
Submitted:
13 January 2025
Posted:
14 January 2025
You are already at the latest version
Abstract
Introduction: The rapid adoption of telerehabilitation in physiotherapy and occupational therapy has transformed healthcare delivery, offering new opportunities for patient-centered care. However, its implementation raises critical ethical and equity-related questions that must be addressed to ensure fair and responsible practices. This review examines how ethical disparities and equity-related challenges are reflected in the existing literature on telerehabilitation.
Objective: To investigate the presence of ethical-disparity and equity-related aspects in the provision of telerehabilitation in physiotherapy and occupational therapy as reflected in the literature.
Methods: A rapid review methodology was employed to explore ethical and equity-related challenges in telerehabilitation. The search included articles published in English and French between 2010 and 2020 from the Medline and Embase databases. Articles were selected based on their relevance to ethical and equity considerations in telerehabilitation. A total of 1,556 sources were initially identified, with 57 articles meeting the eligibility criteria for inclusion in this review. Data were extracted based on variables such as age, gender, ethnicity, morbidity, cost, privacy, confidentiality, and autonomy. The data extraction and analysis were guided by the Progress Plus and Metaverse Equitable Rehabilitation Therapy frameworks. A narrative synthesis approach was used to analyze and discuss the findings. The results highlighted key ethical considerations, including adverse events, patient autonomy, and privacy issues. Equity-related aspects were examined with a significant focus on age demographics, access to rehabilitation services, and gender considerations. Disparities in technology access, socioeconomic status, and ethnicity were also identified.
Conclusions: The review underscores the importance of addressing ethical and equity-related issues in telerehabilitation to ensure a socially just, responsible, and inclusive approach to care. Additionally, it highlights the potential for telerehabilitation to offer personalized interventions that cater to individual patient needs, further advancing equitable and patient-centered rehabilitation practices.
Keywords:
Telehealth
; telerehabilitation
; personalized medicine
; disability
; physiotherapy
; occupational therapy
; ethics
; equity
; rapid review
; digital health
1. Introduction
Telerehabilitation (TR) has become widely used in the world since 2010, particularly for reaching geographically remote populations living in disadvantaged situations [1]. TR has been defined as the provision of rehabilitation services through diverse technological approaches, including the use of various rehabilitation tools for evaluation, assessment, monitoring, prevention, intervention, supervision, education, consultation, and coaching [2]. It has been shown to improve quality of life, maximize functionality, and increase access to rehabilitation services, especially for vulnerable, geographically remote populations and individuals with disabilities [3].
A key aspect of TR is its potential for personalized care, which can address the unique needs of each patient. Tailoring sessions to individual needs, personalized TR offers a more targeted rehabilitation experience [4]. From an equity and ethics perspective, this approach ensures that rehabilitation services are adapted to the specific circumstances of each patient, promoting fairness and accessibility for individuals from diverse backgrounds and varying levels of need. Personalized telerehabilitation, therefore, enhances not only the effectiveness of treatment but also supports ethical and equitable care, ensuring that all patients, regardless of their condition or location, receive appropriate and individualized support [4].
Many studies have reported challenges and barriers to delivering TR services, raising concerns that must be addressed to implement and sustain inclusive, ethical and relevant rehabilitation services for clinicians [5,6]. A scoping review of 22 studies within telemedicine identified four main ethical concerns: confidentiality, accessibility, clinical effectiveness, and the patient-physician relationship [1]. Specific issues arose regarding patient confidentiality and the accessibility of technology, including the absence of reliable high-speed internet, lack of cell phone data plans or lack of up-to-date smartphones that can accommodate telemedicine applications). Moreover, patients with sensory disabilities (e.g., vision, hearing) or dexterity issues may encounter difficulties in using smartphones and certain telemedicine platforms [1]. Moreover, .Nittari's (2020) review on ethical and legal challenges in telemedicine faced by patients highlighted concerns such as the lack of established protocols in telerehabilitation, perceived intrusiveness of monitoring devices, complexity of payment methods and difficulties accessing consultations and treatments in the case of underserved individuals [7]. Other technical and implementation obstacles highlighted by participants included challenges such as insufficient availability of devices at home, limited bandwidth leading to slow connections, and concerns surrounding the privacy and security of both applications and telecommunication channels [8]. Therefore, addressing ethical and equity concerns and obstacles is crucial for the successful implementation and widespread adoption of telerehabilitation services.
While telemedicine has gained substantial attention regarding its potential to enhance healthcare accessibility and delivery, similar considerations have not yet been thoroughly examined for personalized telerehabilitation. As a result, there is a distinct gap in our understanding of the ethical and equity-related issues within telerehabilitation. This rapid review aims to summarize evidence from prior reviews and relevant recent studies, contributing to the development of recommendations for equitable, ethical, and personalized practices in telerehabilitation services.
2. Methodology
This rapid review adheres to the guidelines provided in King et al.'s comprehensive guide [9] and aligns with the Cochrane Rapid Reviews-Interim Guidance from the Cochrane Rapid Reviews Method Group [10]. Rapid reviews, as defined by this guidance, represent a form of knowledge synthesis that expedites the traditional systematic review process by streamlining or omitting specific methods[10]. More detailed information on the review methodology is available in the published protocol [11]. Prospero ID: CRD42020207602.
2.1. Search Strategy
The search process for this rapid review was a collaborative effort involving a librarian from University of Montreal and research team members. The databases Medline and Embase were chosen for their comprehensive coverage of medical literature relevant to telerehabilitation [12]. Essential keywords, including "telerehabilitation" and related terms like "telehealth" and "online-based intervention” were included in the search strategy to ensure a comprehensive search. The search also extended to terms associated with "physiotherapy" and "occupational therapy," contributing to a thorough investigation within the telerehabilitation domain.
2.2. Eligibility Criteria
This review employs a comprehensive approach to telerehabilitation studies involving physiotherapists and occupational therapists. The scope spans diverse age groups, excluding animal studies and includes various technological modalities.
Outcomes cover The International Classification of Functioning, Disability and Health (ICF) domains, in addition to efficacy, technology usability, engagement, acceptance, feasibility, patient satisfaction, health services outcomes, equity, and ethics.
Inclusion criteria for this study, which were detailed elsewhere [11] focus on reviewing articles written in English of French from 2010 to 2020, reflecting the evolution of technology in healthcare. The rationale for this temporal distinction and detailed information on study design criteria are available in the published protocol [11].
2.3. Data Screening and Data Extraction
All identified articles underwent organization and management through Covidence, an online systematic review software[13]. After the completion of database searching, duplicates were removed and two authors (MV and JS) screened all titles and abstracts using the elligibility criteria. Conflicts were resolved through discussion with a third author (MV, JS and DK).
Data was extracted using the Covidence systematic review software and Excel capturing key variables such as study country, design, population, telerehabilitation mode of delivering TR services, intervention descriptions, cost, user digital literacy, use of adaptative equipment, technology access, participant autonomy, data security, ethnicity, adverse events, results, limitations, and ethical concerns related to the use of the technology or the conduct of the research.
The data extraction and analysis in this study were guided by the Metaverse Equitable Rehabilitation THerapy (MERTH) framework, which has five critical domains: 1. Quality of care, 2. health services integration, 3. interoperability, 4. global governance, and 5. Humanization [14]. This framework, developed in two phases, was informed by previous frameworks in digital health, the Metaverse, and health equity concerns (ref). The MERTH framework into our methodology ensures a comprehensive analysis of the data, grounded in contemporary perspectives on health and technology. Additionally, the PROGRESS-Plus framework was employed to identify dimensions across which telerehabilitation (TR) inequities may exist [15]. These dimensions encompass place of residence, race/ethnicity/culture/language, occupation, gender or sex, religion, education, socioeconomic status, social capital, age, disability, and sexual orientation [15]. Three authors extracted 10% of the included and after standardization of the process, one author extracted data from the remaining studies.
