
Submitted:
21 January 2025
Posted:
22 January 2025
You are already at the latest version
Abstract
Background: A circulating Vaccine-Derived Poliovirus Type 2 (cVDPV2) was isolated in environmental samples collected at the Mabella Sawmill Bridge environmental surveillance site in March 2024. The Ministry of Health and its partners responded to the outbreak by conducting a novel oral poliovirus vaccine type 2 (nOPV2) nationwide vaccination campaign among children aged 0-59 months. This study explores Sierra Leone's experience in terms of gaps identified, successes, and outcomes of the campaigns.
Methods: The study employed a descriptive secondary data analysis of the nOPV2 campaign, administrative, and Lot Quality Assessment Survey (LQAS) data collected during the first round of the nOPV2 campaign in Sierra Leone in May 2024. Administrative data was extracted from the national nOPV2 campaign database, while the LQAS data were requested from the WHO server. Stata version 18 and Power BI were used to analyse the administrative and LQAS data.
Results: 1,590,769 children aged 0-59 months were vaccinated against the polio virus in Sierra Leone. The Supplementary Immunization Activity (SIA) coverage for the nOPV vaccination in Sierra Leone was 100% for the first round of the campaign. Also, of the sixteen districts selected for the LQAS survey, twelve districts 75% passed the survey, and four districts 25% failed the LQAS.
Conclusion: The first round of the nOPV2 vaccination campaign in Sierra Leone demonstrated significant success in reaching the majority of the target population, with robust preparatory and implementation strategies contributing to this achievement.
Keywords:
Poliovirus
; children
; vaccination
; coverage
; lot quality assurance survey
1. Introduction
Circulating Vaccine-derived polioviruses Type 2 (cVDPV2) can arise from Sabin strain poliovirus serotypes 1, 2, and 3 found in the oral poliovirus vaccine (OPV) after extended person-to-person transmission [1]. When population vaccination immunity against polioviruses is suboptimal, sustained transmission can result in viral genetic changes that trigger a reversion to neurovirulence and clinical disease identical to that caused by wild poliovirus [2]. Vaccine-derived polioviruses (VDPCs) are divided into multiple categories: The viruses are first classified as cVDPVs when community circulation is confirmed (i.e., an outbreak) [3]. They are also called immunodeficiency-associated (iVDPVs) if isolated from individuals with primary immunodeficiency [4]. Lastly, ambiguous (aVDPVs) is a classification of exclusion when not associated with immune deficiency or community circulation when detected through Acute Flaccid Paralysis (AFP) or Environmental Surveillance (ES) [5].
Environmental surveillance in Jigawa State, Nigeria, first detected a single cVDPV2 emergence (named JIS-1) in January 2018. During the reporting period, the strain was later found in 12 other states in Nigeria and abroad [6]. The first half of 2019 saw the discovery of isolates genetically connected to JIS-1 from environmental surveillance samples and AFP cases, first in Niger and then in Benin, Cameroon, and Ghana [7].
In 2020, about 27 countries worldwide reported 959 human cases of cVDPV2 and 411 cVDPV2-positive environmental samples; 21 of these countries were in Africa, and the remaining six were in the Eastern Mediterranean, European Union, and Western Pacific regions [8]. Compared to 2019, when 366 cVDPV2 cases and 173 cVDPV2-positive environmental samples were recorded, there were more cVDPV2 cases and environmental samples in 2020 [9]. Since 2017, numerous genetically different cVDPV2 outbreaks have been reported in multiple African countries [10,11]. The current epidemic of cVDPV2 affects about twenty-one countries: Angola, Benin, Burkina Faso, Cameroon, Central African Republic, Chad, Côte d'Ivoire, Democratic Republic of the Congo, Ethiopia, Ghana, Guinea, Kenya, Liberia, Mali, Niger, Nigeria, Republic of Congo, Senegal, Sierra Leone, South Sudan, and Togo. Outbreak response activities are being carried out in these countries [9]. In March 2024, Sierra Leone confirmed the presence of a poliovirus variant 3 in the Kambia District and a type two variant in sewage near the Mabella sawmill bridge in the Western Area Urban District [12].
In response to the latest cVDPV outbreak, which started on the 10th of March 2024, a national novel Oral Polio Vaccine (nOPV) campaign planned in the 16 districts to be synchronized with five countries in the West African subregion (Cote d’Ivoire, Guinea, Liberia, Burkina Faso, and Mali). The first round was conducted from the 10th – 13th May 2024.
The Expanded Program on Immunization (EPI) of the Ministry of Health carried out several additional vaccination campaigns in the wake of the nOPV synchronized mass vaccination campaign. Measles, COVID-19, Human Papilloma Virus (HPV), and malaria vaccine introduction were among the immunization campaigns carried out before the response to the cVDPV outbreak.
The documented evidence of the success of immunization activity in the face of many other immunization efforts in Sierra Leone is scanty. Also, there is an absence of research that evaluates the quality of administrative data on polio vaccination against the Lot Quality Assurance Sampling (LQAS) performance tool, as well as community acceptance of the nOPV campaign and cross-border vaccination coverage. Thus, such information is important to evaluate the success of large-scale nOPV campaign activity in Sierra Leone.
Therefore, our study generally looked at the success of such activity in the face of many other immunization efforts by the Ministry of Health. Specifically, the study assessed the quality of administrative data against the LQAS performance, the community acceptance of the nOPV campaign, cross-border vaccination coverage, and the quality of supervision of the campaign.
2. Materials and Methods
Study Setting and Population: Sierra Leone is a country located in West Africa, with a population of over 8 million people [13]. There are 328,710 surviving infants. The country confirmed the cVDPV2 isolation through environmental surveillance on January 8, 2024 [14]. An Environmental Sample (ES) was collected in one of the five ES sites in Sawmill Bridge, Mabella, Freetown. The laboratory result was received on March 8, 2024, which was positive, virus type 2, EPID No, ENV-SIL-WEA-WAU-MSB-MSB-24-001. These isolates were genetically linked to an outbreak in Nigeria. The outbreak was reported to WHO, HG, on March 9, 2024. It was declared a National Public Health Emergency on the 22nd May 2024. The Ministry of Health conducted the first nationwide supplementary immunization activity with nOPV2 in May 2024 to reach eligible children with two doses, targeting 1,584,140 children aged 0-59 months.
Study Design: This study employs descriptive secondary data analysis of the nationwide novel Oral Poliovirus (nOPV) vaccination campaign conducted in response to the 2024 cVDPV2 outbreak in Sierra Leone.
2.1. Pre-Campaign Activities
Coordination of the response: The country declared the cVDPV2 outbreak in March 2024. The Ministry of Health, in collaboration with its partners, set up an emergency operation centre (EOC) to guide and coordinate the response. The EOC formed different response pillars, including surveillance, risk communication, case management, contact tracing, and vaccine pillars. The vaccine pillar was assigned to the EPI program, which planned and coordinated the nOPV2 campaign in collaboration with its partners. The vaccination pillar formed six technical working groups: Leadership, Coordination and Finance, Vaccine Logistics and Supply Chain, Service Delivery Training and Human Resources, Monitoring and Evaluation, Advocacy Communication and Social Mobilization, and Vaccine Safety Surveillance. All pillars had their separate meeting, planning, and reporting to the Incident Manager at the EOC daily.
Readiness Assessment: To assess the national program and district readiness for the campaign, there were five rounds of readiness assessment conducted at both national and district levels. The country reviewed the WHO readiness assessment tool and adapted it to the country’s context.
Training: Training materials were developed for training healthcare workers under six topics. The included Polio epidemiology, nOPV2 vaccine characteristics, management and Supply chain, Vaccination Strategy and administration, Roles and Responsibilities of supervisors, Performance Monitoring, Risk Communication, Social Mobilization, and Vaccine Safety Surveillance. The training was conducted at different levels, starting with National Training of Trainers (nTOT), District and chiefdom supervisors training, and vaccinators training. One week of integrated training was conducted for implementation, with two days each for national, district, and chiefdom supervisors and one day for vaccinators.
