
Submitted:
16 January 2025
Posted:
16 January 2025
You are already at the latest version
Abstract
Background: To elucidate the mechanisms of resistance to treatment in patients with acute myeloid leukemia (AML) except for M3 so as to devise ways to overcome them and improve the treatment outcomes. Methods: For this study, we randomly selected 35 patients with AML who had received combined cytarabine plus idarubicin treatment for new-onset AML at our hospital. Expressions of 23 treatment-resistance-related proteins in the biopsy specimens were evaluated by immunohistochemical staining using the corresponding antibodies, followed by retrospective analysis of the correlations between the expression of the resistance proteins and patient survival. Results: The following four proteins were identified as being particularly significant in relation to treatment resistance and patient prognosis. 1) p53, 2) Multidrug resistance-associated protein 1 (MRP1) (Idarubicin extracellular efflux pump) 3)Aldo-keto reductase family 1 member B10 (AKR1B10) (Idarubicin-inactivating enzyme), and 4)AKR1B1 (AKR1B10 competitive
Keywords:
AML
; Urayasu classification
; prognostic index
; P53
; MRP1
; AKR1B10
; AKR1B1
1. Introduction (A Brief Review)
The efficacy of chemotherapy is dependent on the expressions of cancer-related genes and functional proteins that play important molecular and cellular roles in the development of resistance to anticancer drugs. Drug resistance to anticancer therapy may appear even before the start of treatment (endogenous drug resistance) or develop after the start of treatment (acquired drug resistance). Drug resistance is the main cause of treatment resistance and recurrence in most malignancies. We provide guidelines for the development of future cancer treatments based on a better understanding of the mechanisms of drug resistance, which could be expected to yield better treatment outcomes [1]. We are currently engaged in the study of the poor prognosis associated with treatment resistance caused by the expression of functional proteins involved in drug resistance in hematopoietic malignancies. We have already proposed the Urayasu classification for prognostic classification of large B-cell lymphomas (LBCL) and aggressive T-cell lymphomas (TCL), based on the patterns of expressions of multiple resistance factors even before the start of treatment (endogenous drug resistance) [2,3]. Although the association between gene mutations and patient prognosis in AML is well known [4]. herein, we would like to propose the AML Urayasu classification based on the patterns of expressions, even prior to the start of treatment, of multiple resistance (endogenous) factors. For reference, we shall briefly outline the mechanisms of drug resistance in AML. [5]
(1) Angiogenesis and vascular hyperplasia due to extracellular release of microenvironmental factors, and escape from the immunosurveillance mechanism
1) Non-immune microenvironmental factors
Factors that facilitate overcoming of stress conditions such as hypoxia and hypoglycemia in the tumor microenvironment.
- 1.
GRP94 exists mainly in the endoplasmic reticulum or mitochondria. It is secreted outside the cell and regulates apoptosis, inflammation, and angiogenesis. [6] Upregulation of GRP94 has been observed in various cancers, including multiple myeloma, suggesting the validity of developing treatment agents that can selectively target GRP94. [7]
- 2.
GRP78 is mainly expressed in the endoplasmic reticulum. Expression of GRP78 is associated with cancer, and is a potential therapeutic target as well. [8] Expression of this protein has been identified in high-risk pediatric patients with B-cell acute lymphoblastic leukemia (B-ALL). [9] It has been reported that combined GRP78-CAR-T cell + dasatinib can substantially enhance its effector function. [10]
- 3.
TGFβ1 is involved in cell growth and differentiation, apoptosis, angiogenesis, and cellular immunity. In the early stages of cancer development, it inhibits cell transformation and prevents progression of cancer, whereas in the later stages, it promotes tumor progression through mesenchymal transition, triggering angiogenesis, and inducing immunosuppression.11 Failure of regulation of the TGFβ1 pathway has been reported in many hematological malignancies, including myelofibrosis, AML, and malignant lymphoma. [12]
- 4.
- Tumor necrosis factor α1 (TNFα1) [13]
TNFα is involved in the progression and relapse of AML and is associated with decreased patient survival. [13] We have previously reported that fibrosis caused by TGF-β1 and TNF-α1 produced by hematologic malignancies is associated with a poor prognosis. [14] Soluble TNF initiates TNFR1 signaling, but not TNFR2 signaling, despite receptor binding, unless it does so as the second messenger. [15] TNFR1 is expressed in AML and promotes proliferation of the tumor cells. [16] TNFR1 and Caspase10 expressed in ALL induce cell death [17].
2) Immune microenvironmental factors (3 types)
1. Programmed cell death-1 (PD-1) (CD279) [18]
2. Programmed cell death–ligand 1(PD-L1, CD274) [19]
In AML, PD-L1 expression is known to be associated with a poor prognosis.
3. Programmed cell death –ligand 2 (PD-L2, CD273)[20]
In AML, the tumor cell surface expression of PD-1/PD-L1,2 is clinically significant, and these patients benefit from immune checkpoint inhibitor therapy.
(2) Equilibrative nucleoside transporter 1 (ENT1) decreases drug uptake [21]
In patients with AML, a decrease in cytarabine influx associated with a decrease in tumor ENT1 expression may cause treatment resistance.
(3) Enhanced drug elimination
1. Multidrug resistance 1 (MDR1) [22]: MDR1 can be a useful molecular marker of the prognosis in AML patients.
2. Multidrug resistance-associated protein 1 (MRP1) [23]: Tumor MRP1 expression has a significant effect on the survival in patients with AML.
3 Multidrug resistance-associated protein 4 (MRP4) [24]: MRP4 could become established as a novel promising target to develop agents inhibiting tumor growth and inducing apoptosis.
(4) Changes in drug metabolism
1. Cytochrome P450 3A4 (CYP3A4) [25]: Combined use of FLT3 TKIs and CYP3A4 inhibitors could be a promising strategy for AML.
2. CYP2B6 [26]: CYP2B6 variants are significantly associated with acute leukemia risk.
3. Aldo-keto reductase family 1 member C3 (AKR1C3) [27]: In AML and T-cell acute lymphoblastic leukemia (T-ALL), AKR1C3 expression in the tumor cell cytoplasm degrades doxorubicin hydrochloride taken up into the cytoplasm, causing treatment resistance.
4. AKR1B1 [28]: AKR1B1 induces tumor cell proliferation in the late stage of AML. AKR1B1 is very similar in structure to AR1B10 and the two may competitively inhibit each other's actions.
5. AKR1B10 [29] : The intracellular concentration of daunomycin is decreased mainly by AKR1B1 and AKR1C3; these two proteins also decrease the intracellular concentrations of idarubicin, but only by about one-fifth. AKR1B10 decreases the intracellular concentration of not only daunomycin, but also of idarubicin. AKR1B10 also catalyzes reduction of the carbonyl groups of daunomycin and idarubicin, drugs used in the treatment of AML, taken up by the cytoplasm, converting the drugs into water-soluble inactive alcohols. Similar to AKR1C3, it is also involved in the development of resistance to cisplatin. AKR1B10 is considered to play a central role in the development of cyclophosphamide resistance. On the other hand, AKR1C3 is known to be associated with methotrexate as well as vincristine resistance. AKR1B10 is regulated by genes expressed on chromosome 7q33. In the event of a missing chromosome 7, AKR1B10 regulation fails and the protein function is enhanced. Dasatinib, Bcr-Abl tyrosine kinase inhibitor, has a moderating effect on AKR1B10 and is expected to be applied to treatment of AML because it inhibits the metabolism of daunomycin and Idarubicin. [30] Ibrutinib, a tyrosine kinase inhibitor, has a moderating effect on AKR1C3 and is expected to be applied to the treatment of AML because it inhibits the metabolism of doxorubicin.
(5) Other functional proteins
1. Thymidine phosphorylase (TP) [31]: Expression of TP, which is involved in resistance to malnutrition, angiogenesis, infiltration, and metastasis, in lymphomas is associated with a poor patient prognosis due to its anti-apoptotic and angiogenic effects.
2. P53[32]: After induction chemotherapy for AML, there is a possibility that the p53 protein conformation shifts from short-chain to long-chain p53 protein, leading to treatment resistance.
3. MYC [33]: MYC gene-related abnormalities in AML are associated with other negative prognostic factors, such as complex karyotypes and advanced age, although they are observed in less than 1% of cases.
4. Glutathione sulfate transferase (GST) [34]: The GST1 genotype may be useful for selecting an appropriate chemotherapy regimen for AML.
2. Materials and Methods
2.1. Patients and Sample Collection
We enrolled 35 patients who had received standard combined idarubicin + cytarabine treatment as initial remission-induction therapy for new-onset AML (excluding APL) at our hospital between 2015 and 2020 in this study. The distribution of the disease types in the patients is shown in Table 1. We performed immunohistochemical (IHC) staining of formalin-fixed paraffin-embedded biopsy specimens to determine the expressions of 23 different proteins that have previously been reported as treatment-resistance factors using the corresponding antibodies; positive and negative staining results were determined by observation under an optical microscope. The results were then compiled and statistically analyzed retrospectively. We used variables such as anti-cancer drug metabolic factors in the analysis model and compared the overall survivals (OS) of the patients after the initial remission-induction therapy by the log-rank test. The 2022 ELN risk classification35 was used as the control.
2.2. Immunohistochemistry
Tissue biopsy specimens from the patients were fixed in formalin and embedded in paraffin to prepare tissue blocks, which were then sectioned and subjected to IHC staining. The primary antibodies directed against the major proteins involved in anticancer drug me tabolism were as follows: 1) GRP94: Proteintech (Rosemont, IL 60018, USA), clone 1H10B7 (this monoclonal antibody was generated against the N-terminal region of full-length HSP90b1); 2) CYP3A4: Sigma-Aldrich (St. Louis, MO 63103, USA), SAB1400064 (this polyclonal antibody was generated against CYP3A4.); 3) AKR1C3: Proteintech, 11194-1-AP (this polyclonal antibody was generated against AKRC3.); 4) MDR1 (P-glycoprotein): Proteintech, 22336-1-AP (this polyclonal antibody was generated against MDR1.); 5) MRP1 (CD9): Proteintech, 60232-1-IG (this monoclonal antibody was generated against the N-terminal region of full-length MRP1.); 6) TGF-beta1: Proteintech, 21898-1-AP (this polyclonal antibody was generated against TGF-beta); 7) GRP78: Proteintech, 66574-1-IG (this monoclonal antibody was generated against the N-terminal region of full-length GRP78); 8) glutathione S-transferase-kappa1 (GST): Proteintech, 14535-1-AP (this polyclonal antibody was generated against GST1.); 9) thymidine phosphorylase: Abcam (Cambridge, UK), ab226917 (this polyclonal antibody was generated against thymidine phosphorylase); 10) MRP4 (ABCC4): SANTA CRUZ BIOTECHNOLOGY (Dallas, TX 75220, USA), SC-376262 (this monoclonal antibody was generated against the N-terminal region of full-length MRP4 [amino acid 1-280].); 11) CYP2B6: LifeSpan BioSciences, Inc. (Seattle, WA 98121, USA)., LS-C352084 (this polyclonal antibody was generated against CYP2B6.); 12) TNF1alpha: Sigma-Aldrich, SAB4502982 (this polyclonal antibody was generated against TNF1alpha.).:13) PD-1: 14) PD-L1:, Proteintech, 66248-1-IG, mouse IgG1 monoclonal antibody. Clone 2B11D11: 15) PD-L2 Proteintech,18251-1-AP 16, rabbit IgG polyclonal antibody,: 16) P53:, Cell Signaling Technology, Inc. (3 Trask Lane Danvers, MA 01923, USA.), DO-7 mouse monoclonal antibody #48818;, 17) c-MYC: Abcam (Kendall Sq Cambridge, MA 02139, USA), Y69 clone ab32072; 18) ENT-1 (equilibrative nucleoside transporter 1): Proteintech. 1337-1-AP rabbit IgG polyclonal antibody;. 19) AKR1B1: Sigma-Aldrich (3050 Spruce Street Saint Louis, MO 63103, USA), rabbit polyclonal antibody HPA052751;. 20) AKR1B10:Sigma-Aldrich (3050 Spruce Street Saint Louis, MO 63103 USA), rabbit monoclonal antibody HPA020280. After the immunostaining, two pathologists definitively determined the results of the IHC staining. Positive IHC staining was judged on the basis of more than 50% of the tumor cells showing positive staining, and weakly positive staining was also considered. The concordance rate between the twopathologists for the staining results was about 83%. In the case of disagreement on a staining result between the two pathologists, the final diagnosis was arrived at by consensus.
