Introduction
We performed a 5-6 year-long study on the
CONDITIONS OF COSMETIC SURGERY IN CALIFORNIA [
1]. The original purpose of this study was to collect reliable data to promote cosmetic surgery as a modern way to further improve the life quality of middle-aged men (in addition to the well-known medical methods, like hormone substitution, diet, exercise, et. cetera).
However our initial enthusiasm for cosmetic surgery quickly cooled down when we discovered that the insider reality of cosmetic surgery practices is very much different from the carefully nurtured fabulous external, public image [
2]. However some studies on the medical and legal history of cosmetic surgery quickly revealed that controversies around this activity are not new and it’s deviant nature (from plastic surgery and traditional medicine) having been in the focus of professional- and media attention many times [
3], including several lawsuits and even a congressional hearing [
4] and numerous critical publications. The main criticism is directed against the “beauty doctors” for 1) their “blatant commercialism”, 2) “deceptive advertising” 3) and the lack of proper and necessary specialist training. These activities are regularly resulting in severe bodily disfigurements and deep, emotional scares to thousands of cosmetic surgery clients who became the
victims of some unprofessional, unethical activity (that is camouflaged to be a regular, legitimate, medical and humanitarian service in the interest of a “patient”).
Cosmetic surgery is a commercial activity after all, there a medically educated and licensed person (who could be a
doctor if he was treating sick persons) is selling medical/surgical know-how to healthy persons, consumers (who could be
patients if they were sick) [
5]. (But they aren’t). The cosmetic surgery consumer selects and purchases a surgery to satisfy his/her ideas of “
beauty”. This is, or should be, formally a regular business transaction like buying a car or ordering a diner in a restaurant. But it isn’t. The involvement of the “
white rock” confuses everybody. It gives status to the service provider: he is a “
doctor”, not a merchant or trader. It gives status to the consumer: he is a “
patient” who receives a “
treatment” i.e. something he “
needs” (and not just satisfies her desires). This arrangement is seemingly good and acceptable for everybody, until something goes wrong. What happens when the product (“the beauty on demand”) doesn’t show up? There is no
product warranty, there is no way to
return the unsuccessful surgery. The consumer might believe that he was dealing with a doctor and files a complaint at the MBC, but this licensing agency will not find any malpractice: an ‘asymmetric face’, a ‘bumpy nose’ is not medical malpractice. The unhappy consumer may go to the Courts but the Courts will send her to the MBC (they also believe that everything under the shadow of a white rock is “medical”, i.e. not their subject matter jurisdiction). The constitutionally warranted “
day in court” [
6] means 2-3 minutes before a judge in these cases. The citizen can look for an attorney for help, but the plaintiff’s attorneys are effectively excluded from most of the medical malpractice cases by MICRA [
7]. MICRA caps compensation for what are known as “non-economic” damages – including life-altering situations. It was intended to lower medical malpractice liability insurance premiums for healthcare providers in CA by decreasing their potential tort liability. This law makes the malpractice lawsuits unattractive for consumer attorneys. Consequently most attorneys are representing doctors who have strong legal budget (malpractice insurances).
Large number of medical and legal efforts having been done to adopt cosmetic surgeons and their activities to the regular norms of the American Society (there consumer protection is important), as well as to the historical standards of medical ethics (there the “patients’” interest is paramount and supersedes the monetary interest of the doctors). However it became a depressing reality that organized cosmetic surgeons “
have the power, ability and cohesiveness to stall and frustrate the majority of efforts” [
8] in this direction.
Today, the only way to avoid cosmetic surgery related trouble is to make a good choice and go to an honest and professional surgeon who will really deliver that he promises. That’s the key. But. Cosmetic surgery is a business, an activity for profit. Far away from the ethical code of the American Medical Association (AMA) that requests that “
Under no circumstances may physicians place their own financial interests above the welfare of their patients” [
9]. Crocked “beauty doctors” do everything that they can to avoid objective, fact-based comparison. They are simply misleading in their advertisements and during the pre-operative meetings with their potential clients. They are using (misusing) their psychological education and pursue the ignorant public to sign up for a surgery. What happens after the surgery is no longer their problem that is the attorney’s and the malpractice insurance company’s.
We assume, that it is only about 10% of cosmetic surgeons who are
disturbingly dishonest, while 90% does good or acceptable job. But the consumer’s dilemma remains: how to identify these 10%, potentially very dangerous doctors in time, i.e. before appointing them for a surgery? The MBC knows well who are these controversial actors, but they will not disclose it to the public. Insurance companies are also operating under secretes, the registry of arbitration awards [
10] is also closed for regular persons, like consumers.
The consumers are often totally, desperately (and even fatally) on their own when facing the medical-legal monopoly (conspiracy?) of our society.
There is only one single source of information that is still available for the public (after considerable trouble and expanses) and that is the Court Indexes and the related databases. Retrieving the medical malpractice cases is the only way today to estimate the risk for potential conflict with a doctor. Filing a medical malpractice claim on a Court against a doctor is a very serious form to express very strong complaints, no doubt about that. It is not important if the doctor was found guilty for wrongdoing or not, the bare existence of the legal complaint is a serious “red flag” for any future potential clients of the sued doctors.
Here we present our pilot study for this consumer dilemma.
Methods & Results
A. MBC Records
The Physician and Surgeon Database [11] lists (accessed on Nov. 8
th, 2017) totally
135,375 persons [
12] with “Current” license in California [i.e. the Licensee meets requirements for the practice of medicine in California]. At about
61,196 are active patient care MDs [
13]. The licensees are listed under
138 categories, corresponding to their specialties there primary and secondary specialties are separated.
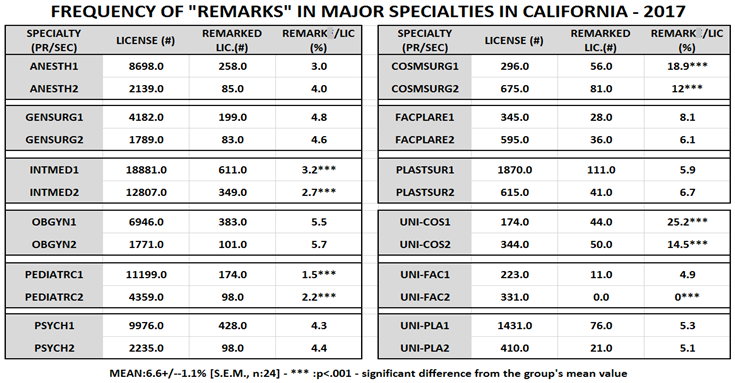
The license’s “secondary status” lists the critical “remarks” (disciplinary actions) against physicians in 37 categories (REF_SecondaryStatusCodeModifier). There are 12.707 remarks altogether [~ one remark/11 licensee = 9 %], issued against 8535 doctors [one or more remark/16 doctors = 6.2 %].
