Submitted:
15 January 2025
Posted:
16 January 2025
You are already at the latest version
Abstract
Recently, Generalized Anxiety Disorder (GAD) has become a more prevalent mental health issue across the population. It is on the rise globally and is particularly affecting higher-income countries, such as the United States; in the United States, anxiety prevalence rose from 5.12% in 2008 to 6.68% in 2018 among adults aged 18 and older, indicating a significant upward trend. Furthermore, evidence suggests there is a significant number of people suffering from undiagnosed GAD, in addition to the diagnosed count. Most of the widely used methods like medication and professional therapy, while decently effective, can be expensive and inaccessible to many people. This literature review explores the effectiveness of mindfulness meditation, specifically Buddhist Vipassana, in managing GAD compared to conventional treatments.
Keywords:
Generalized Anxiety Disorder
; Meditation
; Mental Health
; Vipassana Meditation
; Pharmacotherapy
; Psychotherapy
; Complementary Therapy
Introduction
Background and Context
In today’s society, the rising burden of anxiety on the population cannot be ignored. From 2008 to 2018, the prevalence of anxiety disorders has risen among adult Americans, especially among young adults, with 15% of young adults reporting anxiety in 2018 [1]. The situation has only worsened after the COVID-19 pandemic, for infected patients have shown a higher anxiety rate, and the dramatic changes in daily life as well as economic uncertainty caused by the pandemic have induced further fear and anxiety [2]. As a group, anxiety disorders are the most widespread class of mental health disorders and are the sixth leading cause of disability and impairment in high and low-income countries, with the highest burden being between ages 15 through 34 [5].
One of the most prominent anxiety disorders is GAD, which has been associated with considerable role impairment (difficulty in fulfilling life responsibilities), especially in high-income countries like the U.S., underlining its significance as a public health issue [3]. Furthermore, evidence suggests many cases of GAD go undiagnosed [4], further contributing to its impact on public health by leaving individuals without necessary treatment and support. Clinically, GAD is characterized by the DSM-5 as persistent and excessive anxiety and worry about a number of domains in the person's life, present for at least 6 months [6]. Some of the symptoms of GAD include restlessness, being easily fatigued, difficulty concentrating, irritability, muscle tension, and disturbed sleep; at least three of them need to be present for at least 6 months to meet the DSM-V criteria for GAD [6]. Compared with other anxiety disorders, GAD specifically is also present all over the globe but especially impacts higher-income countries such as the United States3. In addition, the disorder affects twice as many women as men; studies suggest further risk factors include low income and widowed, separated, or divorced marital status [7]. Evidence shows a hereditary basis and genetic factors associated with GAD, as well [8]. Like other anxiety disorders, GAD has a high rate of comorbidity with other anxiety disorders and depression, but GAD has a particularly strong association with major depression5. While many anxiety disorders have an age of onset ranging from late adolescence to early adulthood, GAD has the latest age of onset, with a median age of 31 years old [5,7].
While the pathophysiology and exact mechanism through which GAD occurs and affects victims is not understood, there is still some evidence suggesting specific regions of the brain are impacted by GAD. Brain imaging studies, with the use of functional MRI (fMRI), have long suggested various abnormalities, like overactivity, in the limbic regions, such as the amygdala and insula [5]. In addition, multiple implicated neurotransmitter systems have been identified to have a role in disrupting the central nervous system. Commonly for anxiety disorder patients, the serotonergic neurotransmitter system tends to be characterized by underactivation while the noradrenergic system is characterized by overactivation [9]. These systems regulate and are regulated by other pathways and neuronal circuits in various regions of the brain, so disruptions in them provide an explanation for anxiety disorders. Another disrupted system associated with anxiety disorders is the gamma-aminobutyric acid (GABA) system, with evidence for the role of this system pointing to clinical experience with drugs called benzodiazepines [9,10].
There are two ways that GAD is typically treated today – pharmacotherapy and psychotherapy. One of the most well-established forms is pharmacotherapy. Three of the most prominent pharmacotherapy treatments for GAD are SSRIs, SNRIs, and benzodiazepines. SSRIS and SNRIS are often used as first-line treatments due to their high efficacy rates and relatively few side effects11,13. Selective serotonin reuptake inhibitors (SSRIs) are antidepressants that block the neurotransmitter serotonin from reabsorption (reuptake) into neurons. As a result, serotonin availability is increased, improving serotonin transmission between neurons [11,12,13]. Six SSRIs are widely available: citalopram, fluoxetine, fluvoxamine, paroxetine, sertraline and escitalopram [13]. Serotonin-norepinephrine reuptake inhibitors (SNRIs) are another class of antidepressants that work similarly to SSRIs but improve availability of norepinephrine in addition to serotonin [11,12,13]. Although these antidepressants work effectively and have relatively good safety profiles, it nevertheless typically takes around four weeks for the onset of anxiolytic effects, and until then, patients may experience adverse effects [12]. On the contrary, one of the main advantages of benzodiazepines, which are not antidepressants, is that they start providing anxiolytic effects almost immediately [12]. All known actions of benzodiazepines are mediated by the GABA-A receptor complex. Benzodiazepines act to increase chloride conductance of the GABA-A receptor, causing increased inhibitory neurotransmission [11,13] . However, they have their own complications, as benzodiazepine treatment may be associated with central nervous system (CNS) depression, impaired cognitive functions mainly in elderly patients, and dependency. Although 55 - 94% of anxiety patients are treated with this medication, current guidelines do not recommend it as a first-line treatment [12].
