Submitted:
20 January 2025
Posted:
20 January 2025
You are already at the latest version
Abstract
Background/Objectives: Ataxia is quite common in pediatric neuromotor disorders and with highly heterogeneous etiology. Mobility difficulties and functional limitations reflect the lack of coordination in this population. The aim of this study is to assess the effectiveness of an intensive program of functional partial body weight support treadmill training (FPBWSTT) on mobility and functionality of children with ataxia. Methods: Through a stratified randomized control trial, a sample of 18 children with progressive and non-progressive ataxia and GMFCS II-IV (mean age: 14 years, standard deviation: 2.5) was assessed prior, post-intervention, and 2 months after its end. Motor and functional skills were assessed with Gross Motor Function Measure (GMFM, items D-E), Pediatric Balance Scale (PBS), 10-meter walk test (10MWT), 6min-walk test (6MWT), Scale for Assessment and Rating Ataxia (SARA), Timed-Up and Go (TUG) test, spatiotemporal gait parameters, kinetic and kinematic variables of pelvis and lower limb. Results: Statistically significant interactions and changes in favor of the FPBWSTT were found in all functional assessments and spatiotemporal gait parameters (p0.05), while kinetic variables were insufficiently collected and were not statistically analyzed. Conclusions: The FPBWSTT is more effective on mobility and functionality of children with ataxia, 8-18 years old, compared to typical physiotherapy. The kinematic variables may not be sensitive indicators of change over a short period of time and/or in this population.
Keywords:
functional
; treadmill training
; partial body weight support
; children
; ataxia
1. Introduction
Ataxia in childhood is a clinical manifestation of neuromotor disorders, the occurrence of which is estimated at about 26/100,000 children in Europe and probably reflects a minimum prevalence worldwide [1]. In many countries, including Greece, official data on the prevalence of ataxia in the pediatric population is lacking, while both assessment and intervention strategies seem to have been poorly studied worldwide[2].
The pathogenesis of childhood ataxia is characterized by great heterogeneity, with progressive and non-progressive cerebellar ataxia being its two main types [3]. The causes of this movement disorder can be acquired, such as cerebellar tumor; congenital, such as cerebral palsy; or genetic, such as Friedrich's ataxia [3]. European data show that the highest incidence of ataxia in children is overall ataxia of genetic origin (14.61/100,000 births), while ataxia as a result of CP is the most studied in Europe and the most frequent among non-progressive disorders (10.65/100,000 births) [1]. In accordance with European data, a recent Greek cross-cultural adaptation [4] of the Scale for Assessment and Rating Ataxia (SARA) [5] found a rate of 54.4% of ataxic cerebral palsy and a rate of 62.5% of Friedrich ataxia in the non-progressive and progressive ataxia categories respectively.
The symptoms of ataxia refer to a set of difficulties expressed in each type and etiology of ataxia with different expression in the level of severity and limitations in daily activities [6]. Lack of balance and coordination are the primary difficulties, evident in the quality and quantity of daily activities where children interact. Ataxic gait, dysmetria, dysdiadochokinesia, tremor, nystagmus, dysarthria are some of the key clinical features underlying the symptomatology of cerebellar ataxia, regardless of its etiology [7-9]. According to Hartley et al. [2], investigating the assessment and treatment of children with various types of ataxia, it appeared that over forty different outcome measures were used in the twenty studies included in the systematic review. The majority of these studies focused on balance, gait and gross motor function, identifying gait performance as a basic physiotherapy goal. The few data existing from children with ataxia report reduced cadence, step and stride length, increased step width, variability in gait measures and abnormalities in motor and kinematic characteristics [10-13]. These factors may serve as sensitive indicators of the progression of the ataxia, but also indicate the “instability” of the ataxic gait pattern among the heterogeneity of the population investigated [10-13]. However, it seems that gait performance and parameters’ changes in the pediatric population of ataxia after physiotherapy intervention have been poorly studied, and mainly short-term time frames[2].
Treadmill interventions with and without partial body weight support are suggested as a mean of faster gait acquisition, gross motor and gait parameters’ improvement in pediatric populations with various neuromotor disorders. However, the application of different protocols in different neuromotor populations, coupled with the small sample sizes fail to demonstrate a clear and effective guideline[2,14-17]. An important factor of therapeutic effectiveness is the dosage of training varying in intensity (eg, treadmill speed, incline) or duration[17], prompting the need to standardize and test protocols appropriately designed for specific pediatric populations. The strategy of increasing speed during gait training has been well documented with positive results, but speed alternations, as suggested by Bjornson et al. [18] for children with CP, are so far a rather "challenging" approach, worthy of investigation, especially in ataxia. Cerebellum, the main dysfunctional structure resulting in ataxia, has a regulatory role in gait speed control and its activation during such challenging gait training [19] may be a promising therapeutic intervention. Another suggested therapeutic strategy recorded in adults with neuromotor deficits [20,21] and pediatric populations[22,23] seems to be dual task training, which defines a functional and demanding approach, especially when combined with gait, capable of promoting neuroplasticity[24].
Through this study we aim to investigate a novel functional intervention through integration of different therapeutic approaches, suggested by the literature and adequately adjusted to the pediatric population with ataxia. We anticipate that this study will offer further clinical practical and research suggestions and a better understanding for future therapeutic purposes.
2. Materials and Methods
A stratified randomized controlled trial of a 4-week Functional Partial Body Weight Support Treadmill Training (FPBWSTT) with a 2-month follow-up period was applied to children with ataxia (progressive and non-progressive), aged 8-18 years and GMFCS II-IV. The protocol of the study was applied as was published in March 2022 [25] and following ethical approval from the University of West Attica (study’s protocol: 14η/26-04-2021) and ‘ATTIKON’ General University Hospital of Athens (study’s protocol: Γ ΠAΙΔ, ΕΒΔ 149/20-3-2020) (Supplementary Material).
Participants’ recruitment started in June 2021 and was finally completed in the middle of December 2022, with last data collected in the end of March 2023. The proposed sample size estimation could not been verified with the completion of 5 children per group, as was initially scheduled[25], due to the large heterogeneity among participants at that time period. Despite the fact that an interim statistical analysis was not planned in the design of the protocol, in March 2023, with available data from a total of 18 children with ataxia, a calculation of the primary end point of the GMFM-D was performed, indicating statistically significant differences, which safely led to the adjustment of the sample size and therefore the termination of further sample search [26].
Two- way mixed ANOVA was used for estimating the interaction between intervention and time for all variables. One factor repeated measures ANOVA was used for estimating time measurement variation in each group, while pairwise multiple comparisons were examined through Bonferroni test. Sensitivity analysis was performed for estimation of both percentage and absolute change from baseline to all time assessments, between the two groups, through t-test and ANCOVA model, respectively.
3. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
3.1. Participant characteristics
Thirty five (35) children with ataxia were assessed according to the eligibility criteria. A total of 21 children were randomized to either the experimental or the control group, as shown in the Figure 1. The data from 18 children were finally collected and statistically analyzed, from which only 9 children completed the 3d gait analysis in all three assessment periods. Those data were processed to statistical analysis. The two groups were similar at baseline, in all clinical and demographic features, as well as in their perception of quality of life issues, as shown in Table 1.
3.2. Primary outcomes: Domains D and E of the GMFM-88(%)
The FPBWSTT group was statistically significant improved in GMFM domains D (standing) and E (gait) at 4 weeks by a mean of 6.45% (95% CI 3.34-9.57, p<0.001) for standing and by a mean of 4.68% (95% CI 1.66-7.70, p=0.005) for gait, compared to the control group. These improvements were also maintained at follow- up, by a mean of 5.56% (95% CI 1.46-9.67, p=0.011) and by a mean of 8.51% (95% CI 2.91-14.11, p=0.005) compared to the control group, respectively. Gross motor functionality of standing and gait changed significantly through time for the FPBWSTT group (p<0.005), but no significant changes were found for the control group (p>0.05). This is reinforced by the significant interaction of the groups and time for both variables (p=0.002), as shown in Figure 2 and Figure 3 respectively.
3.3. Secondary outcomes
Analysis of the data of secondary outcome measures are presented in Table 2, showing that in most of them the FPBWSTT group had statistically significant improvement (p<0.05) at four weeks, compared to the control group. The intervention group maintained their improvements in the PBS, 6MWT and spatiotemporal gait parameters at follow- up, as shown in Table 2 and Figure 5. There were baseline differences between the groups, both in stride and step length, with greater values obtained in the control group (Table 3). Interestingly, the slow self-paced 10MWT did not show statistically significant improvement at 4 weeks (mean:0.07m/s, 95% CI -0.04/0.18, p>0.05) and at follow-up (mean:0.05m/s, 95% CI -0.05/0.15, p=0.307), for the FPBWSTT group. This was in stark contrast to the fast self-selected pace of gait at 4 weeks, in which the intervention group showed statistically significant improvement, by a mean of 0.19m/s (95% CI 0.00-0.38, p=0.046).
Percentage change in 4-weeks and 2 months of primary and secondary outcomes of all participants is presented respectively in Figure 4 and Figure 5.
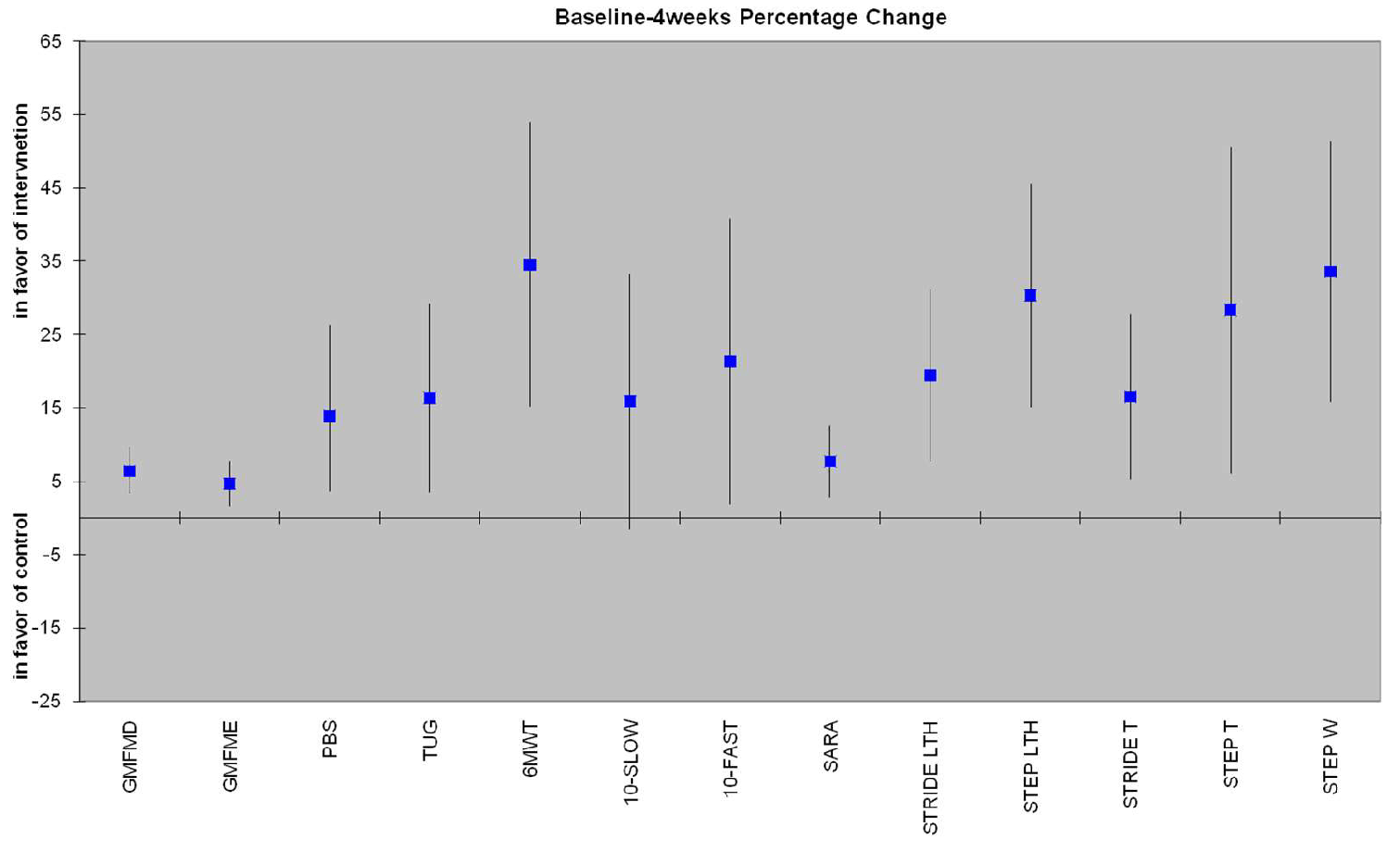
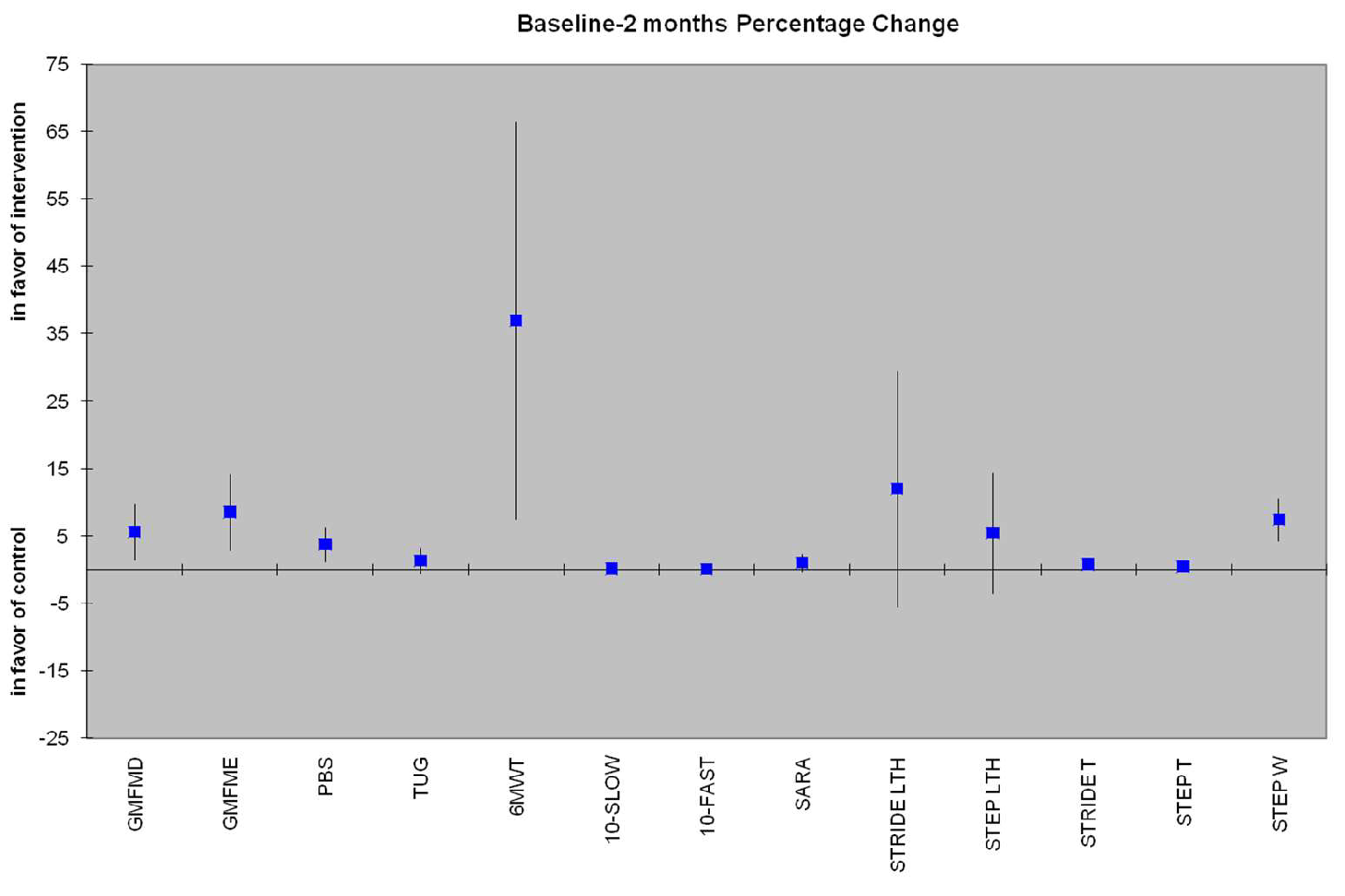
Figure 4.
Percentage change from baseline to 4 weeks of all variables in which all 18 children were assessed. All changes are statistically significant (p<0.05), in favor of the experimental group, except for 10MWT-SLOW, which is marginally statistically significant (p=0.072).
Figure 4.
Percentage change from baseline to 4 weeks of all variables in which all 18 children were assessed. All changes are statistically significant (p<0.05), in favor of the experimental group, except for 10MWT-SLOW, which is marginally statistically significant (p=0.072).
Figure 5.
Percentage change from baseline to 2 months of all variables in which all 18 children were assessed. Most changes were still statistically significant (p<0.05), in favor of the experimental group, except for TUG, 10MWT-SLOW, 10MWT-FAST and SARAgr.
Figure 5.
Percentage change from baseline to 2 months of all variables in which all 18 children were assessed. Most changes were still statistically significant (p<0.05), in favor of the experimental group, except for TUG, 10MWT-SLOW, 10MWT-FAST and SARAgr.
3.3.1. Secondary variables from 3D Analysis
