Submitted:
10 January 2025
Posted:
14 January 2025
You are already at the latest version
Abstract
Sepsis and septic shock are severe medical conditions associated with high morbidity and mortality, necessitating accurate risk stratification to optimize clinical management. Lactate is a well-established biomarker for sepsis prognosis, reflecting tissue hypoxia and anaerobic metabolism. Standard Base Excess (SBE) is commonly used to assess metabolic acidosis, but its prognostic value in sepsis remains uncertain, particularly in the presence of elevated lactate levels. Alactic Base Excess (aBE), calculated as SBE + lactate, has been proposed as an alternative marker to differentiate non-lactate metabolic derangements.
This retrospective cohort study aimed to compare the prognostic accuracy of lactate, SBE, and aBE in predicting mortality among patients with sepsis and septic shock. A total of 218 patients admitted to the intensive care unit (ICU) were analyzed, including 90 survivors and 128 non-survivors. Elevated lactate levels were significantly associated with mortality (p < 0.001) and remained an independent predictor in multivariate analysis (odds ratio [OR]: 1.40, 95% confidence interval [CI]: 1.11–1.77, p = 0.005). SBE showed a weak association with mortality in univariate analysis but lost significance in multivariate models. ABE did not demonstrate significant prognostic value.
Receiver Operating Characteristic (ROC) analysis confirmed lactate as the most reliable predictor, with an area under the curve (AUC) of 0.742. These findings suggest that lactate remains the superior prognostic biomarker in sepsis and septic shock, whereas SBE and aBE do not provide additional predictive value. Further research is needed to explore the dynamic changes in these biomarkers over time to refine risk stratification in septic patients.
Keywords:
sepsis
; septic shock
; lactate
; standart base excess
; alactic base excess
; prognosis
; mortality prediction
1. Introduction
Sepsis and septic shock are life-threatening conditions associated with high morbidity and mortality, requiring prompt diagnosis and appropriate management. Despite advancements in critical care medicine, risk stratification remains a significant challenge, as early identification of high-risk patients is crucial for timely interventions. Various prognostic biomarkers have been investigated to improve mortality prediction in sepsis, with arterial blood gas (ABG) parameters playing a central role in assessing metabolic derangements [1].
Lactate is a well-established biomarker in sepsis, reflecting tissue hypoxia, impaired oxygen utilization, and anaerobic metabolism [2]. Elevated lactate levels are consistently associated with poor clinical outcomes and have been incorporated into sepsis management guidelines. However, lactate alone may not provide a comprehensive assessment of metabolic disturbances in septic patients, particularly in the presence of concurrent acid-base imbalances [3].
Standard Base Excess (SBE) is widely used to evaluate metabolic acid-base disorders by quantifying the amount of acid or base required to return blood pH to 7.4 under standard conditions. However, its interpretation becomes complex in sepsis, where elevated lactate levels significantly influence metabolic acidosis. To address this limitation, Alactic Base Excess (aBE) has been proposed as an alternative parameter that accounts for non-lactate metabolic derangements by incorporating lactate into the base excess calculation (aBE = SBE + lactate). Theoretically, aBE could offer a more accurate assessment of metabolic imbalances unrelated to lactate, such as hyperchloremic acidosis or renal dysfunction [4].
Although lactate, SBE, and aBE are all relevant biomarkers in critically ill patients, their comparative prognostic value in sepsis and septic shock remains inadequately explored. Previous studies have primarily focused on lactate as an isolated predictor of mortality, while the role of SBE and aBE in risk stratification is less well-defined. Moreover, existing research has yielded conflicting results regarding the clinical utility of these parameters in sepsis [5,6]. Therefore, further investigation is needed to determine whether SBE and aBE provide additional prognostic value beyond lactate in critically ill septic patients.
This study aimed to compare the effectiveness of lactate, SBE, and aBE in predicting mortality in sepsis and septic shock and to explore the relationships between these biomarkers.
2. Materials and methods
2.1. Study Design and Participants
This retrospective cohort study was conducted in the medical intensive care unit of Ondokuz Mayıs University Faculty of Medicine between 2022 and 2023. Patients diagnosed with sepsis or septic shock according to the Sepsis-3 criteria were included. Inclusion criteria were age ≥18 years and availability of arterial blood gas analysis at ICU admission. Exclusion criteria included terminal-stage palliative care patients, those who died within the first 24 hours of ICU admission, and cases with incomplete or missing medical records.