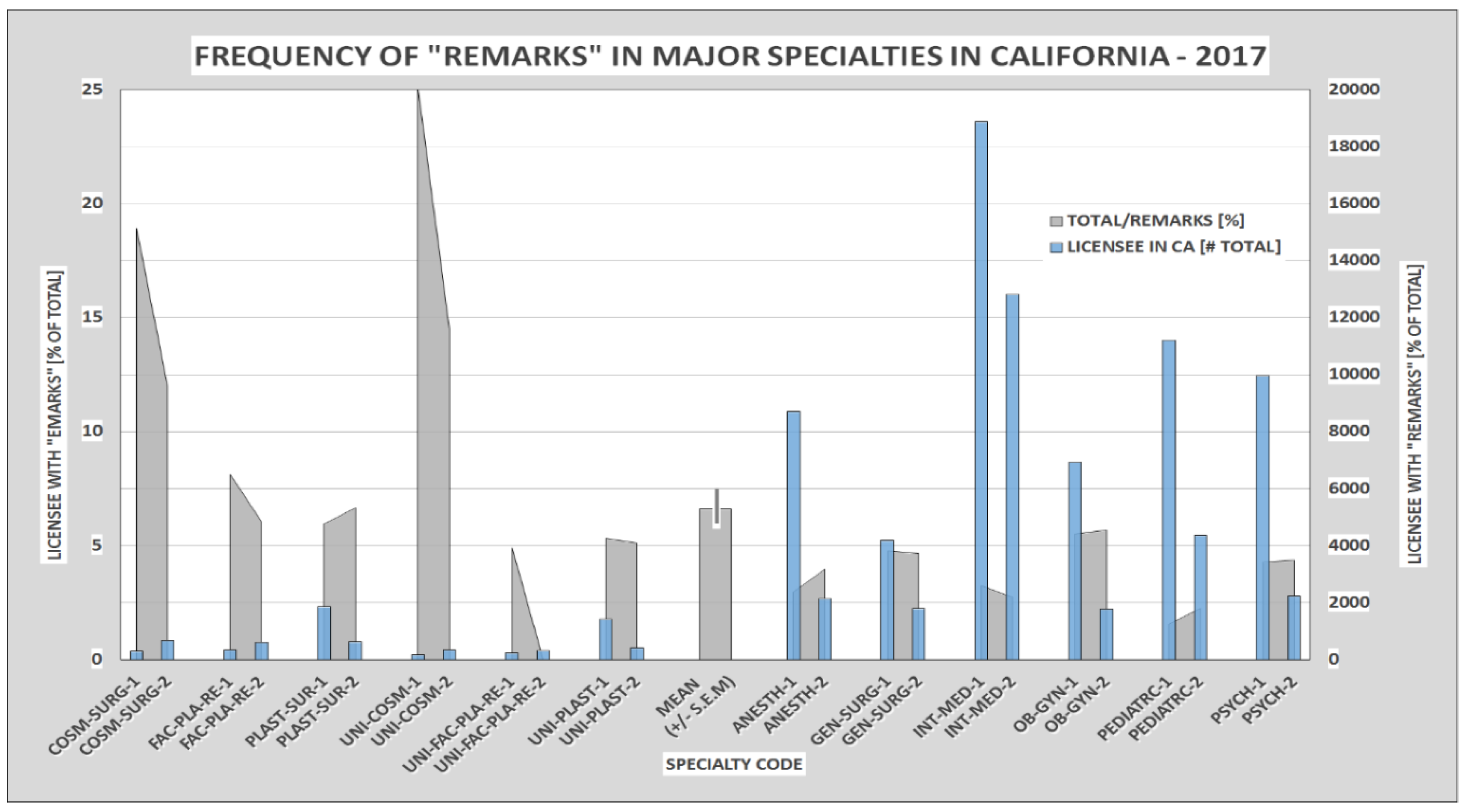
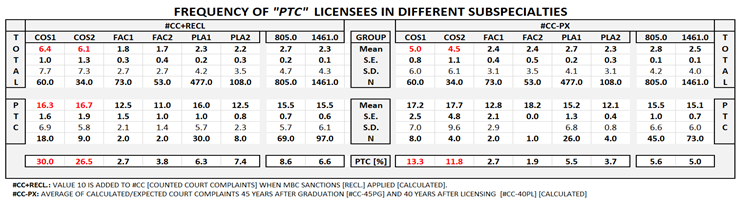
The frequency of remarks and the number of disciplined doctors shows a moderate variation around the 5% resp. 3.3% average in the 6 major medical specialties (anesthesiology, surgery, medicine, gynecology, pediatric and psychology). Somewhat higher frequencies are seen in plastic-/facial plastic surgeries. However remarks against cosmetic surgeons are 4-5-times (SIC!) more frequent than the average for the entire “big” medical profession, which is – of course – a highly significant difference. (Table I. and Figure 1.) Additional information had been provided by the Court records which also support the prominent position of cosmetic surgeons in collecting complaints. (See Table IV).
Figure 1.
Frequency of “remarks” in some major specialties in CA – in 2017. The number of licensees (blue bars, left axis) and the percentage of licensees with “remarks” (green bars, right axis) are compared. The left blue bars and the left edge of the green bars indicates “primary” while the opposite sides indicates the “secondary” specialties. Data were taken from Table I.
Figure 1.
Frequency of “remarks” in some major specialties in CA – in 2017. The number of licensees (blue bars, left axis) and the percentage of licensees with “remarks” (green bars, right axis) are compared. The left blue bars and the left edge of the green bars indicates “primary” while the opposite sides indicates the “secondary” specialties. Data were taken from Table I.
B. COURT Records
Court Indexes and legal tools are another valuable sources of information about a physician. The Court Index of the Superior Court of CA, Los Angeles [
14] and the LexisNexis® [
15] - are examples for his approach.
We have accessed the court history of 1440 randomly selected licensees of total 3572 (accessed on 2017.11.15). This is a pilot study, but the result can be regarded as representative, as it involved 40% of the doctors in question. We identified 2414 different lawsuits for “medical malpractice”, that is in average 1.67 lawsuits/doctor. [This is certainly less than the real number of lawsuits, as the court databases are geographically distributed and no integrative database covers all courts and all cases].
