
Submitted:
18 January 2025
Posted:
20 January 2025
You are already at the latest version
Abstract
Background: This study focuses on the prevalence of Acinetobacter baumannii (A. baumannii) among the hospitalized patients in various hospital departments including ICU, Emergency, Kidney Dialysis units and other departments and its molecular characterization. Objectives: The study aims to isolate and identify A. baumannii strains, investigate their resistance to various antibiotics, and analyze the genes responsible for this resistance using molecular techniques such as polymerase chain reaction (PCR). Methodology: A total of 100 samples were collected from different hospital departments, including the ICU, emergency room, and kidney dialysis units. The study found a high prevalence of MDR A. baumannii isolates, especially in ICU patients. Results: The males were the predominant group, accounting for 60 (60%), while females were 40(40%). The most frequent samples are from urine (43%) and skin (24%). Smaller percentages of samples are pus (12%) and ulcers (5%). Most of the collected samples are from the ICU (42%) and emergency departments (20%). A notable number is also from kidney dialysis units (15%) and environmental sources (13%). Molecular analysis revealed the presence of several resistance genes, including blaOXA-23, blaOXA-24, blaOXA-51, and blaOXA-58, which contribute to carbapenem resistance. Conclusion: The findings emphasize the urgent need for improved infection control measures, antibiotic stewardship, and the development of targeted treatment protocols to mitigate the spread of MDR infections in healthcare settings.
Keywords:
Acinetobacter baumannii
; polymerase chain reaction
; MDR infections
; antimicrobial susceptibility test
Introduction
Acinetobacter baumannii (A. baumannii) is a Gram-negative bacterium associated with hospital-acquired infections, particularly in intensive care units (ICUs). This microorganism is recognized for its significant potential to develop multiple-drug resistance, posing considerable challenges for healthcare practitioners [1]. The prevalence of A. baumannii in ICU settings has risen significantly, contributing to higher morbidity and mortality rates among critically ill patients [2].” “Governmental hospitals in Jordan have observed a rise in infections caused by A. baumannii. Considering the severity of cases in ICUs and the pathogen’s robust resistance mechanisms, implementing effective strategies for disease management has become imperative [3].
The present study involves the epidemiological investigation and antibiotic resistance profiles of A. baumannii and its molecular characterization. These techniques provide insights into genetic variation, distribution patterns, and potential treatment strategies in combating infection [4]. “The increasing prevalence of multidrug-resistant bacteria in healthcare presents a significant global challenge, undermining the efficacy of standard antibiotics and emphasizing the urgent need for ongoing monitoring and advanced diagnostic solutions [5]. “Analyzing the molecular characteristics and antibiotic susceptibilities of A. baumannii is crucial for effective clinical management and infection control strategies in Jordanian governmental hospitals, where healthcare complexities are compounded by resource limitations. A. baumannii is a highly aerobic, nonfermenting coccobacillus belonging to the Moraxellaceae family, initially identified in 1911 as Micrococcus calco-aceticus [6]. Acinetobacter, a genus of opportunistic pathogens, is becoming more common in both community-acquired and nosocomial infections, especially among patients in ICUs and high-dependency units [7].” “A. baumannii has garnered significant attention due to its ability to persist in hospital environments and acquire resistance to multiple classes of antibiotics [6]. The capacity to form biofilms on medical devices, combined with inherent defense mechanisms and the propensity for horizontal gene transfer, establishes it as a formidable pathogen responsible for various infections. These include ventilator-associated pneumonia, mild skin and soft tissue infections, severe bloodstream infections, infections related to prosthetic devices, and pneumonia, especially in immunocompromised and critically ill patients [8,9].”
These efforts are crucial for guiding antibiotic therapy, informing infection control strategies, enhancing patient outcomes, and preventing the dissemination of resistant strains within healthcare environments.” “The current study aims to address knowledge gaps through a systematic analysis of the molecular characteristics and antibiotic susceptibilities of A. baumannii isolates obtained from hospitalized patients in Jordanian government hospitals. Employing advanced molecular techniques, including polymerase chain reaction (PCR), to identify the genetic factors contributing to antibiotic resistance in A. baumannii strains present in the local healthcare setting.” Accordingly, the current study was created to determine the prevalence of A. baumannii, evaluating its resistance profiles, and identifying resistance genes to guide antibiotic therapy using the Vitek 2 Compact system, enhance infection control measures, and improve patient outcomes in resource-limited healthcare settings.
Materials and Methods
Samples Collection and Ethical Consideration
One Hundred isolates were collected in a period extended from July to November 2024 from Irbid Islamic Hospital from different hospital departments including emergency, ICU, kidney dialysis units, surgery unit, and environmental samples. Official permission was obtained from the hospital to collect isolates and data. The data of each isolate include; nationality, age, gender, and source of the sample. This study was approved by the research ethical committee at Zarqa University and the Ministry of Health; ethical approval number; (MOH/REC/2024/382) before collecting samples.
The isolates were sub-cultured on MacConkey agar plates (Mast Group, UK), the plates were incubated at 35°C ± 2°C; under ambient air; for 20-24 hours overnight. A single un-colored colony from each isolate was chosen for purification. The pure culture of each isolate was preserved in 20% glycerol (Cryobank, Mast Group, UK) and frozen at -80°C until used for further investigation.
Identification of A. baumannii
According to the general characteristics of A. baumannii, an oxidase test was performed to the pure culture growth of isolates. The isolates that showed negative oxidase results were confirmed using automated instrument Vitek 2 Compact (BioMérieux, France) with GN ID Cards (BioMérieux, France) according to the WHO recommendation of bacterial phenotypic detection and identification.
Antimicrobial Susceptibility Test
Susceptibility testing of A. baumannii isolates to different antibiotics was determined using the Vitek 2 Compact instrument (BioMérieux, France), with cards AST-GN222 and AST-XN05 (BioMérieux, France). These cards are used for A. baumannii by following the recommendation of Clinical Laboratory Standards Institute (CLSI 2019) guideline. The isolates that showed resistance to carbapenems (Imipenem and Meropenem) will be confirmed using disk diffusion (Mast Group, UK), and E. test (BioMérieux, France).
