Submitted:
10 February 2025
Posted:
11 February 2025
You are already at the latest version
Abstract
Background
Weight loss and energy restriction are potential strategies for reducing cancer risk, particularly if they reduce ectopic body fat and improve insulin resistance. This randomised study compared the effects of intermittent energy restriction (IER) to continuous energy restriction (CER) on hepatic, pancreatic and intramuscular fat, and insulin resistance.
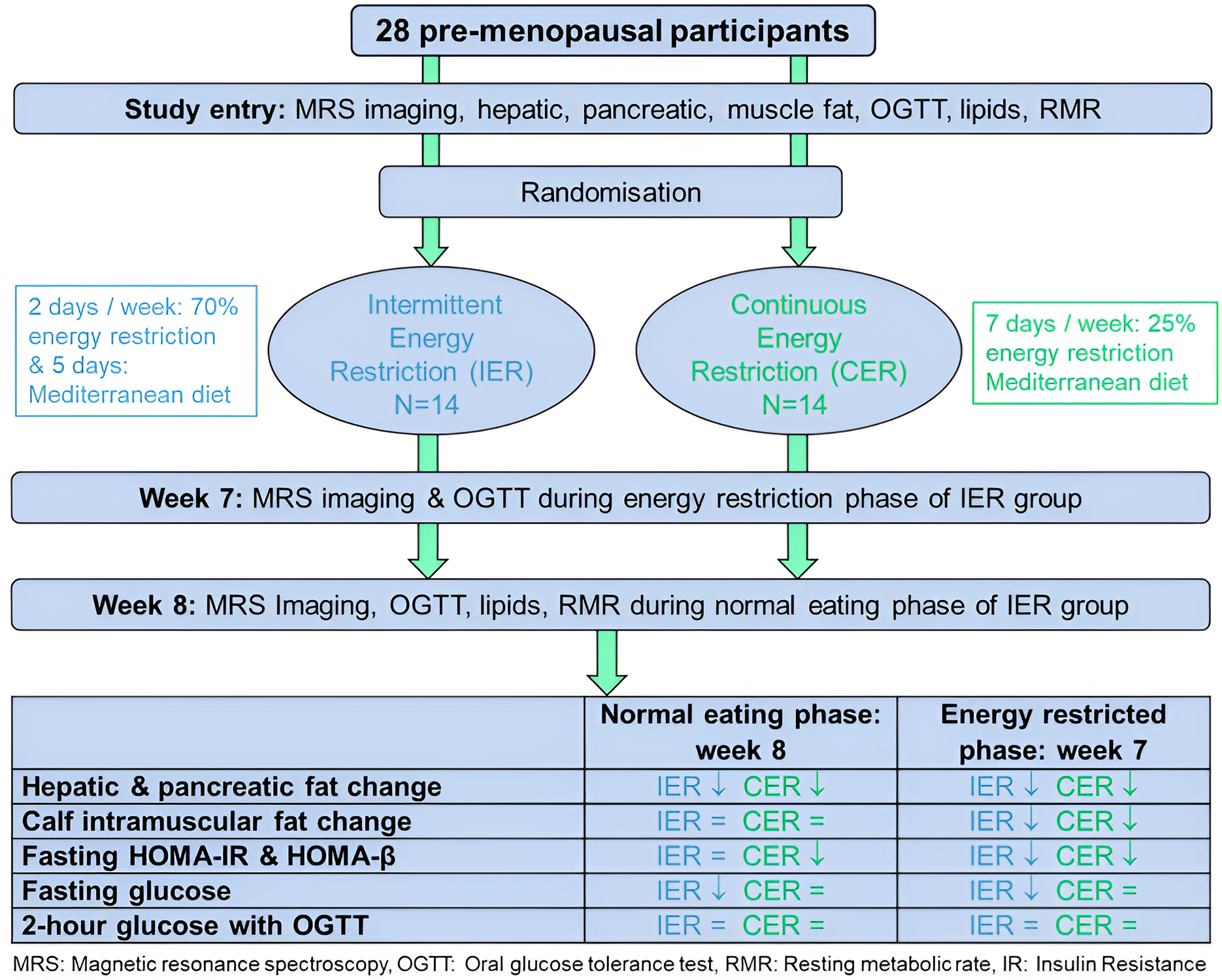
Method Premenopausal women with obesity (n=28) were randomised to two months of 25% energy restriction: IER (2 days/week 600 kcal and 5 days/week Mediterranean diet) versus CER (7 days/week Mediterranean diet). Changes in body weight, hepatic, pancreatic and intramuscular fat (magnetic resonance spectroscopy) and insulin resistance (HOMA and oral glucose tolerance test), body fat and muscle mass (bioelectrical impedance), resting metabolic rate (RMR, indirect calorimetry) were assessed during the energy restricted and normal eating days of IER compared to CER.
Results
9 IER and 11 CER participants completed the trial. IER and CER had comparable reductions in body weight mean (SD): IER -6.7(1.4) kg CER -6.2(2.9) kg, and reductions in hepatic, pancreatic and intramuscular fat stores. Fasting measures of insulin resistance (HOMA IR, HOMA-β and fasting insulin) reduced in the CER group and with IER when assessed immediately after the two low energy days but were not maintained during normal eating days. There were no changes in 2-hour glucose in either group.
Conclusions
IER and CER have comparable reductions in weight and ectopic fat stores. The clinical significance of the failure to maintain beneficial insulin sensitivity across the week with IER is not known and requires further study.
Keywords:
obesity
; cancer risk
; hepatic fat
; pancreatic fat
; intramuscular fat
; insulin resistance
; metabolic rate
; fat free mass
1. Introduction
Obesity, defined as high body mass index, is a well-established risk factor for post-menopausal breast and other cancers[1]. Risk of postmenopausal breast and other cancers have been shown to be specifically linked to excess body fat in combination with increased serum insulin and insulin resistance [2,3,4,5].
Ectopic fat stored in the liver may have specific links to risk of breast and other non-hepatic cancers in women [6] mediated by systemic effects of hyperinsulinemia and insulin resistance [2,5], including direct mitogenic effects of insulin and associated increases in bioavailable sex hormones, increased leptin, reduced adiponectin and chronic inflammation.
Weight loss and energy restriction are potential strategies for reducing cancer risk, particularly if they can reduce ectopic body fat and improve insulin resistance. Some (though not all), previous studies have reported weight independent improvements in markers of HOMA insulin resistance with Intermittent Energy Restriction (IER) diet versus a Continuous Energy Restriction (CER) [7], including subjects with impaired glucose metabolism and pre-diabetes[8]. A study in female C57BL/6J mice reported ectopic and visceral fat stores were mobilised with IER regimens which include spells of 70% energy restriction or greater but fat store mobilisation was not achieved with a daily 25% energy restriction[9].
We conducted a randomised controlled trial to compare the effects of IER versus CER diets on body weight, body fat and magnetic resonance spectroscopy (MRS) measurements of hepatic, pancreatic and intramuscular fat deposition, and markers of insulin resistance in women living with obesity who were at increased risk of breast and other weight related cancers. MRS and insulin resistance measures were assessed during the normal eating phase (during the five normal eating days of the week at least two days after the low calorie days), and the energy restricted phase (when fasted the morning after two restricted days) in the IER group to assess the overall effects of IER across the week vs. CER.
2. Materials and Methods
2.1. Study Design and Participants
The eight-week two arm randomised trial was performed at the family history clinic at the Prevent Breast Cancer Research Unit, Manchester University Foundation Trust (recruitment, dietary intervention advice, measurement of resting energy expenditure and anthropometric measures), the Wolfson Molecular Imaging Centre, The Christie NHS Foundation Trust (MRS) and the endocrine unit at The Christie NHS Foundation Trust (insulin resistance measures) January to November 2015. The study is written in accordance with CONSORT reporting guidelines (Table S1). The IER and CER interventions are described using the Template for Intervention Description and replication (TIDieR) checklist (Table S2) [10].
Women with a family history of breast cancer were recruited by mailed letters from the family history clinic. We also recruited women with no known family history by email to employees at Manchester University Hospitals and The Christie NHS Foundation Trusts and the University of Manchester (Figure 1). Eligibility criteria included being premenopausal aged >30 and ≤45 years, BMI 30-45kg/m2, non–smoker, sedentary (less than 40 minutes moderate exercise per week) and excluded those already losing weight, with previous bariatric surgery or receiving weight loss medications, a previous history of cancer. We excluded individuals with factors which could have weight independent effects on hepatic fat including comorbidities like non-alcoholic fatty liver disease, diabetes, viral hepatitis, fibrosis, human immunodeficiency virus, current or recent (within 6 months) medications i.e. oral contraceptives, tamoxifen, statins, amiodarone, methotrexate, corticosteroids, or alcohol intake > 140 g /week. Also, those who were contraindicated for MR imaging (e.g. pacemaker or body weight > 125 kg).
2.2. Randomisation
Eligible participants were randomised 1:1 to IER or CER by an independent research administrator using a minimisation programme which stratified for whether participants were above or below the predicted median BMI 35 kg/m2. Laboratory staff undertaking serum assays and MRI scanning were blinded to the participant study arm. It was not possible to blind study participants or other staff.
