Submitted:
04 July 2024
Posted:
04 July 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Legionella bacteria can proliferate in poorly maintained water systems, posing risks to users. All Legionella species are potentially pathogenic but Legionella pneumophila (L. pneumophila) is usually the primary focus of testing. However, Legionella anisa (L. anisa) also colonises water distribution systems, is frequently found with L. pneumophila and could be a good indicator for increased risk of nosocomial infection. Anonymized data from three commercial Legionella testing laboratories afforded analysis of 565,750 water samples. Data covered July 2019 to August 2021, including the COVID-19 pandemic. Results confirmed L. anisa commonly colonises water distribution systems, being the most frequently identified non-L. pneumophila species. Proportions of L. anisa and L. pneumophila generally remained similar but increases in L. pneumophila during COVID-19 lockdown suggests static water supplies might favour its growth. Disinfection of hospital water systems was effective but re-colonization did occur, appearing to favour L. pneumophila, although L. anisa colony numbers also increased as a proportion of the total. While L. pneumophila remains the main species of concern as a risk to human health, L. anisa’s role should not be under-estimated, either as a potential infection risk or as an indicator of the need to intervene to control Legionella colonization of water supplies.
Keywords:
Legionella pneumophila
; Legionella anisa
; water systems
; hospital
; disinfection and recolonization
; COVID-19 lockdown
1. Introduction
Mains water supplies are intended to be wholesome and safe for drinking, cooking, and bathing, but are not sterile and can contain pathogenic bacteria. If hot and cold water systems (HCWS) are not well designed or managed, then these waterborne pathogens, including Legionella bacteria, can proliferate to an extent that they pose risks to users of the water system [1]. Controlling the growth of legionellae in large buildings, with complex water systems can be challenging, especially if exacerbated by poor designs that make maintaining safe water temperatures problematic, or building modifications or construction materials that encourage development of biofilms and provide pockets within the water system where legionellae can thrive [1].
At least half of all known Legionella species have been shown to cause human disease, but all species are thought potentially to be pathogenic [2]. The major clinical manifestation of infection due to Legionella species is a type of pneumonia known as Legionnaires’ disease (LD), although non-pneumonic legionellosis (Pontiac Fever) and extrapulmonary infection may occur [2]. Legionella pneumophila (L. pneumophila) is the most commonly detected species amongst clinical cases of legionellosis (in USA more than 90% of isolates are L. pneumophila and 83% L. pneumophila serogroup 1 (Sg1) [3]; in the EU 83% of isolates were L. pneumophila Sg1 in 2020 and 82% in 2020 [4]. Other Legionella species have been reported to cause disease but are less well researched [5,6,7]. Non- L. pneumophila species occasionally cause LD [6,8,9], severe pneumonia [10] and Pontiac Fever [11]. In total, 2-7% cases of legionelloses are estimated to be caused by non- L. pneumophila species [12], most of these confirmed infections occurring in immunosuppressed patients [2]. Non- L. pneumophila species are less-commonly detected in clinical diagnoses or during environmental surveillance due to their slow culture growth and the absence of specific and rapid diagnostic/analytical tools [13].
LD outbreaks are more commonly associated with HCWS than with other system types, although this may reflect the higher number of them compared to other water systems in the built environment [14]. As part of an overall water management strategy, periodic sampling and testing for the presence of legionellae in water systems can be extremely valuable in determining whether the microbiological risk controls applied are effective [1]. For the testing of environmental samples, agar plate culture is still the most widely used standard technique for the detection and quantification of viable Legionella spp. [15,16], however, this technique does favour L. pneumophila over non-pneumophila species [17].
While L. pneumophila is usually the primary focus of testing, L. anisa is also a common coloniser of water distribution systems, although an uncommon hospital-acquired pathogen [18]. Non-pneumonic conditions attributable to L. anisa infections have included chronic endocarditis [19], pleural infection [20], osteomyelitis [9] and mycotic aortic aneurysm [21]. L. anisa has been detected in water samples from cooling towers [22,23] and has been identified as the cause of outbreaks of Pontiac Fever associated with a decorative fountain in a hotel lobby and a water feature in a restaurant [24,25], as well as the occasional cases of LD. The French national Legionella reference centre determined that in 2001-2002 L. anisa was the most frequently-identified non- L. pneumophila species, accounting for 13.8% of environmental water sample isolates, but only 0.8% of clinical isolates [26]. This may suggest that L. anisa is less pathogenic to humans than L. pneumophila [26,27], however, there is also likely to be significant under-reporting of clinical cases due to the diagnostic testing undertaken.
This is supported by data from the UKHSA Legionella Reference Laboratory. Examining isolates retained by the laboratory from environmental and clinical samples submitted, and thus associated with clinical infection, over a period from 2004 – 2021 from a total of 2321 environmental samples 2179 (93.9%) were L. pneumophila and 96 (4.14%) were L. anisa, while during the same period from a total of 1360 clinical samples 1327 (97.6%) were L. pneumophila and only one (0.07%) were L. anisa (V. Chalker, UKHSA, pers comm.).
Only 10 cases of Legionellosis associated with L. anisa were reported by national surveillance systems in New Zealand, Australia, Europe, USA and Japan, from a total of 8066 confirmed cases of legionellosis (i.e. <0.1%) [7]. In a multinational survey of community-acquired pneumonia where Legionella was detected in 508 respiratory tract samples, L. anisa only accounted for 0.2% of cases, whilst L. pneumophila accounted for 91.5% of cases [15].
Some Legionella spp may multiply only in specific protozoan hosts and the inability of L. anisa to multiply in human phagocytic cells may be related to the development of Pontiac Fever rather than pneumonic legionellosis in exposed individuals [28]. Further supporting this is a possible association in cooling towers between the presence of the protozoan Acanthamoeba and L. anisa [23].
To identify and trace strains causing legionellosis, it is important to correctly identify and type the Legionella strains in the patient, but even more in the environment with a particular focus on elucidating the potential pathogenic role of non- L. pneumophila species [12]. Because amoebal co-culture may be required for better recovery [29,30] this methodology is less likely to be available for clinical material [2]. All clinical sample test methods have inherent weaknesses for the identification of Legionella, so more than one test method is advised. Testing from a single specimen type limits the ability to diagnose legionellosis, particularly urinary antigen tests (UAT), and in addition these do not allow the matching of patient isolate and environmental samples [31]. While UAT methods for L. pneumophila Sg1 are considered moderately sensitive and highly specific [32], they do not reliably detect infection by species other than L. pneumophila Sg1 [2]. Thus, total dependence on UAT may miss as many as 40% of cases of legionellosis [33]. The number and distribution of infections caused by non- L. pneumophila legionellae are thus underestimated [7] leading to under-diagnosis of both community-acquired and nosocomial Legionella infection [2].
By contrast, in Denmark, more than 80% of LD cases are diagnosed by polymerase chain reaction (PCR), likely increasing the detection of non-Sg1 cases [34]. Denmark has a relatively high frequency of clinical cases caused by L. pneumophila strains that in other countries are more commonly associated with the environment, with non- L. pneumophila species reportedly causing at least 4.5% of all LD cases [27]. In 2010, to increase the sensitivity of testing methods New Zealand adopted PCR as the primary diagnostic tool for all species of Legionella in respiratory samples [7]. In a Spanish study, a total of 210 urine samples from patients with suspected pneumonia were analysed by UAT and also by a semi-nested PCR technique. UAT detected 4 positive samples (1.9%) for L. pneumophila Sg1, while 15 samples tested positive by PCR (7.1%). Of the 15 positive samples, 4 were positive for L. pneumophila, corresponding to the UAT positive samples, 1 sample was positive for L. anisa and a further 10 were positive for unidentifiable Legionella species [6]. In a Colombian study into hospitalised HIV-associated pneumonia patients, Legionella co-infection was found in 17 pneumonia cases. Bronchioalveolar lavage samples from all patients were culture negative for Legionella, but PCR positive, six of the co-infections being with L. anisa and three with L. pneumophila [35].
While culture is still the primary method used to detect legionellae, this has been revolutionized by the application of Matrix-assisted laser desorption ionization-time-of-flight mass spectrometry (MALDI-ToF MS). This is a widely accepted method for identifying bacterial species grown on agar plates, including legionellae [13,27], accurately identifying bacteria routinely isolated in microbiology laboratories with a high positive predictive value ranging in different studies from 95.4% [36] to 99.2% [37] for a range of bacteria and 99.1% specificity for Legionella [38].
Other detection methods, for example, Lateral Flow or Most Probable Number methods, may compare favourably with culture for the detection of L. pneumophila, however, do not detect non- L. pneumophila species, including L. anisa [1,39].
Multiplex PCR assays have been developed which allow simultaneous detection of Legionella species and L. anisa [5].
Regarding the value of responding to an identified problem in the built environment from legionellae other than L. pneumophila, UK health and safety guidance [40] suggests that their presence or growth in a water system could indicate that suitable growth conditions for L. pneumophila have at some point been achieved. As such, these organisms should be seen as indicators of system colonization and appropriate action taken on their detection [15,41].
While L. pneumophila is the species most frequently cultured from the natural environment, other disease-relevant Legionella species such as L. micdadei, L. bozemanii, L. longbeachae and L. anisa have yet to be extensively explored in premise plumbing systems [23], despite L. anisa first being isolated from environmental samples of cooling tower and potable water sources as long ago as 1980 [22]. After L. pneumophila, L. anisa is the Legionella species most frequently detected in the environment [12,26,27,41,42,43,44,45,46,47], including from both hot water systems and cooling tower systems [44].
L. anisa is frequently found in conjunction with L. pneumophila in hospital water systems [48,49,50] and could be a good indicator for increased risk of nosocomial LD [41]. It has also been suggested that presence of a more abundant Legionella population, including L. anisa, in a water system may limit the detection of L. pneumophila, therefore action should be taken to eradicate all Legionella contamination of hospital water distribution systems [2,41].
In a survey of 20 hospitals across 14 US states, nine (45%) of the hospital water systems were found to be colonized with L. anisa with a sample positivity rate of 57/674 (8.5%). There were no diagnosed infections due to L. anisa, but clinical testing of respiratory specimens was not specific to L. anisa [51]. L. anisa was detected in 29 out of 108 (27%) electronic tap water samples at John Hopkins University School of Medicine, Baltimore. This compared to 25 out of 108 (23%) testing positive for L. pneumophila [52]. In a Japanese study of public buildings, more than 40% of hot water distributions examined were contaminated with L. pneumophila and L. anisa [43]. L. anisa persisted in a Japanese hospital water system for at least the 6 years of the study and caused sporadic contamination of shower heads. Regular shower head flushing was insufficient to eradicate the problem and routine shower head replacement was adopted as a control measure [53]. L. anisa in biofilm in hot water systems can be difficult to remove via thermal disinfection [54] and may also show some degree of biocidal resistance in hot water system biofilm when compared to L. pneumophila [46,55]. L. anisa concentrations in water systems can be reduced using chlorine dioxide disinfectant, however, this can be a protracted process [56].
