
Submitted:
22 January 2025
Posted:
23 January 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
From the time that, in March, 2020, the World Health Organization (WHO) declared the acute respiratory syndrome caused by Coronavirus-2 (SARS-CoV-2), better known as COVID-19, a pandemic, an effective treatment has been sought, without achieving this at 100%. SARS-CoV-2 mainly affects the respiratory airways, but it is also known to damage various organs and systems, giving rise to a slight symptomatology up to, even, death in some cases. Unfortunately, high comorbility has also been found, which is associated with chronic-degenerative diseases that raises the risk of mortality in patients. In this review, a description is made of some common factors in patients affected by COVID-19 with a diagnosis of prior diabetes. In this regard, the therapeutic effects are described of some plant species and their secondary metabolites that, in some previous studies, have demonstrated, to exert certain effects in patients diagnosed with diabetes, emphasizing that, while different vaccines are now available to meet the challenge of the pandemic, the information collected in this work could be useful in the search for alternative clinical therapies based on Traditional Medicine and on the chemistry of some plant-derived secondary metabolites in patients affected by COVID-19 and diabetes.
Keywords:
COVID-19
; Diabetes
; Natural products
; Therapeutic effect
1. Introduction
On March 11, 2020, the World Health Organization (WHO) announced that a disease similar to Severe Acute Respiratory Syndrome (SARS) had become a problem of world health. Tedros Adhanom Ghebreyesus, head of this organism, added: “We can expect that the number of cases or deaths and countries affected will increase in the following days and weeks” [1]. Since that date, the number of contagions increased exponentially in Asia, Europe, and later in America, and then efforts began to treat the disease, to contain it, and to diminish the number of deaths. However, there is no satisfactory treatment to date, although in emerging fashion, some vaccines have been approved to confront the pandemic.
2. COVID-19: Signs and Symptoms
The causal agent of COVID-19, a new variant of the SARS-CoV-2 CoronaViruses (CoV), was detected for the first time in December 2019 in the city of Wuhan, People’s Republic of China (PRC) 2–6]. Taxonomically, it belongs to the Coronaviridae family, which includes other viruses such as SARS and (MERS) [7,8,9,10,11,12], and is constituted by four structural proteins: spike (S), Envelope (E), Membrane (M), and Nucleocapside (N) [9,13,14]. This pathogen is transmitted by means of droplets of saliva or other fluids contained in the sneeze in direct contact with contaminated surfaces, the cough or the breathing of contaminated persons [15]. Little is known about the mechanisms utilized to establish it in the body, but the studies reveal that this is carried out in the respiratory airways and the lungs where the S1-subtype of the S proteins bind with the host cells Angiotensin-Converting Enzyme 2 (ACE2) that, together with some leptins, become the SARS-CoV-2 receptor [7,16,17,18,19]. Proteins such as neuropilin-1, which is in the endothelial cells that line the nasal cavity also favor the entry of this pathogen, not only to the respiratory airways, but also to the central nervous system (CNS) [20,21]. In addition, this panorama can become more dangerous if the patient has some alteration of the immune system [22,23,24]. Once established in the body of the host, this can remain asymptomatic or can present slight signs and symptoms such as cough, fever, weakness and generalized malaise, throat pain, loss of the sense of taste and smell, difficulty in breathing, pain in different parts of the body such as muscular pain, cephalea, chest pain, loss of speech, among others [25,30]. There may be more severe symptoms, such as diarrhea, hepatic and cardiac lesions, pneumonia, pulmonary hyperplasia, sepsis, uncontrolled inflammation of the attacked tissues due to the failure of the immune system, respiratory failure, thrombosis, and alterations in the CNS [3,31,32,33,34,35,36,37,38], which endanger the life of the patient (Figure 1).
3. Treatment of COVID-19
From the beginning and the declaration of the pandemic, therapies have been sought for an adequate treatment of the disease. However, up to October 2020, there was no effective treatment and only very strict measures of hygiene and of social isolation were implemented. Many companies throughout the world focused on creating a vaccine against SARS-CoV-2; currently, some of these have been administered to health-care workers since December 2020. Although the mortality rate of this pandemic is relatively low, there were 1.3 million deaths by mid-November 2020; it is noteworthy that the majority of persons who died presented some chronic pathology, rendering them more susceptible [39]. Among the treatments that have been utilized to cope with the pandemic we are able to cite the antivirals Ribavirin, Remdesivir [40,41,42], Interferon alpha [43,44,45,46], Cyclophilin inhibitors such as Cyclosporin A [47,48,49,50], glycosylation inhibitors such as Chloroquine [51,52,53,54], Kinase inhibitors such as Imatinib [55,56,57], and some monoclonal antibodies that can be employed in vaccines [58,60]. Nonetheless, none of these treatments have proven to be completely effective to diminish the severity of this pandemic.
4. Comorbility
Unfortunately, other factors have been discovered that have been added to the lethality of COVID-19. Age is one of these factors, in various countries, is for people over 44 years old [3,61,62,63,64,65]. Another determinant factor are chronic illnesses in the patients, such as diverse respiratory diseases of the Chronic Obstructive Pulmonary Disease (COPD) type [66,67,68,69,70,71], asthma [72,73], chronic kidney disease [74,75], cardiovascular disease [76,77,78,79,80,81], hypertension [82,83,84,85], and obesity [86,87,88,89,90,91,92,93,94,95,96], as well as diverse forms of diabetes [97,98,99,100,101,102,103,104,105].
4.1. Diabetes and COVID-19
Diabetes mellitus is one of the pandemics that have been increasing dramatically in recent decades; the incidence is no longer exclusive to developed countries, in that various developing countries are now among those in which this metabolic problem is considered a national health problem [106]. The principal sign of diabetes is the elevation of blood glucose levels as a result of different issues including deficient production of insulin, to the lack of response to insulin by the insulin receptors, a deficiency in insulin transporters, or even problems in the immune system [107,108,109,110,111].
Several studies have found that, among the diverse comorbilities that contribute to the mortality of patients with COVID-19, diabetes occupies one of the first places, and it has been proposed that this is due to in these patients, there is a high expression of the angiotensin-converting enzyme 2 receptor (ACE2), which increases mortality up to 2-fold [105,112]- Other studies go further and have proposed that this ACE2 receptor is also highly expressed in the pancreatic cells, and that therefore, SARS-CoV-2 virus would affect the pancreas, causing more severe hyperglycemia [113,114]. At present there is no pharmacological cure in cases of diabetes mellitus, as well as for COVID-19. There are drugs that aid in controlling blood glucose levels in diabetic patients and, as noted in previous paragraphs, palliative therapies are being studied for the signs and symptoms of the disorder cause by the SARS-COV-2 virus. In this respect, although at the moment of writing these lines, the first vaccines against SARS-CoV-2 are being approved, some studies mention that the use of alternative therapies related with the secondary metabolites of different plants could be a useful coadjuvant in diabetic patients infected with SARS-CoV-2.
4.2. Secondary Metabolites with a Potential Effect on Diabetic Patients COVID-19
One example of a secondary metabolite that has been used for diverse respiratory pathologies caused by SARS-CoV-2-like viruses and that also have been assayed previously in diabetes is resveratrol, a compound obtained from diverse plant species such as the grape. Evidence was found that this metabolite significantly inhibits the in-vitro replication of the Middle East Respiratory Syndrome Coronavirus (MERS-CoV) through the inhibition the production of RNA; it has also been reported that it diminishes the expression of the MERS-CoV nucleocapside, a protein essential for its replication [115,120]. Perhaps the key to the clinical effectiveness of resveratrol in diabetes and COVID-19-related disorders is associated with the antioxidant properties. On this regard, it should be taken into consideration that in many chronic-degenerative and in viral-type diseases, an imbalance in oxide-reduction reactions can be present as a risk factor, which can produce free radicals that aggravate such illnesses [121,122]. In most of the cases, when these oxidative imbalances are present and there is an increase of free radicals, endogenous mechanisms are activated to diminish the concentrations of these radicals by means of the so-called endogenous antioxidant agents, such as the enzymes catalase, glutathione peroxidase, and superoxide dismutase, among others [123]. In patients with COVID-19, the so-called “cytokine storm” presents, which leads to states of hyperinflammation, which in turn leads to the generation of free radicals, aggravating the pathological state in these patients as well as in those previously diagnosed with diabetes [124]. In normal health conditions, under stressful conditions, for example physical exercise, the antioxidant protector system is activated that is modulated by the Nuclear factor erythroid 2-related factor 2 (Nrf2) transcription factor, which regulates the endogenous antioxidant response as a natural defense under physiological as well as chronic pathological conditions including diabetes [125,126,127]. Based on the latter, such as alternatives to the pharmacological treatment of patients with COVID-19 and, while the massive production is achieved of the different vaccines that are already being applied, in some countries the proposal is being implemented of nutritional changes in these patients, using the traditional ethnomedical knowledge of natural products. China can be cited as an example, where the State Administration of Traditional Chinese Medicine reports that the administration of a traditional remedy known as the “Qingfei Paidu Decoction”, which is elaborated with Ephedra, Almond, Polyporus, and Citrus aurantium, among other natural products, exhibited an effectivity rate higher than 90% in patients with COVID-19 [9]. Another example is found in Mexico, a country with a very ancient and widely extended herbolistic tradition where popular writings are beginning to be published, inviting the population to protect itself from SARS-CoV-2 by changing the nutritional customs and using herbal remedies as prophylactics [128]. In addition, a study carried out in patients in the Mexican health sector reports that the drug Nasoil®, which possesses, among its active components, the Asclepias curassavica extract, increases the respiratory capacity of patients [129].
