Submitted:
27 January 2025
Posted:
28 January 2025
Read the latest preprint version here
Abstract
Medical errors are a serious and complex problem that affects healthcare systems worldwide, causing considerable harm to patients and their families, as well as economic loss. This document explores medical errors, including their definition, impact, types, and contributing factors. It also delves into diagnostic error, its causes and consequences, as well as strategies to prevent it. Ethical considerations, legal liability, and the crucial role that communication, training, and technology play in improving patient safety are discussed. The document emphasizes the importance of a multidisciplinary approach to addressing medical errors, including improving communication between doctors and patients, continuing education of health professionals, using diagnostic support tools, and implementing reporting systems. and learning from mistakes. It also highlights the need to foster a culture of patient safety and the fundamental role of ethics committees in the management of medical errors.
Keywords:
Introduction
Definition and Scope of the Problem
- Diagnostic errors: They include erroneous, delayed or missed diagnoses, as well as overdiagnosis, which can lead to unnecessary and potentially harmful treatments.
- Treatment errors: They cover errors in prescribing, administering and monitoring medications, as well as errors in surgical procedures and other medical treatments.
- Prevention errors: They refer to the failure to implement preventive measures, such as vaccination or disease screening, which can increase the risk of complications and diseases.
- Communication errors: They include failures in communication between health professionals, as well as between professionals and patients, which can lead to misunderstandings and incorrect clinical decisions.
Impact of Medical Errors on Public Health and the Economy
Historical Perspective of Patient Safety
The Silent Impact: An Analysis of the Types of Medical Errors
Classification of Medical Errors According to Their Seriousness and Consequences
- Mild adverse events: These are errors that cause minimal or temporary harm to the patient, such as a mild allergic reaction to a medication or a small infection at the site of an injection.
- Moderate adverse events: They are errors that cause significant but reversible harm to the patient, such as a bone fracture during a fall in the hospital or an adverse reaction to a medication that requires hospitalization.
- Serious adverse events: These are errors that cause permanent or life-threatening harm to the patient, such as a brain injury during surgery or a severe allergic reaction that causes anaphylactic shock.
- Fatal adverse events: These are errors that result in the death of the patient, such as a fatal medication error or a serious nosocomial infection.
Examples of Medical Error Cases
- Misdiagnosis: A patient with severe abdominal pain is diagnosed with indigestion and sent home, but in reality suffers from acute appendicitis that ruptures, causing peritonitis and putting his life at risk.
- Medication error: A patient receives an excessive dose of an anticoagulant medication, causing severe internal bleeding and requiring an emergency blood transfusion.
- Surgical error: During knee surgery, the surgeon accidentally injures a nerve, causing permanent loss of sensation in the patient's leg.
- Communication error: A patient with a history of allergy to penicillin receives this antibiotic, despite having reported his allergy to the doctor. The patient suffers a severe anaphylactic reaction and requires urgent medical attention.
Contributing Factors to Medical Errors: A Multidimensional Analysis
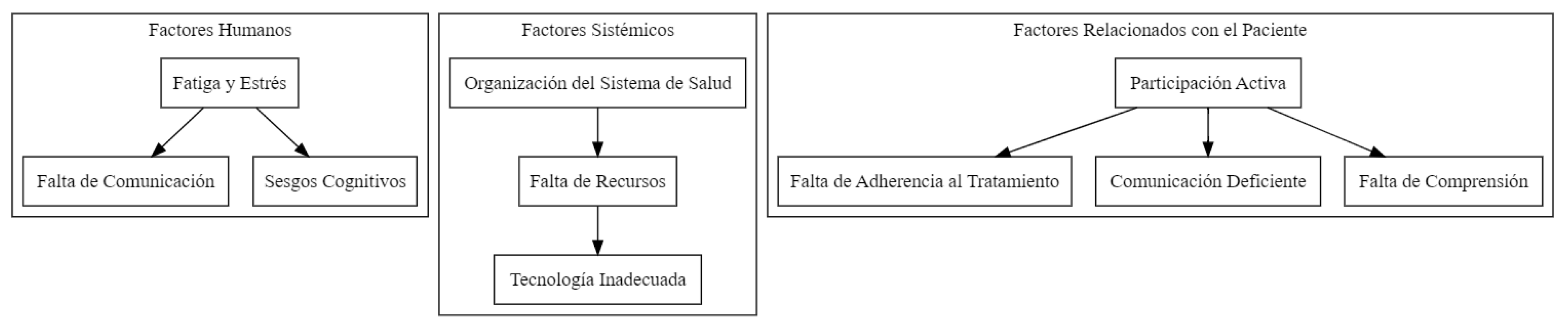
Human Factors: Lack of Healthcare Professionals
- Fatigue and Stress: Excessive workload, long shifts, and lack of adequate rest can negatively affect the cognitive and physical performance of healthcare professionals, increasing the risk of errors. Fatigue can decrease attention, concentration, memory, and decision-making ability, while chronic stress can lead to emotional exhaustion and depersonalization, which can affect empathy and the quality of care provided.
