
Submitted:
14 January 2025
Posted:
15 January 2025
You are already at the latest version
Abstract
Delayed reperfusion of the ischemic heart (I/R) is known to impair recovery of cardiac function and produce a wide variety of myocardial defects including ultrastructural damage, metabolic alterations, subcellular Ca2+-handling abnormalities, activation of proteases and changes in cardiac gene expression. Although I/R-injury has been reported to induce the formation of reactive oxygen species (ROS), inflammation and intracellular Ca2+-overload, generation of oxidative stress is considered to play a critical role in the development of cardiac dysfunction. There occurs an increase in the production of superoxide and hydroxyl radicals as well as oxidants such as hydrogen peroxide and hypochlorous acid in hearts subjected to I/R-injury. In fact, mitochondria are a major source of excessive production of ROS in I/R hearts due to impairment in the electron transport system as well as activation of xanthine oxidase, monoamine oxidase and NADPH oxidase. Nitric oxide synthase, mainly present in the endothelium, is also activated due to I/R injury to produce nitric oxide, which upon combination with superoxide radicals, generates nitrosative stress. Alterations in cardiac function, sarcolemma and sarcoplasmic reticulum Ca2+-handling activities, and mitochondrial oxidative phosphorylation as well as protease activation due to I/R-injury are simulated upon exposing the heart to oxyradical generating system (xanthine plus xanthine oxidase) or H2O2. On the other hand, the activation of endogenous antioxidants such as superoxide dismutase, catalase and glutathione peroxidase as well as the concentration of a transcription factor (Nrf2), which modulates the expression of various endogenous antioxidants, are depressed due to I/R injury in hearts. Furthermore, pretreatment of hearts with antioxidants such as catalase plus superoxide dismutase, N-acetylcysteine and mercaptopropionylglycerine was observed to attenuate the I/R-induced subcellular Ca2+-handling and changes in Ca2+-regulatory activities as well as depress protease activation and improve the recovery of cardiac function. These observations indicate that oxidative stress is intimately involved in the pathological effects of I/R-injury and different antioxidants attenuate I/R-induced subcellular alterations and improve the recovery of cardiac function. Thus, there is a challenge to develop safe and effective antioxidants as well as agents for upregulating the expression of endogenous antioxidants for the therapy of I/R-injury.
Keywords:
ischemia-reperfusion injury
; cardiac dysfunction
; oxidative stress
; antioxidants
; subcellular defects
; Ca2+-handling abnormalities
1. Introduction
It is now well known that myocardial ischemia induces marked alterations in contractile function, cellular metabolism and cardiac ultrastructure due to the lack of both oxygen and substrates. Although reperfusion of the ischemic myocardium is beneficial in improving cardiac function and myocardial changes, delayed reperfusion, after a certain critical time of ischemic insult has been shown to impair the recovery of cardiac function and exacerbate metabolic alterations, induce Ca2+-handling abnormalities and promote damage to the myocardial structure [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15]. These defects due to reperfusion of the ischemic heart are termed as ischemia-reperfusion (I/R)-injury, which is commonly seen in clinical conditions such as acute coronary syndrome, angioplasty, thrombolysis, coronary bypass surgery, cardiac transplantation and stroke. Extensive studies regarding the pathophysiology of I/R-injury to the heart have been carried out to understand its mechanisms involving different factors, signal transduction pathways and mitochondrial alterations [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35]. However, it appears that the mechanisms of I/R-injury induced cardiac dysfunction are similar to those for hypoxia-reoxygenation induced alterations, but are of complex nature because the effects of reperfusion are superimposed upon those for myocardial ischemia. It should be mentioned that I/R-injury also includes a series of events such as reperfusion arrhythmias, myocardial stunning, microvascular damage and cell death, which occur during the development of cardiac dysfunction.
Cardiac dysfunction in hearts subjected to I/R-injury has also been shown to involve oxidative stress, inflammation, endoplasmic reticulum stress, intracellular Ca2+- overload and defects in subcellular organelles such as sarcolemma (SL), sarcoplasmic reticulum (SR), mitochondria (MT) and myofibrils (MF) [36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51]. However, oxidative stress is considered to play a critical role in the development of impaired cardiac performance due to I/R- injury because several defects associated with this pathological condition are elicited as its consequence. Furthermore, different antioxidants have been reported to attenuate the I/R-induced alterations in the heart [7,11,15,36,41,44,48,50,51,52]. It is therefore the objective of this article to provide an updated comprehensive review of various sources for the generation of oxidative stress as well as the role of endogenous antioxidants during the development of I/R-injury. It is also planned to discuss the implications of oxidative stress in inducing cardiac dysfunction due to I/R-injury. Furthermore, this article is intended to include evidence for the involvement of oxidative stress in the I/R-induced subcellular alterations and subsequent impairment of cardiac performance. In addition, the pharmacotherapy of I/R-injury with both endogenous and exogenous antioxidant systems will be described with respect to improving cardiac function in pathological conditions.
2. Generation of Oxidative Stress and Status of Antioxidant Systems in I/R Hearts
Oxidative stress is associated with an increase in the production of reactive oxygen species (ROS) and/or a decrease in the activities of antioxidant defense systems due to I/R- injury in the heart [8,9,14,15,43,44,51]. There are five major types of ROS such as superoxide radicals, hydroxyl radicals, hydrogen peroxide (H2O2), hypochlorous acid and peroxynitrite, which are increased in the heart upon inducing I/R injury. ROS are mainly generated by impairment of electron transport in mitochondria, xanthine + xanthine oxidase reaction, arachidonic acid metabolism, as well as the activation of monoamine oxidase, NADPH oxidase, the endothelium and neutrophils. It should be mentioned that superoxide radicals are rapidly converted into H2O2, which is a precursor of hydroxyl ions in the presence of iron and copper, as well as hypochlorous acid (HOCl) in the presence of myeloperoxidases and chloride ions. Superoxide radicals also react with nitric oxide (produced upon the activation of endothelium) to form peroxynitrite. Although all members of the ROS family are inter-related, hydroxyl radicals are considered to be the most reactive with a very short half-life. It should also be pointed out that low concentrations of ROS produce beneficial effects on the heart by activating different redox-sensitive signal transduction pathways whereas high concentrations of ROS (oxidative stress) produce harmful effects by reacting with cellular proteins, lipids, carbohydrates and DNA. Thus, the I/R injury produces changes in membrane permeability, and protein thiol group oxidation as well as lipid peroxidation, which are considered to be mediated through the generation of oxidative stress.
Excessive generation of ROS by mitochondrial defects and other sources have been demonstrated to be associated with activation of transient receptor potential melastatin 2 (TRPM2), production of endoplasmic reticulum stress (ER stress), DNA damage as well as upregulation of NADPH oxidase, hemeoxygenases and cyclooxygenases [53,54,55,56,57,58,59,60,61,62,63,64,65,66]. ROS have also been shown to produce ventricular arrhythmias, alter apelinergic system and ubiquitin-proteosome axis in addition to inducing different types of cell death such as necrosis, apoptosis, necroptosis, pyroptosis and ferrotosis [67,68,69,70,71,72,73,74,75,76,77,78]. Different endogenous proteins such as perilipin, SESTRIN2, heat shock protein 22 and humanin as well as exosomes and microRNA with antioxidant properties have been reported to protect the harmful effects of ROS in the heart [79,80,81,82,83,84,85]. Various enzymes including superoxide dismutase (SOD), catalase and glutathione peroxidases as well as vitamins such as vitamin E, vitamin A and vitamin C are known to serve as endogenous antioxidants [8,44,49,50,51]. These antioxidants are considered to act through mechanisms involved in either scavenging ROS or inhibiting the generation of ROS in the myocardium. The levels of these antioxidants are not only decreased upon reperfusing the ischemic heart, but these interventions are also effective in attenuating I/R-injury to the heart upon pretreatment. These observations support the view that generation of ROS and development of oxidative stress are intimately involved in the pathogenesis of I/R-injury to the heart [8,49,50,51,86,87].
3. Mechanisms of I/R-Injury Induced Subcellular Defects and Cardiac Dysfunction
Since the status of cardiac function is determined by the coordinated Ca2+-handling activities of different subcellular organelles including SL, SR and MT as well as Ca2+-regulated activity of MF [11,88,89,90], it has been suggested that abnormalities in subcellular function due to oxidative stress play an important role in the development of cardiac dysfunction as a consequence of I/R-injury [8,41,51]. Oxidative stress is known to induce Ca2+-handling abnormalities in SL, SR and MT in addition to producing a loss of Ca2+-sensitivity in MF and thus leads to the development of cardiac dysfunction. It should be pointed out that myocardial ischemia upon occluding the coronary arteries is associated with the lack of oxygen, inability of MT to oxidize substrate and accumulation of hydrogen in cardiomyocytes; these alterations result in increasing the intracellular concentration of Ca2+ upon stimulating SL Na+-H+ exchange and SL Na+- Ca2+-exchange systems. The increased levels of Ca2+ in the ischemic myocardium activate xanthine oxidase and produce ROS through the xanthine plus xanthine oxidase reaction. Furthermore, the inability of MT to oxidize substrate in the ischemic heart is known to depress oxidative phosphorylation, and impair the MT electron transport system, generate ROS and produce cessation of contractile activity. All these changes due to myocardial ischemia are reversible upon reperfusion; however, delayed reperfusion results in marked defects in cardiomyocytes, myocardial interstitium, endothelium and coronary vasculature for the induction of ultrastructural abnormalities as well as impairment of contractile function recovery as a consequence of ROS production [1,2,3,4,5,6,7,8,9,10,11,41,43,51]. Such alterations in cardiomyocytes due to reperfusion of the ischemic heart are associated with increased entry of Ca2+ due to increase in membrane permeability as well as depressions in SL Na+-K+ ATPase and SL Na+- Ca2+-exchange activities. In addition, there occurs a depression in the SR Ca2+-pump activity and leakage of Ca2+ from the SR tubular system due to ROS-induced alterations in SR Ca2+-release channels. These Ca2+-handling abnormalities in SL and SR lead to the development of MT Ca2+-overload and further defects in MT electron transport system, oxidative phosphorylation activity and energy production, in addition to generation of oxidative stress, opening of MT pores and release of cytotoxic substances for the induction of programmed cell death.
Although oxidative stress is considered to be mainly generated by MT, upon inducing I/R injury, the involvement of other systems such as Ca2+-handling abnormalities in SL and SR for the occurrence of MT Ca2+-overload, endothelium nitric oxide synthase for the production of nitric oxide and peroxynitrite, macrophages and leukocytes for the release of proinflammatory cytokines such as tumor necrosis factor-α (TNF-α) as well as interleukins (IL-1β and IL-6) as well as long noncoding RNA-RNA axis and thioredoxin-interacting protein for the generation of oxidative stress during the development of I/R-injury cannot be overlooked [91,92,93,94,95,96,97,98,99]. Furthermore, the activation of both SL and MT associated NADPH oxidases, as well as MT monoamine oxidase (MAO), glucose homeostasis and oxidation of free fatty acids, and arachidonic acid metabolic pathways have been demonstrated to play a critical role for the development of oxidative stress during the initiation and progression of I/R-injury to the heart [20,21,51,100]. It is also noteworthy that the concentrations of different ROS and oxidants are increased whereas those for endogenous antioxidant enzymes are decreased in the heart upon inducing I/R injury [49,50,51,101,102,103]; these observations provide strong evidence for the occurrence of oxidative stress during the development of oxidative stress. Several studies have also shown that transcription factors such as nuclear factor erythroid 2-related factor 2 (Nrf2) and Kelch-like ECH-associated protein 1 (Keap1), which have been shown to modulate the activities of various endogenous antioxidants, protect the occurrence of intracellular Ca2+-overload, inflammation and oxidative stress during the induction of I/R-injury in the heart [104,105,106,107,108,109,110,111,112]. Accordingly, it is evident that different subcellular organelles are not only involved in the generation of oxidative stress and intracellular Ca2+-overload in cardiomyocytes, but are also adversely affected by these pathogenic factors leading to the development of cardiac dysfunction due to I/R-injury.