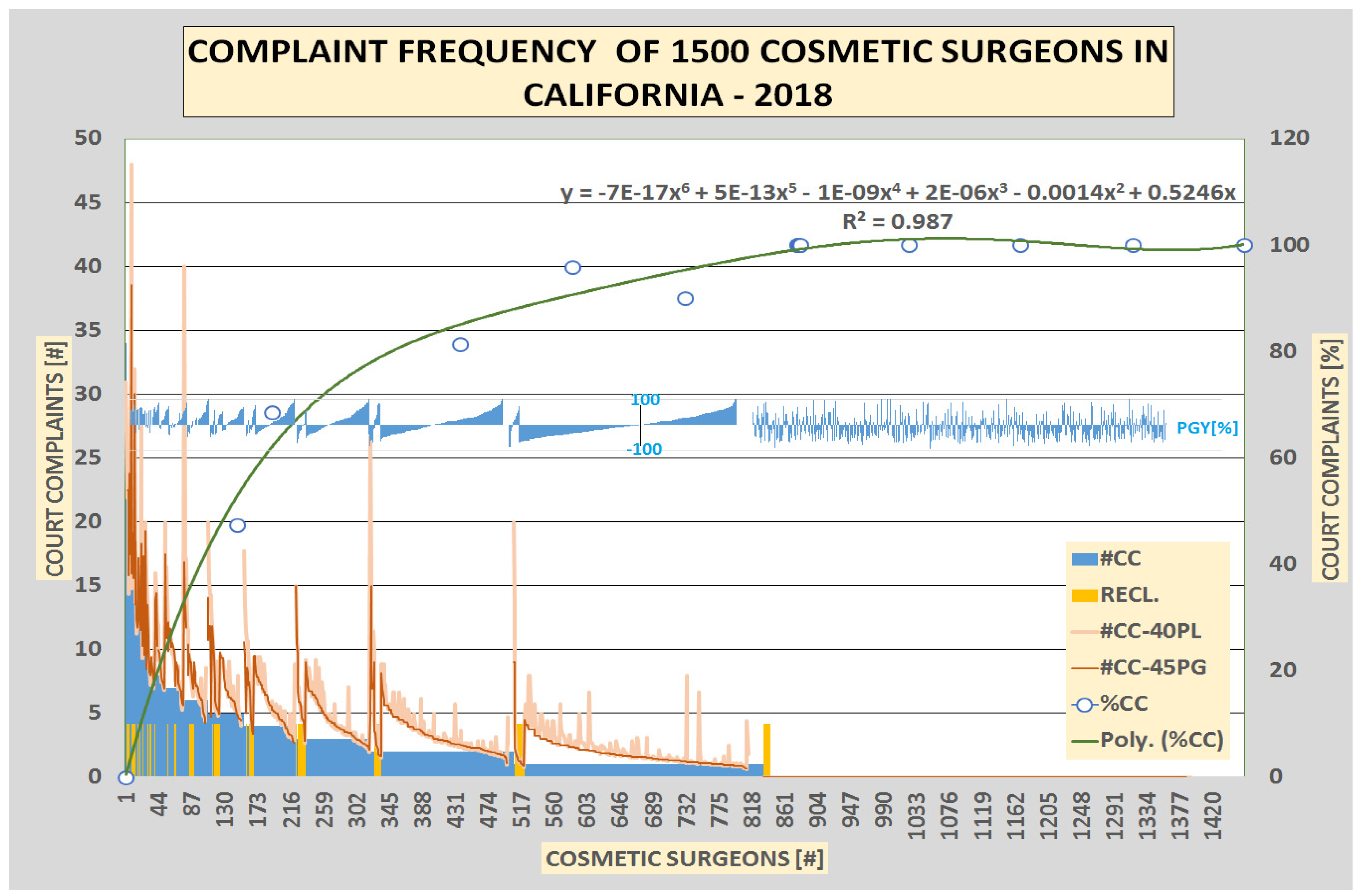
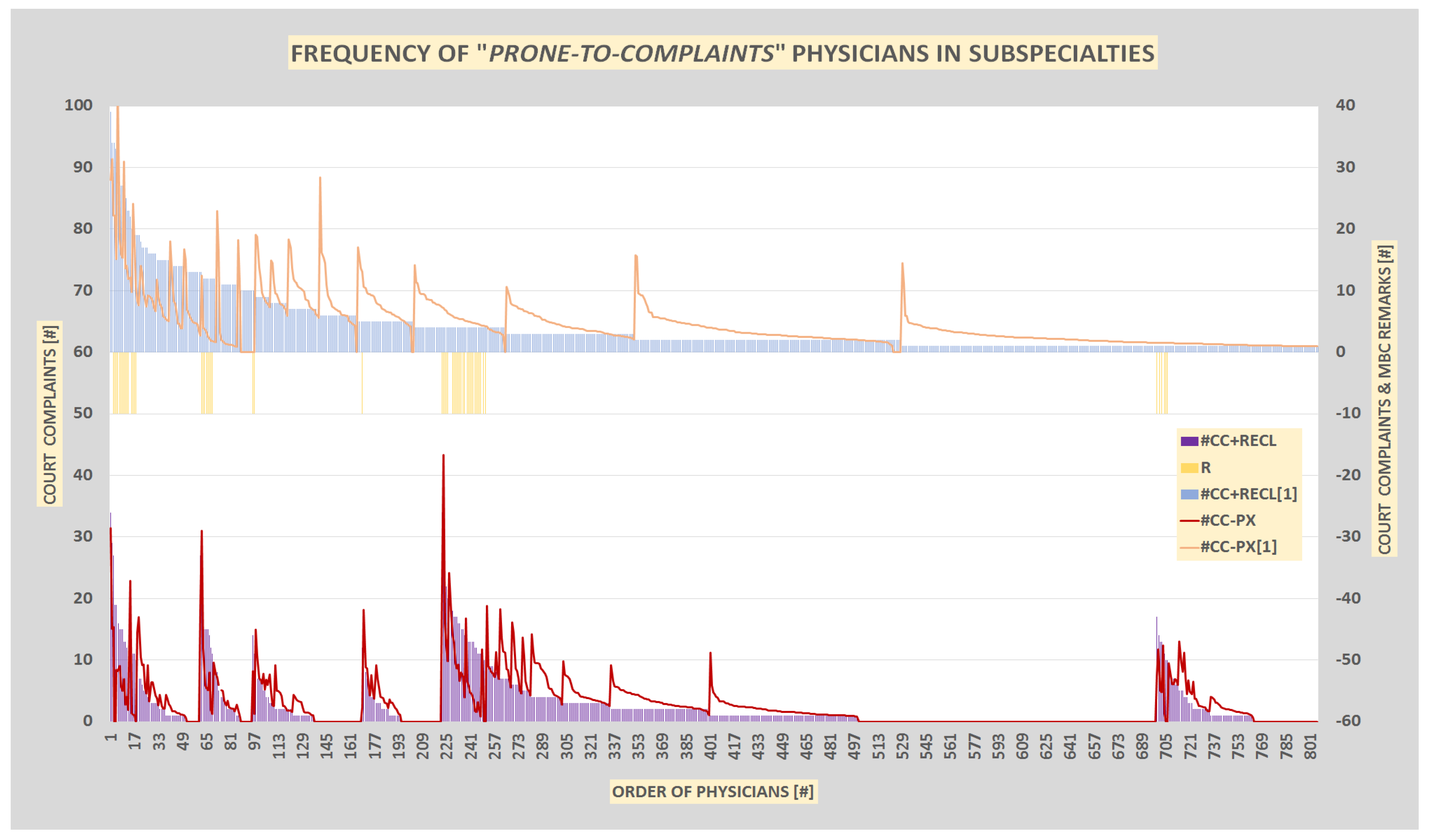
The distribution of court complaints is not even between licensees, not even close. A few doctors are preferentially sued on courts: 20% of doctors are responsible for 60 % of all complaints and 56 % of surgeons covers all complaints [i.e. 44 % of doctors have no lawsuits at all. The 25 most “Prone-to-Complaints” (PTC) doctors [>10 known malpractice complaints; 1.7%] collected 410 court complaints [17%] altogether. (Figure 2.)
This simple counting of the number of court complaints (#CC) provides a general picture about the recent general complaint-burden of the entire specialty in question. However to evaluate the impact of the individual doctors we need to take into consideration the years of the particular doctor in practice [post-graduate years (PGY) or post-licensing years (PLY)] and the patient volume (working hours, turnover) [
16]. In our selection the average PGY and PLY were 30.21+/-0.3 and 25.37+/-0.3 years (mean+/-S. E. M.), respectively. PGY and PLY data have been calculated from the year of graduation and licensing (both available from the licensing board, MBC) however the patient volume is very difficult to estimate.
To eliminate the influence of differences in the PGY and PLY of different doctors, we calculated the expected number of court complaints 45 years after the graduation (#CC-45PG) and 40 years after receiving their license (#CC-40PL), using the equations:
#CC-45PG = #CC/PGY*45 and #CC-40PL = #CC/PLY*40 or #CC-PX = [#CC-45PG + #CC-40PL]/2
(There the #CC are the number of recent, counted Court Complaints for alleged medical malpractice; PGY and PLY are the calculated years after graduation or licensing, respectively.)
