Submitted:
13 January 2025
Posted:
14 January 2025
You are already at the latest version
Abstract
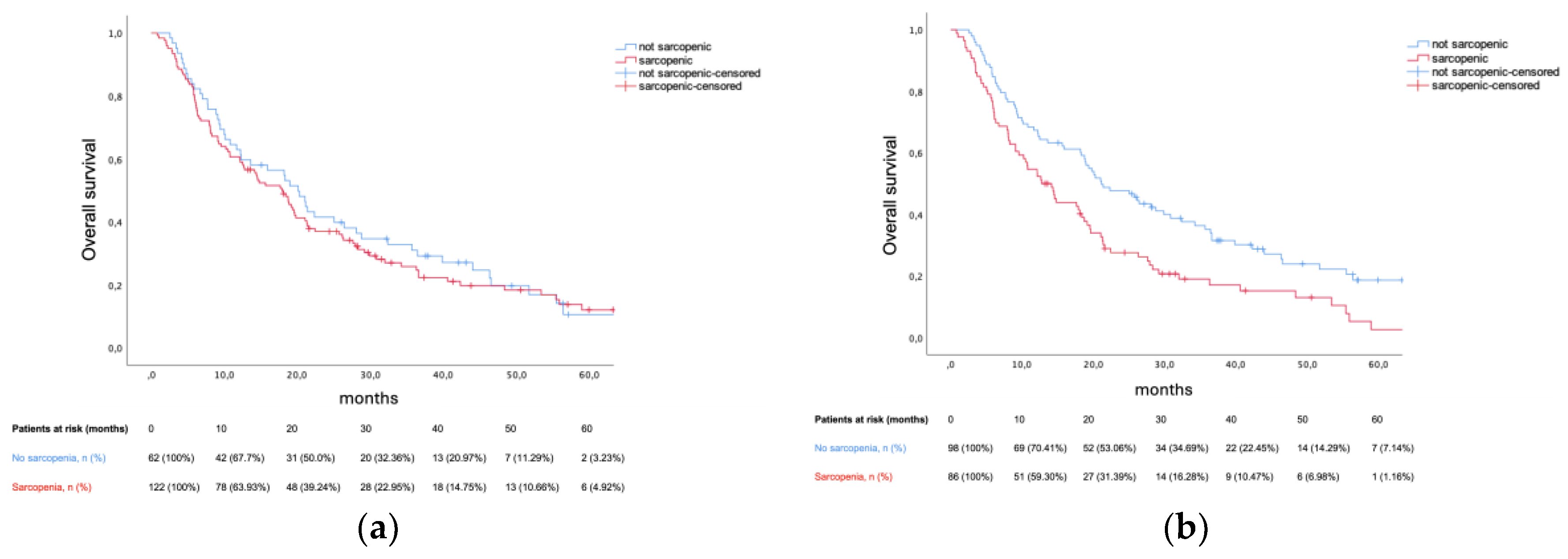
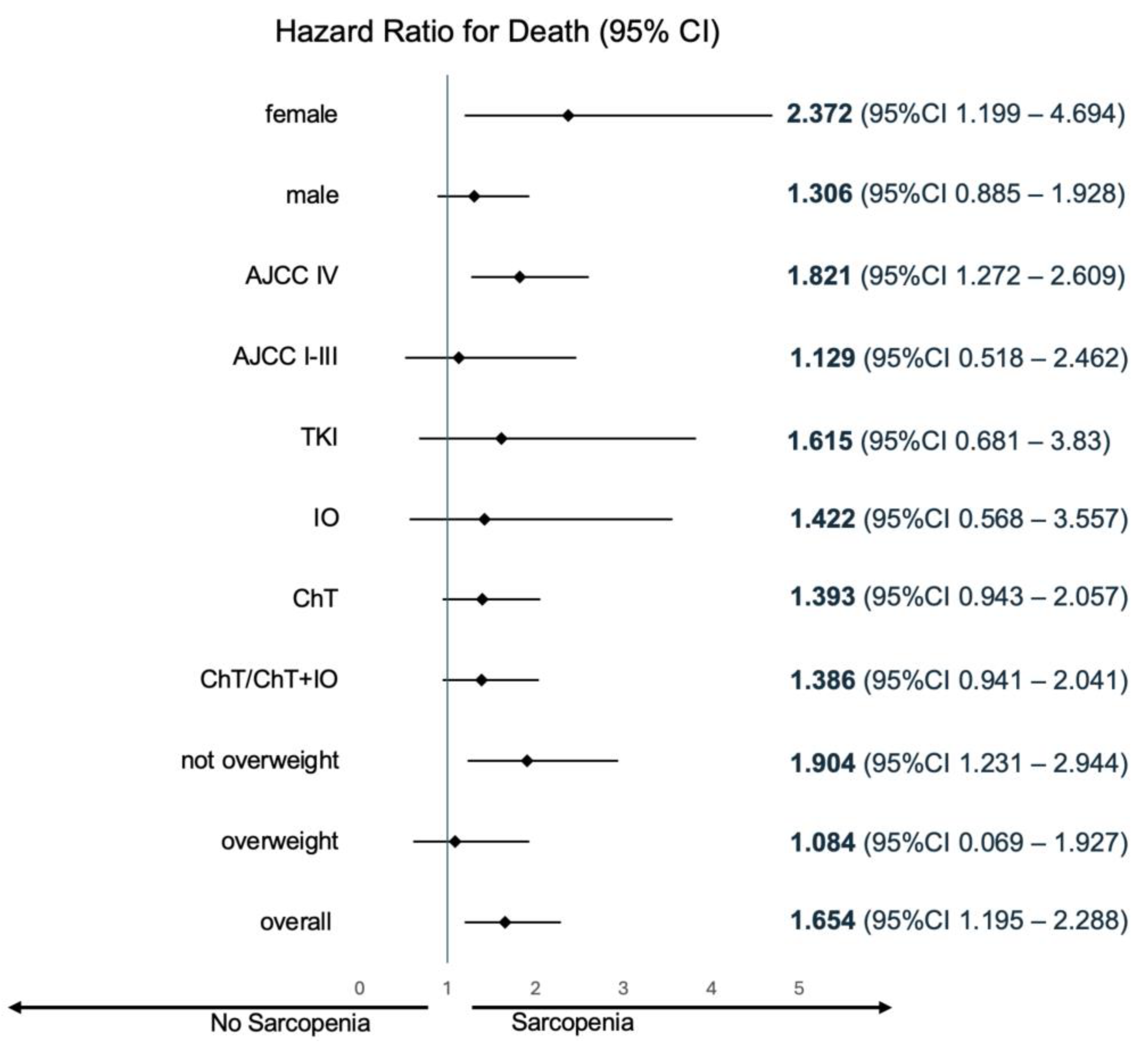
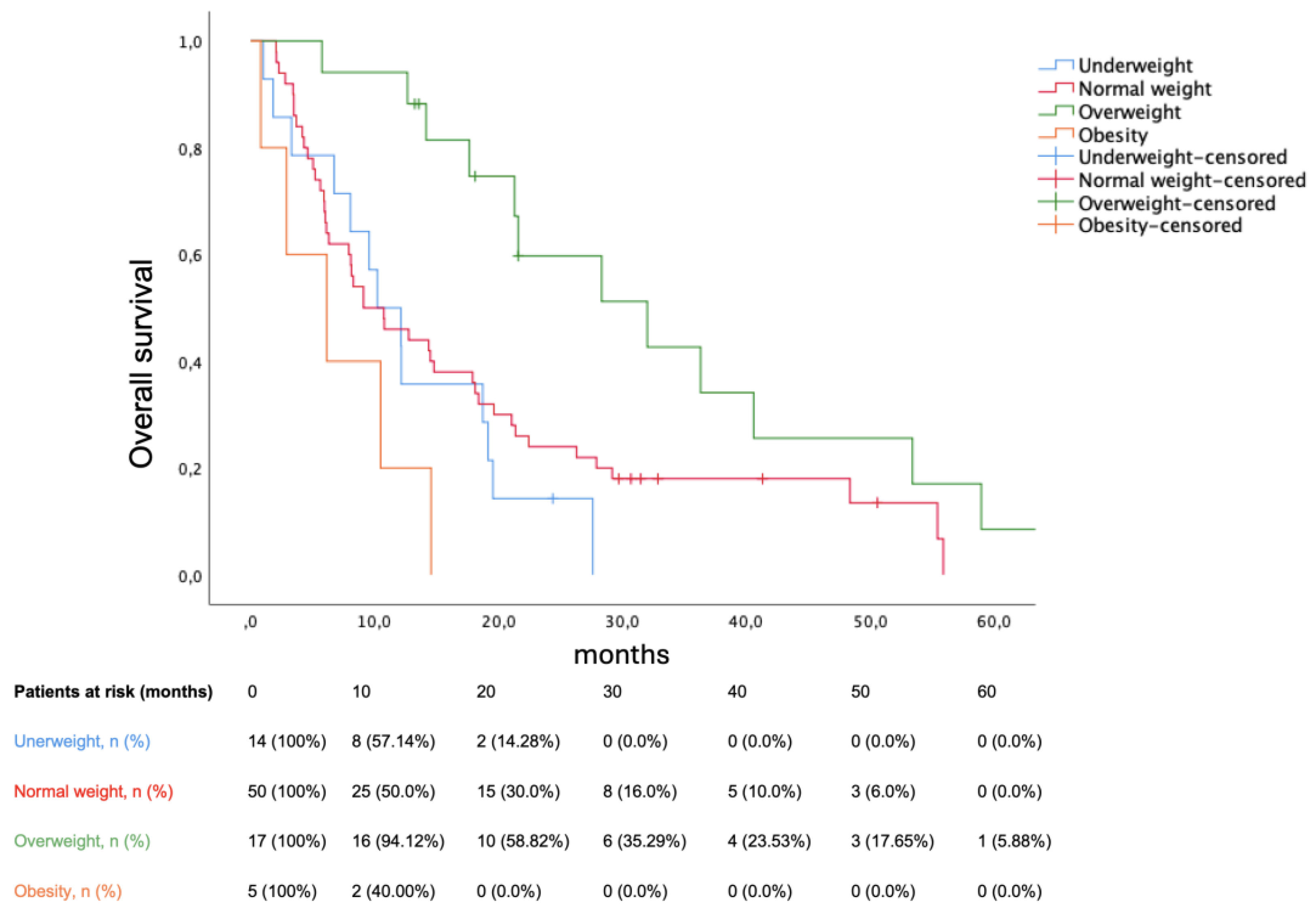
Background/Objectives: Sarcopenia is an emergent prognostic biomarker in clinical oncology. Albeit increasingly defined through skeletal muscle index (SMI) thresholding, literature cut-offs fail to discern heterogeneous baseline muscularity across populations. This study assesses the prognostic impact of using cohort-specific SMI thresholds in a Portuguese metastatic non-small-cell lung cancer (mNSCLC) cohort. Methods: Retrospective study including mNSCLC patients treated between January 2017 and December 2022. ImageJ v1.54g was used to assess cross-sectional CT imaging at the third lumbar vertebra (L3) and calculate L3SMI. Sarcopenia was defined both according to Prado et al. and L3SMI thresholds derived from receiver operating characteristic analysis. Overall survival (OS) was the primary endpoint. Secondary endpoints included first-line (1L) progression-free survival (PFS) and sarcopenia subgroup analysis regarding body mass index impact on OS. Results: The initial cohort included 197 patients. Mean age was 65 years (± 11.31). Most tumors were adenocarcinomas (n = 165) and presented with metastasis (n = 154). SMI was evaluable in 184 patients: cohort-specific thresholds (< 49.96 cm2/m2 for men; < 34.02 cm2/m2 for women) yielded 