
Submitted:
17 January 2025
Posted:
20 January 2025
You are already at the latest version
Abstract
As cases of Legionnaires’ disease increase worldwide, there is uncertainty on whether water management plans should focus on the measurement of Legionella species or specifically on L. pneumophila. This paper makes the case that, for public water systems and buildings, the target organism should be L. pneumophila as it is the overwhelming cause of illness, has simple methods for analysis, and remediation procedures avoid unnecessary costs that produce little public health benefit.
Keywords:
Legionella pneumophila
; Legionella species
; Legionnaires’ disease
; drinking water
; monitoring
; water management
; disinfection
1. Introduction
In the 2020 report “Management of Legionella in Water Systems,” the National Academy of Science, Engineering, and Medicine [1] indicates that the objectives of an environmental monitoring program for Legionella will dictate the choice of methods and the sample strategies (e.g., locations, frequency, and the type of sampling, including bulk water, biofilm, or aerosols). Testing objectives can be different for routine monitoring, assessments of treatment efficacy or remediation, outbreak investigations or for research. The report notes that the various approaches can differ in terms of quantification, assessment of viability, and the range of species detected. The report, however, makes no specific recommendation as to whether these programs should be directed at all Legionella species or more specifically at Legionella pneumophila, or even specific serogroups or sequency types. For outbreak investigations and research studies it is advantageous to use methods that detect a wider range of microbes, but for routine monitoring or treatment studies, it may be advantageous to target the analysis to the microbes of greatest concern. This specificity can be helpful to assess public health risk and avoid unneeded testing and remediation expense. The objective of this paper is to outline the case for monitoring L. pneumophila in public water systems and public buildings and to make the distinction between monitoring in health care settings.
2. Legionella Overview
Legionella is an aerobic, non-encapsulated, non-spore forming, Gram-negative bacterium. The genus Legionella currently includes more than 61 species and 3 subspecies, only half of which have been associated with human infections [2,3]. Therefore, it is incorrect to infer a public health threat from all Legionella species. Legionellae have a requirement for certain amino acids (cysteine) and iron – pointing to their role as intracellular parasites of free-living protozoa because the nutritional requirements for their growth would rarely be found in natural waters [4]. L. pneumophila has at least 16 serotypes.
Legionnaires’ disease is an acute, sometimes fatal (5-30%), infection primarily exhibited as pneumonia with fever, cough, shortness of breath, and myalgias (i.e., soreness or aching of the muscles) [1]. The majority of Legionnaires’ disease cases (from 80 to 90+ percent in Europe and the United States) are linked to L. pneumophila [5-9], and of these infections, Legionella pneumophila serogroup 1 is responsible for about 95% of the Legionnaires' disease cases in the United States [4]. Collier et al. [10] estimated that the hospital cost of a Legionnaires’ disease case was over $37,000 and the overall annual healthcare cost is over $400 million.
Table 1 shows the Legionella species isolated in the European Union in 2020 and demonstrated the preponderance of L. pneumophila infections [11]. L. pneumophila serogroup 1 accounted for 95% of the 885 culture confirmed cases. The second most predominant species, L. longbeachae, is primarily transmitted through dust, compost, and potting soil [12,13]. L. pneumophila serogroup 1 grows better in humans and is able to evade human immune responses so that it survives better in human lungs [1].
The use of the urine antigen test to screen suspected Legionnaires’ disease cases was thought to result in a bias towards detection of L. pneumophila serogroup 1 (the target of the test), but studies where suspected cases were tested by culture or molecular methods continue to demonstrate that >90% of the cases were still caused by L. pneumophila [5,14]. The Japanese Society for Chemotherapy Legionella committee collected culture isolates and clinical information on cases of sporadic community-acquired L. pneumonia between December 2006 and March 2019 [14]. Of the 140 sporadic cases identified, L. pneumophila was the most frequently isolated species (90.7%) followed by L. bozemanii (3.6%), L. dumoffii (3.6%), L. micdadei (1.4%), and L. longbeachae (0.7%). Among the 127 isolates of L. pneumophila, 111 isolates were serogroup 1, two serogroup 2, four serogroup 3, one serogroup 4, one serogroup 5, seven serogroup 6, and one was serogroup 10. Similarly, Beauté et al. [5] compared Community-Acquired Legionnaires’ disease cases with Healthcare Associated (HCA) Legionnaires’ disease cases using 10 years (2008-2017) of data from the European Surveillance System. The study covered 29 EU countries, reporting 40,411 community-acquired and 4,315 HCA cases. 4,884 of the Legionnaires’ disease cases were culture-confirmed, 55% of those did not have a prior urine antigen test diagnosis. For the 2,679 culture-confirmed cases which were initially diagnosed without the use of a urine antigen test (UAT), 97% of the 2,606 cases associated with waterborne bacteria were caused by L. pneumophila; most (74%) were serogroup 1 (Figure 1). Therefore, for both community-acquired and healthcare associated Legionnaires’ disease, L. pneumophila is the overwhelming cause of illness. Moreover, illnesses due to non-pneumophila species of Legionella were rare (1.9-2.5%) for hospital-acquired and community-associated cases of Legionnaires’ disease, respectively [5].
The National Outbreak Reporting System (NORS) collects reports of waterborne disease outbreaks in the United States [16]. The database contains information on 930 Legionella outbreaks from 1973 through 2023. Over 99% of the outbreaks were due to L. pneumophila or unknown Legionella (because no identification was made). Only 9 outbreaks (0.96%) were due to Legionella species other than L. pneumophila. Four of these outbreaks were due to L. anisa, one to L. dumoffii, and four to L. micdadei. Only three non-pneumophila outbreaks were related to drinking water and all of these occurred in hospital systems and all three were due to L. micdadei. The last of these nosocomial Legionella species outbreaks occurred over 20 years ago in 2004. The other six outbreaks were caused by non-potable water (hot tubs, fountains, etc.) and source one was unidentified. Therefore, based on the US NORS data, there is no public health justification to require public water systems or public buildings (other than health care facilities) to monitor or manage for any other species of Legionella other than L. pneumophila. Although outbreaks represent just a fraction of all Legionnaires’ disease cases, they do provide valuable insights into the etiologic agents and mechanisms of transmission for Legionella infections.
Drinking water outbreaks of Legionnaires’ disease have increased in the U.S. since the year 2000 (Figure 2) and currently is the most commonly identified cause of waterborne outbreaks. From 2015-2020, Legionella was associated with 160 (92%) outbreaks, 666 (60%) cases, 462 (97%) hospitalizations, and 68 (97%) deaths related to U.S. community and noncommunity water systems [17]. Similar increases in cases of Legionnaires’ disease have been recorded for a number of developed countries [18]. Although Legionella is regulated in the U.S, under the Surface Water Treatment Rule as a treatment technique, no monitoring for the organism is required and the federal rule does not apply to groundwater systems where approximately one-third of all U.S. outbreaks occur [19].
Legionella also causes a milder disease, called Pontiac fever, which includes fever, myalgias, chills, and headache, but by definition not pneumonia; and most patients recover without treatment (NASEM, 2019). Despite the dramatic increase in Legionnaires’ disease since the year 2000 (Figure 2), similar increases in Pontiac fever have not been reported and outbreaks remain sporadic. Hamilton et al. [21] conducted a review of Legionnaires’ disease and Pontiac fever cases from 2006-2017 that included 136 outbreaks with 115 Legionnaires’ Disease outbreaks, 4 Pontiac fever outbreaks, and 17 mixed outbreaks of Legionnaires’ Disease and Pontiac fever. The researchers found Pontiac fever was mostly associated with non-potable water sources (i.e., fountains, pools, spas, cooling towers, etc.) and only 1% of the cases were associated with potable water (in building water systems) (Figure 3). All the cases of Pontiac fever were caused by L. pneumophila or mixtures of L. pneumophila and other Legionella species. Although Pontiac fever has been attributed to non-pneumophila species [22], it would appear based on the data of Hamilton e al. [21], that the predominate risks are associated with L. pneumophila.
Legionellae are normal inhabitants of the aquatic environment and unlike fecal pathogens their presence does not necessarily indicate a failure of treatment barriers. Moreover, unlike typical fecal-oral pathogens, Legionella can grow in water provided the right temperature and conditions are present. The ecology of Legionella is more complex than most fecal pathogens and often involves intracellular growth in free living amoebae that can amplify the bacterial virulence factors. Although drinking water can be an important route of exposure, other uses of water are also important, including cooling towers, hot tubs and pools, ornamental fountains, and industrial equipment [23]. According to Muder and Victor [24] and the Legionella Database [25,26], there are no reported outbreaks of pneumonia solely due to non-pneumophila Legionella species that have been associated with large aerosol-generating devices, such as cooling towers.
