4. Discussion
Optimal chemoradiotherapy approaches, the appropriate timing for response evaluation of LARC after nCRT, the ideal timing for surgery, and the criteria for selecting the best candidates for delaying surgery with intensive follow-up (“watch and wait approach”), remain unclear. In our previous studies, we explored potential predictors of response to nCRT based on clinical, radiological, and molecular [
16,
17,
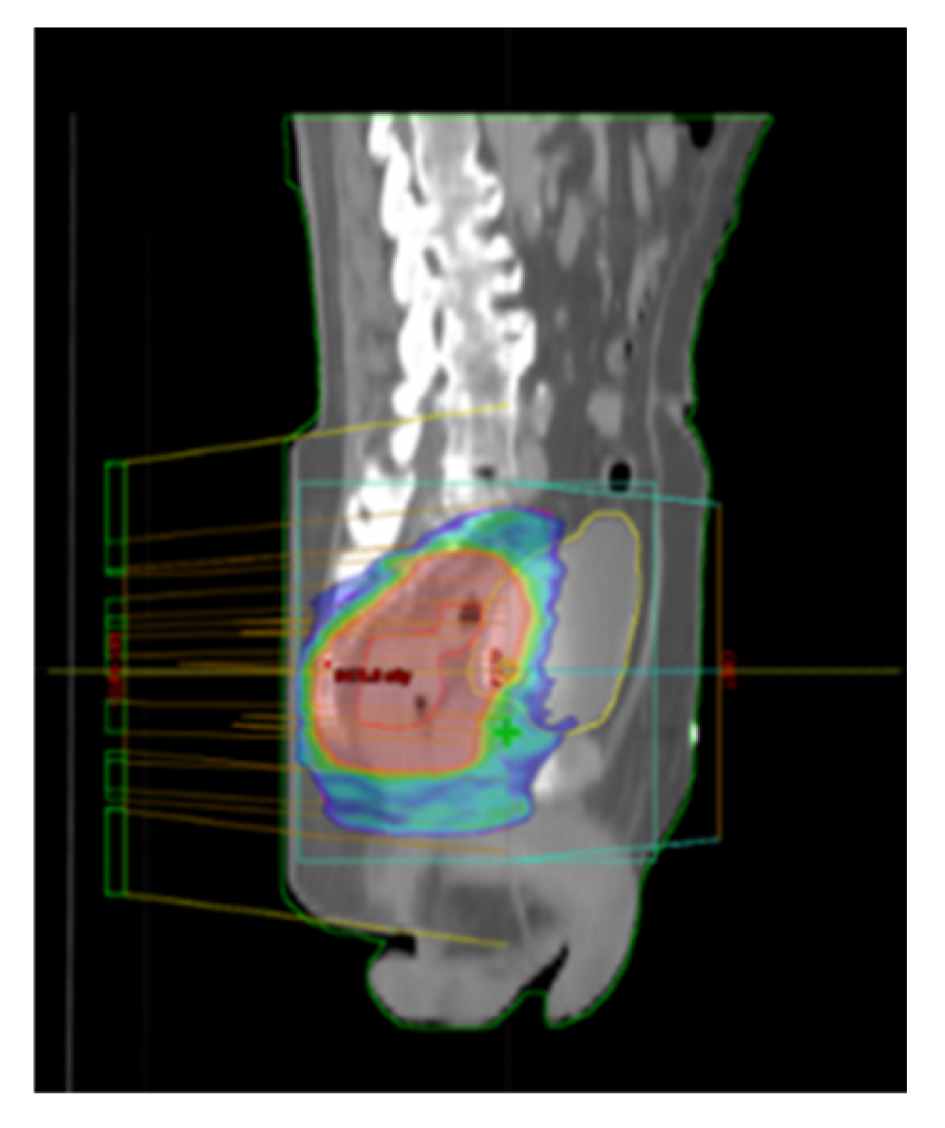
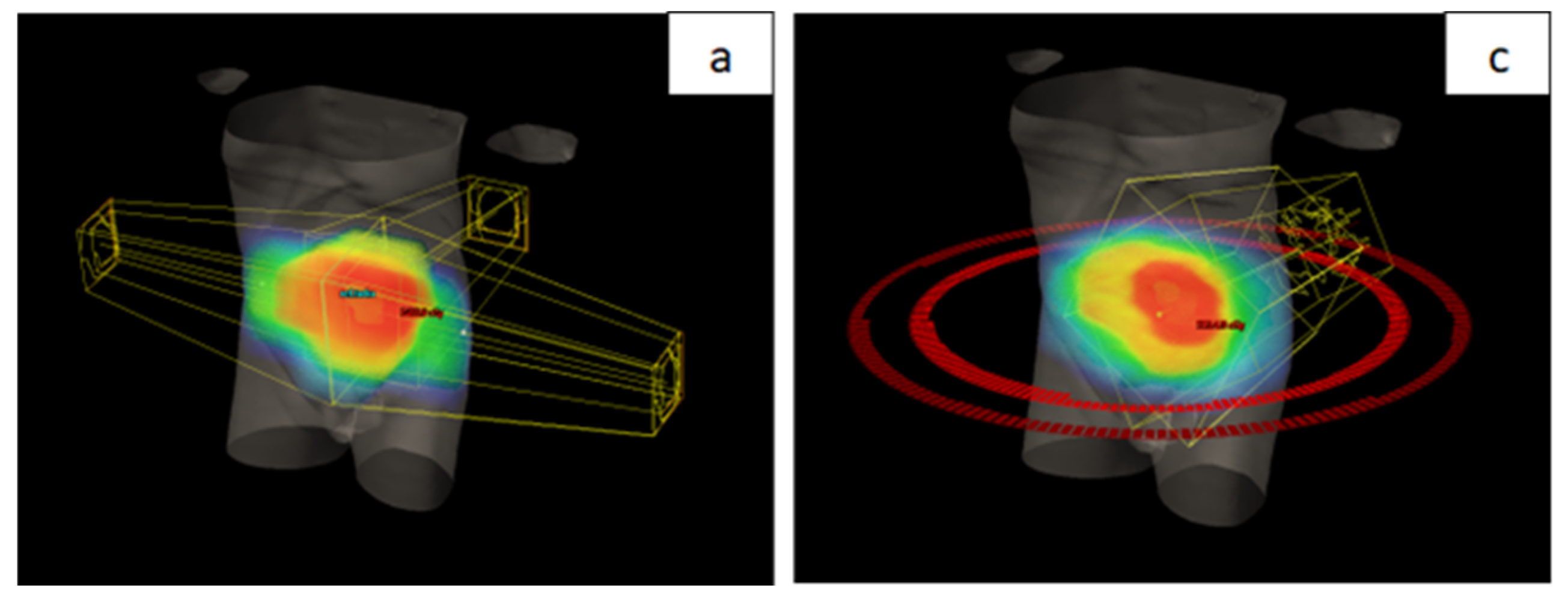
18] The aim of our study was to compare a group of patients treated with a new radiation therapy technique and a group treated with standard CRT as part of neoadjuvant treatment for LARC, with the goal of evaluating the benefits of dose escalation using a SIB technique. In the standard treatment group, RT involved a sequential boost to the area of macroscopic disease, achieving a total dose of 50.4 Gy in 28 fractions using 3D CRT technique. In contrast, the new technique employed VMAT with SIB to the area of macroscopic disease, delivering a total dose of 54 Gy in 25 fractions. It is important to note that both groups received the same CT regimen. Before analyzing differences in toxicity and treatment outcomes, a comparison of the two groups was conducted based on their demographic and disease characteristics. As no significant differences were observed, comparability between the groups was ensured.
Our results showed a significantly higher number of non-hematological toxicities in the group of patients treated with the new radiation therapy technique. However, when toxicities were classified as low-grade (Grade 1 and 2) or high-grade (Grade 3), no significant differences were observed between the groups. Despite the use of the VMAT technique, known for its superior conformality and ability to spare surrounding organs at risk (OAR), toxicity rates were similar between the two groups of patients. This unexpected outcome may be attributed to several factors. First, the higher dose per fraction (2.16 Gy) and the greater total RT dose (54 Gy vs. 50.4 Gy) in the group of patients treated with the new technique could have offset the benefits of the more conformal approach regarding toxicity rates. Additionally, the prospective nature of the group treated with the new technique and stricter assessment of low-grade toxicities may have revealed adverse effects that were not documented in the group treated with the standard approach.
