Submitted:
24 January 2025
Posted:
24 January 2025
You are already at the latest version
Abstract
In recent decades, the world has observed the emergence and reemergence of a multitude of previously non-existent or re-emerging infectious diseases, for which there is a paucity of timely and effective preventative measures. The WHO has published a catalogue of priority pathogens that are likely to trigger future epidemics, with the objective of designing effective prophylactic and therapeutic interventions. The rationale behind these interventions is rooted in a comprehensive understanding of the aetiology, epidemiology and pathogenesis of the target diseases. While it is imperative to acknowledge the pivotal role that evolutionary changes in pathogens play, it is equally important to recognise the influence of a multifaceted interplay of factors on the emergence and re-emergence of infectious diseases. These include changes in human populations, vectors and reservoirs of exposure, and environmental changes. This review summarises the aetiology, epidemiology and pathogenesis of the ten WHO priority diseases, as well as those with a high epidemic potential that are already the focus of specific control programme initiatives, such as HIV/AIDS, tuberculosis, and malaria diseases. Furthermore, the review concentrated on the means of addressing these infections through public health surveillance and response systems. Such systems must be designed to rapidly detect unusual and unexpected disease patterns, track and share information in real time, and rapidly mobilise global responses, which are the most important way to effectively contain transmission.
Keywords:
Priority diseases
; Infection Control
; Public health emergencies
1. Introduction
Infectious diseases have exerted a profound influence on the development of humanity [1]. The introduction of measures such as sanitation, improved nutrition, vaccines, and antimicrobials has led to the erroneous belief that humanity has definitively triumphed over pathogens, or that the risk of infection is confined to underdeveloped nations [2]. However, the assertion that the risk of infection is exclusive to developing nations is demonstrably erroneous, given the persistence of both emerging and re-emerging infectious epidemics [3]. 'Emerging and re-emerging infectious diseases' refer to two categories. Newly emerging infections are caused by novel pathogens. Re-emerging infectious diseases are caused by microorganisms resurging after a period of decline [4]. According to the CDC, diseases of infectious origin are defined as those which have either increased in incidence among the human population within the past two decades, or which are likely to do so in the future [3]. From an epidemiological perspective, infectious diseases exhibit different spread characteristics [5]. An epidemic is defined as the frequent and localised, albeit time-limited, manifestation of an infectious disease, which occurs when there is an increase, often sudden, in the frequency of cases beyond what is normally expected within a population [6]. In contrast, the term pandemic originates from the Greek pân, which means all, and dêmos, which means people, and signifies the widespread dissemination of a disease across multiple continents or, in more expansive terms, over vast geographical areas of the world [7]. The most recent pandemic was declared by the WHO on 11 March 2020 for the new strain of Coronavirus (SARS-CoV-2) [8]. In recent decades, the global community has experienced several outbreaks and re-emergences of infectious diseases, posing significant challenges to global health security and the global economy. Notable epidemics that have emerged include: SARS (severe acute respiratory syndrome) which emerged from China in 2002, H1N1 swine flu, a pandemic that originated from Mexico in 2009 and Middle East respiratory syndrome (MERS), which first emerged from Saudi Arabia in 2014 [9,10,11]. In addition to the aforementioned epidemics, the following diseases have also caused significant global health concerns: Ebola virus disease (2013–2016), Zika virus (2015), Lassa virus (2018), Marburg virus disease (2018), Crimean–Congo haemorrhagic fever (2022) and Rift Valley fever (2019) [12,13,14,15,16]. In addition to the above diseases, it is also important to consider other deadly infectious diseases, which, especially in low-income countries, claim millions of victims worldwide every year. These include HIV/AIDS, tuberculosis and malaria [17]. Despite significant advancements in the field of medicine and public health, these diseases continue to pose significant challenges, particularly in low-income regions. Within the context of low-income nations, the predominant causes of mortality are infectious and parasitic diseases; in contrast, in high-income nations, non-communicable diseases such as heart disease and cancer prevail as the leading causes of death [18,19,20]. In this review, the focus is on three key factors that contribute to the emergence and re-emergence of infectious diseases. These factors are as follows: the agent, defined as the microbial risk; the host, defined as the human vulnerability; and the environment, defined as the human exposure [21,22]. The aforementioned factors include genetic, biological, social and economic elements. The most significant of these determinants are as follows: international trade and commerce, human susceptibility to infection, poverty and social inequality, war and famine, changing ecosystems and microbial change. Furthermore, the identification of the most efficacious courses of action to guide prevention and control strategies is imperative [22]. The enhancement of global surveillance, the utilisation of vaccines, the development of novel pharmaceuticals, the optimisation of vector and zoonotic control, and the dissemination of health education on a more extensive scale are some potential solutions to this issue.
2. Emerging and Reemeerging Infectious Diseases: How and Why They Arise
Epidemics are a natural phenomenon in the context of human history. Despite the fact that infectious diseases have had a profound impact on the course of human history, the collective memory of these diseases remains limited. This is due to the rarity of pandemics [23]. Two notable examples are the Spanish flu pandemic of 1918-1920, which resulted in an estimated 40 million deaths worldwide, and the more recent pandemic, the global novel coronavirus crisis (SARS-CoV-2), which will result in approximately 6.7 million deaths between 2020 and 2022 [24]. Historical analysis indicates that the majority of infections have emerged over millennia, coinciding with the rise and evolution of interactions between humans, animals and their environment [25]. The emerging and re-emerging of infectious diseases has been shown to be a multifaceted phenomenon [3,4]. The three main factors which have been identified in the literature as contributing to this phenomenon are as follows: 1) the agent or microbial hazard; 2) the host, defined as the human being or organism susceptible to infection; and 3) the environment, understood as the physical or biological context in which human exposure to pathogens occurs [26] (Figure 1). It is estimated that between 60% and 80% of emerging infections are of animal origin, suggesting that zoonotic origin is a significant source of emerging diseases [27]. Through close contact with diseased animals carrying a potentially emerging pathogen, humans are susceptible to direct infection. Alternatively, indirect infection may occur through a vector or by ingestion of contaminated water and food. In this respect, the way in which water and food are procured, stored or processed has a decisive influence on the transmission process [28,29]. Evolutionary changes in pathogens represent a pivotal element in the emergence of diseases, exerting influence on characteristics such as species-specificity, geographical distribution, clinical manifestations (including virulence or immune evasion), transmission modalities, and resistance to therapeutic interventions [30,31] (Figure 1). The evolutionary process of a pathogen may involve a range of genetic alterations, including single nucleotide substitutions, gene acquisition from other organisms, and recombination and reassortment events [32]. These evolutionary changes can influence various epidemiological outcomes, such as spillover and outbreak occurrences. The selective pressure exerted by antimicrobials has led to the emergence of bacteria and parasites that are resistant to such agents [33,34]. Furthermore, pathogens with a high mutation rate can lead to the rapid evolution of new variants. This phenomenon is particularly evident in RNA viruses, including influenza, flavivirus and coronavirus, which are distinguished by their high genetic variability and consequent impact on vector and/or host competence, resulting in significant consequences for their dissemination among human populations [35,36,37,38]. In addition to the evolution of pathogens, the emergence and re-emergence of infectious diseases is influenced by a multifaceted interplay of factors, which can be conceptualised as the human environment [21] (Figure 1). A multitude of factors exert a substantial influence on the emergence of such diseases, many of which are also subject to the impact of other conditions. These include, but are not limited to, the processes of globalisation, climate change, urbanisation and population growth, which can lead to the concentration of populations in urban areas characterised by inadequate sanitation [39]. Additional host-related variables worthy of note include demographic shifts, such as an aged population and an increase in immune-compromised individuals [39,40].
3. Pathogens with Epidemic and Pandemic Potential
3.1. Zika Virus
The Zika virus (ZIKV) belongs to the genus Flavivirus. This enveloped, single-stranded RNA arbovirus was first isolated from a rhesus monkey in the Zika forest in Uganda in 1947 [41]. The virus was then isolated in the Aedes africanum mosquito in the same location the following year (1948) [42]. For the following several decades after its discovery, only sporadic and mild cases of infection were reported in Asia and Africa. Nevertheless, the first major outbreak occurred in 2007 outside of the African continent, taking place in the Yap Islands of Micronesia (Pacific Islands) [43]. This was followed by significant further outbreaks in French Polynesia (2013) and Brazil (2015), thus confirming the virus's ability to emerge and spread among the human population [44]. The majority of ZIKV infections are asymptomatic, or mild and non-specific. Manifestations may include fever, arthralgia, rash and conjunctivitis [45]. These generally resolve within 2-7 days although, in certain cases, more severe manifestations may emerge. ZIKV is transmitted through the bite of an infected mosquito. The Aedes genus of mosquito is responsible for the transmission of the Zika virus (ZIKV) on various continents. ZIKV is transmitted by mosquitoes in two cycles: the sylvatic cycle and the urban cycle. In this latter cycle, the main vector of ZIKV is the Aedes aegypti and Aedes albopictus species. The transmission of infection is facilitated by the feeding of the vector on infected humans and subsequent dissemination of virus to other humans and mosquito populations [46]. However, in comparison with other arboviruses, ZIKV infection has been shown to involve additional transmission routes, including infected blood transfusion, sexual transmission and materno-fetal transmission. The Zika virus has been found in semen, indicating potential sexual transmission even where there are no Aedes mosquitoes [47]. Vertical transmission has also been confirmed, linking ZIKV infection to neonatal neurological complication. During the outbreak in Brazil, the Zika virus spread rapidly and led to an unexpected rise in the number of children born with microcephaly [48]. Furthermore, several countries, including Brazil, have reported a significant increase in Guillain-Barré syndrome and other neuronal disorders among adult patients infected with the Zika virus [48]. Consequently, in February 2016, the WHO formally declared this association of Zika infection with clusters of microcephaly to be a Public Health Emergency of International Concern [49]. WHO has classified the Zika virus as a priority because of its links to congenital defects and neurological impairments. However, there are also concerns about its potential for epidemics due to its widespread and abundant presence of Aedes spp. Vectors [50]. The spread of ZIKV is being driven by several key factors including poverty, inadequate/damaged infrastructure, deforestation, urbanisation and climate change [49]. It's possible that the virus's affinity with the urban vector, A. aegypti, and the efficiency of urban transmission between humans has been affected by an adaptive evolutionary process. This would explain the total absence of a ZIKV epidemic before 2007 [51]. The virus's spread is challenging to predict, making planning difficult. The complexity of the virus's epidemiology and transmission dynamics poses significant challenges in predicting future outbreaks and epidemics. The WHO has has issued a call to the global research communities, urging them to prioritise the development of vaccines, improved diagnostics and innovative vector control strategies.
