
Submitted:
22 January 2025
Posted:
23 January 2025
You are already at the latest version
Abstract
Cholangiocarcinoma (CCA) is an aggressive malignancy with limited methods for early detection, necessitating the development of reliable biomarkers for diagnosis and management. However, conventional tumor markers, such as CA19-9 and CEA, exhibit insufficient diagnostic accuracy. Recent advancements in molecular genetics have identified several actionable mutations in CCA, enabling molecularly targeted therapies that improve survival in patients harboring these genetic alterations. Cancer panels, which facilitate multiplex genetic profiling, are critical for identifying these mutations. Studies indicate that several actionable mutations are detected in CCA cases, with patients receiving mutation-guided therapies achieving markedly better outcomes. Liquid biopsies, including cell-free DNA and circulating tumor DNA, offer real-time, non-invasive approaches to monitoring tumor dynamics, heterogeneity, and treatment responses. Furthermore, numerous studies have identified non-coding RNAs in serum and bile as promising biomarkers for the diagnosis and management of CCA. On the other hand, immunotherapy, particularly immune checkpoint inhibitors, has shown efficacy in subsets of CCA patients. However, the success of these therapies is often affected by the status of the tumor immune microenvironment (TME), underscoring the need for comprehensive TME analysis to predict responses to ICIs. Despite these advances, no single biomarker currently demonstrates sufficient sensitivity or specificity for clinical application. The integration of multi-omics approaches with cutting-edge technologies holds promise for enhancing diagnostic accuracy, optimizing treatment stratification, and advancing precision medicine in CCA. These developments highlight the transformative potential of biomarkers to improve early detection, prognostic assessment, and personalized therapeutic interventions for CCA.
Keywords:
cholangiocarcinoma
; mutations
; liquid biopsy
; non-coding RNAs
; tumor immune microenvironment
1. Introduction
The incidence of cholangiocarcinoma (CCA) has been increasing globally, and early detection and curative surgical resection are pivotal for improving the prognosis of patients with CCA. However, the progressive nature of CCA, characterized by a lack of early symptoms, often precludes timely diagnosis. Furthermore, there are currently no effective screening methods for high-risk populations, underscoring the pressing need for the identification of non-invasive biomarkers that can contribute to the detection of lesions and improved outcomes.
Currently, systemic therapy is the primary treatment for CCA patients with advanced stage and post-surgical recurrence. Traditional chemotherapy regimens, such as those involving gemcitabine, cisplatin, or tegafur-gimeracil-oteracil potassium (TS-1), have formed the backbone of systemic treatment for years. However, advances in molecular oncology have unveiled actionable driver mutations in CCA, paving the way for the development and clinical application of molecular targeted therapies tailored to specific genetic alterations. Moreover, significant strides have been made in the immunotherapy field, particularly with the advent of immune checkpoint inhibitors (ICIs). Combining ICIs with conventional cytotoxic agents such as gemcitabine and cisplatin (GC), has demonstrated promising efficacy and is increasingly being adopted in clinical practice for the treatment of CCA. Despite these advancements, the development of robust biomarkers to predict treatment response and guide therapeutic decision-making remains an area of unmet need.
This review aims to provide a comprehensive overview of the role of biomarkers in the management of CCA. We discuss the current state of biomarker development for CCA, encompassing their utility in diagnosis, prognosis, and therapeutic stratification. We also explore emerging trends and challenges in integrating biomarkers into clinical practice, highlighting their potential to shape the future of precision medicine for CCA treatment (Figure 1).
2. Serum and Plasma Biomarkers for Cholangiocarcinoma
CCA is often diagnosed based on elevated levels of hepatic and biliary enzymes and total bilirubin, as well as conventional tumor markers, such as carcinoembryonic antigen (CEA)and carbohydrate antigen 19-9 (CA19-9). The concomitant elevation of CA19-9 and CEA is associated with advanced-stage CCA [1]. However, these conventional tumor markers are not specific to CCA and are frequently negative in the early stages. Additionally, serum levels of these tumor markers are also elevated in benign conditions, such as in cases of obstructive jaundice, further limiting their specificity. Therefore, these tumor marker levels are utilized as an adjunct in the diagnosis of the disease [2]. Previous meta-analysis showed that the diagnostic sensitivity of CA19-9 was 0.72 and the specificity was 0.84; diagnostic accuracy of CA19-9 tends to be same in different control type [3], and elevated CA19-9 level more frequently observed in the patients with advanced tumor stage and poor survival. It should be noted that blood types of Lewis antigen-negative lead to the false negative for this tumor marker even if they carry malignant tumors [4]. Immunohistochemical staining is valuable in the differential diagnosis of CCA. For instance, it has been reported that immunostaining for cytokeratin (CK) 7, CK19, CK20, and caudal type homeobox 2 (CDX2) is useful in distinguishing CCA from metastatic liver cancer [5,6]. CDX2 is a nuclear transcription factor encoded in the epithelial cells of the gastrointestinal tract, from the duodenum to the rectum. It is known to be frequently positive in gastrointestinal cancers, particularly colorectal cancer, with a positivity rate of 84%. In contrast, the expression rate of CDX2 in CCA is significantly lower [7].
A serum-soluble CK 19 fragment (CYFRA 21-1) has also recently emerged as a promising biomarker for intrahepatic CCA (iCCA) compared to CA19-9. Elevated levels of CYFRA 21-1 in patients with iCCA, as opposed to those with benign biliary diseases, have demonstrated notable diagnostic potential [8,9]. Matrix metalloproteinase-7 (MMP-7), a zinc-dependent endopeptidase involved in extracellular matrix remodeling, has also emerged as a candidate biomarker. Elevated serum MMP-7 levels have shown diagnostic value in distinguishing iCCA from non-malignant biliary obstructions in patients with obstructive jaundice [10]. Several matricellular glycoproteins involved in cell adhesion, migration, and survival, are also reported as potential prognostic biomarker [11]. For instance, osteopontin levels are significantly higher in patients with CCA compared to those without malignancies [12]. Preoperative serum osteopontin levels correlate with overall survival (OS) rates following tumor resection [12]. Interleukin-6 (IL-6) has also been proposed as a diagnostic and prognostic marker for biliary tumors. Elevated serum IL-6 levels can distinguish patients with CCA from those with HCC, metastatic colorectal carcinoma, and benign biliary diseases. IL-6 exhibited sensitivity and specificity rates of 73% and 92%, respectively, in differentiating patients with CCA from healthy individuals [13]. Additionally, mucins, glycoproteins essential for epithelial protection, have shown potential as biomarkers. Elevated serum mucin 5AC levels are associated with reduced OS, warranting further validation for clinical integration [14]. Extracellular vesicle (EV)-derived proteins are another promising avenue in CCA biomarker research. Recent case-control studies have indicated that specific profile of serum EV-derived proteins could predict the risk of CCA development in patients with primary sclerosing cholangitis (PSC) [15]. EV-derived protein panels have also demonstrated potential in distinguishing CCA from hepatocellular carcinoma (HCC) and in providing prognostic insights [15].
Altered serum lipid and amino acid levels have been reported in patients with iCCA compared to those with benign biliary diseases [16]. Panels of cancer-associated metabolic alterations have demonstrated superior diagnostic performance over CA19-9 and α-fetoprotein in distinguishing iCCA from HCC, even at early stages [16]. These profiles are also valuable for differentiating distal CCA (dCCA) from pancreatic ductal adenocarcinoma as well as for identifying malignant stenoses [17,18]. A panel of 10 plasma metabolites has also shown prognostic value in predicting post-resection outcomes, aiding in tailoring treatment strategies [19]. However, no single serum or plasma biomarker has exhibited absolute specificity for the diagnosis of CCA, underscoring the necessity of integrating these findings with clinical data and other biomarkers.
3. Genetic Aberrations in Cholangiocarcinoma
CCA is known to exhibit distinct genetic aberration profiles depending on its anatomical location. In addition, differences in etiology across regions contribute to variations in these genetic abnormalities. PSC is a well-recognized risk factor for intrahepatic CCA (iCCA) especially in western countries, whereas liver fluke infection, hepatitis B virus (HBV), and hepatolithiasis are predominant risk factors in Southeast Asia. Multiple studies have reported on the genetic analysis of CCA [20,21,22,23,24], with frequent mutations identified in genes such as TP53, KRAS, SMAD4, CDKN2A/2B, and ARID1A.
In genetic analyses of CCA, actionable genetic alterations were detected in approximately 40% of cases [20]. Mutations in FGFR, IDH1/2, BAP1, and ARID1A were predominantly found in iCCA, while PKA and HER2 mutations were more common in distal CCA (dCCA). Alterations in EGFR, HER2, and ERBB3 were frequently observed in gallbladder cancer. Wardell et al. analyzed the genetic profiles of 412 CCA cases [23] and identified germline mutations in DNA repair genes, including BRCA1/2, MLH1, and MSH2. Jusakul et al. analyzed 489 CCA cases from different regions [22] and found that liver fluke-associated CCAs frequently exhibited ERBB2 amplification and TP53 mutations, whereas non-fluke-associated cases demonstrated a higher prevalence of copy number alterations, elevated PD-1/PD-L2 expression, IDH1/2 and BAP1 mutations, and FGFR rearrangements with epigenetic dysregulation.
Reports utilizing the FoundationOne™ platform, a comprehensive genomic profiling tool, have also provided valuable insights. FGFR alterations and IDH1/2 mutations were predominantly detected in iCCA, with FGFR2 alterations notably associated with younger age, female gender, and better prognosis [21]. A multivariate analysis examining the prognosis of patients with iCCA revealed that TP53 mutations were associated with poor prognosis, whereas FGFR alterations were associated with favorable outcomes. Umemoto et al. analyzed 3,031 cases of CCA using the FoundationOne™ platform [24] and reported a high frequency of ERBB2 amplification in tumor mutation burden (TMB)-high tumors. Furthermore, CDK12 rearrangements were predominantly identified in ERBB2-amplified CCAs. Among CCA cases diagnosed in individuals under 40 years of age, GATA6 amplification, as well as BRAF and FGFR2 rearrangements, were observed. Importantly, molecular-targeted therapies based on genetic abnormalities improved the prognosis of patients with iCCA, and molecular findings underscore the potential for actionable mutations to serve as therapeutic targets.
4. Molecular-Targeted Therapies and Biomarkers
CCA is characterized by multiple driver gene mutations, with mutation frequencies varying according to the tumor’s anatomical location. Genetic testing in oncology includes companion diagnostics and gene panel testing which identifies multiple driver mutations and facilitates appropriate therapeutic strategies. Gene panel testing has shown promise in the clinical management of CCA [25]. Reports indicate that 68% of CCA cases can be treated based on genetic abnormalities, with selection of targeted treatments in 53% of cases. Notably, patients receiving treatments guided by genetic abnormalities demonstrated a significantly improved OS compared to those treated without genetic guidance. Furthermore, utilizing treatments categorized as Clinical Actionability of Molecular Targets (ESCAT) I-II in the European Society for Medical Oncology (ESMO) Scale improved the prognosis of patients with iCCA [26]. Based on these findings, next-generation sequencing (NGS)-based gene panel testing using tumor tissue is recommended for CCA management [27]. So far, several studies have reported favorable outcomes in patients treated with guided agents by genetic alterations as detailed below.
4.1. FGFR2 Gene Fusions/Rearrangements
The fibroblast growth factor receptor (FGFR) family comprises four receptors, FGFR1–4. Ligand binding to FGFR activates downstream signaling pathways, including the JAK-STAT, RAS/MAPK, and PI3K/Akt/mTOR pathways. FGFR2 gene fusions and rearrangements induce constitutive activation of these signaling pathways. Rearrangements of FGFR2 occur in approximately 3.6–7.4% of CCA cases and are predominantly observed in iCCA [28]. FGFR2 gene fusions and rearrangements serve as a biomarker for FGFR2 inhibitors and have been incorporated into companion diagnostics, underscoring their clinical importance in guiding targeted therapy [29,30]. Pemigatinib, an oral FGFR1–3 inhibitor, demonstrated efficacy in a phase II clinical trial targeting cases with FGFR2 fusion/rearrangement, showing an objective response rate (ORR) of 35.5%, a median progression-free survival (PFS) of 6.9 months, and a median OS of 21.1 months [31]. Similarly, another FGFR1-3 inhibitor, infigratinib, showed efficacy in patients with FGFR2 gene fusions/rearrangements, achieving an ORR of 23.1%, a median PFS of 7.3 months, and a median OS of 12.2 months [32]. Additional data regarding a phase II trial of futibatinib have also been reported [33,34]. While pemigatinib and infigratinib are reversible ATP-competitive inhibitors targeting FGFR1–3, futibatinib, an irreversible inhibitor targeting FGFR1–4, demonstrated promising results in pretreated iCCA cases with FGFR2 gene fusions/rearrangements, achieving an ORR of 42%, a median PFS of 9.0 months, and a median OS of 21.7 months [33]. Importantly, irreversible inhibitors have shown efficacy in cases with acquired resistance to reversible FGFR inhibitors.
