
Submitted:
12 February 2025
Posted:
13 February 2025
You are already at the latest version
Abstract
Background: While left-bundle-branch-block-related contraction patterns as well as echocardiography derived strain are variably associated with volumetric response to cardiac resynchronization therapy (CRT), the role of CMR-derived strain parameters is unexplored. Methods: 50 patients receiving CRT implantation were retrospectively analysed, all of which had undergone CMR imaging within one year before, and echocardiography within 6 months before and 6-12 months after CRT implantation. We assessed CMR-derived morphological and functional parameters with regard to echocardiographic response, defined as reduction of left ventricular end-systolic volume ≥15%. Results: Among standard CMR parameters, indexed right ventricular volumes in end-diastole (RVEDVi) (74.5 ±19.5 vs. 94.8 ±30.2 ml/m², P=.006) and end-systole (RVESVi) (43.2 ±13.3 vs. 61.6 ±28.8 ml/m², P=.003) as well as left atrial (LA) area (24.8 ±3.5 vs. 30.4 ±9.5 cm², P=.020) differed significantly between CRT responders and non-responders. In strain analysis, CRT responders showed significantly better LA global longitudinal strain (GLS) (25.1 ±10.4 vs. 15.3 ±10.5, P=.002), LA global circumferential strain (GCS) (27.9 ±14.7 vs. 17.1 ±13.1%, P=.012), RV GLS (-25.0 ±6.5 vs. -18.9 ±7.6%, P=.004) and RV free wall strain (-31.1 ±7.9 vs. -24.9 ±9.5, P=.017). Conclusions: CMR-derived peak septal circumferential strain and RVEDVi correlated with echocardiographic volumetric response to CRT at 6-12 months.
Keywords:
cardiac resynchronization therapy
; strain
; right ventricle
; left-bundle-branch-block
1. Introduction
Cardiac resynchronization therapy (CRT) is a cornerstone in the treatment of heart failure with left bundle branch block (LBBB) and a left ventricular ejection fraction (LVEF) ≤35% [1]. However, about one third of patients do not respond favorably, defined as left ventricular end-diastolic volume (LVESV) reduction ≥15% at 6-12 months, which is a strong predictor of future adverse events [2]. It was thought that patients with the most mechanical dyssynchrony would derive the maximum benefit from CRT, but trial results were disappointing [3,4]. Over the years, various parameters have been proposed to predict CRT response, including end-systolic septal strain, systolic stretch index, right ventricular function and myocardial scarring [5], yet most studies were echocardiography-based and examined one parameter at a time in highly selected patient populations. Using the ability of cardiac magnetic resonance (CMR) based volumetry and feature tracking (FT) derived strain, we sought to examine the correlation of ventricular size and function, various strain parameters, and myocardial scarring with CRT response, defined as LVESV reduction ≥15% at 6-12 months after implant, in a heterogenous patient population.
2. Materials and Methods
2.1. Patient Population
This study retrospectively analyzed patients who underwent CMR scans from January 2012 to January 2022 at our institution within one year prior to successful CRT implantation, who also had a transthoracic echocardiogram within 6 months prior to, and 6-12 months after CRT implantation. A total of 50 patients were included for analysis. Clinical information including age, gender, body height and weight, comorbidities, pre-implant ECG, and pacing parameters 6-12 months post-implant were collected. The operation records were reviewed to confirm successful CRT implantation with the LV lead in the posterolateral or anterolateral non-apical position. All LV leads were multipolar. This study was approved by the local ethics committee. Informed consent was waived for this retrospective study.
2.2. CMR Acquisition
CMR scans were performed on 1.5T (Achieva, Philips Healthcare, Best, The Netherlands) and 3T (Ingenia, Philips Healthcare, Best, The Netherlands) scanners with multi-channel phased-array receiver coils. A standard retrospectively gated balanced steady-state free precession sequence was employed to acquire cine images at the left ventricular short axis and 2-, 3- and 4-chamber-views at a minimum of 25 phases per cardiac cycle. Patients received 0.15 mmol/kg of gadobutrol (Gadovist® 1.0 mmol/mL, Bayer, A.G.; Leverkusen, Germany) in scans performed 2012-2020, and 0.1 mmol/kg of gadobutrol in scans 2021-2022 due to institutional protocol change. Late gadolinium enhancement imaging was performed using a 3D fat-water-separated inversion-recovery sequence (mDIXON) at an inversion time selected based on a Look-Locker sequence starting 5-10 minutes post contrast injection, depending on the contrast agent dose.
2.3. CMR Analysis
Left- (LV) and right-ventricular (RV) volumetry were performed offline using commercially available post-processing software (Philips Intellispace Portal Version 12.1, Philips Medical Systems Nederland, B.V.; Best, The Netherlands). LV short-axis end-diastolic and end-systolic cine images were manually contoured to obtain LV and RV end-diastolic and end-systolic volumes, from which stroke volume and ejection fraction were calculated. LV and RV volumes were indexed to body surface area. Left atrial (LA) and right atrial (RA) area were calculated from end-systolic cine 4-chamber-views. Septal scar was defined as any LGE in the basal or mid-ventricular anteroseptal or inferoseptal segments; lateral scar was similarly defined in the basal or mid-ventricular anterolateral or inferolateral segments. Subendocardial or transmural late gadolinium enhancement (LGE) was classified as ischemic, whereas intramyocardial or epicardial LGE as non-ischemic. Strain analysis was performed on a dedicated post-processing software (QStrain RE version 4.4, Medis, Leiden, The Netherlands). For endocardial strain analysis, LV two-, three- and four-chamber long axis cine images, as well as LV basal, mid-ventricular and apical short axis cine images were contoured and checked for correct tracking to obtain LV global longitudinal strain (GLS), global circumferential strain (GCS), and segmental peak and end-systolic strain (16-segment model). Exemplary strain measurements in the 4-chamber-view are shown in Figure 1. For the, R.V.; GLS as well as the free wall LS was analyzed on four-chamber cine images. LA GLS was analyzed biplane on four- and two-chamber cine images.