2.2. Data Collection
All patient data, including demographic characteristics, severity scores, and laboratory findings, were retrospectively collected from electronic medical records. The severity of illness was assessed using the Acute Physiology and Chronic Health Evaluation II (APACHE II) score, which estimates disease severity based on physiological parameters, and the Sequential Organ Failure Assessment (SOFA) score, which evaluates the extent of organ dysfunction in critically ill patients. Patients were categorized into survivors and non-survivors, and the following variables were analyzed: age, sex, APACHE II, SOFA, and Charlson Comorbidity Index scores; serum creatinine, sodium, and chloride levels; as well as arterial blood gas parameters, including pH, bicarbonate, standard base excess (SBE), lactate, and alactic base excess (aBE), which was calculated as SBE + lactate.
Supportive therapies, including the use of vasopressors, invasive mechanical ventilation, and hemodialysis, were also recorded. The length of ICU stay was measured in days. To address missing data, variables with more than 5% missing values were excluded from the analysis, while those with less than 5% missing data were handled using multiple imputation techniques.
2.3. Statistical Analysis
Statistical analysis was performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). The normality of continuous variables was assessed using the Shapiro-Wilk test. Normally distributed variables were compared using the independent t-test, and results were reported as mean ± standard deviation. Non-normally distributed variables were analyzed using the Mann-Whitney U test, with results presented as median (interquartile range). Categorical variables were compared using the chi-square test and reported as frequency (percentage).
To evaluate the prognostic value of lactate, SBE, and aBE in predicting mortality, receiver operating characteristic curve analysis was conducted. The area under the curve was calculated, and the optimal cut-off value was determined using the Youden Index. Independent predictors of mortality were identified using multivariate logistic regression analysis. Variables with p < 0.10 in univariate analysis were included in the model. Results were reported as odds ratios with 95% confidence intervals. A p-value < 0.05 was considered statistically significant.
3. Results
A total of 218 patients diagnosed with sepsis or septic shock were included in the study, with 90 survivors and 128 non-survivors. There was no significant difference in age (p = 0.990) or sex distribution (p = 0.074) between survivors and non-survivors. However, non-survivors had significantly higher disease severity scores, including APACHE II (28 [23–33] vs. 23 [18–27], p < 0.001) and SOFA (12 [9,10,11,12,13,14] vs. 9 [7,8,9,10,11,12], p < 0.001), compared to survivors (Table 1).
Regarding biochemical markers, standard bicarbonate levels were significantly lower in non-survivors (20 [16,17,18,19,20,21,22,23,24] vs. 22 [18,19,20,21,22,23,24,25], p = 0.030). Similarly, SBE values were significantly more negative in non-survivors (-5.1 [-9.8 – -1] vs. -2.8 [-7.6 – +0.9], p = 0.046). The most striking difference was observed in lactate levels, which were significantly higher in non-survivors (2.9 [2.3–4.1] vs. 1.2 [1.8–2.9], p < 0.001). However, aBE values did not significantly differ between groups (-1.6 [-5.6 – +2.2] vs. -0.5 [-4.8 – +2.2], p = 0.551) (Table 1). Non-survivors required significantly more vasopressor support (97% vs. 71.1%, p < 0.001), invasive mechanical ventilation (86% vs. 38%, p < 0.001), and hemodialysis (57% vs. 36%, p = 0.002) compared to survivors. The median ICU stay did not significantly differ between groups (8 [4,5,6,7,8,9,10,11,12,13,14,15,16] vs. 7 [4,5,6,7,8,9,10,11,12,13] days, p = 0.166).
In the logistic regression analysis, higher APACHE II scores were significantly associated with increased mortality risk (OR: 1.08, 95% CI: 1.02–1.15, p = 0.013). Similarly, elevated lactate levels were found to be a significant predictor of mortality (OR: 1.40, 95% CI: 1.11–1.77, p = 0.005). Vasopressor use was also associated with a higher risk of mortality (OR: 1.32, 95% CI: 1.05–1.68, p = 0.028). Additionally, invasive mechanical ventilation was identified as a significant factor linked to increased mortality (OR: 1.45, 95% CI: 1.10–1.92, p = 0.012) (Table 2).