46.74% sarcopenic patients (n = 86) versus 66.30% (n = 122) per the literature definition. Cohort-specific thresholds predicted both OS (12.75 versus 21.13 months, hazard ratio [HR] 1.654, p = 0.002) and PFS (7.92 versus 9.56 months, HR 1.503, p = 0.01). Conversely, Prado et al. definition lacked prognostic value. Among sarcopenic patients, overweight (HR 0.417, p = 0.01) and obesity (HR 2.723, p = 0.039) had contrasting impacts on OS. Conclusions: Amid reclassification of nearly one-fifth of the cohort, cohort-specific thresholds improved sarcopenia prognostication in mNSCLC. Homogeneity regarding both cancer treatment setting and ethnicity could be key to defining sarcopenia based on SMI.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Procedures
2.2. Patients
2.3. Definitions and Endpoints
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 1L | First-line |
| 95%CI | Ninety-five percent confidence interval |
| AJCC | American Joint Committee on Cancer |
| BMI | Body Mass Index |
| ECOG | Eastern Cooperative Oncology Group |
| EGFR | Epidermal Growth Factor Receptor |
| HR | Hazard Ratio |
| HU | Hounsfield Unit |
| ICDO | International Classification of Diseases for Oncology |
| IO | Immunotherapy |
| L3 | Third lumbar vertebrae |
| (m)NSCLC | (metastatic) non-small-cell lung cancer |
| OS | Overall Survival |
| PFS | Progression-free Survival |
| PS | Performance Status |
| SMA | Skeletal Muscle Area |
| SMI | Skeletal Muscle Index |