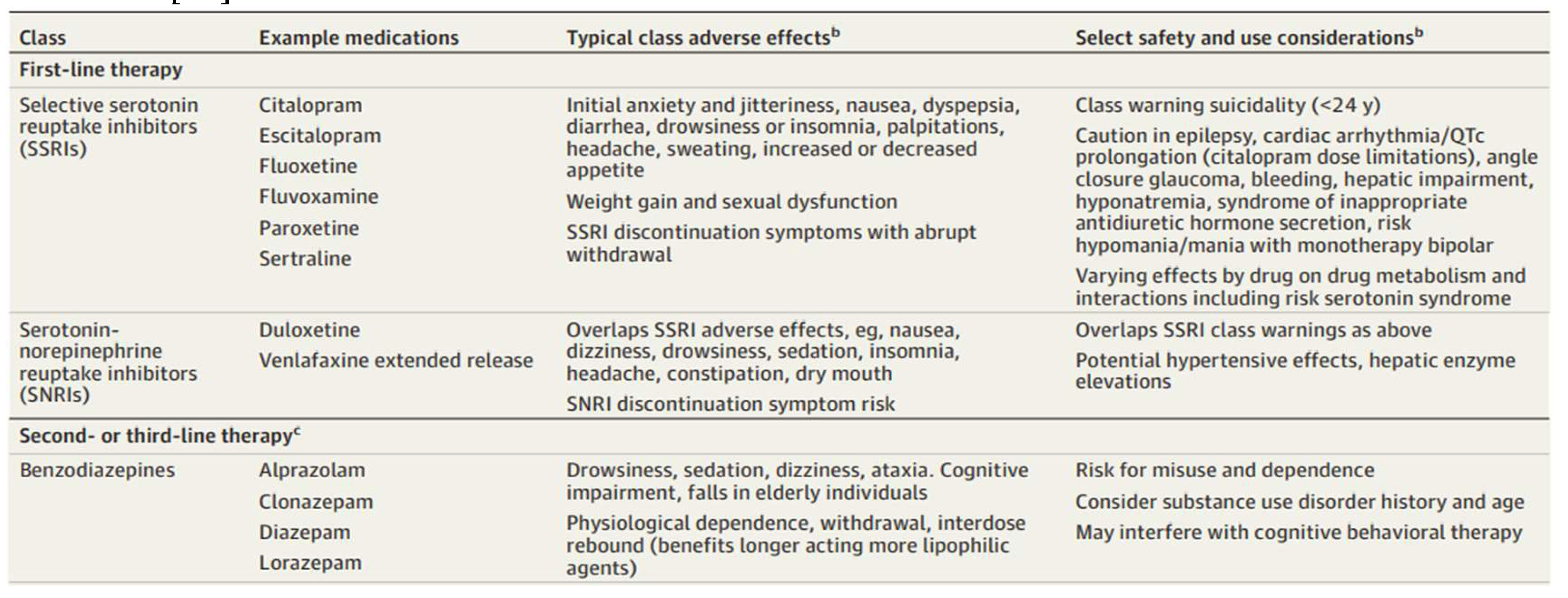
Overview of Pharmacologic Therapy for Anxiety Disorders [1]4
In terms of psychotherapies, Cognitive Behavioral Therapy (CBT) is the most prominent and empirically supported psychological treatment for youth and adult anxiety disorders. A full course of CBT typically consists of 8 to 20 weekly sessions [14]. The primary components of CBT include psychoeducation, cognitive restructuring, and exposure [14]. Psychoeducation helps patients understand their symptoms and the harmful patterns that worsen them. Cognitive restructuring involves recognizing anxiety-provoking thoughts, like catastrophizing, and learning to reframe them, personalized to the patient’s condition (e.g., fear of uncertainty in GAD) [14]. Exposure therapy encourages patients to face sensations they tend to avoid due to anxiety. Combination of CBT and medication may be beneficial for severe anxiety or for patients who don't respond to either treatment alone [14].
