
Submitted:
21 January 2025
Posted:
21 January 2025
You are already at the latest version
Abstract
Background: Freelance nurses (FNs) are independent healthcare professionals not tied to a specific healthcare facility. In Italy, FNs are relatively unknown to the public and many healthcare pro-fessionals, who traditionally view nurses as subordinate workers. This study aimed to validate the Job Satisfaction (JS)-Nursing Italian Score, a tool for assessing JS among nurses, and to compare JS levels between employed nurses and FNs. Methods: A two-phase study design was used: vali-dation and observational. In the validation phase, content validity was assessed using a content validity index, and reliability was evaluated with Cronbach’s alpha and McDonald’s omega. Construct validity was examined via exploratory factor analysis (EFA). In the observational phase, a cross-sectional analysis was conducted with 200 nurses assessing their JS using the JS-Nursing Italian Score. Multiple one-way Welch’s ANOVAs were performed to compare groups. Results: Cronbach’s alpha (α = 0.827) and McDonald’s omega (ω = 0.829) indicated good reliability. Bart-lett’s Sphericity test (p < 0.001) and the Kaiser-Meyer-Olkin measure (0.74) supported the EFA, revealing four factors. Significant differences in JS were found between groups through ANOVA. Conclusion: The JS-Nursing Italian Score is a reliable tool for assessing JS. FNs reported signifi-cantly higher satisfaction compared to employed nurses. Future research should focus on further validating the JS-Nursing Italian Score, expanding its use across diverse settings to enhance nursing well-being.
Keywords:
Freelance Nurses (FNs)
; Well-Being Health Workers
; Job Satisfaction (JS)
; Public Health
1. Introduction
In Italy, freelance nursing (FNs) is relatively unknown to the general population and even to many healthcare professionals, who have traditionally viewed nurses primarily as subordinate workers [1]. However, this perception is gradually shifting due to evolving healthcare needs and the growing recognition of the autonomy that freelancing can offer, supported by national regulations that extend economic protections [1,2]. According to data from the World Health Organization (WHO) and the National Institute of Statistics (ISTAT), the aging population and the rise in chronic diseases are steadily increasing [3,4].
This demographic trend implies a growing demand for community-based healthcare services, a need further emphasized by post-COVID-19 reforms aimed at implementing a One Health model [5,6]. In this context, FNs emerge as key professionals capable of providing personalized care focused on prevention, health education, and individual care, with services accessible at home [1,2]. Nursing is notoriously associated with high levels of stress and burnout due to complex work environments, irregular shifts, and heavy workloads. In Italy, this situation is further exacerbated by wages that are often disproportionate to the demands of the job [7,8,9,10,11,12].
These factors negatively impact nurses' mental and physical health, leading to reduced job satisfaction (JS) and a decline in the quality of care provided [13-20]. Freelancing can offer a potential solution to some of these issues, as greater autonomy and control over one's work can help reduce stress and burnout, thereby improving JS [21,22]. However, FNs also face significant challenges, such as economic insecurity and the need to manage administrative tasks independently [1,2,22,24]. Nurses' JS is influenced by multiple factors. Several studies have highlighted how work-related stress became particularly evident during the COVID-19 pandemic, which imposed extremely demanding and challenging working conditions [25-28].
In response to these pressures, the healthcare system had to adapt rapidly, revealing both the strengths and weaknesses of different nursing work modalities [25,26]. A key aspect that emerges from the comparison between employed nurses and FNs is the perception of autonomy and flexibility in their work [29]. FNs, who have the ability to directly manage their schedules and work methods, often report a greater sense of control and professional fulfillment. This increased autonomy can lead to reduced burnout and improved overall well-being [30].
However, it is important to note that freelancing also involves the responsibility of independently managing the administrative and financial aspects of the practice, which can be an additional source of stress. Moreover, the greater professional autonomy of FNs can foster a more innovative and personalized approach to care, improving the quality of services and increasing patient satisfaction. The personalized attention and the ability of build trusting relationships with patients can positively differentiate the service offered by FNs from those provided by employed nurses [31]. Conversely, employed nurses may benefit from greater economic security and structured support from healthcare institutions, aspects that can reduce anxiety related to job stability. However, the often rigid working conditions and lack of flexibility can contribute to increase stress and dissatisfaction [32].
In Italy, Law 43 of 2006 introduced the figure of the specialist nurse, adopting principles of nursing that are typical of Anglo-Saxon countries [33]. In 2018, IPASVI was replaced by the National Federation of Nursing Professions Orders (FNOPI) through a state law [34], marking a decisive step for the intellectual recognition of the profession, transitioning from a "college" to a "professional order." In terms of freelancing, despite the intramural regulations for physicians in the National Health System (SSN) being in place since 1992 [35], nurses were largely excluded until Law 56 of 2023, which partially abolished the exclusivity constraint for SSN healthcare professionals until 2025. This law allows nurses to work as freelancers outside of service hours with employer authorization. From an economic perspective, only Law 49 of 2023 [36] introduced "fair compensation" for nursing services provided through freelancing to businesses, thereby further enhancing the profession's valuation. Official FNOPI data indicates that the total number of Italian nurses is approximately 500,000, with about 10% operating as freelancers [1,37].
2. Methods
2.1. Aims
2.1.1. Primary:
The study assessed the JS-Nursing Italian Score, a tool for assessing JS among nurses.
Research question: JS-Nursing Italian Score is a valid and reliable instrument for measuring JS among nurses in Italy?
2.1.1. Secondary:
The study compared JS levels between employed nurses and FNs.
Research question: Are there significant differences in JS levels between employed nurses and FNs?
2.2. Study design
The study was a Psychometric and Cross-Sectional Study, conducted in May 2023 in two phases: a validation phase and an observational phase. In the validation phase, we assessed the content, construct, and reliability of the JS-Nursing Italian Score. In the observational phase, we conducted a cross-sectional analysis to compare JS levels between employed nurses and FNs. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [38,39] were followed for evidence reporting (Supplementary File 1).
2.3. Ethical Consideration
This study adhered to the principles outlined in the Helsinki Declaration. All participants were informed about the study's objectives, and the consent was obtained in compliance with all privacy regulations (Art. 13 EU Regulation 679/2016) before survey administration. The data were processed anonymously. Ethical approval was granted by the Istitutional Review Board of Ast Fermo with authorization code INF01/2023.