By monitoring both L. pneumophila and non- L. pneumophila species, changes to building management can be made to address potentially different risks at different times of the year. Higher concentrations of Legionella spp. may occur in buildings and hot water taps during periods of lower water use [11]. Poor water circulation and temporary or permanent water stagnation allows Legionella to colonize water systems [57]. Consequently, building shut-downs or reduced occupancy during the Covid-19 pandemic could have increased colonization, and alerts were issued to assess this risk [58]. Interestingly, examining a subset of the UKHSA Reference Laboratory data over a later timeframe of June 2019 to July 2021, thus spanning the Covid-19 lockdown period in the UK, from a total of 393 environmental samples 359 (91.35%) were L. pneumophila and 31 (7.89%) were L. anisa, while during the same period from a total of 204 clinical samples 194 (95.1%) were L. pneumophila but none (0.0%) was L. anisa (V. Chalker, UKHSA, pers comm.).
This paper describes an analysis of routine water testing for Legionella species undertaken by commercial laboratories over a period from July 2019 to August 2021, therefore spanning the pandemic, and the relationship between the presence of L. anisa and L. pneumophila.
2. Materials and Methods
Through the UK trade body the Legionella Control Association, contacts were made with commercial laboratories that undertake routine water testing for Legionella for a range of clients. Following standard protocols [59,60] water samples from premises were regularly and routinely collected from pre-determined sampling points and delivered to the testing laboratory. Here they were treated and used to inoculate agar plates. Suspect Legionella colonies were identified by MALDI-ToF MS.
Three laboratories agreed to share anonymized data, each providing a database of test results with numbers of samples testing positive for L. pneumophila, L. anisa and a range of other Legionella species.
3. Results
Overview
As this study relied on the goodwill of the laboratories to participate, there were some differences in how they were prepared to share their data. One data set provided information on Legionella-positive samples only, while the other two provided information on the total number of samples tested. In two of the three data sets, the Legionella-positive sample data were also broken down by month, one being from July 2019 to August 2021 and the other from January 2020 to June 2021. For the third data set, the results provided were not time-resolved but were from a similar time frame. Although each data set provided a breakdown of Legionella-positive results into a broad range of species, for the purpose of the current analysis the focus was on L. pneumophila and L. anisa, therefore other species were grouped together as ‘other’.
Legionella Data set 1
This data set provided information on Legionella-positive samples only. Between July 2019 and August 2021, nearly 12,000 positive Legionella samples were recorded. As summarized in Figure S1 (Supplementary Materials; available online), the most prevalent species identified in these samples was L. pneumophila (47%). The next most prevalent species identified was L. anisa (46%). These data are presented in Figure 1 as monthly data over the 26 month period.
Over the 26-month period the general proportion of L. anisa and L. pneumophila remained similar. However, there were some months with large differences, most noticeably April and May 2020 and June 2021.
Expressed as a percentage of the total number of Legionella-positive samples, those identified as L. pneumophila ranged from 35% to 70%, with April and May 2020 the largest percentage of the total at 63% and 70% respectively which also corresponded with a dip in the percentage of samples identified as L. anisa (Table S1, Supplementary Material and Figure 2 below). For L. anisa the overall percentage of the total was generally slightly lower than for L. pneumophila and ranged from 23% to 59%. The 23% value in June 2021 corresponded to a month when the percentage of ‘other Legionella species’ was greatest at 26%, seen clearly in Figure 2, which was an outlier from the proportion of ‘other Legionella species’ usually found.
By March 2020, as the COVID-19 pandemic started to have global impact, lockdown restrictions were applied in the UK leading to reduced building occupancy. This may have influenced the number of samples taken and the number of Legionella-positive samples recorded. In Figure 1, an arrow indicates when the UK COVID-19 lockdown began, more specifically from 23rd March 2020. Initially the number of Legionella-positive samples fluctuated between April 2020 and June 2020, before increasing to its highest in July 2020. This may be due to places of employment being closed for a 3 month period, with stagnation of water supplies, before gradually being reopened. Seasonal fluctuations in positive samples is another potential influence, with higher numbers of positives in the warmer summer/ early autumn period. This may be evident to some extent in August 2019 but more evident in July/August 2020 and July 2021, and in the post-lockdown period May to December 2020, where each month had higher numbers of Legionella-positive samples than in any pre-COVID lockdown months in the data set.
Overall, 23% of Legionella-positive samples were taken in the eight months of the data set pre-COVID and 77% in the 18 months post-COVID. However, the proportion of those samples identified as L. anisa did not alter (approximately 46% of Legionella-positive samples; Figure S2, Supplementary Material). A Chi-square test indicates that there is no significant association between Legionella species and Pre/Post-COVID (p=0.467).
Legionella Data set 2
This data set related to an intervention and intensive sampling exercise in a hospital between January 2020 and June 2021. It provided data on the total number of samples taken and the numbers that were Legionella-positive before and after a site-wide disinfection of all hot and cold water systems with hydrogen peroxide. Out of a total of 613 samples taken, 322 were positive for Legionella (52.5%). Overall, 167 of these were pre-cleaning samples (out of 283; 59.0%) and 155 were post-cleaning samples (out of 330; 47.0%). The most prevalent species identified in these samples was L. pneumophila (49%). The next most prevalent species identified was L. anisa (38%). Figure 3 shows the total number of Legionella-positive samples, by species, before and after the cleaning intervention.
Figure 4 shows a monthly breakdown of the data. Although the data spans an 18-month period, the sampling was not undertaken every month, thus data is missing for April 2020, August to October 2020 and January 2021, and no pre-cleaning samples were taken for the first six months (see Table S2, Supplementary Material). Due to relatively low numbers of some sampling results, statistical analysis was not feasible.
Only post-cleaning samples are available that span the two time-frames of pre and post COVID. Overall, 17% of Legionella-positive samples were taken pre-COVID and 83% post-COVID. The proportion of those samples identified as L. anisa roughly halved post-COVID compared to pre-COVID (from 65% of Legionella-positive samples down to 33%). See Figure 5.
Table 1 presents data where there were both pre and post cleaning samples (n = 282). The breakdown between species identified in Legionella-positive samples pre-cleaning are presented across the rows, and for post-cleaning are presented in columns. For example, out of 61 locations, at 18 L. anisa remained the predominant species identified post-cleaning, six changed to L. pneumophila being the predominant species and three to ‘other Legionella’, with 34 locations going from L. anisa being isolated to None Detected. For L. pneumophila, at 54 out of 81 locations L. pneumophila remained the predominant species identified, eight changed to L. anisa being the predominant species and four to ‘other Legionella’, with 15 locations going from L. pneumophila being isolated to None Detected. This meant that L. anisa went from predominating at 61 locations pre-cleaning to 38 locations post-cleaning, and L. pneumophila went from predominating at 81 locations pre-cleaning to 71 locations post-cleaning. Locations where no Legionellae were detected increased from 115 pre-cleaning to 161 post-cleaning.
As well as the number of Legionella-positive samples, this data set also included Legionella-positive colony count data. Between January 2020 and June 2021, there were over 630,000 positive Legionella colonies recorded. Approximately 70% of these were from pre-cleaning samples and 30% were from post-cleaning samples. The most prevalent species identified in these colonies was L. pneumophila (70%). The next most prevalent species identified was L. anisa (20%). See Table 2.
As also seen from Table 2, pre-cleaning, L. anisa made up 17.2% of the total and L. pneumophila 73.8%. Post-cleaning, of a much lower number of colonies (193,869 compared to 437,204), L. anisa made up a larger proportion at 26.4%, up from 17.2% of the total, and the proportion of L. pneumophila was reduced to 64.1%, down from 73.8%. Out of 282 data points that had pre- and post-cleaning colony counts, counts went down in 136 (48.2%) and were unchanged from None Detected in 103 (36.5%) instances. In only 43 (5.2%) instances were colony counts found to increase post-cleaning. Most notable of these were: a shower hose that went from a pre-clean colony count of 842 CFU L. pneumophila Sg1 to 4,400 CFU comprising 400 L. pneumophila Sg1 and 4,000 L. anisa; a shower hose that went from a pre-clean colony count of 779 CFU L. pneumophila Sg1 to 8,667 CFU L. pneumophila Sg1; a cold tap that went from a pre-clean colony count of 1200 CFU L. anisa to 5,000 CFU L. pneumophila Sg1; a shower hose that went from None Detected pre-clean to a colony count of 5,400 CFU L. anisa. Of the 136 data points showing a reduction in colony counts from pre- to post-cleaning, 19 showed a reduction by >5,000 CFU, most notably: a shower hose that went from a pre-clean colony count of 16,421 CFU L. pneumophila Sg1 to 489 CFU L. pneumophila Sg1; a shower hose that went from a pre-clean colony count of 12,600 CFU L. pneumophila Sg1 to 200 CFU L. pneumophila Sg1; a shower hose that went from a pre-clean colony count of 12,400 CFU L. pneumophila Sg1 to 100 CFU L. pneumophila Sg1; a shower hose that went from a pre-clean colony count of 20,000 CFU L. pneumophila Sg1 to 4,600 CFU L. pneumophila Sg1; a shower hose that went from a pre-clean colony count of 44,200 CFU L. pneumophila Sg1 to 4,400 CFU L. pneumophila Sg1; a shower hose that went from a pre-clean colony count of 20,600 CFU L. pneumophila Sg1 to 3,200 CFU L. pneumophila Sg1. Although not statistically proven, the above data indicated that highest counts were greatly reduced by the hydrogen peroxide disinfection intervention.
Most of the sample points were either showers or wash hand basins with taps incorporating thermostatic mixing valves (TMVs). Data in Table S3 (Supplementary Material) summarises how colony counts and the species isolated compares for both these sample types pre- and post-cleaning, and this is expressed graphically in Sankey diagrams in Figure 6 for shower hoses and Figure 7 for TMVs to show species changes.
A greater proportion of TMVs than showers showed no presence of Legionella both pre- and post-cleaning (35.4% compared to 14.9%) and also more changed from having L. pneumophila Sg1 colony counts pre-clean to None Detected post-clean (8.1% compared to 1.4%). The proportion changing from L. anisa colony counts to None Detected was similar for both sample types. Although Legionella colony counts were not being eliminated, the effect of the cleaning intervention on reducing colony counts appeared to be greater with showers – L. pneumophila Sg1 and L. anisa colony counts were reduced in 23% and 12.2% of samples respectively compared to 7.4% and 1.9% respectively in TMVs. Although there were only a few instances where colony counts were increased post-cleaning compared to the same sample point pre-cleaning, there was some indication that showers were more likely to be recolonized. In 5.4% of shower samples L. pneumophila Sg1 remained the predominant colonizing species with counts increased, compared to 3.1% of TMVs. Also in 5.4% of shower samples L. anisa remained the predominant colonizing species with counts increased, compared to 1.2% of TMVs, and 4.1% of shower samples changed from None Detected to L. anisa pre- to post-clean compared to 1.9% of TMVs, also suggesting the possibility that L. anisa had a greater propensity for recolonization.