3D Analysis was obtained only in a total of 9 children (FPBWSTT group n=5, control group n=4). Kinetic variables were inadequately collected, due to the insufficient placing of the entire foot or due to the coexistence of both feet on the platform during gait.
The values of kinematic variable of pelvis in sagittal plane were highly heterogeneous with extreme values and given the small sample size the statistical analysis of this variable was excluded, as no valid result could be attributed[27]. There were no statistical significant differences between the groups and there were no statistically significant changes for neither of the groups in all kinematic variables analyzed.
4. Discussion
The results of the clinical study, alongside the compliance to the protocol and the absence of adverse effects, indicate that the FPBWSTT can be a highly effective intensive program for children, 8-18 years old with moderate functional severity of ataxia, more than typical physical therapy. The significant improvements in gross motor function in the areas of standing and walking were accompanied with similar changes in ataxia symptoms, functional balance skills, gait speed, dynamic balance control, physical condition and endurance and spatiotemporal gait parameters in favor of the FPBWSTT group, the majority of which were sustained two months after the end of the intensive program. The collection and statistical analysis of the kinematic variables of the 3D gait analysis did not reveal significant differences between groups and neither significantly changed in any of the two groups between the different time measurements. Those findings may indicate that such measurements may not be sensitive enough for detecting functional changes in the specific population and/or at such short time frame.
Children in both groups had similar clinical and demographic features. Confounding factors that could affect the outcome as well as the interpretation of the results, were taken into account through the admission and exclusion criteria of the participants, as well as their recruitment, based on stratification of the type of disorder:each group had one participant with progressive type of ataxia and GMFCS IV, while the remaining participants belonged to the non-progressive ataxia category, between GMFCS II-III. Children who had undergone surgical resection of the posterior fossa tumor (neuroblastoma) as well as the child with ataxia as a result of traumatic brain injury, all had far exceeded the time frame for spontaneous recovery of balance ability, determined to be up to one year [28].
According to the results of the present study, the children who completed the FPBWSTT significantly improved in gross motor function particularly in standing and walking after the end of the intensive program, which were maintained at follow-up. At the same time, statistically significant differences emerged between the two groups in the changes from the initial measurement, both after the end of the 4-week period and after the 2-month period. The domains of standing (domain D) and walking (domain E) in gross motor function, according to the GMFM, are the most representative domains of motor difficulties in children and youth with CP [29,30], as well as in children with ataxia [2,12].
The findings of the present study are even more encouraging than the reference range of 0.8%-5.2% and 2.3%-6.5% suggested by Storm et al. [31] as a Minimum Clinically Important Difference (MCID) for the improvement of GMFM-D in children with cerebral palsy and TBI, respectively, after one month of robotic gait training. Accordingly, the reference range of clinically significant difference for GMFM-E varies from 0.3%-4.9% for children with CP and 2.8%-6.5% for children with TBI. Specifically, in the study there was a total of 182 children, aged 4–18 years with movement disorders as a result of CP and TBI, who followed 20 sessions of 45minutes of each gait training and typical physical therapy (total 90-min session) over a 4 week period [31].