Advocacy Communication and Social Mobilization: To minimize vaccine hesitancy and missed opportunities, robust community and stakeholder engagement meetings were held across all districts. Different media platforms, including radio, TV spots, and social media, were used to sensitize caregivers and create demand for the campaign. Rapid Refusal Resolution Teams (RRRT) were set up in all districts to promptly respond to all refusal cases. Members of the RRTs were drawn from key influencer people within the community.
Vaccination Teams: 4,043 vaccination teams were allocated to all 16 districts based on the approved budget, geography, and special population of the districts (special team) by the EPI program. The training was conducted for all staff and partners deployed for implementing and supervising the nOPV round one activity, including vaccinators, vaccine accountability monitors, and supervisors. A total of 9,102 Vaccinators & Mobilizers, 356 Team supervisors, 230 Chiefdom supervisors, 160 District supervisors, 84 National supervisors and 10 Regional supervisors. The trainings were conducted at national, district, and chiefdom levels.
A total of 80 independent Monitors and 20 LQAS surveyors were also trained to validate the campaign. The teams were allocated to the district and then to health facilities within their districts. Each vaccination team comprised a vaccinator, a recorder, and a social mobilizer. At least two teams were allocated to every health facility. Each vaccination team had a daily target of 100 for rural and 150 for urban.
2.2. Intra-Campaign Activities
Vaccine Management: The nOPV2 vaccine was distributed to all health facilities based on their target population identified in the health facility micro plan. Before the implementation, a cold chain assessment was done to determine the gaps in the CCE requirements. Health facilities without functional CCEs were supplied with vaccine cold boxes lined with adequately conditioned ice packs during the campaign. On the field, every team was assigned a vaccine carrier lined with coolant packs to keep the vaccine in the correct temperature range (+2 to +8 0C). Because of the dangers associated with the use of the nOPV2 vaccine in the environment, Vaccine Accountability Monitors were recruited to ensure every vaccine vail was accounted for.
Vaccination Strategy and Administration: The campaign was conducted across the 16 districts, delivering vaccines to eligible children and communities using House-to-House, Fixed, and Transit vaccination strategies. While most eligible children were vaccinated in the households by the house-to-house teams, special or transit teams were assigned to border crossing points, lorry parks, marketplaces, places of worship, schools, etc., to ensure that children who were missed in the households were vaccinated. At the same time, fixed teams were assigned to the health facilities to vaccinate eligible children who would visit the health facilities for other interventions during the campaign period. Supervisors were allocated to monitor the day-to-day vaccination processes—four teams to a supervisor in rural areas and five teams to a supervisor in urban settlements. National, regional, district, chiefdoms, and team supervisors were deployed to monitor the vaccination exercise. Four days of supervision were conducted to monitor the implementation across all districts. Also, daily debriefings were conducted in all districts either at 7 am – 9 am or evening from 4:30 pm to 7 pm. The meeting provides a platform for supervisors to discuss issues of the day and make action points with the responsible person to act on them before the next day's work. This serves as a corrective means of the problem faced in the field while supervising the implementation so that the intended goal is met by all districts. The national debriefing meeting starts at 8 pm, where regional, national, and districts give updates from their district to the EPI program. To discuss the day's activity implementation, make action points or recommendations for the next day. A National situation room was formed to support and coordinate the activities at the national level. Head of units were drawn to constitute the situation room.
Data collection and reporting: During the nOPV2 campaign, administrative data were collected at different levels. The Monitoring and Evaluation (M&E), Technical Working Group (TWG), in collaboration with Global Polio Eradication Initiative (GPEI) partners, designed and pre-tested the data collection and reporting tools. At the vaccination team level, vaccinators used tally sheets to record the number of children vaccinated for the day.
Administrative data was collected using tally sheets and an electronic-based (Open Digital Kit (ODK) to record the number of children vaccinated each day. The tally sheets consist of the number of children who received the nOPV in each age category, both zero dose and one or more doses, refusals and revisits were used during the implementation phase. Thus, administrative coverages were available day by day. Aggregated vaccination data is summarized by the team supervisors in the daily team vaccination summary sheet and submitted to the chiefdom supervisor. The chiefdom supervisors summarized the summaries from all health facilities within the chiefdom in the Daily Chiefdom Summary Form. The chiefdom supervisors submitted the daily summary form to the district Monitoring and Evaluation Officer, who summarized the data by chiefdoms in the district Excel-linked file. The Excel-linked file was uploaded to Google Drive so that the national M&E team and partners could access the data as they were entered at the district levels. The linked file had a summary sheet and data analysis sheet used at the national level to inform decision-making.
Supportive Supervision: Supportive Supervision exercises were conducted at all implementation levels during the campaign. At the team and health facility levels, one team supervisor was assigned to five teams. At the chiefdom level, each chiefdom had at least one chiefdom supervisor who supported all health facilities within his or her chiefdom. In addition to the district-level supervisors, there were three national supervisors assigned to each district. A supportive supervision checklist was developed by the World Health Organization, which was uploaded to ODK for data collection. All supervisors used the ODK mobile app to collect data during the campaign.
2.3. Post-Campaign Activities
Post-vaccination assessment monitoring was done using the clustered-LQAS campaign evaluation; the survey was conducted two days after the nOPV2 campaign. All 16 districts were selected. In each district, we randomly selected six chiefdoms and a community (village or neighbourhood) in each chiefdom. In each community, ten children were surveyed (one per household). Next, the first household was randomly selected in the cluster according to existing geographical landmarks: the locality map was drafted, divided into smaller sectors according to existing landmarks (streets, playgrounds, rivers, etc.), and randomly selected one industry where the most central household was chosen to start the survey [15]. In the selected household, caregivers were interviewed for the nOPV2 vaccination status of their children, and all eligible children were selected. Children were checked for finger markings and household markings.
2.4. Lot Quality Assurance Survey
Definition: For the clustered LQAS survey, health districts in Sierra Leone were defined as ‘lots.’ Also, an individual vaccinated against polio is defined as a child between 0 and 59 months presenting an indelible ink mark on the fingernail at the time of nOPV vaccination.
Since our objective was a clustered LQAS for the nOPV vaccination, a two-day survey was implemented after the mopping up and the last day of the campaign was confirmed. For the nOPV antigen, 60 eligible individuals were interviewed per lot (district) for vaccination status, each lot was divided into six clusters of 10. In each district, six chiefdoms were randomly selected. Communities (villages or neighbourhoods) were randomly selected in each chiefdom. In each community, 10 (one per household) children were surveyed.
Next, the first household in the cluster was randomly selected according to geographic random sampling: a map of the locality was drafted and divided into four smaller units according to existing landmarks (streets, rivers, etc.) and randomly selected one sector which is the most central household to start the survey [16]. Also, during the campaign, independent monitors were employed to ascertain the quality of administrative data and ensure children missed during the campaign were vaccinated, especially in areas vaccinators have covered. The independent monitors were instructed to participate in the daily vaccination campaign debriefing meetings at the district level and discuss daily findings with health officers and supervisors. The purpose of these meetings was to interpret all information from the field to guide supervisors and strengthen areas of attention.
2.5. Planning the Clustered LQAS Surveys in the Field
The LQAS surveying team planned the nOPV post-vaccination campaign evaluation in collaboration with the Expanded Program on Immunization-Ministry of Health and the World Health Organization. The campaign implementation team was fully aware of the purpose of the LQAS surveys. Independent surveyors were sent across all the selected 16 districts after the nOPV vaccination exercise to evaluate the quality of the administration data reported during the campaign.
Definition of key variables: The following operational definitions were used
ZD: Zero-dose children were defined as those children aged between 0-59 months at the time of the survey who had not received any dose of the novel oral polio vaccine.
Vaccination Indicators: < 4 children missed during the nOPV campaign are characterized as high Supplementary Immunization Activity (SIA) performance, and no action is required as districts in this category are considered to have achieved high-quality campaign performance, and ≥four children missed were categorised as suboptimal SIA performance.
2.6. Data Analysis
The administrative data were analysed using STATA version 18 and Power-Bi software, and statistical calculation for the clustered LQAS data was analysed using Excel. We entered the campaign data and analysed it with Excel. To take corrective action based on objective information, during the campaign, any individual not presenting proof of vaccination is considered unvaccinated, i.e., those without finger markings. Also, children in streets and schools were not sampled during LQAS activity. The impact of the measures taken following the outcomes of the clustered LQAS on nOPV administrative coverage was analyzed. Districts' nOPV administrative data with LQAS findings were compared. The community acceptance of the nOPV campaign, cross-border vaccination coverage, and the quality of supervision of the campaign. Data were represented on graphs and tables.