Although both lactate and SBE showed a significant association with mortality in univariate analysis (Table 1), only lactate remained an independent predictor in multivariate logistic regression analysis (Table 2). aBE was not associated with mortality (Table 1). Therefore, ROC curve analysis for aBE was not performed, and the predictive value of SBE was limited.
The receiver operating characteristic curve analysis for lactate in patients with sepsis and septic shock showed an area under the curve (AUC) of 0.742 (95% CI: 0.672–0.812, p < 0.001), indicating good predictive ability for mortality. In contrast, the AUC for SBE was 0.421 (95% CI: 0.343–0.498, p = 0.046), suggesting poor diagnostic performance (Figure 1). The optimal cutoff value for lactate was determined as 2.0 mmol/L, with a sensitivity of 86.7% and a specificity of 60.0%.
4. Discussion
In this study, we investigated the prognostic value of lactate, standard base excess (SBE), and alactic base excess (aBE) in predicting mortality among patients with sepsis and septic shock. Our findings indicate that lactate is a strong and independent predictor of mortality, whereas SBE and aBE do not provide additional prognostic value. These results have significant implications for risk stratification in sepsis and the use of metabolic biomarkers in clinical practice.
Unlike previous studies, our findings align with existing evidence supporting lactate as a critical biomarker in sepsis prognosis [8,9,10]. Research has shown that lactate levels above 2 mmol/L are associated with significantly increased hospital mortality, even in hemodynamically stable sepsis patients [11]. Additionally, meta-analyses have suggested that changes in lactate levels over time may be more predictive of mortality than a single measurement [12,13]. However, unlike studies evaluating lactate kinetics, this analysis focuses solely on the initial lactate value at ICU admission without assessing variations over time.
Lactate is a well-known biomarker of impaired oxygen utilization, mitochondrial dysfunction, and anaerobic metabolism [14]. Among the patients analyzed, non-survivors had significantly higher lactate levels than survivors, with this difference being statistically significant. The receiver operating characteristic analysis confirmed the strong predictive performance of lactate, with an optimal cutoff of 2.0 mmol/L, providing high sensitivity (86.7%) and acceptable specificity (60.0%). These findings reinforce the importance of early lactate monitoring in sepsis management and suggest that dynamic changes in lactate levels over time may further improve risk assessment.
SBE quantifies the amount of acid or base required to return blood pH to 7.4 under standard conditions, making it a widely used parameter for evaluating metabolic acidosis and overall acid-base balance [4,15]. Several studies have highlighted the clinical relevance of SBE in critically ill patients, particularly in sepsis and trauma, where metabolic acidosis often plays a crucial role in disease progression and outcomes [16,17].
In our analysis, while SBE was significantly associated with mortality in univariate analysis, this association was not maintained in multivariate models, suggesting that its prognostic value is largely overshadowed by lactate. This finding aligns with previous research indicating that lactate, as a marker of impaired tissue oxygenation and anaerobic metabolism, often outperforms SBE in predicting mortality in critically ill patients [8,10]. The stronger predictive role of lactate may stem from its direct reflection of tissue hypoxia and mitochondrial dysfunction, whereas SBE represents a more generalized measure of acid-base balance influenced by multiple metabolic factors.
Additionally, we analyzed aBE, which theoretically isolates non-lactate metabolic disturbances by excluding lactate from the calculation. However, aBE did not show a significant association with mortality. This finding is consistent with prior studies suggesting that while lactate-independent metabolic acidosis contributes to disease severity, its prognostic impact is less pronounced when compared to lactate-driven acidosis [18,19]. Given these results, lactate remains the dominant metabolic marker for risk stratification in critically ill patients, reinforcing the importance of dynamic lactate monitoring in clinical practice.
Several factors may explain the limited prognostic utility of SBE and aBE in sepsis. First, metabolic acidosis in sepsis is primarily driven by lactate accumulation. Since lactate is already a strong prognostic marker, SBE, which inherently incorporates lactate-driven acidosis, may not provide additional independent prognostic value. aBE, which aims to differentiate non-lactate acidosis, may be less relevant in sepsis, where lactate is the dominant driver of metabolic acidosis.