3.2. SARS-CoV-2
Coronavirus disease (Covid-19) is an infectious disease from a new type of coronavirus (CoV), called severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) [52]. The initial cases of the as yet unidentified respiratory illness were reported on 8th December 2019 in Wuhan, China. Local health authorities in China identified an outbreak of pneumonia of unknown origin in Wuhan. The disease then spread to several other countries, leading to the declaration of a Public Health Emergency of International Concern by the WHO on 31st January 2020 [52]. The disease then spread rapidly, resulting in significant mortality, and was characterised by the WHO as a pandemic. SARS-CoV-2 is an enveloped virus with a single-stranded positive-sense RNA genome. It belongs to the Betacoronavirus genus and the Coronaviridae family. Betacoronaviruses cause infections in a wide range of mammals [52]. Like other coronaviruses, they have a high mutation frequency and significant recombination events. This allows them to 'jump' from one species to another. Epidemiological studies suggest the Huanan Seafood Market in Wuhan was the early epicentre of SARS-CoV-2 infection due to its proximity to various animals. This is based on the similarity between SARS-CoV-2 and bat or pangolin CoVs [53]. It is thought that the pangolin may have acted as an intermediate host in the evolution of the virus, increasing its zoonotic potential and transmissibility [3]. As the virus replicates and spreads among humans, new variants such as Alpha, Beta, Delta, and Omicron have been detected, confirming the high mutation capacity of SARS-Cov2 and posing new challenges in controlling the pandemic. SARS-CoV-2 is transmitted primarily through close contact with respiratory droplets from an infected person's mouth or nose. Given the ability of the virus to resist on inanimate surfaces such as plastic, stainless steel, cardboard and copper, the transmission can also occur by touching an infected surface, and subsequently touching the eyes, nose or mouth [54]. The virus can cause a range of symptoms, including fever, cough and fatigue, which can progress to severe respiratory disease. However, some patients may experience no respiratory symptoms at onset and exhibit extra-pulmonary manifestations, including headache, diarrhea, and vomiting [55]. SARS-CoV-2 infection can affect people of all ages, but the highest morbidity and mortality rates are observed in individuals over 65 years old or with other comorbidities (hypertension, diabetes, cardiovascular disorders, respiratory diseases), often requiring hospitalization and intensive care [55]. The WHO has identified Covid-19 as a priority disease due to its potentially devastating consequences. The potential pandemic of the SARS-CoV-2 has resulted in a rapid global spread of the virus, leading to an overload of health systems ill-prepared for an emergency of such magnitude [56]. The consequences resulting from the rapid transmission of the virus have been numerous. Healthcare facilities throughout the country have experienced critical shortages of personal protective equipment and ventilators, especially for patients exhibiting severe symptoms requiring intensive treatment [57]. Furthermore, the virus's capacity for mutation has engendered the development of new variants that have the potential to compromise vaccine efficacy or disease severity, necessitating ongoing global vigilance and representing a matter of urgent concern to the WHO [58]. The pandemic has had far-reaching consequences for public health, the economy and society [57]. Lockdowns, travel restrictions and quarantine have reduced SARS-CoV-2 transmission but but these measures have concomitantly precipitated profound economic adversities for millions of individuals worldwide [58].
3.3. Middle East Respiratory Disease (MERS) and Severe Acute Respiratory Syndrome (SARS)
Middle East Respiratory Disease (MERS), and Severe Acute Respiratory Syndrome (SARS) are two respiratory diseases caused by two viruses belonging to the Betacoronavirus genus [59]. MERS, first detected in Jordan in 2012, has had two major outbreaks: in 2013 in Saudi Arabia, and in 2015 in South Korea [60]. Most patients are severely ill, with a fever, cough, and shortness of breath. There's currently no available vaccine or specific treatment. Treatment is therefore supportive [61]. According to the WHO, 2613 cases of Middle East respiratory syndrome (MERS) have been reported since April 2012. Most cases have been reported from the Arabian Peninsula, with 943 deaths (case-fatality ratio 36% – the highest among all coronaviruses) [62]. In recent times, there have been sporadic imported cases in Europe, North America, Africa, and Asia. MERS-CoV is transmitted between humans less often than other coronaviruses, but sporadic outbreaks still occur [63]. The virus is traced back to bats, with dromedary camels serving as intermediate hosts. These camels are a primary source of MERS-CoV transmission to humans [64]. Other livestock species, including wildlife, can also spread MERS-CoV. Humans can contract the virus from camels, through airborne transmission, or by eating contaminated milk and meat [65].
The first cases of SARS were identified among animal handlers in Guangzhou [66]. These individuals had been in close contact with wild game meat and subsequently infected healthcare workers. The first cases were reported in November 2002 in Guangdong, China, representing the first instance of severe human illness caused by a coronavirus [66]. The virus was traced back to bats and civets, with the spread to humans via both animal-to-human and human-to-human transmission, leading to its global spread [67].
Stringent public health measures, including quarantine and travel restrictions, led to the containment of the disease by 5th July 2003 [68]. By its conclusion, 8,422 cases had been documented by the CDC and WHO, resulting in 916 deaths in 29 countries [10]. The exact means of transmission is unclear, but it is hypothesised that airborne droplets from infected patients may be the primary vector. SARS can cause pneumonia and respiratory failure, often leading to mortality [69]. Both SARS-CoV and MERS-CoV are a global health threat because they can spread quickly and lots of people die [70]. MERS-CoV is more deadly, but its spread has been more restricted. Both viruses have animal reservoirs, which can lead to new variants and outbreaks [70]. We need to understand how these viruses jump from animals to humans, and have better countermeasures – including safe and effective vaccines and therapies – in place, to stop a potential health crisis. The emergence of two highly pathogenic coronaviruses within ten years highlights the need for constant pandemic preparedness. This means that governments, health officials, and international agencies must remain vigilant to detect and respond to cases.
3.4. Ebola Virus Disease and Marburg Virus Disease
Ebola is a rare and serious illness caused by a filovirus. First reported in 1976 in South Sudan and the Democratic Republic of Congo, it takes its name from a village built near the Ebola river [71]. Since then, sporadic outbreaks have occurred, especially in Africa, where it is a serious public health problem. Guinea, Sierra Leone and Liberia accounted for the highest number of deaths (28,000 cases, 11,000 deaths) between 2014 and 2016 [72]. The virus is transmitted through direct contact with mucous membranes or wounds of infected individuals, and through contact with the bodies of deceased individuals (Ebola virus can also resist post-mortem infection) [73]. The Ebola virus can also be spread through contact with contaminated objects or surfaces, or through contact with infected wild animals. The natural reservoir of the virus is believed to be fruit bats [74]. Ebola can persist in the blood of survivors and can last for months or years [73]. The precise mechanisms of resistance remain to be fully elucidated; however, emerging evidence suggests a potential role for macrophages. Notably, pregnant women who have recovered from Ebola appear to transmit the virus to their infants through breast milk, underscoring the complexity of viral transmission dynamics. These characteristics influence the occurrence of epidemics, which are likely generated by survivors infecting susceptible individuals [3]. Initial non-specific symptoms (2-21 days post-infection) overlap with those of numerous ailments. These are then followed by vomiting, diarrhea, skin rashes and sudden bleeding. Severe cases may lead to multi-organ failure, immunological disorders, shock and death. The wide spectrum of symptoms makes differentiation of Ebola virus disease challenging [3]. The main diagnostic methods are ELISA and RT-PCR assays. The treatment of the disease involves the administration of monoclonal antibodies in combination with other therapeutic interventions. Currently, two authorised vaccines are in use. Despite the significant reduction in mortality rate from EVD that has been observed with the administration of monoclonal antibodies (mAbs), the overall case fatality rate remains high at 30% [75].
Marburg virus disease (MVD) is a hemorrhagic fever caused by a filovirus. First identified in 1967 between Germany and present-day Serbia, the most recent outbreak occurred in Guinea in 2023 [76]. It is linked to caves and the habitat of the Rousettus aegyptiacus bat, and has symptoms and fatality rates comparable to those of the Ebola virus [76]. These viruses can spread quickly and easily because they are very deadly, can lie hidden in the body for a long time, spread after healing and do not have specific medicines. The WHO therefore considers them a priority [77]. It is very important for people to take part in stopping the spread of disease by being clean, staying away from infected people and safe funeral practices. The WHO's strategy for monitoring and searching for these viral agents is based on anticipation, reinforcement and cure [77]. There is no approved MVD vaccine; several are in clinical trials [78].
3.5. Crimean-Congo Haemorrhagic Fever
Crimean-Congo haemorrhagic fever (CCHF) is caused by a virus from the Nairovirus genus. It was discovered in Crimea in 1944 and in a Congolese child in 1956 [79]. The virus spreads to humans via tick bites or through contact with infected tissues/blood/body fluids, especially during breeding and slaughter. It infects many different types of wild and domestic animals. Since it can spread without symptoms, it is more infectious among animals than humans, and those involved in breeding, slaughter and veterinary work are the most affected [80].
The lethality rate of this disease is between 10 and 40%. The virus is endemic in Africa, Asia, the Balkans and the Middle East. The last outbreak was described in Iraq in 2022 [81]. The disease has a sudden onset with non-specific symptoms. The incubation period after tick bite is between one and three days (nine max) and between five and six days after contact with infected tissue. Initially, there is fever, headache, dizziness, nausea, muscle pain and stiffness, and sensitivity to light [82]. Next comes the hemorrhagic phase, marked by swelling of the liver, skin and mucus membranes, bleeding from eyes, noses and gums, and blood in the feces and urine. Intravascular coagulopathy and cardiogenic shock can lead to an unfavourable outcome [82]. The disease is diagnosed microbiologically using ELISA and RT-PCR assays. However, in the early stages, patients do not develop an antibody response, so the diagnosis is made by detecting virus RNA in the blood [82]. There is currently no specific therapy or effective vaccine for CCFH. The only possible means of reducing the infection in people is through basic preventive measures [82]. The intricate nature of infection control in animals and ticks, the often-challenging detection of the tick-animal-tick cycle, and the prevalence of asymptomatic animals, underscores the complexity of the disease dynamics.
3.6. RIFT VALLEY FEVER (RVF)
Rift Valley Fever (RVF) is a viral zoonosis transmitted by mosquitoes. It was discovered in 1931 and has since caused sporadic epidemics in Africa, Madagascar, Saudi Arabia and Yemen [83]. A severe epidemic was reported in Kenya, Somalia and Tanzania in 1997-98. The disease is endemic to domestic ruminants and is caused by an arbovirus belonging to the genus Phlebovirus (family Bunyaviridae). The disease has caused significant economic losses due to the death and/or abortion of infected animals. The virus is spread among animals by mosquitoes of the Aedes genus, which can also transmit it vertically [83]. Humans can become infected through the bite of infected mosquitoes or by direct contact with infected animals. There have been a few documented cases of infection resulting from the bite of hematophagous flies [84]. The most at-risk groups are breeders, slaughterers and veterinarians. There is no documented evidence of human-to-human transmission of RVF. The disease can present with mild or severe symptoms, with serious consequences for survivors. The incubation period is 2-6 days. The symptoms of the mild form are comparable to those of influenza or meningitis, and subside after about a week. At this point, an immune response becomes evident. Severe syndromes, on the other hand, may manifest as isolated episodes or concurrently. The severe ocular form affects the macula, causing blindness in half the patients. The meningoencephalitis form causes hallucinations, disorientation, confusion and coma, leading to severe neurological deficits in survivors [85]. The hemorrhagic form causes severe liver failure, frequent bleeding and a 50% mortality rate. These syndromes manifest one to three weeks after symptoms first appear.
