Submitted:
14 January 2025
Posted:
15 January 2025
You are already at the latest version
Abstract
Background: Nurses' clinical reasoning is increasingly recognized as a core competency that enhances the quality and safety of care across various healthcare con-texts. Nurses with refined clinical reasoning skills significantly contribute to improving patient health outcomes and achieving broader health gains. In emergency services, this competency is essential for nurses to assess complex problems rapidly, anticipate com-plications, and prevent the deterioration of patients' conditions. This expertise enables them to discern the severity of clinical situations within a short timeframe and intervene effectively. Objectives: To analyze the clinical reasoning process of nurses; to develop a theory to explain the clinical reasoning process in emergency. Methods: This qualitative study explores the research question: "How is the clinical reasoning process of nurses working in emergency services developed?" The methodology used was grounded theory, with theoreti-cal sampling including 20 expert nurses. Data collection methods included in-depth in-terviews, participant observation, and field notes. Results: The theoretical analysis identi-fied Clinical Reasoning as a substantive theory, comprising two subprocesses: Diagnostic Evaluation and Nursing Therapeutic Intervention. A nurses' clinical reasoning deter-mines two levels of patient severity: Level I: Life-threatening situations (Risk of Life) and Level II: Non-immediate life-threatening situations (Expressed Problems). Interventions are tailored to the identified severity levels. Conclusions: The Nursing Clinical Reasoning Model is a dynamic and continuous process involving diagnostic evaluation and thera-peutic intervention. It is deeply embedded in the relationship between nurse, patient, and family, within a specific context of care. The care context influences the nurse's evaluation, intervention, and the patient's behaviour.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Design
2.3. Rigor and Reflexivity
2.4. Theoretical Framework
2.5. Participants
2.6. Sampling
2.7. Data Collection Techniques
- ▪
- In-Depth Interviews
- ▪
- Participant Observation
- I)
- General observation of clinical reasoning among nurses: This involved observing multiple nurses simultaneously in a specific sector of the emergency department. Interactions between nurses and patients were recorded, focusing on clinical reasoning processes. The researcher accompanied different nurses during their shifts, taking notes on these interventions.
- II)
- Individualized observation of a single participant: At specific moments and in defined contexts, the researcher observed one nurse interacting with a patient during care delivery. The goal was to document the nurse’s actions and the reasoning behind decisions, such as the questions asked, the use of technology for assessments, and consultation of medical records or patient charts.
- ▪
- Field Notes and Memos
2.8. Data analysis
- Identifying Indicators and Grouping into Concepts, indicators were sought in the data and coded, forming clusters around recurring patterns. These were refined into concepts and later into subcategories. Each subcategory was consistently cross-checked with the original data to ensure a solid connection to participants’ experiences.
- Iterative Coding and Question Development, the team continued line-by-line coding until identifying codes that warranted deeper exploration. These codes informed questions that guided further data construction and analysis.
- Collaborative Analysis, researchers debated the coding and analysis to enhance the richness and comprehensiveness of the findings. Emerging concepts and subcategories shaped additional data collection and theoretical sampling.
- Conceptualization and Saturation, data were analyzed early and refined throughout subsequent stages, leading to concepts and subcategories. Properties were identified in the data until the concepts were verified and saturated. Subcategories grouped indicators under a central idea, representing the underlying pattern until no new properties emerged, achieving theoretical saturation.
- Defining and Verifying Relationships, as data emerged, relationships between subcategories were defined, verified, and explained, along with variations within and between them. This process elevated the data to a conceptual level.
- Role of Memos, memo writing played a critical role, aiding in conceptualizing data and developing properties for each category. These properties provided operational definitions, ensuring that the data were conceptually dense and capable of explaining the identified patterns. Once no new properties emerged, saturation was reached, resulting in a comprehensive and detailed explanation of the identified patterns.
