
Submitted:
01 February 2025
Posted:
03 February 2025
You are already at the latest version
Abstract
Introduction: Oral frailty, defined as an age-related decline in oral function, represents a significant risk factor for adverse health outcomes, though it can be mitigated through early intervention. The Oral Frailty Five-item Checklist (OF-5), introduced in 2023, assesses oral frailty using five indicators: reduced number of teeth, difficulty chewing, difficulty swallowing, dry mouth, and low articulatory oral motor skills. Designed for use beyond dental clinics, the OF-5 has demonstrated predictive validity for physical frailty and mortality. Similarly, the Oral Frailty Index-8 (OFI-8) comprises eight items evaluating oral health, social participation, and dental habits. Methods: This study compared the OF-5 and OFI-8 tools and investigated their associations with physical and biological markers. A cross-sectional analysis was conducted on 270 Japanese participants aged ≥ 65 years (mean age: 77.6 ± 7.3 years). The assessments included blood tests, physical measurements, and grip strength evaluation. Participants were categorized by sex and oral frailty risk based on OF-5 scores (non-frailty: ≤ 1; frailty: ≥ 2). Results: Oral frailty, defined as an OF-5 score ≥ 2, was observed in 40.7% of the participants (33.8% in men and 47.4% in women). Both the OF-5 and OFI-8 scores were higher in women than in men. Sex-specific differences in physical and biological markers were evident; men exhibited higher grip strength, whereas women had a higher prevalence of anemia and osteoporosis. Women were also more likely to report reduced masticatory ability and lower levels of social participation. A high concordance rate of over 80% was observed between oral frailty (OF-5 score ≥ 2) and high-risk oral frailty (OFI-8 score ≥ 4). Conclusions: These findings highlight the utility of subjective questionnaires in assessing oral frailty and emphasize the need for longitudinal studies to evaluate their predictive accuracy for physical frailty.
Keywords:
Oral Frailty
; Frailty
; Oral Frailty Five-item Checklist (OF-5)
; Oral Frailty Index-8 (OFI-8)
Introduction
“Oral frailty,” first proposed by the Japanese Geriatrics Society in 2014, is defined as an age-related decline in oral function. It is characterized by an overlap of minor reductions in dental and oral capabilities that may increase the risk of adverse health outcomes [1]. Although oral frailty elevates the risk of further deterioration, it remains reversible with timely and appropriate interventions.
In 2023, the oral frailty five-item checklist (OF-5) was introduced as a new diagnostic criterion for oral frailty. The OF-5 includes five components: fewer teeth, chewing difficulty, swallowing difficulty, dry mouth, and low articulatory oral motor skills [2].
The original OF-5 study evaluated chewing difficulty, swallowing difficulty, and dry mouth using subjective questionnaires, whereas objective assessments were employed for tooth count and articulatory oral motor skills. It is reported that the concordance between subjective and objective evaluations was high.[3] A joint statement released in 2024 by the Japanese Geriatrics Society, Japanese Geriatric Dentistry Society, and Japanese Society for Sarcopenia and Frailty suggested replacing the objective assessment of articulatory oral motor skills with the self-reported question, “Have you had difficulty with clear pronunciation recently?” It also recommended allowing self-reported tooth counts (> 20 teeth) [4]. However, further research is required to determine whether self-reported OF-5 assessments can accurately predict physical frailty outcomes.
Designed for applications beyond dental clinics, the self-reported OF-5 is a versatile tool suitable for use by non-dental healthcare professionals and community members. It has demonstrated strong predictive validity for physical frailty, impairment, and mortality among older adults in Japan [2].
Our recent study involving older adults from the Sasayama-Tamba area of Hyogo Prefecture demonstrated that oral frailty, diagnosed using the OF-5, was associated with systemic frailty and sarcopenia indicators. Additionally, it was correlated with the progression of systemic frailty during follow-up [5]. However, no studies have reported findings from the application of the OF-5 in urban general internal medicine outpatient settings. Moreover, while our previous study employed objective evaluations of tooth count and oral motor skills, no studies have utilized self-reported assessments as proposed in the 2024 statement.
In contrast, the Oral Frailty Checklist/Oral Frailty Index-8 (OFI-8), developed by the Japan Dental Association, comprises eight items: (1) chewing difficulty, (2) swallowing difficulty, (3) denture use, (4) dry mouth, (5) reduced frequency of outings, (6) difficulty chewing hard food, (7) tooth brushing at least twice daily, and (8) regular dental visits. Items (1)–(3) are scored as two points each, whereas the remaining items are scored as one point each, with a maximum score of 11. Scores are categorized as low risk (0–2 points), moderate risk (3 points), or high risk (> 4 points). The OFI-8 has been independently associated with all-cause mortality, even after adjusting for physical and psychological frailty [6].
In our previous study on the OFI-8, the OFI-8 questionnaire was administered to patients attending a general internal medicine outpatient clinic. The OFI-8 scores were higher in women than in men, suggesting that oral frailty is more prevalent among women. In the high-risk group for oral frailty (OFI-8 score ≥ 4), grip strength was significantly lower in both men and women. Additionally, among men, height, hemoglobin levels, red blood cell count, and serum albumin levels were significantly lower in those with an OFI-8 score ≥ 4 [7].
