Submitted:
13 January 2025
Posted:
15 January 2025
You are already at the latest version
Abstract
Background: Dental radiography has undergone a profound transformation, evolving from rudimentary techniques with high radiation exposure and limited clarity to advanced digital modalities prioritizing diagnostic precision and patient safety. Innovations such as digital imaging, three-dimensional visualization, and artificial intelligence (AI) have revolutionized diagnostics, enabling faster, more accurate imaging with significantly reduced radiation doses. Understanding these advancements is crucial for enhancing patient care and minimizing occupational risks for dental professionals. Main Body: This comprehensive review traces the historical development of dental radiography, highlighting key milestones from the first dental X-rays to the advent of digital sensors and cone-beam computed tomography (CBCT). It examines recent technological advancements, including the shift to digital radiography, which has improved image quality and eliminated the need for chemical processing. The integration of AI is explored, emphasizing its role in autonomously detecting dental anomalies, streamlining diagnostic workflows, and facilitating early intervention.A critical analysis compares radiation exposure levels between traditional and modern imaging techniques, underscoring the importance of minimizing exposure through technological innovations and adherence to the ALARA (As Low As Reasonably Achievable) principle. The biological effects of ionizing radiation on tissues, cells, and DNA are discussed, highlighting the necessity for rigorous safety measures.Protective strategies for patients and dental professionals are detailed, including the use of lead aprons, thyroid collars, and proper shielding techniques. The review emphasizes implementing radiation safety protocols in dental practices to mitigate occupational risks. Emerging trends such as portable X-ray units have expanded access to imaging services, benefiting geriatric and homebound patients. Additionally, the integration of automation and robotics, along with the development of novel materials for radiation attenuation, points toward a future of safer, more efficient dental radiography. Conclusion: The evolution of dental radiography reflects a dynamic interplay between technological innovation and a steadfast commitment to safety. Advancements in imaging technology and radiation protection