In a study conducted by Bae et al., comparing the use of a boost dose delivered sequentially with the 3D conformal technique and simultaneously with the IMRT technique, a significantly lower rate of urinary toxicity was observed in the IMRT-SIB group (patients with no toxicity or Grade 1 toxicity were compared to those with Grade 3 toxicity). However, no significant differences were found in other parameters [
19]. The difference compared to our study lies in the absence of an increased RT dose in the IMRT-SIB group, enabling a comparison of techniques without the confounding effect of the total RT dose.
Previous studies aiming to determine gastrointestinal toxicity rates also did not report reduced toxicity with the use of newer RT planning techniques. Gastrointestinal toxicity was observed in 52.5% of patients, which aligns with the findings of our study [
20]. In a study comparing conventional and VMAT-SIB techniques with a RT dose of 45 Gy and a boost to a total dose of 55 Gy, Grade 2 urinary toxicity was reported in 49% of patients, while Grade 2 diarrhea was reported in 42% of patients [
12]. Similar toxicity results were observed in a study conducted by Yang et al., which utilized the VMAT-SIB technique (50 Gy / 58.75 Gy in 25 fractions). Most patients experienced some form of acute toxicity, with a high-grade toxicity rate (Grade 3) of 7.7% [
8].
Further investigation into specific types of toxicities in our study revealed significant differences in urinary system toxicities, with a higher incidence of dysuria and frequent urination observed in the group of patients treated with the new RT technique. The predominant localization of tumors in the distal rectum in this group was associated with higher doses delivered to the urethra due to its close proximity to the mesorectum in this region.
Analysis of toxicity onset during treatment showed significantly earlier occurrence in the group of patients treated with the new RT technique. This difference may be attributed to the higher dose per fraction (2.16 Gy) delivered to the macroscopic tumor area. Notably, this analysis was not part of the data reported in the literature, making our findings a valuable contribution to understanding the timing of toxicity onset. These insights allow for the timely implementation of supportive measures to minimize adverse reactions.
Among the operated patients, sphincter-preserving surgery was achieved in 49 out of 63 patients, representing a higher percentage in the group treated with the new RT technique (77.8%) compared to 35 out of 56 patients in the standard approach (62.5%). However, statistical significance was not achieved. The lack of statistical significance could be attributed to the higher proportion of distally located tumors in the group treated with the new RT technique. Importantly, in 12 patients with distal tumor localization, achieving a cCR allowed for a non-operative management approach, resulting in sphincter preservation. Our findings align with existing literature, where a study utilizing the VMAT-SIB technique (45 Gy/55 Gy) reported a sphincter preservation rate of 88%. However, that study had a higher initial prevalence of stage II disease (42%) compared to our study [
12].
Comparison of the two patient groups revealed a statistically significant lower incidence of PNI in postoperative specimens from patients treated with the new RT technique (p < 0.01). This finding is important given the well-established negative prognostic impact of PNI in colorectal cancer. A meta-analysis of 58 studies involving 22,900 colorectal cancer patients demonstrated that PNI is associated with worse five-year overall survival (OS) (relative risk [RR], 2.09; 95% confidence interval, 1.68–2.61) and DFS (RR, 2.35; 95% CI, 1.66–3.31) [
21].
Analysis of definitive postoperative staging showed significantly higher rates of lower T categories (T0-2), negative nodal status (N0), and earlier stages (I+II) in the group treated with the new RT technique. Literature comparisons suggest that a change in RT technique alone, without dose escalation, does not result in significant improvements in these parameters [
19]. The observed improvements in our study likely reflect the combined effect of VMAT-SIB and increased RT dose.