3. Results
3.1. Demographic Data on the nOPV Vaccination Campaign
The nOPV round 1 vaccination campaign targeted 1,584,140 children across the country. The campaign reached 1,590,769 (100%) of the targeted children in Sierra Leone. The majority, 77.74% (1,236,631), were children aged 12-59 months, and 354,138 (22.26%) were children aged 0- 11 months, respectively. As shown in Table 1.
3.2. Administrative Data on the nOPV Vaccination Campaign by Districts
Thirteen of the sixteen districts achieved a vaccination coverage of ≥95% for administration rates. Districts such as Koinadugu 129%, Falaba 117%, Kailahun 109.1%, Bonthe 105%, Port Loko 103.6%, Pujehun 102.3%, Moyamba 101.5%, Bombali 100.6%, Kono 100.3%, Karene 98.5%, Kenema 96.9%, Western Area Rural 95% and Tonkolili 94.7%. Furthermore, low coverage <95% is seen in Western Area Urban 92.9%, Kambia 75.3%, and Bo 75.3%, respectively. As illustrated Figure 1.
3.3. Cross-Border nOPV Vaccination Coverage
A total of 3,589 children were vaccinated across border districts in Sierra Leone: 2.30% of children aged 0-59 months were vaccinated in Karene, 1.96% () were vaccinated in Kambia, 0.32% in Falaba, 0.21% in Kailahun, 0.19% in Kenema, 0.10% in Pujehun, 0.07% in Kono and 0.05 % in Koinadugu respectively. As illustrated in Figure 2..
3.4. Evaluation of the nOPV2 Campaign Through the Lot Quality Assurance Sampling (LQAS)
A total of 96 clusters across the 16 districts were sampled for the LQAS survey, of the sixteen districts selected, twelve districts 75% passed the survey with no missed children, whereas four districts 25% were rejected for low vaccination coverage by the LQAS rule due to exceeding the threshold of more than four (>4) unvaccinated children which shows a suboptimal performance in those lots. A total of 48 children were left unvaccinated, with the majority, 27 (56%) of the children not vaccinated because vaccination teams did not visit the house, 11 (23%) of the children vaccinated were not finger marked, and 10(21%) of the children were absent from home respectively. As shown in Figure 3.

Table 2.
Number of unvaccinated children by districts, Sierra Leone 2024.
|
Lot |
Clusters |
Number of unvaccinated children (n=48) |
|||
|---|---|---|---|---|---|
| House not visited | No finger marking | Child absent | N (%) |
||
| Bo | 6 | 1 | 0 | 0 | 1 (2%) |
| Bombali | 6 | 0 | 0 | 0 | - |
| Bonthe | 6 | 0 | 0 | 0 | - |
| Falaba | 6 | 0 | 0 | 0 | - |
| Kailahun | 6 | 0 | 0 | 0 | - |
| Kambia | 6 | 0 | 0 | 0 | - |
| Karene | 6 | 0 | 0 | 0 | - |
| Kenema | 6 | 0 | 0 | 0 | - |
| Koinadugu | 6 | 2 | 1 | 1 | 4 (8%) |
| Kono | 6 | 0 | 0 | 0 | - |
| Moyamba | 6 | 0 | 0 | 0 | - |
| Port Loko | 6 | 7 | 0 | 3 | 10 (21%) |
| Pujehun | 6 | 0 | 0 | 0 | - |
| Tonkolili | 6 | 0 | 1 | 0 | 1 (2%) |
| Western Area Rural | 6 | 7 | 2 | 1 | 10 (21%) |
| Western Area Urban | 6 | 10 | 7 | 5 | 22 (46%) |
3.5. LQAS Reasons for a Child Being Absent for Vaccination
Out of the ten children absent for the nOPV vaccination reported by the Lot Quality Assessment Survey, 3 (30%) of the children were absent because they were taken to the farm by their caregivers, 2 (20%) were taken to the market, 2 (20%) travelled with their parents, 2 (20%) of the children went to the playground, and 1 (10%) were based on other activities embarked by their caregivers. As shown in Figure 4.
3.6. Community Awareness and Acceptance of the nOPV Vaccination Campaign
3.7. Number of Children Still Missed After Revisit
One hundred thirteen children were missed for the nOPV vaccination during the first round. Of the 113 children missed, 48 were in Kambia district, 18 in Falaba, 16 in Kailahun, 7 in Koinadugu, 7 in Port Loko, 5 in Moyamba, and 2 in Western Urban Area. Furthermore, no missed child is seen in districts like Bo, Bombali, Karene, Kenema, Kono, Pujehun, Tonkolili, and Western Area Rural, as shown in Figure 7.
4. Discussions
The outcome of the first round of the nOPV vaccination campaign in Sierra Leone demonstrates a major success in the quest to vaccinate children against the polio virus. The campaign effectively exceeds the target for eligible children receiving the polio vaccine. These findings are inconsistent with those in Cameroon and India [3,7]. This shows the effectiveness of the vaccination strategies used in reaching eligible children during the campaign. In a bid to achieve higher coverage and leave no child behind, the Expanded Programme on Immunization employed strategies like robust pre-vaccination readiness assessments across all districts with continuous media and community engagements. The house-to-house and mobile or fixed or transit vaccination strategies prove pivotal in reaching more children. Also, incorporating cross-border vaccination strategies across all border districts influenced the number of children reached during the campaign.
4.1. Quality of Administrative Data Against the LQAS Performance
After the first round of the nOPV2 campaign, an LQAS survey was done to assess vaccination coverage in sixteen districts, which were purposely selected to ascertain the quality of administrative data reported nationwide. The number of districts having high vaccination coverage of ≥95% reported for the administrative data for the nOPV campaign was thirteen out of the sixteen districts, which represents 81.25% of the districts that achieved the set vaccination coverage target. These findings are consistent with studies done in Nepal, Nigeria, and Indonesia [8,9,10]. Furthermore, the LQAS findings revealed that out of the thirteen districts with high vaccination coverage, four of those districts exceeded the threshold of more than four unvaccinated children and did not pass the LQAS, districts such as Port Loko, Tonkolili, Western Area Rural, and Western Area Urban. These findings show some discrepancies with the nOPV administrative data with districts identified with high vaccination coverage during the first round of the campaign this is because most of these districts engage in economic activities that involve the movement of people, which can facilitate the movement of unvaccinated children by their parents and hence can negatively impact the outcome of the LQAS findings in these districts. Western Area Rural and Port Loko indicate a very poor SIA performance, and hence, those districts should conduct a comprehensive mopping up in the entire district within one week after the LQAS has been completed. Also, Bo and Tonkolili districts show high SIA performance, which required no action to be taken, these findings are consistent with the administrative data reported for these districts. Moreover, districts like Koinadugu show moderate SIA performance, which needs quality improvement in subsequent campaigns [19]. Furthermore, the LQAS results revealed that most of the children were missed because their caregivers carried them along to their farms and market, some travelled with parents to other destinations, causing their absence, and some of the children were on the playground during the house-to-house vaccination session that caused missing out from the vaccination. Our findings are similar to a study done in numerous countries, including Pakistan and also Nigeria [12,13,14]. Out of the six districts selected for the LQAS assessment, the campaign achieved a 60% pass mark, which shows a higher quality in the SIA vaccination result and represents the true nature of the vaccination coverage achieved in each district during the campaign. These findings are consistent with findings from Nigeria [21].