Only post-cleaning samples were available that span the two time-frames both pre and post COVID. Overall 13% of Legionella-positive sample colonies were identified pre-COVID and 87% post-COVID. The majority of colonies identified pre-COVID were L. anisa (72%), however, post-COVID the majority of colonies were L. pneumophila (77%). See Figure 8.
Legionella Data set 3
This dataset comprised 553,159 water samples in total, submitted by a range of clients for routine Legionella testing. Of these, 60,075 samples were identified as being positive for Legionella (11% of all samples). The most prevalent species identified in these samples was L. anisa (32,517; around 54% of all positive samples or 6% of all samples). This included 202 samples which yielded L. anisa as well as other species. The next most prevalent species identified was L. pneumophila (17,617; 30% of all positive samples or 3% of all samples). In a further 4,162 samples other Legionella species were identified (7% of all positive samples or <1% of all samples). This is presented in Figure 9 and Table 3.
4. Discussion
Through unprecedented access to data made available from three Legionella testing laboratories, analysis was possible on a total of 565,750 water samples tested for Legionella. One data set also provided a species breakdown of Legionella-positive colony counts totaling over 630,000.
The results supported the previously reported view that L. anisa is a common coloniser of water distribution systems and the most frequently-identified non- L. pneumophila species. Identification of L. anisa among non- L. pneumophila species is probably becoming more apparent, as detection methods such as PCR and MALDI-ToF MS allow for more readily achievable speciation of bacteria routinely isolated in microbiology laboratories, and this may be reflected in the data examined.
Some differences in the proportions of L. anisa compared to L. pneumophila were found in the three databases studied. In data set 1, over a 26-month period the general proportion of L. anisa and L. pneumophila remained similar at 46% and 47% respectively. Where this differed, most noticeably in April and May 2020, the proportion of L. pneumophila positive samples increased to 63% and 70% respectively. This may have been a result of samples taken after a period of premises shutdown following the UK COVID-19 lockdown, suggesting static water supplies might favour growth of L. pneumophila. Although a smaller total number of samples were submitted for analysis in April 2020, this should not have influenced the proportions of L. anisa and L. pneumophila.
Although data set 2 spanned the period before and after COVID-19 lockdown, and indicated a large shift in proportion toward L. pneumophila post-COVID, the greatest influence was more likely to have been the intervention of a hospital site-wide disinfection of all hot and cold water systems with hydrogen peroxide, and subsequent re-colonization. Although sampling locations where no Legionella species were detected had increased from 115 pre-cleaning to 161 post-cleaning, where re-colonization was detected post-cleaning it appeared to favour L. pneumophila. L. anisa positive samples went down from 61 to 38, while L. pneumophila positive samples only fell from 81 to 71. However, examining Legionella colony counts showed that the number of L. anisa colonies increased as a proportion of the total from 17.2% to 26.4% post-cleaning, while the proportion of L. pneumophila was reduced from 73.8% to 64.1% of the total. The total colony counts had however reduced from 437,204 pre-cleaning to 193,869 post-cleaning. Showers appeared to be more likely to be colonized than TMVs and to be recolonized post-cleaning, possible more so with L. anisa.
Data set 3, by recording the total number of water samples tested as well as those found to be Legionella positive, gave an insight that positivity rate was around 10%. However, in these samples L. anisa predominated over L. pneumophila, 54.1% of the total compared to 29.3%.
5. Conclusions
The overall picture from three data sets of routine Legionella monitoring of water samples taken from the built environment was that, while the previous focus has tended to be on L. pneumophila, it is clear that L. anisa is also a major contributor. Samples positive for L. anisa were found in a similar proportion to those positive for L. pneumophila in one data set, and in a much greater proportion in another. The results may also support previous hypotheses (Mulder and Yu 2002, van der Mee-Marquet, et al 2005) that the presence of a more abundant Legionella population, including L. anisa, in a water system may limit the detection of L. pneumophila.
There was some evidence that L. anisa colonization of water supplies may be more sensitive to environmental influences; L. pneumophila may have flourished more in water supplies left static over a shutdown period, and have recolonized water supplies after disinfection, although that may differ according to sample type. There was some indication in a hospital water supply that showers may be more dynamic than TMVs in terms of the reduction of both L. pneumophila and L. anisa post-cleaning, but also in terms of recolonization. While L. pneumophila remains the main Legionella species of concern as a risk to human health, the role of L. anisa should not be under-estimated, either as a potential infection risk or as an indicator of the need to intervene to control Legionella colonization of water supplies. As the evidence from these data sets suggests L.anisa colonization of water systems is more prevalent in the UK than previously thought, public health officials dealing with clinical specimens should be encouraged to consider other screening methods in addition to UAT to detect other Legionella species.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, BC and DS; methodology, CY and BC; formal analysis, CY; data curation, DS; writing—original draft preparation, BC and DS; writing—review and editing, DS and CY; visualization, CY; supervision, Becky Gosling (HSE Science and Research Centre); project administration, Kevin Leddy (HSE headquarters, Bootle); funding acquisition, BC and DS. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Health and Safety Executive, project number PH20835.
Institutional Review Board Statement
This study was reviewed by HSE’s Ethics Committee, which is overseen by University of Sheffield, and deemed low risk as data were anonymized at the point of receipt by the authors.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data supporting reported results can be obtained on request from the corresponding author.
Acknowledgments
The authors would like to acknowledge the support of the Legionella Control Association for facilitating dialogue with water testing laboratories, and to the participating water testing laboratories for supplying test data. We also thank Vicky Chalker (UKHSA) for supplying summary clinical data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Walker, J.T.; McDermott, P.J. Confirming the presence of Legionella pneumophila in your water system: a review of current Legionella Testing Methods. Journal of AOAC International 2021, 104, 1135–1147. [Google Scholar] [CrossRef] [PubMed]
- Muder, R.R.; Yu, V.L. Infection Due to Legionella Species Other Than L. pneumophila. Clinical Infectious Diseases 2002, 35, 990–998. [Google Scholar] [CrossRef] [PubMed]
- Kozak-Muiznieks, N.A.; Lucas, C.E.; Brown, E.; Pondo, T.; Taylor Jr, T.H.; Frace, M.; Miskowski, D.; Winchell, J.M. Prevalence of sequence types among clinical and environmental isolates of Legionella pneumophila serogroup 1 in the United States from 1982 to 2012. Journal of clinical microbiology 2014, 52, 201–211. [Google Scholar] [CrossRef] [PubMed]
- ECDC. Legionnaires' disease Annual Epidemiological Report for 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/legionnaires-disease-annual-epidemiological-report-2021 (accessed on 21 May 2024).
- Cross, K.E.; Mercante, J.W.; Benitez, A.J.; Brown, E.W.; Diaz, M.H.; Winchell, J.M. Simultaneous detection of Legionella species and L. anisa, L. bozemanii, L. longbeachae and L. micdadei using conserved primers and multiple probes in a multiplex real-time PCR. Diagn Microbiol Infect Dis. 2016, 85, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Vaccaro, L.; Izquierdo, F.; Magnet, A.; Hurtado, C.; Salinas, M.A.; Gomes, T.S. First Case of Legionnaire's Disease Caused by Legionella anisa in Spain and the Limitations on the Diagnosis of Legionella non-pneumophila Infections. PLoS ONE 2016, 11, e0159726. [Google Scholar] [CrossRef]
- Chambers, S.T.; Slow, S.; Scott-Thomas, A.; Murdoch, D.R. Legionellosis Caused by Non-Legionella pneumophila Species, with a Focus on Legionella longbeachae. Microorganisms 2021, 9, 291. [Google Scholar] [CrossRef]
- Fallon, R.J.; Stack, B.H.R. Legionnaires' disease due to Legionella anisa. Journal of Infection 1990, 20, 227–229. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, M.C.; Sebti, R.; Hassoun, P.; Mannion, C.; Goy, A.H.; Feldman, T.; Mato, A.; Hong, T. Osteomyelitis of the Patella Caused by Legionella anisa. Journal of Clinical Microbiology 2013, 51, 2791–2793. [Google Scholar] [CrossRef] [PubMed]
- Thacker, L.; Benson, R.F.; Hawes, L.; Mayberry, W.R.; Brenner, D.J. Characterization of a Legionella anisa strain isolated from a patient with pneumonia. Journal of Clinical Microbiology 1990, 28, 122–123. [Google Scholar] [CrossRef]
- Logan-Jackson, A.R.; Flood, M.; Rose, J.B. Enumeration and characterization of five pathogenic Legionella species from large research and educational buildings. Environ. Sci.: Water Res. Technol. 2021, 7, 321. [Google Scholar] [CrossRef]
- Mazzotta, M.; Salaris, S.; Pascale, M.R.; Girolamini, L.; Cristino, S. Occurrence of Legionella spp. In Man-MadeWater Sources: Isolates Distribution and Phylogenetic Characterization in the Emilia-Romagna Region. Pathogens 2021, 10, 552. [Google Scholar] [CrossRef] [PubMed]
- Pascale, M.R.; Mazzotta, M.; Salaris, S.; Girolamini, L.; Grottola, A.; Simone, M.L.; Cordovana, M.; Bisognin, F.; Dal Monte, P.; Bucci Sabattini, M.A.; et al. Evaluation of MALDI–TOF Mass Spectrometry in Diagnostic and Environmental Surveillance of Legionella Species: A Comparison with Culture and Mip-Gene Sequencing Technique. Front. Microbiol. 2020, 11, 589369. [Google Scholar] [CrossRef]
- Crook, B.; Willerton, L.; Smith, D.; Wilson, L.; Poran, V.; Helps, J.; McDermott, P. Legionella risk in evaporative cooling systems and underlying causes of associated breaches in health and safety compliance. International Journal of Hygiene and Environmental Health 2020, 224, 113425. [Google Scholar] [CrossRef]
- Yu, V.L.; Plouffe, J.F.; Castellani Pastoris, M.; Stout, J.E.; Schousboe, M.; Widmer, A.; Summersgill, J.; File, T.; Heath, C.M.; Paterson, D.L.; et al. Distribution of Legionella Species and Serogroups Isolated by Culture in Patients with Sporadic Community-Acquired Legionellosis: An International Collaborative Survey. Journal of Infectious Diseases 2002, 186, 127–128. [Google Scholar] [CrossRef] [PubMed]