Another possible explanation for the lack of prognostic value in SBE and aBE is the influence of various compensatory mechanisms. Unlike lactate, which directly reflects tissue perfusion abnormalities and anaerobic metabolism, SBE and aBE are affected by multiple physiological adaptations, including renal bicarbonate regulation, respiratory compensation, and electrolyte disturbances [20]. For example, patients with sepsis-induced metabolic acidosis may develop compensatory respiratory alkalosis through hyperventilation, normalizing SBE values despite the severity of their condition. Similarly, renal compensation may buffer metabolic acidosis over time, modifying SBE and aBE values independently of sepsis severity [21]. These physiological adaptations likely dilute the prognostic significance of SBE and aBE, explaining their weaker association with mortality compared to lactate.
Previous research on the prognostic value of SBE and aBE has yielded inconsistent results [22,23,24,25]. Some findings suggest that more negative SBE values, indicating severe metabolic acidosis, are associated with increased mortality in critically ill patients. However, differences in patient populations across studies complicate direct comparisons. While some analyses have identified SBE as a predictor of mortality in general ICU settings, its prognostic significance appears to diminish in sepsis-specific cases [22]. Similarly, base excess has shown relevance in trauma-related outcomes but lacks the same predictive strength in sepsis [25]. The present analysis contributes to this discussion by suggesting that SBE and aBE may not serve as reliable independent prognostic markers in sepsis, where lactate remains the dominant indicator. Further investigation is required to determine whether these parameters hold predictive value in specific subgroups, such as patients with concurrent renal failure or electrolyte imbalances.
One of the key strengths of our study is its focused comparison of three metabolic biomarkers within a well-defined cohort of sepsis and septic shock patients. The statistical analyses were robust, and the study design allowed for meaningful comparisons between survivors and non-survivors. However, our study also has several limitations.
First, its retrospective and single-center design may limit the generalizability of our findings. Additionally, we only assessed biomarker levels at ICU admission, without considering dynamic changes over time. Sepsis is a rapidly evolving condition, and serial biomarker measurements may provide better prognostic insights than a single baseline value. Future studies should investigate how trends in lactate, SBE, and aBE correlate with patient outcomes. Furthermore, we did not analyze the impact of sepsis etiology or coexisting conditions on biomarker performance. Since different infection sources and comorbidities can influence metabolic responses, future research should explore whether certain patient subgroups may benefit from SBE- or aBE-based prognostic assessment.
5. Conclusion
Our study confirms that lactate remains the strongest and most reliable predictor of mortality in sepsis and septic shock, while SBE and aBE do not provide additional prognostic value. These findings reinforce the importance of lactate-based risk stratification and suggest that SBE and aBE should be interpreted cautiously in sepsis patients. Future research should focus on incorporating serial biomarker measurements and exploring novel metabolic markers to enhance sepsis prognostication.
Author Contributions
Conceptualization, OK.; methodology, OK, MI.; validation, MI and OYC.; formal analysis, OK.; investigation, TSA and OYC; resources, MI and OK.; data curation, MI and OYC.; writing—original draft preparation, OK.; writing—review and editing, OK, MI, OYC and TSA.; visualization,OYC and MI.; supervision, MI and OYC; project administration, OK.; All authors have read and agreed to the published version of the manuscript.
Funding
None
Institutional Review Board Statement
The study was approved by the Institutional Review Board of Ondokuz Mayis University Hospital, Turkey (Approval No: 2024000579).
Informed Consent Statement
Since it was a retrospective study, informed consent was waived.
Data Availability Statement
The datasets analysed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare that they have no competing interests.