3. Methods for Legionella Detection
The National Academy of Science, Engineering, and Medicine (NASEM, 2020) report provides a more comprehensive review of analytical methods for Legionella monitoring, but this paper will focus on tests that can be used by water utilities. The standard method (ISO 11731:2017) filters a water sample (typically 1 L) through a membrane filter and the membrane is resuspended in a small volume of sterile water and vortexed or sonicated [27]. After sonication one aliquot is treated with an HCl-KCl acid buffer, another aliquot is treated with heat (50oC), and a third aliquot is plated directly on a buffered charcoal yeast extract agar which can contain additional components to increase selectivity (Polymyxin B Sulfate, Vancomycin and Cycloheximide [PCV] or PCV with Glycine [GPCV]). The plates are then incubated at 36±2⁰C for 10 days and suspect colonies confirmed and serotyped using a commercially available rapid Legionella latex slide agglutination test (Figure 4). Although 1 L is typically filtered, the actual volume analyzed is much less (e.g., 5-20 mL) given the number of splits and subsamples. The ISO method is mistakenly referred to as detecting “all” Legionella species (CDC 2024) although the ISO protocol is clear that it does not detect all species of Legionella [27]. Lee et al. [28] examined 28 Legionella spp. on four commercial media and found that 11 of the species (notably L. micdadei and L. bozemanii) did not grow on media containing cefamandole and 8 of the 28 species only grew marginally. Luck et al. [29] reported that glycine-containing media (GVPC) inhibited some of the non-pneumophila strains tested. The complexity of the pretreatment steps, and the experience needed to identify and confirm suspect colonies is beyond the capability of most water utility labs, and utilities using the ISO 11731:2017 method typically outsource these tests to a competent commercial laboratory.
The Legiolert method is another culture assay that is specific for all serotypes of L. pneumophila and amenable for use by water utilities. The test can be configured to use 10- or 100-mL volumes. The water hardness is adjusted, if needed, and the concentrated media added, shaken, and added to a 96-well Quanti-tray which is sealed and incubated at 39oC for 7 days. Turbid and brown colored wells are counted and a Most Probable Number is calculated. Numerous studies have shown the Legiolert test to be equivalent or superior to the ISO 11731method [30-49]. A survey of 12 utilities that used the Legiolert test to monitor raw, finished, and distribution system samples found the test easy to use and felt confident in using the test to detect L. pneumophila in raw and treated waters [42].
There has been an explosion of commercially available quantitative polymerase chain reaction (qPCR) -based assays that detect the DNA of L. pneumophila and species of Legionella. However, many of these qPCR methods use proprietary primers and components and few have been widely evaluated in multiple laboratory studies. Molecular methods hold the promise of more rapid analyses and could be used as a screening or investigative tool. One limitation with the molecular assays is the volume analyzed – which typically is in the range of microliters. Substantial concentration is needed to provide analyzed volumes equivalent to the 100 mL Legiolert test. Another limitation is the ability of molecular methods to determine the viability of recovered Legionella. Some qPCR methods are adding a “viability stain” to the assay – typically a propidium monoazide or propidium iodide – which can pass through damaged cell membranes and intercalate in the DNA, preventing PCR amplification. There is a need for comparison of “viable” qPCR methods as commercial providers also use proprietary methods.
Molecular methods have the potential to detect “viable but not culturable” (VBNC) cells that retain metabolic functions (e.g., enzyme activity or DNA replication) but not produce visible colonies on standard culture media, however, the public health significance of these cells is unclear as Dietersdorfer et al [50] reported that VNBC cells of L. pneumophila infected human macrophages at rates of 100 to 400 times less than culturable cells. Similarly, Cervero-Aragó et al. [51] reported that thermally stressed VBNC L. pneumophila infected amoebae and human macrophages (THP-1) at lower rates of infectivity compared to culturable cells. Analysis of VNBC cells could be of value in assessing remediation efforts since L. pneumophila VNBC cells have been shown to be resuscitated and become cultivatable after passage through free-living amoebae [52]. No waterborne Legionella infections have been directly attributed to VBNC cells.
There are also a number of commercial immunological tests for L. pneumophila and Legionella spp. detection (e.g., lateral flow immunoassays, solid-phase cytometry, and flow cytometry, etc.) that can be used for monitoring, treatment efficacy, remediation, investigations or research. The caveats for these methods are similar to the discussion above, most have proprietary components, may not assess viability, and have limited independent evaluations by multiple laboratories. The point of this discussion is that there are many commercially available Legionella assays (and more are in development), so the analyst must choose the assay that best fits their capabilities and monitoring objectives.
A side-by-side analysis for the Legiolert, the ISO 11731 culture method and a commercially available viability qPCR (Legionella spp., L. pneumophila sg1 and L. pneumophila sg2-15, as a multiplex assay) was recently conducted on drinking water distribution systems samples by Bartrand et al. [53]. Of 143 samples analyzed, L. pneumophila was detected by one of the three methods on only three occasions (Table 2); once by Legiolert and twice by viability qPCR and no positive samples by the ISO 11731 method. The viability qPCR and Legiolert methods detected L. pneumophila in separate samples, so there was no overlap for these results.
The low frequency of detection of L. pneumophila in Table 2 precluded conclusions on the comparison of methods, but the results do challenge the common belief that molecular methods are far superior to culture methods for detection of L. pneumophila in water samples. The study examined disinfected drinking water, so inclusion of a commercially available viability qPCR method (microproof Legionella Quantification LyoKit with Reagent D, Hygiena) was important to allow a direct comparison to the culture methods.
It was also possible to compare the viability qPCR multiplex assay with the ability of the ISO 11731 method for detection of non-pneumophila species in water samples. One of the commonly cited advantages of the ISO 11731 method is its ability to detect “all Legionella species,” despite the fact that the method was developed primarily to detect L. pneumophila and studies mentioned previously have shown that many Legionella species do not grow, or grew only marginally, on certain formulations of BCYE agar. In the study [53], the viability qPCR method detected Legionella species in 53 samples (37%), ranging from <150 to 19,000 genomic units (GU) per 250 mL while only one sample by the ISO 11731 method was positive – and this isolate was identified as L. anisa (Table 3).
Omoregie et al. [49] analyzed 544 drinking water distribution system samples by culture methods (ISO and Legiolert) and 528 samples by regular qPCR (multiplex with targets Legionella spp., L. pneumophila and L. pneumophila sg1) (Table 3). Similar to Bartrand et al. (2024) the occurrence of L. pneumophila in distribution systems was low (1-2%) by either culture or molecular methods, but the occurrence of Legionella spp. was much higher by conventional qPCR (85%) compared to viability qPCR (37%). Similar data from Wang et al. [54], suggests that use of qPCR without consideration of viability overestimated viable Legionella spp. occurrence in disinfected waters.
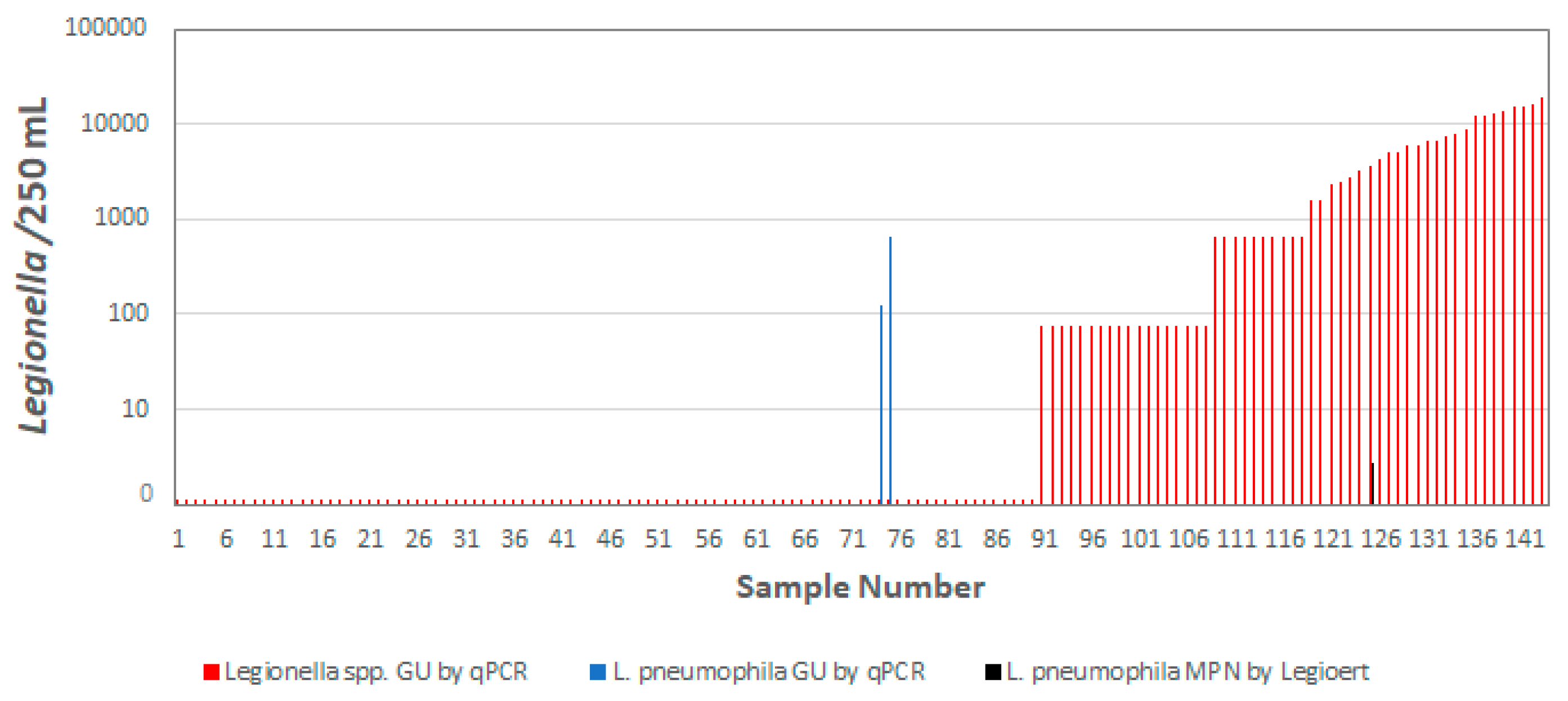
The concentration of Legionella species has not been shown to be a reliable predictor of L. pneumophila occurrence by either the Legiolert method or by viability qPCR. Importantly, the samples that were positive for L. pneumophila by viability q-PCR were negative for Legionella spp. (Figure 4). The one sample positive by Legiolert (1.1 MPN/100 mL) was also positive for Legionella spp. by viability qPCR (3600 GU/250 mL). Similar results were reported by van der Lugt et al. [55] who examined 206 buildings in the Netherlands and detected Legionella spp. in 96.9% of the samples, but L. pneumophila in only 3.1% of the samples. Wéry et al. [56] suggested that Legionella spp. could be antagonistic to L. pneumophila in some cooling tower samples. A Dutch study [57] found that monitoring of Legionella species was not a predictor of L. pneumophila occurrence, in part because of the ecology of the organisms is different.
