isolates of Escherichia coli and Klebsiella pneumoniae isolated from hospitalized patients (SMART 2016). Diagnostic Microbiology and Infectious Disease, 96(4), p.114925.
- Kaye, K.S., Naas, T., Pogue, J.M. and Rossolini, G.M., 2023. Cefiderocol, a siderophore cephalosporin, as a treatment option for infections caused by carbapenem-resistant Enterobacterales. Infectious Diseases and Therapy, 12(3), pp.777-806. [CrossRef]
- Kechagias, K.S., Chorepsima, S., Triarides, N.A. and Falagas, M.E., 2020. Tigecycline for the treatment of patients with Clostridium difficile infection: an update of the clinical evidence. European Journal of Clinical Microbiology & Infectious Diseases, 39, pp.1053-1058.
- Kessel, J., Bender, J., Werner, G., Griskaitis, M., Herrmann, E., Lehn, A., Serve, H., Zacharowski, K., Zeuzem, S., Vehreschild, M.J. and Wichelhaus, T.A., 2021. Risk factors and outcomes associated with the carriage of tigecycline vancomycin-resistant Enterococcus faecium. Journal of Infection, 82(2), pp.227-234.
- Khabbaz, R.F., Moseley, R.R., Steiner, R.J., Levitt, A.M. and Bell, B.P., 2014. Challenges of infectious diseases in the USA. The Lancet, 384(9937), pp.53-63.
- Korczak, L., Majewski, P., Iwaniuk, D., Sacha, P., Matulewicz, M., Wieczorek, P., Majewska, P., Wieczorek, A., Radziwon, P. and Tryniszewska, E., 2024. Molecular mechanisms of tigecycline-resistance among Enterobacterales. Frontiers in Cellular and Infection Microbiology, 14, p.1289396. [CrossRef]
- Korczak, L., Majewski, P., Iwaniuk, D., Sacha, P., Matulewicz, M., Wieczorek, P., Majewska, P., Wieczorek, A., Radziwon, P. and Tryniszewska, E., 2024. Molecular mechanisms of tigecycline-resistance among Enterobacterales. Frontiers in Cellular and Infection Microbiology, 14, p.1289396.
- Korczak, L., Majewski, P., Iwaniuk, D., Sacha, P., Matulewicz, M., Wieczorek, P., Majewska, P., Wieczorek, A., Radziwon, P. and Tryniszewska, E., 2024. Molecular mechanisms of tigecycline-resistance among Enterobacterales. Frontiers in Cellular and Infection Microbiology, 14, p.1289396.
- Kotb, S., Lyman, M., Ismail, G., Abd El Fattah, M., Girgis, S.A., Etman, A., Hafez, S., El-Kholy, J., Zaki, M.E.S., Rashed, H.A.G. and Khalil, G.M., 2020. Epidemiology of carbapenem-resistant Enterobacteriaceae in Egyptian intensive care units using National Healthcare–associated Infections Surveillance Data, 2011–2017. Antimicrobial Resistance & Infection Control, 9, pp.1-9.
- Lamut, A., Peterlin Mašič, L., Kikelj, D. and Tomašič, T., 2019. Efflux pump inhibitors of clinically relevant multidrug resistant bacteria. Medicinal Research Reviews, 39(6), pp.2460-2504. [CrossRef]
- Lee, M., Abbey, T., Biagi, M. and Wenzler, E., 2021. Activity of aztreonam in combination with ceftazidime–avibactam against serine-and metallo-β-lactamase–producing Pseudomonas aeruginosa. Diagnostic microbiology and infectious disease, 99(1), p.115227.
- Li, L., Wang, L., Yang, S., Zhang, Y., Gao, Y., Ji, Q., Fu, L., Wei, Q., Sun, F. and Qu, S., 2024. Tigecycline-resistance mechanisms and biological characteristics of drug-resistant Salmonella Typhimurium strains in vitro. Veterinary Microbiology, 288, p.109927.
- Li, X., Quan, J., Yang, Y., Ji, J., Liu, L., Fu, Y., Hua, X., Chen, Y., Pi, B., Jiang, Y. and Yu, Y., 2016. Abrp, a new gene, confers reduced susceptibility to tetracycline, glycylcine, chloramphenicol, and fosfomycin classes in Acinetobacter baumannii. European Journal of Clinical Microbiology & Infectious Diseases, 35(8), pp.1371-1375.