measures have significantly enhanced diagnostic capabilities while reducing radiation risks. The ongoing integration of AI and cutting-edge technologies heralds a new era in dental care, promising improved diagnostic accuracy, streamlined workflows, and better safeguarding of both patients and practitioners.
Keywords:
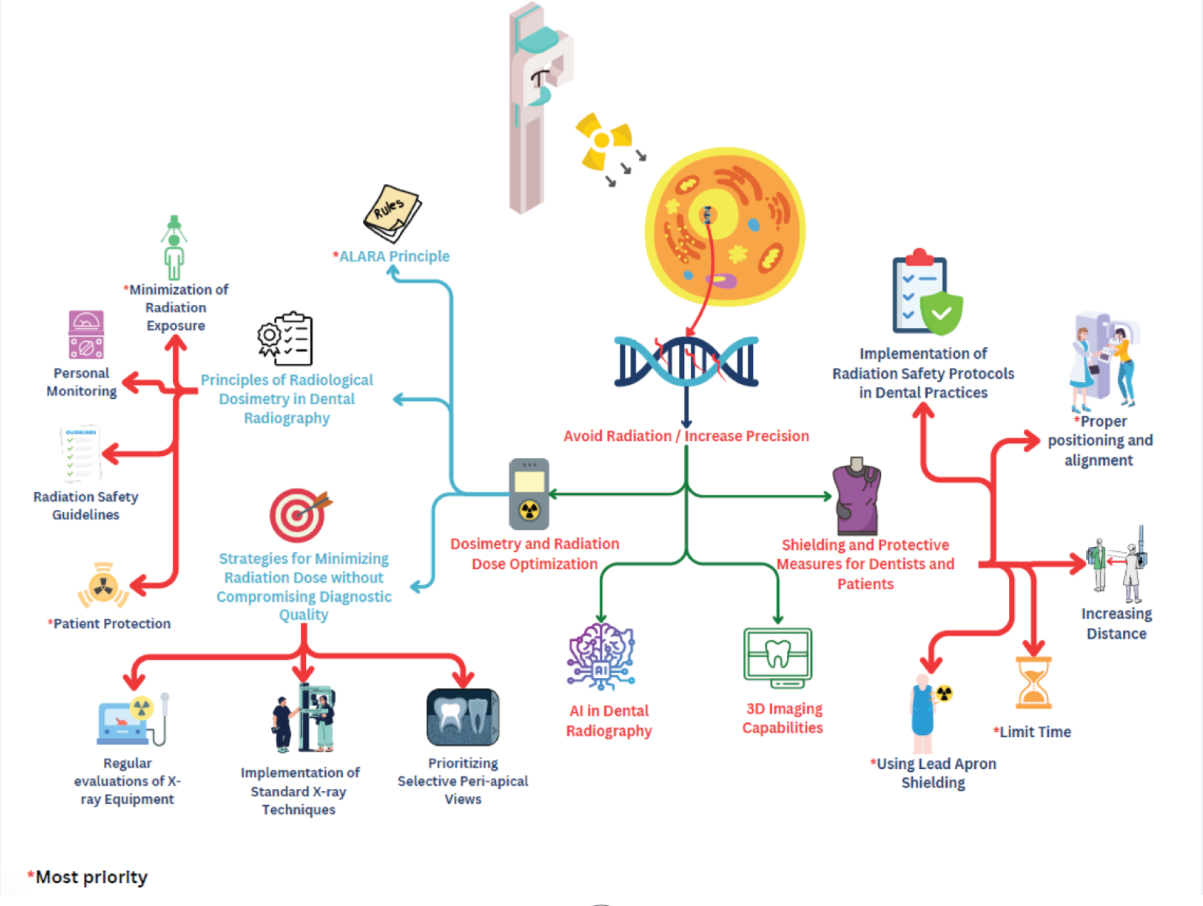
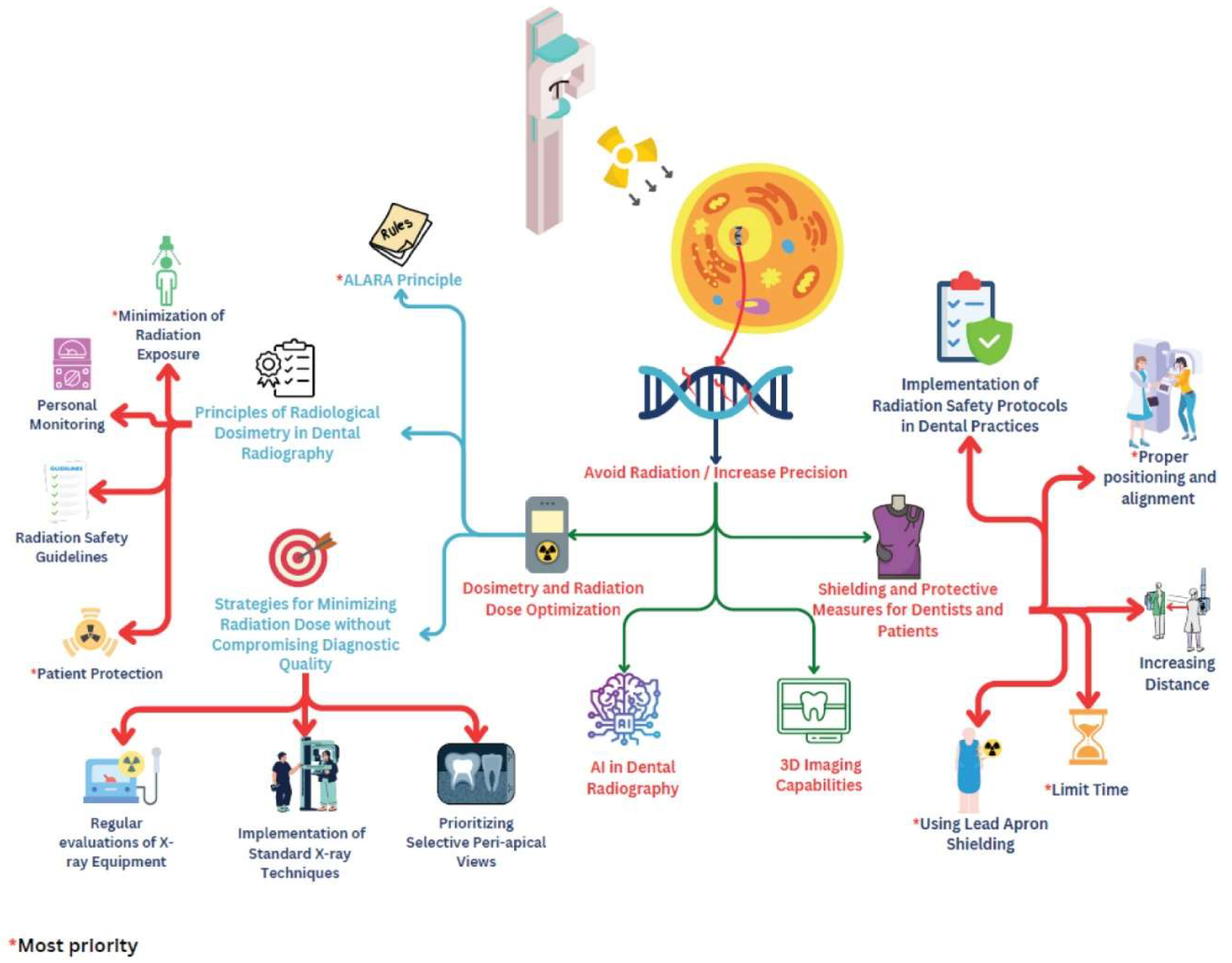
Graphical Abstract
Clinical Relevance
Background
Dental X-ray Techniques and Technologies

Recent Technological Advancements in Dental X-Ray Equipment
Comparative Analysis of Radiation Exposure Levels
Radiation Risks and Safety Measures
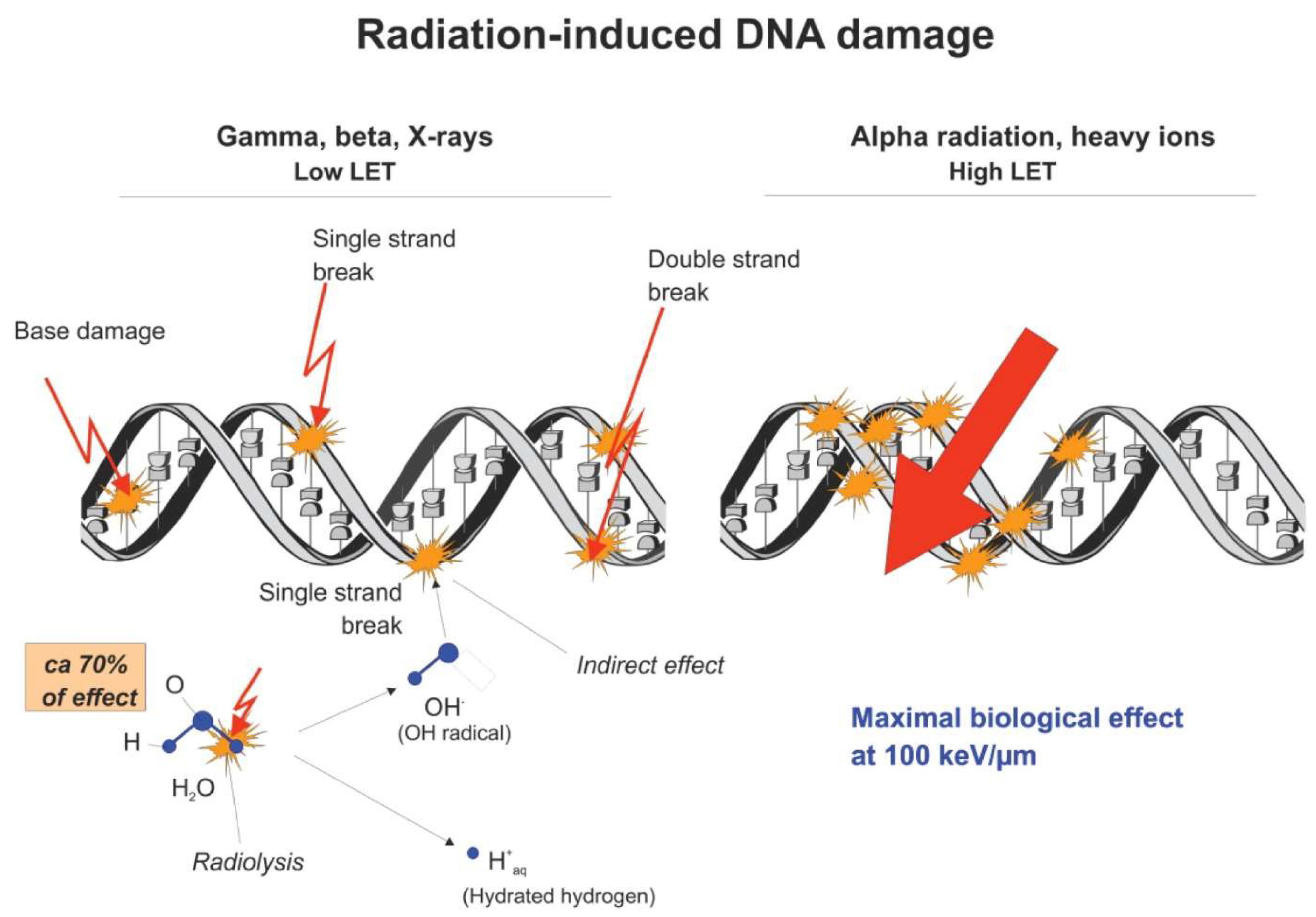
Ionizing Radiation and Biological Effects
3. Factors influencing the severity of biological effects
Dosimetry and Radiation Dose Optimization
Shielding and Protective Measures for Dentists and Patients
Dentist Occupation Risk
Chronic Radiation Exposure and Health Implications
- Intraoral dental X-ray imaging procedure: 1–8 microsievers (μSv)
- Panoramic examinations: 4–30 μSv
- Cephalometric examinations: 2–3 μSv
- CBCT procedures (median values from the literature): 50 μSv or less for small- or medium-sized scanning volumes and 100 μSv for large volumes.
