Submitted:
11 February 2025
Posted:
12 February 2025
You are already at the latest version
Abstract
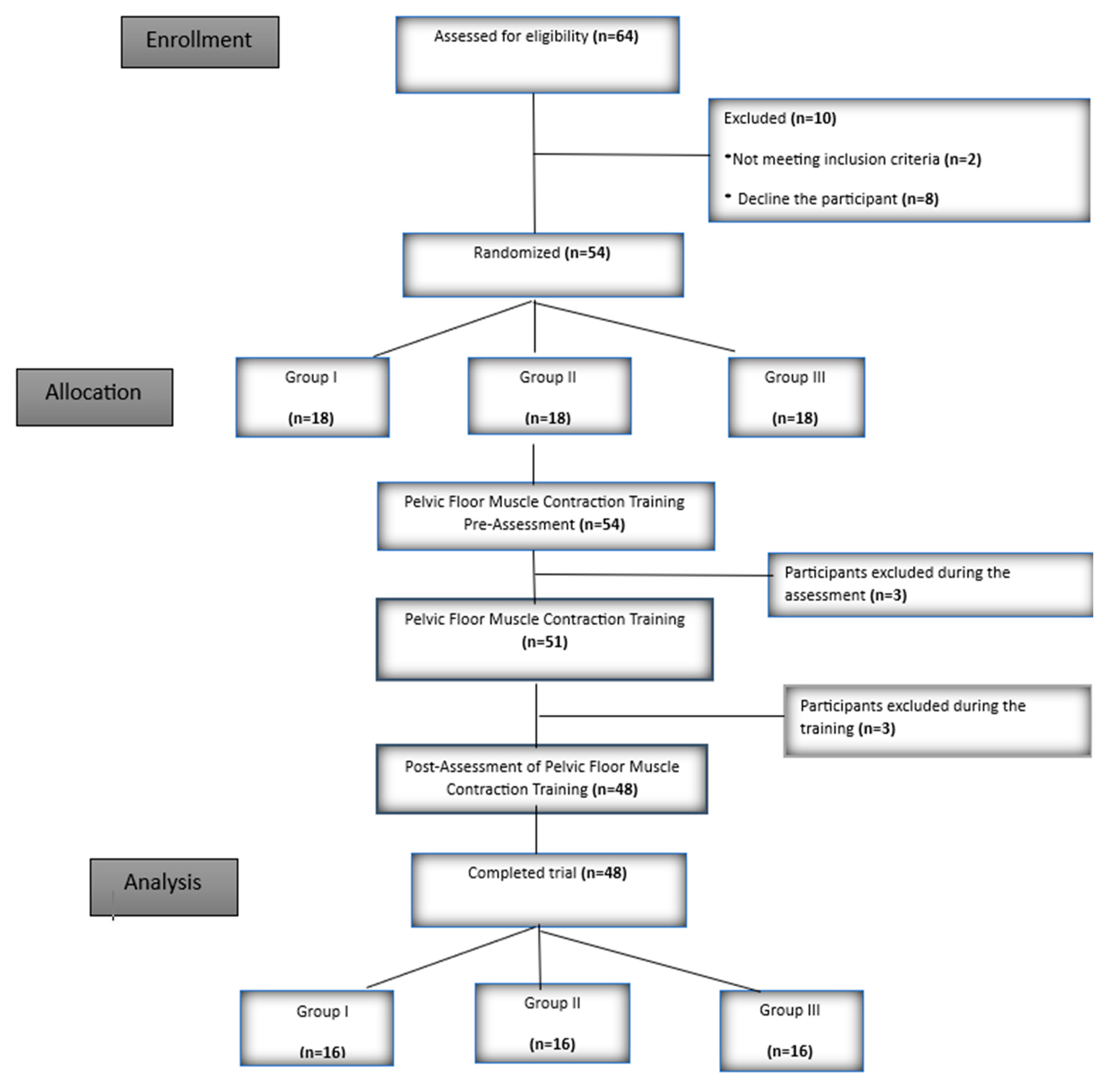
Background/Objectives: The aim of this study was to compare the effects of pelvic floor muscle contraction training (PFMCT) using verbal education, digital vaginal palpation (DVP), or perineometer on the common errors made during pelvic floor muscle contraction (PFMC) in women. Methods: A total of 48 women participated, and they were randomly assigned to three groups (Group I: PFMCT with verbal education, n=16; Group II: PFMCT with DVP, n=16; and Group III: PFMCT with perineometer, n=16). Participants who had not previously received PFMCT were evaluated for pelvic floor muscle strength using the Modified Oxford Scale (MOS) and pelvic floor muscle activation was assessed with electromyographic biofeedback (EMG-BF). Possible errors during pelvic floor muscle contraction (gluteal, adductor and/or abdominal muscle contractions, stop breathing ( breath holding), enhanced inhaling, and straining) were evaluated through inspection, palpation, or EMG-BF. After pre-training evaluations, all participants received training on pelvic floor. After this general training, each group received PFMCT using the specific training method for their group. After the training, the same evaluations were repeated. The sessions were conducted one-on-one and lasted for an average of one hour. Results: After the training, MOS values increased in Group II and Group III, while EMG-BF values only increased in Group II (p<0.05). The amount of incorrect movements during PFMC decreased after the training in all three groups (p<0.05). The abdominal muscle contraction value monitored by EMG-BF only decreased in Group II (p<0.05). Conclusion: Our study demonstrated that the PFMCT applied using the DVP method was more effective in creating more accurate and stronger muscle contractions and reducing common errors when compared to pre- and post-training values. Significant differences were observed between the groups in terms of performance improvements, with Group II showing the most notable progress. These results support the potential for DVP to yield better outcomes when used in PFMT.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Randomization
2.3. Assessments
2.3.1. Assessment of Pelvic Floor Muscle Strength with DVP Before PFMCT
2.3.2. Assessment of Pelvic Floor EMG Muscle Activation Before PFMCT
2.3.3. Assessment of Errors During PFMCT and Before PFMCT
2.4. Training
2.5. Post-PFMCT Assessments
2.6. Sample Size Estimation
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Pelvic Floor Muscle Strength and Activation Values
3.3. The Amount of Errors and Abdominal Muscle Activation Values
3.4. Between-group Comparison of Errors

| Group I | Group II | Group III | Between-group (p) | ||
