
Submitted:
15 February 2025
Posted:
17 February 2025
You are already at the latest version
Abstract
Pancreatic ductal adenocarcinoma (PDAC) is a highly aggressive malignancy with limited treatment options. Identifying reliable prognostic biomarkers is crucial for risk stratification and therapeutic decision-making. This study investigates the prognostic significance of Claudin 18.2 (CLDN18.2), isocitrate dehydrogenase-1 (IDH1) expression, and the neutrophil-to-lymphocyte ratio (NLR) in patients with unresectable PDAC receiving first-line chemotherapy.
This retrospective, single-center study included 72 patients with histologically confirmed unresectable PDAC treated with either FOLFIRINOX (59.7%) or gemcitabine plus nab-paclitaxel (40.3%). Immunohistochemistry was performed to assess CLDN18.2 and IDH1 expression, while NLR was calculated from pre-treatment blood counts. Univariable and multivariable analyses were conducted to evaluate predictors of progression-free survival (PFS) and overall survival (OS).
CLDN18.2 and IDH1 were positively expressed in 18.1% and 2.8% of patients, respectively, while 56.9% had elevated NLR (>3.22). The median PFS was 7.1 months (95% CI: 4.2–9.9), and the median OS was 9.7 months (95% CI: 8.5–10.8). Multivariable analysis identified negative CLDN18.2 expression (HR = 0.38, 95% CI: 0.18–0.81, p = 0.013), positive IDH1 expression (HR = 0.68, 95% CI: 0.19–0.72, p = 0.039), and high NLR (HR = 1.92, 95% CI: 1.03–3.56, p = 0.038) as independent predictors of poorer OS. No independent predictors of PFS were identified.
CLDN18.2 and IDH1 expression, along with NLR, are independent prognostic markers for OS in patients with unresectable PDAC undergoing first-line chemotherapy. These biomarkers may facilitate risk stratification and guide personalized treatment strategies. Further prospective validation is warranted to confirm their clinical utility.
Keywords:
Pancreatic ductal adenocarcinoma
; Claudin 18.2
; Isocitrate dehydrogenase-1
; Neutrophil-to-lymphocyte ratio
; Prognostic biomarkers
; Overall survival
1. Introduction
Pancreatic ductal adenocarcinoma (PDAC), the most prevalent type of pancreatic neoplasm, is a highly aggressive and lethal malignancy due to the lack of early diagnosis and limited treatment response [1,2,3]. Despite advances in understanding PDAC biology and developing novel therapies, the 5-year survival rate remains below 10% [4]. Surgery is the only potentially curative option, but most patients present with unresectable locally advanced or metastatic disease [5]. Consequently, chemotherapy with FOLFIRINOX or gemcitabine is used to alleviate progression and prolong life in unresectable PDAC [4,6]. Immunotherapy is also being explored, despite challenges posed by PDAC non-immunogenic and therapy-resistant microenvironment [7]. Potential immunotherapy targets include claudin 18.2 (CLDN18.2), a specific tight junction protein overexpressed in PDAC [8,9,10,11,12]. The therapeutic antibody zolbetuximab, which targets CLDN18.2, is currently in clinical trials [11,13].
Notably, CLDN18.2 may also serve as a prognostic predictor, as its expression significantly correlated with survival in two prior studies [11,12]. Another molecule overexpressed in PDAC is wild-type isocitrate dehydrogenase-1 (IDH1) [14]. This enzyme protects cancer cells under chemotherapy-induced oxidative stress and may contribute to chemoresistance [15]. Pharmacologic IDH1 inhibition is being investigated in combination with chemotherapy for various malignancies, including PDAC [15,16]. Additionally, the neutrophil-to-lymphocyte ratio (NLR), routinely derived from complete blood counts, has been extensively studied as a marker of immune response and clinical outcomes in PDAC [17,18,19].
Although unresectable PDAC carries a dismal prognosis [1,2,3,4], the identification of predictive biomarkers has the potential to optimize patient stratification, pinpoint therapeutic targets, and refine predictive models. To this end, we conducted the present study to evaluate the prognostic value of immunohistochemical expression of CLDN18.2 and IDH1, as well as the NLR, in patients with unresectable PDAC undergoing first-line chemotherapy.
2. Materials and Methods
2.1. Patients and Procedures
This single-center retrospective study, using data from prospectively collected consecutive patients, was conducted in accordance with the Declaration of Helsinki. The study protocol was reviewed and approved by the Ethics Committee of Medipol Mega University Hospital, Istanbul, Türkiye (approval number: 10840098-772.02-7244; approval date: December 15, 2023) and informed consent was obtained from the patient or first-degree relative. All procedures and patient visits were conducted at the Medipol Mega University Hospital between January 2014 and November 2023. Patients were eligible for inclusion in this study if they met the following criteria: 1) a histologically confirmed diagnosis of unresectable PDAC; 2) treatment with first-line chemotherapy; 3) availability of whole-tissue sections from tumor biopsies for immunohistochemical analysis; and 4) availability of pretreatment complete blood count results for the calculation of the NLR. Patients were excluded from the study if they had any of the following: 1) a history of previous or concurrent malignancies at other sites; 2) a diagnosis of pancreatic neuroendocrine tumor; 3) contraindications to chemotherapy; 4) uncontrolled comorbidities; or 5) incomplete follow-up data.
2.2. Chemotherapy Protocol
All patients were administered either the FOLFIRINOX regimen or the combination of gemcitabine and nab-paclitaxel as first-line treatment for a minimum of three months [6]. The FOLFIRINOX protocol included 5-fluorouracil (400 mg/m2 intravenous bolus on day 1, followed by a 2400 mg/m2 continuous infusion over 46 hours), oxaliplatin (85 mg/m2 intravenously over 2 hours on day 1), and irinotecan (180 mg/m2 intravenously over 90 minutes on day 1). The gemcitabine plus nab-paclitaxel regimen comprised gemcitabine (1000 mg/m2 intravenous infusion over 30−40 minutes, immediately following nab-paclitaxel on days 1, 8, and 15 of each 28-day cycle) and albumin-bound paclitaxel (nab-paclitaxel; 125 mg/m2 intravenous infusion over 30−40 minutes on days 1, 8, and 15 of each 28-day cycle).