References
- Mukherjee, S.; Das, S.; Mukherjee, S.; Ghosh, P.S.; Bhattacharya, S. Arterial Blood Gas as a Prognostic Indicator in Patients with Sepsis. Indian J. Med Microbiol. 2020, 38, 457–460. [Google Scholar] [CrossRef] [PubMed]
- De Backer, D.; Vincent, J.-L. Understanding Hyperlactatemia in Human Sepsis: Are We Making Progress? Am. J. Respir. Crit. Care Med. 2019, 200, 1070–1071. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Fan, M.; Wang, X.; Xu, J.; Wang, Y.; Gill, P.S.; Ha, T.; Liu, L.; Hall, J.V.; Williams, D.L.; et al. Lactate induces vascular permeability via disruption of VE-cadherin in endothelial cells during sepsis. Sci. Adv. 2022, 8, eabm8965. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Camporota, L.; Meessen, J.; Romitti, F.; Pasticci, I.; Duscio, E.; Vassalli, F.; Forni, L.G.; Payen, D.; Cressoni, M.; et al. Understanding Lactatemia in Human Sepsis. Potential Impact for Early Management. Am. J. Respir. Crit. Care Med. 2019, 200, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Cantos, J.; Huespe, I.A.; Sinner, J.F.; Prado, E.M.; Roman, E.S.; Rolón, N.C.; Musso, C.G. Alactic base excess is an independent predictor of death in sepsis: A propensity score analysis. J. Crit. Care 2023, 74, 154248. [Google Scholar] [CrossRef] [PubMed]
- Smuszkiewicz, P.; Jawień, N.; Szrama, J.; Lubarska, M.; Kusza, K.; Guzik, P. Admission Lactate Concentration, Base Excess, and Alactic Base Excess Predict the 28-Day Inward Mortality in Shock Patients. J. Clin. Med. 2022, 11, 6125. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Jansen, T.C.; Van Bommel, J.; Schoonderbeek, F.J.; Visser, S.J.S.; Van Der Klooster, J.M.; Lima, A.P.; Willemsen, S.P.; Bakker, J. Early Lactate-Guided Therapy in Intensive Care Unit Patients: A multicenter, open-label, randomized controlled trial. Am. J. Respir. Crit. Care Med. 2010, 182, 752–761. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, N.I.; Howell, M.D.; Talmor, D.; Nathanson, L.A.; Lisbon, A.; Wolfe, R.E.; Weiss, J.W. Serum Lactate as a Predictor of Mortality in Emergency Department Patients with Infection. Ann. Emerg. Med. 2005, 45, 524–528. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, M.E.; Miltiades, A.N.; Gaieski, D.F.; Goyal, M.; Fuchs, B.D.; Shah, C.V.; Bellamy, S.L.; Christie, J.D. Serum lactate is associated with mortality in severe sepsis independent of organ failure and shock*. Crit. Care Med. 2009, 37, 1670–1677. [Google Scholar] [CrossRef]
- Vincent, J.-L.; e Silva, A.Q.; Couto, L.; Taccone, F.S. The value of blood lactate kinetics in critically ill patients: a systematic review. Crit. Care 2016, 20, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Xu, X. Lactate Clearance Is a Useful Biomarker for the Prediction of All-Cause Mortality in Critically Ill Patients: A systematic review and meta-analysis* Crit. Care Med. 2014, 42, 2118–2125. [Google Scholar] [CrossRef] [PubMed]