Literature data indicate that pCR is associated with improved outcomes, regardless of initial clinical T and N categories, highlighting its importance in assessing LARC response to nCRT [
22]. In our study, among operated patients, pCR was achieved in 13 out of 63 patients (20.6%) treated with the new RT technique, compared to 5 out of 56 patients (8.9%) treated with the standard approach, showing a positive trend without statistical significance (p = 0.06). The lack of significance may be attributed to the 16% of patients in the new technique group who, due to cCR, did not undergo surgery. A study of 385 LARC patients treated with nCRT (50.4 Gy) followed by surgery after six weeks reported a pCR rate of 10.4% [
23]. Similarly, a study employing the VMAT-SIB technique with dose escalation, like ours, observed a pCR rate of 17% [
12], demonstrating the comparability of our results with the literature.
Tumor regression grade (TRG) is an important prognostic factor for assessing the risk of local recurrence, DFS, and OS in patients with LARC [
24]. When comparing individual TRG statuses, significantly better treatment responses were noted in the group treated with the new RT technique. For RCRG classification, statistical significance was observed both for individual categories and when comparing patients with favorable (RCRG1) versus poor responses (RCRG2-3). The divergence between classifications arises from the lack of standardized response alignment in the literature. Extended follow-up will help determine which classification has greater prognostic value in our patient cohort. Research indicates that ypN status and TRG status are independent predictors of OS and recurrence-free survival (RFS). A large study of 237 LARC patients treated with nCRT highlighted the importance of these predictors [
25]. In our comparison of two groups, a statistically significant lower percentage of N-negative cases was observed in the group treated with the new RT technique. Understanding the prognostic value of N status after neoadjuvant treatment can support an individualized approach to intensifying adjuvant chemotherapy in high-risk patient groups.
Guidelines recommend examining at least 12 lymph nodes for accurate staging of rectal cancer [
26]. However, when treatment begins with nCRT, achieving this benchmark can be challenging, as neoadjuvant therapy often reduces both the size and number of lymph nodes in the treated area. Our findings align with the literature, where intensified neoadjuvant treatment in the group treated with the new RT technique was associated with a statistically significant reduction in the number of isolated lymph nodes. A study comparing outcomes based on lymph node evaluation (fewer than 12 vs. 12 or more examined) found a higher percentage of pCR in patients with fewer than 12 isolated lymph nodes [
27]. The exact number of lymph nodes needed for staging in nCRT-treated patients remains undefined. Additional studies show that the number of isolated lymph nodes can vary with factors such as gender, age, initial disease stage, and the presence of LVI. Interestingly, a smaller number of isolated lymph nodes is often associated with better tumor response and improved prognosis [
28].
Data from the literature indicate that response to neoadjuvant therapy strongly correlates with long-term treatment outcomes. Following neoadjuvant treatment, disease downstaging is achieved in 50–60% of patients, while approximately 20% achieve pCR [
29,
30]. Unlike most studies that evaluate the pathological response to neoadjuvant treatment independently of ypTN staging, some approaches emphasize incorporating disease stage into the assessment. It has been demonstrated that the prognostic value of response is particularly significant in patients with ypIII disease. In this group, those with a good response to nCRT and a ypIII stage show survival rates comparable to those with ypII disease (five-year OS: 67% vs. 74%, p = 0.89). Conversely, in patients with a poor pathological response within the ypIII stage, survival outcomes resemble those of patients with stage IV disease (five-year OS: 27% vs. 18%, p = 0.09) [
31].
The study has certain limitations. The sample size is relatively small but meets the minimum criteria for patients with LARC, considering its prevalence and the population size in Serbia (95% confidence level) [
32]. In comparing the approach involving dose escalation with SIB using the VMAT technique against the standard treatment group, limitations include the retrospective nature of the comparator group, leading to incomplete data on toxicity and treatment outcomes. Additionally, the study's single-institution design may limit the generalizability of the findings. Other limitations may include potential selection bias due to the retrospective analysis and the lack of long-term follow-up data, which would provide a more comprehensive understanding of survival and recurrence outcomes. Future multi-institutional, prospective studies with larger sample sizes are warranted to confirm these findings and further validate the results.