2.4. Quality Assessment (Risk of Bias)
We did not use a risk of bias tool for individual studies in our analysis, as our primary aim wasn't to evaluate intervention effectiveness. Nonetheless, we did extract data regarding the overall quality of studies, with particular attention to their inclusion/exclusion criteria and the reporting of ethical and equity considerations. We narrowed our focus to two key questions based on the systematic review appraisal worksheet from the Centre of Evidence-Based Medicine at the University of Oxford: a) Were all relevant studies adequately included? And b) Were the criteria used for inclusion/exclusion appropriate, or did they pose a risk of bias? Additionally, we documented whether each review employed a quality assessment method for the included articles..
2.5. Data Synthesis
The included reviews underwent a narrative synthesis approach for categorizing and summarizing the extracted data based on the PICOTSS structure, MERTH and PROGRESS-Plus frameworks. This hybrid method allowed for the organization of findings into themes and categories, facilitating a comprehensive data analysis (ref?). In the context of this rapid review, we adopted a pragmatic approach by incorporating quantitative data alongside qualitative data for narrative synthesis [16].
2.6. Analysis of Subgroups or Subsets
In our analysis, we conducted thorough subgroup analyses to discern variations and similarities across disciplines, patient groups, settings, and various telerehabilitation (TR) characteristics. This examination provided a more detailed understanding of the unique dynamics within each discipline and the potential ethical and equity gaps between them.
2.7. Changes on the Protocol
We decided not to use a risk of bias tool for individual studies in our analysis, as our primary aim was not to evaluate the effectiveness of interventions. Instead, our focus was on investigating the ethical and equity dimensions of the interventions. considerations. Another change to the protocol was the decision to publish a review of reviews up to 2020. Additionally, we will publish another review that will include recent individual articles from January 2020 to March 2023 to address gaps in the literature identified by the review of reviews.
3. Results
3.1. Search Results and Characteristics of Included Studies
After removing 14 duplicates, the total number of articles that were identified was 1542. Among these, after screening, 57 studies met the inclusion criteria (see the Flowchart in Figure 1). A total of 14 studies focusing on both physiotherapy (PT) and occupational therapy (OT), 38 studies exclusively on PT, and 5 studies exclusively on OT. Supplementary material provides detailed information on these studies, including Table 1 for Physiotherapy and Occupational therapy study characteristics, Table 2 for exclusive physiotherapy study characteristics, and Table 3 for exclusive occupational therapy study characteristics.
3.2. Study Design
The 57 studies included 30 systematic reviews, 16 systematic reviews with meta-analysis, 6 scoping reviews, and 5 narrative or literature reviews with detailed study descriptions.
3.3. Participants’ Conditions
This study included reviews that had individual studies with participants diagnosed with conditions falling into the three categories: neurological (64 studies), orthopedic (31 studies), and cardiorespiratory (13 studies) (Figure 2). For each study, all reported conditions were counted. Specifically, the most frequent neurological conditions were: Stroke, multiple sclerosis(MS), Parkinson, spinal cord injury(SCI), traumatic brain injury (TBI), acquired brain injury (ABI), and Down syndrome (DS). Most frequent orthopedic conditions were Fracture, Knee/replacement, musculoskeletal (MSK), Shoulder, orthopedic related Pain, Elbow. Furthermore, the majority of cardiorespiratory conditions included chronic obstructive pulmonary disease (COPD) and cardiovascular disease (CVD).
3.4. Ethics Considerations
Among the identified ethical dimensions within TR, actual and potential risk for adverse events were mentioned and included as an outcome or comment in 21 review articles [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37]. Autonomy was another ethical consideration, with 20 studies emphasizing the importance of respecting individuals' independence and decision-making within telerehabilitation contexts [21,22,23,24,25,27,29,30,31,32,34,36,38,39,40,41,42,43,44,45]. Additionally, privacy and security concerns were mentioned in 6 studies, [18,27,30,31,46,47] emphasizing the need to protect individuals' private information during telerehabilitation services. However, studies that did not report specific ethical concerns, highlighting potential gaps or variations in the documentation of ethical dimensions across the reviewed literature (Figure 3).
In this study, the results regarding ethical concerns were systematically categorized into three primary domains, with adverse events being the foremost reported and mentioned. This category includes safety, harm, potential risk, complications, and unintended consequences. Following adverse events, autonomy is the second most reported or mentioned domain, which includes aspects such as independence, choice, decision-making, self-management and self-determination. Each subcategory is counted within the context of individual studies included in comprehensive reviews or through comments provided by review authors (Figure 3). Lastly, the privacy and security category addresses aspects of confidentiality, security, data protection, information security, and privacy concerns. The number of studies with ethical aspects varied based on the reporting of variables or outcomes, whether they were reported, mentioned, or not reported. Please refer to Table 1 Equity and Ethics Variable or Reporting Across Included Studies for details (supplementary material). Table 4 presents the ethics themes and illustrative examples in included studies (supplementary material).
3.5. Equity Considerations
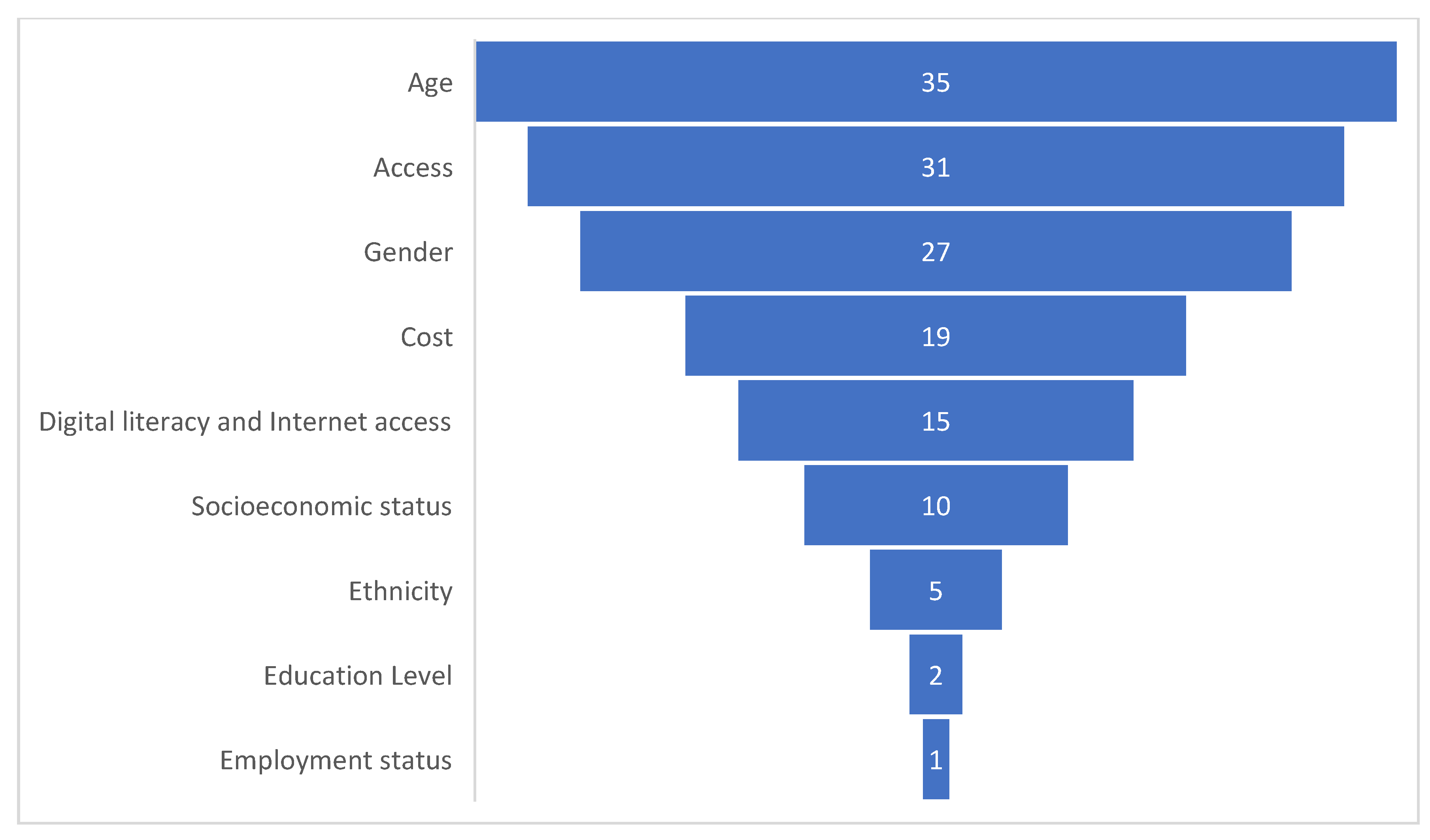
In this rapid review, equity aspects were investigated across various dimensions within the 57 included studies. Age emerged as a frequent consideration with 35 reviews containing information on the age demographics of participants [17,19,21,23,25,26,27,29,30,32,33,34,35,36,38,39,40,41,42,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63]. Access to rehabilitation services was another significant focus, with 31 reviews mentioning aspects of TR access [17,18,19,20,27,28,30,31,32,33,34,38,39,40,41,42,44,46,49,50,52,58,60,61,62,63,64,65,66,67,68]. Gender variables were reported in 27 reviews [17,19,21,23,26,27,29,33,34,35,36,37,38,39,42,43,48,49,52,53,59,61,62,66,68]. Out of the 57 studies included in this review, 19 reviews included at least one study that reported costs, or within the individual studies included, authors commented on the cost of equipment selection [19,21,23,27,29,32,33,35,38,44,45,47,52,53,55,61,64,67,68,69]