Figure 4.
Relationship between Legionella spp. and L. pneumophila occurrence in distribution systems samples. Adapted from Bartrand et al. [53]. For data visualization, qPCR data that was positive but below the limit of detection was set at half the detection limit. For qPCR data that was negative, the value was set to zero.
Figure 4.
Relationship between Legionella spp. and L. pneumophila occurrence in distribution systems samples. Adapted from Bartrand et al. [53]. For data visualization, qPCR data that was positive but below the limit of detection was set at half the detection limit. For qPCR data that was negative, the value was set to zero.
An analysis of viability qPCR Legionella spp. data from the Bartrand et al. [53] study showed that the recommended disinfectant guidelines for management of L. pneumophila in distribution systems would also be effective for managing Legionella spp. (Figure 5). Bartrand et al. [53] recommended maintenance of a 0.2 mg/L residual of either free chlorine or monochloramine for control of L. pneumophila (along with other best management practices including cleaning of storage tanks and pipes, flushing, reduced stagnation, etc.) in drinking water distribution systems. The data shown in Figure 5 demonstrates that the same approach would be effective in managing Legionella spp. as well.
4. Guidelines for Legionella Management
Several guidelines exist for management of Legionella in water samples [58,59] but both are based on the analysis of Legionella spp. rather than specifically L. pneumophila. The America Society of Heating, Refrigeration, and Air-cooling Engineers (ASHARE) ANSI-accredited standard, ASHRAE 188, is often applied to generate water management plans for building water systems [60], and the supplement document (ASHRAE Guideline 12) makes a distinction in risk between L. pneumophila and other species of Legionella [61]. Likewise, the USEPA regulates all Legionella species with a non-enforceable Maximum Contaminant Level Goal (MCLG) of zero. However, as mentioned previously, the standard ISO-11731 method does not recover all species of Legionella, so treating L. pneumophila and non-pneumophila species equally is without any scientific basis. Various species of Legionella differ in their virulence, infectivity, and preferred growth conditions, but L. pneumophila, and specifically serogroup 1, have specific virulence factors that enhance the pathogenicity of this strain to humans [1]. With few exceptions, reported clusters of pneumonia due to non-pneumophila Legionella species have been hospital acquired (nosocomial) [24]. Known cases of pneumonia from public water systems due to species other than L. pneumophila are uncommon, and most cases appear to be sporadic. As previously mentioned [24], there are no reported outbreaks of pneumonia due to non-pneumophila Legionella species that have been associated with large aerosol-generating devices, such as cooling towers.
The European Drinking Water Directive (2020/2184) requires each country to develop a plan to reduce the risk of Legionella (among other contaminants) from water [62]. How various countries are approaching this directive, however, varies. In France, testing of water samples is predominantly focused on the detection of L. pneumophila [1]. Doleans et al. [63] notes that over 95% of the clinical cases in France are caused by L. pneumophila and only 0.8% of the cases are due to L. anisa, but environmental testing shows a much higher ratio of L. anisa (13.8%) compared to L. pneumophila (28.2%); pointing to the importance of considering “pathogenicity over environmental prevalence.”
In contrast, Germany has requirements for testing of Legionella spp. using culture methods, but a change in the test medium (from GVPC to BCYE+AB) in 2019 led to a 39.3% increase in waters exceeding the legal limit - caused exclusively by non-pneumophila Legionella strains [64]. The researchers found that 96.7% of the isolates recovered on GVPC were L. pneumophila, but only 76.4% on BCYE+AB media. The authors note that clinical and epidemiological studies show that the vast majority of clinical legionellosis cases were linked to L. pneumophila and it “did not seem justified to attribute virtually the same virulence to all strains of environmental Legionella spp.” They recommended that in the future that testing in Germany should focus mainly on L. pneumophila.
In the Netherlands, a “hybrid” approach to monitoring has been proposed recognizing the differences in risk between clinical settings and testing of potable water in distribution systems [57]. Testing for Legionella spp. would be required for clinical settings where there was a large population of “at risk” individuals (elderly, smokers, immunosuppressed, etc.), but testing of drinking water networks and in public buildings would focus on management of L. pneumophila. This makes sense since L. micdadei, L. bozemanii, L. dumoffi and L. longbeachae are typically isolated only from people with weakened immune systems - primarily patients undergoing cancer treatment or immune-suppression due to organ transplants [65,66]. As mentioned previously, one Dutch study found that Legionella spp. were detected in 96.9% of the 206 buildings sampled, but L. pneumophila was detected in only 3.1% of the samples [55]. The KWR and Berenschot [57] study found that there was no evidence to prove that monitoring other legionella strains was a good indicator of the presence of L. pneumophila. Report author, van der Wielen stated that “different Legionella strains need different conditions to grow and the presence of any random Legionella species does not necessarily mean that the most pathogenic strains can also grow.” Monitoring for non-pneumophila species results in drastic and expensive and time-consuming measures to keep non-hazardous Legionella strains out of the systems, even though the health benefits are extremely limited.
It would be useful if the European Drinking Water Directive [62] actually spurred more research on quantitative risk assessment for Legionella. As reviewed by Hamilton and Haas [67] there are at least 10 quantitative microbial risk models (QMRA) for determination of risk by L. pneumophila, but to this author’s knowledge there are no risk models for waterborne non-pneumophila Legionella spp. Bentham and Whiley [68] concluded that a QMRA for Legionella spp. may be impractical given the uncertainties but such an exercise may be useful if only to demonstrate that the risk in water is overwhelmingly from L. pneumophila and not from waterborne non-pneumophila Legionella spp. (this would exclude L. longbeachae whose risk is primarily from soil [69]).
An excellent study by Romano Spica et al. [15] developed a mathematical model for estimating the relative economic cost and public health benefit for monitoring and control for L. pneumophila versus for Legionella species. Inputs to the model included data from the European Center for Disease Prevention and Control (ECDC), The European Surveillance System (TESSy), the Italian Ministry of Health, surveys through Aquaitalia (the national Italian association of water treatment professionals and companies), published papers, and interviews with experts and consultants in microbiology, epidemiology, management, and treatment of internal water distribution systems within buildings. The model simulated the costs and benefits of three Legionella monitoring and control strategies for certain categories of non-hospital buildings:
(a) “no additional monitoring” for environmental surveillance and control;
(b) “monitor and control all Legionella pneumophila” strategy; and
(c) “monitor and control Legionella species” strategy.