In the present study, the change in gross motor function in standing position after the end of 4 weeks was 6.81% for FPBWSTT group and only 0.35% for the control group, while the change in gross motor function in gait was 5.30% for FPBWSTT and only 0.62% for the control group. Those findings are in accordance with the pilot study of Peri et al. [12] which investigated the effects of a 4week gait training program in 11 children with ataxia due to TBI and additionally reinforce the clinical significance of gross motor function change in standing and gait domains, in such short time frame. An interesting point found in the present study and confirmed through the research of Peri et al. [12] is that both programs focused on gait training produced greater changes in standing gross mobility than gait. In other words, what is evident is that even if there are no exercises focused on static and dynamic standing skills, gait training contributes significantly to the enhancement of gross motor function in standing.
The exact same trend of change, similar to GMFM-D was found for the PBS, with a clinical significant change, based on proposed reference range after a 6 month period for children with CP up to 6.5 years old [32]. The same study showed a strong correlation between total score of GMFM-66 and PBS. Based on our findings GMFM-D and PBS share common characteristics with a trend change consistent with basic principles of neuroplasticity[33], as practicing a motor activity promotes a type of transfer to the acquisition and improvement of similar activities to the one being trained. It appears that gait training, as a functional activity, and the way in which speed alternations and dual-task functional activities were combined, were able to promote simultaneous or subsequent changes, through a network of neural circuits for other functional activities, in addition to those of gait. Motor training alone is capable of activating angiogenic mechanisms in the motor cortex, cerebellum and promoting the growth and survival of neurons in many brain regions [33,34]. The activity of gait involves activation of somatosensory and motor areas of the whole body and the application of FPBWSTT through both speed and dual-task challenges appears to be sufficiently able of promoting the appropriate synaptic connections and form a fertile environment to support structural brain changes related to standing functional activities.
A statistically and clinically significant difference was also found for gross motor function in gait (GMFM-E), with an interesting continuous improvement observed 2 months after the end of the FPBWSTT. This finding could be due to a possible increase in the relevant daily activities of the children who completed the FPBWSTT as a “habit” formed as a result of the intensive gait program. As supported by theories and research on motor learning, neuroplasticity is an ongoing process, rather than a single record [33]. The consolidation of a motor behavior involves time and repetition that often depend on the time period after the end of the motor training [33], which could explain the continuous increase of GMFM-E, 2 months after the end of the training. Unfortunately, this remains an assumption, based on theoretical knowledge which cannot be directly correlated with other studies, which investigated short-term and post intervention results or GMFM total score of all domains [2].
The change of ataxic symptoms was only significant just after the end of the 4-week program for the FPBWSTT group, without reaching the minimum clinically important difference, reported in adult studies [35,36] and pediatric population [12,37]. It is possible that further clinical reduction of SARA score can be achieved by a more targeted therapeutic approach on functional activities, related to the ataxic signs and increased time practice, as the cerebellum, the main responsible structure causing ataxia requires sufficient temporal processing [34].
Improvements in dynamic balance control following various applications of therapeutic protocols have been reported in children with ataxia with reference in fall risk reduction and functional mobility skills’ improvement [2]. However, the heterogeneity of study protocols in the measurement of TUG and the need of chronological age correlation with a standard reference value [38] restrict the clinical interpretation of TUG’s change seen in the present study. Nevertheless, the improvement and significant change found for the FPBWSTT compared to the control group at 4-weeks indicates the child's developing functional independence [39]. This is reinforced by the improvements of self-selected pace and the significant change of 10MWT-fast, which further points out the ability of adjusting and regulating gait speed, an extremely difficult condition for people with cerebellum deficits [19].Besides the above, the increase of gait speed found for the FPBWSTT is even more apparent in the way that 6MWT changed. Even though 6MWT measures physical condition and endurance, it has been widely used informally for walking speed calculation in children with CP [40], while strong correlation with 10MWT has been supported in adults with neurological deficits [41]. Based on the increased 46,25m with the end of the FPBWSTT, a similar in population, duration and type of intervention study [12] has identified an improvement of 48m post the 4-week gait training. These findings may verify an important reference range for the functional improvements of children with ataxia, after a 4-week, 20 sessions training.
Children who underwent the FPBWSTT significantly reduced their step width at all time periods showing statistically significant changes respectively, compared to children who received their standard program. Despite the fact that children of the FPBWSTT group had significantly shorter stride and stride lengths compared to the control group at baseline, there was a statistically significant increase of their stride and step length after 4 weeks, in contrast to children of the control group who demonstrated even a decline in those gait variables. However, from the absolute changes only that of step length at 4 weeks was statistically significantly improved. The increase in stride length continued further even 2 months after the end of FBPWSTT, while step length showed a slight decrease. This may be due to an increased variability of steps with non-symmetrical bilateral steps at the given time point. In the systematic review by Buckley et al. [10] regarding gait characteristics in adults with ataxia, increased variability of stride length, but not of step length, has been reported at low speeds compared to higher speeds. Given the above, this finding could be due to the difficulty of adapting gait to a walking speed lower than what has now been achieved, as the speed of evaluation of all spatiotemporal characteristics in all three time periods was the same (75%–80% of low self-selected baseline ground speed).
The overall spatiotemporal gait changes are of particular importance, as they highlight an adapting ability and the possibility of adopting a new gait strategy within the same gait speed. Increased step and stride time characterize ataxic gait compared to typical values of adults and children [10,12]. According to the present findings, what theoretically appears as a worsening actually reveals the adaptation of the gait pattern in order to maintain the same pace. It seems that temporal gait variables acted as a compensatory index to maintain walking pace, when spatial parameters (step and stride length) were increased as a result of the FPBWSTT program. This adaptation skill is a well established indicator of improved motor functionality [42].
Kinematic changes
According to current data, joint mobility in children with ataxia has been assessed in relation to the maximum trajectory range achieved during gait, expressed in degrees, compared to a healthy population [12,13] and immediately after gait training [12]. The assessment of the maximum range of motion at a joint and whether this is close to standard reference values is not necessarily an indication of improvement, as it is unknown whether this range of motion is utilized at the appropriate time, during gait. The use of the MGDI index seems to reflect the deviation between the pathological and typical gait, as it is calculated in such way that estimates and compares the absolute value of each momentary deviation with the corresponding value of normal data [43].To our knowledge, the present study is the first in this population to assess changes in mean joint mobility deviations throughout the gait cycle, as derived from standard gait analysis values, relative to a control group and in long term.
During 3D gait analysis of the 9 children, there was inability to collect the kinetic variables, due to incorrect and insufficient placement of the foot on the force recording platform. Additionally, there was a great heterogeneity with extreme values in the kinematic of pelvis in sagittal plane, an observation confirmed in adults with ataxia [44,45].The instability of the trunk and pelvis in all directions of movement and especially in sagittal plane seems to be particularly pronounced in adults with ataxia, maybe due to an effort to maintain an energy-efficient gait [44,45]. In a similar study of Peri et al. [12] changes in pelvic kinematics measured by maximal range of motion after a 4-week gait training showed greater in deviation values from the normal reference ones and increased standard deviation, following a different course of change than the otherwise functional improvements of the participants. It seems that pelvis kinematics’ deterioration or even variability may be part of an effort for trunk stability in a newly adopted gait strategy.