Furthermore, the digital divide in access to technology (internet) and technology literacy were reported in 18 reviews (nine digital literacy comments and nine mentions of access to internet) [18,24,27,28,30,31,36,37,38,39,46,50,60,62,64,66,67,68], while socioeconomic status (SES) was reported in 2 reviews [39,70], one review included 9 studies that reporte[17,19,21,23,25–27,29,30,32–36,38–42,47–63d SES [39]. Ethnicity was reported in 5 reviews [21,22,32,39,58]. However, education [30,70] and employment status [30] received less consideration, with only 2 and 1 review(s) respectively reporting this equity-related aspects (Figure 4).
Table 1 describes how various equity aspects of the studies are explored with examples drawn from publications of included studies (supplementary material). Each theme corresponds to a specific PROGRESS Plus and MERTH domains, highlighting various dimensions of equity-related concerns in telerehabilitation services. Examples were grouped according to these dimensions to provide a comprehensive understanding of the challenges and factors associated with access, gender, cost, digital divide, socioeconomic status (SES), education, and ethnicity. Access is an equity aspect of the MERTH framework and within the PROGRESS-Plus framework is associated with SES includes factors such as income, education, and occupation. Individuals with lower socioeconomic status may face barriers to accessing healthcare services, including telerehabilitation. The distribution of studies according to equity aspects varied based on the reporting of variable or outcomes, whether they reported, mentioned, or not reported. Please refer to Table 1 equity and ethics variable or outcome reporting across included studies for details (supplementary material). Table 5 presents Equity themes and illustrative examples in included studies (supplementary material).
3.6. Quality Assessment (Risk of Bias)
The critical appraisal of the included studies demonstrated different methodological quality across different reviews and trials. Issues such as selection bias, performance bias, detection bias, and attrition bias were commonly identified. Several studies lacked methodological rigour due to small sample sizes, weak research designs, and bias in recruitment procedures. Additionally, inadequate reporting of participant characteristics, intervention details, and outcomes was observed in some studies, limiting the reliability of the findings. Age bias was noted in the exclusion of older individuals from telerehabilitation studies, potentially impacting the generalizability of results. Despite these limitations, some studies demonstrated moderate to good methodological quality, particularly randomized controlled trials, although blinding procedures were often inadequate. Collaborative efforts are needed to approach these methodological challenges and improve the quality of research in telerehabilitation, ensuring more robust evidence to guide clinical practice and policy-making.
4. Discussion
Our analysis found a higher prevalence of TR use for neurological conditions (64 studies) compared to orthopedic (31 studies) and cardiorespiratory conditions. However, these findings may not fully reflect real-world TR use. Telerehabilitation provides continuous, personalized care for neurological conditions, enabling remote monitoring and tailored exercise programs [71].
4.1. Ethics Aspects
Our findings highlight that adverse events are a significant concern in telerehabilitation (TR) interventions. For example, Agostini (2015) [20] stresses the need for better research to assess the benefits and risks of remote rehabilitation. Poor image resolution can lead to misdiagnosis and inappropriate treatment, increasing the risk of secondary injuries [42]. The difficulty in distinguishing actual adverse events from potential risks in our review was compounded by inconsistent reporting and definitions across studies. Some studies followed FDA guidelines, while others lacked clarity. A recent systematic review also recommended including adverse events in future studies for a better understanding of TR’s safety.
Respecting patient autonomy is another key ethical aspect of TR. Chen (2019) [24] notes that participants value flexibility and control over their rehabilitation, while previous research emphasizes the importance of self-management in optimizing outcomes. Greaney (2020) [72] highlights the growing role of self-care in managing chronic conditions, aligning with bioethical principles like autonomy, beneficence, and justice. Engaging in self-management can improve quality of life, clinical outcomes, and self-efficacy, making it a vital ethical strategy for TR.
Our review found it difficult to distinguish between actual adverse events and potential risks, as some studies either omitted or did not report adverse events. Discrepancies in definitions, with some following FDA guidelines and others lacking clarity, further complicated the analysis. A recent systematic review on TR for knee arthroplasty patients recommended including adverse events in future studies for a clearer safety assessment [73]..
In the context of TR, respecting patients' autonomy emerges as an important ethical aspect, as highlighted by Chen (2019)[24], who emphasizes participants' appreciation for flexibility and control over their rehabilitation process. Moreover, former research [34,42] underlined how self-management strategies can empower patients, emphasizing the crucial role of autonomy in optimizing outcomes within telerehabilitation settings.
According to Greaney (2020)[72], the concept of self-care as a strategy for managing chronic conditions is gaining attention, with individuals being increasingly responsible for daily health-related tasks[72]. Engaging in self-management can empower individuals and lead to improvements in quality of life, clinical outcomes, and self-efficacy[72]. From an ethical perspective, self-care aligns with established bioethical principles such as autonomy, beneficence, nonmaleficence, and justice. Therefore, self-care is seen as a comprehensive strategy for improving patient outcomes and an ethical concept consistent with ethical norms and professional obligations [72].
Independence can sometimes result in patients neglecting essential care tasks, leading to poor outcomes. This critique of autonomy suggests that self-care may exceed patients' capabilities, causing feelings of abandonment. Focusing on personal responsibility can shift the clinician-patient relationship towards victim-blaming, marginalizing vulnerable individuals and exacerbating health inequalities, raising further ethical concerns. [72].