The output included the cost of each Legionnaires’ disease case prevented and the economic cost of the control program (e.g., monitoring, mitigation and remediation costs and impacts to workers, building closures, and litigation). The results showed a similar level of public health protection for both options for Legionella monitoring (either L. pneumophila or Legionella spp.) but a 23-770% higher total economic cost for monitoring Legionella spp. rather than L. pneumophila, depending on variables for the levels of bacterial contamination [15]. The conclusion that “under all conditions, the costs of a strategy based on monitoring Legionella species were consistently higher than those of a strategy focused on L. pneumophila, including all serogroups, with similar health outcomes.” Although the authors limit the application of the study to specific building categories under Italian regulations, the study’s finding could provide valuable insights for policymakers in other jurisdictions.
5. Conclusions
The results presented in this paper make a strong case for monitoring L. pneumophila in drinking water and building water systems. Based on the information provided the following conclusions can be drawn:
- For both community-acquired and healthcare associated Legionnaires’ disease, L. pneumophila is the overwhelming cause of illness. Waterborne Illnesses due to non-pneumophila species of Legionella are rare, particularly outside clinical environments.
- Although less well studied, cases of Pontiac Fever have not followed the same 20-year trend in increases in cases of Legionnaires’ disease. Most cases of Pontiac Fever are associated with non-potable sources of water.
- The concentration or occurrence of Legionella species has not been shown to be a reliable predictor of L. pneumophila and the health impacts of Legionella species is low relative to L. pneumophila. Treating counts of L. pneumophila and non-pneumophila species equally is without any scientific basis and results in unnecessary cost with little public health benefit.
- Careful consideration must be taken when selecting an appropriate method for monitoring Legionella in water systems. There are many alternatives to the ISO 11731:2017 that are easier to use and provide more accurate analyses. Although molecular methods hold the promise of more rapid analyses, the commercial kits require additional validation and viability analyses need more research. The Legiolert test has proven to be simple, accurate, and feasible for use by water utilities.
- Although a challenge, it would be useful to develop quantitative risk assessments for L. pneumophila and non-pneumophila species in water.
- Countries continue to determine how to focus their guidelines and whether they should promote routine monitoring and control of Legionella species and/or L. pneumophila. One option would be to consider water in clinically significant settings differently from distribution systems or non-health care buildings. It is prudent to hold health care facilities to a higher water quality standard than for potable water systems or public buildings when severely immunocompromised patients may be present.
If greater efforts to manage the increased risk of Legionnaires’ disease in water are to be realized, it will be necessary to have simple and effective procedures that can be readily implemented by water utilities and building managers with reasonable cost effectiveness while protecting public health. A focus on the measurement and control of the greatest health risk, L. pneumophila, is necessary to achieve this objective.
Author Contributions
M.W.L. Conceptualization, Writing- Original Draft Preparation, Writing—Review and Editing, Project Administration
Funding
This report was prepared with no external funding.
Author
Mark W. LeChevallier was employed by his own company Dr. Water Consulting, LLC. The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The author acknowledges the helpful comments of Patsy Root and Kristin Majeska in the review of this manuscript
Conflicts of Interest
The author declare no conflicts of interest.
References
- NASEM (National Academies of Sciences, Engineering, and Medicine). 2019. Management of Legionella in Water Systems. Washington, DC: The National Academies Press. [CrossRef]
- Khodr, A., E. Kay, L. Gomez-Valero, C. Ginevra, P. Doublet, C. Buchrieser, and S. Jarraud. 2016. Molecular epidemiology, phylogeny, and evolution of Legionella. Infect Genet Evol. 43:108-122.
- Vaccaro, L., F. Izquierdo, A. Magnet, C. Hurtado, M. A. Salinas, T. Santos Gomes, S. Angulo, S. Salso, J. Pelaez, M. I. Tejeda, A. Alhambra, C. Gómez, A. Enríquez, E. Estirado, S. Fenoy, and C. del Aguila. 2016. First case of Legionnaire’s disease caused by Legionella anisa in Spain and the limitations on the diagnosis of Legionella non-pneumophila infections. PLoS ONE 11(9):e016293.
- Fields, B.S., R.F. Benson, R.E. Besser. 2002. Legionella and Legionnaires’ Disease: 25 Years of Investigation. Clinical Microbiology Reviews, 15(3): 506–526. . [CrossRef]
- Beauté, J., D, Plachouras, S. Sandin, J. Giesecke, P. Sparén. 2020. Healthcare-Associated Legionnaires' Disease, Europe, 2008-2017. Emerging Infectious Diseases, 26(10): 2309-2318. [CrossRef]
- Cross, K. E., J. W. Mercante, A. J. Benitez, E. W. Brown, M. H. Diaz, and J. M. Winchell. 2016. Simultaneous detection of Legionella species and L. anisa, L. bozemanii, L. longbeachae, and L. micdadei using conserved primers and multiple probes in a multiplex real-time PCR assay. Diagnostic Microbiology and Infectious Diseases 85(3):295-301.
- Dooling, K. L., K.-A. Toews, L. A. Hicks, L. E. Garrison, B. Bachaus, S. Zansky, L. R. Carpenter, B. Schaffner, E. Parker, S. Petit, A. Thomas, S. Thomas, R. Mansmann, C. Morin, B. White, and G. E. Langley. 2013. Active bacterial core surveillance for Legionellosis—United States, 2011–2013. Morb. Mortal. Wkly. Rep. 64(42):1190-1193.
- von Baum, H., S. Ewig, R. Marre, N. Suttorp, S. Gonschior, T. Welte, and C. Lück. 2008. Community-acquired Legionella pneumonia: New insights from the German competence network for community acquired pneumonia. Clin. Infect. Dis. 46(9):1356-64.
- Yu, V. L., J. F. Plouffe, M. C. Pastoris, J. E. Stout, M. Schousboe, A. Widmer, J. Summersgill, T. File, C. M. Heath, D. L. Paterson, and A. Chereshsky. 2002. Distribution of Legionella species and serogroups isolated by culture in patients with sporadic community-acquired legionellosis: an international collaborative survey. J. Infect. Dis. 186:127-128.
- Collier, S. A., Deng, L., Adam, E. A., Benedict, K. M., Beshearse, E. M., Blackstock, A. J....Beach, M. J. 2021. Estimate of Burden and Direct Healthcare Cost of Infectious Waterborne Disease in the United States. Emerging Infectious Diseases, 27(1), 140-149. [CrossRef]
- ECDC. 2023. European Centre for Disease Prevention and Control. Legionnaires’ disease. https://www.ecdc.europa.eu/en/legionnaires-disease.
- Whiley, H., and R. Bentham. 2011. Legionella longbeachae and legionellosis. Emerging Infectious Diseases 17(4):579-583.
- Chambers, S.T., Slow, S., Scott-Thomas, A. and Murdoch, D.R., 2021. Legionellosis caused by non-Legionella pneumophila species, with a focus on Legionella longbeachae. Microorganisms, 9(2), p.291. [CrossRef]
- Miyashita, N., Higa, F., Aoki, Y., Kikuchi, T., Seki, M., Tateda, K., Maki, N., Uchino, K., Ogasawara, K., Kiyota, H. and Watanabe, A., 2020. Distribution of Legionella species and serogroups in patients with culture-confirmed Legionella pneumonia. Journal of Infection and Chemotherapy, 26(5), pp.411-417. [CrossRef]
- Romano Spica, V., P. Borella, A. Bruno, C. Carboni, M. Exner, P. Hartemann, G. Gianfranceschi, P. Laganà, A. Mansi, M.T. Montagna, and O. De Giglio. 2024. Legionnaires’ Disease Surveillance and Public Health Policies in Italy: A Mathematical Model for Assessing Prevention Strategies. Water, 16(15), p.2167. [CrossRef]
- Centers for Disease Control and Prevention (CDC). 2025. BEAM (Bacteria, Enterics, Amoeba, and Mycotics) Dashboard. Atlanta, Georgia: U.S. Department of Health and Human Services. www.cdc.gov/ncezid/dfwed/BEAM-dashboard.html. Accessed January 2025. https://data.cdc.gov/Foodborne-Waterborne-and-Related-Diseases/NORS/5xkq-dg7x/data_preview. .
- Kunz JM, Lawinger H, Miko S, et al. Surveillance of Waterborne Disease Outbreaks Associated with Drinking Water — United States, 2015–2020. MMWR Surveill Summ 2024;73(No. SS-1):1–23. http://dx.doi.org/10.15585/mmwr.ss7301a1.
- Hammes, F. 2024. https://media.licdn.com/dms/image/v2/D4D22AQFh4Ro1Ifwp7g/feedshare-shrink_800/feedshare-shrink_800/0/1724099223915?e=1738800000&v=beta&t=kd0-cPi70ARvJf5p-l_8JSJTqAX0ozrmEuEw-nVFOuc (accessed 12/24).
