
Submitted:
14 January 2025
Posted:
15 January 2025
You are already at the latest version
Abstract
Purpose: Ankyloglossia or tongue-tie (TT) occurs when the lingual frenulum is visually altered and accompanied by restricted tongue mobility causing feeding and other difficulties with infants. Pre- and post-operative care is reported to be effective to prevent tissue reattachment and ensure feeding success. The purpose of this study was to obtain feedback and insights from caregivers and health professionals for an evidence-based pre- and post-operative exercise protocol for breastfeeding infants undergoing surgical management for TT.
Methods: A qualitative approach was used to evaluate an evidence-based pre- and post-operative exercise protocol for infants with TT, through virtual semi-structured interviews with healthcare professionals and caregivers of children with TT. Five caregivers and eight current practicing clinicians were interviewed to obtain feedback on the protocol. Results were analysed using thematic analysis.
Results: Four themes were generated from participants: 1) Parental confidence and competence; 2) The need for individualised and adaptable instruction; 3) Supporting the caregiver and infant equally; and 4) Regular and periodic support and adjustment to protocol. Conclusion: Key findings from the qualitative interviews included: fostering parental confidence and education; adaptability and flexibility in care; and clinician reassurance throughout the process. Participants suggested these factors would contribute to greater adherence to care protocols and improved outcomes for both infants and their families. This research emphasizes the importance of providing care that extends beyond exercise logistics, and instead, recommends a mindful, family-centred approach that empowers and motivates caregivers throughout the process.
Keywords:
tongue-tie
; ankyloglossia
; infants
; exercises
; pre- and post-operative care
1. Introduction
Ankyloglossia, or tongue-tie (TT) is a congenital condition of the oral cavity where an unusually short and tight lingual frenulum restricts tongue mobility and function [1]. For infants under twelve months, TT is commonly associated with bottle and breastfeeding difficulties, such as an ineffective latch, nipple pain, mastitis, and poor weight gain due to ineffective sucking and swallowing functions [1]. TT is reported in 7% to 10% of infants, depending on specificity of diagnostic criteria [2,3]. The consensus statement by the Australian Dental Association (ADA) in 2020 proposes a recommended management pathway for TT, including non-surgical management as a first line approach followed by surgical management if non-surgical intervention is unsuccessful [4]. Non-surgical options include positioning and lactation training, feeding therapy, stretching and lingual massage [5,6]. Surgical interventions to improve tongue mobility and function include frenotomy (incision or lasering of the frenulum), frenectomy (removal of the frenulum) or frenuloplasty (complete release of frenulum) [7]. However, the statement currently does not include any recommendations for pre- and post-operative care, nor does it consider the perspectives and needs of relevant stakeholders, who in this case, are the caregivers that will directly implement the exercises.
Anecdotal evidence recognises that pre- and post-operative care supports symptom resolution and may prevent re-attachment of the restrictive tie following surgical intervention [8]. However, there is a significant lack of agreement, consistency, and high-quality evidence regarding the exercises being used in clinical practice [4]. There are currently no universally agreed upon pre- and/or post-operative care protocols consistently adhered to by health professionals working with infants and children with TT. Additionally, there is no evidence regarding caregiver opinions of factors that would support the adherence and successful implementation of pre- and post-operative care. Pre-operative care includes lingual exercises, myofunctional therapy, and lactation or breastfeeding support [9,10,11]. Post-operative care for infants includes the continuation of lingual exercises, wound management (antiseptic, gauze, or analgesics application), follow-up breastfeeding sessions, recommended diet, and oral hygiene care [9,10,11,12,13,14,15,16,17]. Several studies have explored a variety of pre- and post-operative care methods, including the frequency, dosage, and duration of their administration, but many lack control variables and the use of reliable and valid measures to compare the effectiveness of different exercise techniques. This ultimately results in limited high-quality evidence to determine the most appropriate care regime [13].
Research has shown that caregiver involvement in administering pre- and post-operative care is associated with improved functional outcomes following the surgical management of TT [12,13,18]. Therefore, a comprehensive understanding of the perspectives of caregivers regarding the fundamental components that comprise a successful and effective pre- and post-operative care protocol is essential for both clinicians and parents. Quality support can and does relate to optimal clinical outcomes and ultimately restoration of breastfeeding function. Parents are key stakeholders in the implementation of care protocols for their children undergoing surgical management for TT. The current study actively sought feedback from parents and health professionals regarding a pre- and post-surgery protocol for active wound management. The protocols included detailed written instructions (e.g., type, duration, and frequency), accompanied by pictures, video demonstrations, and audio explanations. A brief rationale for each exercise was provided, written in both parent and clinician-friendly language. Exercises were divided into two categories: 1) extra-oral and 2) intra-oral. This evidence-based pre- and post- surgery care protocol is collectively referred to as the exercise protocol (EP). The pre-operative portion was composed of up of eight exercises, including stimulation of the cheeks (intra- and extra-orally), lips, rooting reflex, gums, roof of mouth, sucking reflex, and tongue. The post-operative care portion was made up of six exercises, including stimulation of the cheeks (intra- and extra-orally), lips, gums, roof of mouth, and tongue. The protocol established a frequency of performing each exercise every four to six hours, with each lasting twenty to forty seconds for several repetitions. To address the current gap, the overarching aim of the study was to gather opinions and feedback from caregivers and health professionals regarding the pre- and post-operative exercise protocol for infants with tongue tie.
2. Materials and Methods
Ethical clearance was obtained from the Curtin University Human Research Ethics Committee (HREC2024-0106, Approval Date: March 12, 2024). This study employed a qualitative Participatory Action Research (PAR) approach and used individual semi-structured interviews to explore the feedback and opinions from parents and health professionals regarding the evidence-based pre- and post-operative care protocols. Individual interviews were chosen to generate and facilitate an in-depth exploration of participants’ perspectives, lived experiences, and opinions on the protocol [19]. PAR aims to gather and analyse data to “take action and make a change” and prioritizes experiential knowledge to generate practical information that has value for practice in a collaborative, cyclical process of reflection, action, and change [20]. By involving parents, who directly experience the challenges of implementing aftercare, and health professionals, who guide and oversee these practices, PAR ensured the feedback regarding pre- and post-operative care was relevant, realistic, and responsive to those most affected [21]. By conducting individual semi-structured interviews and employing a PAR approach, this ensured the feedback regarding the protocol was grounded in practical knowledge generated through real-world experiences, increasing the potential for successful future implementation and improving outcomes for parents and health professionals involved in tongue-tie aftercare [21].