RVF has non-specific clinical symptoms, so RVF is investigated using RT-PCR, antigen detection tests or viral isolation. Antibodies are only detectable five to six days after onset [84]. Viral isolation, a common concern in all priority diseases, is difficult because it is highly biohazardous. This necessitates the use of laboratories with cutting-edge biocontainment capabilities, as this viral agent poses a serious threat as a biological weapon. The disease causes mild symptoms in humans and is short-lived, with no specific treatment available. In severe cases, intensive care and management are required; the most effective method of preventing the spread of the disease is vaccination of cattle and strict adherence to safe husbandry and slaughter practices. A vaccine for humans is available but not authorised or available to buy [83]. Rainy periods are causing more cases of RVF, so we need better forecasting models to stop outbreaks in animals and humans.
3.7. LASSA FEVER
Lassa fever is a viral hemorrhagic fever caused by a virus belonging to the Arenaviridae family. It is endemic to Benin, Guinea, Liberia, Nigeria, Mali, Sierra Leone and Togo [85]. The precise incidence of infection is uncertain; however, it is estimated that cases range from 30,000 to 50,000 per year. The estimated mortality rate falls within the range of 5,000 and 10,000, resulting in an estimated annual mortality rate of approximately 1 per cent (although it has been observed to reach as high as 15 per cent in hospitalised patients suffering from serious illnesses) [86]. The natural reservoir for the infection is the multimammate mouse. The prevalence of the disease in Africa is such that its eradication is impracticable. Humans contract the disease through contact with these rodents. Although rare, human-to-human transmission can occur through contact with blood or body fluids [86]. Unlike other haemorrhagic fevers, the onset of Lassa fever is gradual. The incubation period is the duration between infection and the onset of symptoms and can vary between 2 and 21 days. Initial symptoms are comparable to those of numerous other syndromes and include fever, general weakness and malaise. These are followed by additional symptoms such as sore throat, abdominal and chest pain, vomiting and diarrhoea. In severe cases, the disease can cause facial swelling, lung swelling, and internal bleeding. Recovery from Lassa fever is slow. Patients must be closely monitored for Lassa fever sequelae, which can cause sudden deafness and neurological disorders [87]. Pregnancy increases the risk of complications, with high maternal and fetal mortality in the third trimester. The disease must be microbiologically diagnosed using RT-PCR, enzyme immunoassays or antigen detection. No infection tests are available for this or other hemorrhagic fevers; testing must be done in specialized centers. There are no treatments or vaccines for Lassa fever. As mentioned, controlling the infection reservoir is impossible due to the huge spread of these rodents [88]. The only forms of prevention are hygiene and airtight storage.
3.8. “DISEASE X”
The term 'Pathogen X' is used by the World Health Organization (WHO) to denote a hypothetical virus or bacterium that has the potential to cause a major new epidemic or pandemic [89]. The primary purpose of utilising this term is to encourage both scientists and governments to recognise the possibility of previously unknown microorganisms causing human diseases [89]. This realisation underscores the need for concerted efforts to be made in order to ensure preparedness for such eventualities. The adoption of this approach has the potential to facilitate a more expeditious and efficacious response to health threats, through the implementation of prompt preventative measures and the acceleration of vaccine development and dissemination within a substantially reduced timeframe.
4. Overcoming Challenges: The Neglected Pandemics – HIV/AIDS, Tuberculosis and Malaria
The ten diseases classified as 'priority' by the World Health Organization (WHO) are deemed to be of such concern on account of their pandemic potential and the paucity of existing surveillance systems and specific action plans. Conversely, although surveillance systems and action plans for diseases such as HIV/AIDS, tuberculosis and malaria have been implemented, death and illness rates remain high [90] (Figure 2).
The WHO is working to address these diseases in impoverished communities, but they continue to be a leading cause of mortality in low-income countries. Nevertheless, as a consequence of the Global Fund initiative, which was launched in 2002, significant advances have been made in the reduction of the overall burden of HIV, malaria and tuberculosis. Indeed, the rate of DALYS for these diseases was reduced by 56% between 2000 and 2021 [91]. However, it is evident that we are still far from achieving the objective of stopping these epidemics by 2030, which is part of the specific health goals of the Sustainable Development Goals [92].
4.1. HIV Infection and AIDS
Recent decades have seen notable shifts in the global HIV/AIDS pandemic. Effective antiretroviral therapy, prevention methodologies, and enhanced public consciousness regarding HIV transmission and treatment have contributed to a decrease in new infections and mortality. Globally, 2023 saw an estimated 39.9 million people living with HIV, including 1.4 million children (under 14) and 38.6 million adults (over 15) [93]. Key risk factors include behaviors such as sex with men, being transgender, injecting drugs, sex work, and imprisonment. The most impacted region by HIV is Sub-Saharan Africa, including South Africa, Nigeria, Mozambique and Uganda [94]. Within, there are cultures where subjects relating to HIV and AIDS are often avoided and misconceptions concerning transmission and prevention methods are prevalent. These factors also impede access to healthcare due to stigma and discrimination relating to gender identity, sexuality, prior incarceration and HIV-infected status [94]. The lack of a vaccine and effective treatment means the disease can continue to spread. The development of new strategies to combat the spread of HIV has focused on enhancing data collection by national health services. This is a strategy that can be applied universally to any infection with a similar epidemiology. This approach is particularly relevant for 'key' populations, where the burden of HIV is high and access to health services is often constrained by social stigmatisation [95]. A comprehensive understanding of the habits of these individuals, along with access to their health data and the assurance of their safety, is paramount for the effective prevention and treatment of infections of this nature.
4.2. Malaria's Impact Worldwide
The WHO's World Malaria Report, updated to 2023, states that 263 million cases and 567 thousand deaths were caused by malaria that year [96]. Despite various malaria control programmes, including vector control, chemoprophylaxis, rapid diagnostic tests and timely treatment, malaria remains a significant health problem. The African continent is the most affected, accounting for 95% of cases and 96% of deaths [97]. Following a decline in cases until 2015, there has been a resurgence, partly due to the emergence of artemisinin and insecticide resistance, and the SARS-coronavirus-2 (Covid-19) pandemic. This poses a threat to particularly vulnerable populations such as children under five and pregnant women. However, a vaccine offering moderate protection against malaria was approved in Oct 2021 [98]. Genetic studies on malaria vectors, in conjunction with geographical and environmental analysis of endemic regions, are of pivotal importance in the development of surveillance systems. These systems employ the aforementioned characteristics, in conjunction with other socio-demographic factors, to create useful models for the development of elimination strategies.
4.3. Tuberculosis: Old Disease- New Threat
Tuberculosis is a preventable and treatable disease. In 2023, it re-emerged as the world's leading infectious disease, following a three-year period in which it was overtaken by Coronavirus disease (Covid-19) [99]. It is estimated that tuberculosis caused almost twice as many deaths as HIV/AIDS. In 2023, the global burden of tuberculosis was estimated to be highest in 30 high-burden countries, with India (26%), Indonesia (10%), China (6.8%), the Philippines (6.8%) and Pakistan (6.3%) accounting for 56% of cases. The highest incident rate was observed in Africa [100]. The incidence and mortality of tuberculosis are linked to health coverage and access to services. Individuals identified as being most at risk include those who are imprisoned, displaced, economically disadvantaged, malnourished, HIV-positive, and those experiencing compromised immune systems. Eradicating tuberculosis remains far off, linked to inadequate progress towards universal health coverage [101]. Achieving the full potential of all strategies to halt TB requires universal access to treatment. These diseases are both the consequence and cause of poverty and inequality. Inadequate resources pose a significant threat to populations, leaving them vulnerable to the threat of disease. To eliminate outbreaks, services must be available to all, particularly the poor, and essential medicines and vaccines must be distributed fairly, especially in the most deprived countries [102]. Interventions in the health sector and those aimed at the social and cultural factors behind the diseases can tackle their causes and use health services more effectively.
5. Conflict and Infectious Diseases
A recent analysis of the European Centre for Disease Prevention and Control's (ECDC) Surveillance Atlas of Infectious Disease reveals a worrying trend in the continent's recent outbreak of various infectious pathogens [103]. The atlas documents a resurgence of pathogens that had previously been in circulation, with some showing alarming trends in their prevalence. While certain diseases, including tuberculosis, a leading cause of mortality worldwide, show no signs of abatement, other diseases such as sexually transmitted infections are re-emerging with a resurgence in cases that have doubled or tripled in the post-covid-19 era. In 2023, for instance, the European Union/European Economic Area (EU/EEA) reported 41,051 cases of syphilis, 230,199 cases of chlamydia, 96,969 cases of gonorrhoea, and 28,751 cases of hepatitis C virus infection [104]. In the context of the global spread of infectious diseases, it is imperative to acknowledge the significant yet often overlooked aspect of the numerous conflicts that have occurred and continue to occur in various parts of the world. There is a well-documented and well-evidenced history of the catastrophic consequences of the interconnection of infectious diseases and warfare [105] (Figure 3). It is therefore vital to recognise the relationship between these two phenomena. The advent of war gives rise to a plethora of conditions that engender the propagation of infectious diseases, chiefly by modifying the living conditions of the affected population. The consequences of war for public health are profound, and even infections that are typically preventable through vaccination can become problematic in the context of protracted conflict. This phenomenon is exemplified by the recent measles and hepatitis B epidemics in Syria and Yemen, respectively [106]. The destruction or overcrowding of sanitation facilities, shortages of food and clean water, and poor hygienic conditions are all factors that predispose to the expansion of new or re-emerging pathogens (Figure 3). Furthermore, large-scale movements of people, whether military personnel or refugees, can lead to the dissemination of diseases across a wide geographical area. The impact of epidemics on conflict outcomes is significant, increasing the vulnerability of affected populations [105]. Historical examples of pandemics that have impacted world conflicts include the bubonic plague, cholera, the Spanish flu and tuberculosis. The recent malaria outbreak in the Democratic Republic of Congo highlights the pressing need for interdisciplinary programmes that ensure prompt access to screening tests, isolation, and containment. Following a significant increase in mortality rates during the First World War, tuberculosis was recognised as a war disease. Given that the majority of contemporary conflicts are occurring in tuberculosis-endemic countries, tuberculosis continues to pose a significant threat not only to individuals residing in conflict-affected areas, but also to the population of neighbouring countries [107]. The internal displacement of significant numbers of people to safer locations within the country or internationally still poses a major threat today. Following the conflict that broke out in Ukraine in February 2022, the country is the fourth with the highest incidence of tuberculosis in Europe and the fifth globally in terms of drug-resistant tuberculosis cases (WHO Report, 2023). The spread of tuberculosis is facilitated by two key factors: the lack of access to adequate medical care and the presence of large populations in confined spaces lacking proper ventilation [107]. The ongoing armed conflict has led to a resurgence in new cases, reversing the downward trend that had been observed until 2020. This situation underscores the critical importance of addressing not only the immediate health concerns posed by the pandemic, but also the underlying factors that contribute to the high prevalence of MDR-TB. The armed conflict has the potential to severely impede efforts to combat the disease, primarily by limiting access to diagnostic services and anti-TB medications. Moreover, the substantial influx of refugees into neighbouring countries has placed considerable pressure on national health systems, further exacerbating the challenges posed by the pandemic [107]. It is therefore vital to emphasise the need for effective screening programmes to contain the disease, isolate those with active TB, and prevent its uncontrolled spread. The role of armed conflict as a driver for the spread of HIV and sexually transmitted diseases is well-documented. A seminal study of the post-First World War period revealed that sexually transmitted infections (STIs) became the second most common cause of disability among American soldiers. A 15% increase in the incidence of HIV has been observed in certain regions of Ukraine since the onset of the Russian-Ukrainian conflict [108] (Figure 3). The factors contributing to this increase include uncontrolled sexual intercourse, reduced access to healthcare and contraception, abuse, and the spread of new viral strains resulting from displacement. Moreover, the economic disadvantage engendered by war has been demonstrated to result in a significant number of women engaging in sex work as a means of income [108]. Moreover, the cessation of treatment in individuals with a positive diagnosis has been demonstrated to result in an escalation of viral load, which in turn engenders an elevated level of infectivity. Consequently, the implementation of programmes for the early detection of sexually transmitted diseases in migrants from war-affected countries is of paramount importance in order to counteract the spread of such diseases [105].
