
Submitted:
10 January 2025
Posted:
13 January 2025
You are already at the latest version
Abstract
Simulation has evolved from basic practice to Immersive Extended Reality (I-XR). This systematic review examined 56 published studies on the impact of I-XR, including virtual reality (VR), augmented reality (AR), and mixed reality (MR), on the education of medical and nursing students, specifically their skill competency and knowledge acquisition. The results demonstrate the significant potential of I-XR in healthcare education, with 42.5% of VR studies, 42.9% of AR studies, and the single MR study also demonstrating greater improvements in clinical skills and knowledge acquisition compared to non-I-XR training conditions. In contrast, only 2.5% of VR studies and 7.14% of AR studies favored non-I-XR methods. It is important, however, to acknowledge the 26.8% of studies that showed mixed results (some evidence for the I-XR methods on some outcomes, but also some evidence for the non-immersive (non-I-XR) methods, on other outcomes). Notably, the review also identified a critical gap in the theoretical foundations of I-XR learning, highlighting an urgent need for research to inform the effective pedagogical implementation of these powerful tools.
Keywords:
medical/healthcare education
; conventional simulation-based learning
; immersive extended reality(I-XR)
; learning theory
1. Introduction
Simulation-based training is a pedagogical approach that employs simulated scenarios or environments to improve clinical skills, mainly among health field workers. The objective is to replicate real-world situations to provide a realistic and immersive experience without exposing patients to real risks (Becker & Hermosura, 2019). Simulation-based training complements conventional teaching methods, focusing on improving skill acquisition, decision-making, and teamwork (Ajemba et al., 2024). Such clinical experiences can help to create an opportunity for students to apply didactic content to clinical practice which allows students to bridge knowledge, skills, and competency (Hultquist & Bradshaw, 2016).
Halsted's "see one, do one, teach one" model, while groundbreaking in 1890, is now criticized for prioritizing rapid experience over deliberate skill development and patient safety (Ayub, 2022; Baskaran et al., 2023). This approach raises concerns about inadequate preparation, potentially leading to medical errors and a lack of emphasis on critical thinking and self-reflection (Rohrich, 2006). Modern medical education is shifting towards comprehensive training models that prioritize patient safety and incorporate simulation, deliberate practice, and feedback (Ayub, 2022; Baskaran et al., 2023).
Simulation-based medical education (SBME) (Saleem & Khan, 2023) offers a viable solution to bridge this gap. SBME enables deliberate practice and standardized training in a safe learning environment. It incorporates a wide array of techniques, ranging from basic mannequin-based simulations and standardized actor-patients to complex multimedia scenarios (Shah et al., 2022; Ziv, 2003). Through SBME, students can build confidence and competence, and ultimately enhance patient safety and the overall quality of care.
SBME has three primary objectives: (1) the execution of clinical skills, (2) supervised practice of that skill, and ultimately, (3) the independent and confident performance of clinical skills. This educational approach extends beyond technical proficiency to encompass the development of exteroceptive awareness in aspiring professionals. Exteroceptive awareness, the ability to perceive and interpret external stimuli, is crucial for stress management, confidence building, and overall well-being (Baskaran et al., 2023). Specifically, cultivating exteroceptive awareness helps regulate the sympathetic nervous system and manage stress responses in high-pressure situations, such as surgical procedures, thereby enabling healthcare professionals to maintain composure and perform optimally.
Specifically, significant positive effects for SBME (vs. non-simulated methods) have been shown for theory knowledge, analytic skills, learning interest and understanding, satisfaction, cooperative ability, problem-solving ability, teaching success, and situation awareness (Su & Zeng, 2023). Additionally, SBME proves effective for assessing teamwork and communication among healthcare providers (Dodson et al., 2023; Sezgin & Bektas, 2023). These benefits translate into improved patient outcomes and reduced healthcare costs (Le Cook et al., 2013; Issenberg et al., 2005), establishing it as a fundamental pillar of healthcare clinical training (Saleem & Khan, 2023) that provides a safe and effective environment for learners to develop crucial skills and decision-making abilities (Pottle, 2023).
1.1. Integration of I-XR in Healthcare Education
Recent technological advancements have further propelled SBME to include methods like virtual reality (VR), augmented reality (AR), and mixed reality (MR) (Tang et al., 2016). These methods are thought to help better equip healthcare students with practical experience and readiness for actual scenarios and procedures (Horowitz et al., 2022; Wu & Norvell, 2022). Such technologies are increasingly seen as having promise for teaching in the healthcare professions, even though the largest market is still in the entertainment and the gaming industry (Bankar et al., 2023; Wohlgenannt et al., 2022).
Extended reality (XR) is an umbrella term used to include VR, AR, and MR (Aebersold et al., 2020), but typically refers to computer-generated images in the wearer’s field of vision and includes the range of the user’s view of the world that can exist from fully visible to fully occluded (Zhang et al., 2023), and thus blurs the line between the digital world and the physical world (Chengoden et al., 2023). Finally, Immersive Extended Reality (I-XR) is characterized as a screen-based simulation that highlights the 3D nature of the simulated patients, graphics, sound, and navigation through the environment (McGrath et al., 2018). The use of I-XR for healthcare education is becoming increasingly more recognized as it allows an almost unlimited number of clinical scenarios to be simulated, with the ability to allow real-time feedback on student progress and patient status (Lu & Bowman, 2021), and can improve users’ motivation, engagement and enjoyment in educational learning across different domains by providing powerful experiential learning (Fokides et al., 2021; Tonteri et al., 2023). As more healthcare educators pioneer innovative methods, I-XR is emerging at the forefront of teaching and learning and is preparing healthcare students with practical skills, hands-on experience, and preparedness for real-world scenarios and procedures (Horowitz et al., 2022). Embracing these changes represents innovative steps towards cultivating a more knowledgeable, proficient, and self-assured healthcare workforce, benefiting patients, and enhancing healthcare education.
1.2. Review of I-XR Studies for Training Effectiveness in Healthcare Education
Whether I-XR methodologies specifically improve student learning outcomes compared to non-immersive (non-I-XR) methods is still up for debate. Historically, the majority of meta-analytic studies focused on medical students’ surgical skills (Zhang et al., 2023). Within the last five years, there has been a surge of systematic reviews and statistical meta-analyses seeking to explore whether I-XR (specifically VR, AR, MR) methodologies improve students’ learning outcomes across domain-specific skills, procedural outcomes, and even non-technical skills (e.g., empathy, self-efficacy, teamwork). Despite the number of reviews, the results are still inconclusive and often dependent on how “knowledge acquisition” and “skill performance” are operationalized. For instance, a meta-analysis of 11 studies on VR endoscopy training for medical students found that while VR improved procedure completion and overall performance ratings compared to traditional methods, it resulted in fewer independent completions and showed no difference in other behavioral outcomes (Khan et al., 2018). Another VR systematic review of nine studies revealed that only two showed improved knowledge acquisition in healthcare professionals compared to control groups (Abbas et al., 2023), suggesting that while VR can enhance knowledge, it may not be consistently superior to other methods. However, the same review found significant increases in skill performance in 19 out of 21 studies comparing VR to control methodologies (Abbas et al., 2023), indicating a stronger impact on practical skills. Other recent reviews (Dicheva et al., 2023; Huai et al., 2024; Jallad & Işık, 2022; Uslu-Sahan et al., 2023) show positive effects of I-XR on nursing students' knowledge, skill performance, skill acquisition, and clinical reasoning. These varied results suggest that the effectiveness of I-XR may depend on factors such as the specific technology used, the type of training, and the outcome being measured. Further research is needed to fully understand the conditions under which I-XR can optimize learning outcomes in healthcare education.