4.2. The Community Awareness and Acceptance of the nOPV Campaign
Nationally, more than three-fourths of caregivers were aware of the nOPV2 vaccination campaign before the implementation. This was achieved following the pre-vaccination strategies adopted by the Expanded Programme on Immunization, which involves conducting periodic readiness assessments, 8 weeks, 6 weeks, 4 weeks, 2 weeks, and 1 week. The national nOPV vaccination readiness assessment findings revealed that caregivers in Western Area Urban and Rural show low awareness of the nOPV campaign, which is contrary to studies done in Ethiopia and Pakistan [16,17]. This disparity occurred because in urban areas, a misleading impression of protection could make people less interested in vaccination programs, and emphasis on other health problems could make people forget about the nOPV campaign [23]. Healthcare providers may give priority to rural areas if they believe urban areas are already adequately covered, and they may disregard important indicators due to the overabundance of information in cities. In rural locations, stronger community links and more direct communication can also lead to better awareness, hence reducing the amount of information about the campaign in cities. Overall, 113 children in Sierra Leone were missed from taking the nOPV vaccination during the first round after revisits were made, similar to a study done in Pakistan and Nigeria [18,19]. Kambia district has the highest number of missed children after revisits, followed by Falaba, Kailahun, Koinadugu, and Port Loko. The higher refusal rate shown by these districts depicts low acceptance of the nOPV vaccine. Despite the high awareness of the nOPV vaccination campaign in these districts, refusal rates are stubbornly high, inconsistent with findings from Pakistan [24], a phenomenon puzzling to public health providers. This discrepancy suggests deeper-rooted factors beyond mere lack of knowledge. It’s likely a combination of historical mistrust, cultural beliefs, and practical access barriers are at play.
4.3. Cross-Border nOPV Vaccination Coverage
Effective cross-border vaccination coverage with the nOPV2 vaccine was implemented to reach more eligible children, especially children travelling in and out of the country, this is important for achieving global polio eradication goals. During the nOPV2 cross-border vaccination campaign, a total number of 3,589 children were vaccinated in cross-border districts, constituting a vaccination coverage of 0.21%. High cross-border vaccination coverage is seen in Karene and Kambia districts with the novel Oral Polio Vaccine (nOPV) due to their location along the Guinea border, which experiences significant cross-border movement. Our findings are similar to a study in China [26]. This necessitates focused vaccination efforts to prevent polio spread. Targeted campaigns, collaboration with Guinea, strong community engagement, and enhanced surveillance in these regions contribute to higher vaccination coverage. This strategic vaccination strategy acts as a preventive shield, preventing the virus from gaining a foothold in previously polio-free areas, minimizing the likelihood of polio outbreaks, and ultimately contributing to the global eradication effort.
4.4. The Quality of the Round 1 nOPV Campaign Supervision in Sierra Leone
The quality of the nOPV campaign supervision in Sierra Leone hinges on numerous factors, such as timely reporting of vaccination data promoting data accuracy, completeness, and data integrity of nOPV2 vaccination data. Also, the campaign achieved high vaccination coverage, which was influenced by the strategic campaign implementation ranging from selecting competent health personnel, informed training, cold chain management, logistics, and supply chain efficiency, monitoring and surveillance systems, community engagement, and communication strategies, as well as examining the incidence of polio cases within the population. This concerted effort by the Ministry of Health, District Health Management Teams (DHMTs), and Partners. The strides made by the Expanded Programme on Immunization (EPI) in strengthening vaccination supervision in the country underscores the importance of quality, reliable, and accurate vaccination outcomes that reflect expected results. These strategies are consistent with the polio vaccine campaign strategies employed in Nigeria [27].
4.5. Study Limitations
The nationwide implementation of the polio campaign ensures the representativeness of data across all districts, thus increasing the study's findings' relevance to all Sierra Leonean children under five. However, the incomplete and inconsistent data reported by supervisors during the polio campaign created a huge gap in achieving high-quality supervision data. Also, in terms of the vaccination protocols, vaccination teams failed to document administrative data correctly as per the vaccination guidelines set for the campaign, this may result in incomplete, inaccurate, or inconsistent recording of administrative data, which has an impact on the LQAS. Similarly, the LQAS survey might not cover the full variability in vaccination coverage or the campaign implementation because only six clusters are selected in each district, which cannot substantiate the exact outcome of the polio campaign.
5. Conclusions
The first round of the nOPV vaccination campaign in Sierra Leone demonstrated significant success in reaching most of the target population, with robust preparatory and implementation strategies contributing to this achievement. However, gaps in coverage and challenges such as missed households and inadequate marking of vaccinated children highlight areas for improvement. Continuous monitoring, targeted interventions in low-coverage districts, and enhanced community engagement will be essential in achieving and sustaining high vaccination coverage in future campaign rounds.
Author Contributions
Conceptualization: DMK, ENS, AKK, SL, NCK, manuscript acquisition: ENS, DMK, AKK, SL, NCK, and HB; Methodology: DMK, ENS, AKK, SL, and NCK, formal analysis: SL, AKK, and ENS, writing review and editing: DMK, AKK, PBJ, AN, AC, ENS, HB, JMK, EGS, MTMK, and TS; Visualization, DMK, AKK, SL, HB, and ENS. All authors have read and agreed to the published version of the manuscript. All authors agree to be accountable for all aspects of the work in this article.
Funding
There was no funding for this project.
Institutional Review Board Statement
The study was not considered human subject research hence IRB is not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data underlying this article were provided by and are the property of the Ministry of Health of Sierra Leone. The data will be shared on reasonable request with the ministry's permission.
Acknowledgments
This study was conducted by the Expanded Programme on Immunization (EPI), Ministry of Health- Sierra Leone. The authors thank the healthcare workers, Independent Monitors, and LQAS surveyors in Sierra Leone. We are also grateful to our partners, UNICEF and WHO.
Conflicts of Interest
The authors declare that no competing interests exist.
References
- World Health Organization. Polio Global Eradication Initiative [Internet]. World Health Organization; [cited 2024 May 5]. Available from: http://polioeradication.org/.
- Badizadegan ND, Wassilak SGF, Estívariz CF, Wiesen E, Burns CC, Bolu O, et al. Increasing Population Immunity Prior to Globally-Coordinated Cessation of Bivalent Oral Poliovirus Vaccine (bOPV). Pathogens. 2024 Sep 17;13(9):804. [CrossRef]
- Aroop Mohanty, , Ranjana Rohilla, , Kamran Zaman et al. Vaccine Derived Poliovirus (VDPV). Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10241397/pdf/1124-9390_31_1_2023_174-185.pdf.
- Guo J, Bolivar-Wagers S, Srinivas N, Holubar M, Maldonado Y. Immunodeficiency-related vaccine-derived poliovirus (iVDPV) cases: A systematic review and implications for polio eradication. Vaccine. 2015 Mar;33(10):1235–42. [CrossRef]
- Alleman MM, Jorba J, Riziki Y, Henderson E, Mwehu A, Seakamela L, et al. Vaccine-derived poliovirus serotype 2 outbreaks and response in the Democratic Republic of the Congo, 2017–2021. Vaccine. 2023 Apr;41:A35–47. [CrossRef]
- Adamu US, Archer WR, Braka F, Damisa E, Siddique A, Baig S, et al. Progress Toward Poliomyelitis Eradication — Nigeria, January 2018–May 2019. MMWR Morb Mortal Wkly Rep. 2019 Jul 26;68(29):642–6. [CrossRef]
- Cooper LV, Erbeto TB, Danzomo AA, Abdullahi HW, Boateng K, Adamu US, et al. Effectiveness of poliovirus vaccines against circulating vaccine-derived type 2 poliomyelitis in Nigeria between 2017 and 2022: a case-control study. Lancet Infect Dis. 2024 Apr;24(4):427–36. [CrossRef]
- Itiakorit H, Sathyamoorthi A, O’Brien BE, Nguyen D. COVID-19 Impact on Disparity in Childhood Immunization in Low- and Middle-Income Countries Through the Lens of Historical Pandemics. Curr Trop Med Rep. 2022 Dec 19;9(4):225–33. [CrossRef]
- WHO, 2023 [Internet]. [cited 2024 May 23]. Available from: http://polioeradication.org/.
- Adesola RO, Idris I, Opuni E. Public health concerns surrounding the cVDPV2 outbreak in Africa: Strategies for prevention and control with a special focus on Nigeria. Health Sci Rep. 2023 May;6(5):e1269. [CrossRef]
- Morais A, Morais J, Felix M, Neto Z, Madaleno V, Umar AS, et al. Genetic and epidemiological description of an outbreak of circulating vaccine-derived polio-virus type 2 (cVDPV2) in Angola, 2019–2020. Vaccine. 2023 Apr;41:A48–57. [CrossRef]
- World Health Organization. Sierra Leone Confirms New Cases of Polio Variant, Implements Comprehensive Response Plan [Internet]. [cited 2024 Dec 12]. Available from: https://www.afro.who.int/countries/sierra-leone/news/sierra-leone-confirms-new-cases-polio-variant-implements-comprehensive-response-plan.