Risk Mitigation Strategies for Dental Professionals
Emerging Trends in Dentist Radiation Protection
Conclusion
Statements and Declrations
Consent for publication
Data Availability Statement
Funding Statement
Conflict of Interest Disclosure
Ethics Approval and Consent to Participate
Patient Consent Statement
Permission to Reproduce Material from Other Sources
Clinical Trial Registration
Author Contributions
Acknowledgments
Declaration Regarding the Use of AI-Assisted Readability Enhancement
References
- Pauwels, R. History of dental radiography: Evolution of 2D and 3D imaging modalities. Med Phys Int, 2020, 8, 235–77. [Google Scholar]
- Sunilkumar, A.P.; Parida, B.K.; You, W. Recent Advances in Dental Panoramic X-ray Synthesis and its Clinical Applications. IEEE Access 2024, 1. [Google Scholar] [CrossRef]
- Anil, S.; Porwal, P.; Porwal, A. Transforming Dental Caries Diagnosis Through Artificial Intelligence-Based Techniques. Cureus 2023, 15, e41694. [Google Scholar] [CrossRef]
- Ludovici, G.M.; Cascone, M.G.; Huber, T.; et al. Cytogenetic biodosimetry techniques in the detection of dicentric chromosomes induced by ionizing radiation: A review. Eur. Phys. J. Plus 2021, 136, 482. [Google Scholar] [CrossRef]
- Radiation effects on cells & DNA | Let’s talk science (2020). Available at: https://letstalkscience.ca/educational-resources/backgrounders/radiation-effects-on-cells-dna.
- Dental radiographs. (2011). The Journal of the American Dental Association, 142, 1101. [CrossRef]
- Visbal, J.H.W.; Pedraza, M.C.C.; Khoury, H.J. Protección Radiológica en Radiología Dental. CES Odontología 2021, 34, 52–67. [Google Scholar] [CrossRef]
- More, C.V.; Alsayed, Z.; Badawi, M.S.; Thabet, A.A.; Pawar, P.P. Polymeric composite materials for radiation shielding: a review. Environmental Chemistry Letters 2021, 19, 2057–2090. [Google Scholar] [CrossRef]
- Hagi, F.S. The History of Dental Radiology: A Review. History 2023, 141. [Google Scholar]
- Gunderman, R. (2016). On the 120th anniversary of the X-ray, a look at how it changed our view of the world. The Conversation. https://theconversation.com/on-the-120th-anniversary-of-the-x-ray-a-look-at-how-it-changed-our-view-of-the-world-50154.
- Molteni, R. The way we were (and how we got here): fifty years of technology changes in dental and maxillofacial radiology. Dentomaxillofacial Radiology 2020, 20200133. [Google Scholar] [CrossRef]
- Molteni, R. The way we were (and how we got here): fifty years of technology changes in dental and maxillofacial radiology. Dentomaxillofacial Radiology 2020, 20200133. [Google Scholar] [CrossRef]
- Martins, M.V.; Baptista, L.; Luís, H.; Assunção, V.; Araújo, M.; Realinho, V. Machine Learning in X-ray diagnosis for Oral Health: A Review of Recent progress. Computation 2023, 11, 115. [Google Scholar] [CrossRef]
- Zhu, J.; Chen, Z.; Zhao, J.; Yu, Y.; Li, X.; Shi, K.; Zhang, F.; Yu, F.; Shi, K.; Sun, Z.; Lin, N.; Zheng, Y. Artificial intelligence in the diagnosis of dental diseases on panoramic radiographs: a preliminary study. BMC Oral Health 2023, 23. [Google Scholar] [CrossRef] [PubMed]
- Erdelyi, R.; Duma, V.; Sinescu, C.; Dobre, G.M.; Bradu, A.; Podoleanu, A. Dental diagnosis and treatment assessments: between X-rays radiography and optical coherence tomography. Materials 2020, 13, 4825. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, R.; Bornstein, M.M.; Yeung, W.K.A.; Montalvao, C.; Colsoul, N.; Parker, Q.A. (2019). Facts and fallacies of radiation risk in dental radiology.