All other kinematic variables did not show a specific change trend in any of the two groups, which differs from the findings reported by Peri et al. [12]. The latter argue that changes in knee and ankle mobility close to standard values may be indicators of the effectiveness of a therapeutic program. The pilot study of Peri et al. [12] applied 20 sessions of typical physiotherapy alongside with the 20 sessions of gait training, which aimed to improve balance skills and correct the movement pattern. On the other hand, in the present study neither the standard physiotherapy nor FPBWSTT specifically focused on "correction" or facilitation techniques aimed at improving joint mobility. Changes in some kinematic variables could be expected at over a longer time period, perhaps as an indication of a "consolidated" gait, without being clear whether these changes will align with the reference standard values. What needs further clarification is whether these variables are associated with functional improvements in this population and whether physiotherapy should aim in “correction” of those.
5. Conclusions
In overall, it seems that FPBWSTT is a feasible physiotherapy program, more effective than typical physiotherapy, with statistically and clinically significant improvements in the mobility and functionality of children with ataxia. The FPBWSTT positively influenced children with ataxia by producing changes in standing and walking gross motor function, clinical signs of ataxia, functional skills and dynamic balance control, gait cadence, physical condition and endurance, and improvement and adjustment of spatiotemporal parameters of gait, most of which were remained even 2 months after the end of the program. However, the kinematic variables did not demonstrate a consistent trend of change, suggesting that these parameters may not be sensitive indicators in the identification of functional improvements over short time periods, in small samples or in reference to the specific population.
Supplementary Materials
The following supporting information refers to the study protocol and can be downloaded at: DOI: 10.1136/bmjopen-2021-056943
Author Contributions
Conceptualization: AL, SL and VS; Methodology: AL, SL, VS, MP and AG; Software: AL, GG and AG; Validation: VS; Formal Analysis: AL and AG; Investigation: AL, GG and MT; Resources: AL; Data Curation: AL, AG and VS; Writing-Original Draft Preparation: AL; Writing-Review & Editing: AL, SL, MP and VS; Visualization: AL; Supervision: VS; Project Administration: AL; Funding Acquisition: -.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the University of West Attica (study’s protocol: 14η/26-04-2021) and the Review Board of ‘ATTIKON’ General University Hospital of Athens (study’s protocol: Γ ΠAΙΔ, ΕΒΔ 149/20-3-2020).
Informed Consent Statement
Written informed consent was obtained from all participants involved in the study. Parents and children above the age of 16 years old were asked to sign the consent form.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We are deeply grateful to all children and their families who spent some of their time participating to the research study, during a difficult period with covid pandemic. We would also like to thank all the colleagues for their help in the sample search and especially those from the pediatric faculty "Motivation and Movement: Child’s Functional Therapy" for their valuable contribution and support to the research process.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Musselman, K.E.; Stoyanov, C.T.; Marasigan, R.; Jenkins, M.E.; Konczak, J.; Morton, S.M.; Bastian, A.J. Prevalence of ataxia in children: a systematic review. Neurology 2014, 82, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Hartley, H.; Cassidy, E.; Bunn, L.; Kumar, R.; Pizer, B.; Lane, S.; Carter, B. Exercise and Physical Therapy Interventions for Children with Ataxia: A Systematic Review. Cerebellum 2019, 18, 951–968. [Google Scholar] [CrossRef] [PubMed]
- Pavone, P.; Praticò, A.D.; Pavone, V.; Lubrano, R.; Falsaperla, R.; Rizzo, R.; Ruggieri, M. Ataxia in children: early recognition and clinical evaluation. Ital J Pediatr. 2017, 43, 6. [Google Scholar] [CrossRef] [PubMed]
- Lepoura, A.; Lampropoulou, S.; Galanos, A.; Papadopoulou, M.; Sakellari, V. Scale for Assessment and Rating Ataxia (SARA) in Children with Ataxia: Greek Cultural Adaptation and Psychometric Properties. Open Access Journal of Neurology & Neurosurgery 2023, 18, e555976. [Google Scholar]
- Schmitz-Hübsch, T.; du Montcel, S.T.; Baliko, L.; Berciano, J.; Boesch, S.; Depondt, C.; Giunti, P.; Globas, C.; Infante, J.; Kang, J.S.; Kremer, B.; Mariotti, C.; Melegh, B.; Pandolfo, M.; Rakowicz, M.; Ribai, P.; Rola, R.; Schöls, L.; Szymanski, S.; van de Warrenburg, B.P.; Dürr, A.; Klockgether, T.; Fancellu, R. Scale for the assessment and rating of ataxia: development of a new clinical scale. Neurology. 2006, 66, 1717–1720. [Google Scholar] [CrossRef]
- Pinto, W.B.; Pedroso, J.L.; Souza, P.V.; Albuquerque, M.V.; Barsottini, O.G. Non-progressive cerebellar ataxia and previous undetermined acute cerebellar injury: a mysterious clinical condition. Arq Neuropsiquiatr. 2015, 73, 823–827. [Google Scholar] [CrossRef]
- Panzeri, D.; Bettinelli, M.S.; Biffi, E.; Rossi, F.; Pellegrini, C.; Orsini, N.; Recchiuti, V.; Massimino, M.; Poggi, G. Application of the Scale for the Assessment and Rating of Ataxia (SARA) in pediatric oncology patients: A multicenter study. Pediatr Hematol Oncol. 2020, 37, 687–695. [Google Scholar] [CrossRef]
- Sullivan, R.; Yau, W.Y.; O'Connor, E.; Houlden, H. Spinocerebellar ataxia: an update. J Neurol. 2019, 266, 533–544. [Google Scholar] [CrossRef]
- Steinlin, M. Non-progressive congenital ataxias. Brain Dev. 1998, 20, 199–208. [Google Scholar] [CrossRef]
- Buckley, E.; Mazzà, C.; McNeill, A. A systematic review of the gait characteristics associated with Cerebellar Ataxia. Gait Posture. 2018, 60, 154–163. [Google Scholar] [CrossRef]