All this evidence leads us to think that several of the products focusing on patients with diabetes that were cited in diverse publications could be effective in patients with COVID-19 thanks to its antioxidant properties. For this reason, we will present herein a brief description of some of these natural products or secondary metabolites with potential use in these patients.
4.2.1. Copper and N-Acetylcysteine
Copper possess multiple properties, among which antiviral activity and the inhibition of inflammatory processes are highlighted. On the other hand, N-acetylcysteine is a precursor of the amino acid L-cysteine, which acts as a free radical scavenger of Reactive Oxygen Species. It has been proposed that the combination of these would aid in diminishing the severity of the inflammatory events in the respiratory airways of patients with COVID-19 [129]. In this case, one should bear in mind that N-acetylcysteine has also been utilized in studies for the treatment of diabetes; for example, it can be mentioned that the administration of N-acetylcysteine in C57BL/6J mice t treated with Streptozotocin (STZ) activates the endogenous antioxidant systems and protects against thrombotic events [130], while promoting the peripheral uptake of glucose and diminishing plasma and hepatic cholesterol in models with diabetic animals [131].
4.2.2. Quercetin
This is a flavonoid widely found in diverse plants species with anti-inflammatory, anticancer, and antioxidant properties [132,133]. Paradoxically, quercetin could possess pro-oxidant effects, but there is evidence that, when administered with vitamin C, it could diminish this risk in patients with COVID-19 [133]. When administered in animals with diabetes, it was found that it diminishes the levels of lipid peroxidation [134,135]. In addition, quercetin has the advantage of penetrating the Blood-Brain Barrier (BBB), something that could be beneficial in diabetic patients recovering from COVID-19 [136].
4.2.3. Houttuynia cordata
This is a perennial herbaceous plant of the Saururaceae Family of Asian origin, with evidence of its effectiveness in respiratory disorders such as pneumonia. A study indicates that Houttuynia cordata exerts an inhibitory effect on the 3C-like protease (3CLpro) and on the RNA-dependent RNA polymerase (RdRp) of SARS CoV [137]. There is also evidence that the aqueous extract of this plant, administered together with metformin, inhibits the production of inflammatory cytokines and diminishes the degree of glucose tolerance in mice fed with a carbohydrate-rich diet [138]. Another study demonstrated that the administration of the alcoholic extract of Houttuynia cordata increased the plasma levels of insulin, something that was related with an upregulation in the expression of the GLUT-2 and GLUT-4 transporters of the glucose [139].
4.2.4. Laurus nobilis
A case that attracts out attention is one that was reported in Italy. The majority of SARS-CoV-2 contagions were concentrated in the northern part of the country, while in the South few cases had been detected in May 2020 [140]. It is proposed that this could have been due to that, in the South of Italy, there are more wooded zones with different species such as Laurus nobilis, which is a typically Mediterranea tree, this specie could possess a protector effect due to the emission of volatile organic immunomodulatory compounds. In the study of potentially protector compounds, by means of in-silico analysis in Laurus nobilis, the authors described a potential activity of the laurusides against COVID-19 [140,141]. L. nobilis specie is widely distributed worldwide and has also been associated with beneficial effects in reducing glycemia when its triturated leaves (powder) have been supplemented in cookies in diabetic subjects [142]. Something similar was also found using capsules containing between 1 and 3 g of the leaves extract of L. nobilis that were administered to patients with type 2 diabetes [143]. In our laboratory, we are currently working with the methanolic extract of L. nobilis in mice treated with Streptozotocin, and it was found that after the intragastric (i.g.) administration of this extract during 6 weeks, the rise in the blood glucose levels was avoided in hyperglycemic animals (Figure 2).
4.2.5. Naringenin
Naringenin is a flavonoid found in diverse citric plants, such as orange and grapefruit, with antiviral, anti-inflammatory, and antioxidant properties. Recently, it was determined that it is capable of inhibiting the protease 3CLpro, and it recude the activity of ACE2 receptors in molecular docking studies [144,145]. It is logical to think that, due to its antioxidant properties, it could also exert a therapeutic effect on diabetic patients. In effect there is a review article on these actions in diverse in-vitro and animal models, finding that this is achieved because of the capacity of increasing glucose uptake tissues such as muscle [146]. Another study reports that naringenin, in 25-50-mg/kg doses combined with Lisinopril (10 mg/kg) in rats treated with Streptozotocin attenuated renal oxidative stress [147].
4.2.6. Naringin
Molecular docking studies showed that there has been evidence that naringin, a flavonoid-like compound present in various citrics such as orange, was capable of inhibiting the protease (6LU7) of SARS-CoV-2s due to its antioxidant and anti-inflammatory properties [148,149]. On the other hand, it was also found that naringin increased the expression of mRNA and protein of transcription factor FoxM1 in pancreatic beta cells in diabetic rats, while it diminished the blood values of some parameters such as glucose [150], glucose-6-fosfatase activity, and an uptake of blood glucose by peripheral tissues such as skeletal muscle [151].
4.2.7. Azadirachta indica
As mentioned in previous paragraphs, our Laboratory has been focused on searching for alternative therapies for ther treatment of diabetes. Since 2006, we have utilized a great variety of extracts of plant origin in chemical models of diabetes in mice. We have found various plants with a clear glucose-lowering effect on these models, such as Moringa oleifera, Passiflora edulis, and Azadirachta indica, all with high antioxidant activity and perhaps possessing promoter effects in improvement glucose uptake [152]. In this way, we focus on specialized literature about the possible effects of A. indica or its active metabolites against COVID-19, finding seven publications which highlighted that some of the secondary metabolites of this tree can inhibit the expression of the M and E proteins of the virus. Within secondary metabolites are mentioned nimocin, phytosterol, beta-amyrin, and nimbolin-A, among others, are mentioned. These recent works are summed up in Table 1 [153,154,155,156,157,158,159].
4.2.8. Vitamin C
Several years ago, it was determined that the vitamin C (ascorbate), contained in many fruits (e.g., orange, grapefruit, lemon), has many pharmacological and therapeutic properties. For example, it is a metabolite with antioxidant properties that, in diabetic patients, is found at low plasma levels, which increases glucose intolerance [160,161]. To these properties we must add the properties of being capable of increasing the production of the PGE1 and PGI2 and promoting the formation of lipoxin A4, which in turn also possesses anti-inflammatory and antioxidant properties with the consequent therapeutic benefit for patients with diabetes or with other associated pathologies [162]. These properties can contribute to the cytokine storm that has been described in patients with COVID-19; in fact, there is evidence that the intravenous administration of vitamin C at high doses for various days in these patients reduces the probabilities of their being admitted to intensive care units as well as the mortality rate of [163]. Other results reported with these high doses of vitamin C (e.g., 12 g) in reference to the cytokine storm is a reduction of Interleukin 6 (IL-6) and Interleukin 10 (IL-10), as well as an increase in the number of assisted ventilation-free days in patients with COVID-19 [164].
5. Conclusions
We described the recent findings on alternative therapies in the treatment of COVID-19 and diabetes. However, we think that several of the examples described in this review deserve to be taken into account once that effective therapies are established against both pathologies, in that surely physicians will confront both in their patients sooner or later. Several of the examples of cited contain information on the antiviral and hypoglycemic activity of secondary metabolites or natural extracts of plants that have been in use for a long time in Traditional Medicine. It is a good time to pick up again and reevaluate the potential that these compounds have for health, in order for them to taken into account, not only in the search for effective drugs for treatment, but also for their inclusion in prophylactic measures from the nutritional level or nutritional supplementation in each country, above all in those considered as developing nations. At the time of writing these lines, the first vaccines against SARS-CoV-2 are arriving at diverse parts of the world to be administered to health personnel in the first line of defense against the pandemic. Notwithstanding this, it will be several months before the greater part of the population will be protected against the virus, and although safety is lacking in terms of there not being secondary adverse effects due to the utilization in record time of these vaccines in humans. We think that this opens up the possibility of continuing to search for alternate therapies that are clinically safe and with ease-of-access in the population in general. Therefore, it can be affirmed that the review article that took shape in this writing still has continuity and could be expanded in the near future.
Perspectives
Despite of the development of the vaccine against SARS-CoV-2, it is vital to continue efforts in the search for molecules that improving the patients’ quality life, while they have COVID-19 and also when they overcome the disease the diabetes persist. On the other hand, diabetes is a critical factor in the survival of patients who are facing this pathogen. It would be convenient count on drugs that can aid to overcoming these pandemics simultaneously and improve their life expectancy, providing a better better treatment and with the employment of fewer drugs because the abuse of drugs has repercussions on health, on generating processes of toxicity in diverse organs, such as liver, kidney, and digestive tract. In this regard, this review has the aim of serve as a base for the elaboration of research projects focused on the clinical evaluation of the beneficial effects of some natural products or nutritional supplements that can function as auxiliaries in diabetic patiens with COVID-19.
References
- World Health Organization, WHO. (2020). Coronavirus disease 2019 (COVID-19) situation report–52. March 12, 2020. https://www.who.int/docs/default-source/coronaviruse/20200312-sitrep-5 2-covid-19.pdf?sfvrsn¼e2bfc9c0_2 (accessed on 26 October 2020).
- World Health Organization, WHO (2020). World experts and funders set priorities for COVID-19. https://www.who.int/news-room/detail/12-02-2020-world-experts-and-funders-set-priorities-for-covid-19-research (accessed on 28 October 2020).