2.3. Statistical Analysis
To confirm the association between the OS and poor prognostic factors/factors involved in anticancer drug metabolism after idarubicin plus cytarabine treatment as the initial induction therapy, survival curves were plotted by the Kaplan-Meier method and factors significantly associated with the OS were evaluated by the log-rank test. The significance level in the statistical tests was set at 0.05 (two-tailed) and p <0.05 was considered as indicative of a statistically significant difference. Statistical analyses were performed using EZR version 2.7-1 software (Saitama Medical Center, Jichi Medical University, Saitama, Japan) 30 Multiple comparisons were not considered because of the exploratory nature of this study.
3. Results
Kaplan-Meier Survival Curves and Comparisons Among Groups (Log Rank Test)
As shown in Figure 1, the median OS was not reached in the 35 patients after the initial remission-induction therapy. The 5-year survival was 72%. A log-rank test was performed to compare the OS rates of the patients in relation to the patterns of expressions of anti-cancer drug metabolic factors. There were no significant differences in the OS rates among the patients included in the Adverse group according to the European Leukemia Net (ELN) classification. However, the patients in this group showed significant differences in the expressions of 3 factors, namely, p53, MRP1, and AKR1B10. Furthermore, there were no significant differences in the expression rate of AKR1B1, which competitively inhibits the metabolic degradation of idarubicin by AKR1B10; the effect of idarubicin is enhanced by AKR1B1 inhibiting AKR1B10, which results in a relatively good prognosis.
As shown in Figure 2, the results of univariate analysis showed that the decrease in OS rates differed significantly among patients showing different patterns of expression of p53, MPR1, AKR1B10, and AKR1B1 (a competitive inhibitor of AKR1B10). We added the expression of ENT1, a pump that promotes the influx of cytarabine into the blast cells in AML, to these factors, and based on the patterns of expression, we performed a stratified analysis of the OS rates. The results showed significant differences in the OS rates among patients showing different patterns of expressions of the combinations of p53 and MRP1, AKR1B1 and AKR1B10, AKR1B10 and MRP1, as well as p53 and ENT1. We had high hopes for the significance of the expressions of idarubicin-metabolizing enzyme AKR1B10 (poor prognosis) and cytarabine influx pump ENT1 (good prognosis) used in remission-induction therapy, but unfortunately, no significant differences in the OS related to the expressions of these proteins was observed, although a trend towards a good prognosis associated with their expressions was recognized.
Figure 2 The results of univariate analysis showed that the decrease in OS rates differed significantly among patients showing different patterns of expression of p53, MPR1, AKR1B10, and AKR1B1 (a competitive inhibitor of AKR1B10).
Figure 2.
Overall survival of AML patients with and without expression of the prognostic factors. —Comparison of the Kaplan-Meier survival curves (OS) and prognostic factors, positive/negative on immunostaining between 2 groups (log-rank test)—*The combinations of the 2 groups are indicated in black texts and black lines when both groups are negative, and in red, green, and blue when they are not, respectively. See Table 2 for the correlation between p53 and other factors. A. A remarkably significant difference was observed in the combination of P53 and MRP1 (p < 0.01).p53 (-) MRP1 (+), n = 1, OS 12 months, 2-year OS 0%p53 (+) MRP1 (-), n = 3, OS 14 months, 2-year OS 0%p53 (-) MRP1 (-), n = 31, 50% OS Not reached, 5-year OS 82%. B. A significant difference was observed in the combination of AKR1B10 and its competitive inhibitor AKR1B1 (p < 0.01).AKR1B1 (-) AKR1B10 (+), n = 13, OS 22 months, 5-year OS 43%AKR1B1 (-) AKR1B10 (-), n = 18, OS Not reached, 5-year OS 82%. C. A remarkably significant difference in the expression of the combination of MRP1 and AKR1B10 was observed (p < 0.01).MRP1 (+) AKR1B10 (+), n = 1, OS 12 months, 2-year OS 0%MRP1 (-) AKR1B10 (+), n = 16, OS Not reached, 5-year OS 56%MRP1 (-) AKR1B10 (-), n = 18, OS Not reached, 5-year OS 82%. D. No significant difference in the expression of the combination of AKR1B10 and p53; the association was observed (NS).AKR1B10 (+) p53 (+), n = 3, OS 14 months, 2-year OS 0%AKR1B10 (+) p53 (-), n = 14, OS Not reached, 5-year OS 74%AKR1B10 (-) p53 (-), n = 18, OS Not reached, 5-year OS 82%. E. No significant difference in the expression of the combination of ENT1 and AKR1B10; the association was observed (NS).ENT1 (-) AKR1B10 (+), n = 2, OS 22 months, 2-year OS 0%ENT1 (+) AKR1B10 (+), n = 15, OS Not reached, 5-year OS 78%ENT1 (+) AKR1B10 (-), n = 16, OS Not reached, 5-year OS 100%ENT1 (-) AKR1B10 (-), n = 2, OS Not reached, 5-year OS 100%F. A remarkably significant difference was observed in the expression of the combination of ENT1 and AKR1B10 (p < 0.01).ENT1 (+) p53 (+), n = 3, OS 14 months, 2-year OS 0%ENT1 (-) p53 (-), n = 4, OS 22 months, 5-year OS 52%ENT1 (-) p53 (-), n = 28, OS Not reached, 5-year OS 82%ENT1 (-) p53 (-), n = 4, OS Not reached, 5-year OS 100%.
Figure 2.
Overall survival of AML patients with and without expression of the prognostic factors. —Comparison of the Kaplan-Meier survival curves (OS) and prognostic factors, positive/negative on immunostaining between 2 groups (log-rank test)—*The combinations of the 2 groups are indicated in black texts and black lines when both groups are negative, and in red, green, and blue when they are not, respectively. See Table 2 for the correlation between p53 and other factors. A. A remarkably significant difference was observed in the combination of P53 and MRP1 (p < 0.01).p53 (-) MRP1 (+), n = 1, OS 12 months, 2-year OS 0%p53 (+) MRP1 (-), n = 3, OS 14 months, 2-year OS 0%p53 (-) MRP1 (-), n = 31, 50% OS Not reached, 5-year OS 82%. B. A significant difference was observed in the combination of AKR1B10 and its competitive inhibitor AKR1B1 (p < 0.01).AKR1B1 (-) AKR1B10 (+), n = 13, OS 22 months, 5-year OS 43%AKR1B1 (-) AKR1B10 (-), n = 18, OS Not reached, 5-year OS 82%. C. A remarkably significant difference in the expression of the combination of MRP1 and AKR1B10 was observed (p < 0.01).MRP1 (+) AKR1B10 (+), n = 1, OS 12 months, 2-year OS 0%MRP1 (-) AKR1B10 (+), n = 16, OS Not reached, 5-year OS 56%MRP1 (-) AKR1B10 (-), n = 18, OS Not reached, 5-year OS 82%. D. No significant difference in the expression of the combination of AKR1B10 and p53; the association was observed (NS).AKR1B10 (+) p53 (+), n = 3, OS 14 months, 2-year OS 0%AKR1B10 (+) p53 (-), n = 14, OS Not reached, 5-year OS 74%AKR1B10 (-) p53 (-), n = 18, OS Not reached, 5-year OS 82%. E. No significant difference in the expression of the combination of ENT1 and AKR1B10; the association was observed (NS).ENT1 (-) AKR1B10 (+), n = 2, OS 22 months, 2-year OS 0%ENT1 (+) AKR1B10 (+), n = 15, OS Not reached, 5-year OS 78%ENT1 (+) AKR1B10 (-), n = 16, OS Not reached, 5-year OS 100%ENT1 (-) AKR1B10 (-), n = 2, OS Not reached, 5-year OS 100%F. A remarkably significant difference was observed in the expression of the combination of ENT1 and AKR1B10 (p < 0.01).ENT1 (+) p53 (+), n = 3, OS 14 months, 2-year OS 0%ENT1 (-) p53 (-), n = 4, OS 22 months, 5-year OS 52%ENT1 (-) p53 (-), n = 28, OS Not reached, 5-year OS 82%ENT1 (-) p53 (-), n = 4, OS Not reached, 5-year OS 100%.