4. Pharmacotherapy and Cardioprotection of I/R-Induced Injury
Extensive experimental work in the area of pharmacotherapy and cardioprotection has been carried out to investigate the beneficial effects of several interventions in preventing the I/R injury in the heart [8,44,51,113]. Different pharmacologic agents such as hypoglycemic drugs [114,115], aldosterone inhibitors [116], regulatory interventions including SIRT1 (regulator of autophagy), STING (stimulator of interferon genes) and AMP-activated protein kinase [117,118,119] as well as nanomedicines [120] were found to attenuate the I/R-injury. Likewise, some interventions such as nitric oxide, heme oxygenase 1, propofal and adiponectin, which affects diverse molecular targets, were observed to partially prevent the I/R-injury in the heart [121,122,123,124]. Furthermore, different types of RNAs (circular RNA, noncoding RNA and micro RNA) have also been reported to exert beneficial effects in attenuating the I/R-injury through some complex mechanisms [125,126,127]. Some phytochemicals, natural products and micronutrients have been claimed to protect I/R-injury upon improving the antioxidant status [128,129,130]. Although it may well be that all these interventions indicated in this section may partially depress the I/R-injury by reducing the formation of ROS or increasing the concentrations of different antioxidants; however, the involvement of other mechanisms such as alterations in inflammation, reduction in intracellular Ca2+-overload and inhibition of protease activation cannot be ruled out with any certainty.
In view of the depressed endogenous antioxidant levels in the I/R hearts, several investigators have used redox sensitive therapy for preventing the I/R-injury. In this regard, supplementation with exogenous antioxidant preparations [51,52,126,131,132] and administration of interventions which up-regulate the transcription factor, Nrf2, [107,110,111] for increasing the antioxidant status were shown to exert beneficial effects against I/R-injury. Various proteins such as humanin, berberine, sestrin, taurine, fisetin, quercetin and polydatin with antioxidant properties were also observed to attenuate I/R- injury in the heart [81,122,133,134,135,136,137]. Different vitamins such as vitamins A, C and E with antioxidant activities have also been shown to exert beneficial effects against I/R injury [138,139]. Some gases such as molecular hydrogen and hydrogen sulfide [109,131,140,141,142,143] as well as ischemic preconditioning [90,144] have also been reported to exert beneficial actions. All these observations showing cardioprotective effects of various interventions in I/R hearts due to their antioxidant activities support the view that oxidative stress plays a pivotal role in the development of I/R-injury.
5. Evidence for the Involvement of Oxidative Stress in I/R-Induced Cardiac Dysfunction
In order to provide further evidence for the occurrence of oxidative stress in the impairment of cardiac function recovery upon reperfusion of the ischemic heart, we have analyzed some information from some experiments, which were carried out for inducing I/R-injury in the isolated perfused hearts pretreated in the absence and presence of some antioxidants. It should be mentioned that isolated heats were subjected to 30 min of global ischemia before inducing reperfusion for 30 to 60 min. Furthermore, the effects of I/R-induced injury were compared with those obtained from hearts perfused with or without oxyradical generating system (xanthine plus xanthine oxidase) as well as H2O2, a well-known oxidant, for 30 min.
The data [87] in Figure 1 show that the left ventricular developed pressure (LVDP) (A) was depressed whereas the left ventricular end diastolic pressure (LVEDP) (B) was markedly increased upon reperfusion indicating the impairment of cardiac function due to I/R-injury. Furthermore, the biomarkers of oxidative stress (H2O2 content and MDA content) were also increased in the I/R hearts (Figure 1 C and D). Treatment of hearts with an antioxidant mixture (SOD plus catalase) was observed to attenuate the I/R-induced changes in cardiac function and biomarkers of oxidative stress. It is also pointed out myocardial Ca2+-content in control, I/R and SOD plus catalase treated I/R hearts were 8.4±1.2, 22.6±2.9 and 9.8±1.6 µmol/g dry wt., respectively [87].
Figure 2 shows that depressed LV function in I/R hearts was associated with markedly decreased SL Na+-K+ ATPase (Figure 2A) activity as well as increased protease activities for matrix metalloproteinase (MMP) (Figure 2B) and calpain (Figure 2C) [145]. These effects of I/R-injury were attenuated when reperfusion of the ischemic hearts was carried out in the presence of well-known antioxidants namely N-acetylcysteine (NAC) or mercaptopropionyl glycine (MGP) (Figure 2). The depressed LVDP was shown to be associated with reduced Na+-K+ ATPase activities in hearts perfused with xanthine plus xanthine oxidase (X+XO) (Figure 2D) and was also observed to be associated with increased activities of both MMP and calpain (Figure 2E and F). The data in Figure 3 show that Na+-Ca2+ exchange (A), ATP-dependent Ca2+-uptake (B) and Ca2+-stimulated ATP activities (C) were depressed upon reperfusing the ischemic hearts (I/R hearts). These alterations due to I/R were attenuated when the I/R was carried out in the presence of SOD plus catalase [146,147,148].
Likewise, Figure 3 D-F show depressions in the SL Na+-Ca2+ exchange, ATP-dependent Ca2+-uptake and Ca2+-stimulated ATP activities, respectively, upon perfusion with X+XO. These changes due to ROS generating system were attenuated in the presence of SOD plus catalase [146,147,148]. It should also be noted that SR Ca2+-uptake, Ca2+-stimulated ATPase, Ca2+-release and ryanodine binding activities were depressed in the I/R hearts (Figure 4), but when the reperfusion of the ischemic hearts was carried out in the presence of SOD plus catalase, these alterations (except that for Ca2+-stimulated ATPase) were attenuated [149]. Furthermore, perfusion of hearts with X+XO or H2O2 [149] was also observed to depress SR Ca2+-uptake, Ca2+-stimulated ATPase, Ca2+-release and ryanodine binding activities (Figure 5). These observations indicate that defects in both SL and SR organelles due to I/R-injury are not only prevented by antioxidants mixture, but are simulated by ROS generating systems.
The effects of I/R-injury and ROS generating system on MT and MF have also been examined. The data in Figure 6 show that MT state 3 respiration (A) and ADP/O ratio index (B) were depressed upon subjecting the heart to I/R-injury and these effects were attenuated by SOD plus catalase [150]. Furthermore, perfusing the hearts with X+XO or H2O2 [150] was found to depress MT state 3 respiration and ADP/O ratio index (Figure 6 C and D).
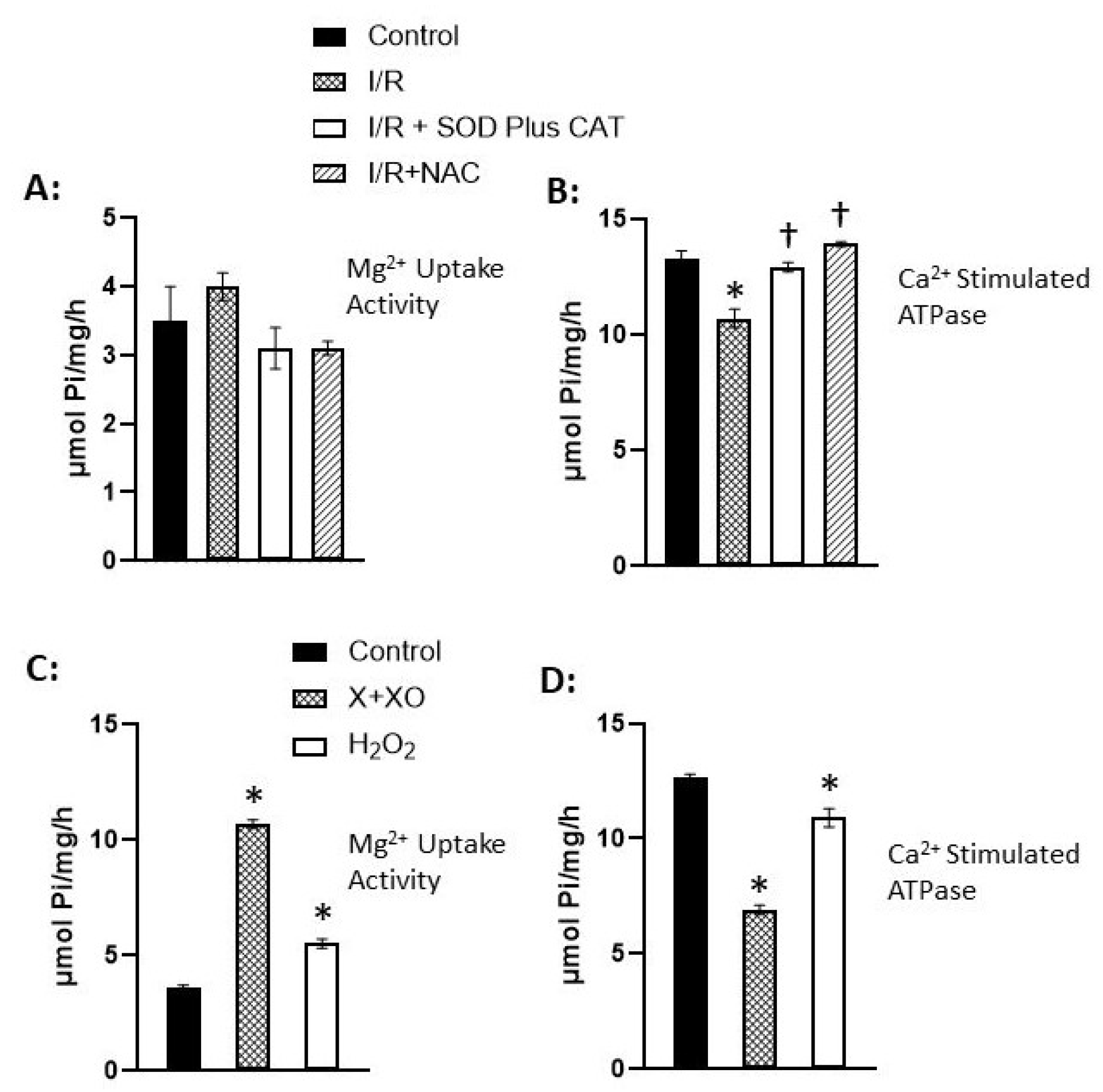
The data in Figure 7 indicate depression in MF Ca2+-stimulated ATPase activity due to I/R was prevented in the presence of SOD plus catalase or N-acetylcysteine (Figure 7B) [151,152]. It should also be noted that MF Mg2+- ATPase activity was increased whereas MF Ca2+-stimulated ATPase activity was depressed by perfusing the hearts with X+XO or H2O2 (Figure 7 C and D). These observations suggest that both I/R injury and ROS generating system produce similar changes in the MT and MF and the effects of I/R-injury were attenuated by antioxidants.
6. Conclusions
It is now well known that delayed reperfusion of the ischemic heart produces marked alterations in myocardial metabolism and cardiac ultrastructure in addition to impairing the recovery of cardiac function. Such changes in the ischemic-reperfused hearts (I/R-injury) are associated with increased formation of superoxide and hydroxyl radicals as well as oxidants including H2O2, hypochlorous acid and peroxynitrite, which are collectively termed as reactive oxygen species (ROS). It is noteworthy that MT are the major source of ROS production due to defects in the electron transport system as well as xanthine oxidase as a consequence of reperfusion of the ischemic hearts. There also occurs the activation of endothelium nitric oxide synthase and formation of nitric oxide, which combines with superoxide radicals to generate peroxynitrite. On the other hand, the concentrations of endogenous antioxidants including superoxide dismutase, catalase, and glutathione peroxidase (which antagonizes the actions of ROS) are decreased due to the induction of reperfusion. It should also be mentioned that the levels of transcription factor, Nrf2, which regulates the status of several antioxidants, are also depressed upon reperfusion. Thus, there occurs an imbalance between the excessive formation of ROS and reduced levels of antioxidants due to reperfusion, which leads to the generation of oxidative stress. Although various defects such as inflammation, subcellular alterations, intracellular Ca2+-overload, activation of proteases and changes in cardiac gene expression occur in the ischemia-reperfused hearts, these abnormalities seem to be the consequence of oxidative stress generation during the development of I/R-injury.
Impaired recovery of cardiac function due to I/R-injury has been shown to be associated with depression in SL Na+-K+ ATPase, Na+-Ca2+ exchange and ATP-dependent Ca2+-pump activities. These SL alterations would increase the entry of Ca2+ into cardiomyocytes and elevate the intracellular concentration of Ca2+. Furthermore, I/R-injury has been demonstrated to induce changes in the SR Ca2+-pump activity and promote the leakage of Ca2+ to further raise the intracellular concentration of Ca2+ and cause the recurrence of MT Ca2+-overload, depression in the oxidative phosphorylation and energy production, opening MT pores for the leakage of cytotoxic material and development of programmed cellular death. The occurrence of Ca2+-handling abnormalities in the SL and SR organelles is also associated with the development of intracellular Ca2+-overload, activation of proteases such as MMP and calpain, depression in the cardiac gene expression and loss of MF Ca2+-sensitivity. Furthermore, treatment of the heart with different antioxidants has been shown to attenuate I/R-induced Ca2+-handling defects in subcellular organelles, activation of proteases, loss of MF Ca2+ sensitivity and development of cardiac dysfunction. It is thus evident that oxidative stress plays an important role in impairing the recovery of cardiac function due to I/R-injury. Accordingly, it is suggested that efforts should be made to develop safe and effective interventions for the upregulation of endogenous antioxidants for improving cardiovascular abnormalities associated with I/R-injury.