Although the OF-5 and OFI-8 share common items, such as chewing difficulty, swallowing difficulty, and dry mouth, the OF-5 uniquely incorporates objective evaluations of tooth count and oral motor skills. However, the comparative efficacy of the OF-5 and OFI-8 in predicting physical frailty remains underexplored.
The objectives of this study were as follows:
1. To quantify the number of individuals meeting the criteria for each item in the OF-5 and OFI-8, stratified by sex.
2. To calculate the prevalence of oral frailty or high oral frailty risk as determined by each method.
3. To evaluate the concordance rate between the two assessment methods.
4. To explore the characteristics of each assessment tool.
Additionally, this study aimed to assess sex differences in physical and blood markers among individuals classified as having oral frailty using the OF-5. Using the OF-5, the study also investigated whether individuals with suspected oral frailty (OF-5 score ≥ 2) exhibited differences in physical and biological markers, including height, weight, blood indices, and grip strength, compared with those with lower OF-5 scores.
Materials and Methods
This was a cross-sectional study. All patients aged ≥ 65 years who were enrolled in this study were Japanese and provided informed consent. A total of 270 patients were enrolled, with a mean age of 77.6±7.3 years. The cohort included 133 men (mean age, 77.0±7.5 years) and 137 women (mean age, 78.3±7.1 years) who were admitted to the Osaka Dental University and the National Cerebral and Cardiovascular Center between February 2024 and September 2024.
Blood tests, physical measurements (height and weight), grip strength measurements, and OF-5 and OFI-8 questionnaires were administered to all participants. Five internal medicine outpatient physicians performed oral assessments using the questionnaire. The results of the questionnaire were tabulated, and the participants were divided into two groups by sex: the oral non-frailty group (OF-5 score ≤ 1) and the oral frailty group (OF-5 score ≥ 2). The differences in blood parameters, physical parameters, and grip strength were analyzed between the groups. The maximum grip strength was measured using a grip strength tester (GRIP-A; Takei Ltd., Niigata, Japan) [7].
The study protocol was approved by the Ethics Committees of Osaka Dental University and National Cerebral and Cardiovascular Center. All procedures involving human participants were performed in accordance with the ethical standards of the institutional and/or national research committee where the studies were conducted (IRB approval number 111351 at Osaka Dental University) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The requirement for written informed consent was waived, as participants were given the opportunity to opt out due to the retrospective nature of the study.
Questionnaires
The OF-5 and OFI-8 were used in this study. The following 10 questions were asked to all participants, including three common questions shared by the OF-5 and OF-8.
OF-5 specific questions
| OF-5 specific questions |
|
| |
| Questions common to OF-5 and OFI-8 |
|
| |
| |
| OFI-8 specific questions |
|
| |
| |
| |
|
For the OF-5 evaluation, the OF-5 score was determined by the number of applicable items from questions ① through ⑤. Based on the questionnaire results, participants were classified by sex into two groups: the oral non-frailty group (scores ≤ 1) and the oral frailty group (scores ≥ 2). These classifications were then used for further analysis.
For the OFI-8 evaluation, the standard scoring protocol was applied. Participants received two points for each “yes” response to Items ③, ④, or ⑥. For Items ⑤, ⑦, and ⑨, one point was given for each “yes” response. For Items ⑧ or ⑩, one point was given for each “no” response. The maximum possible score was 11. The screening criterion was defined as the sum of the OFI-8 scores. The higher the OFI-8 score, the higher the risk of oral frailty; that is, 0–2 points indicated a low risk, 3 points indicated a moderate risk, and > 4 points indicated a high risk. In this study, participants were categorized by sex, OFI-8 score ≤ 3 (low-to moderate-risk group), and OFI-8 score ≥ 4 (high-risk group). The characteristics of each group were examined. Additionally, the number of applicable items for each question on the OFI-8 and OF-5 was analyzed.
Statistical Analysis
The results are expressed as the mean ± standard deviation (SD) or percentage. Student’s t-test was used for intergroup comparisons. Categorical variables are expressed as absolute (n) and relative frequency (%) and were analyzed using Fisher’s exact test. Statistical significance was set at p < 0.05.
Results
Participant Characteristics and Findings
Male participants were significantly taller, heavier, and exhibited greater grip strength than female participants (all p < 0.001). Hemoglobin levels and hematocrit values were higher in men (p < 0.001), while women exhibited lower hemoglobin and red blood cell counts. Creatinine levels were higher in men than in women, likely reflecting a greater muscle mass. Malignancies were more common in men (p = 0.005), whereas osteoporosis was more prevalent in women (p = 0.035). (Table 1)
Oral Frailty and Functional Differences
The overall prevalence of oral frailty, defined as an OF-5 score of ≥ 2, was 40.7%. The prevalence was significantly higher in women than in men (47.4% vs. 33.8%, p = 0.016). Women were also more likely to report reduced masticatory ability, self-reported difficulty in eating hard foods (p = 0.054), and a decreased frequency of going out (p = 0.015). Additionally, the proportion of individuals with < 20 natural teeth was significantly higher among women (p = 0.020). (Table 1)
OF-5 and OFI-8 Scoring Analysis
The distribution of OF-5 scores differed by sex, with men most frequently scoring 1 and women most frequently scoring 2. Scores of ≥ 3 were rare in both sexes. The overall mean OF-5 score was 1.3 (1.2 for men and 1.5 for women), with women showing significantly higher scores. Similarly, for the OFI-8, female participants exhibited higher overall scores (mean: 3.7 vs. 3.0, p = 0.012). These results suggest that oral frailty is more prevalent in women. For the OFI-8, male scores were concentrated between 2 and 4 points, whereas female scores showed a wider range. The distribution of OFI-8 approached normality, in contrast to that of OF-5. The maximum score for the OFI-8 was 11, whereas the maximum score for the OF-5 was 5 (Figure 1A and B).