4.2. Mutations in the IDH Gene
Isocitrate dehydrogenase (IDH) is an enzyme that catalyzes the conversion of isocitrate to α-ketoglutarate. Mutant IDH enzymes further convert α-ketoglutarate to 2-hydroxyglutarate (2-HG), which promotes tumorigenesis by inducing epigenetic changes and impairing DNA repair. IDH1 mutations are detected in approximately 20% of iCCA cases. Our research has revealed an association between IDH1 mutations and methylation of antigen-presentation-related genes, leading to their decreased expression and the development of an immune-cold tumor immune microenvironment (TME) in CCA [35,36]. Therefore, increased serum levels of 2-HC can be a surrogate marker for IDH1/2 mutation [37].
Ivosidenib is a small-molecule inhibitor targeting mutant IDH1, and its efficacy has been demonstrated in the phase III clinical trial [38]. The PFS was significantly prolonged in the ivosidenib group (median PFS of 2.7 months) compared to the placebo group (1.4 months). Median OS was 10.3 months in the ivosidenib group vs. 7.5 months in the placebo group. Notably, after adjusting for crossover, a significant difference in OS was observed between the two groups. Based on these findings, ivosidenib has been approved by the U.S. Food and Drug Administration (FDA) and is recommended as a second-line treatment for IDH1-mutant CCA.
4.3. Activating Mutations in the KRAS and BRAF Genes
Activation of the RAS/MAPK pathway is a common feature across various cancer types. In CCA, KRAS mutations are found in 9–40% of cases, with a higher prevalence in iCCA. Mutations in BRAF, particularly the V600E variant, have been identified as actionable targets. A phase II clinical trial investigating the combination of the BRAF inhibitor dabrafenib and the MEK inhibitor trametinib has shown promising results in pretreated patients carrying BRAF V600E-mutantion [39]. Although this trial included multiple rare cancers with BRAF V600E, the ORR ranged from 46% to 53% for biliary tract cancers. This combination therapy is also recommended for BRAF V600E-mutant CCA.
4.4. HER2 Gene Amplification/Overexpression
Amplification or overexpression of HER2, a receptor tyrosine kinase involved in cell proliferation, is observed in 3–19% of CCA cases, with a higher prevalence in gallbladder cancer. HER2-targeted therapies are recommended for HER2-positive CCA in the NCCN guidelines. In a phase II trial evaluating the combination of pertuzumab and trastuzumab in HER2-positive, previously treated CCA cases, this combination therapy achieved an ORR of 23.1%, a median PFS of 4.0 months, and a median OS of 10.9 months [40]. Additionally, the irreversible HER1, HER2, and HER4 inhibitor and anti-HER2 antibody has demonstrated efficacy in phase II clinical trials [41,42]. Other therapies, such as antibody-drug conjugates combining trastuzumab and the topoisomerase inhibitor deruxtecan, have also shown favorable outcomes in HER2-activated tumors [43].
4.5. Other Biomarkers for Molecular Targeted Agents
The efficacy of pembrolizumab, an anti-PD-1 antibody, has been validated in the phase II KEYNOTE-158 trial for solid tumors exhibiting microsatellite instability-high (MSI-high) or mismatch repair deficiency (dMMR) [44,45]. However, the frequency of CCA with MSI-high or TMB-high is approximately only 2%. On the other hand, it is reported that 27.5% of biliary tract cancers carry genetic alterations within the genes involved in homologous recombination, suggesting that platinum agents or poly (ADP-ribose) polymerase inhibitors may be promising agents [46]. Neurotrophic receptor kinase (NTRK) fusion-positive solid tumors can be treated effectively with entrectinib and larotrectinib, although the prevalence of NTRK gene fusions in CCA cases is low [47,48].
5. Emerging Biomarkers and Their Future Perspectives
5.1. Tumor Cells and Cell-Free DNA in Peripheral Blood
The detection of tumor cells in the blood (circulating tumor cells: CTCs) has been reported, yet their clinical application remains an ongoing challenge due to the difficulty in isolating a single CTC among blood cells. Detection of tumor cells generally relies on epithelial markers including CKs and epithelial cell adhesion molecules, while excluding leukocyte markers such as CD45. However, the heterogeneity of CTCs and variability in their biomarker expression, particularly during epithelial-to-mesenchymal transition, complicate the detection of cancer cells in blood. This variability underscores the need for multipronged approaches to detect and characterize CTCs effectively. Characterization of CTCs is key strategies for utilizing liquid biopsies in diagnosis, monitoring of treatment efficacy, and disease surveillance [49].
In CCA, higher CTC counts have consistently been associated with poor prognosis. Previous study reported that CTC was detected in 17% of patients with CCA in 7.5 mL of their blood, which correlated with tumor extension and poor prognosis [12,14,50,51,52,53,54,55,56]. Baseline CTC detection was linked to reduced OS in nonresectable cases. Notably, similar detection rates of CTCs were observed across two clinical trials despite differences in sample volume and methodology [57,58]. CTCs are not merely considered prognostic markers but also substrates for metastasis, contributing to disease progression. In metastatic CCA, even the detection of as few as 1–3 CTCs correlated with poorer OS [59]. Although, most CTCs do not survive in circulation [49], recent techniques have enhanced the sensitivity of detection [60]. Combining multiple affinity reagents, such as heparan sulfate-based probe SCH45, nucleic acid aptamers, and anti-EpCAM in microfluidic systems, has enabled the detection of CTC in nearly 100% of bile samples in CCA cases [61]. Furthermore, combining central and peripheral venous sampling has also improved detection rates from 40% to 54% [59]. These innovations highlight the growing importance of CTCs in precision oncology.
On the other hand, circulating nucleic acids, including cell-free DNA (cfDNA) and circulating tumor DNA (ctDNA), have gained significant attention for their potential in cancer management. In CCA, cfDNA and ctDNA analyses have shown promise for both diagnostic and prognostic applications. The evaluation of ctDNA offers several advantages over traditional tissue biopsies, including reduced invasiveness and ability to capture tumor heterogeneity [62,63]. ctDNA carries tumor-specific genetic alterations, making it an invaluable tool for liquid biopsy. In advanced CCA cases, ctDNA was detectable in approximately 90% of patients, with variant allele fractions correlating strongly with tumor burden and stage of the disease [64,65]. Although detection of ctDNA is challenging in early stage, advancements in detection of ctDNA will improve its sensitivity [66]. cfDNA testing also provides insight into mutational burden, dynamic tumor evolution, and acquired resistance mechanisms, aiding in patient stratification and therapy selection [53,67,68,69,70,71]. The prognostic significance of ctDNA also lies in its ability to reflect tumor dynamics and therapeutic responses. While ctDNA analyses have shown high sensitivity and specificity in detecting advanced CCA, most studies have focused on patients with established malignancies. Thus, early detection remains a critical challenge, particularly in identifying high-risk populations [72]. The detection of ctDNA carrying altered methylation is also reported as a complementary strategy, enhancing diagnostic accuracy and guiding clinical management [73,74,75]. Achieving concordance between mutations identified in ctDNA and tumor tissues is essential for validating cfDNA testing. Notably, better concordance has been observed in iCCA compared to dCCA, possibly due to differences in tumor location and patterns of cfDNA release [69]. Detecting gene fusions, such as FGFR2 fusions in iCCA, can also be useful for the diagnosis of CCA because these alterations could be a driver for the development of CCA. However, current liquid biopsy panels face challenges for the detection of fusion genes and rearrangement, and innovative platforms beyond next-generation sequencing may help address these limitations [70,76].
Liquid biopsies using cfDNA and ctDNA hold significant promise for capturing the intrapatient molecular heterogeneity, allowing for real-time monitoring of tumor progression, assessment of therapeutic responses, and detection of minimal residual disease after surgery [72]. As technologies continue to evolve, the integration of liquid biopsy data with imaging and pathology could lead to a more comprehensive and dynamic understanding of cancer status. These advancements underscore the potential for liquid biopsies to revolutionize the clinical management of CCA, paving the way for earlier diagnosis, improved prognostication, and personalized treatment strategies. Combining these methods with cutting-edge technologies, such as single-cell sequencing, microfluidic systems, and methylation profiling, could significantly enhance their clinical utility.
5.2. Non-Coding RNAs
Non-coding RNAs (ncRNAs) are a diverse group of RNA molecules that do not code for proteins but play critical roles in various biological processes. These include microRNAs (miRNAs), long non-coding RNAs (lncRNAs), and circular RNAs (circRNAs). Recent studies have demonstrated that miRNAs, lncRNAs, and circRNAs are involved in regulating cell proliferation, invasion, metastasis, and the development of drug resistance in CCA, highlighting their potential as diagnostic and prognostic biomarkers (Figure 2) [77,78].
5.2.1. MicroRNAs
Various studies have shown that miRNAs are associated with the response to systemic chemotherapy in CCA. For instance, overexpression of miR-21 in CCA has been reported to downregulate the tumor suppressor gene phosphatase and tensin homolog (PTEN) and to be associated with the acquisition of gemcitabine resistance [79]. Elevated levels of serum miR-200c-3p have been linked to increased recurrence rates and decreased OS following surgical resection in CCA patients [80]. Similarly, plasma miR-183-5p, which is known to promote immunosuppressive macrophages and upregulate programmed death-ligand 1 (PD-L1) expression, has been associated with higher recurrence rates and worse OS in patients with iCCA [54]. By leveraging the stability of non-coding RNA in body fluids and their role in critical biological processes, these markers offer a minimally invasive approach for improving the management of CCA. For example, bile-derived miR-200c-3p was found to be more abundant in CCA patients compared to individuals with biliary obstruction caused by gallstones [52].
Regarding the role of miRNA as biomarkers for the response to systemic therapy, the miR-130a-3p may promote resistance to gemcitabine by inhibiting the expression of peroxisome proliferator-activated receptor gamma (PPARG), which is involved in nucleotide metabolism [81]. Additionally, miR-200b, miR-210, let-7a, and miR-181c, among others, have been shown to contribute to gemcitabine resistance by inhibiting apoptosis. Furthermore, miR-1249 and miR-200b/c might contribute to gemcitabine and 5-FU resistance through the induction of CD+133 cells, which are thought to be associated with cancer stem cells [82,83]. MiR-125a-5p is upregulated in CCA compared to normal tissues and is associated with decreased sensitivity to gemcitabine. Several other tumor-derived miRNAs have been identified as playing important roles in gemcitabine resistance in CCA [84,85,86,87].
5-FU is another drug commonly used in the treatment of CCA, and several studies have clarified the role of miRNAs in mediating 5-FU resistance. Overexpression of miR-20a-5p has been found to suppress 5-FU resistance induced by the onco-lncRNA FALEC and to promote apoptosis [88]. On the other hand, miR-328 has been reported to inhibit tumor growth and to enhance apoptosis induced by 5-FU [89]. MiR-200b/c inhibits tumor migration and enhances the sensitivity of CCA cells to 5-FU [82]. MiR-885-5p may increase the sensitivity of CCA cells to 5-FU by targeting myotrophin (MTPN), a protein associated with cell migration and invasion [90].
Platinum-based chemotherapy, particularly cisplatin in combination with GC, is currently the standard treatment for advanced CCA. However, the development of cisplatin resistance remains a significant challenge in CCA therapy. MiR-199a-3p is a miRNA associated with cisplatin resistance in various types of tumors, including CCA. Upregulation of miR-199a-3p has been shown to enhance CCA cell sensitivity to cisplatin by inhibiting the expression of multidrug resistance protein 1 [91]. MiR-637 is involved in drug resistance in various cancers, and its downregulation in CCA is associated with resistance to cisplatin. Furthermore, miR-520c-3p has been reported to induce the suppression of cancer stemness and epithelial-mesenchymal transition (EMT), thereby enhancing CCA cell sensitivity to cisplatin [92].