2.9. Ethical Considerations
3. Results
3.1. Sociodemographic Characteristics
3.2. Clinical Reasoning as a Central Concept
3.2.1. Nurses’ Clinical Reasoning Process
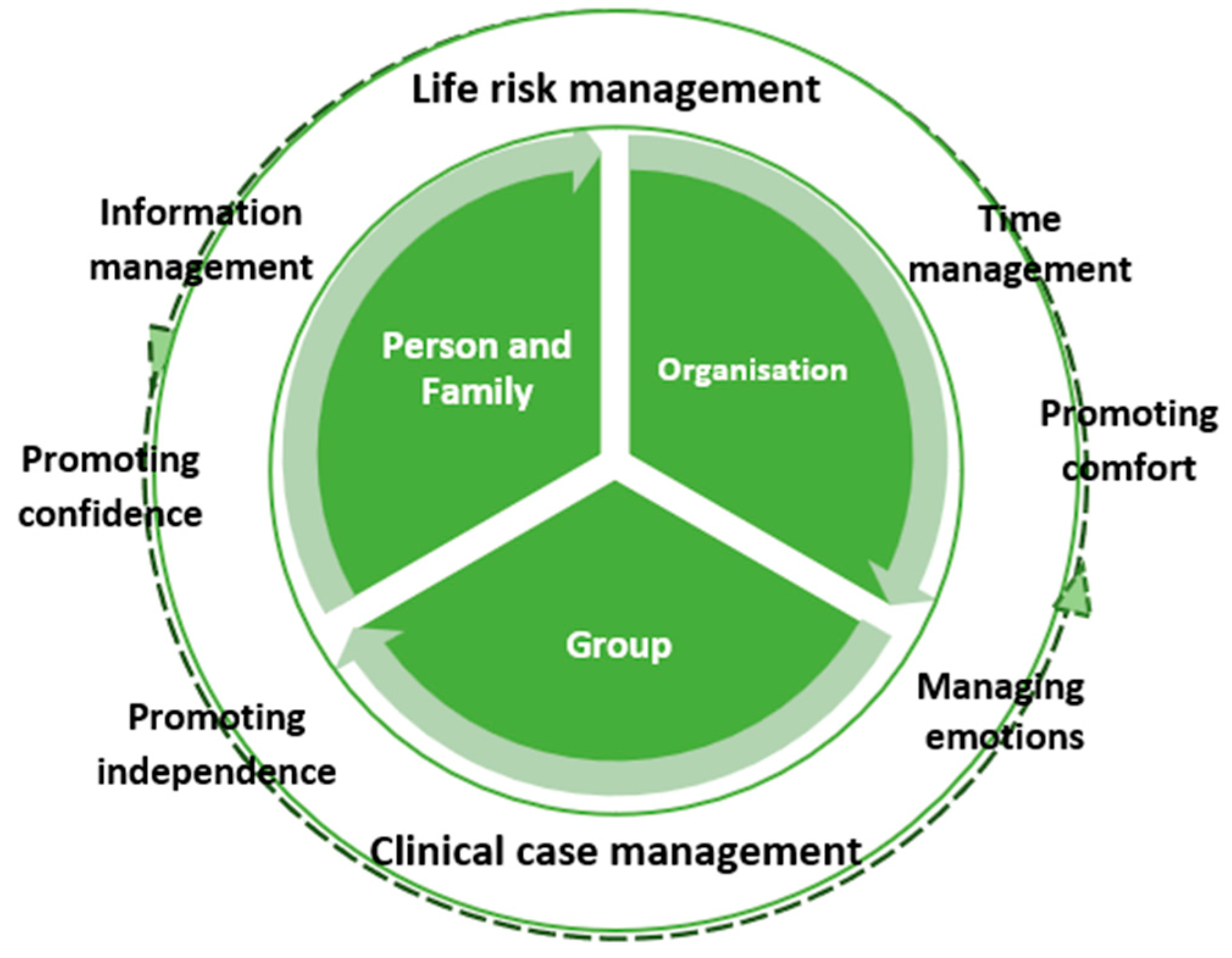
- Management of Life Risk: Nurses closely monitor respiratory, cardiac, and neurological functions, establishing priorities based on the level of risk. Continuous assessment allows for immediate intervention when the patient’s life is in danger.
- Time Management: Nurses must predict and anticipate problems, adjusting the timing to meet the patient’s needs. This skill is crucial for the effectiveness of the intervention.