- Tian, S.; Hu, N.; Lou, J.; Chen, K.; Kang, X.; Xiang, Z.; Chen, H.; Wang, D.; Liu, N.; Liu, D.; Chen, G.; Zhang, Y.; Li, D.; Li, J.; Lian, H.; Niu, S.; Zhang, L.; Zhang, J. Characteristics of COVID-19 infection in Beijing. J. Infection 2020, 80, 401–406. [Google Scholar] [CrossRef]
- Beijing Health Commission. Update on the novel coronavirus pneumonia outbreak. February 10, 2020. Beijing: Beijing Health Commission; 2020. http://wjw.beijing.gov.cn/xwzx_20031/wnxw/202002/t20200211_1628034.html (accessed on 28 October 2020).
- Lu, H.; Stratton, C.W.; Tang, Y.W. Outbreak of pneumonia of unknownetiology in Wuhan China: the mystery and the miracle. J. Med.Virol. 2020, 92, 401–402. [Google Scholar] [CrossRef]
- Ren, L.L.; Wang, Y.M.; Wu, Z.Q.; Xiang, Z.C.; Guo, L.; Xu, T.; Jiang, Y.Z.; Xiong, Y.; Li, Y.J.; Li, X.W.; Li, H.; Fan, G.H.; Gu, X.Y.; Xiao, Y.; Gao, H.; Xu, J.Y.; Yang, F.; Wang, X.M.; Wu, C.; Chen, L.; Liu, Y.W.; Liu, B.; Yang, J.; Wang, X.R.; Dong, J.; Li, L.; Huang, C.L.; Zhao, J.P.; Hu, Y.; Cheng, Z.S.; Liu, L.L.; Qian, Z.H.; Qin, C.; Jin, Q.; Cao, B.; Wang, J.W. Iden-tification of a novel coronavirus causing severe pneumonia in human: a descriptive study. Chin Med J. 2020, 133, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Yang, L.X.; Wang, G.X.; Hu, B.; Zhang, L.; Zhang, W.; Guo1, H.; Jiang, R.D.; Liu, M.Q.; Chen, Y.; Shen, X.R.; Wang, X.; Zheng, X.S.; Zhao, K.; Chen, Q.J.; Deng, F.; Liu, L.L.; Yan, B.; Zhan, F.X.; Wang, Y.Y.; Xiao, G.F.; Shi, Z.L. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Zhao, S.; Yu, B.; Chen, M.Y.; Wang, W.; Song, G.Z.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; Yuan, M.L.; Zhang, Y.L.; Dai, F.H.; Liu, Y.; Wang, Q.M.; Zheng, J.J.; Xu, L.; Holmes, E.C.; Zhang, W.Z. A new coronavirus associated with human respiratory disease in China. Nature. 2020, 579, 265–269. [Google Scholar] [CrossRef]
- Han, Y.J.; Ren, Z.G.; Li, X.X.; Yan, J.L.; Ma, C.Y.; Wu, D.D.; Ji, X.Y. Advances and challenges in the prevention and treatment of COVID-19. Int. J. Med. Sci. 2020, 17, 1803–1810. [Google Scholar] [CrossRef] [PubMed]
- García, L.F. Immune response, inflammation and the clinical spectrum of COVID-19. Front. Immunol. 2020, 11, 1441. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization WHO. (2020). Naming the coronavirus disease (COVID-19) and the virus that causes it. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 28 October 2020).
- De Groot RJ, Baker SC, Baric R, Enjuanes L, Gorbalenya AE, Holmes KV, Perlman S, Poon L, Rootier PJM, Talbot PJ, Woo PCY, Ziebuhr J. (2012). Family coronaviridae: Part ii. The positive sense single stranded RNA viruses. In: Virus taxonomy: Classification and nomenclature of viruses. King A, Adams M, Carstens E, Lefkowitz E (eds.). Elsevier/Academic Press: Amsterdam, Boston, pp. 806–820.
- Schoeman, D.; Fielding, B.C. Coronavirus envelope protein: current knowledge. Virol. J. 2019, 16, 69. [Google Scholar] [CrossRef] [PubMed]
- Li, F. Receptor Recognition Mechanisms of Coronaviruses: a Decade of Structural Studies. 2015, 89, 1954–1964. [CrossRef]
- Centers for Disease Control and Prevention. 2019 Novel Coronavirus (2019-nCoV) Transmission. https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/how-covid-spreads.html?CDC AA refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fprepare%2Ftransmission.html (accessed on 6 November 2020).
- Walls, A.C.; Park, Y.J.; Tortorici, M.A.; Wall, A.; Mcguire, A.T.; Veesler, D. Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell. 2020, 181, 281–292. [Google Scholar] [CrossRef]
- Li, W.; Moore, M.J.; Vasilieva, N.; Sui, J.; Wong, S.K.; Berne, M.A.; Somasundaran, M.; Sullivan, J.L.; Luzuriaga, K.; Greenough, T.C.; Choe, H.; Farzan, M. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 2003, 426, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Kruger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; Muller, M.A.; Drosten, C.; Pohlmann, S. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020, 181, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Perlman, S.; Netland, J. Coronaviruses post-sars: Update on replication and pathogenesis. Nat. Rev. Microbiol. 2009, 7, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Cantuti-Castelvetri L, Ohja R, Pedro, L, Djannatian M, Franz, J, Kuivanen S, Kallio K, Kaya T, Anastasina M, Smura T, Levanov L, Szirovicza L, Tobi A, Kallio-Kokko H, Osterlund P, Joensuu M, Meunier F, Butcher S, Winkler M, Mollenhauer B, Helenius A, Gokce O, Teesalu T, Hepojoki J, Vapalahti O, Stadelmann C, Balistreri G, Simons M. (2020). Neuropilin-1 facilitates SARS-CoV-2 cell entry and provides a possible pathway into the central nervous system. bioRxiv. [CrossRef]
- García, L.F. Immune response, inflammation, and the clinical spectrum of COVID-19. Front. Immunol. 2020, 11, 1441. [Google Scholar] [CrossRef] [PubMed]
- Perlman, S.; Dandekar, A.A. Immunopathogenesis of coronavirus infections: implications for SARS. Nat. Rev. Immunol. 2005, 5, 917–927. [Google Scholar] [CrossRef]
- Tay, M.Z.; Poh, M.C.; Rénia, L.; MacAry, A.P.; Ng, L.F.P. The trinity of COVID-19: immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Sch€onrich, G.; Raftery, M.J.; Samstag, Y. Devilishly radical NETwork in COVID-19: Oxidative stress, neutrophil extracellular traps (NETs), and T cell suppression. Adv. Biol. Reg. 2020, 77, 100741. [Google Scholar] [CrossRef]
- Esakandari1, H.; Nabi-Afjadi, M.; Fakkari-Afjadi, J.; Farahmandian, N.; Miresmaeili, S.M.; Bahrein, E. A comprehensive review of COVID-19 characteristics. Biol. Procs. Online. 2020, 22, 19. [Google Scholar] [CrossRef] [PubMed]
- Lovato, A.; de Filippis, C.; Marioni, G. Upper airway symptoms in coronavirus disease 2019 (COVID-19). Am. J. Otolaryngol. 2020, 41, 102474. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Zhong, Z.; Ji, P.; Li, H.; Li, B.; Pang, J.; Zhang, J.; Zhao, C. Clinicopathological characteristics of 8697 patients with COVID-19 in China: a meta-analysis. Fam Med Commun Health. 2020, 8, e000406. [Google Scholar] [CrossRef]
- Yan, C.; Cui, J.; Huang, L.; Du, B.; Chen, L.; Xue, G.; Li, S.; Zhang, W.; Zhao, L.; Sun, Y.; Yao, H.; Li, N.; Zhao, H.; Feng, Y.; Liu, S.; Zhang, Q.; Liu, D.; Yuan, J. Rapid and visual detection of 2019 novel coronavirus (SARS-CoV-2) by a reverse transcription loopmediated isothermal amplification assay. Clin. Microbiol. Infect. 2020, 26, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Rettner R. (2020). How does the new coronavirus compare with the flu? Live Sci. 25.
- Paranjpe I, Russak A, De Freitas JK, Lala A, Miotto R, Vaid A, Johnson KW, Danieletto M, Golden E, Meyer D, Singh M, Somani S, Manna S, Nangia U, Kapoor A, O’Hagan A, O’Reilly PF, Huckins LM, Glowe P, Kia A, Timsina P, Freeman RM, Levin MA, Jhan J, Firpo A, Kovatch P, Finkelstein J, Aberg JA, Bagiella E, Horowitz CR, Murphy B, Fayad BZ, Narula J, Nestler EJ, Fuster V, Cordon-Cardo C, Charney DS, Reich DL, Just AC, Bottinger EP, Charney AW, Glicksberg BS, Nadkarni GN. (2020). Clinical Characteristics of Hospitalized Covid-19 Patients in New York City. medRxiv. [CrossRef]
- Ruan Q, Yang K, Wang W, Jiang L, Song J. (2020). Clinical predictors of mortality due to covid-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; Guan, L.; Wei, Y.; Li, H.; Wu, X.; Xu, J.; Tu, S.; Zhang, Y.; Chen, H.; Cao, B. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet. 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Conti, P.; Ronconi, G.; Carafa, A.; Gallenga, C.E.; Ross, R.; Frydas, I.; Kritas, S.K. Induction of pro-inflammatory cytokines (IL-1 and IL-6) and lung inflammation by coronavirus-19 (COVID-19 or SARS-CoV-2): Anti-inflammatory strategies. J. Biol. Regul. Homeost. Agents. 2020, 34, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; Tai, Y.; Bai, C.; Gao, T.; Song, J.; Xia, P.; Dong, J.; Zhao, J.; Wang, F.S. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Martín-Giménez, V.M.; Inserra, F.; Tajer, C.D.; Mariani, J.; Ferder, L.; Reiter, R.J.; Manuch, W. Lungs as target of COVID-19 infection: Protective common molecular mechanisms of vitamin D and melatonin as a new potential synergistic treatment. Life Sci. 2020, 254, 117808. [Google Scholar] [CrossRef]
- Belen-Apak, F.B.; Sarıalioğlu, F. Pulmonary intravascular coagulation in COVID-19: possible pathogenesis and recommendations on anticoagulant/thrombolytic therapy. J. Thromb. Thrombolysis. 2020, 50, 278–280. [Google Scholar] [CrossRef]
- Li Y, Xiao SY. (2020). Hepatic involvement in COVID-19 patients: Pathology, pathogenesis, and clinical implications. J. Med. Virol. [CrossRef]
- Rothan, H.A.; Byrareddy, S.N. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J. Autoimmunity 2020, 109, 102433. [Google Scholar] [CrossRef]
- World Health Organization, WHO. (2020). COVID-19 Weekly Epidemiological Update. www.who.int/publications/m/item/weekly-epidemiological-update---24-november-2020 (accessed on 24 November 2020).