- Collins, et al S. Collins1,2, F. Jorgensen2, C. Willis2 and J. Walker Real-time PCR to supplement gold-standard culture-based detection of Legionella in environmental samples. Journal of Applied Microbiology 2015, 119, 1158–1169. [CrossRef]
- Lee, T.C.; Vickers, R.M.; Yu, V.L.; Wagener, M.M. Growth of 28 Legionella species on selective culture media: a comparative study. Journal of Clinical Microbiology 1993, 31, 2764–2768. [Google Scholar] [CrossRef] [PubMed]
- Yu, V.L.; Stout, J.E. Legionella anisa and hospital water systems. J Infect Chemother 2004, 10, 133. [Google Scholar] [CrossRef] [PubMed]
- Compain, F.; Bruneval1, P.; Jarraud, S.; Perrot, S.; Aubert, S.; Napoly, V.; Ramahefasolo, A.; Mainardi, J.-L.; Podglajen, I. Chronic endocarditis due to Legionella anisa: a first case difficult to diagnose. New Microbe and New Infect 2015, 8, 113–115. [Google Scholar] [CrossRef]
- Bornstein, N.; Mercatello, A.; Marmet, D.; Surgot, M.; Deveaux, Y.; Fleurette, J. Pleural infection caused by Legionella anisa. Journal of Clinical Microbiology 1989, 27, 2100–2101. [Google Scholar] [CrossRef]
- Tanabe, M.; Nakajima, H.; Nakamura, A.; Ito, T.; Nakamura, M.; Shimono, T.; Wada, H.; Shimpo, H.; Nobori, T.; Ito, M. Mycotic Aortic Aneurysm Associated with Legionella anisa. Journal of Clinical Microbiology 2009, 47, 2340–2343. [Google Scholar] [CrossRef]
- Gorman, G.W.; Feeley, J.C.; Steigerwalt, A.; Edelstein, P.H.; Moss, W.; Brenner, D.J. Legionella anisa: a new species of Legionella isolated from potable waters and a cooling tower. Applied and Environmental Microbiology 1985, 49, 305–309. [Google Scholar] [CrossRef]
- Logan-Jackson, A.; Rose, J.B. Co-occurrence of Five Pathogenic Legionella spp. and Two Free-Living Amoebae Species in a Complete Drinking Water System and Cooling Towers. Pathogens 2021, 10, 1407. [Google Scholar] [CrossRef] [PubMed]
- Fenstersheib, M.D.; Miller, M.; Diggins, C.; Liska, S.; Detwiler, L.; Werner, S.B.; Lindquist, D.; Thacker, W.L.; Benson, R.F. Outbreak of Pontiac fever due to Legionella anisa. Lancet 1990, 336, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.F.; Benson, R.F.; Brown, E.W.; Rowland, J.R.; Crosier, S.C.; Schaffner, W. Epidemiologic Investigation of a Restaurant- Associated Outbreak of Pontiac Fever. Clinical Infectious Diseases 2003, 37, 1292–1297. [Google Scholar] [CrossRef] [PubMed]
- Doleans, A.; Aurell, H.; Reyrolle, M.; Lina, G.; Freney, J.; Vandenesch, F.; Etienne, J.; Jarraud, S. Clinical and Environmental Distributions of Legionella Strains in France Are Different. Journal of Clinical Microbiology 2004, 42, 458–460. [Google Scholar] [CrossRef]
- Svarrer, C.W.; Uldum, S.A. The occurrence of Legionella species other than Legionella pneumophila in clinical and environmental samples in Denmark identified by mip gene sequencing and matrix-assisted laser desorption ionization time-of-flight mass spectrometry. Clin Microbiol Infect 2012, 18, 1004–1009. [Google Scholar] [CrossRef] [PubMed]
- Fields, B.S.; Barbaree, J.M.; Sanden, G.N.; Morrill, W.E. Virulence of a Legionella anisa Strain Associated with Pontiac Fever: an Evaluation Using Protozoan, Cell Culture, and Guinea Pig Models. Infection and Immunity 1990, 58, 3139–3142. [Google Scholar] [CrossRef] [PubMed]
- La Scola, B.; Mezi, L.; Weiller, P.J.; Raoult, D. Isolation of Legionella anisa Using an Amoebic Coculture Procedure. 39Journal of Clinical Microbiology 2001, 39, 365–366. [Google Scholar] [CrossRef] [PubMed]
- Pagnier, I.; Croce, O.; Robert, C.; Raoult, D.; La Scola, B. Genome sequence of Legionella anisa, isolated from a respiratory sample, using an amoebal coculture procedure. Genome Announc. 2014, 2, e00031-14. [Google Scholar] [CrossRef]
- Peci, A.; Winter, A.-L.; Gubbay, J.B. Evaluation and Comparison of Multiple Test Methods, Including Real-time PCR, for Legionella Detection in Clinical Specimens. Front. Public Health 2016, 4, 175. [Google Scholar] [CrossRef]
- Kawasaki, T.; Nakagawa, N.; Murata, M.; Yasuo, S.; Yoshida, T.; Ando, K.; Okamori, S.; Okada, Y. Diagnostic accuracy of urinary antigen tests for legionellosis; a systematic review and meta-analysis. Respiratory Investigation 2021. [Google Scholar] [CrossRef] [PubMed]
- Fields, B.S.; Benson, R.F.; Besser, R.E. Legionella and Legionnaires’ Disease: 25 Years of Investigation. Clinical Microbiology Reviews 2002, 15, 506–526. [Google Scholar] [CrossRef]
- Uldum, S.A.; Schjoldager, L.G.; Baig, S.; Cassell, K. A Tale of Four Danish Cities: Legionella pneumophila Diversity in Domestic Hot Water and Spatial Variations in Disease Incidence. Int. J. Environ. Res. Public Health 2022, 19, 2530. [Google Scholar] [CrossRef]
- Head, B.M.; Trajtman, A.; Bernard, K.; Burdz, T.; Vélez, L.; Herrera, M.; Rueda, Z.V.; Keynan, Y. Legionella co-infection in HIV-associated pneumonia. Diagnostic Microbiology and Infectious Disease 2019, 95, 71–76. [Google Scholar] [CrossRef]
- Seng, P.; Drancourt, M.; Gouriet, F.; La Scola, B.; Fournier, P.-E.; Rolain, J.M.; Raoult, D. Ongoing Revolution in Bacteriology: Routine Identification of Bacteria by Matrix-Assisted Laser Desorption Ionization Time-of-Flight Mass Spectrometry. Clinical Infectious Diseases 2009, 49, 543–551. [Google Scholar] [CrossRef] [PubMed]
- La Scola, B.; Raoult, D. Direct Identification of Bacteria in Positive Blood Culture Bottles by Matrix-Assisted Laser Desorption Ionisation Time-of-Flight Mass Spectrometry. PLoS ONE 2009, 4, e8041. [Google Scholar] [CrossRef]
- Gaiaa, V.; Casatia, S.; Tonolla, M. Rapid identification of Legionella spp. By MALDI-TOF MS based protein mass fingerprinting. Systematic and Applied Microbiology 2011. [Google Scholar] [CrossRef] [PubMed]
- Boczek, L.A.; Tang, M.; Formal, C.; Lytle, D.; Ryu, H. Comparison of two culture methods for the enumeration of Legionella pneumophila from potable water samples. Journal of Water and Health 2021, 19, 468–477. [Google Scholar] [CrossRef]
- Health and Safety Executive. Legionnaires’ disease Technical guidance HSG274 Part 2: The control of Legionella bacteria in hot and cold water systems. Available online: https://www.hse.gov.uk/pubns/books/hsg274.htm (accessed on 21 May 2024).
- van der Mee-Marquet, N.; Domelier, A.-S.; Arnault, L.; Bloc, D.; Laudat, P.; Hartemann, P.; Quentin, R. Legionella anisa, a Possible Indicator of Water Contamination by Legionella pneumophila. Journal of Clinical Microbiology 2006, 44, 56–59. [Google Scholar] [CrossRef]
- Wilkinson, I.J.; Sangster, N.; Ratcliff, R.M.; Mugg, P.A.; Davos, D.E.; Lanser, J.E. Problems Associated with Identification of Legionella Species from the Environment and Isolation of Six Possible New Species. Applied and Environmental Microbiology 1990, 56, 796–802. [Google Scholar] [CrossRef]
- Edagawa1, A.; Kimura, A.; Doi, H.; Tanaka, H.; Tomioka, K.; Sakabe, K.; Nakajima, C.; Suzuki, Y. Detection of culturable and nonculturable Legionella species from hot water systems of public buildings in Japan. Journal of Applied Microbiology 2008, 105, 2104–2114. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.K.; Shim, J.I.; Kim, H.E.; Yu, J.Y.; Kang, Y.H. Distribution of Legionella Species from Environmental Water Sources of Public Facilities and Genetic Diversity of L. pneumophila Serogroup 1 in South Korea. Applied and Environmental Microbiology 2010, 76, 6547–6554. [Google Scholar] [CrossRef] [PubMed]
- Fleres, G.; Couto, N.; Lokate, M.; van der Sluis, L.W.M.; Ginevra, C.; Jarraud, S.; Deurenberg, R.H.; Rossen, J.W.; García-Cobos, S.; Friedrich, A.W. Detection of Legionella anisa in Water from Hospital Dental Chair Units and Molecular Characterization by Whole-Genome Sequencing. Microorganisms 2018, 6, 71. [Google Scholar] [CrossRef]
- Girolamini, L.; Salaris, S.; Pascale, M.R.; Mazzotta, M.; Cristino, S. Dynamics of Legionella Community Interactions in Response to Temperature and Disinfection Treatment: 7 Years of Investigation. Microbial Ecology 2021. [Google Scholar] [CrossRef]
- Salinas, M.B.; Fenoy, S.; Magnet, A.; Vaccaro, L.; Gomes, T.D.S.; Angulo, S.; Hurtado, C.; Ollero, D.; Valdivieso, E.; del Águila, D.; et al. Are pathogenic Legionella non- pneumophila a common bacteria in Water Distribution Networks? Water Res 2021, 196, 117013. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.S.S.; Caiaffa Filho, H.H.; Sinto, S.I.; Sabbaga, E.; Barone, A.A.; Mendes, C.M.F. An outbreak of nosocomial Legionnaires’ disease in a renal transplant unit in Sao Paulo, Brazil. Journal of Hospital Infection 1991, 18, 243–248. [Google Scholar] [CrossRef]
- Koide, M.; Owan, T.; Nakasone, C.; Yamamoto, N.; Haranaga, S.; Higa, F.; Tateyama, M.; Yamane, N.; Fujita, J. Prospective Monitoring Study: Isolating Legionella pneumophila in a Hospital Water System Located in the Obstetrics and Gynecology Ward after Eradication of Legionella anisa and Reconstruction of Shower Units. Jpn. J. Infect. Dis. 2007, 60, 5–9. [Google Scholar] [CrossRef]
- Girolamini, L.; Salaris, S.; Lizzadro, J.; Mazzotta, M.; Pascale, M.R.; Pellati, T.; Cristino, S. How Molecular Typing Can Support Legionella Environmental Surveillance in Hot Water Distribution Systems: A Hospital Experience. Int. J. Environ. Res. Public Health 2020, 17, 8662. [Google Scholar] [CrossRef] [PubMed]
- Stout, J.E.; Muder, R.R.; Mietzner, S.; Wagener, M.M.; Perri, M.B.; DeRoos, K.; Goodrich, D.; Arnold, W.; Williamson, T.; Ruark, O.; et al. Role of Environmental Surveillance in Determining the Risk of Hospital-Acquired Legionellosis: A National Surveillance Study with Clinical Correlations. Infect Control Hosp Epidemiol 2007, 28, 818–824. [Google Scholar] [CrossRef]
- Syndnor, E.R.M.; Bova, G.; Gimburg, A.; Cosgrove, S.E.; Perl, T.M.; Maragakis, L.L. Electronic-eye faucets; Legionella species contamination in healthcare settings. Infection Control and Hospital Epidemiology 2012, 33, 235–240. [Google Scholar] [CrossRef]
- Yamamoto, N.; Kubota, T.; Tateyama, M.; Koide, M.; Nakasone, C.; Tohyama, M.; Shinzato, T.; Higa, F.; Kusano, N.; Kawakami, K.; et al. Isolation of Legionella anisa from multiple sites of a hospital water system: the eradication of Legionella contamination. J Infect Chemother 2003, 2003 9, 122–125. [Google Scholar] [CrossRef]
- Krøjgaard, L.H.; Krogfelt, K.A.; Albrechtsen, H.J.; Uldum, S.A. Cluster of Legionnaires’ disease in a newly built block of flats, Denmark, December 2008 – January 2009. Euro Surveill. 2011, 16, 19759. [Google Scholar] [CrossRef] [PubMed]
- Farhat, M.; Moletta-Denat, M.; Frère, J.; Onillon, S.; Trouilhé, M.-C.; Robinea, E. Effects of Disinfection on Legionella spp., Eukarya, and Biofilms in a Hot Water System. Applied and Environmental Microbiology 2012, 78, 6850–6858. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.E.; Stout, J.E.; Yu, V.L. Controlling Legionella in Hospital Drinking Water: An Evidence-Based Review of Disinfection Methods. Infection Control and Hospital Epidemiology 2011, 32, 166–173. [Google Scholar] [CrossRef]
- Nisar, M.A.; Ross, K.E.; Brown, M.H.; Bentham, R.; Whiley, H. Water Stagnation and Flow Obstruction Reduces the Quality of Potable Water and Increases the Risk of Legionelloses. Front. Environ. Sci. 2020, 8, 611611. [Google Scholar] [CrossRef]
- Legionella Control Association webinar – Legionella dangers emerging from lockdown. Available online: https://www.legionellacontrol.org.uk/video-media/view/?id=17 (accessed on 15 January 2024).