The results are also mixed as to whether one kind of immersive technology (AR, VR, MR) is more effective than another. For example, a systematic review of VR head-mounted displays in medical education (Kovoor et al., 2021) showed significant increases in learning surgical procedures in seven of the 11 studies reviewed compared to other immersive methodologies, but no differences when directly compared with AR. Yet, when assessing anatomy knowledge, only one of the six studies reviewed showed increased anatomy knowledge using VR. The authors concluded that VR technologies outperformed conventional methods for learning surgical skills, but they were not superior for learning anatomy knowledge. Yet, in another meta-analysis, VR methodologies proved to be more effective in improving nursing students’ performance skills compared to other mixed reality methodologies (Chen et al., 2023).
Despite the mixed evidence for I-XR technologies compared to non-immersive technologies in learning procedural skills and knowledge acquisition, the specific teaching and learning processes remain under-explored. Therefore, how these methods use or adhere to learning theories to understand the delivery of skills and knowledge could be another overlooked possibility for the mixed evidence.
For example, educational learning theories offer valuable frameworks for understanding how students acquire knowledge and develop skills. Researchers have identified thirteen key theoretical perspectives relevant to medical education, including cognitivism, constructivism, experiential learning, and reflective learning, among others (Kaufman & Mann, 2011; Mann, 2011). These theories guide a range of pedagogical approaches, from optimizing information presentation (Issa et al., 2013) to fostering reflective practice (Van Merriënboer & Sweller, 2010).
However, despite the potential benefits of integrating learning theories into I-XR research, several studies have identified a concerning trend. Many studies on I-XR in healthcare education either poorly described or completely omitted their pedagogical approaches (Kivuti-Bitoket al., 2022). In one study, less than 3% of papers on VR simulations incorporated a conceptual framework or theory in their design, and self-initiated training was the most common mode (Jiang & Fryer, 2024).
This lack of theoretical grounding raises concerns about the rigor and generalizability of I-XR research in healthcare education. Without a clear theoretical foundation, it becomes difficult to understand why certain interventions are effective and how they can be optimized for different learning contexts. This highlights a critical need for researchers to explicitly integrate learning theories into the design, implementation, and evaluation of I-XR training programs.
1.3. Summary
In sum, I-XR is transforming healthcare education by providing immersive and engaging learning experiences that enhance skill acquisition, knowledge retention, and preparedness for clinical practice. This technology aligns with the evolving needs of healthcare training, offering adaptable and flexible solutions for integrating cutting-edge techniques. As technology continues to advance, I-XR is poised to play an increasingly vital role in shaping the future of healthcare education. However, realizing the full potential of I-XR depends on equipping healthcare educators with the necessary skills and resources to integrate these technologies into high-quality patient care training effectively.
1.4. Purpose
This systematic review aimed to examine the effectiveness of I-XR training for healthcare students (e.g., medical and nursing). The review focused on comparing I-XR training methods to traditional, non-immersive approaches. Specifically, we sought to determine whether I-XR training leads to greater improvements in both skill competency and knowledge acquisition. Skill competency and knowledge acquisition were assessed across multiple domains, including performance skills, objective performance measures, clinical reasoning, internship grades, problem-solving skills, and skills knowledge.
This review offers several unique contributions to the field. First, it examines six distinct outcomes related to skill competency and knowledge acquisition. Second, it focuses on both graduate medical and nursing education across a wide range of techniques, providing a comprehensive overview of I-XR's potential in healthcare training. Third, recognizing that the effectiveness of I-XR may depend on the specific alternative being compared, the review analyzes results according to the type of non-immersive (comparison) group used (e.g., didactic instruction, manikin-based training, simulated patients). Fourth, unlike many reviews that focus on a single technology, this review encompasses the full breadth of I-XR techniques, including AR, VR, and MR. Finally, it assesses each study for its integration of pedagogical approaches and learning theory, providing insights into best practices for implementing I-XR in healthcare education.
2. Methods
2.1. Search Strategy
Consistent with Best Evidence in Medical Education (BEME) recommendations, the search was performed on the inclusive databases of PubMed and Google Scholar in January 2023 and again on April 1, 2024, and followed the Joanna Briggs Institute for scoping reviews. Search terms included “simulation in medical (or nursing) education” and “augmented reality (AR)” [or virtual reality (VR)” or “mixed reality (MR)”] and “skill outcome” (or “skill performance”). We selected articles based on the PRISMA method (see Figure 1). We have adhered to the PRISMA guidelines. This review was not pre-registered.
2.2. Inclusion and Exclusion Criteria
Only English articles were included. Only peer-reviewed empirical articles between the dates of January 1, 2016, and April 1, 2024, were included. XR papers surged in 2017, so this window captures the increase from 2016 to the present (Velev & Zlateva, 2017). No dissertations, letters to the editor, commentaries, or opinion pieces were included. Only articles with a control group were included, which could include a within-subject pre-posttest design, or a true, external comparison group. We also only included articles that focused on objective performance measures of skill competency and knowledge acquisition (i.e., performance skills, internship grades, performance measures, clinical reasoning or judgment, and problem-solving skills). Lastly, we included only articles that included graduate medical or nursing students. Studies were excluded if they were outside the indicated dates, did not include a control group or pre-post design, did not include medical or nursing graduate students (e.g., undergraduates), were not available in English, or were not in a peer-reviewed journal. Studies that solely included measures of confidence, self-esteem, or other non-technical skills were excluded from the process. For cases in which the studies included these measures but also included skill competency and/or knowledge acquisition measures, we reported only on the latter.
The initial search with parameters yielded 11,434 articles. Duplications were removed and titles and abstracts were evaluated for topic appropriateness. We also reviewed additional papers using the ancestral method (i.e., reviewing the references of included papers) that did not come up in our original search. After screening, 156 papers were left to review (see Figure 1). After reading these papers fully, 56 were included in the final data set (n = 100 removed for reasons indicated above) [Appendix A].
2.3. Data Extraction
We extracted the year, student sample size, field (e.g., medical, nursing), type of I-XR (AR/VR/MR), comparison group types, outcome measures, and any mention of learning theory. We also included a description of each study’s methods, results, and descriptive statistics for comparisons of interest (Table 1). At least three researchers reviewed each paper for the accuracy of these variables. Two coders coded the year, student sample, field, learning theory, and type of I-XR method. The agreement was > 95% on the first pass. The first and second authors coded the type of comparison groups and outcome measures, as well as made the final assessment for each. Initial agreement exceeded 85%. If codes were discrepant, the first author made the final decision.
2.4. Data Coding
Outcome measures (i.e. skill competency and knowledge acquisition) were initially operationalized with six categories based on past literature: “performance skills, including “direct observation of procedure” (DOPS); “performance measures” (Objective Structured Clinical Exams (OSCE), Global Operative Laparoscopic Assessment (GOALS), Global Rating Scale (GRS), Academic Achievement Test (AAT); “clinical judgment or clinical reasoning” (Laster Clinical Judgment Rubric (LCJR); “skills knowledge” (e.g., Mini-Clinical Evaluation Exercise (CEX), Mini-CEX, Neurological Physical Exam (NPE), multi-choice questions of skills (MCQ); “grade in internship”; and “problem-solving skills”. We then felt it necessary to subdivide “performance skills” into specific modifiers, regardless of the actual behavior (e.g., “performance skills errors,” “performance skills time,” “performance skills injury,” “performance skills dexterity”). Finally, we added an additional category: “performance skills other”, for cases in which the performance skill was not one of those noted above. If studies had more than one outcome measure, we evaluated each outcome separately. Therefore, the total number of measures exceeded the number of studies.