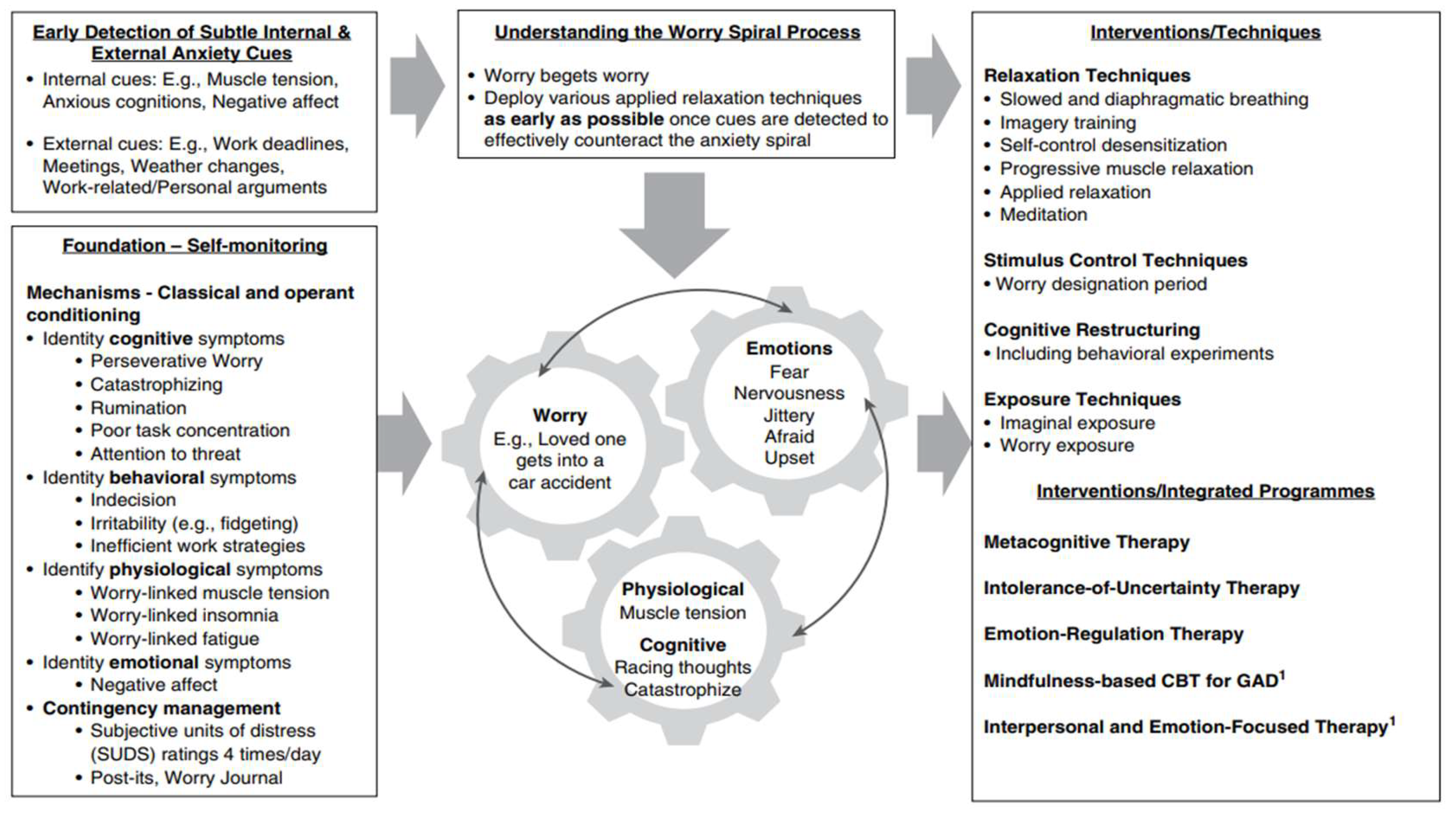
Integration of core principles, mechanisms, and techniques of CBT for GAD [17]
Problem Statement and Rationale
Practically speaking, both pharmacotherapy and psychotherapy present accessibility problems for a vast number of patients suffering from GAD. They can both be extremely costly; of the two, psychotherapy tends to be the more expensive due to the need for professionals and highly tailored therapy sessions. Hence, psychotherapy can also be inconvenient, given that patients regularly need to carve out space in their schedules to meet with professionals and travel to those sessions. On the other hand, pharmacotherapy treatments like SSRIS, SNRIS, and benzodiazepines all have shown various significant adverse effects, potentially worsening their patients’ overall wellbeing. Medication also tends to provide short-term relief, as it treats only the symptoms of disorders rather than their underlying causes. A form of treatment for GAD that is truly effective in the long-term, is accessible to everyone, and can be done in a flexible manner is greatly needed.
Significance and Purpose
Thus, the purpose of this review is to evaluate meditation, with an emphasis on mindfulness meditation like Buddhist Vipassana, for its effectiveness in dealing with anxiety and to compare it with first line treatment options for anxiety disorders. This review compares meditation with other treatments because meditation has the potential to be a treatment method that is also free, accessible, versatile, and easily integrable into daily life. It is hypothesized that meditation could prove to be an effective alternative treatment to conventional medication and therapy that anxiety patients could independently implement themselves. Additionally, meditation could be a fantastic supplement to medication and therapy if combining them significantly increases their effectiveness.