- Information Management: Informing the patient and family about the care provided, procedures, and addressing questions is a fundamental part of the intervention. Transparent communication helps engage the patient and family in the care process.
- Promotion of Comfort and Trust: Creating an environment that promotes comfort and trust is essential in emergency care nursing. This includes symptom management, ensuring privacy, and the presence of family. Nurses also provide comfort in other ways, such as blankets, adjusting lighting, and controlling noise. Additionally, fostering trust is vital by showing a genuine interest in the patient and their family.
- Management of Emotions: Understanding the emotions expressed by the patient is crucial, especially in health crises. Nurses help patients rationalize their emotions, thereby reducing suffering and enabling them to adapt to the new reality.
- Promotion of Autonomy: This concept centers on the patient’s autonomy in the clinical decision-making process, directly related to their health literacy and their ability to recognize the limits of their own decisions. Nurses focus on promoting autonomy in the emergency service, aiming to equip patients to actively participate in the health-illness process by providing tools and information necessary for making informed decisions about their health. By integrating health literacy with the patient’s decision-making ability, nurses aim to maximize their independence, both within the emergency service and for discharge or potential hospitalization, ensuring the patient is as prepared as possible to manage their health autonomously.
3.3. Nature of Nursing Therapeutic Intervention
3.4. Clinical Reasoning Process of Nurses
4. Discussion
- Diagnostic Assessment Process: This enables the nurse to perform a quick initial analysis to determine whether there is a life-threatening risk or not. This initial assessment is crucial as it defines the priority and urgency of the intervention. To carry out this assessment, the nurse collects data, evaluating signs and symptoms, the patient’s general health status, history, and other relevant information [6,12]. The nurse systematically carries out continuous re-evaluation to monitor the evolution of the patient’s condition, adjusting their assessment and intervention accordingly. This is a dynamic feature of clinical reasoning, requiring flexibility and adaptation to rapid changes in the clinical condition, as the emergency department deals with patients facing highly complex and unpredictable clinical situations.
- Nursing Therapeutic Intervention Process: This corresponds to the nurse’s actions based on their assessment and re-evaluation. In the emergency department, the nurse provides an active and immediate response based on the prior diagnostic assessment. This process is focused on managing the immediate life risk and ensuring adequate and humane care for the patient. After identifying problems such as respiratory, cardiac, or neurological complications, the therapeutic intervention focuses on quick and precise actions to stabilize the patient. In the emergency department, where every second counts, nurses constantly face high-pressure situations, requiring excellent time management to prioritize critical interventions to save lives. However, Nursing Therapeutic Intervention Process is not only about treating acute clinical conditions [34,35]. Communication and information are also essential parts of the process [36]. Nurses need to provide information to the patient and their family about ongoing procedures, the patient’s status, and the next steps to be taken. This not only facilitates the patient’s autonomy in care but also promotes trust and safety in an environment often marked by fear and uncertainty. In this sense, nurses play an important role in managing the patient’s and family’s emotions, helping them cope with the emotional impact of a health emergency. Thus, Nursing Therapeutic Intervention Process goes beyond the application of techniques and procedures; it is a complex and comprehensive process that involves technical management, time, communication, comfort, and emotions, ensuring the patient receives the best possible care, both physically and emotionally, in an emergency context.