| SNOMED | Systemized Nomenclature of Medicine |
| TKI | Tyrosine Kinase Inhibitor |
| ULSSJ | Unidade Local de Saúde São José |
References
- Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-263. [CrossRef]
- Jemal A, Schafer EJ, Sung H, et al. The Burden of Lung Cancer in Women Compared With Men in the US. JAMA Oncol. 2023;9(12):1727-1728. [CrossRef]
- Jha P. Avoidable global cancer deaths and total deaths from smoking. Nat Rev Cancer. 2009;9(9):655-664. [CrossRef]
- Adams SJ, Stone E, Baldwin DR, Vliegenthart R, Lee P, Fintelmann FJ. Lung cancer screening. Lancet. 2023;401(10374):390-408. [CrossRef]
- van Meerbeeck JP, Franck C. Lung cancer screening in Europe: where are we in 2021? Transl Lung Cancer Res. 2021;10(5):2407-2417. [CrossRef]
- Thai AA, Solomon BJ, Sequist LV, Gainor JF, Heist RS. Lung cancer. Lancet. 2021;398(10299):535-554. [CrossRef]
- Hendriks LE, Kerr KM, Menis J, et al. Oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023;34(4):339-357. [CrossRef]
- Hendriks LE, Kerr KM, Menis J, et al. Non-oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023;34(4):358-376. [CrossRef]
- Baracos VE, Arribas L. Sarcopenic obesity: hidden muscle wasting and its impact for survival and complications of cancer therapy. Ann Oncol. 2018;29 Suppl 2:ii1-ii9. [CrossRef]
- Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis [published correction appears in Age Ageing. 2019 Jul 1;48(4):601. doi: 10.1093/ageing/afz046]. Age Ageing. 2019;48(1):16-31. [CrossRef]