2.1. Participants
A total of 13 participants were recruited for the qualitative interviews: five parents from a local tongue-tie community advisory group. Eight clinicians were also recruited and included: one paediatric dentist; one general dentist; two International Board-Certified Lactation Consultants (IBCLCs); and four Speech-Language Pathologists (SLPs). A summary of participant demographics is shown in Table 1 and Table 2. Individual semi-structured virtual interviews were conducted with both groups to gather formative feedback on the EP and clinician-user perspectives.
2.2. Materials
2.3. Procedure
To gather qualitative feedback and insights regarding the EP, 13 individual semi-structured virtual interviews were conducted via videoconference over a two-month period. Prior to data collection, an information sheet was provided to participants and written informed consent was obtained. One week prior to the scheduled interviews, participants were sent an online link to the EP for review. Interview question guides were developed and tailored to the different contexts of parents and health professionals for use within the interviews and provided one week prior. Interviews with five parent participants lasted between 29 and 77 minutes, with an average duration of 51 minutes. Interviews with eight clinician participants lasted between 31 and 65 minutes, with an average duration of 48 minutes.
2.4. Analysis
All virtual interviews were videotaped, and audio was recorded and transcribed [22,23]. Transcripts were cross-checked by the research team and sent to participants for review within one week. Thematic analysis (TA) software (NVivo14) was used to identify, generate and analyse patterns and themes across data collected from the parents and clinicians [25]. Each transcript was independently familiarised and coded by two different researchers to enhance trustworthiness and reliability of interpretation. Final themes were developed and agreed upon via collaborative discussion within the research team, shown in Figure 1. Researchers engaged in frequent cross-checking and debriefing to reduce researcher bias and enhance overall credibility.
3. Results
A range of disciplines were represented within the clinician semi-structured interviews, with the majority being speech pathologists (n = 4), along with several other areas of expertise. The experience of clinicians ranged from 5 to 29 years. A variety of client ages was reported, and all clinicians had experience with delivering pre- and/or post-operative care for infants undergoing tongue-tie surgery. Four main themes and ten subthemes were generated from thematic analysis of the participants’ experiences and opinions of the protocol. These main themes and subthemes are explored in Table 4.

Table 3.
Distribution Locations of Study Infographic and Recruitment Survey QR Code for Health Professionals.
Table 3.
Distribution Locations of Study Infographic and Recruitment Survey QR Code for Health Professionals.
| Event/Platform | Location | Date |
|---|---|---|
| Australian Society for Tethered Oral Tissues (ASTOT) Symposium | Gold Coast, Queensland | March 2024 |
| International Consortium of Oral Ankylofrenula Professionals (ICAP) Conference | Cleveland, Ohio, United States of America | May 2024 |
| Speech Pathology Australia (SPA) Conference | Perth, Western Australia | May 2024 |
| International Consortium of oral Consortium Professionals (ICAP) Active Members Group (186 members) | May 2024 |
Table 4.
Main Themes and Subthemes Identified with Supporting Quotes.
| Main Theme | Subtheme | Supporting Quotes |
|---|---|---|
| Setting Them up for Success: Empowering Parental Confidence and Competence | I Do, We Do, You Do | “Maybe a demonstration would come in handy with handing out hard copies as well. Even just like when you're at the appointment, you're bringing along the caregiver as well, who's going to be doing it. And you can give them that sort of demonstration on baby and show them how it works with their child.” (P1) |
| “I think perhaps it would be a face-to-face conversation with a health professional who can show the exercises on your baby in real time to show how it works and then with some opportunity for the parent to give it a go and practise and then receive feedback from that health professional.” (P3) =’’ | ||
| “I think them really being prepared and seeing how baby responds before, so doing the stretch and seeing the baby's not crying or even if baby does cry, as soon as we pick them up and snuggle and cuddle, they calm down really quickly. That has really helped to reassure them.” (C3) | ||
| “But just to have the physician do them first because you do find that because you're scared you’re going to squeeze too hard, you're scared you’re going to tear their lips open.” (P2) | ||
| Knowledge is Power: Empowered Through Education | “You know, I feel that education is key for this. Like, we have to empower parents to take in all the information, you know, make it as easy for them to understand and then let them make their own decisions.” (C4) | |
| “Knowledge is power, so you’ve got to deliver it in a way that’s not scaring the bejeezus out of them.” (C5) | ||
| “And I think if parents know the reason, then they're more motivated to do it, or perhaps they may feel more accountable.” (P3) | ||
| “And then I think what was really valuable was the specificity. Like you've given a rationale which I think is really important and will help with adherence.” (C8) | ||
| Cool, Calm, and Collected: Starting Regulated | “Also just starting with a regulated baby. So, if the baby is already going crazy and upset, we first have to co-regulate before we would start this. Otherwise, we're setting them up to have that negative association with all of these mouth exercises, which we really don't want to do.” (C6). | |
| “But if you're trying to get the baby's tongue moving in a certain way, the tension can't be there. They have to be in a relaxed state, like a quiet alert state, especially for a young infant.” (C4) | ||
| “Consideration needs to be made around when bub is most comfortable.” (P2) | ||
| “Because an unsettled baby doing exercises and trying to feed is just not good for anybody. I think it's more stressful in that parent child interaction and I really do think that impacts attachment and bonding and just the enjoyment of feeding as well.” (P3) | ||
| Fun Filled Connection | “And I tell parents to be really silly, make silly faces, be happy, give a whole positive experience and only do that at times when the infant is in a state to accept play. Not when they're tired, not when they're hungry.” (C4) | |
| “The more fun oral play we can be doing, even if it's just brief moments, then the more baby’s going to be comfortable with that, and the more mum’s going to see that they're comfortable with that and be comfortable doing it.” (C3) | ||
| “If you can just foster that connection during it... So, I do think that like having that real big hit of like, you know, the love hormones and the cuddles and the cuteness before having to do those exercises... just like lock eyes, skin to skin cuddles. I don't know, anything...playing, laughing, joking, to then move into the exercises and then go back to that connection.” (P5) | ||
| “And with a focus on deregulation - downregulation of that nervous system of both mum and baby, and just encouraging that connection from heart to heart, from mum to bub, just into a real place of harmony. And just helping the mum fall in love with her baby over and over and over.” (C5) | ||
| “It doesn’t matter how much you’ve stretched, it does not matter if you can’t get the brain and the heart and the emotional health and wellbeing of that dyad to a point where they can go baby, we’ve got this. I’ve got you. You’ve got me. We’ve got this sweetheart, I’m with you.” (C5) | ||