2.3. Dietary Interventions
The IER and CER interventions both involved an overall 25% energy restriction below estimated requirements. Baseline energy requirements for each participant were estimated using indirect calorimetry (Fitmate GS portable desktop indirect calorimeter (Cosmed, Rome Italy).
The IER group was prescribed a low carbohydrate energy restricted diet (600 kcal, <50g carbohydrate, 50 g protein day) (70% energy restriction) for two consecutive days and ~1900 kcal Mediterranean diet for the remaining five days of the week. Each of the two low carbohydrate 600 kcal energy restricted days included approximately 300g of lean protein foods e.g. lean meat, fish, eggs, tofu, Quorn, textured vegetable protein, three portions of low fat dairy foods, five portions of low carbohydrate vegetables, one portion of low carbohydrate fruit and two pints of low energy drinks. The five unrestricted days were based on a Mediterranean diet which provides 30% energy from fat (15% monounsaturated fat [MUFA] 8% polyunsaturated [PUFA] 7% saturated [SFA]), 25% energy from protein and 45% from low glycaemic load carbohydrate and allows up to 10 units of alcohol per week. Participants randomised to CER were prescribed a daily 25% energy restricted Mediterranean diet (approximately 1500kcal/day) for seven days/week. The Mediterranean diet provides 30% energy from fat (15% MUFA, 8% PUFA, 7% SFA), 25% energy from protein and 45% from low glycaemic load carbohydrate and allows up to 10 units of alcohol per week. The IER and CER diets were matched for energy and had an optimal macronutrient composition for limiting hepatic fat fraction (HFF) : 45% energy from carbohydrate, 25% from protein and 30% from fat (15% MUFA, 7% SFA and 8% PUFA) and allowed up to 10 units of alcohol per week.
Foods eaten on the IER and CER diets were self-selected by the patients and not provided by the study team. The IER and CER groups received clear instructions of how to follow their allocated diet in a face-to-face dietary consultation with one of the trial dietitians (45-60 minute appointment) at the Prevent Breast Cancer Research Unit who had experience of delivering intermittent and daily diets. Both groups received comprehensive written instructions of how to follow the diets at home, including recommended portion sizes, recipes, and suggested meal plans. They also received appropriate behavioural techniques to promote dietary adherence i.e. self-monitoring of diet and weight, and goal setting. Both groups were counselled to maintain their current sedentary lifestyle to allow any effects of diet change to be assessed without confounding effects from changes in physical activity level.
Participants had a telephone call from their allocated dietitian one week after starting the diet to check that they had started the diet, their understanding of the diet and to provide any trouble shooting advice. Both groups attended the Prevent Breast Cancer Research Unit in weeks 2, 4, and 6 for a face-to-face review and weigh in with their allocated dietitian with phone calls in week 3, 5 and 7 to discuss adherence and any problems with the diet. Both groups were asked to record paper or online (My Food 24 https://www.myfood24.org/) 7-day food records during study weeks 3, 5 and 8. This allowed the team to assess adherence to their allocated diet and served as an important tool to enhance adherence.
2.4. Outcome Measures and Relevant Methods
2.4.1. Primary Outcome Measure
The primary outcome measure was change in quantity of intrahepatic fat (hepatic fat fraction HFF) determined using MRS after 8 weeks of the dietary interventions at least two days after the energy restricted days, on normal eating days in the IER group. MRS was used to measure water and fat in the organ as reported previously (11) on a 1.5T Philips Achieva 1.5T scanner (Best, The Netherlands). Details of the acquisition and processing of the MRS data are provided in Supplementary file 1.
2.4.2. Secondary Outcome Measures and Relevant Methods
Secondary outcomes were changes in the following parameters after eight weeks on the diets on normal eating days in the IER group:
- Quantity of pancreatic fat fraction (PFF) and calf intramyocellular and extramyocellular fat fraction (CIFF) determined using MRS, as above with further details in Supplementary file 1.
- Body weight, total body fat and fat free mass were assessed with bioelectrical impedance (Tanita 180, Tokyo, Japan) after fasting for 5 or more hours.
- Measures of insulin resistance determined using an Oral Glucose Tolerance Testing (OGTT) i.e. fasting homeostasis model assessment (HOMA)-IR (insulin resistance) and HOMA-β (beta cell function) (version 2.23 http://www.ocdem.ox.ac.uk/), fasting and 2 hour glucose, average C–peptide (insulin production) insulin and glucose and glucose area under the curve from serum measurements taken at baseline and after 60, 90, 120, 150, 180 minutes across the OGTT. Insulin and C-peptide samples were centrifuged immediately after collection to separate the serum from the cells and samples stored at -70°C, and were measured at the University of Aarhus, Denmark. Samples for blood glucose and lipids were analysed the same day at the Endocrine Unit at Christie Hospital.
- Resting metabolic rate (RMR) estimated from oxygen consumption over 5-15 minutes steady state minutes under standardised conditions i.e. after fasting for 5 or more hours, avoiding caffeine and exercise for 2 hours of more and after 20 minutes lying at complete rest using the (Fitmate GS portable desktop indirect calorimeter, Cosmed, Rome Italy). RMR was estimated from oxygen consumption using the Weir equation RMR [kcal/day] = (3.9+1.1*RQ)*VO2[ml/min]*1.44 assuming a fixed respiratory quotient (RQ) of 0.85 [11]. This was reported as the actual value and as percentage of RMR predicted with the Mifflin equation to standardise for changes in body weight.
- Fasting lipids (total, LDL HDL cholesterol and triglycerides), blood pressure.
- Hepatic fat fraction from MRS and insulin resistance measures were also assessed during the energy restricted phase (when fasted the morning after two restricted days) in the IER group to assess the overall effects of IER across the week vs. CER.
- Dietary intake of mean daily energy, protein, carbohydrate, total fat, SFA, PUFA, MUFA, fibre (Englyst method) and weekly alcohol intakes in the IER and CER groups were assessed using either the paper or online food diaries (My Food 24 https://www.myfood24.org/) completed at baseline and study weeks 3, 5 and 8. The IER group were also asked to record their adherence to the 2-day IER each week in a study diary sheet. Weekly leisure physical activity level (International physical activity questionnaire long version [IPAQ]) in metabolic equivalent minutes/ day (MET) was assessed at baseline, week 4 and week 8 to indicate whether participants remain sedentary throughout the trial[12].
- Serious adverse events were recorded within the study using the Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0[13].
2.5. Statistical Methods
The sample size of 14 subjects per group was chosen to detect a difference of 15% in the reduction of hepatic fat fraction between the two different diets, assuming an estimated 20% drop-out rate. Calculations assume a two-sided t-test with estimated standard deviation of 10% and the conventional 5% significance level.
The analysis was performed on a per-protocol basis amongst participants who had completed 8 weeks on their allocated diet, as the study aimed to investigate the mechanistic effect of diet rather than an intention to treat comparison of the two diets. Statistical significance was assessed at the two-sided 5% significance level.
Descriptive statistics were presented using means, standard deviations, and ranges for normally distributed variables. Mixed effects models were used to account for the multiple observations per patient using generalized linear latent and mixed models (GLLAMM) performed in STATA version 16. An interaction term between time and randomised group was used to assess whether there was a significant difference in the change over time between the groups. Insulin resistance and lipid biomarker analyses were adjusted for day of the menstrual cycle [14,15].
Individual participant change in hepatic and pancreatic fat between baseline and week 8 were reported in waterfall plots. Pearson correlation analyses were performed for the relationship between changes in hepatic and pancreatic with weight and with the insulin resistance variables HOMA-IR , HOMA-β and 2-hour glucose within the OGTT. Dietary intake and leisure time physical activity at baseline and across the IER and CER interventions were reported.
3. Results
3.1. Recruitment and Retention and Participants Recruited to the Study
Twenty-eight participants were recruited and randomised to IER (n=14) and CER (n=14), 16 were recruited from the family history clinic who all had an estimated lifetime breast cancer risk with the Tyrer Cuzick model of ≥17%[16]. Clinic recruitment was via a mailed invitation letter (1% uptake, 16/1153 invitations sent) and a further 12 were women with no known family history of breast cancer were recruited from promotional emails and posters within the hospitals and the university where the research was taking place.
Five of the IER group withdrew prior to week 7 (3 loss of contact, 1 had a large dermoid ovarian cyst detected on the MRI scan, 1 was diagnosed with ovarian cancer). Three of the CER group withdrew prior to week 7 (1 did not tolerate the OGTT and 2 did not wish to complete 8 weeks of the diet). At the end of the study there were nine completers of the 14 recruited to IER (64%) and 11 completers of the 14 recruited to CER (79%), see Figure 1 Consolidated Standards of Reporting Trials (CONSORT).
Table 1. Mean (SD) age of the completers was 40.1 (5.6) years and mean (SD) BMI was 34.7 (4.3) kg/m2. The cohort was white (19/20, 95%) and included 1 black African participant (1/20, 5%).