2.4. Echocardiographic Analysis and Definition of CRT Response
Pre- and post-implant transthoracic echocardiograms were analyzed on commercially available software (IntelliSpace Cardiovascular 4.1, Philips Medical systems Nederland, B.V.; Best, The Netherlands) at apical two- and four-chamber views for bi-plane LV end-diastolic and end-systolic volumes and ejection fraction. CRT responders were defined as ≥15% reduction in LV end-systolic volume post CRT implant [2].
2.5. Statistical Analysis
Continuous variables are expressed as mean ± standard deviation (SD), categorical variables as numbers and percentages. Continuous variables were compared by an independent samples Student’s t-test or non-parametric tests in case of non-normal distribution. Equality of variances was assessed using Levene’s test. Categorical variables were compared between CRT responders and non-responders using a χ² test, or Fisher’s exact test when any cell had an expected count of less than 5. Data was analyzed with SPSS (version 26, Statistical Package for the Social Sciences, International Business Machines, Inc, Armonk, NY) and R (version 4.4.1, R Foundation for Statistical Computing, Vienna, Austria). Two-sided P-values <.05 were considered statistically significant.
3. Results
Fifty subjects with a mix of ischemic and non-ischemic cardiomyopathy were included. The average age was 68.1±10.5 years and 66% were male; 52% had a history of atrial fibrillation and 22% had valve surgery. The full baseline characteristics, divided into CRT-responders and non-responders, are shown in Table 1. The overall response rate was 64%. No correlation was seen with comorbidities including hypertension, diabetes, chronic kidney disease, atrial fibrillation or history of valve surgery.
3.1. Basic CMR Parameters and CRT Response
Basic anatomical and functional CMR parameters are shown in Table 2 and late gadolinium enhancement (LGE) findings in Table 3. One person did not receive contrast agent and was excluded from LGE analysis. Patients with CRT response showed significantly lower right ventricular end-diastolic volume index (RVEDVi, 74.5 ±19.5 vs. 94.8 ±30.2 ml/m², P=.006), right ventricular end-systolic volume index (RVESVi, 43.2 ±13.3 vs. 61.6 ±28.8 ml/m², P=.003), and LA area (24.8 ±3.5 vs. 30.4 ±9.5 cm²). In contrast, left ventricular end-diastolic volume index (LVEDVi), LV GLS, LV GCS and parameters associated with mechanical dyssynchrony in LBBB as apical rocking and septal flash did not correlate with CRT response, nor did the presence, etiology and location of scar.
3.2. Strain Measurements and CRT Response
Short and long axis strain measurements of responders and non-responders are shown in Table 4 and Table 5. CRT responders showed significantly better LA global longitudinal strain (GLS) (25.1 ±10.4 vs. 15.3 ±10.5, P=.002), LA global circumferential strain (GCS) (27.9 ±14.7 vs. 17.1 ±13.1%, P=.012), RV GLS (-25.0 ±6.5 vs. -18.9 ±7.6%, P=.004) and RV free wall strain (-31.1 ±7.9 vs. -24.9 ±9.5). Other strain parameters were not associated with CRT response. Importantly, peak and end-systolic septal and lateral LS and CS did not correlate with CRT response. Scatter plots of RVEDVi and peak septal circumferential strain versus LVESV change at 6-12 months are shown in Figure 2. A receiver-operator-characteristic (ROC) for RV GLS, RVESVi and LA GLS is depicted in Figure 3.
4. Discussion
This study examined the correlation of a comprehensive panel of CMR parameters to CRT response in a patient population that reflects the real-world clinical complexity. For example, 52% had atrial fibrillation and 22% had a history of valve surgery. The overall response rate of 64% in this study is on par with that reported elsewhere [3]. To our knowledge, this is the first study to show the discriminatory value of right ventricular and left atrial strain on CRT response against parameters including scar etiology and location, volumetry and a comprehensive list of LV strain parameters. The main findings are:
- (1)
- RV volumes and strain measurements correlated with CRT response
- (2)
- LA area and strain measurements correlated with CRT response
- (3)
- Left ventricular strain parameters and the presence and location of scar did not correlate with CRT response.
4.1. LV Strain and CRT Response
In contrast to previous reports, none of the left ventricular strain parameters examined correlated with CRT response. [6,7]. Differences in study population, study methodology and post processing software could be accountable and further research is necessary to further assess the potential discriminatory value of left ventricular strain measurements.
4.2. The RV and CRT Response
Previous reports on the RV and CRT response are mixed. A metanalysis of 17 studies with echocardiography-derived RV functional parameters found no correlation with CRT response [8] for any of the examined parameters. Studies using CMR, which is considered the gold standard for right ventricular measurements, found mixed results. In two studies, RVEF and tricuspid annular plane systolic excursion (TAPSE) in CMR were reported to correlate with CRT response [9,10]. Another study found no correlation between RV function in CMR and mortality after CRT but did not report CRT response and had a highly selected patient population with a mean RVEDVi of only 64 ml/m², which is much lower than that in our cohort [11]. Additionally, none of the aforementioned CMR-studies examined RV strain, less than 20% of subjects had atrial fibrillation and only 1% of subjects had undergone valvular surgery.