The proportions of individuals with an OF-5 score ≥ 2 (defined as OF-5(+)) and an OFI-8 score ≥ 4 (defined as OFI-8(+)) within the overall sample, separated by sex, are shown in Figure 2 using a Venn diagram. Among the 45 men diagnosed as OF-5(+), 38 were also diagnosed as OFI-8(+), resulting in 84.4% of OF-5(+) men being OFI-8(+). Among the 65 women diagnosed as OF-5(+), 54 were also diagnosed as OFI-8(+), resulting in 83.1% of OF-5(+) women being OFI-8(+). (Figure 2)
Clinical Associations with Oral Frailty
In men, oral frailty (OF-5 ≥ 2) was significantly associated with age (p = 0.021) and, unexpectedly, elevated white blood cell counts. No significant differences were observed in height, weight, grip strength, or other clinical indicators. In women, oral frailty was not significantly associated with age (p = 0.673) (Table 2).
Discussion
In this study, the oral frailty assessment tools OF-5 and OF-8 were simultaneously administered to patients attending general internal medicine outpatient clinics for lifestyle-related diseases and other conditions. The number of respondents who met the criteria for each question was analyzed, and potential differences in physical indicators were examined. This study demonstrated that these questionnaire-based tools can be effectively and efficiently implemented in general internal medicine settings.
Approximately 40% of patients attending general internal medicine outpatient clinics had an OF-5 score ≥ 2. Women were more likely to exhibit reduced masticatory ability and fewer teeth than men, resulting in higher OF-5 scores. The prevalence of oral frailty was similar between men and women, affecting over 40% of the population. The observed 40% prevalence of oral frailty was consistent with several previous studies [2,8,9].
Women had higher rates of tooth loss and oral frailty scores, potentially influenced by age-related changes and postmenopausal effects, such as osteoporosis. Women also reported a lower frequency of going out, potentially indicating the risk of declining mental health and reduced social interactions. Although men generally exhibit better physical function, the progression of oral frailty in men could adversely affect their dietary quality and nutritional intake. Targeted dental care and nutritional guidance for individuals with high OF-5 and OFI-8 scores may help mitigate systemic health risks. Therefore, interventions to preserve bone density and enhance masticatory function are critical in women.
Figure 2 shows the proportions of individuals with an OF-5 score ≥ 2 (defined as OF-5(+)) and an OFI-8 score ≥ 4 (defined as OFI-8(+)) among the overall participants. Based on these results, a cutoff of ≥ 2 points on the OF-5 aligned well with a high-risk classification (≥ 4 points) on the OFI-8, with over 80% concordance. This supports the OF-5 cutoff as a valid marker for diagnosing oral frailty and highlights the utility of an OFI-8 score of ≥ 4 for identifying high-risk individuals.
In our previous epidemiological study, the prevalence of low articulatory oral motor skills, as assessed by dentists using oral diadochokinesis (ODK), was relatively high at 36.0% (43.1% in men and 24.2% in women) [5]. However, in the present study, where low articulatory oral motor skills were evaluated based on subjective responses to a questionnaire, the prevalence was significantly lower at 11.5% overall (15.0% in men and 8.0% in women) compared with the ODK-based assessments. For the other four items of the OF-5, no substantial differences in prevalence rates were observed between participants in the previous epidemiological study and outpatients in the current study. However, regarding low articulatory oral motor skills, subjective evaluation using a questionnaire appears to underestimate articulatory oral motor skills compared with objective assessment using the ODK. On the other hand, regarding the question of whether the number of teeth is ≥ 20, previous epidemiological studies relied on measurements conducted by dentists, whereas this study used self-reported data. However, there were no significant differences in the proportion of respondents who met this criterion. These findings suggest that the self-reported assessments of number of teeth are generally accurate.
In our previous study, a longitudinal analysis revealed that initial OF-5 scores predicted increased physical frailty after 2–3 years, particularly in those with higher baseline scores [5]. The OF-5 was a significant factor for frailty progression in both sexes. A longitudinal study is needed to determine whether the assessment of OF-5 using only a questionnaire can serve as a predictor of worsening physical frailty in the future.
Over 80% of individuals with an OF-5 score ≥ 2 was also categorized as high risk for oral frailty with an OFI-8 score ≥ 4. The OF-5 questionnaire demonstrated ease of use and strong alignment with the OFI-8 for the identification of oral frailty. The OF-5 allows for a simpler evaluation of oral frailty, as it diagnoses oral frailty when two of its five items are met. In contrast, the OF-8 includes a mix of two- and one-point questions, resulting in uneven weighting among the items, which may occasionally complicate the scoring process. Given the high concordance rate between the OF-5 and OF-8, the simpler OF-5 tool may be more suitable for use in busy clinical settings.