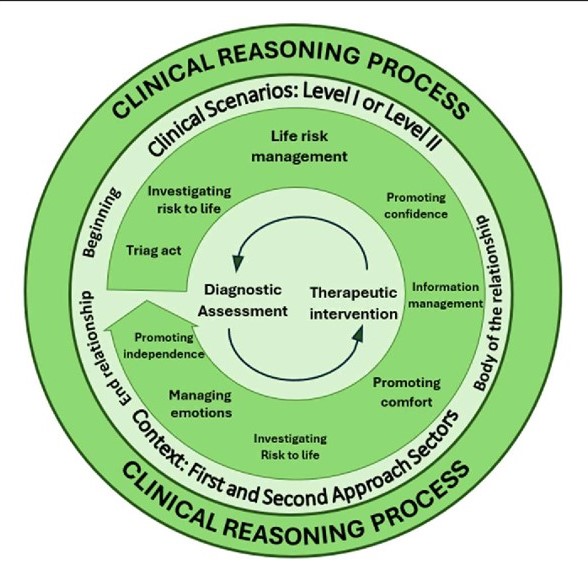
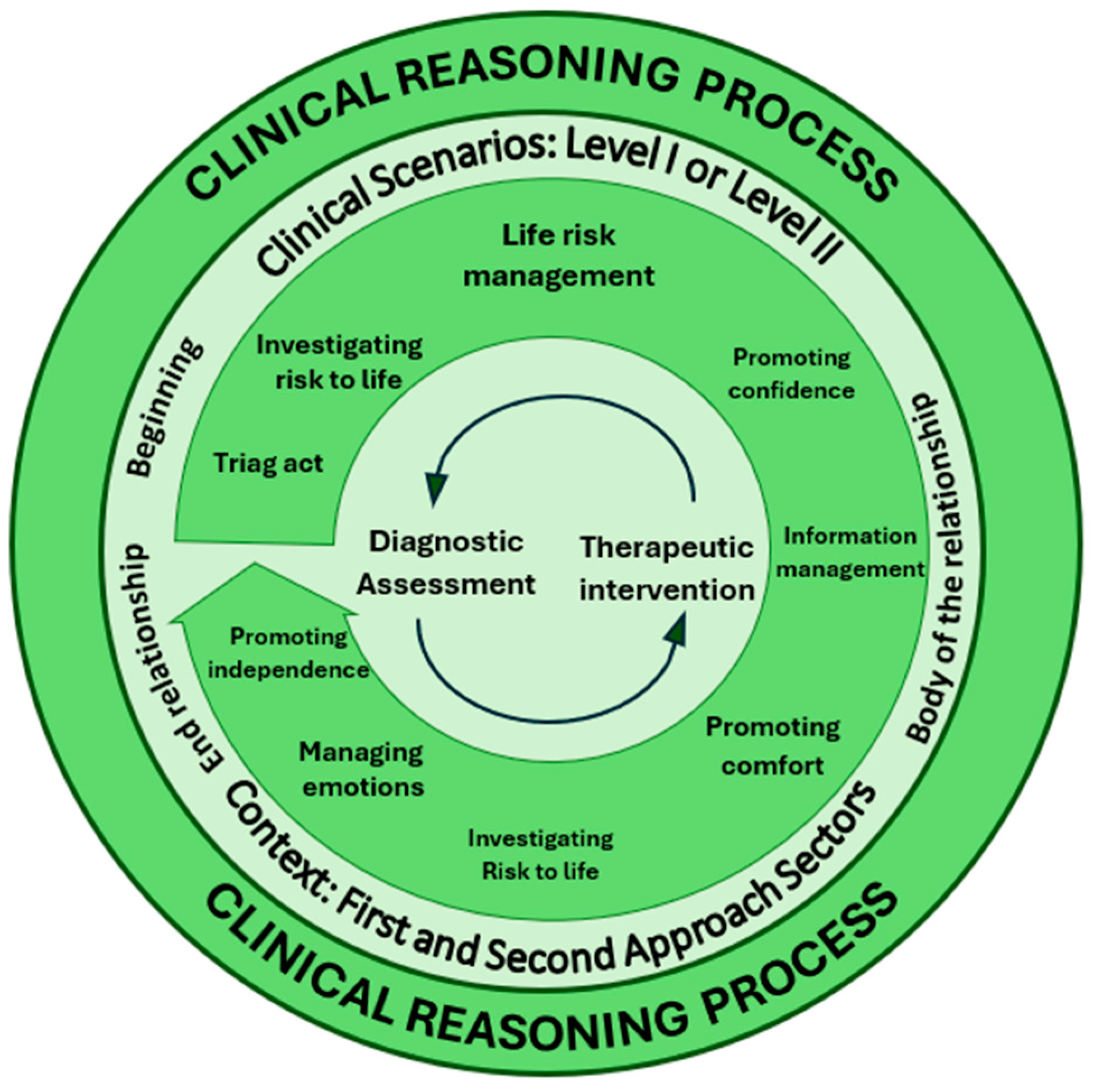
- Duality of the Clinical Reasoning Process, the process consists of two main components: Diagnostic Evaluation and Therapeutic Intervention. These are operationalized through various elements in clinical practice: in evaluation, the nurse focuses on identifying whether there is a life risk or detecting problems expressed by the patient; in intervention, the nurse’s actions are centered on managing life risk, providing information to the patient and family, promoting comfort, and managing emotions. These elements ensure person-centred care tailored to the patient’s clinical condition. The circular arrows at the center of the diagram symbolize the continuous, dynamic interplay between the two processes. This connection resembles the functioning of the human brain, where the: left hemisphere, often linked to logic and analysis, corresponds to data collection and interpretation during diagnostic evaluation and right hemisphere, associated with creativity and intuition, is responsible for organizing actions and fostering active reflection during therapeutic interventions.