2.4. Sample and Inclusion Criteria
This study included FNs and nurses employed by public and private facilities operating in Italy. A key inclusion criterionwas the participants' registration with the Professional Nursing Association. To ensure a representative sample of the nursing population in Italy, participants were recruited through a targeted sampling strategy using LinkedIn, a professional networking platform. The survey was conducted over a one-month period from May 1, 2023, to May 31, 2023. This method allowed us to reach a broad and diverse group of nurses across various sectors.
2.5. Study Setting
The study setting encompassed nursing activities conducted both in hospital wards and in community care settings across Italy. This approach allowed for the evaluation of working conditions and professional experiences in various healthcare settings, providing a more comprehensive and representative overview of the diverse operational realities of nurses in Italy.
2.6. Instrument
To select the most suitable questionnaire for the chosen cohort of nurses, a preliminary bibliographic search was carried out on PubMed and CINAHL, along with an in-depth analysis of the Italian regulatory context. It was determined that the Quality of Nursing Work Life Survey (QNWL) was the most appropriate questionnaire for this purpose [40]. However, the Italian version of this questionnaire had not been exclusively tested on a nursing population, but rather on a mixed cohort that included medical personnel [41]. Questionnaires for assessing burnout [42,43] or measuring resilience [44] did not fully align with the survey's objectives. For these reasons, a specific survey was developed.
The questionnaire consists of an initial demographic section to describe the sample (age, gender, years of work experience, type of contract, and care setting), followed by 10 questions categorized in four domains: work relationship (colleagues/patients; questions 5, 7 and 10); external relations (institutional/professional; questions 8 and 9); general quality of life (family/personal; questions 1 and 2); work-related stress factor (internal/external; questions 3, 4 and 6). Each question was scored using a 5-point Likert scale [45], where the satisfaction level was assigned a score: 1 = "not satisfied", 2 = "slightly satisfied", 3 = "satisfied", 4 = "fairly satisfied", and 5 = "very satisfied" (Supplementary File 2 Italin and English versions).
2.7. Data Analysis
Descriptive statistics [median, mode, interquantile range (IQR)] were used to analyze the characteristics of the sample. The Content Validity Index (I-CVI) was assessed to evaluate content validity. Internal consistency was investigated by calculating Cronbach's alpha and MacDonald’s Omega coefficients, while construct validity was assessed through an Exploratory Factor Analysis (EFA). One-Way Welch’s ANOVA was performed individually to identity significant differences between variable groups. Data Analysis was performed using the software Jamovi V.2.3.21.0 [46].
3. Results
3.1. Sample Characteristics
A total of 200 questionnaires were correctly completed, divided into 46 FNs and 154 employees, with 108 working in public health services and 46 in private facilities, with 165 respondents being women (82.5%) and 35 being men (17.5%). The median age of the respondents was 39 years (IQR = 16.3), and the median years of service was 15 years (IQR = 14.5). The Shapiro-Wilk test indicated a non-normal distribution for both age (W = 0.951, p <.001) and years of service (W = 0.961, p <.001). A descriptive analysis of the sample was conducted using the median, mode, and IQR, stratifying the cited variables by gender, type of employment, and setting (summary Table 1).
This analysis revealed that 108 nurses (54%) reported working in public settings, 46 (23%) in private settings, and 46 (23%) as freelancers. Additionally, 98 nurses (49%) reported working in hospitals, 60 (30%) in community health centers, and 42 (21%) in home care settings.
3.2. Content Validity Index
The content validity was assessed using the Content Validity Index (I-CVI). Ten nurses with more than 10 years of experience, working in the three settings under study, evaluated the relevance of the questions using a Likert scale ranging from 1 (not relevant) to 4 (highly relevant). All 10 items immediately received a relevance rating of > 0.8. No critical issues were reported.
3.3. Reliability
The questionnaire results were assessed using Cronbach's α coefficient and McDonald's ω coefficient. Both values indicated good levels of reliability overall (α = 0.827, ω = 0.829) and with the exclusion of individual items (α range [0.798-0.831], ω range [0.8-0.832]). The results of the Kaiser-Meyer-Olkin measure (0.74) and Bartlett's test of sphericity (p < .001) supported the conduct of an exploratory EFA. The EFA factor pattern, both without rotation and with orthogonal Varimax rotation, revealed the presence of 4 factors. The instrument explained 58.49% of the total variance. The factor loadings are reported in Table 2; except for Item 10, all items presented factor loadings higher than Stevens' cutoff (0.4) [47].
3.4. Comparison Between Multiple Groups
The global scores of the participants were stratified by sample characteristics, revealing several differences between the groups thus created (Table 3); Figure 1 graphically presents the descriptive statistics of the analyzed groups.
From the descriptive analysis of the global JS scores (Global Score) divided by gender, type of contract, and work setting, it emerges that women (N=165) report an average global score of 34.4 (median 35, mode 29, SD 6.68, and IQR 11.0), while men (N = 35) have an overall average score of 30.3 (median 28, mode 29, SD 8.35, and IQR 14.5). Regarding the type of contract, FNs (N = 46) reported an average score of 41.8 (median 42, mode 43, SD 3.43, and IQR 4.00). Nurses employed in the private sector (N = 46) achieved an average score of 37.8 (median 38, mode 37, SD 4.03, and IQR 4.75), while those in the public sector (N = 108) had an average score of 25.5 (median and mode 29, SD 4.52, and IQR 5.00).
Regarding the work setting, nurses working in home care (N = 42) achieved an average score of 38.1 (median 40, mode 42, SD 6.35, and IQR 7.75), those in hospitals (N = 98) 32.2 (median 32, mode 26, SD 7.14, and IQR 11.00), while nurses engaged in community care (N = 60) achieved an average score of 33.0 (median 32, mode 29, SD 6.54, and IQR 8.00). In summary, women show higher JS than men, with a higher average score and less dispersion, as indicated by the lower IQR. FNs have the highest satisfaction scores compared to those in the private and public sectors. Regarding the care setting, nurses working in home care report the highest satisfaction, followed by those in community care, and finally, those working in hospitals (Figure 1).
To test the significance of the differences observed in relation to the type of employment, setting, and gender of the participants concerning the global score, the normality of the data distribution and homoscedasticity were tested to assess the feasibility of performing a factorial ANOVA. The normality tests (Shapiro-Wilk, p = 0.056; Kolmogorov-Smirnov, p = 0.428) indicated no significant deviation from normality in the data. However, Levene's test was significant (F = 2.43, p = 0.016), violating the principle of homoscedasticity. Unable to perform factorial ANOVA, Welch's correction for one-way ANOVA was used, repeated separately for each investigated variable. The normality of the distribution was further evaluated using the Kolmogorov-Smirnov test (KS test), with significant values obtained for all three investigated variables (Table 4).