2.3. Data Collection
The following variables were collected from all patients included in the study: age, sex, smoking history, alcohol consumption, presence of weight loss, presence of jaundice at initial presentation, history of diabetes, presence of metastasis at initial presentation, primary tumor localization, presence of visceral metastasis at initial presentation, and type of first-line chemotherapy regimen administered.
2.4. Immunohistochemistry
Immunohistochemistry targeting CLDN18.2 and IDH1 was performed on whole-tissue sections of tumor biopsies, including tru-cut biopsies and samples from resection materials. Sections of 2 μm thickness were prepared from paraffin-embedded blocks. Automated immunohistochemical staining was conducted on a BenchMark ULTRA instrument (Ventana Medical Systems, Tucson, AZ, USA) for all cases. A rabbit polyclonal antibody against Claudin-18.2 (ER1902-86, 1:250 dilution; HuaBio, Hangzhou, China) and a mouse monoclonal antibody clone H09 against IDH1 R132H (1:20 dilution; Dianova, Hamburg, Germany) were used. Both antibodies were applied using the UltraView DAB IHC Detection Kit (Ventana Medical Systems) according to the manufacturer’s protocol. Claudin-18.2 staining was further amplified using the UltraView Amplification Kit (Ventana Medical Systems). Appropriate positive controls were included on each slide, consisting of IDH1-positive oligodendroglioma tissue and normal human stomach tissue expressing claudin-18.2.
Stained samples were evaluated independently by two qualified pathologists. The evaluation of claudin-18.2 immunostaining was performed using a dual-component scoring system, which involved assessing the staining intensity and quantifying the percentage of tumor cells stained at various intensities relative to the total tumor cell count in the sample. The staining intensity was graded on a scale of 0 to 3, with 0 indicating no membrane or cytoplasmic reactivity, 1 indicating weak membrane or cytoplasmic reactivity, 2 indicating moderate membrane or cytoplasmic reactivity, and 3 indicating strong membrane or cytoplasmic reactivity (Figure 1).
Complete basolateral and lateral membrane staining was taken into consideration when assessing the staining intensity. Samples were classified as CLDN18.2-positive if they exhibited a staining intensity of 2 or higher in at least 40% of the tumor cells [20]. For the determination of IDH1 expression status, samples were considered IDH1-positive if they demonstrated granular cytoplasmic staining with a minimum intensity of 1 in any proportion of tumor cells (Figure 2) [21].
2.5. Calculation of Neutrophil-to-Lymphocyte Ratio
The NLR prior to chemotherapy was determined by dividing the absolute neutrophil count by the absolute lymphocyte count [19]. For the purpose of analysis, patients were dichotomized into two groups based on the median NLR value (3.22) observed in the study cohort, i.e., NLR ≤ 3.22 versus NLR > 3.22.
2.6. Survival Endpoints
Progression-free survival (PFS) was defined as the time interval from the initiation of chemotherapy until objective disease progression or death from any cause, whichever occurred first [22]. Overall survival (OS) was measured from the start of chemotherapy until death from any cause or the date of last follow-up, if the patient remained alive [22]. The surveillance protocol was implemented following the commencement of chemotherapy and continued until the final follow-up visit, which took place in March 2024.
2.7. Data Analysis
Data are presented using descriptive statistics. Continuous variables were compared using Student’s t-tests, whereas categorical variables were analyzed with chi-square tests. Survival curves were generated using the Kaplan-Meier method. Variables demonstrating an association at a significance level of P <0.20 in univariable analysis were retained in multivariable Cox regression models to identify the independent predictors of survival endpoints. The results of multivariable analyses are reported as adjusted hazard ratios (HRs) accompanied by their corresponding 95% confidence intervals (CIs). All statistical analyses were performed using SPSS, version 22 (IBM, Armonk, NY, USA), with two-sided tests at a 5% level of significance.
3. Results
3.1. Patient Characteristics
The study included 72 patients (33 women and 39 men) with a mean age of 63.5 years (range: 42−88 years). Table 1 presents an overview of the patient general characteristics. Over half of the participants had a history of smoking (54.2%) and diabetes (61.1%). The most common presenting symptoms were weight loss (61.1%) and jaundice (58.3%). The primary tumor was most frequently located in the head (45.8%) and body (43.1%) of the pancreas. At initial diagnosis, 42.3% of patients had metastatic disease, with 35.3% having visceral metastases. First-line chemotherapy consisted of FOLFIRINOX (59.7%) and gemcitabine plus nab-paclitaxel (40.3%). Immunohistochemical analysis revealed positive expression of CLDN18.2 in 13 patients (18.1%) and IDH1 in 2 patients (2.8%). Additionally, 41 patients (56.9%) had an elevated NLR above 3.22.
3.2. Progression-Free Survival
The median PFS was 7.1 months (95% CI = 4.2−9.9 months; Figure 3). Table 2 presents the results of univariable and multivariable analyses for different pretreatment variables in relation to PFS. In the univariable analysis, only positive IDH1 expression was associated with less favorable PFS (P = 0.033). However, after adjusting for potential confounders in the multivariable analysis, this association was no longer significant, and no independent predictors of PFS were identified.
3.3. Overall Survival
The median OS was 9.7 months (95% CI = 8.5−10.8 months; Figure 4). Table 3 summarizes the results of univariable and multivariable analyses for different pretreatment variables in relation to OS. In the univariable analysis, negative CLDN18.2 expression (P = 0.006), positive IDH1 expression (P = 0.039), and high NLR (P = 0.038) were associated with less favorable OS. Notably, these three variables were the only factors that showed independent associations with OS in the multivariable analysis. The adjusted HRs were 0.38 (95% CI = 0.18−0.81, P = 0.013) for CLDN18.2 expression, 0.68 (95% CI = 0.19−0.72, P = 0.039) for IDH1 expression, and 1.92 (95% CI = 1.03−3.56, P = 0.038) for NLR.
4. Discussion
In this retrospective study utilizing prospectively collected data from patients with unresectable PDAC undergoing first-line chemotherapy, we found that negative CLDN18.2 expression, positive IDH1 expression, and elevated NLR were independently associated with less favorable OS. However, none of these three biomarkers emerged as independent predictors of PFS.