- Holsinger, H., Tucker, N., Regli, S., Studer, K., Roberts, V.A., Collier, S., Hannapel, E., Edens, C., Yoder, J.S. and Rotert, K., 2022. Characterization of reported legionellosis outbreaks associated with buildings served by public drinking water systems: United States, 2001–2017. Journal of Water and Health, 20(4), pp.702-711. [CrossRef]
- Benedict, K. M.; Reses, H.; Vigar, M.; Roth, D. M.; Roberts, V. A.; Mattioli, M.; Colley, L.A. et al. 2017. Surveillance for waterborne disease outbreaks associated with drinking water—United States, 2013–2014. Morbidity and Mortality Weekly Report, 66:44:1216. [CrossRef]
- Hamilton, K.A., A.J. Prussin, W. Ahmed & C.N. Haas. 2018. Outbreaks of Legionnaires’ Disease and Pontiac Fever 2006–2017. Current Environmental Health Reports. 5:263–271. [CrossRef]
- Fields BS, Barbaree JM, Sanden GN, Morrill WE. 1990. Virulence of a Legionella anisa strain associated with Pontiac fever: an evaluation using protozoan, cell culture, and guinea pig models. Infect Immun. 58(9):3139-42. PMID: 2117580.
- Garrison LE, Kunz JM, Cooley LA, et al. 2016. Vital Signs: Deficiencies in Environmental Control Identified in Outbreaks of Legionnaires’ Disease — North America, 2000–2014. MMWR Morb Mortal Wkly Rep 65:576 – 584. [CrossRef]
- Muder, R. R., and L. Y. Victor. 2002. Infection due to Legionella species other than L. pneumophila. Clin. Infect. Dis. 35(8):990-998. [CrossRef]
- Gonçalves, I.G., Fernandes, H.S., Melo, A., Sousa, S.F., Simoes, L.C. and Simoes, M., 2021. LegionellaDB–a database on legionella outbreaks. Trends in Microbiology, 29(10), pp.863-866. [CrossRef]
- LegionellaDB. 2024. LegionellaDB, A database on Legionella outbreaks. https://legionelladb.biosim.pt/ (accessed 12/24).
- ISO, 2017. Water Quality – Enumeration of Legionella. ISO 11731:2017. International Organization for Standardization, Geneva, Switzerland. https://www.iso.org/standard/61782.html.
- Lee, T.C., R.M. Vickers, V.L. Yu, M.M. Wagener. 1993. Growth of 28 Legionella Species on Selective Culture Media: a Comparative Study. J. Clin. Microbiol., 31(10): 2764-2768.
- Luck, P.C., Igel, L., Helbig, J.H., Kuhlisch, E., Jatzwauk, L., 2004. Comparison of commercially available media for the recovery of Legionella species. Int. J. Hyg. Environ. Health 207, 589–593.
- Sartory, D.P., Spies, K., Lange, B., Schneider, S., Langer, B., 2017. Evaluation of a most probable number method for the enumeration of Legionella pneumophila from potable and related water samples. Letters in Applied Microbiology 64, 271–275.
- Spies, K., Pleischl, S., Lange, B., Langer, B., Hübner, I., Jurzik, L., Luden, K., Exner, M., 2018. Comparison of the LegiolertTM/Quanti-Tray® MPN test for the enumeration of Legionella pneumophila from potable water samples with the German regulatory requirements methods ISO 11731-2 and ISO 11731. International journal of hygiene and environmental health 221, 1047–1053.
- Petrisek, R., Hall, J., 2017. Evaluation of a most probable number method for the enumeration of Legionella pneumophila from North American potable and nonpotable water samples. Journal of Water and Health 16, 25–33.
- CDC. 2024. Laboratory Testing for Legionella. https://www.cdc.gov/legionella/php/laboratories/index.html (Accessed 12/2024.
- Rech, M.M., Swalla, B.M., Dobranic, J.K., 2018. Evaluation of Legiolert for Quantification of Legionella pneumophila from Non-potable Water. Current Microbiology 75, 1282–1289.
- Barrette, I., 2019. Comparison of Legiolert and a Conventional Culture Method for Detection of Legionella pneumophila from Cooling Towers in Québec. Journal of AOAC International 102, 1235–1240.
- Scaturro, M., Buffoni, M., Girolamo, A., Cristino, S., Girolamini, L., Mazzotta, M., Bucci Sabattini, M.A., Zaccaro, C.M., Chetti, L., Laboratory, M.A.N., 2020. Performance of Legiolert test vs. ISO 11731 to confirm Legionella pneumophila contamination in potable water samples. Pathogens 9, 690.
- Boczek, L.A., Tang, M., Formal, C., Lytle, D., Ryu, H., 2021. Comparison of two culture methods for the enumeration of Legionella pneumophila from potable water samples. Journal of Water and Health 19, 468–477.
- Checa, J., Carbonell, I., Manero, N., Martí, I., 2021. Comparative study of Legiolert with ISO 11731-1998 standard method-conclusions from a Public Health Laboratory. Journal of Microbiological Methods 186, 106242.
- Dowdell, K.S., Greenwald, H.D., Joshi, S., Grimard-Conea, M., Pitell, S., Song, Y., Ley, C., Kennedy, L.C., Vosloo, S., Huo, L., 2022. Legionella pneumophila Occurrence in Reduced-Occupancy Buildings in 11 Cities during the COVID-19 Pandemic. medRxiv. [CrossRef]
- Hirsh, M., Baron, J.L., Mietzner, S., Rihs, J.D., Stout, J.E., 2021. Cross-reactivity of the IDEXX Legiolert Method with other Gram-negative Bacteria and Waterborne Pathogens Leads to False-Positive Assay Results. Letters in Applied Microbiology 72, 750–756. [CrossRef]
- Inoue, H., Baba, M., Tayama, S., 2020. Evaluation of Legiolert for quantification of Legionella pneumophila from bath water samples. Biocontrol Science 25, 179–182.
- LeChevallier, M.W. 2019a. Monitoring distribution systems for Legionella pneumophila using Legiolert. AWWA Water Science. 2019:e1122. [CrossRef]
- LeChevallier, M.W. 2019b. Occurrence of culturable Legionella pneumophila in drinking water distribution systems. AWWA Wat Sci. 2019;e1139. . [CrossRef]
- Li, Y., Yang, K., Fu, L., Gong, L., Liu, L., Gao, J., 2021. Comparison of the Legiolert enzyme-substrate method and the conventional cultivation for the detection of Legionella pneumophila in water samples from public places. Journal of Public Health and Preventive Medicine 51–54.
- Mapili, K., Pieper, K.J., Dai, D., Pruden, A., Edwards, M.A., Tang, M., Rhoads, W.J., 2020. Legionella pneumophila Occurrence in Drinking Water Supplied by Private Wells. Letters in Applied Microbiology. [CrossRef]
- Maqbool, A., 2019. Potential for Human Exposure to Legionella near Newtown Creek in Brooklyn, New York. Senior Projects Spring 2019. 176. https://digitalcommons.bard.edu/senproj_s2019/176.
- McCuin, R.M., Bartrand, T.A., Clancy, J.L., 2021. Legionella pneumophila recovery using Legiolert and a traditional culture method. AWWA Water Science 3, e1228.
- Niu, C., Zhang, Yajie, Zhang, Yong, 2022. Evaluation of a Most Probable Number Method for Detection and Quantification of Legionella pneumophila. Pathogens 11, 789. [CrossRef]
- Omoregie, E., Szczerba, A., Novak, J., Rubinstein, I., Chuang, Y., Wu, J., Wang, J., Kretz, C., Hughes, S., Capetanakis, A., 2022. Legionella monitoring in the New York City water distribution system 2017 to 2019. AWWA Water Science 4, e1272.
- Dietersdorfer, E., A. Kirschner, B. Schrammel, A. Ohradanova-Repic, H. Stockinger, R. Sommer, J. Walochnik, and S. Cervero-Arago. 2018. Starved viable but non-culturable (VBNC) Legionella strains can infect and replicate in amoebae and human macrophages. Water Research 141:428-438. [CrossRef]
- Cervero-Aragó, S., B. Schrammel, E. Dietersdorfer, R. Sommer, C. Lück, J. Walochnik, and A. Kirschner. 2019. Viability and infectivity of viable but nonculturable Legionella pneumophila strains induced at high temperatures. Water research 158: 268-279. [CrossRef]
- Steinert, M., L. Emödy, R. Amann, and J. Hacker.1997. Resuscitation of viable but nonculturable Legionella pneumophila Philadelphia JR32 by Acanthamoeba castellanii. Applied and environmental microbiology 63, no. 5 (1997): 2047-2053. [CrossRef]
- Bartrand, T.A., M. LeChevallier, J.L. Clancy, G. Burlingame, R. McCuin. 2024. Occurrence of Legionella pneumophila in Drinking Water Distribution Systems. The Water Research Foundation, Denver, CO. https://www.waterrf.org/research/projects/occurrence-legionella-pneumophila-drinking-water-distribution-systems.