The post hoc tests confirmed these significances, except for the differences between the overall scores in the hospital and the community setting (Table 5).
4. Discussion
This study aimed to validate the JS-Nursing Italian Score, a tool for assessing JS among nurses, and to compare JS levels between employed nurses and FNs. By analysing these aspects, the study seeks to provide an empirical basis for future policies and interventions that can improve working conditions and, consequently, the quality of nursing care [48-50]. Our research involved a sample of Italian nurses divided among public employees, private employees, and freelancers. This composition reflects the structure of the nursing sector in Italy, where the majority of nurses are employed in the public sector, with a growing but still minority presence of freelancers [51].
This scenario is not unique to Italy, many European countries have a similar distribution. For example, in France and Germany, the majority of nurses are still employed in the public sector, whereas in countries like the United Kingdom, the appeal of freelancing is growing but remains a minority choice compared to public employment [52]. In terms of work settings, most of our participants operate in hospitals, followed by territorial facilities and home care contexts. This is in line with the general trend observed in numerous European countries where hospital work is prevalent [53]. However, in countries like the Netherlands, Belgium, and Finland, there is a progressive shift towards home and territorial care, with the intent of decongesting hospitals and providing more personalized care to patients [54].
This trend may not yet be fully developed in the Italian healthcare context as the policies for territorial and home care are relatively recent, having been significantly implemented only after the COVID-19 pandemic. Therefore, more time will be needed before more specific and comprehensive data on these changes become available [55]. Analysing the JS-Nursing Italian Score questionnaire, significant differences were highlighted among the categories of nurses examined. FNs reported higher scores in all four domains of the questionnaire: work relationships, external relationships, general quality of life, and work-related stress factors [56,57]. In terms of work relationships, greater autonomy and flexibility in managing their work seem to play a crucial role for freelancers. The ability to self-determine work hours and methods can significantly contribute to a positive perception of work relationships. This autonomy is less present among employee nurses, who often have to adhere to rigid hierarchies and predefined schedules. In various European contexts, where the culture of flexible work is more developed, a positive correlation between work autonomy and professional satisfaction is observed [58].
Regarding external relationships, freelancers feel a greater respect and recognition of their professional competence. This may be due to the need to maintain high standards to attract and retain clients. In countries where the freelancing model is well-established, such as the Netherlands, healthcare professionals often enjoy greater social and professional consideration [59-61]. This recognition not only improves job satisfaction but can also positively influence the quality of service offered. General quality of life is another domain where freelancers excel. The ability to manage their free time and family life is significantly enhanced by flexible hours. This aspect was particularly emphasized during the COVID-19 pandemic, when many employed nurses worldwide faced exhausting shifts and a high workload, especially in intensive care units [62-64].
About work-related stress factors, freelancers reported lower stress levels compared to employees. The ability to choose assignments and work hours based on personal needs significantly reduces stress. This is a strength of freelance work that clearly emerges even in international contexts. In Nordic countries, where the culture of work well-being is particularly developed, freelancers often report a lower incidence of burnout and work-related stress [65]. These results are corroborated by international literature, which highlights how the pandemic further accentuated the differences between employed and freelance nurses. In typically North American countries, recent studies have shown that freelancers tend to report higher job satisfaction, thanks to flexibility and the possibility of obtaining higher compensation [66].
However, these differences can vary significantly depending on the national context and specific labor market regulations. In Italy, the regulation of freelance work is still evolving and could benefit from a comparative analysis with more established healthcare systems in several clinical setting and increasingly of high technological impact [67-70]. Finally, the factor analysis of the JS-Nursing Italian Score confirmed the validity of the instrument, with high loading values for most items, indicating good internal consistency.
These results suggest that the questionnaire is a valid tool for measuring JS among Italian nurses. However, to further strengthen the validity and reliability of the tool, it will be necessary to apply it to larger and more diverse national samples, as well as in international contexts. This study provides an empirical basis for analysing the working conditions of nurses and promoting future measures that increase professional autonomy and work flexibility, which could significantly contribute to improving JS, reducing stress levels, and enhancing the quality of nursing care. Additionally, a more in-depth international comparison could offer further insights to optimize work practices and health policies, taking into account the cultural and organizational specificities of different national contexts.
4.1. Limitations
This study presents several limitations that should be considered when interpreting the results. Firstly, the sample used, although diverse, may not be representative of the entire Italian nursing population. Additionally, the validation of the JS-Nursing Italian Score questionnaire is still preliminary and requires further verification on larger samples to confirm its reliability and validity. Another limitation is the cross-sectional design of the study, which does not allow for establishing causal relationships between the variables examined. Perceptions of JS can be influenced by numerous external factors not considered in this study, such as regional economic conditions and specific local healthcare policies. Finally, the data collection was based on self-assessments by the participants, which could introduce social desirability bias or result in responses that are not entirely accurate.
4.2. Implications for nursing practice and nursing policy
In terms of limitations, our study has several strengths worth considering. Firstly, it is easily repeatable and reproducible in different healthcare settings, both in terms of the healthcare system and the care models use. Secondly, having obtained objective quantitative results, it could serve as a reference study for the objectification of organizational well-being among nurses in Italy, and beyond. Furthermore, it could encourage specific research on this topic, particularly regarding stress and organizational well-being for nurses across multiple care settings.
5. Conclusion
This study provides a preliminary overview of the differences in JS perceptions between employed and FNs in Italy. The results indicate that FNs report higher satisfaction in the four domains analysed: work relationships, external relationships, general quality of life, and work-related stress factors, suggesting that autonomy and work flexibility are key elements for improving JS among nurses. Consequently, promoting more flexible work models and offering greater opportunities for freelancing could help improve the well-being and satisfaction of Italian nurses, with potential benefits for the quality of care provided. Looking ahead, it will be essential to conduct further research on larger and more diverse samples to confirm and expand these findings. Longitudinal studies could offer a deeper insight into the temporal dynamics in JS and identify causal factors not addressed in our research.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Supplementary File 1: STROBE Statement—checklist; Supplementary File 1: Questionnaire JS-Nursing Italian Score (English and Italian version).