The prediction of expected lawsuits (#CC-PG45 and #CC-PL40) provides, understandably, a different set of PTC persons than the courted #CC values. The persons with high predicted values are in the risk to collect numerous additional “real” complaints - as they have many active years before them - if they don’t improve their relation to their consumers. By this way, the #CC are the picture of “today”, while the #CC-PG45 and #CC-PL40 values are the visions of the “future”.
Figure 2.
Complaint Frequency of 1440 Cosmetic Surgeons in California – 2018. The number of individual court complaints (for medical malpractice) (#CC) of 1440 cosmetic surgeon were sorted in descending order and compared to the share in the total 2440 (100%) court complaints accumulated by all entire specialty (%CC). MBC sanctions [RECL: 86 licensees] were indicated by yellow bars. The estimated number of future court complaints 40, 45 years after licensing and graduation, respectively (#CC-40PL and #CC-40PG) are indicated by the two brownish lines. The variation of the age of the physicians are indicated by the variation of PGY around the mean PGY=30 years and expressed as PGY [%] (oscillating blue line across the middle of the figure).
Figure 2.
Complaint Frequency of 1440 Cosmetic Surgeons in California – 2018. The number of individual court complaints (for medical malpractice) (#CC) of 1440 cosmetic surgeon were sorted in descending order and compared to the share in the total 2440 (100%) court complaints accumulated by all entire specialty (%CC). MBC sanctions [RECL: 86 licensees] were indicated by yellow bars. The estimated number of future court complaints 40, 45 years after licensing and graduation, respectively (#CC-40PL and #CC-40PG) are indicated by the two brownish lines. The variation of the age of the physicians are indicated by the variation of PGY around the mean PGY=30 years and expressed as PGY [%] (oscillating blue line across the middle of the figure).
C. IDENTIFICATION of the “Prone-to-Complaints” [PTC] Licensees
The actual number of court complaints (#CC) combined with the two calculated prognostic values (#CC-PG45, #CC-PL40, 3CC-PX) might provide a simple numerical approach to identify “established” and “developing” PTC medical service providers. Licensees who already collected (#CC) or have the calculated potential (#CC-PG45 or #CC-PG40 or #CC-PX) to collect more than 10 court complains were regarded to be PTC persons.
We regarded even the doctors with MBC-remarks [RECL.] as PTC personalities (even in the absence of any court record) as the MBC remark is always the consequence of some extremely serious complaint against that doctor. A remark against a licensee doesn’t necessarily means that he/she has many court complaint too.
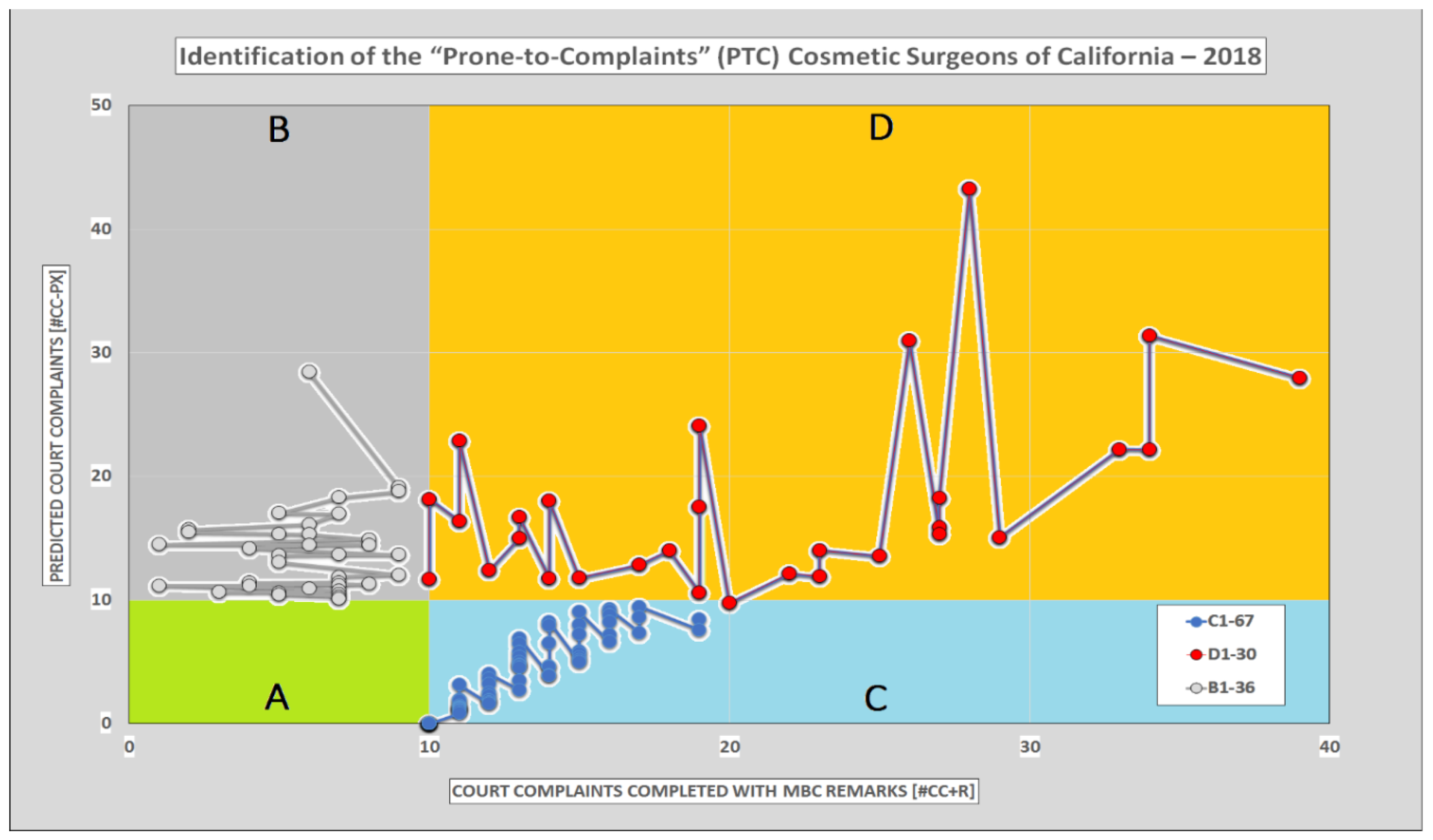
The #CC [>10], #CC-PG45 [>10], #CC-PL40 [>10] and MBC remarks [given value =10] altogether identified 133 licensees. (Table III, Figure 3).
Figure 3.
Identification of the “Prone-to-Complaints” (PTC) Cosmetic Surgeons of California – 2018. The recent Court Complaints completed with eventual MBC remarks (#CC-R) of 1440 cosmetic/plastic surgery licensees were plotted against the calculated (predicted) numbers of Court Complaints (#CC-PX). Licensees with 10 or more recent (blue area, C), predicted (grey area, B) or both (yellow area, D) Court Complaints were identified as PTC individuals. This method identified 133 PTC persons [D: 30 (2.1%), C: 67 (4.6%), B: 36 (2.5%)] while the remaining (green area), A: 1307 (90.8%) remained in the non-PTC category (belonging to A), green empty area). Compare to Table III.
Figure 3.