- Li, Y.Y., Wang, J., Wang, R. and Cai, Y., 2020. Double-carbapenem therapy in the treatment of multidrug resistant Gram-negative bacterial infections: a systematic review and meta-analysis. BMC Infectious Diseases, 20, pp.1-13. [CrossRef]
- Lowe, M., Shuping, L. and Perovic, O., 2022. Carbapenem-resistant Enterobacterales in patients with bacteremia at tertiary academic hospitals in South Africa, 2019-2020: An update. South African Medical Journal, 112(8), pp.545-552.
- Luchao Lv, L., Wan, M., Wang, C., Gao, X., Yang, Q., Partridge, S.R., Wang, Y., Zong, Z., Shen, J., Jia, P. and Song, Q., 2020. The emergence of a Plasmid-Encoded Resistance-Nodulation-Division Efflux Pump Conferring Resistance to Multiple Drugs, Including Tigecycline, in Klebsiella pneumoniae.
- Marot, J.C., Jonckheere, S., Munyentwali, H., Belkhir, L., Vandercam, B. and Yombi, J.C., 2012. Tigecycline-induced acute pancreatitis: about two cases and review of the literature. Acta Clinica Belgica, 67(3), pp.229-232.
- Moore, I.F., Hughes, D.W. and Wright, G.D., 2005. Tigecycline is modified by the flavin-dependent monooxygenase TetX. Biochemistry, 44(35), pp.11829-11835.
- Mzimela, B.W., Nkwanyana, N.M. and Singh, R., 2021. Clinical outcome of neonates with Carbapenem-resistant Enterobacteriaceae infections at the King Edward VIII Hospital’s neonatal unit, Durban, South Africa. Southern African Journal of Infectious Diseases, 36(1), p.223.
- Ni WenTao, N.W., Han YuLiang, H.Y., Liu Jie, L.J., Wei ChuanQi, W.C., Zhao Jin, Z.J., Cui JunChang, C.J., Wang Rui, W.R. and Liu YouNing, L.Y., 2016. Tigecycline treatment for carbapenem-resistant Enterobacteriaceae infections: a systematic review and meta-analysis.
- Olayiwola, J.O., Ojo, D.A., Balogun, S.A. and Ojo, O.E., 2021. Global Spread of Carbapenem-Resistant Enterobacteriaceae: A Challenging Threat to the Treatment of Bacterial Diseases in Clinical Practice. International Journal of Research and Innovation in Applied Science, 6(10), pp.52-60. [CrossRef]
- Onuk, S.E.V.D.A., Coruh, A., Kilic, A.Y.Ş.E.G.Ü.L., EREN, E. and GÜNDOĞAN, K., 2023. The frequency of ESBL producing bacterial infections and related antimicrobial susceptibility in ICU patients: A five-year longitudinal study ESBL producing bacterial infections in ICU. ANNALS OF CLINICAL AND ANALYTICAL MEDICINE.
- Park, D.R., 2005. Antimicrobial treatment of ventilator-associated pneumonia. Respiratory care, 50(7), pp.932-955.
- Park, S.H., Kim, J.S., Kim, H.S., Yu, J.K., Han, S.H., Kang, M.J., Hong, C.K., Lee, S.M. and Oh, Y.H., 2020. Prevalence of carbapenem-resistant Enterobacteriaceae in Seoul, Korea. Journal of Bacteriology and Virology, 50(2), pp.107-116. [CrossRef]
- Paveenkittiporn, W., Lyman, M., Biedron, C., Chea, N., Bunthi, C., Kolwaite, A. and Janejai, N., 2021. Molecular epidemiology of carbapenem-resistant Enterobacterales in Thailand, 2016–2018. Antimicrobial Resistance & Infection Control, 10(1), p.88.
- Perovic, O., Ismail, H., Quan, V., Bamford, C., Nana, T., Chibabhai, V., Bhola, P., Ramjathan, P., Swe Swe-Han, K., Wadula, J. and Whitelaw, A., 2020. Carbapenem-resistant Enterobacteriaceae in patients with bacteremia at tertiary hospitals in South Africa, 2015 to 2018. European Journal of Clinical Microbiology & Infectious Diseases, 39, pp.1287-1294.