The antibiotics with the breakpoints used for A. baumannii isolates mentioned in the guideline of CLSI 2019 are Penicillins (Piperacillin 16-128 μg/mL), and β-Lactam. combination agents (Ampicillin-sulbactam 8/4-32/16 μg/mL), (Piperacillin-tazobactam 16/4-128/4 μg/mL), (Ticarcillin-clavulanate 16/2-128/2 μg/mL), Cephalosporins I, II, III, and IV (Ceftazidime 8-32 μg/mL, Cefepime 8-32 μg/mL, Cefotaxime 8-64 μg/mL, Ceftriaxone 8-64 μg/mL), Carbapenems (Doripenem 2-8 μg/mL, Imipenem 2-8 μg/mL, Meropenem 2-8 μg/mL), Lipopeptides (Colistin 2-4 μg/mL, Polymyxin-b 2-4 μg/mL), Aminoglycosides (Gentamicin 4-16 μg/mL, Tobramycin 4-16 μg/mL, Amikacin 16-64 μg/mL), Tetracycline (4-16 μg/Ml), Fluoroquinolones (Ciprofloxacin 1-4 μg/mL, Levofloxacin 2-8 μg/mL, Ofloxacin 2-8 μg/mL), Folate pathway antagonists (Trimethoprim-sulfamethoxazole 2/38-4/76 μg/mL).
DNA Extraction
Genomic DNA was extracted from A. baumannii isolates using Quick–DNA miniprep plus kit (ZymoO Research, USA) according to manufacturer’s instructions quick protocol.
Detection of MDR Genes
Conventional PCR was performed using a programmable thermocycler (S1000 thermal cycler BIO-RAD, USA) for the detection of OXA genes genes encoding bla OXA-23, bla OXA- 24, and bla OXA-51, and for Efflux genes encoding for AdeA, AdeB, AdeC, and AdeS. PCR was carried out in 25 µl reaction volumes with 10µl of master mix (GoTaq Green Master Mix Promega, USA), 2 µl of diluted primers (Genewiz, USA), and 2 µl of extracted Genomic DNA of A. baumannii isolates and then nuclease-free water was added to make up the final volume. The annealing temperatures for each primer pair and amplicon size are included in Table 1.
The amplification condition of polymerase chain reaction was as follow: Pre-denaturation temperature 95°C for 5 min, 30 cycles at 95°C for 30 sec, followed by annealing at 53°C for 35 sec and extension at 72°C for 5 min. Negative control tubes containing master mix without template DNA were included in each run. PCR products were separated on 1% Agarose gel. The eluted DNA was stored at -20°C [9].
A. baumannii NCTC 13301 was used as a positive control for OXA carbapenemases genes and Klebsiella pneumonia NCTC 13443 was used as a positive control for Metallo- β-lactamase (NDM-1), the cultures were obtained from The National Collection of Type Cultures (NCTC) [10].
Agarose Gel Electrophoresis
By using 1% agarose gels electrophoresis containing 15% Red safe stain, the amplified products and the PCR DNA marker were separated for 40-50 minutes at 120 volts and then visualized using a gel documentation system including UV camera, screen, and printer (Alpha Innotech, USA).
Statistical Analysis
Statistical analysis was performed using Statistical Package for Social Sciences (SPSS) software, version 21, and P value less than 0.05 was considered statistically significant for the analysis of variance (ANOVA).
Results
Demographic Data Results
Sex and Age
Figure 1 shows the distribution of A. baumannii samples according to sex. Males were the predominant group, accounting for 60 (60%), while females were 40 (40%).
The participants' ages ranged from 7 to 95, with an average age of about 39.7. The median age is 44, and the most common (mode) age is 45 as illustrated in Figure 2. This wide age range can help analyze how different age groups respond to treatments or conditions.
Samples Characteristics
Sample Type
Figure 2 demonstrate, the most frequent A. baumannii samples are from urine (43%) and skin (24%), followed by pus (12%) and ulcers (5%) and nasal (4%). Blood, sputum and wound only one sample each.
Prevalence of A. baumannii Among the Hospital Departments
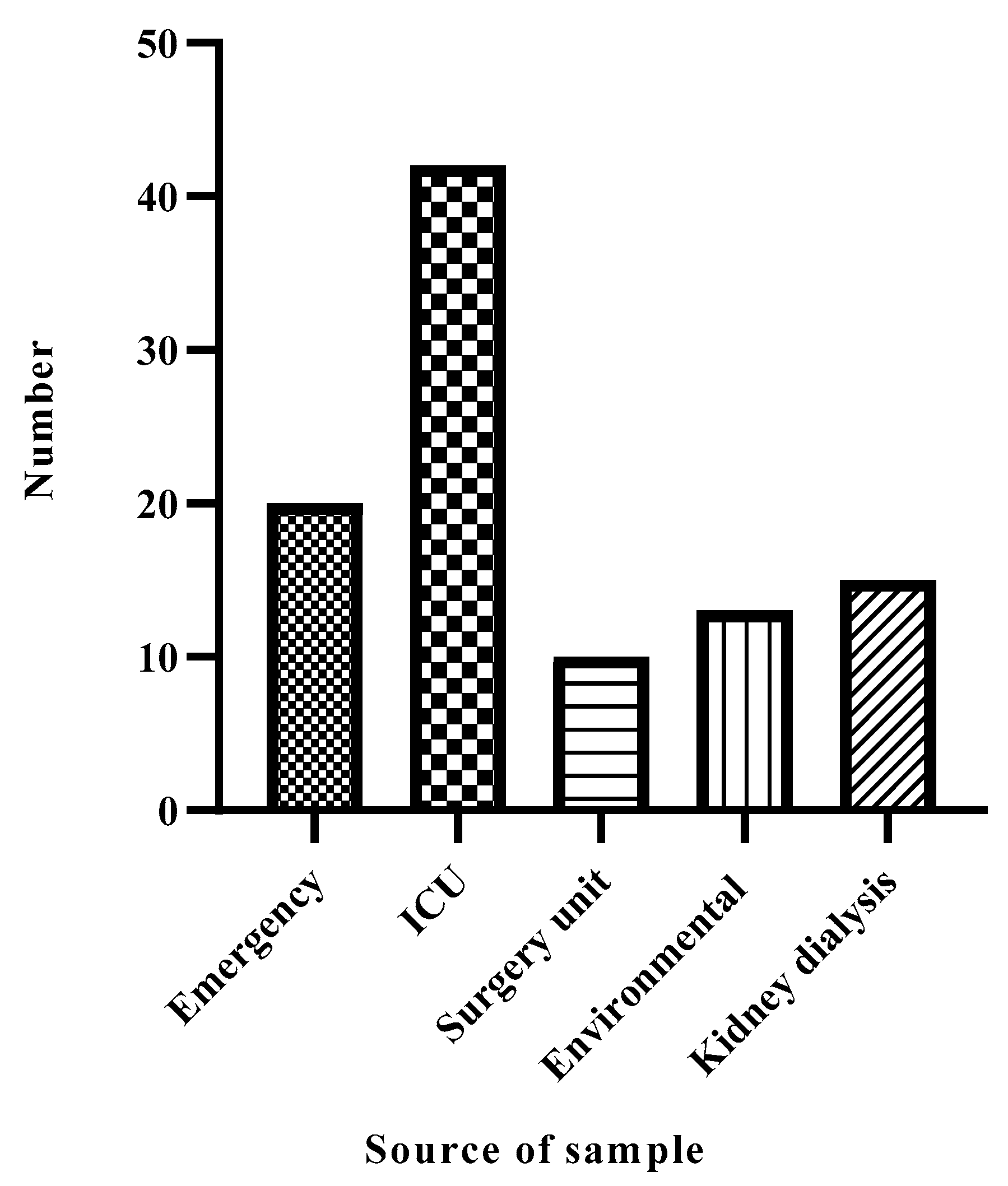
Figure 5 show, most of the collected samples are from the ICU (42%) and emergency departments (20%). A notable number are also from kidney dialysis units (15%) and environmental sources (13%).