Identification of the “Prone-to-Complaints” (PTC) Cosmetic Surgeons of California – 2018. The recent Court Complaints completed with eventual MBC remarks (#CC-R) of 1440 cosmetic/plastic surgery licensees were plotted against the calculated (predicted) numbers of Court Complaints (#CC-PX). Licensees with 10 or more recent (blue area, C), predicted (grey area, B) or both (yellow area, D) Court Complaints were identified as PTC individuals. This method identified 133 PTC persons [D: 30 (2.1%), C: 67 (4.6%), B: 36 (2.5%)] while the remaining (green area), A: 1307 (90.8%) remained in the non-PTC category (belonging to A), green empty area). Compare to Table III.
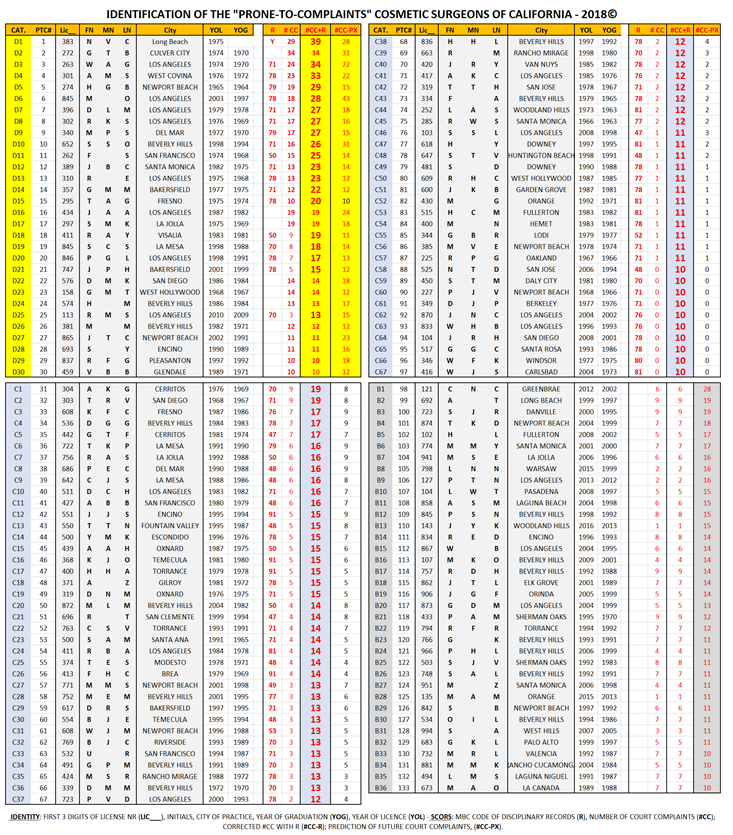
Table III.
Identification of the “Prone-to-Complaints” Cosmetic Surgeons of California – 2018.
Table III.
Identification of the “Prone-to-Complaints” Cosmetic Surgeons of California – 2018.
| List of the 133 Identified PTC Licensees [Preliminary*] - (See APPENDIX) |
D. SPECIALTY Profile
The recent collection of 1440 licensees contains 3 subspecialties (cosmetic, COS; facial- reconstructive, FAC; and plastic, PLA) each further divided into two subgroups, primary and secondary (1 and 2), depending on the physicians priority to practice them. These subspecialties are very different from each other, regarding their patients/consumers, priorities, ethical commitments, et cetera. Therefore, it was important for us to examine the possible differences in the frequency of PTC actors. However, many doctors register and practice different subspecialties in combination or alternatingly during their active time as surgeons. Others register, say plastic surgery as primary specialty, but in reality they practice exclusively cosmetic surgery. Therefore the classification for PTC frequency analyses is difficult and has its limitations. However it is still possible to approach the question, with proper caution, because there are 805 physicians in our pool who are registered to practice only one subspecialty [referred as UNI specialists in this study]. They may have other registered subspecialty within other medical discipline, but outside the COS, FAC, PLA group. (Combination of specialties ENT (Ear, Nose & Throat) and COS are, for example, rather popular today). (Figure 4, Table IV).
The subspecialty search for PTC persons showed one significant difference, namely that cosmetic surgery is heavily populated by PTC personalities. There are more PTC doctors (30%), more complaints (6%) in the COS1, COS2 groups than in in any other groups. The difference is statistically strongly significant, up to 5-fold differences. We found the less PTC doctors and less complaints in the FAC1, 2 groups. Generally there is no difference between primary (1) and secondary (2) specialties regarding the PTC doctors and consumer complaints.
Figure 4.
Frequency of “Prone-to-Complaints” Physicians in Subspecialties. The actual and predicted (PGL40) complaint frequencies (#CC) of 805 UNI specialists are plotted together (upper part of the figure) or separated into 6 sub-specialty groups (lower part of the figure in order of: COS1, COS2, FAC1, FAC2, PLA1, PLA2). The presence of MBC remarks (R), (sanctions), are indicated by yellow bars. A value of 10 had been added to the #CC of the affected licensees (#CC+RECL) to combine the information from MBC (remarks, sanctions) and Courts (malpractice complaints) to a single numerical value which is suitable for statistical analyzes. (See even Table IV for statistical evaluation).
Figure 4.
Frequency of “Prone-to-Complaints” Physicians in Subspecialties. The actual and predicted (PGL40) complaint frequencies (#CC) of 805 UNI specialists are plotted together (upper part of the figure) or separated into 6 sub-specialty groups (lower part of the figure in order of: COS1, COS2, FAC1, FAC2, PLA1, PLA2). The presence of MBC remarks (R), (sanctions), are indicated by yellow bars. A value of 10 had been added to the #CC of the affected licensees (#CC+RECL) to combine the information from MBC (remarks, sanctions) and Courts (malpractice complaints) to a single numerical value which is suitable for statistical analyzes. (See even Table IV for statistical evaluation).