5.2.2. LncRNAs
Long non-coding RNAs (lncRNAs) are non-coding RNA molecules longer than 200 nucleotides and have been implicated in both carcinogenesis and tumor suppression [93]. Numerous lncRNAs localized in exosomes have been secreted into plasma, urine, and bile as highly tissue-specific circulating RNAs, which may serve as non-invasive biomarkers [94]. Several lncRNAs have been identified in serum and urine EVs from patients with CCA, PSC, and healthy controls. In serum-derived EVs, metastasis-associated in lung adenocarcinoma transcript-1 (MALAT1) and LOC100190986 showed high accuracy in distinguishing between CCA and PSC. In addition, LOC100134868 derived from urinary EVs demonstrated a high diagnostic value between CCA and healthy controls [94]. Most lncRNAs are significantly expressed in the tissues, cells, and bile of CCA and have diagnostic and prognostic potential as CCA biomarkers. Bile-associated some lncRNAs exhibited higher levels in CCA patients compared to control subjects with bile duct obstruction. Ge et al. discovered two lncRNAs, ENST00000588480.1 and ENST00000517758.1, to be highly expressed in exosomes derived from bile of CCA patients [95]. When combined for diagnosis, the area under the curve (AUC), sensitivity, and specificity were 0.709, 82.9%, and 58.9%, respectively, with sensitivity surpassing that of serum CA19-9. It was also reported that higher expression of these two lncRNAs in CCA patients was associated with poor survival, suggesting their potential as predictive markers for monitoring CCA [95]. On the other hand, lncRNA-NEF was downregulated in iCCA tissues, and its overexpression suppressed tumor cell migration and invasion by inhibiting runt-related transcription factor 1 (RUNX1), demonstrating good diagnostic characteristics to distinguish iCCA from healthy controls. Furthermore, low expression of lncRNA-NEF in iCCA patients was associated with significantly shorter OS, suggesting its potential as a biomarker [78]. Another study found that deleted in lymphocytic leukemia 1 (DLEU1) has been shown to correlate with advanced tumor lymph node metastasis (TNM stage) and can be used as a prognostic marker for CCA [96]. MALAT1 has been linked to poor prognosis in pCCA patients, with overexpression associated with decreased OS, worsened TNM stage, increased tumor size, and metastasis. Shi et al. reported that MALAT1 in plasma could serve as a useful diagnostic biomarker for pCCA [97]. Another study found that prostate cancer-associated transcript 1 (PCAT1) contributes to cancer progression via the Wnt/β-catenin signaling pathway and is elevated in extrahepatic CCA [98]. Overexpression of PCAT1 was associated with adverse outcomes in CCA patients, making it a useful prognostic marker.
H19 is upregulated in CCA tissues and is associated with tumor size, TNM stage, postoperative recurrence, and OS. It has been observed to have moderate sensitivity in distinguishing CCA tissues from normal tissues, with an AUC of 0.7422. Furthermore, when combined with other lncRNAs, the diagnostic sensitivity and specificity for differentiating CCA tissues from normal tissues increased [99,100]. Jiang et al. reported that the expression level of colon cancer-associated transcript (CCAT)1 in CCA tumor tissues was significantly higher compared to adjacent normal tissues. Increased expression of CCAT1 was associated with lower histological differentiation, lymph node invasion, and advanced TNM stage. Patients with overexpression of CCAT1 had significantly poorer OS, making CCAT1 an independent prognostic factor for CCA [101]. CCAT2 expression is elevated in CCA and inversely correlates with OS in CCA patients. Thus, CCAT2 holds practical value as a prognostic marker for these patients, with AUCs for OS and PFS of 0.702 and 0.715, respectively [102]. Zinc finger E-box binding homeobox 1 (ZEB1)-AS1 is also overexpressed in CCA and has been shown to promote tumor growth and metastasis in both in vivo and in vitro experiments. High expression of ZEB1-AS1 was associated with lymph node invasion, advanced TNM stage, and shortened survival [103].
5.2.3. CircRNAs
Circular RNAs (circRNAs) are covalently closed single-stranded RNAs; they are typically produced from the intermediate exons of protein-coding genes [104]. Due to their tissue specificity and stability—circRNAs are less susceptible to degradation by ribonuclease R; they are considered promising candidates as cancer biomarkers [105,106]. The expression of circRNA Cdr1 as is significantly upregulated in tumor tissues compared to adjacent normal tissues, and it is strongly associated with lymph node invasion, progression of the TNM stage, and postoperative recurrence. Furthermore, Cdr1 as was identified as a novel independent prognostic biomarker for predicting overall survival (OS) in CCA patients, with a sensitivity of 83.3% and specificity of 58.3% [107]. Xu et al. found that levels of circ-CCAC1 were elevated in EVs derived from the bile and serum of CCA patients [108]. The diagnostic capability of circ-CCAC1 in serum was comparable to that of serum CA19-9, while in bile samples, it outperformed CA19-9. Interestingly, combining EV-derived circ-CCAC1 from bile or serum with CA19-9 enhanced diagnostic performance compared to either marker alone. The study also confirmed that high expression of circ-CCAC1 was an independent prognostic marker for iCCA and that circ-CCAC1 expression could predict postoperative recurrence in iCCA patients.
Additionally, hsa_circ_0000284 (cir-HIPK3) was reported to be upregulated in plasma exosomes from CCA patients [109]. Another study identified that hsa_circ_0020256 (cir-NSMCE4A) was highly expressed in exosomes secreted by tumor-associated macrophages and promoted proliferation, migration, and invasion of CCA cells [110]. This study also demonstrated a negative correlation between the expression of cir-NSMCE4A and both time to recurrence and OS in CCA patients. Moreover, high levels of hsa_circ_0030998 (cir-LAMP1) were associated with an increased rate of postoperative recurrence [111]. Hsa_circ_0003930 (cir-GGNBP2) was associated with worse prognosis in patients after surgical resection. An increase in cir-GGNBP2 was reported as an independent risk factor for OS and RFS, suggesting its potential as a prognostic marker for iCCA [112]. Zhang et al. reported decreased expression of hsa_circ_0059961 (cir-ITCH) in CCA tissues [113]. Their study found a positive correlation between the expression of cir-ITCH and survival, with patients exhibiting high levels of cir-ITCH having better OS compared to those with low expression. Additionally, patients with high expression of hsa_circ_0008621 (cir-HMGCS1) in iCCA tissues had significantly shorter survival after radical resection and higher cumulative recurrence rates, indicating that cir-HMGCS1 may serve as an independent prognostic indicator for cumulative recurrence in iCCA patients [114].
6. Tumor Immune Microenvironment and Treatment Using Immune Checkpoint Inhibitors
CCA has demonstrated responsiveness to molecular targeted agents (MTAs) as well as ICIs. MTAs focus on inhibiting driver mutations implicated in tumor progression, showing promise in advanced CCA cases resistant to first-line chemotherapy. Conversely, ICIs have also emerged as a transformative approach in CCA treatment. The TOPAZ-1 trial demonstrated that combining durvalumab (a PD-L1 inhibitor) with GC significantly improved OS, PFS, and response rates in unresectable or metastatic biliary tract cancer compared to chemotherapy alone [115]. Similarly, the KEYNOTE-966 trial validated the efficacy of combining ICIs with GC as first-line therapy in advanced CCA cases [116]. TME plays a crucial role in determining the efficacy of ICIs, emphasizing the need to consider TME characteristics as potential biomarkers for CCA treatment.
Transcriptomic studies have classified the immune landscape of CCA into several subtypes, reflecting their impact on immune evasion and patient outcomes. Job et al. identified four immune subclasses—immune-desert, immunogenomic, myeloid, and mesenchymal—based on transcriptomic data from 198 iCCA samples [117]. The immune-desert subclass, lacking immune cells-related gene signatures, represented 46–48% of cases. Another classification by Martin-Serrano et al. divided CCAs into inflamed (35%) and non-inflamed (65%) classes [118]. Non-inflamed tumors included “hepatic stem-like,” enriched with stemness pathways and IDH1/2 and BAP1 mutations; “tumor classical,” linked to cell cycle activation and poor prognosis; and “desert-like,” driven by Wnt/β-catenin signaling and a paucity of immune cells. Inflamed tumors were subdivided into “immune classical,” characterized by metabolic pathway activation, and “inflammatory stroma,” associated with oncogenic pathways like TGF-β and KRAS. Zhu et al. further detailed spatial immunophenotypes of CCA, identifying inflamed, excluded, and ignored classes [119]. Inflamed tumors featured immune cell infiltration and activation of IFN-γ and IL-6/JAK/STAT pathways, making them potential targets for ICIs. In contrast, excluded and ignored phenotypes, defined by TGF-β, Wnt/β-catenin signaling, and angiogenesis, exhibited immune exclusion or evasion, possibly reducing ICI efficacy.
Mutations in IDH1/2, FGFR2, KRAS, and BAP1 genes are considered to play important roles in shaping the TME in CCA. IDH1/2 mutations, predominantly seen in non-inflamed iCCAs, drive the production of 2-HG, induce hypermethylation of genes involved in antigen presentation, and suppress the infiltration of CD4+ and CD8+ T cells [35,120]. Similarly, FGFR2 gene fusions/rearrangements are also linked to low immune cell infiltration [121,122]. Activation of the Wnt/β-catenin pathway further exacerbates immune evasion by downregulating chemokines and tumor-infiltrating lymphocytes (TILs) [122,123]. KRAS mutations, through toll-like receptor 4 (TLR4) activation, promote immunosuppressive macrophages and myeloid-derived suppressor cells (MDSCs), which inhibit CD8+ T cells. Preclinical studies suggest that KRAS inhibition may reverse these effects, enhancing anti-tumor immunity in pancreatic cancer model [124]. Pembrolizumab showed durable responses in dMMR/MSI-H non-colorectal cancers, with an ORR of 40.8% and a complete response rate of 13.5% [125]. However, these mutations are rare in CCA.
Most CCAs exhibit a non-inflamed TME and would be resistant to ICIs, thus understanding mechanisms underlying immune evasion and resistance in CCA is crucial. The non-inflamed TME often results from genetic alterations, such as IDH1/2 mutations and FGFR2 gene fusions, which suppress antigen presentation and foster an immunosuppressive microenvironment [36]. Therefore, these genetic alterations might be a biomarker for representing non-inflamed TME status, where ICI-based treatment may not be effective. Thus, combining targeted therapies, such as IDH1/2 or FGFR inhibitors, with ICIs may restore anti-tumor immunity. Preclinical models suggest that these combinations can reinvigorate immune responses by reducing immunosuppressive signaling and enhancing antigen presentation [126,127].
Efforts to identify predictive biomarkers are critical for optimizing ICI use. Advances in multi-omics analyses and liquid biopsies may enable precise classification of TME subtypes and real-time monitoring of treatment responses. Additionally, integrating experimental models, such as organoids and single-cell technologies, with genomic and proteomic studies could unveil novel biomarkers and therapeutic targets.
7. Conclusions
CCA poses significant challenges in diagnosis and monitoring, differing from HCC, where many cases develop in cirrhotic livers under routine surveillance programs [128,129]. Over half of CCA cases occur in patients without underlying hepatobiliary diseases, which do not warrant inclusion in monitoring programs. The absence of high-risk group definitions and effective biomarkers for early detection complicates CCA surveillance efforts. Current research highlights the potential of liquid biopsy techniques, including bile-derived cfDNA and ctDNA, which detect molecular alterations in body fluid, for early and accurate diagnosis [18,130]. Bile cfDNA, analyzed for mutations and methylation, is also a promising biomarker for the detection of CCA [130,131,132]. Additionally, combining liquid biopsy matrices with advanced technologies, such as single-cell analysis, could revolutionize CCA management [133]. Investments in research integrating experimental models and large patient cohorts are essential to developing novel biomarkers, offering hope for noninvasive and effective diagnostic strategies.
Author Contributions
Original draft preparation, review, and editing by N.N.
Funding
This research was supported in part by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (KAKENHI: 24K10393, N. Nishida).
Data Availability Statement
Data in this review paper are openly available from references.
Acknowledgments
We would like to thank Editage (www.editage.com) for the English language editing.
Conflicts of Interest
There are no conflicts of interest to disclose.