The principle of autonomy, increasingly emphasized in healthcare, has roots in individual rights and self-determination but can sometimes conflict with other ethical principles like beneficence and justice. The "autonomy conundrum" arises when vulnerable individuals struggle to exercise autonomy due to their circumstances. This struggle is particularly evident in chronic illness, where autonomy fluctuates between periods of dependence and independence. Higher-order cognitive skills required for self-management may surpass the capabilities of individuals, especially without adequate support [72]. In the context of telerehabilitation, physiotherapists and occupational therapists should carefully consider the complex needs of patients with chronic illnesses. It's crucial to provide comprehensive support, reporting physical, mental, and social aspects, to facilitate effective self-management and promote autonomy while ensuring patients aren't overwhelmed.
Privacy concerns highlight the need for strong security measures to protect patient data in telerehabilitation. Guy et al.'s qualitative study found that all participants emphasized the importance of maintaining confidentiality in telerehabilitation [74]. The literature on ethical principles in TR emphasizes the need for user agreements that follow legal guidelines to protect patient information. Informed consent through electronic forms is essential for addressing ethical concerns. While two-factor authentication improves security, challenges in fully protecting medical data persist despite encryption [75]. Furthermore, Iacono (2016) highlights the necessity of involving policymakers and professionals to respond to clinician concerns and ensure the secure delivery of TR services [46].
Therapists can utilize clinical guidelines to guide their telerehabilitation practice, ensuring adherence to evidence-based recommendations and best practices[76]. For example, a clinical guideline on telerehabilitation was developed by a volunteer guideline development group convened by the American Physical Therapy Association. The guideline comprises several recommendations, including guidance regarding risks, harms, costs of implementation, privacy and security[76].
4.2. Equity Aspects
Rochette's 2013 study [77] highlighted that eliminating travel to rehab centers benefits those with limited mobility or healthcare access, especially in low-resource settings where mobile phones are more available, which is supported by other studies [30]. Similarly, Laver [27] outlined the importance of rapid and remote access to healthcare professionals for tailored support, which has been shown to enhance adherence to Internet-based interventions. Guay [68] also suggested that knowing they have access to professional support at any time and place may easy concerns for caregivers.
A recent study on the acceptability of TR for individuals with stroke and caregivers identified barriers, including technical (e.g., devices, internet) and environmental (e.g., space, lack of human contact) issues. While technical challenges are significant, they become equity issues when they disproportionately affect certain demographic groups, such as those from lower-income households or rural areas, who struggle with access to technology [78]. These challenges become equity issues when they disproportionately affect certain demographic groups based on factors like income, race level of ability, or geographic location. For instance, individuals from lower-income households or rural areas may face greater difficulties accessing reliable internet connections or necessary equipment for telerehabilitation sessions [38].
Although age was often reported as an equity-related variable, most studies did not address its implications. Similarly, while some studies included gender data, they lacked discussion on its impact on telerehabilitation. Inconsistent gender reporting across studies makes comparisons challenging and may reveal gender biases and disparities in telerehabilitation. For instance, Appleby [29] noted a gender bias in favor or men and . Hewitt (2020)[53] reported a similar bias for women, both related to higher number of participants in these respective genders depending of the studies. Additionally, Yadav (2019)[49] found differences in the delivery of appropriate care between men and women within intervention groups, further emphasizing the importance of considering gender-related factors in telerehabilitation research and practice. For example, a recent study indicated that male patients exhibited a greater reliance on telehealth services than their female counterparts [79].
A scoping review identified a gap in understanding how sex and gender affect rehabilitation participation and outcomes, revealing disparities in access, adherence, and outcomes, with women facing worse outcomes and a higher caregiving burden. The literature mainly focuses on rehabilitation in high-income countries, neglecting global and condition-based needs, and often conflates sex and gender, complicating analysis [80]. The review recommends using social science and intersectional approaches in future research to explore how gender and social norms influence rehabilitation disparities. Additionally, sexual orientation, particularly for LGBTQIA2S+ individuals, is often overlooked and should be included in future studies. Healthcare systems should prioritize individualized, gender-sensitive care to address these disparities.[80].
Despite the emphasis on reporting costs in telerehabilitation (TR) studies, comprehensive cost reporting remains lacking [6]. Recent studies continue to highlight limited attention to the cost-effectiveness of TR [81,82]. While low-cost technologies like phone systems are suggested for telerehabilitation, there is little evidence on their cost-effectiveness, with many studies missing data on investment costs or resource use.
Telerehabilitation offers a solution to access gaps in rehabilitation services, but a digital divide persists, particularly among marginalized communities. This divide refers to the gap between those with easy access to technology and those without [83]. Despite improvements in broadband access, certain demographic groups with chronic conditions and those with lower incomes continue to face barriers to accessing TR services [84]. . From a human rights perspective, the gap encompasses access to technology, digital literacy, and economic opportunities. Additionally, both clinicians and patients often lack the technical skills to navigate information technologies, highlighting the need for comprehensive training and support [83]. Rehabilitation professionals should prioritize targeted interventions, policy advocacy, and training. Technology costs and low-resource settings exacerbate disparities, highlighting the need for more diversity and inclusion in telerehabilitation research. Personalized telerehabilitation, by tailoring interventions to each patient's unique needs and circumstances, can help address these disparities. This approach ensures services are accessible, effective, and relevant, enhancing patient engagement and outcomes, while bridging the equity gap, especially for racialized populations with limited access to resources and technology.
4.3. Limitation
The metrics from individual studies were gathered from the included reviews. Each study included in the reviews was not accessed individually. It is possible that some of the included studies were encountered more than once, as they may have been included in multiple review papers.
5. Conclusions
This study examines the current state and trends in telerehabilitation research, focusing on interventions, target populations, and ethical and equity considerations. Telerehabilitation shows promise in addressing access gaps, particularly for individuals in remote areas or with limited mobility. However, barriers like technical issues, equipment availability, and human interaction challenges must be addressed. Equity is crucial for TR’s success, as the digital divide exacerbates disparities in technology access and digital literacy, especially in racialized communities. Inadequate demographic reporting highlights the need for diversity and inclusion in TR research. Improved reporting can guide policy and resource allocation to ensure accessibility for all, promoting digital health equity. Collaboration among clinicians, patients, developers, and policymakers is key to advancing equitable telerehabilitation services.