- Walowski CO, Braun W, Maisch MJ, et al. Reference Values for Skeletal Muscle Mass - Current Concepts and Methodological Considerations. Nutrients. 2020;12(3):755. Published 2020 Mar 12. [CrossRef]
- MacDonald AJ, Greig CA, Baracos V. The advantages and limitations of cross-sectional body composition analysis. Curr Opin Support Palliat Care. 2011;5(4):342-349. [CrossRef]
- Shen W, Punyanitya M, Wang Z, et al. Total body skeletal muscle and adipose tissue volumes: estimation from a single abdominal cross-sectional image. J Appl Physiol (1985). 2004;97(6):2333-2338. [CrossRef]
- Prado CM, Lieffers JR, McCargar LJ, et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol. 2008;9(7):629-635. [CrossRef]
- Martin L, Birdsell L, Macdonald N, et al. Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J Clin Oncol. 2013;31(12):1539-1547. [CrossRef]
- Fearon K, Strasser F, Anker SD, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol. 2011;12(5):489-495. [CrossRef]
- Zhuang CL, Huang DD, Pang WY, et al. Sarcopenia is an Independent Predictor of Severe Postoperative Complications and Long-Term Survival After Radical Gastrectomy for Gastric Cancer: Analysis from a Large-Scale Cohort. Medicine (Baltimore). 2016;95(13):e3164. [CrossRef]
- Itoh S, Yoshizumi T, Kimura K, et al. Effect of Sarcopenic Obesity on Outcomes of Living-Donor Liver Transplantation for Hepatocellular Carcinoma. Anticancer Res. 2016;36(6):3029-3034. PMID: 27272822.