In our previous study using the OFI-8, individuals with an OFI-8 score ≥ 4, classified as high risk for oral frailty, exhibited significantly lower grip strength and cystatin C-related indices in both men and women. Additionally, in men, albumin and hemoglobin levels were significantly lower when the OFI-8 score was ≥ 4. Significant associations have been observed between OFI-8 scores and physical as well as blood parameters [7].
In the present analysis, individuals classified as having oral frailty with an OF-5 score ≥ 2 did not show significantly lower values for grip strength, albumin, or hemoglobin in either men or women. Compared to the OF-5, the OFI-8 includes more items, such as those related to social participation and oral hygiene behaviors, which are closely linked to systemic health and daily activities. This broader scope of the OFI-8 may explain its clearer association with physical and blood parameters compared with the OF-5.
This study has several limitations that must be acknowledged. First, as this was a cross-sectional study, a cause-and-effect relationship could not be established. A prospective follow-up study is required to assess causal associations between the OF-5 and other indices. Second, this study did not objectively assess oral function using the seven items specified by the Japanese Society of Gerodontology [10], leaving the precise oral function of individuals with an OF-5 score ≥ 2 or an OFI-8 score ≥ 4 unknown. However, the primary aim of this study was to investigate the prevalence of oral frailty diagnosed using the OF-5 and OFI-8 among patients attending a general internal medicine outpatient clinic, and to determine whether oral function assessed via a questionnaire is associated with objective clinical indicators, without relying on specialized dental skills or equipment. Therefore, we believe that the use of professional dental instruments and techniques was not essential for achieving the objectives of this study.
Conclusion
The progression of oral frailty varies across sex and age groups, highlighting the importance of providing tailored health support. Future studies should explore the relationship between oral function and systemic health risks to develop effective preventive strategies. The strong concordance between the OF-5 and OFI-8 underscores their complementary utility in identifying individuals at risk for oral frailty. These findings emphasize the need for sex-specific approaches to assess and manage oral health risks in clinical practice.
Author Contributions
Conceptualization: H.K., and K.E.; methodology: H.K.; software: H.K., and F.Y.; validation: all authors; formal analysis: H.K., and K.E.; investigation: all authors; resources: H.K., and F.Y.; data curation: H.K., N.K., and K.Y.; writing―original draft preparation: H.K.; writing―review and editing: H.K., and H.S.; visualization: H.K.; supervision: H.S.; project administration: H.K., and H.S.; funding acquisition: none. All authors have read and agreed to the published version of the manuscript.
Sources of Financial Support That Require Acknowledgment
This study was supported by Osaka Dental University. This research received no external funding.
Approval Code Issued by the Institutional Review Board (IRB) and the Name of the Institution(s) that Granted the Approval
IRB approval number 111351 at Osaka Dental University
Acknowledgements
We would like to thank all the medical staff of Osaka Dental University and the National Cerebral and Cardiovascular Center who supported this study. We would like to thank Editage (www.editage.com) for English language editing.
Conflicts of interest
The authors declare no conflict of interest.
References
- Tanaka, T.; Takahashi, K.; Hirano, H.; et al. Oral Frailty as a Risk Factor for Physical Frailty and Mortality in Community-Dwelling Elderly. J Gerontol A Biol Sci Med Sci. 2018, 73, 1661–1667. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Hirano, H.; Ikebe, K.; et al. Oral frailty five-item checklist to predict adverse health outcomes in community-dwelling older adults: A Kashiwa cohort study. Geriatr Gerontol Int. 2023, 23, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, M.; Shirobe, M.; Motokawa, K.; et al. Validation of self-reported articulatory oral motor skill against objectively measured repetitive articulatory rate in community-dwelling older Japanese adults: The Otassha Study. Geriatr Gerontol Int. 2023, 23, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Hirano, H.; Ikebe, K.; et al. Consensus statement on “Oral frailty” from the Japan Geriatrics Society, the Japanese Society of Gerodontology, and the Japanese Association on Sarcopenia and Frailty. Geriatr Gerontol Int. 2024, 24, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Kusunoki, H.; Hasegawa, Y.; Nagasawa, Y.; et al. Oral Frailty and Its Relationship with Physical Frailty in Older Adults: A Longitudinal Study Using the Oral Frailty Five-Item Checklist. Nutrients. 2024, 17, 17. [Google Scholar] [CrossRef]
- Tanaka, T.; Hirano, H.; Ohara, Y.; et al. Oral Frailty Index-8 in the risk assessment of new-onset oral frailty and functional disability among community-dwelling older adults. Arch Gerontol Geriatr. 2021, 94, 104340. [Google Scholar] [CrossRef]
- Kusunoki, H.; Ekawa, K.; Kato, N.; et al. Association between oral frailty and cystatin C-related indices-A questionnaire (OFI-8) study in general internal medicine practice. PLoS One. 2023, 18, e0283803. [Google Scholar] [CrossRef] [PubMed]
- Miyahara, S.; Maeda, K.; Kawamura, K.; et al. Concordance in oral frailty five-item checklist and oral hypofunction: Examining their respective characteristics. Arch Gerontol Geriatr. 2024, 118, 105305. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, M.; Shirobe, M.; Motokawa, K.; et al. Prevalence of oral frailty and its association with dietary variety, social engagement, and physical frailty: Results from the Oral Frailty 5-Item Checklist. Geriatr Gerontol Int. 2024, 24, 371–377. [Google Scholar] [CrossRef]
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; et al. Oral hypofunction in the older population: Position paper of the Japanese Society of Gerodontology in 2016. Gerodontology. 2018, 35, 317–324. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A. Distribution of OF-5 score and their association with OFI-8 in men (Ⅰ) and women (Ⅱ). B. Distribution of OFI-8 score and their association with OF-5 in men (Ⅰ) and women (Ⅱ).