- Statistics Sierra Leone. 2015 Population and Housing Census [Internet]. 2015 [cited 2024 Jan 9]. Available from: https://www.statistics.sl/images/StatisticsSL/Documents/final-results_-2015_population_and_housing_census.pdf.
- World Health Organization. Sierra Leone concludes First Roind of a Nationwide Polio Vaccination. [cited 2024 Jun 7]; Available from: https://www.afro.who.int/countries/sierra-leone/news/sierra-leone-concludes-first-round-nationwide-polio-vaccination#:~:text=Freetown%2C%20Sierra%20Leone%2C%2022,Gavi%2C%20the%20Vaccine%20Alliance%20have.
- World Health Organization. Operational Manual On Lot Quality Assurance Sampling (LQAS) to assess nOPV2 Coverage May-June 2024 Sierra Leone [Internet]. [cited 2024 Nov 30]. Available from: file:///Users/user/Desktop/LQAS.%20Operational%20Manual%20revised_SAW%202.pdf.
- Global Polio Eradication Initiative. Assessing vaccination Coverage levels using clustered Lot Quality Assurance Sampling [Internet]. [cited 2024 Jan 9]. Available from: https://polioeradication.org/wp-content/uploads/2016/09/Assessing-Vaccination-Coverage-Levels-Using-Clustered-LQAS_Apr2012_EN.pdf.
- Russo G, Miglietta A, Pezzotti P, Biguioh RM, Bouting Mayaka G, Sobze MS, et al. Vaccine coverage and determinants of incomplete vaccination in children aged 12–23 months in Dschang, West Region, Cameroon: a cross-sectional survey during a polio outbreak. BMC Public Health. 2015 Dec;15(1):630.
- Wallace AS, Bohara R, Stewart S, Subedi G, Anand A, Burnett E, et al. Impact of an Intervention to Use a Measles, Rubella, and Polio Mass Vaccination Campaign to Strengthen Routine Immunization Services in Nepal. J Infect Dis. 2017 Jul 1;216(suppl_1):S280–6. [CrossRef]
- Brown AE, Okayasu H, Nzioki MM, Wadood MZ, Chabot-Couture G, Quddus A, et al. Lot Quality Assurance Sampling to Monitor Supplemental Immunization Activity Quality: An Essential Tool for Improving Performance in Polio Endemic Countries. J Infect Dis. 2014 Nov;210(suppl_1):S333–40. [CrossRef]
- Luman ET, Chu SY. When and Why Children Fall Behind with Vaccinations. Am J Prev Med. 2009 Feb;36(2):105–11. [CrossRef]
- Etsano A, Gunnala R, Shuaib F, Damisa E, Mkanda P, Banda R, et al. Progress Toward Poliomyelitis Eradication — Nigeria, January 2013–September 2014. 2014;63(46). [CrossRef]
- Asmare G, Madalicho M, Sorsa A. Disparities in full immunization coverage among urban and rural children aged 12-23 months in southwest Ethiopia: A comparative cross-sectional study. Hum Vaccines Immunother. 2022 Nov 30;18(6):2101316. [CrossRef]
- Ameyaw EK, Kareem YO, Ahinkorah BO, Seidu AA, Yaya S. Decomposing the rural–urban gap in factors associated with childhood immunisation in sub-Saharan Africa: evidence from surveys in 23 countries. BMJ Glob Health. 2021 Jan;6(1):e003773. [CrossRef]
- Khowaja A, Ali Khan S, Nizam N, Bin Omer S, Zaidi A. Parental perceptions surrounding polio and self-reported non-participation in polio supplementary immunization activities in Karachi, Pakistan: a mixed methods study. Bull World Health Organ. 2012 Nov 1;90(11):822–30. [CrossRef]
- Murakami H, Kobayashi M, Hachiya M, Khan ZS, Hassan SQ, Sakurada S. Refusal of oral polio vaccine in northwestern Pakistan: A qualitative and quantitative study. Vaccine. 2014 Mar;32(12):1382–7. [CrossRef]
- Wang HB, Zhang LF, Yu WZ, Wen N, Yan DM, Tang JJ, et al. Cross-border collaboration between China and Myanmar for emergency response to imported vaccine derived poliovirus case. BMC Infect Dis. 2015 Dec;15(1):18. [CrossRef]
- Upfill-Brown AM, Voorman A, Chabot-Couture G, Shuaib F, Lyons HM. Analysis of vaccination campaign effectiveness and population immunity to support and sustain polio elimination in Nigeria. BMC Med. 2016 Dec;14(1):60. [CrossRef]
Figure 1.
nOPV2 Vaccination coverage per district, Sierra Leone, 2024.
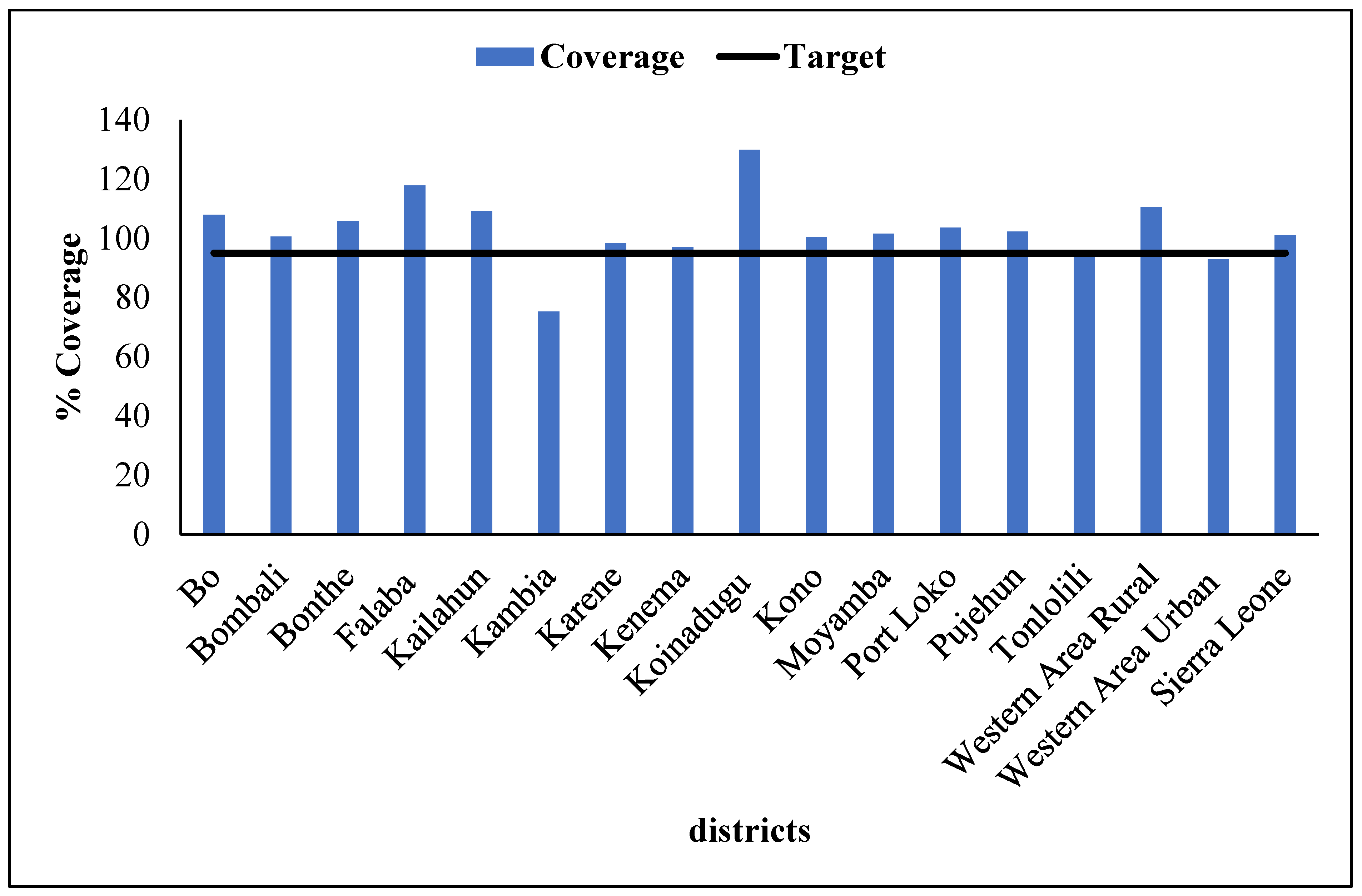
Figure 2.