- Momattin, H.; Mohammed, K.; Zumla, A.; Memish, Z.A.; Al-Tawfiq, J.A. Therapeutic options for middle east respiratory syndrome coronavirus (MERS-CoV): possible lessons from a systematic review of SARS-CoV therapy. Int. J. Infect. Diseases. 2013, 17, e792–e798. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Kim, K.H.; Yi, J.; Choi, S.J.; Choe, P.G.; Park, W.B.; Kim, N.J.; Oh, M.D. In vitro antiviral activity of ribavirin against severe fever with thrombocytopenia syndrome virus. Korean J. Intern. Med. 2017, 32, 731–737. [Google Scholar] [CrossRef]
- Agostini, M.L.; Andres, E.L.; Sims, A.C.; Graham, R.L.; Sheahan, T.P.; Lu, X.; Smith, E.C.; Case, J.B.; Feng, J.Y.; Jordan, R.; Ray, A.S.; Cihlar, T.; Siegel, D.; Mackman, R.L.; Clarke, M.O.; Baric, R.S.; Denison, M.R. Coronavirus susceptibility to the antiviral remdesivir (GS5734) is mediated by the viral polymerase and the proofreading exoribonuclease. mBio. 2018, 9, e00221–18. [Google Scholar] [CrossRef] [PubMed]
- Samuel, C.E. Antiviral Actions of Interferons. Clin. Microbiol. Rev. 2001, 14, 778–809. [Google Scholar] [CrossRef]
- Morgenstern, B.; Michaelis, M.; Baer, P.C.; Doerr, H.W.; Cinatl, J. Ribavirin and interferon-β synergistically inhibit SARS-associated coronavirus replication in animal and human cell lines. Biochem. Biophys. Res. Commun. 2005, 326, 905–908. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Chen, V.; Shannon, C.P.; Wei, X.S.; Xiang, X.; Wang, X.; Wang, Z.H.; Tebbutt, S.J.; Kollmann, T.R.; Fish, E.N. Interferon-α2b treatment for COVID-19. Front. Inmmunol. 2020, 11, 1061. [Google Scholar] [CrossRef] [PubMed]
- Davoudi-Monfared, E.; Rahmani, H.; Khalili, H.; Hajiabdolbaghi, M.; Salehi, M.; Abbasian, L.; Kazemzadeh, H.; Yekaninejad, M.S. A randomized clinical trial of the efficacy and safety of interferon-1a in treatment of severe COVID-19. Antimicrob. Agents Chemother. 2020, 64, e01061–20. [Google Scholar] [CrossRef] [PubMed]
- De Wilde, A.H.; Pham, U.; Posthuma, C.C.; Snijder, E.J. Cyclophilins and cyclophilin inhibitors in nidovirus replication. Virol. 2018, 522, 46–55. [Google Scholar] [CrossRef]
- Tanaka, Y.; Sato, Y.; Sasaki, T. Suppression of coronavirus replication by cyclophilin inhibitors. Viruses. 2013, 5, 1250–1260. [Google Scholar] [CrossRef] [PubMed]
- Ma-Lauera Y, Zhenga Y, Maleševićc M, von Brunna B, Fischerd G, von Brunn A. (2020). Influences of cyclosporin A and non-immunosuppressive derivatives on cellular cyclophilins and viral nucleocapsid protein during human coronavirus 229E replication. Antiv. Res.173, 104620. [CrossRef]
- Poulsen NN, von Brunn A, Hornum M, Jensen MB. (2020). Cyclosporine and COVID-19: risk or favorable?. Am. J. Transplant. [CrossRef]
- Keyaerts, E.; Vijgen, L.; Maes, P.; Neyts, J.; Ranst, M.V. In vitro inhibition of severe acute respiratory syndrome coronavirus by chloroquine. Biochem. Biophys. Res. Commun. 2004, 323, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Touret, F.; de Lamballerie, X. Of chloroquine and COVID-19. Antivir. Res. 2020, 177, 104762. [Google Scholar] [CrossRef]
- Ibáñez S, Martínez O, Valenzuela F, Silva F, Valenzuela O. (2020). Hydroxychloroquine and chloroquine in COVID-19: should they be used as standard therapy? Clin. Rheumatol. [CrossRef]
- Gautret, P.; Lagier, L.C.; Parolaa, P.; Hoanga, V.T.; Meddeba, L.; Mailhea, M.; Doudier, B.; Courjone, J.; Giordanengo, V.; Vieiraa, V.E.; Dupont, H.T.; Stéphane Honoréi, S.; Colsona, P.; Chabrièrea, E.; La Scolaa, B.; Rolaina, J.M.; Brouqui, P.; Raoult, D. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. Int. J.Antimicrob. Agents. 2020, 56, 105949. [Google Scholar] [CrossRef]
- Coleman, C.M.; Sisk, J.M.; Mingo, R.M.; Nelson, E.A.; White, J.M.; Frieman, M.B. Abelson Kinase Inhibitors are potent inhibitors of severe acute respiratory syndrome coronavirus and middle east respiratory syndrome coronavirus fusion. J. Virol. 2016, 90, 8924–8933. [Google Scholar] [CrossRef]
- Morales-Ortega, A.; Bernal-Bello, D.; Llarena-Barroso, C.; Frutos-Pérez, B.; Duarte-Millán, M.A.; de Viedma-García, V.G.; Farfán-Sedano, A.I.; Canalejo-Castrillero, E.; Ruiz-Giardín, J.M.; Ruiz-Ruiz, J.; San Martín-López, J.V. Imatinib for COVID-19: A case report. Clin. Immunol. 2020, 218, 108518. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, M. COVID-19-driven endothelial damage: complement, HIF-1, and ABL2 are potential pathways of damage and targets for cure. Ann. Hematol. 2020, 99, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- Shanmugaraj, B.; Siriwattananon, K.; Wangkanont, K.; Phoolcharoen, W. Perspectives on monoclonal antibody therapy as potential therapeutic intervention for Coronavirus disease-19 (COVID-19). Asian Pac. J. Allergy Immunol. 2020, 38, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Sempowski, G.D.; Saunders, K.O.; Acharya, P.; Wiehe, K.J.; Haynes, B.J. Pandemic preparedness: developing vaccines and therapeutic antibodies for COVID-19. Cell. 2020, 181, 1458–1463. [Google Scholar] [CrossRef] [PubMed]
- Saghazadeha, A.; Rezaei, N. Towards treatment planning of COVID-19: Rationale and hypothesis for the use of multiple immunosuppressive agents: Anti-antibodies, immunoglobulins, and corticosteroids. Int. Immunopharmacol. 2020, 84, 106560. [Google Scholar] [CrossRef]
- Lauc, G.; Sinclair, D. Biomarkers of biological age as predictors of COVID-19 disease severity. Aging. 2020, 12, 6490–6491. [Google Scholar] [CrossRef] [PubMed]
- Mueller, A.L.; McNamara, M.S.; Sinclair, D.A. Why does COVID-19 disproportionately affect older people? Aging. 2020, 12, 9959–9981. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, N.M.; Selim, L.A. Characterisation of COVID-19 pandemic in paediatric age group: a systematic review and meta-Analysis. J. Clin. Virol. 2020, 128, 104395. [Google Scholar] [CrossRef]
- Imam, Z.; Odish, F.; Gill, I.; O’Connor, D.; Armstrong, J.; Vanood, A.; Ibironke, O.; Hanna, A.; Ranski, A.; Halalau, A. Older age and comorbidity are independent mortality predictors in a large cohort of 1305 COVID-19 patients in Michigan, United States. J. Intern. Med. 2020, 288, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Giannouchos TV, Sussman RA, Mier JM, Poulas K, Farsalinos K. (2020). Characteristics and risk factors for COVID-19 diagnosis and adverse outcomes in Mexico: an analysis of 89,756 laboratory–confirmed COVID-19 cases. Eur. J. Resp. [CrossRef]
- Burki, T.K. Coronavirus in China. Lancet Respir Med. 2020, 8, 238. [Google Scholar] [CrossRef]
- Li, X.; Ma, X. Acute respiratory failure in COVID-19: is it “typical” ARDS? Critical Care. 2020, 24, 198. [Google Scholar] [CrossRef] [PubMed]
- Goh, K.J.; Choong, M.C.; Cheong, E.H.; Kalimuddin Wen, S.D.; Phua, G.C.; Chan, K.S.; Mohideen, S.H. Rapid progression to acute respiratory distress Syndrome: review of current understanding of critical illness from coronavirus disease 2019 (COVID-19) Infection. Ann. Acad. Med. Singap. 2020, 49, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Grieco, D.L.; Bongiovanni, F.; Chen, L.; Menga, L.S.; Cutuli, S.L.; Pintaudi1, G.; Carelli, S.; Michi1, T.; Torrini, F.; Lombardi, G.; Anzellotti1, G.M.; De Pascale, G.; Urbani, A.; Bocci, M.G.; Tanzarella, E.S.; Bello, G.; Dell’Anna, A.M.; Maggiore, S.M.; Brochard, L.; Antonelli, M. Respiratory physiology of COVID-19- induced respiratory failure compared to ARDS of other etiologies. Crit Care. 2020, 24, 529. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.M.; Tam, A.; Shaipanich, T.; Hackett, T.L.; Singhera, G.K.; Dorscheid, D.R.; Sin, D.D. ACE-2 expression in the small airway epithelia of smokers and COPD patients: implications for COVID-19. Eur. Respir. J. 2020, 55, 2000688. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Meng, M.; Kumar, R.; Wu, Y.; Huang, J.; Lian, N.; Deng, Y.; Lin, S. The impact of COPD and smoking history on the severity of COVID-19: A systemic review and meta-analysis. J. Med. Virol. 2020, 92, 1915–1921. [Google Scholar] [CrossRef]
- Liu, S.; Zhi, Y.; Ying, S. COVID-19 and asthma: reflection during the pandemic. Clinic. Rev. Allerg. Immunol. 2020, 59, 78–88. [Google Scholar] [CrossRef]