Abbreviations
The following abbreviations are used in this manuscript:
| CA19-9 | Carbohydrate antigen 19-9 |
| CCA | Cholangiocarcinoma |
| CEA | Carcinoembryonic antigen |
| cfDNA | Cell-free DNA |
| ctDNA | Circulating tumor DNA |
| dCCA | Distal CCA |
| CA19-9 | Carbohydrate antigen 19-9 |
| CTCs | Circulating tumor cells |
| DDR | DNA damage response |
| dMMR | Mismatch repair deficiency |
| EpCAM | Epithelial cell adhesion molecules |
| HBV | Hepatitis B virus |
| HCCs | Hepatocellular carcinomas |
| iCCA | Intrahepatic CCA |
| ICIs | Immune checkpoint inhibitors |
| IL-6 | Interleukin-6 |
| MMP-7 | Matrix metalloproteinase-7 |
| MTAs | Molecular targeted agents |
| NGS | Next-generation sequencing |
| ORR | Objective response rate |
| OS | Overall survival |
| PARP | Poly ADP-ribose polymerase |
| PFS | Progression-free survival |
| TILs | Tumor-infiltrating lymphocytes |
| TME | Tumor immune microenvironment |
References
- Izquierdo-Sanchez, L.; Lamarca, A.; La Casta, A.; Buettner, S.; Utpatel, K.; Klumpen, H.J.; Adeva, J.; Vogel, A.; Lleo, A.; Fabris, L.; et al. Cholangiocarcinoma landscape in Europe: Diagnostic, prognostic and therapeutic insights from the ENSCCA Registry. J Hepatol. 2022, 76, 1109–1121. [Google Scholar] [CrossRef]
- Bowlus, C.L.; Arrive, L.; Bergquist, A.; Deneau, M.; Forman, L.; Ilyas, S.I.; Lunsford, K.E.; Martinez, M.; Sapisochin, G.; Shroff, R.; et al. AASLD practice guidance on primary sclerosing cholangitis and cholangiocarcinoma. Hepatology. 2023, 77, 659–702. [Google Scholar] [CrossRef]
- Liang, B.; Zhong, L.; He, Q.; Wang, S.; Pan, Z.; Wang, T.; Zhao, Y. Diagnostic Accuracy of Serum CA19-9 in Patients with Cholangiocarcinoma: A Systematic Review and Meta-Analysis. Med Sci Monit. 2015, 21, 3555–3563. [Google Scholar] [CrossRef] [PubMed]
- Macias, R.I.R.; Cardinale, V.; Kendall, T.J.; Avila, M.A.; Guido, M.; Coulouarn, C.; Braconi, C.; Frampton, A.E.; Bridgewater, J.; Overi, D.; et al. Clinical relevance of biomarkers in cholangiocarcinoma: critical revision and future directions. Gut. 2022, 71, 1669–1683. [Google Scholar] [CrossRef]
- Tot, T. Adenocarcinomas metastatic to the liver: the value of cytokeratins 20 and 7 in the search for unknown primary tumors. Cancer. 1999, 85, 171–177. [Google Scholar] [CrossRef]
- Dhanasekaran, R.; Suzuki, H.; Lemaitre, L.; Kubota, N.; Hoshida, Y. Molecular and immune landscape of hepatocellular carcinoma to guide therapeutic decision-making. Hepatology. 2023. [Google Scholar] [CrossRef] [PubMed]
- Tot, T. Identifying colorectal metastases in liver biopsies: the novel CDX2 antibody is less specific than the cytokeratin 20+/7- phenotype. Med Sci Monit. 2004, 10, BR139–143. [Google Scholar] [PubMed]
- Uenishi, T.; Yamazaki, O.; Tanaka, H.; Takemura, S.; Yamamoto, T.; Tanaka, S.; Nishiguchi, S.; Kubo, S. Serum cytokeratin 19 fragment (CYFRA21-1) as a prognostic factor in intrahepatic cholangiocarcinoma. Ann Surg Oncol. 2008, 15, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Chen, W.; Liang, P.; Hu, W.; Zhang, K.; Shen, S.; Chen, J.; Zhang, Z.; Chen, B.; Han, Y.; et al. Serum CYFRA 21-1 in Biliary Tract Cancers: A Reliable Biomarker for Gallbladder Carcinoma and Intrahepatic Cholangiocarcinoma. Dig Dis Sci. 2015, 60, 1273–1283. [Google Scholar] [CrossRef]
- Leelawat, K.; Narong, S.; Wannaprasert, J.; Ratanashu-ek, T. Prospective study of MMP7 serum levels in the diagnosis of cholangiocarcinoma. World J Gastroenterol. 2010, 16, 4697–4703. [Google Scholar] [CrossRef]
- Sirica, A.E. Matricellular proteins in intrahepatic cholangiocarcinoma. Adv Cancer Res. 2022, 156, 249–281. [Google Scholar] [PubMed]
- Loosen, S.H.; Roderburg, C.; Kauertz, K.L.; Pombeiro, I.; Leyh, C.; Benz, F.; Vucur, M.; Longerich, T.; Koch, A.; Braunschweig, T.; et al. Elevated levels of circulating osteopontin are associated with a poor survival after resection of cholangiocarcinoma. J Hepatol. 2017, 67, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Goydos, J.S.; Brumfield, A.M.; Frezza, E.; Booth, A.; Lotze, M.T.; Carty, S.E. Marked elevation of serum interleukin-6 in patients with cholangiocarcinoma: validation of utility as a clinical marker. Ann Surg. 1998, 227, 398–404. [Google Scholar] [CrossRef]
- Matull, W.R.; Andreola, F.; Loh, A.; Adiguzel, Z.; Deheragoda, M.; Qureshi, U.; Batra, S.K.; Swallow, D.M.; Pereira, S.P. MUC4 and MUC5AC are highly specific tumour-associated mucins in biliary tract cancer. Br J Cancer. 2008, 98, 1675–1681. [Google Scholar] [CrossRef]
- Lapitz, A.; Azkargorta, M.; Milkiewicz, P.; Olaizola, P.; Zhuravleva, E.; Grimsrud, M.M.; Schramm, C.; Arbelaiz, A.; O’Rourke, C.J.; La Casta, A.; et al. Liquid biopsy-based protein biomarkers for risk prediction, early diagnosis, and prognostication of cholangiocarcinoma. J Hepatol. 2023, 79, 93–108. [Google Scholar] [CrossRef]
- Banales, J.M.; Inarrairaegui, M.; Arbelaiz, A.; Milkiewicz, P.; Muntane, J.; Munoz-Bellvis, L.; La Casta, A.; Gonzalez, L.M.; Arretxe, E.; Alonso, C.; et al. Serum Metabolites as Diagnostic Biomarkers for Cholangiocarcinoma, Hepatocellular Carcinoma, and Primary Sclerosing Cholangitis. Hepatology. 2019, 70, 547–562. [Google Scholar] [CrossRef]
- Macias, R.I.R.; Munoz-Bellvis, L.; Sanchez-Martin, A.; Arretxe, E.; Martinez-Arranz, I.; Lapitz, A.; Gutierrez, M.L.; La Casta, A.; Alonso, C.; Gonzalez, L.M.; et al. A Novel Serum Metabolomic Profile for the Differential Diagnosis of Distal Cholangiocarcinoma and Pancreatic Ductal Adenocarcinoma. Cancers (Basel). 2020, 12. [Google Scholar] [CrossRef]
- Urman, J.M.; Herranz, J.M.; Uriarte, I.; Rullan, M.; Oyon, D.; Gonzalez, B.; Fernandez-Urien, I.; Carrascosa, J.; Bolado, F.; Zabalza, L.; et al. Pilot Multi-Omic Analysis of Human Bile from Benign and Malignant Biliary Strictures: A Machine-Learning Approach. Cancers (Basel). 2020, 12. [Google Scholar] [CrossRef]
- Tan, J.; Shu, M.; Liao, J.; Liang, R.; Liu, S.; Kuang, M.; Peng, S.; Xiao, H.; Zhou, Q. Identification and validation of a plasma metabolomics-based model for risk stratification of intrahepatic cholangiocarcinoma. J Cancer Res Clin Oncol. 2023, 149, 12365–12377. [Google Scholar] [CrossRef]
- Nakamura, H.; Arai, Y.; Totoki, Y.; Shirota, T.; Elzawahry, A.; Kato, M.; Hama, N.; Hosoda, F.; Urushidate, T.; Ohashi, S.; et al. Genomic spectra of biliary tract cancer. Nat Genet. 2015, 47, 1003–1010. [Google Scholar] [CrossRef]
- Javle, M.; Bekaii-Saab, T.; Jain, A.; Wang, Y.; Kelley, R.K.; Wang, K.; Kang, H.C.; Catenacci, D.; Ali, S.; Krishnan, S.; et al. Biliary cancer: Utility of next-generation sequencing for clinical management. Cancer. 2016, 122, 3838–3847. [Google Scholar] [CrossRef] [PubMed]
- Jusakul, A.; Cutcutache, I.; Yong, C.H.; Lim, J.Q.; Huang, M.N.; Padmanabhan, N.; Nellore, V.; Kongpetch, S.; Ng, A.W.T.; Ng, L.M.; et al. Whole-Genome and Epigenomic Landscapes of Etiologically Distinct Subtypes of Cholangiocarcinoma. Cancer Discov. 2017, 7, 1116–1135. [Google Scholar] [CrossRef] [PubMed]
- Wardell, C.P.; Fujita, M.; Yamada, T.; Simbolo, M.; Fassan, M.; Karlic, R.; Polak, P.; Kim, J.; Hatanaka, Y.; Maejima, K.; et al. Genomic characterization of biliary tract cancers identifies driver genes and predisposing mutations. J Hepatol. 2018, 68, 959–969. [Google Scholar] [CrossRef] [PubMed]
- Umemoto, K.; Yamamoto, H.; Oikawa, R.; Takeda, H.; Doi, A.; Horie, Y.; Arai, H.; Ogura, T.; Mizukami, T.; Izawa, N.; et al. The Molecular Landscape of Pancreatobiliary Cancers for Novel Targeted Therapies From Real-World Genomic Profiling. J Natl Cancer Inst. 2022, 114, 1279–1286. [Google Scholar] [CrossRef]
- Verlingue, L.; Malka, D.; Allorant, A.; Massard, C.; Ferte, C.; Lacroix, L.; Rouleau, E.; Auger, N.; Ngo, M.; Nicotra, C.; et al. Precision medicine for patients with advanced biliary tract cancers: An effective strategy within the prospective MOSCATO-01 trial. Eur J Cancer. 2017, 87, 122–130. [Google Scholar] [CrossRef]
- Verdaguer, H.; Sauri, T.; Acosta, D.A.; Guardiola, M.; Sierra, A.; Hernando, J.; Nuciforo, P.; Miquel, J.M.; Molero, C.; Peiro, S.; et al. ESMO Scale for Clinical Actionability of Molecular Targets Driving Targeted Treatment in Patients with Cholangiocarcinoma. Clin Cancer Res. 2022, 28, 1662–1671. [Google Scholar] [CrossRef]
- Mosele, F.; Remon, J.; Mateo, J.; Westphalen, C.B.; Barlesi, F.; Lolkema, M.P.; Normanno, N.; Scarpa, A.; Robson, M.; Meric-Bernstam, F.; et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: a report from the ESMO Precision Medicine Working Group. Ann Oncol. 2020, 31, 1491–1505. [Google Scholar] [CrossRef]
- Maruki, Y.; Morizane, C.; Arai, Y.; Ikeda, M.; Ueno, M.; Ioka, T.; Naganuma, A.; Furukawa, M.; Mizuno, N.; Uwagawa, T.; et al. Molecular detection and clinicopathological characteristics of advanced/recurrent biliary tract carcinomas harboring the FGFR2 rearrangements: a prospective observational study (PRELUDE Study). J Gastroenterol. 2021, 56, 250–260. [Google Scholar] [CrossRef]
- Nishida, N. The role of FGFR inhibitors in the treatment of intrahepatic cholangiocarcinoma-unveiling the future challenges in drug therapy. Hepatobiliary Surg Nutr. 2023, 12, 790–794. [Google Scholar] [CrossRef]
- Speckart, J.; Rasmusen, V.; Talib, Z.; GnanaDev, D.A.; Rahnemai-Azar, A.A. Emerging Therapies in Management of Cholangiocarcinoma. Cancers (Basel). 2024, 16. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Sahai, V.; Hollebecque, A.; Vaccaro, G.; Melisi, D.; Al-Rajabi, R.; Paulson, A.S.; Borad, M.J.; Gallinson, D.; Murphy, A.G.; et al. Pemigatinib for previously treated, locally advanced or metastatic cholangiocarcinoma: a multicentre, open-label, phase 2 study. Lancet Oncol. 2020, 21, 671–684. [Google Scholar] [CrossRef] [PubMed]
- Javle, M.; Roychowdhury, S.; Kelley, R.K.; Sadeghi, S.; Macarulla, T.; Weiss, K.H.; Waldschmidt, D.T.; Goyal, L.; Borbath, I.; El-Khoueiry, A.; et al. Infigratinib (BGJ398) in previously treated patients with advanced or metastatic cholangiocarcinoma with FGFR2 fusions or rearrangements: mature results from a multicentre, open-label, single-arm, phase 2 study. Lancet Gastroenterol Hepatol. 2021, 6, 803–815. [Google Scholar] [CrossRef] [PubMed]