| Addcont Pre-T | Yes | 10 (%62,5) | 10 (%62,5) | 7 (%43,8) | 0,467 (χ²=1,524) |
| No | 6 (%37,5) | 6 (%37,5) | 9 (%56,3) | ||
| Addcont Post-T | Yes | 1 (%6,3) | 2 (%12,5) | 3 (%18,8) | 0,552 (χ²=1,189) |
| No | 15 (%93,8) | 14 (%87,5) | 13 (%81,3) | ||
| Glcont Pre-T | Yes | 11 (%68,8) | 9 (%56,3) | 11 (%68,8) | 0,695 (χ²=0,729) |
| No | 5 (%31,3) | 7 (%43,8) | 5 (%31,3) | ||
| Glcont Post-T | Yes | 2 (%12,5) | 3 (%18,8) | 3 (%18,8) | 0,855 (χ²=0,312) |
| No | 14 (%87,5) | 13 (%81,3) | 13 (%81,3) | ||
| SB Pre-T | Yes | 4 (%25) | 4 (%25) | 5 (%31,3) | 0,901 (χ²=0,208) |
| No | 12 (%75) | 12 (%75) | 11 (%68,8) | ||
| SB Post-T | Yes | 0 (%0) | 2 (%12,5) | 2 (%12,5) | 0,181 (χ²=3,423) |
| No | 16 (%100) | 14 (%87,5) | 14 (%87,5) | ||
| EI Pre-T | Yes | 1 (%6,3) | 2 (%12,5) | 3 (%18,8) | 0,552 (χ²=1,189) |
| No | 15 (%93,8) | 14 (%87,5) | 13 (%81,3) | ||
| EI Post-T | Yes | 0 (%0) | 1 (%6,3) | 0 (%0) | 0,326 (χ²=2,24) |
| No | 16 (%100) | 15 (%93,8) | 16 (%100) | ||
| St Pre-T | Yes | 4 (%25) | 2 (%12,5) | 2 (%12,5) | 0,564 (χ²=1,146) |
| No | 12 (%75) | 14 (%87,5) | 14 (%87,5) | ||
| St Post-T | Yes | 1 (%6,3) | 1 (%6,3) | 3 (%18,8) | 0,433 (χ²=1,673) |
| No | 15 (%93,8) | 15 (%93,8) | 13 (%81,3) |
3.5. Within-Group Comparison of Errors
3.6. Statistical Power Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Talasz, H.; Kofler, M.; Kalchschmid, E.; Pretterklieber, M.; Lechleitner, M. Breathing with the pelvic floor? Correlation of pelvic floor muscle function and expiratory flows in healthy young nulliparous women. Int Urogynecol J 2010, 21, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Bø, K.; Berghmans, B. Evidence-Based Physical Therapy for the Pelvic Floor bridging science and clinical practice (Second Edition); Elsevier Churchill Livingstone, 2015. [Google Scholar] [CrossRef]
- Fitz, F.F.; Paladini, L.M.; Ferreira, L.d.A.; Gimenez, M.M.; Bortolini, M.A.T.; Castro, R.A. Ability to contract the pelvic floor muscles and association with muscle function in incontinent women. International urogynecology journal 2020, 31, 2337–2344. [Google Scholar] [CrossRef]
- Mateus-Vasconcelos, E.C.L.; Ribeiro, A.M.; Antonio, F.I.; Brito, L.G.d.O.; Ferreira, C.H.J. Physiotherapy methods to facilitate pelvic floor muscle contraction: A systematic review. Physiotherapy theory and practice 2018, 34, 420–432. [Google Scholar] [CrossRef]
- Thompson, J.A.; O'Sullivan, P.B.; Briffa, N.K.; Neumann, P. Assessment of voluntary pelvic floor muscle contraction in continent and incontinent women using transperineal ultrasound, manual muscle testing and vaginal squeeze pressure measurements. Int Urogynecol J Pelvic Floor Dysfunct 2006, 17, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Neels, H.; De Wachter, S.; Wyndaele, J.-J.; Van Aggelpoel, T.; Vermandel, A. Common errors made in attempt to contract the pelvic floor muscles in women early after delivery: A prospective observational study. European Journal of Obstetrics & Gynecology and Reproductive Biology 2018, 220, 113–117. [Google Scholar]