- Ravoor, J., Amirthalingam, S., Mohan, T. and Rangasamy, J., 2020. Antibacterial, anti-biofilm, and angiogenic calcium sulfate-nano MgO composite bone void fillers for inhibiting Staphylococcus aureus infections. Colloid and Interface Science Communications, 39, p.100332. [CrossRef]
- Rempel, S., Stanek, W.K. and Slotboom, D.J., 2019. ECF-type ATP-binding cassette transporters. Annual review of biochemistry, 88, pp.551-576. [CrossRef]
- Rizzo, K., Horwich-Scholefield, S. and Epson, E., 2019. Carbapenem and cephalosporin resistance among Enterobacteriaceae in healthcare-associated infections, California, USA. Emerging Infectious Diseases, 25(7), p.1389.
- Rodrigues, Y.C., Lobato, A.R.F., Quaresma, A.J.P.G., Guerra, L.M.G.D. and Brasiliense, D.M., 2021. The spread of NDM-1 and NDM-7-producing Klebsiella pneumoniae is driven by multiclonal expansion of high-risk clones in healthcare institutions in the state of Pará, Brazilian Amazon Region. Antibiotics, 10(12), p.1527.
- Rodvold, K.A., Gotfried, M.H., Cwik, M., Korth-Bradley, J.M., Dukart, G. and Ellis-Grosse, E.J., 2006. Serum, tissue and body fluid concentrations of tigecycline after a single 100 mg dose. Journal of Antimicrobial Chemotherapy, 58(6), pp.1221-1229.
- Sader, H.S., Mendes, R.E., Streit, J.M., Carvalhaes, C.G. and Castanheira, M., 2022. Antimicrobial susceptibility of Gram-negative bacteria from intensive care unit and non-intensive care unit patients from United States hospitals (2018–2020). Diagnostic Microbiology and Infectious Disease, 102(1), p.115557.
- Saeed, N.K., Alkhawaja, S., Azam, N.F.A.E.M., Alaradi, K. and Al-Biltagi, M., 2019. Epidemiology of carbapenem-resistant Enterobacteriaceae in a Tertiary Care Center in the Kingdom of Bahrain. Journal of laboratory physicians, 11(02), pp.111-117.
- Sah, R., BEGUM, S. and Anbumani, N., 2022. Colistin and Tigecycline susceptibility among carbapenemase producing Enterobacteriaceae at a tertiary care hospital of South India. Microbes and Infectious Diseases, 3(2), pp.387-397.
- Seifert, H., Blondeau, J. and Dowzicky, M.J., 2018. In vitro activity of tigecycline and comparators (2014–2016) among key WHO ‘priority pathogens’ and longitudinal assessment (2004–2016) of antimicrobial resistance: a report from the TEST study. International journal of antimicrobial agents, 52(4), pp.474-484.
- Seifert, H., Blondeau, J., Lucassen, K. and Utt, E.A., 2022. Global update on the in vitro activity of tigecycline and comparators against isolates of Acinetobacter baumannii and rates of resistant phenotypes (2016–2018). Journal of Global Antimicrobial Resistance, 31, pp.82-89.
- Sekyerea, J.O., Pedersenb, T., Sivertsenb, A., Govindena, U., Essacka, S.Y., Moodleyc, K., Samuelsenb, O. and Sundsfjordb, A., 2016. Molecular epidemiology of carbapenem, colistin, and tigecycline resistant Enterobacteriaceae in Durban, South Africa.
- Sheykhsaran, E., Baghi, H.B., Soroush, M.H. and Ghotaslou, R., 2019. An overview of tetracyclines and related resistance mechanisms. Reviews and Research in Medical Microbiology, 30(1), pp.69-75.
- Shi, S., Xu, M., Zhao, Y., Feng, L., Liu, Q., Yao, Z., Sun, Y., Zhou, T. and Ye, J., 2023. Tigecycline–Rifampicin Restrains Resistance Development in Carbapenem-Resistant Klebsiella pneumoniae. ACS Infectious Diseases, 9(10), pp.1858-1866.