- Therapeutic Relationship as the Context of Clinical Reasoning, the Clinical reasoning does not occur in isolation but within the therapeutic relationship between nurse, patient, and family. This relationship unfolds in three phases: 1. Beginning of the relationship, where the nurse collects initial data upon first contact; 2. Body of the relationship, during which the nurse deepens the assessment and actively intervenes; 3. End of the relationship, marking the conclusion of direct intervention, often involving information delivery or patient referral. This ongoing interaction ensures the process is not only technical but also relational, addressing the emotional and psychological needs of both patient and family [34,35,36].
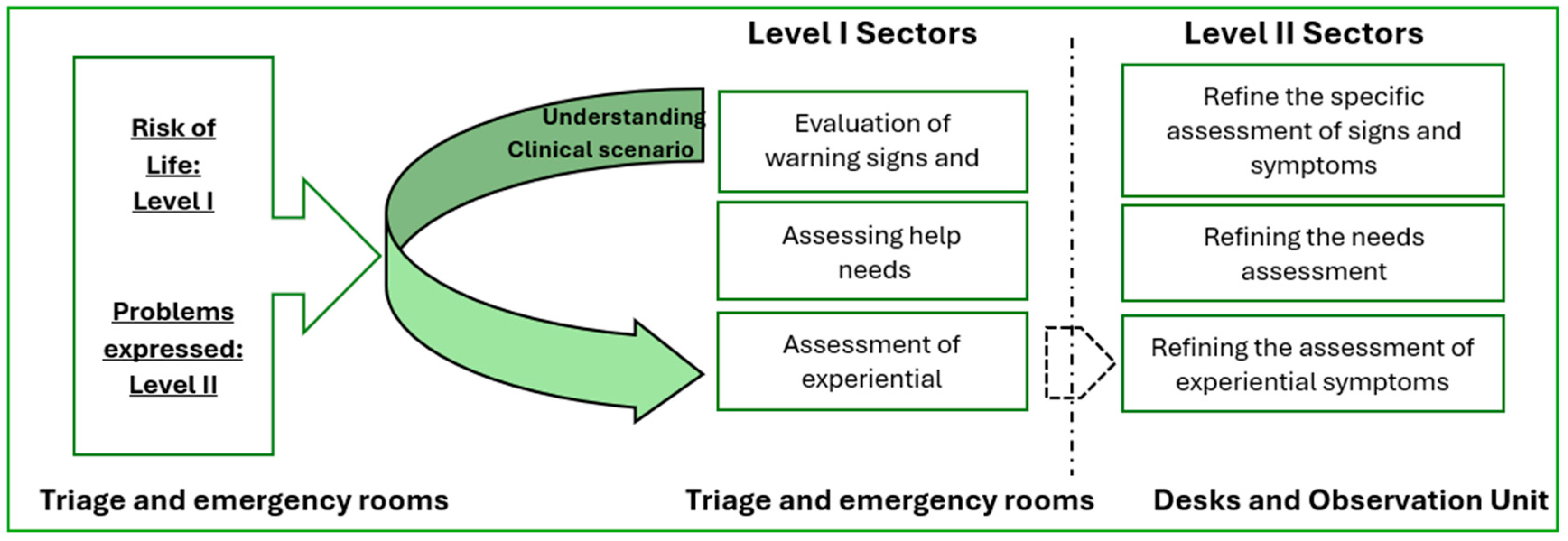
- Scenarios for the Clinical Reasoning, this process occurs for two key scenarios: Level I – Life Risk, where the primary focus is on evaluating and intervening in critical life-threatening situations; Level II – Patient-Expressed Problems, where the intervention focuses on symptoms or issues raised by the patient, which, while not immediately life-threatening, require attention to prevent complications. These scenarios guide nurses in prioritizing and directing their actions in emergency environments.