Comparison groups were grouped into seven categories, also based on previous literature. These groups included learning with: “print materials” (e.g., study guides, books, technical manuals), “teacher-led” (e.g., didactic/instructor-led), “electronic materials” (e.g., video tutorial, e-learning/computer materials), “practice” (e.g., BOX trainer, dissection, mannikin, simulated patient, case-based learning (CBL), or hands-on with instructor that was not immersive-XR). If a study had multiple comparison methods (e.g., electronic materials and practice), we coded it as “combined”. However, if a study included some students learning through print materials (comparison 1), and some learning via practice, the study was evaluated twice, in this case – once for each comparison group. If all students had additional training of some sort (including the I-XR group), we did not include that training as a comparison group. In those cases, the comparison group was coded as “did nothing additional”. Finally, some studies were pre-post studies with a comparison group. In those cases, the results were assessed concerning differences between the I-XR group and the comparison group(s) after the training, rather than any pre-post change.
We gave each study one of five final assessments (Table 1): (1) “Positive” (total support for I-XR methods on all outcomes for all comparisons), (2) “Negative” (total support for the control methods on all outcomes for all comparisons), (3) “No difference” (I-XR and control methods produced no differences on all variable and comparisons), (4) “Mixed Evidence Positive” or (5) “Mixed Evidence Negative”. “Mixed Evidence Positive” was used for cases in which the I-XR methods produced enhanced effects on more outcomes compared to the non-immersive (comparison) methods. Similarly, “Mixed Evidence Negative” was used for cases in which the comparison methods produced enhanced effects on more outcomes compared to the I-XR methods. Thus, “Mixed Evidence Positive” was given to any study that favored the I-XR methods, even if on some of the variables there were no differences with the comparison, or there were some differences that favored the comparison methods (as long as that number was fewer than those favoring the I-XR methods). A similar logic was used for Mixed Evidence Negative, except that the evidence favored the comparison methods. There was only one instance where “Mixed” without a qualifier was used. This was because there were two outcomes and one favored each.
2.5. Assessing Article Quality and Bias
There are several ways in which article quality and bias can be addressed, including the Critical Appraisal Skills Program (2024) instrument (Chen et al., 2017), the Mixed Methods Appraisal Tool (MMAT) (Hong et al., 2018), the Joanna Briggs Institute (JBI) tool (2014) , the Medical Education Research Study Quality Instrument (MERSQI) (Jaros & Dallaghan, 2024), the Newcastle-Ottawa Scale for Education (NOS-E) (Wells et al., 2014) [48], and the Quality Assessment of Diagnostic Accuracy Studies revised (QUADAS-2) (Whiting et al., 2011). In our exploration of the literature, we found that the most common assessments were the MERSQI, NOS-E, and QUADAS-2. Because both the MERSQI and the NOS-E evaluate different aspects of study design and quality, we chose to evaluate each study on both.
The MERSQI is used as a measure to assess the quality of educational studies across eight domains: 1) study design, 2) sampling, 3) response rate, 4) type of data, 5) validity of evidence for evaluation measures, 6) data analysis sophistication, 7) data analytic appropriateness, and 8) outcome. The maximum score for study design, validity of evidence, outcome, and type of data is “3”. For sampling design and response rate, the maximum score is “1.5”. For data analysis sophistication, the max score is “2”, and for data analysis appropriateness, the max score is “1”. Scores are summed, with the max score being 16. We also included the items from the NOS-E, which evaluates a study on sample representation, comparison groups, retention, and blinding conditions. Sample representation, selection of the comparison group, retention, and blinding conditions were all scored with a maximum of “1”, whereas the comparably of the comparison group was divided into randomized and non-randomized studies, each having a max score of “2”. Scores are summed, with the max score being eight. The max score for the total of both scales was thus “24”. The average MERSQI-2 plus NOS-E score across the 56 studies was 18.5, showing generally high quality of articles included (range: 15-22) (see Table 2).
To assess bias, we chose the QUADAS-2. The QUADAS-2 includes 11 items that assess risk of bias with “yes”/ ”no”/ ”unclear” marks. We included a total “yes” score that summed across the 11 statements, indicating bias. The average QUADAS-2 score across studies was 7.12 (range: 2-11), showing moderately high bias despite high study quality (see Table 2).
3. Results
3.1. Descriptive Findings
Of the 56 articles reviewed, 40 (71.43%) were VR studies, 14 were AR (25.0%), one study was an MR study, and one study was a VR/AR study because it was unclear whether the training was VR or AR based on the description of the apparatus (1.8%) (see Figure 3).
Most studies were published in 2020 (n = 13, 23.2%) (Figure 4).
80.4% (n = 45 studies) were performed on medical graduate students (n = 3641 individuals), compared to 19.6% of studies (n = 11) that were performed on nursing graduate students (n = 1085 individuals) (Figure 5).
The types of comparison techniques used across studies included: “print” (n = 13, 21.0%), “teacher” (n = 8, 12.9%), “electronic” (n = 10, 16.1%), “practice” (n = 15, 24.2%), “combined methods” (n = 6, 9.7%) , “pre-post” (n = 3, 4.8%), or “did nothing additional” (n = 7, 11.3%) (Figure 6).
“Performance skills” variables across studies included: “time”, n = 13, 11.3%; “errors”, n = 5, 4.4%; “dexterity’, n = 0, 0%; “injury”, n = 1, 0.9%; “other specific/DOPS”, n= 46, 40.0%) “skills knowledge’ (n = 28, 24.4%), “grade in internship” (n = 1, 0.9%), “performance measures” (n = 15, 13.0%), clinical judgment/reasoning skills” (n = 5, 4.4%), “problem-solving skills” (n = 1, 0.9%) (Figure 7). The average number of variables assessed in a study was two (range: 1- 12).
Table 2 also shows whether any learning theories were mentioned within the included studies. Approximately seventy-five percent of the studies did not mention any learning theory. Thirteen studies included one or more theories. The most commonly mentioned theory was cognitive load (n = 6). Simulation theory/NLN/Jeffries theory was mentioned three times, and self-regulated theory and Bloom’s theory were mentioned twice. Situated learning theory, directed self-regulated theory, simulation-based mastery learning, constructive alignment theory, deliberate practice, Kolb’s theory, and experiential learning theory were each mentioned once.
3.2. Overall Study Assessments of I-XR Skill Competency
Overall, we found that 42.5% of studies reported that VR was more effective than comparison (non-immersive) methodologies (Positive), 42.9% of AR studies were more effective than non-immersive methodologies (Positive), and the one MR (100%) was more effective than the comparison (Positive) (Figure 8). In addition, 25.0%, 21.4%, 0.0% of studies reported no difference between the VR, AR, MR group and the comparison groups, respectively (No difference). The one study classified as VR/AR also showed no change compared to the comparison (No difference). These percentages are compared to 35.0% (VR), 14.3% (AR) and 0.0% (MR) of studies showed mixed results (Mixed Evidence Positive or Mixed Evidence Negative). Finally, only two studies (one VR (2.5%) and one AR (7.14%)) favored the training comparisons (Negative).
4. Discussion
This review provides compelling evidence for the effectiveness of I-XR training in healthcare education. A substantial majority of studies (42.9%) demonstrated that I-XR methodologies led to universally improved outcomes compared to traditional training comparison methods. These percentages reflect improved outcomes on all measures, thus underscoring the findings' robustness. Only a small minority (3.6%) of studies universally favored comparison (non-immersive) approaches.
It is important, however, to acknowledge that 26.8% of I-XR studies showed mixed results (Mixed Positive, n = 10, 17.9%; Mixed Negative, n = 4, 7.1%; Mixed, n = 1, 1.8%). The effectiveness of I-XR is therefore not universal and may depend on various factors such as the specific technology used, the type of training, and the implementation context. Further research is needed to identify the conditions under which I-XR is most effective and to develop evidence-based guidelines for its optimal use.