- Milne, S.C.; Hocking, D.R.; Georgiou-Karistianis, N.; Murphy, A.; Delatycki, M.B.; Corben, L.A. Sensitivity of spatiotemporal gait parameters in measuring disease severity in Friedreich ataxia. Cerebellum. 2014, 13, 677–688. [Google Scholar] [CrossRef] [PubMed]
- Peri, E.; Panzeri, D.; Beretta, E.; Reni, G.; Strazzer, S.; Biffi, E. Motor Improvement in Adolescents Affected by Ataxia Secondary to Acquired Brain Injury: A Pilot Study. Biomed Res Int. 2019, 2019, 8967138. [Google Scholar] [CrossRef] [PubMed]
- Vasco, G.; Gazzellini, S.; Petrarca, M.; Lispi, M.L.; Pisano, A.; Zazza, M.; Della Bella, G.; Castelli, E.; Bertini, E. Functional and Gait Assessment in Children and Adolescents Affected by Friedreich's Ataxia: A One-Year Longitudinal Study. PLoS One. 2016, 11, e0162463. [Google Scholar] [CrossRef]
- Damiano, D.L.; DeJong, S.L. A systematic review of the effectiveness of treadmill training and body weight support in pediatric rehabilitation. J Neurol Phys Ther. 2009, 33, 27–44. [Google Scholar] [CrossRef]
- Molina-Rueda, F.; Aguila-Maturana, A.M.; Molina-Rueda, M.J.; Miangolarra-Page, J.C. Pasarelarodante con o sin sistema de suspension del peso corporal enninos con paralisis cerebral infantil: revision sistematica y metaanalisis [Treadmill training with or without partial body weight support in children with cerebral palsy: systematic review and meta-analysis]. Revista de Neurologia. 2010, 51, 135–145. [Google Scholar]
- Qian, G.; Cai, X.; Xu, K.; Tian, H.; Meng, Q.; Ossowski, Z.; Liang, J. Which gait training intervention can most effectively improve gait ability in patients with cerebral palsy? A systematic review and network meta-analysis. Front Neurol. 2023, 13, 1005485. [Google Scholar] [CrossRef]
- Valentin-Gudiol, M.; Bagur-Calafat, C.; Girabent-Farrés, M.; Hadders-Algra, M.; Mattern-Baxter, K.; Angulo-Barroso, R. Treadmill interventions with partial body weight support in children under six years of age at risk of neuromotor delay: a report of a Cochrane systematic review and meta-analysis. Eur J Phys Rehabil Med. 2013, 49, 67–91. [Google Scholar]
- Bjornson, K.F.; Moreau, N.; Bodkin, A.W. Short-burst interval treadmill training walking capacity and performance in cerebral palsy: a pilot study. Dev Neurorehabil. 2019, 22, 126–133. [Google Scholar] [CrossRef]
- Hamacher, D.; Herold, F.; Wiegel, P.; Hamacher, D.; Schega, L. Brain activity during walking: A systematic review. Neurosci Biobehav Rev. 2015, 57, 310–327. [Google Scholar] [CrossRef]
- San Martín Valenzuela, C.; Moscardó, L.D.; López-Pascual, J.; Serra-Añó, P.; Tomás, J.M. Effects of Dual-Task Group Training on Gait, Cognitive Executive Function, and Quality of Life in People With Parkinson Disease: Results of Randomized Controlled DUALGAIT Trial. Arch Phys Med Rehabil. 2020, 101, 1849–1856e1. [Google Scholar] [CrossRef]
- Yang, Y.R.; Chen, Y.C.; Lee, C.S.; Cheng, S.J.; Wang, R.Y. Dual-task-related gait changes in individuals with stroke. Gait Posture. 2007, 25, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Elhinidi, E.I.; Ismaeel, M.M.; El-Saeed, T.M. Effect of dual-task training on postural stability in children with infantile hemiparesis. J Phys Ther Sci. 2016, 28, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.Y.; Lee, E.J.; Kwon, H.Y. The effects of dual-task training on balance and gross motor function in children with spastic diplegia. J Exerc Rehabil. 2021, 17, 21–27. [Google Scholar] [CrossRef]
- Koch, I.; Poljac, E.; Müller, H.; Kiesel, A. Cognitive structure, flexibility, and plasticity in human multitasking-An integrative review of dual-task and task-switching research. Psychol Bull. 2018, 144, 557–583. [Google Scholar] [CrossRef]
- Lepoura, A.; Lampropoulou, S.; Galanos, A.; Papadopoulou, M.; Sakellari, V. Study protocol of a randomised controlled trial for the effectiveness of a functional partial body weight support treadmill training (FPBWSTT) on motor and functional skills of children with ataxia. BMJ Open. 2022, 12, e056943. [Google Scholar] [CrossRef]
- Herson, J.; Wittes, J. The Use of Interim Analysis for Sample Size Adjustment. Drug Information Journal. 1993, 27, 753–760. [Google Scholar] [CrossRef]
- Kwak, S.K.; Kim, J.H. Statistical data preparation: management of missing values and outliers. Korean J Anesthesiol. 2017, 70, 407–411. [Google Scholar] [CrossRef]
- Küper, M.; Döring, K.; Spangenberg, C.; Konczak, J.; Gizewski, E.R.; Schoch, B.; Timmann, D. Location and restoration of function after cerebellar tumor removal-a longitudinal study of children and adolescents. Cerebellum. 2013, 12, 48–58. [Google Scholar] [CrossRef]
- Dodd, K.J.; Taylor, N.F.; Graham, H.K. A randomized clinical trial of strength training in young people with cerebral palsy. Dev Med Child Neurol. 2003, 45, 652–657. [Google Scholar] [CrossRef]
- Mattern-Baxter, K.; McNeil, S.; Mansoor, J.K. Effects of home-based locomotor treadmill training on gross motor function in young children with cerebral palsy: a quasi-randomized controlled trial. Arch Phys Med Rehabil. 2013, 94, 2061–2067. [Google Scholar] [CrossRef]
- Storm, F.A.; Petrarca, M.; Beretta, E.; Strazzer, S.; Piccinini, L.; Maghini, C.; Panzeri, D.; Corbetta, C.; Morganti, R.; Reni, G.; Castelli, E.; Frascarelli, F.; Colazza, A.; Cordone, G.; Biffi, E. Minimum Clinically Important Difference of Gross Motor Function and Gait Endurance in Children with Motor Impairment: A Comparison of Distribution-Based Approaches. Biomed Res Int. 2020, 2020, 2794036. [Google Scholar] [CrossRef]
- Chen, C.L.; Shen, I.H.; Chen, C.Y.; Wu, C.Y.; Liu, W.Y.; Chung, C.Y. Validity, responsiveness, minimal detectable change, and minimal clinically important change of Pediatric Balance Scale in children with cerebral palsy. Res Dev Disabil. 2013, 34, 916–922. [Google Scholar] [CrossRef] [PubMed]
- Kleim, J.A.; Jones, T.A. Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. J Speech Lang Hear Res. 2008, 51, S225–S239. [Google Scholar] [CrossRef] [PubMed]
- Nichols-Larsen DS, Kegelmeyer DA, Buford JA, Kloos AD, Heathcock JC, Michele Basso D. Neurologic Rehabilitation : Neuroscience and Neuroplasticity in Physical Therapy Practice. McGraw-Hill Education; 2016.
