
Submitted:
13 January 2025
Posted:
14 January 2025
You are already at the latest version
Abstract
OBJECTIVE– Sleep deprivation is a common problem in the society and bedtime procrastination has emerged as a major cause of poor sleep among the healthy individuals across various nations. We attempted to study the bedtime procrastination, sleep behavior, subjective well-being in the Indian population.
METHODS – This was a cross-sectional study. The recruited participants were evaluated on the Bedtime procrastination scale(BtP), WHO-5 Well Being index, Patient Health Questionnaire-2 (PHQ -2), Generalized Anxiety Disorder 2-item (GAD -2), Munich Chronotype questionnaire (MCTQ) and Single-Item Sleep Quality Scale (SQS).
RESULTS – A total of 401 participants were recruited to the study. Symptoms of anxiety were higher in the female participants compared to males. Among females, there was a significant positive correlation of Bedtime procrastination score with symptoms of anxiety(r=0.23) and depression(r=0.15) and a negative correlation with subjective well-being(r=-0.23). A significant negative correlation was found between ages of women and BtP score(r=-0.15). Among the male participants, there was a significant negative correlation of age with BtP score(r=-0.3) and anxiety(r=-0.19). Here too, BtP score was positively correlated with depression(r=0.18) and anxiety(r=0.35).
CONCLUSION- Bedtime procrastination has a close and intricate association with anxiety, depression, sleep quality and subjective well-being. It needs to be targeted for the promotion and prevention of mental health.
Keywords:
Bedtime Procrastination
; Sleep Quality
; Subjective Well-Being
; Anxiety
; Depression
; Sleep
Introduction
The Centre for Disease Control (CDC) classifies sleep deprivation as a public health epidemic associated with the development of a variety of diseases [1]. The American Academy of Sleep Medicine and Sleep Research Society developed a consensus recommending a minimum 7 hours of sleep per night for adults, otherwise associated with adverse health outcomes like metabolic disturbances, mental health disorders and increased risk of death [2].
While the effects of good sleep are well known, incidences of poor sleep have increased in post-pandemic era with significant effects on the functionality of a person. An online survey reported that 61% of the 41,000 respondents from India slept for less than 6 hours of uninterrupted sleep in the past 1 year [3]. A survey done by Gupta et al., after COVID-19 lockdown in the Indian population on a sample size of 958 observed significant change in sleep habits compared to the pre-lockdown, in terms of later bedtime, delayed sleep onset and increased day time napping. Reduced sleep and an increased incidence of depressive symptoms were observed across different occupational groups [4]. Dunn et al reported poor sleep quality, prolonged latency and excessive daytime sleepiness more in the later years of college due to academic requirements among university students in India [5]. Chronic sleep deprivation has significant effects on memory span, decision making, executive function, planning, social cognition, and verbal learning [6].
The term “Revenge Bedtime procrastination” has gained fame post-pandemic on various social media platforms, glorifying it as a cause of sleep deprivation in healthy individuals. Zhang et al in a study in 2020 studied effects of smartphone addiction and bedtime procrastination on sleep quality of university students [7]. They found a positive relationship between bedtime procrastination and poor sleep quality. Similar studies have been conducted on the Indian population to show the detrimental effects of smartphone dependency on general health profile [8], sleep quality [9,10], cyberchondriac behavior, health anxiety and subjective well-being [11].
Kroese et al first introduced this phenomenon called Bedtime Procrastination, defining it as “failing to go to bed at the intended time, while no external circumstances prevent a person from doing so”. Bedtime procrastination (BtP) is widespread among young people [12,13]. Furthermore, studies were conducted to understand its prevalence and association with sleep quality, depression and anxiety [10,14,15,16,17]. A meta-analysis by Hill et al studying BtP reported bedtime procrastination was moderately negatively associated with sleep duration (z = −0.31; CI: −0.37, −0.24), sleep quality (z = −0.35; CI: −0.42, −0.27) and moderately positively associated with daytime fatigue (z = 0.32; CI: 0.25, 0.38) [18].
To our knowledge, only one study has been done in India by Shukla et al to determine the prevalence of BtP among Indian university students [19]. Despite the absence of published research exploring the causes and impacts of bedtime procrastination, we hypothesize that this phenomenon is widespread within the general Indian population. We believe it contributes to diminished subjective sleep quality, adversely affects mental health, and compromises subjective well-being. Our study seeks to provide a comprehensive assessment of the prevalence of bedtime procrastination among individuals in India, exploring into the underlying factors that contribute to this behavior. Additionally, we aim to examine the subsequent effects of bedtime procrastination on sleep quality, psychological health, and overall well-being, shedding light on a critical issue that may be influencing many individuals' daily lives.