Author Contributions
Conceptualization, G.C. (Giovanni Cangelosi) and F.P.; methodology, G.C. (Giovanni Cangelosi) and S.M.; software, M.P.; validation, S.M. and G.C. (Giovanni Cangelosi) ; formal analysis, M.P.; investigation, G.C. (Giovanni Cangelosi) and D.B.; data curation, G.C. (Giovanni Cangelosi) ; writing—original draft preparation, G.C. (Gabriele Caggianelli), S.M., M.S., S.P., G.B., F.B., M.P., and S.M.P.; writing—review and editing, G.C. (Gabriele Caggianelli), S.M.P,, S.M., and F.P.; visualization, G.C. (Gabriele Caggianelli), S.M., M.S., and F.P.; supervision, G.C. (Giovanni Cangelosi) and F.P.; project administration, G.C. (Giovanni Cangelosi) and F.P. All authors have read and agreed to the published version of the manuscript. G.C. (Giovanni Cangelosi) & S.M. contributed equally as first authors; M.S. & F.P. contributed equally as last authors.
Funding
This research received no external funding.
Institutional Review Board Statement
This study adhered to the principles outlined in the Helsinki Declaration. Ethical approval was granted by the Istitutional Review Board of Ast Fermo with authorization code INF 01/2023, date February 22, 2023.
Informed Consent Statement
All participants were informed about the study's objectives, and the consent was obtained in compliance with all privacy regulations (Art. 13 EU Regulation 679/2016) before survey administration. The data were processed anonymously.
Data Availability Statement
The data that support the findings of this study are available on the text and Supplementary materials.
Conflicts of Interest
The authors declare no competing interest.
References
- Federazione Nazionale Ordini Professioni Infermieristiche (FNOPI). Vademecum della Libera Professione Infermieristica, 2020. Available online: https://www.fnopi.it/le-politiche-professionali/libera-professione/#1572340301684-c38d9ace-6c6e (accessed on 15 January 2025).
- Parlamento della Repubblica Italiana. Legge 21 aprile 2023, n. 49. Disposizioni in materia di equo compenso delle prestazioni Professionali. Available online: https://www.gazzettaufficiale.it/ eli/id/2023/05/05/23G00051/sg (accessed on 15 January 2025).
- World Health Organization (WHO). Italy, Data. Available online: https://data.who.int/countries/380 (accessed on 15 January 2025).
- Istituto Nazionale di Statistica (ISTAT). Noi Italia 2024. Available online: https://noi-italia.istat.it/ (accessed on 15 January 2025).
- Ministero della Salute Italiano. Decreto 23 maggio 2022, n. 77, Regolamento recante la definizione di modelli e standard per lo sviluppo dell'assistenza territoriale nel Servizio sanitario nazionale. Available online: https://www.gazzettaufficiale.it/eli/id/2022/06/22/22G00085/sg (accessed on 15 January 2025).
- Ministero della Salute Italiano. Piano Nazionale di Ripresa e Resilienza, PNRR Salute, Il nuovo modello di assistenza territoriale in un’ottica One Health. Available online: https://www.pnrr.salute.gov.it/portale/pnrrsalute/ (accessed on 15 January 2025).
- American Nurse Association (ANA). Nurse Burnout: What Is It & How to Prevent It, 2024. Available online: https://www.nursingworld.org/content-hub/resources/workplace/what-is-nurse-burnout-how-to-prevent-it/ (accessed on 15 January 2025).
- World Health Organization (WHO). Guidelines on mental health at work, 2022. Available online: https://www.who.int/publications/i/item/9789240053052 (accessed on 15 January 2025).
- Cañadas-De la Fuente, G.A.; Gómez-Urquiza, J.L.; Ortega-Campos, E.M.; Cañadas, G.R.; Albendín-García, L.; De la Fuente-Solana, E.I. Prevalence of burnout syndrome in oncology nursing: A meta-analytic study. Psychooncology 2018, 27, 1426–1433. [Google Scholar] [CrossRef]
- Petrelli, F.; Cangelosi, G.; Scuri, S.; Davidici, C.; Lavorgna, F.; Debernardi, G.; Benni, A.; Veprini, A.; Nguyen, C.T.T.; Caraffa, A.; Grappasonni, I. Burnout syndrome: A preliminary study of a population of nurses in Italian prisons. Clin. Ter. 2020, 171, 4. [Google Scholar] [CrossRef]
- Pien, L.C.; Cheng, Y.; Lee, F.C.; Cheng, W.J. The effect of multiple types of workplace violence on burnout risk, sleep quality, and leaving intention among nurses. Ann. Work Expo Health 2024, 77, wxae052. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Oe, M.; Ishida, T.; Matsuoka, M.; Chiba, H.; Uchimura, N. Workplace violence and its effects on burnout and secondary traumatic stress among mental healthcare nurses in Japan. Int. J. Environ. Res. Public Health 2020, 17, 2747. [Google Scholar] [CrossRef] [PubMed]
- O'Donovan, R.; De Brún, A.; McAuliffe, E. Healthcare professionals' experience of psychological safety, voice, and silence. Front. Psychol. 2021, 12, 626689. [Google Scholar] [CrossRef] [PubMed]
- Kelly, L.A.; Lefton, C.; Fischer, S.A. Nurse leader burnout, satisfaction, and work-life balance. J. Nurs. Adm. 2019, 49, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Alwhaibi, M.; Alhawassi, T.M.; Balkhi, B.; Al Aloola, N.; Almomen, A.A.; Alhossan, A.; Alyousif, S.; Almadi, B.; Bin Essa, M.; Kamal, K.M. Burnout and depressive symptoms in healthcare professionals: A cross-sectional study in Saudi Arabia. Healthcare 2022, 10, 2447. [Google Scholar] [CrossRef]
- Khamisa, N.; Oldenburg, B.; Peltzer, K.; Ilic, D. Work related stress, burnout, job satisfaction and general health of nurses. Int. J. Environ. Res. Public Health 2015, 12, 652–666. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.B.; Lee, S.H. The nursing work environment, supervisory support, nurse characteristics, and burnout as predictors of intent to stay among hospital nurses in the Republic of Korea: A path analysis. Healthcare 2023, 11, 1653. [Google Scholar] [CrossRef]
- Waltz, L.A.; Muñoz, L.; Weber Johnson, H.; Rodriguez, T. Exploring job satisfaction and workplace engagement in millennial nurses. J. Nurs. Manag. 2020, 28, 673–681. [Google Scholar] [CrossRef]