6. Conclusion
The emergence of new infectious diseases has been recognised as an unpredictable phenomenon for millennia even prior to the discovery of causative infectious agents. Despite the significant advancements in developing countermeasures (diagnostic, therapeutic and preventive), the ease of global travel and increasing global interdependence have greatly complicated the establishment of the necessary measures to contain such diseases. These diseases have the capacity to not only affect human health, but also economic stability. Emerging and re-emerging infections pose a significant threat to global public health, as demonstrated by the recent 2019 novel Coronavirus (nCoV) pandemic and the emergence and subsequent spread of other infectious pathogens. The ability of these pathogens to spread rapidly and cause large-scale outbreaks is due to a number of interconnected factors, including globalisation, climate change, deforestation and drug resistance. In the context of the ongoing emergence, resurgence and spread of infectious diseases, human interaction with domestic and wild animals, and environmental changes resulting from human activities, have become pivotal elements in understanding the epidemiology of these diseases. Furthermore, it is crucial to recognise the impact of these changes in terms of increasing opportunities for microbes to thrive. In view of the above, what efficacious strategies are currently available to combat these infections? In order to address these infections, it is imperative to employ a multifaceted approach that encompasses the following: 1) Rapidly detect unusual and unexplained disease outbreaks; 2) Track and exchange information in real time; 3) The mobilisation of a swift and decisive response effort that can rapidly extend on a global scale; 4) The containment of transmission with the objective of achieving rapid outcomes (Figure 4). The realisation of these points is contingent upon the successful resolution of the following national surveillance system deficiencies: 1) the lack of a comprehensive surveillance strategy for significant diseases, 2) the inadequate initial epidemiological investigations, laboratory diagnostics, and rapid field investigations, 3) the utilisation of erroneous case definitions, 4) delays in reporting and the inadequacy of data and information analysis at all levels, 5) the absence of feedback to peripheral levels, and 6) the insufficiency of preparedness to control epidemics. The following measures are proposed to address the gaps: firstly, the integration of laboratory science and epidemiology with a view to enhancing the effectiveness of public health practice. Secondly, the strengthening of public health infrastructures in order to provide support for surveillance, research and the implementation of prevention and control programmes. Thirdly, the provision of the public health workforce with the knowledge and tools required. Fourthly, the prompt implementation of prevention strategies and the enhancement of communication of public health information regarding emerging diseases (Figure 4).
The implementation of the aforementioned measures has been the result of a gradual and methodical process that requires careful planning. However, there are a number of measures that have the potential to be activated in a relatively short period of time. These include:
-The enhancement of coverage and acceptability of vaccines through the utilisation of nasal sprays, with the associated reduction in costs and reliance on "cold chain" logistics;
-The reduction of antimicrobial usage in agriculture and food production;
-The control of vector and zoonotic diseases by means of the use of safe insecticide.
Whatever measures are implemented to prevent epidemics recurring, retraining medical personnel and enhancing diagnostics must be a priority. This is key to a fast and effective response to often non-specific clinical demands.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, X.X. and Y.Y.; methodology, X.X.; software, X.X.; validation, X.X., Y.Y. and Z.Z.; formal analysis, X.X.; investigation, X.X.; resources, X.X.; data curation, X.X.; writing—original draft preparation, X.X.; writing—review and editing, X.X.; visualization, X.X.; supervision, X.X.; project administration, X.X.; funding acquisition, Y.Y. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Karlsson, E.K.; Kwiatkowski, D.P.; Sabeti, P.C. Natural selection and infectious disease in human populations. Nature reviews. Genetics 2014, 15, 379–393. [Google Scholar] [CrossRef] [PubMed]
- Seal, S.; Dharmarajan, G.; Khan, I. Evolution of pathogen tolerance and emerging infections: A missing experimental paradigm. eLife 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Li, W.; Wang, Z.; Yang, W.; Li, E.; Xia, X.; Yan, F.; Chiu, S. Emerging and reemerging infectious diseases: global trends and new strategies for their prevention and control. Signal transduction and targeted therapy 2024, 9, 223. [Google Scholar] [CrossRef] [PubMed]
- Ristori, M.V.; Guarrasi, V.; Soda, P.; Petrosillo, N.; Gurrieri, F.; Longo, U.G.; Ciccozzi, M.; Riva, E.; Angeletti, S. Emerging Microorganisms and Infectious Diseases: One Health Approach for Health Shared Vision. Genes 2024, 15. [Google Scholar] [CrossRef] [PubMed]
- Hauri, A.M.; Uphoff, H. [Tasks, principles and methods of applied infectious disease epidemiology/field epidemiology]. Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz 2005, 48, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Talisuna, A.O.; Okiro, E.A.; Yahaya, A.A.; Stephen, M.; Bonkoungou, B.; Musa, E.O.; Minkoulou, E.M.; Okeibunor, J.; Impouma, B.; Djingarey, H.M.; et al. Spatial and temporal distribution of infectious disease epidemics, disasters and other potential public health emergencies in the World Health Organisation Africa region, 2016-2018. Globalization and health 2020, 16, 9. [Google Scholar] [CrossRef]
- Gollakner, R.; Capua, I. Is COVID-19 the first pandemic that evolves into a panzootic? Veterinaria italiana 2020, 56, 7–8. [Google Scholar] [CrossRef]
- Biondo, C.; Ponzo, E.; Midiri, A.; Ostone, G.B.; Mancuso, G. The Dark Side of Nosocomial Infections in Critically Ill COVID-19 Patients. Life 2023, 13. [Google Scholar] [CrossRef]
- Cunha, C.B.; Opal, S.M. Middle East respiratory syndrome (MERS): a new zoonotic viral pneumonia. Virulence 2014, 5, 650–654. [Google Scholar] [CrossRef]
- Cherry, J.D.; Krogstad, P. SARS: the first pandemic of the 21st century. Pediatric research 2004, 56, 1–5. [Google Scholar] [CrossRef]
- Mena, I.; Nelson, M.I.; Quezada-Monroy, F.; Dutta, J.; Cortes-Fernandez, R.; Lara-Puente, J.H.; Castro-Peralta, F.; Cunha, L.F.; Trovao, N.S.; Lozano-Dubernard, B.; et al. Origins of the 2009 H1N1 influenza pandemic in swine in Mexico. eLife 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Sayres, L.; Hughes, B.L. Contemporary Understanding of Ebola and Zika Virus in Pregnancy. Clinics in perinatology 2020, 47, 835–846. [Google Scholar] [CrossRef] [PubMed]
- Murphy, H.L.; Ly, H. Pathogenicity and virulence mechanisms of Lassa virus and its animal modeling, diagnostic, prophylactic, and therapeutic developments. Virulence 2021, 12, 2989–3014. [Google Scholar] [CrossRef] [PubMed]
- Cuomo-Dannenburg, G.; McCain, K.; McCabe, R.; Unwin, H.J.T.; Doohan, P.; Nash, R.K.; Hicks, J.T.; Charniga, K.; Geismar, C.; Lambert, B.; et al. Marburg virus disease outbreaks, mathematical models, and disease parameters: a systematic review. The Lancet. Infectious diseases 2024, 24, e307–e317. [Google Scholar] [CrossRef] [PubMed]
- Alhilfi, R.A.; Khaleel, H.A.; Raheem, B.M.; Mahdi, S.G.; Tabche, C.; Rawaf, S. Large outbreak of Crimean-Congo haemorrhagic fever in Iraq, 2022. IJID regions 2023, 6, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Youssouf, H.; Subiros, M.; Dennetiere, G.; Collet, L.; Dommergues, L.; Pauvert, A.; Rabarison, P.; Vauloup-Fellous, C.; Le Godais, G.; Jaffar-Bandjee, M.C.; et al. Rift Valley Fever Outbreak, Mayotte, France, 2018-2019. Emerging infectious diseases 2020, 26, 769–772. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease Health Financing Collaborator, N. Health sector spending and spending on HIV/AIDS, tuberculosis, and malaria, and development assistance for health: progress towards Sustainable Development Goal 3. Lancet 2020, 396, 693–724. [Google Scholar] [CrossRef]