Several previous investigations have evaluated CLDN18.2 expression in pancreatic cancer. In a seminal study, Sahin et al. [8] examined the expression of CLDN18.2 in various solid tumors, including 10 PDAC samples. CLDN18.2 expression was identified in 80% of the samples, with 60% exhibiting a staining intensity ≥ 2. Subsequently, Wöll et al. [9] reported that 59.2% of primary PDAC samples were CLDN18.2-positive by immunohistochemistry, with 54.6% displaying staining intensities ≥ 2. Although they did not investigate the relationship between CLDN18.2 expression and prognosis, their findings suggested that a considerable number of pancreatic neoplasms would be eligible for a CLDN18.2-targeting approach [9]. In a study of 130 patients with surgically resected PDAC, Park et al. [10] reported positive immunohistochemical expression of CLDN18.2 in 31.5% of specimens.
Notably, the positive CLDN18.2-expressing group showed no statistically significant difference in median OS compared to the negative CLDN18.2-expressing group (17.4 months versus 20.6 months, respectively). In a separate study, Wang et al. [11] analyzed the expression of CLDN18.2 in 93 primary PDACs, 86 para-cancer tissues, and 13 normal pancreatic tissues using immunohistochemistry. They found that CLDN18.2 was expressed in 88 (94.6%) of the reported PDACs, with 50 (56.8%) cases showing strong immunostaining [11]. Furthermore, CLDN18.2 expression correlated with cancer survival in PDAC patients with stage III, stage IV, and distant metastasis [11]. Recently, Kayikcioglu and Yüceer [12] examined 68 patients with PDAC and detected a CLDN18.2 expression ≥ 2 in 23.5% of the samples. Interestingly, they found that higher CLDN18.2 expression was associated with longer OS [12]. At least two factors may explain the conflicting findings on the prognostic value of CLDN18.2 expression in pancreatic cancer.
First, differences in immunohistochemistry methods, staining clones, expression patterns, and scoring systems can lead to heterogeneous CLDN18.2 positivity and its association with clinical outcomes. Second, patient characteristics, such as disease stage and treatment, may also influence the observed relationship between CLDN18.2 and survival.
In the present study, both the rate of CLDN18.2 positivity (18.1%) and its favorable impact on OS were generally consistent with the findings reported by Kayikcioglu and Yüceer [12]. This observation may appear counterintuitive, considering that CLDN18.2 is a promising immunotherapy target in PDAC [9,11,13]. However, our findings suggest that negative CLDN18.2 expression may be associated with a highly aggressive tumor behavior in unresectable pancreatic malignancies, rendering these neoplasms less suitable for clinical trials investigating zolbetuximab. This hypothesis warrants further investigation to elucidate the underlying mechanisms and potential implications for patient selection in CLDN18.2-targeted therapies.
Another finding from our study is that patients with positive IDH1 expression and a high NLR had less favorable OS. As for IDH1, the most likely mechanism mediating the observed effect is that isocitrate is changed by this enzyme into alpha-ketoglutarate and NADPH, which shield cancer cells from chemotherapy-induced oxidative stress [16,23]. Targeting IDH1 is an attractive strategy for cancers with IDH1 overexpression [23]. Several small molecule inhibitors of mutant IDH1, like ivosidenib, have been developed and are being evaluated in clinical trials for various cancers [23], and combining IDH1 inhibitors with chemotherapy warrants further study in PDAC with IDH1 expression [24].
Lowering the NLR by targeting inflammation and enhancing anti-tumor immunity is another potential approach [25], and anti-inflammatory agents [26], neutrophil-depleting therapies [27], and immune checkpoint inhibitors [28] are all being explored in PDAC. Stratifying patients based on CLDN18.2, IDH1, and NLR status may potentially help identify subgroups most likely to benefit from targeted treatments for unresectable PDAC with the goal of improving OS.
Although our study identified these biomarkers as independent predictors of OS, we did not observe a significant association with PFS. This discrepancy may be attributed to several factors. First, CLDN18.2 and IDH1 are molecules that reflect intrinsic tumor biology, while NLR is an indicator of the host’s systemic inflammatory response. Collectively, these factors play a pivotal role in determining a patient’s OS, as they represent the complex interplay between the tumor and the host’s immune system. In contrast, PFS may be more directly influenced by the efficacy of specific treatment modalities, rather than these underlying biological factors [22].
Secondly, it is important to consider that OS is a more objective and definitive endpoint, as it measures the time from diagnosis or treatment initiation to death from any cause. PFS, on the other hand, relies on more subjective assessments of disease progression based on radiologic findings and clinical criteria, which may be prone to interpretation bias [22]. Finally, the relatively small sample size of our study may have limited its statistical power to detect significant associations between these biomarkers and PFS.
Our findings should be interpreted in the context of several additional limitations. First, the retrospective, single-center design with a convenience sample may limit the generalizability of the results. Larger prospective studies are necessary to validate the prognostic significance of these biomarkers. Second, the evaluation of CLDN18.2 and IDH1 immunohistochemical expression was based on a single biopsy sample for each patient, which may not fully capture the spatial heterogeneity within the tumor [11]. Examining multiple biopsy sites could provide a more comprehensive assessment. Third, the molecular mechanisms underlying the prognostic impact of these biomarkers and their interplay with chemotherapy response were not specifically investigated.
In conclusion, our study demonstrates that the immunohistochemical expression of CLDN18.2 and IDH1, as well as the NLR, are independent prognostic factors for OS in patients with unresectable PDAC treated with first-line chemotherapy. These findings highlight the potential of these biomarkers for risk stratification and treatment personalization in this challenging disease setting. However, further prospective validation and mechanistic investigations are warranted to confirm their clinical relevance and explore their therapeutic implications in PDAC.