- Goyal, L.; Meric-Bernstam, F.; Hollebecque, A.; Valle, J.W.; Morizane, C.; Karasic, T.B.; Abrams, T.A.; Furuse, J.; Kelley, R.K.; Cassier, P.A.; et al. Futibatinib for FGFR2-Rearranged Intrahepatic Cholangiocarcinoma. N Engl J Med. 2023, 388, 228–239. [Google Scholar] [CrossRef] [PubMed]
- Goyal, L.; Meric-Bernstam, F.; Hollebecque, A.; Valle, J.W.; Morizane, C.; Karasic, T.B.; Abrams, T.A.; Furuse, J.; Kelley, R.K.; Cassier, P.A.; et al. Plain language summary of the FOENIX-CCA2 study: futibatinib for people with advanced bile duct cancer. Future Oncol. 2024, 20, 2811–2822. [Google Scholar] [CrossRef]
- Nishida, N.; Aoki, T.; Morita, M.; Chishina, H.; Takita, M.; Ida, H.; Hagiwara, S.; Minami, Y.; Ueshima, K.; Kudo, M. Non-Inflamed Tumor Microenvironment and Methylation/Downregulation of Antigen-Presenting Machineries in Cholangiocarcinoma. Cancers (Basel). 2023, 15. [Google Scholar] [CrossRef]
- Nishida, N.; Kudo, M. Genetic/Epigenetic Alteration and Tumor Immune Microenvironment in Intrahepatic Cholangiocarcinoma: Transforming the Immune Microenvironment with Molecular-Targeted Agents. Liver Cancer. 2024, 13, 136–149. [Google Scholar] [CrossRef]
- Borger, D.R.; Goyal, L.; Yau, T.; Poon, R.T.; Ancukiewicz, M.; Deshpande, V.; Christiani, D.C.; Liebman, H.M.; Yang, H.; Kim, H.; et al. Circulating oncometabolite 2-hydroxyglutarate is a potential surrogate biomarker in patients with isocitrate dehydrogenase-mutant intrahepatic cholangiocarcinoma. Clin Cancer Res. 2014, 20, 1884–1890. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Macarulla, T.; Javle, M.M.; Kelley, R.K.; Lubner, S.J.; Adeva, J.; Cleary, J.M.; Catenacci, D.V.; Borad, M.J.; Bridgewater, J.; et al. Ivosidenib in IDH1-mutant, chemotherapy-refractory cholangiocarcinoma (ClarIDHy): a multicentre, randomised, double-blind, placebo-controlled, phase 3 study. Lancet Oncol. 2020, 21, 796–807. [Google Scholar] [CrossRef]
- Subbiah, V.; Kreitman, R.J.; Wainberg, Z.A.; Gazzah, A.; Lassen, U.; Stein, A.; Wen, P.Y.; Dietrich, S.; de Jonge, M.J.A.; Blay, J.Y.; et al. Dabrafenib plus trametinib in BRAFV600E-mutated rare cancers: the phase 2 ROAR trial. Nat Med. 2023, 29, 1103–1112. [Google Scholar] [CrossRef]
- Javle, M.; Borad, M.J.; Azad, N.S.; Kurzrock, R.; Abou-Alfa, G.K.; George, B.; Hainsworth, J.; Meric-Bernstam, F.; Swanton, C.; Sweeney, C.J.; et al. Pertuzumab and trastuzumab for HER2-positive, metastatic biliary tract cancer (MyPathway): a multicentre, open-label, phase 2a, multiple basket study. Lancet Oncol. 2021, 22, 1290–1300. [Google Scholar] [CrossRef]
- Harding, J.J.; Piha-Paul, S.A.; Shah, R.H.; Murphy, J.J.; Cleary, J.M.; Shapiro, G.I.; Quinn, D.I.; Brana, I.; Moreno, V.; Borad, M.; et al. Antitumour activity of neratinib in patients with HER2-mutant advanced biliary tract cancers. Nat Commun. 2023, 14, 630. [Google Scholar] [CrossRef] [PubMed]
- Harding, J.J.; Fan, J.; Oh, D.Y.; Choi, H.J.; Kim, J.W.; Chang, H.M.; Bao, L.; Sun, H.C.; Macarulla, T.; Xie, F.; et al. Zanidatamab for HER2-amplified, unresectable, locally advanced or metastatic biliary tract cancer (HERIZON-BTC-01): a multicentre, single-arm, phase 2b study. Lancet Oncol. 2023, 24, 772–782. [Google Scholar] [CrossRef] [PubMed]
- Ohba, A.; Morizane, C.; Kawamoto, Y.; Komatsu, Y.; Ueno, M.; Kobayashi, S.; Ikeda, M.; Sasaki, M.; Furuse, J.; Okano, N.; et al. Trastuzumab Deruxtecan in Human Epidermal Growth Factor Receptor 2-Expressing Biliary Tract Cancer (HERB; NCCH1805): A Multicenter, Single-Arm, Phase II Trial. J Clin Oncol. 2024, 42, 3207–3217. [Google Scholar] [CrossRef] [PubMed]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of Pembrolizumab in Patients With Noncolorectal High Microsatellite Instability/Mismatch Repair-Deficient Cancer: Results From the Phase II KEYNOTE-158 Study. J Clin Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef]
- Marabelle, A.; Fakih, M.; Lopez, J.; Shah, M.; Shapira-Frommer, R.; Nakagawa, K.; Chung, H.C.; Kindler, H.L.; Lopez-Martin, J.A.; Miller, W.H., Jr.; et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol. 2020, 21, 1353–1365. [Google Scholar] [CrossRef]
- Mavroeidi, I.A.; Burghofer, J.; Kalbourtzis, S.; Taghizadeh, H.; Webersinke, G.; Piringer, G.; Kasper, S.; Schreil, G.; Liffers, S.T.; Reichinger, A.; et al. Understanding homologous recombination repair deficiency in biliary tract cancers: clinical implications and correlation with platinum sensitivity. ESMO Open. 2024, 9, 103630. [Google Scholar] [CrossRef]
- Hong, D.S.; DuBois, S.G.; Kummar, S.; Farago, A.F.; Albert, C.M.; Rohrberg, K.S.; van Tilburg, C.M.; Nagasubramanian, R.; Berlin, J.D.; Federman, N.; et al. Larotrectinib in patients with TRK fusion-positive solid tumours: a pooled analysis of three phase 1/2 clinical trials. Lancet Oncol. 2020, 21, 531–540. [Google Scholar] [CrossRef]
- Doebele, R.C.; Drilon, A.; Paz-Ares, L.; Siena, S.; Shaw, A.T.; Farago, A.F.; Blakely, C.M.; Seto, T.; Cho, B.C.; Tosi, D.; et al. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: integrated analysis of three phase 1-2 trials. Lancet Oncol. 2020, 21, 271–282. [Google Scholar] [CrossRef]
- Lin, D.; Shen, L.; Luo, M.; Zhang, K.; Li, J.; Yang, Q.; Zhu, F.; Zhou, D.; Zheng, S.; Chen, Y.; et al. Circulating tumor cells: biology and clinical significance. Signal Transduct Target Ther. 2021, 6, 404. [Google Scholar] [CrossRef]
- Yang, J.D.; Campion, M.B.; Liu, M.C.; Chaiteerakij, R.; Giama, N.H.; Ahmed Mohammed, H.; Zhang, X.; Hu, C.; Campion, V.L.; Jen, J.; et al. Circulating tumor cells are associated with poor overall survival in patients with cholangiocarcinoma. Hepatology. 2016, 63, 148–158. [Google Scholar] [CrossRef]
- Liang, K.H.; Yeh, T.S.; Wu, R.C.; Yeh, C.N.; Yeh, C.T. GALNT14 genotype is associated with perineural invasion, lymph node metastasis and overall survival in resected cholangiocarcinoma. Oncol Lett. 2017, 13, 4215–4223. [Google Scholar] [CrossRef]
- Pan, Y.; Shao, S.; Sun, H.; Zhu, H.; Fang, H. Bile-derived exosome noncoding RNAs as potential diagnostic and prognostic biomarkers for cholangiocarcinoma. Front Oncol. 2022, 12, 985089. [Google Scholar] [CrossRef]
- Uson Junior, P.L.S.; Majeed, U.; Yin, J.; Botrus, G.; Sonbol, M.B.; Ahn, D.H.; Starr, J.S.; Jones, J.C.; Babiker, H.; Inabinett, S.R.; et al. Cell-Free Tumor DNA Dominant Clone Allele Frequency Is Associated With Poor Outcomes in Advanced Biliary Cancers Treated With Platinum-Based Chemotherapy. JCO Precis Oncol. 2022, 6, e2100274. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Xin, H.; Zhou, Z.; Hu, Z.; Sun, R.; Yao, N.; Sun, Q.; Borjigin, U.; Wu, X.; Fan, J.; et al. Tumor-derived exosomes induce immunosuppressive macrophages to foster intrahepatic cholangiocarcinoma progression. Hepatology. 2022, 76, 982–999. [Google Scholar] [CrossRef] [PubMed]
- Lurje, I.; Czigany, Z.; Bednarsch, J.; Gaisa, N.T.; Dahl, E.; Knuchel, R.; Miller, H.; Ulmer, T.F.; Strnad, P.; Trautwein, C.; et al. Genetic Variant of CXCR1 (rs2234671) Associates with Clinical Outcome in Perihilar Cholangiocarcinoma. Liver Cancer. 2022, 11, 162–173. [Google Scholar] [CrossRef]
- Shu, L.; Li, X.; Liu, Z.; Li, K.; Shi, A.; Tang, Y.; Zhao, L.; Huang, L.; Zhang, Z.; Zhang, D.; et al. Bile exosomal miR-182/183-5p increases cholangiocarcinoma stemness and progression by targeting HPGD and increasing PGE2 generation. Hepatology. 2024, 79, 307–322. [Google Scholar] [CrossRef]
- Valle, J.W.; Wasan, H.; Lopes, A.; Backen, A.C.; Palmer, D.H.; Morris, K.; Duggan, M.; Cunningham, D.; Anthoney, D.A.; Corrie, P.; et al. Cediranib or placebo in combination with cisplatin and gemcitabine chemotherapy for patients with advanced biliary tract cancer (ABC-03): a randomised phase 2 trial. Lancet Oncol. 2015, 16, 967–978. [Google Scholar] [CrossRef]
- Iyer, R.V.; Pokuri, V.K.; Groman, A.; Ma, W.W.; Malhotra, U.; Iancu, D.M.; Grande, C.; Saab, T.B. A Multicenter Phase II Study of Gemcitabine, Capecitabine, and Bevacizumab for Locally Advanced or Metastatic Biliary Tract Cancer. Am J Clin Oncol. 2018, 41, 649–655. [Google Scholar] [CrossRef]
- Frundt, T.; von Felden, J.; Krause, J.; Heumann, A.; Li, J.; Riethdorf, S.; Pantel, K.; Huber, S.; Lohse, A.W.; Wege, H.; et al. Circulating tumor cells as a preoperative risk marker for occult metastases in patients with resectable cholangiocarcinoma. Front Oncol. 2022, 12, 941660. [Google Scholar] [CrossRef]
- Gopinathan, P.; Chiang, N.J.; Bandaru, A.; Sinha, A.; Huang, W.Y.; Hung, S.C.; Shan, Y.S.; Lee, G.B. Exploring Circulating Tumor Cells in Cholangiocarcinoma Using a Novel Glycosaminoglycan Probe on a Microfluidic Platform. Adv Healthc Mater. 2020, 9, e1901875. [Google Scholar] [CrossRef]
- Chang, J.L.; Huang, C.J.; Tsai, Y.C.; Chiang, N.J.; Huang, Y.S.; Hung, S.C.; Shan, Y.S.; Lee, G.B. An integrated microfluidic system for automatic detection of cholangiocarcinoma cells from bile. Lab Chip. 2024, 24, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Rompianesi, G.; Di Martino, M.; Gordon-Weeks, A.; Montalti, R.; Troisi, R. Liquid biopsy in cholangiocarcinoma: Current status and future perspectives. World J Gastrointest Oncol. 2021, 13, 332–350. [Google Scholar] [CrossRef] [PubMed]
- Lamarca, A.; Kapacee, Z.; Breeze, M.; Bell, C.; Belcher, D.; Staiger, H.; Taylor, C.; McNamara, M.G.; Hubner, R.A.; Valle, J.W. Molecular Profiling in Daily Clinical Practice: Practicalities in Advanced Cholangiocarcinoma and Other Biliary Tract Cancers. J Clin Med. 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Taniguchi, H.; Ikeda, M.; Bando, H.; Kato, K.; Morizane, C.; Esaki, T.; Komatsu, Y.; Kawamoto, Y.; Takahashi, N.; et al. Clinical utility of circulating tumor DNA sequencing in advanced gastrointestinal cancer: SCRUM-Japan GI-SCREEN and GOZILA studies. Nat Med. 2020, 26, 1859–1864. [Google Scholar] [CrossRef]
- Wintachai, P.; Lim, J.Q.; Techasen, A.; Lert-Itthiporn, W.; Kongpetch, S.; Loilome, W.; Chindaprasirt, J.; Titapun, A.; Namwat, N.; Khuntikeo, N.; et al. Diagnostic and Prognostic Value of Circulating Cell-Free DNA for Cholangiocarcinoma. Diagnostics (Basel). 2021, 11. [Google Scholar] [CrossRef]
