
Submitted:
29 January 2025
Posted:
30 January 2025
You are already at the latest version
Abstract
Background: Telmisartan, a widely used angiotensin II receptor blocker (ARB) with partial peroxisome proliferator-activated receptor-gamma (PPAR-γ) activity, may confer additional cardiovascular and metabolic benefits. However, evidence comparing telmisartan with other ARBs in terms of major cardiovascular outcomes and risk of new-onset diabetes remains limited
Method: 59767 patients with hypertension and ARB use between January 1, 2007 to December 31, 2017 were identified from the Chang Gung Research Database (CGRD), a multi-institutional electronic medical record database in Taiwan. Patients prescribed telmisartan or other ARBs for at least six months were included. Propensity score matching (1:4) was applied to balance baseline characteristics. Primary outcomes were new-onset diabetes mellitus(DM), major adverse cardiovascular events (MACE) (non-fatal myocardial infarction, non-fatal stroke and CV death) and all cause mortality.Secondary outcomes include hospitalization for heart failure and malignancy.The risks of new-onset DM, MACE, and mortality were compared between two groups using Cox proportional hazards models. In addition, we performed analyzes using Fine and Gray sub-distribution hazard models that considered death a competing risk.
Result: A total of 15,160 patients (telmisartan: 3,032; other ARBs: 12,128) were included after matching. Telmisartan users had a significantly lower risk of 3P-MACE (aHR 0.88, 95% CI 0.80–0.97, p = 0.0074) and non-fatal MI (aHR 0.68, 95% CI 0.52–0.90, p = 0.006) compared to other ARB users. No significant differences were observed for new-onset DM (aHR 1.06, 95% CI 0.88–1.28, p = 0.54), cardiovascular death (aHR 0.86, 95% CI 0.62–1.18, p = 0.35), or other outcomes such as stroke or hospitalization for heart failure.
Conclusion: Telmisartan is associated with superior cardiovascular protection which mainly attributed to reducing risks of non-fatal MI compared to other ARBs, while exhibiting a neutral effect on risk of new-onset DM. These findings suggest telmisartan may be a preferred ARB for hypertensive patients at high cardiovascular risk. Further prospective studies are warranted to validate these results and explore the underlying mechanisms.
Keywords:
telmisartan
; new-onset diabetes mellitus
; cardiovascular outcome
; hypertension
Background
Hypertension remains one of the leading global health challenges, contributing significantly to the burden of cardiovascular disease (CVD) and associated morbidity and mortality [1]. Angiotensin II receptor blockers (ARBs) are a cornerstone in the management of hypertension, particularly for patients with concurrent cardiovascular or renal risk factors [2,3]. The effects of different ARBs on renin–angiotensin–aldosterone system (RAAS), insulin resistance (IR),inflammation and oxidative stress may have further impact beyond their BP lowering effect [4,5,6,7].
Among the ARBs, telmisartan stands out due to its unique pharmacological profile. Telmisartan possesses partial peroxisome proliferator-activated receptor-gamma (PPAR-γ) agonist activity, a property shared with certain antidiabetic drugs such as thiazolidinediones [8]. Animal studies showed telmisartan improved insulin resistance and reversed glucose tolerance in pre-diabetic or diabetic hypertensive rats possibly through restoring adiponectin [9,10]. Several meta-analyses revealed telmisartan reduces fasting glucose, insulin levels, and improving homeostasis model assessment index (HOMA) in patients with metabolic syndrome,impaired fast glucose and diabetes mellitus [11,12,13]. Additionally, telmisartan's long half-life and high lipophilicity allow for sustained receptor blockade and enhanced blood pressure control [14]. These characteristics have led to the hypothesis that telmisartan might offer superior protection against cardiovascular events and new-onset diabetes compared to other ARBs.
Despite the established efficacy of telmisartan in major clinical trials, such as the ONTARGET and TRANSCEND studies [15,16], evidence directly comparing telmisartan with other ARBs in real-world settings is scarce. Most existing research has focused on class-wide effects of ARBs, overlooking potential differences among individual agents. In particular, the impact of telmisartan on major cardiovascular outcomes (e.g., 3P-MACE) and its effect on the risk of new-onset diabetes relative to other ARBs remain underexplored.To address this knowledge gap, we conducted a large, population-based, retrospective cohort study comparing telmisartan to other ARBs.. This study aims to provide insights into whether telmisartan's unique properties translate into measurable clinical advantages, thereby informing optimal ARB selection in hypertensive patients
Methods
Data Source
The study used the Chang Gung Research Database (CGRD), a de-identified dataset derived from the electronic medical records of the Chang Gung Memorial Hospital (CGMH) system. This system includes four tertiary medical centers and three teaching hospitals spread across different regions of Taiwan, providing a total of 10,050 beds and admitting approximately 280,000 patients each year [17], which constitutes roughly 10% of all medical services provided in Taiwan. In contrast to Taiwan's National Healthcare Insurance Research Database, which lacks detailed laboratory data and examination reports, the CGRD offers researchers easy access to these types of data, enabling more comprehensive analysis.
To maintain confidentiality, all potentially identifiable information about patients and healthcare providers is encrypted before being released to researchers. Consequently, patient consent was waived for this study. The study protocol was approved by the Institutional Review Board of the Chang Gung Medical Foundation, Taiwan. (IRB No: 202300720B0).
Patient Selection and Study Design
Patients with the principal diagnosis of hypertension from January 1, 2007 to December 31, 2017 were identified from the CGRD. Hypertension was identified by the principal diagnosis according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) diagnosis codes 401.xx-405.xx and ICD-10-CM diagnosis codes I10-I15, N262 when more than 2 outpatient visits or one inpatient admission recorded in the CGRD. Figure 1 illustrated the process of patient enrollment. Patients who were less than 20 years of age and with incomplete demographic data were not included in the study. Since we aimed to compared telmisartan with other ARB medications, we excluded patients without ARB based anti-hypertensive treatments. Patients with combination therapy with two kinds of ARB were also excluded. Steroid use affect the blood glucose hemostasis and we exclude patients with steroid use and patients with autoimmune disease who may receive long term steroid or immunosuppresants use. Patients with a diagnosis of DM and pre-DM status before index date were also excluded. Patients with malignancy were also excluded due to high risk of mortality.We obtained medication data from outpatient claims and pharmacy refill records for chronic illnesses. Patients were classified as ARB users if they were prescribed telmisartan or another ARB continuously for six months or longer, either through outpatient visits or pharmacy refills. We excluded patients from the non-telmisartan ARB group if they had taken telmisartan for even a single day during the 6-month exposure period. This was done to ensure consistent use of the study drugs in both groups.The index date was defined as 6-month after exposure to telmisartan or non-telmisartan ARB for the patients. Finally, 59767 patients with diagnosis of hypertension receiving ARB treatments were included in the study. Among 59767 patients, there were 3032 telmisartan users and 56735 non-telmisartan ARB users.