- Hennig, C.; Schüler, I.M.; Scherbaum, R.; Buschek, R.; Scheithauer, M.; Jacobs, C.; Mentzel, H. Frequency of dental X-ray diagnostics in children and adolescents: What is the radiation exposure? Diagnostics 2023, 13, 394. [Google Scholar] [CrossRef] [PubMed]
- Clement, C.H.; Ruehm, W.; Harrison, J.; Applegate, K.E.; Cool, D.; Larsson, C.; Cousins, C.; Lochard, J.; Bouffler, S.; Cho, K.; Kai, M.; Laurier, D.; Liu, S.; Рoманoв, C.A. Keeping the ICRP recommendations fit for purpose. Journal of Radiological Protection 2021, 41, 1390–1409. [Google Scholar] [CrossRef]
- Tuieng, R.J.; Cartmell, S.H.; Kirwan, C.C.; Sherratt, M.J. The effects of ionising and Non-Ionising electromagnetic radiation on extracellular matrix proteins. Cells 2021, 10, 3041. [Google Scholar] [CrossRef]
- Liu, L.; Huang, B.; Lu, Y.; Zhao, Y.; Tang, X.; Shi, Y. Interactions between electromagnetic radiation and biological systems. iScience 2024, 109201. [Google Scholar] [CrossRef]
- Sahani, R.; Dixit, A. A comprehensive review on zinc oxide bulk and nanostructured materials for ionizing radiation detection and measurement applications. Materials Science in Semiconductor Processing 2022, 151, 107040. [Google Scholar] [CrossRef]
- Al-Salihi, A.; Al-Saedi, A.; Abdullah, K.; Safaa, M.; Sikhi, B.; Alaa, T. Review: Dosimetry in Dental Radiology. Kirkuk University Journal-Scientific Studies 2021, 16, 1–12. [Google Scholar] [CrossRef]
- Storozynsky, Q.; Hitt, M.M. The impact of Radiation-Induced DNA damage on CGAS-STING-Mediated immune responses to cancer. International Journal of Molecular Sciences 2020, 21, 8877. [Google Scholar] [CrossRef]
- Cheng, L. (2019). Factors modifying cellular response to ionizing radiation (Doctoral dissertation, Department of Molecular Bioscience, The Winner-Gren Institute, Stockholm University).
- Simmarasan, M.; Mohan, K.R.; Vakayil, A. Knowledge, attitude, and practice of radiation protection safety measures among dental students in a dental college. Journal of Dental Research and Reviews 2023, 10, 13–18. [Google Scholar] [CrossRef]
- Berdufi, I.; Cfarku, F.; Shyti, M. Occupational radiation exposure for dental radiation workers and diagnostic radiology workers in Albania. International Conference on Pioneer and Innovative Studies 2023, 1, 189–193. [Google Scholar] [CrossRef]
- Benavides, E.; Krecioch, J.R.; Connolly, R.T.; Allareddy, T.; Buchanan, A.; Spelic, D.; O’Brien, K.K.; Keels, M.A.; Mascarenhas, A.K.; Duong, M.; Aerne-Bowe, M.J.; Ziegler, K.M.; Lipman, R.D. Optimizing radiation safety in dentistry. The Journal of the American Dental Association 2024, 155, 280–293e4. [Google Scholar] [CrossRef]
- Klingler, S.; Biel, P.; Tschanz, M.; Schulze, R. CBCTs in a Swiss university dental clinic: a retrospective evaluation over 5 years with emphasis on radiation protection criteria. Clinical Oral Investigations 2023, 27, 5627–5636. [Google Scholar] [CrossRef]
- Rasoul Tohidnia, M.; Rasool, A.; Fatemeh, A.; Rahimi, S.A.; Neda, A.; Hosna, S. EVALUATION OF RADIATION PROTECTION PRINCIPLES OBSERVANCE IN DENTAL RADIOGRAPHY CENTERS (WEST OF IRAN): CROSS-SECTIONAL STUDY. Radiat Prot Dosimetry. 2020, 190, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Rijken, J.; Jeffries, C.; Baldock, C. Radiation protection in radiotherapy is too conservative. Physical and Engineering Sciences in Medicine 2021, 44, 607–611. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.I.; Kamboj, S. Applying ALARA Principles in the Design of New Radiological Facilities. Health Physics 2022, 122, 452–462. [Google Scholar] [CrossRef] [PubMed]
- Frane, N.; Bitterman, A. Radiation Safety and Protection. [Updated 2023 May 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557499/.