- Hashimoto, T.; Nakamura, Y.; Oki, E.; Kobayashi, S.; Yuda, J.; Shibuki, T.; Bando, H.; Yoshino, T. Bridging horizons beyond CIRCULATE-Japan: a new paradigm in molecular residual disease detection via whole genome sequencing-based circulating tumor DNA assay. Int J Clin Oncol. 2024, 29, 495–511. [Google Scholar] [CrossRef]
- Mody, K.; Cleary, S.P. A Review of Circulating Tumor DNA in Hepatobiliary Malignancies. Front Oncol. 2018, 8, 212. [Google Scholar] [CrossRef]
- Ettrich, T.J.; Schwerdel, D.; Dolnik, A.; Beuter, F.; Blatte, T.J.; Schmidt, S.A.; Stanescu-Siegmund, N.; Steinacker, J.; Marienfeld, R.; Kleger, A.; et al. Genotyping of circulating tumor DNA in cholangiocarcinoma reveals diagnostic and prognostic information. Sci Rep. 2019, 9, 13261. [Google Scholar] [CrossRef]
- Okamura, R.; Kurzrock, R.; Mallory, R.J.; Fanta, P.T.; Burgoyne, A.M.; Clary, B.M.; Kato, S.; Sicklick, J.K. Comprehensive genomic landscape and precision therapeutic approach in biliary tract cancers. Int J Cancer. 2021, 148, 702–712. [Google Scholar] [CrossRef]
- Berchuck, J.E.; Facchinetti, F.; DiToro, D.F.; Baiev, I.; Majeed, U.; Reyes, S.; Chen, C.; Zhang, K.; Sharman, R.; Uson Junior, P.L.S.; et al. The clinical landscape of cell-free DNA alterations in 1671 patients with advanced biliary tract cancer. Ann Oncol. 2022, 33, 1269–1283. [Google Scholar] [CrossRef]
- Kurzrock, R.; Aggarwal, C.; Weipert, C.; Kiedrowski, L.; Riess, J.; Lenz, H.J.; Gandara, D. Prevalence of ARID1A Mutations in Cell-Free Circulating Tumor DNA in a Cohort of 71,301 Patients and Association with Driver Co-Alterations. Cancers (Basel). 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.J.; Ivanics, T.; Gravely, A.; Gallinger, S.; Sapisochin, G.; O’Kane, G.M. Optimizing Circulating Tumour DNA Use in the Perioperative Setting for Intrahepatic Cholangiocarcinoma: Diagnosis, Screening, Minimal Residual Disease Detection and Treatment Response Monitoring. Ann Surg Oncol. 2023, 30, 3849–3863. [Google Scholar] [CrossRef] [PubMed]
- Vedeld, H.M.; Folseraas, T.; Lind, G.E. Detecting cholangiocarcinoma in patients with primary sclerosing cholangitis - The promise of DNA methylation and molecular biomarkers. JHEP Rep. 2020, 2, 100143. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.A.; Richards, D.; Cohn, A.; Tummala, M.; Lapham, R.; Cosgrove, D.; Chung, G.; Clement, J.; Gao, J.; Hunkapiller, N.; et al. Clinical validation of a targeted methylation-based multi-cancer early detection test using an independent validation set. Ann Oncol. 2021, 32, 1167–1177. [Google Scholar] [CrossRef]
- Andersen, L.B.; Mahler, M.S.K.; Andersen, R.F.; Jensen, L.H.; Raunkilde, L. The Clinical Impact of Methylated Homeobox A9 ctDNA in Patients with Non-Resectable Biliary Tract Cancer Treated with Erlotinib and Bevacizumab. Cancers (Basel). 2022, 14. [Google Scholar] [CrossRef]
- Kasi, P.M.; Lee, J.K.; Pasquina, L.W.; Decker, B.; Vanden Borre, P.; Pavlick, D.C.; Allen, J.M.; Parachoniak, C.; Quintanilha, J.C.F.; Graf, R.P.; et al. Circulating Tumor DNA Enables Sensitive Detection of Actionable Gene Fusions and Rearrangements Across Cancer Types. Clin Cancer Res. 2024, 30, 836–848. [Google Scholar] [CrossRef]
- Castro-Oropeza, R.; Melendez-Zajgla, J.; Maldonado, V.; Vazquez-Santillan, K. The emerging role of lncRNAs in the regulation of cancer stem cells. Cell Oncol (Dordr). 2018, 41, 585–603. [Google Scholar] [CrossRef]
- Liang, Z.; Zhu, B.; Meng, D.; Shen, X.; Li, X.; Wang, Z.; Li, L. Down-regulation of lncRNA-NEF indicates poor prognosis in intrahepatic cholangiocarcinoma. Biosci Rep. 2019, 39. [Google Scholar] [CrossRef]
- Meng, F.; Henson, R.; Lang, M.; Wehbe, H.; Maheshwari, S.; Mendell, J.T.; Jiang, J.; Schmittgen, T.D.; Patel, T. Involvement of human micro-RNA in growth and response to chemotherapy in human cholangiocarcinoma cell lines. Gastroenterology. 2006, 130, 2113–2129. [Google Scholar] [CrossRef]
- Shen, L.; Chen, G.; Xia, Q.; Shao, S.; Fang, H. Exosomal miR-200 family as serum biomarkers for early detection and prognostic prediction of cholangiocarcinoma. Int J Clin Exp Pathol. 2019, 12, 3870–3876. [Google Scholar]
- Asukai, K.; Kawamoto, K.; Eguchi, H.; Konno, M.; Asai, A.; Iwagami, Y.; Yamada, D.; Asaoka, T.; Noda, T.; Wada, H.; et al. Micro-RNA-130a-3p Regulates Gemcitabine Resistance via PPARG in Cholangiocarcinoma. Ann Surg Oncol. 2017, 24, 2344–2352. [Google Scholar] [CrossRef] [PubMed]
- Peng, F.; Jiang, J.; Yu, Y.; Tian, R.; Guo, X.; Li, X.; Shen, M.; Xu, M.; Zhu, F.; Shi, C.; et al. Direct targeting of SUZ12/ROCK2 by miR-200b/c inhibits cholangiocarcinoma tumourigenesis and metastasis. Br J Cancer. 2013, 109, 3092–3104. [Google Scholar] [CrossRef]
- Carotenuto, P.; Hedayat, S.; Fassan, M.; Cardinale, V.; Lampis, A.; Guzzardo, V.; Vicentini, C.; Scarpa, A.; Cascione, L.; Costantini, D.; et al. Modulation of Biliary Cancer Chemo-Resistance Through MicroRNA-Mediated Rewiring of the Expansion of CD133+ Cells. Hepatology. 2020, 72, 982–996. [Google Scholar] [CrossRef] [PubMed]
- Silakit, R.; Kitirat, Y.; Thongchot, S.; Loilome, W.; Techasen, A.; Ungarreevittaya, P.; Khuntikeo, N.; Yongvanit, P.; Yang, J.H.; Kim, N.H.; et al. Potential role of HIF-1-responsive microRNA210/HIF3 axis on gemcitabine resistance in cholangiocarcinoma cells. PLoS One. 2018, 13, e0199827. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.; Qin, X.; Zhou, Y.; Li, G.; Liu, Z.; Geng, X.; Yue, H. Long non-coding RNA LINC00665 promotes gemcitabine resistance of Cholangiocarcinoma cells via regulating EMT and stemness properties through miR-424-5p/BCL9L axis. Cell Death Dis. 2021, 12, 72. [Google Scholar] [CrossRef]
- Obata, T.; Tsutsumi, K.; Ueta, E.; Oda, T.; Kikuchi, T.; Ako, S.; Fujii, Y.; Yamazaki, T.; Uchida, D.; Matsumoto, K.; et al. MicroRNA-451a inhibits gemcitabine-refractory biliary tract cancer progression by suppressing the MIF-mediated PI3K/AKT pathway. Mol Ther Nucleic Acids. 2023, 34, 102054. [Google Scholar] [CrossRef]
- Tokuhisa, A.; Tsunedomi, R.; Kimura, Y.; Nakajima, M.; Nishiyama, M.; Takahashi, H.; Ioka, T.; Kobayashi, S.; Eguchi, H.; Nagano, H. Exosomal miR-141-3p Induces Gemcitabine Resistance in Biliary Tract Cancer Cells. Anticancer Res. 2024, 44, 2899–2908. [Google Scholar] [CrossRef]
- Du, H.; Hou, S.; Zhang, L.; Liu, C.; Yu, T.; Zhang, W. LncRNA FALEC increases the proliferation, migration and drug resistance of cholangiocarcinoma through competitive regulation of miR-20a-5p/SHOC2 axis. Aging (Albany NY). 2023, 15, 3759–3770. [Google Scholar] [CrossRef]
- Zhang, L.; Ma, D.; Li, F.; Qiu, G.; Sun, D.; Zeng, Z. Lnc-PKD2-2-3/miR-328/GPAM ceRNA Network Induces Cholangiocarcinoma Proliferation, Invasion and 5-FU Chemoresistance. Front Oncol. 2022, 12, 871281. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, W.; Chen, L.; Chen, W.; Xu, S.; Tang, L.; Yang, Y.; Li, Q.; Jiang, Q.; Miao, L. The ATO/miRNA-885-5p/MTPN axis induces reversal of drug-resistance in cholangiocarcinoma. Cell Oncol (Dordr). 2021, 44, 907–916. [Google Scholar] [CrossRef]
- Li, Q.; Xia, X.; Ji, J.; Ma, J.; Tao, L.; Mo, L.; Chen, W. MiR-199a-3p enhances cisplatin sensitivity of cholangiocarcinoma cells by inhibiting mTOR signaling pathway and expression of MDR1. Oncotarget. 2017, 8, 33621–33630. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Jiang, X.; Li, Z.; Huang, L.; Ji, D.; Yu, L.; Zhou, Y.; Cui, Y. SP1-induced HOXD-AS1 promotes malignant progression of cholangiocarcinoma by regulating miR-520c-3p/MYCN. Aging (Albany NY). 2020, 12, 16304–16325. [Google Scholar] [CrossRef]
- Kopp, F.; Mendell, J.T. Functional Classification and Experimental Dissection of Long Noncoding RNAs. Cell. 2018, 172, 393–407. [Google Scholar] [CrossRef] [PubMed]
- Lapitz, A.; Arbelaiz, A.; O’Rourke, C.J.; Lavin, J.L.; Casta, A.; Ibarra, C.; Jimeno, J.P.; Santos-Laso, A.; Izquierdo-Sanchez, L.; Krawczyk, M.; et al. Patients with Cholangiocarcinoma Present Specific RNA Profiles in Serum and Urine Extracellular Vesicles Mirroring the Tumor Expression: Novel Liquid Biopsy Biomarkers for Disease Diagnosis. Cells. 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Ge, X.; Wang, Y.; Nie, J.; Li, Q.; Tang, L.; Deng, X.; Wang, F.; Xu, B.; Wu, X.; Zhang, X.; et al. The diagnostic/prognostic potential and molecular functions of long non-coding RNAs in the exosomes derived from the bile of human cholangiocarcinoma. Oncotarget. 2017, 8, 69995–70005. [Google Scholar] [CrossRef]
- Li, J.; Jiang, X.; Xu, Y.; Kang, P.; Huang, P.; Meng, N.; Wang, H.; Zheng, W.; Wang, H.; Wang, Z.; et al. YY1-induced DLEU1/miR-149-5p Promotes Malignant Biological Behavior of Cholangiocarcinoma through Upregulating YAP1/TEAD2/SOX2. Int J Biol Sci. 2022, 18, 4301–4315. [Google Scholar] [CrossRef]
- Shi, J.; Li, X.; Zhang, F.; Kong, L.; Zhang, X.; Cheng, Y.; Guan, Q.; Cao, X.; Zhu, W.; Ou, K.; et al. The Plasma LncRNA Acting as Fingerprint in Hilar Cholangiocarcinoma. Cell Physiol Biochem. 2018, 49, 1694–1702. [Google Scholar] [CrossRef]
- Zhang, F.; Wan, M.; Xu, Y.; Li, Z.; Leng, K.; Kang, P.; Cui, Y.; Jiang, X. Long noncoding RNA PCAT1 regulates extrahepatic cholangiocarcinoma progression via the Wnt/beta-catenin-signaling pathway. Biomed Pharmacother. 2017, 94, 55–62. [Google Scholar] [CrossRef]
- Xu, Y.; Wang, Z.; Jiang, X.; Cui, Y. Overexpression of long noncoding RNA H19 indicates a poor prognosis for cholangiocarcinoma and promotes cell migration and invasion by affecting epithelial-mesenchymal transition. Biomed Pharmacother. 2017, 92, 17–23. [Google Scholar] [CrossRef]
- Han, B.W.; Ye, H.; Wei, P.P.; He, B.; Han, C.; Chen, Z.H.; Chen, Y.Q.; Wang, W.T. Global identification and characterization of lncRNAs that control inflammation in malignant cholangiocytes. BMC Genomics. 2018, 19, 735. [Google Scholar] [CrossRef]
- Jiang, X.M.; Li, Z.L.; Li, J.L.; Zheng, W.Y.; Li, X.H.; Cui, Y.F.; Sun, D.J. LncRNA CCAT1 as the unfavorable prognostic biomarker for cholangiocarcinoma. Eur Rev Med Pharmacol Sci. 2017, 21, 1242–1247. [Google Scholar] [PubMed]