This dual potential of meditation—as both a standalone and complementary treatment—aligns with the principles of Buddhist Vipassana meditation, a practice rooted in deep mindfulness and insight [15]. It involves extraordinary attentiveness to the six senses (seeing, hearing, smelling, tasting, touch, and thought) while cultivating equanimity, or an attitude of non-interference toward whatever arises [15]. Through this Vipassana meditation, a practitioner learns to observe both positive and negative experiences without reacting. By not engaging with negativity, it loses its power and eventually dissolves, leading to purification. Vipassana operates on the principle that ordinary experiences, when met with mindfulness and equanimity, yield profound insights and purification. Mindfulness entails precise, rich, and continuous awareness of each moment, while equanimity means allowing the senses to function without interference, even at the subconscious level. Suffering, often caused by resistance to pain, is reduced by learning to experience pain without attaching to it, thereby separating it from resistance. Likewise, craving is a form of grasping around pleasure. When awareness is complete and interference is absent, one senses the pure state of “I am” and simultaneously realizes that the self is a process rather than a fixed entity. This realization leads to profound freedom and happiness that are independent of external circumstances. In Vipassana, this path to insight is complemented by the cultivation of loving-kindness and compassion, which form the other half of the practice.
Objectives
The objectives of this review are to assess the effectiveness of meditation as a treatment for anxiety, particularly in comparison with pharmacotherapy and psychotherapy, to investigate whether meditation can function as a standalone treatment for anxiety or if it works best as a complementary treatment alongside existing therapies, and to explore the potential benefits of meditation in terms of accessibility, cost-effectiveness, and flexibility, particularly for patients who face barriers to conventional treatments.
Scope and Limitations
The scope of this review includes SSRIs, SNRIs, and benzodiazepines under the pharmacotherapy type of treatment and CBT under the psychotherapy type of treatment. Although there exist many other forms of pharmacotherapy and psychotherapy, SSRIs, SNRIs, benzodiazepines, and CBT are among the most clinically studied and proven forms of treatment for GAD and hence were included in the review.
Although this review places an emphasis on Vipassana meditation since it’s one of the most relatively well-documented forms of meditation in Western medicine, there aren’t widely available studies testing its effect on GAD. Hence, studies incorporating MBSR, a secularized version of Vipassana utilizing the same principles, and more general forms of mindfulness meditation were used in the review.
Results
Many forms of conventional treatment to GAD have been shown to be efficacious. One meta-analysis focusing on CBT compares efficacy rates of the treatment on anxiety across various studies has results of the effect size from 0.33 to 0.57 to 0.82 [16].
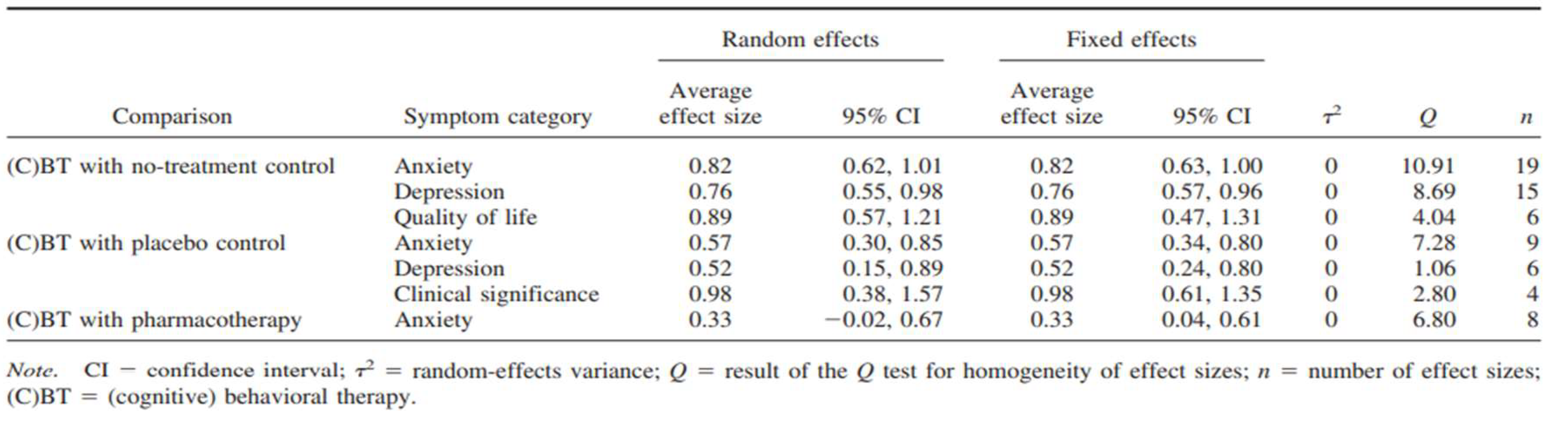
Average Effect Sizes for Posttest of the Symptom Categories Comparing Therapy Approaches [16]
When comparing the effect on symptoms between these treatments, CBT is demonstrated to be a highly effective treatment for GAD, alleviating core anxiety symptoms, reducing related depressive symptoms, and enhancing quality of life [16]. Additionally, CBT is recognized as the only empirically supported treatment for GAD (Chambless & Ollendick, 2001), showing significant reductions in acute symptoms and sustaining treatment benefits for up to two years [17]. According to another study’s results, CBT has displayed a larger effect size on treating GAD than pharmacotherapy does (g = 0.76 vs. g = 0.38) [18]. However, the study also notes that the two treatment methodologies are often tested using different controls and that there is some publication bias towards psychotherapies.