- Soraci, L., Cherubini, A., Paoletti, L., Filippelli, G., Luciani, F., Laganà, P., Gambuzza, M.E., Filicetti, E., Corsonello, A. and Lattanzio, F., 2023. Safety and tolerability of antimicrobial agents in the older patient. Drugs & Aging, 40(6), pp.499-526. [CrossRef]
- Stein, G.E. and Babinchak, T., 2013. Tigecycline: an update. Diagnostic microbiology and infectious disease, 75(4), pp.331-336.
- Su, W., Wang, W., Li, L., Zhang, M., Xu, H., Fu, C., Pang, X. and Wang, M., 2024. Mechanisms of tigecycline resistance in Gram-negative bacteria: A narrative review. Engineering Microbiology, p.100165.
- Sun, C., Yu, Y. and Hua, X., 2023. Resistance mechanisms of tigecycline in Acinetobacter baumannii. Frontiers in Cellular and Infection Microbiology, 13, p.1141490. [CrossRef]
- Swaminathan, S. and Kundu, P., 2020. Tigecycline: Role in the Management of cIAI and cSSTI in the Indian Context. Indian Journal of Clinical Medicine, 10(1-2), pp.24-30.
- Tamma, P.D., Goodman, K.E., Harris, A.D., Tekle, T., Roberts, A., Taiwo, A. and Simner, P.J., 2017. Comparing the outcomes of patients with carbapenemase-producing and non-carbapenemase-producing carbapenem-resistant Enterobacteriaceae bacteremia. Clinical Infectious Diseases, 64(3), pp.257-264.
- Tootla, H.D., Prentice, E., Moodley, C., Marais, G., Nyakutira, N., Reddy, K., Bamford, C., Niehaus, A., Whitelaw, A. and Brink, A., 2024. Carbapenem-resistant Enterobacterales among hospitalized patients in Cape Town, South Africa: clinical and microbiological epidemiology. JAC-Antimicrobial Resistance, 6(2), p.dlae051. [CrossRef]
- Turner, A.M., Li, L., Monk, I.R., Lee, J.Y.H., Ingle, D.J., Duchene, S., Sherry, N.L., Stinear, T.P., Kwong, J.C., Gorrie, C.L. and Howden, B.P., 2023. Rifaximin prophylaxis causes resistance to the last-resort antibiotic daptomycin. medRxiv, pp.2023-03.
- Varma, M., Reddy, L.R., Vidyasagar, S., Holla, A. and Bhat, N.K., 2018. Risk factors for carbapenem resistant enterobacteriaceae in a teritiary hospital—A case control study. Indian Journal of Medical Specialities, 9(4), pp.178-183. [CrossRef]
- Venter, H., Mowla, R., Ohene-Agyei, T. and Ma, S., 2015. RND-type drug efflux pumps from Gram-negative bacteria: molecular mechanism and inhibition. Frontiers in microbiology, 6, p.135560.
- Viechtbauer, W. and Cheung, M.W.L., 2010. Outlier and influence diagnostics for meta-analysis. Research synthesis methods, 1(2), pp.112-125.
- Vink, J.P., Otter, J.A. and Edgeworth, J.D., 2020. Carbapenemase-producing Enterobacteriaceae–once positive always positive?. Current Opinion in Gastroenterology, 36(1), pp.9-16.
- Vogelaers, D., Blot, S., Van den Berge, A. and Montravers, P., 2021. Antimicrobial lessons from a large observational cohort on intra-abdominal infections in intensive care units. Drugs, 81(9), pp.1065-1078.
- Wang, J., Pan, Y., Shen, J. and Xu, Y., 2017. The efficacy and safety of tigecycline for the treatment of bloodstream infections: a systematic review and meta-analysis. Annals of clinical microbiology and antimicrobials, 16, pp.1-10.
- Wang, L., Tong, X., Huang, J., Zhang, L., Wang, D., Wu, M., Liu, T. and Fan, H., 2020. Triple versus double therapy for the treatment of severe infections caused by carbapenem-resistant Enterobacteriaceae: A systematic review and meta-analysis. Frontiers in Pharmacology, 10, p.487865.