- Wang, H., Edwards, M., Falkinham, J.O., Pruden, A., 2012. Molecular Survey of the Occurrence of Legionella spp., Mycobacterium spp., Pseudomonas aeruginosa, and Amoeba Hosts in Two Chloraminated Drinking Water Distribution Systems. Applied and Environmental Microbiology. 78, 6285–6294. [CrossRef]
- van der Lugt, W., S.M. Euser, J.P. Bruin, J.W. den Boer, and E.P. Yzerman. 2019. Wide-scale study of 206 buildings in the Netherlands from 2011 to 2015 to determine the effect of drinking water management plans on the presence of Legionella spp. Water research, 161, pp.581-589. [CrossRef]
- Wéry, N., V. Bru-Adan, C. Minervini, J.P. Delgénes, L. Garrelly and J.J. Godon. 2008. Dynamics of Legionella spp. and bacterial populations during the proliferation of L. pneumophila in a cooling tower facility. Applied and environmental microbiology, 74(10), pp.3030-3037. [CrossRef]
- AIHA. 2015. Recognition, Evaluation, and Control of Legionella in Building Water Systems. American Industrial Hygiene Association. Falls Church, VA.
- KWR, Berenschot, 2021. Towards a More Effective Legislation for Legionella Control in Drinking Water Systems. Sent to the Dutch House of Representatives by the Minister of Infrastructure and Water Management by letter on November 16 2021. https://open.overheid.nl/documenten/ronl-d2695abf-d88e-4e42-ad99-31d38403cdb9/pdf.
- CDC, 2021. Toolkit for Controlling Legionella in Common Sources of Exposure (Legionella Control Toolkit) [WWW Document]. https://www.cdc.gov/control-legionella/media/pdfs/Control-Toolkit-All-Modules.pdf (Accessed 12/2024).
- ASHRAE (American Society of Heating, Refrigerating and Air-Conditioning Engineers). 2018. Standard 188 legionellosis: Risk management for building water systems. Atlanta, GA: ASHRAE.
- ASHRAE. 2020. ASHRAE Guideline 12-2020. Minimizing the risk of legionellosis associated with building water systems. Atlanta, GA: ASHRAE.
- European Drinking Water Directive. 2020. Directive (EU) 2020/2184 of the European Parliament and of the Council of 16 December 2020 on the quality of water intended for human consumption. https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32020L2184.
- Doleans, A., H. Aurell, M. Reyrolle, G. Lina, J. Freney, F. Vandenesch, J. Etienne, and S. Jarraud. 2004. Clinical and environmental distributions of Legionella strains in France are different. Journal of Clinical Microbiology, 42(1), pp.458-460. [CrossRef]
- Zacharias, N., F. Waßer, L. Freier, K. Spies, C. Koch, S. Pleischl, N.T. Mutters, and T. Kistemann. 2023. Legionella in drinking water: the detection method matters. Journal of Water and Health, 21(7), pp.884-894. [CrossRef]
- Rucinski, S. L., M. P. Murphy, K. D. Kies, S. A. Cunnignham, A. N. Schuetz, and R. Patel. 2018. Eight years of clinical Legionella PCR testing illustrate seasonal patterns. Clin. Infect. Dis. [CrossRef]
- Cunha, B. A., A. Burillo, and E. Bouza. 2016. Légionnaires’ disease. Lancet. 387(10016):376-385. [CrossRef]
- Hamilton, K.A. and C.N. Haas. 2016. Critical review of mathematical approaches for quantitative microbial risk assessment (QMRA) of Legionella in engineered water systems: research gaps and a new framework. Environmental Science: Water Research & Technology, 2(4), pp.599-613. [CrossRef]
- Bentham, R. and H. Whiley. 2018. Quantitative microbial risk assessment and opportunist waterborne infections–are there too many gaps to fill?. International journal of environmental research and public health, 15(6), p.1150. [CrossRef]
- Kenagy, E., P.C. Priest, C.M. Cameron, D. Smith, P. Scott, V. Cho, P. Mitchell and D.R. Murdoch. 2017. Risk factors for Legionella longbeachae legionnaires’ disease, New Zealand. Emerging infectious diseases, 23(7), p.1148.
Figure 1.
Data from the European Surveillance System for Legionnaires’ disease cases that were culture-confirmed. Adapted from Beauté et al. [5] and Romano Spica et al. [15].
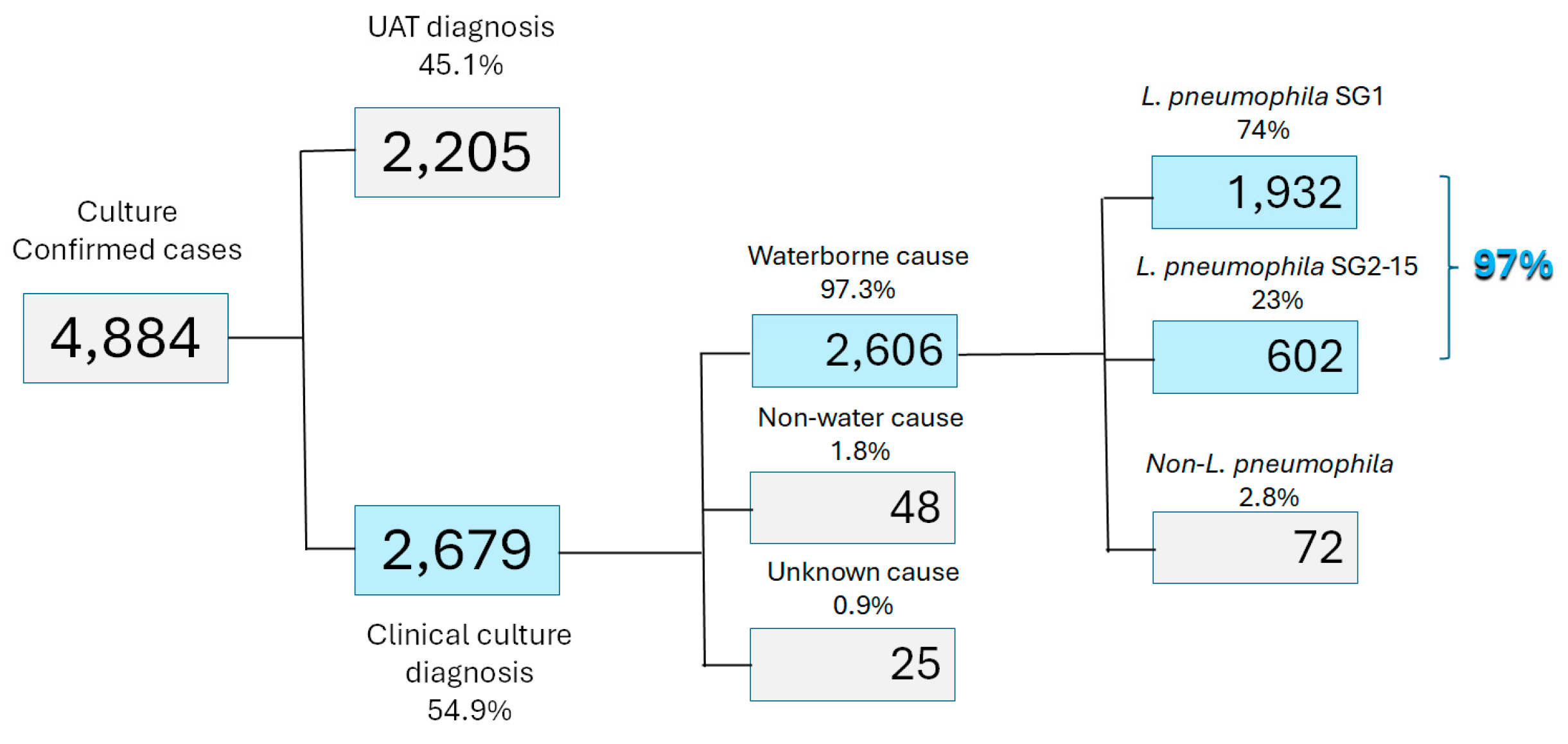
Figure 2.
Etiology of drinking water associated outbreaks (n=928) in the US, 1971-2014. From Benedict et al. [20].
Figure 2.
Etiology of drinking water associated outbreaks (n=928) in the US, 1971-2014. From Benedict et al. [20].