Figure 1.
A. Distribution of OF-5 score and their association with OFI-8 in men (Ⅰ) and women (Ⅱ). B. Distribution of OFI-8 score and their association with OF-5 in men (Ⅰ) and women (Ⅱ).
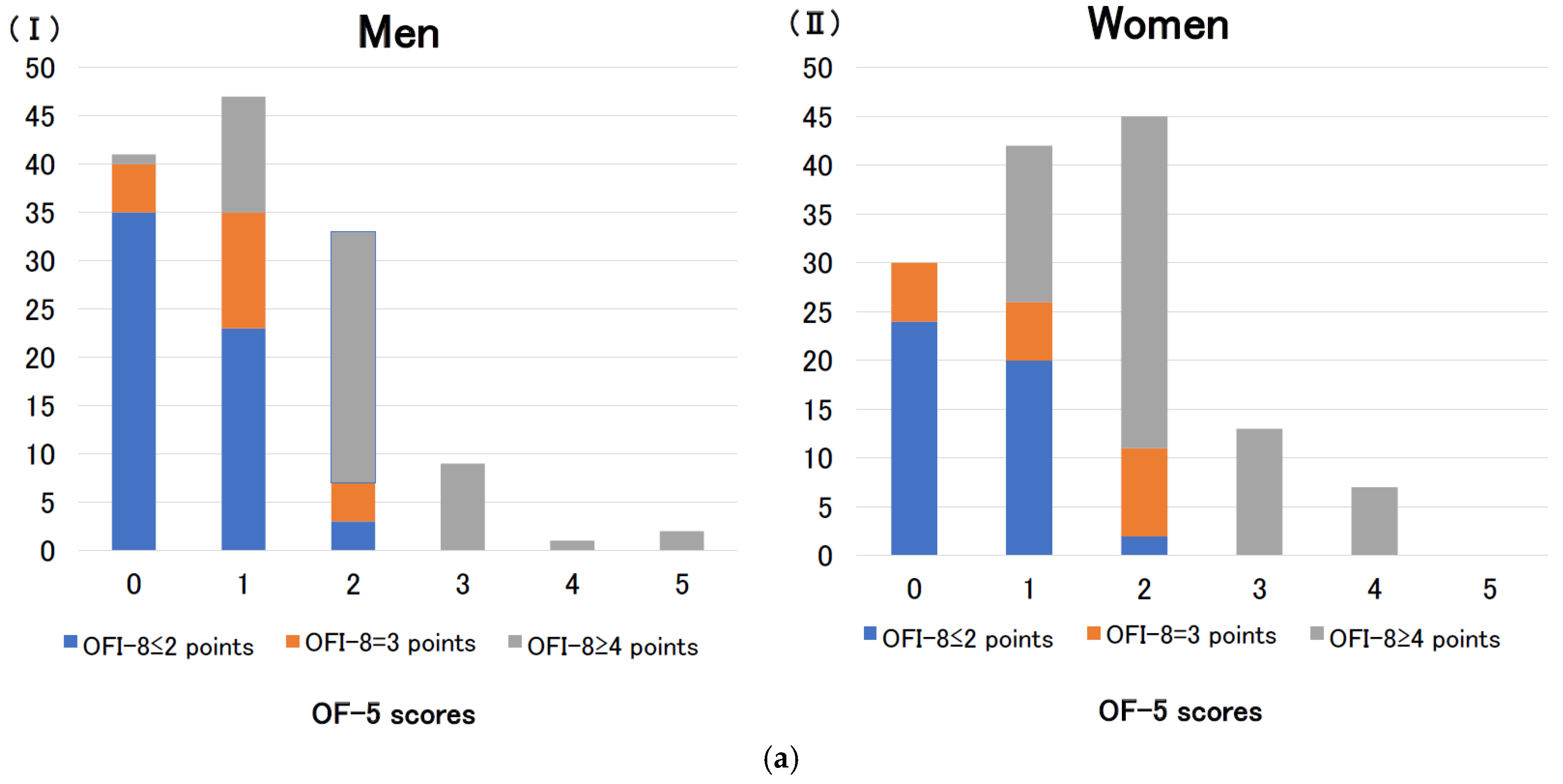
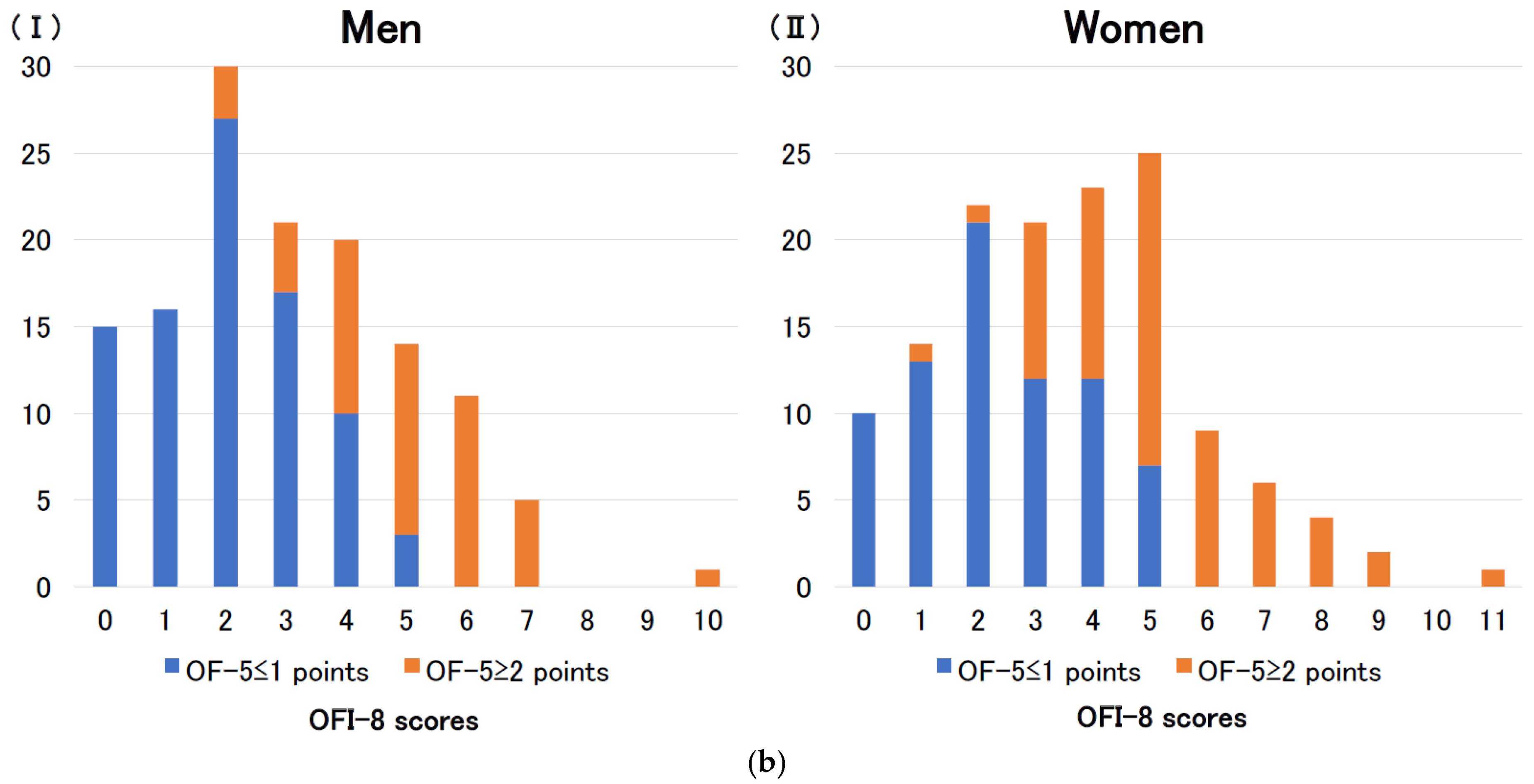
Figure 2.
The proportions of individuals with an OF-5 score ≥ 2 (defined as OF-5(+)) and an OFI-8 score ≥ 4 (defined as OFI-8(+)) within the overall sample in men (A) and women (B). Notes: x (y), number of patients (%).
Figure 2.
The proportions of individuals with an OF-5 score ≥ 2 (defined as OF-5(+)) and an OFI-8 score ≥ 4 (defined as OFI-8(+)) within the overall sample in men (A) and women (B). Notes: x (y), number of patients (%).