4.3. The LA and CRT Response
Consistent with previous reports [12,13,14], we showed that larger LA size and impaired LA GLS and GCS were associated with CRT non-response. Presence of atrial fibrillation could not be accountable, since its incidence as well as biventricular pacing percentage was similar in responders and non-responders (Table 5). Although LA dysfunction may signify more advanced LV disease, there was no significant difference in LVEDVi, LV GLS and LV GCS. The mechanism linking LA function and CRT response remains unclear and should be the focus of further studies.
4.4. Scar and CRT Response
Previous studies reported lower rates of CRT response in the presence of septal scar [15,16]. This finding could not be replicated in our study, which may be due to the small sample size. Similarly, we could not reproduce the adverse effect of ischemic cardiomyopathy on post-CRT reverse remodeling.
Lateral scar on CMR has been associated with worse lateral circumferential strain and CRT non-response for concordantly placed LV leads [17], which again could not be reproduced in our study. Among our subjects with lateral scar, all but one had LGE ≤50% wall thickness. It is plausible that more extensive (>50% wall thickness) lateral scar would negatively impact CRT response.
4.5. Limitations
A limitation of this study is the small sample size, prohibiting meaningful subgroup analyses. As no Bonferroni correction was performed for the large number of variables tested, all results should be considered hypothesis-generating. Not all patient characteristics were profiled, including their list of medications, blood pressure, smoking status and history of chemotherapy. Our study is based on strain analysis by one of several commercially available postprocessing software (QStrain RE version 4.4, Medis, Leiden, The Netherlands). Whether the results are reproducible on other platforms is unclear, as strain measurements have been shown to vary depending on the postprocessing software used [18].
5. Conclusions
In our hypothesis-generating retrospective analysis, CMR-derived strain measurements of the LA and, R.V.; but not the, L.V.; correlated with CRT response, defined as LVESV reduction ≥15% at 6-12 months.
This article is a revised and expanded version of a paper entitled ‘Right ventricular and left atrial strain predict Volumetric response to cardiac resynchronization therapy’, which was presented at the CMR 2025 congress in Washington on January 31th, 2025 [19].
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. The R-scripts used for the statistical analysis.
Author Contributions
Conceptualization, S.C., S.K. and P.D..; methodology, S.C. and P.D.; software, S.K..; validation, P.D. and J.L.; formal analysis, S.C. and P.D..; investigation, S.C. and P.D.; resources, S.K. and H.D..; data curation, P.D., S.M.W. and J.L..; writing—original draft preparation, S.C. and P.D..; writing—review and editing, W.M.W., R.E.B., M.E., C.S., D.H., N.S., C.K., H.D., S.K. and P.D..; visualization, P.D..; supervision, P.D. and S.K..; project administration, S.K. and H.D..; funding acquisition, S.K.. All authors have read and agreed to the published version of the manuscript.”
Funding
SK and PD were supported by a grant from Philips Healthcare. SK and RB were funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation)—SFB-1470—B06. DH was funded by the Berlin University Alliance (OX|BER Research Partnership/Flexible Funds). JL was funded by the Kaltenbach doctorate fund of the Deutsche Herzstiftung. The APC was funded by the publication fund of the Charité Universitätsmedizin Berlin.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the Charité Universitätsmedizin Berlin (EA1/143/23, date of approval: June 21, 2023).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
Data is available from the corresponding author upon reasonable request.
Conflicts of Interest
SK received funding from the DZHK (German Centre for Cardiovascular Research) and by the BMBF (German Ministry of Education and Research), a research grant from Philips Healthcare and lecture honoraria from Medis, NL. PD received travel subsidies from Philips Healthcare. CS is an employee of Philips Healthcare.
Abbreviations
The following abbreviations are used in this manuscript:
| CMR | Cardiac magnetic resonance |
| CRT | Cardiac resynchronization therapy |
| CS | Circumferential strain |
| ECV | Extracellular volume |
| FT | Feature tracking |
| GCS | Global circumferential strain |
| GLS | Global longitudinal strain |
| LA | Left atrium |
| LBBB | Left bundle branch block |
| LGE | Late gadolinium enhancement |
| LS | Longitudinal strain |
| LV | Left ventricule |
| LVEDd | Left ventricular end-diastolic diameter |
| LVEDV | Left ventricular end-diastolic volume |
| LVEDVi | Left ventricular end-diastolic volume index |
| LVEF | Left ventricular ejection fraction |
| LVESV | Left ventricular end-systolic volume |
| NYHA | New York Heart Association |
| RA | Right atrium |
| ROC | Receinver operator characteristic |
| RV | Right ventricle |
| RVEDVi | Right ventricular end-diastolic volume index |
| RVEF | Right ventricular ejection fraction |
| RVESVi | Right ventricular end-systolic volume index |
| SD | Standard deviation |
| T | Tesla |
| TAPSE | Tricuspid annular plane systolic excursion |
References
- Chung, M.K.; Patton, K.K.; Lau, C.P.; Dal Forno ARJ, Al-Khatib, S. M.; Arora, V.; et al. 2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing for the avoidance and mitigation of heart failure. Heart Rhythm. 2023, 20, e17–e91. [Google Scholar] [CrossRef] [PubMed]