3.2. Changes in Weight and MRS Fat Stores with IER and CER
Examples of MR spectra from liver, pancreas and calf muscle are shown in Figure S1 and Figure S2. The spectra contain two prominent signals, from water at a frequency of 4.7 ppm and from fat (CH2)N chains at ~1.3 ppm. The spectra were fitted to a model consisting of water and fat signals and the output of the model was the water and fat content of the tissue voxel in instrumental units. The fat fraction was calculated as the ratio of the fat signal to the sum of the fat and water signals.
Mean (SD) and minimum and maximum weight and MRS fat stores at baseline week 7 and week 8 are reported in Table 2. Between baseline and week 8 there was comparable absolute and percentage weight loss between the groups mean (SD): IER -6.7 (1.4) kg -7.2 (1.6) % , CER -6.2 (2.9) kg 6.3 (3.1) %. Both groups experienced comparable reductions in HFF% and PFF% at week 7 and 8 and reductions in CIFF % at week 7 only. There was no interaction for change in weight or any of the fat stores at week 7 or week 8 between IER and CER in the GLLAMM model (Table 3).
3.3. Waterfall Plots of Changes in HFF and PFF with IER and CER
3.4. Change in Measures of Insulin Resistance with IER and CER
At week 7 immediately after the two low calorie days of IER, both groups experienced reductions in all fasting measures of insulin resistance i.e. HOMA IR, HOMA-β and fasting insulin. Glucose tolerance tests at week 7 showed small reductions in area under the curve for glucose and 2 hour glucose with CER, which both increased slightly with IER (Table 2). However, there was no interaction in change in these parameters between the groups with the GLLAMM model (Table 3).
At week 8 the CER group had a reduction in HOMA IR and HOMA-β which were unchanged in the IER group. The IER group had a reduction in fasting glucose which did not change with CER (Table 2). These different changes had significant diet group interactions with the GLLAMM model (Table 3). There were no changes in 2 hour glucose at week 7 or 8 in either group.
3.5. Change in Lipid Measurement with IER and CER
3.6. Changes in Fat Free Mass and Resting Energy Expenditure with IER and CER
Both groups had reductions in FFM and RMR at week 8 (Table 2). There were no differences between change over time in the groups
3.7. Adherence to the IER and CER Dietary Interventions
Completers in the IER group received all scheduled dietitian calls and face to face reviews and reported undertaking 100% of their allocated low energy days during the trial. Self-reported dietary intake at baseline and across the study (average of intakes reported at week 3, 5 and 8) are reported in Table S3. Both groups reported reductions in energy, carbohydrate, total sugar, total, SFA and MUFA/ PUFA fat, alcohol and maintained protein, and dietary fibre. There were no differences in change in dietary intake between the IER and CER groups (Table S4). Reported leisure physical activity is reported in Table S5, which did not change over time in either group.
3.8. Adverse Events
There were 2 serious adverse events in the intermittent group. One participant had identified a large dermoid ovarian cyst identified at baseline scan which required surgery. Another participant had lesions identified in week 7 scan which were confirmed as ovarian cancer. These events were not believed to relate to the dietary interventions or participation in the study.
3.9. Correlations Between Change in Hepatic and Pancreatic Fat and Change in Insulin Resistance Variables at 8 Weeks
Across all participants (n=19) percentage reductions in weight had modest correlations with percentage change in hepatic fat; r=0.301, p=0.198 and change in pancreatic fat 0.348, p=0.133. Changes in HOMA-IR had better correlations with reductions in hepatic fat fraction (r=0.425, p=0.070) than with changes in pancreatic fat (r=0.186, p=0.070). Similarly changes in HOMA-β appeared better correlated with change in hepatic fat r=0.369, p=0.12 compared to change in pancreatic fat r=0.184, p=0.45. Changes in hepatic and pancreatic stores did not correlate with changes in 2 hour glucose in the OGTT with respective correlations of r=0.166, p=0.50 and r=0.238, p=0.33. These correlations were comparable within the IER and CER groups (data not shown).
4. Discussion
Two months of IER or CER led to comparable reductions in body fat and hepatic and pancreatic percentage fat fraction, fasting lipids, FFM, RMR in the IER and CER groups. Both groups had favourable changes in fasting insulin resistance measures at week 7 when the IER group were assessed immediately after the two low energy days. However, measures at week 8 in the normal eating phase of IER found fasting (HOMA IR, HOMA-β) measures of insulin resistance were lowered with CER but not IER. Whilst the IER group had a reduction in fasting glucose which did not change with CER. Neither group had changes in 2 hour glucose with the OGTT.
There are few data on changes in HFF and PFF alongside weight loss with energy matched IER and CER diets. Our findings align with those of the HELENA trial which reported comparable reductions in body weight and these fat stores amongst healthy men and women aged 35–65 years with overweight and obesity[17,18]. Reductions in HFF but not PFF in the current study were correlated with reductions in insulin resistance. The importance of HFF rather than PFF for impacting on insulin resistance has previously been reported [18,19].
There were large variations in changes in hepatic and pancreatic fat between individuals in both groups. This variation does not appear to be simply associated with magnitude of weight loss which is major driver of reductions in HFF in subjects with Metabolic dysfunction-Associated Steatohepatitis (MASH) [20]. Changes in hepatic fat are likely to be influenced by many other factors including the gut microbiome, muscle mass and genetics factors[21].
We observed modest reductions in CIFF at week 7 in both groups but no difference between IER and CER. Reductions in skeletal muscle triglyceride content have been reported alongside continuous low energy diets and 15% weight loss in subjects with obesity[22]. However a previous MRS imaging study failed to observe changes in CIFF with 10% weight loss with CER amongst subjects with overweight BMI 25–30 kg/m2 [23]. The effects of IER and CER on changes in CIFF may depend on the nature of the IER. Some previous studies have shown acute increases in CIFF with longer spells of total fasting which promote lipolysis, circulating FFA and lipid disposition in skeletal muscle [24]. However, a previous intermittent fasting study involving 26 hour periods of total fasting reported increased mRNA of PLIN5 a marker of lipid droplet formation which is thought to protect myocytes against lipotoxicity, which was not seen with an isoenergetic CER [25].The effects of IER and CER on CIFF are likely to require more detailed biopsy and histochemical analysis rather than MRS imaging studies.
In contrast to previous studies, we did not report improvements in fasting insulin resistance during normal eating days of IER. Previous reports have concluded equivalent effects of IER and CER or modest beneficial effects of IER vs CER on insulin resistance [7]. Many of the previous studies used a simplistic HOMA equation based on fasting insulin and glucose which models hepatic insulin resistance. The current study used the HOMA2 calculator which provides an estimate of overall insulin resistance based on hepatic and peripheral effects. Thus, discrepant findings may reflect potential differential effects of IER on hepatic and peripheral insulin resistance. Some beneficial effects on normal eating days in previous studies could have been erroneous due to unintentional sampling around low energy days of the IER diets. The current study was a tightly controlled metabolic study where we were confident that samples were collected when planned thus ensuring normal eating days samples were not collected when participants had just completed a low energy day. However, the current study had small numbers and our findings may be driven by several outliers who had large rebounds in insulin resistance around the normal eating days of the diet and may not reflect changes in a broader population.
Failure to improve post prandial glycaemic control measures after the fasting days with IER align to previous reports of IER especially in women [26]. This is unlikely to be evidence of harm, but most likely reflects a physiological glucose sparing response during times of energy restriction which increases lipolysis and circulating free fatty acids which is higher in women compared to men. Sexually dimorphic rates of fat mobilisation with energy restriction and subsequent re disposition location in the post restricted state have been reported with men experiencing more hepatic lipid re-accumulation and women more muscle lipid re-accumulation [27]. Neither the IER nor CER group had improvements in post prandial glycaemia despite weight loss. The failure to improve post-prandial glycaemia alongside a 5% weight loss with IER and CER was previously reported by Antoni [28]. This may reflect that our population and that in the previous Antoni study were mainly normoglycaemic ; only 4 of our cohort had baseline 2 hour OGTT vales in the prediabetic range (>7.9 and <11.00 mmol/L).
We reported reductions in HOMA-β cell function with CER but not IER. Changes in HOMA-β cell function alongside weight loss varies according to the levels of pancreatic function and the degree of insulin resistance of the individuals. Some studies have reported weight loss to be associated with improved β cell function in patients with severe obesity and impaired glucose tolerance [29]. However the reductions in β cell function reported herein are consistent with the observed reciprocal and proportionate decrease of HOMA–IR [30].
We reported decreased fasting glucose with IER not CER. This preferential reduction in fasting glucose compared to CER has previously been reported in a number of comparison trials[28,31,32], but by no means consistently [33,34]. This finding may be a type 1 error due to the small numbers in the study.
IER and CER had comparable reductions in resting metabolic rate which is consistent with a number of previous reports in subjects undertaking alternate day fasting and 5:2 diets [35]. This and previous studies have assessed RMR during the normal eating phase of the IER. Future studies should assess RMR during the fasting phase aswell as the normal eating phase. Fasting and calorie restriction may lead to acute increases in resting energy expenditure due to the increased metabolic cost of glucogenesis and ketogenesis[36]. However, any such effects are likely to be counteracted by reductions in diet induced thermogenesis and physical activity observed during spells of energy restriction or fasting[37].