References
- Xu, J.; Willging, A.; Bramstedt, K.A. A scoping review of the ethical issues within telemedicine: Lessons from COVID-19 pandemic. J. Health Soc. Sci. 2021, 6, 31–40. [Google Scholar]
- Kazuko Shem, I.I.; Alexander, M. Chapter 2. Getting Started: Mechanisms of Telerehabilitation. In Telerehabilitation; Alexander, M., Ed.; Elsevier: Amsterdam, Netherlands, 2022; pp. 5–20. [Google Scholar] [CrossRef]
- Seron, P.; Oliveros, M.J.; Gutierrez-Arias, R.; Fuentes-Aspe, R.; Torres-Castro, R.C.; Merino-Osorio, C.; Nahuelhual, P.; Inostroza, J.; Jalil, Y.; Solano, R.; et al. Effectiveness of Telerehabilitation in Physical Therapy: A Rapid Overview. Phys Ther 2021, 101. [Google Scholar] [CrossRef] [PubMed]
- Federico, S.; Cacciante, L.; De Icco, R.; Gatti, R.; Jonsdottir, J.; Pagliari, C.; Franceschini, M.; Goffredo, M.; Cioeta, M.; Calabrò, R.S.; et al. Telerehabilitation for Stroke: A Personalized Multi-Domain Approach in a Pilot Study. J Pers Med 2023, 13. [Google Scholar] [CrossRef]
- Baroni, M.P.; Jacob, M.F.A.; Rios, W.R.; Fandim, J.V.; Fernandes, L.G.; Chaves, P.I.; Fioratti, I.; Saragiotto, B.T. The state of the art in telerehabilitation for musculoskeletal conditions. Arch Physiother 2023, 13, 1. [Google Scholar] [CrossRef] [PubMed]
- Kairy, D.; Lehoux, P.; Vincent, C.; Visintin, M. A systematic review of clinical outcomes, clinical process, healthcare utilization and costs associated with telerehabilitation. Disabil Rehabil 2009, 31, 427–447. [Google Scholar] [CrossRef]
- Nittari, G.; Khuman, R.; Baldoni, S.; Pallotta, G.; Battineni, G.; Sirignano, A.; Amenta, F.; Ricci, G. Telemedicine Practice: Review of the Current Ethical and Legal Challenges. Telemed J E Health 2020, 26, 1427–1437. [Google Scholar] [CrossRef]
- Mahmoudi, E.; Meade, M.A. Disparities in access to health care among adults with physical disabilities: Analysis of a representative national sample for a ten-year period. Disabil Health J 2015, 8, 182–190. [Google Scholar] [CrossRef]
- King, V.J.; Stevens, A.; Nussbaumer-Streit, B.; Kamel, C.; Garritty, C. Paper 2: Performing rapid reviews. [CrossRef]
- Garritty, C.; Gartlehner, G.; Nussbaumer-Streit, B.; King, V.J.; Hamel, C.; Kamel, C.; Affengruber, L.; Stevens, A. Cochrane Rapid Reviews Methods Group offers evidence-informed guidance to conduct rapid reviews. J Clin Epidemiol 2021, 130, 13–22. [Google Scholar] [CrossRef]
- Veras, M.; Sigouin, J.; Auger, C.; Auger, L.-P.; Ahmed, S.; Boychuck, Z.; Cavallo, S.; Lévesque, M.; Lovo, S.; Miller, W.C.; et al. A rapid review protocol of physiotherapy and occupational therapy telerehabilitation to inform ethical and equity concerns. DIGITAL HEALTH 2024, 10, 20552076241260367. [Google Scholar] [CrossRef]
- Matchar, D.B. Chapter 1: Introduction to the Methods Guide for Medical Test Reviews. Journal of General Internal Medicine 2012, 27, 4–10. [Google Scholar] [CrossRef]
- Covidence systematic reviews software. Veritas Health Innovations: Melbourne, Australia. Available at: www.covidence.org.
- Veras, M.; Labbé, D.R.; Furlano, J.; Zakus, D.; Rutherford, D.; Pendergast, B.; Kairy, D. A framework for equitable virtual rehabilitation in the metaverse era: Challenges and opportunities. Front Rehabil Sci 2023, 4, 1241020. [Google Scholar] [CrossRef] [PubMed]
- O'Neill, J.; Tabish, H.; Welch, V.; Petticrew, M.; Pottie, K.; Clarke, M.; Evans, T.; Pardo Pardo, J.; Waters, E.; White, H.; et al. Applying an equity lens to interventions: Using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol 2014, 67, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Mays, N.; Pope, C.; Popay, J. Systematically reviewing qualitative and quantitative evidence to inform management and policy-making in the health field. J Health Serv Res Policy 2005, 10 (Suppl. S1), 6–20. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.; Yamabayashi, C.; Syed, N.; Kirkham, A.; Camp, P.G. Exercise Telemonitoring and Telerehabilitation Compared with Traditional Cardiac and Pulmonary Rehabilitation: A Systematic Review and Meta-Analysis. Physiother Can 2016, 68, 242–251. [Google Scholar] [CrossRef]
- Chirra, M.; Marsili, L.; Wattley, L.; Sokol, L.L.; Keeling, E.; Maule, S.; Sobrero, G.; Artusi, C.A.; Romagnolo, A.; Zibetti, M.; et al. Telemedicine in Neurological Disorders: Opportunities and Challenges. Telemed J E Health 2019, 25, 541–550. [Google Scholar] [CrossRef]
- Ninnis, K.; Van Den Berg, M.; Lannin, N.A.; George, S.; Laver, K. Information and communication technology use within occupational therapy home assessments: A scoping review. British Journal of Occupational Therapy 2018, 82, 141–152. [Google Scholar] [CrossRef]
- Agostini, M.; Moja, L.; Banzi, R.; Pistotti, V.; Tonin, P.; Venneri, A.; Turolla, A. Telerehabilitation and recovery of motor function: A systematic review and meta-analysis. Journal of Telemedicine and Telecare 2015, 21, 202–213. [Google Scholar] [CrossRef]
- Amatya, B.; Galea, M.P.; Kesselring, J.; Khan, F. Effectiveness of telerehabilitation interventions in persons with multiple sclerosis: A systematic review. Mult Scler Relat Disord 2015, 4, 358–369. [Google Scholar] [CrossRef]
- Amatya, B.; Khan, F.; Galea, M. Rehabilitation for people with multiple sclerosis: An overview of Cochrane Reviews. Cochrane Database Syst Rev 2019, 1, Cd012732. [Google Scholar] [CrossRef]
- Chen, J.; Jin, W.; Zhang, X.-X.; Xu, W.; Liu, X.-N.; Ren, C.-C. Telerehabilitation Approaches for Stroke Patients: Systematic Review and Meta-analysis of Randomized Controlled Trials. Journal of Stroke and Cerebrovascular Diseases 2015, 24, 2660–2668. [Google Scholar] [CrossRef]
- Chen, Y.; Abel, K.T.; Janecek, J.T.; Zheng, K.; Cramer, S.C. Home-based technologies for stroke rehabilitation: A systematic review. Int J Med Inform 2019, 123, 11–22. [Google Scholar] [CrossRef]
- Dávila Castrodad, I.M.; Recai, T.M.; Abraham, M.M.; Etcheson, J.I.; Mohamed, N.S.; Edalatpour, A.; Delanois, R.E. Rehabilitation protocols following total knee arthroplasty: A review of study designs and outcome measures. Annals of translational medicine 2019, 7 (Suppl. S7), S255. [Google Scholar] [CrossRef]
- Khan, F.; Amatya, B.; Kesselring, J.; Galea, M. Telerehabilitation for persons with multiple sclerosis. Cochrane Database Syst Rev 2015, 2015, CD010508. [Google Scholar] [CrossRef] [PubMed]
- Laver, K.E.; Adey-Wakeling, Z.; Crotty, M.; Lannin, N.A.; George, S.; Sherrington, C. Telerehabilitation services for stroke. Cochrane Database Syst Rev 2020, 1, Cd010255. [Google Scholar] [CrossRef] [PubMed]
- Almojaibel, A.A. Delivering Pulmonary Rehabilitation for Patients with Chronic Obstructive Pulmonary Disease at Home Using Telehealth: A Review of the Literature. Saudi J Med Med Sci 2016, 4, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Appleby, E.; Gill, S.T.; Hayes, L.K.; Walker, T.L.; Walsh, M.; Kumar, S. Effectiveness of telerehabilitation in the management of adults with stroke: A systematic review. PLoS ONE 2019, 14, e0225150. [Google Scholar] [CrossRef] [PubMed]