Author Contributions
P.S.T. searched the literature and analyzed the data; both P.O. and P.S.T. wrote the manuscript; N.S.D. conceived, designed and prepared the final draft of this article. All authors have agreed to the published version of the manuscript.
Funding
This project did not receive any external funding.
Data Availability Statement
The original contributions presented in this study are included in the article.
Acknowledgments
The infrastructural support of this article was provided by the St. Boniface Hospital Albrechtsen Research Centre.
Conflicts of Interest
The authors have no conflict of interest.
References
- Sharma, G.P.; Varley, K.G.; Kim, S.W.; Barwinsky, J.; Cohen, M.; Dhalla, N.S. Alterations in energy metabolism and ultrastructure upon reperfusion of the ischemic myocardium after coronary occlusion. Am J Cardiol 1975, 36, 234–243. [Google Scholar] [CrossRef]
- Nayler, W.G.; Panagiotopoulos, S.; Elz, J.S.; Daly, M.J. Calcium-mediated damage during post-ischemic reperfusion. J Mol Cell Cardiol 1988, 20 (Suppl. 2), 41–54. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.G.; Smith, T.W.; Marsh, J.D. Mechanisms of reoxygenation-induced calcium overload in cultured chick embryo heart cells. Am J Physiol 1988, 254, H1133–H1141. [Google Scholar] [CrossRef]
- Jennings, R.B.; Reimer, K.A. The cell biology of acute myocardial ischemia. Annu Rev Med 1991, 42, 225–246. [Google Scholar] [CrossRef]
- Bolli, R.; Marban, E. Molecular and cellular mechanisms of myocardial stunning. Physiol Rev 1999, 79, 609–634. [Google Scholar] [CrossRef]
- Piper, M.H.; Meuter, K.; Schafer, C. Cellular mechanisms of ischemia-reperfusion injury. Ann Thorac Surg 2003, 75, S644–S648. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.W.; Gilbert, T.B.; Poston, R.S.; Silldorff, E.P. Myocardial reperfusion injury: Etiology, mechanisms, and therapies. J Extra Corpor Technol 2004, 36, 391–411. [Google Scholar] [CrossRef] [PubMed]
- Dhalla, N.S.; Elmoselhi, A.B.; Hata, T.; Makino, N. Status of myocardial antioxidants in ischemia-reperfusion injury. Cardiovasc Res 2000, 47, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Neuzil, J.; Rayner, B.S.; Lowe, H.C.; Witting, P.K. Oxidative stress in myocardial ischemia reperfusion injury: A renewed focus on a long-standing area of heart research. Redox Rep 2005, 10, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Milei, J.; Grana, D.R.; Forcada, P.; Ambrosio, G. Mitochondrial oxidative and structural damage in ischemia-reperfusion in human myocardium. Current knowledge and future directions. Front Biosci 2007, 12, 1124–1130. [Google Scholar] [CrossRef]
- Dhalla, N.S.; Saini, H.K.; Tappia, P.S.; Sethi, R.; Mengi, S.A.; Gupta, S.K. Potential role and mechanisms of subcellular remodeling in cardiac dysfunction due to ischemic heart disease. J Cardiovasc Med 2007, 8, 238–250. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, R.; Libuy, M.; Feliu, F.; Hasson, D. Oxidative stress-related biomarkers in essential hypertension and ischemia-reperfusion myocardial damage. Dis Markers 2013, 35, 773–790. [Google Scholar] [CrossRef]
- Neri, M.; Riezzo, I.; Pascale, N.; Pomara, C.; Turillazzi, E. Ischemia/reperfusion injury following acute myocardial infarction: A critical issue for clinicians and forensic pathologists. Mediators Inflamm 2017, 2017, 7018393. [Google Scholar] [CrossRef]
- Zhou, T.; Chuang, C.C.; Zuo, L. Molecular characterization of reactive oxygen species in myocardial ischemia-reperfusion injury. Biomed Res Int 2015, 2015, 864946. [Google Scholar] [CrossRef]
- Kurian, G.A.; Rajagopal, R.; Vedantham, S.; Rajesh, M. The role of oxidative stress in myocardial ischemia and reperfusion injury and remodeling: Revisited. Oxidative Med Cell Longev 2016, 2016, 165450. [Google Scholar] [CrossRef]
- Morciano, G.; Pinton, P. Modulation of mitochondrial permeability transition pores in reperfusion injury: Mechanisms and therapeutic approaches. Eur J Clin Invest 2025, 55, e14331. [Google Scholar] [CrossRef]
- Liu, Y.; Wu, H.; Zhou, G.; Zhang, D.; Yang, Q.; Li, Y.; Yang, X.; Sun, J. Role of M6a Methylation in Myocardial Ischemia-Reperfusion Injury and Doxorubicin-Induced Cardiotoxicity. Cardiovasc Toxicol 2024, 24, 918–928. [Google Scholar] [CrossRef]
- Li, J.; Zhang, Y.; Tang, R.; Liu, H.; Li, X.; Lei, W.; Chen, J.; Jin, Z.; Tang, J.; Wang, Z.; Yang, Y.; Wu, X. Glycogen synthase kinase-3β: A multifaceted player in ischemia-reperfusion injury and its therapeutic prospects. J Cell Physiol 2024, 239, e31335. [Google Scholar] [CrossRef]
- Balderas, E.; Lee, S.H.J.; Rai, N.K.; Mollinedo, D.M.; Duron, H.E.; Chaudhuri, D. Mitochondrial calcium regulation of cardiac metabolism in health and disease. Physiology 2024, 39. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, E.; Aoki, T.; Endo, Y.; Kazmi, J.; Hagiwara, J.; Kuschner, C.E.; Yin, T.; Kim, J.; Becker, L.B.; Hayashida, K. Organ-specific mitochondrial alterations following ischemia-reperfusion injury in post-cardiac arrest syndrome: A comprehensive review. Life 2024, 14, 477. [Google Scholar] [CrossRef]
- Yan, Z.; Xing, Z.; Xue, T.; Zhao, J.; Li, G.; Xu, L.; Sun, Q. Insulin-like growth factor-1 in myocardial ischemia-reperfusion injury: A review. Medicine 2024, 103, e37279. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, R.; Yan, Y.; He, B.; Miao, C.; Fang, Y.; Wan, H.; Zhou, G. Exosomes-mediated signaling pathway: A new direction for treatment of organ ischemia-reperfusion injury. Biomedicines 2024, 12, 353. [Google Scholar] [CrossRef] [PubMed]
- Liao, W.; Wen, Y.; Yang, S.; Duan, Y.; Liu, Z. Research progress and perspectives of N-methyl-D-aspartate receptor in myocardial and cerebral ischemia-reperfusion injury: A review. Medicine 2023, 102, e35490. [Google Scholar] [CrossRef]
- Omorou, M.; Huang, Y.; Gao, M.; Mu, C.; Xu, W.; Han, Y.; Xu, H. The forkhead box O3 (FOXO3): a key player in the regulation of ischemia and reperfusion injury. Cell Mol Life Sci 2023, 80, 102. [Google Scholar] [CrossRef]
- Galeone, A.; Grano, M.; Brunetti, G. Tumor necrosis factor family members and myocardial ischemia-reperfusion injury: State of the art and therapeutic implications. Int J Mol Sci 2023, 24, 4606. [Google Scholar] [CrossRef] [PubMed]
- Popov, S.V.; Mukhomedzyanov, A.V.; Voronkov, N.S.; Derkachev, I.A.; Boshchenko, A.A.; Fu, F.; Sufianova, G.Z.; Khlestkina, M.S.; Maslov, L.N. Regulation of autophagy of the heart in ischemia and reperfusion. Apoptosis 2023, 28, 55–80. [Google Scholar] [CrossRef] [PubMed]
- Mahdiani, S.; Omidkhoda, N.; Rezaee, R.; Heidari, S.; Karimi, G. Induction of JAK2/STAT3 pathway contributes to protective effects of different therapeutics against myocardial ischemia/reperfusion. Biomed Pharmacother 2022, 155, 113751. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Wu, J.; Yang, Z.; Wang, X.; Zhang, D.; Ma, J. Mitochondrial quality control in cardiac ischemia/reperfusion injury: new insights into mechanisms and implications. Cell Biol Toxicol 2023, 39, 33–51. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Liu, X.; Zhou, J.; Li, T. Mitochondrial DNA is a vital driving force in ischemia-reperfusion injury in cardiovascular diseases. Oxid Med Cell Longev 2022, 2022, 6235747. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Liu, D.; Zhao, L.; Zhou, D.; Rong, J.; Zhang, L.; Xia, Z. Myocardial ischemia/reperfusion injury: Mechanisms of injury and implications for management. Exp Ther Med 2022, 23, 430. [Google Scholar] [CrossRef] [PubMed]
- Maslov, L.N.; Popov, S.V.; Mukhomedzyanov, A.V.; Naryzhnaya, N.V.; Voronkov, N.S.; Ryabov, V.V.; Boshchenko, A.A.; Khaliulin, I.; Prasad, N.R.; Fu, F.; Pei, J.M.; Logvinov, S.V.; Oeltgen, P.R. Reperfusion cardiac injury: Receptors and the signaling mechanisms. Curr Cardiol Rev 2022, 18, 63–79. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Y.; Yu, M.L.; Lu, S.F. Purinergic signaling in myocardial ischemia-reperfusion injury. Purinergic Signal 2023, 19, 229–243. [Google Scholar] [CrossRef]
- Casin, K.M.; Calvert, J.W. Dynamic regulation of cysteine oxidation and phosphorylation in myocardial ischemia-reperfusion injury. Cells 2021, 10, 2388. [Google Scholar] [CrossRef]
- Chen, L.; Shi, D.; Guo, M. The roles of PKC-δ and PKC-ε in myocardial ischemia/reperfusion injury. Pharmacol Res 2021, 170, 105716. [Google Scholar] [CrossRef]
- Zheng, J.; Chen, P.; Zhong, J.; Cheng, Y.; Chen, H.; He, Y.; Chen, C. HIF-1α in myocardial ischemia-reperfusion injury. Mol Med Rep 2021, 23, 352. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.; Kang, P.M. A systematic review on advances in management of oxidative stress-associated cardiovascular diseases. Antioxidants 2024, 13, 923. [Google Scholar] [CrossRef]
- Chen, X.; Yang, Y.; Zhou, Z.; Yu, H.; Zhang, S.; Huang, S.; Wei, Z.; Ren, K.; Jin, Y. Unraveling the complex interplay between Mitochondria-Associated Membranes (MAMs) and cardiovascular inflammation: Molecular mechanisms and therapeutic implications. Int Immunopharmacol 2024, 141, 112930. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhao, Y.; Gong, N. Endoplasmic reticulum stress signaling modulates ischemia/reperfusion injury in the aged heart by regulating mitochondrial maintenance. Mol Med 2024, 30, 107. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Dhalla, N.S. The role of pro-inflammatory cytokines in the pathogenesis of cardiovascular disease. Int J Mol Sci 2024, 25, 1082. [Google Scholar] [CrossRef]
- Ruan, Y.; Zeng, J.; Jin, Q.; Chu, M.; Ji, K.; Wang, Z.; Li, L. Endoplasmic reticulum stress serves an important role in cardiac ischemia/reperfusion injury. Exp Ther Med 2020, 20, 268. [Google Scholar] [CrossRef]
- Shah, A.K.; Bhullar, S.K.; Elimban, V.; Dhalla, N.S. Oxidative stress as a mechanism for functional alterations in cadiac hypertrophy and heart failure. Antioxidants 2021, 10, 931. [Google Scholar] [CrossRef] [PubMed]