The study has several limitations. The small, short term study was powered to show a relatively large difference in change in HFF% of 15% but was not powered to show smaller potentially important clinically significant differences between the groups. Furthermore, the drop out from the study meant we did not achieve the sample size of 9 per group required.
We studied changes in HFF, PFF and associated metabolism in premenopausal women with overweight or obesity who are a target group for weight control for the prevention of weight related cancers including breast cancer [38,39,40]. Previous human studies suggest discrepant effects in men and women whereby women have greater reductions in steatosis alongside weight loss [41] and greater sensitivity to energy restriction [42]. At baseline only 21% of the cohort had hepatic steatosis (defined as HFF >5%)[43] and 21% had pancreatic steatosis (defined as PFF >6.2% ) [44], 7% had both and 64% had neither. Different effects may be seen in a population with hepatic steatosis and insulin resistance. Most of the cohort were Caucasian hence findings herein do not inform changes which could be seen in other ethnic groups or in groups of older women or men.
Strengths include both diets having been designed to optimise reductions in HFF and were matched for energy and macronutrient content to allow the nutrient independent effects of IER or CER patterns of eating to be assessed. The study included sedentary non-smokers to remove any other confounding lifestyle related effects.
This study adds to the body of literature suggesting broadly comparable reductions in weight and key adipose stores and metabolic effects between IER and CER. It also adds to the literature on the differential effects of an IER diet during both the fasting and normal eating phases of the week. The clinical significance of the failure to maintain beneficial insulin sensitivity effects across the week on normal eating days is not known and requires further study. The findings in this study relate to a 5:2 diet and do not necessarily reflect other patterns of intermittent fasting such as alternate day fasting or time restricted eating.
The equivalent reductions hepatic fat with IER vs CER in the current study amongst our population of healthy premenopausal women may not be applicable to other populations. A recent study amongst 60 patients with Metabolic-Associated Fatty Liver Disease in China reported equivalent weight loss with IER compared to CER. However IER was associated with greater reduction in hepatic steatosis, hepatic fibrosis and liver stiffness [45]. Future larger scale randomised trials of IER vs CER amongst participants with increased ectopic fat stores and impaired insulin resistance will inform the relative ability of IER and CER to normalise these parameters and potentially reduce risk of obesity associated cancers and other obesity related conditions.
5. Conclusions
The findings after 8 weeks of IER and CER indicate significant and similar reductions in weight, (MRS-determined) ectopic-fat and insulin resistance. This profile supports further evaluation of these energy restricted dietary approaches for cancer prevention.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Supplementary File 1 MRS measurements of intra-organ fat. Fig. S1. 1H MR spectra from muscle (upper trace), pancreas tail (middle trace) and liver (bottom trace). Fig. S2. AMARES fits for muscle, liver and pancreas. Table S1 Consort checklist. Table S2 Tidier checklist. Table S3 Average daily dietary intake and at baseline and leisure time physical activity throughout the 8-week IER or CER dietary interventions for completers. Table S4 Generalized linear latent and mixed models (GLLAMM) analysis: parameter coefficient (95% CI) for changes in dietary intake between baseline and throughout the 8 week IER or CER dietary interventions for completers. Table S5 Self-reported leisure time physical activity levels at baseline and across the trial (average reported at week 4 and 8) for completers in the IER and CER groups.
Author Contributions
MH: AR, AH, GE designed the study. MH, NP, MP delivered the dietary interventions, MH, MP, PC, SW, NP,KL,LM performed data acquisition and management. MH, PC, AR, AH were involved in the analysis and interpretation of other data. SW performed interpretation of the MRS images. MH wrote the draft manuscript. All co-authors were involved in editing the manuscript and read and approved the final manuscript.
Funding
The study was funded by Pancreatic Cancer UK (registered charity number 05658041) and Prevent Breast Cancer (registered charity number 1109839). The funders had no role in the design, analysis, or decision to submit this manuscript. MH and AGR are funded by the NIHR Manchester Biomedical Research Centre (NIHR203308).
Institutional Review Board Statement
The Trial was performed in accordance with the ethical principals in the Declaration of Helsinki was granted ethics approval by NRES Committee South Central-Oxford B (ref14/SC/1097).The trial registration number is ISRCTN10803394 (http://www.isrctn.com/ISRCTN10803394).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The protocol for the study, raw data supporting the conclusions of this article and diet resources used will be made available by the authors on request.
Acknowledgments
Jan Frystyk, Aarhus for insulin measurements. David Morris for help with the MRS imaging. Phil Foden for statistical input. David Jenkins University of Manchester for producing the waterfall plots.
Conflicts of Interest
Professor Harvie and Professor Howell has co-authored three self-help books for the public to follow intermittent diets. All author proceeds are paid directly to the charity Prevent Breast Cancer (Registered Charity Number: 1109839) to fund breast cancer research.
References
- Wcrf. Diet, nutrition, physical activity and breast cancer survivors. 2018.
- Kristensson, F.M.; Andersson-Assarsson, J.C.; Peltonen, M.; Jacobson, P.; Ahlin, S.; Svensson, P.A.; Sjöholm, K.; Carlsson, L.M.S.; Taube, M. Breast Cancer Risk After Bariatric Surgery and Influence of Insulin Levels: A Nonrandomized Controlled Trial. JAMA Surg 2024, 159, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, N.M.; Arthur, R.; Manson, J.E.; Chlebowski, R.T.; Kroenke, C.H.; Peterson, L.; Cheng, T.D.; Feliciano, E.C.; Lane, D.; Luo, J. , et al. Association of Body Fat and Risk of Breast Cancer in Postmenopausal Women With Normal Body Mass Index: A Secondary Analysis of a Randomized Clinical Trial and Observational Study. JAMA Oncol 2019, 5, 155–163. [Google Scholar] [CrossRef]
- Mahamat-Saleh, Y.; Rinaldi, S.; Kaaks, R.; Biessy, C.; Gonzalez-Gil, E.M.; Murphy, N.; Le Cornet, C.; Huerta, J.M.; Sieri, S.; Tjønneland, A. , et al. Metabolically defined body size and body shape phenotypes and risk of postmenopausal breast cancer in the European Prospective Investigation into Cancer and Nutrition. Cancer Med 2023, 12, 12668–12682. [Google Scholar] [CrossRef]
- Dashti, S.G.; Simpson, J.A.; Viallon, V.; Karahalios, A.; Moreno-Betancur, M.; Brasky, T.; Pan, K.; Rohan, T.E.; Shadyab, A.H.; Thomson, C.A. , et al. Adiposity and breast, endometrial, and colorectal cancer risk in postmenopausal women: Quantification of the mediating effects of leptin, C-reactive protein, fasting insulin, and estradiol. Cancer Med 2022, 11, 1145–1159. [Google Scholar] [CrossRef] [PubMed]
- Venniyoor, A.; Al Farsi, A.A.; Al Bahrani, B. The Troubling Link Between Non-alcoholic Fatty Liver Disease (NAFLD) and Extrahepatic Cancers (EHC). Cureus 2021, 13, e17320. [Google Scholar] [CrossRef] [PubMed]
- Cioffi, I.; Evangelista, A.; Ponzo, V.; Ciccone, G.; Soldati, L.; Santarpia, L.; Contaldo, F.; Pasanisi, F.; Ghigo, E.; Bo, S. Intermittent versus continuous energy restriction on weight loss and cardiometabolic outcomes: a systematic review and meta-analysis of randomized controlled trials. J Transl Med 2018, 16, 371. [Google Scholar] [CrossRef]
- Gabel, K.; Kroeger, C.M.; Trepanowski, J.F.; Hoddy, K.K.; Cienfuegos, S.; Kalam, F.; Varady, K.A. Differential Effects of Alternate-Day Fasting Versus Daily Calorie Restriction on Insulin Resistance. Obesity (Silver Spring) 2019, 27, 1443–1450. [Google Scholar] [CrossRef]
- Varady, K.A.; Allister, C.A.; Roohk, D.J.; Hellerstein, M.K. Improvements in body fat distribution and circulating adiponectin by alternate-day fasting versus calorie restriction. The Journal of nutritional biochemistry 2010, 21, 188–195. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M. , et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. Bmj 2014, 348, g1687. [Google Scholar] [CrossRef]
- Nieman, D.C.; Austin, M.D.; Benezra, L.; Pearce, S.; McInnis, T.; Unick, J.; Gross, S.J. Validation of Cosmed's FitMate in measuring oxygen consumption and estimating resting metabolic rate. Res.Sports Med. 2006, 14, 89–96. [Google Scholar] [CrossRef]