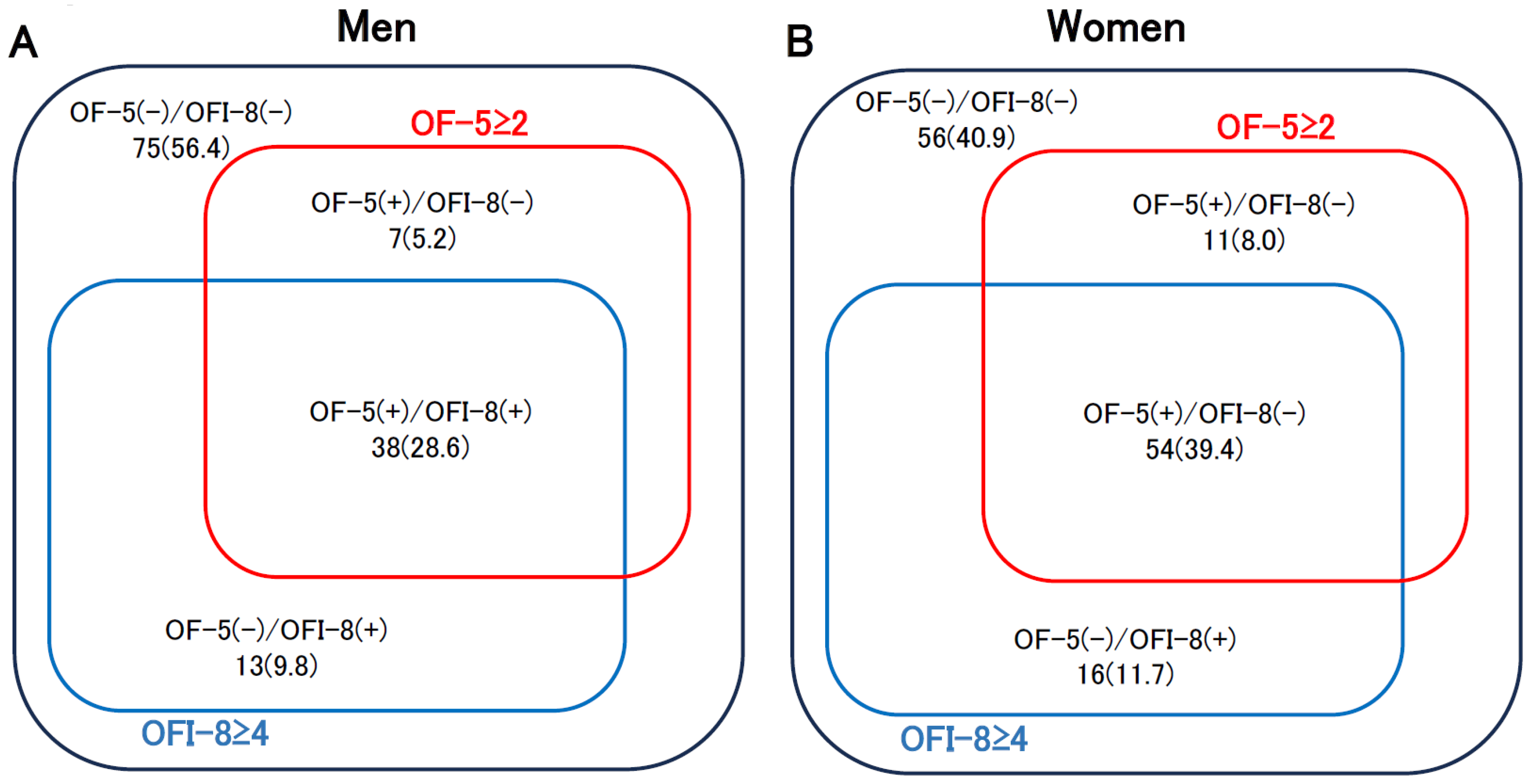

Table 1.
Baseline Characteristics of the Participants Stratified by Sex and the OF-5 and OFI-8 Questionnaires.
Table 1.
Baseline Characteristics of the Participants Stratified by Sex and the OF-5 and OFI-8 Questionnaires.
| Total (n = 270) |
Men (n = 133) |
Women (n = 137) |
p | ||
|---|---|---|---|---|---|
| Age (years) | 77.6±7.3 | 77.0±7.5 | 78.3±7.1 | 0.143 | |
| Height (cm) | 158.1±9.1 | 164.8±6.8 | 151.7±5.9 | <0.001 | |
| Weight (kg) | 59.6±11.8 | 66.1±10.7 | 53.2±9.0 | <0.001 | |
| Body mass index: BMI | 23.7±3.4 | 24.3±3.1 | 23.1±3.5 | 0.003 | |
| Grip strength (kg) | 23.0±8.8 | 29.5±7.1 | 16.6±4.4 | <0.001 | |
| White blood cells (/μL) | 5875±1574 | 5986±1596 | 5767±1551 | 0.255 | |
| Red blood cells (×104/μL) | 426±52 | 435±57 | 417±45 | 0.004 | |
| Hemoglobin (g/dL) | 13.2±1.6 | 13.7±1.6 | 12.8±1.4 | <0.001 | |
| Hematocrit (%) | 39.8±4.6 | 41.0±4.6 | 38.7±4.3 | <0.001 | |
| Platelets(×104/μL) | 21.3±5.1 | 20.5±4.8 | 22.1±5.3 | 0.007 | |
| Total protein (g/dL) | 7.0±0.4 | 7.0±0.4 | 7.1±0.4 | 0.140 | |
| Albumin (g/dL) | 4.1±0.4 | 4.2±0.4 | 4.1±0.4 | 0.793 | |
| Creatine (mg/dL) | 0.95±0.40 | 1.09±0.46 | 0.82±0.28 | <0.001 | |
| Hypertension, n(%) | 232(85.9) | 118(88.7) | 114(83.2) | 0.223 | |
| Comorbidities | |||||
| Diabetes, n(%) | 60(22.2) | 34(25.6) | 26(19.0) | 0.241 | |
| Dyslipidemia, n(%) | 148(54.8) | 66(49.6) | 82(59.9) | 0.112 | |
| Osteoporosis, n(%) | 20(7.4) | 5(3.8) | 15(10.9) | 0.035 | |
| Malignant neoplasm, n(%) | 23(8.5) | 16(12.0) | 7(5.1) | 0.005 | |
| Cardiovascular disease, n(%) | 71(26.3) | 41(30.8) | 30(21.9) | 0..100 | |
| Cerebrovascular disease, n(%) | 30(11.1) | 14(10.5) | 16(11.7) | 0.847 | |
| Questions | |||||
| OF-5 specific questions |
|
90(33.3) | 35(26.3) | 55(40.1) | 0.020 |
|
31(11.5) | 20(15.0) | 11(8.0) | 0.086 | |
| Questions common to OFI-5 and OFI-8 |
|
56(20.7) | 19(14.3) | 37(27.0) | 0.011 |
|
75(27.8) | 34(25.6) | 41(29.9) | 0.497 | |
|
101(37.4) | 46(34.6) | 55(40.1) | 0.380 | |
| OFI-8 specific questions |
|
156(57.8) | 75(56.4) | 81(59.1) | 0.712 |
|
76(28.1) | 28(21.1) | 48(35.0) | 0.015 | |
|
38(14.1) | 13(9.7) | 25(18.2) | 0.054 | |
|
57(21.1) | 32(24.1) | 25(18.2) | 0.297 | |
|
55(20.4) | 25(18.8) | 30(21.9) | 0.549 | |
| Questionnaire score results | |||||
| OF-5 score | 1.3±1.1 | 1.2±1.1 | 1.5±1.0 | 0.025 | |
| Oral frailty, ≥2 OF-5 score, n(%) | 110(40.7) | 45(33.8) | 65(47.4) | 0.016 | |
| OFI-8 score | 3.3±2.1 | 3.0±2.0 | 3.7±2.2 | 0.012 | |
| OFI-8 score≦2, n(%) | 107(39.6) | 61(45.9) | 46(33.6) | 0.047 | |
| OFI-8 score=3, n(%) | 42(15.6) | 21(15.8) | 21(15.3) | 1.000 | |
| OFI-8 score≧4, n(%) | 121(44.8) | 51(38.3) | 70(51.1) | 0.038 | |
Table 2.