- Dhalla, N.S.; Elimban, V.; Shah, A.K.; Nusier, M. Mechanisms of cardiac dysfunction in heart failure due to myocardial infarction. J Integr Cardiol 2019, 2, 3–7. [Google Scholar] [CrossRef]
- Dhalla, N.S.; Temsah, R.M.; Netticadan, T. Role of oxidative stress in cardiovascular diseases. J Hypertens 2000, 18, 655–673. [Google Scholar] [CrossRef]
- Dhalla, N.S.; Elimban, V.; Bartekova, M.; Adameova, A. Involvement of oxidative stress in the development of subcellular defects and heart disease. Biomedicines 2022, 10, 393. [Google Scholar] [CrossRef]
- Saini, H.K.; Xu, Y.J.; Zhang, M.; Liu, P.P.; Kirshenbaum, L.A.; Dhalla, N.S. Role of tumor necrosis factor-alpha and other cytokines in ischemia-reperfusion-induced injury in the heart. Exp Clin Cardiol 2005, 10, 213–222. [Google Scholar] [PubMed]
- Ambrosio, G.; Zweier, J.L.; Flaherty, J.T. The relationship between oxygen radical generation and impairment of myocardial energy metabolism following post-ischemic reperfusion. J Mol Cell Cardiol 1991, 23, 1359–1374. [Google Scholar] [CrossRef] [PubMed]
- Sinning, C.; Westermann, D.; Clemmensen, P. Oxidative stress in ischemia and reperfusion: Current concepts, novel ideas and future perspectives. Biomark Med 2017, 11, 11031–11040. [Google Scholar] [CrossRef] [PubMed]
- Bartekova, M.; Barancik, M.; Ferenczyova, K.; Dhalla, N.S. Beneficial effects of N-acetylcysteine and N–N-mercaptopropionylglycine on Ischemia reperfusion injury in the heart. Curr Med Chem 2018, 25, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, R.; Ceconi, C.; Curello, S.; Guarnieri, C.; Caldarera, C.M.; Albertini, A.; Visioli, O. Oxygen-mediated myocardial damage during ischemia and reperfusion: Role of the cellular defenses against oxygen toxicity. J Mol Cell Cardiol 1985, 17, 937–945. [Google Scholar] [CrossRef]
- Arduini, A.; Mezzetti, A.; Porreca, E.; Lapenna, D.; DeJulia, J.; Marzio, L.; Polidoro, G.; Cuccurullo, F. Effect of ischemia and reperfusion on antioxidant enzymes and mitochondrial inner membrane proteins in perfused rat heart. Biochim Biophys Acta 1988, 970, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Dhalla, N.S.; Shah, A.K.; Adameova, A.; Bartekova, M. Role of oxidative stress in cardiac dysfunction and subcellular defects due to ischemia-reperfusion injury. Biomedicines 2022, 10, 1473. [Google Scholar] [CrossRef] [PubMed]
- San-Martín-Martínez, D.; Serrano-Lemus, D.; Cornejo, V.; Gajardo, A.I.J.; Rodrigo, R. Pharmacological basis for abrogating myocardial reperfusion injury through a multi-target combined antioxidant therapy. Clin Pharmacokinet 2022, 61, 1203–1218. [Google Scholar] [CrossRef] [PubMed]
- Matsushima, S.; Sadoshima, J. Yin and Yang of NADPH oxidases in myocardial ischemia-reperfusion. Antioxidants 2022, 11, 1069. [Google Scholar] [CrossRef]
- Chen, C.L.; Zhang, L.; Jin, Z.; Kasumov, T.; Chen, Y.R. Mitochondrial redox regulation and myocardial ischemia-reperfusion injury. Am J Physiol Cell Physiol 2022, 322, C12–C23. [Google Scholar] [CrossRef]
- Wang, M.; Liu, Y.; Liang, Y.; Naruse, K.; Takahashi, K. Systematic understanding of pathophysiological mechanisms of oxidative stress-related conditions-diabetes mellitus, cardiovascular diseases, and ischemia-reperfusion injury. Front Cardiovasc Med 2021, 8, 649785. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Wang, Z.; Carmone, C.; Keijer, J.; Zhang, D. Role of oxidative DNA damage and repair in atrial fibrillation and ischemic heart disease. Int J Mol Sci 2021, 22, 3838. [Google Scholar] [CrossRef] [PubMed]
- Dambrova, M.; Zuurbier, C.J.; Borutaite, V.; Liepinsh, E.; Makrecka-Kuka, M. Energy substrate metabolism and mitochondrial oxidative stress in cardiac ischemia/reperfusion injury. Free Radic Biol Med 2021, 165, 24–37. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.; Qu, C.; Rao, Z.; Wu, D.; Zhao, J. Bidirectional regulation mechanism of TRPM2 channel: role in oxidative stress, inflammation and ischemia-reperfusion injury. Front Immunol 2024, 15, 1391355. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.L.; Cai, M.R.; Zhang, M.Q.; Cui, S.; Zhang, T.R.; Cheng, W.H.; Wu, Y.H.; Ou, W.J.; Jia, Z.H.; Zhang, S.F. Chinese herbal medicine alleviates myocardial ischemia/reperfusion injury by regulating endoplasmic reticulum stress. Evid Based Complement Alternat Med 2021, 2021, 4963346. [Google Scholar] [CrossRef] [PubMed]
- Wiklund, L.; Sharma, A.; Patnaik, R.; Muresanu, D.F.; Sahib, S.; Tian, Z.R.; Castellani, R.J.; Nozari, A.; Lafuente, J.V.; Sharma, H.S. Upregulation of hemeoxygenase enzymes HO-1 and HO-2 following ischemia-reperfusion injury in connection with experimental cardiac arrest and cardiopulmonary resuscitation: Neuroprotective effects of methylene blue. Prog Brain Res 2021, 265, 317–375. [Google Scholar] [CrossRef]
- Thompson, J.; Maceyka, M.; Chen, Q. Targeting ER stress and calpain activation to reverse age-dependent mitochondrial damage in the heart. Mech Ageing Dev 2020, 192, 111380. [Google Scholar] [CrossRef] [PubMed]
- Dubois-Deruy, E.; Peugnet, V.; Turkieh, A.; Pinet, F. Oxidative stress in cardiovascular diseases. Antioxidants 2020, 9, 864. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Cheng, C.K.; Zhang, C.L.; Huang, Y. Interplay between oxidative stress, cyclooxygenases, and prostanoids in cardiovascular diseases. Antioxid Redox Signal 2021, 34, 784–799. [Google Scholar] [CrossRef]
- Bugger, H.; Pfeil, K. Mitochondrial ROS in myocardial ischemia reperfusion and remodeling. Biochim Biophys Acta Mol Basis Dis 2020, 1866, 165768. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Toan, S. Pathological roles of mitochondrial oxidative stress and mitochondrial dynamics in cardiac microvascular ischemia/reperfusion injury. Biomolecules 2020, 10, 85. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Murugesan, P.; Huang, K.; Cai, H. NADPH oxidases and oxidase crosstalk in cardiovascular diseases: novel therapeutic targets. Nat Rev Cardiol 2020, 17, 170–194. [Google Scholar] [CrossRef] [PubMed]
- Fibbi, B.; Marroncini, G.; Naldi, L.; Peri, A. The Yin and Yang effect of the apelinergic system in oxidative stress. Int J Mol Sci 2023, 24, 4745. [Google Scholar] [CrossRef] [PubMed]
- Qiu, M.; Chen, J.; Li, X.; Zhuang, J. Intersection of the ubiquitin-proteasome system with oxidative stress in cardiovascular disease. Int J Mol Sci 2022, 23, 12197. [Google Scholar] [CrossRef] [PubMed]
- Szyller, J.; Jagielski, D.; Bil-Lula, I. Antioxidants in arrhythmia treatment-still a controversy? A review of selected clinical and laboratory research. Antioxidants 2022, 11, 1109. [Google Scholar] [CrossRef] [PubMed]
- Adameova, A.; Shah, A.K.; Dhalla, N.S. Role of oxidative stress in the genesis of ventricular arrhythmias. Int J Mol Sci 2020, 21, 4200. [Google Scholar] [CrossRef] [PubMed]
- Luan, X.; Chen, P.; Miao, L.; Yuan, X.; Yu, C.; Di, G. Ferroptosis in organ ischemia-reperfusion injuries: recent advancements and strategies. Mol Cell Biochem 2025, 480, 19–41. [Google Scholar] [CrossRef]
- Wang, R.; Chen, X.; Li, X.; Wang, K. Molecular therapy of cardiac ischemia-reperfusion injury based on mitochondria and ferroptosis. J Mol Med 2023, 101, 1059–1071. [Google Scholar] [CrossRef] [PubMed]
- Fratta Pasini, A.M.; Stranieri, C.; Busti, F.; Di Leo, E.G.; Girelli, D.; Cominacini, L. New insights into the role of ferroptosis in cardiovascular diseases. Cells 2023, 12, 867. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Yan, Y.; Niu, F.; Wang, Y.; Chen, X.; Su, G.; Liu, Y.; Zhao, X.; Qian, L.; Liu, P.; Xiong, Y. Ferroptosis: a cell death connecting oxidative stress, inflammation and cardiovascular diseases. Cell Death Discov 2021, 7, 193. [Google Scholar] [CrossRef] [PubMed]
- Lillo-Moya, J.; Rojas-Solé, C.; Muñoz-Salamanca, D.; Panieri, E.; Saso, L.; Rodrigo, R. Targeting ferroptosis against ischemia/reperfusion cardiac injury. Antioxidants 2021, 10, 667. [Google Scholar] [CrossRef]
- Tian, K.; Yang, Y.; Zhou, K.; Deng, N.; Tian, Z.; Wu, Z.; Liu, X.; Zhang, F.; Jiang, Z. The role of ROS-induced pyroptosis in CVD. Front Cardiovasc Med 2023, 10, 1116509. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, J.; Zhang, D.; Yu, P.; Zhang, J.; Yu, S. Research progress on the role of pyroptosis in myocardial ischemia-reperfusion injury. Cells 2022, 11, 3271. [Google Scholar] [CrossRef] [PubMed]
- Adameova, A.; Horvath, C.; Abdul-Ghani, S.; Varga, Z.V.; Suleiman, M.S.; Dhalla, N.S. Interplay of oxidative stress and necrosis-like cell death in cardiac ischemia/reperfusion injury: A focus on necroptosis. Biomedicines 2022, 10, 127. [Google Scholar] [CrossRef]
- Cinato, M.; Andersson, L.; Miljanovic, A.; Laudette, M.; Kunduzova, O.; Borén, J.; Levin, M.C. Role of perilipins in oxidative stress-implications for cardiovascular disease. Antioxidants 2024, 13, 209. [Google Scholar] [CrossRef]
- Rongjin, H.; Feng, C.; Jun, K.; Shirong, L. Oxidative stress-induced protein of SESTRIN2 in cardioprotection effect. Dis Markers 2022, 2022, 7439878. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Liu, Y.; Men, H.; Zheng, Y. Protective mechanism of humanin against oxidative stress in aging-related cardiovascular diseases. Front Endocrinol 2021, 12, 683151. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, M.; Liang, Y.; Wang, C.; Naruse, K.; Takahashi, K. Treatment of oxidative stress with exosomes in myocardial ischemia. Int J Mol Sci 2021, 22, 1729. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Kang, P.M. Oxidative stress and antioxidant treatments in cardiovascular diseases. Antioxidants 2020, 9, 1292. [Google Scholar] [CrossRef]
- Wu, W.; Lai, L.; Xie, M.; Qiu, H. Insights of heat shock protein 22 in the cardiac protection against ischemic oxidative stress. Redox Biol 2020, 34, 101555. [Google Scholar] [CrossRef] [PubMed]