- Ekelund, U.; Sepp, H.; Brage, S.; Becker, W.; Jakes, R.; Hennings, M.; Wareham, N.J. Criterion-related validity of the last 7-day, short form of the International Physical Activity Questionnaire in Swedish adults. Public Health Nutr. 2006, 9, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Institute, N.I.o.H.N.C. Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0. 14.6.2010 ed.; U.S.DEPARTMENT OF HEALTH AND HUMAN SERVICES: USA, 2010. [Google Scholar]
- Hummel, J.; Kullmann, S.; Wagner, R.; Heni, M. Glycaemic fluctuations across the menstrual cycle: possible effect of the brain. Lancet Diabetes Endocrinol 2023, 11, 883–884. [Google Scholar] [CrossRef] [PubMed]
- Mumford, S.L.; Dasharathy, S.; Pollack, A.Z.; Schisterman, E.F. Variations in lipid levels according to menstrual cycle phase: clinical implications. Clin Lipidol 2011, 6, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Tyrer, J.; Duffy, S.W.; Cuzick, J. A breast cancer prediction model incorporating familial and personal risk factors. Stat.Med. 2004, 23, 1111–1130. [Google Scholar] [CrossRef]
- Schübel, R.; Nattenmüller, J.; Sookthai, D.; Nonnenmacher, T.; Graf, M.E.; Riedl, L.; Schlett, C.L.; von Stackelberg, O.; Johnson, T.; Nabers, D. , et al. Effects of intermittent and continuous calorie restriction on body weight and metabolism over 50 wk: a randomized controlled trial. Am J Clin Nutr 2018, 108, 933–945. [Google Scholar] [CrossRef]
- Jiang, Y.; Spurny, M.; Schübel, R.; Nonnenmacher, T.; Schlett, C.L.; von Stackelberg, O.; Ulrich, C.M.; Kaaks, R.; Kauczor, H.U.; Kühn, T. , et al. Changes in Pancreatic Fat Content Following Diet-Induced Weight Loss. Nutrients 2019, 11. [Google Scholar] [CrossRef]
- Deng, M.; Li, Z.; Chen, S.; Wang, H.; Sun, L.; Tang, J.; Luo, L.; Zhang, X.; Xu, H.; Dai, Z. Exploring the heterogeneity of hepatic and pancreatic fat deposition in obesity: implications for metabolic health. Front Endocrinol (Lausanne) 2024, 15, 1447750. [Google Scholar] [CrossRef] [PubMed]
- Koutoukidis, D.A.; Koshiaris, C.; Henry, J.A.; Noreik, M.; Morris, E.; Manoharan, I.; Tudor, K.; Bodenham, E.; Dunnigan, A.; Jebb, S.A. , et al. The effect of the magnitude of weight loss on non-alcoholic fatty liver disease: A systematic review and meta-analysis. Metabolism 2021, 115, 154455. [Google Scholar] [CrossRef]
- Albhaisi, S.; Chowdhury, A.; Sanyal, A.J. Non-alcoholic fatty liver disease in lean individuals. JHEP Rep 2019, 1, 329–341. [Google Scholar] [CrossRef]
- Goodpaster, B.H.; Theriault, R.; Watkins, S.C.; Kelley, D.E. Intramuscular lipid content is increased in obesity and decreased by weight loss. Metabolism 2000, 49, 467–472. [Google Scholar] [CrossRef]
- Larson-Meyer, D.E.; Heilbronn, L.K.; Redman, L.M.; Newcomer, B.R.; Frisard, M.I.; Anton, S.; Smith, S.R.; Alfonso, A.; Ravussin, E. Effect of calorie restriction with or without exercise on insulin sensitivity, beta-cell function, fat cell size, and ectopic lipid in overweight subjects. Diabetes Care 2006, 29, 1337–1344. [Google Scholar] [CrossRef]
- Ahmed, S.; Singh, D.; Khattab, S.; Babineau, J.; Kumbhare, D. The Effects of Diet on the Proportion of Intramuscular Fat in Human Muscle: A Systematic Review and Meta-analysis. Front Nutr 2018, 5, 7. [Google Scholar] [CrossRef]
- Liu, B.; Hutchison, A.T.; Thompson, C.H.; Lange, K.; Wittert, G.A.; Heilbronn, L.K. Effects of Intermittent Fasting or Calorie Restriction on Markers of Lipid Metabolism in Human Skeletal Muscle. J Clin Endocrinol Metab 2021, 106, e1389–e1399. [Google Scholar] [CrossRef]
- Heilbronn, L.K.; Civitarese, A.E.; Bogacka, I.; Smith, S.R.; Hulver, M.; Ravussin, E. Glucose tolerance and skeletal muscle gene expression in response to alternate day fasting. Obes.Res. 2005, 13, 574–581. [Google Scholar] [CrossRef] [PubMed]
- Browning, J.D.; Baxter, J.; Satapati, S.; Burgess, S.C. The effect of short-term fasting on liver and skeletal muscle lipid, glucose, and energy metabolism in healthy women and men. J Lipid Res 2012, 53, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Antoni, R.; Johnston, K.L.; Collins, A.L.; Robertson, M.D. Intermittent v. continuous energy restriction: differential effects on postprandial glucose and lipid metabolism following matched weight loss in overweight/obese participants. Br J Nutr 2018, 119, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Rothberg, A.E.; Herman, W.H.; Wu, C.; IglayReger, H.B.; Horowitz, J.F.; Burant, C.F.; Galecki, A.T.; Halter, J.B. Weight Loss Improves β-Cell Function in People With Severe Obesity and Impaired Fasting Glucose: A Window of Opportunity. J Clin Endocrinol Metab 2020, 105, e1621–1630. [Google Scholar] [CrossRef]
- Kahn, S.E.; Prigeon, R.L.; Schwartz, R.S.; Fujimoto, W.Y.; Knopp, R.H.; Brunzell, J.D.; Porte, D., Jr. Obesity, body fat distribution, insulin sensitivity and Islet beta-cell function as explanations for metabolic diversity. J Nutr 2001, 131, 354s–360s. [Google Scholar] [CrossRef]
- Pinto, F.C.S.; Silva, A.A.M.; Souza, S.L. Repercussions of intermittent fasting on the intestinal microbiota community and body composition: a systematic review. Nutr Rev 2022, 80, 613–628. [Google Scholar] [CrossRef]
- Gao, Y.; Tsintzas, K.; Macdonald, I.A.; Cordon, S.M.; Taylor, M.A. Effects of intermittent (5:2) or continuous energy restriction on basal and postprandial metabolism: a randomised study in normal-weight, young participants. Eur J Clin Nutr 2022, 76, 65–73. [Google Scholar] [CrossRef]
- Schroor, M.M.; Joris, P.J.; Plat, J.; Mensink, R.P. Effects of Intermittent Energy Restriction Compared with Those of Continuous Energy Restriction on Body Composition and Cardiometabolic Risk Markers - A Systematic Review and Meta-Analysis of Randomized Controlled Trials in Adults. Adv Nutr 2024, 15, 100130. [Google Scholar] [CrossRef]
- He, S.; Wang, J.; Zhang, J.; Xu, J. Intermittent Versus Continuous Energy Restriction for Weight Loss and Metabolic Improvement: A Meta-Analysis and Systematic Review. Obesity (Silver Spring) 2021, 29, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Dote-Montero, M.; Sanchez-Delgado, G.; Ravussin, E. Effects of Intermittent Fasting on Cardiometabolic Health: An Energy Metabolism Perspective. Nutrients 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Webber, J.; Macdonald, I.A. The cardiovascular, metabolic and hormonal changes accompanying acute starvation in men and women. Br J Nutr 1994, 71, 437–447. [Google Scholar] [CrossRef]
- de Groot, L.C.; van Es, A.J.; van Raaij, J.M.; Vogt, J.E.; Hautvast, J.G. Adaptation of energy metabolism of overweight women to alternating and continuous low energy intake. Am J Clin Nutr 1989, 50, 1314–1323. [Google Scholar] [CrossRef]
- Harvie, M.; Howell, A.; Vierkant, R.A.; Kumar, N.; Cerhan, J.R.; Kelemen, L.E.; Folsom, A.R.; Sellers, T.A. Association of gain and loss of weight before and after menopause with risk of postmenopausal breast cancer in the Iowa women's health study. Cancer Epidemiol.Biomarkers Prev. 2005, 14, 656–661. [Google Scholar] [CrossRef] [PubMed]
- Eliassen, A.H.; Colditz, G.A.; Rosner, B.; Willett, W.C.; Hankinson, S.E. Adult weight change and risk of postmenopausal breast cancer. JAMA 2006, 296, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Rosner, B.; Eliassen, A.H.; Toriola, A.T.; Hankinson, S.E.; Willett, W.C.; Natarajan, L.; Colditz, G.A. Short-term weight gain and breast cancer risk by hormone receptor classification among pre- and postmenopausal women. Breast Cancer Res.Treat. 2015, 150, 643–653. [Google Scholar] [CrossRef]
- Rinaldi, R.; De Nucci, S.; Donghia, R.; Donvito, R.; Cerabino, N.; Di Chito, M.; Penza, A.; Mongelli, F.P.; Shahini, E.; Zappimbulso, M. , et al. Gender Differences in Liver Steatosis and Fibrosis in Overweight and Obese Patients with Metabolic Dysfunction-Associated Steatotic Liver Disease before and after 8 Weeks of Very Low-Calorie Ketogenic Diet. Nutrients 2024, 16. [Google Scholar] [CrossRef]
- Bosch de Basea, L.; Boguñà, M.; Sánchez, A.; Esteve, M.; Grasa, M.; Romero, M.D.M. Sex-Dependent Metabolic Effects in Diet-Induced Obese Rats following Intermittent Fasting Compared with Continuous Food Restriction. Nutrients 2024, 16. [Google Scholar] [CrossRef]
- Nassir, F.; Rector, R.S.; Hammoud, G.M.; Ibdah, J.A. Pathogenesis and Prevention of Hepatic Steatosis. Gastroenterol Hepatol (N Y) 2015, 11, 167–175. [Google Scholar] [PubMed]
- Singh, R.G.; Yoon, H.D.; Wu, L.M.; Lu, J.; Plank, L.D.; Petrov, M.S. Ectopic fat accumulation in the pancreas and its clinical relevance: A systematic review, meta-analysis, and meta-regression. Metabolism 2017, 69, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.Y.; Tian, F.; Qian, X.L.; Ying, H.M.; Zhou, Z.F. Effect of 5:2 intermittent fasting diet versus daily calorie restriction eating on metabolic-associated fatty liver disease-a randomized controlled trial. Front Nutr 2024, 11, 1439473. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Characteristics of those completing the study and included in the analysis are reported in.