Methods
Study Design
The study was a web-based cross-sectional study conducted under the Department of Psychiatry of a tertiary center in Lucknow. A self-reporting questionnaire was created using Google Forms. Convenience sampling was used to collect data. The questionnaire was circulated to all the contacts in the University including students, professors and workers using the email ID database available at the university portal. Further, the questionnaire was made available to a larger population by circulating the questionnaire link on social media networking sites like WhatsApp, Twitter, Facebook, Instagram, Telegram. Duplication of respondents was eliminated as only a single response was admissible for one email-ID.
Participants residing in India and of ages between 18– 60 years were included in the study. The exclusion criteria included patients reporting diagnosed psychiatric disorders (except personality disorders), sleeping disorders or respiratory illnesses like asthma, Chronic Obstructive Pulmonary Diseases (COPD). The sample size for this study was found to be 385, considering expected prevalence 50% and 95% confidence interval with 5% margin of error in an infinite population using the iface sample size estimation software (https://sampsize.sourceforge.net/iface/).
Study Instruments
We created a Google Form consisting of multiple parts. The first part included personal details like e-mail ID, age, gender, residence, highest completed level of education, co-morbidities and any recreational drug use practices.
Bedtime procrastination scale [20]: A nine-item questionnaire originally developed by Kroese et al., with a five-point Likert scale. It consists of five negative and four positive statements. Each item can score from 1 (almost never) to 5 (almost always) while items 2, 3, 7, and 9 are reverse coded. Hence, the range of total scores is 9-45, with larger scores indicating a higher frequency of engaging in bedtime procrastination.
WHO-5 Well-Being Index [21]: It is a five-item questionnaire consisting of five statements answered on a Likert scale. It is a simple tool for screening general well-being.
Patient Health Questionnaire-2 [22]: It is a two-item scale used to inquire about the frequency of depressed mood and anhedonia. Its score ranges from 0-6. A score of 3 or more is indicative of likely depression.
Generalized Anxiety Disorder 2-item [23]: It consists of two questions to be answered by the subject for initial screening of generalized anxiety disorder. The score ranges from 0-6 and 3 is the preferred cut-off.
Munich Chronotype questionnaire (MCTQ) [24]: It is a self-reporting questionnaire to test typical sleep behavior over the 4 past weeks for work days and work-free days separately.
Single-Item Sleep Quality Scale (SQS) [25]: It is a self-rated, global sleep quality assessment tool. The questionnaire requires the respondent to rate the overall quality of sleep over a 7-day recall period on a discretizing VAS, whereby the respondent marks an integer score from 0 to 10, according to the following five categories: 0 = terrible, 1–3 = poor, 4–6 = fair, 7–9 = good, and 10 = excellent.
Data Analysis
The data obtained from Google Forms will be tabulated in Excel sheets and the prevalence of Bedtime procrastination will be determined for different subgroups and compared.
In our study, categorical variables was analysed using Pearson’s chi-square test and continuous variables were analysed using t-test. p- values less than 0.05 were considered statistically significant. Statistical analysis was performed using the IBM Statistical Package for Social Sciences (IBM SPSS version 24.0).
Results
Total number of participants in the study was 401 of which 176 were males and 224 were females (Figure 1). The general characteristics of the dataset are given in Table 1. The result shows, 2.8% of men went to sleep between 9-10 PM, 52% between 10-12 PM, 25% between 12-1 while a few after 1 AM(18%). Among women, 3% go to sleep before 10 PM, 45 % between 10 to 12 AM, 26% between 12 to 1 AM while around 23 % go to sleep after 1 AM. Around 51% of males woke up between 6-8 AM, 20% between 8-9 and around 30% woke up after 9 AM. Among women, 50% woke up between 6-8 AM, 19% between 8-9 AM and only 12 % woke up after 9 AM (Figure 2). More than 40% of the participants use their electronic gadget for more than 6 hours per day on an average and professional work is the single most common reason for use of electronic gadget (Table 2).
Symptoms of anxiety were significantly higher in the female group (2.19±1.5) compared to the male group (1.5±1.38) (t (398)=4.4, p<0.05). Subjective well-being was slightly higher in males (54.7±20.02) than in the females(52.03±20.0) (t(398)= 1.98, p=0.04). A significantly higher number of females(n=74) screened positive for depression using GAD-2(Chi-square= 9.409, p =0.002) (Table 3).
Among males, there was a significant negative correlation of age of participants with bedtime procrastination score(r=-0.3) and anxiety(r=-0.19). Sleep latency had a significant negative correlation with subjective well-being(r=-0.24) and sleep quality(r=-0.24) while a positive correlation with procrastination time((r=0.4). The duration of sleep has a significant negative correlation with procrastination time(r=-0.27). A significant positive correlation has been reported between procrastination time with bedtime procrastination score(r=0.2), depression(r=0.27) and anxiety(r=0.29) while a negative correlation was reported with subjective well-being (r=-0.19) and sleep quality(r=-0.3). The bedtime procrastination score has a significant positive correlation with depression(r=0.18) and anxiety(r=0.35); whereas a negative correlation is seen with sleep quality(r=-0.25) (Table 4A).