- British Standard BS7592:2022; Sampling for Legionella bacteria in water systems — Code of practice.
- British Standard BS EN ISO 11731:2017. Water quality — Enumeration of Legionella.
Figure 1.
Data Set 1 - Total number of Legionella-positive samples recorded, by date and species.
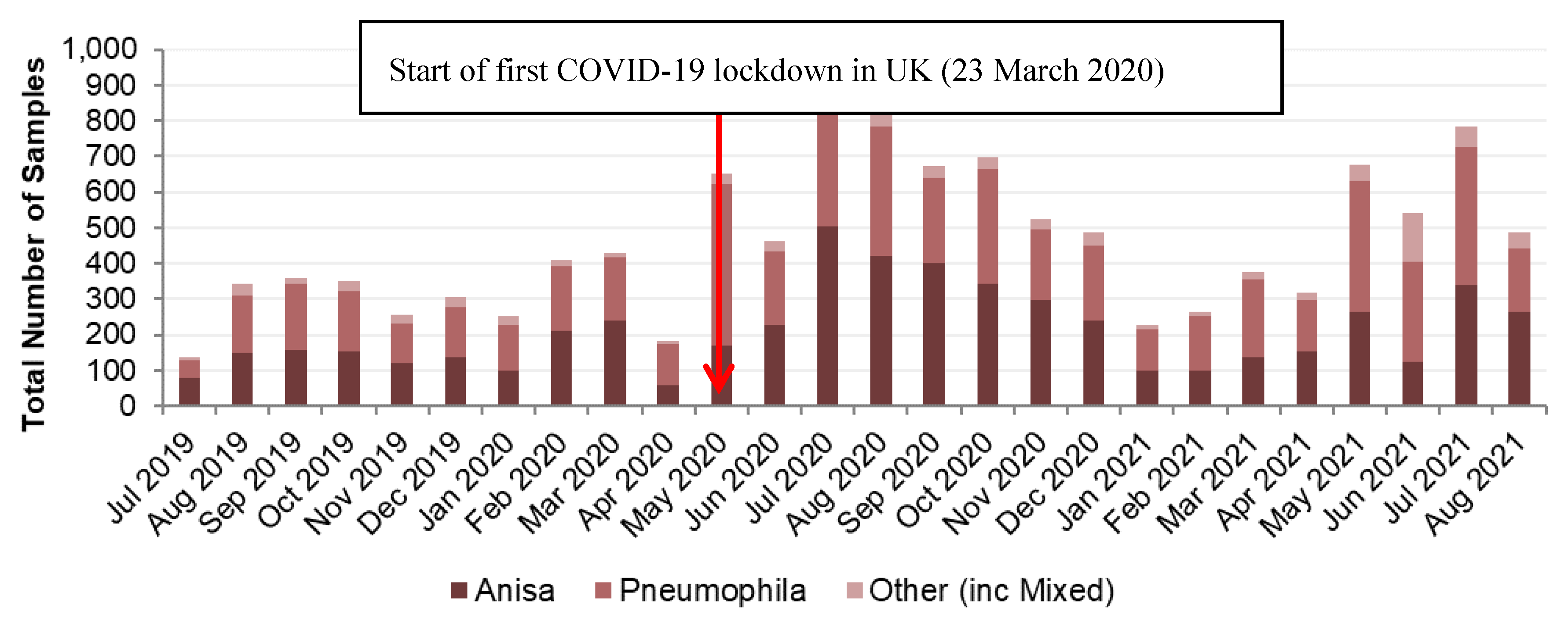
Figure 2.
Data Set 1 - Proportion of Legionella-positive samples recorded, by date and species.
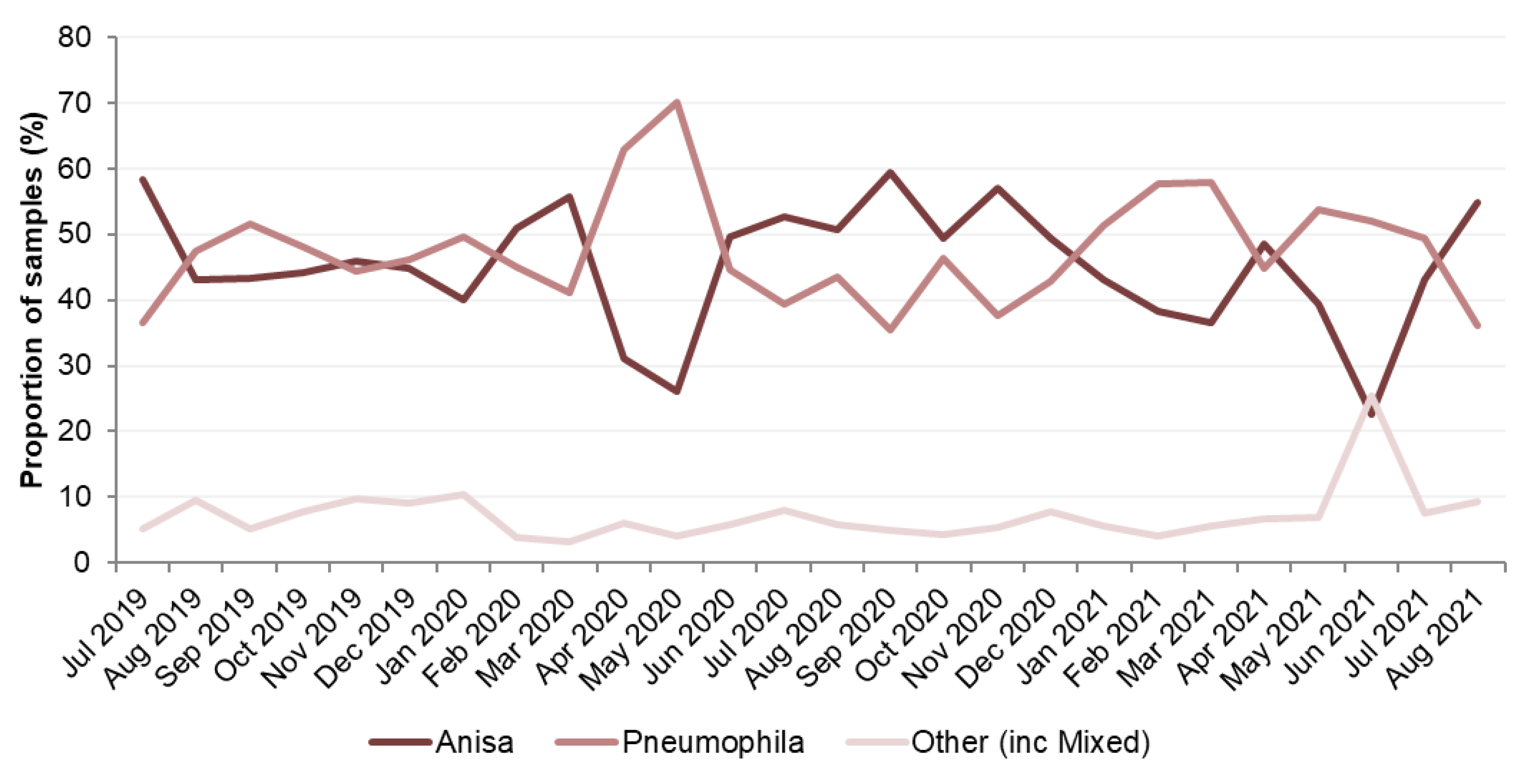
Figure 3.
Data Set 2 - Total number of Legionella-positive samples recorded, by species for pre and post cleaning.
Figure 3.
Data Set 2 - Total number of Legionella-positive samples recorded, by species for pre and post cleaning.