Comparison of Physical and Biological Markers Between the Oral Non-Frailty and Oral Frailty Groups Determined by the OF-5, Stratified by Sex.
Table 2.
Comparison of Physical and Biological Markers Between the Oral Non-Frailty and Oral Frailty Groups Determined by the OF-5, Stratified by Sex.
| Men (n = 133) | Women (n = 137) | |||||
|---|---|---|---|---|---|---|
| Oral non-frailty, 0–1 OF-5 score (n = 88) |
Oral frailty, ≥2 OF-5 score (n = 45) |
p | Oral non-frailty, 0–1 OF-5 score (n = 72) |
Oral frailty, ≥2 OF-5 score (n = 65) |
p | |
| Age (year-old) | 75.9±7.4 | 79.1±7.5 | 0.021 | 78.0±7.1 | 78.6±7.1 | 0.673 |
| Height (cm) | 165.4±7.2 | 163.5±5.9 | 0.131 | 151.9±5.0 | 151.5±6.8 | 0.701 |
| Body weight (kg) | 67.3±11.5 | 63.9±8.6 | 0.088 | 53.9±9.1 | 52.4±8.9 | 0.328 |
| Body mass index | 24.5±3.2 | 23.9±2.9 | 0.300 | 23.3±3.7 | 22.8±3.3 | 0.360 |
| Grip strength (kg) | 30.2±7.0 | 28.1±7.3 | 0.114 | 17.0±4.1 | 16.1±4.8 | 0.248 |
| White blood cells (/μL) | 5769±1405 | 6410±1859 | 0.028 | 5663±1525 | 5884±1584 | 0.408 |
|
Red blood cells (×104/μL) |
438±59 | 429±54 | 0.414 | 419±42 | 415±49 | 0.590 |
| Hemoglobin (g/dL) | 13.8±1.7 | 13.5±1.4 | 0.404 | 12.8±1.5 | 12.7±1.4 | 0.702 |
| Hematocrit (%) | 41.3±4.9 | 40.5±4.0 | 0.327 | 38.7±4.3 | 38.6±4.3 | 0.900 |
| Platelets (×104/μL) | 20.5±5.0 | 20.5±4.5 | 0.981 | 22.3±5.2 | 22.1±5.4 | 0.846 |
| Total protein (g/dL) | 7.0±0.4 | 7.0±0.5 | 0.931 | 7.1±0.4 | 7.1±0.4 | 0.957 |
| Albumin (g/dL) | 4.2±0.4 | 4.1±0.4 | 0.375 | 4.2±0.4 | 4.1±0.3 | 0.767 |
| Creatinine (mg/dL) | 1.12±0.52 | 1.03±0.30 | 0.299 | 0.83±0.22 | 0.82±0.33 | 0.870 |
| Hypertension, n(%) | 79(89.8) | 39(86.7) | 0.576 | 64(88.9) | 50(76.9) | 0.070 |
| Diabetes, n(%) | 22(25.0) | 12(26.7) | 0.836 | 11(15.3) | 15(23.1) | 0.280 |
| Dyslipidemia, n(%) | 45(51.1) | 21(46.7) | 0.715 | 47(65.3) | 35(53.8) | 0.222 |
| Osteoporosis, n(%) | 5(5.7) | 0(0.0) | 0.167 | 5(6.9) | 10(15.4) | 0.170 |
| Malignant neoplasm, n(%) | 10(11.4) | 6(13.3) | 0.782 | 3(4.2) | 4(6.2) | 0.708 |
| Cardiovascular disease, n(%) | 28(31.8) | 13(28.9) | 0.843 | 17(23.6) | 13(20.0) | 0.682 |
| Cerebrovascular disease, n(%) | 8(9.1) | 6(13.3) | 0.552 | 9(12.5) | 7(10.8) | 0.796 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