Author Contributions
Conceptualization, E.K. and H.M.; methodology, E.K.,A.B.,H.M.; software, E.K, A.B.,H.M.; validation, E.K.,A.B.,Ö.A.,Ö.Y,F.Ö.,E.K. and Ö.F.Ö.; formal analysis, A.B.H.M.,; investigation, E.K.,F.Ö.,E.K., H.M.,Ö.A.,Ö.Y.; resources, E.K., A.B.,H.M.; data curation, E.K.,A.B.,H.M., Ö.A.,Ö.Y,F.Ö.,E.K..; writing—original draft preparation, E.K.,, H.M.; writing—review and editing, E.K., H.M.; visualization, E.K., H.M.; supervision, A.B.; project administration, A.B, E.K..; funding acquisition:no funding. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Istanbul Medipol University (approval number: 10840098-772.02-7244; approval date: December 15,2023)
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Park W, Chawla A, O’Reilly EM. Pancreatic cancer: a review. JAMA. 2021; 326:851- 862. [CrossRef]
- Ushio J, Kanno A, Ikeda E, Ando K, Nagai H, Miwata T, Kawasaki Y, Tada Y, Yokoyama K, Numao N, Tamada K, Lefor AK, Yamamoto H. Pancreatic ductal adenocarcinoma: epidemiology and risk factors. Diagnostics (Basel). 2021; 11:562. [CrossRef]
- Bekkali NLH, Oppong KW. Pancreatic ductal adenocarcinoma epidemiology and risk assessment: Could we prevent? Possibility for an early diagnosis. Endosc Ultrasound. 2017;6(Suppl 3): S58-S61. [CrossRef]
- Principe DR, Underwood PW, Korc M, Trevino JG, Munshi HG, Rana A. The current treatment paradigm for pancreatic ductal adenocarcinoma and barriers to therapeutic efficacy. Front Oncol. 2021; 11:688377. [CrossRef]
- Słodkowski M, Wroński M, Karkocha D, Kraj L, Śmigielska K, Jachnis A. Current approaches for the curative-intent surgical treatment of pancreatic ductal adenocarcinoma. Cancers (Basel). 2023; 15:2584. [CrossRef]
- Orlandi E, Citterio C, Anselmi E, Cavanna L, Vecchia S. FOLFIRINOX or gemcitabine plus nab-paclitaxel as first line treatment in pancreatic cancer: a real-world comparison. Cancer Diagn Progn. 2024; 4:165-171. [CrossRef]
- Chouari T, La Costa FS, Merali N, Jessel MD, Sivakumar S, Annels N, Frampton AE. Advances in immunotherapeutics in pancreatic ductal adenocarcinoma. Cancers (Basel). 2023; 15:4265. [CrossRef]
- Sahin U, Koslowski M, Dhaene K, Usener D, Brandenburg G, Seitz G, Huber C, Türeci O. Claudin-18 splice variant 2 is a pan-cancer target suitable for therapeutic antibody development. Clin Cancer Res. 2008; 14:7624-7634. [CrossRef]
- Wöll S, Schlitter AM, Dhaene K, Roller M, Esposito I, Sahin U, Türeci Ö. Claudin 18.2 is a target for IMAB362 antibody in pancreatic neoplasms. Int J Cancer. 2014; 134:731-739. [CrossRef]
- Park S, Shin K, Kim IH, Hong T, Kim Y, Suh J, Lee M. Clinicopathological features and prognosis of resected pancreatic ductal adenocarcinoma patients with claudin-18 overexpression. J Clin Med. 2023; 12:5394. [CrossRef]
- Wang X, Zhang CS, Dong XY, Hu Y, Duan BJ, Bai J, Wu YY, Fan L, Liao XH, Kang Y, Zhang P, Li MY, Xu J, Mao ZJ, Liu HT, Zhang XL, Tian LF, Li EX. Claudin 18.2 is a potential therapeutic target for zolbetuximab in pancreatic ductal adenocarcinoma. World J Gastrointest Oncol. 2022; 14:1252-1264. [CrossRef]
- Kayikcioglu E, Yüceer RO. The role of claudin 18.2 and HER-2 in pancreatic cancer outcomes. Medicine (Baltimore). 2023;102: e32882. [CrossRef]
- Türeci Ӧ, Mitnacht-Kraus R, Wöll S, Yamada T, Sahin U. Characterization of zolbetuximab in pancreatic cancer models. Oncoimmunology. 2018;8:e1523096. [CrossRef]
- Zarei M, Lal S, Parker SJ, Nevler A, Vaziri-Gohar A, Dukleska K, Mambelli-Lisboa NC, Moffat C, Blanco FF, Chand SN, Jimbo M, Cozzitorto JA, Jiang W, Yeo CJ, Londin ER, Seifert EL, Metallo CM, Brody JR, Winter JM. Posttranscriptional the upregulation of IDH1 by HuR establishes a powerful survival phenotype in pancreaticcancer cells. Cancer Res. 2017; 77:4460-4471. [CrossRef]
- Liu Y, Xu W, Li M, Yang Y, Sun D, Chen L, Li H, Chen L. The regulatory mechanisms and inhibitors of isocitrate dehydrogenase 1 in cancer. Acta Pharm Sin B. 2023; 13:1438-1466. [CrossRef]
- Golub D, Iyengar N, Dogra S, Wong T, Bready D, Tang K, Modrek AS, Placantonakis DG. Mutant isocitrate dehydrogenase inhibitors as targeted cancer therapeutics. Front Oncol. 2019; 9:417. [CrossRef]
- Xiang ZJ, Hu T, Wang Y, Wang H, Xu L, Cui N. Neutrophil-lymphocyte ratio (NLR) was associated with prognosis and immunomodulatory in patients with pancreatic ductal adenocarcinoma (PDAC). Biosci Rep. 2020;40: BSR20201190. [CrossRef]
- Pointer DT Jr, Roife D, Powers BD, Murimwa G, Elessawy S, Thompson ZJ, Schell MJ, Hodul PJ, Pimiento JM, Fleming JB, Malafa MP. Neutrophil to lymphocyte ratio, not platelet to lymphocyte or lymphocyte to monocyte ratio, is predictive of patient survival after resection of early-stage pancreatic ductal adenocarcinoma. BMC Cancer. 2020; 20:750. [CrossRef]
- Iwai N, Okuda T, Sakagami J, Harada T, Ohara T, Taniguchi M, Sakai H, Oka K, Hara T, Tsuji T, Komaki T, Kagawa K, Yasuda H, Naito Y, Itoh Y. Neutrophil to lymphocyte ratio predicts prognosis in unresectable pancreatic cancer. Sci Rep. 2020; 10:18758. [CrossRef]
- Jia K, Chen Y, Sun Y, Hu Y, Jiao L, Ma J, Yuan J, Qi C, Li Y, Gong J, Gao J, Zhang X, Li J, Zhang C, Shen L. Multiplex immunohistochemistry defines the tumor immune microenvironment and immunotherapeutic outcome in CLDN18.2-positive gastriccancer. BMC Med. 2022; 20:223. [CrossRef]
- Camelo-Piragua S, Jansen M, Ganguly A, Kim JC, Louis DN, Nutt CL. Mutant IDH1-Specific immunohistochemistry distinguishes diffuse astrocytoma from astrocytosis. Acta Neuropathol. 2010; 119:509-511. [CrossRef]
- Delgado A, Guddati AK. Clinical endpoints in oncology - a primer. Am J Cancer Res.2021; 11:1121-1131.