- Emergency Department Sectors, the Clinical reasoning is influenced by the physical and functional context in which it unfolds. Emergency department sectors can be divided into: First-Approach Sectors, such as triage and emergency rooms, where nurses perform rapid, initial evaluations to determine the severity of the situation; and Second-Approach Sectors, such as observation rooms and desks, where nurses deepen diagnostic evaluations and adjust interventions more precisely as additional patient data becomes available.
Limitations of This Study
Implications for the Profession and Patients
- Continuous Training Programs: Develop programs that enhance nurses’ clinical reasoning skills and competencies, especially in complex settings.
- Nursing Education Curricula: Enrich nursing curricula with strategies and methodologies that strenGrounded Theoryhen clinical reasoning from the early stages of education.
- Clinical Practices Improvement: Equip nursing professionals to respond more effectively to critical patient needs, ensuring timely interventions and reducing health complications.
- This research underscores the significance of investing in nurse capacity-building to improve care quality, directly benefiting the safety and well-being of patients in high-demand clinical settings.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Acknowledgments
Conflicts of Interest
Abbreviations
| CE | Ethics Committee |
| GT | Grounded Theory |
References
- El Hussein MT, Olfert M, Hakkola J. Clinical judgment conceptualization scoping review protocol. Teaching and Learning in Nursing. 2022;17(1):84-101. [CrossRef]
- Koufidis C, Manninen K, Nieminen J, Wohlin M, Silén C. Grounding judgement in context: A conceptual learning model of clinical reasoning. Medical Education. 2020;54(11):1019-1028. [CrossRef]
- McHugh C, Way J. What is Reasoning? Mind. 2018;127(505):167-196. [CrossRef]
- Abu Arra AY, Ayed A, Toqan D, et al. The factors influencing nurses’ clinical decision-making in emergency department. INQUIRY: The Journal of Health Care Organization, Provision, and Financing. 2023;60. [CrossRef]
- Bijani M, Abedi S, Karimi S, et al. Major challenges and barriers in clinical decision-making as perceived by emergency medical services personnel: A qualitative content analysis. BMC Emerg Med. 2021;21:11. [CrossRef]
- Alfaro-LeFevre R. Applying nursing process: A tool for critical thinking. 9ª ed. Lippincott Williams & Wilkins; 2019.
- Benner P. From novice to expert: Excellence and power in clinical nursing practice. Addison-Wesley; 1984.
- Benner P, Tanner C, Chesla C. Expertise in nursing practice: Caring, clinical judgment, and ethics. Journal of Nursing Education. 2009;45(6):204-211.
- Mendonça S, Lima Basto M, Ramos A. Estratégias de raciocínio clínico dos enfermeiros que cuidam de clientes em situação clínica: revisão sistemática da literatura. RIASE. 2016;2(3):753-773. [CrossRef]
- Simmons B. Clinical reasoning: concept analysis. J Adv Nurs. 2010;66(5):1151-1158. [CrossRef]
- Thompson C, Aitken L, Doran D, Dowding D. An agenda for clinical decision making and judgement in nursing research and education. International Journal of Nursing Studies. 2013;50(12):1720-1726. [CrossRef]
- Tanner CA. Thinking like a nurse: A research-based model of clinical judgment in nursing. Journal of Nursing Education. 2006;45(6):204-211. [CrossRef]
- Hall LM, Prescott PA. The nurse-patient relationship: A review of the literature and implications for clinical decision-making. J Clin Nurs. 2009;18(13):1803-1812. [CrossRef]
- Luo QQ, Petrini MA. A review of clinical reasoning in nursing education: based on high-fidelity teaching method. Front Nurs. 2018;3:175-183. [CrossRef]
- Levett-Jones T. Clinical Reasoning: Learning to Think like a Nurse. Frenchs Forest: Pearson; 2013.