Covariates and Study Outcomes
Baseline demographic and clinical characteristics were identified using International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) codes prior to 2016 or ICD-10-CM codes later. Baseline characteristics in our study included age, sex, follow up duration, comorbidities, medications, laboratory datas. The comorbidities in question were dyslipidemia,coronary artery disease, atrial fibrillation, myocaridal infarction, heart failure, stroke, peripheral artery disease , chronic kidney disease, venous thromboembolism including deep vein thrombosis and pulmonary embolism,gout, HBV/HCV/liver cirrhosis, chronic obstructive pulmonary disease (COPD), obstructive sleep apnea, dementia. A comorbid condition was defined if the patients had at least 1 inpatient diagnoses or 2 outpatient diagnoses of a given disease reported in the year prior to the index date. Most of the diagnostic codes used for these comorbidities have been validated in previous national database studies [18,19]. Baseline medications use were defined as medications prescribed at least twice or refilling a prescription for a chronic illness at least once in the year prior to the index date. Baseline laboratory results including hemoglobin,creatinine, LDL, cholesterol, triglyceride,sugar and glycohemoglobin were obtained using the most recent record within 3 months prior to the index date.
Outcome Measurement
The primary outcomes were the diagnosis of new onset DM, major adverse cardiovascular events(MACE) including non-fatal myocaridial infarction, non-fatal stroke,cardiovascular death, hospitalization for heart failure. The secondary outcomes was malignancy and all cause mortality. The diagnosis of new onset DM was defined on the basis of the new principal diagnosis according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) diagnosis codes 250 and ICD-10-CM diagnosis codes E11 when more than 2 outpatient visits or one inpatient admission and the new prescription of oral antidiabetic drugs (use of at least one of the oral anti-diabetic agents including metformin, sulfonylurea, glinides,sodium-glucose cotransporter 2 inhibitors(SGLT2i), glucagon-like peptide-1 receptor agonist(GLP-1 RA), thiazolidinediones (TZD), acarbose, dipeptidyl peptidase-4 inhibitors (DPP4-inhibitors) or insulin during follow-up.
The diagnosis of non-fatal myocaridial infarction, non-fatal stroke and hospitalization for heart failure was based on the principal diagnosis in the emergency department or hospitalization. The causes of death were obtained from data linked to the Taiwan Death Registry. The patients were followed up after index date until an incident diagnosis of new onset DM, non-fatal myocaridial infarction, non-fatal stroke, hospitalization for heart failure,death or 31 December 2022, whichever occurred first.
Statistical Analysis
The baseline characteristics had substantial difference between the study groups (telmisartan vs non-telmisartan ARBs), which may induce selection bias. Thus, We used propensity score matching (PSM) to balance the distribution of baseline characteristics between the two groups [20]. Propensity score was defined as the probability of a patient to receive telmisartan treatment, which was calculated by the logistic regression model that included all the covariates listed in Table 1. To enhance statistical power, a 1:4 matching ratio was implemented. We assessed the quality of matching using the absolute standardized mean difference (ASMD) between the groups post-matching. An absolute value of less than 0.1 was considered to indicate an non-substantial difference between the groups. The risk of new onset DM between the telmisartan and non-telmisartan ARBs group was comparing using Cox proportional hazard model. We used Fine and Gray sub-distributional hazards model, which considered all-cause mortality as a competing risk to compare the time-to-new onset DM outcome between the 2 groups.Subgroups analyses were conducted on mortality stratified by age groups, sex, smoking status, diabetes, heart failure, hyperlipidemia and CKD stage. Statistical analyses were performed using SAS Version 9.4 (SAS Institute, Cary, NC). A two-sided P value of <0.05 was considered significant.
Results
Subject Characteristics
A total of 59767 patients with hypertension and ARB use from January 2007 to December 2017 were extracted from CGRD. Among these patients, 3032(5%) received telmisartan and 56736(95%) received non-telmisartan ARBs. The baseline characteristics of each group before and after PS matching are listed in Table 1. The mean age (years) of telmisartan group was 59.90 ± 14.14 and that of non-telmisartan ARBs group was 62.29 ± 14.31. Before PS matching, patients received telmisartan were younger and had lower rate of included comorbidities except dyslipidemia. Telmisartan group are more likely to receive calcium channel blockers whereas non-telmisartan ARBs are more likely to receive diuretics including thiazide, loop diuretics or K sparing diuretics. Telmisartan group had higher hemoglobin,LDL,cholesterol and triglyceride whereas non-telmisartan ARBs group patients had higher blood sugar. After the PS matching, all ASMD values were less than 0.1, suggestive of well-balanced baseline demographic and clinical characteristics between groups.
Risk of New-Onset DM and MACE Between Telmisartan Group and Non-Telmisartan ARB Group
Table 2. shows the risk of new-onset DM,3P-MACE (non-fatal MI,non-fatal stroke,CV death),hospitalization for heart failure,malignancy and all-cause mortality in telmisartan group compared to non-telmisartan ARBs group after IPTW. The Cox proportional hazards model with competing risk analysis showed no difference in risks of new-onset DM(aHR: 1.06, 95% CI 0.88-1.28, p=0.540) between the two groups during 36months of follow up. The telmisartan group had lower incidence rate of 3P-MACE compared to non-telmisartan ARBs(6.96 vs. 7.98 events per 100 person-years),resulting in a lower risk of 3P-MACE(aHR: 0.88, 95% CI: 0.80–0.97, p=0.007). The primary driver of the 3P-MACE risk reduction is the significant decrease in the risk of non-fatal myocardial infarction (aHR: 0.68, 95% CI: 0.52–0.90, p=0.006). There was no significant risk difference in hospitalization for heart failure(aHR: 0.85, 95% CI: 0.63–1.15, p=0.3004).Regarding other secondary outcomes, there was no significant difference between the two groups regarding the risk of malignancy (aHR:0.83, 95% CI: 0.65–1.06, p=0.1301) or all cause mortality (aHR: 1.04, 95% CI: 0.88–1.23, p=0.6472). Figure 2 revealed cumulative incidence rate for study outcomes between telmisartan and non-telmisartan ARBs group.
Subgroup Analysis
To verify whether clinical conditions modified the association between the two groups and primary outcomes, we performed subgroup analyses for 3P-MACE (Figure 3). The results were generally consistent in favored of telmisartan group regardless of age, gender, dyslipidemia, myocardial infarction/coronary heart disease, heart failure, stroke, atrial fibrillation and chronic kidney disease.
Discussion
This study provides a comprehensive comparison between telmisartan and non-telmisartan angiotensin receptor blockers (ARBs) in hypertensive patients without DM or pre-DM, with a particular focus on major cardiovascular outcomes, mortality, and risk of new-onset diabetes. The results demonstrate that while most clinical outcomes were comparable between the two groups, telmisartan was associated with a significantly lower risk of non-fatal myocardial infarction (MI) compared to non-telmisartan ARBs (aHR 0.69, P=0.03). This finding suggests that telmisartan may provide additional cardioprotective benefits in patients without DM or pre-DM, particularly in the prevention of MI. Other outcomes, including cardiovascular (CV) death, all-cause mortality, non-fatal stroke, and hospitalization for heart failure, did not differ significantly between telmisartan and non-telmisartan users, indicating that all ARBs may offer comparable efficacy in managing these hypertension-related complications.