A significant negative correlation was found between ages of the female participants with bedtime procrastination score (r=-0.15), depressive symptoms(r=-0.16), anxiety symptoms(r=-0.15) and sleep quality(r=-0.13). Sleep latency has a significant negative correlation with duration of sleep(r=-0.15), subjective wellbeing (r=-0.14) and sleep quality(r=-0.13) and a significant positive correlation with procrastination time (r=0.17). The duration of sleep has a significant negative correlation with bedtime procrastination score (r=-0.18) and a significant positive correlation with sleep quality(r=0.32). A significant positive correlation has been reported between procrastination time with bedtime procrastination score(r=0.15) and anxiety(r=0.19). The bedtime procrastination score has a significant positive correlation with depression(r=0.15) and anxiety(r=0.23); whereas a negative correlation is seen with subjective wellbeing(r=-0.23) and sleep quality(r=-0.24). Anxiety and depression have a significant negative correlation with sleep quality and subjective well-being (Table 4B).
Discussion
The demographic analysis revealed a predominance of participants aged 18 to 50 years, primarily from urban areas, and a slight female majority. In males, we saw a decrease in bedtime procrastination scores and depressive symptoms with increasing age. A similar trend was noted in the female group, in addition to a decrease in GAD-2 score and overall improvement in the perceived sleep quality with age.
Bedtime procrastination is widespread among young people [12,13]. The age-related trends observed in our male and female cohorts may suggest that older adults may adopt healthier sleep practices, possibly due to increased awareness of the consequences of poor sleep or shifts in lifestyle priorities. This might also be because young adults, mostly university students or in their early career, have compromised sleep due to academic burdens or career progression. A cross-sectional study intending to detect EDTS among college students found that students taking professional courses and in science streams seem to be more at risk [26].
In our study, there was no significant difference among both the genders in reporting perceived poor sleep quality using the single item SQS. However, females had fewer hours of sleep. This is in conjunction with the study done by Shad et al [27] in college students of medical and non-medical backgrounds, that sleep quality did not significantly differ by gender.
Various studies have had different findings in this arena, two studies reported that females had significantly better sleep times and quality than males [28,29]. While a study by Kaur found that sleep quality was worse among female undergraduate non-medical students [30].
Our analysis revealed increased screening rates for anxiety and depression and decreased perceived sleep quality and overall well-being score with increasing BtP score. Two studies found an independent association between depression and BtP, where the severity of depression increased with increasing BtP, eventually contributing to depression [15,16].
Furthermore, studies have shown that anxiety has a positive effect on BtP [14], which is expected since people with high anxiety levels also have high avoidance behavior and may regulate negative emotions through BtP [31]. A study done by Li et al reported higher procrastination scores were associated with higher risks of insomnia symptoms [32].
While for students the main cause of procrastination was studying, professionals procrastinated mainly for leisure or for the completion of work. Other responses included stress, surrounding atmosphere, irregular schedule and children. In a qualitative study by Nauts et al., individuals with BtP reported that when they were tired and stressed at the end of the day, they opted to delay their bedtime and engage in different activities despite knowing its negative impact on their sleep [33]. They distinguished between deliberate procrastination, mindless procrastination and strategic delay.
Paula Magalhães and colleagues further distinguished bedtime procrastination and While-in-Bed Procrastination as different entities. Their study reported 59.5% of participants engaging in While-in-bed procrastination while the rest procrastinated before going to bed [34]. From the data collected by the short MCTQ tool, we were able to calculate both bedtime procrastination and while-in-bed procrastination among the participants. Bedtime procrastination could only be calculated among participants who had different workdays and weekend schedules. While-in-bed procrastination seems to be highly prevalent among the participants with 117 males and females reporting more than 15 minutes of procrastination while in bed. The individuals with more procrastination time had higher Bedtime procrastination scores and fewer hours of sleep and perceived sleep quality as poor. They also had higher scores for anxiety and depression and low scores for perceived general well-being. More procrastination time was related to increased sleep latency.
Alarm dependency was seen in 71.75% (287) participants. 50% of participants took more than 5 minutes to get out of bed after waking up. 32% of participants had a delayed sleep schedule on weekends only.
Our data mainly comprised students pursuing professional courses (37.4%) and salaried persons (35.6%). A longitudinal study done to find correlation between work settings and sleep revealed that persons without children had longer and better sleep in doing work from home(WFH) as compared to office(WFO) [35]. Also, WFH persons had higher wellbeing compared to WFO. Although in our study, participants with WFH mentioned children as a cause of delay to going to bed but had equal risk of high bedtime procrastination scores and poor sleep and low well-being scores.
All participants had personal electronic gadgets. 40% of them spent more than 6 hours on gadgets. 30.6% used electronic devices mainly for professional work,28.4% for studies, 20.4% for social media usage and 18.9% mainly for entertainment. 110 participants (27.5%) used their gadgets before going to sleep, in bed while 84 in late at night before going to bed. We found no correlation between usage of electronic gadgets before bedtime and sleep disturbances or poor mental health.