- Lack of Communication: Effective communication between members of the healthcare team is essential to ensure patient safety. Lack of clarity in the transmission of information, ambiguous verbal orders, lack of coordination between different professionals involved in patient care, and linguistic or cultural barriers can lead to misunderstandings and errors.
- Cognitive Biases: Cognitive biases are systematic thinking patterns that can lead to erroneous judgments and decisions. In the medical context, these biases can influence the way professionals collect, interpret and process clinical information, which can lead to diagnostic and treatment errors. Some common cognitive biases in medical practice include confirmation bias (the tendency to seek information that confirms pre-existing beliefs), anchoring bias (the tendency to rely too much on the first information received), and availability bias (the tendency to overestimate the probability of events that are easily remembered).
Systemic Factors: The Context of Health Care
- Organization of the Health System: The way the healthcare system is organized and managed can influence patient safety. Lack of clear protocols, fragmentation of care, lack of continuity of care, and lack of adequate supervision can increase the risk of errors. Additionally, pressure to reduce costs and increase efficiency can lead to work overload and staff reduction, which can compromise the quality of care.
- Lack of Resources: Lack of human, material and financial resources can limit the ability of healthcare professionals to provide safe, quality care. Staff shortages can lead to work overload and burnout, while a lack of adequate medical equipment and supplies can make diagnosis and treatment difficult.
- Inadequate Technology: Medical technology, while it can improve the efficiency and accuracy of care, can also be a source of errors if not used appropriately. Lack of training in the use of new technologies, lack of interoperability between different information systems and technical failures can contribute to medical errors.
Patient-Related Factors: The Importance of Active Participation
- Lack of Adherence to Treatment: Treatment adherence refers to the degree to which patients follow medical recommendations. Non-adherence can be due to a variety of factors, such as lack of understanding of instructions, medication side effects, financial barriers, or lack of social support. Non-adherence can lead to complications and the need for additional treatments, increasing the risk of errors.
- Poor Communication: Effective communication between patients and healthcare professionals is essential to ensure safe and quality care. Patients should feel comfortable asking questions, expressing concerns, and sharing relevant information about their medical history and symptoms. Lack of communication can lead to misunderstandings, misdiagnoses, and inappropriate treatments.
- Lack of Understanding: Patients may have difficulty understanding complex medical information, which may impact their ability to make informed decisions about their health and follow treatment recommendations. Lack of understanding can be due to a variety of factors, such as the use of medical jargon, lack of appropriate educational materials, or language or cultural barriers.
Diagnostic Error: Definition and Types
- Missed or missing diagnosis: When no explanation is found for the patient's symptoms, despite the diagnostic tests performed.
- Wrong diagnosis: When the initial diagnosis turns out to be incorrect and the true cause of the symptoms is discovered later.
- Delayed diagnosis: When the correct diagnosis is established, but with a significant delay that may have negatively affected the patient's prognosis or treatment.
Factors of Diagnostic Error in Medicine
I. Cognitive Factors
-
Cognitive BiasesCognitive biases are systematic tendencies in thinking that can lead to deviations from rational judgment. In the context of medical diagnosis, some of the most common biases include:
- ∘
- Confirmation bias: The tendency to search for, interpret and remember information that confirms preconceived hypotheses, ignoring or minimizing information that contradicts them.
- ∘
- Anchor bias: The tendency to rely excessively on the first information received, even if it is incomplete or inaccurate, and to insufficiently adjust the diagnosis as new information becomes available.
- ∘
- Availability bias: The tendency to overestimate the probability of diseases that are easier to remember or have been encountered recently, which can lead to missing less common diagnoses.
- ∘
- Overconfidence bias: The tendency to overestimate one's own diagnostic capacity and underestimate the possibility of error.