In a previous meta-analysis of randomized clinical trials demonstrated that the use of the studied ARBs did not result in a significant difference in the risk of MI and stroke [21]. Furthermore, a recently published observational study has demonstrated that there is no difference in the risk of major adverse cardiovascular events (MACEs) and all-cause mortality among patients with hypertension who are using seven ARBs, without the presence of cardiovascular disease [22]. However, our results demonstrated that in patients with hypertension without DM or pre-DM, after propensity matching with comorbidities, telmisartan was associated with a lower risk of non-fatal MI in the three-year follow-up when compared to non-telmisartan ARBs. In a recent retrospective study by Yoo YG et al., it was reported that telmisartan was associated with a lower risk of MI when compared with valsartan and losartan use [23].
The half-lives of ARBs can be classified as either long or short. Telmisartan has the longest half-life of 24 hours among all ARBs [24]. Previous research has demonstrated that ARBs with long half-lives exhibited lower risk for MI compared with ARBs with short half-lives [23]. Therefore, our results are in accordance with the findings of the study by Yoo.
In addition, telmisartan has unique pharmacological characteristics that may account for the lower incidence of non-fatal MI in comparison to other ARBs observed in our study. It has been reported that the highly lipophilic telmisartan can influence peroxisome proliferator-activated receptor gamma (PPAR-γ) target gene expression by functioning as a partial agonist of PPAR-γ [25]. Furthermore, telmisartan has been demonstrated to induce PPAR-γ activity in the absence of Angiotensin type 1 receptor (AGTR1), indicating that its activation is independent of an AGTR1 blockade [26]. PPAR-γ activation has been proven to have benefits to ameliorate lipid oxidation [27], and inflammation [28]. Moreover, PPAR-γ plays a pivotal role in the pathogenesis of cardiovascular disease. In atherosclerotic lesions, PPAR-γ is highly expressed and its activation exerts anti-inflammatory effects in cardiovascular cells [29]. As a partial agonist of PPAR-γ, telmisartan has also been shown to enhance nitric oxide bioavailability and mitigates atherosclerotic changes through its PPAR-γ-mediated effects [30]. In the context of myocardial ischemic/reperfusion injury, telmisartan has been demonstrated to exert protective effects against microvascular dysfunction, at least in part through PPAR-γ-mediated mechanisms [31]. Consequently, telmisartan confers additional metabolic benefits beyond the control of blood pressure, potentially improving endothelial function and reducing the progression of atherosclerosis, which may contribute to the observed reduction in the risk of non-fatal MI.
With regard to cerebrovascular disease (non-fatal stroke) and heart failure, the present study did not reveal any beneficial effects associated with telmisartan when compared with other ARBs. Similarly, previous reports indicated that the risk of stroke is not different among different ARBs [21,22]. Moreover, in the context of heart failure, the adjusted hazard ratios for heart failure were also found to be similar across different ARBs in a previous study [23]. In the prevention of new-onset type 2 diabetes, ARBs have been reported to exert a beneficial effect in this regard [32]. Telmisartan is termed ”cardiometabolic sartan” due to its unique peroxisome PPAR-γ inducing property. A meta-analysis showed that telmisartan had benefit on fasting glucose, insulin and homeostasis model assessment(HOMA) index for patients with metabolic syndrome [11]. However, the metabolic benefits of telmisartan did not translate into the prevention of new-onset diabetes mellitus in hypertensive patients without prediabetes in current study. A nationwide population-based cohort study also found no association between telmisartan use and a lower risk of diabetes [33], which aligns with our findings. Further prospective studies are needed to validate the impact of telmisartan on the risk of developing DM.
Despite the robustness of the data and the large cohort size, this study has several limitations. Firstly, as an observational study based on propensity score matching, it is not possible to establish the causality. Although propensity score matching helps to balance covariates between the telmisartan and non-telmisartan groups, the possibility of residual confounding remains. It is likely that patients prescribed telmisartan may differ in unmeasured ways from those prescribed other ARBs, which could potentially affect the outcomes. Furthermore, although the study encompassed a heterogeneous range of comorbidities and medications in the analysis, other potential confounding factors, such as dietary habits, exercise routines, and treatment adherence, were not controlled for, which could have an impact on cardiovascular outcomes. A further limitation is the duration of the follow-up period. Although the three-year follow-up period is sufficient to observe major cardiovascular events, longer-term studies are necessary to fully understand the chronic effects of telmisartan versus other ARBs, particularly concerning all-cause mortality and the progression of comorbid conditions such as new-onset diabetes and malignancy. Finally, this study was conducted in a specific population with particular inclusion and exclusion criteria, such as the exclusion of patients with a history of diabetes or malignancy. These exclusions may limit the generalizability of the results to all hypertensive patients, particularly those with more complex medical histories or additional risk factors. It would therefore be beneficial for future studies to include a broader patient population to ensure that the findings are applicable to a wider clinical context.
This study suggests that telmisartan reduces the risk of non-fatal MI compared to other ARBs in hypertensive patients without diabetes or prediabetes, indicating potential additional cardioprotective benefits, especially for those at high risk for ischemic heart disease. However, both telmisartan and other ARBs offer similar protection against stroke, heart failure, and mortality. Clinicians should tailor ARB selection based on patient risk profiles and preferences, with telmisartan being a favorable option for MI prevention in high-risk patients. Further research with longer follow-up and diverse populations is needed to validate these findings.
Author Contributions
Research idea and study design: C.L, S.C.H,K.H.C,C.C.H; Data Acquisition: C.L.Y,W.Y.H,W.C.S, P.Y.F, Y.R.L ; Statistical analysis: Y.R.L,J.J.C ; Data interpretation: C.L, W.C.S, P.Y.F, K.H.C; Writing: C.L, S.C.H,K.H.C,C.C.H ; Supervision/mentorship: C.C.H, C.L. All authors read and approved the final manuscript.
Funding
The authors declare that they receive no funding.
Institutional Review Board Statement
The implementation and publication of this study was approved by the Institutional Review Board, Chang Gung Medical Foundation, Taiwan (IRB No: 202300720B0, approved on May 30,2023).
Informed Consent Statement
Not applicable.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Acknowledgments
We thank all the clinicians and patients enrolled in this study. The authors thank the statistical assistance and wish to acknowledge the support of the Ministry of Science and Technology of Taiwan (Grant MOST 112-2410-H-182A-001-) and the Maintenance Project of the Center for Artificial Intelligence in Medicine (Grant CMRPG3K0331, CLRPG3H0016 to Dr. Kuo) at Chang Gung Memorial Hospital for study design and monitor, data analysis and interpretation.
Conflicts of Interest
Non declared.