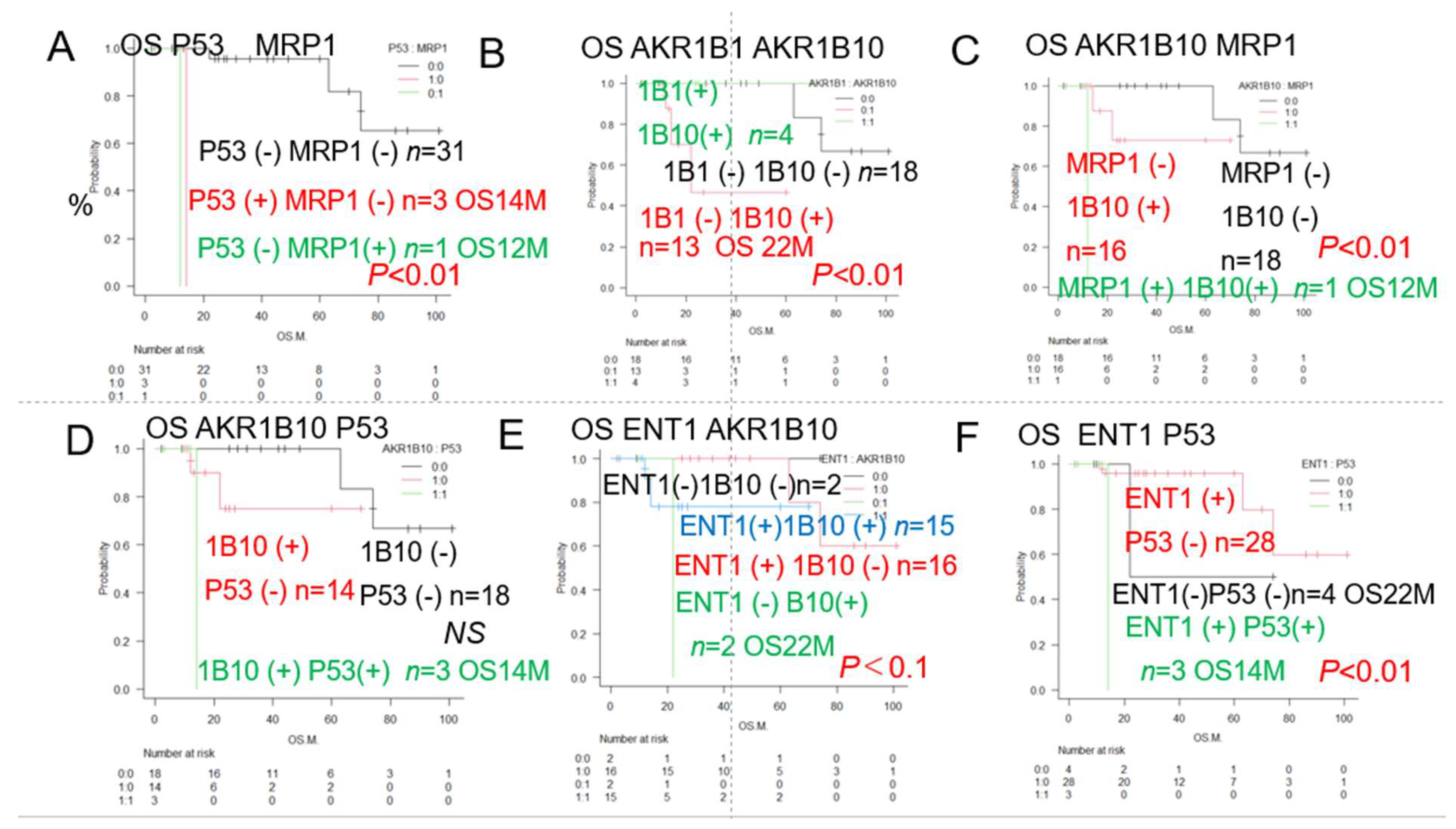
Table 2 is a summary of the results of analysis of the IHC staining patterns for 23 different proteins/antibodies. Results of survival assessed by the Kaplan-Meier method, the median cumulative survival rate and 95% confidence interval (CI), as well as the results of comparison among the groups (p-value: log rank test) are shown. Poor prognostic factors were evaluated based on the differences in survival. Significant (p < 0.05) poor prognostic factors are marked with (#). The conventional prognostic factors associated with classification of the patients into the Favorable group, Intermediate group, and Adverse group (Figure 1B) per the ELN classification, as well as complex karyotypes and del(7) showed a trend towards correlation with the OS, but no significant differences were observed. However, significant correlations between expressions of p53, MRP1, and AKR1B10 and decreased OS were observed, as shown in Figure 1. Conversely, a trend towards improved OS was shown in patients showing tumor AKR1B1 (competitive inhibitor of AKR1B10) expression, but the difference was not statistically significant. Of the combined expressions of 2 factors that showed the most significant associations with the OS, at least 11 combinations included p53. Of these, the combination of p53 and MRP1, in particular, showed the most significant association with the OS (Figure 2A). A significant association with the OS was observed for the combined expression of AKR1B10 and ALR1B1 as well (Figure 2B). Therefore, we focused on the patterns of expression of 4 factors, namely, p53, MRP1, AKR1B10, and AKR1B1, and devised the AML Urayasu classification, a prognostic classification based on the mechanisms underlying the development of drug resistance, as shown in Figure 3.
As shown in Figure 3, in addition to the combination of p53 and MRP1, we would like to propose the following AML Urayasu classification using AKR1B10, an enzyme that degrades the remission-induction therapy agent idarubicin, and AKR1B1, a competitive inhibitor of AKR1B10. Specifically, based on Figure 2A, the poor prognosis group was defined as Group 3, which consisted of patients showing p53-positivity or MRP1-positivity (n = 4). The other favorable prognosis groups that consisted of patients with the p53-negative/MRP1-negative patterns (n = 31) were defined as Group 1 and Group 2. Group 2 included patients who were AKR1B10-positive/AKR1B1-negative (n = 9) and Group 1 included others (AKR1B10-positive/AKR1B1-positive or AKR1B10-negative/AKR1B1-negative, AKR1B10-negative/AKR1B1-positive). Significant differences in the OS were observed among all the groups. These results are also shown in Table 2.
Figure 3
Figure 3.
Overall survival of TCL patients with and without expression of the prognostic factors (TCL Urayasu classification). —Kaplan-Meier survival curves and comparisons among the 3 groups (Groups 1-3) (log-rank test)—A. AML Urayasu classification (The first step) Immunostaining for p53 and MRP1 was performed for all the 35 cases enrolled in this study.Group 3: The median OS in the 4 cases that were p53(+) or MRP1(+) was 12-14 months (p < 0.01), indicating an absolutely poor prognosis. The median OS was not reached in the remaining 31 cases of Group 1 + Group 2, which were p53-negative and MRP1-negative, and showed a 5-year survival rate of 82% (p < 0.01), indicative of a good prognosis.B. AML Urayasu classification (The second step)Immunostaining for AKR1B1 and AKR1B10 was performed in the 31 cases of Group 1 + Group 2 which were p53-negative and MRP1-negative.Group 1 consisted of 22 patients, including 4 patients who were AKR1B10-positive/AKR1B1-positive (5-year OS 100%) and 18 patients who were AKR1B10-negative/AKR1B1-negative (5-year OS 82%).Group 2 consisted of 9 patients who were AKR1B10-positive/AKR1B1-negative (2-year OS 63%).
Figure 3.
Overall survival of TCL patients with and without expression of the prognostic factors (TCL Urayasu classification). —Kaplan-Meier survival curves and comparisons among the 3 groups (Groups 1-3) (log-rank test)—A. AML Urayasu classification (The first step) Immunostaining for p53 and MRP1 was performed for all the 35 cases enrolled in this study.Group 3: The median OS in the 4 cases that were p53(+) or MRP1(+) was 12-14 months (p < 0.01), indicating an absolutely poor prognosis. The median OS was not reached in the remaining 31 cases of Group 1 + Group 2, which were p53-negative and MRP1-negative, and showed a 5-year survival rate of 82% (p < 0.01), indicative of a good prognosis.B. AML Urayasu classification (The second step)Immunostaining for AKR1B1 and AKR1B10 was performed in the 31 cases of Group 1 + Group 2 which were p53-negative and MRP1-negative.Group 1 consisted of 22 patients, including 4 patients who were AKR1B10-positive/AKR1B1-positive (5-year OS 100%) and 18 patients who were AKR1B10-negative/AKR1B1-negative (5-year OS 82%).Group 2 consisted of 9 patients who were AKR1B10-positive/AKR1B1-negative (2-year OS 63%).
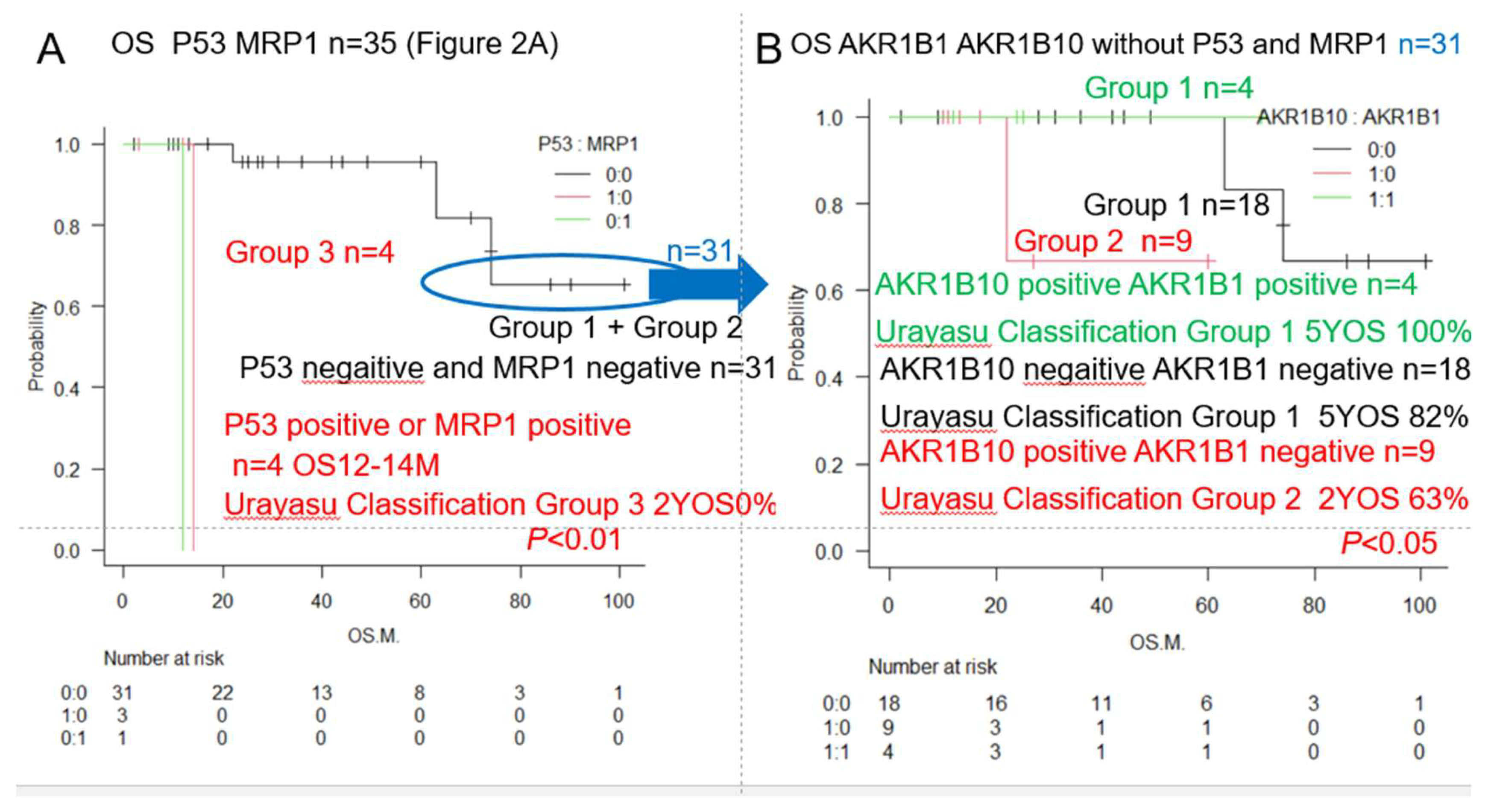
Figure 4 illustrates a case that is thought-provoking with regard to the AML Urayasu classification established on the basis of the results of IHC staining. The patient was a 74-year-old female who was diagnosed as having a complex-karyotype AML and received combined idarubicin + cytarabine treatment as the initial remission-induction therapy, but CR was not achieved. As re-induction therapy, she received combined venetoclax + azacitidine treatment, but CR was not achieved and the patient died 3 months later. Consent for autopsy could not be obtained. The patient showed tumor p53-positivity and was classified into Group 3. The tumor was MRP1-negative, AKR1B10-positive, and AKR1B1-negative. Her disease was resistant to the combined treatment with idarubicin + cytarabine as the initial remission-induction therapy. A possible reason for this is that her tumor cells were p53-positive and AKR1B10-positive/AKR1B1 (competitive inhibitor of AKR1B10)-negative, which could have led to rapid metabolism of idarubicin within the AML blast cells, which was therefore no longer able to suppress tumor cell growth. The patient received combined venetoclax + azacitidine treatment as re-induction therapy for remission, but remission was not achieved. The reason for this may be that the venetoclax was rapidly metabolized within the AML blast cells due to an increase in the expression of CYP3A4, which metabolizes venetoclax.