- Yang M, Shen Y, Tan L, Li W. Prognostic Value of Sarcopenia in Lung Cancer: A Systematic Review and Meta-analysis. Chest. 2019;156(1):101-111. [CrossRef]
- Baldessari C, Guaitoli G, Valoriani F, et al. Impact of body composition, nutritional and inflammatory status on outcome of non-small cell lung cancer patients treated with immunotherapy. Clin Nutr ESPEN. 2021;43:64-75. [CrossRef]
- Wu CT, Hsu PC, Chang JW, et al. Comprehensive assessment of pretreatment sarcopenia impacts on patients with EGFR-mutated NSCLC treated with afatinib. Thorac Cancer. 2023;14(25):2548-2557. [CrossRef]
- Topcu A, Ozturk A, Yurtsever I, et al. The effect of sarcopenia on erlotinib therapy in patients with metastatic lung adenocarcinoma. Bosn J Basic Med Sci. 2022;22(6):982-991. Published 2022 Oct 23. [CrossRef]
- Irving BA, Weltman JY, Brock DW, Davis CK, Gaesser GA, Weltman A. NIH ImageJ and Slice-O-Matic computed tomography imaging software to quantify soft tissue. Obesity (Silver Spring). 2007;15(2):370-376. [CrossRef]
- Balakrishnan R, Thurmond DC. Mechanisms by Which Skeletal Muscle Myokines Ameliorate Insulin Resistance. Int J Mol Sci. 2022;23(9):4636. Published 2022 Apr 22. [CrossRef]
- Kimura M, Naito T, Kenmotsu H, et al. Prognostic impact of cancer cachexia in patients with advanced non-small cell lung cancer. Support Care Cancer. 2015;23(6):1699-1708. [CrossRef]
- Shoji F, Matsubara T, Kozuma Y, et al. Relationship Between Preoperative Sarcopenia Status and Immuno-nutritional Parameters in Patients with Early-stage Non-small Cell Lung Cancer. Anticancer Res. 2017;37(12):6997-7003. [CrossRef]
- Suzuki Y, Okamoto T, Fujishita T, et al. Clinical implications of sarcopenia in patients undergoing complete resection for early non-small cell lung cancer. Lung Cancer. 2016;101:92-97. [CrossRef]
- Kim EY, Lee HY, Kim KW, et al. Preoperative Computed Tomography-Determined Sarcopenia and Postoperative Outcome After Surgery for Non-Small Cell Lung Cancer. Scand J Surg. 2018;107(3):244-251. [CrossRef]
- Srdic D, Plestina S, Sverko-Peternac A, Nikolac N, Simundic AM, Samarzija M. Cancer cachexia, sarcopenia and biochemical markers in patients with advanced non-small cell lung cancer-chemotherapy toxicity and prognostic value. Support Care Cancer. 2016;24(11):4495-4502. [CrossRef]
- Stene GB, Helbostad JL, Amundsen T, et al. Changes in skeletal muscle mass during palliative chemotherapy in patients with advanced lung cancer. Acta Oncol. 2015;54(3):340-348. [CrossRef]
- Wang Y, Chen P, Huang J, et al. Assessment of sarcopenia as a predictor of poor overall survival for advanced non-small-cell lung cancer patients receiving salvage anti-PD-1 immunotherapy. Ann Transl Med. 2021;9(24):1801. [CrossRef]
- Feng Y, Wang L, Guo F, et al. Predictive impact of sarcopenia in advanced non-small cell lung cancer patients treated with immune checkpoint inhibitors: A retrospective study. Heliyon. 2024;10(5):e27282. Published 2024 Mar 3. [CrossRef]
- Madeddu C, Busquets S, Donisi C, et al. Effect of Cancer-Related Cachexia and Associated Changes in Nutritional Status, Inflammatory Status, and Muscle Mass on Immunotherapy Efficacy and Survival in Patients with Advanced Non-Small Cell Lung Cancer. Cancers (Basel). 2023;15(4):1076. Published 2023 Feb 8. [CrossRef]
- Bolte FJ, McTavish S, Wakefield N, et al. Association of sarcopenia with survival in advanced NSCLC patients receiving concurrent immunotherapy and chemotherapy. Front Oncol. 2022;12:986236. Published 2022 Sep 23. [CrossRef]