- Dang L, Yen K, Attar EC. IDH mutations in cancer and progress toward development of targeted therapeutics. Ann Oncol. 2016; 27:599-608. [CrossRef]
- Zarei M, Hajihassani O, Hue JJ, Graor HJ, Rothermel LD, Winter JM. Targeting wild-type IDH1 enhances chemosensitivity in pancreatic cancer. bioRxiv [Preprint]. 2023 Mar 29:2023.03.29.534596. [CrossRef]
- Luo X, Yu B, Jiang N, Du Q, Ye X, Li H, Wang WQ, Zhai Q. Chemotherapy-induced reduction of neutrophil-to-lymphocyte ratio is associated with better survival in pancreatic adenocarcinoma: a meta-analysis. Cancer Control. 2020; 27:1073274820977135. [CrossRef]
- Vunnam N, Young MC, Liao EE, Lo CH, Huber E, Been M, Thomas DD, Sachs JN. Nimesulide, a COX-2 inhibitor, sensitizes pancreatic cancer cells to TRAIL-induced apoptosis by promoting DR5 clustering. Cancer Biol Ther. 2023; 24:2176692. [CrossRef]
- Nielsen SR, Strøbech JE, Horton ER, Jackstadt R, Laitala A, Bravo MC, Maltese G, Jensen ARD, Reuten R, Rafaeva M, Karim SA, Hwang CI, Arnes L, Tuveson DA, Sansom OJ, Morton JP, Erler JT. Suppression of tumor-associated neutrophils by lorlatinib attenuates pancreatic cancer growth and improves treatment with immune checkpoint blockade. Nat Commun. 2021; 12:3414. [CrossRef]
- Li HB, Yang ZH, Guo QQ. Immune checkpoint inhibition for pancreatic ductal adenocarcinoma: limitations and prospects: a systematic review. Cell Commun Signal. 2021; 19:117. [CrossRef]
Figure 1.
Cytoplasmic/membranous Claudin-18.2 expression in pancreatic ductal adenocarcinoma (PDAC) with increasing intensity (A: negative, B: 1+, C: 2+, D:3+). Inset (E): positive control (normal stomach).
Figure 1.
Cytoplasmic/membranous Claudin-18.2 expression in pancreatic ductal adenocarcinoma (PDAC) with increasing intensity (A: negative, B: 1+, C: 2+, D:3+). Inset (E): positive control (normal stomach).
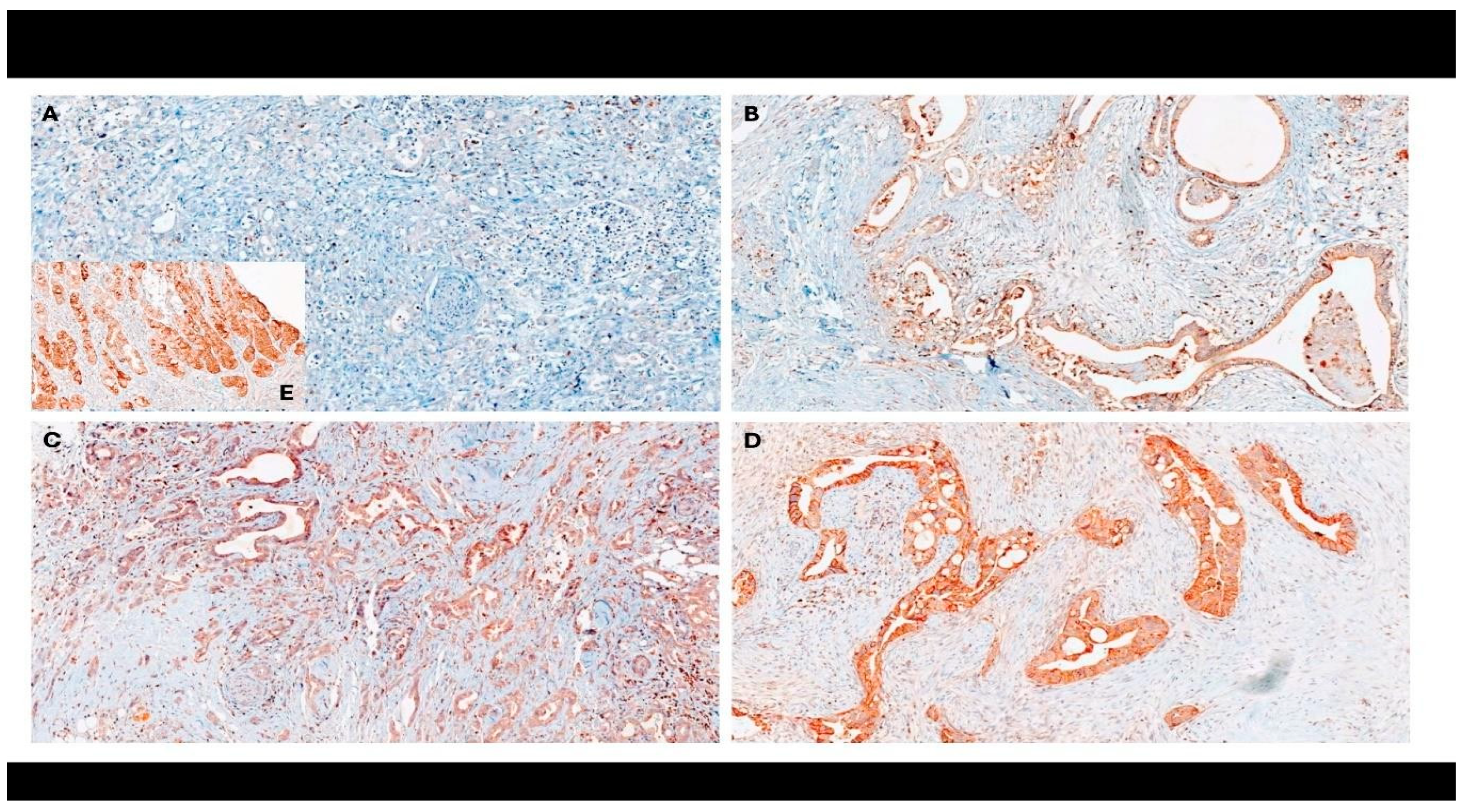
Figure 2.