Red font indicates positivity and black font indicates negativity. HE is an abbreviation for hematoxylin-eosin stain.The patient was a 74-year-old female. Her diagnosis was AML, complex karyotype. She died by 3 months after the diagnosis due to resistance to the second-line treatment. Staining slides 1 and 2 show numerous blast cells at 40x and 400x in HE-stained sections. Slides 3 and 4 show positive staining of several blast cells for CD34, suggesting the diagnosis of acute leukemia. Slides 5 and 6 show positive results of myeloperoxidase (MPO) staining, and the patient was diagnosed as having AML. Slides 7 and 8 show positive staining for p53 and the patient was classified into Group 3, a group with an extremely poor prognosis, according to the Urayasu classification for AML. Slides 9 and 10 showed negative staining of the tumor cells for MRP1. Slides 11 and 12 show positive staining for AKR1B10-positive, indicating that idarubicin is likely quickly metabolized within the blast cells. Furthermore, slides 13 and 14 show negative staining for AKR1B1, which competitively inhibits AKR1B10, as the reason for the patient becoming refractory to treatment. Slides 15 and 16 show positive staining of the tumor cells for GRP94, which is expressed in many AML cells, conferring upon the tumor the ability to adapt to the microenvironment. Slides 17 and 18 show positive staining of the tumor cells for CYP3A4, which is involved in the metabolism of idarubicin, cytarabine as well as venetoclax. Slides 19 and 20 show positive staining of the tumor cells for ENT-1 expression, which functions as an intracellular influx pump for cytarabine.
Figure 5 shows a summary of the prognostic factors associated with treatment resistance in the LBCL Urayasu classification [2], TCL Urayasu classification[2], and AML Urayasu classification (this article) in an easy-to-understand Venn diagram with 3 circles. The prognostic factor common to all the 3 diseases is the proliferation activator p53. The microenvironmental factor, GRP94, and idarubicin-detoxifying enzyme AKR1C3 are common prognostic factors in TCL and LBCL. In AML and LBCL, the shared prognostic factor is the idarubicin extracellular efflux pump, MRP1. In TCL, microenvironmental factors as well as 5 types of survival activators (PD-1, PD-L1, TP, GRP78, GRP94) are also important prognostic factors. In LBCL, CYP3A4 which detoxifies doxorubicin and the doxorubicin efflux pump, MDR1, are important prognostic factors. In AML, AKR1B10, which detoxifies idarubicin and AKR1B1, which blocks the detoxification of idarubicin are important prognostic factors.
Table 3 shows a comparison of the AML Urayasu classification and the 2022 ELN risk classification. Our analysis of the OS yielded slightly better results; this was thought to be because a higher proportion of patients were classified into the Favorable and Intermediate groups, and a lower proportion is classified into the Adverse prognosis group by the AML Urayasu classification, making it easier to extract groups with a good prognosis.
4. Discussion
In general, IHC with visualization under an optical microscope is considered as a very useful test, as it allows confirmation of the positivity/negativity while also allowing the tumor cells to be identified. The result of IHC was rated as weakly positive when 50% or more of the tumor cells show positive staining. In this study of patients with AML, immunostaining was performed using antibodies against 23 curative treatment resistance factors [6-34] as determined from a review of the literature. Based on the results, we propose a new prognostic classification called the AML Urayasu classification that we believe would be useful to predict the efficacy of the initial 3+7 remission induction combination therapy of idarubicin + cytarabine in patients with new-onset AML. Our AML Urayasu classification (1) through (3), derived from the results shown in Figure 3 and Table 2 is as follows: (1) Group 1 (Favorable prognosis): Of the 35 patients, 22 (63%) showed the following IHC pattern: p53(-)/MRP1(-), and AKR1B10(+)/AKR1B1(+) or AKR1B10(-)/AKR1B1(-). The 5-year OS of the patients in this group was 82%-100% (In the ELN AML recommendation, [35] which is the conventional prognostic classification, n = 562, 37%, 59%, 5-year OS: approximately 50%, median OS: 4 years); (2) Group 2 (Intermediate prognosis): Of the 35 patients, 9 patients (26%) showed the following staining pattern: p53(-)/MRP1(-) and AKR1B10(+)/AKR1B1(-). Their 5-year OS was 68% (ENL classification, n = 355, 23%, 5-year OS: approximately 20%, median OS: approximately 15 months); Group 3 (Adverse prognosis): Of the 35 patients, four (11%) showed the following staining pattern: p53(+) or MRP1(+). Their median survival was 12-14 months, and the 2-year OS was 0% (ENL classification, n = 616, approximately 40%, 5-year OS: 8%, median OS: approximately 15 months). Even though the AML Urayasu classification is based on IHC results of a small number of patients, we expect that it will contribute to stratification of the treatment and advances in treatment methods, as it is based on treatment-resistance mechanisms. In this AML analysis, as shown in Table 2, there was no significant difference in the OS as compared with the ELN classification. Table 3 shows a comparison of the AML Urayasu classification and the 2022 ELN risk classification. Our analysis of the OS yielded slightly better results; this was thought to be because a higher proportion of patients were classified into the Favorable and Intermediate groups, and a lower proportion is classified into the Adverse prognosis group by the AML Urayasu classification, making it easier to extract groups with a good prognosis. The AML Urayasu classification was able to identify a higher proportion of patients with a favorable prognosis than the ELN classification. These groups may not necessarily require allogeneic transplantation. Furthermore, the fact that the cause of treatment resistance is clarified in this method through analysis at the level of functional proteins is important for considering future treatment methods.For example, in the case of AML Urayasu classification Group 3, in patients with p53–positivity, it is difficult to induce remission with chemotherapy alone, [32] and in patients with BCL2-positivity and CYP3A4 (venetoclax-metabolic enzyme)-negativity, venetoclax should be used. [36] Furthermore, in patients showing MCL1-positivity, a treatment approach including azacitidine should be considered. [37] In Figure 4, we describe a case that is thought-provoking with regard to the AML Urayasu classification established based on the results of IHC staining. The patient showed p53-positivity and was classified into Group 3; she was MRP1 [23] (doxorubicin efflux pump)-negative, AKR1B10-positive, and AKR1B1-negative. Her disease was resistant to the initial remission-induction therapy of idarubicin +cytarabine. This could be attributable to the loss of tumor suppressor function due to p53 positivity, [32] making it difficult to suppress proliferation with chemotherapy alone, as well as because idarubicin was rapidly metabolized within the AML blast cells due to the AKR1B10-positive/AKR1B1 (competitive inhibitor of AKR1B10)-negative staining result. [29] The patient was treated with venetoclax + azacitidine as re-induction therapy for remission induction, [38] but remission was not achieved. The reason for this could be that the expression of CYP3A4, which metabolizes venetoclax, caused rapid metabolism of venetoclax within the AML blast cells. [36] The patient died by 3 months after the diagnosis.In the future, it may be possible to devise individualized AKR1B10 inhibitor therapy for each case. AKR1B10 shows 70.6% amino acid sequence homology with aldose reductase AKR1B1, and the structures and substrate specificities are also extremely similar. Since many compounds that inhibit AKR1B10 also inhibit AKR1B1 to a similar extent, compounds that selectively inhibit each enzyme have been sought and generated. [39] HCCFA, 7-hydroxy-2-(4-methoxyphenylimino)-2H-chromene-3-carboxylic acid benzylamide (HMPC) is a compound generated through such a process, and it strongly and selectively inhibits AKR1B10. [39] AKR1B10 causes cisplatin resistance as well. It is also considered to cause strong resistance to cyclophosphamide, and there are concerns that the cyclophosphamide effect in cyclophosphamide + Total body irradiation or cyclophosphamide + busulfan used for pre-allogenic transplantation conditioning will be compromised and the relapse rate will increase. [39] In addition, AKR1B10 is regulated by genes on chromosome 7q33. If chromosome 7 is missing, AKR1B10 regulation would fail and the enzyme would become active. The Bcr-Abl tyrosine kinase inhibitor dasatinib has a moderating effect on AKR1B10 and is expected to be applied to treatment because it inhibits the metabolism of daunomycin or idurubicin. [29,40] NSAIDs such as N-phenyl-anthranilic acid, diclofenac, and glycyrrhetinic acid competitively inhibit AKR1B10. [41] Based on the above, inhibitors such as HCCFA, dasatinib, and NSAIDs are considered as promising for stratified treatments as AKR1B10 inhibitors in patients with AML.There are reports that MRP1 is expressed in some cases of normal-karyotype AML. [23,42] The patient with MRP1-positivity in this case series had Inversion 16+ 8 trisomy. Her disease relapsed about 11 months after diagnosis and she became treatment-resistant due to MRP1 expression. MRP1 is located on chromosome 16 at p13.13-p13.12. AML with inversion of chromosome 16, inv(16)(p13q22), often lacks MRP1 gene expression, and is known to be associated with a good prognosis and to respond well to chemotherapy. [43] However, in this case, it was considered that MRP1 was unexpectedly expressed, causing resistance of the malignancy to chemotherapy. The relationships among the treatment resistance factors included in the Urayasu classification in AML, TCL, [3] and LBCL[2] are summarized in Figure 5. The following is a discussion of Figure 5. Of the treatment resistance factors, p5332 expression is shared by all 3 diseases. The positivity rate for p53 is high in the order of TCL (10/16, 67%), LBCL (15/42, 36%), and AML (5/35, 9%). In other words, the cause of a poor prognosis in patients with TCL is largely because of the expression of p53. p53 is an important tumor suppressor, and loss of p53 function due to mutation or other causes can lead to cancer development. p53 mutation is noted in over 50% of human cancers. However, there are currently no drugs approved for the clinical treatment of cancers harboring p53 mutations. [44] The commonly expressed treatment resistance factors between TCL and LBCL include GRP94 and AKR1C3. The positivity rate for the microenvironmental factor GRP94 is high in the order of AML (33/35, 94%), LBCL (38/42, 90%), and TCL (10/16, 67%). Many tumor cells in AML and LBCL, as well as TCL, use GRP94 to adapt to their environment, which may contribute to the development of treatment resistance and recurrence. The positivity rate for the enzyme AKR1C3, which inactivates doxorubicin, cyclophosphamide, and vincristine, is high in the order of LBCL (26/42, 62%), AML (17/35, 46%), and TCL (6/16, 38%). Thus, in LBCL, for which R-CHOP therapy and Pola-RCHP therapy are standard treatments, AKR1C3 could contribute to acquired treatment resistance. AML with p53 (3/35, 9%) and MRP1 (1/35, 3%) carries a poor prognosis, and although the positivity rate for both is low at 12%, an MRP1 inhibitor has been developed. [45,46] In addition to microenvironmental factors that have a significant impact on the prognosis of TCL, AML cells become resistant to treatment when they express the enzyme AKR1B10, which metabolizes the anthracycline-based anticancer drug idarubicin. [29] AKR1B1 shows 70.6% amino acid sequence homology with AKR1B10, and the structures and substrate specificities are also extremely similar. Since many compounds that inhibit AKR1B10 also competitively inhibit AKR1B1 to a similar extent, reducing AKR1B10 activity would eliminate treatment resistance. [39] The Abl tyrosine kinase inhibitor dasatinib has a moderating effect on AKR1B10, and is expected to be applied to the treatment of AML, because it inhibits the metabolism of daunomycin and idurubicin. [29] AKR1B10 is considered to play a central role in cisplatin resistance and cyclophosphamide resistance. [29] In fact, caution is needed, as AKR1B10-positivity in AML may compromise the efficacy of high-dose cyclophosphamide, which is used as a conditioning regimen for allogeneic hematopoietic stem cell transplantation. AKR1B10 is regulated by genes on chromosome 7q33. If chromosome 7 is missing, AKR1B10 fails to be regulated and would become active. As shown in Table 2, we investigated the impact of deletion of chromosome 7 and AKR1B10 on the OS, and found that 6 out of the 35 patients showed both deletion of chromosome 7 and AKR1B10-positivity, and tended to have an absolutely poor prognosis. On the other hand, in TCL, the tumor cells show excellent microenvironmental adaptability, and in LBCL, the tumor cells are considered to have even better anticancer drug detoxification ability.