References
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef] [PubMed]
- Brenner, B.M.; Cooper, M.E.; De Zeeuw, D.; Keane, W.F.; Mitch, W.E.; Parving, H.-H.; Remuzzi, G.; Snapinn, S.M.; Zhang, Z.; Shahinfar, S. Effects of Losartan on Renal and Cardiovascular Outcomes in Patients with Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2001, 345, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Lewis, E.J.; Hunsicker, L.G.; Clarke, W.R.; Berl, T.; Pohl, M.A.; Lewis, J.B.; Ritz, E.; Atkins, R.C.; Rohde, R.; Raz, I.; et al. Renoprotective Effect of the Angiotensin-Receptor Antagonist Irbesartan in Patients with Nephropathy Due to Type 2 Diabetes. N. Engl. J. Med. 2001, 345, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Ragonesi, P.D. Effects of angiotensin II receptor blockers on insulin resistance. Hypertens. Res. 2010, 33, 778–778. [Google Scholar] [CrossRef]
- Guo, L.L.; Pan, Y.; Jin, H.M. Adiponectin is positively associated with insulin resistance in subjects with type 2 diabetic nephropathy and effects of angiotensin II type 1 receptor blocker losartan. Nephrol. Dial. Transplant. 2009, 24, 1876–1883. [Google Scholar] [CrossRef]
- Yamana, A.; Arita, M.; Furuta, M.; Shimajiri, Y.; Sanke, T. The angiotensin II receptor blocker telmisartan improves insulin resistance and has beneficial effects in hypertensive patients with type 2 diabetes and poor glycemic control. Diabetes Res. Clin. Pr. 2008, 82, 127–131. [Google Scholar] [CrossRef]
- Hinoi, T.; Tomohiro, Y.; Kajiwara, S.; Matsuo, S.; Fujimoto, Y.; Yamamoto, S.; Shichijo, T.; Ono, T. Telmisartan, an Angiotensin II Type 1 Receptor Blocker, Improves Coronary Microcirculation and Insulin Resistance among Essential Hypertensive Patients without Left Ventricular Hypertrophy. Hypertens. Res. 2008, 31, 615–622. [Google Scholar] [CrossRef]
- Kurtz, T.W.; Pravenec, M. Antidiabetic mechanisms of angiotensin-converting enzyme inhibitors and angiotensin II receptor antagonists: beyond the renin-angiotensin system. J. Hypertens. 2004, 22, 2253–2261. [Google Scholar] [CrossRef]
- Younis, F.; Oron, Y.; Limor, R.; Stern, N.; Rosenthal, T. Prophylactic treatment with telmisartan induces tissue-specific gene modulation favoring normal glucose homeostasis in Cohen-Rosenthal diabetic hypertensive rats. Metabolism 2012, 61, 164–174. [Google Scholar] [CrossRef]
- Zhao, Z.-Q.; Luo, R.; Li, L.-Y.; Tian, F.-S.; Zheng, X.-L.; Xiong, H.-L.; Sun, L.-T. Angiotensin II Receptor Blocker Telmisartan Prevents New-Onset Diabetes in Pre-Diabetes OLETF Rats on a High-Fat Diet: Evidence of Anti-Diabetes Action. Can. J. Diabetes 2013, 37, 156–168. [Google Scholar] [CrossRef]
- Takagi, H.; Niwa, M.; Mizuno, Y.; Goto, S.-N.; Umemoto, T. Telmisartan as a metabolic sartan: The first meta-analysis of randomized controlled trials in metabolic syndrome. J. Am. Soc. Hypertens. 2013, 7, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Suksomboon, N.; Poolsup, N.; Prasit, T. Systematic review of the effect of telmisartan on insulin sensitivity in hypertensive patients with insulin resistance or diabetes. J. Clin. Pharm. Ther. 2011, 37, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Qiao, S.; Han, D.-W.; Rong, X.-R.; Wang, Y.-X.; Xue, J.-J.; Yang, J. Telmisartan Improves Insulin Resistance: A Meta-Analysis. Am. J. Ther. 2018, 25, e642–e651. [Google Scholar] [CrossRef] [PubMed]
- White, W.B.; Lacourciere, Y.; Davidai, G. Effects of the angiotensin II receptor blockers telmisartan versus valsartan on the circadian variation of blood pressure impact on the early morning period. Am. J. Hypertens. 2004, 17, 347–353. [Google Scholar] [CrossRef]
- The ONTARGET Investigators Telmisartan, Ramipril, or Both in Patients at High Risk for Vascular Events. New Engl. J. Med. 2008, 358, 1547–1559. [CrossRef]
- Yusuf, S.; Teo, K.; Anderson, C.S.; Pogue, J.; Dyal, L.; Copland, I.; Schumacher, H.; Dagenais, G.; Sleight, P.; The Telmisartan Randomised AssessmeNt Study in ACE iNtolerant Subjects with Cardiovascular Disease (TRANSCEND) Investigators. Effects of the angiotensin-receptor blocker telmisartan on cardiovascular events in high-risk patients intolerant to angiotensin-converting enzyme inhibitors: a randomised controlled trial. Lancet 2008, 372, 1174–1183. [Google Scholar] [CrossRef]
- Shao, S.; Chan, Y.; Yang, Y.K.; Lin, S.; Hung, M.; Chien, R.; Lai, C.; Lai, E.C. The Chang Gung Research Database—A multi-institutional electronic medical records database for real-world epidemiological studies in Taiwan. Pharmacoepidemiol. Drug Saf. 2019, 28, 593–600. [Google Scholar] [CrossRef]
- Wu, C.-S.; Lai, M.-S.; Gau, S.S.-F.; Wang, S.-C.; Tsai, H.-J. Concordance between Patient Self-Reports and Claims Data on Clinical Diagnoses, Medication Use, and Health System Utilization in Taiwan. PLOS ONE 2014, 9, e112257. [Google Scholar] [CrossRef]
- Hsieh, C.-Y.; Chen, C.-H.; Li, C.-Y.; Lai, M.-L. Validating the diagnosis of acute ischemic stroke in a National Health Insurance claims database. J. Formos. Med Assoc. 2015, 114, 254–259. [Google Scholar] [CrossRef]
- Xu, S.; Ross, C.; Raebel, M.A.; Shetterly, S.; Blanchette, C.; Smith, D. Use of Stabilized Inverse Propensity Scores as Weights to Directly Estimate Relative Risk and Its Confidence Intervals. Value Heal. 2010, 13, 273–277. [Google Scholar] [CrossRef]
- Tsoi, B.; Akioyamen, L.E.; Bonner, A.; Frankfurter, C.; Levine, M.; Pullenayegum, E.; Goeree, R.; O’reilly, D. Comparative Efficacy of Angiotensin II Antagonists in Essential Hypertension: Systematic Review and Network Meta-Analysis of Randomised Controlled Trials. Hear. Lung Circ. 2018, 27, 666–682. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Kang, J.; Park, J.; Seo, W.; Lee, S.; Lim, W.; Jeon, K.; Hwang, I.; Kim, H. Long-term mortality and cardiovascular events of seven angiotensin receptor blockers in hypertensive patients: Analysis of a national real-world database: A retrospective cohort study. Heal. Sci. Rep. 2023, 6, e1056. [Google Scholar] [CrossRef] [PubMed]
- Yoo, Y.-G.M.; Lim, M.-J.M.; Kim, J.-S.; Jeong, H.-E.; Ko, H.B.; Shin, J.-Y. Risk of myocardial infarction, heart failure, and cerebrovascular disease with the use of valsartan, losartan, irbesartan, and telmisartan in patients. Medicine 2023, 102, e36098. [Google Scholar] [CrossRef] [PubMed]
- Abraham, H.M.A.; White, C.M.; White, W.B. The Comparative Efficacy and Safety of the Angiotensin Receptor Blockers in the Management of Hypertension and Other Cardiovascular Diseases. Drug Saf. 2014, 38, 33–54. [Google Scholar] [CrossRef]
- Benson, S.C.; Pershadsingh, H.A.; Ho, C.I.; Chittiboyina, A.; Desai, P.; Pravenec, M.; Qi, N.; Wang, J.; Avery, M.A.; Kurtz, T.W. Identification of Telmisartan as a Unique Angiotensin II Receptor Antagonist With Selective PPARγ–Modulating Activity. Hypertension 2004, 43, 993–1002. [Google Scholar] [CrossRef]
- Schupp, M.; Janke, J.; Clasen, R.; Unger, T.; Kintscher, U. Angiotensin Type 1 Receptor Blockers Induce Peroxisome Proliferator–Activated Receptor-γ Activity. Circulation 2004, 109, 2054–2057. [Google Scholar] [CrossRef]
- Kersten, S.; Desvergne, B.; Wahli, W. Roles of PPARs in health and disease. Nature 2000, 405, 421–424. [Google Scholar] [CrossRef]
- Zhu, W.; et al. PPAR-γ agonist pioglitazone regulates dendritic cells immunogenicity mediated by DC-SIGN via the MAPK and NF-κB pathways. International immunopharmacology 41, 24-34 (2016).