IDH1 expression in pancreatic ductal adenocarcinoma. A: Positive control (oligodendroglioma), B: Negative, C-D: Patchy, granular cytoplasmic staining in tumor cells.
Figure 2.
IDH1 expression in pancreatic ductal adenocarcinoma. A: Positive control (oligodendroglioma), B: Negative, C-D: Patchy, granular cytoplasmic staining in tumor cells.
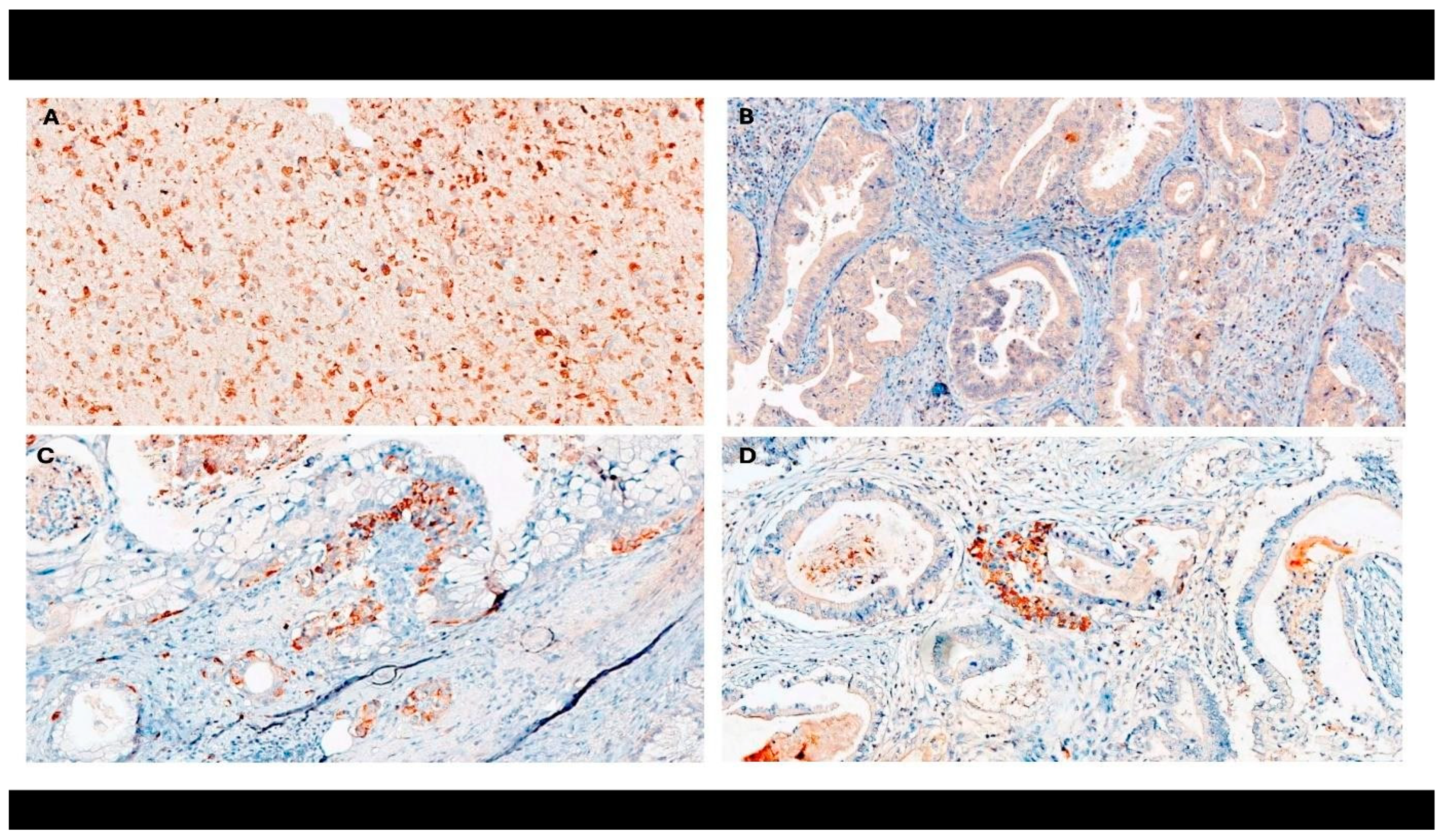
Figure 3.
Kaplan-Meier plot of progression-free survival in patients with pancreatic ductal adenocarcinoma (n = 72).
Figure 3.
Kaplan-Meier plot of progression-free survival in patients with pancreatic ductal adenocarcinoma (n = 72).