- Brækken, I.H.; Villumstad, T.K.; Evensen, N.M. Randomised controlled pilot trial to assess effect of electrical stimulation of weak pelvic floor muscles. Archives of Gynecology and Obstetrics 2024, 309, 2921–2929. [Google Scholar] [CrossRef]
- Dietz, H.; Wilson, P.; Clarke, B. The use of perineal ultrasound to quantify levator activity and teach pelvic floor muscle exercises. International urogynecology journal 2001, 12, 166–169. [Google Scholar] [CrossRef]
- Fine, P.; Burgio, K.; Borello-France, D.; Richter, H.; Whitehead, W.; Weber, A.; Brown, M.; Network, P.F.D. Teaching and practicing of pelvic floor muscle exercises in primiparous women during pregnancy and the postpartum period. American journal of obstetrics and gynecology 2007, 197, 107–e101. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, B.d.F.; Franco, G.R.; Feitosa, S.M.; Yuaso, D.R.; Castro, R.d.A.; Girão, M.J.B.C. Physiotherapy for perineal consciousness: A comparison between pelvic floor muscle training alone and with biofeedback. Fisioterapia em Movimento 2012, 25, 639–648. [Google Scholar] [CrossRef]
- Zachry, T.; Wulf, G.; Mercer, J.; Bezodis, N. Increased movement accuracy and reduced EMG activity as the result of adopting an external focus of attention. Brain research bulletin 2005, 67, 304–309. [Google Scholar] [CrossRef]
- Benjaminse, A.; Gokeler, A.; Dowling, A.V.; Faigenbaum, A.; Ford, K.R.; Hewett, T.E.; Onate, J.A.; Otten, B.; Myer, G.D. Optimization of the anterior cruciate ligament injury prevention paradigm: Novel feedback techniques to enhance motor learning and reduce injury risk. journal of orthopaedic & sports physical therapy 2015, 45, 170–182. [Google Scholar]
- Chua, L.K.; Jimenez-Diaz, J.; Lewthwaite, R.; Kim, T.; Wulf, G. Superiority of external attentional focus for motor performance and learning: Systematic reviews and meta-analyses. Psychol Bull 2021, 147, 618–645. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. Journal of psychiatric research 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Güngen, C.; Ertan, T.; Eker, E.; Yaşar, R.; Engin, F. Standardize mini mental test’in Türk toplumunda hafif demans tan› s› nda geçerlik ve güvenilirliği. Türk Psikiyatri Dergisi 2002, 13, 273–281. [Google Scholar]
- Akbayrak, T.K.S. Kadın Sağlığında Fizyoterapi ve Rehabilitasyon; Hipokrat Kitabevi&Pelikan Kitabevi, 2016. [Google Scholar]
- Arranz-Martín, B.; García-Gallego, P.; Romay-Barrero, H.; Navarro-Brazález, B.; Martínez-Torres, C.; Torres-Lacomba, M. Bladder Base Displacement during Abdominal Muscles Contraction and Functional Activities in Primiparous Women Assessed by Transabdominal Ultrasound: A Descriptive Study. J Clin Med 2021, 11. [Google Scholar] [CrossRef]