Nevertheless, in the realm of pharmacotherapy, all SSRIs, SNRIs, and benzodiazepines have all shown significant efficacy (g = 0.36, 0.42, and 0.38 respectively) [19]. Initially, BZs can rapidly alleviate symptoms due to their quick onset of action, often reaching peak efficacy within just days of starting treatment. However, this efficacy tends to diminish after approximately four weeks of continuous use, after which their effectiveness can plateau [19]. Antidepressants (ADs) like SSRIs and SNRIs, on the other hand, generally require a longer period to reach their full therapeutic effect, typically taking between four to eight weeks [19]. This extended onset can be challenging for patients to tolerate, especially due to the side effects that may accompany early stages of AD use. Meanwhile, BZs present a range of adverse effects of their own, particularly with long-term use, which is associated with cognitive impairments and an elevated risk of dementia [19].
As for meditation, a paper by Koszycki et al. studied the effectiveness of mindfulness-based stress reduction (MBSR) versus cognitive behavioral group therapy (CBGT) for social anxiety disorder (SAD) [20]. MBSR is a secularized form of Vipassana meditation that applies similar principles. SAD, like GAD, is another type of anxiety disorder. The study found that although MBSR didn’t reduce SAD symptoms as effectively as CBGT did, MBSR “was equally efficacious in improving functioning, mood and subjective well-being.” Furthermore, a different study by Hoge et al that evaluated efficacy of MBSR specifically on GAD concluded that MBSR does indeed beneficially affect GAD symptoms, with an effect size of 1.06 and a significant reduction in most clinical outcome measures (questionnaires like CGI-S, CGI-I, BAI, and PSQI to report various psychological symptoms) but not all (HAM-A) [21].
It was also observed that patients who learned mindfulness meditation had improved coping during a laboratory stress paradigm, raising the possibility that mindfulness may imbue some resilience to stressful psychological challenges. Additionally, one study observed that mindfulness meditation training helped reduce the stress response in individuals with GAD, as evidenced by changes in HPA axis hormones and inflammatory markers, suggesting it may enhance resilience to psychological stress [22]. Another study indicated that even brief mindfulness meditation training supports self-regulation and improves heart rate, benefits commonly seen in long-term practitioners [23].
Furthermore, one more study confirmed that mindfulness meditation reduces state anxiety by activating a network of brain regions, notably the anterior cingulate cortex (ACC), anterior insula, and ventromedial prefrontal cortex (vmPFC) [24]. Additionally, in contrast to experienced Zen meditators, participants with brief meditation training were able to effectively reduce amygdala activation when exposed to negative emotional stimuli (Taylor et al., 2011). The observed link between vmPFC activation and anxiety relief offers valuable insight into how mindfulness meditation may regulate self-referential processes. Moreover, increased activation in the ACC and anterior insula correlated with more substantial reductions in state anxiety.
Conclusions
In conclusion, the efficacy of mindfulness meditation as a treatment for GAD demonstrates promising, albeit varied, results when compared with established treatments such as cognitive-behavioral therapy (CBT) and pharmacotherapy. CBT consistently achieves strong effect sizes in reducing both anxiety and comorbid depressive symptoms, with effects that are often maintained long after treatment. Pharmacotherapy, particularly with SSRIs and SNRIs, also provides significant relief, although the delayed onset of therapeutic benefits and risk of side effects can complicate its long-term use. Benzodiazepines offer rapid symptom relief but are typically unsuitable for prolonged treatment due to diminishing efficacy and potential adverse effects with extended use.
Mindfulness meditation, particularly in the form of mindfulness-based stress reduction (MBSR), adds a valuable alternative by directly targeting stress responses and enhancing emotional regulation. Although there just isn’t much literature available that directly compares the efficacy rates of meditation to pharmacotherapy and psychotherapy in treating GAD, meditation’s capacity to reduce symptoms and to improve functioning, mood, and subjective well-being provides an appealing complement to more traditional interventions and merits further research to investigate its full potential as a treatment. Furthermore, the neurophysiological changes associated with mindfulness, including enhanced activation in brain regions linked to self-regulation and anxiety reduction, suggest a unique mechanism by which mindfulness may support resilience and emotional stability in patients with GAD.