- Weiner, L.M., Webb, A.K., Limbago, B., Dudeck, M.A., Patel, J., Kallen, A.J., Edwards, J.R. and Sievert, D.M., 2016. Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2011–2014. infection control & hospital epidemiology, 37(11), pp.1288-1301. [CrossRef]
- Wilson, L.A. and Kuruvilla, T.S., 2023. Evaluation of in vitro activity of tigecycline against multidrug-resistant clinical isolates. APIK Journal of Internal Medicine, 11(3), pp.150-153. [CrossRef]
- Woodworth, K.R., 2018. Vital signs: containment of novel multidrug-resistant organisms and resistance mechanisms—United States, 2006–2017. MMWR. Morbidity and mortality weekly report, 67.
- World Health Organization, 2014. Antimicrobial resistance: global report on surveillance. World Health Organization.
- Yaghoubi, S., Zekiy, A.O., Krutova, M., Gholami, M., Kouhsari, E., Sholeh, M., Ghafouri, Z. and Maleki, F., 2022. Tigecycline antibacterial activity, clinical effectiveness, and mechanisms and epidemiology of resistance: narrative review. European Journal of Clinical Microbiology & Infectious Diseases, pp.1-20.
- Yaghoubi, S., Zekiy, A.O., Krutova, M., Gholami, M., Kouhsari, E., Sholeh, M., Ghafouri, Z. and Maleki, F., 2022. Tigecycline antibacterial activity, clinical effectiveness, and mechanisms and epidemiology of resistance: narrative review. European Journal of Clinical Microbiology & Infectious Diseases, pp.1-20.
- Yu, W.L., Lee, N.Y., Wang, J.T., Ko, W.C., Ho, C.H. and Chuang, Y.C., 2020. Tigecycline therapy for infections caused by extended-spectrum β-lactamase-producing enterobacteriaceae in critically ill patients. Antibiotics, 9(5), p.231. [CrossRef]
- Yu, W.L., Lee, N.Y., Wang, J.T., Ko, W.C., Ho, C.H. and Chuang, Y.C., 2020. Tigecycline therapy for infections caused by extended-spectrum β-lactamase-producing Enterobacteriaceae in critically ill patients. Antibiotics, 9(5), p.231. [CrossRef]
- Zeng, M., Xia, J., Zong, Z., Shi, Y., Ni, Y., Hu, F., Chen, Y., Zhuo, C., Hu, B., Lv, X. and Li, J., 2023. Guidelines for the diagnosis, treatment, prevention, and control of infections caused by carbapenem-resistant gram-negative bacilli. Journal of Microbiology, Immunology and Infection, 56(4), pp.653-671. [CrossRef]
- Zha, L., Pan, L., Guo, J., French, N., Villanueva, E.V. and Tefsen, B., 2020. Effectiveness and safety of high dose tigecycline for the treatment of severe infections: a systematic review and meta-analysis. Advances in therapy, 37, pp.1049-1064.
- Zha, L., Pan, L., Guo, J., French, N., Villanueva, E.V. and Tefsen, B., 2020. Effectiveness and safety of high dose tigecycline for the treatment of severe infections: a systematic review and meta-analysis. Advances in therapy, 37, pp.1049-1064.
- Zhang, R.M., Sun, J., Sun, R.Y., Wang, M.G., Cui, C.Y., Fang, L.X., Liao, M.N., Lu, X.Q., Liu, Y.X., Liao, X.P. and Liu, Y.H., 2021. Source tracking and global distribution of the tigecycline non-susceptible tet (X). Microbiol Spectr 9: e0116421. [CrossRef]
- Zhang, S., Wen, J., Wang, Y., Wang, M., Jia, R., Chen, S., Liu, M., Zhu, D., Zhao, X., Wu, Y. and Yang, Q., 2022. Dissemination and prevalence of plasmid-mediated high-level tigecycline resistance gene tet (X4). Frontiers in Microbiology, 13, p.969769. [CrossRef]
- Zhang, S., Wen, J., Wang, Y., Wang, M., Jia, R., Chen, S., Liu, M., Zhu, D., Zhao, X., Wu, Y. and Yang, Q., 2022. Dissemination and prevalence of plasmid-mediated high-level tigecycline resistance gene tet (X4). Frontiers in Microbiology, 13, p.969769. [CrossRef]
- Zhang, Y., Wang, Q., Yin, Y., Chen, H., Jin, L., Gu, B., Xie, L., Yang, C., Ma, X., Li, H. and Li, W., 2018. Epidemiology of carbapenem-resistant Enterobacteriaceae infections: report from the China CRE Network. Antimicrobial agents and chemotherapy, 62(2), pp.10-1128. [CrossRef]
- Zhou, C.C., Huang, F., Zhang, J.M. and Zhuang, Y.G., 2023. Population pharmacokinetics of tigecycline: a systematic review. Drug Design, Development and Therapy, pp.1885-1896.