- Rossi S, Di Noia V, Tonetti L, et al. Does sarcopenia affect outcome in patients with non-small-cell lung cancer harboring EGFR mutations?. Future Oncol. 2018;14(10):919-926. [CrossRef]
- Topcu A, Ozturk A, Yurtsever I, et al. The effect of sarcopenia on erlotinib therapy in patients with metastatic lung adenocarcinoma. Bosn J Basic Med Sci. 2022;22(6):982-991. Published 2022 Oct 23. [CrossRef]
- Wu CT, Hsu PC, Chang JW, et al. Comprehensive assessment of pretreatment sarcopenia impacts on patients with EGFR-mutated NSCLC treated with afatinib. Thorac Cancer. 2023;14(25):2548-2557. [CrossRef]
- Atkins JL, Wannamathee SG. Sarcopenic obesity in ageing: cardiovascular outcomes and mortality. Br J Nutr. 2020;124(10):1102-1113. [CrossRef]
- Kroenke CH, Neugebauer R, Meyerhardt J, et al. Analysis of Body Mass Index and Mortality in Patients With Colorectal Cancer Using Causal Diagrams. JAMA Oncol. 2016;2(9):1137-1145. [CrossRef]
- da Silva Dias D, Machado M, Trabulo C, Gosálbez B, Ravasco P. Impact of Body Composition on Prognosis and Dose-Limiting Toxicities on Metastatic Colorectal Cancer. Front Nutr. 2022;8:671547. Published 2022 Jan 27. [CrossRef]

| Variable | Total (n = 197) |
|---|---|
| Age, mean ± standard deviation | 65 ± 11.31 |
| Sex, n (%) | |
| Male | 135 (68.53%) |
| Female | 62 (31.47%) |
| Smoking status, n (%) | |
| (Former) Smoker | 103 (52.28%) |
| Never Smoker | 30 (15.23%) |
| Unreported | 64 (32.49%) |
| ECOG performance status, n (%) | |
| 0 | 50 (25.38%) |
| 1 | 106 (53.81%) |
| ≥ 2 | 41 (20.81%) |
| AJCC stage, n (%) | |
| I–III | 43 (21.83%) |
| IV | 154 (78.17%) |
| Histology, n (%) | |
| Adenocarcinoma | 165 (83.76%) |
| Squamous cell carcinoma | 23 (11.68%) |
| Other | 9 (4.57%) |
| Metastatic sites, n (%) | |
| ≤ 2 | 156 (79.19%) |
| > 2 | 41 (20.81%) |
| PD-L1 tumor proportion score, n (%) | |
| < 1 % | 92 (46.70%) |
| 1–50 % | 42 (21.32%) |
| > 50 % | 40 (20.3%) |
| Unreported | 23 (11.68%) |
| First-line treatment, n (%) | |
| Chemotherapy | 113 (57.36%) |
| Immunotherapy | 35 (17.77%) |
| Tyrosine kinase inhibitor | 36 (18.27%) |
| Chemoimmunotherapy | 13 (6.60%) |
| Variable | Total (n=184) |
|---|---|
| BMI group, n (%) | |
| < 18.5 kg/m2 | 18 (9.78%) |
| ≥ 18.5 kg/m2 and < 25 kg/m2 | 94 (51.1%) |
| ≥ 25 kg/m2 and < 30 kg/m2 | 72 (39.13%) |
| ≥ 30 kg/m2 | 20 (10.87%) |
| BMI (kg/m2), mean ± standard deviation | |
| Male (n=125) | 24.15 ± 4.75 |
| Female (n=59) | 24.27 ± 4.12 |
| SMI (cm2/m2), mean ± standard deviation | |
| Male (n=125) | 48.52 ± 9.31 |
| Female (n=59) | 37.69 ± 6.14 |
| Sarcopenia (Prado et al.)1, n (%) | |
| Male (n=125) | 89 (71.20%) |
| Female (n=59) | 33 (55.93%) |
| Sarcopenia (cohort-specific)2, n (%) | |
| Male (n=125) | 73 (58.40%) |
| Female (n=59) | 13 (22.03%) |
| Univariate Cox Regression Analysis | Multivariate Cox Regression Analysis | |||
|---|---|---|---|---|
| Variable | p-value | HR (95% CI) | p-value | HR (95% CI) |
| Sarcopenia | 0.002 | 1.65 (1.19–2.29) | 0.019 | 1.50 (1.07–2.11) |
| Underweight | 0.002 | 2.29 (1.37–3.86) | 0.012 | 1.99 (1.16–3.40) |
| Overweight | 0.074 | - | - | - |
| Obesity | 0.895 | - | - | - |
| ECOG PS ≥ 1 | 0.009 | 1.68 (1.14–2.47) | 0.008 | 1.69 (1.14–2.49) |
| Ab initio CNS M1 | 0.569 | - | - | - |
| ≥ 2 M1 sites | 0.113 | - | - | - |
| KRAS mutant | 0.402 | - | - | - |
| Squamous cell | 0.581 | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