- Bray, F.; Laversanne, M.; Cao, B.; Varghese, C.; Mikkelsen, B.; Weiderpass, E.; Soerjomataram, I. Comparing cancer and cardiovascular disease trends in 20 middle- or high-income countries 2000-19: A pointer to national trajectories towards achieving Sustainable Development goal target 3.4. Cancer treatment reviews 2021, 100, 102290. [Google Scholar] [CrossRef]
- Boutayeb, A. The double burden of communicable and non-communicable diseases in developing countries. Transactions of the Royal Society of Tropical Medicine and Hygiene 2006, 100, 191–199. [Google Scholar] [CrossRef]
- Boutayeb, A.; Boutayeb, S. The burden of non communicable diseases in developing countries. International journal for equity in health 2005, 4, 2. [Google Scholar] [CrossRef]
- Church, D.L. Major factors affecting the emergence and re-emergence of infectious diseases. Clinics in laboratory medicine 2004, 24, 559–586. [Google Scholar] [CrossRef] [PubMed]
- Morse, S.S. Factors in the emergence of infectious diseases. Emerging infectious diseases 1995, 1, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Martin, P.M.; Martin-Granel, E. 2,500-year evolution of the term epidemic. Emerging infectious diseases 2006, 12, 976–980. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.T.; Liang, L.T.; Rosen, J.M. COVID-19: a comparison to the 1918 influenza and how we can defeat it. Postgraduate medical journal 2021, 97, 273–274. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.A.; Sankaran, N. Emergence of epidemic diseases: zoonoses and other origins. Faculty reviews 2022, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- Ellwanger, J.H.; Veiga, A.B.G.; Kaminski, V.L.; Valverde-Villegas, J.M.; Freitas, A.W.Q.; Chies, J.A.B. Control and prevention of infectious diseases from a One Health perspective. Genetics and molecular biology 2021, 44, e20200256. [Google Scholar] [CrossRef] [PubMed]
- Ellwanger, J.H.; Chies, J.A.B. Zoonotic spillover: Understanding basic aspects for better prevention. Genetics and molecular biology 2021, 44, e20200355. [Google Scholar] [CrossRef]
- Rodriguez-Lazaro, D.; Cook, N.; Ruggeri, F.M.; Sellwood, J.; Nasser, A.; Nascimento, M.S.; D'Agostino, M.; Santos, R.; Saiz, J.C.; Rzezutka, A.; et al. Virus hazards from food, water and other contaminated environments. FEMS microbiology reviews 2012, 36, 786–814. [Google Scholar] [CrossRef]
- Endale, H.; Mathewos, M.; Abdeta, D. Potential Causes of Spread of Antimicrobial Resistance and Preventive Measures in One Health Perspective-A Review. Infection and drug resistance 2023, 16, 7515–7545. [Google Scholar] [CrossRef]
- Bonneaud, C.; Longdon, B. Emerging pathogen evolution: Using evolutionary theory to understand the fate of novel infectious pathogens. EMBO reports 2020, 21, e51374. [Google Scholar] [CrossRef]
- Holden, M.T.; Hauser, H.; Sanders, M.; Ngo, T.H.; Cherevach, I.; Cronin, A.; Goodhead, I.; Mungall, K.; Quail, M.A.; Price, C.; et al. Rapid evolution of virulence and drug resistance in the emerging zoonotic pathogen Streptococcus suis. PloS one 2009, 4, e6072. [Google Scholar] [CrossRef] [PubMed]
- LaTourrette, K.; Garcia-Ruiz, H. Determinants of Virus Variation, Evolution, and Host Adaptation. Pathogens 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.; Antunes, W.; Mota, S.; Madureira-Carvalho, A.; Dinis-Oliveira, R.J.; Dias da Silva, D. An Overview of the Recent Advances in Antimicrobial Resistance. Microorganisms 2024, 12. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, G.; Trinchera, M.; Midiri, A.; Zummo, S.; Vitale, G.; Biondo, C. Novel Antimicrobial Approaches to Combat Bacterial Biofilms Associated with Urinary Tract Infections. Antibiotics 2024, 13. [Google Scholar] [CrossRef] [PubMed]
- Howard, C.R.; Fletcher, N.F. Emerging virus diseases: can we ever expect the unexpected? Emerging microbes & infections 2012, 1, e46. [Google Scholar] [CrossRef]
- Enserink, M. Emerging infectious diseases. Nipah virus (or a cousin) strikes again. Science 2004, 303, 1121. [Google Scholar] [CrossRef]
- LeDuc, J.W. WHO program on emerging virus diseases. Archives of virology. Supplementum 1996, 11, 13–20. [Google Scholar] [CrossRef]
- McNicholl, J.M.; Downer, M.V.; Udhayakumar, V.; Alper, C.A.; Swerdlow, D.L. Host-pathogen interactions in emerging and re-emerging infectious diseases: a genomic perspective of tuberculosis, malaria, human immunodeficiency virus infection, hepatitis B, and cholera. Annual review of public health 2000, 21, 15–46. [Google Scholar] [CrossRef]
- Baker, R.E.; Mahmud, A.S.; Miller, I.F.; Rajeev, M.; Rasambainarivo, F.; Rice, B.L.; Takahashi, S.; Tatem, A.J.; Wagner, C.E.; Wang, L.F.; et al. Infectious disease in an era of global change. Nature reviews. Microbiology 2022, 20, 193–205. [Google Scholar] [CrossRef]
- Heffernan, C. Climate change and multiple emerging infectious diseases. Veterinary journal 2018, 234, 43–47. [Google Scholar] [CrossRef]
- Wikan, N.; Smith, D.R. Zika virus: history of a newly emerging arbovirus. The Lancet. Infectious diseases 2016, 16, e119–e126. [Google Scholar] [CrossRef] [PubMed]
- Kauffman, E.B.; Kramer, L.D. Zika Virus Mosquito Vectors: Competence, Biology, and Vector Control. The Journal of infectious diseases 2017, 216, S976–S990. [Google Scholar] [CrossRef] [PubMed]
- Duffy, M.R.; Chen, T.H.; Hancock, W.T.; Powers, A.M.; Kool, J.L.; Lanciotti, R.S.; Pretrick, M.; Marfel, M.; Holzbauer, S.; Dubray, C.; et al. Zika virus outbreak on Yap Island, Federated States of Micronesia. The New England journal of medicine 2009, 360, 2536–2543. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.; Ortiz, K.; Ansari, A.; Gershwin, M.E. The Zika outbreak of the 21st century. Journal of autoimmunity 2016, 68, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.F.; Choi, G.K.; Yip, C.C.; Cheng, V.C.; Yuen, K.Y. Zika fever and congenital Zika syndrome: An unexpected emerging arboviral disease. The Journal of infection 2016, 72, 507–524. [Google Scholar] [CrossRef] [PubMed]
- Boyer, S.; Calvez, E.; Chouin-Carneiro, T.; Diallo, D.; Failloux, A.B. An overview of mosquito vectors of Zika virus. Microbes and infection 2018, 20, 646–660. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, F.M.E.; Pietrobon, A.J.; Oliveira, L.M.; Oliveira, L.; Sato, M.N. Maternal-Fetal Interplay in Zika Virus Infection and Adverse Perinatal Outcomes. Frontiers in immunology 2020, 11, 175. [Google Scholar] [CrossRef] [PubMed]
- Possas, C.; Brasil, P.; Marzochi, M.C.; Tanuri, A.; Martins, R.M.; Marques, E.T.; Bonaldo, M.C.; Ferreira, A.G.; Lourenco-de-Oliveira, R.; Nogueira, R.M.R.; et al. Zika puzzle in Brazil: peculiar conditions of viral introduction and dissemination - A Review. Memorias do Instituto Oswaldo Cruz 2017, 112, 319–327. [Google Scholar] [CrossRef]
- McCloskey, B.; Endericks, T. The rise of Zika infection and microcephaly: what can we learn from a public health emergency? Public health 2017, 150, 87–92. [Google Scholar] [CrossRef]
- Gardner, L.; Chen, N.; Sarkar, S. Vector status of Aedes species determines geographical risk of autochthonous Zika virus establishment. PLoS neglected tropical diseases 2017, 11, e0005487. [Google Scholar] [CrossRef]
- Talavera-Aguilar, L.G.; Murrieta, R.A.; Kiem, S.; Cetina-Trejo, R.C.; Baak-Baak, C.M.; Ebel, G.D.; Blitvich, B.J.; Machain-Williams, C. Infection, dissemination, and transmission efficiencies of Zika virus in Aedes aegypti after serial passage in mosquito or mammalian cell lines or alternating passage in both cell types. Parasites & vectors 2021, 14, 261. [Google Scholar] [CrossRef]
- Biondo, C.; Midiri, A.; Gerace, E.; Zummo, S.; Mancuso, G. SARS-CoV-2 Infection in Patients with Cystic Fibrosis: What We Know So Far. Life 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Worobey, M.; Levy, J.I.; Malpica Serrano, L.; Crits-Christoph, A.; Pekar, J.E.; Goldstein, S.A.; Rasmussen, A.L.; Kraemer, M.U.G.; Newman, C.; Koopmans, M.P.G.; et al. The Huanan Seafood Wholesale Market in Wuhan was the early epicenter of the COVID-19 pandemic. Science 2022, 377, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. The Journal of hospital infection 2020, 104, 246–251. [Google Scholar] [CrossRef]