- Hamblin, M.; Chang, L.; Fan, Y.; Zhang, J.; Chen, Y.E. PPARs and the Cardiovascular System. Antioxidants Redox Signal. 2009, 11, 1415–1452. [Google Scholar] [CrossRef]
- Ikejima, H.; Imanishi, T.; Tsujioka, H.; Kuroi, A.; Kobayashi, K.; Shiomi, M.; Muragaki, Y.; Mochizuki, S.; Goto, M.; Yoshida, K.; et al. Effects of telmisartan, a unique angiotensin receptor blocker with selective peroxisome proliferator-activated receptor-γ-modulating activity, on nitric oxide bioavailability and atherosclerotic change. J. Hypertens. 2008, 26, 964–972. [Google Scholar] [CrossRef]
- Zeng, X.-C.; Li, X.-S.; Wen, H. Telmisartan protects against microvascular dysfunction during myocardial ischemia/reperfusion injury by activation of peroxisome proliferator-activated receptor gamma. BMC Cardiovasc. Disord. 2013, 13, 1–10. [Google Scholar] [CrossRef]
- Geng, D.-F.; Jin, D.-M.; Wu, W.; Xu, Y.; Wang, J.-F. Angiotensin receptor blockers for prevention of new-onset type 2 diabetes: A meta-analysis of 59,862 patients. Int. J. Cardiol. 2012, 155, 236–242. [Google Scholar] [CrossRef]
- Chang, C.-H.; Chang, Y.-C.; Wu, L.-C.; Lin, J.-W.; Chuang, L.-M.; Lai, M.-S. Different angiotensin receptor blockers and incidence of diabetes: a nationwide population-based cohort study. Cardiovasc. Diabetol. 2014, 13, 91–91. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of patient selection.
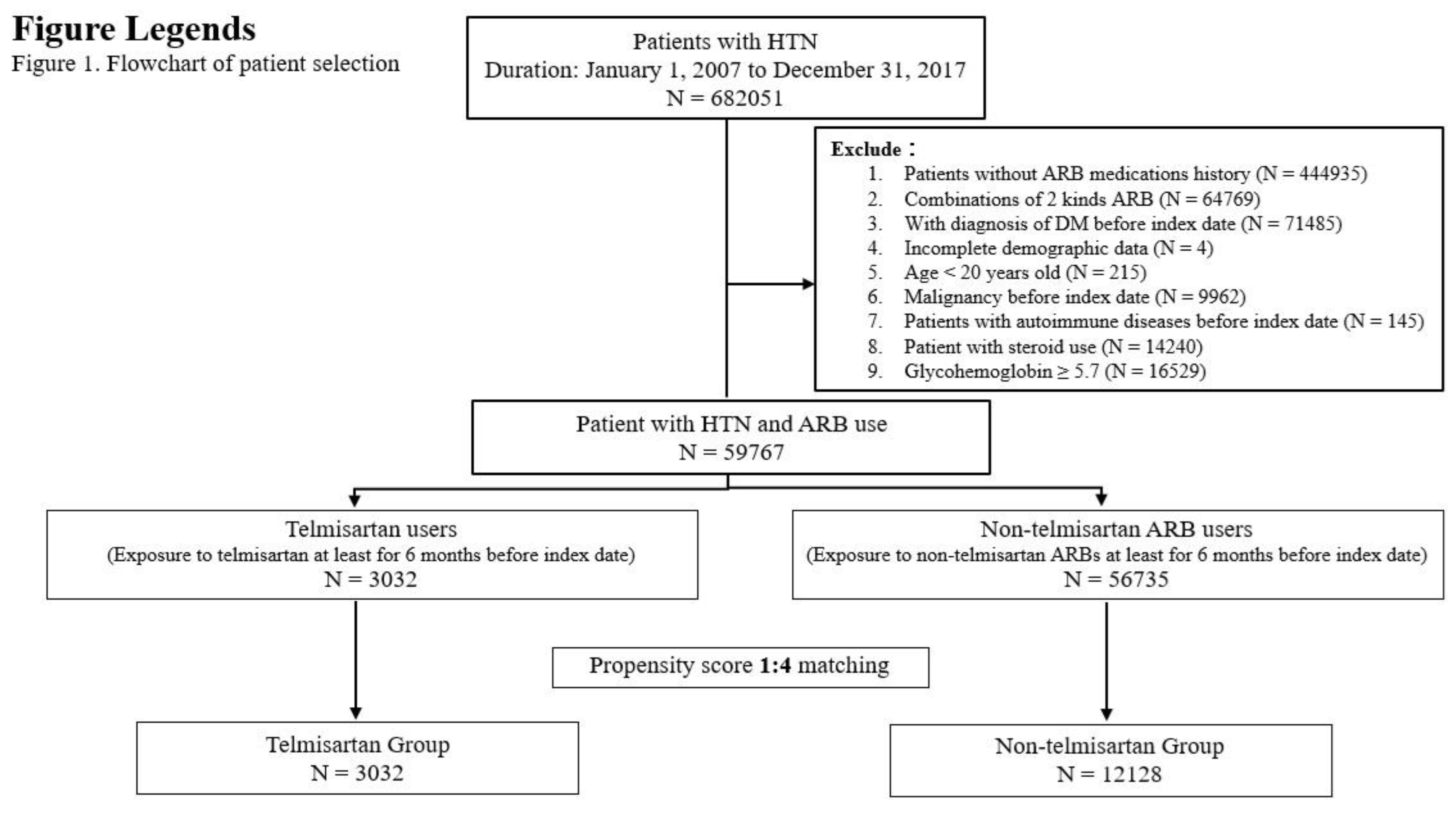
Figure 2.