- Alvandi, M.; Javid, R.N.; Shaghaghi, Z.; Farzipour, S.; Nosrati, S. An in-depth analysis of the adverse effects of ionizing radiation exposure on cardiac catheterization staffs. Current Radiopharmaceuticals 2024, 17. [Google Scholar] [CrossRef]
- Engström, A.; Isaksson, M.; Larsson, P.; Lundh, C.; Båth, M. Lead aprons and thyroid collars: to be, or not to be? Journal of Radiological Protection 2023, 43, 031516. [Google Scholar] [CrossRef]
- Federal Guidance Report No. 14: Radiation Protection Guidance for Diagnostic and Interventional X-ray Procedures | US EPA. (2024, January 11). US EPA. https://www.epa.gov/radiation/federal-guidance-report-no-14-radiation-protection-guidance-diagnostic-and-interventional.
- Lakhwani, O.; Dalal, V.; Jindal, M.; Nagala, A. Radiation protection and standardization. Journal of Clinical Orthopedics and Trauma 2019, 10, 738–743. [Google Scholar] [CrossRef]
- Hussein, S.M.; Abdelsalam, N.; Hashem, N.; Ibrahim, B.A. Knowledge, Attitude and Practice of Radiation Safety among Dentists in Ismailia City, Egypt. Journal of High Institute of Public Health 2024, 23–31. [Google Scholar] [CrossRef]
- California Dental Association. (2023, September 28). Radiation safety in dental practice: a study guide. CDA. https://www.cda.org/Home/Resource-Library/Resources/radiation-safety-in-dental-practice-a-study-guide.
- University of Washington School of Dentistry. (2023, August 11). Radiation Safety Policy - UW School of Dentistry. UW School of Dentistry. https://dental.washington.edu/policies/clinic-policy-manual/radiation-safety/.
- Mah, E.; Ritenour, E.R.; Yao, H. A review of dental cone-beam CT dose conversion coefficients. Dentomaxillofacial Radiology 2021, 50. [Google Scholar] [CrossRef] [PubMed]
- Physics, V. (2022, May 20). X-rays and radiation safety principles in dentistry. Versant Medical Physics and Radiation Safety. https://www.versantphysics.com/2022/05/20/dental-xrays/.
- Panwar, A.; Gupta, S.; Kamarthi, N.; Malik, S.; Goel, S.; Sharma, A. Awareness of radiation protection among dental practitioners in UP and NCR region, India: A questionnaire-based study. Journal of Oral and Maxillofacial Radiology 2022, 10, 13. [Google Scholar] [CrossRef]
- Martins, G.C.; Rocha, T.G.; De Lima Azeredo, T.; De Castro Domingos, A.; Visconti, M.A.; Villoria, E.M. Hand-held dental X-ray device: Attention to correct use. Imaging Science in Dentistry 2023, 53, 265. [Google Scholar] [CrossRef] [PubMed]
- Grischke, J.; Johannsmeier, L.; Eich, L.; Griga, L.; Haddadin, S. Dentronics: Toward robotics and artificial intelligence in dentistry. Dental Materials 2020, 36, 765–778. [Google Scholar] [CrossRef]
- Liu, L.; Watanabe, M.; Ichikawa, T. Robotics in Dentistry: A Narrative review. Dentistry Journal 2023, 11, 62. [Google Scholar] [CrossRef]
- Chang, Q.; Guo, S.; Zhang, X. Radiation shielding polymer composites: Ray-interaction mechanism, structural design, manufacture and biomedical applications. Materials & Design 2023, 233, 112253. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