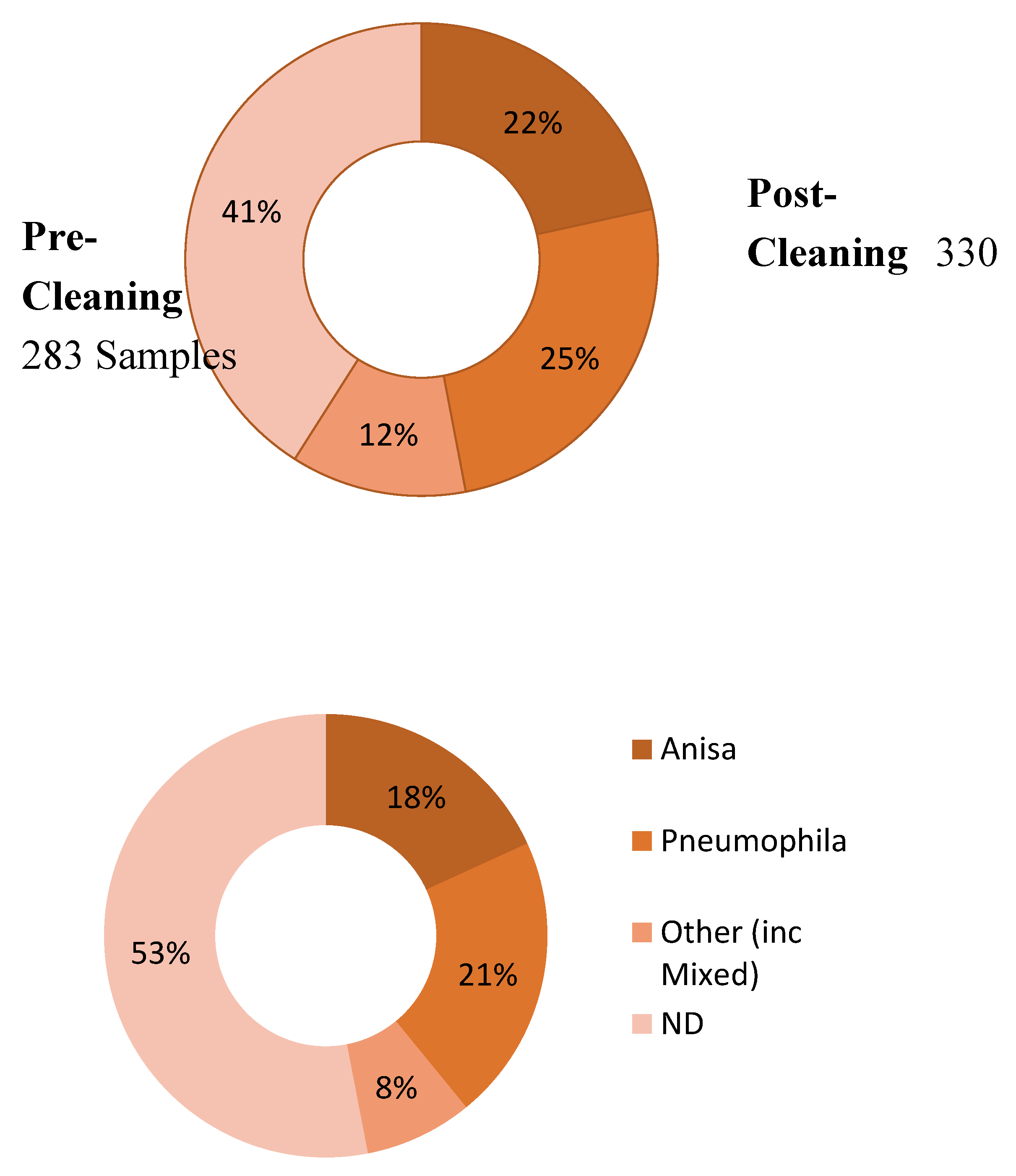
Figure 4.
Data Set 2 - Total number of Legionella-positive samples recorded, by date for pre and post cleaning.
Figure 4.
Data Set 2 - Total number of Legionella-positive samples recorded, by date for pre and post cleaning.
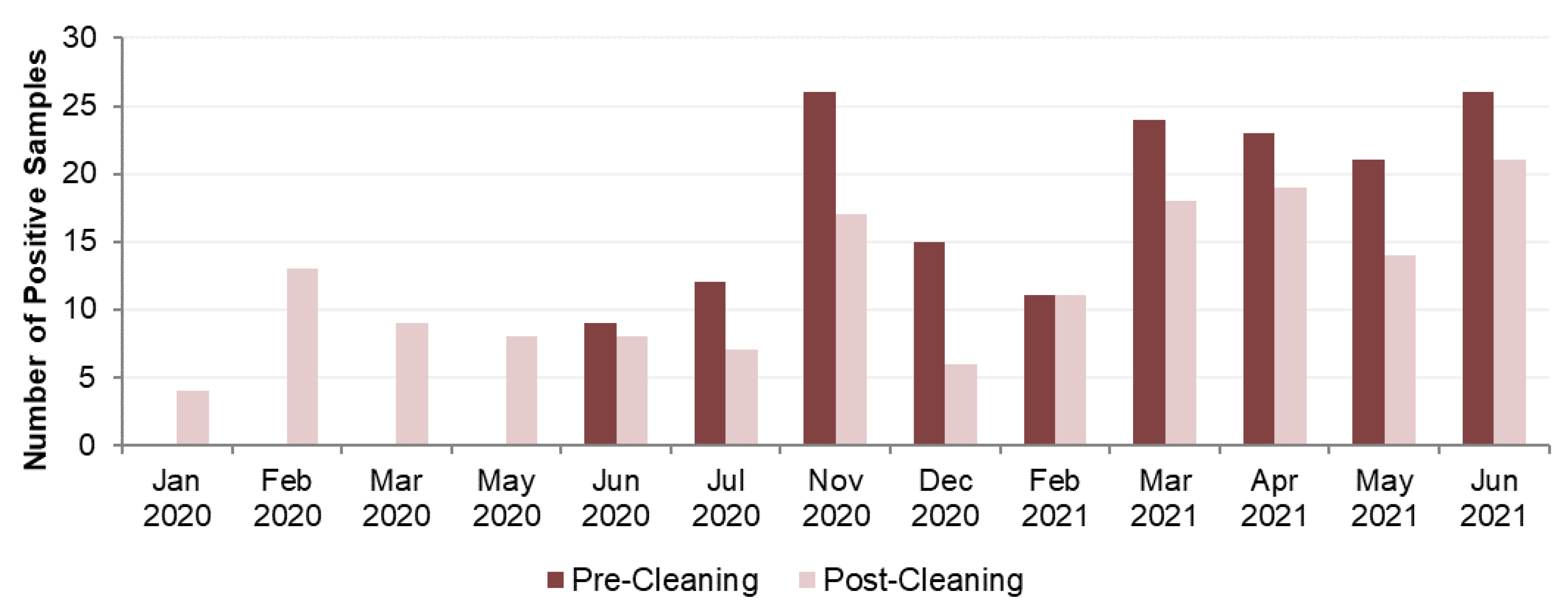
Figure 5.
Data Set 2 -Number of Legionella-positive samples recorded before and after the COVID-19 outbreak, by species.
Figure 5.
Data Set 2 -Number of Legionella-positive samples recorded before and after the COVID-19 outbreak, by species.
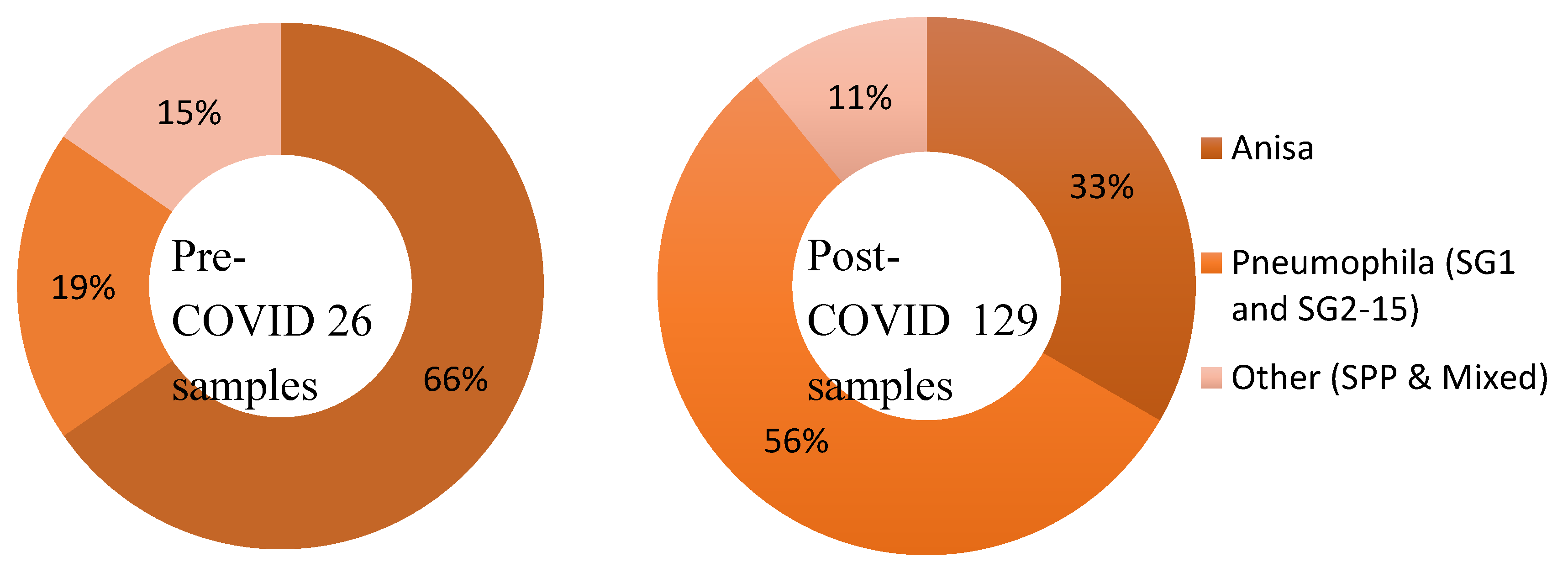
Figure 6.
Data Set 2 – Changes in species isolated pre- and post-cleaning in shower hoses .