- Haas, S.A.; Lange, T.; Saugel, B.; Petzoldt, M.; Fuhrmann, V.; Metschke, M.; Kluge, S. Severe hyperlactatemia, lactate clearance and mortality in unselected critically ill patients. Intensiv. Care Med. 2015, 42, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Gladden, L.B. Lactate metabolism: a new paradigm for the third millennium. J. Physiol. 2004, 558, 5–30. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A. Determinants of blood pH in health and disease. Crit. Care 2000, 4, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Noritomi, D.T.; Soriano, F.G.; Kellum, J.A.; Cappi, S.B.; Biselli, P.J.C.; Libório, A.B.; Park, M. Metabolic acidosis in patients with severe sepsis and septic shock: A longitudinal quantitative study. Crit. Care Med. 2009, 37, 2733–2739. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Moreno, R. Clinical review: Scoring systems in the critically ill. Crit. Care 2010, 14, 207–207. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.W.; Mackenhauer, J.; Roberts, J.C.; Berg, K.M.; Cocchi, M.N.; Donnino, M.W. Etiology and Therapeutic Approach to Elevated Lactate Levels. Mayo Clin. Proc. 2013, 88, 1127–1140. [Google Scholar] [CrossRef]
- Al-Jaghbeer, M.; Kellum, J.A. Acid–base disturbances in intensive care patients: etiology, pathophysiology and treatment. Nephrol. Dial. Transplant. 2014, 30, 1104–1111. [Google Scholar] [CrossRef] [PubMed]
- Seifter, J.L.; Chang, H.-Y. Disorders of Acid-Base Balance: New Perspectives. Kidney Dis. 2016, 2, 170–186. [Google Scholar] [CrossRef] [PubMed]
- Dubin, A.; Menises, M.M.; Masevicius, F.D.; Moseinco, M.C.; Kutscherauer, D.O.; Ventrice, E.; Laffaire, E.; Estenssoro, E. Comparison of three different methods of evaluation of metabolic acid-base disorders*. Crit. Care Med. 2007, 35, 1264–1270. [Google Scholar] [CrossRef]
- Cusack, R.; Rhodes, A.; Lochhead, P.; Jordan, B.; Perry, S.; Ball, J.; Grounds, R.; Bennett, E. The strong ion gap does not have prognostic value in critically ill patients in a mixed medical/surgical adult ICU. Intensiv. Care Med. 2002, 28, 864–869. [Google Scholar] [CrossRef]
- Park, M.; Maciel, A.T.; Noritomi, D.T.; de Azevedo, L.C.P.; Taniguchi, L.U.; Neto, L.M.d.C. Effect of Paco2 variation on standard base excess value in critically ill patients. J. Crit. Care 2009, 24, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Taniguchi, L.; Noritomi, D.; Libório, A.; Maciel, A.; Cruz-Neto, L. Clinical utility of standard base excess in the diagnosis and interpretation of metabolic acidosis in critically ill patients. Braz. J. Med Biol. Res. 2008, 41, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Diao, M.-Y.; Wang, T.; Cui, Y.-L.; Lin, Z.