- Berton, A.; Longo, U.G.; Candela, V.; Fioravanti, S.; Giannone, L.; Arcangeli, V.; Alciati, V.; Berton, C.; Facchinetti, G.; Marchetti, A.; et al. Virtual Reality, Augmented Reality, Gamification, and Telerehabilitation: Psychological Impact on Orthopedic Patients' Rehabilitation. J Clin Med 2020, 9. [Google Scholar] [CrossRef]
- Blood, k. The use of Telehealth by Physical Therapis: A review of literature. Gerinotes: Academy of Geriatrics Physical Therapy 2019, 26, 22–29. [Google Scholar]
- Flodgren, G.; Rachas, A.; Farmer, A.J.; Inzitari, M.; Shepperd, S. Interactive telemedicine: Effects on professional practice and health care outcomes. Cochrane Database Syst Rev 2015, 2015, CD002098. [Google Scholar] [CrossRef]
- Jin, K.; Khonsari, S.; Gallagher, R.; Gallagher, P.; Clark, A.M.; Freedman, B.; Briffa, T.; Bauman, A.; Redfern, J.; Neubeck, L. Telehealth interventions for the secondary prevention of coronary heart disease: A systematic review and meta-analysis. European Journal of Cardiovascular Nursing 2019, 18, 260–271. [Google Scholar] [CrossRef]
- Slattery, B.W.; Haugh, S.; O'Connor, L.; Francis, K.; Dwyer, C.P.; O'Higgins, S.; Egan, J.; McGuire, B.E. An Evaluation of the Effectiveness of the Modalities Used to Deliver Electronic Health Interventions for Chronic Pain: Systematic Review With Network Meta-Analysis. J Med Internet Res 2019, 21, e11086. [Google Scholar] [CrossRef] [PubMed]
- van der Meij, E.; Anema, J.R.; Otten, R.H.; Huirne, J.A.; Schaafsma, F.G. The Effect of Perioperative E-Health Interventions on the Postoperative Course: A Systematic Review of Randomised and Non-Randomised Controlled Trials. PLoS ONE 2016, 11, e0158612. [Google Scholar] [CrossRef] [PubMed]
- van Egmond, M.A.; van der Schaaf, M.; Vredeveld, T.; Vollenbroek-Hutten, M.M.R.; van Berge Henegouwen, M.I.; Klinkenbijl, J.H.G.; Engelbert, R.H.H. Effectiveness of physiotherapy with telerehabilitation in surgical patients: A systematic review and meta-analysis. Physiotherapy 2018, 104, 277–298. [Google Scholar] [CrossRef] [PubMed]
- Veras, M.; Kairy, D.; Rogante, M.; Giacomozzi, C.; Saraiva, S. Scoping review of outcome measures used in telerehabilitation and virtual reality for post-stroke rehabilitation. Journal of Telemedicine and Telecare 2016, 23, 567–587. [Google Scholar] [CrossRef]
- Zhou, L.; Parmanto, B. Reaching People With Disabilities in Underserved Areas Through Digital Interventions: Systematic Review. J Med Internet Res 2019, 21, e12981. [Google Scholar] [CrossRef]
- Batsis, J.A.; DiMilia, P.R.; Seo, L.M.; Fortuna, K.L.; Kennedy, M.A.; Blunt, H.B.; Bagley, P.J.; Brooks, J.; Brooks, E.; Kim, S.Y.; et al. Effectiveness of Ambulatory Telemedicine Care in Older Adults: A Systematic Review. J Am Geriatr Soc 2019, 67, 1737–1749. [Google Scholar] [CrossRef]
- Cottrell, M.A.; Galea, O.A.; O'Leary, S.P.; Hill, A.J.; Russell, T.G. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: A systematic review and meta-analysis. In Clin Rehabil, England, 2017; Vol. 31, pp. 625–638. [CrossRef]
- Du, S.; Liu, W.; Cai, S.; Hu, Y.; Dong, J. The efficacy of e-health in the self-management of chronic low back pain: A meta analysis. International Journal of Nursing Studies 2020, 106, 103507. [Google Scholar] [CrossRef]
- Mani, S.; Sharma, S.; Omar, B.; Paungmali, A.; Joseph, L. Validity and reliability of Internet-based physiotherapy assessment for musculoskeletal disorders: A systematic review. Journal of Telemedicine and Telecare 2016, 23, 379–391. [Google Scholar] [CrossRef]
- Gilbert, A.W.; Jaggi, A.; May, C.R. What is the patient acceptability of real time 1:1 videoconferencing in an orthopaedics setting? A systematic review. In Physiotherapy, © 2017 Chartered Society of Physiotherapy: England, 2018; Vol. 104, pp. 178–186. [CrossRef]
- Tchero, H.; Tabue Teguo, M.; Lannuzel, A.; Rusch, E. Telerehabilitation for Stroke Survivors: Systematic Review and Meta-Analysis. J Med Internet Res 2018, 20, e10867. [Google Scholar] [CrossRef]
- Salomè, A.; Sasso D'Elia, T.; Franchini, G.; Santilli, V.; Paolucci, T. Occupational Therapy in Fatigue Management in Multiple Sclerosis: An Umbrella Review. Mult Scler Int 2019, 2019, 2027947. [Google Scholar] [CrossRef]
- Iacono, T.; Stagg, K.; Pearce, N.; Hulme Chambers, A. A scoping review of Australian allied health research in ehealth. BMC Health Serv Res 2016, 16, 543. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, E.; Cotea, C.; Pullman, S.; Nasveld, P. Self-management and rehabilitation in osteoarthritis: Is there a place for internet-based interventions? Telemed J E Health 2013, 19, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Rintala, A.; Hakala, S.; Paltamaa, J.; Heinonen, A.; Karvanen, J.; Sjögren, T. Effectiveness of technology-based distance physical rehabilitation interventions on physical activity and walking in multiple sclerosis: A systematic review and meta-analysis of randomized controlled trials. Disabil Rehabil 2018, 40, 373–387. [Google Scholar] [CrossRef] [PubMed]
- Yadav, L.; Haldar, A.; Jasper, U.; Taylor, A.; Visvanathan, R.; Chehade, M.; Gill, T. Utilising Digital Health Technology to Support Patient-Healthcare Provider Communication in Fragility Fracture Recovery: Systematic Review and Meta-Analysis. Int J Environ Res Public Health 2019, 16. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-Y.; Guan, B.-S.; Li, Z.-K.; Yang, Q.-H.; Xu, T.-J.; Li, H.-B.; Wu, Q.-Y. Application of telehealth intervention in Parkinson’s disease: A systematic review and meta-analysis. Journal of Telemedicine and Telecare 2018, 26, 3–13. [Google Scholar] [CrossRef]
- Gövercin, M.; Missala, I.M.; Marschollek, M.; Steinhagen-Thiessen, E. Virtual rehabilitation and telerehabilitation for the upper limb: A geriatric review. GeroPsych: The Journal of Gerontopsychology and Geriatric Psychiatry 2010, 23, 79–90. [Google Scholar] [CrossRef]
- Grona, S.L.; Bath, B.; Busch, A.; Rotter, T.; Trask, C.; Harrison, E. Use of videoconferencing for physical therapy in people with musculoskeletal conditions: A systematic review. Journal of Telemedicine and Telecare 2017, 24, 341–355. [Google Scholar] [CrossRef]
- Hewitt, S.; Sephton, R.; Yeowell, G. The Effectiveness of Digital Health Interventions in the Management of Musculoskeletal Conditions: Systematic Literature Review. J Med Internet Res 2020, 22, e15617. [Google Scholar] [CrossRef]
- Pastora-Bernal, J.M.; Martín-Valero, R.; Barón-López, F.J.; Estebanez-Pérez, M.J. Evidence of Benefit of Telerehabitation After Orthopedic Surgery: A Systematic Review. J Med Internet Res 2017, 19, e142. [Google Scholar] [CrossRef]
- Schröder, J.; van Criekinge, T.; Embrechts, E.; Celis, X.; Van Schuppen, J.; Truijen, S.; Saeys, W. Combining the benefits of tele-rehabilitation and virtual reality-based balance training: A systematic review on feasibility and effectiveness. Disabil Rehabil Assist Technol 2019, 14, 2–11. [Google Scholar] [CrossRef]