- Unruh, L.; Zhang, N.J. The hospital work environment and job satisfaction of newly licensed registered nurses. Nurs. Econ. 2014, 32, 296–305. [Google Scholar] [PubMed]
- Gómez-Gascón, T.; Martín-Fernández, J.; Gálvez-Herrer, M.; Tapias-Merino, E.; Beamud-Lagos, M.; Mingote-Adán, J.C.; Grupo EDESPROAP-Madrid. Effectiveness of an intervention for prevention and treatment of burnout in primary health care professionals. BMC Fam. Pract. 2013, 14, 173. [Google Scholar] [CrossRef]
- Keith, A.C.; Warshawsky, N.; Talbert, S. Factors that influence millennial generation nurses' intention to stay: An integrated literature review. J. Nurs. Adm. 2021, 51, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Perkins, R.T.; Bamgbade, S.; Bourdeanu, L. Nursing leadership roles and its influence on the millennial psychiatric nurses' job satisfaction and intent to leave. J. Am. Psychiatr. Nurses Assoc. 2023, 29, 15–24. [Google Scholar] [CrossRef]
- Coomber, B.; Barriball, K.L. Impact of job satisfaction components on intent to leave and turnover for hospital-based nurses: A review of the research literature. Int. J. Nurs. Stud. 2007, 44, 297–314. [Google Scholar] [CrossRef] [PubMed]
- Al Maqbali, M.A. Factors that influence nurses' job satisfaction: A literature review. Nurs. Manag. (Harrow) 2015, 22, 30–37. [Google Scholar] [CrossRef]
- Oyama, N.; Seki, M.; Nakai, M.; Miyamoto, K.; Nagao, K.; Morimitsu, R. Depressive symptoms, burnout, resilience, and psychosocial support in healthcare workers during the COVID-19 pandemic: A nationwide study in Japan. PCN Rep. 2023, 2, e136. [Google Scholar] [CrossRef] [PubMed]
- Raei, M.; Shahrbaf, M.A.; Salaree, M.M.; Yaghoubi, M.; Parandeh, A. Prevalence and predictors of burnout among nurses during the COVID-19 pandemic: A survey in teaching hospitals. Work 2024, 77, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- Scuri, S.; Tesauro, M.; Petrelli, F.; Argento, N.; Damasco, G.; Cangelosi, G.; Nguyen, C.T.T.; Savva, D.; Grappasonni, I. Use of an online platform to evaluate the impact of social distancing measures on psycho-physical well-being in the COVID-19 era. Int. J. Environ. Res. Public Health 2022, 19, 6805. [Google Scholar] [CrossRef] [PubMed]
- Gülşen, M.; Ertuğrul, B.; Taşkın, G.; Aytar, A.; Genç, Y.K. The relationship between burnout and work engagement levels of nurses and physiotherapists working during the COVID-19 pandemic period. Work 2024, 77, 0–0. [Google Scholar] [CrossRef] [PubMed]
- Brunetto, Y.; Farr-Wharton, R. A Case Study Examining the Impact of Public-Sector Nurses' Perception of Workplace Autonomy on Their Job Satisfaction: Lessons for Management. Int. J. Manag. Organ. Behav. 2004, 8(5), 521–539. [Google Scholar]
- Malinowska-Lipień, I.; Gabryś, T.; Kózka, M.; Gniadek, A.; Brzostek, T. Nurses' Intention to Leave Their Jobs in Relation to Work Environment Factors in Polish Hospitals: Cross-Sectional Study. Med. Pr. 2023, 74(5), 377–387. [Google Scholar] [CrossRef] [PubMed]
- Lacour, F.; Estrate, M. Au-delà du soin, une collaboration des infirmiers libéraux en réseau de santé [Beyond Care, the Collaboration of Freelance Nurses in a Healthcare Network]. Soins 2013, (775), 56–58. [Google Scholar] [CrossRef]
- Dutra, C.K.D.R.; Guirardello, E.B. Nurse Work Environment and Its Impact on Reasons for Missed Care, Safety Climate, and Job Satisfaction: A Cross-Sectional Study. J. Adv. Nurs. 2021, 77(5), 2398–2406. [Google Scholar] [CrossRef] [PubMed]
- Parlamento della Repubblica Italiana. Legge 43 del 1 Febbraio 2006, Disposizioni in Materia di Professioni Sanitarie Infermieristiche, Ostetrica, Riabilitative, Tecnico-Sanitarie e della Prevenzione e Delega al Governo per l'Istituzione dei Relativi Ordini Professionali. Gazzetta Ufficiale, 17 February 2006. Available online: https://www.gazzettaufficiale.it/eli/id/2006/02/17/006G0050/sg (accessed on 15 January 2025).
- Parlamento della Repubblica Italiana. Legge 3 del 11 Gennaio 2018, Delega al Governo in Materia di Sperimentazione Clinica di Medicinali Nonché Disposizioni per il Riordino delle Professioni Sanitarie e per la Dirigenza Sanitaria del Ministero della Salute. Gazzetta Ufficiale, 31 January 2018. Available online: https://www.gazzettaufficiale.it/eli/id/2018/1/31/18G00019/sg (accessed on 15 January 2025).
- Presidenza del Consiglio dei Ministri Italiano. Decreto Legislativo 502 del 30 Dicembre del 1992, Riordino della Disciplina in Materia Sanitaria, a Norma dell'Articolo 1 della Legge 23 Ottobre 1992, N. 421. Gazzetta Ufficiale, 7 January 1994. Available online: https://www.gazzettaufficiale.it/eli/id/1994/01/07/094A0049/sg (accessed on 15 January 2025).
- Presidenza del Consiglio dei Ministri Italiano. Misure Urgenti a Sostegno delle Famiglie e delle Imprese per l'Acquisto di Energia Elettrica e Gas Naturale, Nonché in Materia di Salute e Adempimenti Fiscali. Gazzetta Ufficiale, 30 March 2023. Available online: https://www.gazzettaufficiale.it/eli/id/2023/03/30/23G00042/sg (accessed on 15 January 2025).
- Federazione Nazionale Ordini Professioni Infermieristiche (FNOPI). Infermieri per Voi. Available online: https://infermieripervoi.it/ (accessed on 15 January 2025).
- Strengthening the Reporting of Observational Studies in Epidemiology (STROBE). Available online: https://www.strobe-statement.org/ (accessed on 15 January 2025).
- Skrivankova, V.W.; Richmond, R.C.; Woolf, B.A.R.; Yarmolinsky, J.; Davies, N.M.; Swanson, S.A.; VanderWeele, T.J.; Higgins, J.P.T.; Timpson, N.J.; Dimou, N.; Langenberg, C.; Golub, R.M.; Loder, E.W.; Gallo, V.; Tybjaerg-Hansen, A.; Davey Smith, G.; Egger, M.; Richards, J.B. Strengthening the Reporting of Observational Studies in Epidemiology Using Mendelian Randomization: The STROBE-MR Statement. JAMA 2021, 326(16), 1614–1621. [Google Scholar] [CrossRef] [PubMed]
- Brooks, B.A. Development of an Instrument to Measure Quality of Nurses' Worklife. ProQuest Dissertations & Theses, University of Illinois at Chicago, Health Sciences Center. 2001. 3008064.