- Baj, J.; Karakula-Juchnowicz, H.; Teresinski, G.; Buszewicz, G.; Ciesielka, M.; Sitarz, R.; Forma, A.; Karakula, K.; Flieger, W.; Portincasa, P.; et al. COVID-19: Specific and Non-Specific Clinical Manifestations and Symptoms: The Current State of Knowledge. Journal of clinical medicine 2020, 9. [Google Scholar] [CrossRef]
- Filip, R.; Gheorghita Puscaselu, R.; Anchidin-Norocel, L.; Dimian, M.; Savage, W.K. Global Challenges to Public Health Care Systems during the COVID-19 Pandemic: A Review of Pandemic Measures and Problems. Journal of personalized medicine 2022, 12. [Google Scholar] [CrossRef]
- Singh, S.; McNab, C.; Olson, R.M.; Bristol, N.; Nolan, C.; Bergstrom, E.; Bartos, M.; Mabuchi, S.; Panjabi, R.; Karan, A.; et al. How an outbreak became a pandemic: a chronological analysis of crucial junctures and international obligations in the early months of the COVID-19 pandemic. Lancet 2021, 398, 2109–2124. [Google Scholar] [CrossRef]
- Jee, Y. WHO International Health Regulations Emergency Committee for the COVID-19 outbreak. Epidemiology and health 2020, 42, e2020013. [Google Scholar] [CrossRef]
- Chong, Z.X.; Liew, W.P.P.; Ong, H.K.; Yong, C.Y.; Shit, C.S.; Ho, W.Y.; Ng, S.Y.L.; Yeap, S.K. Current diagnostic approaches to detect two important betacoronaviruses: Middle East respiratory syndrome coronavirus (MERS-CoV) and severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Pathology, research and practice 2021, 225, 153565. [Google Scholar] [CrossRef]
- Omrani, A.S.; Shalhoub, S. Middle East respiratory syndrome coronavirus (MERS-CoV): what lessons can we learn? The Journal of hospital infection 2015, 91, 188–196. [Google Scholar] [CrossRef]
- Rasmussen, S.A.; Gerber, S.I.; Swerdlow, D.L. Middle East respiratory syndrome coronavirus: update for clinicians. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2015, 60, 1686–1689. [Google Scholar] [CrossRef] [PubMed]
- Oraby, T.; Tyshenko, M.G.; Balkhy, H.H.; Tasnif, Y.; Quiroz-Gaspar, A.; Mohamed, Z.; Araya, A.; Elsaadany, S.; Al-Mazroa, E.; Alhelail, M.A.; et al. Analysis of the Healthcare MERS-CoV Outbreak in King Abdulaziz Medical Center, Riyadh, Saudi Arabia, June-August 2015 Using a SEIR Ward Transmission Model. International journal of environmental research and public health 2020, 17. [Google Scholar] [CrossRef] [PubMed]
- Pavli, A.; Tsiodras, S.; Maltezou, H.C. Middle East respiratory syndrome coronavirus (MERS-CoV): prevention in travelers. Travel medicine and infectious disease 2014, 12, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Omrani, A.S.; Al-Tawfiq, J.A.; Memish, Z.A. Middle East respiratory syndrome coronavirus (MERS-CoV): animal to human interaction. Pathogens and global health 2015, 109, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Khalafalla, A.I. Zoonotic diseases transmitted from the camels. Frontiers in veterinary science 2023, 10, 1244833. [Google Scholar] [CrossRef]
- Xu, R.H.; He, J.F.; Evans, M.R.; Peng, G.W.; Field, H.E.; Yu, D.W.; Lee, C.K.; Luo, H.M.; Lin, W.S.; Lin, P.; et al. Epidemiologic clues to SARS origin in China. Emerging infectious diseases 2004, 10, 1030–1037. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Zhao, S.; Teng, T.; Abdalla, A.E.; Zhu, W.; Xie, L.; Wang, Y.; Guo, X. Systematic Comparison of Two Animal-to-Human Transmitted Human Coronaviruses: SARS-CoV-2 and SARS-CoV. Viruses 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A. The severe acute respiratory syndrome: impact on travel and tourism. Travel medicine and infectious disease 2006, 4, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Luu, B.; McCoy-Hass, V.; Kadiu, T.; Ngo, V.; Kadiu, S.; Lien, J. Severe Acute Respiratory Syndrome Associated Infections. Physician assistant clinics 2023, 8, 495–530. [Google Scholar] [CrossRef]
- Petrosillo, N.; Viceconte, G.; Ergonul, O.; Ippolito, G.; Petersen, E. COVID-19, SARS and MERS: are they closely related? Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases 2020, 26, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Breman, J.G.; Heymann, D.L.; Lloyd, G.; McCormick, J.B.; Miatudila, M.; Murphy, F.A.; Muyembe-Tamfun, J.J.; Piot, P.; Ruppol, J.F.; Sureau, P.; et al. Discovery and Description of Ebola Zaire Virus in 1976 and Relevance to the West African Epidemic During 2013-2016. The Journal of infectious diseases 2016, 214, S93–S101. [Google Scholar] [CrossRef] [PubMed]
- Den Boon, S.; Marston, B.J.; Nyenswah, T.G.; Jambai, A.; Barry, M.; Keita, S.; Durski, K.; Senesie, S.S.; Perkins, D.; Shah, A.; et al. Ebola Virus Infection Associated with Transmission from Survivors. Emerging infectious diseases 2019, 25, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Chiappelli, F.; Bakhordarian, A.; Thames, A.D.; Du, A.M.; Jan, A.L.; Nahcivan, M.; Nguyen, M.T.; Sama, N.; Manfrini, E.; Piva, F.; et al. Ebola: translational science considerations. Journal of translational medicine 2015, 13, 11. [Google Scholar] [CrossRef] [PubMed]
- Leroy, E.M.; Kumulungui, B.; Pourrut, X.; Rouquet, P.; Hassanin, A.; Yaba, P.; Delicat, A.; Paweska, J.T.; Gonzalez, J.P.; Swanepoel, R. Fruit bats as reservoirs of Ebola virus. Nature 2005, 438, 575–576. [Google Scholar] [CrossRef] [PubMed]
- El Ayoubi, L.W.; Mahmoud, O.; Zakhour, J.; Kanj, S.S. Recent advances in the treatment of Ebola disease: A brief overview. PLoS pathogens 2024, 20, e1012038. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Sharma, D.; Kumar, S.; Sharma, A.; Rijal, R.; Asija, A.; Adhikari, S.; Rustagi, S.; Sah, S.; Al-Qaim, Z.H.; et al. Emergence of Marburg virus: a global perspective on fatal outbreaks and clinical challenges. Frontiers in microbiology 2023, 14, 1239079. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, J.P.; Souris, M.; Valdivia-Granda, W. Global Spread of Hemorrhagic Fever Viruses: Predicting Pandemics. Methods in molecular biology 2018, 1604, 3–31. [Google Scholar] [CrossRef] [PubMed]
- Mohapatra, R.K.; Sarangi, A.K.; Kandi, V.; Chakraborty, S.; Chandran, D.; Alagawany, M.; Chakraborty, C.; Dhama, K. Recent re-emergence of Marburg virus disease in an African country Ghana after Guinea amid the ongoing COVID-19 pandemic: Another global threat? Current knowledge and strategies to tackle this highly deadly disease having feasible pandemic potential. International journal of surgery 2022, 106, 106863. [Google Scholar] [CrossRef] [PubMed]
- Okesanya, O.J.; Olatunji, G.D.; Kokori, E.; Olaleke, N.O.; Adigun, O.A.; Manirambona, E.; Lucero-Prisno, D.E. , 3rd. Looking Beyond the Lens of Crimean-Congo Hemorrhagic Fever in Africa. Emerging infectious diseases 2024, 30, 1319–1325. [Google Scholar] [CrossRef] [PubMed]
- Papa, A.; Tsergouli, K.; Tsioka, K.; Mirazimi, A. Crimean-Congo Hemorrhagic Fever: Tick-Host-Virus Interactions. Frontiers in cellular and infection microbiology 2017, 7, 213. [Google Scholar] [CrossRef] [PubMed]
- Kodama, C.; Alhilfi, R.A.; Aakef, I.; Khamasi, A.; Mahdi, S.; Hasan, H.M.; Khaleel, R.I.; Naji, M.M.; Esmaeel, N.K.; Haji-Jama, S.; et al. Epidemiological analysis and potential factors affecting the 2022-23 Crimean-Congo hemorrhagic fever outbreak in Iraq. European journal of public health 2025, 35, i6–i13. [Google Scholar] [CrossRef] [PubMed]
- Frank, M.G.; Weaver, G.; Raabe, V.; State of the Clinical Science Working Group of the National Emerging Pathogens, T. ; Education Center's Special Pathogens Research, N.; State of the Clinical Science Working Group of the National Emerging Pathogens Training Education Center's Special Pathogens Research, N. Crimean-Congo Hemorrhagic Fever Virus for Clinicians-Epidemiology, Clinical Manifestations, and Prevention. Emerging infectious diseases 2024, 30, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Alkan, C.; Jurado-Cobena, E.; Ikegami, T. Advancements in Rift Valley fever vaccines: a historical overview and prospects for next generation candidates. NPJ vaccines 2023, 8, 171. [Google Scholar] [CrossRef] [PubMed]
- Hartman, A. Rift Valley Fever. Clinics in laboratory medicine 2017, 37, 285–301. [Google Scholar] [CrossRef] [PubMed]