A significant gap in the theoretical foundation of I-XR teaching and learning approaches was also revealed. Many studies lacked a clear articulation of the learning theories guiding their pedagogical strategies. This omission hinders the development of effective, evidence-based practices and may stem from a limited understanding of how best to teach and learn in these emerging digital environments. While I-XR offers exciting possibilities for simulation, interaction, and experiential learning, traditional pedagogical models designed for physical classrooms may not translate effectively to the virtual realm. For example, some studies have indicated challenges in maintaining student engagement, fostering collaboration, and ensuring equitable access in virtual learning environments (Zweifach & Triola, 2019).
These challenges underscore the need for further research to explore pedagogical approaches specifically for virtual learning environments. Future studies should prioritize the development of robust pedagogical frameworks specifically for I-XR, grounded in established learning theories. Additionally, more research is needed to determine the conditions under which I-XR training is most effective, considering factors such as the type of technology, the learning objectives, and the characteristics of the learners. By addressing these critical areas, the full potential of I-XR can be unlocked, optimizing its use in healthcare education to enhance the training of future healthcare professionals.
4.1. Limitations
While I-XR technology holds immense promise for revolutionizing healthcare education, a critical appraisal of the current landscape necessitates overcoming significant limitations. First, the existing body of research is hampered by methodological weaknesses, notably the prevalence of high bias in published studies. This bias, a well-documented phenomenon across academic research, may lead to an inflated perception of I-XR's positive effects, obscuring a clear and objective understanding of its true impact on learning outcomes and clinical performance.
Second, the inherent limitations of I-XR technology itself pose substantial barriers to widespread adoption. The acquisition and maintenance of I-XR equipment, software, and dedicated simulation spaces often entail significant financial investment, potentially creating disparities in access to this technology, particularly for institutions with limited resources.
Moreover, users may experience physiological side effects, such as cybersickness (including nausea, dizziness, and disorientation), eye strain, and headaches, which can hinder learning, diminish user engagement, and impede the seamless integration of I-XR into educational practices (Kolcun et al., 2023). Furthermore, the effective implementation of I-XR necessitates careful planning, technical expertise, and ongoing support. Challenges include the time and effort required for content creation, customization, and integration with existing curricula, as well as the need for dedicated technical support to troubleshoot issues and ensure smooth operation.
Addressing these limitations will require a multi-pronged approach. Future research should prioritize rigorous methodologies, including randomized controlled trials with well-defined comparison groups and objective outcome measures, to mitigate bias and provide a more robust evidence base for I-XR's efficacy. Technological advancements are urgently needed to reduce costs, enhance user comfort, and minimize physiological side effects, making I-XR more accessible and user-friendly.
Finally, fostering collaborative partnerships between educators, technology developers, and institutional stakeholders is crucial to addressing logistical challenges, developing best practices for implementation, and facilitating the seamless integration of I-XR into healthcare education. By acknowledging and proactively addressing these limitations, we can pave the way for the successful and impactful integration of I-XR, ultimately transforming healthcare education and improving patient care.
4.2. Future Directions
The future of healthcare education stands at the precipice of a transformative era fueled by the remarkable potential of I-XR technologies. These technologies, encompassing VR, AR, and MR, offer unprecedented opportunities to create engaging and effective learning experiences that bridge the gap between theoretical knowledge and practical application. However, successfully integrating I-XR into healthcare education requires a thoughtful and comprehensive approach beyond mere technological adoption. It demands a fundamental shift in pedagogical thinking, prioritizing the application of established learning theories, such as experiential learning and embodied cognition, to guide the design and implementation of I-XR curricula. Experiential learning emphasizes the importance of active engagement and hands-on experiences in the learning process, while embodied cognition highlights the interconnectedness of mind and body, suggesting that learning is enhanced when it involves physical interaction and sensory immersion (Macrine & Fugate, 2022). By grounding I-XR experiences in these theoretical frameworks, educators can create immersive and impactful learning environments that foster deep understanding, critical thinking, and skill acquisition.
Furthermore, the effective integration of I-XR necessitates a collaborative ecosystem where medical education leaders, faculty, and technology developers work in concert. This collaboration should focus on establishing a shared vision for I-XR integration that aligns with the goals of healthcare education, providing comprehensive faculty training to empower them to adapt their curricula and pedagogy, and encouraging active faculty participation in the development of future I-XR applications. To ensure consistency and quality, standardized methods for educating, assessing, and certifying I-XR instructors are essential.
While dedicated virtual simulation centers currently represent a significant step towards realizing the potential of I-XR in healthcare education, the future points towards increased accessibility and versatility. Imagine a future where I-XR transcends the confines of specialized centers, seamlessly integrating with mobile devices and wearable technology. This would empower healthcare professionals with a powerful toolkit readily available at their fingertips, enabling them to access course content, patient information, and real-time patient data during rounds using wearable devices or smartphones.
Problem-based learning, a cornerstone of medical education, could be further enhanced through I-XR, with virtual patients and dynamic case scenarios providing a safe and engaging environment for students to hone their clinical reasoning and decision-making skills. As I-XR technology becomes more affordable and accessible, collaborations will drive the development of innovative applications tailored to the diverse needs of individual learners and healthcare disciplines, fostering personalized learning experiences.
The future of I-XR also holds the promise of even richer and more immersive experiences. Haptic feedback devices will enable students to simulate procedures with unparalleled realism, developing muscle memory and refining their dexterity. Realistic visuals and soundscapes will transport students to diverse clinical settings, from bustling emergency rooms to serene operating theaters, fostering a deeper understanding of contexts and enhancing their ability to adapt to different environments. The key to unlocking the full potential of I-XR lies in integrating learning theory into I-XR experiences and creating immersive and impactful learning environments that optimize teaching, learning, and evaluation. This, coupled with ongoing innovation and collaboration, will ensure that healthcare education remains at the forefront of technological advancement and pedagogical excellence.
Author Contributions
The first author conceived the idea, coded all articles, and co-wrote the manuscript. The second author completed all searches and initially coded all articles and contributed to the writing of the manuscript. The third author co-wrote the manuscript.
Funding
The authors received no financial support for this work.
Data Availability Statement
Data spreadsheet for coding of articles is available from the first author via email request.
Acknowledgements
A special thanks to Amyah Campbell and Shannon Montague who helped with article scoring. The authors would like to thank Payton Chance who helped with coding the articles included in the review, Rochely Negron who helped with the graphing and counting of the articles, and Syd Seymour who helped with the databasing of the articles. In addition, Shannon Montague and Amayah Campbell helped with quality and bias assessment for each article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Abbas, J.R.; Chu, M.M.; Jeyarajah, C.; Isba, R.; Payton, A.; McGrath, B.; Tolley, N.; Bruce, I. Virtual reality in simulation-based emergency skills training: A systematic review with a narrative synthesis. Resusc Plus 2023, 16. [Google Scholar] [CrossRef] [PubMed]
- Aebersold, M.; Dunbar, D.M. Virtual and augmented realities in nursing education: State of the science. Annu Rev Nurs Res. 2020, 39, 225–242. [Google Scholar] [CrossRef] [PubMed]
- Ajemba, M.N.; Ikwe, C.; Iroanya, J.C. Effectiveness of simulation-based training in medical education: assessing the impact of simulation-based training on clinical skills acquisition and retention: A systematic review. World Journal of Advanced Research and Reviews 2024, 21, 1833–1843. [Google Scholar] [CrossRef]
- Ayub, S.M. See one, do one, teach one: Balancing patient care and surgical training in an emergency trauma department. J Glob Health 2022, 12. [Google Scholar] [CrossRef]
- Bankar, M.N.; Bankar, N.J.; Singh, B.R.; Bandre, G.R.; Shelke, Y.P.; Bankar, M.; Shelke, Y.P. The role of E-content development in medical teaching: How far have we come? Cureus 2023, 15. [Google Scholar] [CrossRef]
- Baskaran, R.; Mukhopadhyay, S.; Ganesananthan, S. Enhancing medical students’ confidence and performance in integrated structured clinical examinations (ISCE) through a novel near-peer, mixed model approach during the COVID-19 pandemic. BMC Med Educ. 2023, 23, 128. [Google Scholar] [CrossRef]
- Becker, L.R.; Hermosura, B.A. (2019). Comprehensive healthcare simulation: obstetrics and gynecology. Springer. (pp. 11–24). ISBN 978-3-319-98994-5.