5. Conclusions
In summary, when performing IHC diagnosis of AML pathology, it is possible to evaluate the prognosis and divide the patients into 3 prognostic groups according to the new Urayasu classification for AML (Group 1 [favorable prognosis], Group 2 [intermediate prognosis], and Group 3 [poor prognosis]) with at least 4 additional treatment resistance proteins (4 factors [p53, MRP1, AKR1B10, AKR1B1]). In the future, we would like to attempt to improve the treatment outcomes of new-onset AML by using MRP1 and AKR1B10 inhibitors, a stratified treatment approach based on the AML Urayasu classification. Furthermore, hereafter, we plan to analyze a larger number of cases, as well as analyze other hematological malignancies and summarize the results. The analysis method is IHC staining for 4 treatment resistance proteins, which allows one to obtain quick results, and is also simple and inexpensive. Furthermore, it is remarkable that our Urayasu classification classifies approximately twice as many patients into the favorable prognosis group as the ELN classification. We would like to conduct further validation by analyzing a larger number of cases in the future.6. Patents
Author Contributions
Planning of the study authors: HT, MN Study conduct authors: HT, MF Reporting authors: HT, MN TO The conceptionauthors: HT, MN The designauthors: HT, MN, CF Acquisition of dataauthors: MF, ST, SK, HA, MO, TS A analysis and interpretation of the dataauthors: HT, MN, MA, TN, HN, HIH.
Funding
This research received no external funding.
Institutional Review Board Statement
I “The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
None of the patients was involved in the design of this study. The results will be made known to the study participants on the homepage of our website. No additional data available.
Ethics approval statement
Juntendo Urayasu Hospital Ethics Committee.
Acknowledgments
We greatly appreciate the assistance we received from Kotobiken Medical Laboratories Inc. (Tokyo, Japan) for the immunohistochemical analysis.
Competing interests
A Conflict of Interest statement is not providedfor each of the authors. .
Abbreviations
The following abbreviations are used in this manuscript:
| AML | Acute myeloid leukemia |
| IHC | Immunohistochemical staining |
| MRP1 | Multidrug resistance-associated protein 1 |
| AKR1B10 | Aldo-keto reductase family 1 member B10 |
| AKR1B1 | Aldo-keto reductase family 1 member B1 |
| AKR1C3 | Aldo-keto reductase family 1 member C3 |
| OS | Overall survival |
| ELN | European Leukemia net |
| LBCL | Large B-cell lymphoma |
| TCL | Aggressive T-cell lymphoma |
| GRP94 | Glucose-regulated protein 94 |
| GRP78 | Glucose-regulated protein 78 |
| B-ALL | B-cell acute lymphoblastic leukemia |
| TGFβ1 | Transforming growth factor β1 |
| TNFα1 | Tumor necrosis factor α1 |
| TNFR | Tumor necrosis factor receptor |
| PD-1 | Programmed cell death-1 |
| PD-L1 | Programmed cell death–ligand 1 |
| ENT1 | Equilibrative nucleoside transporter 1 |
| MDR1 | Multidrug resistance 1 |
| MRP1 | Multidrug resistance-associated protein 1 |
| CYP3A4 | Cytochrome P450 3A4 |
| FLT3 | fms related receptor tyrosine kinase 3 |
| TKI | Tyrosin kinase inhibitor |
| CYP2B6 | Cytochrome P450 2B6 |
| AKR1C3 | Aldo-keto reductase family 1 member C3 |
| AKR1B10 | Aldo-keto reductase family 1 member B10 |
| AKR1B1 | Aldo-keto reductase family 1 member B1 |
| TP | Thymidine phosphorylase |
| GST | Glutathione sulfate transferase |
| APL | Acute promyeloid leukemia |
| CBF | Core binding factor |
| CR | Complete remission |
| PD | Progressive disease |
| M | Months |
| NS | Not significant |
| NR | Not reached |
| MCL1 | Myeloid cell leukemia sequence 1 |
| Y | Years |
| ER | Endoplasmic reticulum |
| BCL2 | B-cell/CLL lymphoma 2 |
| Del | Deletion |
| MTX | Methotrexate |
| C | Cyclophosphamide |
| OH | Oncovin hydroxyl doxorubicin; |
| HCCFA | 7-hydroxy-2-(4-methoxyphenylimino)-2H-chromene-3-carboxylic acid benzylamide |
| NSAIDs | N-phenyl-anthranilic acid, diclofenac, and glycyrrhetinic acid |
References
- Talha Bin Emran , Asif Shahriar, Ariful Islam, and Mohammad Mahmudul Hassan et al.. Multidrug Resistance in Cancer: Understanding Molecular Mechanisms, Immunoprevention and Therapeutic Approaches. Front Oncol 2022 Jun 23:12:891652.
- Hideaki Nitta , Haruko Takizawa, Toru Mitsumori , Hiroko Iizuka-Honma, Miki Ando and Masaaki Noguchi et al. Possible New Histological Prognostic Index for Large B-Cell Lymphoma. J. Clin. Med. 2023, 12, 6324. [CrossRef]
- Hideaki Nitta , Haruko Takizawa , Toru Mitsumori, Miki Ando , and Masaaki Noguchi et al. A New Histology-Based Prognostic Index for Aggressive T-Cell lymphoma: Preliminary Results of the "TCL Urayasu Classification" J Clin Med . 2024 Jun 30;13(13):3870. [CrossRef]
- Klaus H Metzeler, Tobias Herold, Jan Braess, and Karsten Spiekermann et al.. Spectrum and prognostic relevance of driver gene mutations in acute myeloid leukemia Blood . 2016 Aug 4;128(5):686-98. Epub 2016 Jun 10. [CrossRef]
- Sebastian E. Koschade, Brandts, and Olivier Ballo et al. Relapse surveillance of acute myeloid leukemia patients in first remission after consolidation chemotherapy: diagnostic value of regular bone marrow aspirations. Annals of Hematology 2022, 101:1703–1710.
- Xiaofeng Duan, Stephen Iwanowycz, Soo Ngoi, Megan Hill 2 Qiang Zhao and Bei Liu et al. Molecular Chaperone GRP94/GP96in Cancers: Oncogenesis and Therapeutic Target. . Front Oncol. 2021. PMID: 33898309 Free PMC article. Review.