- Zhu, Y., Zhao, F. and Jin, P., 2023. Clinical Manifestations and Risk Factors of Tigecycline-Associated Thrombocytopenia. Infection and Drug Resistance, pp.6225-6235. [CrossRef]
- Zou, C., Xu, C., Yu, R., Shan, X., Schwarz, S., Li, D. and Du, X.D., 2024. Tandem amplification of a plasmid-borne tet (A) variant gene confers tigecycline resistance in Escherichia coli. Journal of Antimicrobial Chemotherapy, 79(6), pp.1294-1302. [CrossRef]
Figure 1.
A clustered bar graph representing CRE distribution in Mthatha and surrounding wards.
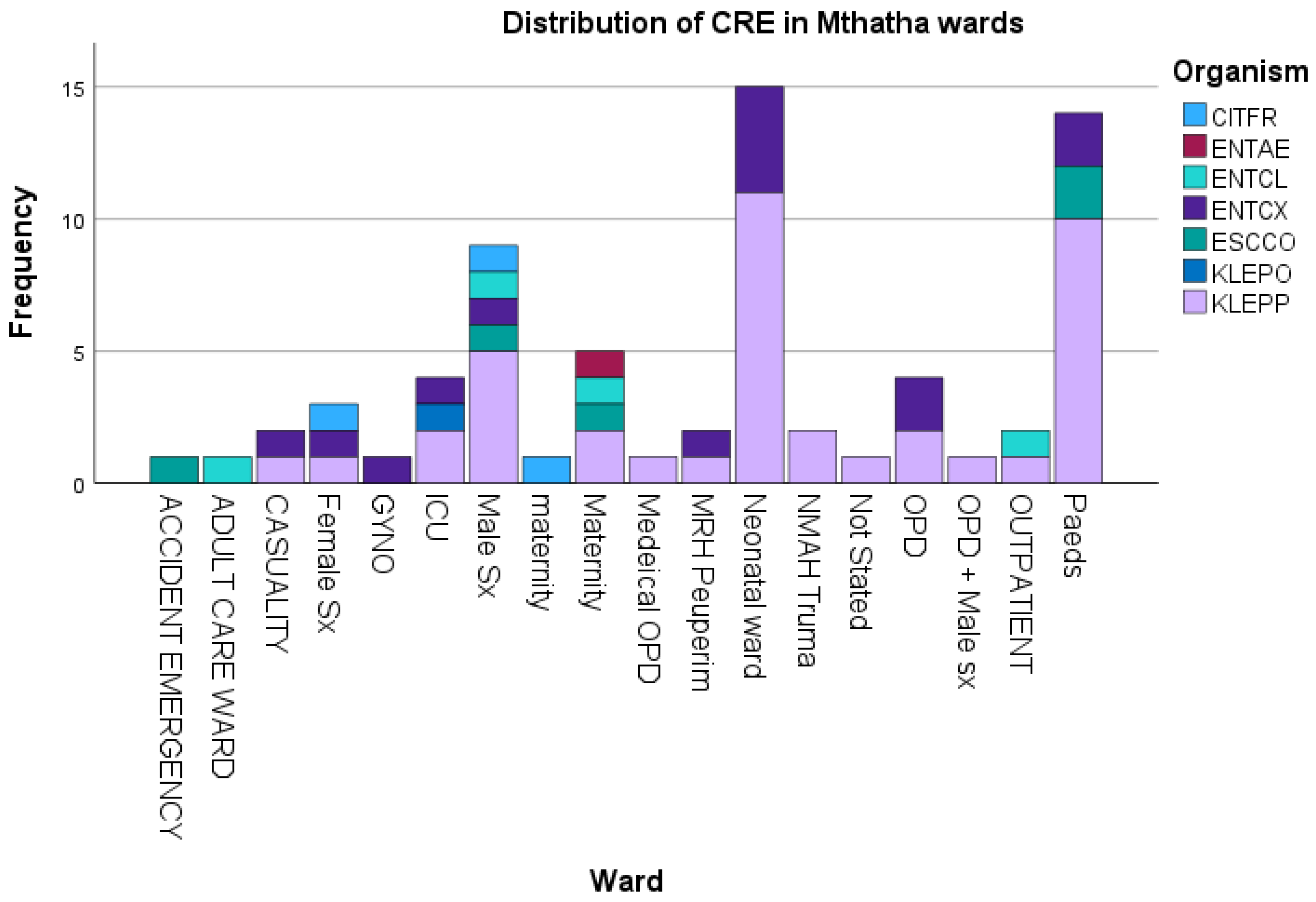
Figure 2.