-
HeuristicsHeuristics are mental shortcuts that allow doctors to make quick decisions in situations of uncertainty. Although they can be useful in clinical practice, they can also lead to errors if applied inappropriately. Some examples of heuristics include:
- ∘
- Representativeness heuristic: The tendency to diagnose a disease based on the similarity of the patient's symptoms to a typical case, without adequately considering other possibilities.
- ∘
- Availability heuristic: The tendency to diagnose diseases that are more common or have been found recently, without adequately considering the actual prevalence of the disease in the population.
-
Limitations of Human ReasoningIn addition to biases and heuristics, human reasoning has inherent limitations that can contribute to diagnostic errors. These limitations include:
- ∘
- Limited information processing capacity: Clinicians must process large amounts of clinical information in a short period of time, which can lead to errors due to cognitive overload.
- ∘
- Fatigue and stress: Fatigue and stress can affect attention span, memory, and judgment, increasing the likelihood of errors.
- ∘
- Lack of knowledge or experience: Doctors can make diagnostic errors if they do not have the knowledge or experience necessary to recognize a particular disease.
II. Systemic Factors
- Lack of Time: Healthcare pressure and lack of time in medical consultations are important factors that can lead to diagnostic errors. Physicians often have to care for a large number of patients in a limited time, which can make it difficult to take a complete history and physical examination, as well as consider all possible diagnostic hypotheses.
- Assistance Pressure: The pressure of care, especially in emergency departments or during times of high demand, can increase the stress and fatigue of doctors, which can affect their diagnostic ability. Furthermore, the need to make quick decisions in emergency situations can lead to errors due to lack of reflection and analysis.
- Poor Communication: Poor communication between different health professionals caring for the same patient can be an important cause of diagnostic errors. Failure to share relevant information, misinterpretation of test results, or lack of coordination in patient follow-up can lead to delays in diagnosis or misdiagnoses.
III. Patient Related Factors
- Complexity of the Cases: Some patients present with complex or atypical clinical symptoms, which can make diagnosis difficult. Rare diseases, unusual presentations of common diseases, or the presence of comorbidities can increase diagnostic uncertainty and the probability of error.
- Comorbidities: The presence of multiple diseases or medical conditions in the same patient can complicate the diagnostic process. Interactions between different diseases, overlapping symptoms, and difficulty distinguishing the effects of each disease can lead to diagnostic errors.
- Training and training in clinical reasoning and decision making: Clinicians should receive ongoing training in clinical reasoning skills, including the identification and mitigation of cognitive biases.
- Improved communication and teamwork: It is essential to promote effective communication and fluid collaboration between the different health professionals who care for the same patient.
- Use of diagnostic support tools: Checklists, decision support systems, and other tools can help doctors structure the diagnostic process and reduce the likelihood of errors.
- Patient participation in the diagnostic process: Patients should be informed and empowered to actively participate in their own care, including communicating their symptoms and concerns, and reviewing test results.
- Improvement of the organization of the health system: Systemic factors that contribute to diagnostic errors, such as lack of time, pressure of care, and poor communication, need to be addressed.
Addressing Contributing Factors: Toward Safer Health Care
- Communication Improvement: Encourage open and effective communication between members of the healthcare team and between professionals and patients. This involves using clear and understandable language, actively listening, checking understanding, and encouraging patient participation in decision-making.
- Training and Training: Provide ongoing training to healthcare professionals on patient safety, effective communication, teamwork and error management. Training in clinical reasoning and decision-making skills can also help reduce cognitive biases and improve diagnostic accuracy.
- Optimization of Health Systems: Improve the organization and management of the health system, guaranteeing the availability of adequate resources, the implementation of clear protocols and continuity of care. Foster a culture of safety in which mistakes are seen as opportunities for learning and improvement, rather than cause for blame or punishment.
- Technology Implementation: Use technology effectively to improve patient safety, such as implementing electronic clinical information systems, early warning systems, and decision support tools.
- Patient Empowerment: Encourage the active participation of the patient in their care, providing clear and understandable information about their disease and its treatment, and promoting adherence to treatment.
Overdiagnosis and Its Implications
Diagnostic and Therapeutic Cascades
Diagnostic Error in Primary Care
The Impact of Diagnostic Error on Health
Consequences for the Patient's Health
- Increased morbidity: Morbidity refers to the presence of a disease or medical condition. Diagnostic errors can increase morbidity by delaying the initiation of appropriate treatment, which can lead to long-term complications and sequelae. For example, a late diagnosis of cancer can reduce the chances of survival and increase the risk of metastasis.