Sleep latency had a significant negative correlation with durations of sleep, subjective wellbeing and sleep quality and a significant positive correlation with procrastination time.
The prevalence of Bedtime Procrastination was evident in the respondents, although much less participants reasoned it to leisure but for making up for work or studies. More procrastination time led to altered sleep quality by affecting their sleep latency which in turn affected their mental and overall well-being. No other risk factor was identified in the study that predisposed the individuals to BtP or poor sleep quality.
Our study included an array of healthy individuals belonging to different sectors of profession and age. We tried to address problems developing with bedtime procrastination as there is lack of such data from Indian population. Since a significant proportion of our sample came from a professional background, we cannot generalize our findings to a larger subset of the population. Also, we worked with a limited sample size. Since it was a cross-sectional study we cannot conclude our study regarding bedtime procrastination and cognitive dysfunction in an individual.
A wider survey including a larger sample to study the sleep patterns of the general Indian population can help to make better strategies for the prevention of mental health problems.
Conclusion
We concluded that a positive correlation exists between increased bedtime procrastination score and depression and anxiety while it reduced the feeling of subjective well-being. It was associated with a poor sleep quality and higher sleep latency. Previous literature suggests similar detrimental effects of electronic gadgets and work pressure affecting sleep quality but only a handful of them coming from the Indian subcontinent. We also noted that bedtime procrastination and poor sleep quality were higher in the younger age group compared to older people. We also showed that a lot of people attributed their bedtime procrastination to professional activities rather than leisure activities. Bedtime procrastination has become a rising problem in our society and more work in this area is required to tackle it and spread awareness among the society.
References
- Ramos AR. Sleep Deprivation, Sleep Disorders, and Chronic Disease. Prev Chronic Dis 2023, 20, 230197. [CrossRef]
- Watson NF, Badr MS, Belenky G, et al. Recommended Amount of Sleep for a Healthy Adult: A Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep 2015, 38, 843–844.
- LocalCircles. 61% Indians are getting less than 6 hours of uninterrupted sleep. LocalCircles. Available online: https://www.localcircles.com/a//press/page/world-sleep-day-survey (accessed on 12 January 2025).
- Gupta R, Grover S, Basu A, et al. Changes in sleep pattern and sleep quality during COVID-19 lockdown. Indian J Psychiatry 2020, 62, 370. [CrossRef]
- Dunn C, Goodman O, Szklo-Coxe M. Sleep duration, sleep quality, excessive daytime sleepiness, and chronotype in university students in India: A systematic review. J Health Soc Sci 2022, 7, 36–52. [Google Scholar]
- Ramrakhiyani VC, Deshmukh SV. Study of the incidence and impact of chronic sleep deprivation in Indian population with special emphasis on neuropsychology testing. Sleep Med 2019, 14, 23–28. [Google Scholar]
- Zhang MX, Wu AMS. Effects of smartphone addiction on sleep quality among Chinese university students: The mediating role of self-regulation and bedtime procrastination. Addict Behav 2020, 111, 106552. [Google Scholar] [CrossRef] [PubMed]
- Mishra S, Kar SK, Shankar A. Internet addiction and health profile among medical, dental and nursing graduates of India. Minerva Psychiatry; 64. Epub ahead of print August 2023. [CrossRef]
- Chatterjee S, Kar SK. Smartphone Addiction and Quality of Sleep among Indian Medical Students. Psychiatry 2021, 84, 182–191. [Google Scholar] [CrossRef]
- Haque S, Singh S, Narayan J, et al. Effect of smartphone use on sleep and mental health status of Indian medical students: a cross-sectional study. Int J Res Med Sci 2024, 12, 3737–3746. [Google Scholar] [CrossRef]
- Agrawal V, Khulbe Y, Singh A, et al. The digital health dilemma: Exploring cyberchondria, well-being, and smartphone addiction in medical and non-medical undergraduates. Indian J Psychiatry 2024, 66, 256. [Google Scholar] [CrossRef]
- Kadzikowska-Wrzosek, R. Insufficient Sleep among Adolescents: The Role of Bedtime Procrastination, Chronotype and Autonomous vs. Controlled Motivational Regulations. Curr Psychol 2020, 39, 1031–1040. [Google Scholar] [CrossRef]