Figure 1.
Characteristics of those completing the study and included in the analysis are reported in.

Figure 2.
Waterfall plot of percentage change in study participants.
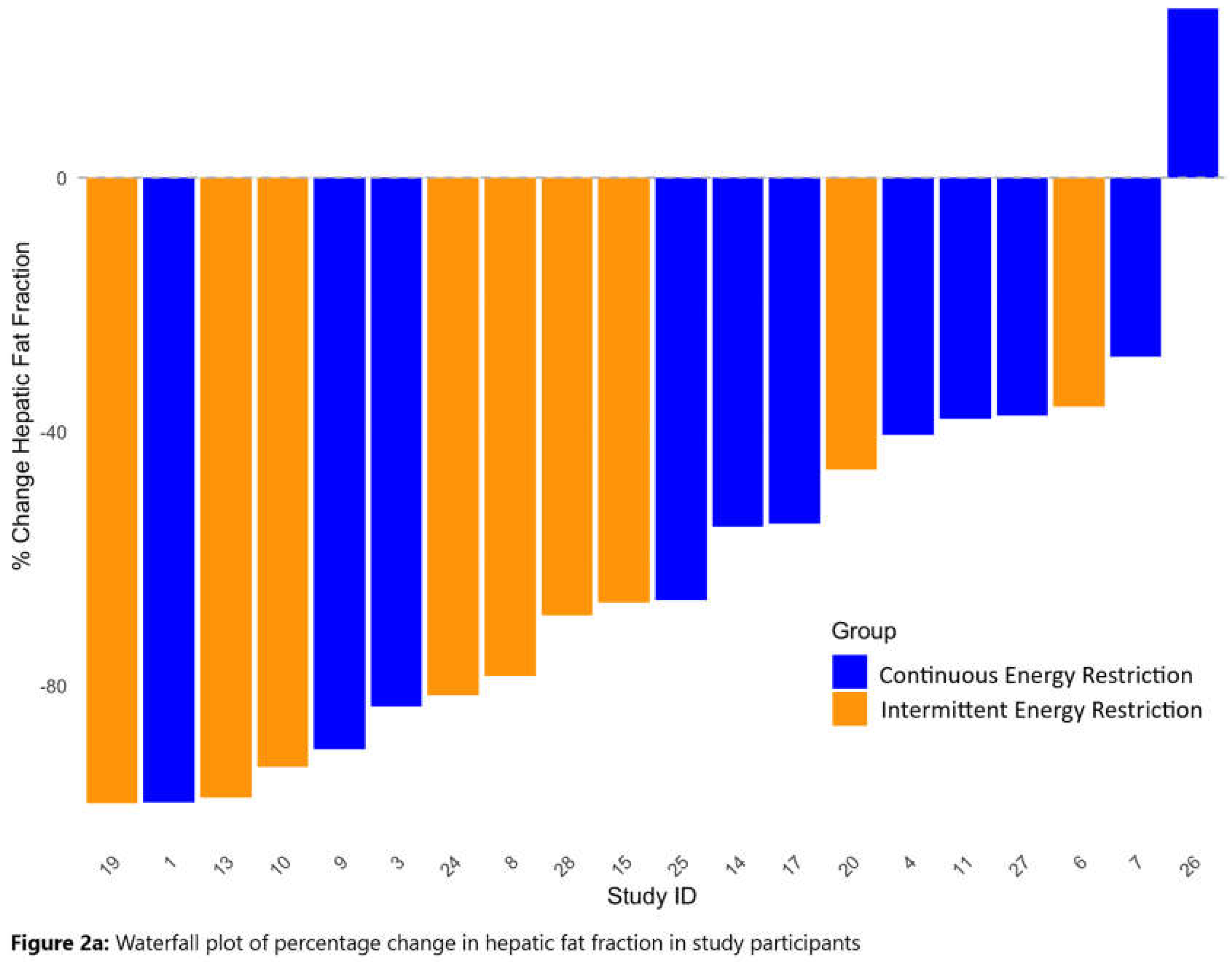
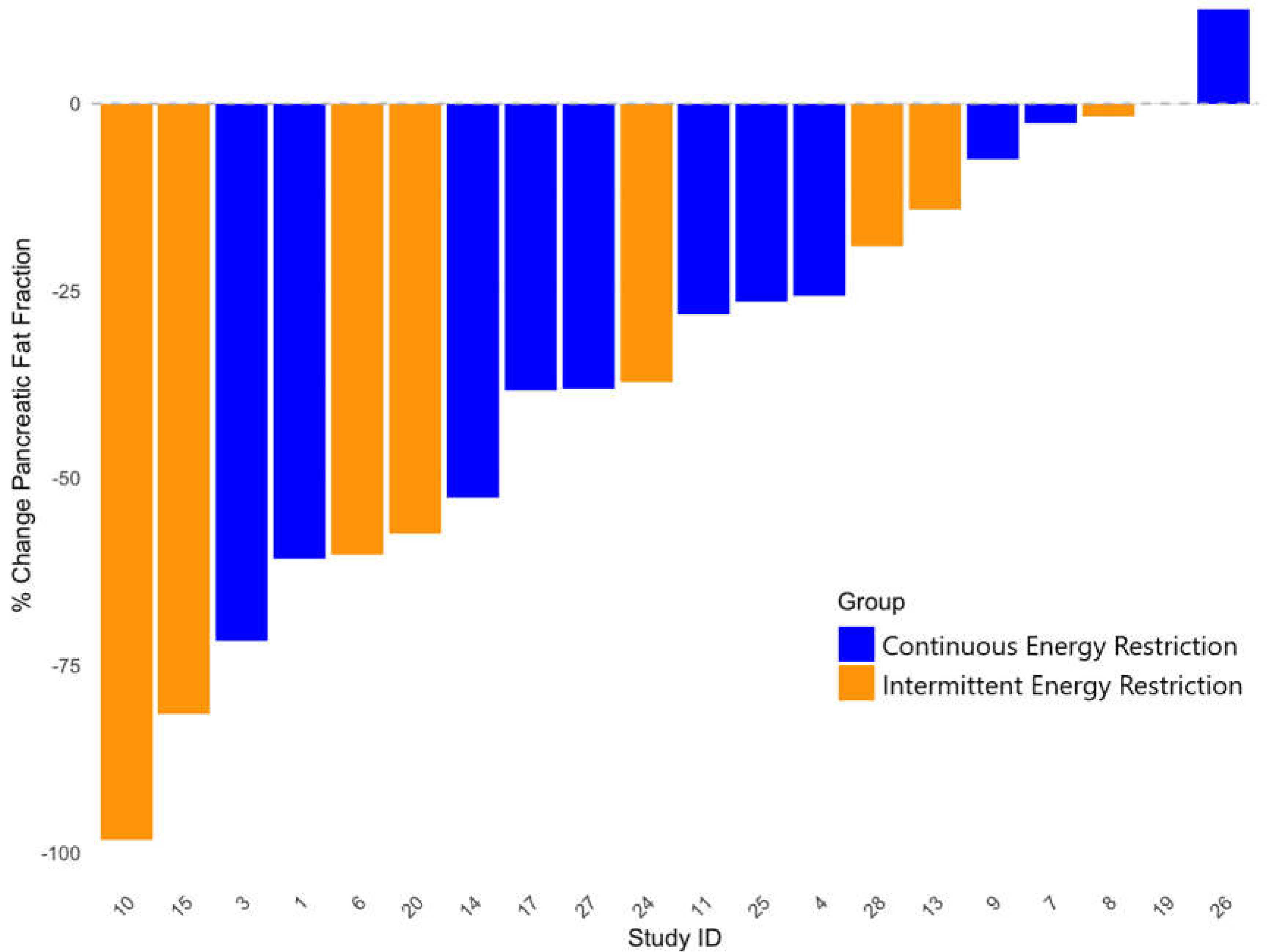

Table 1.