- Chhiba, K.D.; Patel, G.B.; Vu, T.H.T.; Chen, M.M.; Guo, A.; Kudlaty, E.; Mai, Q.; Yeh, C.; Muhammad, L.N.; Harris, K.E.; Bochner, B.S.; Grammar, L.C.; Greenberger, P.A.; Kalhan, R.; Kuang, F.L.; Saltoun, C.A.; Schleimer, R.P.; Stevens, W.W.; Peters, A.T. Prevalence and characterization of asthma in hospitalized and nonhospitalized patients with COVID-19. J. Allergy Clin. Immunol. 2020, 146, 307–314.e4. [Google Scholar] [CrossRef] [PubMed]
- Adapa, S.; Chenna, A.; Balla, M.; Merugu, G.P.; Koduri, N.M.; Daggubati, S.R.; Gayam, V.; Naramala, S.; Konala, V.M. COVID-19 pandemic causing acute kidney injury and impact on patients with chronic kidney disease and renal transplantation. J. Clin. Med. Res. 2020, 12, 352–361. [Google Scholar] [CrossRef] [PubMed]
- Adapa, S.; Aeddula, N.R.; Konala, V.M.; Chenna, A.; Naramala, S.; Madhira, B.R.; Gayam, V.; Balla, M.; Muppidi, V.; Bose, S. COVID-19 and renal failure: challenges in the delivery of renal replacement therapy. J. Clin. Med. Res. 2020, 12, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Bansal, M. Cardiovascular disease and COVID-19. Diabetes Metab. Syndr. 2020, 14, 247–250. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; Huang, H.; Yang, B.; Huang, C. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in wuhan, china. JAMA Cardiol. 2020, 5, 802–807. [Google Scholar] [CrossRef]
- Dixon, D.L.; Van Tassell, B.W.; Vecchié, A.; Bonaventura, A.; Talasaz, A.H.; Kakavand, H.; D’Ascenzo, F.; Perciaccante, A.; Castagno, D.; Ammirati, E.; Biondi-Zoccai, G.; Stevens, M.P.; Abbate, A. Cardiovascular considerations in treating patients with corona virus disease 2019 (COVID-19). J. Cardiovasc. Pharmacol. 2020, 75, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Huang, Z.; Lin, L.; Lv, J. Coronavirus disease 2019 (COVID-19) and cardiovascular disease: A viewpoint on the potential influence of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers on onset and severity of severe acute respiratory syndrome coronavirus 2 infection. J. Am. Heart Assoc. 2020, 9, e016219. [Google Scholar] [CrossRef] [PubMed]
- Pallarés-Carratalá, V.; Górriz-Zambrano, C.; Morillas-Ariño, C.; Llisterri-Caro, J.L.; Gorriz, J.L. COVID-19 y enfermedad cardiovascular y renal: ¿Dónde estamos?¿hacia dónde vamos?. Semergen 2020, 46 (Suppl. 1), 78–87. [Google Scholar] [PubMed]
- Li, B.; Yang, J.; Zhao, F.; Zhi, L.; Wang, X.; Liu, L.; Bi, Z.; Zhao, Y. Prevalence and impact of cardiovascular metabolic diseases on COVID-19 in China. Clin. Res. Cardiol. 2020, 109, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Tadic, M.; Cuspidi, C.; Mancia, G.; Dell’Oro, R.; Grassi, G. COVID-19, hypertension and cardiovascular diseases: Should we change the therapy? Pharmacol. Res. 2020, 158, 104906. [Google Scholar] [CrossRef] [PubMed]
- Tadic, M.; Cuspidi, C.; Grassi, G.; Mancia, G. COVID-19 and arterial hypertension: Hypothesis or evidence? J. Clin. Hypertens. 2020, 22, 1120–1126. [Google Scholar] [CrossRef]
- Kulkarni, S.; Jenner, B.L.; Wilkinson, I. COVID-19 and hypertension. J. Renin Angiotensin Aldosterone Syst. 2020, 21, 1470320320927851. [Google Scholar] [CrossRef] [PubMed]
- Farha S. (2020). COVID-19 and pulmonary hypertension. Cleve. Clin. J. Med. ccc021. [CrossRef]
- Hussain, A.; Mahawar, K.; Xia, Z.; Yang, W.; EL-Hasani, S. Obesity and mortality of COVID-19. Meta-analysis. Obes. Res. Clin. Pract. 2020, 14, 295–300. [Google Scholar] [CrossRef]
- Caci, G.; Albini, A.; Malerba, M.; Noonan, D.M.; Pochetti, P.; Polosa, R. COVID-19 and obesity: Dangerous liaisons. J. Clin. Med. 2020, 9, 2511. [Google Scholar] [CrossRef]
- Ritter, A.; Kreis, N.N.; Louwen, F.; Yuan, J. Obesity and COVID-19: Molecular mechanisms linking both pandemics. Int. J. Mol. Sci. 2020, 21, 5793. [Google Scholar] [CrossRef]
- Maier, H.E.; Lopez, R.; Sanchez, N.; Ng, S.; Gresh, L.; Ojeda, S.; Burger-Calderon, R.; Kuan, G.; Harris, E.; Balmaseda, A.; Gordon, A. Obesity increases the duration of influenza A virus shedding in adults. J. Infect. Dis. 2018, 218, 1378–1382. [Google Scholar] [CrossRef] [PubMed]
- Moser, J.A.S.; Galindo-Fraga, A.; Ortiz-Hernández, A.A.; Gu, W.; Hunsberger, S.; Galán-Herrera, J.F.; Guerrero, M.L.; Ruiz-Palacios, G.M.; Beigel, J.H. Underweight, overweight, and obesity as independent risk factors for hospitalization in adults and children from influenza and other respiratory viruses. Influenza Other Respir. Viruses. 2019, 13, 3–9. [Google Scholar] [CrossRef]
- Sanchis-Gomar, F.; Lavie, C.J.; Mehra, M.R.; Henry, B.M.; Giuseppe Lippi, G. Obesity and outcomes in COVID-19: When an epidemic and pandemic collide. Mayo Clin. Proc. 2020, 95, 1445–1453. [Google Scholar] [CrossRef]
- Popkin, B.M.; Shufa Du, S.; Green, W.D.; Beck, M.A.; Algaith, T.; Herbst, C.H.; Alsukait, R.F.; Alluhidan, M.; Alazemi, N.; Shekar, M. Individuals with obesity and COVID-19: A global perspective on the epidemiology and biological relationships. Obes. Rev. 2020, 21, e13128. [Google Scholar] [CrossRef]
- De Lusignan, S.; Dorward, J.; Correa, A.; Jones, N.; Akinyemi, O.; Amirthalingam, G.; Andrews, N.; Byford, R.; Dabrera, G.; Elliot, A.; Ellis, J.; Ferreira, F.; Bernal, J.L.; Okusi, C.; Ramsay, M.; Sherlock, J.; Smith, G.; Williams, J.; Howsam, G.; Zambon, M.; Joy, M.; Hobbs, F.D.R. Risk factors for SARS-CoV-2 among patients in the Oxford Royal College of General Practitioners Research and Surveillance Centre primary care network: a cross-sectional study. Lancet Infect. Dis. 2020, 20, 1034–1042. [Google Scholar] [CrossRef]
- Rychter, A.M.; Zawada, A.; Ratajczak, A.E.; Dobrowolska, A.; Krela-Kaźmierczak, I. Should patients with obesity be more afraid of COVID-19? Obes. Rev. 2020, 21, e13083. [Google Scholar] [CrossRef]
- Petrova, D.; Salamanca-Fernández, E.; Rodríguez, B.M.; Navarro, P.P.; Jiménez, M.J.J.; Sánchez, M.J. Obesity as a risk factor in Covid-19: Possible mechanisms and implications. Aten. Primaria. 2020, 52, 496–500. [Google Scholar] [CrossRef]
- El Chaar, M.; King, K.; Galvez, L.A. Are black and hispanic persons disproportionately affected by COVID-19 because of higher obesity rates?. Surg. Obes. Relat. Dis. 2020, 16, 1096–1099. [Google Scholar] [CrossRef] [PubMed]
- Singer M. (2020). Deadly companions: COVID-19 and diabetes in Mexico. Med. Antrhopol. [CrossRef]
- Hussain, A.; Bhowmik, B.; Do Vale Moreira, N.C. COVID-19 and diabetes: Knowledge in progress. Diabetes Res. Clin. Pract. 2020, 162, 108142. [Google Scholar] [CrossRef] [PubMed]
- Tadic, M.; Cuspidi, C.; Sala, C. COVID-19 and diabetes: Is there enough evidence? J. Cli.n Hypertens. (Greenwich). 2020, 22, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Lau, E.S.H.; Ma, R.C.W.; Kong, P.S.A.; Wild, H.S.; Goggins, W.; Chow, E.; So, W.Y.; Chan, C.N.J.; Luk, O.Y.A. Secular trends in all-cause and cause-specific mortality rates in people with diabetes in Hong Kong, 2001–2016: a retrospective cohort study. Diabetol. 2020, 63, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Cuschieri, A.; Grech, S. COVID-19 and diabetes: The why, the what and the how. J. Diabetes Complications. 2020, 34, 107637. [Google Scholar] [CrossRef] [PubMed]
- Erener, S. Diabetes, infection risk and COVID-19. Mol. Metab. 2020, 39, 101044. [Google Scholar] [CrossRef] [PubMed]
- Muniyappa, R.; Gubbi, S. COVID-19 pandemic, coronaviruses, and diabetes mellitus. Am. J. Physiol. Endocrinol. Metab. 2020, 318, E736–E741. [Google Scholar] [CrossRef]
- Jeong, I.K.; Yoon, K.H.; Lee, M.K. Diabetes and COVID-19: Global and regional perspectives. Diabetes Res. Clin. Pract. 2020, 166, 108303. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Arora, A.; Sharma, P.; Anikhindi, S.A.; Bansal, N.; Singla, V.; Khare, S.; Srivastava, A. Is diabetes mellitus associated with mortality and severity of COVID19? A meta-analysis. Diabetes Metab. Syndr. 2020, 14, 535–545. [Google Scholar] [CrossRef]
- Bukhman, G.; Bavuma, C.; Gishoma, C.; Gupta, N.; Kwan, G.F.; Laing, R.; Beran, D. Endemic diabetes in the world’s poorest people. Lancet Diabetes Endocrinol. 2015, 3, 402–403. [Google Scholar] [CrossRef] [PubMed]
- Ruíz, J. Diabetes mellitus. Rev. Med. Suisse. 2012, 8, 88–90. [Google Scholar]
- Caruso, R.; Magon, A.; Irene Baroni, I.; Dellafore, F.; Arrigoni, C.; Pittella, F.; Ausili, D. Health literacy in type 2 diabetes patients: a systematic review of systematic reviews. Acta Diabetol. 2018, 55, 1–12. [Google Scholar] [CrossRef]
- IDF. (2019). Diabetes atlas. www.diabetesatlas.org (accessed on 29 December 2020).