E. GEOGRAPHIC Profile
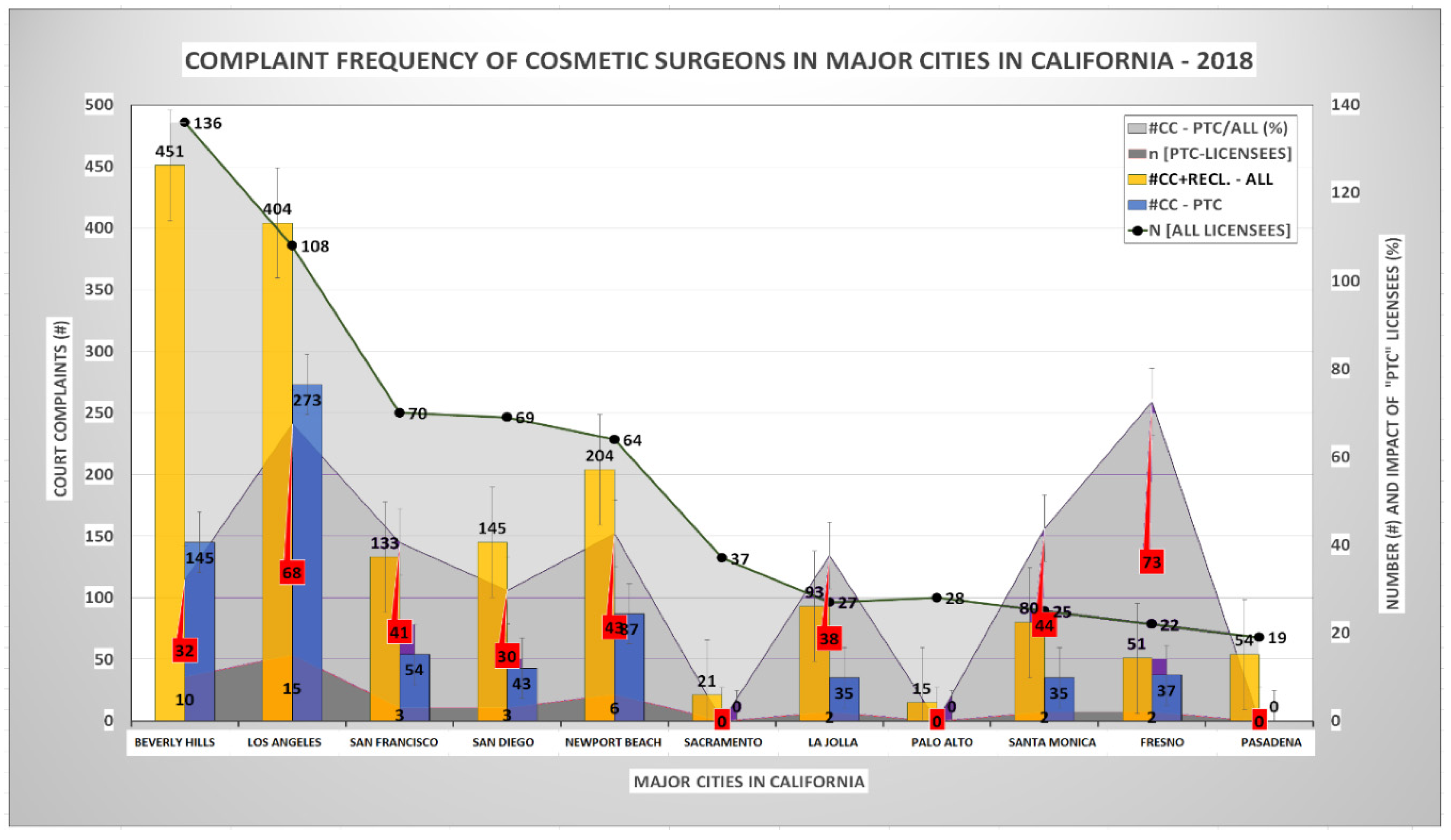
Investigation on the 10 largest cities in California showed that there is a significant correlation between the number of cosmetic surgeons acting in that areas and the number of actual or predicted number of complaints against them, [R2=0.85 and R2=0.87, respectively]. The correlation between the number of doctors and the number of PTC persons or the complaints against PTC licensees is much less significant [R2=0.67 and R2=0.59, respectively]. The possible interpretation is that the number of doctors is not the only determinant of the size of the PTC subgroup. The geographic differences are large. As much as 68-73% of all complaints are directed against PTC doctors in Los Angeles and Fresno. At the same timer Sacramento, Palo Alto and Pasadena have no PTC doctor related complaints at all.
Los Angeles is clearly the largest contributor to the PTC doctors and associated complaints. [As much as 14 cosmetic surgeons (13.5%) have already been the subject of MBC investigations and were “awarded” with sanctions].
Figure 5.
“Prone-to-Complaints” (PTC) Cosmetic Surgeons in California – 2018. The PTC-licensees related statistics for 11 largest cities in CA are sorted in descending order of the number of licensees (N, light grey area). The number of all complaints (#CC+RECL-ALL) and the number of complaints against PTC doctors (#CC+RECL-PTC) are indicated by yellow and blue bars, respectively. The number of PTC doctors (n, dark gray area) and the proportion of complaints against PRC doctors to the complaints against all doctors (#CC-PTC/ALL (%) are indicated by middle-grey areas. A value of 10 had been added to the #CC values when MBC remarks (sanctions) were present (RECL). The inserted numerical values indicate the number of cases and the result of the statistical analyzes (MEAN+/- S. E. M).
Figure 5.
“Prone-to-Complaints” (PTC) Cosmetic Surgeons in California – 2018. The PTC-licensees related statistics for 11 largest cities in CA are sorted in descending order of the number of licensees (N, light grey area). The number of all complaints (#CC+RECL-ALL) and the number of complaints against PTC doctors (#CC+RECL-PTC) are indicated by yellow and blue bars, respectively. The number of PTC doctors (n, dark gray area) and the proportion of complaints against PRC doctors to the complaints against all doctors (#CC-PTC/ALL (%) are indicated by middle-grey areas. A value of 10 had been added to the #CC values when MBC remarks (sanctions) were present (RECL). The inserted numerical values indicate the number of cases and the result of the statistical analyzes (MEAN+/- S. E. M).
F. ESTIMATION of the Annual Medical Malpractice Risk
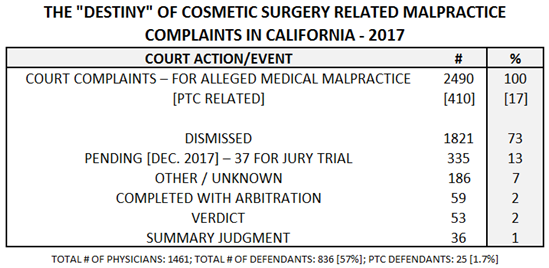
Our recent sample of cosmetic/plastic surgeons and their medical malpractice court cases in California contain 1440 licensees, 2414 (100%) court cases altogether. The recent status and outcome of these cases (November 2017) are summarized in Table V.
The 355 pending cases (on 2017.11.21) were owned by 831 doctors which means that at a given date 831/1462, 57% of all licensees having unsettled, ongoing malpractice allegations. This indicates a very high level of malpractice-complaint risk for Californian cosmetic/plastic surgeons, considering that the estimated annual malpractice risk in other states is ~13% [
17]. [An alternative explanation of this 4.4x difference might be that the transition time of malpractice complaints is much longer in CA than in other states]. However to be sued or convicted for malpractice are two different events: at least 75% a court accusations becomes dismissed without any consequences for the targeted doctor and only a fraction results in monetary sanctions or disciplinary actions.
The “beauty” doctor’s attitude to court complaints (and complaints to the MBC) is therefore rather relaxed.
“Complaint? And what? I will be cleared anyway.” The attitude of medical malpractice insurance companies seems to support this view. The Doctors Company, for example, recognized that doctors are spending too much time with malpractice lawsuits (as much as 10% of their professional time) and encourages their members to focus on their work instead and let the Company’s aggressive lawyers take care of the court trouble [
18]. The company’s opinion is that “
the overwhelming majority of malpractice lawsuits are found to be at best fruitless, and at worst frivolous” [
19]. The Doctors Company emphasizes that it provides the most “
relentless” and “
the industry’s most aggressive” defense of medical malpractice claims against its members, creating an atmosphere in which The Doctors Company has self-proclaimed “
they resolve to fight rather than settle”. The PTC doctors can sleep well in this sunny state.
G. ESTIMATION of the Future Development of Malpractice Complaints
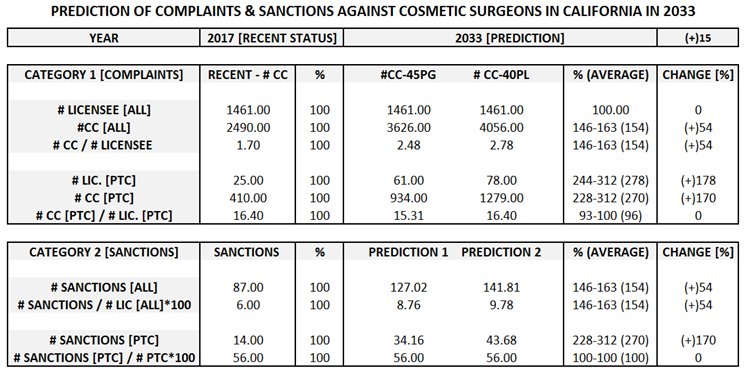
It is challenging to compare the average recent #CC values with the calculated average #CC-PG45 and #CC-PL40 (which predicts the #CC in about 20 years from now, in 2038) and speculate about a trend for the development of PTC persons in the cosmetic surgery business.