- Teixeira CRS, Pereira MCA, Kusumota L, et al. Evaluation of nursing students about learning with clinical simulation. Revista Brasileira de Enfermagem. 2015;68(2):284-291, 311-319. [CrossRef]
- Tanner CA. Clinical judgment and evidence-based practice: Toward pedagogies of integration. Journal of Nursing Education. 2008;47(8):335-336. [CrossRef]
- Del Bueno D. A crisis in critical thinking. Nursing Education Perspectives. 2005;26(5):278-282.
- Eisenhauer LA, Hurley AC, Dolan N. Nurses’ reported thinking during medication administration. Journal of Nursing Scholarship. 2007;39(1):82-87. [CrossRef]
- Fero LJ, Witsberger CM, Wesmiller SW, Zullo TG, Hoffman LA. Critical thinking ability of new graduate and experienced nurses. Journal of Advanced Nursing. 2009;65(1):139-148. [CrossRef]
- Koharchik L, Caputi L, Robb M, Culleiton AL. Fostering clinical reasoning in nursing students. American Journal of Nursing. 2015;115(1):58-61. [CrossRef]
- Woods A, Doan-Johnson S. Executive summary: Toward a taxonomy of nursing practice errors. Nursing Management. 2002;33(10):45-48. [CrossRef]
- Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Implications of nurse staffing and patient outcomes: Review and research. Nursing Research. 2016;65(5):123-134.
- Borzo SR, Cheraghi F, Khatibian M, et al. Clinical reasoning skill of nurses working in teaching medical centers in dealing with practical scenarios of King’s model concepts. BMC Med Educ. 2024;24:280. [CrossRef]
- Bae J, Lee J, Choi M, et al. Development of the clinical reasoning competency scale for nurses. BMC Nurs. 2023;22:138. [CrossRef]
- New South Wales (NSW). Health Incident Management Guidelines. NSW Ministry of Health; 2008.
- Charmaz K, Thornberg R. The pursuit of quality in grounded theory. Qualitative Research in Psychology. 2021;18(3):305-327. [CrossRef]
- Glaser BG. Theoretical sensitivity. Sociology Press; 1978.
- Queirós J. The knowledge of expert nurses and the practical-reflective rationality. Investigación y Educación en Enfermería. 2015;33(1):83-91. [CrossRef]
- Rubin HJ, Rubin IS. Qualitative interviewing: The art of hearing data. 3rd ed. Sage Publications; 2011.
- Patton MQ. Qualitative research and evaluation methods. 4th ed. Sage Publications; 2015.
- Streubert HJ, Carpenter DR. Qualitative Research in Nursing: Advancing the Humanistic Imperative. 5th ed. Lippincott Williams & Wilkins; 2011.
- Dilley P. Interviews and the philosophy of qualitative research. The Journal of Higher Education. 2004;75(1):127-132. [CrossRef]
- Lopes M. A Relação Enfermeiro-Doente como intervenção terapêutica. Formasau formação e Saúde, lda; 2006.
- Sapeta P. Cuidar em Fim de Vida. O Processo de Interacção Enfermeiro-Doente. Edição Lusociência; 2011.
- Phaneuf M. Comunicação, entrevista, relação de ajuda e validação. Loures: Lusociência; 2005.
- Schön DA. The Reflective Practitioner: How Professionals Think in Action. New York: Basic Books; 1983.
- O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: A synthesis of recommendations. Acad Med. 2014;89(9):1245-1251. [CrossRef]

| Number of participants | 20 |
|---|---|
| Age | M=36,8 years; DP=5,72 |
| Gender | 11 females 9 males |
| Average years of experience | M=14,9 anos; DP=5,37 |
| Average years of experience in emergency | M=11,3; DP=5.46 |
| Level of education | 10 BN 10 MN |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