- Iaocharoen, P.; Lekskulchai, O.; Chiengthong, K.; Bunyavejchevin, S.; Tanprasertkul, C.; Somprasit, C. The Correlations between Three Methods of Pelvic Floor Muscle Strength Assessment in Nulliparous Women: 2D Transperineal Ultrasound, Modified Oxford Scale, and PFX2® Perineometer. Asian Medical Journal and Alternative Medicine 2023, 23, 72–80. [Google Scholar]
- Porrón-Irigaray, A.; Rodríguez-López, E.S.; Acevedo-Gómez, M.B.; Ojedo-Martín, C.; Benito-de-Pedro, M. Coactivation of the Pelvic Floor and Gluteus Medius Muscles While Walking and Running in Female Runners. Sensors (Basel) 2024, 24, 1356. [Google Scholar] [CrossRef]
- Chmielewska, D.; Stania, M.; Sobota, G.; Kwaśna, K.; Błaszczak, E.; Taradaj, J.; Juras, G. Impact of different body positions on bioelectrical activity of the pelvic floor muscles in nulliparous continent women. BioMed research international 2015, 2015, 905897. [Google Scholar] [CrossRef]
- Kurtoglu, A.; Ciftci, R.; Car, B.; Konar, N. Investigation of Deltoid Muscle Activation From Different Angles in Body Building Athletes. The Medical Bulletin of Sisli Etfal Hospital 2023, 57, 410. [Google Scholar] [CrossRef]
- Navarro Brazález, B.; Sánchez Sánchez, B.; Prieto Gómez, V.; De La Villa Polo, P.; McLean, L.; Torres Lacomba, M. Pelvic floor and abdominal muscle responses during hypopressive exercises in women with pelvic floor dysfunction. Neurourology and urodynamics 2020, 39, 793–803. [Google Scholar] [CrossRef]
- Abe-Takahashi, Y.; Kitta, T.; Ouchi, M.; Okayauchi, M.; Chiba, H.; Higuchi, M.; Togo, M.; Shinohara, N. Reliability and validity of pelvic floor muscle strength assessment using the MizCure perineometer. BMC Women's Health 2020, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Şahin, Ü.K. Stres İnkontinansı Olan Kadınlarda Pelvik Taban Kas Eğitimine Ek Olarak Uygulanan Eksternal Elektrik Stimülasyonunun Etkileri. 2020.
- Vermandel, A.; De Wachter, S.; Beyltjens, T.; D’Hondt, D.; Jacquemyn, Y.; Wyndaele, J.J. Pelvic floor awareness and the positive effect of verbal instructions in 958 women early postdelivery. International urogynecology journal 2015, 26, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Keshwani, N.; McLean, L. State of the art review: Intravaginal probes for recording electromyography from the pelvic floor muscles. Neurourol Urodyn 2015, 34, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Kaçar, R. Effect of core muscle endurance on pain, posture and upper extremity function in upper strings players. Master's Thesis, Gazi Üniversitesi, 2024. [Google Scholar]
- Neumann, P.; Gill, V. Pelvic floor and abdominal muscle interaction: EMG activity and intra-abdominal pressure. Int Urogynecol J Pelvic Floor Dysfunct 2002, 13, 125–132. [Google Scholar] [CrossRef]