Figure 3.
Distribution of A. baumannii according to source of sample.
Patients Diagnosis
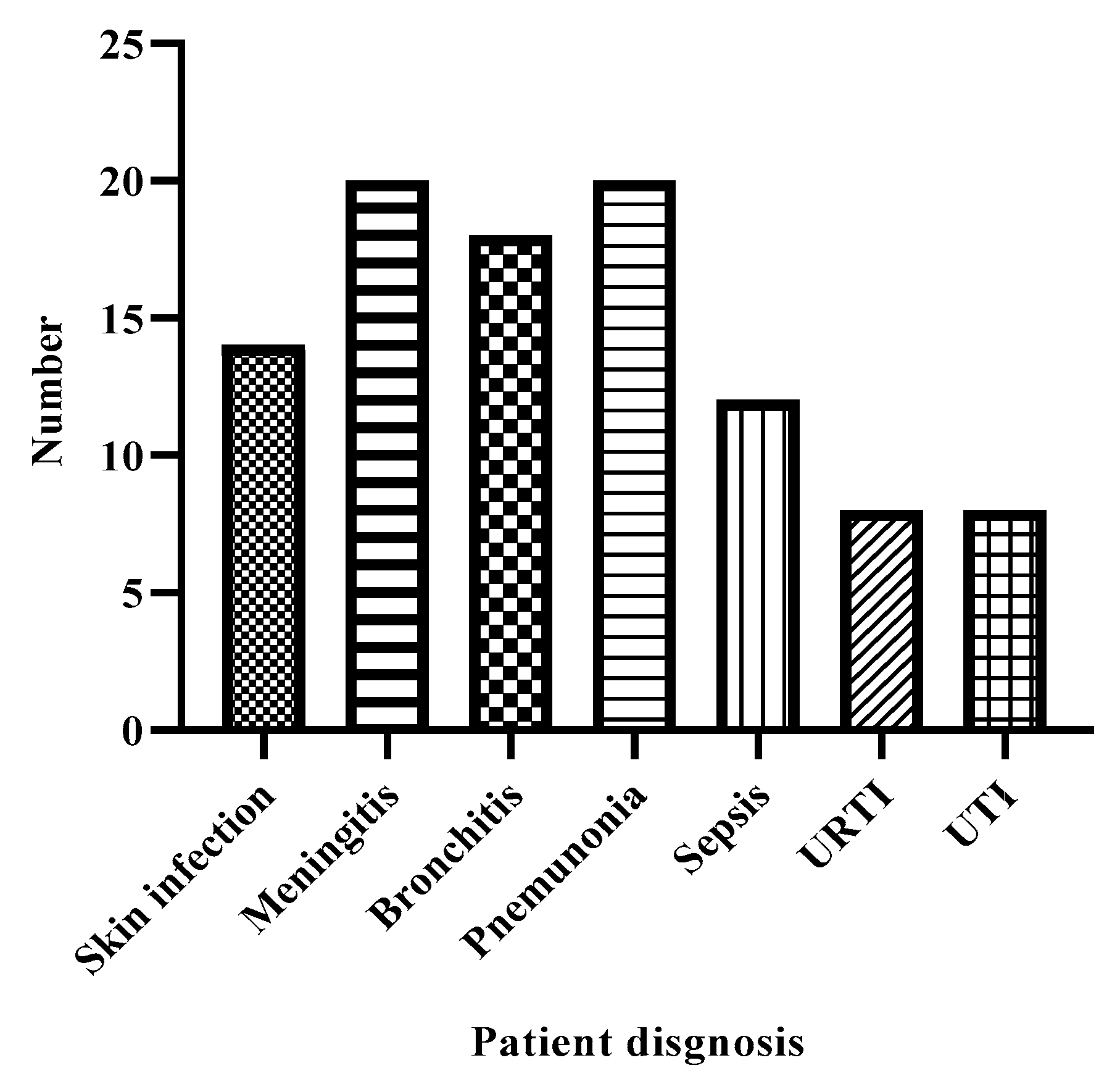
The most common diagnoses associated with A. baumannii among participants were meningitis (20%), pneumonia (20%), and bronchitis (18%), emphasizing the prevalence of respiratory and infectious diseases. Sepsis was also notable, accounting for 12% of cases, reflecting its clinical importance.
Figure 4.
Distribution of A. baumannii according to patient diagnosis.
Correlations Coefficient Analysis
The correlations between variables in this study were examined using Pearson’s correlation coefficient to assess the strength and direction of the linear relationships. A significance level p-value≤0.05 was was considered statistically significant. The Pearson correlation coefficient (r) values range from -1 to +1, with values closer to +1 or -1 indicating stronger relationships.
Gender and Sample Type
A Pearson correlation coefficient of 0.206 was identified between gender and sample type, which is statistically significant at the 0.05 level (p = 0.04). Although the correlation is weak, it indicates a slight variation in sample type based on gender.

Table 2.
Correlation between gender and Sample Type.
| Gender | Sample Type | ||
| Gender | Pearson Correlation | 1 | .206* |
| Sig. (2-tailed) | .040 | ||
| N | 100 | 100 | |
| Sample Type | Pearson Correlation | .206* | 1 |
| Sig. (2-tailed) | .040 | ||
| N | 100 | 100 | |
*Correlation is significant at the 0.05 level (2-tailed).
Age and Diagnosis
The Pearson correlation between age and diagnosis is not statistically significant (r = 0.150, p = 0.136), indicating no strong relationship between the participant's age and the diagnosis they received. This suggests that the diagnosis might be relatively independent of age in this dataset.
Table 3.