- Garzaro, G.; Clari, M.; Donato, F.; Dimonte, V.; Mucci, N.; Easton, S.; Van Laar, D.; Gatti, P.; Pira, E. A Contribution to the Validation of the Italian Version of the Work-Related Quality of Life Scale. Med. Lav. 2020, 111(1), 32–45. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E. MBI: Maslach Burnout Inventory; Manual; University of California: Palo Alto, CA, USA, 1891. [Google Scholar]
- Sirigatti, S.; Stefanile, C. Adattamento e Taratura per l’Italia. In Maslach, C.; Jackson, S., Eds.; MBI Maslach Burnout Inventory; Organizzazioni Speciali: Firenze, Italy, 1993, 33–42.
- Connor, K.M.; Davidson, J.R. Development of a New Resilience Scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Likert, R. Technique for the Measure of Attitudes. Arch. Psychol. 1932, 22, 140. [Google Scholar]
- The jamovi project. Jamovi Version 2.3, 2002. Available online: https://www.jamovi.org (accessed on 15 January 2025).
- Steven, J.P. Applied Multivariate Statistics for the Social Sciences; Routledge: New York, NY, USA, 2009. [Google Scholar] [CrossRef]
- Van der Heijden, B.I.; Brown Mahoney, C.; Xu, Y. Impact of Job Demands and Resources on Nurses' Burnout and Occupational Turnover Intention Towards an Age-Moderated Mediation Model for the JD-R Framework. Int. J. Environ. Res. Public Health 2019, 16(11), 2011. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P. Understanding the Burnout Experience: Recent Research and Its Implications for Psychiatry. World Psychiatry 2016, 15(2), 103–111. [Google Scholar] [CrossRef] [PubMed]
- Bowling, N.A.; Hammond, G.D. A Meta-Analytic Examination of the Construct Validity of the Michigan Organizational Assessment Questionnaire Job Satisfaction Subscale. J. Vocat. Behav. 2008, 73(1), 63–77. [Google Scholar] [CrossRef]
- Albolino, S.; Tartaglia, R.; Bellandi, T.; Amicosante, A.M.; Bianchini, E.; Biggeri, A. Patient Safety and Incident Reporting: Survey of Italian Healthcare Workers. Qual. Saf. Health Care 2010, 19 (Suppl 3), i8–i12. [Google Scholar] [CrossRef]
- Gray, P.; Senabe, S.; Naicker, N.; Kgalamono, S.; Yassi, A.; Spiegel, J.M. Workplace-Based Organizational Interventions Promoting Mental Health and Happiness Among Healthcare Workers: A Realist Review. Int. J. Environ. Res. Public Health 2019, 16(22), 4396. [Google Scholar] [CrossRef] [PubMed]
- Aust, B.; Leduc, C.; Cresswell-Smith, J.; O'Brien, C.; Rugulies, R.; Leduc, M.; Dhalaigh, D.N.; Dushaj, A.; Fanaj, N.; Guinart, D.; Maxwell, M.; Reich, H.; Ross, V.; Sadath, A.; Schnitzspahn, K.; Tóth, M.D.; van Audenhove, C.; van Weeghel, J.; Wahlbeck, K.; Arensman, E.; Greiner, B.A.; MENTUPP Consortium Members. The Effects of Different Types of Organizational Workplace Mental Health Interventions on Mental Health and Wellbeing in Healthcare Workers: A Systematic Review. Int. Arch. Occup. Environ. Health 2024, 97(5), 485–522. [CrossRef]
- Smets, T.; Pivodic, L.; Piers, R.; Pasman, H.R.W.; Engels, Y.; Szczerbińska, K.; Kylänen, M.; Gambassi, G.; Payne, S.; Deliens, L.; Van den Block, L. The Palliative Care Knowledge of Nursing Home Staff: The EU FP7 PACE Cross-Sectional Survey in 322 Nursing Homes in Six European Countries. Palliat. Med. 2013, 27(1), 96–105. [Google Scholar] [CrossRef]
- Presidenza del Consiglio dei Ministri Italiano. Decreto Ministeriale 71, Modelli e Standard per lo Sviluppo dell'Assistenza Territoriale nel Servizio Sanitario Nazionale. Gazzetta Ufficiale, 3 May 2022. Available online: https://www.gazzettaufficiale.it/eli/id/2022/05/03/22A02656/sg (accessed on 15 January 2025).