Cumulative incidence rate for study outcomes between telmisartan and Non-telmisartan ARB.
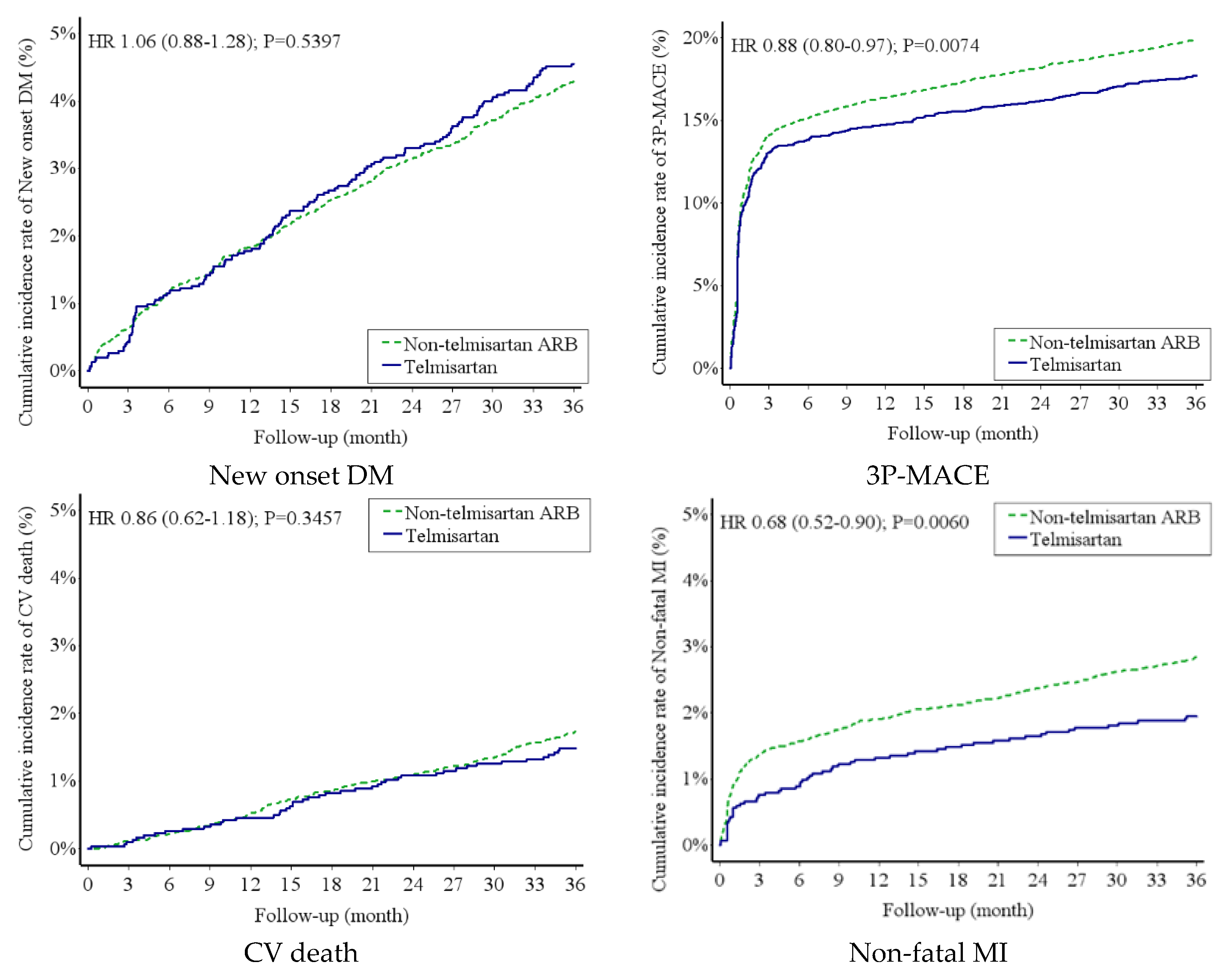
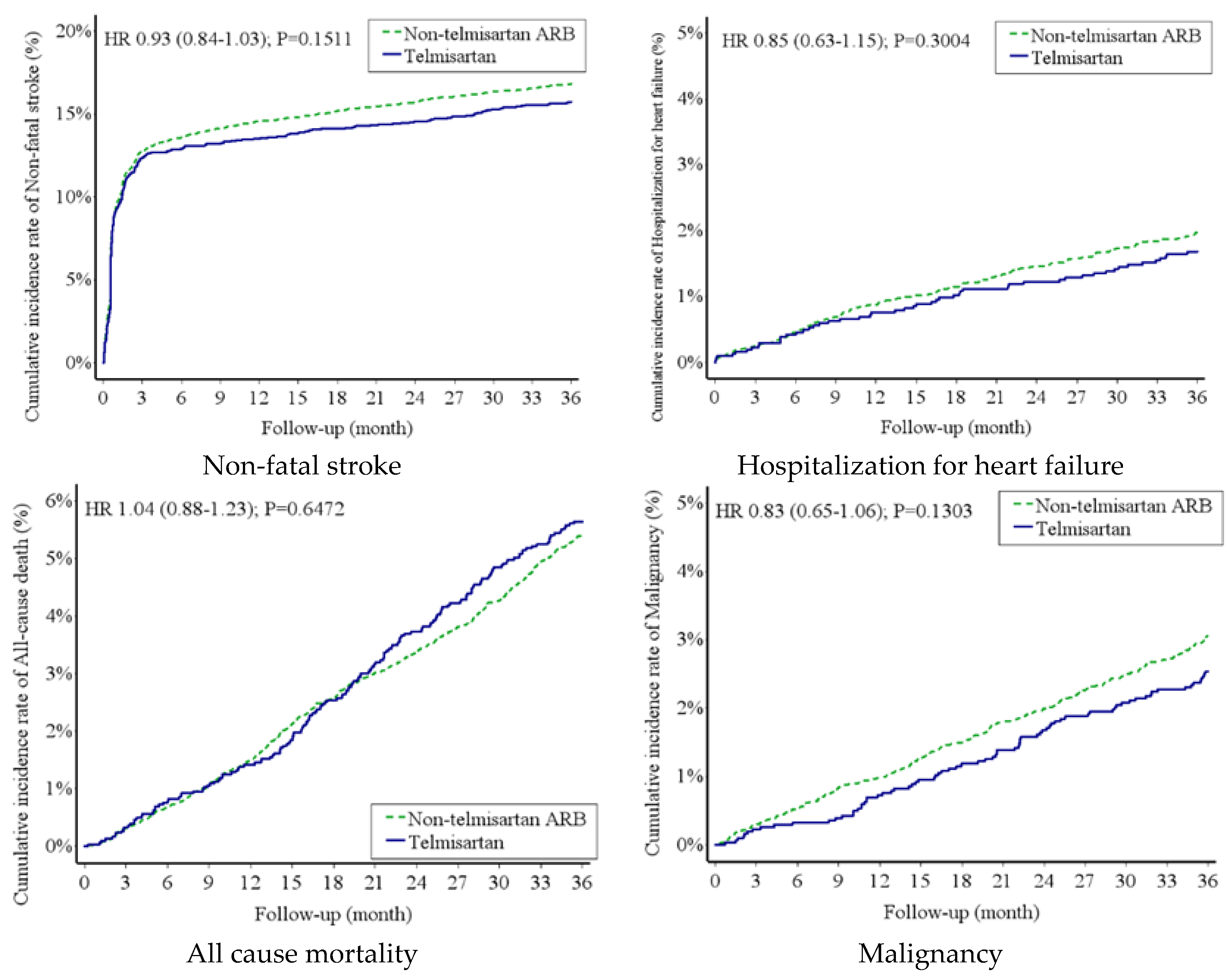
Figure 3.