- Kura, B.; Szeiffova Bacova, B.; Kalocayova, B.; Sykora, M.; Slezak, J. Oxidative stress-responsive microRNAs in heart injury. Int J Mol Sci 2020, 21, 358. [Google Scholar] [CrossRef] [PubMed]
- Haramaki, N.; Stewart, D.B.; Aggarwal, S.; Ikeda, H.; Reznick, A.Z.; Packer, L. Networking antioxidants in the isolated rat heart are selectively depleted by ischemia-reperfusion. Free Radic Biol Med 1998, 25, 329–339. [Google Scholar] [CrossRef]
- Dhalla, N.S.; Golfman, L.; Takeda, S.; Takeda, N.; Nagano, M. Evidence for the role of oxidative stress in acute ischemic heart disease: A brief review. Can J Cardiol 1999, 15, 587–593. [Google Scholar]
- Saini, H.K.; Machackova, J.; Dhalla, N.S. Role of reactive oxygen species in ischemic preconditioning of subcellular organelles in the heart. Antioxid Redox Signal 2004, 6, 393–404. [Google Scholar] [CrossRef] [PubMed]
- Bhullar, S.K.; Shah, A.K.; Dhalla, N.S. Role of angiotensin II in the development of subcellular remodeling in heart failure. Explor Med 2021, 2, 352–371. [Google Scholar] [CrossRef]
- Tappia, P.S.; Shah, A.K.; Ramjiawan, B.; Dhalla, N.S. Modification of ischemia/reperfusion-induced alterations in subcellular organelles by ischemic preconditioning. Int J Mol Sci 2022, 23, 3425. [Google Scholar] [CrossRef] [PubMed]
- Bhosale, G.; Sharpe, J.A.; Sundier, S.; Duchen, M. Calcium signaling as mediator of cell energy demand and a trigger to cell death. Ann NY Acad Sci 2015, 1350, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Badalzadeh, R.; Mokhtari, B.; Yavari, R. Contribution of apoptosis in myocardial reperfusion injury and loss of cardioprotection in diabetes mellitus. J Physiol Sci 2015, 65, 201–215. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, R.; Guardigli, G.; Mele, D.; Percoco, G.F.; Ceconi, C.; Curello, S. Oxidative stress during myocardial ischemia and heart failure. Curr Pharm Des 2004, 10, 1699–1711. [Google Scholar] [CrossRef] [PubMed]
- Neri, M.; Fineschi, V.; Di Paolo, M.; Pomara, C.; Riezzo, I.; Turillazzi, E.; Cerretani, D. Cardiac oxidative stress and inflammation cytokines response after myocardial infarction. Curr Vasc Pharmacol 2015, 13, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhang, F.; Zhou, H.; Hu, Y.; Guo, D.; Fang, X.; Chen, Y. Interplay of TNF-α, soluble TNF receptors and oxidative stress in coronary chronic total occlusion of the oldest patients with coronary heart disease. Cytokine 2020, 125, 154836. [Google Scholar] [CrossRef]
- Xiong, W.; Qu, Y.; Chen, H.; Qian, J. Insight into long noncoding RNA-miRNA-mRNA axes in myocardial ischemia-reperfusion injury: The implications for mechanism and therapy. Epigenomics 2019, 11, 1733–1748. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Sun, W.; Guo, Z.; Liu, B.; Yu, H.; Zhang, J. Long noncoding RNAs in myocardial ischemia-reperfusion inury. Oxidative Med Cell Longev 2021, 2021, 8889123. [Google Scholar] [CrossRef]
- Li, Q.; Li, Z.; Fan, Z.; Yang, Y.; Lu, C. Involvement of non-coding RNAs in the pathogenesis of myocardial ischemia/reperfusion injury. Int J Mol Med 2021, 47, 42. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.F.; Yoshioka, J. The emerging role of thioredoxin-interacting protein in myocardial ischemia-reperfusion injury. J Cardiovasc Pharmacol Ther 2017, 22, 219–229. [Google Scholar] [CrossRef]
- Zhang, C.; He, M.; Ni, L.; He, K.; Su, K.; Deng, Y.; Li, Y.; Xia, H. The role of arachidonic acid metabolism in myocardial ischemia-reperfusion injury. Cell Biochem Biophys 2020, 78, 255–265. [Google Scholar] [CrossRef]
- Bartekova, M.; Adameova, A.; Gorbe, A.; Ferenczyova, K.; Pechanova, O.; Lazou, A.; Dhalla, N.S.; Ferdinandy, P.; Giricz, Z. Natural and synthetic antioxidants targeting cardiac oxidative stress and redox signaling in cardiometabolic diseases. Free Radic Biol Med 2021, 169, 446–477. [Google Scholar] [CrossRef]
- Dubois-Deruy, E.; Peugnet, V.; Turkieh, A.; Pinet, F. Oxidative stress in cardiovascular diseases. Antioxidants 2020, 9, 864. [Google Scholar] [CrossRef] [PubMed]
- Kleikers, P.W.M.; Wingler, K.; Hermans, J.J.R.; Diebold, I.; Altenhofer, S.; Radermacher, K.A.; Janssen, B.; Gorlach, A.; Schmidt, H.H.H.W. NADPH oxidases as a source of oxidative stress and molecular target in ischemia/reperfusion injury. J Mol Med 2012, 90, 1391–1406. [Google Scholar] [CrossRef]
- Yang, F.; Smith, M.J. Metal profiling in coronary ischemia-reperfusion injury: Implications for KEAP1/NRF2 regulated redox signaling. Free Radic Biol Med 2024, 210, 158–171. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Huang, C.; Liu, H.; Zhang, M.; Liu, L.; Zhai, Y.; Zhang, J.; Yang, J.; Yang, J. The mechanism of the NFAT transcription factor family involved in oxidative stress response. J Cardiol 2024, 83, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Pan, W.; Zhang, Y.; Tan, M.; Yin, Y.; Li, Y.; Zhang, L.; Han, L.; Bai, J.; Jiang, T.; Li, H. Comprehensive overview of Nrf2-related epigenetic regulations involved in ischemia-reperfusion injury. Theranostics 2022, 12, 6626–6645. [Google Scholar] [CrossRef] [PubMed]
- Sadrkhanloo, M.; Entezari, M.; Orouei, S.; Zabolian, A.; Mirzaie, A.; Maghsoudloo, A.; Raesi, R.; Asadi, N.; Hashemi, M.; Zarrabi, A.; Khan, H.; Mirzaei, S.; Samarghandian, S. Targeting Nrf2 in ischemia-reperfusion alleviation: From signaling networks to therapeutic targeting. Life Sci 2022, 300, 120561. [Google Scholar] [CrossRef] [PubMed]
- Mata, A.; Cadenas, S. The antioxidant transcription factor Nrf2 in cardiac ischemia-reperfusion injury. Int J Mol Sci 2021, 22, 11939. [Google Scholar] [CrossRef]
- Yarmohammadi, F.; Hayes, A.W.; Karimi, G. The cardioprotective effects of hydrogen sulfide by targeting endoplasmic reticulum stress and the Nrf2 signaling pathway: A review. Biofactors 2021, 47, 701–712. [Google Scholar] [CrossRef]
- Ucar, B.I.; Ucar, G.; Saha, S.; Buttari, B.; Profumo, E.; Saso, L. Pharmacological protection against ischemia-reperfusion injury by regulating the Nrf2-Keap1-ARE signaling pathway. Antioxidants 2021, 10, 823. [Google Scholar] [CrossRef] [PubMed]
- Tavakoli, R.; Tabeshpour, J.; Asili, J.; Shakeri, A.; Sahebkar, A. Cardioprotective effects of natural products via the Nrf2 signaling pathway. Curr Vasc Pharmacol 2021, 19, 525–541. [Google Scholar] [CrossRef]
- Zhang, X.; Yu, Y.; Lei, H.; Cai, Y.; Shen, J.; Zhu, P.; He, Q.; Zhao, M. The Nrf-2/HO-1 signaling axis: A ray of hope in cardiovascular diseases. Cardiol Res Pract 2020, 2020, 5695723. [Google Scholar] [CrossRef] [PubMed]
- Kakavand, H.; Aghakouchakzadeh, M.; Coons, J.C.; Talasaz, A.H. Pharmacologic prevention of myocardial ischemia-reperfusion injury in patients with acute coronary syndrome undergoing percutaneous coronary intervention. J Cardiovasc Pharmacol 2021, 77, 430–449. [Google Scholar] [CrossRef] [PubMed]
- Osorio-Llanes, E.; Villamizar-Villamizar, W.; Ospino Guerra, M.C.; Díaz-Ariza, L.A.; Castiblanco-Arroyave, S.C.; Medrano, L.; Mengual, D.; Belón, R.; Castellar-López, J.; Sepúlveda, Y.; Vásquez-Trincado, C.; Chang, A.Y.; Bolívar, S.; Mendoza-Torres, E. Effects of metformin on ischemia/reperfusion injury: New evidence and mechanisms. Pharmaceuticals 2023, 16, 1121. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Zhang, D. Research progress on the effects of novel hypoglycemic drugs in diabetes combined with myocardial ischemia/reperfusion injury. Ageing Res Rev 2023, 86, 101884. [Google Scholar] [CrossRef]
- Dragasevic, N.; Jakovljevic, V.; Zivkovic, V.; Draginic, N.; Andjic, M.; Bolevich, S.; Jovic, S. The role of aldosterone inhibitors in cardiac ischemia-reperfusion injury. Can J Physiol Pharmacol 2021, 99, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Zhu, C.; Wang, W.; Li, M.; Ma, C.; Gao, B. SIRT1 is a regulator of autophagy: Implications for the progression and treatment of myocardial ischemia-reperfusion. Pharmacol Res 2024, 199, 106957. [Google Scholar] [CrossRef]
- Lv, J.; Zhu, X.; Xing, C.; Chen, Y.; Bian, H.; Yin, H.; Gu, X.; Su, L. Stimulator of interferon genes (STING): Key therapeutic targets in ischemia/reperfusion injury. Biomed Pharmacother 2023, 167, 115458. [Google Scholar] [CrossRef] [PubMed]
- Ding, R.; Wu, W.; Sun, Z.; Li, Z. AMP-activated protein kinase: An attractive therapeutic target for ischemia-reperfusion injury. Eur J Pharmacol 2020, 888, 173484. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Liu, Y.; Liu, Y.; Huang, H.; Roy, S.; Song, Z.; Guo, B. Recent advances in nanomedicines for imaging and therapy of myocardial ischemia-reperfusion injury. J Control Release 2023, 353, 563–590. [Google Scholar] [CrossRef]
- Russo, I.; Barale, C.; Melchionda, E.; Penna, C.; Pagliaro, P. Platelets and cardioprotection: The role of nitric oxide and carbon oxide. Int J Mol Sci 2023, 24, 6107. [Google Scholar] [CrossRef]
- Ryter, S.W. Therapeutic potential of heme oxygenase-1 and carbon monoxide in acute organ injury, Critical illness, and inflammatory disorders. Antioxidants 2020, 9, 1153. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Li, Y.; Zeng, Y.; Zhou, X.; Zhang, S.; Ren, Y. Construction of preclinical evidence for propofol in the treatment of reperfusion injury after acute myocardial infarction: A systematic review and meta-analysis. Biomed Pharmacother 2024, 174, 116629. [Google Scholar] [CrossRef] [PubMed]
- Yue, H.; Zhang, Q.; Chang, S.; Zhao, X.; Wang, M.; Li, W. Adiponectin protects against myocardial ischemia-reperfusion injury: a systematic review and meta-analysis of preclinical animal studies. Lipids Health Dis 2024, 23, 51. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.Y.; Liu, Z.; Lu, J.H.; Yang, S.Y.; Hu, X.Y.; Liang, G.Y. The function of circular RNAs in myocardial ischemia-reperfusion injury: Underlying mechanisms and therapeutic advancement. Cardiovasc Drugs Ther 2024. [On line ahed of print]. [Google Scholar] [CrossRef] [PubMed]