Correlations between age and diagnosis.
| Age | Diagnosis | ||
| Age | Pearson Correlation | 1 | .150 |
| Sig. (2-tailed) | .136 | ||
| N | 100 | 100 | |
| Diagnosis | Pearson Correlation | .150 | 1 |
| Sig. (2-tailed) | .136 | ||
| N | 100 | 100 | |
Antimicrobial Susceptibility Testing for A. baumannii
Ten antibiotics were tested against A. baumannii, including Vancomycin, Oxacillin, Tigecycline, Teicoplanin, Erythromycin, Amikacin, Linezolid, Gentamycin, Rifampin, and Levofloxacin. These antibiotics were tested for resistance (R), sensitivity (S), and intermediate resistance (I) against each isolate. Vancomycin showed the highest rate of resistance (71%), while the highest sensitivity rate was for Erythromycin (52%).
Table 4.
Antimicrobial susceptibility testing for A. baumannii.
| Antibiotic | Sensitivity | Frequency | Percent | Valid Percent | Cumulative Percent |
| Vancomycin | R | 71 | 71.0 | 71.0 | 71.0 |
| S | 27 | 27.0 | 27.0 | 98.0 | |
| I | 2 | 2.0 | 2.0 | 100.0 | |
| Oxacillin | R | 66 | 66.0 | 66.0 | 66.0 |
| S | 34 | 34.0 | 34.0 | 100.0 | |
| I | 0 | 0.0 | 0.0 | ||
| Tigecycline | R | 52 | 52.0 | 52.0 | 52.0 |
| S | 39 | 39.0 | 39.0 | 91.0 | |
| I | 9 | 9.0 | 9.0 | 100.0 | |
| Teicoplanin | R | 49 | 49.0 | 49.0 | 49.0 |
| S | 49 | 49.0 | 49.0 | 98.0 | |
| I | 2 | 2.0 | 2.0 | 100.0 | |
| Erythromycin | R | 48 | 48.0 | 48.0 | 48.0 |
| S | 52 | 52.0 | 52.0 | 100.0 | |
| I | 0 | 0.0 | 0.0 | ||
| Amikacin | R | 47 | 47.0 | 47.0 | 47.0 |
| S | 49 | 49.0 | 49.0 | 96.0 | |
| I | 4 | 4.0 | 4.0 | 100.0 | |
| Linezolid | R | 45 | 45.0 | 45.0 | 45.0 |
| S | 49 | 49.0 | 49.0 | 94.0 | |
| I | 6 | 6.0 | 6.0 | 100.0 | |
| Gentamycin | R | 50 | 50.0 | 50.0 | 50.0 |
| S | 47 | 47.0 | 47.0 | 97.0 | |
| I | 3 | 3.0 | 3.0 | 100.0 | |
| Rifampin | R | 53 | 53.0 | 53.0 | 53.0 |
| S | 47 | 47.0 | 47.0 | 100.0 | |
| I | 0 | 0.0 | 0.0 | ||
| Levofloxacin | R | 67 | 67.0 | 67.0 | 67.0 |
| S | 33 | 33.0 | 33.0 | 100.0 | |
| I | 0 | 0.0 | 0.0 |
Detection of Oxa and Efflux Genes Among the Isolates
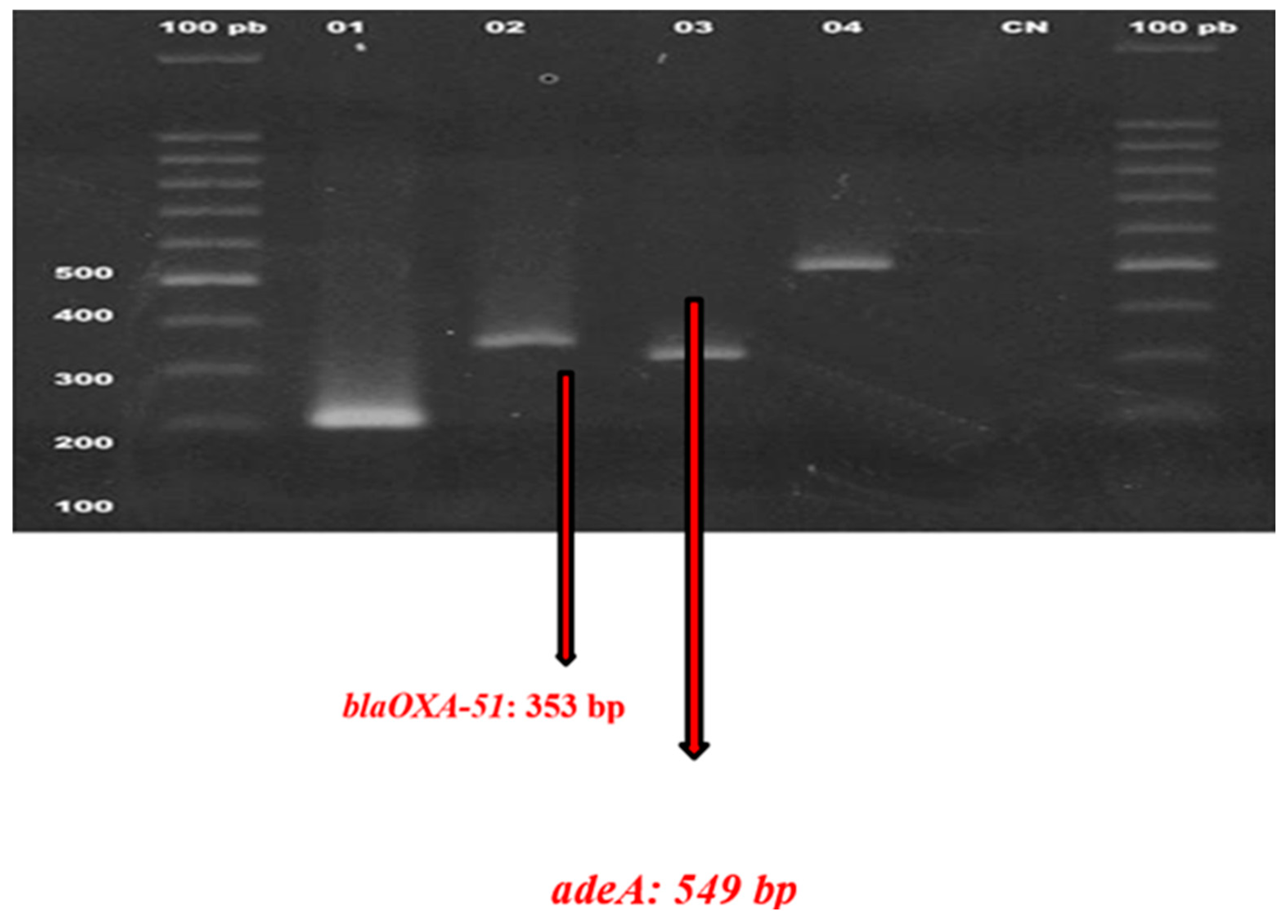
The polymerase chain reaction (PCR) was used to amplify and identify particular antibiotic resistance genes in the A. baumannii isolates. Conventional PCR was used to target genes including blaOXA-23, blaOXA-24, and blaOXA-51 to detect carbapenem resistance, a vital component of multidrug-resistant (MDR) A. baumannii. The PCR amplification adhered to a standardized technique, with meticulously regulated conditions, including particular annealing temperatures for each primer pair, facilitating precise amplification of the targeted resistance genes. The following examination of PCR results by agarose gel electrophoresis validated the existence of these genes, indicating a significant incidence of carbapenemase-producing isolates. This molecular characterisation offered significant insights into the genetic foundation of resistance, underscoring the essential need for molecular monitoring in addressing multidrug-resistant diseases in healthcare environments
| Target genes | PrevalenceRate% | P-value |
| OXA genes | ||
| blaOXA-51 | 15% | 0.06 |
| blaOXA-23 | 80% | 0.005 |
| blaOXA-24 | 77% | 0.02 |
| Efflux genes | ||
| AdeA | 5% | 0.07 |
| AdeB | 8% | 0.75 |
| AdeC | 14% | 0.15 |
| AdeS | 7% | 0.75 |
Figure 5.