| Guidelines Guide, but Flexibility Heals: Individualized and Adaptable | A Balancing Act | “And to talk about how to make it achievable for that specific family and to fit it into their day, rather than it being like “Here it is. Go and do it.” I think a discussion of “How does your family work? How can we build this into your routine as much as possible? How can we set you up to succeed?” It's definitely not straightforward. It's not a one-size fits all approach for everyone.” (P3) |
| “I think spending some time with the parents trying to figure out what's the best time for them to do the stretches helps them to work it into their routine.” (C3) | ||
| “And I give different options because I don't think there's a one-size-fits-all. It depends on the day, and time of the day. Depends on what's going on in that...in the world of that family.” (C4) | ||
| “And then just on the bad days like prioritising which exercise is vital...Like, which one do you start with? Because if your baby really, really cracks it or something's really bad or there's been a family emergency and you've just got to get one done, which is it? What one are we prioritising?” (P5) | ||
| Never Wake a Sleeping Baby: Respecting Sleep Needs and Protocol Flexibility | “I think the sleep part is really important. If you can note down to make that part parent friendly, like if you can let them sleep if they are sleeping for seven hours...Yeah, counterintuitive as a parent after you've just rocked them to sleep for three hours. I guess like knowing about that would be good. That would definitely be a part of a good protocol I think” (P5) | |
| “I think that that instruction should be in there like, you know, try to do this at a point where you don't have to wake your baby up to do it, you know, try and get...try not to make this something that's disruptive to your sleep” (C4) | ||
| “I also wonder if there needs to be a little bit of flexibility in that tool allowing parents the flexibility in saying, you know, sometimes particularly overnight, you're not going to wake up before your baby is showing hunger cues to do the exercises and then feed them.” (P3) | ||
| Nurturing the Nurturer: Supporting the Caregiver | Fear of Failure and Damaging Parent-Child Bond | “Most parents will take things very literally, so if they don't do it every four to six hours, some parents may be like “I've ruined it. I failed. I'm doing my child a disservice.” […] and knowing you're not going to ruin your baby if you miss one of these rounds of exercises.” (P3) |
| “And if you miss one, you do, you feel like you're the worst parent ever and that you've ruined everything. And now we've ruined everything and we're going to go back to square one. So maybe just some wording around that.” (P5) | ||
| “If you’re told black and white, this is exactly what you have to do, and you don’t do it, you feel like a failure constantly.” (P1) | ||
| “I think they're...my main nurturing tips that it's OK, or even a video after the hand washing, with a little message from a mum [...] saying “It's OK. You only have like, 24 more to go. You're going to get through this, it's going to be OK. Your baby's not going to hate you,” because that's genuinely what you think [...]” (P5) | ||
| The Mother Load: “It’s just too much” | “A lot of it has to do with especially maternal anxiety. If I’ve got a mother that is highly anxious and her baby’s crying it triggers her anxiety. She’s less likely to adhere to a stretching post care protocol.” (C5) | |
| “I had a partner. I wasn't on my own and I didn't have other children, so he was my first child, so it was literally like literally like me and him 24/7 so I could focus all my attention. I wasn't working or anything like that. And coming from me, I still feel like maybe it is a lot.” (P1) | ||
| “I think there will be families that are going to read it and go “Far out. That's a lot.” You know, every four to six hours.” (P2) | ||
| “Because after doing the exercises, you almost want to run away and have a shower, hand the baby off to somebody and remove the trauma from you because you know you have to do it in six hours' time again. It sounds really dramatic, but that is how it feels when you're in the thick of it.” (P5) | ||
| “You’re Doing Great”: Empowering Parents through Reassurance in Navigating Challenges and Adjustments | Access to Ongoing Guidance: Checking in and Following Up | “And then also I allow them access to me, which I know not every provider would necessarily want, but I tell them “You're not going to bother me. Please message me photos if you want feedback, please video a stretch if you want feedback. [...] if I can respond, I will, and I really do want to see that.” I think that's been helpful, just the reassurance for them.” (C6) |
| “So yeah, after that sort of time. Even maybe day three, day four sort of thing to say. Look, just checking in, making sure everyone's going OK. Any questions? Anything you've noticed those sorts of things at that point, I think people would really appreciate that too.” (P1) | ||
| “Follow up would be good. It's not about that authoritative sort of focus. It's more “do you need further support? Is there anything we can help you with if you're having trouble getting them done? Is there anything that can be done to help you get them done?” Things might change for the family, so it's really important that they know that they do have that support there and that it's OK to ask for that help.” (P2) | ||
| Boosting Spirits Through Emotional Encouragement | “Comes down to like that whole reassurance that you don't have to complete every exercise, every single time, every minute of every day, like taking that pressure off to make sure that people are aware of that. That's really the main point.” (P1) | |
| “And just again, reassurance around yes, it looks it might look like it's a lot, but once you're actually doing it, you'll get into a rhythm. You'll get used to it. We don't expect you to be doing this day one straight away.” (P2) | ||
| “So, a reminder, I remind them that that's it's not forever. You don't have to do this for, you know for more than the four weeks recommend when it comes to the stretches.” (C2) | ||
| “It's just reassuring, connection, support. I think it all goes back to that, yeah.” (P5) |
3.1. Theme 1: Setting Them Up for Success - Parental Confidence and Competence
Key subthemes identified by participants underscored the importance of fostering caregiver confidence and competence in successfully implementing the EP. This was achieved through a combination of practical education from clinicians, hands-on guidance, and fostering a supportive, regulated environment for both the parent and infant. Caregivers emphasised the value of direct, face-to-face instruction from healthcare professionals, which allowed them to observe, practice, and receive immediate feedback on their technique, thereby alleviating anxiety, and enhancing their perceived ability to carry out the exercises independently and confidently. Educating parents about the purpose and significance of the exercises—along with the potential risks of non-adherence—supported parents to understand their significance, empowering them to feel more “accountable” and “motivated.” The emotional state of both caregiver and infant was also highlighted as a crucial factor in successful protocol implementation. Starting exercises when both the caregiver and infant were “regulated” —a state in which both individuals are emotionally balanced, physiologically calm, and able to engage in interactions without signs of distress—was seen as essential for reducing stress and preventing negative associations with the exercises. Strategies such as co-regulation—where both parent and child are in a state of “harmony”—along with creating a positive, playful environment, helped strengthen the parent-child bond and fostered a sense of connection within the dyad. This supportive, nurturing atmosphere not only promoted emotional well-being but also increased caregiver comfort and confidence, thereby enhancing their competence in following the protocol effectively.