- Increased mortality: In severe cases, diagnostic errors can have fatal consequences. A study published in the British Medical Journal estimated that medical errors, including diagnostic errors, are the third leading cause of death in the United States.
- Decreased quality of life: Even when not fatal, diagnostic errors can significantly affect a patient's quality of life. Chronic pain, disability, anxiety and depression are just some of the possible long-term consequences of a misdiagnosis or delayed diagnosis.
Emotional and Psychological Consequences
- Anxiety and stress: Uncertainty and the lack of a clear diagnosis can generate high levels of anxiety and stress. Prolonged waiting for a diagnosis or receiving a misdiagnosis can be emotionally draining experiences.
- Depression: The diagnosis of a serious illness or the lack of effective treatment can lead to depression. Additionally, the feeling of having been ignored or mistreated by the healthcare system can contribute to feelings of hopelessness and sadness.
- Loss of confidence in the health system: A diagnostic error can erode patient trust in health professionals and the system in general. This can make it difficult to seek medical care in the future and affect the doctor-patient relationship.
- Impact on family relationships: An erroneous or late diagnosis can generate tensions and conflicts within the family. Family members may experience feelings of guilt, frustration, and helplessness as they watch their loved one suffer without a clear diagnosis or effective treatment.
Economic Impact
- Additional medical expenses: Misdiagnosis or late diagnosis can lead to unnecessary tests and treatments, increasing medical expenses for the patient and the healthcare system.
- Loss of productivity: Undiagnosed or misdiagnosed illnesses can lead to decreased work productivity, resulting in loss of income for the patient and their family.
- Litigation costs: In some cases, diagnostic errors can lead to medical negligence claims, resulting in legal and compensation costs for healthcare professionals and healthcare institutions.
- Burden on the health system: Diagnostic errors can increase the demand for health services, which can overload the system and affect the care of other patients.
| Consequence | Description |
| Patient harm | It can manifest as physical harm, such as injuries or health complications, or as psychological harm, such as anxiety, depression, or loss of trust in the health system. |
| Delay or avoidance of appropriate treatment | A wrong or late diagnosis can lead to the patient not receiving the necessary treatment in time, which can aggravate their condition and decrease their chances of recovery. |
| Unnecessary or dangerous treatment | An incorrect diagnosis can result in the administration of treatments that the patient does not need, which may be ineffective or even harmful to their health. |
| Psychological repercussions | A diagnostic error, especially a serious one, can have a significant emotional impact on the patient and their families, including anxiety, depression, post-traumatic stress, and loss of trust in health professionals. |
| Financial implications | Medical errors can result in additional expenses for the patient and their family, such as additional treatment costs, loss of income due to inability to work, and legal expenses in the event of malpractice lawsuits. |
| Malpractice Lawsuits | Patients affected by medical errors can file legal claims against the healthcare professionals or institutions involved, seeking compensation for damages suffered. |
| Impact on the reputation of the professional and the institution | Medical errors, especially if made public, can damage the reputation of the healthcare professional and the institution where the error occurred, which can affect the trust of patients and the community at large. |
Strategies for Preventing Diagnostic Errors
Improved Doctor-Patient Communication
- Active listening: The doctor must pay full attention to the patient, avoiding interruptions and demonstrating genuine interest in their history and concerns.
- Open-ended questions: The use of open-ended questions allows the patient to express their symptoms and concerns in their own words, providing valuable information for diagnosis.
- Clear and simple language: Avoid the use of medical jargon and explain medical concepts in terms understandable to the patient.
- Empathy and validation: Recognize and validate the patient's emotions, demonstrating understanding and support.
- Shared decision making: Involve the patient in the decision-making process, explaining the different treatment options and their risks and benefits, and respecting their preferences and values.
Education and Training in Clinical Reasoning and Decision Making
Use of Diagnostic Support Tools
Clinical Importance
Implementation of Error Notification and Learning Systems
Patient Participation in the Diagnostic Process
Ethical Considerations in the Prevention and Management of Medical Errors
The Importance of Transparency and Open Communication with the Patient
- Reduce anxiety and uncertainty: Knowing what happened and why can help the patient better understand their situation and feel more in control.
- Facilitate informed decision making: Knowing the consequences of the error and the available treatment options allows the patient to make informed decisions about their care.