- Kenawy, M.A.; Abdel-Hamid, Y.M.; Beier, J.C. Rift Valley Fever in Egypt and other African countries: Historical review, recent outbreaks and possibility of disease occurrence in Egypt. Acta tropica 2018, 181, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Reyna, R.A.; Littlefield, K.E.; Shehu, N.; Makishima, T.; Maruyama, J.; Paessler, S. The Importance of Lassa Fever and Its Disease Management in West Africa. Viruses 2024, 16. [Google Scholar] [CrossRef]
- Shieh, W.J.; Demby, A.; Jones, T.; Goldsmith, C.S.; Rollin, P.E.; Ksiazek, T.G.; Peters, C.J.; Zaki, S.R. Pathology and Pathogenesis of Lassa Fever: Novel Immunohistochemical Findings in Fatal Cases and Clinico-pathologic Correlation. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2022, 74, 1821–1830. [Google Scholar] [CrossRef] [PubMed]
- Marien, J.; Borremans, B.; Kourouma, F.; Baforday, J.; Rieger, T.; Gunther, S.; Magassouba, N.; Leirs, H.; Fichet-Calvet, E. Evaluation of rodent control to fight Lassa fever based on field data and mathematical modelling. Emerging microbes & infections 2019, 8, 640–649. [Google Scholar] [CrossRef]
- Lawrence, P.; Heung, M.; Nave, J.; Henkel, C.; Escudero-Perez, B. The natural virome and pandemic potential: Disease X. Current opinion in virology 2023, 63, 101377. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.; Schultz Hansen, K. Relative Burdens of the COVID-19, Malaria, Tuberculosis, and HIV/AIDS Epidemics in Sub-Saharan Africa. The American journal of tropical medicine and hygiene 2021, 105, 1510–1515. [Google Scholar] [CrossRef]
- Davis, S.L. Human rights and the Global Fund to Fight AIDS, Tuberculosis, and Malaria. Health and human rights 2014, 16, 134–147. [Google Scholar] [PubMed]
- Strong, K.; Noor, A.; Aponte, J.; Banerjee, A.; Cibulskis, R.; Diaz, T.; Ghys, P.; Glaziou, P.; Hereward, M.; Hug, L.; et al. Monitoring the status of selected health related sustainable development goals: methods and projections to 2030. Global health action 2020, 13, 1846903. [Google Scholar] [CrossRef] [PubMed]
- Payagala, S.; Pozniak, A. The global burden of HIV. Clinics in dermatology 2024, 42, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Kharsany, A.B.; Karim, Q.A. HIV Infection and AIDS in Sub-Saharan Africa: Current Status, Challenges and Opportunities. The open AIDS journal 2016, 10, 34–48. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.R.; Rao, A.; Rucinski, K.B.; Lyons, C.; Viswasam, N.; Comins, C.A.; Olawore, O.; Baral, S. HIV-Related Implementation Research for Key Populations: Designing for Individuals, Evaluating Across Populations, and Integrating Context. Journal of acquired immune deficiency syndromes 2019, 82 Suppl 3, S206–S216. [Google Scholar] [CrossRef]
- Ba Konko Cire, E.H.; Roh, M.E.; Diallo, A.; Gadiaga, T.; Seck, A.; Thiam, S.; Gaye, S.; Diallo, I.; Lo, A.C.; Diouf, E.; et al. Mass drug administration to reduce malaria incidence in a low-to-moderate endemic setting: short-term impact results from a cluster randomised controlled trial in Senegal. medRxiv : the preprint server for health sciences. [CrossRef]
- Oladipo, H.J.; Tajudeen, Y.A.; Oladunjoye, I.O.; Yusuff, S.I.; Yusuf, R.O.; Oluwaseyi, E.M.; AbdulBasit, M.O.; Adebisi, Y.A.; El-Sherbini, M.S. Increasing challenges of malaria control in sub-Saharan Africa: Priorities for public health research and policymakers. Annals of medicine and surgery 2022, 81, 104366. [Google Scholar] [CrossRef]
- Segala, F.V.; Di Gennaro, F.; Ictho, J.; L'Episcopia, M.; Onapa, E.; Marotta, C.; De Vita, E.; Amone, J.; Iacobelli, V.; Ogwang, J.; et al. Impact of antimalarial resistance and COVID-19 pandemic on malaria care among pregnant women in Northern Uganda (ERASE): protocol of a prospective observational study. BMC infectious diseases 2022, 22, 668. [Google Scholar] [CrossRef]
- Falzon, D.; Zignol, M.; Bastard, M.; Floyd, K.; Kasaeva, T. The impact of the COVID-19 pandemic on the global tuberculosis epidemic. Frontiers in immunology 2023, 14, 1234785. [Google Scholar] [CrossRef]
- A spotlight on the tuberculosis epidemic in South Africa. Nature communications 2024, 15, 1290. [CrossRef]
- Collaborators, G.B.D.T. Global, regional, and national age-specific progress towards the 2020 milestones of the WHO End TB Strategy: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet. Infectious diseases 2024, 24, 698–725. [Google Scholar] [CrossRef]
- Yenet, A.; Nibret, G.; Tegegne, B.A. Challenges to the Availability and Affordability of Essential Medicines in African Countries: A Scoping Review. ClinicoEconomics and outcomes research : CEOR 2023, 15, 443–458. [Google Scholar] [CrossRef] [PubMed]
- Sundermann, A.J.; Kumar, P.; Griffith, M.P.; Waggle, K.D.; Srinivasa, V.R.; Raabe, N.; Mills, E.G.; Coyle, H.; Ereifej, D.; Creager, H.M.; et al. Genomic Surveillance for Enhanced Healthcare Outbreak Detection and Control. medRxiv : the preprint server for health sciences 2024. [CrossRef]
- Nerlander, L.; Champezou, L.; Gomes Dias, J.; Aspelund, G.; Berlot, L.; Constantinou, E.; Diaz, A.; Epstein, J.; Fogarassy, E.; Hernando, V.; et al. Sharp increase in gonorrhoea notifications among young people, EU/EEA, July 2022 to June 2023. Euro surveillance : bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin 2024, 29. [Google Scholar] [CrossRef] [PubMed]
- Marou, V.; Vardavas, C.I.; Aslanoglou, K.; Nikitara, K.; Plyta, Z.; Leonardi-Bee, J.; Atkins, K.; Condell, O.; Lamb, F.; Suk, J.E. The impact of conflict on infectious disease: a systematic literature review. Conflict and health 2024, 18, 27. [Google Scholar] [CrossRef]
- Mehtar, S.; AlMhawish, N.; Shobak, K.; Reingold, A.; Guha-Sapir, D.; Haar, R.J. Measles in conflict-affected northern Syria: results from an ongoing outbreak surveillance program. Conflict and health 2021, 15, 95. [Google Scholar] [CrossRef] [PubMed]
- Gebreyohannes, E.A.; Wolde, H.F.; Akalu, T.Y.; Clements, A.C.A.; Alene, K.A. Impacts of armed conflicts on tuberculosis burden and treatment outcomes: a systematic review. BMJ open 2024, 14, e080978. [Google Scholar] [CrossRef] [PubMed]
- Kvasnevska, Y.; Faustova, M.; Voronova, K.; Basarab, Y.; Lopatina, Y. Impact of war-associated factors on spread of sexually transmitted infections: a systemic review. Frontiers in public health 2024, 12, 1366600. [Google Scholar] [CrossRef]
Figure 1.
The multifactorial nature of emergent and reemergent infectious diseases. Genetic changes in pathogens affect their biology, including how easily they spread, how they evade the immune system, how harmful they are, and how resistant they become to antimicrobials. These changes allow the most adaptable pathogen to thrive in a specific environment. Environmental change can also impact the geographical distribution of reservoir hosts and vectors, increasing the likelihood of spread to new areas. Human activities, such as globalisation, help pathogens to spread quickly and extensively. Overcrowding and unsanitary conditions in cities increase the risk of new pathogens emerging and spreading.
Figure 1.
The multifactorial nature of emergent and reemergent infectious diseases. Genetic changes in pathogens affect their biology, including how easily they spread, how they evade the immune system, how harmful they are, and how resistant they become to antimicrobials. These changes allow the most adaptable pathogen to thrive in a specific environment. Environmental change can also impact the geographical distribution of reservoir hosts and vectors, increasing the likelihood of spread to new areas. Human activities, such as globalisation, help pathogens to spread quickly and extensively. Overcrowding and unsanitary conditions in cities increase the risk of new pathogens emerging and spreading.
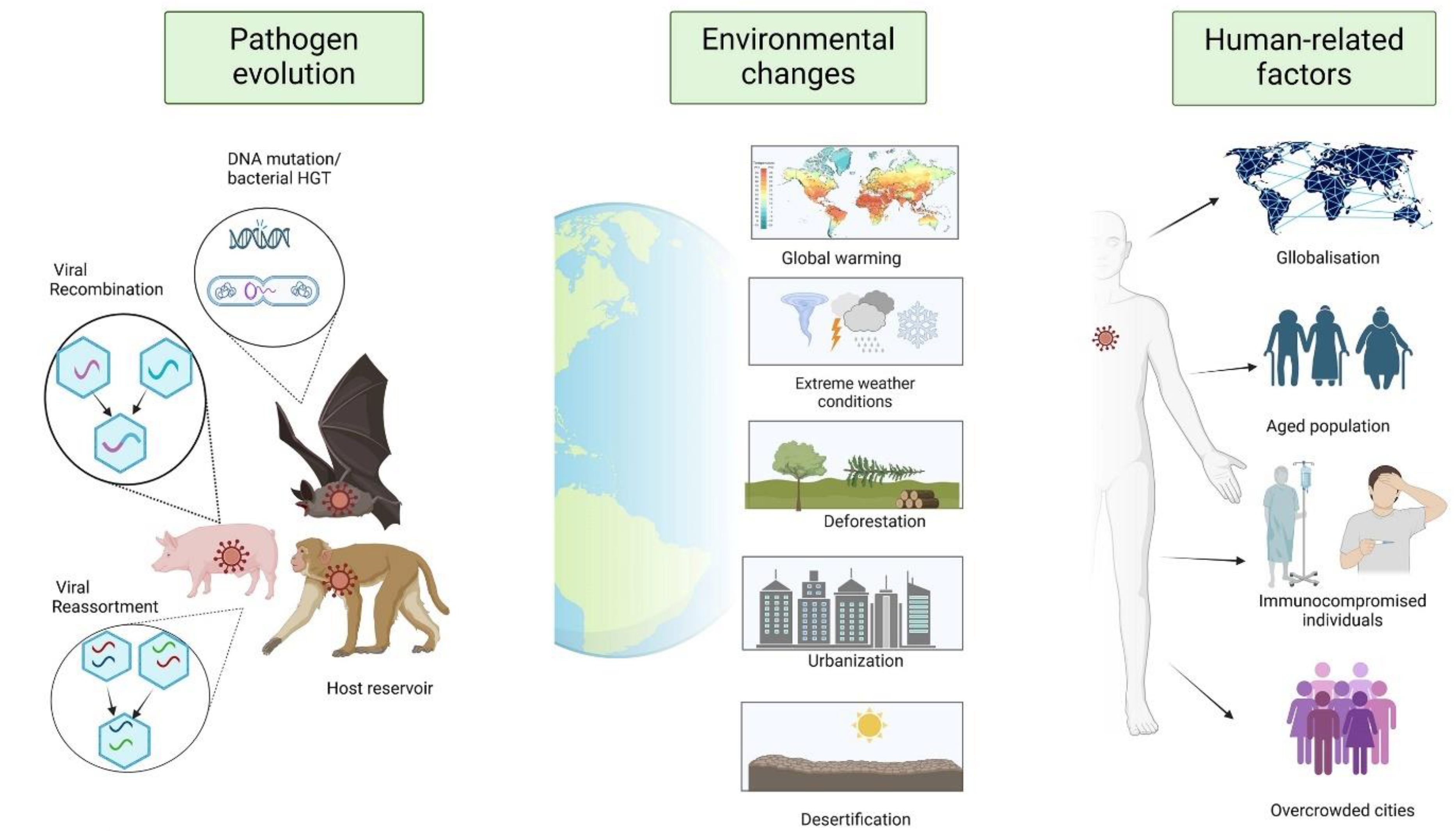
Figure 2.
The most recent WHO data on the worldwide incidence of HIV/AIDS, tuberculosis and malaria. Numbers of this magnitude highlight how these diseases represent a serious public health problem despite the fact that they are well known and have been the subject of action plans for several years.
Figure 2.
The most recent WHO data on the worldwide incidence of HIV/AIDS, tuberculosis and malaria. Numbers of this magnitude highlight how these diseases represent a serious public health problem despite the fact that they are well known and have been the subject of action plans for several years.
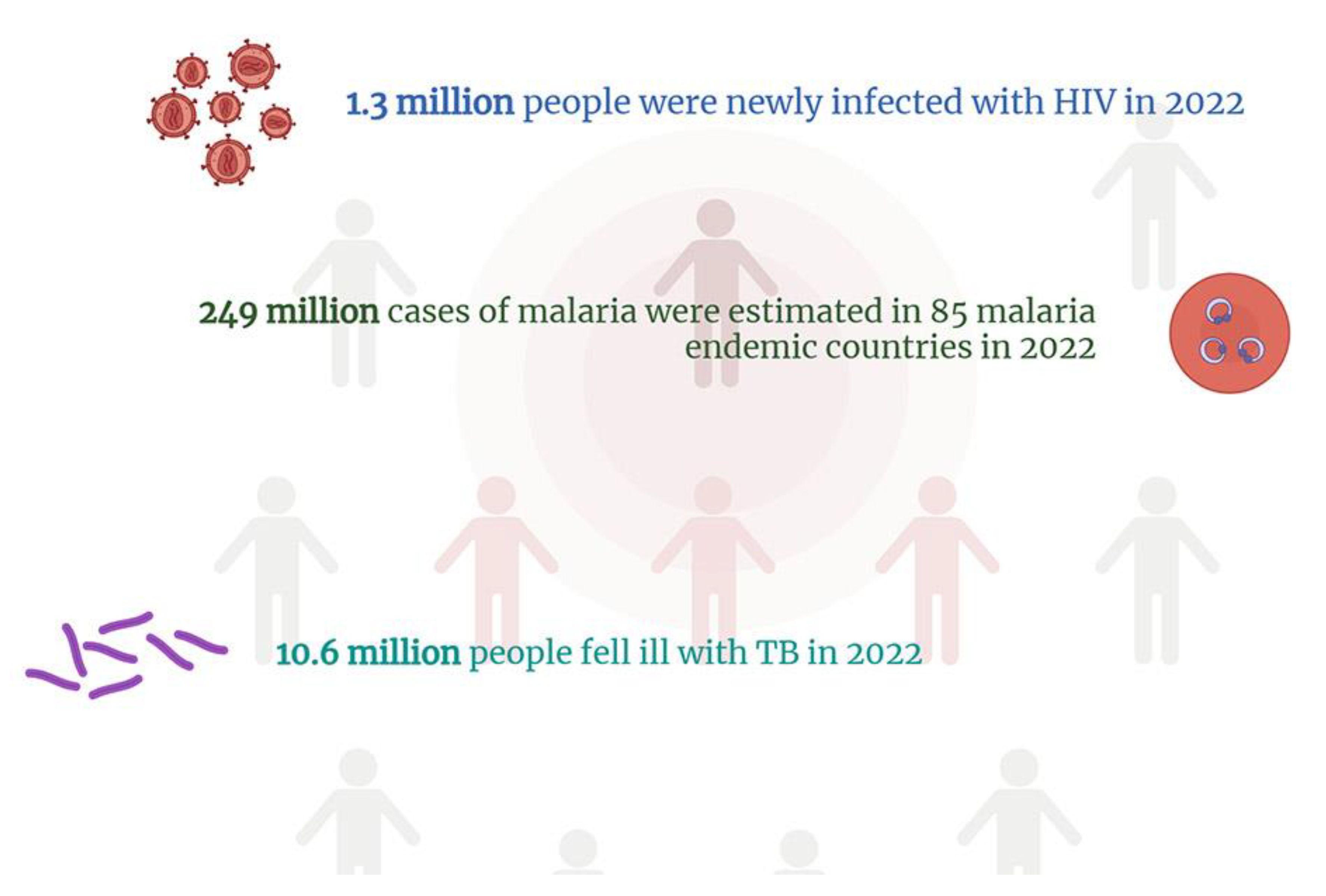
Figure 3.