Discussion
Restatement of Key Findings
This literature review examines the effectiveness of mindfulness meditation, particularly Buddhist Vipassana, compared to conventional treatments like pharmacotherapy and psychotherapy for managing GAD. Ultimately, there is limited knowledge regarding direct comparisons between the efficacy of meditation, pharmacotherapy, and psychotherapy efficacy rates. Additionally, the precise underlying mechanisms of neither mindfulness meditation nor GAD are fully understood, as many complex factors influence them.
Implications and Significance/ Connection to Objectives
Many insights into optimizing treatments for GAD can be drawn from the available research and data. Firstly, it would still be worthwhile to keep pharmacotherapy as a first-line treatment for anxiety disorders like GAD. SSRIs, SNRIs, and benzodiazepines have all concretely demonstrated significant efficacy in reducing GAD symptoms relatively quickly, targeting specific chemical pathways. While antidepressants like SSRIs and SNRIs can have adverse effects, taking an initial combined approach of antidepressants and benzodiazepines can mitigate those side effects while boosting anxiolytic effects earlier and for a longer range of time. However, medication tends to only deal with symptoms, rather than addressing underlying causes of disorders.
CBT as a psychotherapy is empirically supported to provide lasting anxiolytic effects for GAD for multiple years, meaning a longer-term solution. CBT also promotes healthy lifestyle changes that help patients learn how to independently tackle some of the root causes of anxiety. However, CBT may not be for everyone, as it is known to have problems with retention; for instance, some patients start CBT but do not complete the treatment. Furthermore, its need for professionals to give regular, highly tailored therapy sessions means that it is often less affordable and much more time-intensive, so certain patients may not have the time or resources for it.
Unlike CBT, mindfulness meditation like Vipassana is a journey that patients undertake by themselves, as opposed to having a structured format, so it provides more flexibility for practitioners, who can use it as often as they find helpful. Mindfulness meditation fosters resilience by encouraging self-reflection, helping individuals cultivate stability regardless of external circumstances, unlike CBT’s focus on external behaviors. Although meditation requires immense focus as well as a genuine effort to shift one’s lifestyle and has not been empirically supported as an effective standalone treatment method for GAD, it may still provide help for those who can’t afford other conventional treatments.
In addition to being a potential independent solution for individuals with limited access to therapy or medications, meditation’s value as a complementary treatment warrants attention. Evidence suggests that mindfulness meditation can counteract some of the adverse effects of pharmacotherapy, such as restlessness or irritability, by increasing self-awareness and reducing agitation. Combining mindfulness meditation with CBT may also help patients improve retention rates, as meditation’s focus on emotional regulation could enhance their commitment to structured therapies. Additionally, meditation’s broader applications for overall well-being, beyond addressing anxiety symptoms, make it a holistic tool that could supplement conventional treatments.
Further Research
Future studies should aim to investigate the efficacy and application of meditation as a treatment for anxiety disorders through several avenues. First, comparative clinical trials could directly assess the long-term effectiveness of meditation practices, such as Vipassana and Mindfulness-Based Stress Reduction (MBSR), in comparison to pharmacotherapy and psychotherapy. Such trials would help determine whether meditation can be considered a viable alternative to first-line treatments.
Another promising area is the development of personalized meditation protocols that account for individual differences in anxiety triggers and patient profiles. Identifying which techniques work best for specific groups of patients could enhance the overall efficacy of meditation-based interventions.
Further research should also focus on the neurobiological mechanisms behind meditation’s effects on anxiety. Studies could examine how meditation influences brain structures, such as the amygdala and prefrontal cortex, and neurotransmitter systems, providing insights into the physiological changes associated with this practice.
Additionally, it would be valuable to explore preventative applications of meditation. Investigating whether regular meditation practice can reduce the likelihood of developing Generalized Anxiety Disorder (GAD) in at-risk populations, such as students or healthcare workers, could expand its role as a proactive mental health strategy.
The potential of combining meditation with traditional treatments should also be examined. Research could determine whether integrating meditation with pharmacotherapy or psychotherapy reduces medication dosages or improves therapy adherence, thereby optimizing treatment outcomes.
Finally, digital and app-based meditation could provide a scalable and cost-effective method for delivering meditation interventions and may help integrate meditation into existing treatments. These resources could bridge the gap for individuals unable to attend in-person therapy or purchase costly medications. Research should assess whether such meditation is as effective as in-person treatment sessions in managing anxiety symptoms.
This study provides a valuable foundation for future research by highlighting both the efficacy and limitations of existing treatments for anxiety disorders. By comparing meditation with pharmacotherapy and psychotherapy, it underscores the need for more accessible, sustainable, and long-term solutions for anxiety management. The findings offer a roadmap for future studies to build upon, particularly in exploring meditation’s unique advantages as a standalone or complementary treatment. Further research could refine and expand upon these insights to develop more personalized, preventative, and scalable approaches to mental health care, ensuring that effective treatments reach broader and more diverse populations.