- Kroese FM, Evers C, Adriaanse MA, et al. Bedtime procrastination: A self-regulation perspective on sleep insufficiency in the general population. J Health Psychol 2016, 21, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Campbell RL, Bridges AJ. Bedtime procrastination mediates the relation between anxiety and sleep problems. J Clin Psychol 2023, 79, 803–817. [Google Scholar] [CrossRef]
- Guo J, Meng D, Ma X, et al. The impact of bedtime procrastination on depression symptoms in Chinese medical students. Sleep Breath 2020, 24, 1247–1255. [Google Scholar] [CrossRef]
- Hou X, Hu J. Depression and bedtime procrastination: Chain mediation of brooding and perceived stress. Heliyon 2023, 9, e22672. [Google Scholar] [CrossRef] [PubMed]
- Ma X, Meng D, Zhu L, et al. Bedtime procrastination predicts the prevalence and severity of poor sleep quality of Chinese undergraduate students. J Am Coll Health J ACH 2022, 70, 1104–1111. [Google Scholar] [CrossRef]
- Hill VM, Rebar AL, Ferguson SA, et al. Go to bed! A systematic review and meta-analysis of bedtime procrastination correlates and sleep outcomes. Sleep Med Rev 2022, 66, 101697. [Google Scholar] [CrossRef]
- Shukla A, Andrade C. Prevalence of Bedtime Procrastination in University Students and Reexamination of the Bedtime Procrastination Scale. Prim Care Companion CNS Disord 2023, 25, 22m03334. [Google Scholar]
- Kroese FM, De Ridder DTD, Evers C, et al. Bedtime procrastination: introducing a new area of procrastination. Front Psychol; 5. Epub ahead of print June 19, 2014. [CrossRef]
- Topp CW, Østergaard SD, Søndergaard S, et al. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother Psychosom 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Kroenke K, Spitzer RL, Williams JBW. The Patient Health Questionnaire-2: validity of a two-item depression screener. Med Care 2003, 41, 1284–1292. [Google Scholar] [CrossRef]
- Plummer F, Manea L, Trepel D, et al. Screening for anxiety disorders with the GAD-7 and GAD-2: a systematic review and diagnostic metaanalysis. Gen Hosp Psychiatry 2016, 39, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Jankowski, KS. Composite Scale of Morningness: psychometric properties, validity with Munich ChronoType Questionnaire and age/sex differences in Poland. Eur Psychiatry 2015, 30, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Snyder E, Cai B, DeMuro C, et al. A New Single-Item Sleep Quality Scale: Results of Psychometric Evaluation in Patients With Chronic Primary Insomnia and Depression. J Clin Sleep Med JCSM Off Publ Am Acad Sleep Med 2018, 14, 1849–1857. [Google Scholar]
- Kaur G, Singh A. Excessive daytime sleepiness and its pattern among Indian college students. Sleep Med 2017, 29, 23–28. [Google Scholar] [CrossRef]
- Shad R, Thawani R, Goel A. Burnout and Sleep Quality: A Cross-Sectional Questionnaire-Based Study of Medical and Non-Medical Students in India. Cureus 2015, 7, e361. [Google Scholar]
- Giri P, Baviskar M, Phalke D. Study of sleep habits and sleep problems among medical students of pravara institute of medical sciences loni, Western maharashtra, India. Ann Med Health Sci Res 2013, 3, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Manzar MD, Zannat W, Kaur M, et al. Sleep in university students across years of university education and gender influences. Int J Adolesc Med Health 2015, 27, 341–348. [Google Scholar] [CrossRef]
- Kaur, G. A study on the sleep quality of Indian college students. JSM Brain Sci 2018, 3, 1018. [Google Scholar]
- Ball TM, Gunaydin LA. Measuring maladaptive avoidance: from animal models to clinical anxiety. Neuropsychopharmacol Off Publ Am Coll Neuropsychopharmacol 2022, 47, 978–986. [Google Scholar] [CrossRef]
- Li X, Buxton OM, Kim Y, et al. Do procrastinators get worse sleep? Cross-sectional study of US adolescents and young adults. SSM - Popul Health 2020, 10, 100518. [Google Scholar] [CrossRef] [PubMed]
- Nauts S, Kamphorst BA, Stut W, et al. The Explanations People Give for Going to Bed Late: A Qualitative Study of the Varieties of Bedtime Procrastination. Behav Sleep Med 2019, 17, 753–762. [Google Scholar] [CrossRef]
- Magalhães P, Cruz V, Teixeira S, et al. An Exploratory Study on Sleep Procrastination: Bedtime vs. While-in-Bed Procrastination. Int J Environ Res Public Health 2020, 17, 5892. [Google Scholar] [CrossRef]
- Massar SAA, Ong JL, Lau T, et al. Working-from-home persistently influences sleep and physical activity 2 years after the Covid-19 pandemic onset: a longitudinal sleep tracker and electronic diary-based study. Front Psychol 2023, 14, 1145893. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram showing recruitment of participants to the study.