- Schatton, C.; Synofzik, M.; Fleszar, Z.; Giese, M.A.; Schöls, L.; Ilg, W. Individualized exergame training improves postural control in advanced degenerative spinocerebellar ataxia: A rater-blinded, intra-individually controlled trial. Parkinsonism Relat Disord. 2017, 39, 80–84. [Google Scholar] [CrossRef]
- Schmitz-Hübsch, T.; Fimmers, R.; Rakowicz, M.; Rola, R.; Zdzienicka, E.; Fancellu, R.; Mariotti, C.; Linnemann, C.; Schöls, L.; Timmann, D.; Filla, A.; Salvatore, E.; Infante, J.; Giunti, P.; Labrum, R.; Kremer, B.; van de Warrenburg, B.P.; Baliko, L.; Melegh, B.; Depondt, C.; Schulz, J.; du Montcel, S.T.; Klockgether, T. Responsiveness of different rating instruments in spinocerebellar ataxia patients. Neurology. 2010, 74, 678–684. [Google Scholar] [CrossRef]
- Ilg, W.; Schatton, C.; Schicks, J.; Giese, M.A.; Schöls, L.; Synofzik, M. Video game-based coordinative training improves ataxia in children with degenerative ataxia. Neurology. 2012, 79, 2056–2060. [Google Scholar] [CrossRef]
- Verbecque, E.; Schepens, K.; Theré, J.; Schepens, B.; Klingels, K.; Hallemans, A. The Timed Up and Go Test in Children: Does Protocol Choice Matter? A Systematic Review. Pediatr Phys Ther. 2019, 31, 22–31. [Google Scholar] [CrossRef]
- Nicolini-Panisson, R.D.; Donadio, M.V. Timed "Up & Go" test in children and adolescents. Rev Paul Pediatr. 2013, 31, 377–383. [Google Scholar]
- Fitzgerald, D.; Hickey, C.; Delahunt, E.; Walsh, M.; OʼBrien, T. Six-Minute Walk Test in Children With Spastic Cerebral Palsy and Children Developing Typically. Pediatr Phys Ther. 2016, 28, 192–199. [Google Scholar] [CrossRef]
- Cheng, D.K.; Nelson, M.; Brooks, D.; Salbach, N.M. Validation of stroke-specific protocols for the 10-meter walk test and 6-minute walk test conducted using 15-meter and 30-meter walkways. Top Stroke Rehabil. 2020, 27, 251–261. [Google Scholar] [CrossRef]
- Elder, G.C.; Kirk, J.; Stewart, G.; Cook, K.; Weir, D.; Marshall, A.; Leahey, L. Contributing factors to muscle weakness in children with cerebral palsy. Dev Med Child Neurol. 2003, 45, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Darras, N.; Tziomaki, M.; Pasparakis, D. Motion Graph Deviation Index (MGDI): An index that enhances objectivity in clinical motion graph analysis. ΕΕΧOΤ 2015, 67, 53–60. [Google Scholar]
- Matsushima, A.; Yoshida, K.; Genno, H.; Murata, A.; Matsuzawa, S.; Nakamura, K.; Nakamura, A.; Ikeda, S. Clinical assessment of standing and gait in ataxic patients using a triaxial accelerometer. Cerebellum Ataxias. 2015, 2, 9. [Google Scholar] [CrossRef] [PubMed]
- Chini, G.; Ranavolo, A.; Draicchio, F.; Casali, C.; Conte, C.; Martino, G.; Leonardi, L.; Padua, L.; Coppola, G.; Pierelli, F.; Serrao, M. Local Stability of the Trunk in Patients with Degenerative Cerebellar Ataxia During Walking. Cerebellum. 2017, 16, 26–33. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of the study according to the Consolidated Standards of Reporting Trials “CONSORT” guidelines, Paediatric center: private faculty for the evaluation of all the assessments beside the 3D: three-dimensional gait analysis at ELEPAP Athens.
Figure 1.
Flow chart of the study according to the Consolidated Standards of Reporting Trials “CONSORT” guidelines, Paediatric center: private faculty for the evaluation of all the assessments beside the 3D: three-dimensional gait analysis at ELEPAP Athens.
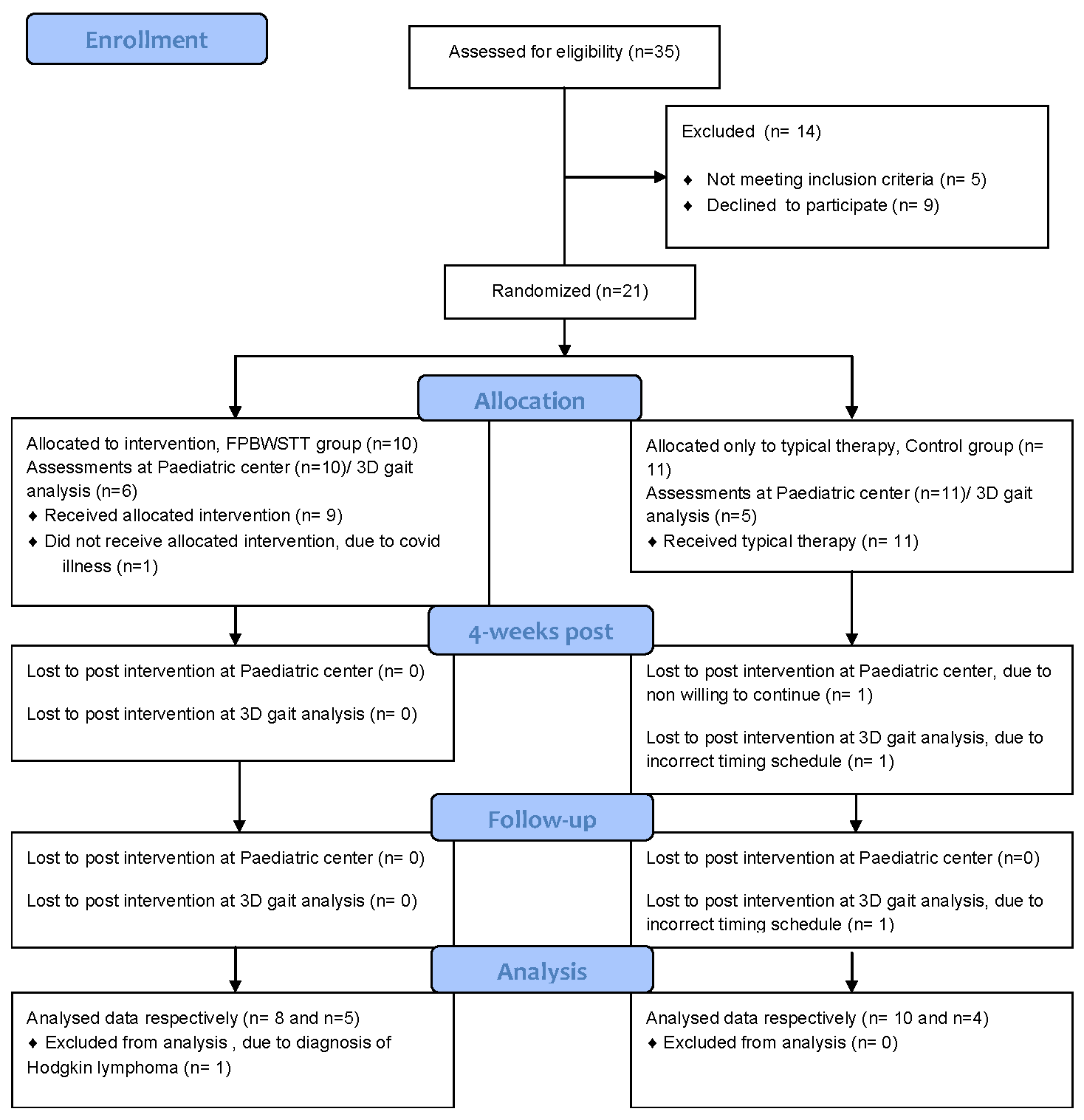
Figure 2.