Limitations
While this review provides valuable insights, it faces various obstacles that limit its scope. For one, the lack of widely available data surrounding meditation efficacy for anxiety disorders and the lack of standardization of evaluating efficacy across and within treatment types makes drawing a definite comparison challenging. The thematic analysis method used, though effective for identifying broad patterns, may lack the precision of quantitative meta-analyses. Lastly, the review does not account for individual variability in treatment responses, which could affect the generalizability of its conclusions. Future studies should aim to address these limitations through more rigorous, large-scale trials and personalized approaches.
Closing Statement
In summary, mindfulness meditation, while not yet rivaling the established efficacy of pharmacotherapy and psychotherapy as standalone treatments for GAD, presents significant potential as a complementary or alternative approach. Its emphasis on resilience and emotional stability, coupled with its accessibility and flexibility, underscores the importance of continued research. Exploring ways to integrate meditation into conventional care while addressing its barriers will be crucial for realizing its full therapeutic potential. Future studies should investigate methods to standardize meditation practices for clinical trials and assess the long-term benefits of combining meditation with conventional treatments like CBT and pharmacotherapy. Future studies should investigate methods to standardize meditation practices for clinical trials [20,21] and assess the long-term benefits of combining meditation with conventional treatments like CBT and pharmacotherapy [22,20]. Future studies should investigate methods to standardize meditation practices for clinical trials and assess the long-term benefits of combining meditation with conventional treatments like CBT and pharmacotherapy.
Methods
Search Strategy and Inclusion Criteria
The literature for this review was sourced primarily from Google Scholar and PubMed. Search terms included keywords such as anxiety, Generalized Anxiety Disorder (GAD), pharmacotherapy, SSRIs, SNRIs, benzodiazepines, psychotherapy, Cognitive Behavioral Therapy (CBT), mindfulness meditation, Vipassana meditation, and Mindfulness-Based Stress Reduction (MBSR). Inclusion criteria required that sources be generally well-cited, with a preference for studies referenced in at least 200 other works. However, for niche topics where fewer studies were available, the threshold was lowered to at least 50 citations. Additionally, sources were required to be relatively recent, with most published within the last two decades, to ensure relevance to current treatment practices and trends.
Data extraction
Key data points were systematically extracted from the selected studies to facilitate comparison and analysis. Extracted information included efficacy rates for various treatment modalities, physical observations on patients' conditions, documented drawbacks and adverse effects of treatment methods, and insights into the mechanisms by which each treatment operates. This data provided a comprehensive basis for evaluating the comparative effectiveness of pharmacotherapy, psychotherapy, and meditation in managing anxiety disorders.
Synthesis Method
A thematic analysis was employed to synthesize findings from the included studies. The analysis focused on key themes such as efficacy, treatment accessibility, and the potential of meditation as both a standalone and complementary intervention. Studies were organized into categories based on treatment types—pharmacotherapy, psychotherapy, and meditation—to facilitate a structured comparison. A narrative synthesis approach was then applied to highlight commonalities and differences in outcomes across the different treatment modalities. This method allowed for a nuanced discussion of the benefits and limitations of each approach, with particular attention given to the unique advantages offered by meditation practices, including their accessibility and potential for long-term effectiveness.
Acknowledgements
I would like to express my gratitude to my mentors at Polygence for their invaluable guidance and support throughout this research process. Their insights and feedback were instrumental in shaping the direction of this review. I am also deeply thankful for the encouragement and inspiration provided by my family. Finally, I appreciate the countless researchers and practitioners whose work made this review possible, contributing to a deeper understanding of anxiety treatments and meditation practices.
References
- Goodwin, R.D.; Weinberger, A.H.; Kim, J.H.; Wu, M.; Galea, S. Trends in anxiety among adults in the United States, 2008–2018: Rapid increases among young adults. Journal of Psychiatric Research 2020, 130, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Pashazadeh Kan, F.; Raoofi, S.; Rafiei, S.; Khani, S.; Hosseinifard, H.; Tajik, F.; Raoofi, N.; Ahmadi, S.; Aghalou, S.; Torabi, F.; Dehnad, A.; Rezaei, S.; Hosseinipalangi, Z.; Ghashghaee, A. A systematic review of the prevalence of anxiety among the general population during the COVID-19 pandemic. Journal of Affective Disorders 2021, 293, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Ruscio, A.M.; Hallion, L.S.; Lim CC, W.; Jeon, Y.J.; Wang, L.; Tonillo, D. Cross-sectional comparison of the epidemiology of DSM-5 generalized anxiety disorder across the globe. JAMA Psychiatry 2017, 74, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.; Stead, T.S.; Mangal, R.; Ganti, L. General anxiety disorder in youth: A national survey. Health Psychology Research 2022, 10, 39578. [Google Scholar] [CrossRef]
- Means-Christensen, A.J.; Roy-Byrne, P.P.; Sherbourne, C.D.; Craske, M.G.; Stein, M.B. Relationships among pain, anxiety, and depression in primary care. Depression and Anxiety 2008, 25, 593–600. [Google Scholar] [CrossRef]
- Holmes, M.; Newman, M.G. Generalized anxiety disorder. In M. Hersen, J. C. Thomas, & D. L. Segal (Eds.), Comprehensive Handbook of Personality and Psychopathology (pp. 101–122). Hoboken, NJ: Wiley. 2006.