3.2. Theme 2: Guidelines Guide, but Flexibility Heals - Individualised and Adaptable
Further central themes identified by participants was the importance of tailoring post-operative exercise protocols to the individual needs and circumstances of each family. Many participants emphasised that a rigid, one-size-fits-all approach was often ineffective and instead highlighted the need for flexibility in the protocol and implementation process. Adapting the protocol to accommodate family dynamics, including the parents' age, capacity, and daily routines, was seen as crucial for ensuring adherence. Some suggested the inclusion of "priority exercises" for days when full protocol completion is not feasible, with one clinician emphasising that “it’s better to do something, even if you can’t do everything.” The need for flexibility was also noted with respect to sleep patterns. Both parents and clinicians advocated for the preservation of the infant's sleep by avoiding unnecessary sleep disruptions to complete exercises, due to this feeling “counterintuitive” after “rocking them to sleep for three hours.” Acknowledging the emotional and psychological strain on caregivers, particularly mothers, was also deemed crucial in protocol flexibility and adaptability. Many parents expressed feelings of guilt or failure when unable to adhere strictly to the protocol, underscoring the need for reassurance and supportive communication from clinicians to mitigate additional stress. Participants agreed that fostering a compassionate, adaptable approach to the protocol would not only ease the emotional burden on caregivers but also increase the likelihood of successful long-term adherence.
3.3. Theme 3: Nurturing the Nurturer - Supporting the Caregiver
A prominent theme that emerged was the significant emotional and psychological burden that post-operative exercises place on caregivers, particularly mothers. It was highlighted that many parents interpret exercise instructions literally, leading to feelings of “failure” and “guilt” when unable to adhere to the prescribed exercises. Missing a session, even for legitimate reasons, often triggered significant stress, with parents expressing concerns that they had "failed" or "ruined everything" in terms of their infant’s wound healing. This sense of failure was compounded by a fear that the child might develop negative associations with the caregiver, associating them with pain or discomfort during the exercises, jeopardising the parent-child bond. Caregivers suggested that incorporating words of encouragement and reassurance from other parents into the protocol could alleviate these feelings and support their emotional well-being. Validation of their efforts, even when they were unable to fully comply with the protocol, was seen as crucial for managing emotional strain and preventing feelings of inadequacy. Many parents, particularly first-time mothers or those with limited external support, described the post-operative exercise regimen as “overwhelming” and emotionally draining. Several parents emphasised that administering post-operative exercises often effectuates significant emotional distress, particularly surrounding the fear that their child may develop negative emotional responses toward them or associate them with pain. Additionally, several parents likened the experience to a cycle of “trauma”, where the emotional strain of administering the exercises led to stress and anxiety, making it difficult to maintain adherence. They suggested reassurance could mitigate these feelings, through supportive communication both within the EP and directly from providers. Participants stressed the importance of acknowledging the psychological burden caregivers face within the protocol and incorporating flexibility or supportive strategies to reduce the emotional strain. This recognition would help caregivers feel understood and supported, ultimately facilitating higher levels of adherence to the prescribed exercises and improving both the caregiver's and child's well-being.
3.4. Theme 4: You’re Doing Great - Empowering Parents Through Reassurance in Navigating Challenges and Adjustments
The critical role of ongoing guidance, emotional support, and reassurance in empowering parents to successfully navigate the challenges of post-operative care also emerged as core theme. Both parents and clinicians emphasised the importance of regular follow-up and check-ins, providing parents with opportunities to ask questions, clarify uncertainties, and receive feedback on aspects such as stretching positions, infant comfort, and pain management. This continuous support was seen as essential for validating parents' efforts, boosting their confidence, and reinforcing their ability to implement the exercises effectively. These check-ins also offered a safe space for parents to voice concerns, overcome "whitecoat syndrome," and receive encouragement from clinicians, all of which contributed to a positive and supportive care experience. In addition to logistical guidance, emotional encouragement was also identified as a key factor in sustaining motivation and adherence. Participants noted that while the exercise regimen may feel overwhelming initially, regular reassurance that a routine would eventually develop helped reduce anxiety. Emphasising the temporary nature of the post-operative care plan, with the message that "it's not forever," was highlighted as an effective strategy to alleviate stress and maintain motivation. Clinicians also emphasised the importance of focusing on effort rather than perfection, which helped reduce apprehension and supported parents in feeling more confident and competent in conducting the exercises.
4. Discussion
The current study solicited feedback regarding an evidence based pre- and post-operative care exercise protocol for infants who underwent tongue tie surgery. Thematic analysis identified four themes that addressed different facets of caregiver holistic wellness related to successful implementation of the exercise protocol. There is currently no literature that addresses the priorities and opinions regarding supports for adherence and successful implementation of a care protocol from the perspective of caregivers and health professionals. Holistic factors driving treatment success and adherence were explored and quality of care defined from caregivers and clinicians perspectives. With a scarce evidence-base, existing pre- and post-operative exercise protocols need to consider emerging research, ethical considerations, and stakeholder’s perspectives. This study addressed the gap by presenting qualitative feedback centred on empowerment and motivation of caregivers, and highlighted that in addition to the exercise types, frequency, and dosage, a holistic and family-centred approach must be considered to ensure overall success and adherence to pre- and post-operative management.
Empowering and motivating caregivers in the context of an infant treatment EP requires fortitude within a clinician and caregiver relationship. Our findings advocate for ongoing clinician guidance, access, emotional encouragement and recognition of an individualised approach as key facilitators in caregiver adherence. These findings corroborate similar studies within infant neonatal literature, concluding that a sense of ‘family with the staff’ and empathy from clinicians contributed to greater therapeutic success and caregiver wellbeing outcomes [26,27,28,29]. Additionally, the emotional capacity of the clinician should be respected. Clinician burnout and compassion fatigue are excessively evident within modern medical literature but lacking application to the TT context [30,31].
Participants defined ‘setting up for success’ by placing value on in-person, face-to-face education and in-depth demonstrations from their providers. These recommendations align with the perspectives of parents and nurses in neonatal and surgical literature, that upskilled caregivers reduce dependency on clinicians. Proficiency instils caregiver autonomy and self-confidence when providing home care for their infants. This is suggested to facilitate positive overall health outcomes and recovery for the infant [32,33]. Based on our findings, fostering a meaningful experience centred on caregiver autonomy empowers parents to confidently provide care for their child, rather than experiencing feelings of inadequacy or hesitation [26].