- Guthrie, R.A.; Guthrie, D.W. Pathophisiology of diabetes mellitus. Crit. Care Nurs. Q. 2004, 27, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Forbes, J.M.; Cooper, M.E. Mechanisms of diabetic complications. Physiol. Rev. 2013, 93, 137–188. [Google Scholar] [CrossRef] [PubMed]
- De Almeida-Pititto, B.; Dualib, P.M.; Zajdenverg, L.; Rodrigues-Dantas Dias de Souza, F.; Rodacki, M.; Casaccia-Bertoluci, M. Severity and mortality of COVID 19 in patients with diabetes, hypertension and cardiovascular disease: a meta-analysis. Diabetol. Metab. Synd. 2020, 12, 75. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Long, X.; Zhang, B.; Zhang, W.; Chen, X.; Zhang, Z. ACE2 expression in pancreas may cause pancreatic damage after SARS-CoV-2 infection. Clin. Gastroenterol. Hepatol. 2020, 18, 2128–2130.e2. [Google Scholar] [CrossRef] [PubMed]
- Lima-Martínez MM, Carrera-Boada C, Madera-Silva MD, Marín W, Contreras M. (2020). COVID-19 and diabetes: a bidirectional relationship. Clin. Investig. Arterioscler. S0214-9168, 30105–4. [CrossRef]
- Drago, L.; Nicola, L.; Ossola, F.; De Vecchi, E. In vitro antiviral activity of resveratrol against respiratory viruses. J. Chemother. 2008, 20, 393–394. [Google Scholar] [CrossRef]
- Lin, A.C.; Ho, C.T.; Chuo, W.H.; Li, S.; Wang, T.T.; Lin, C.C. Effective inhibition of MERS-CoV infection by resveratrol. Infect. Diseases. 2017, 17, 144. [Google Scholar] [CrossRef]
- Marinella, M.A. Indomethacin and resveratrol as potential treatment adjuncts for SARS-CoV-2/COVID-19. Int. J. Clin. Pract. 2020, 74, e13535. [Google Scholar] [CrossRef]
- Ramdani, L.H.; Bachari, K. Potential therapeutic effects of resveratrol against SARS-CoV-2. Acta Virol. 2020, 64, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Öztürk, E.; Arslan, A.K.K.; Yerer, M.B.; Bishayee, A. Resveratrol and diabetes: A critical review of clinical studies. Biomed. Pharmacother. 2017, 95, 230–234. [Google Scholar] [CrossRef]
- Kulashekar, M.; Stom, S.M.; Peuler, J.D. Resveratrol’s potential in the adjunctive management of cardiovascular disease, obesity, diabetes, alzheimer disease, and cancer. J. Am. Osteopath. Assoc. 2018, 118, 596–605. [Google Scholar] [CrossRef] [PubMed]
- Luc, K.; Schramm-Luc, A.; Guzik, T.J.; Mikolajczyk, T.P. Oxidative stress and inflammatory markers in prediabetes and diabetes. J. Physiol. Pharmacol. 2019, 70, 809–824. [Google Scholar] [CrossRef]
- Camini, F.C.; Caetano, C.C.; Almeida, L.T.; De Brito Magalhães, C. Implications of oxidative stress on viral pathogenesis. Arch. Virol. 2017, 162, 907–917. [Google Scholar] [CrossRef] [PubMed]
- Fregoso-Aguilar TA, Hernández-Navarro BC, Mendoza-Pérez JA. (2016). Endogenous antioxidants: A review of their role in oxidative stress. In Morales-González JA, Morales-González A, Madrigal-Santillán EO (eds.). The transcription factor NRF2: A master regulator of oxidative stress. InTech. Croatia. 3–19. [CrossRef]
- Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, MansonJJ (2020). COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet. 395, 1033–1034. [CrossRef]
- Vargas-Mendoza, N.; Morales-González, A.; Madrigal-Santillán, E.O.; Madrigal-Bujaidar, E.; Álvarez-González, I.; García-Melo, L.F.; Anguiano-Robledo, L.; Fregoso-Aguilar, T.; Morales-Gonzalez, J.A. Antioxidant and adaptative response mediated by Nrf2 during physical exercise. Antioxidants. 2019, 8, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Morales-González, A.; Bautista, M.; Madrigal-Santillán, E.; Posadas-Mondragón, A.; Anguiano-Robledo, L.; Madrigal-Bujaidar, E.; Álvarez-González, I.; Fregoso-Aguilar, T.; Gayosso-Islas, E.; Sánchez-Moreno, C.; Morales-González, J.A. Nrf2 modulates cell proliferation and antioxidants defenses during liver regeneration induced by partial hepatectomy. Int. J. Clin. Exp. Pathol. 2017, 10, 7801–7811. [Google Scholar] [PubMed]
- Matzinger, M.; Fischhuber, K.; Heiss, E.H. Activation of Nrf2 signaling by natural products-can it alleviate diabetes? Biotechnol. Adv. 2018, 36, 1738–1767. [Google Scholar] [CrossRef]
- Morales RY. (2020). Manual de prevención y tratamiento para COVID-19 con plantas medicinales de los Altos de Chiapas. Colectividad Nichim Otanil. México. 72 pags. https://www.chiapasparalelo.com/trazos/cultura/2020/06 (accessed on 6 January 2021).
- Cuevas-Barragan, C.E.; Buenrostro-Nava, M.T.; Palos-Gómez, G.M.; Ramirez-Padilla, E.A.; Mendoza-Macias, B.I.; Rivas-Caceres, R.R. Use of Nasoil® via intranasal to control the harmful effects of Covid-19. Microb Pathog. 2020, 149, 104504. [Google Scholar] [CrossRef] [PubMed]
- Andreou A, Trantza S, Filippou D, Sipsas N, Tsiodras S. (2020). COVID-19: The potential role of copper and N-acetylcysteine (NAC) in a combination of candidate antiviral treatments against SARS-CoV-2. In vivo. 34: 1567-1588.