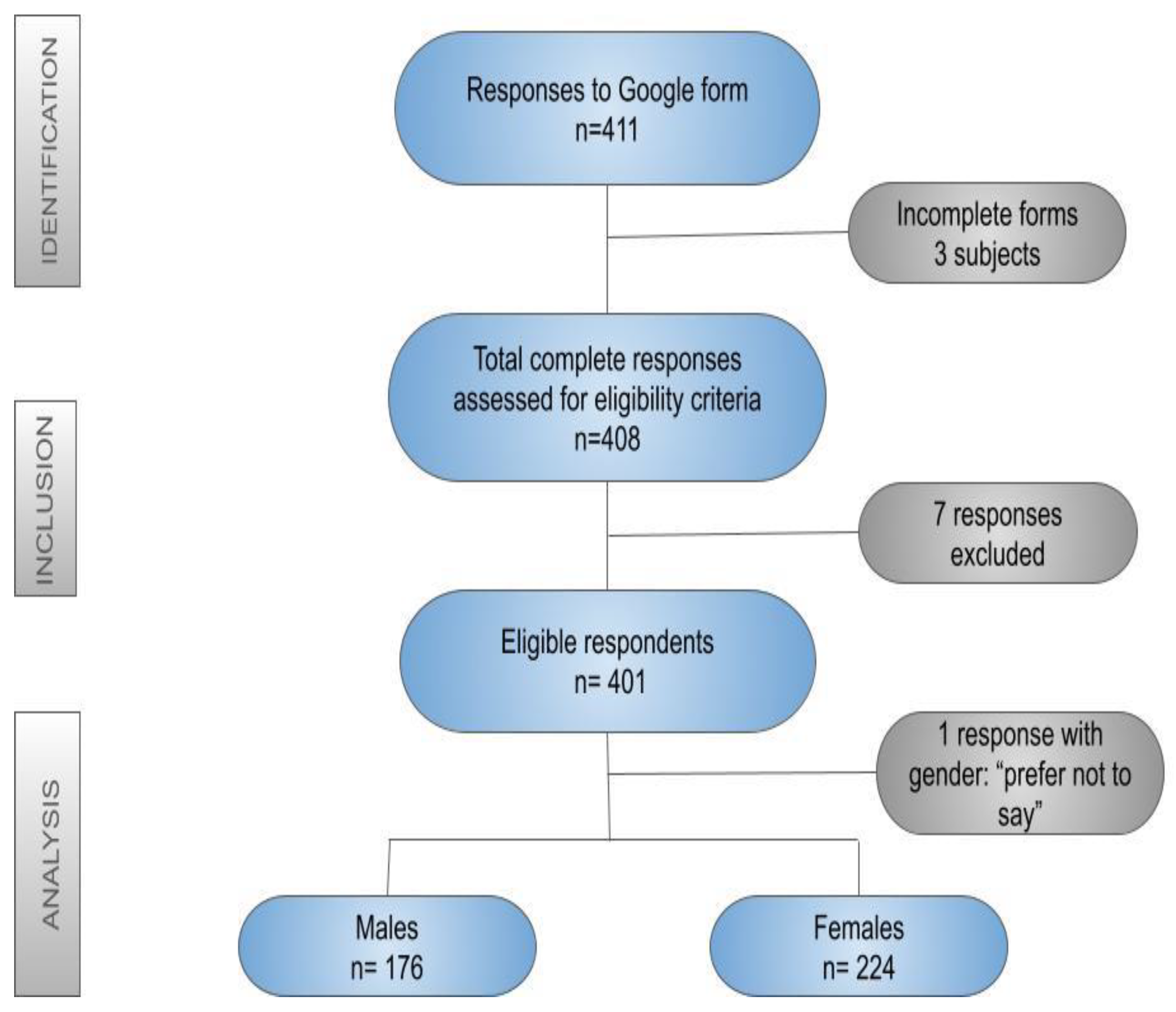
Figure 2.
Bed-time and wake-up time of male and female participants.