- Bø, K.; Kvarstein, B.; Hagen, R.R.; Larsen, S. Pelvic floor muscle exercise for the treatment of female stress urinary incontinence: II. Validity of vaginal pressure measurements of pelvic floor muscle strength and the necessity of supplementary methods for control of correct contraction. Neurourology and urodynamics 1990, 9, 479–487. [Google Scholar] [CrossRef]
| Grup I (n=16) | Grup II (n=16) | Grup III (n=16) | ||
| Median (IQR) | Median (IQR) | Median (IQR) | P (value) | |
| Age (years) | 46,5 (43,5 – 49,75) | 43 (40 – 49) | 44,5 (43 – 48,5) | 0,382 (kw=1,927) a |
| BMI (kg/m2) | 28,85 (24 – 30,25) | 26,8 (24,1- 29,35) | 25,95 (22,53 – 29,48) | 0,507 (kw=1,36) a |
| Gravida (n) | 3 (2- 3) | 3 (2,25- 4) | 3 (2,25- 4) | 0,665 (kw=0,817) a |
| Parity (n) | 2,5 (2- 3) | 3 (2- 3) | 3 (2- 3) | 0,986 (kw=0,029) a |
| Abortion (n) | 0 (0- 0) | 0 (0- 0,75) | 0 (0- 0) | 0,745 (kw=0,588) a |
| Curretage (n) | 0 (0- 1) | 0 (0- 0,75) | 1 (0- 1) | 0,23 (kw=2,942) a |
| Primary(n) | 5 (%31,3) | 5 (%31,3) | 3 (%18,8) | |
| Education High school(n) | 6 (%37,5) | 5 (%31,3) | 5 (%31,3) | 0,826 (χ²=1,503) b |
| Undergraduate and Graduate(n) | 5 (%31,3) | 6 (%37,5) | 8 (%50) | |
| Vaginal (n) | 10 (%62,5) | 13 (%81,3) | 8 (%50) | |
| Mode of delivery Cesarian(n) | 3 (%18,8) | 2 (%12,5) | 3 (%18,8) | 0,356 (χ²=4,392) b |
| Vaginal and Cesarian(n) | 3 (%18,8) | 1 (%6,3) | 5 (%31,3) |
| Group I | Group II | Group III | Between-group (p) | |||||
| A.M. ± S.D. | Med (IQR) | A.M. ± S.D. | Med (IQR) | A.M. ± S.D. | Med (IQR) | |||
| MOS-(Pre-T) | 2,56 ± 0,73 | 2 (2- 3) | 2,69 ± 0,7 | 3 (2- 3) | 2,5 ± 0,63 | 2 (2- 3) | 0,721 (kw=0,654)a | |
| MOS-(Post-T) | 2,69 ± 0,7 | 3 (2- 3) | 2,94 ± 0,57 | 3 (3- 3) | 2,88 ± 0,72 | 3 (2- 3) | 0,497(kw=1,399) a | |
| Within-group (p) | 0,157 (z=-1,414)c | 0,046* (z=2)c | 0,014* (z=-2,449)c | |||||
| MOS difference | -0,13 ± 0,34 | 0 (0- 0) | -0,25 ± 0,45 | 0 (-0,75- 0) | -0,38 ± 0,5 | 0 (-1- 0) | 0,271 (kw=2,611) a | |
| vaginalEMG-(Pre-T) (cont) | 34,03 ± 22,34 | 28,15 (17,88- 37,88) | 34,77 ± 23,3 | 26,85 (20,08- 39,8) | 30,03 ± 15,62 | 29,6 (19,13- 35,93) | 0,861(kw=0,298) a | |
| vaginalEMG-(Post-T) (cont) | 33,22 ± 28,33 | 25,4 (13,75- 39,08) | 39,46 ± 24,95 | 33,95 (24,2- 46,13) | 39,35 ± 38,45 | 29,2 (18,8- 43,63) | 0,285(kw=2,509) a | |
| Within-group (p) | 0,379 (z=-0,879)c | 0,025* (t=-2,498)d | 0,932 (z=-0,085)c | |||||
| n | % | n | % | n | % | p | ||
| vaginal EMG difference | increase | 5 | 31,3 | 11 | 68,8 | 7 | 43,8 | 0,097(χ²=4,675) b |
| decrease | 11 | 68,8 | 5 | 31,3 | 9 | 56,3 | ||
| Group I | Group II | Group III | ||||||
| A.M. ± S.D. | Med (IQR) | A.M. ± S.D. | Med (IQR) | A.M. ± S.D. | Med (IQR) | Between-group (p) | ||
| tAoE-Pre-T | 1,88 ± 1,67 | 2 (0 - 3,5) | 1,69 ± 1,35 | 1,5 (1 - 2,75) | 1,88 ± 1,02 | 2 (1 - 3) | 0,802 (kw=0,442)a | |