- . [CrossRef]
- Wang, B.; Aw, T.Y.; Stokes, K.Y. N-acetylcysteine attenuates systemic platelet activation and cerebral vessel thrombosis in diabetes. Redox Biol. 2018, 14, 218–228. [Google Scholar] [CrossRef]
- Lasram, M.M.; Dhouib, I.B.; Annabi, A.; El Fazaa, S.; Gharbi, N. A review on the possible molecular mechanism of action of N-acetylcysteine against insulin resistance and type-2 diabetes development. Clin. Biochem. 2015, 48, 1200–1208. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Yao, J.; Han, C.; Yang, J.; Chaudhry, M.T.; Wang, S.; Liu, H.; Yin, Y. Quercetin, inflammation and immunity. Nutrients. 2016, 8, 167. [Google Scholar] [CrossRef] [PubMed]
- Nair, M.P.; Kandaswami, C.; Mahajan, S.; Chadha, K.C.; Chawda, R.; NairandSchwartz, S.A.H. The flavonoid, quercetin, differentially regulates Th-1 (IFNgamma) and Th-2 (IL4) cytokine gene expression by normal peripheral blood mononuclear cells. Biochim Biophys Acta. 2002, 1593, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Colunga-Biancatelli, R.M.L.; Berrill, M.; Catravas, J.D.; Marik, P.E. Quercetine and vitamin C: An experimental, Synergistic therapy for the prevention and treatment of SARS-COVD-2 related disease (COVID-19). Front. Inmmunol. 2020, 11, 1451. [Google Scholar] [CrossRef]
- Chen, S.; Jiang, H.; Wu, X.; Fan, J. Therapeutic effects of quercetin on inflammation, obesity, and type 2 diabetes. Mediators Inflamm. 2016, 2016, 9340637. [Google Scholar] [CrossRef]
- Eid, M.H.; Haddad, P.S. The antidiabetic potential of quercetin: underlying mechanisms. Curr. Med. Chem. 2017, 24, 355–364. [Google Scholar] [PubMed]
- Bai, L.; Li, X.; He, L.; Zheng, Y.; Lu, H.; Li, J.; Zhong, L.; Tong, R.; Jiang, Z.; Shi, J.; Li, J. Antidiabetic potential of flavonoids from traditional chinese medicine: A review. Am. J. Chin. Med. 2019, 47, 933–957. [Google Scholar] [CrossRef] [PubMed]
- Lau, K.M.; Lee, K.M.; Koon, C.M.; Cheung, C.S.F.; Lau, C.P.; Ho, H.M.; Lee, M.Y.H.; Au, S.W.N.; Cheng, C.H.K.; Lau, C.B.S.; Tsui, S.K.W.; Wan, D.C.C.; Waye, M.M.Y.; Wong, K.B.; Wong, C.K.; Lam, C.W.K.; Leung, P.C.; Fung, K.P. Immunomodulatory and anti-SARS activities of Houttuynia cordata. J. Ethnopharmacol. 2008, 118, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.H.; Bose, S.; Shin, N.R.; Chin, Y.W.; Choi, Y.H.; Kim, H. Pharmaceutical impact of Houttuynia cordata and metformin combination on high-fat-diet-induced metabolic disorders: Link to intestinal microbiota and metabolic endotoxemia. Front. Endocrinol. 2018, 24, 620. [Google Scholar] [CrossRef]
- Kumar, M.; Prasad, S.K.; Krishnamurthy, S.; Hemalatha, S. Antihyperglycemic activity of Houttuynia cordata Thunb. in streptozotocin-induced diabetic rats. Adv. Pharmacol. Sci. 2014, 2014, 1–27. [Google Scholar] [CrossRef]
- Roviello, V.; Roviello, G.N. Lower COVID-19 mortality in Italian forested areas suggests immunoprotection by Mediterranean plants. Environ. Chem. Lett. 2020, 14, 1–12. [Google Scholar] [CrossRef]
- Boukhatem, M.N.; Setzer, W.N. Aromatic herbs, medicinal plant-derived essential oils, and phytochemical extracts as potential therapies for coronaviruses: Future perspectives. Plants. 2020, 9, 800. [Google Scholar] [CrossRef]
- Khan, I.; Shah, S.; Ahmad, J.; Abdullah, A.; Johnson, S.K. Effect of incorporating bay leaves in cookies on postprandial glycemia, appetite, palatability, and gastrointestinal well-being. J. Am. Coll. Nutr. 2017, 36, 514–519. [Google Scholar] [CrossRef]
- Khan, A.; Zaman, G.; Anderson, R.A. Bay leaves improve glucose and lipid profile of people with type 2 diabetes. J. Clin. Biochem. Nutr. 2009, 44, 52–56. [Google Scholar] [CrossRef]
- Khaerunnisa S, Kurniawan H, Awaluddin R, Suhartati S, Soetjipto S. (2020). Potential inhibitor of COVID-19 main protease (Mpro) from several medicinal plant compounds by molecular docking study. Preprints. 2020030226. [CrossRef]
- Tutunchi, H.; Naeini, F.; Ostadrahimi, A.; Hosseinzadeh-Attar, M.J. Naringenin, a flavanone with antiviral and anti-inflammatory effects: A promising treatment strategy against COVID-19. Phytother. Res. 2020, 34, 3137–3147. [Google Scholar] [CrossRef]
- Den Hartogh, D.J.; Tsiani, E. Antidiabetic properties of naringenin: A citrus fruit polyphenol. Biomolecules. 2019, 9, 99. [Google Scholar] [CrossRef]
- Kulkarni, Y.A.; Suryavanshi, S.V. Combination of naringenin and lisinopril ameliorates nephropathy in Type-1 diabetic rats. Endocr. Metab. Immune Disord. Drug Targets. 2020, 21, 1. [Google Scholar] [CrossRef]
- Alrasheid, A.H.; Babiker, M.Y.; Awad, T.A. Evaluation of certain medicinal plants compounds as new potential inhibitors of novel corona virus (COVID-19) using molecular docking analysis. In silico Pharmacol. 2021, 9, 1–7. [Google Scholar] [CrossRef]
- Jain, A.S.; Sushma, P.; Dharmashekar, C.; Beelagi, M.S.; Prasad, S.K.; Shivamallu, C.; Prasad, A.; Syed, A.; Marraiki, N.; Prasad, N.S. In silico evaluation of flavonoids as effective antiviral agents on the spike glycoprotein of SARS-CoV-2. Saudi J. Biol. Sci. 2021, 28, 1040–1051. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, M.; Thotakura, B.; Sekaran, S.P.C.; Jyothi, A.K.; Sundaramurthi, I. Naringin ameliorates streptozicin-induced diabetes through forkhead box M1-mediated beta cell proliferation. Cells Tissues Organ. 2018, 206, 242–253. [Google Scholar] [CrossRef]
- Alam, M.A.; Subhan, N.; Rahman, M.M.; Uddin, S.J.; Reza, H.M.; Sarker, S.D. Effect of citrus flavonoids, naringin and naringenin, on metabolic syndrome and their mechanisms of action. Adv. Nutr. 2014, 5, 404–417. [Google Scholar] [CrossRef]
- Mendoza-Pérez JA, Fregoso-Aguilar T. (2013). Chemistry of natural antioxidants and studies performed with different plants collected in México. In Morales-Gonzalez JA (ed.) Oxidative stress and Chronic degenerative diseases: A role for antioxidants. InTech, Croatia. Pages 59–85.
- Borkotoky S, Banerjee M. (2020). A computational prediction of SARS-CoV-2 structural protein inhibitors from Azadirachta indica (Neem). J. Biomol. Struct. Dyn. 1–17. [CrossRef]
- Khan, F.R.; Kazmi, S.M.R.; Iqbal, N.T.; Iqbal, J.; Ali, S.T.; Abbas, S.A. A quadruple blind, randomised controlled trial of gargling agents in reducing intraoral viral load among hospitalised COVID-19 patients: A structured summary of a study protocol for a randomised controlled trial. Trials. 2020, 21, 785. [Google Scholar] [CrossRef]
- Garg S, Anand A, Lamba Y, Roy A. (2020). Molecular docking analysis of selected phytochemicals against SARS-CoV-2 Mpro receptor. Vegetos. 1–16. [CrossRef]
- Ogidigo JO, Iwuchukwu EA, Ibeji CU, Okpalefe O, Soliman MES. (2020). Natural phyto, compounds as possible noncovalent inhibitors against SARS-CoV2 protease: computational approach. J. Biomol. Struct. Dyn. 1–18. [CrossRef]
- Baildya, N.; Khan, A.A.; Ghosh, N.N.; Dutta, T.; Chattopadhyay, A.P. Screening of potential drug from Azadirachta Indica (Neem) extracts for SARS-CoV-2: An insight from molecular docking and MD-simulation studies. J. Mol. Struct. 2021, 1227, 129390. [Google Scholar] [CrossRef] [PubMed]
- Parida, P.K.; Paul, D.; Chakravorty, D. The natural way forward: Molecular dynamics simulation analysis of phytochemicals from Indian medicinal plants as potential inhibitors of SARS-CoV-2 targets. Phytother. Res. 2020, 34, 3420–3433. [Google Scholar] [CrossRef]
- Adithya J, Nair B, Aishwarya S, Nath LR. (2020). The plausible role of Indian traditional medicine in combating Corona Virus (SARS-CoV 2): a mini-review. Curr. Pharm. Biotechnol. [CrossRef]
- Will, J.C.; Byers, T. Does diabetes mellitus increase the requirement for vitamin C? . Nutrition Revs. 1996, 54, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.; Willis, J.; Gearry, R.; Skidmore, P.; Fleming, E.; Frampton, C.; Carr, A. Inadequate vitamin C status in prediabetes and type 2 diabetes mellitus: associations with glycaemic control, obesity, and smoking. Nutrients. 2017, 9, 1–15. [Google Scholar] [CrossRef]
- Das, U.N. Vitamin C for Type 2 Diabetes Mellitus and Hypertension. Arch. Med. Revs. 2019, 50, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Rowe, S. The emerging role of vitamin C in the prevention and treatment of COVID-19. Nutrients. 2020, 12, 3286. [Google Scholar] [CrossRef]
- Liu, F.; Zhu, Y.; Zhang, J.; Li, Y.; Peng, Z. Intravenous high-dose vitamin C for the treatment of severe COVID-19: study protocol for a multicentre randomised controlled trial. BMJ Open. 2020, 10, e039519. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Progression of signs and symptoms of COVID-19, from mild to severe and that cause death in the patient.
Figure 1.
Progression of signs and symptoms of COVID-19, from mild to severe and that cause death in the patient.