- Lee AS. Glucose-regulated proteins in cancer: molecular mechanisms and therapeutic potential. Nat Rev Cancer. 2014 Apr;14(4):263-76. [CrossRef]
- Amos Olalekan Akinyemi , Xiaoqi Liu , and Zhiguo Li et al. Unveiling the dark side of glucose-regulated protein 78 (GRP78) in cancers and other human pathology: a systematic review. Mol Med . 2023 Aug 21;29(1):112. [CrossRef]
- Tania Angeles-Floriano, Guadalupe Rivera-Torruco, Alhelí Bremer, Lourdes Alvarez-Arellano and Ricardo Valle-Rios et al. Cell surface expression of GRP78 and CXCR4 is associated with childhood high-risk acute lymphoblastic leukemia at diagnostics. Scientific Reports 2022 12:2322 | . [CrossRef]
- Nikhil Hebbar , Rebecca Epperly,Stephen Gottschalk, and M Paulina Velasquez et al.. CAR T cells redirected to cell surface GRP78 display robust anti-acute myeloid leukemia activity and do not target hematopoietic progenitor cells Nat Commun 2022 Jan 31;13(1):587. [CrossRef]
- Sulsal Haque and John C Morris. Transforming growth factor-β: A therapeutic target for cancer. Hum Vaccin Immunother. 2017 Aug 3;13(8):1741-1750. [CrossRef]
- Matthew A. Timmins and Ingo Ringshausen. Transforming Growth Factor-Beta Orchestrates Tumour and Bystander Cells in B-Cell Non-Hodgkin Lymphoma. Cancers 2022, 14, 1772. [CrossRef]
- H T Idriss, and J H Naismith TNF alpha and the TNF receptor superfamily: structure-function relationship(s) Microsc Res Tech 2000 Aug 1;50(3):184-95. [CrossRef]
- H Takizawa, M Fujishiro, S Tomita, T Mitsumori, H Nitta, H Iizuka-Honma, M Ando, and M Noguchi. et al. Role of TGF-beta1 and TNF-alpha1 produced by neoplastic cells in the pathogenesis of fibrosis in patients with hematologic neoplasms. J Clin Exp Hematop . 2023 Jun 28;63(2):83-89. [CrossRef]
- Prada JP, Wangorsch G, Lang, Dandekar T, and Wajant H.et al. A systems-biology model of the tumor necrosis factor (TNF) interactions with TNF receptor 1 and 2. Bioinformatics. 2021 May 5;37(5):669-676. PMID: 32991680. [CrossRef]
- F Vinante, A Rigo, and M Chilosi, G Pizzolo et al. Serum levels of p55 and p75 soluble TNF receptors in adult acute leukaemia at diagnosis: correlation with clinical and biological features and outcome. Br J Haematol 1998 Sep;102(4):1025-34. [CrossRef]
- Adam Cisterne, Rana Baraz, Kenneth F Bradstock, and Linda J Bendall et al. . Silencer of death domains controls cell death through tumour necrosis factor-receptor 1 and caspase-10 in acute lymphoblastic leukemia. PLoS One 2014 Jul 25;9(7):e103383. [CrossRef]
- Huizhen Cao, Tianyu Wu, Yunxiao Sun, and Youjie Li et al.. Progress of research on PD-1/PD-L1 in leukemia Front Immunol 2023 Sep 26:14:1265299. [CrossRef]
- Ayfer Geduk, Elif B Atesoglu, and Sibel Balcı.. Programmed Cell Death Ligand 1 Expression Level and Prognostic Significance in Acute Myeloid Leukemia Indian J Hematol Blood Transfus. 2022 Jul;38(3):464-472. Epub 2021 Jul 27. [CrossRef]
- Julie B Mortensen, Ida Monrad, Peter Kamper, and Francesco d'Amore et al. Soluble programmed cell death protein 1 (sPD-1) and the soluble programmed cell death ligands 1 and 2 (sPD-L1 and sPD-L2) in lymphoid malignancies Eur J Haematol . 2021 Jul;107(1):81-91. Epub 2021 Apr 12. [CrossRef]
- Myrna Candelaria, Carmen Corrales-Alfaro, Silvia Vidal-Millán, Luis A Herrera et al. Expression Levels of Human Equilibrative Nucleoside Transporter 1 and Deoxycytidine Kinase Enzyme as Prognostic Factors in Patients with Acute Myeloid Leukemia Treated with Cytarabine Chemotherapy . 2016;61(6):313-8. [CrossRef]
- Lenilton Silva da Silveira Júnior, Victor de Lima Soares, Valeria Soraya de Farias Sales, and André Ducati Luchessi et al. P-glycoprotein and multidrug resistance-associated protein-1 expression in acute myeloid leukemia: Biological and prognosis implications Int J Lab Hematol . 2020 Oct;42(5):594-603. [CrossRef]
- Desiree Kunadt, Christian Dransfeld, Markus Schaich, and Friedrich Stölzel et al . Multidrug-related protein 1 (MRP1) polymorphisms rs129081, rs212090, and rs212091 predict survival in normal karyotype acute myeloid leukemia Ann Hematol . 2020 Sep;99(9):2173-2180. Epub 2020 Jul 3. [CrossRef]
- Sabrina Copsel, Ariana Bruzzone ,Carina Shayo , and Carlos Davio et al. Multidrug resistance protein 4/ ATP binding cassette transporter 4: a new potential therapeutic target for acute myeloid leukemia Oncotarget. 2014 Oct 15;5(19):9308-21. [CrossRef]
- Yu-Ting Chang, Daniela Hernandez, Mark J Levis, and Richard J Jones et al. Role of CYP3A4 in bone marrow microenvironment-mediated protection of FLT3/ITD AML from tyrosine kinase inhibitors. Blood Adv. 2019 Mar 26;3(6):908-916. [CrossRef]
- Xuan Xiong, Dongke Yu, Hongtao Xiao, and Rongsheng Tong et al. Association between CYP2B6 c.516G >T variant and acute leukaemia. A protocol for systematic review and meta-analysis. Medicine (2021) 100:32.
- Kshitij Verma, Tianzhu Zang, Trevor M. Penning, and Paul C. Trippier, Potent and Highly Selective Aldo-Keto Reductase 1C3 (AKR1C3) Inhibitors Act as Chemotherapeutic Potentiators in Acute Myeloid Leukemia and T-Cell Acute Lymphoblastic Leukemia. J Med Chem. 2019 April 11; 62(7): 3590–3616. [CrossRef]
- Brian Laffin and J. Mark Petrash. Expression of the aldo-ketoreductases AKR1B1 and AKR1B10inhumancancers. Front Pharmacol. 2012; 3: 104. [CrossRef]
- Penning TM, Jonnalagadda S, Trippier PC, and Rižner TL et al. Aldo-Keto Reductases and Cancer Drug Resistance. Pharmacol Rev. 2021 Jul;73(3):1150-1171. [CrossRef]
- Neslihan Büküm, Eva Novotná, Petr Solich, and Vladimír Wsól et all. Inhibition of AKR1B10-mediated metabolism of daunorubicin as a novel off-target effect for the Bcr-Abl tyrosine kinase inhibitor dasatinib. Biochem Pharmacol 2021 Oct:192:114710. [CrossRef]
- Xingcao, Peter M Clifford, Rekha Bhat, Mini Abraham, and J Steve Hou et al. Thymidine phosphorylase expression in B-cell lymphomas and its significance: a new prognostic marker? Anal Quant Cytopathol Histpathol 2013 Dec;35(6):301-5.
- Nina Anensen, AnneMargrete Oyan, Oystein Bruserud and BjornTore Gjertsen et al. A distinct p53 protein isoform signature reflects the onset of induction chemotherapy for acute myeloid leukemia Clin Cancer Res . 2006 Jul 1;12(13):3985-92. [CrossRef]
- Ruby Tang , Amy Cheng , Fabian Guirales , and Wilson Yeh, c-MYC Amplification in AML. J Assoc Genet Technol . 2021;47(4):202-212.
- S M Davies, L L Robison, J A Ross, and J P Perentesis et al. Glutathione S-transferase polymorphisms and outcome of chemotherapy in childhood acute myeloid leukemia. J Clin Oncol 2001 Mar 1;19(5):1279-87. [CrossRef]
- Hartmut D€ohner,Andrew H. Wei, Agnieszka Wierzbowska and Bob L€oweb et al.. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 2022 Sep 22;140(12):1345-1377. [CrossRef]
- Ayaka Otsuki , Masaki Kumondai , Masamitsu Maekawa,and Nariyasu Mano et al. Plasma Venetoclax Concentrations in Patients with Acute Myeloid Leukemia Treated with CYP3A4 Inhibitors Yakugaku Zasshi . 2024;144(7):775-779. [CrossRef]
- Andrew H Wei , Andrew W Roberts, Phuong Khanh Morrow, and Anthony Stein. Targeting MCL-1 in hematologic malignancies: Rationale and progress Blood Rev . 2020 Nov:44:100672. Epub 2020 Feb 21. [CrossRef]
- Courtney D DiNardo, Brian A Jonas, Jalaja Potluri, and Keith W Pratz Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. N Engl J Med . 2020 Aug 13;383(7):617-629. [CrossRef]
- Satoshi Endo, Shuang Xia , Toshiyuki Matsunaga, and Akira Ikari. Synthesis of Potent and Selective Inhibitors of Aldo-Keto Reductase 1B10 and Their Efficacy against Proliferation, Metastasis, and Cisplatin Resistance of Lung Cancer Cells. J Med Chem . 2017 Oct 26;60(20):8441-8455. Epub 2017 Oct 13. [CrossRef]
- Megumi Kikuya, Kenta Furuichi , Kousei Ito, and Shigeki Aoki et al. Aldo-keto reductase inhibitors increase the anticancer effects of tyrosine kinase inhibitors in chronic myelogenous leukemia. J Pharmacol Sci . 2021 Sep;147(1):1-8. Epub 2021 May 23. [CrossRef]
- Satoshi Endo, Toshiyuki Matsunaga, Ossama El-Kabbani, and Akira Hara Selective inhibition of the tumor marker AKR1B10 by antiinflammatory N-phenylanthranilic acids and glycyrrhetic acid. Biol Pharm Bull . 2010;33(5):886-90. [CrossRef]
- Saba Kamil, Shaheen Kouser, Nehad Khan, and Ramsha Khan . Unveiling the Significance of MRP 1 in Achieving Complete Remission Following Induction Therapy in Acute Myeloid Leukemia Curr Mol Med . 2024 Jul 9. [CrossRef]
- B J Kuss, R G Deeley, and D F Callen. The biological significance of the multidrug resistance gene MRP in inversion 16 leukemias. Leuk Lymphoma. 1996 Feb;20(5-6):357-64. [CrossRef]
- Cen Zhang, Juan Liu, Tianliang Zhang, Wenwei Hu,and Zhaohui Feng. Gain-of-function mutant p53 in cancer progression and therapy J Mol Cell Biol 2020 Sep 1;12(9):674-687. [CrossRef]
- Kimberley M Hanssen , Michelle Haber, and Jamie I Fletcher Targeting multidrug resistance-associated protein 1 (MRP1)-expressing cancers: Beyond pharmacological inhibition Drug Resist Updat. 2021 Dec:59:100795. Epub 2021 Dec 10. [CrossRef]
- Amanda Tivnan, Zaitun Zakaria, Jann N Sarkaria , and Jochen H M et al. Prehn. Inhibition of multidrug resistance protein 1 (MRP1) improves chemotherapy drug response in primary and recurrent glioblastoma multiforme Front Neurosci . 2015 Jun 16:9:218. eCollection 2015. [CrossRef]
Figure 1.
Overall survival of AML patients with and without expression of the prognostic factors. —comparison of the Kaplan-Meier survival curves and disease/existing prognostic factors between 2 groups (log-rank test)—Comparison of the overall survival OS after initial (3+7) remission-induction therapy with idarubicin + cytarabine. A. The median OS for AML (n = 35) was not reached, and 5-year OS was 72%. *Hereafter, the red letters indicate the OS when the AML blast cells showed positive immunostaining. The black letters indicate the OS when the blast cells showed negative immunostaining. B. The Adverse group (n = 10) as classified according to the ELN classification did not show a significant difference in the OS rate; the median OS was not reached, and the 5-year OS was 72% (NS). C. p53-positivity was associated with a significantly reduced OS (n = 3; median OS 14 months, 2-year OS 0%, p < 0.01). D. MRP1-positivity was associated with a significantly reduced OS (n = 1; OS 12 months; 5-year OS 72%, p < 0.01). E. AKR1B10-positivity was associated with a significantly reduced OS (n = 17; Median OS Not reached; 5-year OS 63%, p < 0.05). E. AKR1B1-positivity had no significant effect on the OS, but it probably inhibited AKR1B10 and enhanced the effect of idarubicin, resulting in a very good prognosis (n = 4; Median OS Not reached; 2-year OS 72%, NS).
Figure 1.