- Bai, J.G.; Tang, R.F.; Shang, J.F.; Qi, S.; Yu, G.D.; Sun, C. Upregulation of long non-coding RNA CCAT2 indicates a poor prognosis and promotes proliferation and metastasis in intrahepatic cholangiocarcinoma. Mol Med Rep. 2018, 17, 5328–5335. [Google Scholar] [CrossRef]
- Jiang, X.; Li, J.; Wang, W.; Hu, Z.; Guan, C.; Zhao, Y.; Li, W.; Cui, Y. AR-induced ZEB1-AS1 represents poor prognosis in cholangiocarcinoma and facilitates tumor stemness, proliferation and invasion through mediating miR-133b/HOXB8. Aging (Albany NY). 2020, 12, 1237–1255. [Google Scholar] [CrossRef] [PubMed]
- Angenard, G.; Merdrignac, A.; Louis, C.; Edeline, J.; Coulouarn, C. Expression of long non-coding RNA ANRIL predicts a poor prognosis in intrahepatic cholangiocarcinoma. Dig Liver Dis. 2019, 51, 1337–1343. [Google Scholar] [CrossRef]
- Wang, X.P.; Song, J.; Liu, G.T.; Wang, J.J.; Guo, H.F. Upregulation of gastric adenocarcinoma predictive long intergenic non-coding RNA promotes progression and predicts poor prognosis in perihilar cholangiocarcinoma. Oncol Lett. 2018, 16, 3964–3972. [Google Scholar] [CrossRef]
- Hu, Z.; Huang, L.; Wang, W.; Guan, C.; Zhao, Y.; Liu, L.; Jiang, X. Long Non-coding RNA FOXD2-AS1 Promotes Proliferation, Migration, and Invasion in Cholangiocarcinoma Through Regulating miR-760/E2F3 Axis. Dig Dis Sci. 2022, 67, 546–558. [Google Scholar] [CrossRef]
- Jiang, X.M.; Li, Z.L.; Li, J.L.; Xu, Y.; Leng, K.M.; Cui, Y.F.; Sun, D.J. A novel prognostic biomarker for cholangiocarcinoma: circRNA Cdr1as. Eur Rev Med Pharmacol Sci. 2018, 22, 365–371. [Google Scholar]
- Xu, Y.; Leng, K.; Yao, Y.; Kang, P.; Liao, G.; Han, Y.; Shi, G.; Ji, D.; Huang, P.; Zheng, W.; et al. A Circular RNA, Cholangiocarcinoma-Associated Circular RNA 1, Contributes to Cholangiocarcinoma Progression, Induces Angiogenesis, and Disrupts Vascular Endothelial Barriers. Hepatology. 2021, 73, 1419–1435. [Google Scholar] [CrossRef]
- Wang, S.; Hu, Y.; Lv, X.; Li, B.; Gu, D.; Li, Y.; Sun, Y.; Su, Y. Circ-0000284 arouses malignant phenotype of cholangiocarcinoma cells and regulates the biological functions of peripheral cells through cellular communication. Clin Sci (Lond). 2019, 133, 1935–1953. [Google Scholar] [CrossRef]
- Chen, S.; Chen, Z.; Li, Z.; Li, S.; Wen, Z.; Cao, L.; Chen, Y.; Xue, P.; Li, H.; Zhang, D. Tumor-associated macrophages promote cholangiocarcinoma progression via exosomal Circ_0020256. Cell Death Dis. 2022, 13, 94. [Google Scholar] [CrossRef]
- Xu, Y.; Gao, P.; Wang, Z.; Su, Z.; Liao, G.; Han, Y.; Cui, Y.; Yao, Y.; Zhong, X. Circ-LAMP1 contributes to the growth and metastasis of cholangiocarcinoma via miR-556-5p and miR-567 mediated YY1 activation. J Cell Mol Med. 2021, 25, 3226–3238. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Lan, T.; Liu, H.; Liu, C.; Dai, J.; Xu, L.; Cai, Y.; Hou, G.; Xie, K.; Liao, M.; et al. IL-6-induced cGGNBP2 encodes a protein to promote cell growth and metastasis in intrahepatic cholangiocarcinoma. Hepatology. 2022, 75, 1402–1419. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhao, Y.; Wang, W.; Yu, S.; Liu, L.; Sun, D.; Li, W.; Jiang, X. Upregulation of circ_0059961 suppresses cholangiocarcinoma development by modulating miR-629-5p/SFRP2 axis. Pathol Res Pract. 2022, 234, 153901. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.P.; Dong, Z.N.; Wang, S.W.; Zheng, Y.M.; Zhang, C.; Zhou, Y.Q.; Zhao, Y.J.; Zhao, Y.; Wang, F.; Peng, R.; et al. circHMGCS1-016 reshapes immune environment by sponging miR-1236-3p to regulate CD73 and GAL-8 expression in intrahepatic cholangiocarcinoma. J Exp Clin Cancer Res. 2021, 40, 290. [Google Scholar] [CrossRef]
- Oh, D.Y.; Ruth He, A.; Qin, S.; Chen, L.T.; Okusaka, T.; Vogel, A.; Kim, J.W.; Suksombooncharoen, T.; Ah Lee, M.; Kitano, M.; et al. Durvalumab plus Gemcitabine and Cisplatin in Advanced Biliary Tract Cancer. NEJM Evid. 2022, 1, EVIDoa2200015. [Google Scholar] [CrossRef]
- Kelley, R.K.; Ueno, M.; Yoo, C.; Finn, R.S.; Furuse, J.; Ren, Z.; Yau, T.; Klumpen, H.J.; Chan, S.L.; Ozaka, M.; et al. Pembrolizumab in combination with gemcitabine and cisplatin compared with gemcitabine and cisplatin alone for patients with advanced biliary tract cancer (KEYNOTE-966): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2023, 401, 1853–1865. [Google Scholar] [CrossRef]
- Job, S.; Rapoud, D.; Dos Santos, A.; Gonzalez, P.; Desterke, C.; Pascal, G.; Elarouci, N.; Ayadi, M.; Adam, R.; Azoulay, D.; et al. Identification of Four Immune Subtypes Characterized by Distinct Composition and Functions of Tumor Microenvironment in Intrahepatic Cholangiocarcinoma. Hepatology. 2020, 72, 965–981. [Google Scholar] [CrossRef]
- Martin-Serrano, M.A.; Kepecs, B.; Torres-Martin, M.; Bramel, E.R.; Haber, P.K.; Merritt, E.; Rialdi, A.; Param, N.J.; Maeda, M.; Lindblad, K.E.; et al. Novel microenvironment-based classification of intrahepatic cholangiocarcinoma with therapeutic implications. Gut. 2023, 72, 736–748. [Google Scholar] [CrossRef]
- Zhu, C.; Ma, J.; Zhu, K.; Yu, L.; Zheng, B.; Rao, D.; Zhang, S.; Dong, L.; Gao, Q.; Zhang, X.; et al. Spatial immunophenotypes predict clinical outcome in intrahepatic cholangiocarcinoma. JHEP Rep. 2023, 5, 100762. [Google Scholar] [CrossRef]
- Montironi, C.; Castet, F.; Haber, P.K.; Pinyol, R.; Torres-Martin, M.; Torrens, L.; Mesropian, A.; Wang, H.; Puigvehi, M.; Maeda, M.; et al. Inflamed and non-inflamed classes of HCC: a revised immunogenomic classification. Gut. 2023, 72, 129–140. [Google Scholar] [CrossRef]
- Lin, Y.; Peng, L.; Dong, L.; Liu, D.; Ma, J.; Lin, J.; Chen, X.; Lin, P.; Song, G.; Zhang, M.; et al. Geospatial Immune Heterogeneity Reflects the Diverse Tumor-Immune Interactions in Intrahepatic Cholangiocarcinoma. Cancer Discov. 2022, 12, 2350–2371. [Google Scholar] [CrossRef] [PubMed]
- Mody, K.; Jain, P.; El-Refai, S.M.; Azad, N.S.; Zabransky, D.J.; Baretti, M.; Shroff, R.T.; Kelley, R.K.; El-Khouiery, A.B.; Hockenberry, A.J.; et al. Clinical, Genomic, and Transcriptomic Data Profiling of Biliary Tract Cancer Reveals Subtype-Specific Immune Signatures. JCO Precis Oncol. 2022, 6, e2100510. [Google Scholar] [CrossRef] [PubMed]
- Spranger, S.; Bao, R.; Gajewski, T.F. Melanoma-intrinsic beta-catenin signalling prevents anti-tumour immunity. Nature. 2015, 523, 231–235. [Google Scholar] [CrossRef]
- Das, S.; Shapiro, B.; Vucic, E.A.; Vogt, S.; Bar-Sagi, D. Tumor Cell-Derived IL1beta Promotes Desmoplasia and Immune Suppression in Pancreatic Cancer. Cancer Res. 2020, 80, 1088–1101. [Google Scholar] [CrossRef]
- Maio, M.; Ascierto, P.A.; Manzyuk, L.; Motola-Kuba, D.; Penel, N.; Cassier, P.A.; Bariani, G.M.; De Jesus Acosta, A.; Doi, T.; Longo, F.; et al. Pembrolizumab in microsatellite instability high or mismatch repair deficient cancers: updated analysis from the phase II KEYNOTE-158 study. Ann Oncol. 2022, 33, 929–938. [Google Scholar] [CrossRef]
- Diggs, L.P.; Ruf, B.; Ma, C.; Heinrich, B.; Cui, L.; Zhang, Q.; McVey, J.C.; Wabitsch, S.; Heinrich, S.; Rosato, U.; et al. CD40-mediated immune cell activation enhances response to anti-PD-1 in murine intrahepatic cholangiocarcinoma. J Hepatol. 2021, 74, 1145–1154. [Google Scholar] [CrossRef]
- Wabitsch, S.; Tandon, M.; Ruf, B.; Zhang, Q.; McCallen, J.D.; McVey, J.C.; Ma, C.; Green, B.L.; Diggs, L.P.; Heinrich, B.; et al. Anti-PD-1 in Combination With Trametinib Suppresses Tumor Growth and Improves Survival of Intrahepatic Cholangiocarcinoma in Mice. Cell Mol Gastroenterol Hepatol. 2021, 12, 1166–1178. [Google Scholar] [CrossRef]
- Lau, G.; Obi, S.; Zhou, J.; Tateishi, R.; Qin, S.; Zhao, H.; Otsuka, M.; Ogasawara, S.; George, J.; Chow, P.K.H.; et al. APASL clinical practice guidelines on systemic therapy for hepatocellular carcinoma-2024. Hepatol Int. 2024, 18, 1661–1683. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. Electronic address, e.e.e.; European Association for the Study of the, L. EASL Clinical Practice Guidelines on the management of hepatocellular carcinoma. J Hepatol. 2025, 82, 315–374. [Google Scholar] [CrossRef]
- Liu, F.; Hao, X.; Liu, B.; Liu, S.; Yuan, Y. Bile liquid biopsy in biliary tract cancer. Clin Chim Acta. 2023, 551, 117593. [Google Scholar] [CrossRef]
- Gou, Q.; Zhang, C.Z.; Sun, Z.H.; Wu, L.G.; Chen, Y.; Mo, Z.Q.; Mai, Q.C.; He, J.; Zhou, Z.X.; Shi, F.; et al. Cell-free DNA from bile outperformed plasma as a potential alternative to tissue biopsy in biliary tract cancer. ESMO Open. 2021, 6, 100275. [Google Scholar] [CrossRef] [PubMed]
- Vedeld, H.M.; Grimsrud, M.M.; Andresen, K.; Pharo, H.D.; von Seth, E.; Karlsen, T.H.; Honne, H.; Paulsen, V.; Farkkila, M.A.; Bergquist, A.; et al. Early and accurate detection of cholangiocarcinoma in patients with primary sclerosing cholangitis by methylation markers in bile. Hepatology. 2022, 75, 59–73. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Liu, Z.; Chen, L.; Wang, Z.; Zhai, Y.; Qian, P.; Zhao, Y.; Zhu, L.; Jiang, H.; Wu, X.; et al. Liquid Biopsy-Based Accurate Diagnosis and Genomic Profiling of Hard-to-Biopsy Tumors via Parallel Single-Cell Genomic Sequencing of Exfoliated Tumor Cells. Anal Chem. 2024, 96, 14669–14678. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The candidate of biomarkers in the diagnosis, therapeutic selection, and monitoring of recurrence in cholangiocarcinoma. In addition to conventional serum biomarkers, novel biomarker candidates for the diagnosis, therapeutic selection, and monitoring of recurrence in cholangiocarcinoma (CCA) have been illustrated. Gene panel testing plays a critical role in determining the suitability of molecular targeted therapies for CCA. Moreover, biomarkers such as circulating tumor DNA (ctDNA), cell-free DNA (cfDNA), non-coding RNAs, extracellular vesicle-derived protein panels, and plasma metabolite panels have been reported for applications including diagnosis, evaluation of disease progression, and prognostic prediction. However, at present, these novel biomarkers, apart from gene panel testing, remain in the developmental stage.