-F. [Prognostic value of arterial lactate content combined with base excess in patients with sepsis: a retrospective study]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2013, 25, 211–4. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Receiver Operating Characteristic (ROC) Curve for lactate and SBE in patients with sepsis and septic shock. The area under the curve (AUC) for lactate is 0.742 (95% CI: 0.672–0.812; p < 0.001). The AUC for SBE is 0.421 (95% CI: 0.343–0.498; p = 0.046).
Figure 1.
Receiver Operating Characteristic (ROC) Curve for lactate and SBE in patients with sepsis and septic shock. The area under the curve (AUC) for lactate is 0.742 (95% CI: 0.672–0.812; p < 0.001). The AUC for SBE is 0.421 (95% CI: 0.343–0.498; p = 0.046).
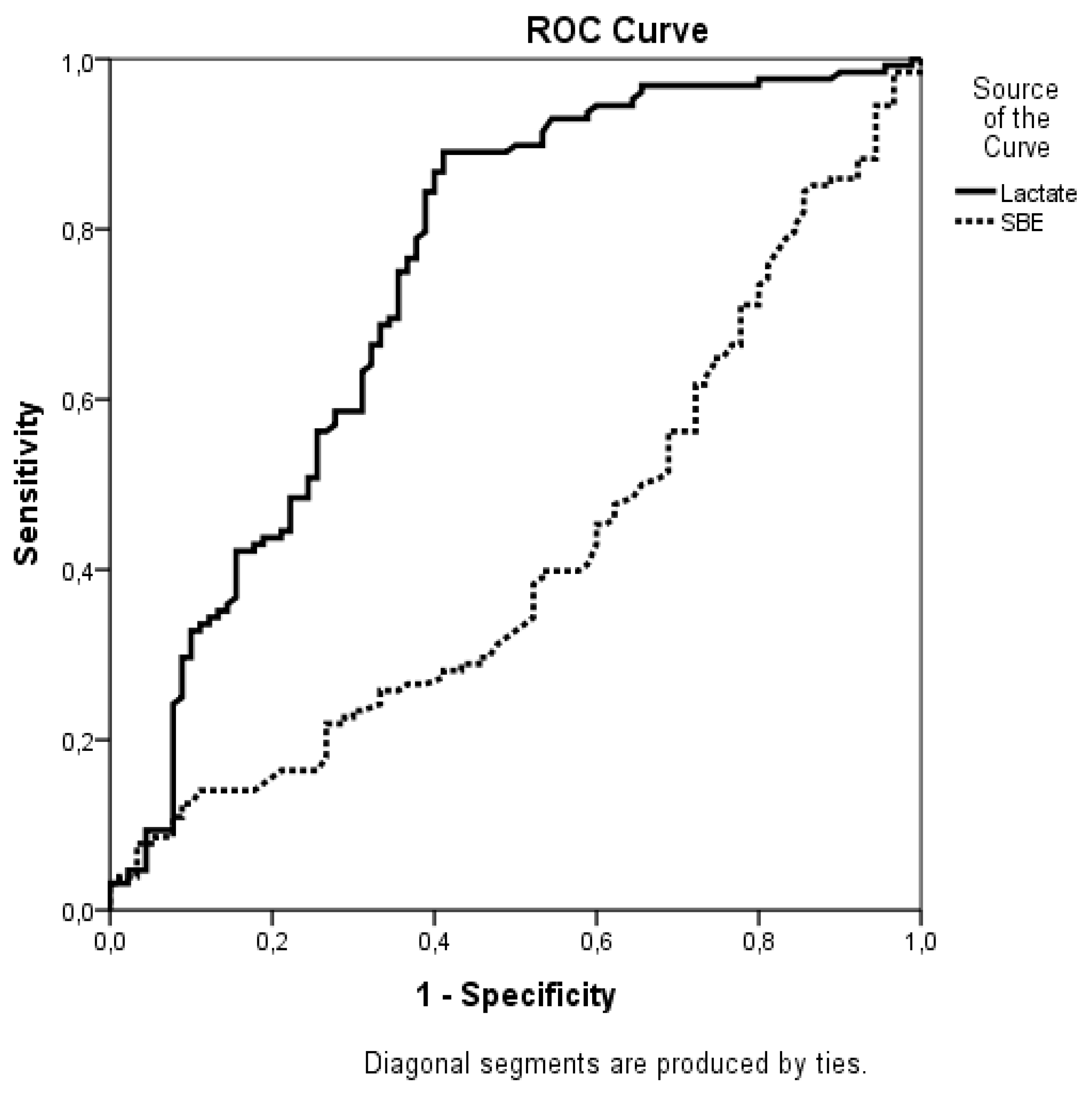

Table 1.
Demographic and clinical characteristics between survivors and non-survivors in patients with sepsis and septic shock.
Table 1.
Demographic and clinical characteristics between survivors and non-survivors in patients with sepsis and septic shock.
| Variables a |
Survivors N=90 |
Nonsurvivors N=128 |
P value univariate |
| Age |
71 (60-80) | 71 (59-79) | 0.990 |
| Male |
41 (46) | 74 (58) | 0.074 |
| APACHE II |
23 (18-27) | 28 (23-33) | <0.001 |
| SOFA |
9 (7-12) | 12 (9-14) | <0.001 |
| Charlson Comorbidity Index | 3 (2-5) |
3 (2-5) | 0.978 |
| Creatinin |
2.33 (0.96-3.79) | 1.9 (1.3-2.9) | 0.401 |
| Serum sodium |
134 (138-144) | 139 (134-1449 | 0.704 |
| Serum chloride |
101 (96-107) | 101 (94-106) | 0.472 |
| PH |
7.38 (7.30-7.46) | 7.38 (7.27-7.46) | 0.717 |
| Standart HCO3 |
22 (18-25) | 20 (16-24) | 0.030 |
| SBE |
-2.8 ( -7.6 - +0.9) | -5.1 (-9.8 - -1) | 0.046 |
| Lactate |
1.2 (1.8-2.9) | 2.9 ( 2.3 - 4.1) | <0.001 |
| ABE |
-0.5 (-4.8- +2.2) | -1.6 (-5.6 - +2.2) | 0.551 |
| Vasopressor use |
64 (71.1) | 124 (97) | <0.001 |
| IMV |
34 (38) | 110 (86) | <0.001 |
| Hemodialysis |
32 (36) | 73 (57) | 0.002 |
| Length of ICU days |
7 (4-13) | 8 (4-16) | 0.166 |
a Data are presented as median (interquartile range) for continuous variables and n (%) for categorical variables. Abbreviations: APACHE II, Acute Physiology and Chronic Health Evaluation II; SOFA, Sequential Organ Failure Assessment; HCO₃, bicarbonate; SBE, standard base excess; ABE, alactic base excess; IMV, invasive mechanical ventilation; ICU, intensive care unit.
Table 2.
Logistic Regression Analysis of Factors Associated with Mortality.
| Variables | OR | %95 CI | P value |
| APACHE II score | 1.08 | 1.02-1.15 | 0.013 |
| Lactate level | 1.40 | 1.11-1.77 | 0.005 |
| Vasopressore use | 1.32 | 1.05-1.68 | 0.028 |
| IMV | 1.45 | 1.10-1.92 | 0.012 |
Abbreviations: APACHE II; Acute Physiology and Chronic Health Evaluation II, OR; Odds Ratio, CI; Confidence Interval, IMV; Invasive Mechanical Ventilation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