- Ypenburg, C.; van Bommel, R.J.; Borleffs, C.J.; Bleeker, G.B.; Boersma, E.; Schalij, M.J.; Bax, JJ. Long-term prognosis after cardiac resynchronization therapy is related to the extent of left ventricular reverse remodeling at midterm follow-up. J Am Coll Cardiol. 2009, 53, 483–90. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.S.; Leon, A.R.; Tavazzi, L.; Sun, J.P.; Nihoyannopoulos, P.; Merlino, J.; et al. Results of the Predictors of Response to CRT (PROSPECT) trial. Circulation. 2008, 117, 2608–16. [Google Scholar] [CrossRef] [PubMed]
- Bordachar, P.; Lafitte, S.; Réant, P.; Reuter, S.; Clementy, J.; Mletzko, R.U.; et al. Low value of simple echocardiographic indices of ventricular dyssynchrony in predicting the response to cardiac resynchronization therapy. Eur J Heart Fail. 2010, 12, 588–92. [Google Scholar] [CrossRef] [PubMed]
- Gorcsan, J.; Anderson, C.P.; Tayal, B.; Sugahara, M.; Walmsley, J.; Starling, R.C.; Lumens, J. Systolic Stretch Characterizes the Electromechanical Substrate Responsive to Cardiac Resynchronization Therapy. JACC: Cardiovascular Imaging. 2019, 12, 1741–52. [Google Scholar] [CrossRef] [PubMed]
- Zweerink, A.; Nijveldt, R.; Braams, N.J.; Maass, A.H.; Vernooy, K.; de Lange, F.J.; et al. Segment length in cine (SLICE) strain analysis: a practical approach to estimate potential benefit from cardiac resynchronization therapy. J Cardiovasc Magn Reson. 2021, 23, 4. [Google Scholar] [CrossRef] [PubMed]
- Zweerink, A.; van Everdingen, W.M.; Nijveldt, R.; Salden OAE, Meine, M. ; Maass, A.H.; et al. Strain imaging to predict response to cardiac resynchronization therapy: a systematic comparison of strain parameters using multiple imaging techniques. ESC Heart Fail. 2018, 5, 1130–40. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Bax, J.J.; Vallakati, A.; Goel, S.; Lavie, C.J.; Kassotis, J.; et al. Meta-Analysis of the Relation of Baseline Right Ventricular Function to Response to Cardiac Resynchronization Therapy. Am J Cardiol. 2016, 117, 1315–21. [Google Scholar] [CrossRef] [PubMed]
- Manca, P.; Cossa, S.; Matta, G.; Scalone, A.; Tola, G.; Schintu, B.; et al. Right ventricular function assessed by cardiac magnetic resonance predicts the response to resynchronization therapy. J Cardiovasc Med (Hagerstown). 2020, 21, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Alpendurada, F.; Guha, K.; Sharma, R.; Ismail, T.F.; Clifford, A.; Banya, W.; et al. Right ventricular dysfunction is a predictor of non-response and clinical outcome following cardiac resynchronization therapy. J Cardiovasc Magn Reson. 2011, 13, 68. [Google Scholar] [CrossRef] [PubMed]
- Zegard, A.; Okafor, O.; Moody, W.; Marshall, H.; Qiu, T.; Stegemann, B.; et al. Right ventricular function and long-term clinical outcomes after cardiac resynchronization therapy: A cardiovascular magnetic resonance study. Pacing Clin Electrophysiol. 2022, 45, 1075–84. [Google Scholar] [CrossRef] [PubMed]
- Feneon, D.; Behaghel, A.; Bernard, A.; Fournet, M.; Mabo, P.; Daubert, J.C.; et al. Left atrial function, a new predictor of response to cardiac resynchronization therapy? Heart Rhythm. 2015, 12, 1800–6. [Google Scholar] [CrossRef] [PubMed]
- Galli, E.; Oger, E.; Aalen, J.M.; Duchenne, J.; Larsen, C.K.; Sade, E.; et al. Left atrial strain is a predictor of left ventricular systolic and diastolic reverse remodelling in CRT candidates. Eur Heart J Cardiovasc Imaging. 2022, 23, 1373–82. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Chen, Z.; Song, Y.; Wang, J.; Yang, S.; Yu, S.; et al. CMR feature tracking-based left atrial mechanics predicts response to cardiac resynchronization therapy and adverse outcomes. Heart Rhythm. 2024, 21, 1354–62. [Google Scholar] [CrossRef] [PubMed]
- Aalen, J.M.; Donal, E.; Larsen, C.K.; Duchenne, J.; Lederlin, M.; Cvijic, M.; et al. Imaging predictors of response to cardiac resynchronization therapy: left ventricular work asymmetry by echocardiography and septal viability by cardiac magnetic resonance. Eur Heart J. 2020, 41, 3813–23. [Google Scholar] [CrossRef] [PubMed]
- Larsen, C.K.; Smiseth, O.A.; Duchenne, J.; Galli, E.; Aalen, J.M.; Lederlin, M.; et al. Cardiac Magnetic Resonance Identifies Responders to Cardiac Resynchronization Therapy with an Assessment of Septal Scar and Left Ventricular Dyssynchrony. J Clin Med. 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.J.; Umar, F.; Panting, J.R.; Stegemann, B.; Leyva, F. Left ventricular lead position, mechanical activation, and myocardial scar in relation to left ventricular reverse remodeling and clinical outcomes after cardiac resynchronization therapy: A feature-tracking and contrast-enhanced cardiovascular magnetic resonance study. Heart Rhythm. 2016, 13, 481–9. [Google Scholar] [PubMed]
- Militaru, S.; Panovsky, R.; Hanet, V.; Amzulescu, M.S.; Langet, H.; Pisciotti, M.M.; et al. Multivendor comparison of global and regional 2D cardiovascular magnetic resonance feature tracking strains vs tissue tagging at 3T. Journal of Cardiovascular Magnetic Resonance 2021, 23, 54. [Google Scholar] [CrossRef] [PubMed]
- Doeblin, P.; Shing, C.; Li, J.; Werhahn, S.; Beyer, R.; Estepa, M.; et al. Right ventricular and left atrial strain predict Volumetric response to cardiac resynchronization therapy. Journal of Cardiovascular Magnetic Resonance 2025, 27, 101241. [Google Scholar] [CrossRef]
Figure 1.