Extrapolation of the recent #CC values suggests that the number of PTC licensee will rapidly increase by about 200% and the malpractice complaints against them also by about 200% - that will be ~ 130% above the (“normal”, time related) increase of complaint against the entire cosmetic surgery industry - in CA, during the next 20 years or so. (Table II)
Prediction of the feature on the individual level might be difficult, however a statistical look at the future, for a longer perspective, will definitely provide valuable insights. Exercising some friendly and collegial supervision over the developing (“maturing”) PTC doctors might initiate some positive changes in their conflicting personalities and slow down the “legal carrier” of these surgical artisans.
Discussion
1. The Cosmetic Surgeon’s “Mission Impossible”
Every physician is living in some kind of (manifest or concealed) conflict of interest with their patients. To cure a disease is directly against the personal monetary interest of the physician: a cured patient is a lost consumer, at least temporarily. This conflict is well recognized by the medical societies and that is the origin of the medical ethics. It is clear for most physicians today that ethical rules, like “don’t cause harm” or “prioritize the pat’s interest” [above your own] are essential to build good-will, maintain the trust of the patients and promote the long-term prosperity of the entire medical community.
No physician is an almighty God who can perform miracles. The real power of physicians – that is based on science and understanding and not just on empty psychology – is very, very limited. Most patients know that and not expect from their physicians that they will solve every possible and impossible bodily discomforts for them. They can forgive the shortcomings of medicine and their doctors if the relationship between physician and patient is open, transparent and honest. There is only one major source of conflict between doctors and patients and that is
dishonesty, when the doctor consciously and intentionally lies to his patient [
20]. No person can accept betrayal of genuine trust.
Doctors as highly respected professionals are enjoying the duties and privileges of “professional autonomy” [
21], which means that they can decide almost everything regarding their profession, nobody can or will interfere. This privilege involve supervision, “regular peer review” of each other and keeping the profession clean from crocked actors. As the “
noblesse oblige” the professional autonomy has its obligation too.
Can the cosmetic surgery avoid violating the two most important ethical rules of the medical profession? Where is the limit of tolerance - of the society, courts, other “regular doctors” - for that type of misuse of an honorable profession and its well-deserved professional privileges? There seems to exist two major, very difficult dilemmas for our cosmetic surgeons: a) maximizing profit without hurting too much of their consumers; b) be honest with their consumers, without losing them as clients.
Cosmetic surgery is a commercial activity which is primarily profit oriented, there licensed doctors are selling medical technology and know-how to consumers. It has nothing to do with the traditional doctor/patient relationship, because the doctor is not treating any disease and the consumer is healthy (not patient).
The commercial medicine is a relatively new phenomenon. The difference between the traditional (patient oriented) and the new commercial (profit oriented) medicine is well recognized – and criticized – by the medical experts, but poorly understood by the general public [
22]. The most obvious nature of the cosmetic surgery is the excessive and over-promising advertisement, and its ability to gain non-realistic expectations. The patient’s interest is not primary for cosmetic surgeons which is against the ethical code of the medical profession. [AMA] [
23].
2. The Consumer’s “Mission Impossible”
Consumers usually want to know exactly what are they buying, and the consumer laws provide effective support for them. Medical services are exceptions. There is no warranty for the outcome of any medical action. The “doctor always does his best, but the nature and nurture not always cooperate” – says that – and that is never the doctor’s fault. Cosmetic surgeons are very skillfully using (misusing) this public ignorance.
California has a very doctor-friendly climate. It is impossible to obtain the complaint history of a doctor.
- 1)
The MBC is very slow and bureaucratic organization, there often only public scandals results in necessary actions [24, 25]. The board’s collaboration with the HQES-OAG [
26], that is necessary to the enforcement of medical laws, is the constant source of frustration for the legislator [
27].
- 2)
The plaintiff’s attorneys are practically banned by the MICRA [
28] from the medical malpractice market. An unhappy cosmetic surgery consumer has serious difficulties to find an attorney who is willing to represent him/her before the Court. To be a
pro se litigant and try to represent yourself before judges is just a wasting of time and emotional resources.
- 3)
There are numerous cosmetic surgery related societies. Each one is proudly announcing in their society rules their non-compromising commitment to the quality and high ethical standards. But these are only empty words; in reality the member’s loyalty to each other and their commercial success is much higher than their commitment to their consumers, or the Ethical Code of the profession. Complaint to these societies will remain unanswered [
29]. (It is a well-known observation by persons in published, media cases as well as the authors personal experience based on investigative contacts with several societies in CA, like California Society of Plastic Surgeons, CSPS or Los Angeles Society of Plastic Surgeons, LASPS; AAAASF; The Rhynoplasty Society, American Board of Cosmetic Surgery in CA, ABCS-CA; Aesthetic Surgery Education and Research Foundation, ASERF; American Society of Plastic Surgery, ASPS; California Society of Facial Plastic Surgery, CSFPS) [
30].
Consequently the cosmetic surgery consumers are and remain desperately alone in any kind of consumer complaints against the massive, well-organized, professional money-making pact/conspiracy of “beauty-doctors”. [
31] [This opinion is also based on media references, publicly available rapports (few) and our own very personal and thorough professional investigations] [
32]
There are numerous trade organizations in America - which are serving, primarily, the monetary interest of a branch. People are used to it and the consumer laws and associations seems to provide some fundamental protection against the excesses of these trade organizations. However trade organization which are “camouflaged” to Professional Medical Societies are outside of the protective eyes of the legislator and they are permitted to exist and benefit “big” of the public ignorance. People loves and respect their doctors. It is the result of the humanitarian image of the traditional (patient oriented) doctors, that millions of medical professionals built up under thousands years. The key to this success is the doctors’ commitment to the Ethical Code of the Medical profession, most importantly the principle of “
don’t make harm” (Hippocrates) and the
doctors’ ability to place their own monetary interest second to the health related interest of their patients [
33]. Cosmetic surgeons [with numerous exceptions, of course] often violate these [and other] fundamental ethical rules.
The 20/80 rule (“
the law of the vital few”) [
34] is well recognized by experts monitoring medical activities. It is a well-established observation that a small group of doctors accounts for large parts of all patient complaints. Additionally it is feasible to predict which doctors are at high risk of incurring more complaints in the near future [35, 36]
(The Pareto principle (also known as the 80/20 rule, the law of the vital few, or the principle of factor sparsity) [
1] states that, for many events, roughly 80% of the effects come from 20% of the causes)
3. Caveat Emptor [37]: Un-Orthodox Ways of Getting Informed About a Doctor in California
The “Caveat emptor” is a common law doctrine that places the burden on buyers to reasonably examine property before making a purchase. A buyer who fails to meet this burden is unable to recover for defects in the product that would have been discovered had this burden been met.
However the buyer of a cosmetic surgery cannot examine the expected product before purchasing it and there is no way to return a defective product. Therefore a cosmetic surgery client has to rely on the information about his tentative cosmetic surgeon.