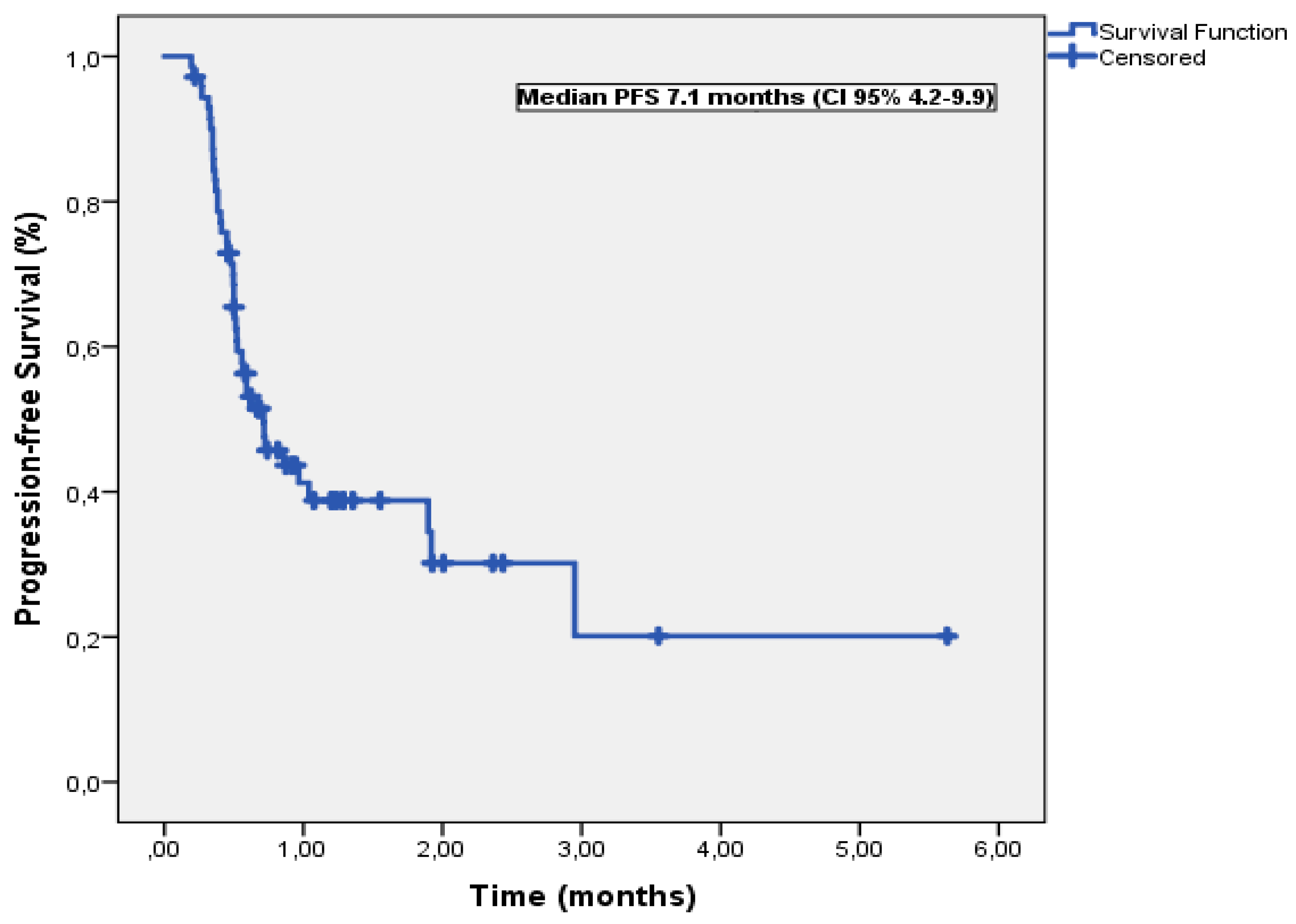
Figure 4.
Kaplan-Meier plot of overall survival in patients with pancreatic ductal adenocarcinoma (n = 72).
Figure 4.
Kaplan-Meier plot of overall survival in patients with pancreatic ductal adenocarcinoma (n = 72).
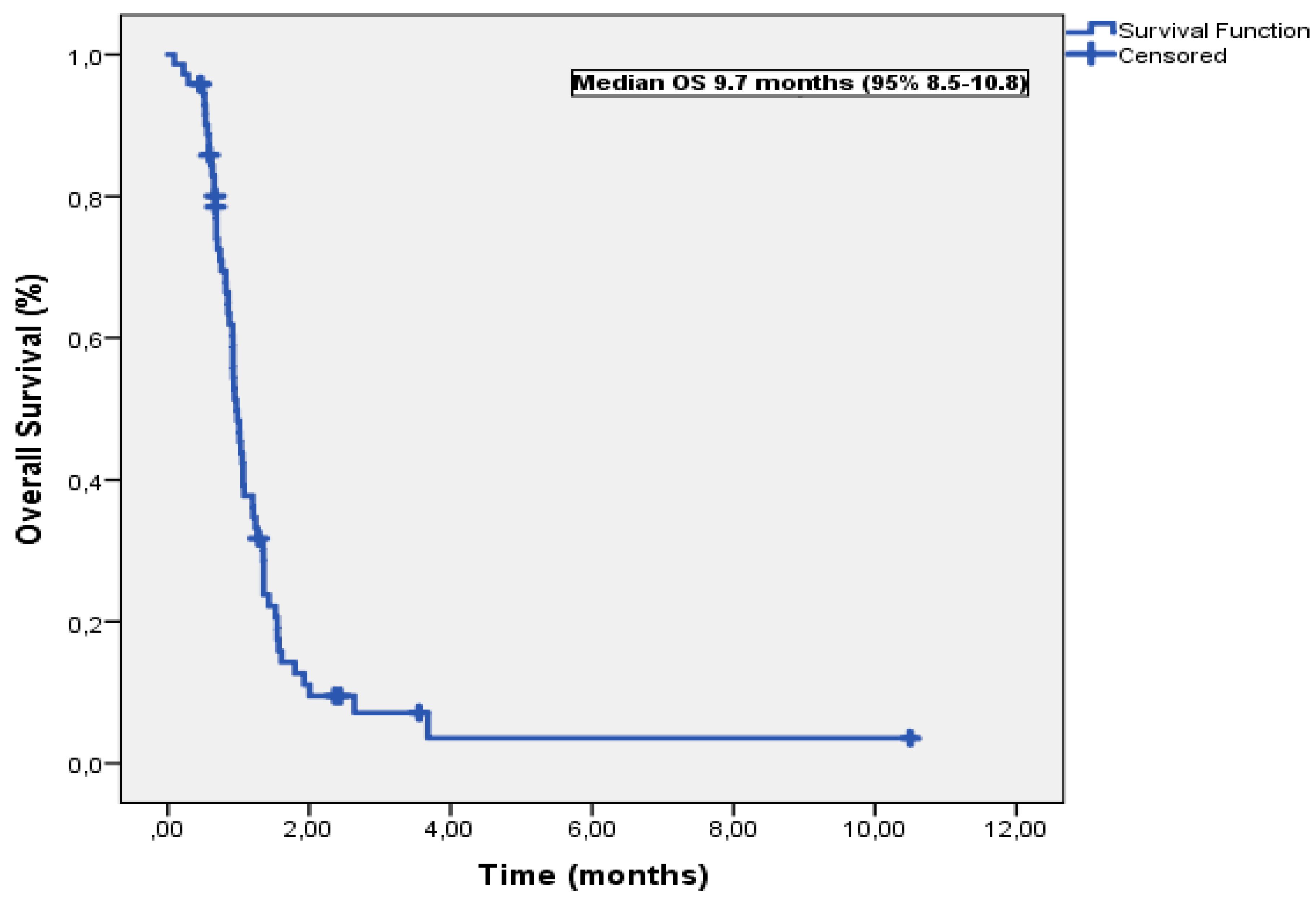

Table 1.