- Strengthen the doctor-patient relationship: Honesty and transparency can foster trust and mutual respect, which is essential for an effective therapeutic relationship.
- Relieve emotional burden: Admitting a mistake and apologizing can help a doctor deal with guilt and prevent burnout.
- Encourage learning and improvement: Recognizing errors and analyzing their causes can help doctors learn from them and take steps to prevent future errors.
- Improve reputation: Honesty and transparency can strengthen patients' trust in the doctor and the health institution.
The Physician's Duty to Report Errors and Their Consequences
Nursing, Allied Health, and Interprofessional Team Interventions
- Avoid scheduling long periods of wakefulness. Long shifts with more than 17 hours of wakefulness can negatively affect task performance, which is equivalent to the legal limit for alcohol intoxication.
- Avoid scheduling more than 4 consecutive 12-hour shifts.
- Avoid short rest periods. Rest periods of less than 8 hours can cause excessive fatigue during the next shift.
- Avoid extending work hours beyond what was previously scheduled for the day.
Improve Healthcare Team Outcomes
The Role of Ethics Committees in the Management of Medical Errors
Functions of the Ethics Committees
- Protection of Human Rights: Ethics committees are essential to protect the rights of patients and ensure that medical practices are carried out ethically. Its creation is justified by the need to legislate on the use of human organs and critical end-of-life decisions, which highlights its role in preventing abuses and errors in medical care.
- Evaluation of Research Projects: Health research ethics committees are responsible for evaluating projects to ensure the protection of participants and scientific integrity. This includes reviewing research protocols that could be related to medical errors, ensuring that ethical practices are followed and that risks to patients are minimized[5,8].
- Confidence Building: These committees not only address ethics in research, but also foster trust between healthcare professionals and patients. By establishing a framework for ethical discussion, committees help resolve conflicts and make consistent decisions, which is essential for the management of medical errors.
- Independence and Autonomy: The independence of ethics committees is crucial to their effectiveness. They must operate without outside influences to fairly evaluate cases of medical errors and ensure that decisions are made based on sound ethical principles.
Legal Liability for Diagnostic Errors: A Legal Analysis
- Negligence: Omission of due diligence. That is, the doctor does not do what he should do according to the standards of the profession. For example, not performing the necessary diagnostic tests for the patient's symptoms.
- Imprudence: Hasty or reckless action, without taking due precautions. For example, performing a medical procedure without having the necessary training or experience.
References
- **Instituto de Medicina.** (1999). *To Err is Human: Building a Safer Health System*. Washington, DC: National Academy Press.
- **Organización Mundial de la Salud.** (s.f.). *Estimaciones sobre errores médicos*.
- **Sociedad para Mejorar el Diagnóstico en Medicina (SIDM).** (s.f.). *Clasificación de los errores de diagnóstico*.
- **British Medical Journal.** (s.f.). *Estudio sobre errores médicos en Estados Unidos*.
- **Instituto de Medicina (IOM).** (s.f.). *Informe sobre la fatiga durante el trabajo por turnos*.
- **Academias Nacionales de Ciencias, Ingeniería y Medicina de los Estados Unidos.** (s.f.). *Recomendaciones para la transferencia de pacientes*.
- **Instituto de Medicina (IOM).** (s.f.). *Recomendaciones para la programación de turnos de enfermería*.
- **Instituto de Medicina.** (2001). *Crossing the Quality Chasm: A New Health System for the 21st Century*. Washington, DC: National Academy Press.
- **World Health Organization.** (2019). *Global Patient Safety Action Plan 2021–2030*. Geneva: WHO.
- **Agency for Healthcare Research and Quality.** (2020). *Patient Safety: Achievements and Challenges*. Rockville, MD: AHRQ.
- **National Institute for Health and Care Excellence.** (2021). *Patient Safety and Quality Improvement*. London: NICE.
- **American Medical Association.** (2022). *Addressing Medical Errors: A Guide for Physicians*. Chicago, IL: AMA.
- **Institute for Healthcare Improvement.** (2023). *Reducing Medical Errors: Strategies for Improvement*. Cambridge, MA: IHI.
- **European Commission.** (2023). *Patient Safety in Europe: Current Challenges and Future Directions*. Brussels: EC.
- **Canadian Patient Safety Institute.** (2023). *Safer Healthcare Now!: A National Patient Safety Initiative*. Edmonton, AB: CPSI.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