Exemplary measurement of peak and end-systolic regional left-ventricular endocardial longitudinal strain in the 4-chamber-view (QStrain RE version 4.4, Medis, Leiden, The Netherlands).
Figure 1.
Exemplary measurement of peak and end-systolic regional left-ventricular endocardial longitudinal strain in the 4-chamber-view (QStrain RE version 4.4, Medis, Leiden, The Netherlands).
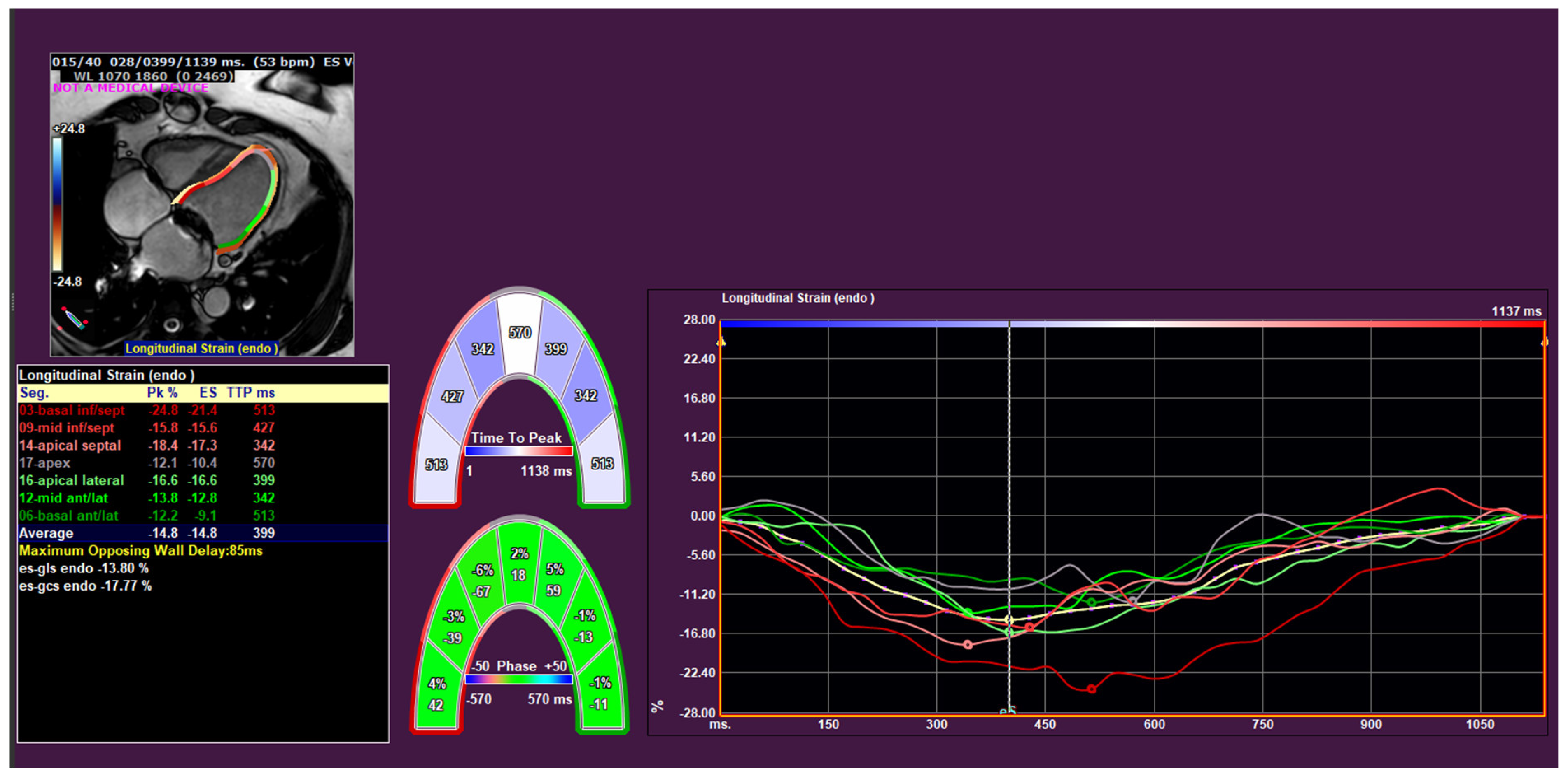
Figure 2.
Boxplots of A) right ventricular end-systolic volume index (RVESVi), B) right ventricular global longitudinal strain (RV GLS), C) RV free wall strain and D) left atrial global longitudinal strain (LA GLS) for cardiac resynchronisation therapy responders and non-responders. Created using R version 4.4.1. Code available in the Supplementary Materials.
Figure 2.
Boxplots of A) right ventricular end-systolic volume index (RVESVi), B) right ventricular global longitudinal strain (RV GLS), C) RV free wall strain and D) left atrial global longitudinal strain (LA GLS) for cardiac resynchronisation therapy responders and non-responders. Created using R version 4.4.1. Code available in the Supplementary Materials.