General characteristics of patients with pancreatic ductal adenocarcinoma (n = 72).
| Variable | n (%) |
| Age, years | |
| <60 | 23 (31.9) |
| >60 | 49 (68.1) |
| Sex | |
| Female | 33 (45.8) |
| Male | 39 (54.2) |
| Smoking history | |
| Negative | 33 (45.8) |
| Positive | 39 (54.2) |
| Alcohol consumption | |
| Absent | 39 (54.2) |
| Present | 33 (45.8) |
| Presence of weight loss | |
| No | 28 (38.9) |
| Yes | 44 (61.1) |
| Presence of jaundice at initial presentation | |
| No | 30 (41.7) |
| Yes | 42 (58.3) |
| History of diabetes | |
| Negative | 28 (38.9) |
| Positive | 44 (61.1) |
| Presence of metastasis at initial presentation | |
| No | 158 (57.7) |
| Yes | 104 (42.3) |
| Primary tumor localization | |
| Head | 33 (45.8) |
| Body | 31 (43.1) |
| Tail | 8 (11.1) |
| Presence of visceral metastasis at initial presentation | |
| No | 88 (64.7) |
| Yes | 47 (35.3) |
| First-line chemotherapy regimen | |
| FOLFIRINOX | 43 (59.7) |
| Gemcitabine plus nab-paclitaxel | 29 (40.3) |
Table 2.
Univariable and Multivariable Analyses of Risk Factors for Progression-Free Survival.
| Variable | Median PFS (months) | Univariable P | Multivariable-adjusted P | HR (95% CI) |
| Age, years | ||||
| <60 | 8.6 | 0.42 | ||
| >60 | 7.1 | |||
| Sex | ||||
| Female | 8.6 | 0.26 | ||
| Male | 5.9 | |||
| Smoking history | ||||
| Negative | 9.6 | 0.20 | ||
| Positive | NR | |||
| Alcohol consumption | ||||
| Absent | 9.1 | 0.04 | 0.47 | 2.5 (0.19−31.9) |
| Present | 5.6 | |||
| Presence of weight loss | ||||
| No | 10.4 | 0.91 | ||
| Yes | 9.6 | |||
| Presence of jaundice at initial presentation | ||||
| No | 10.4 | 0.84 | ||
| Yes | 5.9 | |||
| History of diabetes | ||||
| Negative | 10.4 | 0.74 | ||
| Positive | 12.8 | |||
| Presence of metastasis at initial presentation | ||||
| No | 19.2 | 0.36 | ||
| Yes | 8.6 | |||
| Primary tumor localization | ||||
| Head | 7.2 | 0.73 | ||
| Body | 7.1 | |||
| Tail | 7.1 | |||
| Presence of visceral metastasis at initial presentation | ||||
| No | 9.6 | 0.33 | ||
| Yes | 5.9 | |||
| First-line chemotherapy regimen | ||||
| FOLFIRINOX | 7.2 | 0.34 | ||
| Gemcitabine plus nab-paclitaxel | 7.1 | |||
| CLDN18.2 expression | ||||
| Negative | 6.2 | 0.29 | ||
| Positive | 13.9 | |||
| IDH1 expression | ||||
| Negative | 7.1 | 0.033 | 0.98 | 0.10 (0.05−2.12) |
| Positive | 3.7 | |||
| NLR | ||||
| ≤ 3.22 | 18.9 | 0.10 | 0.20 | 1.61 (0.77−3.39) |
| > 3.22 | 6.2 | |||
* PFS, progression-free survival; HR, hazard ratio; CI, confidence interval; NR, not reached; CLDN, claudin; IDH, isocitrate dehydrogenase; NLR, neutrophil-to-lymphocyte ratio.
Table 3.
Univariable and Multivariable Analyses of Risk Factors for Overall Survival.
| Variable | Median OS (months) | Univariable P | Multivariable-adjusted P | HR (95% CI) |
| Age, years | ||||
| <60 | 10.5 | 0.15 | ||
| >60 | 9.4 | |||
| Sex | ||||
| Female | 10.1 | 0.26 | ||
| Male | 9.7 | |||
| Smoking history | ||||
| Negative | 10.6 | 0.35 | ||
| Positive | 12.3 | |||
| Alcohol consumption | ||||
| Absent | 15.7 | 0.67 | ||
| Present | 10.7 | |||
| Presence of weight loss | ||||
| No | 10.4 | 0.91 | ||
| Yes | 9.6 | |||
| Presence of jaundice at initial presentation | ||||
| No | 14.2 | 0.57 | ||
| Yes | 10.3 | |||
| History of diabetes | ||||
| Negative | 14.8 | 0.28 | ||
| Positive | 13.9 | |||
| Presence of metastasis at initial presentation | ||||
| No | 20.3 | 0.40 | ||
| Yes | 9.9 | |||
| Primary tumor localization | ||||
| Head | 9.8 | 0.33 | ||
| Body | 9.4 | |||
| Tail | 13.5 | |||
| Presence of visceral metastasis at initial presentation | ||||
| No | 11.3 | 0.93 | ||
| Yes | 9.2 | |||
| First-line chemotherapy regimen | ||||
| FOLFIRINOX | 10.1 | 0.16 | ||
| Gemcitabine plus nab-paclitaxel | 9.4 | |||
| CLDN18.2 expression | ||||
| Negative | 9.2 | 0.006 | 0.013 | 0.38 (0.18−0.81) |
| Positive | 15.2 | |||
| IDH1 expression | ||||
| Negative | 9.8 | 0.011 | 0.039 | 0.68 (0.19−0.72) |
| Positive | 5.3 | |||
| NLR | ||||
| ≤ 3.22 | 12.0 | 0.016 | 0.038 | 1.92 (1.03−3.56) |
| > 3.22 | 9.4 | |||
*OS, overall survival; HR, hazard ratio; CI, confidence interval; CLDN, claudin; IDH, isocitrate dehydrogenase; NLR, neutrophil-to-lymphocyte ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