Detection of blaOXA-51 and adeA using gel electrophoresis.
Discussion
This study aims to investigate the prevalence and molecular characteristics of A. baumannii isolates in hospitalized patients, focusing on those with multidrug resistance (MDR) in a governmental hospital in Irbid, Jordan. The findings indicated a high prevalence of MDR A. baumannii infections, particularly in ICU patients. A majority of the isolates showed resistance to multiple antibiotics, with the highest resistance rates observed for vancomycin (71%) and oxacillin (66%).
In 2018, the World Health Organization (WHO) classified carbapenem-resistant Acinetobacter baumannii (CRAB) as the top priority for antibiotic research and development. This classification highlights the critical need for new therapeutic options. Carbapenem resistance serves as a key indicator due to its strong correlation with extensive co-resistance to multiple other antibiotic classes, making CRAB a significant challenge in clinical settings [11].
The findings highlight that A. baumannii has emerged as a critical nosocomial pathogen, especially in ICUs. This is largely attributed to immunocompromised state of patients and their frequent exposure to invasive procedures, including mechanical ventilation and catheterization [12]. This aligns with previous studies indicating the heightened risk of A. baumannii infections in critically ill patients [13].
Numerous studies align with the findings of this research. For example, a study conducted in Greek hospitals reported a high incidence of A. baumannii infections among ICU patients, demonstrating substantial resistance to multiple antibiotic classes, including carbapenems [14]. The study revealed that 85% of isolates exhibited resistance to imipenem and meropenem, aligning with the findings of this research, which also demonstrated a high prevalence of carbapenem resistance among the tested isolates. Furthermore, a study conducted in Vietnam revealed that 91% of A. baumannii isolates were resistant to carbapenems, 92% were multidrug-resistant, and 6% showed resistance to colistin. The dominant genotypes among carbapenem-resistant A. baumannii (CRAB) were ST2, ST571, and ST16, each associated with unique antimicrobial resistance (AMR) gene profiles.
Additionally, a study by Al-Tamimi et al. (2022) [15] investigating isolates from various Jordanian hospitals reported that the blaOXA-51 gene was detected in all A. baumannii samples, highlighting the extensive distribution of this gene within Jordanian healthcare settings [15]. These findings are consistent with the current study, which also identified blaOXA-51 in isolates, suggesting that this gene is a prevalent molecular marker in the region.
blaOXA genes, such as blaOXA-51, blaOXA-23, and blaOXA-24, play a pivotal role in the resistance mechanisms of A. baumannii. These genes encode carbapenemase enzymes and are located on both chromosomal DNA and plasmids, facilitating their widespread dissemination [16]. Research by Wong et al. has revealed that carbapenem resistance in clinical isolates of A. baumannii is predominantly driven by the overexpression of OXA-23 or OXA-51. This increased expression is linked to the insertion of the ISAba1 element into the promoter regions of these genes, which enhances their transcriptional activity and contributes to resistance [17].
Also, the enhanced activity of efflux pumps plays a synergistic role alongside beta-lactamases in driving antibiotic resistance [18]. The overexpression of the AdeABC efflux pump in A. baumannii is strongly linked to resistance against carbapenems and cephalosporins [19]. This pump is a member of the resistance-nodulation-division (RND) family and operates as a three-component system. The AdeB component functions as the primary transporter, actively expelling antibiotics from the bacterial cell. AdeA acts as a membrane fusion protein, while AdeC serves as an outer membrane protein [20]. Notably, the AdeB component has broad substrate specificity, capable of transporting a wide range of molecules, including hydrophilic and hydrophobic compounds, as well as positively charged or neutral antibiotics [21].
Contrarily, a study conducted by Nguyen and Joshi (2021) [22] in Vietnam demonstrated that a smaller proportion of A. baumannii isolates (55%) exhibited resistance to vancomycin, compared to 71% in the present study [21,22]. The lower resistance rates in that study may be attributed to differences in antibiotic prescription practices and infection control measures in Vietnam compared to Jordan.
A study by Harding et al. (2018) [23] conducted in the United States highlighted that efflux pumps were the predominant mechanism driving resistance in A. baumannii, with less emphasis on the role of blaOXA genes. This finding contrasts with the current study, which focuses on carbapenemase-producing genes such as blaOXA-23 and blaNDM-1. The variation suggests potential geographic differences in the primary resistance mechanisms of A. baumannii, reflecting the influence of local selective pressures and antimicrobial usage patterns [23].
The high prevalence of MDR A. baumannii in Jordanian hospitals, particularly in the ICU, highlights the urgent need for stringent infection control measures. The findings support the implementation of comprehensive antimicrobial stewardship programs that focus on optimizing antibiotic use to curb the spread of resistant strains [24]. Additionally, the identification of specific resistance genes such as blaOXA-23 provides valuable information for the development of targeted molecular diagnostics, which can improve the timely identification of MDR infections and guide appropriate treatment choices [4].
Limitations and Future Research
Despite the comprehensive nature of the study, there are several limitations. First, the study was conducted in a single governmental hospital, which may limit the generalizability of the findings to other healthcare settings in Jordan. Future research should expand the study to include multiple hospitals across different regions. Furthermore, while PCR analysis provided insights into the molecular mechanisms of resistance, whole-genome sequencing could offer a more detailed understanding of the genetic diversity and transmission patterns of A. baumannii in hospital environments.