Baseline characteristics of the participants completing the study.
| IER | CER | |
|---|---|---|
| N = 9 | N = 11 | |
| Age (years) | 38.9 (6.1) (25 - 45) | 42.2 (5.7) (31 - 45) |
| BMI (kg/m2) | 34.0 (2.6) (31.0 - 38.3) | 35.5 (4.4) (29.8 - 43.4) |
| Increased risk of breast cancer *Population risk n (%) | 5 (55%) 4 (45%) | 8 (73%)3 (27%) |
| Ethnicity n (%)White British/ White otherBlack African | 9 (100%)0 (0%) | 10 (91%)1 (9%) |
| Deprivation score **1 (most deprived)2345 (least deprived) | 0 (0%)6 (43%)2 (14%)2(14%4 (29%) | 2(14%)2(14%)1 (7%)3 (21%)10 (43%) |
| Body fat-% | 41.4 (3.9) (35.2 - 48.1) | 43.2 (3.7) (34.9 - 47.6) |
| Body fat - kg | 38.5 (5.8) (32.0 - 48.0) | 42.4(9.8) (26.3 - 60.5) |
| Fat free mass - kg | 54.2 (5.7) (44.2 - 62.6) | 54.7 (5.5) (49.0 - 66.6) |
| Waist circumference - cm | 113.1 (6.6) (102.0 - 124.0) | 114.4 (13.2) (91.3 – 132.0) |
| Hip circumference - cm | 117.3 (6.9) (110.1 – 129.3) | 122.1 (9.8) (111.3 - 139.2) |
| Hepatic fat fraction- % | 3.27 (3.30) (0.42 - 9.00) | 5.16 (3.94) (0.15 - 11.78) |
| Pancreatic fat fraction- % | 4.15 (2.96) (0.04 - 9.82) | 5.50 (6.35) (0.21 - 22.3) |
| Calf fat fraction % | 6.37 (2.41) (3.71 - 9.59) | 7.26 (2.01) (5.34 - 11.84) |
| Fasting glucose - mmol / L | 5.1 (0.3) (4.6 - 5.7) | 4.8 (0.3) (4.5 - 5.3) |
| 2 hour glucose mmol/L | 5.7 (1.3) (3.6 - 7.6) | 6.3 (1.6) (4.7 - 9.2) |
| Fasting insulin - mmol / L | 93.5 (26.1) (65 - 155) | 92.6 (32.5) (49 - 139) |
| Fasting C peptide ng / ml | 3.4 (0.8) (2.7 - 4.6) | 3.3 (0.9) (2.2 - 4.6) |
| HOMA1-IR | 1.71 (0.36) (1.3 - 2.6) | 1.77 (0.72) (0.9 - 3.2) |
| HOMA1-%B | 135.3 (23.9) (102.3 -171.2) | 154 (46.5) (107.5 - 267) |
| Total Cholesterol | 5.0 (0.96) (4.0 - 6.6) | 5.4 (0.9) (4.0 - 6.9) |
| LDL cholesterol | 3.2 (0.9)(2.4 - 4.6) | 3.4 (0.7) (2.3 - 4.4) |
| HDL cholesterol | 1.3 (0.2) (1.1 - 1.6) | 1.4 (0.2) (1.1 - 1.7) |
| Triglyceride | 1.0 (0.2) (0.8 - 1.2) | 1.4 (0.7) (0.7 - 2.6) |
| Systolic blood pressure mm hg | 127 (17) (115 - 167) | 127 (11) (109 - 142) |
| Resting energy expenditure - Kj | 6452 (894) (5266 - 7912) | 6464 (849) (5308 - 8008) |
| Mean (SD)(minimum maximum) *Estimated lifetime risk with Tyrer Cuzick model ≥17% ** https://www.gov.uk/government/statistics/english-indices-of-deprivation-2010 | ||
Table 2.
Adiposity and metabolic markers at baseline and week 7 and week 8 for completers (per protocol analysis).
Table 2.
Adiposity and metabolic markers at baseline and week 7 and week 8 for completers (per protocol analysis).
| Variable | Group | N | Baseline | Week 7 | Week 8 |
|---|---|---|---|---|---|
| Weight and body fat measures | |||||
| Body weight-kg | IER | 9 | 92.7 (9.0), 83.9-109.4 | No data | 86.0 (8.9), 78.0-102.5 |
| CER | 11 | 97.1 (15.0), 7.3-127.2 | No data | 90.9 (14.7), 73.7-122.0 | |
| Body fat (kg) | IER | 9 | 38.5 (5.8), 32.0-48.0 | No data | 34.1 (6.2), 26.1-44.2 |
| CER | 11 | 42.4 (9.8), 26.3-60.5 | No data | 38.2 (9.5), 26.6-58.3 | |
| Hepatic fat (%) | IER | 9 | 3.3 (3.3), 0.42-8.97 | 1.2 (1.3), 0.06-3.75 | 1.0 (1.0), 0.01-2.70 |
| CER | 11 | 5.2 (3.9), 0.15-11.78 | 2.7 (2.4), 0.02-7.02 | 2.5 (2.4), 0.015-7.57 | |
| Pancreatic fat (%) | IER | 9 | 4.2 (3.0), 0.04-9.82 | 2.6 (2.3), 0.04-7.68 | 2.1 (2.0), 0.04-6.26 |
| CER | 11 | 5.5 (6.4), 0.21-22.30 | 4.2 (5.3), 0.22-19.20 | 3.9 (4.7), 0.13-16.40 | |
| Calf fat fraction %a | IER | 8 | 6.4 (2.4), 3.71-9.59 | 5.3 (2.3), 2.87-9.77 | 5.6 (2.1), 3.18-8.74 |
| CER | 11 | 7.3 (2.0), 5.34-11.84 | 7.0 (2.0), 4.68-10.24 | 6.9 (1.7), 3.19-9.41 | |
| Fat free mass-kg | IER | 9 | 54.2 (5.7), 44.2-62.6 | No data | 52.0 (5.2), 42.7-60.6 |
| CER | 11 | 54.7 (5.5), 49.0-66.7 | No data | 52.8 (5.4), 46.4-63.8 | |
| Oral glucose tolerance test | |||||
| Fasting HOMA-IRb | IER | 9 | 1.7 (0.4), 1.3-2.6 | 1.2 (0.2), 0.8-1.5 | 1.6 (0.7), 1.0-3.2 |
| CER | 10 | 1.8 (0.7), 0.9-3.2 | 1.3 (0.4), 0.9-2.0 | 1.3 (0.4), 0.8-2.1 | |
| Fasting HOMA-βb | IER | 9 | 135.3 (23.9),102.3-171.2 | 114.1 (21.4),85.2-154.2 | 143.9 (44.1),101.7-216.6 |
| CER | 10 | 157.5 (47.7),107.5-266.8 | 127.6 (25.8),96.0-166.7 | 119.3 (24.3),89.0-166.4 | |
| Fasting insulin b (pmol/l) | IER | 9 | 93.5 (26.1),65.0-155.0 | 63.0 (14.8),42.0-85.0 | 88.5 (35.1),56.7-162.7 |
| CER | 10 | 95.8 (32.4),49.0-139.3 | 74.7 (23.6),46.7-114.3 | 78.8 (45.3),45.0-203.0 | |
| Fasting glucoseb (mmol/l) | IER | 9 | 5.1 (0.4), 4.6-5.7 | 4.9 (0.4), 4.4-5.5 | 4.8 (0.4), 4.4-5.3 |
| CER | 10 | 4.8 (0.3), 4.4-5.3 | 4.8 (0.2), 4.5-5.1 | 4.9 (0.4), 4.5-5.8 | |
| Two hour glucose b (mmol/l) | IER | 9 | 5.7 (1.3), 3.6-7.6 | 5.8 (0.9), 4.9-7.6 | 5.4 (1.8), 2.8-9.3 |
| CER | 10 | 6.5 (1.6), 4.7-9.2 | 5.8 (1.3), 4.0-8.6 | 5.8 (1.6), 4.6-9.9 | |
| Area under the curve OGTT over 180 minutes OGTT | |||||
| Glucose/ mmol/ L b | IER | 8 | 6.2 (0.9), 5.0-7.5 | 6.3 (0.8), 5-7.4 | 6.0 (1.2), 4.4-8.3 |
| CER | 10 | 6.4 (1.1), 5.0-8.3 | 6.1 (1.1), 4.9-8.4 | 6.1 (1.2), 4.6-8.8 | |
| Insulin pmol/ L b | IER | 9 | 360.1 (162.0),191.2-669.2 | 325.6 (128.6),209.1-610.7 | 329.3 (127.0),162.6-585.6 |
| CER | 10 | 451.2 (288.1),147.3-1170.9 | 337.7 (122.0),186.4-515.6 | 316.2 (164.9),158.6-724.2 | |
| C-peptide (ng/ ml) b | IER | 9 | 9.5 (3.0), 5.5-13.8 | 10.0 (2.3), 6.6-12.7 | 8.9 (2.1), 4.9-11.6 |
| CER | 10 | 9.6 (3.1), 6.0-16.5 | 9.1 (2.6), 5.8-13.0 | 8.7 (3.1), 5.8-15.3 | |