Information about a doctor is extremely restricted for the public. There are public consumer ratings, of course, however these ratings are manipulated by the rated persons and therefore they are serving, mostly, as advertisements. The media frequently picks some extreme cause if the unhappy consumer is laud enough, but these causes have mostly entertainment value and will not change anything. We have experienced that some doctors learned to control the media: their attorneys often effectively threaten the publisher and the negative publication is gone in 24 hrs.
There remains only tree ways to obtain some realistic picture about the real value of a doctor’s medical works and develop some legal strategy for public protection. They are a) utilizing public court databases; b) distributing information via direct, non-mediated (uncensored), personal, social media; c) organizing direct, collective, unmediated public efforts to restrain unprofessional, dishonest surgery service providers.
We used the available (public) Court Databases and related proprietary services (LexisNexis) to monitor complaints against cosmetic/plastic surgeons in California. This is an effective method, because initiation of a lawsuit against a physician for medical malpractice is certainly qualifying as a serious complaint. The bare existence of a court record is a sign of failure for the targeted doctor (no matter what the outcome of the case might have been).
Utilizing the public information in Court Databases against the medical community has a history in USA. This method was first used by the consumer’s attorneys (CAALA) in the battle against doctors over MICRA controversies. In 1985, when a telephone hotline opened up to warn doctors about litigious patients (SIC!), CAALA retaliated by creating a hotline that patients could call to see whether their doctor had been sued for malpractice during the prior 10 years [
38].
We are well aware of the existence of fake claims against medical professionals by claimants who has clearly and only monetary motives. However the malpractice risk according to physician specialty – that exists for every practicing doctor - is statistically measurable. The annual risk for malpractice lawsuit is estimated to be ~6-7% for all medical specialties in America and ~13% for plastic surgery. [
39] The estimated average number of a “normal” plastic surgeon is one claim every 100/13=7.7 years, or ~5 after 40 active years in practice.
The average frequency of malpractice lawsuits is relatively low in our pilot material, only ~1.7 court complaint / cosmetic-plastic surgeon (all times, all ages) [
40] and the predicted average max. 40 years after licensing or 45 years after graduation is ~3/doctor. The average time in practice for doctors in our pilot material is ~25.2 years after licensing (1217 licensee) or 30.1 years after graduation (1200 licensee). We certainly underestimated the number of malpractice lawsuits
We identified 25 cosmetic/plastic surgeons who were defendants in 10 or more malpractice lawsuits. However this count didn’t take the number of years in practice into consideration. Considering the years after graduation and licensing we calculated the expected number of lawsuits at the end of the physicians’ carrier (after 40-45 years in active practice). By this way we predicted, that additional 36 physicians have the potential to pass our 10 Court Complaints / doctor limit some times in the future, during their active period as cosmetic surgeons.
Disciplinary actions against a physician by the licensing agency (with or without the involvement of any Court) are probably the most alarming form of expressed and significant dissatisfaction with the professional actions of a licensee. Generally less than 5% of the doctors have remarks from the MBC, but cosmetic surgeons keeps the “record” with 12-18%.
Disciplinary actions (86) added further persons to our list of PTC physicians, (mostly those who hadn’t been identified by their court history, some having no court records at all).
Our 3 way of identifying “risky doctors” lead (all-together) to the list of 133 licensees who we classify as PTC physicians. It is 9.2% of all cosmetic/plastic surgeons in our pilot collection of 1440 licensees.
4. Past Behavior Is the Best Predictor of Future Behavior
Our statistical data provides information about a large group of physicians and events in the past (malpractice lawsuits, disciplinary notes). The value of this kind of studies to predict medico-legal events at the individual doctor level is, of course, the subject of discussion. [
42] The individual predictive value is certainly low for doctors with few (not above the average) complaints, however it is increasing, exponentially, with increasing number of previous complaints. It had been suggested, that
recurrence was virtually certain for doctors who had experienced 10 or more complaints, with 97% incurring another complaint within a year. [
42]
“Doctors named in a third complaint had a 38% chance of being the subject of a further complaint within a year, and a 57% probability of being complained against again within 2 years (
Figure 2A). Doctors named in a fifth complaint had a 59% 1-year complaint probability and a 79% 2-year complaint probability. Recurrence was virtually certain for doctors who had experienced 10 or more complaints, with 97% incurring another complaint within a year.”
Doctors with PTC label might – and certainly will – argue, that they have especially difficult, complex consumers and they have nothing to do with the high number of complaints against their surgery practices. This argument might work for traditional (patient oriented doctors) who has little or no influence to choose their patients. A commercial (profit oriented) doctor, cosmetic surgeon, has maximal discretion as medical professional to select his clients. The freedom of a cosmetic surgeon to select his/her consumers (healthy buyers of medically not necessary services) is certainly not limited by medical necessity, rather by monetary/profit considerations. The vast majority of cosmetic/plastic surgeons has not this kind of problems, 85% of all doctors on our pilot material has no or less than 3 court records.
[The personal, professional quality of doctors (experience, education, manual skills) is certainly varying. A below average quality doctor can be very valuable for sick patients and under special circumstances, due to the attitude, that “a doctor with some shortcomings is still better, than no doctor at all.” It is certainly not true for commercial doctors, there “only the best is good enough”, i.e. worth for the private money of an already wellbeing consumer. Consequently the worst cosmetic surgeons are under the worst economic pressure and “need to take any case”. Not surprisingly they will end up as PTC actors.]
Consequently we are confident that our selection criteria is very generous and it pinpoints only individuals who will almost certainly be the subject of further serious consumer complaints.
We want to be on the safe side and not accidentally target anybody, even if the purpose of our pilot study is not to present an absolutely certain prediction of future medico-legal events on the individual physicians level. We want to assist and guide potential cosmetic surgery consumers to select their future cosmetic surgeon, knowingly what they are doing and avoid physicians with documented history of serious consumer complaints, i.e. not falling blindly for the glamorous marketing efforts of crocked actors. This initiative is certainly necessary when the designated authorities (MBC, Courts, HQES of OAG, and Professional Societies) are not up to their duty to supervise the quality of a service provided by licensed commercial doctors and enforce the obedience to the well-established standards of good medical care/service and to the professional Ethical Code of the AMA.
5. “Draining the Swamps” [43] in California
The medical/pharmaceutical industry developed to the most controversial area of the modern American life. This is a complex area that engages many persons. Everybody has some opinion about it, mostly without knowing what they are speaking about. In such “messed up” situations we can’t expect reliable guidelines from medical-, legal- or political authorities. We need to go back to the core facts and start the problem solving from the beginning. The core facts, the statistics, tells us very clearly, that our health care system is sick, the medical organizations often misuse the traditional professional autonomy in their own interest, there is no adequate supervision over the activity of doctors. We should face the facts, that there are some doctors, probably not more than 10% of all, who are not benefiting their patients and without them we (“The People”) would feel much better.
There were numerous efforts before to condemn the cosmetic surgery for its eccentric nature and profoundly deviant practices. However all these efforts failed, this specialty grows and gains in power. The services of “beauty doctors” are attractive for the (ignorant) public and the actors are skilled to keep their weaknesses concealed from the potential consumers. Dreaming about beauty can cost whatever it wants to cost. Therefor we prefer a continued positive attitude toward cosmetic surgery as a specialty and will focus our critics toward those doctors who are responsible for most of the bad reputation of this “beauty industry”.
Identifying the PTC actors is the first step to clean up this specialty from fraudulent doctors, provide the potential consumers the possibility to make informed decision when choosing his or her “body-sculptor” and, by that way, secure the consumer rights even in this white-rock territory.