- Weisberg, R.B. Overview of generalized anxiety disorder: Epidemiology, presentation, and course. The Journal of Clinical Psychiatry 2006, 70 (Suppl 2), 4–9. [Google Scholar] [CrossRef]
- Brawman-Mintzer, O.; Lydiard, R.B. Biological basis of generalized anxiety disorder. Journal of Clinical Psychiatry 1997, 58, 16–26. [Google Scholar]
- Adwas, A.A.; Jbireal, J.M.; Azab, A.E. Anxiety: Insights into signs, symptoms, etiology, pathophysiology, and treatment. East African Scholars Journal of Medical Sciences 2019, 2, 80–91. [Google Scholar]
- Nemeroff, C.B. The role of GABA in the pathophysiology and treatment of anxiety disorders. Psychopharmacology Bulletin 2003, 37, 133–146. [Google Scholar]
- Nutt, D.J. Overview of diagnosis and drug treatments of anxiety disorders. CNS Spectrums 2005, 10, 49–56. [Google Scholar] [CrossRef]
- Bandelow, B.; Michaelis, S.; Wedekind, D. Treatment of anxiety disorders. Dialogues in Clinical Neuroscience 2017, 19, 93–107. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, L.; Nutt, D. Anxiolytics. Psychiatry 2007, 6, 284–288. [Google Scholar] [CrossRef]
- Szuhany, K.L.; Simon, N.M. Anxiety disorders: A review. JAMA 2022, 328, 2431–2445. [Google Scholar] [CrossRef] [PubMed]
- Young, S. Purpose and method of Vipassana meditation. The Humanistic Psychologist 1994, 22, 53–61. [Google Scholar] [CrossRef]
- Mitte, K. Meta-analysis of cognitive-behavioral treatments for generalized anxiety disorder: A comparison with pharmacotherapy. Psychological Bulletin 2005, 131, 785–802. [Google Scholar] [CrossRef] [PubMed]
- Hoyer, J.; Newman, M.G. (2020). Generalized anxiety disorder and worrying: A comprehensive handbook for clinicians and researchers. New York, NY: Springer.
- Carl, E.; Witcraft, S.M.; Kauffman, B.Y.; Gillespie, E.M.; Becker, E.S.; Cuijpers, P.; Powers, M.B. Psychological and pharmacological treatments for generalized anxiety disorder (GAD): A meta-analysis of randomized controlled trials. Cognitive Behaviour Therapy 2020, 49, 1–21. [Google Scholar] [CrossRef]
- Gomez, A.F.; Barthel, A.L.; Hofmann, S.G. Comparing the efficacy of benzodiazepines and serotonergic anti-depressants for adults with generalized anxiety disorder: A meta-analytic review. Expert Opinion on Pharmacotherapy 2018, 19, 883–894. [Google Scholar] [CrossRef]
- Koszycki, D.; Benger, M.; Shlik, J.; Bradwejn, J. Randomized trial of a meditation-based stress reduction program and cognitive behavior therapy in generalized social anxiety disorder. Behaviour Research and Therapy 2007, 45, 2518–2526. [Google Scholar] [CrossRef]
- Hoge, E.A.; Bui, E.; Marques, L.; Metcalf, C.A.; Morris, L.K.; Robinaugh, D.J.; Simon, N.M.; Palitz, S. A. Randomized controlled trial of mindfulness meditation for generalized anxiety disorder: Effects on anxiety and stress reactivity. The Journal of Clinical Psychiatry 2013, 74, 16662–16668. [Google Scholar] [CrossRef]
- Hoge, E.A.; Bui, E.; Palitz, S.A.; Schwarz, N.R.; Owens, M.E.; Johnston, J.M.; Simon, N.M. The effect of mindfulness meditation training on biological acute stress responses in generalized anxiety disorder. Psychiatry Research 2018, 262, 328–332. [Google Scholar] [CrossRef]
- Zeidan, F.; Johnson, S.K.; Gordon, N.S.; Goolkasian, P. Effects of brief and sham mindfulness meditation on mood and cardiovascular variables. The Journal of Alternative and Complementary Medicine 2010, 16, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Zeidan, F.; Martucci, K.T.; Kraft, R.A.; McHaffie, J.G.; Coghill, R.C. Neural correlates of mindfulness meditation-related anxiety relief. Social Cognitive and Affective Neuroscience 2014, 9, 751–759. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