- Ge, T.; Ning, B.; Wu, Y.; Chen, X.; Qi, H.; Wang, H.; Zhao, M. MicroRNA-specific therapeutic targets and biomarkers of apoptosis following myocardial ischemia-reperfusion injury. Mol Cell Biochem 2024, 479, 2499–2521. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.; Cai, R.P.; Su, Y.M.; Wu, Q.; Su, Q. Mesenchymal stem cell-derived exosomal noncoding RNAs as alternative treatments for myocardial ischemia-reperfusion injury: Current status and future perspectives. J Cardiovasc Transl Res 2023, 16, 1085–1098. [Google Scholar] [CrossRef]
- Su, X.; Zhou, M.; Li, Y.; Zhang, J.; An, N.; Yang, F.; Zhang, G.; Yuan, C.; Chen, H.; Wu, H.; Xing, Y. Protective effects of natural products against myocardial ischemia/reperfusion: Mitochondria-targeted therapeutics. Biomed Pharmacother 2022, 149, 112893. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Yu, L.T.; Cheng, B.R.; Xu, J.L.; Cai, Y.; Jin, J.L.; Feng, R.L.; Xie, L.; Qu, X.Y.; Li, D.; Liu, J.; Li, Y.; Cui, X.Y.; Lu, J.J.; Zhou, K.; Lin, Q.; Wan, J. Promising therapeutic candidate for myocardial ischemia/reperfusion injury: What are the possible mechanisms and roles of phytochemicals? Front Cardiovasc Med 2022, 8, 792592. [Google Scholar] [CrossRef] [PubMed]
- Mauerhofer, C.; Grumet, L.; Schemmer, P.; Leber, B.; Stiegler, P. Combating ischemia-reperfusion injury with micronutrients and natural compounds during solid organ transplantation: Data of clinical trials and lessons of preclinical findings. Int J Mol Sci 2021, 22, 10675. [Google Scholar] [CrossRef]
- Yoshitomi, T.; Nagasaki, Y. Self-assembling antioxidants for ischemia-reperfusion injuries. Antioxid Redox Signal 2022, 36, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Ertugrul, I.A.; van Suylen, V.; Damman, K.; de Koning, M.L.Y.; van Goor, H.; Erasmus, M.E. Donor heart preservation with hydrogen sulfide: A systematic review and meta-analysis. Int J Mol Sci 2021, 22, 5737. [Google Scholar] [CrossRef] [PubMed]
- An, N.; Zhang, G.; Li, Y.; Yuan, C.; Yang, F.; Zhang, L.; Gao, Y.; Xing, Y. Promising antioxidative effect of berberine in cardiovascular diseases. Front Pharmacol 2022, 13, 865353. [Google Scholar] [CrossRef]
- Baliou, S.; Adamaki, M.; Ioannou, P.; Pappa, A.; Panayiotidis, M.I.; Spandidos, D.A.; Christodoulou, I.; Kyriakopoulos, A.M.; Zoumpourlis, V. Protective role of taurine against oxidative stress. Mol Med Rep 2021, 24, 605. [Google Scholar] [CrossRef]
- Prem, P.N.; Sivakumar, B.; Boovarahan, S.R.; Kurian, G.A. Recent advances in potential of Fisetin in the management of myocardial ischemia-reperfusion injury-A systematic review. Phytomedicine 2022, 101, 154123. [Google Scholar] [CrossRef] [PubMed]
- Ferenczyova, K.; Kalocayova, B.; Bartekova, M. Potential implications of quercetin and its derivatives in cardioprotection. Int J Mol Sci 2020, 21, 1585. [Google Scholar] [CrossRef]
- Sun, Z.; Wang, X. Protective effects of polydatin on multiple organ ischemia-reperfusion injury. Bioorg Chem 2020, 94, 103485. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Xu, Y.; Liehn, E.A.; Rusu, M. Vitamin C as scavenger of reactive oxygen species during healing after myocardial infarction. Int J Mol Sci 2024, 25, 3114. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.K.; Dhalla, N.S. Effectiveness of some vitamins in the prevention of cardiovascular disease: A narrative review. Front Physiol 2021, 12, 729255. [Google Scholar] [CrossRef] [PubMed]
- Kura, B.; Slezak, J. The protective role of molecular hydrogen in ischemia/reperfusion injury. Int J Mol Sci 2024, 25, 7884. [Google Scholar] [CrossRef]
- Saengsin, K.; Sittiwangkul, R.; Chattipakorn, S.C.; Chattipakorn, N. Hydrogen therapy as a potential therapeutic intervention in heart disease: from the past evidence to future application. Cell Mol Life Sci 2023, 80, 174. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Li, X.; Zhang, Z.; Liu, L.; Zhou, Y.; Liu, F. Protective mechanism and clinical application of hydrogen in myocardial ischemia-reperfusion injury. Pak J Biol Sci 2020, 23, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Wu, S.; Mao, C.; Qu, Y.; Xu, Z.; Xie, Y.; Jiang, D.; Song, Y. Therapeutic potential of hydrogen sulfide in ischemia and reperfusion injury. Biomolecules 2024, 14, 740. [Google Scholar] [CrossRef]
- Gheitasi, I.; Akbari, G.; Savari, F. Physiological and cellular mechanisms of ischemic preconditioning microRNAs-mediated in underlying of ischemia/reperfusion injury in different organs. Mol Cell Biochem 2024. [Online ahead of print]. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.B.; Hryshko, L.; Freed, D.; Dhalla, N.S. Activation of proteolytic enzymes and depression of the sarcolemma Na+-K+-ATPase in ischemia-reperfused heart may be mediated through oxidative stress. Can J Physiol Pharmacol 2012, 90, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Dixon, I.M.C.; Kaneko, M.; Hata, T.; Panagia, V.; Dhalla, N.S. Alterations in cardiac membrane Ca2+ transport during oxidative stress. Mol Cell Biochem 1990, 99, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, T.; Dhalla, N.S. Effect of oxygen free radicals on cardiac contractile activity and sarcolemmal Na+-Ca2+ exchange. J Cardiovasc Pharmacol Ther 1996, 1, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, T.; Dhalla, N.S. Relationship between mechanical dysfunction and depression of sarcolemmal Ca2+-pump activity in hearts perfused with oxygen free radicals. Mol Cell Biochem 1996, 160/161, 179–185. [Google Scholar] [CrossRef]
- Temsah, R.M.; Netticadan, T.; Chapman, D.; Takeda, S.; Mochizuki, S.; Dhalla, N.S. Alterations in sarcoplasmic reticulum function and gene expression in ischemic-reperfused rat heart. Am J Physiol 1999, 277, H584–H594. [Google Scholar] [CrossRef]
- Makazan, Z.; Saini, H.K.; Dhalla, N.S. Role of oxidative stress in alterations of mitochondrial function in ischemic-reperfused hearts. Am J Physiol Heart Circ Physiol 2007, 292, H1986–H1994. [Google Scholar] [CrossRef]
- Maddika, S.; Elimban, V.; Chapman, D.; Dhalla, N.S. Role of oxidative stress in ischemia-reperfusion-induced alterations in myofibrillar ATPase activities and gene expression in the heart. Can J Physiol Pharmacol 2009, 87, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Kaneko, M.; Chapman, D.C.; Dhalla, N.S. Alterations in cardiac contractile proteins due to oxygen free radicals. Biochim. Biophys. Acta. 1991, 1074, 95–100. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Effect of ischemia-reperfusion with or without oxyradical scavenger mixture (SOD plus CAT) on cardiac function (A and B) and myocardial markers for oxidative stress (C and D). Hearts were subjected to 30 min global ischemia followed by 60 min reperfusion (I/R) in the absence or presence of 80 µg/mL superoxide dismutase (SOD) plus 10 µg/mL catalase (CAT). Control hearts in each experiment were perfused with normal medium for appropriate time. The data are based on the analysis of information in Dhalla et al. [87]. LV = left ventricle; DP= developed pressure; EDP= end diastolic pressure; MDA = malondialdehyde, * p < 0.05 vs. respective control value, † p < 0.05 vs. respective I/R value.
Figure 1.
Effect of ischemia-reperfusion with or without oxyradical scavenger mixture (SOD plus CAT) on cardiac function (A and B) and myocardial markers for oxidative stress (C and D). Hearts were subjected to 30 min global ischemia followed by 60 min reperfusion (I/R) in the absence or presence of 80 µg/mL superoxide dismutase (SOD) plus 10 µg/mL catalase (CAT). Control hearts in each experiment were perfused with normal medium for appropriate time. The data are based on the analysis of information in Dhalla et al. [87]. LV = left ventricle; DP= developed pressure; EDP= end diastolic pressure; MDA = malondialdehyde, * p < 0.05 vs. respective control value, † p < 0.05 vs. respective I/R value.
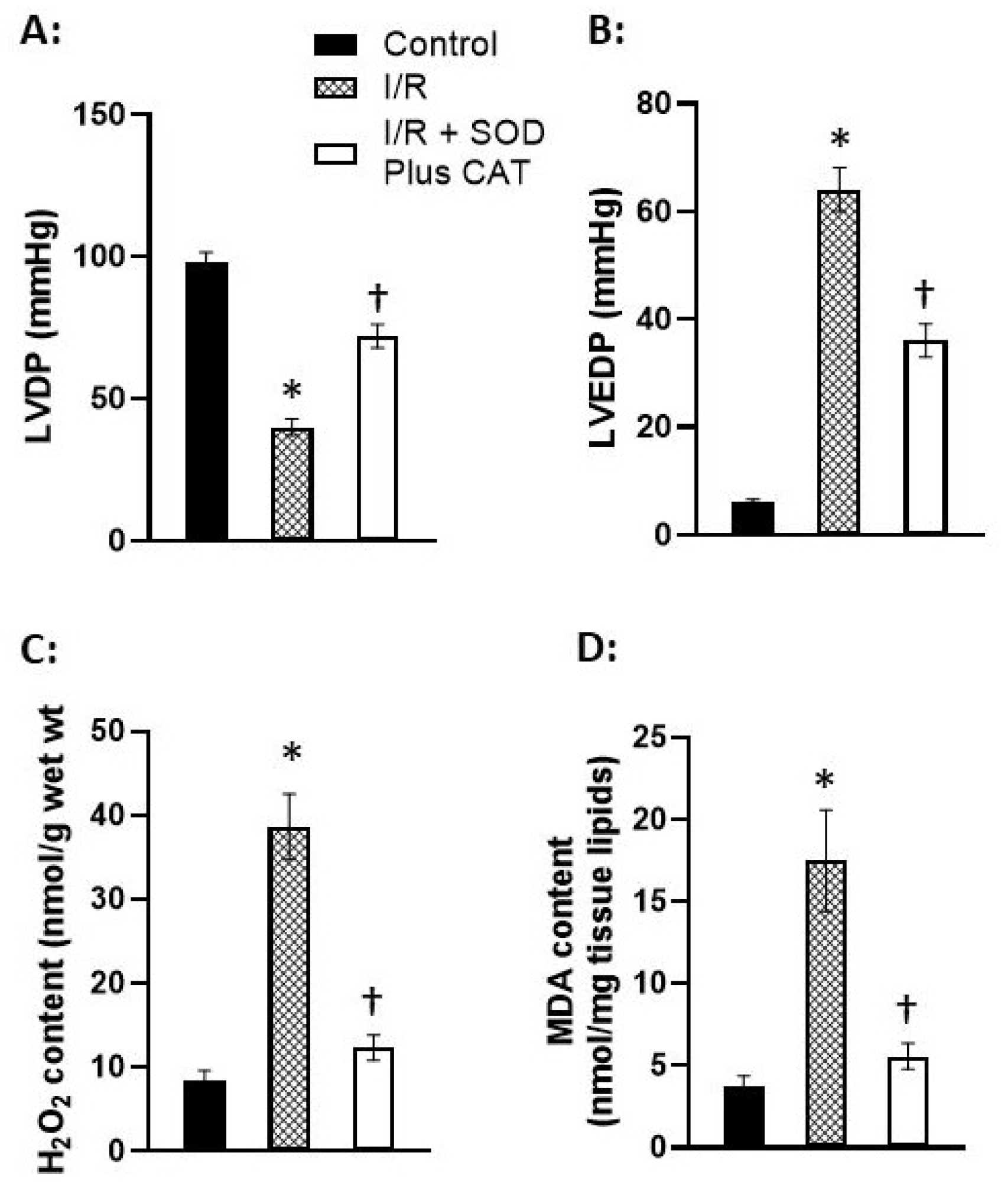
Figure 2.
Effect of ischemia-reperfusion (I/R) with or without some antioxidants (A, B and C) as well as perfusion with xanthine plus xanthine oxidase (X + XO) or H2O2 on sarcolemmal Na+-K+ ATPase activity (D) and protease activities (E and F) in isolated perfused hearts. Hearts were subjected to 30 min global ischemia followed by 30 min reperfusion (I/R) in the absence and presence of 100 µM N-acetylcysteine (NAC) or 300 µM mercaptopropionylglycine (MGP). Hearts were also perfused for 30 min with 2 mM xanthine (X) plus 60 mU/mL xanthine oxidase (XO) mixture or 100 mM H2O2 followed by 30 min reperfusion. Control hearts in each experiment were perfused with normal medium for 60 min. The data are based on the analysis of information in Singh et al. [145]. MMP = matrix metalloproteinase, *p < 0.05 vs. respective control value, †p < 0.05 vs. respective I/R value.
Figure 2.
Effect of ischemia-reperfusion (I/R) with or without some antioxidants (A, B and C) as well as perfusion with xanthine plus xanthine oxidase (X + XO) or H2O2 on sarcolemmal Na+-K+ ATPase activity (D) and protease activities (E and F) in isolated perfused hearts. Hearts were subjected to 30 min global ischemia followed by 30 min reperfusion (I/R) in the absence and presence of 100 µM N-acetylcysteine (NAC) or 300 µM mercaptopropionylglycine (MGP). Hearts were also perfused for 30 min with 2 mM xanthine (X) plus 60 mU/mL xanthine oxidase (XO) mixture or 100 mM H2O2 followed by 30 min reperfusion. Control hearts in each experiment were perfused with normal medium for 60 min. The data are based on the analysis of information in Singh et al. [145]. MMP = matrix metalloproteinase, *p < 0.05 vs. respective control value, †p < 0.05 vs. respective I/R value.