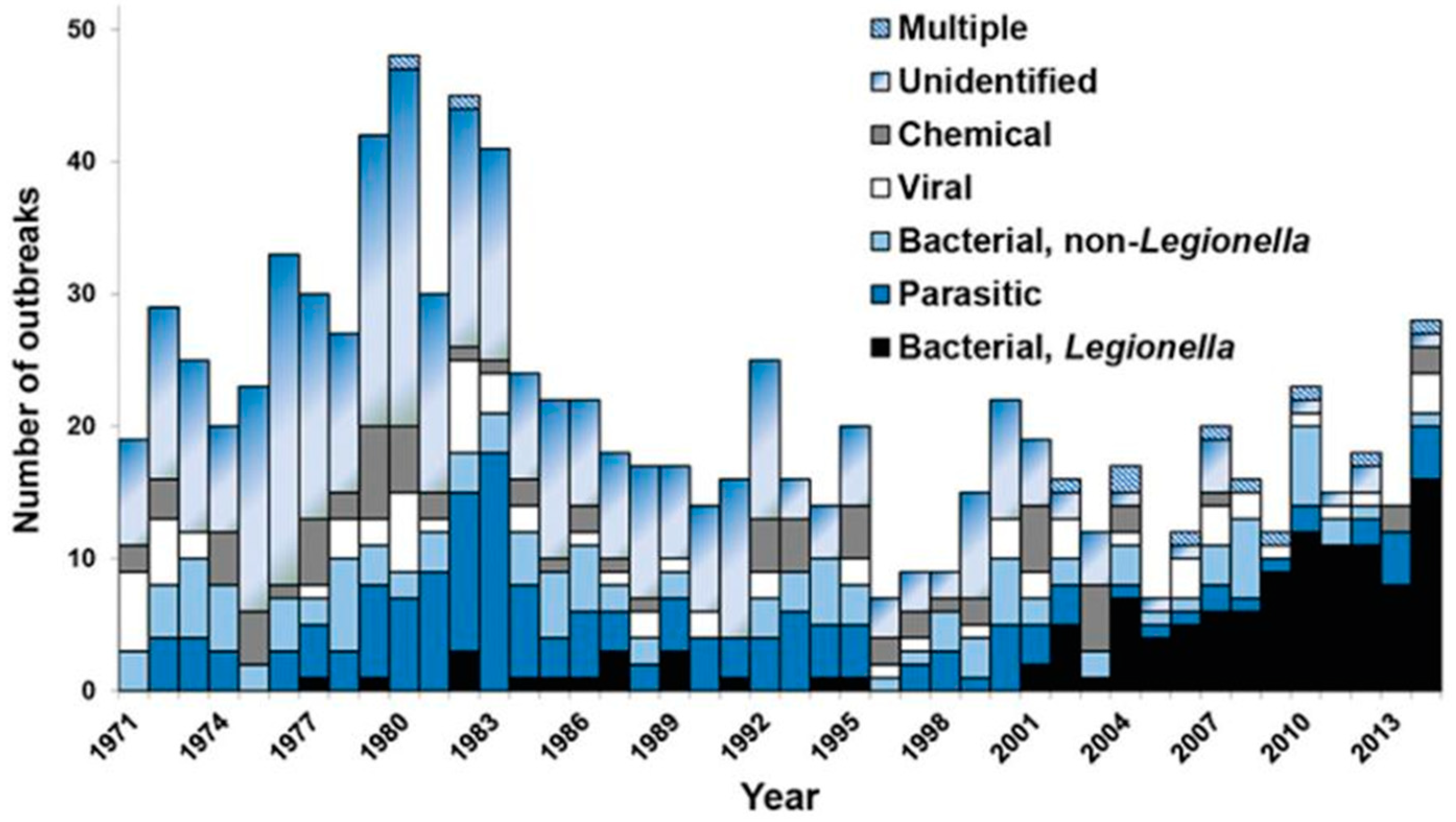
Figure 3.
Figure 3. Comparison of Legionnaires’ Disease (LD) and Pontiac Fever (PF) Cases 2006-2017. Adapted from Hamilton et al. [21].
Figure 3.
Figure 3. Comparison of Legionnaires’ Disease (LD) and Pontiac Fever (PF) Cases 2006-2017. Adapted from Hamilton et al. [21].
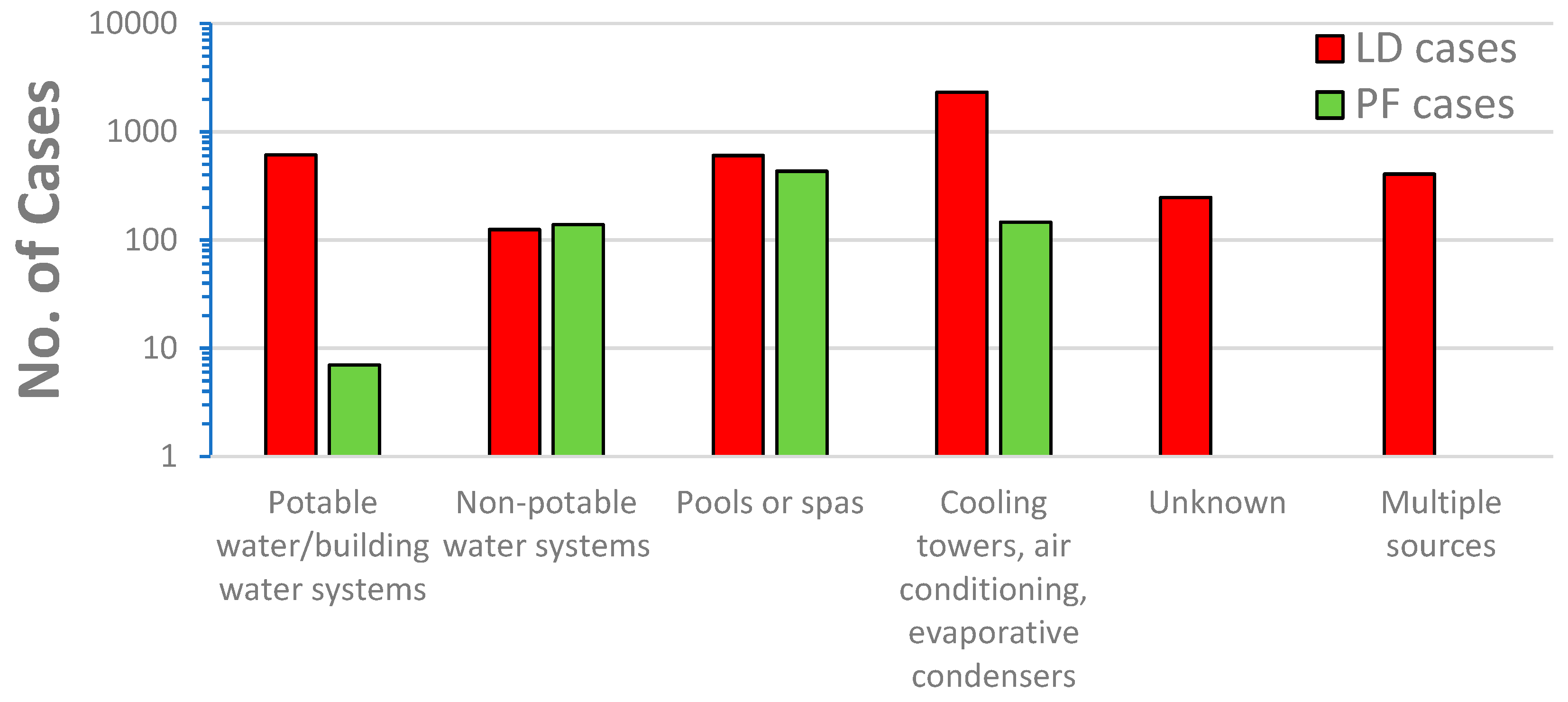
Figure 4.
Legionella and non-target colonies on BCYE medium. Photo credit: Dan Broder. Used with permission.
Figure 4.
Legionella and non-target colonies on BCYE medium. Photo credit: Dan Broder. Used with permission.