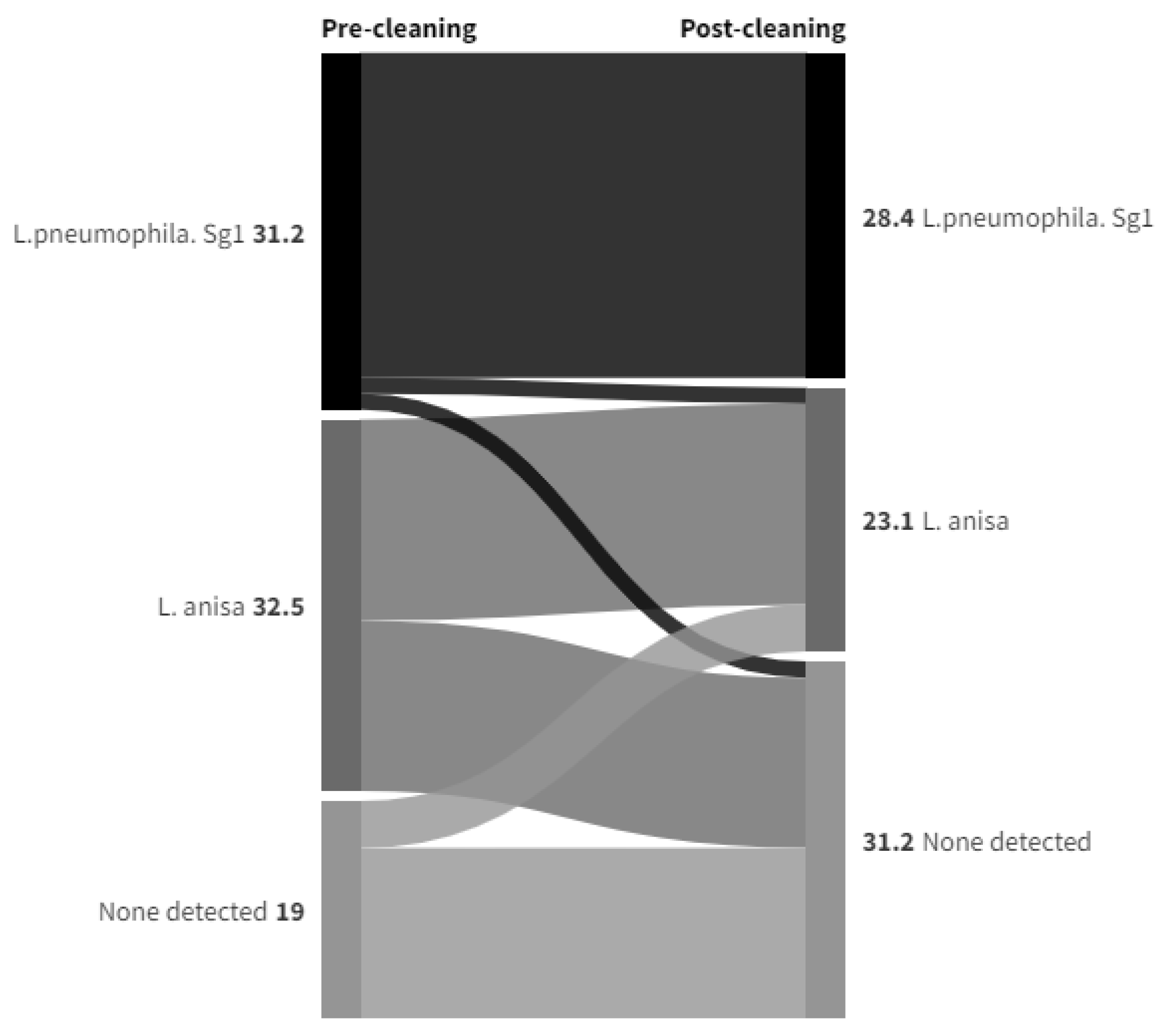
Figure 7.
Data Set 2 – Changes in species isolated pre- and post-cleaning in TMVs .
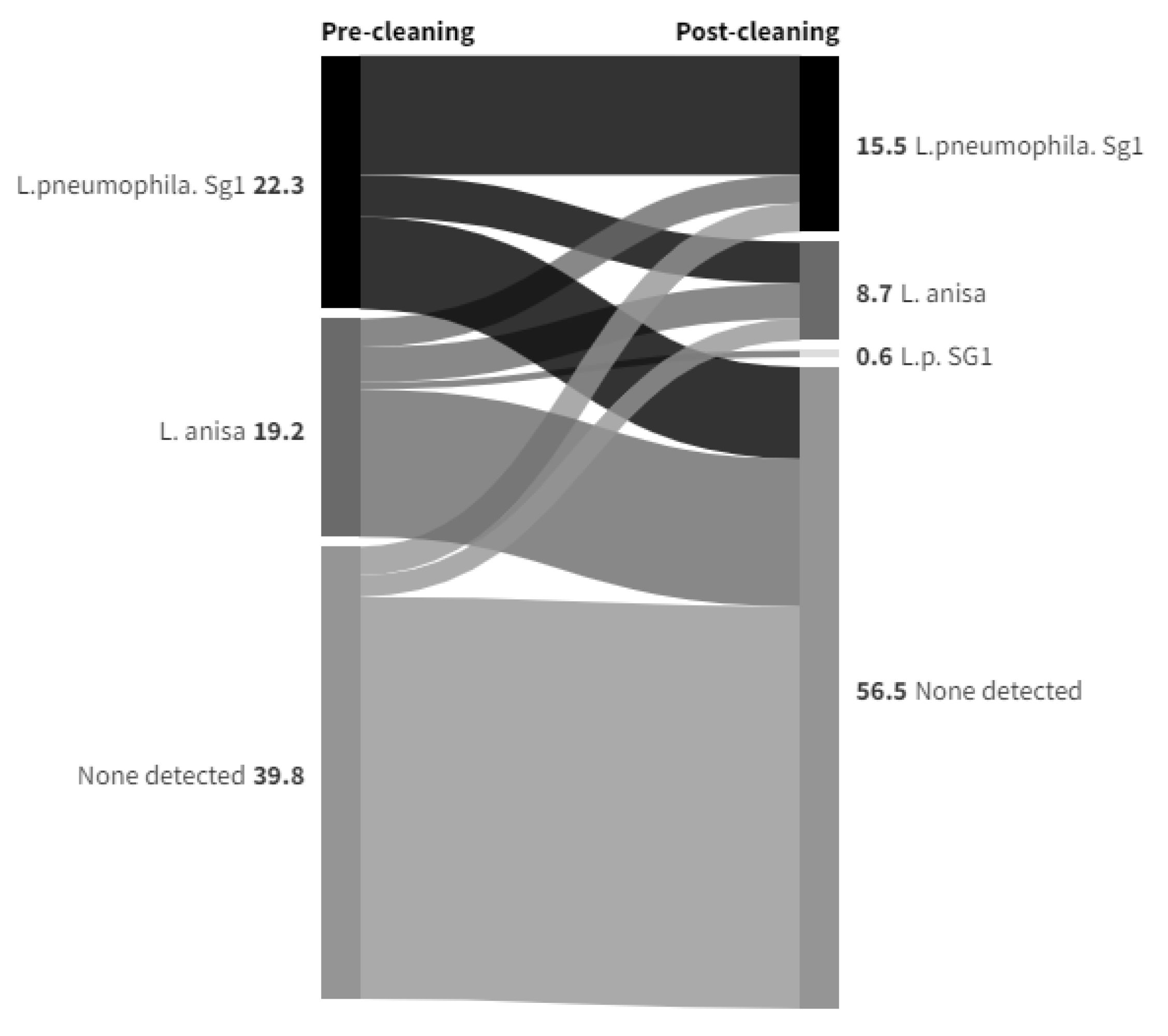
Figure 8.
Data Set 2 - Number of Legionella-positive samples recorded before and after the COVID-19 outbreak, by species.
Figure 8.
Data Set 2 - Number of Legionella-positive samples recorded before and after the COVID-19 outbreak, by species.
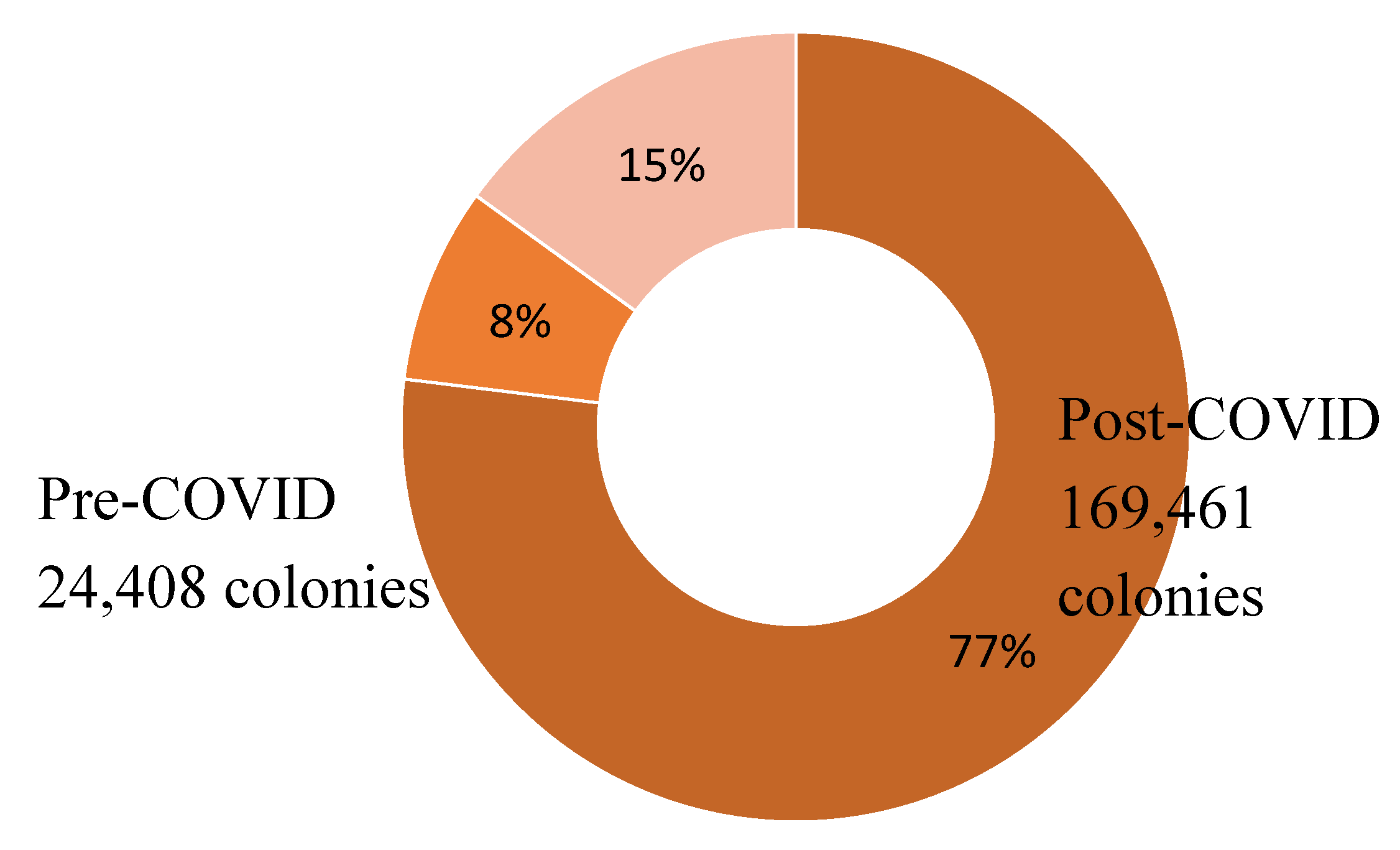
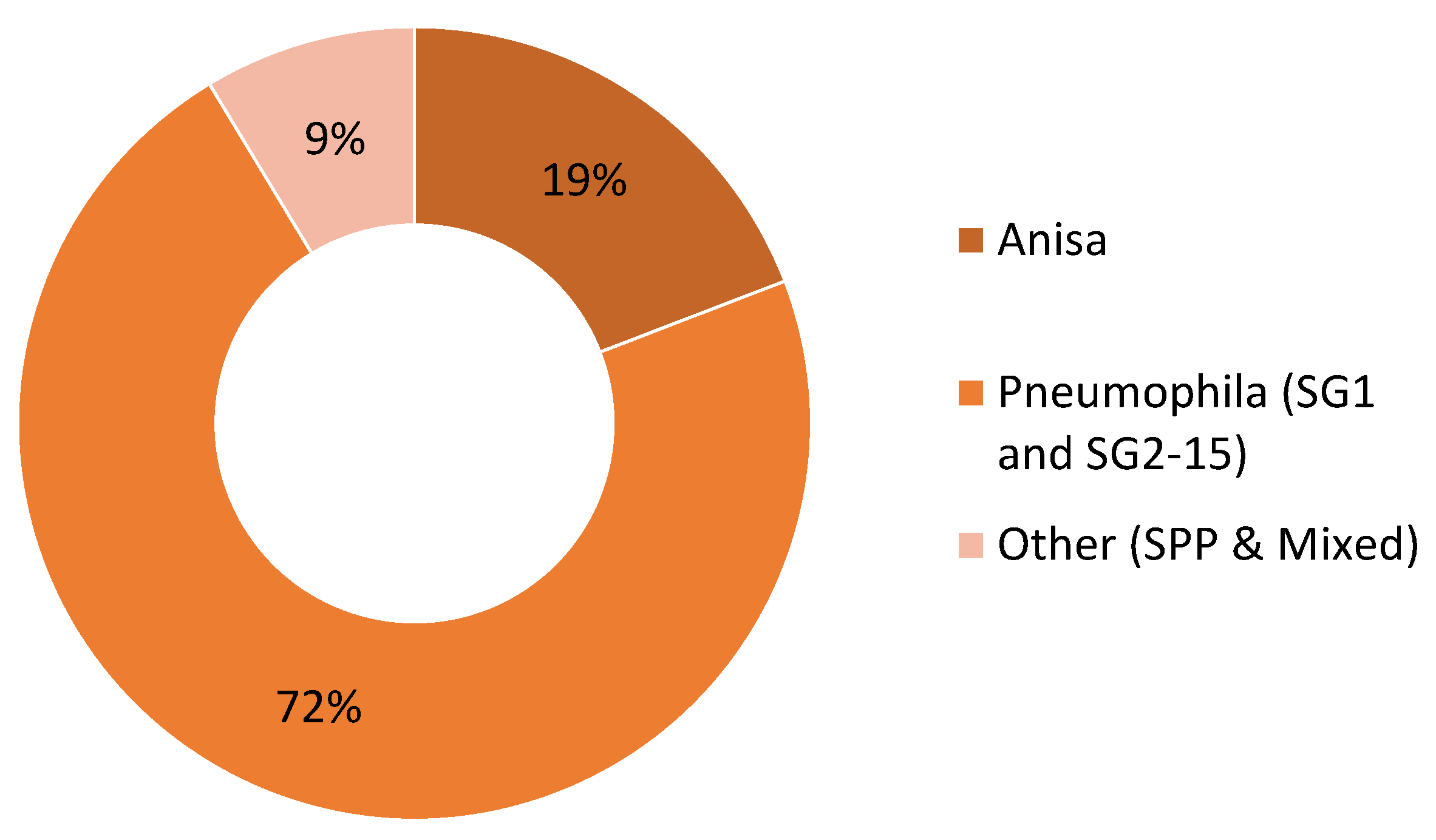
Figure 9.
Data Set 3 - Total number of Legionella-positive samples recorded, by species.
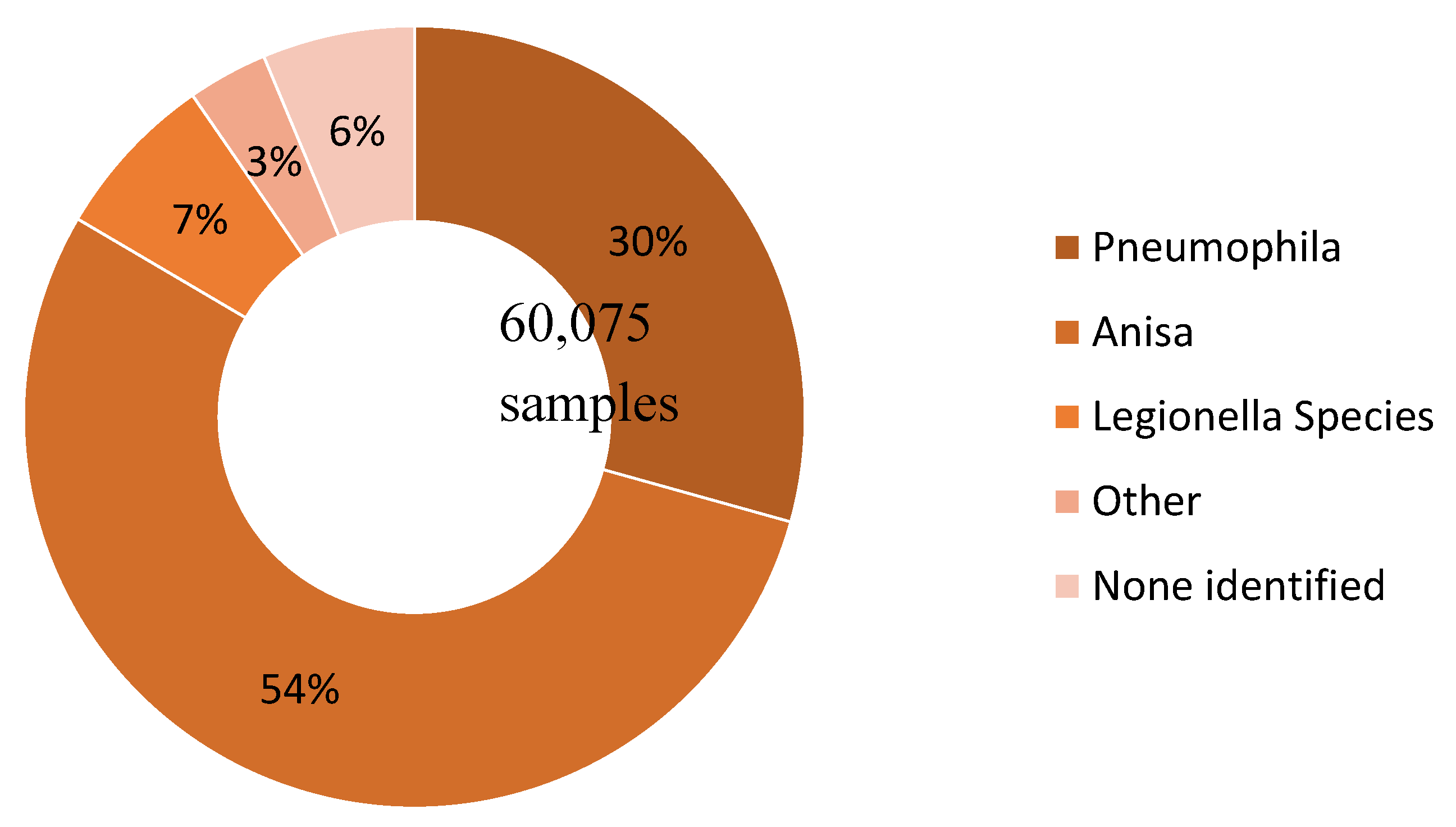

Table 1.
Data Set 2 - The effect of cleaning on the species identified in the Legionella-positive samples.
Table 1.
Data Set 2 - The effect of cleaning on the species identified in the Legionella-positive samples.
| Post-Cleaning Sample | Grand Total | |||||
|---|---|---|---|---|---|---|
| Anisa | Pneumophila | Other | ND | |||
| Pre-Cleaning Sample | Anisa | 18 | 6 | 3 | 34 | 61 |
| Pneumophila | 8 | 54 | 4 | 15 | 81 | |
| Other | 6 | 6 | 4 | 9 | 25 | |
| ND | 6 | 5 | 1 | 103 | 115 | |
| Grand Total | 38 | 71 | 12 | 161 | 282 | |
Table 2.
Data Set 2 - Total number of colonies recorded, by date and species for pre and post cleaning.
Table 2.
Data Set 2 - Total number of colonies recorded, by date and species for pre and post cleaning.
| Date | Pre-Cleaning Sample Colonies | Post-Cleaning Sample Colonies | ||||||
|---|---|---|---|---|---|---|---|---|