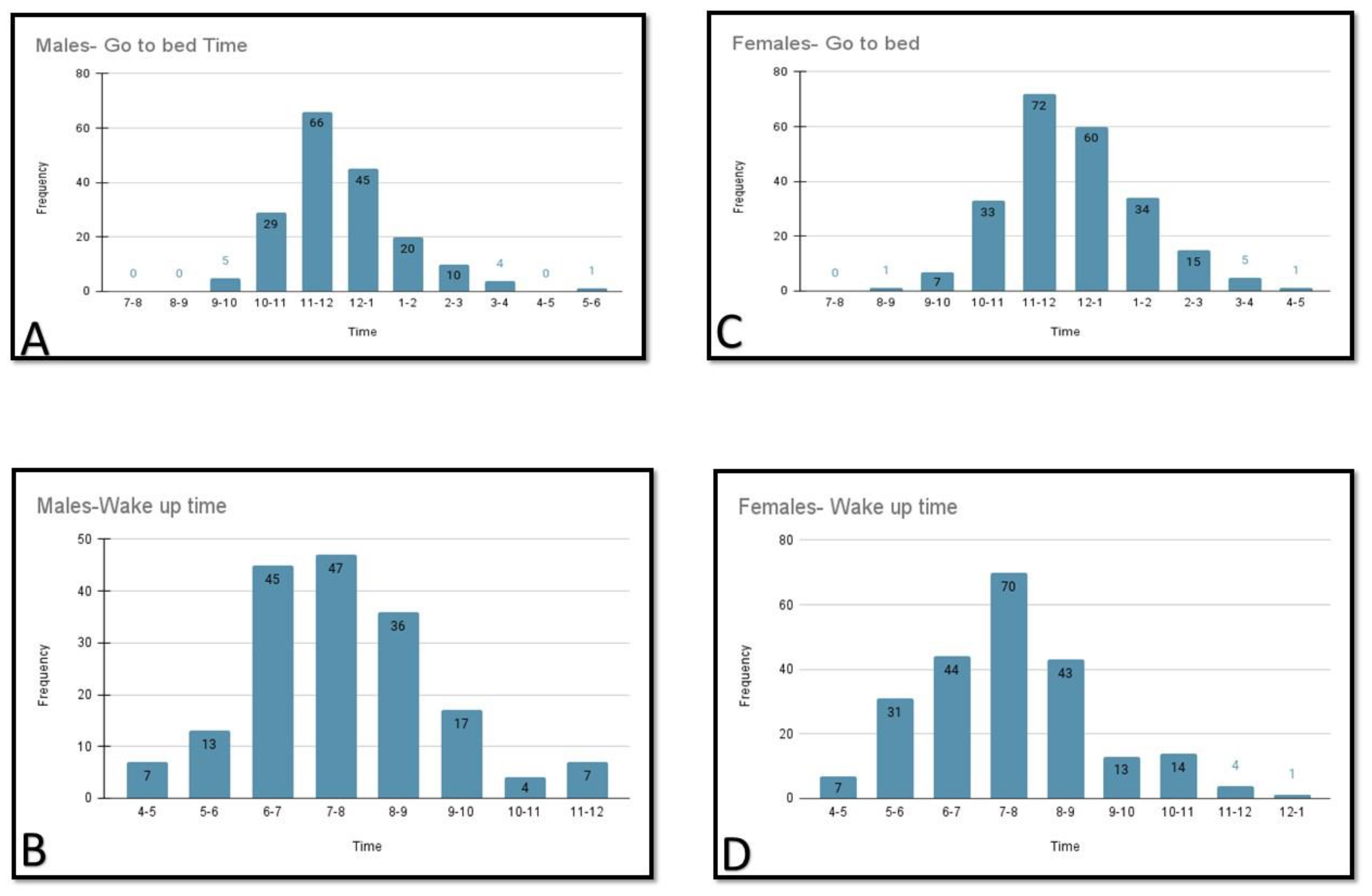

Table 1.
Socio-demographic characteristics of the participants.
| Domain | n (%) |
|---|---|
Age group
|
191 (47.63%) 196 (48.87%) 14 (3.49%) |
Gender
|
176 (43.89%) 224 (55.86%) 1 (0.25%) |
Occupation
|
150 (37.4%) 143 (35.6%) 40 (9.9%) 30 (7.48%) 15 (3.74%) 8 (1.99%) 15 (3.74%) |
Religion
|
361 (90%) 20 (4.98%) 4 (0.99%) 16 (3.99%) |
Domicile
|
322 (80.29%) 51 (12.71%) 28 (6.98%) |
Table 2.
Usage of electronic gadgets among the study participants.
| Question asked | Total responses | Male | Female |
|---|---|---|---|
| Do you have a personal electronic gadget? | 401 | 176 | 224 |
How many hours in a day do you spend on electronic gadgets?
|
21 (5.2%) 85 (21.2%) 134 (33.4%) 96 (23.9%) 65 (16.2%) |
9 39 55 46 27 |
12 46 79 50 37 |
Single major reason for using electronic gadget?
|
123 (30.6%) 114 (28.4%) 82 (20.4%) 76 (18.9%) 1 (0.2%) 2 (0.49%) 1 (0.2%) 2 (0.49%) |
71 39 32 32 0 1 0 2 |
52 75 50 44 1 1 1 0 |
Table 3.
Comparison of anxiety, depression and subjective well-being level between female and male participants.
Table 3.
Comparison of anxiety, depression and subjective well-being level between female and male participants.
| Variables | Females (n=224) Mean ± SD |
Males (n=176) Mean ± SD |
Test of significance |
|---|---|---|---|
| GAD-2 | 2.191± 1.545 | 1.534 ± 1.389 | t=4.412, df=398, p=0.0001 |
| PHQ-2 | 1.987 ± 1.531 | 1.721 ± 1.384 | t=1.799, df=398, p=0.0728 |
| WHO-5 | 52.035 ± 20.003 | 54.704 ± 20.022 | t= 1.983, df=398, p=0.048 |
GAD-2
|
74 (33.03%) 150 (66.97%) |
34 (19.32%) 142 (80.68%) |
Chi-square= 9.409 p=0.002 |
PHQ-2
|
68 (30.36%) 156 (69.64%) |
46 (26.14%) 130 (73.86%) |
Chi-square=0.862 p=0.353 |
GAD-2: Generalized Anxiety Disorder 2-item; PHQ-2: Patient Health Questionnaire-2 item; WHO-5: WHO-5 Well-being Index. *Number of positive test results (cutoff score: 3).