Cross-border nOPV2 vaccination coverage, Sierra Leone 2024.
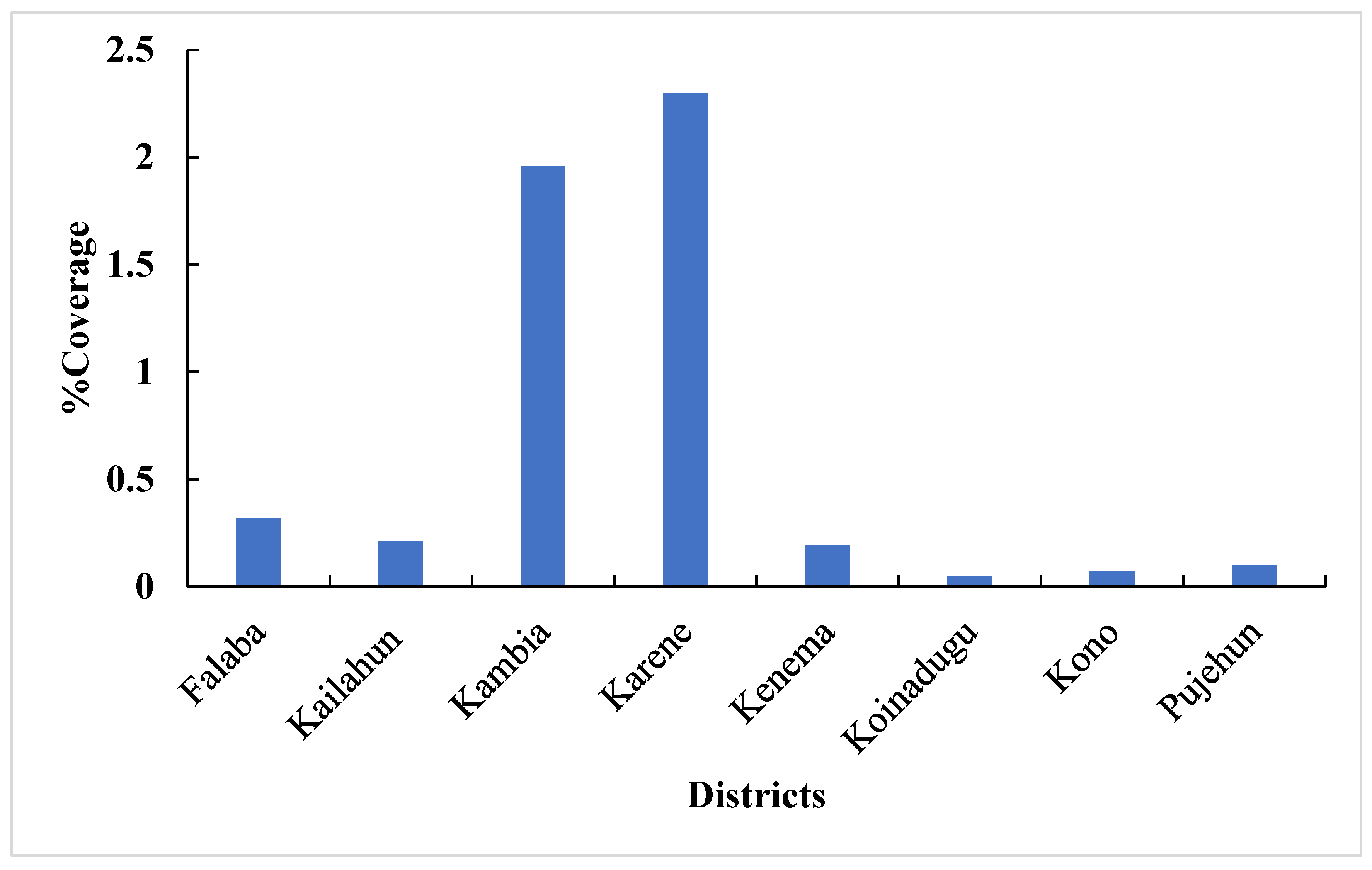
Figure 3.
Map of Sierra Leone showing districts where LQAS was conducted, May 2024.
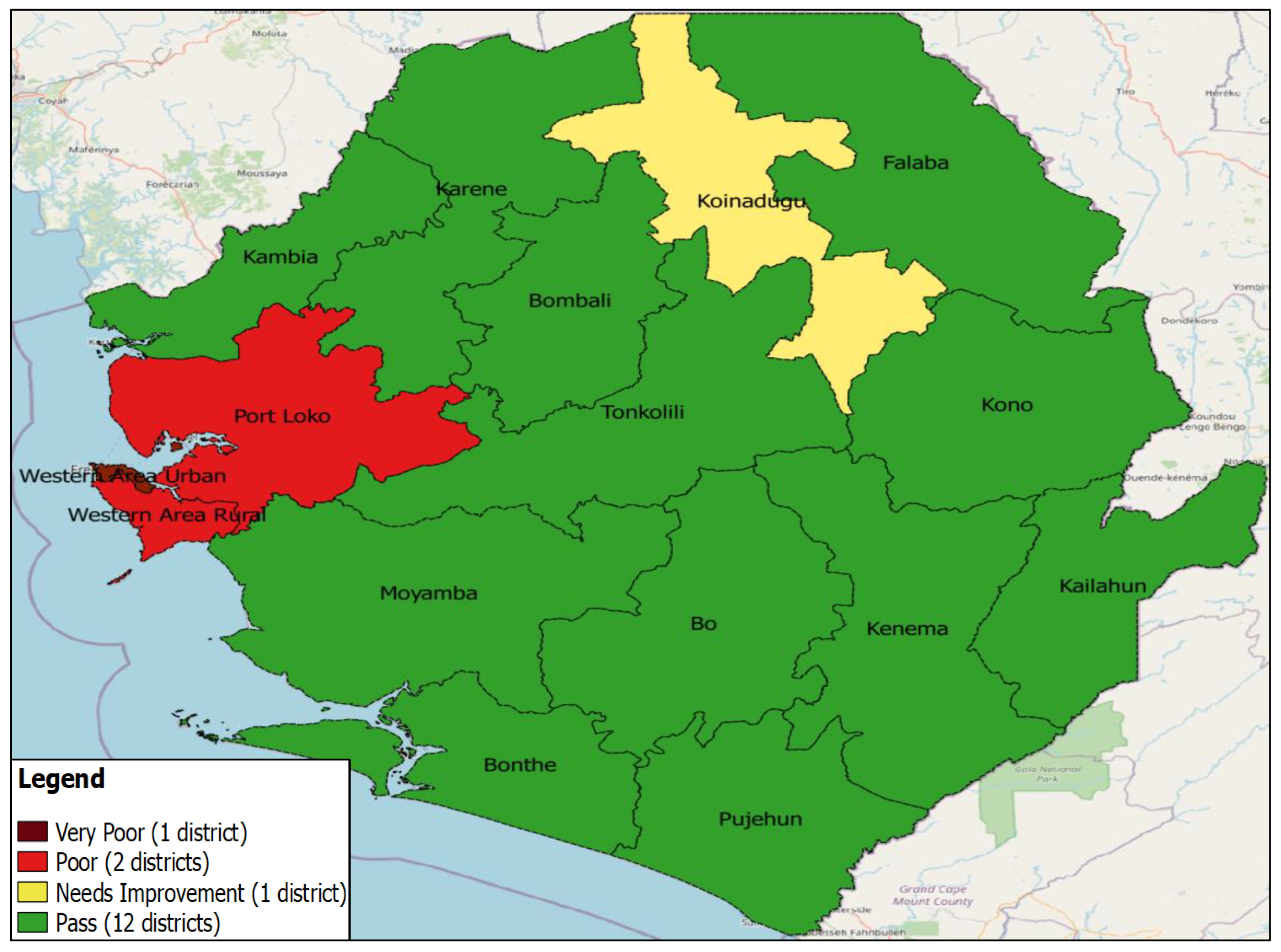
Figure 4.