- Labrague, L.J.; McEnroe-Petitte, D.M.; Leocadio, M.C.; Van Bogaert, P.; Cummings, G.G. Stress and Ways of Coping Among Nurse Managers: An Integrative Review. J. Clin. Nurs. 2018, 27(7–8), 1346–1359. [CrossRef]
- Niskala, J.; Kanste, O.; Tomietto, M.; Miettunen, J.; Tuomikoski, A.M.; Kyngäs, H.; Mikkonen, K. Interventions to Improve Nurses' Job Satisfaction: A Systematic Review and Meta-Analysis. J. Adv. Nurs. 2020, 76(7), 1498–1508. [Google Scholar] [CrossRef] [PubMed]
- Yasin, Y.M.; Kerr, M.S.; Wong, C.A.; Bélanger, C.H. Factors Affecting Nurses' Job Satisfaction in Rural and Urban Acute Care Settings: A PRISMA Systematic Review. J. Adv. Nurs. 2020, 76, 963–979. [Google Scholar] [CrossRef] [PubMed]
- Monsen, K.A.; de Blok, J. Buurtzorg: Nurse-Led Community Care. Creat. Nurs. 2013, 19, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Lumillo-Gutiérrez, I.; Salto, G.E. Buurtzorg Nederland, a Proposal for Nurse-Led Home Care. Enferm. Clin. (Engl. Ed.) 2021, 31, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Hegedüs, A.; Schürch, A.; Bischofberger, I. Implementing Buurtzorg-Derived Models in the Home Care Setting: A Scoping Review. Int. J. Nurs. Stud. Adv. 2022, 4, 100061. [Google Scholar] [CrossRef]
- Mao, X.; Hou, T.; Wang, H.; Tang, Y.; Ni, C.; Zhang, Y.; Zhang, J.; Deng, W.; Chen, L.; Wang, X.; Li, Z.; Jia, Y.; Dong, W.; Qian, X. Status and Influencing Factors of Nurses' Burnout: A Cross-Sectional Study During COVID-19 Regular Prevention and Control in Jiangsu Province, China. Glob. Ment. Health (Camb.) 2024, 11, e54. [Google Scholar] [CrossRef]
- Mao, X.; Lin, X.; Liu, P.; Zhang, J.; Deng, W.; Li, Z.; Hou, T.; Dong, W. Impact of Insomnia on Burnout Among Chinese Nurses Under the Regular COVID-19 Epidemic Prevention and Control: Parallel Mediating Effects of Anxiety and Depression. Int. J. Public Health 2023, 68, 1605688. [Google Scholar] [CrossRef] [PubMed]
- Sihvola, S.; Nurmeksela, A.; Mikkonen, S.; Peltokoski, J.; Kvist, T. Resilience, Job Satisfaction, Intentions to Leave Nursing and Quality of Care Among Nurses During the COVID-19 Pandemic—A Questionnaire Study. BMC Health Serv. Res. 2023, 23. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, A.M.; Al-Hniti, M.; Bani Salameh, A.; Alkaid-Albqoor, M.; Ahmad, M. Predictors of Job Satisfaction of Registered Nurses Providing Care for Older Adults. J. Nurs. Manag. 2021, 29, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Thiessen, N.J.; Leslie, K.; Stephens, J.M.L. An Examination of Self-Employed Nursing Regulation in Three Canadian Provinces. Policy Polit. Nurs. Pract. 2023, 24, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Sguanci, M.; Mancin, S.; Gazzelloni, A.; Diamanti, O.; Ferrara, G.; Morales Palomares, S.; Parozzi, M.; Petrelli, F.; Cangelosi, G. The Internet of Things in the Nutritional Management of Patients with Chronic Neurological Cognitive Impairment: A Scoping Review. Healthcare 2024, 13, 23. [Google Scholar] [CrossRef]
- Cangelosi, G.; Mancin, S.; Pantanetti, P.; Nguyen, C.C.T.; Morales Palomares, S.; Biondini, F.; Sguanci, M.; Petrelli, F. Lifestyle Medicine Case Manager Nurses for Type Two Diabetes Patients: An Overview of a Job Description Framework—A Narrative Review. Diabetology 2024, 5, 375–388. [Google Scholar] [CrossRef]
- Colombo, S.; Golzio, L.E.; Bianchi, G. The Evolution of Health-, Safety- and Environment-Related Competencies in Italy: From HSE Technicians to HSE Professionals and, Eventually, to HSE Managers. Safety Sci. 2019, 118, 724–739. [Google Scholar] [CrossRef]
- Cangelosi, G.; Mancin, S.; Morales Palomares, S.; Pantanetti, P.; Quinzi, E.; Debernardi, G.; Petrelli, F. Impact of School Nurse on Managing Pediatric Type 1 Diabetes with Technological Devices Support: A Systematic Review. Diseases 2024, 12, 173. [Google Scholar] [CrossRef]
Figure 1.
Descriptive Characteristics of Analyzed Groups.
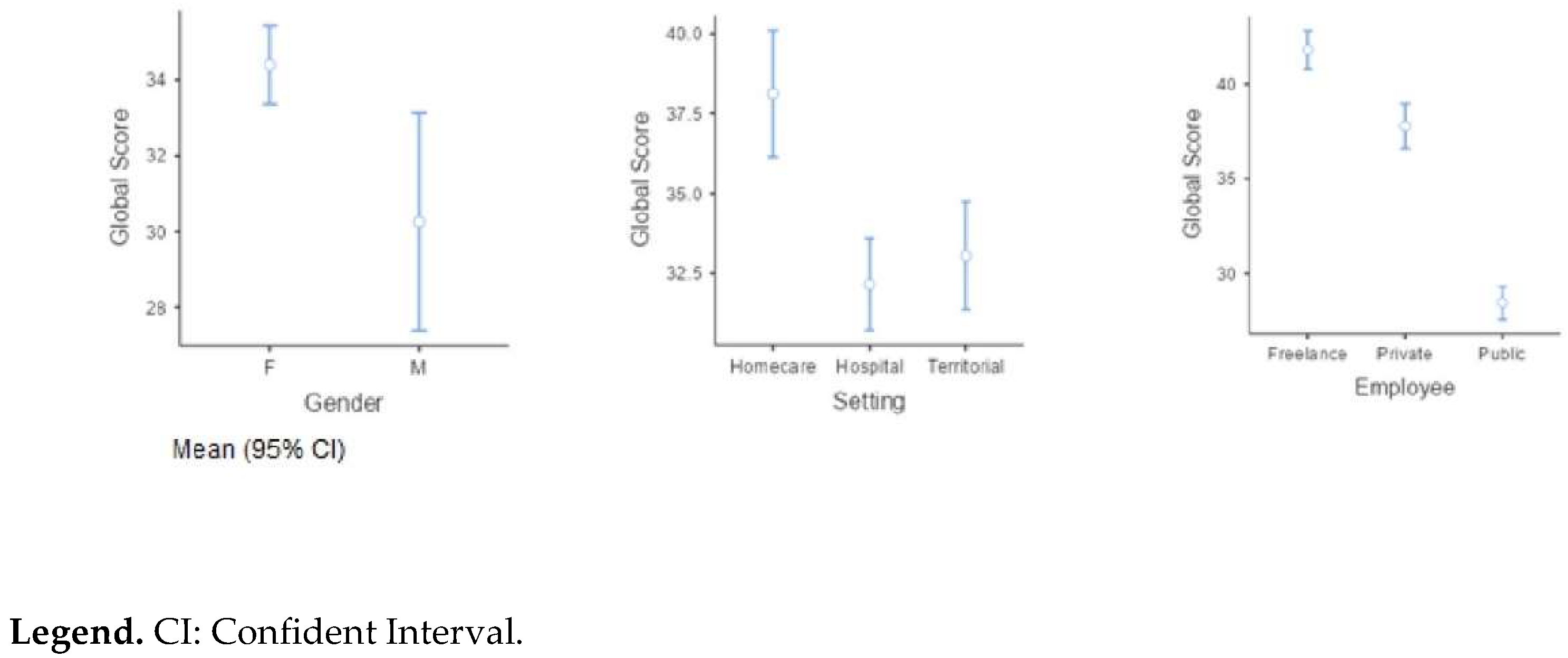

Table 1.