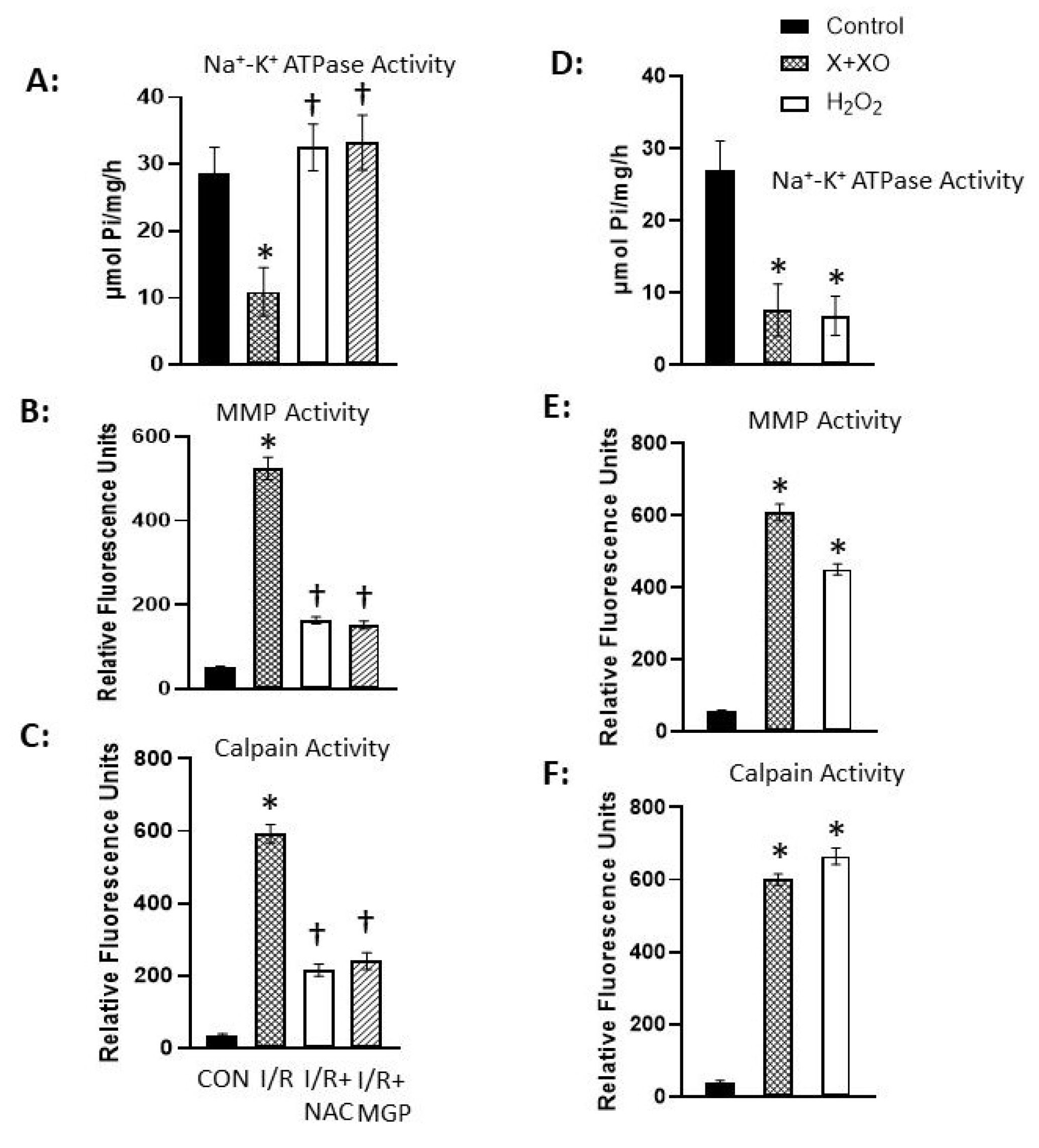
Figure 3.
Influence of ischemia-reperfusion (I/R) with or without oxyradical scavenger (SOD plus CAT) as well as perfusion with xanthine plus xanthine oxidase (X + XO) or H2O2 on sarcolemmal Na+-Ca2+ exchange, Ca2+-uptake and Ca2+-stimulated ATPase activities in isolated perfused hearts. Hearts were subjected to 30 min global ischemia followed by 5 min reperfusion (I/R) in the absence or presence of 50 U/mL superoxide dismutase (SOD) plus 50 U/mL catalase (CAT). Hearts were also perfused with 2 mM xanthine (X) plus 100 mU/mL xanthine oxidase for 20 min in the absence or presence of SOD plus CAT. Control hearts in each experiment were perfused with normal medium for appropriate period. The data are based on the analysis of information in our papers Dixon et al. [146], Matsubara and Dhalla [147] and Matsubara and Dhalla [148]. * p < 0.05 vs. respective control, † p < 0.05 vs. respective I/R or X + XO group.
Figure 3.
Influence of ischemia-reperfusion (I/R) with or without oxyradical scavenger (SOD plus CAT) as well as perfusion with xanthine plus xanthine oxidase (X + XO) or H2O2 on sarcolemmal Na+-Ca2+ exchange, Ca2+-uptake and Ca2+-stimulated ATPase activities in isolated perfused hearts. Hearts were subjected to 30 min global ischemia followed by 5 min reperfusion (I/R) in the absence or presence of 50 U/mL superoxide dismutase (SOD) plus 50 U/mL catalase (CAT). Hearts were also perfused with 2 mM xanthine (X) plus 100 mU/mL xanthine oxidase for 20 min in the absence or presence of SOD plus CAT. Control hearts in each experiment were perfused with normal medium for appropriate period. The data are based on the analysis of information in our papers Dixon et al. [146], Matsubara and Dhalla [147] and Matsubara and Dhalla [148]. * p < 0.05 vs. respective control, † p < 0.05 vs. respective I/R or X + XO group.
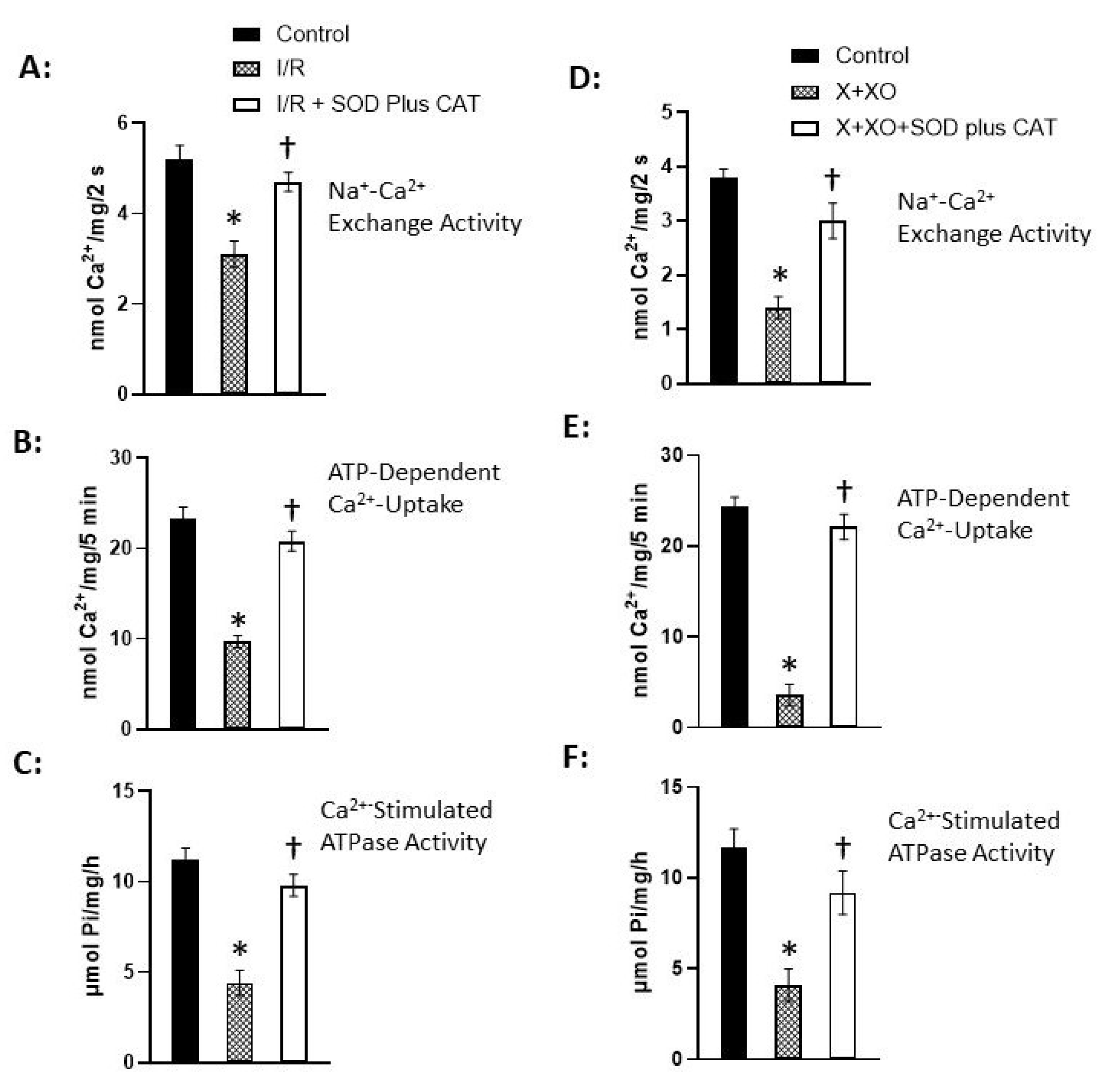
Figure 4.
Effect of ischemia-reperfusion (I/R) with or without oxyradical scavenger (SOD plus CAT) on sarcoplasmic reticular Ca2+-uptake and Ca2+-release activities and ryanodine binding in isolated perfused hearts. Hearts were subjected to 30 min global ischemia followed by 60 min reperfusion (I/R) in the absence or presence of 50 U/mL superoxide dismutase (SOD) and 75 U/mL catalase. Control hearts in each experiment were perfused with normal medium for appropriate time period. The data are based on the analysis of information in our paper Temsah et al. [149]. * p < 0.05 vs. respective control value, † p < 0.05 vs. respective I/R value.
Figure 4.
Effect of ischemia-reperfusion (I/R) with or without oxyradical scavenger (SOD plus CAT) on sarcoplasmic reticular Ca2+-uptake and Ca2+-release activities and ryanodine binding in isolated perfused hearts. Hearts were subjected to 30 min global ischemia followed by 60 min reperfusion (I/R) in the absence or presence of 50 U/mL superoxide dismutase (SOD) and 75 U/mL catalase. Control hearts in each experiment were perfused with normal medium for appropriate time period. The data are based on the analysis of information in our paper Temsah et al. [149]. * p < 0.05 vs. respective control value, † p < 0.05 vs. respective I/R value.
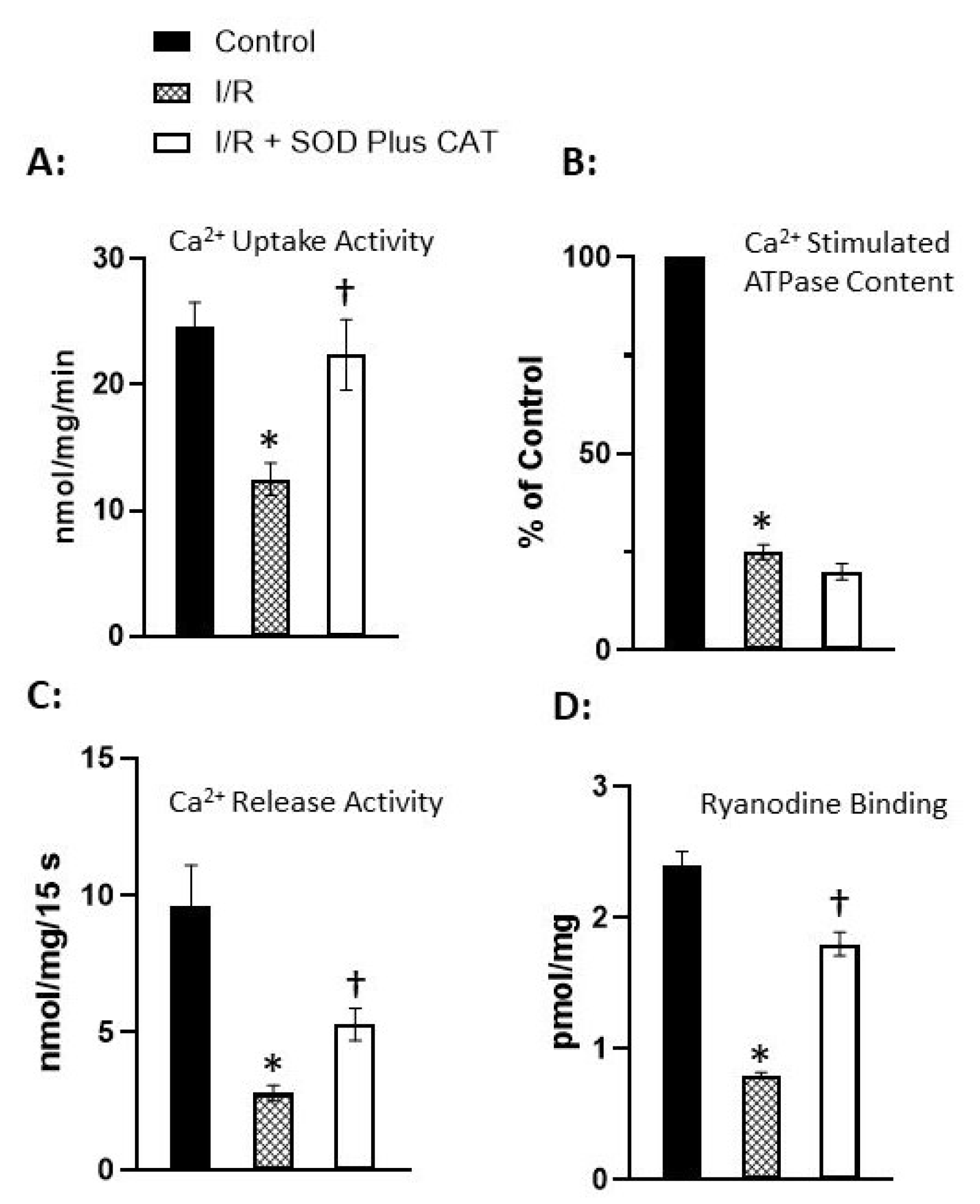
Figure 5.