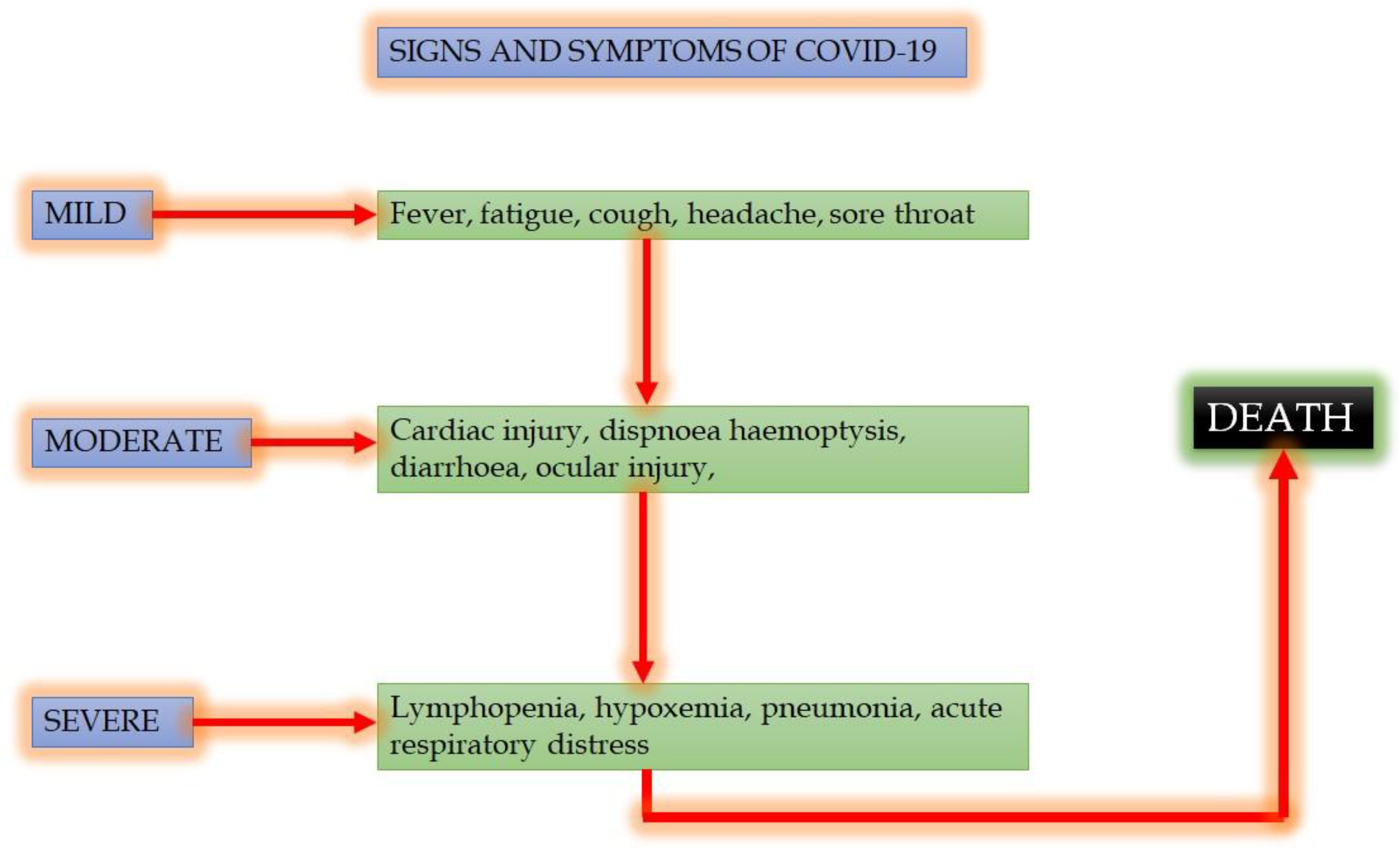
Figure 2.
Blood glucose in mice under different treatments for 6 weeks. *P <0.05 Diabetic mice plus L. nobilis vs. diabetic mice from week 1. Two-way repeated measures Analysis of VAriance (ANOVA) (own data).
Figure 2.
Blood glucose in mice under different treatments for 6 weeks. *P <0.05 Diabetic mice plus L. nobilis vs. diabetic mice from week 1. Two-way repeated measures Analysis of VAriance (ANOVA) (own data).
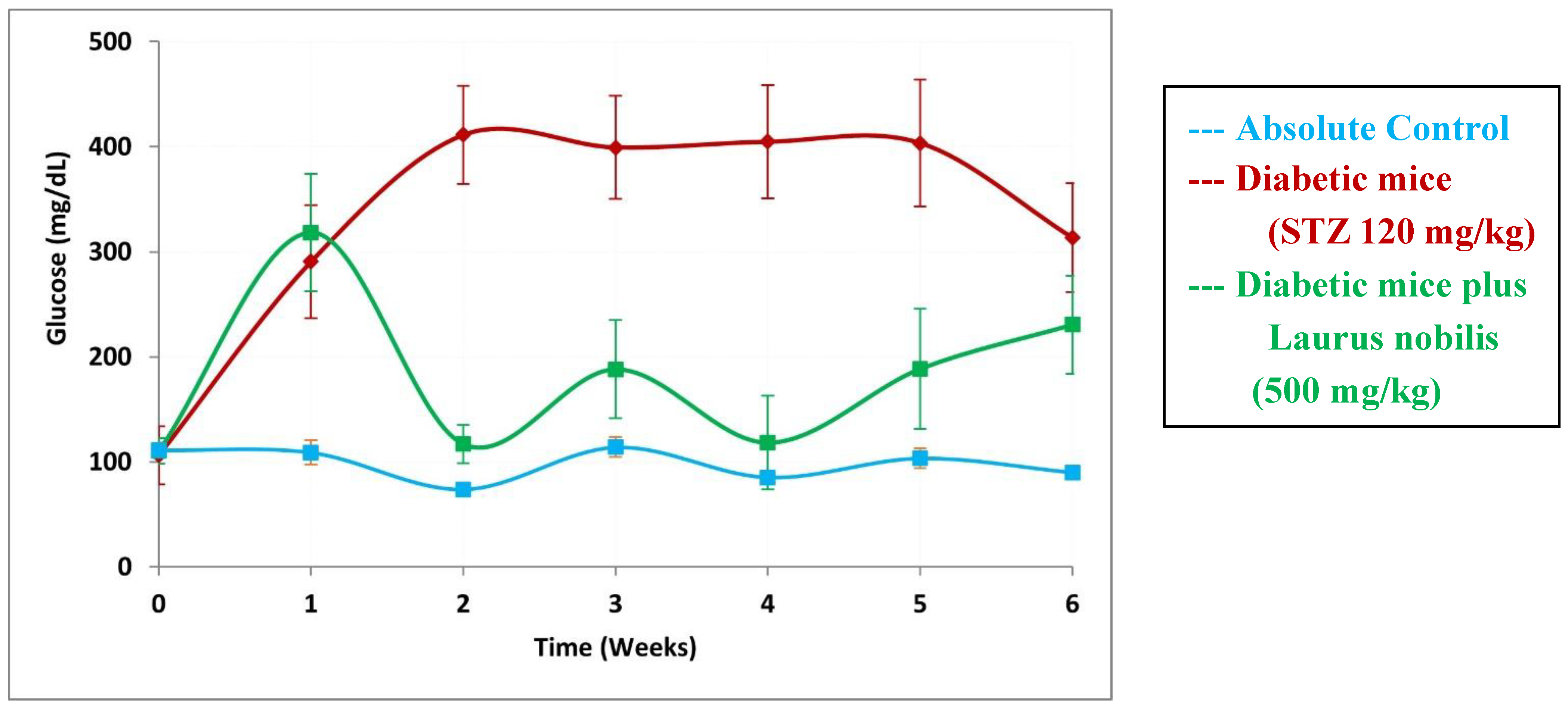

Table 1.
Studies on Azadirachta indica and COVID-19.
| Authors | Study type | Findings |
|---|---|---|
| Borkotoky and Banerjee, 2020 [153] | Docking and simulation methods to identify small molecule inhibitors of SARS-CoV-2 Membrane (M) and Envelope (E) proteins, which are essential for virus assembly and budding. | Of the 70 compounds monitored, we found that five compounds interacted with protein E and two interacted with protein M (nimocin and nimbolin) |
| Khan et al., 2020 [154] | PCR studies in humans to compare the effectiveness of an oral solution based on A. indica with other substances | Reduction of the intraviral oral burden confirmed with real time-PCR i |
| Adithya et al., 2020 [155] | Comparative study comparing information on Ayurvedic Medicine and its antiviral effects | Seven of the plants most used in Ayurvedic Medicine are mentioned ( including A. indica) have antiviral potential |
| Garg et al., 2020 [156] | Molecular docking of the 38 bioactive compounds of five plants effective against SARS-COV-2. | Some of the compounds, such as nimbin, inhibit inhibin the expression of the protein Mpro of COVID-19 |
| Ogidigo et al., 2020 [157] | Computer study of the compounds of two plants with antiviral properties compared with FDA drugs-of-reference | Six compounds including nimbolin had strong inhibitory reactions with the Mpro of COVID-19 |
| Baildya et al., 2021 [158] | Molecular docking and molecular dynamic study of the extracts of different parts A. indica against PLpro del COVID-19 | All compounds presented inhibition in the protein PLpro (above all DesaCetylGedunin (DCG), found in Neem seed) |
| Parida et al., 2020 [159] | molecular dynamic study on the effectiveness of 55 Ayurvedic on SARS-COV-2 | Withanolide R and 2,3-Dihydrowithaferin A were the compounds that interacted with the proteases and the spikes of the virus, but more evaluation is required |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