- Chen, C.Y.; Huang, T.W.; Kuo, K.N.; Tam, K.W. Evidence-based health care: a roadmap for knowledge translation. J Chin Med Assoc. 2017, 80, 747–749. [Google Scholar] [CrossRef]
- Chen, F.Q.; Leng, Y.F.; Ge, J.F.; Wang, D.W.; Li, C.; Chen, B.; Sun, Z.L. Effectiveness of virtual reality in nursing education: meta-analysis. J Med Internet Res. 2020, 22. [Google Scholar] [CrossRef]
- Chengoden, R.; Victor, N.; Huynh-The, T.; Yenduri, G.; Jhaveri, R.H.; Alazab, M.; Gadekallu, T.R. Metaverse for healthcare: A survey on potential applications, challenges, and future directions. IEEE Access 2023, 11, 12765–12795. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. Available online: http://www.casp-uk.net/. (accessed on 25 April 2024).
- Dicheva, N.K.; Rehman, I.U.; Husamaldin, L.; Aleshaiker, S. (2023). Improving nursing educational practices and professional development through smart education in smart cities: A systematic literature review. In Proceedings of the 2023 IEEE International Smart Cities Conference, Bucharest, Romania, 24 September (pp. 1–7).
- Dodson, T.M.; Reed, J.M.; Cleveland, K. Exploring undergraduate nursing students’ ineffective communication behaviors in simulation: A thematic analysis. Teach Learn Nurse 2023, 18, 480–485. [Google Scholar] [CrossRef]
- Fokides, E.; Atsikpasi, P.; Arvaniti, P.A. Lessons learned from a project examining the learning outcomes and experiences in 360o videos. Journal of Educational Studies and Multidisciplinary Approaches 2021, 1, 50–70. [Google Scholar] [CrossRef]
- Hong, Q. N.; Gonzalez-Reyes, A.; Pluye, P. Improving the usefulness of a tool for appraising the quality of qualitative, quantitative, and mixed methods studies, the Mixed Methods Appraisal Tool (MMAT). Journal of Evaluation in Clinical Practice 2018, 24, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, M.L.; Stone, D.S.; Sibrian, J.; DuPee, C.; Dang, C. An innovative approach for graduate nursing student achievement of leadership, quality, and safety competencies. J Prof Nurs. 2022, 43, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Huai, P.; Li, Y.; Wang, X.; Zhang, L.; Liu, N.; Yang, H. The effectiveness of virtual reality technology in student nurse education: A systematic review and meta-analysis. Nurse Educ Today 2024, 138, 106189. [Google Scholar] [CrossRef]
- Hultquist, B.L., & Bradshaw, M.J. (Eds.). Innovative teaching strategies in nursing and related health professions, 7th ed; Jones & Bartlett Publishers. ISBN 978-1284107074.
- Issa, T.; Isaias, P.T.; Kommers, P. Guest editors’ introduction- Special issue on digital society and e-technologies. Pacific Asia Journal of the Association for Information Systems 2013, 5. [Google Scholar] [CrossRef]
- Issenberg, B.S; Mcgaghie, W.C.; Petrusa, E.R.; Lee, Gordon D. ; Scalese, R.J. Features and uses of high-fidelity medical simulations that lead to effective learning: A BEME systematic review. Med Teach. 2005, 27, 10–28. [Google Scholar] [CrossRef]
- Jallad, S.T.; Işık, B. The effectiveness of virtual reality simulation as a learning strategy in the acquisition of medical skills in nursing education: a systematic review. Ir J Med Sci. 2022, 191, 1407–1426. [Google Scholar] [CrossRef]
- Jaros, S.; Dallaghan, G.B. Medical education research study quality instrument: an objective instrument susceptible to subjectivity. Med Educ Online 2024, 29. [Google Scholar] [CrossRef]
- Jiang, J. , & Fryer, L.K. The effect of virtual reality learning on students' motivation: A scoping review. J Comput Assist Learn. 2024, 40, 360–373. [Google Scholar] [CrossRef]
- Joanna Briggs Institute. Joanna Briggs Institute Reviewers’ Manual: 2014 Edition. Available online: http://www.joannabriggs.org/sumari.html (accessed on day month year).
- Kaufman, D.M.; Mann, K.V. (2010). Teaching and learning in medical education: how theory can inform practice. In Understanding Medical Education: Evidence, Theory, and Practice. Swanwick, T. (Eds.). Wiley Online Library: New York, USA. (pp. 16–36). ISBN: 978-1-405-19680-2. [CrossRef]
- Khan, R.; Plahouras, J.; Johnston, B.C.; Scaffidi, M.A.; Grover, S.C.; Walsh, C.M. Virtual reality simulation training for health professions trainees in gastrointestinal endoscopy. Cochrane Database Syst Rev. 2018, 8. [Google Scholar] [CrossRef]
- Kivuti-Bitok, L.W.; Cheptum, J.J.; Mutwiri, M.; Wanja, S.; Ngune, I. Virtual reality and serious gaming in re-engineering clinical teaching: a review of literature of the experiences and perspectives of clinical trainers. Afr J Health Nurs Midwifery 2022, 6, 53–86. [Google Scholar] [CrossRef]
- Kolcun, K.; Zellefrow, C.; Karl, J.; Ulloa, J.; Zehala, A.; Zeno, R.; Tornwall, J. Identifying best practices for virtual nursing clinical education: A scoping review. J Prof Nurs. 2023, 48, 128–146. [Google Scholar] [CrossRef] [PubMed]
- Kovoor, J.G.; Gupta, A.K.; Gladman, M.A. Validity and effectiveness of augmented reality in surgical education: a systematic review. Surgery 2021, 170, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Le Cook, B.; Manning, W.; Alegria, M. Measuring disparities across the distribution of mental health care expenditures. The Journal of Mental Health Policy and Economics 2013, 16, 3–PMC3662479. [Google Scholar]
- Lu, F.; Bowman, D.A. (2021). Evaluating the potential of glanceable AR interfaces for authentic everyday uses. 2021 IEEE Virtual Reality and 3D User Interfaces. (pp. 768–777). [CrossRef]
- Macrine, S.L.; Fugate, J.M.B. (Eds.) (2022). Movement Matters: How Embodied Cognition Informs Teaching and Learning. MIT Press. [CrossRef]
- Mann, K.V. Theoretical perspectives in medical education: past experience and future possibilities. Medical Education 2011, 45, 60–68. [Google Scholar] [CrossRef]
- McGrath, J.L.; Tekman, J.M.; Dev, P.; Danforth, D.R.; Mohan, D.; Kman, N.; Crichlow, A.; Bond, W.F. Using virtual reality simulation environments to assess competence for emergency medicine learners. Acad Emerg Med. 2018, 25, 186–195. [Google Scholar] [CrossRef]
- Pottle, J. Virtual reality and the transformation of medical education. Future Healthc J. 2019, 6, 181–185. [Google Scholar] [CrossRef]
- Rohrich, R.J. See one, do one, teach one: An old adage with a new twist. Plastic Reconstructive Surgery 2006, 118, 257–258. [Google Scholar] [CrossRef]
- Saleem, M.; Khan, Z. Healthcare Simulation: An effective way of learning in health care. Pak J Med Sci. 2023, 39, 1185–1190. [Google Scholar] [CrossRef]
- Sezgin, M.G.; Bektas, H. Effectiveness of interprofessional simulation-based education programs to improve teamwork and communication for students in the healthcare profession: A systematic review and meta-analysis of randomized controlled trials. Nurse Educ Today 2023, 120. [Google Scholar] [CrossRef]
- Shah, N.K.; Taunk, N.K.; Maxwell, R.; Wang, X.; Hubley, E.; Anamalayil, S.; Trotter, J.W.; Li, T. Comparison of virtual reality platforms to enhance medical education for procedures. Front Virtual Real. 2022. [Google Scholar] [CrossRef]
- Su, Y.; Zeng, Y. Simulation-based training versus non-simulation-based training in anesthesiology: A meta-analysis of randomized controlled trials. Heliyon 2023, 9. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.S.; Cheng, D.L.; Mi, E.; Greenberg, P.B. Augmented reality in medical education: A systematic review. Can Med Educ J. 2020, 11, 81–96. [Google Scholar] [CrossRef] [PubMed]
- Tonteri, T.; Holopainen, J.; Lumivalo, J.; Tuunanen, T.; Parvinen, P.; Laukkanen, T. (2023). Immersive virtual reality in experiential learning: A value co-creation and co-destruction approach. In Proceedings of the 56th Hawaii International Conference on System Sciences, Hawaii, USA, January 2023, pp. 1313–1322. https://scholarspace.manoa.hawaii.edu/server/api/core/bitstreams/cb46cecd-c8e2-4f8e-9c37-c44af3ae0d32/content.