The findings also suggested it was counterproductive to focus solely on reducing infant tension without first addressing caregiver anxiety. Acknowledged within TT literature, heightened caregiver stress and anxiety is rooted in a lack of education and uncertainty towards the surgical procedure [34,35]. Subsequently, this study found these emotions stemmed from fear and guilt when implementing post-operative care on their child. Similarly studies in the infant mental health literature show fear of jeopardising the parent-infant bond overwhelmingly dictates caregiver adherence within treatment protocols [36,37]. Participants commented on embedding a routine of play, fun, and skin-on-skin contact within the required post-operative practices, additionally supporting the neonatal evidence-base [38,39]. Taken together, this study and the current literature advocate for caregiver empowerment, restoring control and harmony within the parent-infant dyad to prevent negative associations.
Additional to clinician support, parents expressed a desire for peer encouragement, particularly mother-to-mother and parent-to-parent support, emphasising the value of shared experiences. Emerging literature supports the concept of peer mentoring and lived experience roles within caregiver mental health practices [40]. Adopting this within the context of protocol implementation for TT suggests that validation from those who have faced similar challenges would mitigate feelings of isolation and anxiety. Considering this, recent literature is placing higher regard for a family-centred care model within an infant health population, calling for ‘individualisation’ over ‘standardisation’ [26]. Participants disclaimed that with the challenges inflicted by parenthood, it is unlikely and unrealistic that a protocol would be adhered to flawlessly. This is similarly implied within nursing literature, which states standardised protocols cannot successfully address all aspects of patient-centred care [41]. The argument for flexibility stems from caregivers calling for a ‘low demand’ exercise regime which prioritises infant sleep routines. Infant sleep literature shows that sleep disturbances leads to increased symptoms of anxiety, depression, and fatigue among new parents, thereby can impact their capacity and adherence to a treatment protocol [42]. These findings collectively argue that standardisation, while ideal, should serve as a foundation with a degree of flexibility based on clinical judgement and specific patient needs; negotiating a balance between ‘caregiver wants’ and ‘protocol needs. This is asserted to be integral in supporting a family-centred approach for TT management.
The current study highlighted that focusing solely on the exercises provided is a simplistic view, and rather clinicians must consider other factors such as the capacity of caregivers, providing education and upskilling, and providing ongoing support and reassurance. There is an emphasis on the necessity for standardised pre- and post-operative care protocols by clinicians and the TT literature. However, the finding from the current study underscore the importance of adopting a family-centred, needs-oriented approach to TT pre- and post-operative care. Therefore, these two frameworks are not mutually exclusive but can and should be integrated to complement one another effectively. The voices of both caregivers and clinicians are important in TT management, and this study allowed clinicians with various years of experience to share their experiences and insights.
This study was limited to the inclusion of a relatively small sample size of 13 parents and clinicians, representing the views of clinicians from Australia, Canada, and America. Caregiver participants were all mothers and Australian, and hence did not represent lived experiences from the perspectives of fathers nor caregivers in other countries. Additionally, the time taken by families and clinicians to comprehensively review each modality of the protocol varied among participants. The protocol was typically sent to participants one week prior to the scheduled interview, however, for some this was not possible due to re-scheduling the interview at an earlier than expected date. Some participants had also not independently reviewed the protocol prior to their interview and hence were required to review in real time. This could have impacted the amount and specificity of feedback provided and could have resulted in variability in the depth of understanding of the pre- and post-operative exercise protocol content. During interviews, occasional leading and closed-ended questions were evident, which may have led participants in a pre-conceived direction unknowingly, reducing the reliability of data collection.
Future research should focus on developing tools to identify and characterise caregiver needs and wants necessary to facilitate successful implementation of the EP to efficiently, and optimally setup a triad framework whereby the clinician, the infant, and the caregivers can support each other on all levels to optimise and realise wellness outcomes for all parties.
Key Implications for Clinical Practice
- Holistic, Family-Centred Care. Emphasising the well-being of the both the infant and caregiver throughout the treatment journey, from diagnosis to aftercare.
- Interdisciplinary Collaboration. Highlighting the necessity of coordinated care between healthcare providers in pre-and post-operative exercises.
- Consistency Across Providers. Unified treatment philosophies and consistent messaging across healthcare providers to enhance caregiver confidence and pre- and post-operative care adherence.
- Tailored Aftercare Strategies. Provision of enhanced and tailored support, including focus on parent’s emotional wellness, stress management and practical guidance for pre- and post-operative exercises.
- Flexible but Standardised Protocols. To balance the pre-and post-operative care protocols with consideration for wellness and recovery, to optimise outcomes for infant, mother and family.
5. Conclusions
This study sought to contribute to the profession’s knowledge base by gathering feedback on an evidence-based protocol from a community advisory group of caregivers and current practicing healthcare professionals. The research highlighted the importance of empowering and building caregiver capacity through education, ongoing clinician support, and peer encouragement, which collectively increase confidence and autonomy. The findings outline that a family-centred approach is vital for successful implementation, advocating for individualisation over strict standardisation. This aligns with contemporary literature that emphasises the value of adapting care to meet the unique needs of families- specifically both the patient and the caregivers. The present study acknowledges the need for broader representation to capture varying perspectives internationally, hence a sample from individual countries may be beneficial to delineate varying perspectives. Nevertheless, our study contributes valuable insights into the caregiver experience and highlights areas for future research. The study recommends a pilot evaluation of the proposed care protocol, using standardised outcome measures to assess its effectiveness. Overall, the study concludes by calling for a paradigm shift in clinical practices regarding TT management, one which seeks to prioritise holistic, family-centred care to enhance caregiver confidence and capacity to support treatment adherences.
Data Availability Statement
The data sets generated and analyzed during the current study are not publicly available due to ethics only being provided for this study.
Acknowledgments
We would like to thank the infant participants, caregivers and health professionals who participated in this project. We would also like to extend special thanks to Ella Beadle and Megan van der Linde for their valued contributions to the study.
Informed Consent Statement
Written informed consent has been obtained from the patient's parent to publish this paper.
Originality and Verification
This submission is original research. We confirm that this research has been presented but not published elsewhere.
References
- Hatami A, Dreyer CW, Meade MJ, Kaur S. Effectiveness of tongue-tie assessment tools in diagnosing and fulfilling lingual frenectomy criteria: a systematic review. Aust Dent J. 2022;67(3):212-9. [CrossRef]
- Unger C, Chetwynd E, Costello R. Ankyloglossia identification, diagnosis, and frenotomy: a qualitative study of community referral pathways. J Human Lact. 2020;36(3):519-27. [CrossRef]
- O’Connor ME, Gilliland AM, LeFort Y. Complications and misdiagnoses associated with infant frenotomy: results of a healthcare professional survey. Int Breastfeed J. 2022;17(1):1-9. [CrossRef]
- Australian Dental Association. Ankyloglossia and Oral Frena Consensus Statement. 2020. https://ada.org.au/unauthorized-access.