- Shukla, H.; Nair, S.R.; Thakker, D. Role of telerehabilitation in patients following total knee arthroplasty: Evidence from a systematic literature review and meta-analysis. Journal of Telemedicine and Telecare 2016, 23, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Simek, E.M.; McPhate, L.; Haines, T.P. Adherence to and efficacy of home exercise programs to prevent falls: A systematic review and meta-analysis of the impact of exercise program characteristics. Prev Med 2012, 55, 262–275. [Google Scholar] [CrossRef] [PubMed]
- Speyer, R.; Denman, D.; Wilkes-Gillan, S.; Chen, Y.W.; Bogaardt, H.; Kim, J.H.; Heckathorn, D.E.; Cordier, R. Effects of telehealth by allied health professionals and nurses in rural and remote areas: A systematic review and meta-analysis. J Rehabil Med 2018, 50, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Srikesavan, C.; Bryer, C.; Ali, U.; Williamson, E. Web-based rehabilitation interventions for people with rheumatoid arthritis: A systematic review. Journal of Telemedicine and Telecare 2018, 25, 263–275. [Google Scholar] [CrossRef]
- Velayati, F.; Ayatollahi, H.; Hemmat, M. A Systematic Review of the Effectiveness of Telerehabilitation Interventions for Therapeutic Purposes in the Elderly. Methods Inf Med 2020, 59, 104–109. [Google Scholar] [CrossRef]
- Wake, E.; Atkins, H.; Willock, A.; Hawkes, A.; Dawber, J.; Weir, K.A. Telehealth in trauma: A scoping review. Journal of Telemedicine and Telecare 2020, 28, 412–422. [Google Scholar] [CrossRef]
- Wang, X.; Hunter, D.J.; Vesentini, G.; Pozzobon, D.; Ferreira, M.L. Technology-assisted rehabilitation following total knee or hip replacement for people with osteoarthritis: A systematic review and meta-analysis. BMC Musculoskeletal Disorders 2019, 20, 506. [Google Scholar] [CrossRef]
- Hung Kn, G.; Fong, K.N. Effects of telerehabilitation in occupational therapy practice: A systematic review. Hong Kong J Occup Ther 2019, 32, 3–21. [Google Scholar] [CrossRef]
- Yeroushalmi, S.; Maloni, H.; Costello, K.; Wallin, M.T. Telemedicine and multiple sclerosis: A comprehensive literature review. Journal of Telemedicine and Telecare 2019, 26, 400–413. [Google Scholar] [CrossRef]
- Davis, A.M. Osteoarthritis year 2011 in review: Rehabilitation and outcomes. Osteoarthritis and Cartilage 2012, 20, 201–206. [Google Scholar] [CrossRef]
- T. Johansson and C. Wild, "Telerehabilitation in stroke care--a systematic review," (in eng), no. 1758-1109 (Electronic). [CrossRef]
- Knepley, K.D.; Mao, J.Z.; Wieczorek, P.; Okoye, F.O.; Jain, A.P.; Harel, N.Y. Impact of Telerehabilitation for Stroke-Related Deficits. Telemedicine and e-Health 2020, 27, 239–246. [Google Scholar] [CrossRef]
- Guay, C.; Auger, C.; Demers, L.; Mortenson, W.B.; Miller, W.C.; Gélinas-Bronsard, D.; Ahmed, S. Components and Outcomes of Internet-Based Interventions for Caregivers of Older Adults: Systematic Review. J Med Internet Res 2017, 19, e313. [Google Scholar] [CrossRef] [PubMed]
- Sarfo, F.S.; Ulasavets, U.; Opare-Sem, O.K.; Ovbiagele, B. Tele-Rehabilitation after Stroke: An Updated Systematic Review of the Literature. J Stroke Cerebrovasc Dis 2018, 27, 2306–2318. [Google Scholar] [CrossRef] [PubMed]
- Kebapci, A.; Ozkaynak, M.; Lareau, S.C. Effects of eHealth-Based Interventions on Adherence to Components of Cardiac Rehabilitation: A Systematic Review. Journal of Cardiovascular Nursing 2020, 35. [Google Scholar] [CrossRef] [PubMed]
- Nuara, A.; Fabbri-Destro, M.; Scalona, E.; Lenzi, S.E.; Rizzolatti, G.; Avanzini, P. Telerehabilitation in response to constrained physical distance: An opportunity to rethink neurorehabilitative routines. J Neurol 2022, 269, 627–638. [Google Scholar] [CrossRef]
- Greaney, A.M.; Flaherty, S. Self-care as care left undone? The ethics of the self-care agenda in contemporary healthcare policy. Nursing Philosophy 2020, 21. [Google Scholar] [CrossRef]
- Pang, D.; Sun, A.; Wang, F.; Lu, J.; Guo, Y.; Ding, W. The efficacy and safety of telerehabilitation for patients following total knee arthroplasty: A overviews of systematic reviews. Biomed Eng Online 2023, 22, 97. [Google Scholar] [CrossRef]
- Guy, M.; Blary, A.; Ladner, J.; Gilliaux, M. Ethical Issues Linked to the Development of Telerehabilitation: A Qualitative Study. Int J Telerehabil 2021, 13, e6367. [Google Scholar] [CrossRef]
- ÖZden, F.; Lembarkİ, Y. The Ethical Necessities and Principles in Telerehabilitation. Sağlık Hizmetleri ve Eğitimi Dergisi 2020, 3, 35–37. [Google Scholar] [CrossRef]
- Lee, A.C.; Deutsch, J.E.; Holdsworth, L.; Kaplan, S.L.; Kosakowski, H.; Latz, R.; McNeary, L.L.; O'Neil, J.; Ronzio, O.; Sanders, K.; et al. Telerehabilitation in Physical Therapist Practice: A Clinical Practice Guideline from the American Physical Therapy Association. Phys Ther 2024. [Google Scholar] [CrossRef]
- Rochette, A.; Korner-Bitensky, N.; Bishop, D.; Teasell, R.; White, C.L.; Bravo, G.; Côté, R.; Green, T.; Lebrun, L.H.; Lanthier, S.; et al. The YOU CALL-WE CALL randomized clinical trial: Impact of a multimodal support intervention after a mild stroke. Circ Cardiovasc Qual Outcomes 2013, 6, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Ouédraogo, F.; Auger, L.P.; Moreau, E.; Côté, O.; Guerrera, R.; Rochette, A.; Kairy, D. Acceptability of Telerehabilitation: Experiences and Perceptions by Individuals with Stroke and Caregivers in an Early Supported Discharge Program. Healthcare 2024, 12. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.; Amit, S.; Kafy, A.A. Gender disparity in telehealth usage in Bangladesh during COVID-19. SSM Ment Health 2022, 2, 100054. [Google Scholar] [CrossRef] [PubMed]
- Ott, J.; Champagne, S.N.; Bachani, A.M.; Morgan, R. Scoping 'sex' and 'gender' in rehabilitation: (mis)representations and effects. Int J Equity Health 2022, 21, 179. [Google Scholar] [CrossRef]
- Duruflé, A.; Le Meur, C.; Piette, P.; Fraudet, B.; Leblong, E.; Gallien, P. Cost effectiveness of a telerehabilitation intervention vs home based care for adults with severe neurologic disability: A randomized clinical trial. Digit Health 2023, 9, 20552076231191001. [Google Scholar] [CrossRef]
- Veras, M.; Stewart, J.; Deonandan, R.; Tatmatsu-Rocha, J.C.; Higgins, J.; Poissant, L.; Kairy, D. Cost-Analysis of a Home-Based Virtual Reality Rehabilitation to improve Upper Limb Function in Stroke Survivors. Global Journal of Health Sciences. Canadian Cener of Science and Education. 2020, 12, 1–98. [Google Scholar] [CrossRef]
- Sanders, C.K.; Scanlon, E. The Digital Divide Is a Human Rights Issue: Advancing Social Inclusion Through Social Work Advocacy. J Hum Rights Soc Work 2021, 6, 130–143. [Google Scholar] [CrossRef]
- Saeed, S.A.; Masters, R.M. Disparities in Health Care and the Digital Divide. Curr Psychiatry Rep 2021, 23, 61. [Google Scholar] [CrossRef]
Figure 2.