Subgroup analysis of the risks of 3P-MACE between telmisartan group and non-telmisartan ARBs.
Figure 3.
Subgroup analysis of the risks of 3P-MACE between telmisartan group and non-telmisartan ARBs.
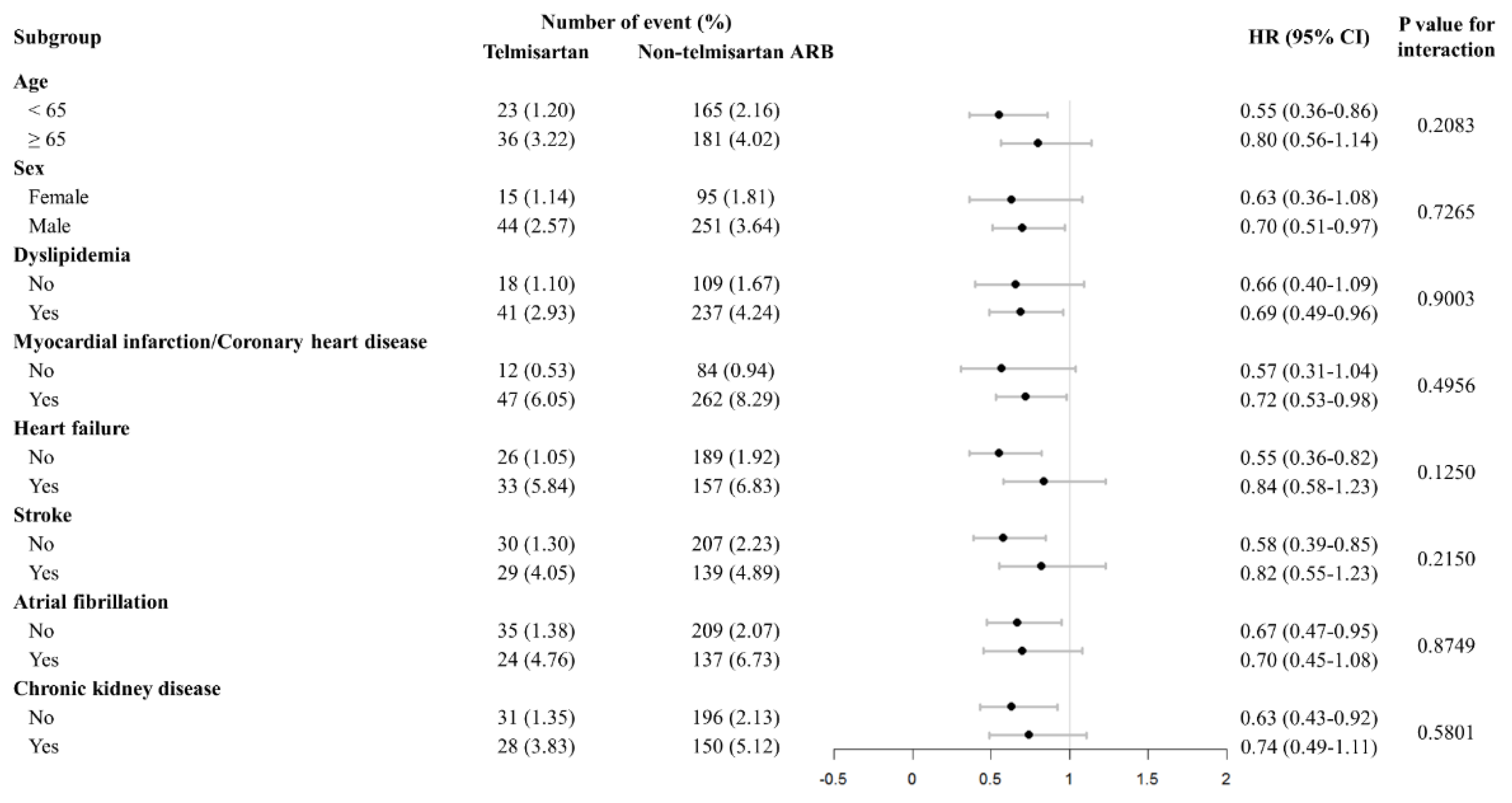

Table 1.
Demographic Characteristic of Study Population before and after Propensity Scores Matching.
Table 1.
Demographic Characteristic of Study Population before and after Propensity Scores Matching.