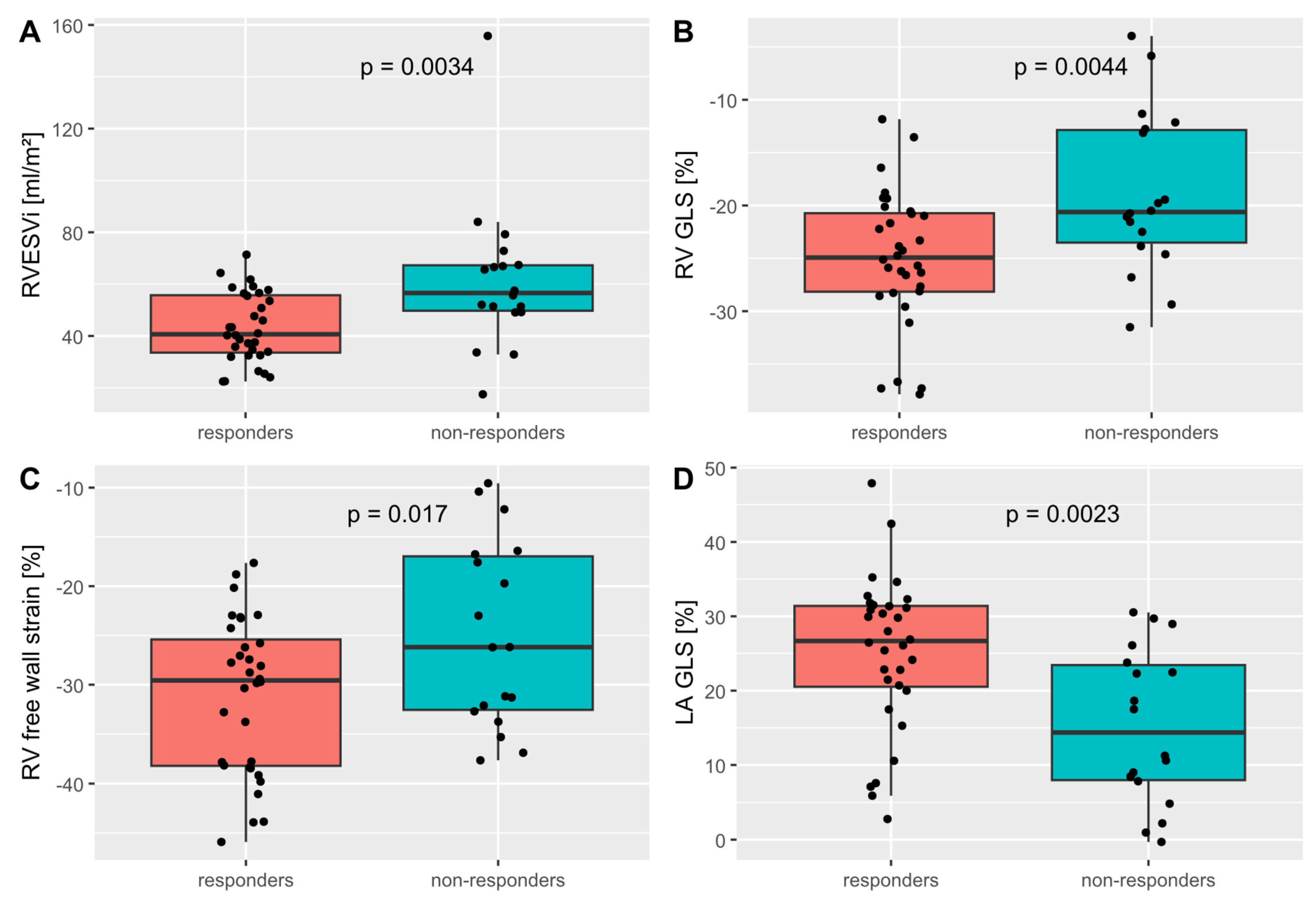
Figure 3.
Receiver-operator-characteristic (ROC) for response to cardiac resynchronisation therapy (CRT), defined as ≥15% reduction in left-ventricular end-systolic volume post CRT implant, for the predictor variables right ventricular global longitudinal strain (RV GLS), right ventricular end-systolic volume index (RVESVi) and left atrial global longitudinal strain (LA GLS).
Figure 3.
Receiver-operator-characteristic (ROC) for response to cardiac resynchronisation therapy (CRT), defined as ≥15% reduction in left-ventricular end-systolic volume post CRT implant, for the predictor variables right ventricular global longitudinal strain (RV GLS), right ventricular end-systolic volume index (RVESVi) and left atrial global longitudinal strain (LA GLS).