| Lipids | |||||
| Total cholesterol (mmol/L) b | IER | 9 | 5.0 (1.0), 4.0-6.6 | 4.4 (0.8), 3.6-6.0 | 4.3 (0.7), 3.7-5.9 |
| CER | 10 | 5.3 (0.9), 4.0-6.9 | 4.6 (0.9), 3.2-5.6 | 4.6 (0.7), 3.4-5.3 | |
| Triglyceride (mmol/L) b | IER | 9 | 1.0 (0.2), 0.8-1.2 | 0.8 (0.1), 0.6-0.9 | 0.8 (0.2), 0.6-1.2 |
| CER | 10 | 1.4 (0.7), 0.7-2.6 | 1.1 (0.4), 0.7-1.9 | 1.2 (0.6), 0.6-2.5 | |
| HDL (mmol/L) b | IER | 9 | 1.3 (0.2), 1.1-1.6 | 1.1 (0.2), 0.8-1.5 | 1.1 (0.2), 0.8-1.5 |
| CER | 10 | 1.3 (0.2), 1.1-1.6 | 1.1 (0.1), 1.0-1.2 | 1.1 (0.2), 0.7-1.4 | |
| LDL (mmol/L) b | IER | 9 | 3.2 (0.9), 2.4-4.6 | 2.9 (0.7), 2.3-4.3 | 2.8 (0.6), 2.3-4.1 |
| CER | 10 | 3.3 (0.7), 2.3-4.4 | 3.0 (0.8), 1.8-4.2 | 2.9 (0.6), 2.2-3.7 | |
| TC:HDL ratiob | IER | 9 | 3.8 (0.6), 3.2-5.1 | 3.9 (0.5), 3.4-4.8 | 3.8 (0.4), 3.3-4.6 |
| CER | 10 | 4.0 (0.5), 3.1-4.9 | 4.2 (0.9), 2.9-5.6 | 4.3 (0.8), 2.8-5.1 | |
| Systolic blood pressure | IER | 9 | 127 (17), 114 - 167 | n/a | 114 (11), 98 - 134 |
| CER | 11 | 126 (11), 109 - 142 | n/a | 118 (12), 109 - 142 | |
| Resting metabolic rate - kJ/ day | IER | 9 | 6489 (899) 5297 - 7958 | 6109 (648) 4853 7255 | 5969 (192) 5832 6104 |
| CER | 11 | 6205 (851), 5339 - 8054 | 5972 (108), 5192 - 8862 | 6735 (1166), 5448 - 8062 | |
Mean (SD), minimum and maximum. HDL high density lipoprotein, LDL low density lipoprotein, TC total cholesterol, OGTT oral glucose tolerance test. a 1 of the IER patients with Charcot–Marie–Tooth disease did not have CIFF assessed. b 1 of the IER patients did not have final OGTT or lipid blood tests.
Table 3.
Generalized linear latent and mixed models (GLLAMM) analysis: parameter coefficient (95% CI) for changes in adiposity and metabolic markers in the IER and CER groups between baseline and week 7 and baseline and week 8 adjusted for day of menstrual cycle.
Table 3.
Generalized linear latent and mixed models (GLLAMM) analysis: parameter coefficient (95% CI) for changes in adiposity and metabolic markers in the IER and CER groups between baseline and week 7 and baseline and week 8 adjusted for day of menstrual cycle.
| Variable | Week 7 vs. baseline | Week 8 vs. baseline (95% CI)a | CER vs IER interaction week 7 to baselinea | CER vs IER interaction week 8 to baselinea | ||
|---|---|---|---|---|---|---|
| Body weight (kg) | Not assessed | -6.6(-7.5 to -5.8)P<0.001 | Not assessed | 0.6 (-1.3 to 2.6)P=0.53 | ||
| Body fat (kg) | Not assessed | -4.4 (-5.0 to -3.7)P<0.001 | Not assessed | 0.4 (-1.3 to 2.0)P=0.66 | ||
| Hepatic fat (%) | -2.1(-3.5 to –0.6)P=0.005 | -2.4 (-3.9 to –0.8)P= 0.003 | -0.3 (-2.2 to 1.6)P=0.75 | -0.3 (-2.3 to 1.7)P=0.78 | ||
| Pancreatic fat (%) | -1.5 (-2.8 to -0.2)P=0.020 | -2.1 (-3.7 to -0.5)P = 0.011 | 0.2 (-1.3 to 1.8)P=0.78 | 0.5 (-1.4 to 2.5)P=0.58 | ||
| Calf fat fraction % | -1.1 (-2.2 to -0.03P= 0.044 | -0.8 (-1.8 to 0.2)P=0.11 | 0.9 (-1.1 to 2.2)P = 0.39 | 0.4 (-1.0 to 1.8)P = 0.57 | ||
| Oral Glucose Tolerance Test | ||||||
| Fasting HOMA-IR | -0.5 (-0.7 to -0.4)P <0.001 | -0.09 (-0.6 to 0.4)P = 0.73 | 0.02 (-0.3 to 0.4)P = 0.90 | -0.5 (-1.1 to 0.1)P= 0.14 | ||
| Fasting HOMA-β | -20.7 (-29.0 to 12.4)P<0.001 | 8.5 (-21.4 to 38.5)P=0.58 | -8.6 (-30.9 to 13.6)P= 0.45 | -46.7 (-85.6 to -7.8)P=0.019 | ||
| Fasting insulin (pmol/l) | -30.2 (-42.3 to -18.1)P<0.001 | -5.0 (-32.3 to 22.3)P =0.72 | 9.3 (-8.6 to 27.2)P =0.31 | -12.0 (-50.5 to 26.5)P =0.54 | ||
| ariable | Week 7 vs. baseline | Week 8 vs. baselinea | CER vs IER interaction week 7 to baselinea | CER vs IER interaction week 8 to baselinea | ||
| Fasting glucose (mmol/l) | -0.2 (-0.4 to -0.001)P =0.049 | -0.2 (-0.4 to -0.1)P =0.05 | 0.2 (-0.1 to 0.4)P=0.17 | 0.3 (0.01 to 0.5)P = 0.041 | ||
| Two hour glucose (mmol/l) | 0.009 (-0.8 to 0.8)P =0.98 | -0.4 (-1.9 to 1.2)P =0.66 | -0.7 (-1.7 to 0.2)P =0.12 | -0.3 (-2.2 to 1.6)P =0.75 | ||
| Area under the curve for 180 minute OGTT | ||||||
| Glucose | (-0.3 to 0.5)P = 0.50 | -0.2 (-0.9 to 0.5)P=0.55 | -0.4 (-0.9 to 0.08)P=0.099 | -0.09 (-1.0 to 0.9)P=0.86 | ||
| Insulin | -28.7 (-79.0 to 21.5)P=0.26 | -31.2(-96.2 to 33.9)P=0.35 | -79.4 (-230.6 to 71.7)P =0.30 | -103.6 (-289.9 to 82.7)P= 0.28 | ||
| C-peptide | 0.4 (-0.3 to 1.2)P=0.27 | -0.6 (-2.3 to 1.1)P=0.49 | -1.0 (-2.4 to 0.4)P=0.16 | -0.3 (-2.6 to 2.0)P=0.80 | ||
| Total cholesterol (mmol/L) | -0.5 (-1.0 to -0.03)P=0.038 | -0.7 (-1.2 to -0.2)P=0.007 | -0.1 (-0.8 to 0.6)P=0.73 | 0.06 (-0.7 to 0.6)P = 0.85 | ||
| Triglyceride (mmol/L) | -0.2 (-0.3 to 0.003)P=0.046 | -0.2 (-0.3 to -0.2)P<0.001 | -0.1 (-0.4 to 0.2)P=0.57 | 0.006 (-0.3 to 0.3)P=0.97 | ||
| HDL (mmol/L) | -0.2 (-0.3 to -0.08)P=0.001 | -0.2 (-0.3 to -0.05)P=0.008 | -0.05 (-0.2 to 0.09)P=0.48 | -0.06 (-0.3 to 0.1)P=0.55 | ||
| LDL (mmol/L) | -0.3 (-0.7 to 0.1)P=0.20 | -0.4 (-0.8 to -0.001)P=0.49 | -0.01 (-0.5 to 0.5)P=0.97 | -0.03 (-0.5 to 0.4)P=0.91 | ||
| Fat free mass | -2.3 (-3.0 to -1.6)P<0.001 | 0.3 (-0.8 to 1.4)P = 0.57 | ||||
| RMR (kJ/day) | No data | -423 (-774 to -64)P= 0.021 | No data | -141 (-748 to 465)P = 0.65 | ||
| % of predicted RMR estimated with the Mifflin equation | No data | -2.2(-7.3 to 2.9)P= 0.39 | No data | -3.0 (-11.7 to 5.8)P=0.51 | ||
A = Parameter coefficient (95% CI).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