Overall survival of AML patients with and without expression of the prognostic factors. —comparison of the Kaplan-Meier survival curves and disease/existing prognostic factors between 2 groups (log-rank test)—Comparison of the overall survival OS after initial (3+7) remission-induction therapy with idarubicin + cytarabine. A. The median OS for AML (n = 35) was not reached, and 5-year OS was 72%. *Hereafter, the red letters indicate the OS when the AML blast cells showed positive immunostaining. The black letters indicate the OS when the blast cells showed negative immunostaining. B. The Adverse group (n = 10) as classified according to the ELN classification did not show a significant difference in the OS rate; the median OS was not reached, and the 5-year OS was 72% (NS). C. p53-positivity was associated with a significantly reduced OS (n = 3; median OS 14 months, 2-year OS 0%, p < 0.01). D. MRP1-positivity was associated with a significantly reduced OS (n = 1; OS 12 months; 5-year OS 72%, p < 0.01). E. AKR1B10-positivity was associated with a significantly reduced OS (n = 17; Median OS Not reached; 5-year OS 63%, p < 0.05). E. AKR1B1-positivity had no significant effect on the OS, but it probably inhibited AKR1B10 and enhanced the effect of idarubicin, resulting in a very good prognosis (n = 4; Median OS Not reached; 2-year OS 72%, NS).
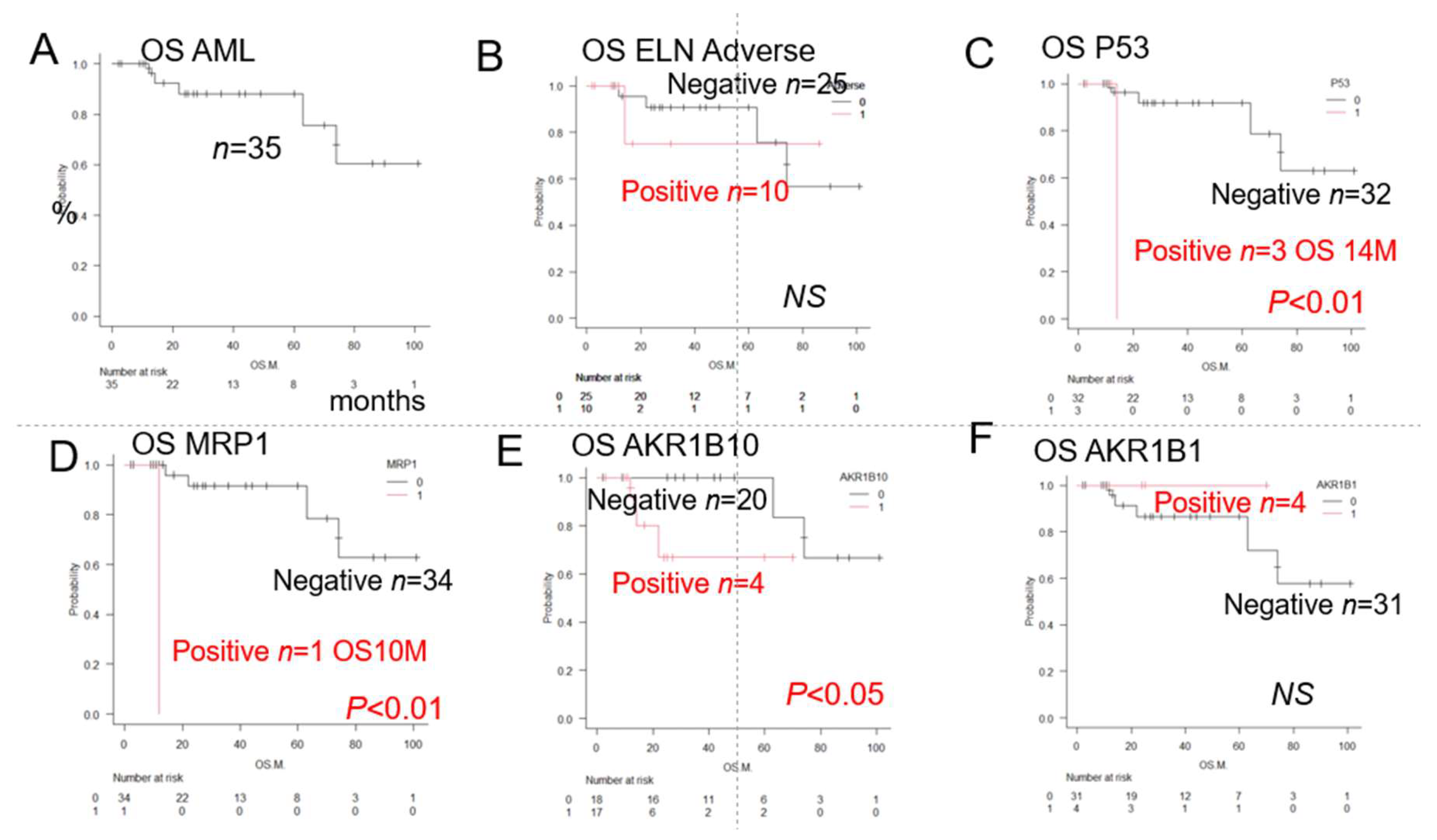
Figure 4.
Results of immunohistochemical staining of the bone marrow at disease onset in a representative patient classified into Group 3 of the AML Urayasu classification.
Figure 4.
Results of immunohistochemical staining of the bone marrow at disease onset in a representative patient classified into Group 3 of the AML Urayasu classification.
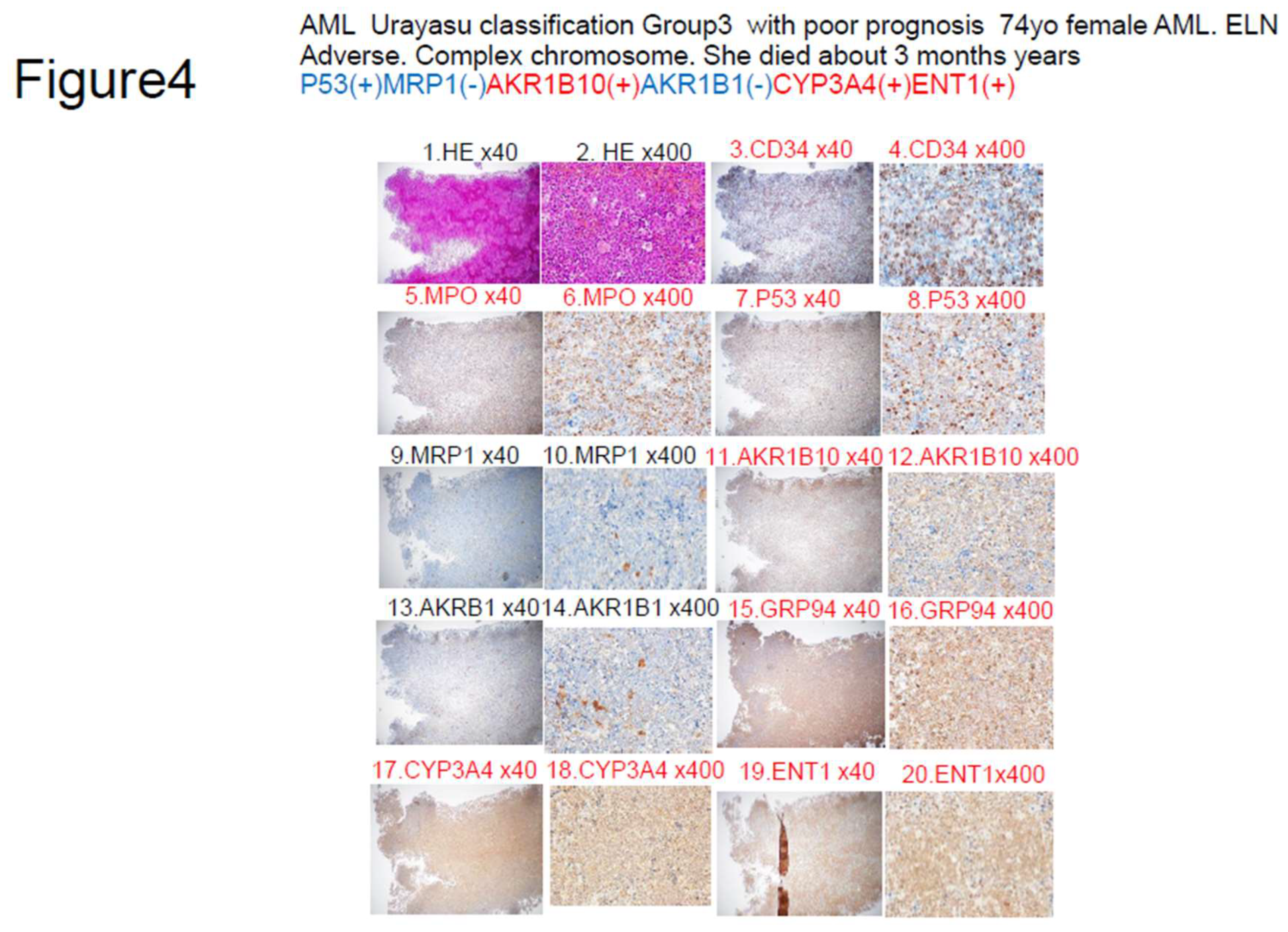
Figure 5.
A summary of the prognostic factors associated with treatment resistance in the LBCL Urayasu classification [2], TCL Urayasu classification[2], and AML Urayasu classification (this article) in an easy-to-understand Venn diagram with 3 circles.
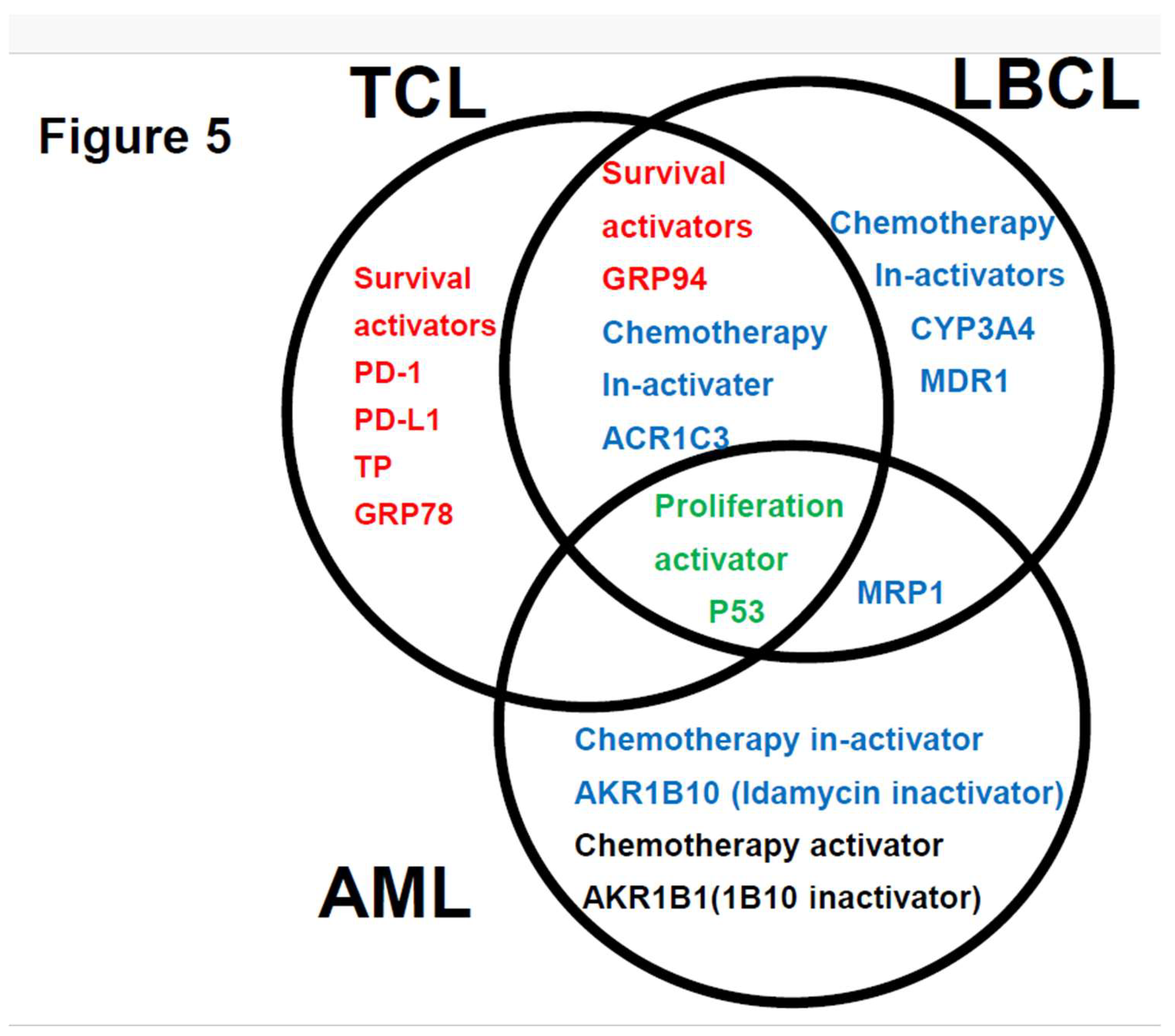

Table 1.