Reasons for a child being absent for the nOPV vaccination, Sierra Leone 2024.
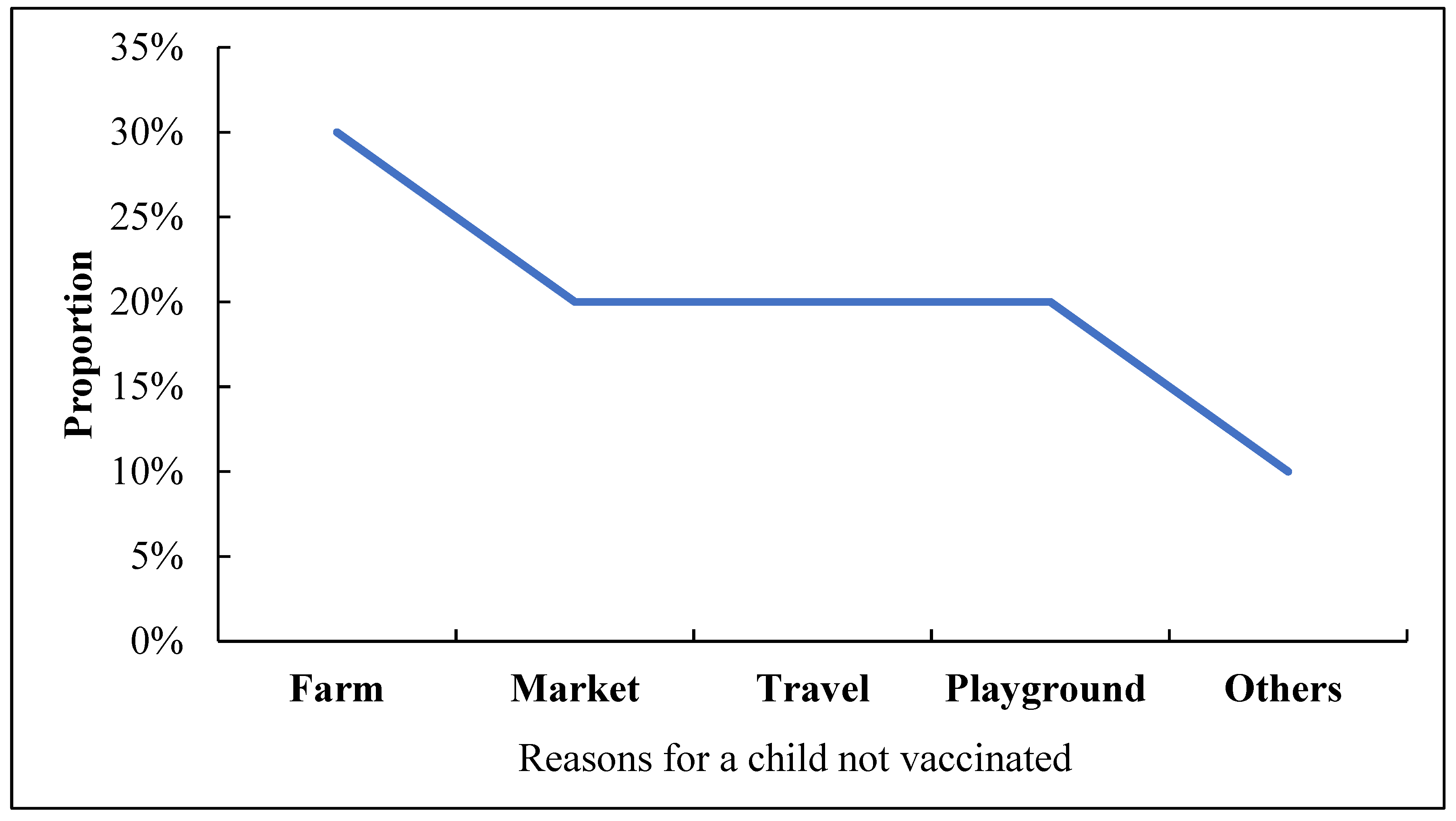
Figure 5.
The proportion of Caregivers informed about the nOPV campaign, Sierra Leone, 2024.
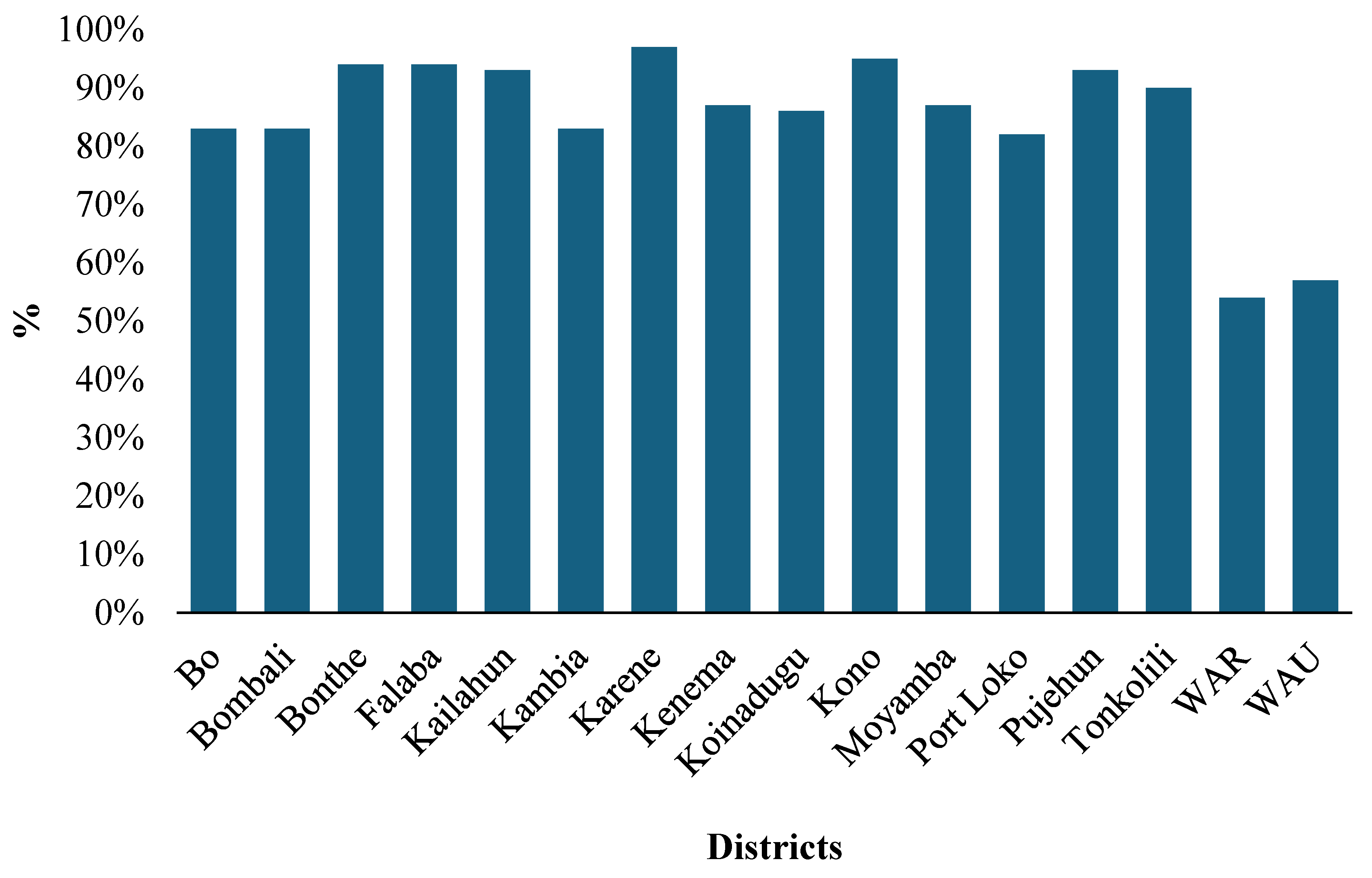
Figure 6.