The catastrophic consequences of the profound interconnection between infectious diseases and warfare. Infectious diseases have a significant impact during conflicts, spreading rapidly among military personnel and the population. History shows that warfare creates the perfect conditions for disease to spread, due to its disruptive effect on living conditions. Destruction or overcrowding of health facilities, food shortages, drinking water shortages, and suboptimal hygiene all contribute to the spread of pathogens. Large-scale movements of people, whether military personnel or refugees, spread diseases, even in regions far from the conflict. The absence of access to healthcare services resurges vaccine-preventable diseases. Conflict increases unprotected sex, which transmits infections like STIs and HIV.
Figure 3.
The catastrophic consequences of the profound interconnection between infectious diseases and warfare. Infectious diseases have a significant impact during conflicts, spreading rapidly among military personnel and the population. History shows that warfare creates the perfect conditions for disease to spread, due to its disruptive effect on living conditions. Destruction or overcrowding of health facilities, food shortages, drinking water shortages, and suboptimal hygiene all contribute to the spread of pathogens. Large-scale movements of people, whether military personnel or refugees, spread diseases, even in regions far from the conflict. The absence of access to healthcare services resurges vaccine-preventable diseases. Conflict increases unprotected sex, which transmits infections like STIs and HIV.
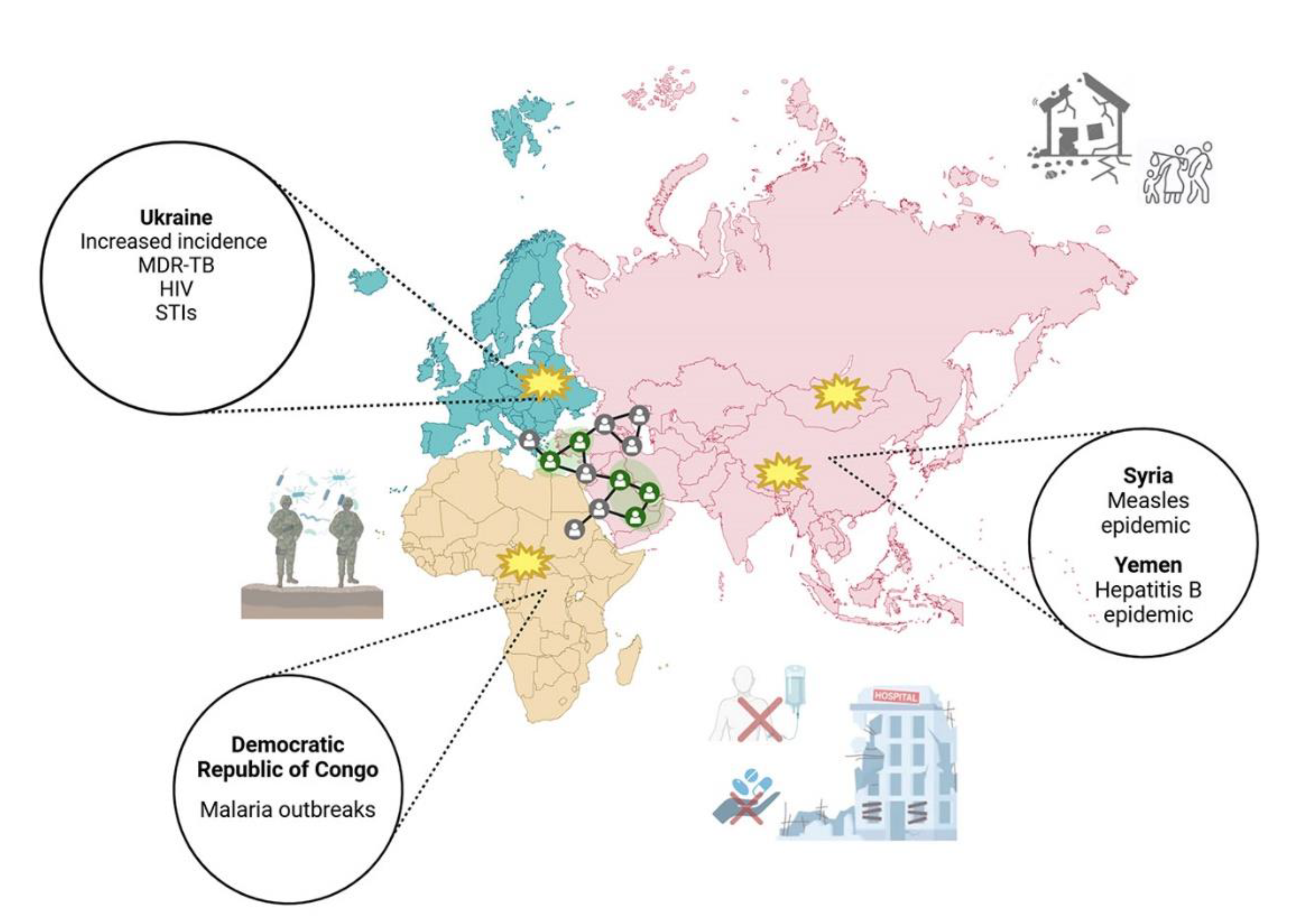
Figure 4.
Schematic representation of the measures deemed necessary for the enhancement of public health, with a focus on the timely diagnosis and prevention of infectious diseases.
Figure 4.
Schematic representation of the measures deemed necessary for the enhancement of public health, with a focus on the timely diagnosis and prevention of infectious diseases.
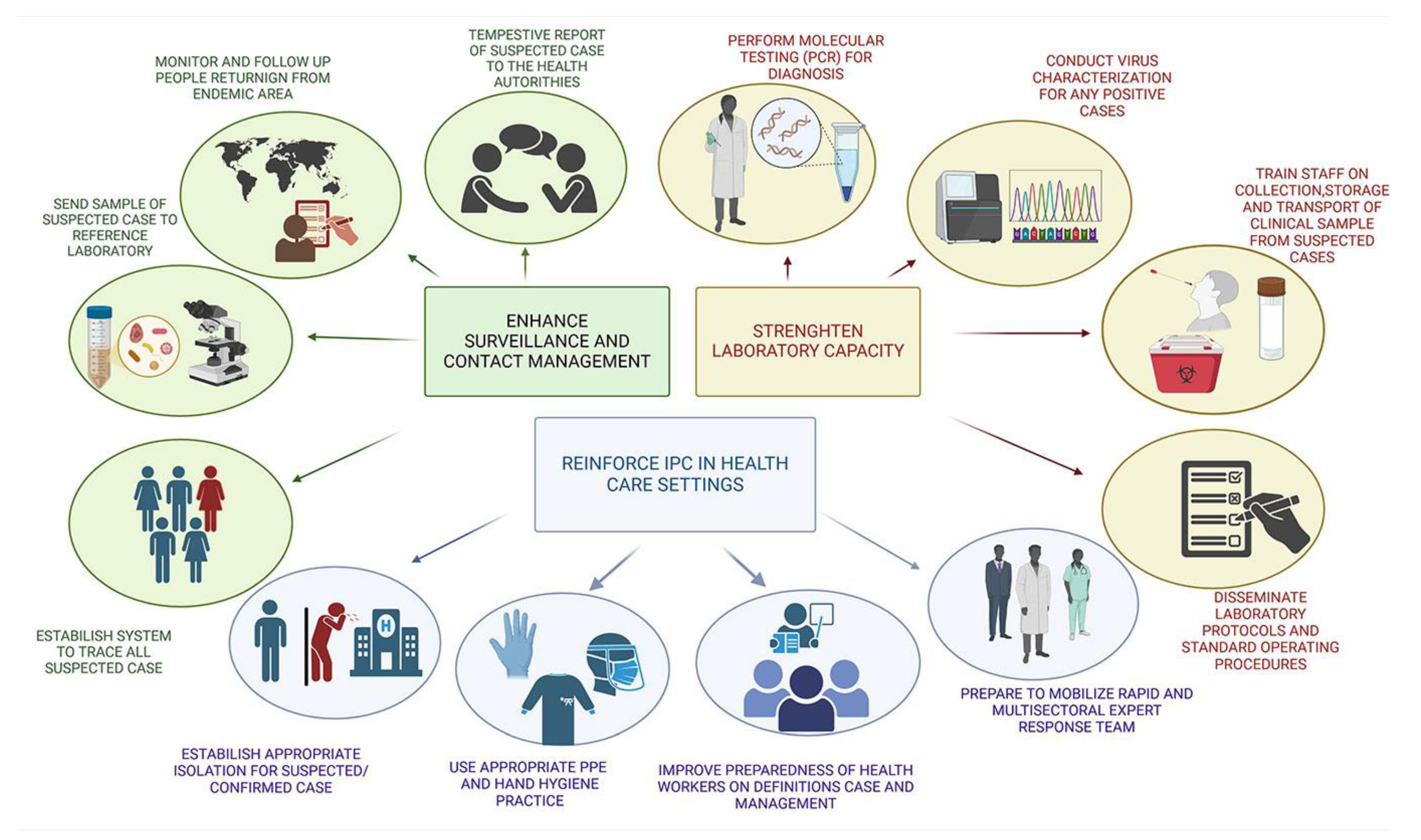
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