The findings of this study align with research from various geographic regions, demonstrating that A. baumannii continues to pose a significant challenge in hospital environments globally. A similar study by Al-Sheboul et al. (2022) [25] in Jordan noted an alarming rise in the prevalence of A. baumannii in ICUs, where 90% of the isolates were multidrug-resistant. This is comparable to the high resistance rates observed in the present study. Both studies emphasize the role of ICU settings as high-risk environments due to the frequent use of invasive devices and the high patient turnover. The presence of carbapenemase genes such as blaOXA-23 and blaOXA-24 in both studies underscores the prevalence of these genes in Jordanian hospitals, likely contributing to the spread of carbapenem-resistant A. baumannii [4].
Internationally, studies conducted in European and Asian countries reflect similar resistance patterns. For instance, a study by Dijkshoorn, Nemec, and Seifert (2007) [26] in Europe found that A. baumannii isolates exhibited widespread resistance to aminoglycosides, fluoroquinolones, and carbapenems—comparable to the resistance patterns observed in the current study. The widespread dissemination of carbapenem-resistant A. baumannii in Europe and Jordan could suggest a potential link between international healthcare networks and the global spread of resistant strains through travel or medical tourism [27].
However, a notable difference in antibiotic resistance patterns can be observed in studies from lower-middle-income countries (LMICs) compared to high-income countries. For example, a study conducted in India by Rajan et al. (2023) [28] revealed a lower prevalence of blaOXA-23 (45%) compared to the nearly ubiquitous presence of this gene in the Jordanian isolates [15]. This disparity may be due to differences in antibiotic usage practices, infection control measures, and healthcare infrastructure between LMICs and more resource-constrained settings.
This study contributes to the expanding body of evidence underscoring the significant threat posed by multidrug-resistant (MDR) A. baumannii in healthcare environments. To effectively address and mitigate the spread of this pathogen, ongoing surveillance efforts and the implementation of advanced molecular diagnostic technologies are crucial.
The current study provides valuable insights into the molecular epidemiology of A. baumannii in a governmental hospital in Jordan. However, future research should expand the scope to include multiple healthcare facilities across different regions. This would provide a more comprehensive understanding of the epidemiological trends and resistance mechanisms of A. baumannii in Jordan. Additionally, future studies should incorporate the whole-genome sequencing (WGS) to provide more detailed insights into the clonal relationships and transmission dynamics of A. baumannii within hospital environments [27].
One of the most important findings of this study is the prevalence of carbapenemase-producing A. baumannii strains, particularly those harboring blaOXA-23, and blaOXA-24 genes. These resistance mechanisms are concerning as they limit the efficacy of carbapenem antibiotics, which are often used as a last resort for treating severe infections. Molecular surveillance programs that regularly monitor the presence of these resistance genes are essential for containing the spread of MDR strains.
In conclusion, A. baumannii continues to be a formidable nosocomial pathogen, posing significant challenges to healthcare systems worldwide. Through enhanced molecular surveillance, judicious use of antibiotics and improved infection control practices [29], healthcare providers can mitigate the impact of MDR A. baumannii infections and improve the prognosis for affected patients in Jordan and beyond.
Acknowledgements
The authors would like to thank the staff members of the Faculty of Allied Medical Sciences at Zarqa University.
Conflicts of Interest
none
References
- Peleg AY, Seifert H and Paterson DL. Acinetobacter baumannii: emergence of a successful pathogen. Clinical microbiology reviews 2008, 21, 538–582. [Google Scholar] [CrossRef] [PubMed]
- Antunes LC, Visca P and Towner KJ. Acinetobacter baumannii: evolution of a global pathogen. Pathogens and disease 2014, 71, 292–301. [Google Scholar] [CrossRef] [PubMed]
- AlFaris EaM, Al-Karablieh N, Odat NA, et al. Carbapenem-resistant Acinetobacter baumannii from Jordan: Complicated Carbapenemase Combinations. Jordan Journal of Biological Sciences 2024; 17.
- Perez F, Hujer AM, Hujer KM, et al. Global challenge of multidrug-resistant Acinetobacter baumannii. Antimicrobial agents and chemotherapy 2007, 51, 3471–3484. [Google Scholar] [CrossRef] [PubMed]
- Duan Z, Li X, Li S, et al. Nosocomial surveillance of multidrug-resistant Acinetobacter baumannii: a genomic epidemiological study. Microbiology Spectrum 2024, 12, e02207–02223. [Google Scholar]
- Jiang Y, Ding Y, Wei Y, et al. Carbapenem-resistant Acinetobacter baumannii: A challenge in the intensive care unit. Frontiers in microbiology 2022, 13, 1045206. [Google Scholar]
- Torres HA, Vázquez EG, Yagüe G, et al. [Multidrug resistant Acinetobacter baumanii:clinical update and new highlights]. Rev Esp Quimioter 2010, 23, 12–19. [Google Scholar]
- Gedefie A, Demsis W, Ashagrie M, et al. Acinetobacter baumannii Biofilm Formation and Its Role in Disease Pathogenesis: A Review. Infect Drug Resist, 2021. [CrossRef]
- Jia W, Li C, Zhang H, et al. Prevalence of genes of OXA-23 carbapenemase and AdeABC efflux pump associated with multidrug resistance of Acinetobacter baumannii isolates in the ICU of a comprehensive hospital of Northwestern China. International journal of environmental research and public health 2015, 12, 10079–10092. [Google Scholar] [CrossRef]
- Hou C and Yang F. Drug-resistant gene of blaOXA-23, blaOXA-24, blaOXA-51 and blaOXA-58 in Acinetobacter baumannii. International journal of clinical and experimental medicine 2015; 8: 13859.
- Tacconelli E, Carrara E, Savoldi A, et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. The Lancet infectious diseases 2018; 18: 318-327.
- Ayoub Moubareck C and Hammoudi Halat, D. Insights into Acinetobacter baumannii: A Review of Microbiological, Virulence, and Resistance Traits in a Threatening Nosocomial Pathogen. Antibiotics (Basel), 2020. [Google Scholar] [CrossRef]
- Agyepong N, Fordjour F and Owusu-Ofori A. Multidrug-resistant Acinetobacter baumannii in healthcare settings in Africa. Frontiers in Tropical Diseases 2023; 4: 1110125.
- Karampatakis T, Antachopoulos C, Tsakris A, et al. Molecular epidemiology of carbapenem-resistant Acinetobacter baumannii in Greece: an extended review (2000–2015). Future Microbiology 2017; 12: 801-815.