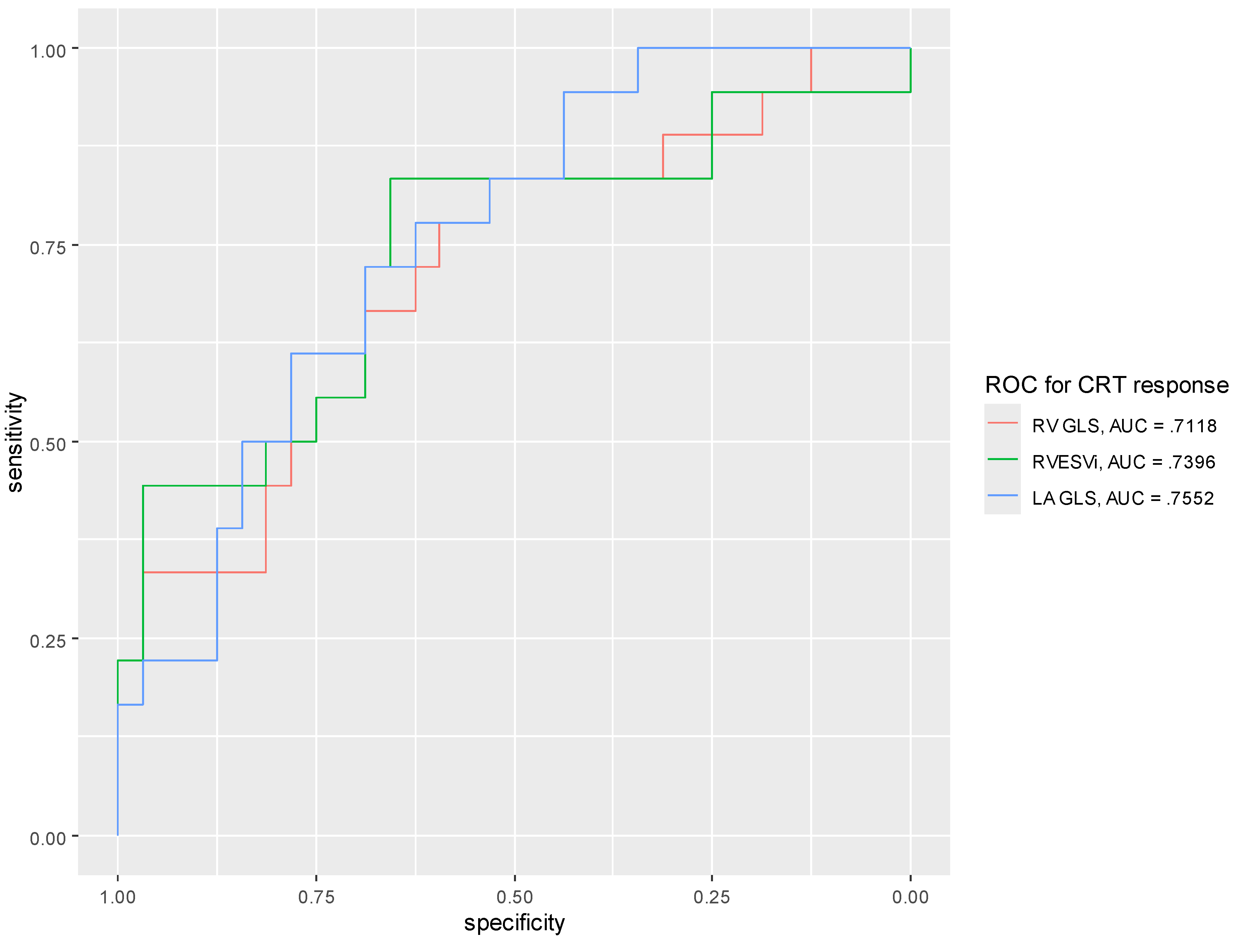

Table 1.
Baseline parameters of CRT responders and non-responders.
| Parameter | Sample size (n) | All subjects | Responders (n=32) | Non-responders (n=18) | P-value |
| Age (years) | 50 | 68.1 ±10.5 | 67.7 ±11.4 | 68.9 ±9.0 | .71 |
| Male gender (n) | 50 | 33 (66%) | 19/32 (59%) | 14/18 (78%) | .23 |
| BMI (kg/m2) | 50 | 27.0 ±4.3 | 26.4 ±3.9 | 28.0 ±4.9 | .19 |
| Hypertension (n) | 50 | 29 (58%) | 19/32 (59%) | 10/18 (56%) | >.99 |
| Diabetes mellitus (n) | 50 | 14 (28%) | 8/32 (25%) | 6/18 (33%) | .53 |
| Chronic kidney disease (n) | 50 | 23 (46%) | 12/32 (38%) | 11/18 (61%) | .14 |
| Atrial fibrillation (n) | 50 | 26 (52%) | 15/32 (47%) | 11/18 (61%) | .39 |
| Valve surgery (n) | 50 | 11 (22%) | 5/32 (16%) | 6/18 (33%) | .17 |
| NYHA II (n) | 48 | 30 (62.5%) | 22/31 (71%) | 8/17 (47%) | .13 |
| NYHA III (n) | 48 | 18 (36%) | 9/31 (29%) | 9/17 (53%) | |
| LBBB (n) | 50 | 41 (82%) | 26/32 (81%) | 15/18 (83%) | >.99 |
| QRS duration (ms) | 50 | 150.3 ±27.6 | 150.3 ±27.5 | 150.3 ±28.6 | >.99 |
| Biventricular pacing (%) | 44 | 97.1 ±3.8 | 97.5 ±3.4 | 96.5 ±4.6 | .72† |
| Baseline echo LVEDV (ml) | 50 | 202.6 ±66.9 | 200 ±65.9 | 207.3 ±70.3 | .71 |
| Baseline echo LVESV (ml) | 50 | 142.4 ±59.0 | 140.7 ±57.9 | 145.4 ±62.5 | .79 |
| Baseline echo LVEF (%) | 50 | 31.0 ±11.4 | 30.5 ±12.2 | 31.9 ±10.1 | .69 |
| LVEDV change (%) | 50 | -16.9 ±26.1 | -31.6 ±17.8 | 9.3 ±15.5 | <.001 |
| LVESV change (%) | 50 | -19.1 ±35.8 | -40.5 ±17.5 | 19.0 ±27.1 | <.001 |
Data as mean ±SD or n (%). BMI body mass index, LBBB left bundle branch block, LV left ventricular, LVEDV LV end-diastolic volume, LVEF LV ejection fraction, LVESV LV end-systolic volume, NYHA New York Heart Association. †non-parametric test due to non-normal distribution (per Kolmogorov-Smirnov test).