- Uslu-Sahan, F.; Bilgin, A.; Ozdemir, L. Effectiveness of virtual reality simulation among BSN students: A meta-analysis of randomized controlled trials. Comput Inform Nurs. 2023, 41, 921–929. [Google Scholar] [CrossRef]
- Van Merriënboer, J.J. , & Sweller, J. Cognitive load theory in health professional education: design principles and strategies. Med Educ. 2010, 44, 85–93. [Google Scholar] [CrossRef]
- Velev, D.; Zlateva, P. Virtual reality challenges in education and training. Int J Learn Teach. 2017, 3, 33–37. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. (2014). Newcastle-Ottawa quality assessment scale cohort studies. University of Ottawa. https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Wohlgenannt, I.; Simmon, A.; Stieglitz, S. Virtual reality. Bus Inf Syst Eng. 2020, 62, 455–461. [Google Scholar] [CrossRef]
- Wu, A.W.; Norvell, M. To improve patient safety, lean in. J Patient Saf Risk Manag. 2022, 27, 3–5. [Google Scholar] [CrossRef]
- Zhang, J.; Lu, V.; Khanduja, V. The impact of extended reality on surgery: a scoping review. Int Orthop. 2023, 47, 611–621. [Google Scholar] [CrossRef]
- Ziv, A.; Wolpe, P.R.; Small, S.D.; Glick, S. Simulation-based medical education: An ethical imperative. Acad Med. 2003, 78, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Zweifach, S.M.; Triola, M.M. Extended reality in medical education: driving adoption through provider-centered design. Digital Biomark. 2019, 3, 14–21. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA Flowchart.
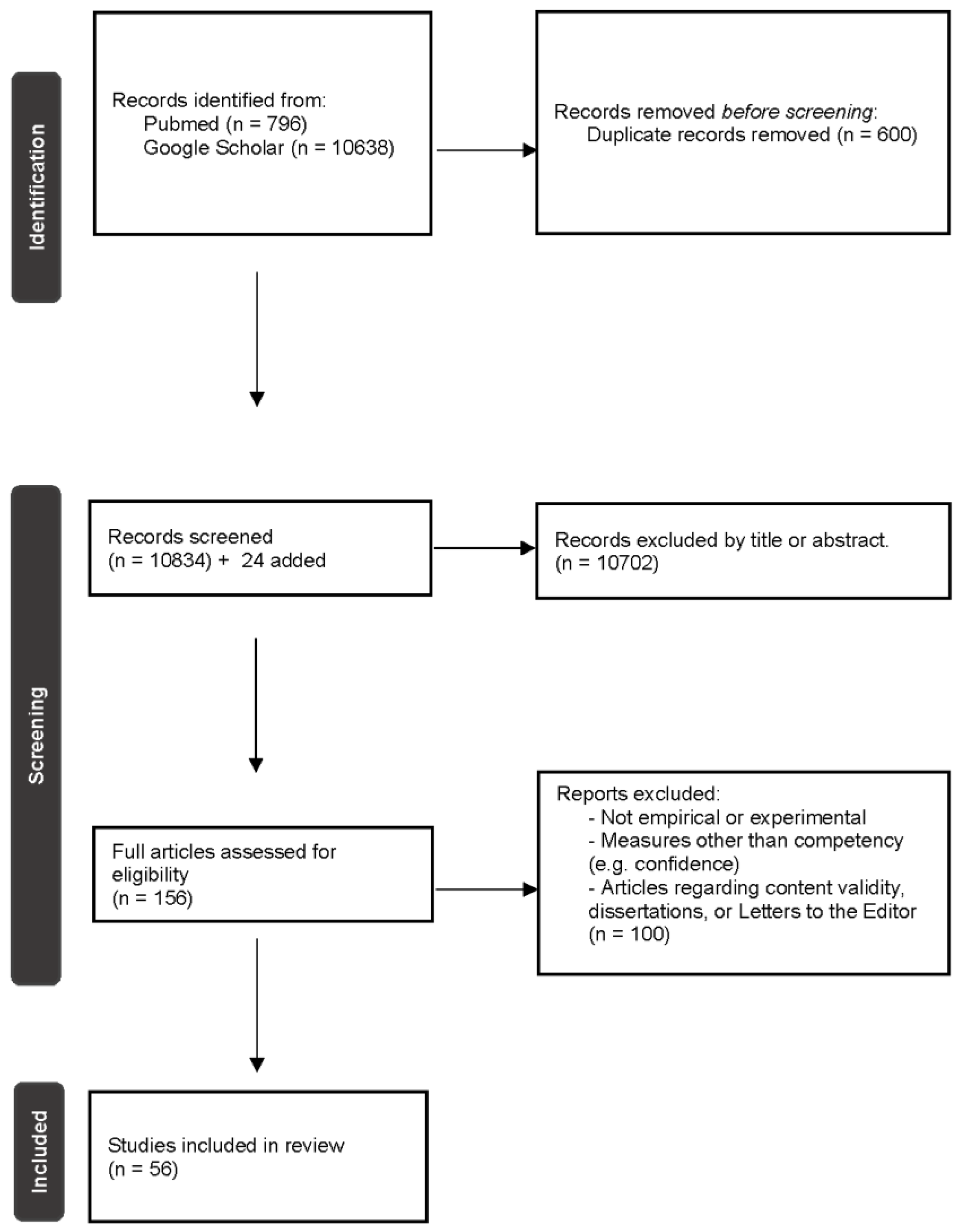
Figure 3.
Percentages of Immersive Techniques Used (l-XR.).