Sample Characteristics.
| Gender | N | Median | Mode | IQR | Setting | Emplyee | N | Median | Mode | IQR | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Years of service | F | 165 | 15 | 15 | 14.0 | Years of service | Domiciliary | Freelance | 26 | 9 | 10 | 10.25 | |
| M | 35 | 15 | 6 | 19.0 | Private | 8 | 14 | 1 | 16 | ||||
| Age | F | 165 | 40 | 39 | 15.0 | Public | 8 | 16 | 30 | 20.5 | |||
| M | 35 | 39 | 33 | 19.5 | Hospital | Freelance | 8 | 8.5 | 5 | 9 | |||
| Employee | N | Median | Mode | IQR | Private | 26 | 16 | 5 | 17.5 | ||||
| Years of service | Freelance | 46 | 7.5 | 6 | 10.8 | Public | 64 | 17 | 15 | 13 | |||
| Private | 46 | 15.5 | 5 | 19.8 | Territorial | Freelance | 12 | 5.5 | 2 | 13.25 | |||
| Public | 108 | 16 | 15 | 13.0 | Private | 12 | 17.5 | 12 | 20.5 | ||||
| Age | Freelance | 46 | 30.5 | 25 | 10.8 | Public | 36 | 14.50 | 12 | 7.25 | |||
| Private | 46 | 39 | 33 | 16.5 | Age | Domiciliary | Freelance | 26 | 32 | 25 | 12.25 | ||
| Public | 108 | 42 | 39 | 13.5 | Private | 8 | 38.5 | 46 | 15.75 | ||||
| Setting | N | Median | Mode | IQR | Public | 8 | 44 | 41 | 11.75 | ||||
| Years of service | Domiciliary | 42 | 10 | 10 | 10.8 | Hospital | Freelance | 8 | 31.50 | 26 | 10.75 | ||
| Hospital | 98 | 16.5 | 15 | 15.8 | Private | 26 | 40.5 | 33 | 17.75 | ||||
| Territorial | 60 | 14 | 12 | 11.3 | Public | 64 | 45.5 | 50 | 12.5 | ||||
| Age | Domiciliary | 42 | 35.5 | 26 | 13.5 | Territorial | Freelance | 12 | 29 | 25 | 6.75 | ||
| Hospital | 98 | 44 | 33 | 16.0 | Private | 12 | 41 | 39 | 15.5 | ||||
| Territorial | 60 | 39 | 39 | 12.3 | Public | 36 | 39 | 39 | 9.25 |
Legend: IQR= Interquartile Range; F= Female; M= Male; ᵃ There is more than one mode, only the first is reported.
Table 2.
Factor Loadings.
| Factor | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | Uniqueness | |||||||
| Item 1 | 0.118 | 0.105 | 0.9783 | 0.128 | 0.00149 | ||||||
| Item 2 | 0.207 | 0.249 | 0.4623 | 0.129 | 0.66506 | ||||||
| Item 3 | 0.198 | 0.190 | -0.0889 | 0.347 | 0.79668 | ||||||
| Item 4 | 0.197 | 0.108 | 0.2147 | 0.723 | 0.38014 | ||||||
| Item 5 | 0.754 | 0.123 | 0.1207 | 0.232 | 0.34848 | ||||||
| Item 6 | 0.216 | 0.227 | 0.2763 | 0.484 | 0.59171 | ||||||
| Item 7 | 0.851 | 0.192 | 0.1824 | 0.216 | 0.15890 | ||||||
| Item 8 | 0.129 | 0.845 | 0.1661 | 0.234 | 0.18625 | ||||||
| Item 9 | 0.223 | 0.793 | 0.1873 | 0.179 | 0.25491 | ||||||
| Item 10 | 0.330 | 0.139 | 0.1437 | 0.259 | 0.78431 | ||||||
Table 3.
Descriptive Analysis of Global Scores.
| Global Score | Gender | N | Mean | Median | Mode | SD | IQR |
|---|---|---|---|---|---|---|---|
| F | 165 | 34.4 | 35 | 29 | 6.68 | 11.0 | |
| M | 35 | 30.3 | 28 | 29 | 8.35 | 14.5 | |
| Global Score | Employee | N | Mean | Median | Mode | SD | IQR |
| Freelance | 46 | 41.8 | 42 | 43 | 3.43 | 4.00 | |
| Private | 46 | 37.8 | 38 | 37 | 4.03 | 4.75 | |
| Public | 108 | 25.5 | 29 | 29 | 4.52 | 5.00 | |
| Global Score | Setting | N | Mean | Median | Mode | SD | IQR |
| Home care | 42 | 38.1 | 40 | 42 | 6.35 | 7.75 | |
| Hospital | 98 | 32.2 | 32 | 26 | 7.14 | 11.00 | |
| Territorial | 60 | 33.0 | 32 | 29 | 6.54 | 8.00 |
Legend: SD = Standard Deviation; IQR = Interquartile Range; F = Female; M = Male.
Table 4.
One-way ANOVA (Welch).
| Dependent Variable | Grouping Variable | Normality Test | Normality p | F | df1 | df2 | p |
|---|---|---|---|---|---|---|---|
| Global Score | Gender | KS test | 0.106 | 7.58 | 1 | 43.7 | 0.009 |
| Employee | KS test | 0.166 | 213 | 2 | 102 | <.001 | |
| Setting | KS test | 0.372 | 12.6 | 2 | 106 | <.001 |
Legend: p = p-value; F = F-statistic; df1: Degrees of freedom (numerator); df2: Degrees of freedom (denominator)
Table 5.
Post hoc test (Games-Howell) for each variable.
| POST HOC TEST (Games-Howell): Gender | ||||
|---|---|---|---|---|
| F | M | |||
| F | Mean Difference | - | 4.14 | |
| p-value | - | 0.009 | ||
| M | Mean Difference | - | ||
| p-value | - | |||
| POST HOC TEST (Games-Howell): Employee | ||||
| Freelance | Private | Public | ||
| Freelance | Mean Difference | - | 4.02 | 13.34 |
| p-value | - | <.001 | <.001 | |
| Private | Mean Difference | - | 9.32 | |
| p-value | - | <.001 | ||
| Public | Mean Difference | - | ||
| p-value | - | |||
| POST HOC TEST (Games-Howell): Setting | ||||
| Homecare | Hospital | Territorial | ||
| Homecare | Mean Difference | - | 5.97 | 5.07 |
| p-value | - | <.001 | <.001 | |
| Hospital | Mean Difference | - | -0.897 | |
| p-value | - | 0.699 | ||
| Territorial | Mean Difference | - | ||
| p-value | - | |||
Legend: F = Female; M = Male.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