Outcome of perfusion with xanthine plus xanthine oxidase (X + XO) or H2O2 on sarcoplasmic reticular Ca2+-uptake and Ca2+-release activities and ryanodine binding in isolated perfused hearts. Hearts were also perfused for 20 min with 2 mM xanthine (X) plus 0.03 U/mL xanthine oxidase or 300 µM H2O2. Control hearts in each experiment were perfused with normal medium for appropriate time period. The data are based on the analysis of information in our paper Temsah et al. [149]. * p < 0.05 vs. respective control value.
Figure 5.
Outcome of perfusion with xanthine plus xanthine oxidase (X + XO) or H2O2 on sarcoplasmic reticular Ca2+-uptake and Ca2+-release activities and ryanodine binding in isolated perfused hearts. Hearts were also perfused for 20 min with 2 mM xanthine (X) plus 0.03 U/mL xanthine oxidase or 300 µM H2O2. Control hearts in each experiment were perfused with normal medium for appropriate time period. The data are based on the analysis of information in our paper Temsah et al. [149]. * p < 0.05 vs. respective control value.
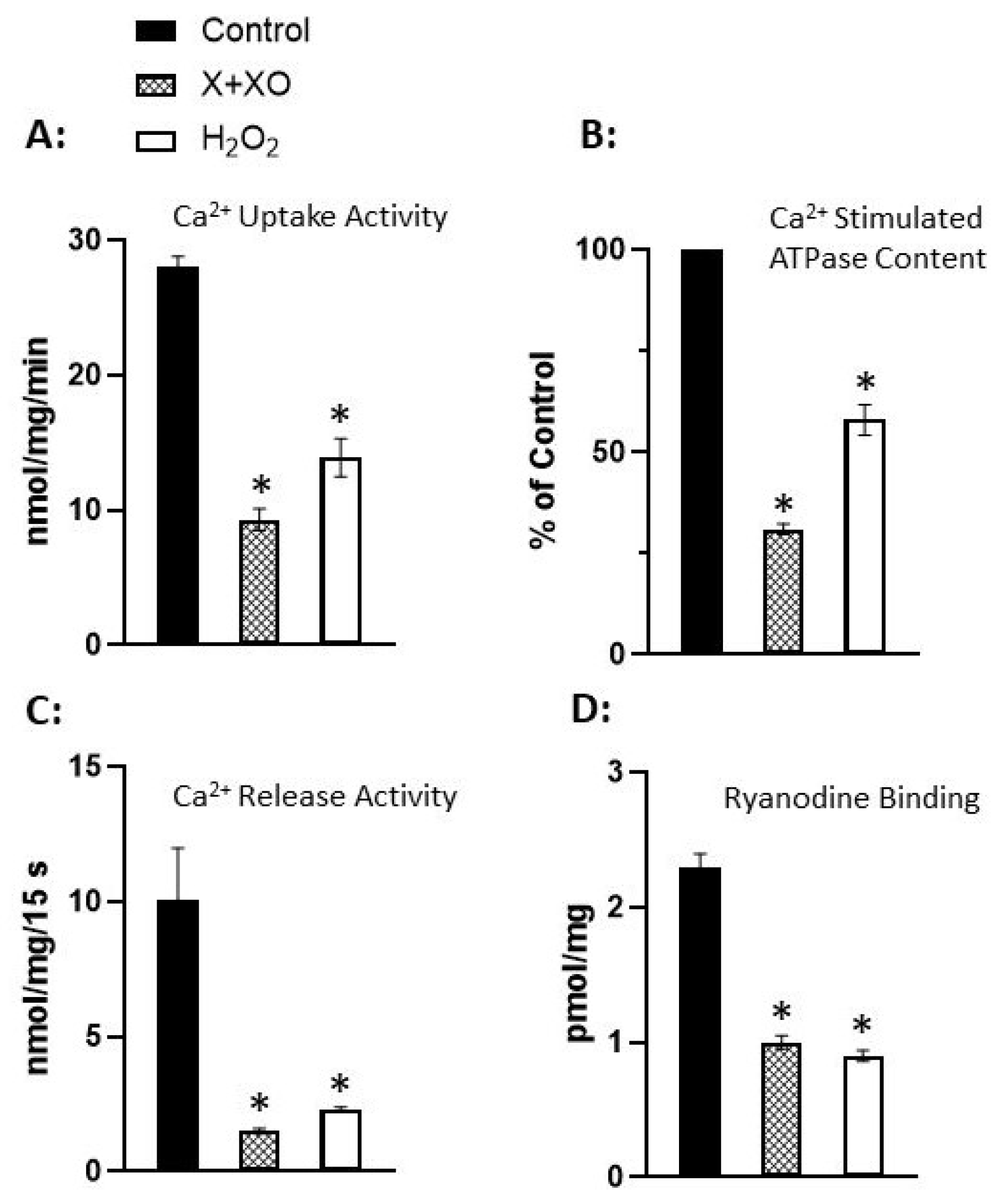
Figure 6.
Effect of ischemia-reperfusion (I/R) in the absence or presence of oxyradical scavenger mixture (SOD plus CAT) as well as perfusion with oxyradical generating mixture (X plus XO) or H2O2 on mitochondrial function in isolated perfused hearts. Hearts were subjected to 30 min global ischemia followed by 30 min reperfusion in the absence or presence of 50 U/mL superoxide dismutase plus 75 U/mL catalase. Hearts were also perfused for 30 min with 2 mM xanthine (X) plus 60 mU/mL oxidase or 100 µM H2O2. Control hearts in each experiment were perfused with normal medium for appropriate time. The data are based on the analysis of information in our paper Makazan et al. [150]. * p < 0.05 vs. respective control value, † p < 0.05 vs. respective I/R value.
Figure 6.
Effect of ischemia-reperfusion (I/R) in the absence or presence of oxyradical scavenger mixture (SOD plus CAT) as well as perfusion with oxyradical generating mixture (X plus XO) or H2O2 on mitochondrial function in isolated perfused hearts. Hearts were subjected to 30 min global ischemia followed by 30 min reperfusion in the absence or presence of 50 U/mL superoxide dismutase plus 75 U/mL catalase. Hearts were also perfused for 30 min with 2 mM xanthine (X) plus 60 mU/mL oxidase or 100 µM H2O2. Control hearts in each experiment were perfused with normal medium for appropriate time. The data are based on the analysis of information in our paper Makazan et al. [150]. * p < 0.05 vs. respective control value, † p < 0.05 vs. respective I/R value.
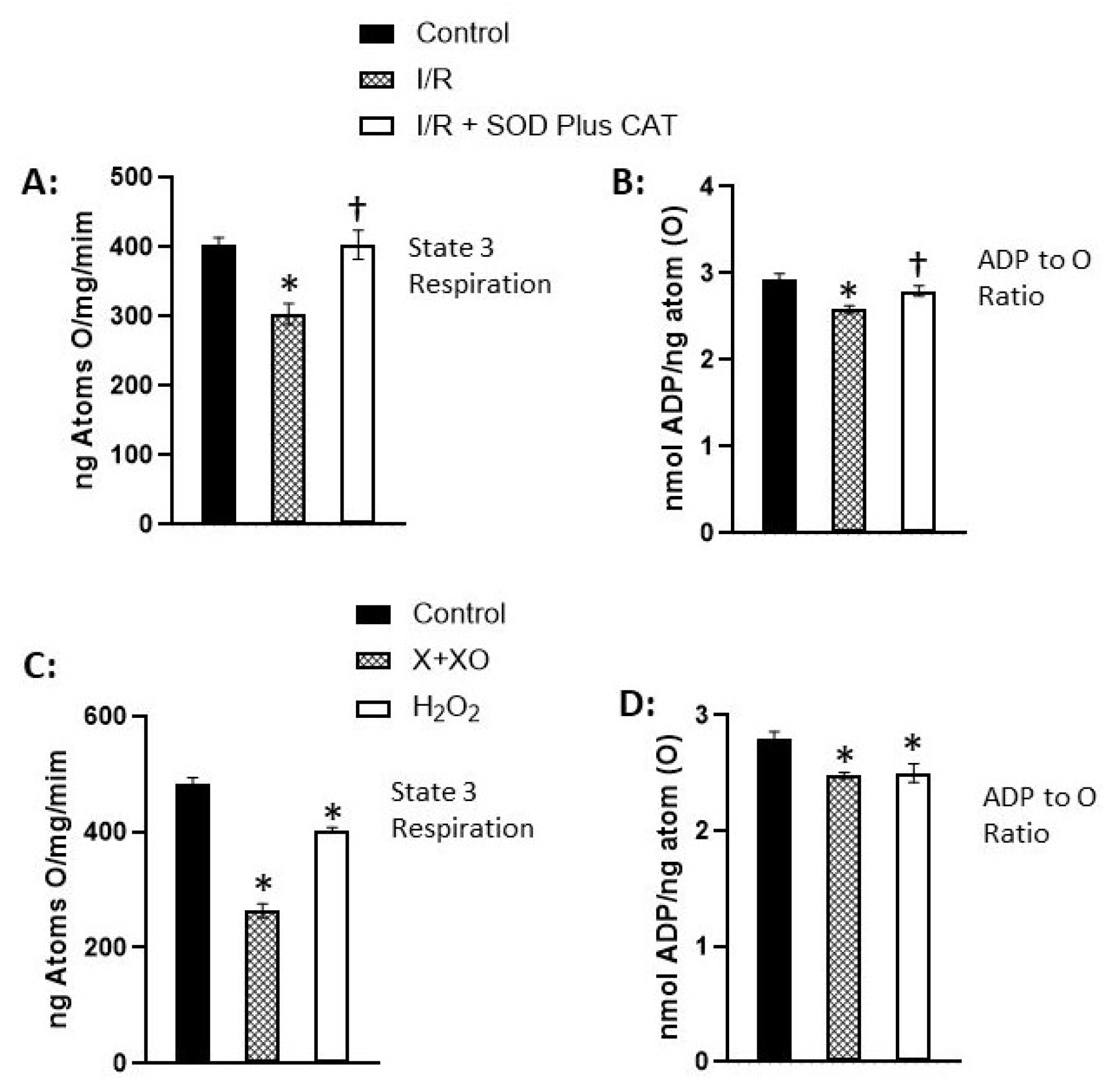
Figure 7.
Influence of ischemia-reperfusion (I/R) with or without oxyradical scavenger and antioxidant as well as perfusion with xanthine plus xanthine oxidase (X + XO) or H2O2 on cardiac function (A) and myofibrillar ATPase activities in isolated perfused hearts. Hearts were subjected to 30 min global ischemia followed by 30 min reperfusion (I/R) in the absence and presence of 80 µg/mL superoxide dismutase (SOD) plus 10 µg/mL catalase (CAT) or 100 µM N-acetylcysteine (NAC). Hearts were also perfused for 30 min with 2 mM xanthine (X) plus 60 mU/mL xanthine oxidase or 100 µM H2O2 followed by 30 min reperfusion. Control hearts in each experiment were perfused with normal medium for appropriate period. The data are based on the analysis of information in our papers Maddika et al. [151] and Suzuki et al. [152]. * p < 0.05 vs. respective control value, † p < 0.05 vs. respective I/R value.
Figure 7.
Influence of ischemia-reperfusion (I/R) with or without oxyradical scavenger and antioxidant as well as perfusion with xanthine plus xanthine oxidase (X + XO) or H2O2 on cardiac function (A) and myofibrillar ATPase activities in isolated perfused hearts. Hearts were subjected to 30 min global ischemia followed by 30 min reperfusion (I/R) in the absence and presence of 80 µg/mL superoxide dismutase (SOD) plus 10 µg/mL catalase (CAT) or 100 µM N-acetylcysteine (NAC). Hearts were also perfused for 30 min with 2 mM xanthine (X) plus 60 mU/mL xanthine oxidase or 100 µM H2O2 followed by 30 min reperfusion. Control hearts in each experiment were perfused with normal medium for appropriate period. The data are based on the analysis of information in our papers Maddika et al. [151] and Suzuki et al. [152]. * p < 0.05 vs. respective control value, † p < 0.05 vs. respective I/R value.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