| tAoE-Post-T | 0,25 ± 0,68 | 0 (0 - 0) | 0,56 ± 1,15 | 0 (0 - 0,75) | 0,81 ± 0,83 | 1 (0 - 1,75) | 0,061 (kw=5,595)a | |
| Within-group (p) | 0,004* (z=-2,848)c | 0,007* (z=-2,684)c | 0,003* (t=3,597)c | |||||
| Difference of tAoE | 1,63 ± 1,54 | 2 (0 - 2,75) | 1,13 ± 1,45 | 1 (0 - 2) | 1,06 ± 1,18 | 1 (0 - 2) | 0,57 (kw=1,123)a | |
| Abd EMG-(Pre-T) (cont) | 13,82 ± 10,39 | 8,65 (5,43- 20,63) | 18,75 ± 14,32 | 14,45 (8,38- 20,48) | 23,19 ± 17,18 | 18,85 (9,9- 37,63) | 0,177 (kw=3,468)a | |
| Abd EMG-(Post-T) (cont) | 17,15 ± 15,62 | 14,25 (5,35- 23,25) | 16,16 ± 13,84 | 10,7 (6,13- 21,33) | 26,48 ± 22,01 | 18,5 (8,95- 40,73) | 0,305 (kw=2,378)a | |
| Within-group (p) | 0,535 (z=-0,621)c | 0,016* (t=2,699)d | 0,532 (z=-0,625)c | |||||
| EMG difference (cont) | 3,33 ± 14,4 | 0,1 (-9,6- 3,18) | 2,59 ± 3,84 | 1,9 (-0,35- 5) | 3,29 ± 9,57 | 0,15 (-10,55- 3,18) | 0,139 (kw=3,946)a | |
| n | % | n | % | n | % | p | ||
| Abd EMG difference | increase | 8 | 50 | 4 | 25 | 7 | 43,8 | 0,322 (χ²=2,265)b |
| decrease | 8 | 50 | 12 | 75 | 9 | 56,3 | ||
| group | Addcont Post-T | ||||
| yes | no | Within-group (p) | |||
| Group I | addcont Pre-T | yes | 1 (%6,3) | 9 (%56,3) | 0,004* |
| no | 0 (%0) | 6 (%37,5) | |||
| Group II | addcont Pre-T | yes | 2 (%12,5) | 8 (%50) | 0,008* |
| no | 0 (%0) | 6 (%37,5) | |||
| Group III | addcont Pre-T | yes | 3 (%18,8) | 4 (%25) | 0,125 |
| no | 0 (%0) | 9 (%56,3) | |||
| group | Glcont Post-T | ||||
| yes | no | Within-group (p) | |||
| Group I | Glcont Pre-T | yes | 2 (%12,5) | 9 (%56,3) | 0,004* |
| no | 0 (%0) | 5 (%31,3) | |||
| Group II | Glcont Pre-T | yes | 3 (%18,8) | 6 (%37,5) | 0,031* |
| no | 0 (%0) | 7 (%43,8) | |||
| Group III | Glcont Pre-T | yes | 3 (%18,8) | 8 (%50) | 0,008* |
| no | 0 (%0) | 5 (%31,3) | |||
| group | SB Post-T | ||||
| yes | no | Within-group (p) | |||
| Group I | SB Pre-T | yes | (%0) | 4 (%25) | - |
| no | (%0) | 12 (%75) | |||
| Group II | SB Pre-T | yes | 1 (%6,3) | 3 (%18,8) | 0,625 |
| no | 1 (%6,3) | 11 (%68,8) | |||
| Group III | SB Pre-T | yes | 2 (%12,5) | 3 (%18,8) | 0,25 |
| no | 0 (%0) | 11 (%68,8) | |||
| group | EI Post-T | ||||
| yes | no | Within-group (p) | |||
| Group I | EI Pre-T | yes | (%0) | 1 (%6,3) | - |
| no | (%0) | 15 (%93,8) | |||
| Group II | EI Pre-T | yes | 1 (%6,3) | 1 (%6,3) | 1 |
| no | 0 (%0) | 14 (%87,5) | |||
| Group III | EI Pre-T | yes | (%0) | 3 (%18,8) | - |
| no | (%0) | 13 (%81,3) | |||
| group | St Post-T | ||||
| yes | no | Within-group (p) | |||
| Group I | St Pre-T | yes | 1 (%6,3) | 3 (%18,8) | 0,25 |
| no | 0 (%0) | 12 (%75) | |||
| Group II | St Pre-T | yes | 0 (%0) | 2 (%12,5) | 1 |
| no | 1 (%6,3) | 13 (%81,3) | |||
| Group III | St Pre-T | yes | 1 (%6,3) | 1 (%6,3) | 1 |
| no | 2 (%12,5) | 12 (%75) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