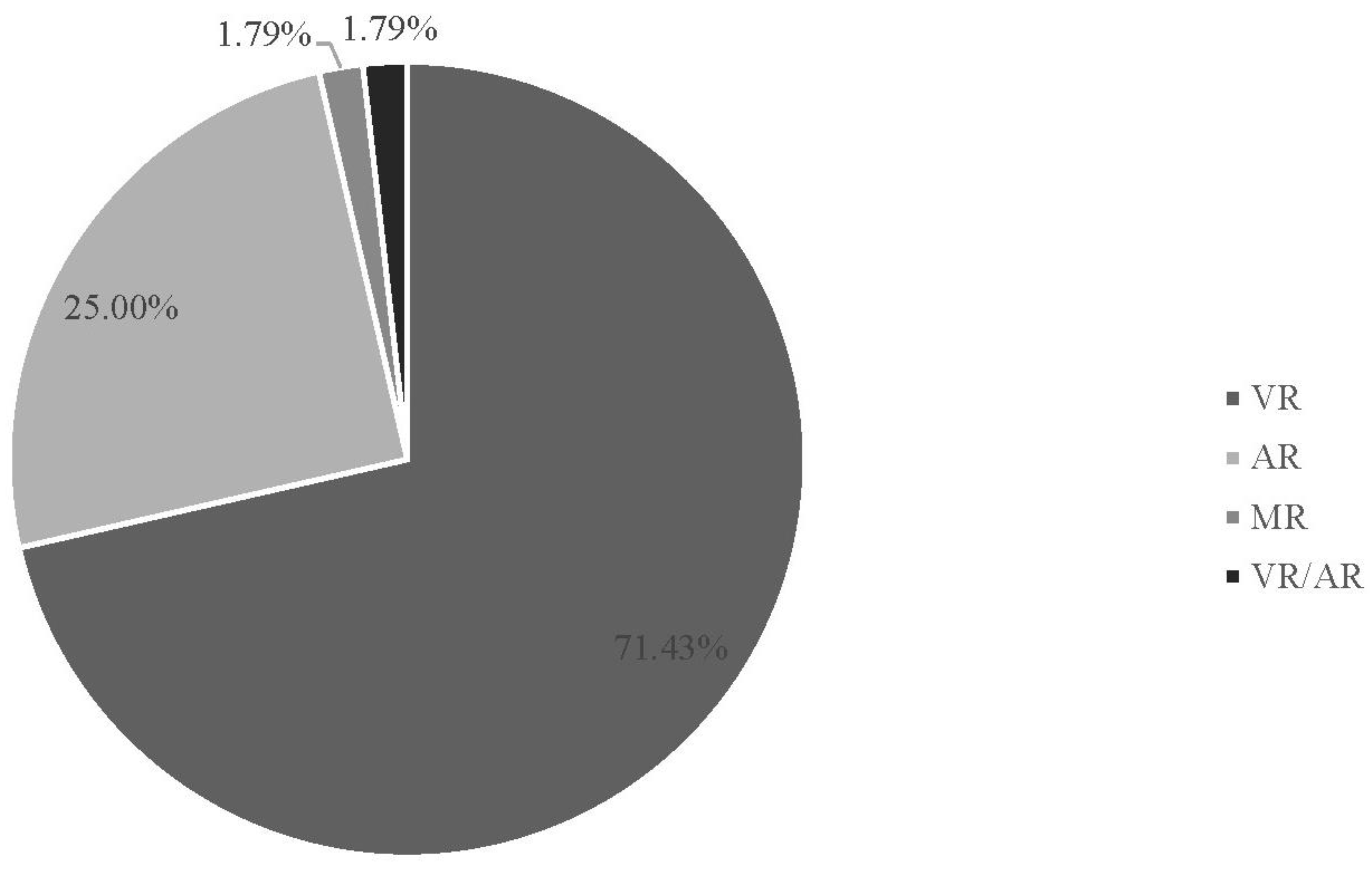
Figure 4.
Percentage of Studies by Year.
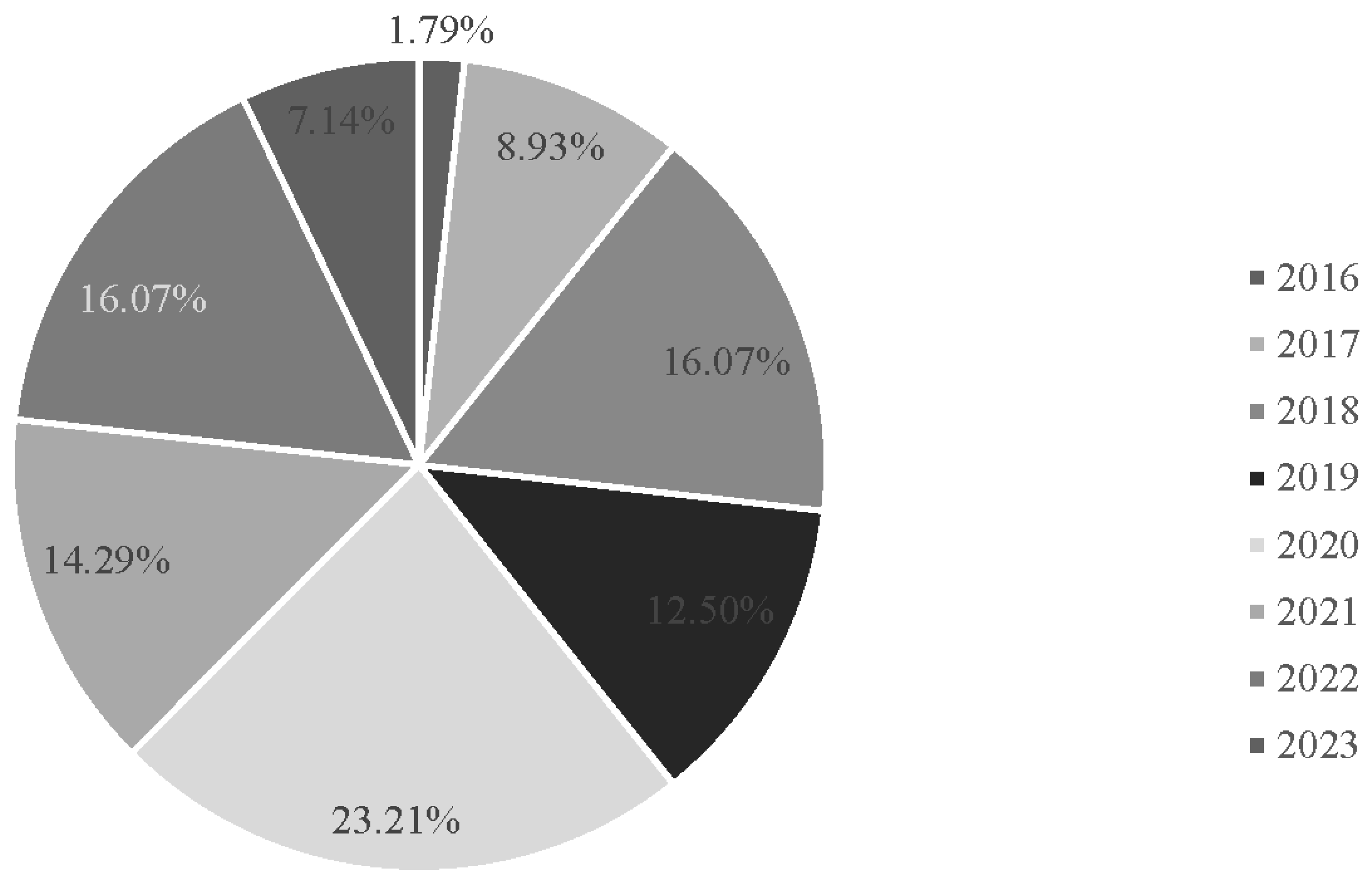
Figure 5.
Percentage of Student Type Reviewed.