- Walsh J, Tunkel D. Diagnosis and treatment of ankyloglossia in newborns and infants: a review. JAMA Otolaryngol Head Neck Surg. 2017;143(10):1032-9. [CrossRef]
- Akbari D, Bogaardt H, Lau T, Docking K. Ankyloglossia in Australia: Practices of health professionals. Int J Pediatr Otorhinolaryngol. 2023;171:111649. [CrossRef]
- Shekher R, Lin L, Zhang R, Hoppe IC, Taylor JA, Bartlett SP, et al. How to treat a tongue-tie: an evidence-based algorithm of care. Plast Reconstr Surg Glob Open. 2021;9(1). [CrossRef]
- Messner AH, Lalakea ML. Ankyloglossia: controversies in management. Int J Pediatr Otorhinolaryngol. 2000;54(2-3):123-31. [CrossRef]
- Ferrés-Amat E, Pastor-Vera T, Rodriguez-Alessi P, Mareque-Bueno J, Ferrés-Padró E. The prevalence of ankyloglossia in 302 newborns with breastfeeding problems and sucking difficulties in Barcelona: a descriptive study. Eur J Paediatr Dent. 2017;18(4):319-25. [CrossRef]
- Ferrés-Amat E, Pastor-Vera T, Ferrés-Amat E, Mareque-Bueno J, Prats-Armengol J, Ferrés-Padró E. Multidisciplinary management of ankyloglossia in childhood. Treatment of 101 cases. A protocol. Med Oral Patol Oral Cir Bucal. 2016;21(1):e39. [CrossRef]
- Ferrés-Amat E, Pastor-Vera T, Rodríguez-Alessi P, Ferrés-Amat E, Mareque-Bueno J, Ferrés-Padró E. Management of ankyloglossia and breastfeeding difficulties in the newborn: breastfeeding sessions, myofunctional therapy, and frenotomy. Case Rep Pediatr. 2016;2016. [CrossRef]
- Baxter R, Hughes L. Speech and feeding improvements in children after posterior tongue-tie release: a case series. Int J Clin Pediatr. 2018;7(3):29-35. [CrossRef]
- Bhandarkar KP, Dar T, Karia L, Upadhyaya M. Post Frenotomy Massage for Ankyloglossia in Infants—Does It Improve Breastfeeding and Reduce Recurrence? Matern Child Health J. 2022;26(8):1727-31. [CrossRef]
- Garrocho-Rangel A, Herrera-Badillo D, Pérez-Alfaro I, Fierro-Serna V, Pozos-Guillén A. Treatment of ankyloglossia with dental laser in paediatric patients: Scoping review and a case report. Eur J Paediatr Dent. 2019;20(2):155-63. [CrossRef]
- Ghaheri BA, Cole M, Fausel SC, Chuop M, Mace JC. Breastfeeding improvement following tongue-tie and lip-tie release: A prospective cohort study. Laryngoscope. 2017;127(5):1217-23. [CrossRef]
- Jaikaria A, Pahuja SK, Thakur S, Negi P. Treatment of partial ankyloglossia using Hazelbaker Assessment Tool for Lingual Frenulum Function (HATLFF): A case report with 6-month follow-up. Natl J Maxillofac Surg. 2021;12(2):280. [CrossRef]
- Jaikumar S, Srinivasan L, Babu SK, Gandhimadhi D, Margabandhu M, et al. Laser-assisted frenectomy followed by post-operative tongue exercises in ankyloglossia: a report of two cases. Cureus. 2022;14(3). [CrossRef]
- Harun NA, Rashidi NAM, Teni NFM, Ardini YD, Jamani NA. Mothers' Perceptions and Experiences on Tongue-tie and Frenotomy: A Qualitative Study. Malay J Med Health Sci. 2022;18(2). [CrossRef]
- Dunwoodie K, Macaulay L, Newman A. Qualitative interviewing in the field of work and organisational psychology: Benefits, challenges and guidelines for researchers and reviewers. Appl Psychol. 2023;72(2):863-89. [CrossRef]
- De Oliveira B. Participatory action research as a research approach: Advantages, limitations and criticisms. Qual Res J. 2023;23(3):287-97. [CrossRef]
- Cornish F, Breton N, Moreno-Tabarez U, Delgado J, Rua M, de-Graft Aikins A, et al. Participatory action research. Nat Rev Methods Primers. 2023;3(1):34. [CrossRef]
- Microsoft Corporation. Microsoft Teams [Internet]. 2024. Available from: https://www.office.com/.
- Microsoft Corporation. Microsoft Streams [Internet]. 2024. Available from: https://www.office.com/.
- Microsoft Corporation. Microsoft Word [Internet]. 2024. Available from: https://www.office.com/.
- Nvivo14 [Internet]. 2024. Available from: https://lumivero.com/product/nvivo/.
- Schütz Hämmerli N, Stoffel L, Schmitt K-U, Khan J, Humpl T, Nelle M, et al. Enhancing parents’ well-being after preterm birth—A qualitative evaluation of the “transition to home” model of care. Int J Environ Res Public Health. 2022;19(7):4309. [CrossRef]
- Russell G, Sawyer A, Rabe H, Abbott J, Gyte G, Duley L, et al. Parents’ views on care of their very premature babies in neonatal intensive care units: a qualitative study. BMC Pediatr. 2014;14:1-10. [CrossRef]
- Fernández-Medina IM, Granero-Molina J, Hernández-Padilla JM, Jimenez-Lasserrotte MdM, Ruiz-Fernández MD, Fernández-Sola C. Socio-family support for parents of technology-dependent extremely preterm infants after hospital discharge. J Child Health Care. 2022;26(1):42-55. [CrossRef]
- Bry A, Wigert H. Psychosocial support for parents of extremely preterm infants in neonatal intensive care: a qualitative interview study. BMC Psychol. 2019;7(1):76. [CrossRef]
- Bhutani J, Bhutani S, Balhara YPS, Kalra S. Compassion fatigue and burnout amongst clinicians: a medical exploratory study. Indian J Psychol Med. 2012;34(4):332-7. [CrossRef]
- Weintraub A, Geithner E, Stroustrup A, Waldman E. Compassion fatigue, burnout and compassion satisfaction in neonatologists in the US. J Perinatol. 2016;36(11):1021-6. [CrossRef]
- Chan SH, Shorey S. Effectiveness of psychosocial interventions on the psychological outcomes of parents with preterm infants: A systematic review and meta-analysis. J Pediatr Nurs. 2024;74:23-34. [CrossRef]
- Staveski SL, Parveen V, Madathil SB, Kools S, Franck LS. Parent education discharge instruction program for care of children at home after cardiac surgery in Southern India. Cardiol Young. 2016;26(6):1213-20. [CrossRef]
- Lee P. Pre and post procedure parent education to reduce anxiety related to tongue-tie [dissertation]. Grand Canyon University; 2018.