Figure 1.
The candidate of biomarkers in the diagnosis, therapeutic selection, and monitoring of recurrence in cholangiocarcinoma. In addition to conventional serum biomarkers, novel biomarker candidates for the diagnosis, therapeutic selection, and monitoring of recurrence in cholangiocarcinoma (CCA) have been illustrated. Gene panel testing plays a critical role in determining the suitability of molecular targeted therapies for CCA. Moreover, biomarkers such as circulating tumor DNA (ctDNA), cell-free DNA (cfDNA), non-coding RNAs, extracellular vesicle-derived protein panels, and plasma metabolite panels have been reported for applications including diagnosis, evaluation of disease progression, and prognostic prediction. However, at present, these novel biomarkers, apart from gene panel testing, remain in the developmental stage.
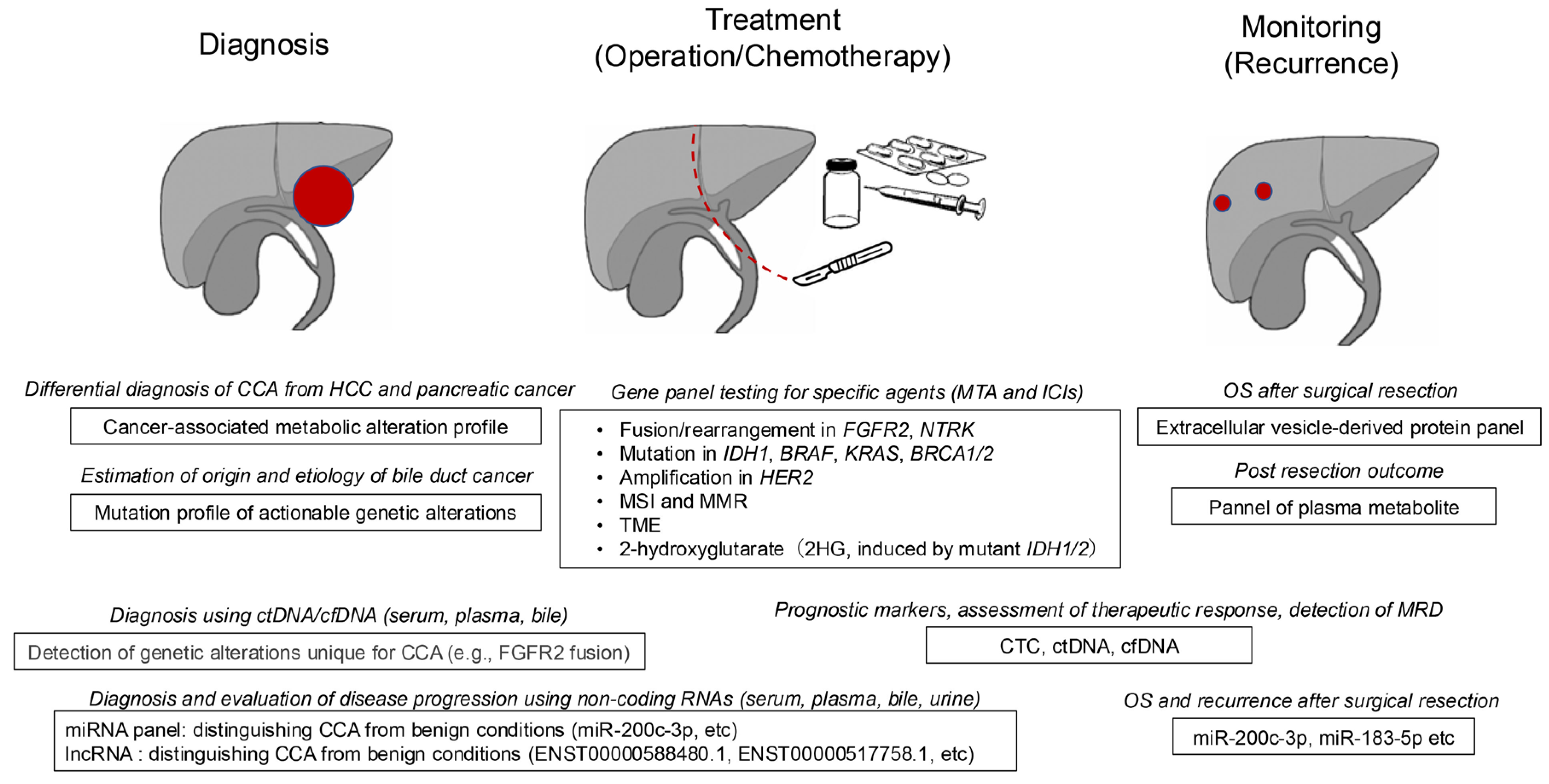
Figure 2.
Development of non-coding RNA as biomarkers for cholangiocarcinoma. Non-coding RNAs (ncRNAs) are functional RNAs that are not translated into proteins. Among the various types of ncRNAs, the shortest are microRNAs (miRNAs), which are approximately 20–25 nucleotides in length. miRNAs function by binding to target mRNAs and inhibiting their translation. Primary miRNAs (pri-miRNAs) are processed through several sequential cleavage steps to produce mature miRNAs. In contrast, ncRNAs longer than 500 nucleotides are collectively referred to as long non-coding RNAs (lncRNAs). These include intronic, exonic, promoter-associated, and enhancer-associated lncRNAs, which are generated through transcription and alternative splicing. Similarly, circular RNAs (circRNAs) are predominantly derived from precursor mRNAs (pre-mRNAs) via alternative splicing. CircRNAs can be classified into exonic, exonic-intronic, and intronic circRNAs based on their composition. These non-coding RNAs are closely associated with the initiation, progression, and chemoresistance of cholangiocarcinoma (CCA) and hold promise as potential biomarkers for clinical applications.
Figure 2.
Development of non-coding RNA as biomarkers for cholangiocarcinoma. Non-coding RNAs (ncRNAs) are functional RNAs that are not translated into proteins. Among the various types of ncRNAs, the shortest are microRNAs (miRNAs), which are approximately 20–25 nucleotides in length. miRNAs function by binding to target mRNAs and inhibiting their translation. Primary miRNAs (pri-miRNAs) are processed through several sequential cleavage steps to produce mature miRNAs. In contrast, ncRNAs longer than 500 nucleotides are collectively referred to as long non-coding RNAs (lncRNAs). These include intronic, exonic, promoter-associated, and enhancer-associated lncRNAs, which are generated through transcription and alternative splicing. Similarly, circular RNAs (circRNAs) are predominantly derived from precursor mRNAs (pre-mRNAs) via alternative splicing. CircRNAs can be classified into exonic, exonic-intronic, and intronic circRNAs based on their composition. These non-coding RNAs are closely associated with the initiation, progression, and chemoresistance of cholangiocarcinoma (CCA) and hold promise as potential biomarkers for clinical applications.
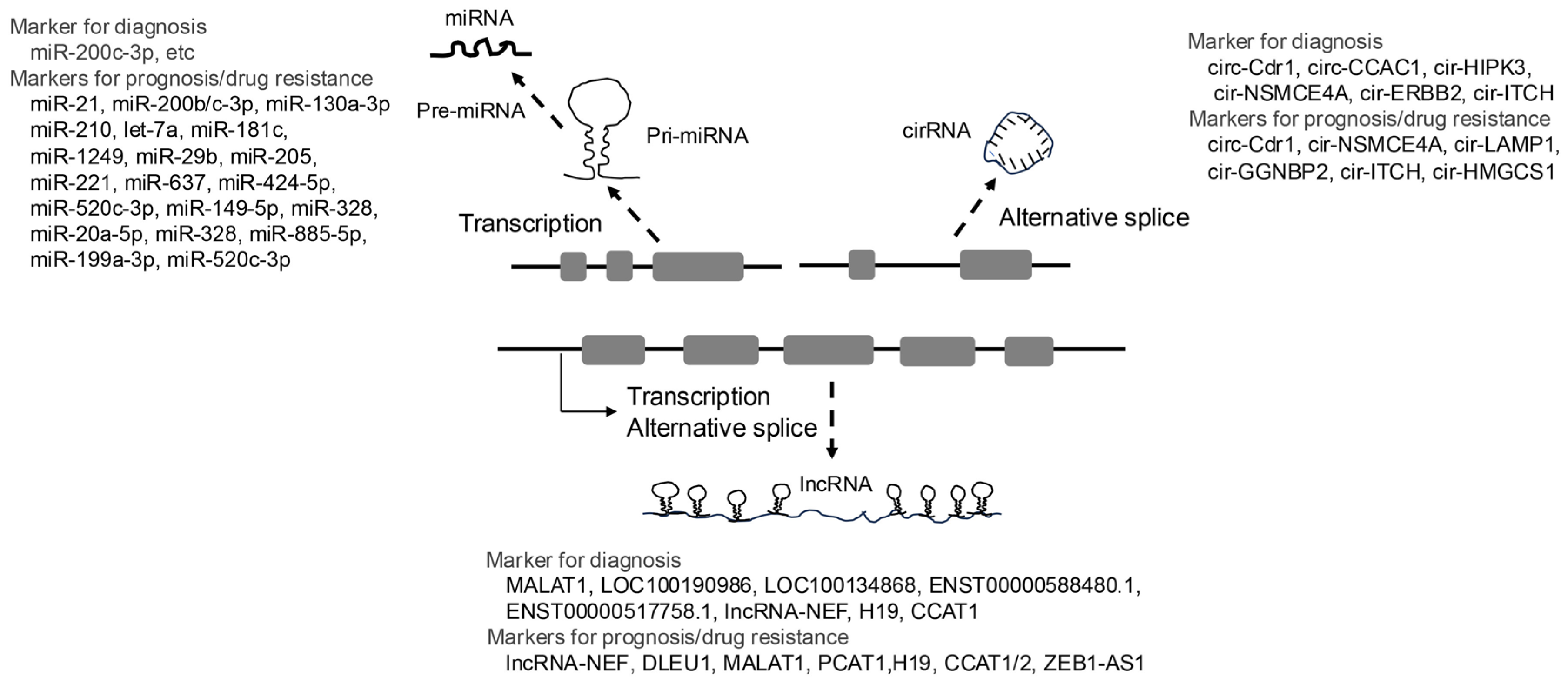
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