| Variable | Before | After Propensity Score Matching | ||||
|---|---|---|---|---|---|---|
| Telmisartan | Non-telmisartan ARB | P-value a | Telmisartan | Non-telmisartan ARB | P-value a | |
| (N = 3032) | (N = 56735) | (N = 3032) | (N = 12128) | |||
| Age, yearsb | 59.90 ± 14.14 | 62.29 ± 14.31 | <0.0001* | 59.90 ± 14.14 | 59.96 ± 14.27 | 0.8344 |
| Age group | <0.0001* | 0.7554 | ||||
| ˂65 years old | 1913 (63.09) | 31349 (55.26) | 1913 (63.09) | 7631 (62.92) | ||
| 65-74 years old | 573 (18.90) | 12342 (21.75) | 573 (18.90) | 2248 (18.54) | ||
| ≥75 years old | 546 (18.01) | 13044 (22.99) | 546 (18.01) | 2249 (18.54) | ||
| Sex (Male) | 1714 (56.53) | 32045 (56.48) | 0.9582 | 1714 (56.53) | 6888 (56.79) | 0.7931 |
| Follow up duration (years) | 5.92 ± 4.43 | 5.42 ± 4.62 | <0.0001* | 5.92 ± 4.43 | 5.89 ± 4.60 | 0.7580 |
| Comorbidity | ||||||
| Dyslipidemia | 1400 (46.17) | 26296 (46.35) | 0.8509 | 1400 (46.17) | 5594 (46.12) | 0.9610 |
| Coronary artery disease | 777 (25.63) | 16769 (29.56) | <0.0001* | 777 (25.63) | 3162 (26.07) | 0.6170 |
| Atrial fibrillation | 504 (16.62) | 11824 (20.84) | <0.0001* | 504 (16.62) | 2037 (16.80) | 0.8194 |
| Peripheral artery disease | 483 (15.93) | 10882 (19.18) | <0.0001* | 483 (15.93) | 1940 (16.00) | 0.9294 |
| Chronic kidney disease | 732 (24.14) | 15444 (27.22) | 0.0002* | 732 (24.14) | 2929 (24.15) | 0.9924 |
| Venous thromboembolism (DVT/PE) | 449 (14.81) | 9961 (17.56) | 0.0001* | 449 (14.81) | 1822 (15.02) | 0.7673 |
| Gout | 672 (22.16) | 14214 (25.05) | 0.0003* | 672 (22.16) | 2716 (22.39) | 0.7849 |
| HBV | 441 (14.54) | 9904 (17.46) | <0.0001* | 441 (14.54) | 1787 (14.73) | 0.7919 |
| HCV | 441 (14.54) | 9942 (17.52) | <0.0001* | 441 (14.54) | 1781 (14.69) | 0.8452 |
| Liver cirrhosis | 449 (14.81) | 10091 (17.79) | <0.0001* | 449 (14.81) | 1821 (15.01) | 0.7760 |
| Chronic obstructive pulmonary disease | 544 (17.94) | 12536 (22.10) | <0.0001* | 544 (17.94) | 2173 (17.92) | 0.9747 |
| Obstructive sleep apnea | 440 (14.51) | 9841 (17.35) | <0.0001* | 440 (14.51) | 1781 (14.69) | 0.8094 |
| Dementia | 451 (14.87) | 9966 (17.57) | 0.0001* | 451 (14.87) | 1820 (15.01) | 0.8555 |
| Myocardial infarction | 456 (15.04) | 10455 (18.43) | <0.0001* | 456 (15.04) | 1837 (15.15) | 0.8829 |
| Heart failure | 565 (18.63) | 12527 (22.08) | <0.0001* | 565 (18.63) | 2298 (18.95) | 0.6934 |
| Stroke | 716 (23.61) | 16574 (29.21) | <0.0001* | 716 (23.61) | 2844 (23.45) | 0.8481 |
| Drug | ||||||
| Aspirin | 257 (8.48) | 5044 (8.89) | 0.4344 | 257 (8.48) | 1037 (8.55) | 0.8959 |
| Clopidogrel | 24 (0.79) | 600 (1.06) | 0.1603 | 24 (0.79) | 84 (0.69) | 0.5623 |
| Fibrate | 62 (2.04) | 1250 (2.20) | 0.5620 | 62 (2.04) | 250 (2.06) | 0.9544 |
| Statin | 635 (20.94) | 11855 (20.90) | 0.9496 | 635 (20.94) | 2470 (20.37) | 0.4812 |
| Beta-blockers | 773 (25.49) | 13974 (24.63) | 0.2821 | 773 (25.49) | 3095 (25.52) | 0.9777 |
| Calcium channel blockers | 1621 (53.46) | 27200 (47.94) | <0.0001* | 1621 (53.46) | 6416 (52.90) | 0.5801 |
| Diuretic(Thiazide) | 621 (20.48) | 14937 (26.33) | <0.0001* | 621 (20.48) | 2444 (20.15) | 0.6859 |
| Diuretic(Loop) | 144 (4.75) | 3989 (7.03) | <0.0001* | 144 (4.75) | 570 (4.70) | 0.9084 |
| Diuretic(K sparing) | 13 (0.43) | 888 (1.57) | <0.0001* | 13 (0.43) | 52 (0.43) | 1.0000 |
| Laboratory data | ||||||
| Hemoglobin | 13.43 ± 2.14 | 13.26 ± 2.06 | 0.0049* | 13.52 ± 2.01 | 13.50 ± 2.02 | 0.6477 |
| Creatinine | 1.24 ± 1.47 | 1.22 ± 1.32 | 0.5070 | 1.26 ± 1.44 | 1.27 ± 1.46 | 0.7738 |
| LDL | 115.15 ± 32.78 | 111.67 ± 32.00 | <0.0001* | 114.42 ± 32.23 | 114.10 ± 32.12 | 0.6225 |
| Cholesterol | 190.52 ± 35.27 | 186.71 ± 35.08 | <0.0001* | 189.77 ± 35.20 | 189.36 ± 35.10 | 0.5616 |
| Triglyceride | 139.98 ± 76.19 | 135.99 ± 76.74 | 0.0226* | 138.42 ± 76.50 | 138.54 ± 78.32 | 0.9418 |
| Sugar | 101.21 ± 16.42 | 103.10 ± 20.18 | <0.0001* | 102.29 ± 17.95 | 102.42 ± 19.53 | 0.7241 |
| Glycohemoglobin | 5.38 ± 0.24 | 5.40 ± 0.22 | 0.2704 | 5.40 ± 0.22 | 5.40 ± 0.22 | 0.8625 |
Data are presented as mean ± standard deviation and n (%); a Chi-squared test; b Student’s t-test; *P < 0.05.
Table 2.
Risks of study outcomes in patients with Telmisartan group and non-telmisartan ARBs group.
| Number of events (events/100 person-year) | aHR (95% CI)a | P-valuea | aHR (95% CI)b | P-valueb | ||
|---|---|---|---|---|---|---|
| Telmisartan | Non-telmisartan ARB | |||||
| New onset DM | 138 (1.56) | 521 (1.47) | 1.06 (0.88-1.28) | 0.5397 | 1.06 (0.88-1.28) | 0.5395 |
| 3P-MACE | 537 (6.96) | 2414 (7.98) | 0.88 (0.80-0.97) | 0.0074* | 0.88 (0.80-0.97) | 0.0073* |
| CV death | 45 (0.50) | 210 (0.58) | 0.86 (0.62-1.18) | 0.3457 | 0.86 (0.62-1.18) | 0.3458 |
| Non-fatal MI (AMI+PCI+CABG+TT) | 59 (0.66) | 346 (0.97) | 0.68 (0.52-0.90) | 0.0060* | 0.68 (0.52-0.90) | 0.0059* |
| Non-fatal stroke | 477 (6.08) | 2041 (6.58) | 0.93 (0.84-1.03) | 0.1511 | 0.93 (0.84-1.03) | 0.1499 |
| All-cause mortality | 171 (1.93) | 659 (1.86) | 1.04 (0.88-1.23) | 0.6472 | - | - |
| Hospitalization for heart failure | 51 (0.57) | 239 (0.66) | 0.85 (0.63-1.15) | 0.3004 | 0.85 (0.63-1.15) | 0.3004 |
| Malignancy | 77 (0.86) | 371 (1.04) | 0.83 (0.65-1.06) | 0.1303 | 0.83 (0.65-1.06) | 0.1301 |
a: The adjusted hazard ratios were calculated by the cox proportional hazard model and adjusted using the inverse probability of treatment weighting method which measured based on the selected covariates listed in Table 1; b: Fine and Gray subdistribution hazard mode.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