- Al-Tamimi M, Albalawi H, Alkhawaldeh M, et al. Multidrug-resistant Acinetobacter baumannii in Jordan. Microorganisms 2022; 10: 849.
- Kyriakidis I, Vasileiou E, Pana ZD, et al. Acinetobacter baumannii antibiotic resistance mechanisms. Pathogens 2021; 10: 373.
- Wong MH-y, Chan BK-w, Chan EW-c, et al. Over-expression of IS Aba1-Linked intrinsic and exogenously acquired OXA type carbapenem-hydrolyzing-class D-ß-Lactamase-encoding genes is key mechanism underlying Carbapenem Resistance in Acinetobacter baumannii. Frontiers in microbiology 2019; 10: 2809.
- Cecchini T, Yoon E-J, Charretier Y, et al. Deciphering multifactorial resistance phenotypes in Acinetobacter baumannii by genomics and targeted label-free proteomics. Molecular & Cellular Proteomics 2018; 17: 442-456.
- Huang L, Sun L, Xu G, et al. Differential susceptibility to carbapenems due to the AdeABC efflux pump among nosocomial outbreak isolates of Acinetobacter baumannii in a Chinese hospital. Diagnostic microbiology and infectious disease 2008; 62: 326-332.
- Magnet S, Courvalin P and Lambert T. Resistance-nodulation-cell division-type efflux pump involved in aminoglycoside resistance in Acinetobacter baumannii strain BM4454. Antimicrobial agents and chemotherapy 2001; 45: 3375-3380.
- Diep DTH, Tuan HM, Ngoc KM, et al. The clinical features and genomic epidemiology of carbapenem-resistant Acinetobacter baumannii infections at a tertiary hospital in Vietnam. Journal of Global Antimicrobial Resistance. [CrossRef]
- Nguyen M and Joshi S. Carbapenem resistance in Acinetobacter baumannii, and their importance in hospital-acquired infections: a scientific review. Journal of applied microbiology 2021; 131: 2715-2738.
- Harding CM, Hennon SW and Feldman MF. Uncovering the mechanisms of Acinetobacter baumannii virulence. Nature Reviews Microbiology 2018; 16: 91-102.
- Capuozzo, M.; Zovi, A.; Langella, R.; Ottaiano, A.; Cascella, M.; Scognamiglio, M.; Ferrara, F. Optimizing Antibiotic Use: Addressing Resistance Through Effective Strategies and Health Policies. Antibiotics 2024, 13, 1112. [Google Scholar] [CrossRef] [PubMed]
- Al-Sheboul, S.A.; Al-Moghrabi, S.Z.; Shboul, Y.; Atawneh, F.; Sharie, A.H.; Nimri, L.F. Molecular Characterization of Carbapenem-Resistant Acinetobacter baumannii Isolated from Intensive Care Unit Patients in Jordanian Hospitals. Antibiotics 2022, 11, 835. [Google Scholar] [CrossRef] [PubMed]
- Dijkshoorn, L. , Nemec, A. & Seifert, H. An increasing threat in hospitals: multidrug-resistant Acinetobacter baumannii. Nat Rev Microbiol. [CrossRef]
- Rodríguez-Baño J, Gutiérrez-Gutiérrez B, Machuca I, Pascual A. Treatment of Infections Caused by Extended-Spectrum-Beta-Lactamase-, AmpC-, and Carbapenemase-Producing Enterobacteriaceae. Clin Microbiol Rev. 2018 Feb 14;31(2):e00079-17. [CrossRef] [PubMed]
- Rajan V, Vijayan A, Puthiyottu Methal A, Lancy J, Sivaraman GK (2023) Genotyping of Acinetobacter baumannii isolates from a tertiary care hospital in Cochin, South India. Access Microbiol 5(000662):v4. [CrossRef]
- Owais D, Al-Groom RM, AlRamadneh TN, Alsawalha L, Khan MSA, Yousef OH, Burjaq SZ. Antibiotic susceptibility and biofilm forming ability of Staphylococcus aureus isolated from Jordanian patients with diabetic foot ulcer. Iran J Microbiol. 2024 Aug;16(4):450-458. [CrossRef] [PubMed]
Figure 1.
Distribution of A. baumannii according to sex.
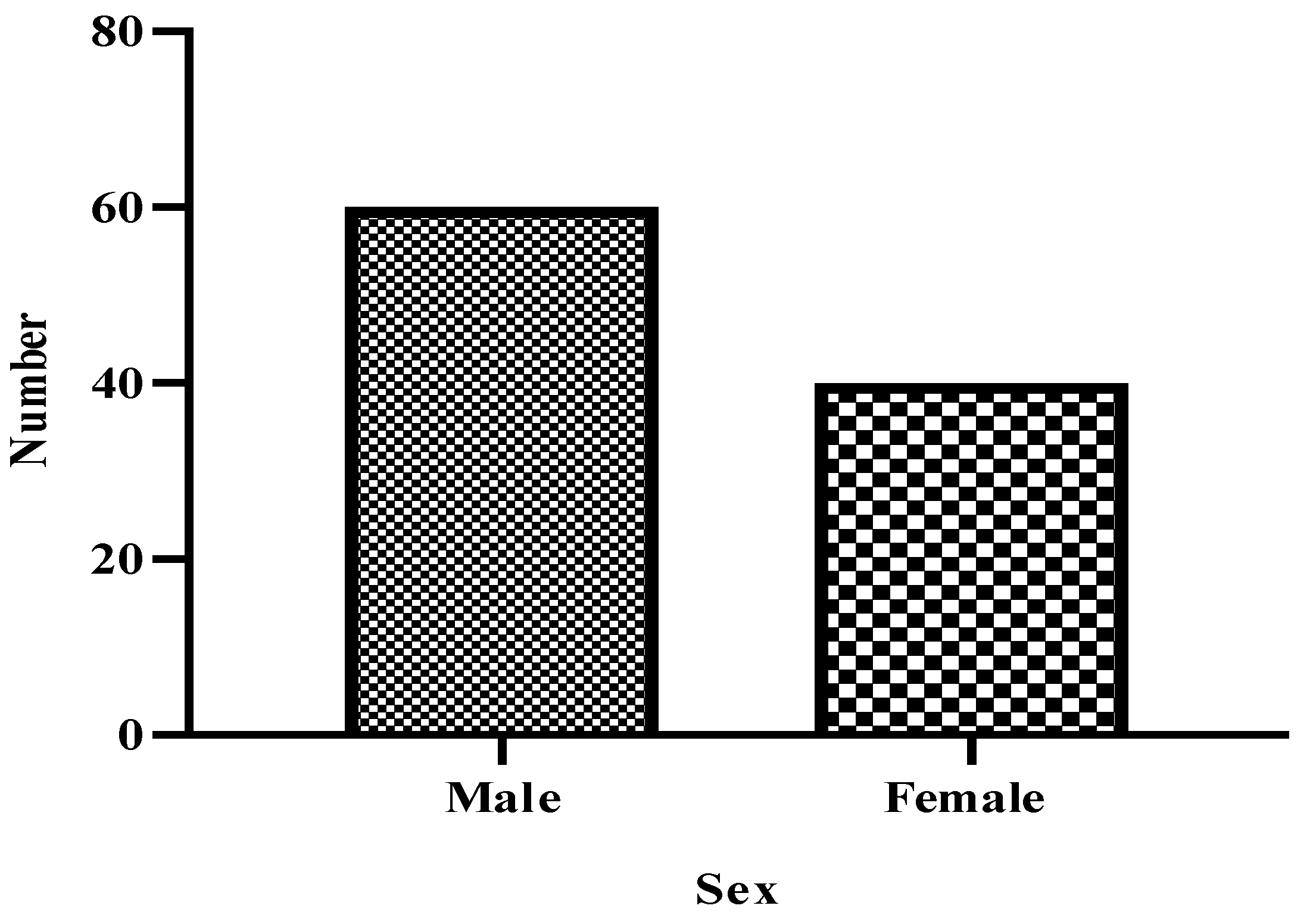
Figure 2.