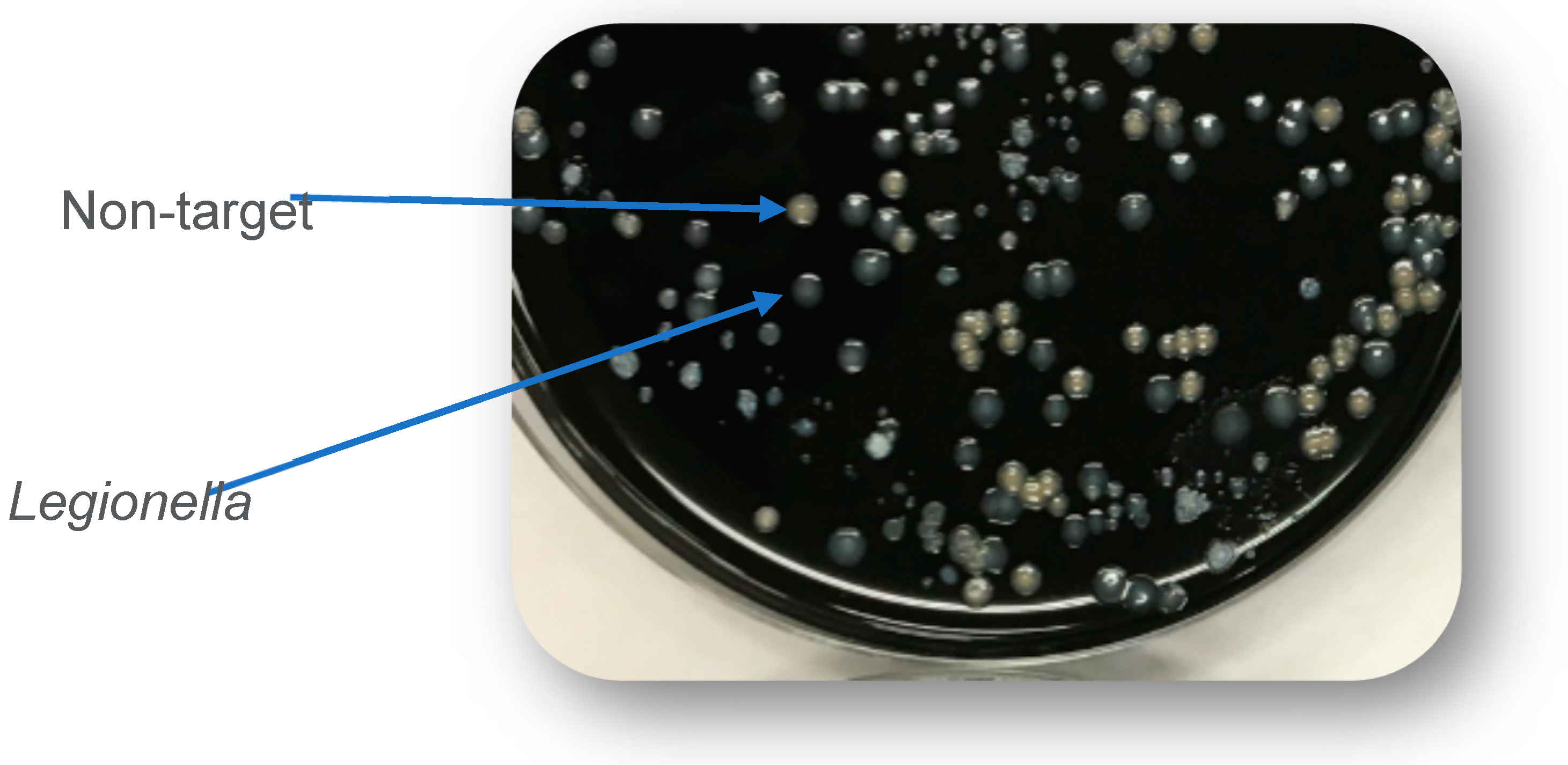
Figure 5.
Relationship between the concentration of Legionella spp. (measured by viability q-PCR) and free chlorine (top) and monochloramine (bottom). The verticle line is drawn at 0.2 mg/L. The number of samples was 122 for free chlorine and 21 for total chlorine. Data from Bartrand et al., [53].
Figure 5.
Relationship between the concentration of Legionella spp. (measured by viability q-PCR) and free chlorine (top) and monochloramine (bottom). The verticle line is drawn at 0.2 mg/L. The number of samples was 122 for free chlorine and 21 for total chlorine. Data from Bartrand et al., [53].
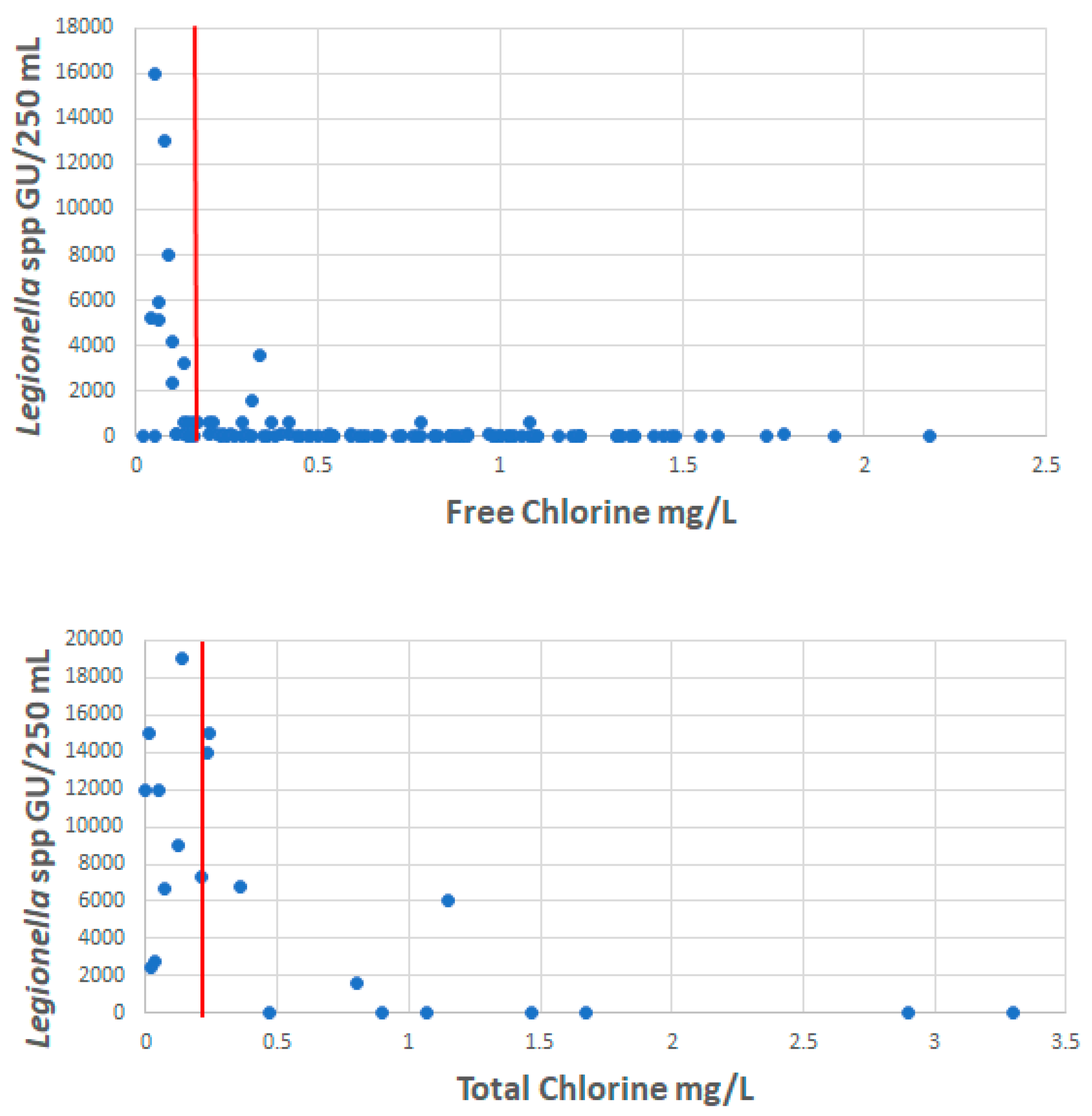

Table 1.
European Centre for Disease Prevention and Control Legionnaires' disease in Europe, Surveillance Report 2020.
Table 1.
European Centre for Disease Prevention and Control Legionnaires' disease in Europe, Surveillance Report 2020.
| Species | Number in 2020 | Percent of Cases |
| L. pneumphila | 843 | 95.2 |
| L. anisa | 1 | 0.1 |
| L. bozemanii | 6 | 0.7 |
| L. longbeachae | 17 | 1.9 |
| L. micdadei | 7 | 0.8 |
| L. other species | 11 | 1.2 |
| L. species unknown | 15 | 1.7 |
Table 2.
Comparison of Methods for Detection of L. pneumophila.
| Drinking Water Distribution System Samples (n=143) | # L. pneumophila positive (Percent) |
|---|---|
| Samples positive by the ISO 11731 method | 0 |
| Samples positive by Legiolert | 1 (0.7%) |
| Samples positive by viability qPCR | 2 (1.4%) |
Adapted from Bartrand et al. [53].
Table 3.
Compilation of Results from Side-by-Side Comparison of Legionella Detection via Different Methods.
Table 3.
Compilation of Results from Side-by-Side Comparison of Legionella Detection via Different Methods.
| Bartrand et al. [53] |
Omoregie et al. [49] |
Wang et al. [54] |
|
|---|---|---|---|
| Samples analyzed | 143 | 544 or 528 1 | 56 |
| Legiolert (L. pneumophila) positive samples (%) | 0.7% | 2.2% | ND |
| ISO method (L. pneumophila) positive samples (%) | 0% | 1.1% | 1.8% |
| viability qPCR/qPCR (L. pneumophila) positive samples (%) | 1.4% | 0.95% | 5.6% |
| Legionella spp. positive samples by v-qPCR2 or qPCR3 (%) | 37% 2 | 84.8% 3 | 86.3% 3 |
1 544 by culture methods, 528 by qPCR; 2 viability qPCR, 3 qPCR. ND, not done.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