National coverage of caregivers informed about the nOPV campaign, Sierra Leone, 2024.
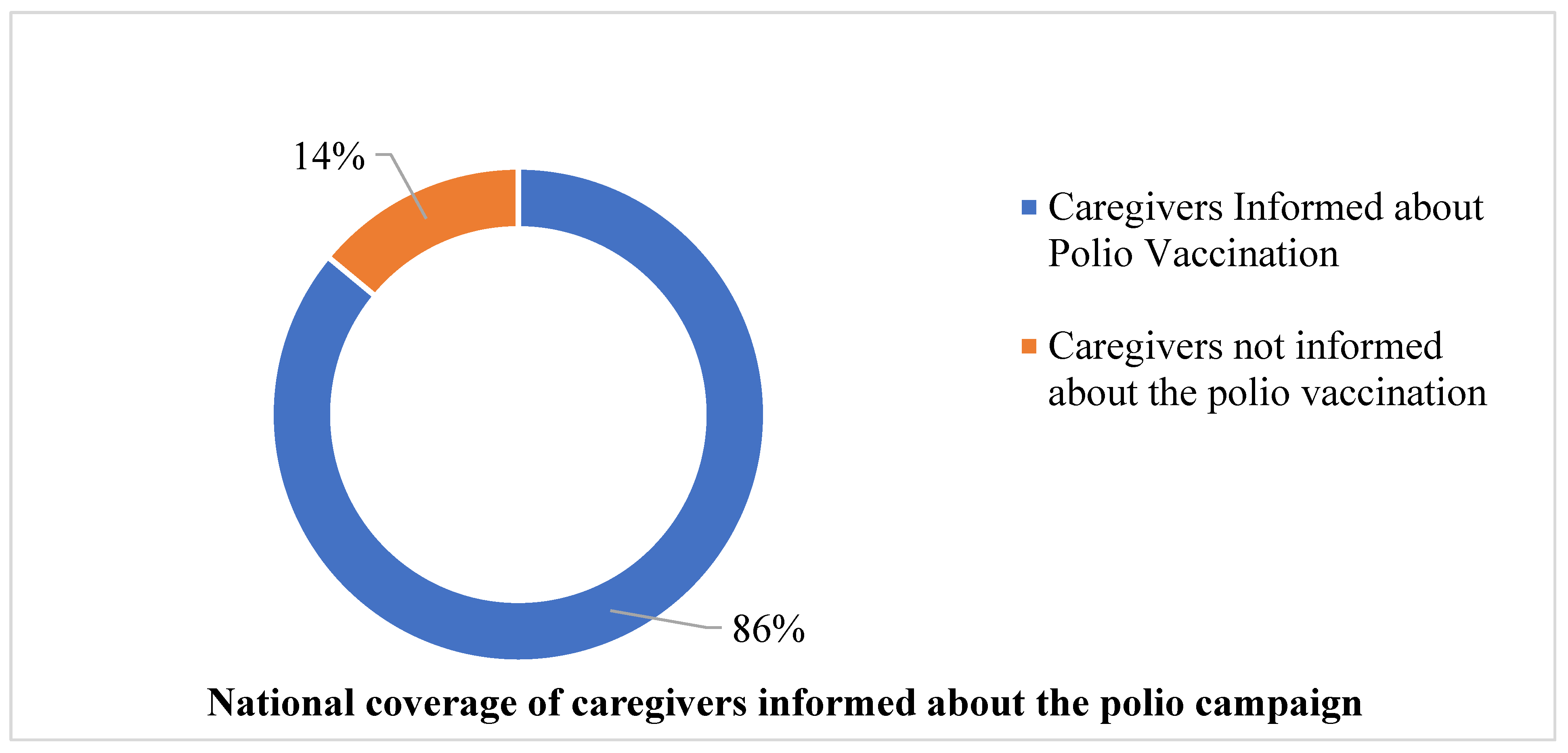
Figure 7.
Number of children missed after revisit, Sierra Leone, 2024.
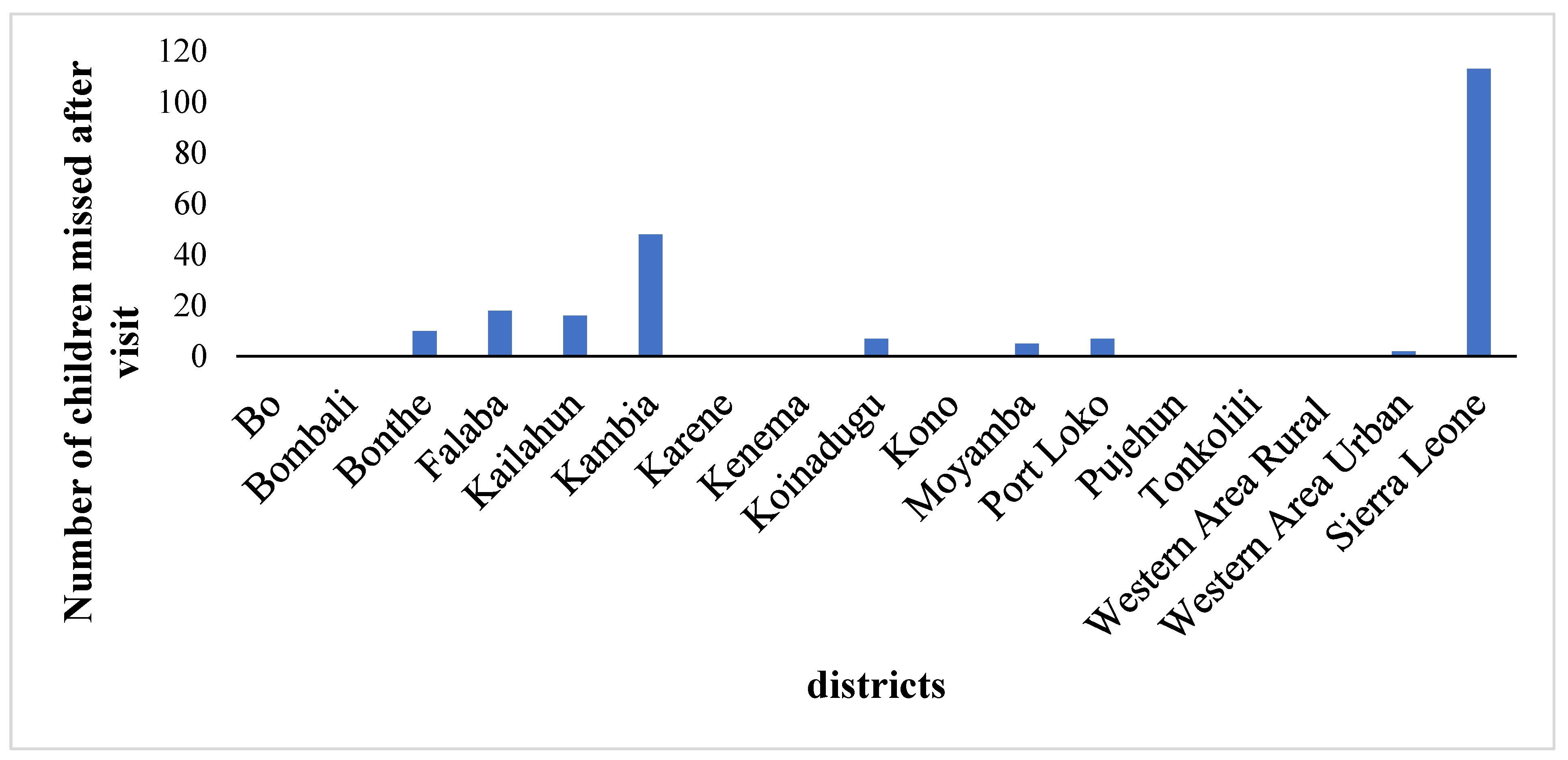
Table 1.
Age distribution of children vaccinated.
| Variable | Sub-variable | Frequency | Percent |
|---|---|---|---|
| Age (months) | 0-11 months | 354,138 | 22.26 |
| 12-59 months | 1,236,631 | 77.74 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