A boxplot showing CRE distribution by gender.

Table 2.
Showing the association between Tigecycline resistance and risk factors by P-values and R-values.
Table 2.
Showing the association between Tigecycline resistance and risk factors by P-values and R-values.
| Tigecycline susceptibility | ||||||
|---|---|---|---|---|---|---|
| Tigecycline Resistance Risk factor | No. of CRE (%) | S | R | I | P-value | r2 |
| Wards | 0.1631 | 0.4182 | ||||
| Accident Emergency | 1.43 | 100 | 0 | 0 | ||
| Adult care | 1.43 | 100 | 0 | 0 | ||
| Casualty | 2.86 | 100 | 0 | 0 | ||
| Female Surgical | 4.29 | 100 | 0 | 0 | ||
| Gyno | 1.43 | 100 | 0 | 0 | ||
| ICU | 5.71 | 75 | 25 | 0 | ||
| Male Surgical | 14.29 | 100 | 0 | 0 | ||
| Maternity | 8.57 | 100 | 0 | 0 | ||
| Neonatal | 24.29 | 94.11 | 0 | 5.88 | ||
| Trauma | 2.86 | 100 | 0 | 0 | ||
| Not stated (unknown) | 1.43 | 100 | 0 | 0 | ||
| OPD | 11.43 | 100 | 0 | 0 | ||
| Pediatrics | 20 | 100 | 0 | 0 | ||
| Age | 0.0011 | 0.9501 | ||||
| 0-1 | 42.86 | 98.57 | 0 | 1.43 | ||
| 2_15 | 2.8 | 100 | 0 | 0 | ||
| 16-29 | 11.42 | 100 | 0 | 0 | ||
| 30-43 | 8.57 | 98.57 | 1.43 | 0 | ||
| 44-56 | 8.57 | 100 | 0 | 0 | ||
| 57-70 | 11.42 | 100 | 0 | 0 | ||
| 71-83 | 7.14 | 100 | 0 | 0 | ||
| 84-96 | 5.71 | 100 | 0 | 0 | ||
| 97-109 | 0 | 0 | 0 | 0 | ||
| Gender | 0.001 | 0.991 | ||||
| Males | 47.88 | 97.05 | 2.94 | 100 | ||
| Females | 50.7 | 100 | 100 | 2.94 | ||
| Not Started | 1.43 | 100 | 100 | 100 | ||
| Prio-exposureto antibiotics | 0.0478 | 0.967 | ||||
| antibiotics intake | 75.71 | 98.11 | 1.88 | 0 | ||
| No-antibiotics taken | 24.29 | 94.41 | 0 | 5.88 | ||
| Invasive Procedure | ||||||
| underwent procedure | 5.63 | 75 | 25 | 0 | <0.0001 | |
| No procedure done | 94.37 | 98.51 | 1.49 | 0 | ||
| Hospitalization duration | 0.3679 | |||||
| Prolong | 10 | 98.69 | 1.41 | 0 | ||
| standardized | 90 | 98.68 | 0 | 1.41 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