Distribution of A. baumannii according to type of sample.
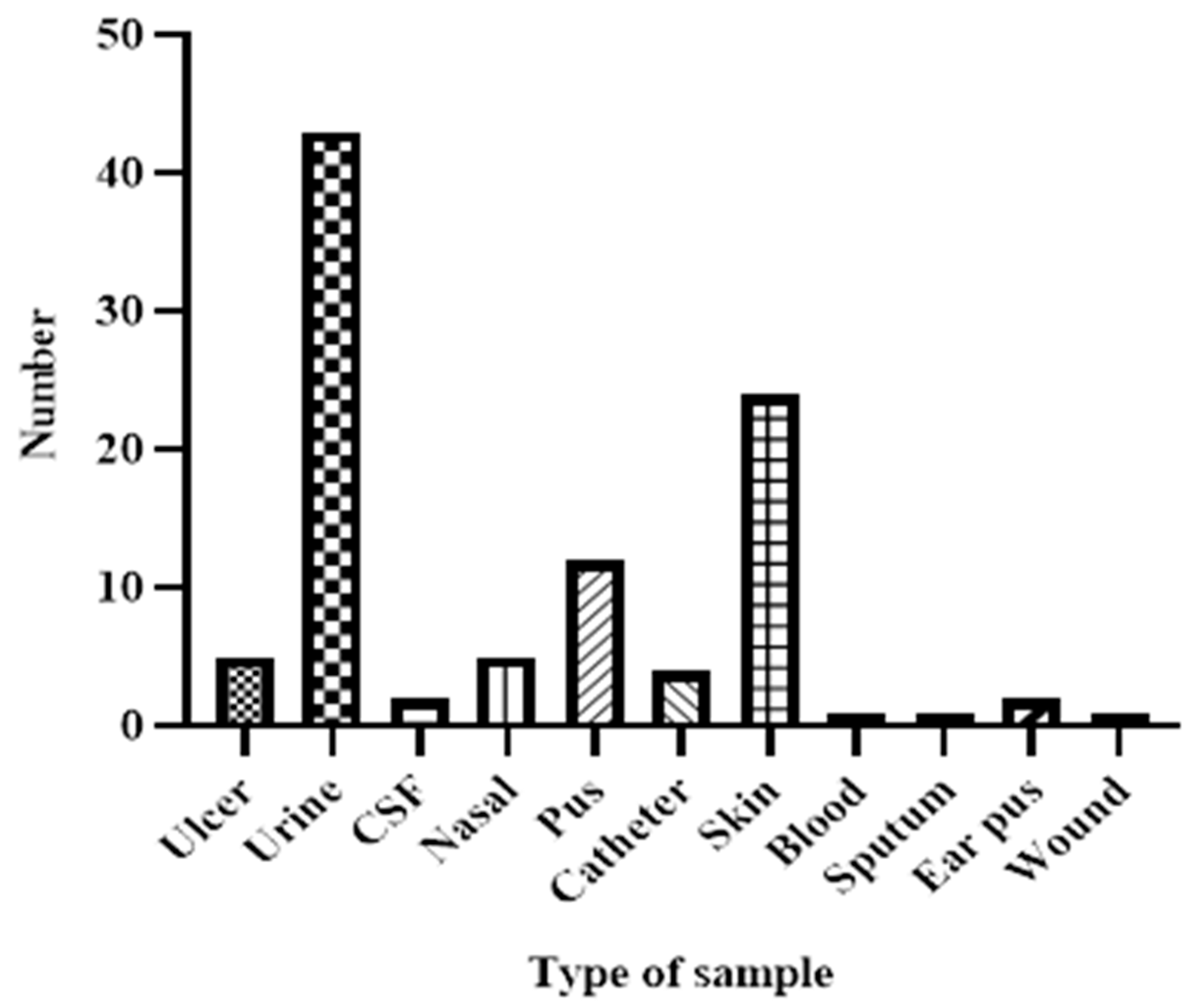
Table 1.
Primers used with their respective annealing temperatures.
| Genes | Primers sequences |
Amplicon size |
References |
| blaOXA-51 |
F:TAATGCTTTGATCGGCCTTG R: TGGATTGCACTTCATCTTGG |
760 | [3,10] |
| blaOXA-23 |
F: GATCGGATTGGAGAACCAGA R: ATTTCTGACCGCATTTCCAT |
774 | [3,10] |
| blaOXA-24 |
F: TTCCCCTAACATGAATTTGT R: GTACTAATCAAAGTTGTGAA |
828 | [3,10] |
| AdeA |
F: GGCGTATTGGGCAATCTTTTGT R: GTCACCGACTTTCAAGCCTTTG |
1157 | [3,9] |
| AdeB |
F: TGGCGGAATGAAGTATGT R: GCAGTGCGGCAGGTTAG |
1323 | [3,9] |
| AdeC |
F: GACAATCGTATCTCGTGGACTC R: AGCAATTTTCTGGTCAGTTTCC |
1331 | [3,9] |
| AdeS |
F:GTGGACGTTAGGTCAAGTTCTG R:TGTTATCTTTTGCGGCTGT ATT |
949 | [3,9] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