Characteristics of the patients included in this analysis (n=35).
| Age > 60 years (%) | 13(37%) |
| Male (%) | 20(57%) |
| Chromosome | |
| CBF t(8;21) (q22;q22) n=7, inv(16) (p12q22) n=1 | 8 (23%) |
| Normal | 10 (29%) |
| Complex chromosome | 8 (23%) |
| Chromosome 7 deletion | 9(26%) |
| European Leukemia Net | |
| Favorable | 12 (34%) |
| Intermediate | 13(37%) |
| Adverse | 10(29%) |
| Induction chemotherapy | |
| Idarubicin + cytarabine | 35(100%) |
| Outcome | |
| CR | 27(77%) |
| Non-relapse | 18(51%) |
| Relapse | 9(26%) |
| PD | 8(23%) |
| Allogeneic transplantation | 10(29%) |
Notes: CBF: core binding factor; CR: complete remission; PD: progressive disease.
Table 2.
The results of univariate analysis showed that the decrease in OS rates differed significantly among patients showing many different patterns of expression.
Table 2.
The results of univariate analysis showed that the decrease in OS rates differed significantly among patients showing many different patterns of expression.
| Category | Factors (♯Significant difference:) | n | Median OS(months) | Years (Y) survival rate | p value | Figure |
|---|---|---|---|---|---|---|
| Total | AML | 35 | NR | 5Y 73% | 1A | |
| ELN | ELN Favourable group | 12 | NR | 5Y 93% | NS | |
| ELN Intermediate group | 13 | NR | 5Y76% | NS | ||
| ELN Adverse group | 10 | NR | 5Y72% | NS | 1B | |
| Chromosome abnormality | Deletion chromosome 7 | 9 | NR | 5Y78% | NS | |
| Complex chromosome | 8 | NR | 5Y73% | NS | ||
| 12 | 74 | 5Y62% | NS | |||
| ER stress proteins | GRP94 | 33 | NR | 5Y73% | NS | |
| TGFβ1 | 27 | 63 | 5Y90% | NS | ||
| GRP78 | 30 | NR | 5Y90% | NS | ||
| TNFα1 | 20 | NR | 5Y82% | NS | ||
| OH metabolic enzyme | AKR1C3 | 16 | NR | 5Y68% | NS | |
| AKR1B1 | 4 | NR | 5Y72% | NS | 1F | |
| AKR1B10 (♯) | 17 | NR | 5Y63% | *P<0.05 | 1E | |
| C metabolic enzyme | CYP2B6 | 0 | ||||
| CHOP metabolic enzyme | CYP3A4 | 5 | NR | 3Y73% | ||
| OH efflux pump | MDR1 | 5 | NR | 3Y72% | ||
| MRP1 (♯) | 1 | 12 | 1Y0% | *p<0.01 | 1D | |
| MTX efflux pump | MRP4 | 0 | NS | |||
| Immune checkpoint | PD-1 | 0 | NS | |||
| PD-L1 | 1 | NR | 5Y100% | NS | ||
| PD-L2 | 20 | 74 | 5Y74% | NS | ||
| Others | TP | 4 | 74 | 5Y100% | NS | |
| p53 (♯) | 3 | 14 | 2Y0% | *p<0.01 | 1C | |
| GST | 28 | NR | 5Y88% | NS | ||
| MYC | 28 | 74 | 5Y82% | NS | ||
| ENT-1 | 31 | NR | 5Y88% | NS | ||
| Fibrosis (Silver stain positive) | 11 | NR | 5Y74% | p>0.05 | ||
| BCL2 | 28 | 74 | 5Y84% | p>0.05 | ||
| MCL1 | 16 | NR | 5Y88% | p>0.05 | ||
| Significant combination | ||||||
| Urayasu classification G3 | P53(+) or MRP1(+) (♯) | 4 | 13 | 2Y0% | **p<0.01 | 2A, 3,5 |
| Urayasu classification G2 | P53(-) MRP1(-) AKR1B10(+) 1B1(-) (♯) | 9 | NR | 2Y63% | *p<0.05 | 3,5 |
| Urayasu classification G1 | P53(-) MRP1(-) AKR1B10(-) 1B1(-) (♯) | 22 | NR | 5Y82% | *p<0.05 | 3,5 |
| Urayasu classification G1 | P53(-) MRP1(-) AKR1B10(+) 1B1(+) (♯) | 3 | NR | 5Y100% | *p<0.05 | 3,5 |
| P53 ENT1 (♯) P53(+) ENT1(+) | 3 | 14 | 2Y 0% | **p<0.01 | 2F | |
| MRP1 ENT1 (♯) MRP1(+) ENT1(+) | 1 | 12 | 2Y 0% | **p<0.01 | ||
| AKR1B10, AKR1B1 (♯) 1B10(+) 1B1(-) | 13 | 22 | 5Y 44% | **p<0.01 | 2B | |
| MRP1, AKR1B10 (♯) MRP1(+) 1B10(+) | 1 | 12 | 2Y 0% | **p<0.01 | 2C | |
| P53, BCL2 (♯) P53(+) BCL2(+) | 3 | 14 | 2Y 0% | *p<0.05 | ||
| P53, MCL1 (♯) P53(+) MCL1(+) | 3 | 14 | 2Y0% | **p<0.01 | ||
| P53, PD-L1 (♯) P53(+) PD-L1(-) | 2 | 14 | 2Y0% | **p<0.01 | ||
| P53, PD-L2 (♯) P53(+) PD-L2 (+) | 3 | 14 | 2Y0% | *p<0.05 | ||
| P53, CYP3A4 (♯) P53(+) CYP3A4(+) | 1 | NR | NR | **p<0.01 | ||
| P53, GRP78 (♯) P53(+) GRP78(+) | 3 | 14 | 2Y0% | **p<0.01 | ||
| P53, GRP94 (♯) P53,(+) GRP94(+) | 3 | 14 | 2Y0% | **p<0.01 | ||
| P53, AKR1C3 (♯) P53(+) AKR1C3(+) | 2 | 14 | 2Y0% | **p<0.01 | ||
| P53, TGF beta1 (♯) P53(+) TGF beta1(+) | 3 | 14 | 2Y0% | *p<0.05 | ||
| P53, MYC (♯) P53(+) MYC(+) | 3 | 14 | 2Y0% | *p<0.05 | ||
| P53, GST (♯) P53(+) GST(+) | 1 | NR | NR | *p<0.05 | ||
| Combinations with a tendancy towards association with the OS | ||||||
| Del 7, AKRB10(♯) Del 7(+) 1B10(+) | 6 | 14 | 2Y 0% | NS | ||
| BCL2, MCL1 | 23 | NS | ||||
| AKR1B10, P53 | 35 | NS | ||||
| ENT1, AKR1B10 | NS | 2E | ||||
| P53, AKR1B10 P53(+) AKR1B10(+) | 3 | 14 | 2Y 0% | NS | 2D |
Notes: OS: overall survival; AML: acute myeloid leukemia; NR: not reached; ELN: European leukemia net; ER: endoplasmic reticulum; GRP94: glucose regulated protein 94; TGFβ1: transforming growth factor β1; OH: oncovin hydroxyl doxorubicin; GRP78: glucose regulated protein 78;TNFα1: tumor necrosis factor α1; AKR1C3: aldo-keto reductase family 1 member C3; AKR1B1: aldo-keto reductase family 1 member B1; AKR1B10; aldo-keto reductase family 1 member B10;C: cyclophosphamide; CYP2B6: cytochrome P450 2B6; CYP3A4: cytochrome P450; MDR1: multidrug resistance; MRP1 multidrug resistance-associated protein 1; MTX: methotrexate; PD-1: programmed cell death-1; PD-L1: programmed cell death–ligand 1; TP: thymidine phosphorylase; GST: glutathione sulfate transferase; ENT1: equilibrative nucleoside transporter 1;BCL2: B-cell/CLL lymphoma 2; MCL1; myeloid cell leukemia sequence 1;Del: deletion.
Table 3.
Comparision of the AML Urayasu classification and 2022 ELN risk classification.
| Classification | Group 1 (Favorable) | Group 2 (Intermediate) | Group 3 (Adverse) | Figure |
|---|---|---|---|---|
| AML Urayasu | P53(-)MRP(-)AKR1B10(+) | P53(-)MRP(-)AKR1B10(+) | P53(+) or MRP1(+) | 1CDEF |
| Classification | AKR1B1(+) or | AKR1B1(-) | 2AB3AB | |
| P53(-)MRP(-)AKR1B10(-) | ||||
| AKR1B1(-) | ||||
| Cases n=22 (63%) | Cases n=9 (26%) | Cases n=4 (11%) | ||
| OS 5Y 82%-100% | OS 2Y 63% | OS 2Y 0% | ||
| Median OS NR | Median OS NR | Median OS 12-14M | ||
| ELN AML risk | Cases n=562 (37%) | Cases n=355 (23%) | Cases n=616 (40%) | 1B |
| Classification | OS 5Y 50% | OS 5Y 20% | OS 5Y 8% | |
| Median OS 4Y | Median OS 15M | Median OS 10M |
Notes: OS: overall survival; ELN: European Leukemia Net; NR: not reached; Y: years; M: months.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