- Ray S, Hairston TK, Giorgi M, Links AR, Boss EF, Walsh J. Speaking in tongues: what parents really think about tongue-tie surgery for their infants. Clin Pediatr. 2020;59(3):236-44. [CrossRef]
- David Vainberg L, Vardi A, Jacoby R. The experiences of parents of children undergoing surgery for congenital heart defects: A holistic model of care. Front Psychol. 2019;10:2666. [CrossRef]
- Wang L-L, Ma J-J, Meng H-H, Zhou J. Mothers’ experiences of neonatal intensive care: A systematic review and implications for clinical practice. World J Clin Cases. 2021;9(24):7062. [CrossRef]
- The Sydney Children’s Hospitals Network. Developmentally supportive care for newborn infants: Practical guideline. 2022. Contract No.: 2006-0027.
- Warre R, O’Brien K, Lee SK. Parents as the primary caregivers for their infant in the NICU: benefits and challenges. Neoreviews. 2014;15(11):e472-e7. [CrossRef]
- Castles C, Stewart V, Slattery M, Bradshaw N, Roennfeldt H. Supervision of the mental health lived experience workforce in Australia: A scoping review. Int J Ment Health Nurs. 2023;32(6):1654-71. [CrossRef]
- Rycroft-Malone J, Fontenla M, Seers K, Bick D. Protocol-based care: The standardisation of decision-making? J Clin Nurs. 2009;18(10):1490-500. [CrossRef]
- Ball, H. L., Taylor, C. E., Thomas, V., Douglas, P. S., & the SBY, w. g. (2020). Development and evaluation of ‘Sleep, baby & You’—An approach to supporting parental well-being and responsive infant caregiving. PLoS One, 15(8). [CrossRef]
Figure 1.
Example of Coding Tree for Theme Development.
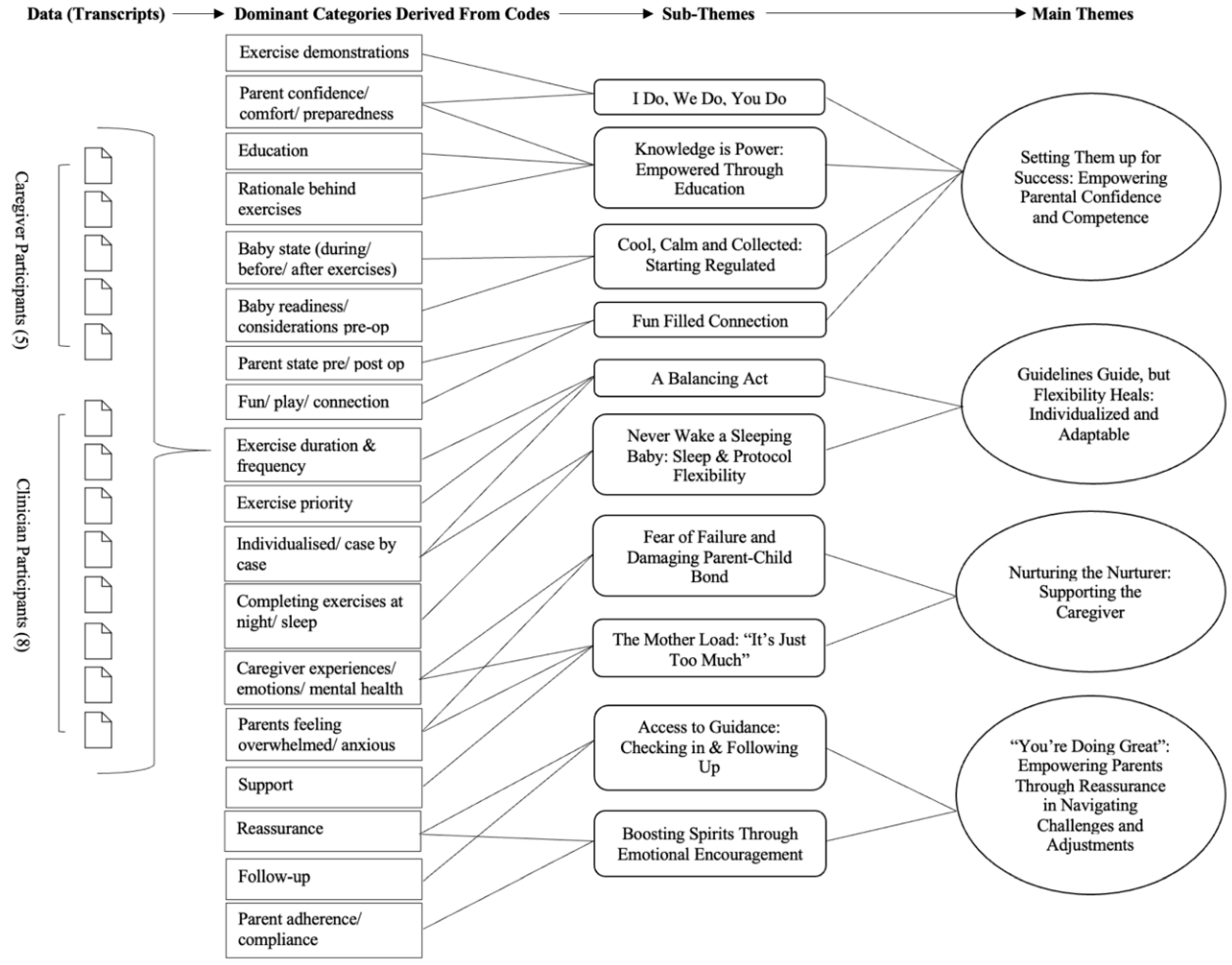
Figure 2.
Example of Draft Pre- and Post-Operative Care Protocol Exercise Page.