Table 2.
Standard CMR parameters of CRT responders and non-responders.
| Parameter | Sample size (n) | All subjects | Responders (n=32) | Non-responders (n=18) | P-value |
| LVEDd (mm) | 50 | 64.3 ±8.7 | 63.1 ±9 | 66.4 ±7.8 | .18 |
| Septal thickness (mm) | 50 | 12.3 ±3.1 | 12.7 ±2.9 | 11.6 ±3.3 | .11 |
| Posterior thickness (mm) | 50 | 7.7 ±1.6 | 7.8 ±1.5 | 7.6 ±1.7 | .19 |
| LVEDVi (ml/m2) | 50 | 122.5 ±37.7 | 115.7 ±37.1 | 134.7 ±36.5 | .06 |
| LVEF (%) | 50 | 32.9 ±9.6 | 33.6 ±9.5 | 31.7 ±9.9 | .69 |
| RVEDVi (ml/m2) | 50 | 81.8 ±25.6 | 74.5 ±19.5 | 94.8 ±30.2 | .006 |
| RVESVi (ml/m2) | 50 | 49.8 ±21.9 | 43.2 ±13.3 | 61.6 ±28.8 | .003 |
| RVEF (%) | 50 | 40.0 ±11.8 | 41.8 ±11.1 | 36.9 ±12.5 | .17 |
| LA area (cm²) | 50 | 26.8 ±8.3 | 24.8 ±6.8 | 30.4 ±9.5 | .020 |
| RA area (cm²) | 50 | 23.9 ±8.0 | 22.5 ±5.9 | 26.4 ±10.6 | .10 |
| Septal flash (n) | 49 | 35 (71.4%) | 23/31 (74%) | 12/18 (67%) | .74 |
| Apical rocking (n) | 49 | 31 (63.3%) | 18/31 (58%) | 13/18 (72%) | .37 |
Data as mean ±SD or n (%). ECV extracellular volume, LA left atrium, LV left ventricular, LVEDd LV end-diastolic diameter, LVEDVi LV end-diastolic volume index, RA right atrium, RV right ventricular, RVEDVi RV end-diastolic volume index, RVEF RV ejection fraction, RVESVi RV end-systolic volume index.
Table 3.
Scarring on late gadolinium enhancement imaging in CRT responders and non-responders.
| Parameter | All subjects (n=49) | Responders (n=32) | Non-responders (n=17) | P-value |
|---|---|---|---|---|
| Any scar (n) | 27 (55%) | 17 (53%) | 10 (59%) | .77 |
| Ischemic scar (n) | 15 (31%) | 8 (25%) | 7 (41%) | .33 |
| Septal scar (n) | 13 (27%) | 9 (28%) | 4 (24%) | >.99 |
| Lateral scar (n) | 10 (20%) | 5 (16%) | 5 (29%) | .29 |
Table 4.
CMR short axis strain measurements of CRT responders and non-responders.
| Parameter | All subjects (n=50) | Responders (n=32) | Non-responders (n=18) | P-value |
|---|---|---|---|---|
| LV GCS (%) | -14.5 ±6.6 | -14.9 ±6.0 | -13.8 ±6.0 | .56 |
| Peak septal CS (%) | -14.9 ±8.9 | -16.0 ±8.8 | -12.9 ±9.0 | .23 |
| Peak lateral CS (%) | -22.3 ±10.5 | -23.9 ±11.5 | -19.5 ±7.9 | .16 |
| End-systolic septal CS (%) | -10.3 ±10.2 | -11.3 ±9.6 | -8.5 ±11.3 | .37 |
| End-systolic lateral CS (%) | -19.3 ±10.1 | -20.0 ±11.3 | -17.9 ±7.5 | .48 |
Data as mean ±SD or n (%). CS circumferential strain, GCS global circumferential strain, LA left atrium, LV left ventricular, RV right ventricular. One subject was excluded from strain analysis due to insufficient image quality.
Table 5.
CMR long axis strain measurements of CRT responders and non-responders.
| Parameter | All subjects (n=50) | Responders (n=32) | Non-responders (n=18) | P-value |
|---|---|---|---|---|
| LV GLS (%) | -10.4 ±3.9 | -11.1 ±3.8 | -9.2 ±4.0 | .10 |
| Peak septal LS (%) | -10.7 ±5.1 | -10.9 ±4.6 | -10.3 ±6.2 | .67 |
| Peak lateral LS (%) | -24.8 ±9.4 | -26.1 ±10.1 | -22.4 ±7.5 | .18 |
| End-systolic septal LS (%) | -6.2 ±7.7 | -6.4 ±7.8 | -5.9 ±7.7 | 82 |
| End-systolic lateral LS (%) | -21.2 ±11.4 | -22.2 ±13.2 | -19.3 ±7.0 | .38 |
| RV GLS (%) | -22.8 ±7.4 | -25.0 ±6.5 | -18.9 ±7.6 | .004 |
| RV free wall GLS (%) | -28.9 ±8.9 | -31.1 ±7.9 | -24.9 ±9.5 | .017 |
| LA GLS (%) | 21.6 ±11.3 | 25.1 ±10.4 | 15.6 ±10.4 | .002 |
| LA GCS (%) | 24.0 ±15.0 | 27.9 ±14.7 | 17.1 ±13.1 | .012 |
Data as mean ±SD or n (%). GLS global longitudinal strain, LA left atrium, LS longitudinal strain, LV left ventricular, RV right ventricular. One subject was excluded from strain analysis due to insufficient image quality. One subject was excluded from longitudinal strain analysis due to incorrect triggering in the long axis images.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