| Anisa | Pneumophila | Other | Total | Anisa | Pneumophila | Other | Total | |
| Jan 2020 | 40 | 1,520 | 0 | 1,560 | ||||
| Feb 2020 | 12,920 | 80 | 1,268 | 14,268 | ||||
| Mar 2020 | 5,820 | 360 | 2,400 | 8,580 | ||||
| May 2020 | 2,920 | 2,120 | 1,460 | 6,500 | ||||
| Jun 2020 | 4,762 | 7,630 | 0 | 12,392 | 3,081 | 1,540 | 0 | 4,621 |
| Jul 2020 | 3,180 | 460 | 6,400 | 10,040 | 3,340 | 0 | 180 | 3,520 |
| Nov 2020 | 11,080 | 25,080 | 4,200 | 40,360 | 1,260 | 10,820 | 1,400 | 13,480 |
| Dec 2020 | 2,520 | 8,280 | 0 | 10,800 | 120 | 3,180 | 0 | 3,300 |
| Feb 2021 | 2,821 | 26,496 | 0 | 29,317 | 408 | 19,635 | 4,400 | 24,443 |
| Mar 2021 | 11,673 | 50,127 | 2,120 | 63,920 | 8,937 | 37,380 | 0 | 46,317 |
| Apr 2021 | 28,875 | 39,480 | 17,260 | 85,615 | 940 | 11,540 | 3,860 | 16,340 |
| May 2021 | 3,400 | 111,440 | 0 | 114,840 | 0 | 20,880 | 200 | 21,080 |
| Jun 2021 | 6,680 | 53,540 | 9,700 | 69,920 | 11,460 | 15,240 | 3,160 | 29,860 |
| Total | 74,991 | 322,533 | 39,680 | 437,204 | 51,246 | 124,295 | 18,328 | 193,869 |
Table 3.
Data Set 3 - Total number of Legionella-positive samples recorded, by species.
| Species Detected | Count | (Proportion) |
|---|---|---|
| Legionella pneumophila | 17,617 | (29.3%) |
| Legionella anisa | 32,517 | (54.1%) |
| Legionella species | 4,162 | (6.9%) |
| Other | 1,992 | (3.3%) |
| Blank (no species identified) | 3,787 | (6.3%) |
| TOTAL | 60,075 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