Mean value of standing gross motor function (GMFM-D) of the two groups at baseline, 4 weeks and 2 months.
Figure 2.
Mean value of standing gross motor function (GMFM-D) of the two groups at baseline, 4 weeks and 2 months.

Figure 3.
Mean value of gait gross motor function (GMFM-E) of the two groups at baseline, 4 weeks and 2 months.
Figure 3.
Mean value of gait gross motor function (GMFM-E) of the two groups at baseline, 4 weeks and 2 months.


Table 1.
Comparison of demographic, clinical and quality of life characteristics between groups.
| Characteristics | FPBWSTT Group | Control Group | p-value |
| Age (years), mean±SD | 14.69±2.05 | 13.45±2.73 | 0.304 |
| Sex, male/female | 7(87.5%)/1(12.5%) | 7(70%)/3(30%) | 0.588 |
| Weight (kg), mean±SD | 41.56±8.79 | 46.55±14.53 | 0.407 |
| Height(cm), mean±SD | 157.38±11.17 | 151.90±14.67 | 0.397 |
| BMI, mean±SD | 16.86±2.20 | 19.72±3.56 | 0.058 |
| Type of ataxia, non-P/P | 7(87.5%)/1(12.5%) | 9(90%)/1(10%) | 1.000 |
| GMFCS, II/III/IV | 6(75%)/1(12.5%)/1(12.5%) | 7(70%)/2(20%)/1(10%) | 0.909 |
| Laterality, right/left | 8(100%)/0(0%) | 9(90%)/1(10%) | 1.000 |
| Child’s quality of life questionnaire | |||
| Friends-Family, mean±SD | 7.18±0.92 | 6.81±0.82 | 0.375 |
| Participation, mean±SD | 6.06±2.31 | 5.65±1.79 | 0.675 |
| Communication, mean±SD | 6.58±1.28 | 6.00±1.50 | 0.395 |
| Use of limbs, mean±SD | 5.99±1.78 | 6.23±1.62 | 0.683 |
| Self-care, median±IR | 7.00±0.0 | 7.00±0.0 | 0.537 |
| Equipment, mean±SD | 4.21±1.38 | 4.21±0.76 | 1.00 |
| Pain-discomfort mean±SD | 2.98±0,77 | 2.98±0.93 | 0.991 |
| Sense of happiness median±IR | 7.00±1.0 | 7.00±0.5 | 0.573 |
| Assistance with questionnaire completion, mean±SD | 2.38±1.06 | 2.40±1.07 | 0.961 |
Values are presented numerically, unless otherwise stated. There are no statistically significant differences between the two groups at the baseline assessment (p>0.05). Quality of life questionnaire scored on a Likert scale, from 1: bad - 9: very good., except for the last question with a choice of 1: no - 4: yes, very. FPBWSTT Group: Cerebral palsy ataxia(n=5)* [*subsequent genetic testing revealed a variant of CACNA1A (n=1)] , Neuroblastoma (n=1) [2 years since surgical resection of tumor], CACNA1A (n=1) (previous CP diagnosis), Friedreich Ataxian=1; Control Group.: Cerebral palsy ataxia (n=4), Neuroblastoma(n=1) [3.5 years since surgical resection of tumor], CACNA1A (n=1), Un-known reason ataxia (n=1), Gillespie syndrome (n=1), TBI ataxia (n=1) [6 years since the injury], Menkes-like ataxia (n=1).
Table 2.
Sensitivity Analysis Using ANCOVA Model (Baseline vs. 4-Week & 2-Month Outcomes).
| Secondary Outcome |
4-Week Mean Difference (95% CI) |
p-value | 2-Month Mean Difference (95% CI) | p-value2 |
| PBS | 3.73 (1.13 - 6.33) | 0.008 | 3.85 (-0.14 to 7.71) | 0.05 |
| TUG (sec) | 2.19 (0.7 - 3.67) | 0.007 | 1.29 (-0.53 to 3.10) | 0.151 |
| 10MWT-SLOW (m/sec) | 0.07 (0.04 - 0.18) | 0.193 | 0.05 (0.05 - 0.15) | 0.307 |
| 10MWT-FAST (m/sec) | 0.19 (0 - 0.38) | 0.046 | 0.04 (-0.12 to 0.21) | 0.620 |
| 6MWT (m) | 56.09 (29.22 - 82.96) | <0.005 | 36.92 (7.34 - 66.50) | 0.018 |
| SARAgr | 1.22 (0.44 - 2.01) | 0.005 | 1.00 (-0.31 to 2.34) | 0.125 |
| Step Length (cm) | 8.84 (1.67 - 16.01) | 0.019 | 5.36 (-3.64 to 14.35) | 0.224 |
| Stride Length (cm) | 8.29 (-3.98 to 20.57) | 0.170 | 12 (-5.52 to 29.54) | 0.165 |
| Step Time (sec) | 0.38 (0.01 - 0.74) | 0.043 | 0.45 (0.01 - 0.90) | 0.048 |
| Stride Time (sec) | 0.45 (0.16 - 0.75) | 0.005 | 0.77 (0.05 - 1.49) | 0.038 |
| Step Width (cm) | 6.74 (4.20 - 9.29) | <0.005 | 7.41 (4.18 - 10.64) | <0.005 |
Table 3.
Mixed two-way ANOVA for the STEP LENGTH and STRIDE LENGTH variables.
| STEP LENGTH | STRIDE LENGTH | ||||||
| Groups | Time | Time | |||||
| Baseline | 4-week | 2months | Baseline | 4-week | 2months | ||
| mean±SD | mean±SD | mean±SD | mean±SD | mean±SD | mean±SD | ||
| FPBWSTT | 22.85±7.56 | 28.19±8.69* | 27.49±8.65 | 47.72±12.74 | 54.79±14.69 | 58.16±18.66 | |
| Control | 38.01±7.04 | 35.99±9.63 | 32.88±7.00 | 72.29±17.77 | 68.51±18.27 | 64.57±16.63 | |
| Comparison between groups by time | p<0.005 | p=0.094 | p=0.163 | p=0.005 | p=0.104 | p=0.453 | |
| Interaction between group and time | F(2.32)=6.94, p<0.005 | F(2.32)=6.34, p=0.005 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