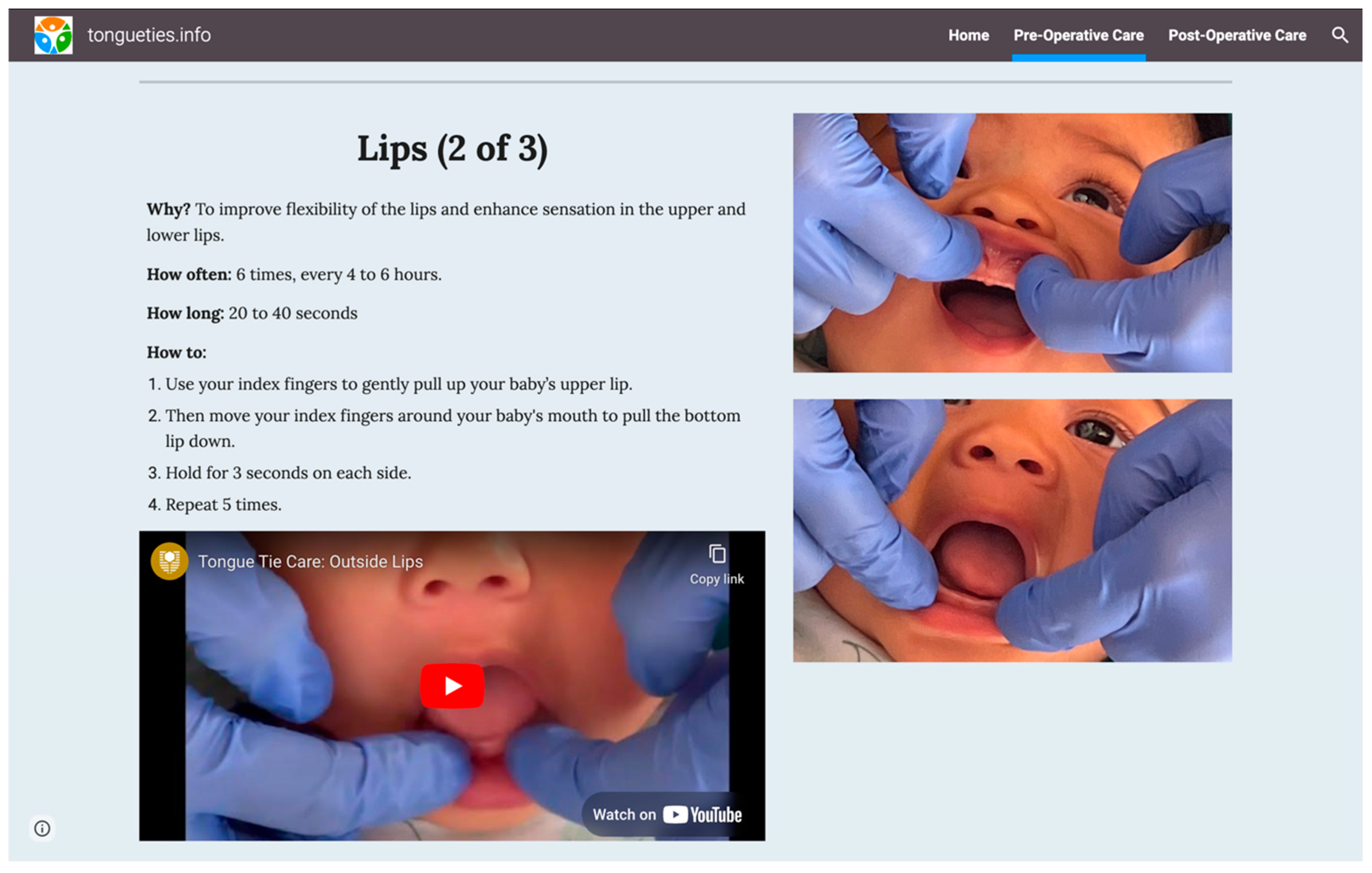
Table 1.
Demographics of Clinician Participants.
| Participant | Healthcare Background/Discipline | Years of Experience | Client Age Range | Pre-op/Post-op Exercises |
|---|---|---|---|---|
| C1 | Paediatric Dentist | 16 | 2 weeks – 14 years | Yes |
| C2 | Dentist | 28 | All ages | Yes |
| C3 | Speech-Language Pathologist/ Certified Orofacial Myologist/ Certified IBCLC | 20 | All ages | Yes |
| C4 | RN/ Midwife/ IBCLC | 20 | All ages | Yes |
| C5 | Osteopath | 20 | Infants | Yes |
| C6 | Speech-Language Pathologist/ Certified Orofacial Myologist | 12 | All ages | Yes |
| C7 | Speech-Language Pathologist /OMT | 29 | All ages | Yes |
| C8 | Speech-Language Pathologist /OMT | 5 | 3+ years | Yes |
Note: OMT – Oral Myofunctional Therapist, RN – Registered Nurse, IBCLC – International Board-Certified Lactation Consultant.
Table 2.
Demographics of Caregiver Participants.
| Participant | Healthcare Background | Age of Child’s Tongue-Tie Diagnosis | Age at Time of Procedure | Procedure Type | Pre-/Post-Operative Exercises |
|---|---|---|---|---|---|
| P1 | Medical Administration Role | Shortly after birth | 4 months old | Laser (Paediatric Dentist) | None provided. |
| P2 | Carer Peer Worker in Hospital | At birth | 10 years old | Supposedly cut during tonsillectomy | None provided. |
| P3 | Speech Pathologist (early intervention & paediatric feeding) | Child 1: 2 weeks old Child 2: 2 days old |
Child 1: 4-5 weeks old Child 2: 1 week old |
Child 1: Scissors, then laser (following unsuccessful initial surgery) Child 2: Laser |
Child 1: None provided. Child 2: ‘Vague’ post-op provided (every 4-6 hours, unclear instructions for how long). |
| P4 | Speech Pathologist | Child 1: 11 months Child 2: At birth. |
Child 1: 18 months Child 2: 4 weeks |
Child 1: Laser (ENT) Child 2: Laser (Dentist) |
Child 1: SP suggested functional exercises (e.g., funny faces, licking lips, licking ice-cream etc.) Child 2: Pre- and post-op exercises were provided (as part of feeding programme/structured programme on app). |
| P5 | Various Medical Administration Roles, Phlebotomist. | 2 weeks old | Surgery 1: 4 weeks old Surgery 2: 5 months old |
Surgery 1: Scissors Surgery 2: Laser |
Surgery 1: None provided. Surgery 2: Only post provided (sweeps & stretches, every 6hrs for 2 weeks) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