Distribution of health conditions of participants in included studies.
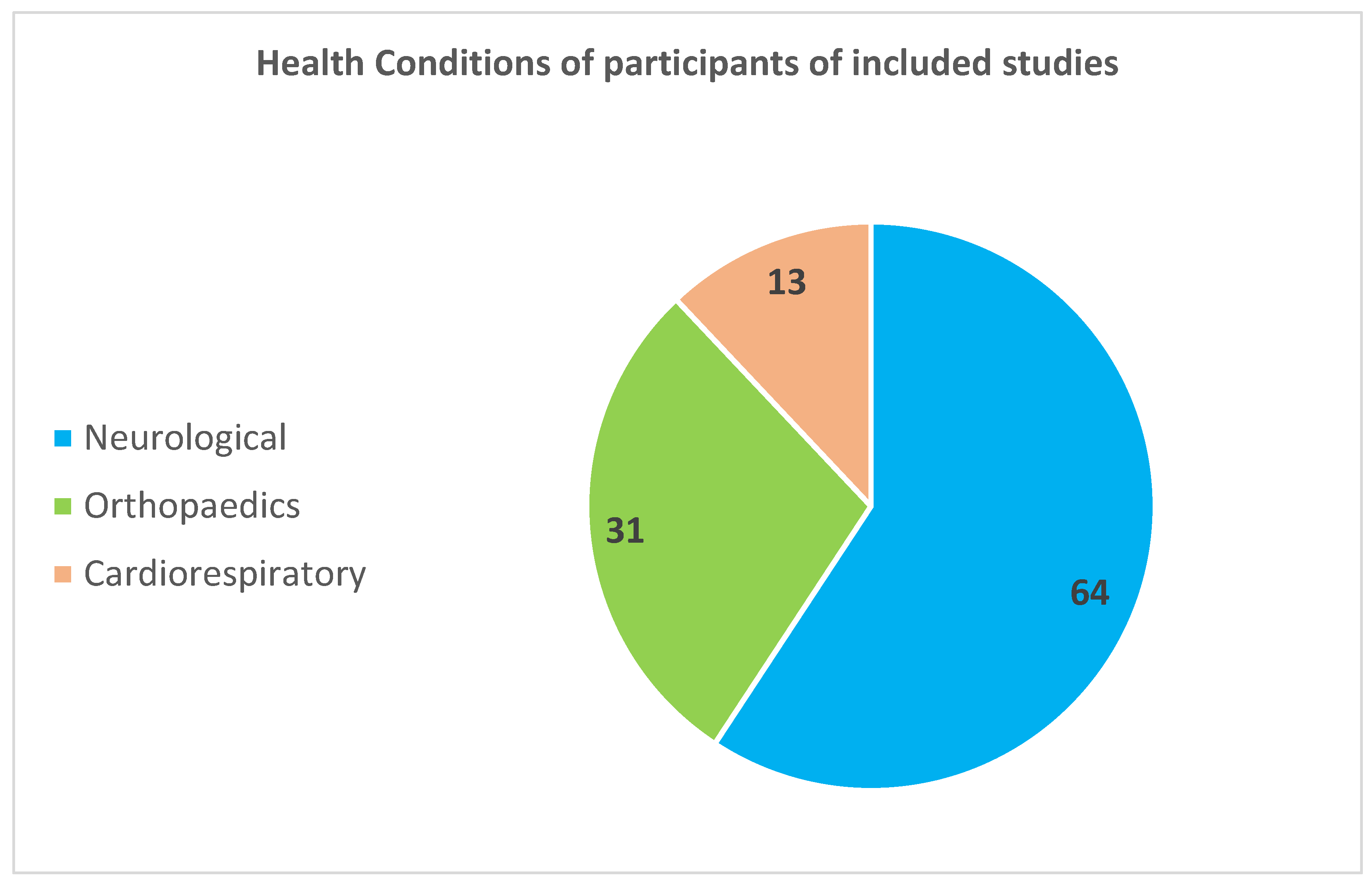
Figure 3.
Number of Studies Reporting Ethical Aspects.
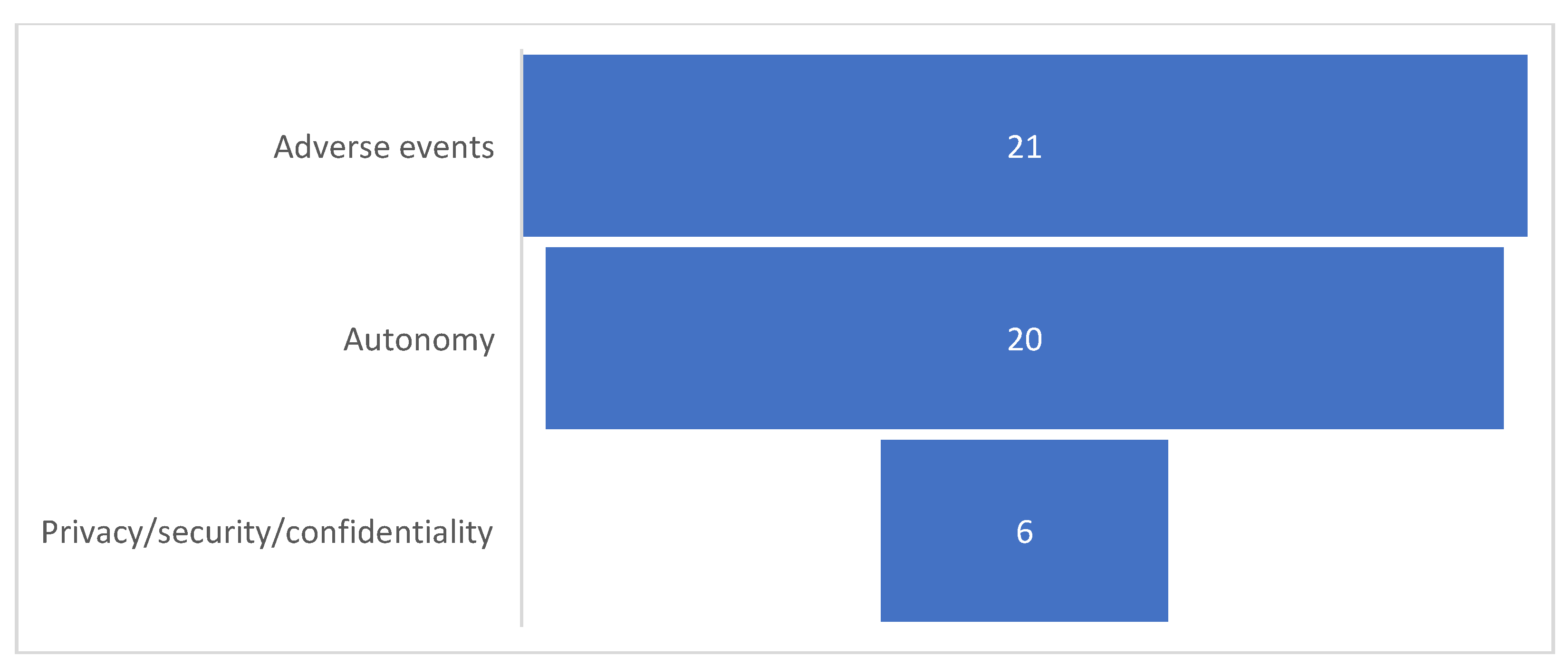
Figure 4.
Number of studies reporting equity aspects of the research.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