Table 4.
(A) Association of bedtime procrastination with other study variables among males (n=176).
| Variables | Age of the participants | Sleep latency in minutes | Hours of sleep | Procrastination time(minutes) | BtP Score | PHQ-2 Score | GAD-2 Score | WHO-5 Score |
|---|---|---|---|---|---|---|---|---|
| Sleep latency in minutes | R= -0.0056 P=0.937 |
** | ** | ** | ** | ** | ** | ** |
| Hours of sleep | R= -0.0941 P=0.215 |
R= -0.044 P= 0.562 |
** | ** | ** | ** | ** | ** |
| Procrastination time(minutes) | R= -0.0822 P=0.279 |
R=0.4034 P<0.00001 |
R= -0.276 P=0.0002 |
** | ** | ** | ** | ** |
| BtP Score | R= -0.396 P<0.00001 |
R=0.0242 P=0.750 |
R= -0.0614 P=0.421 |
R=0.2003 P=0.0076 |
** | ** | ** | ** |
| PHQ-2 Score | R= -0.192 P= 0.011 |
R=0.1203 P=0.1117 |
R= -0.0586 P=0.444 |
R=0.2708 P=0.0003 |
R=0.1891 P=0.0119 |
** | ** | ** |
| GAD-2 Score | R= -0.1098 P= 0.146 |
R=0.1011 P=0.181 |
R= -0.1297 P= 0.088 |
R= 0.2961 P= 0.00007 |
R=0.3561 P<0.00001 |
R=0.5769 P<0.00001 |
** | ** |
| WHO-5 Score | R=0.1021 P=0.177 |
R= - 0.246 P=0.0009 |
R=0.0469 P=0.536 |
R= -0.1948 P= 0.0095 |
R= -0.1471 P=0.0515 |
R= -0.3933 P <0.00001 |
R= -0.2971 P=0.00006 |
** |
| SISS (Sleep quality) | R=0.0505 P= 0.506 |
R= -0.2487 P=0.0009 |
R=0.1403 P=0.063 |
R= -0.3029 P=0.00004 |
R= -0.2555 P= 0.0006 |
R= -0.2362 P= 0.0016 |
R= -0.2811 P=0.00016 |
R= 0.418 P<0.00001 |
Table 4.
(B) Association of bedtime procrastination with other study variables among females (n=224).
Table 4.
(B) Association of bedtime procrastination with other study variables among females (n=224).
| Variables | Age of the participants | Sleep latency in minutes | Hours of sleep | Procrastination time (minutes) | BtP Score | PHQ-2 Score | GAD-2 Score | WHO-5 Score |
|---|---|---|---|---|---|---|---|---|
| Sleep latency in minutes | R= -0.0881 P= 0.189 |
** | ** | ** | ** | ** | ** | ** |
| Hours of sleep | R= -0.1091 P= 0.104 |
R= -0.1573 P= 0.0187 |
** | ** | ** | ** | ** | ** |
| Procrastination time(minutes) | R= 0.0244 P= 0.716 |
R=0.1732 P=0.0094 |
R= -0.1257 P=0.0597 |
** | ** | ** | ** | ** |
| BtP Score | R= -0.1518 P= 0.0229 |
R=0.1042 P=0.1199 |
R= -0.1812 P=0.0066 |
R=0.1541 P=0.0210 |
** | ** | ** | ** |
| PHQ-2 Score | R= -0.1671 P=0.0123 |
R= 0.0839 P=0.211 |
R=0.016 P=0.8117 |
R= 0.1128 P=0.0921 |
R=0.1578 P=0.0181 |
** | ** | ** |
| GAD-2 Score | R= -0.1593 P=0.0172 |
R=0.054 P=0.4212 |
R= -0.0522 P=0.4387 |
R=0.1904 P=0.0042 |
R=0.2303 P=0.0005 |
R= 0.6355 P<0.00001 |
** | ** |
| WHO-5 Score | R=0.038 P=0.572 |
R= -0.1486 P=0.0257 |
R=0.0581 P=0.3868 |
R=-0.0769 P=0.2511 |
R= - 0.2326 P=0.0004 |
R= -0.6183 P<0.00001 |
R= -0.4855 P <0.00001 |
** |
| SISS | R= -0.1335 P= 0.045 |
R= -0.1347 P=0.0435 |
R=0.3271 P<0.00001 |
R= -0.1253 P=0.0618 |
R= -0.2419 P=0.0003 |
R= -0.2163 P=0.0011 |
R= -0.3065 P<0.00001 |
R=0.3785 P<0.00001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