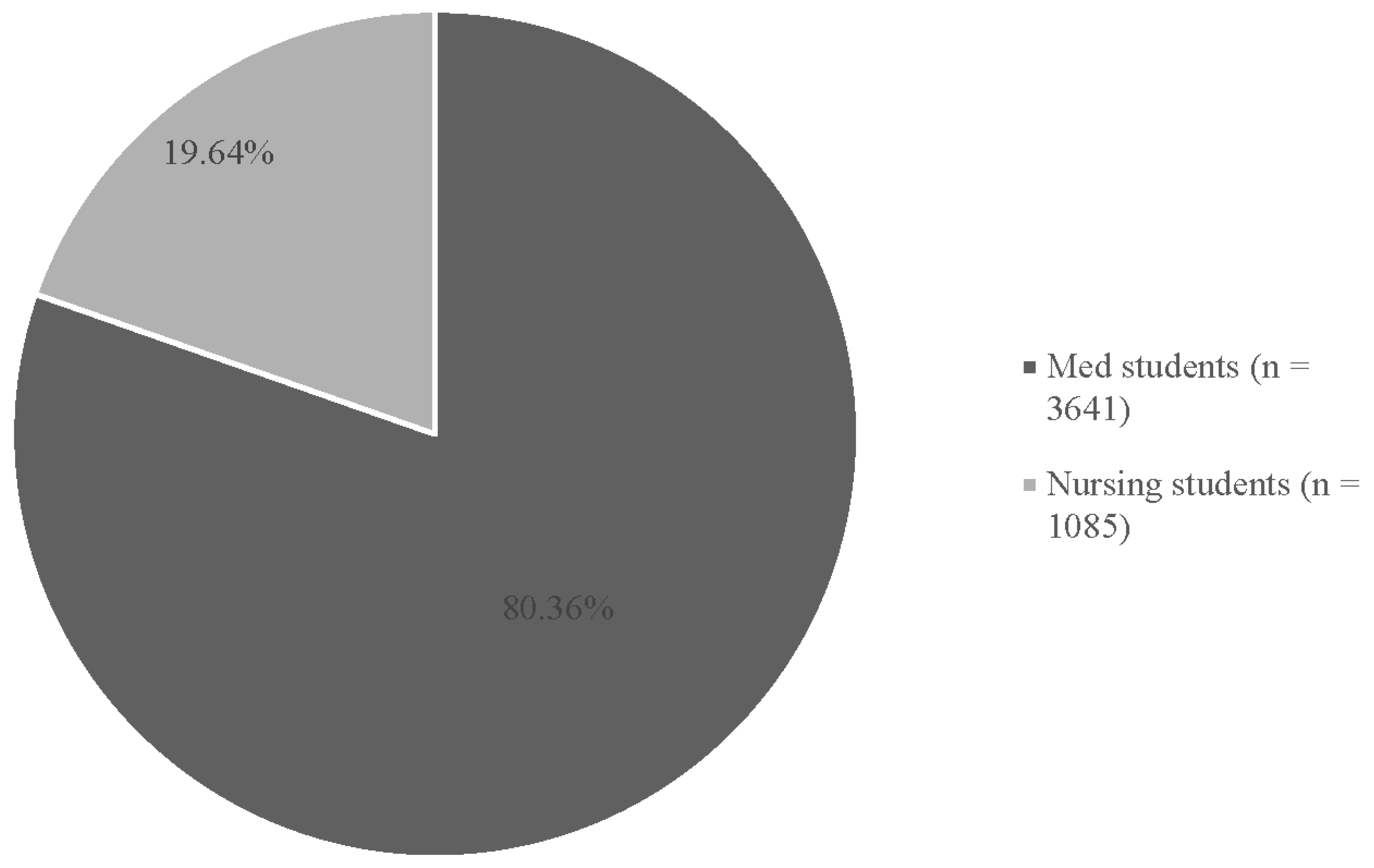
Figure 6.
Percentage of Types of Control Groups (n = 62 Control group across 56 Studies).
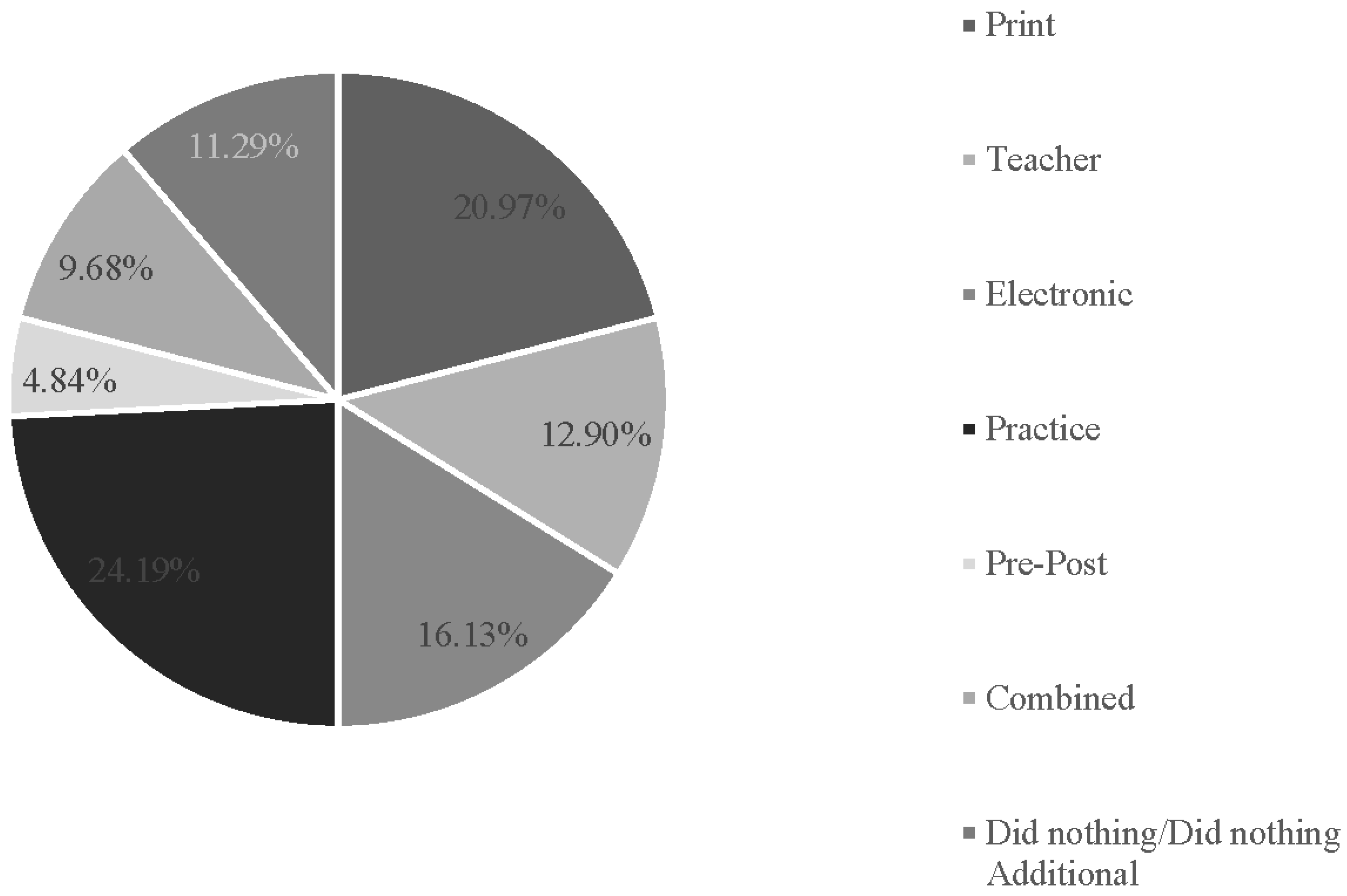
Figure 7.
Percentage of Outcomes (115 over 56 Studies).
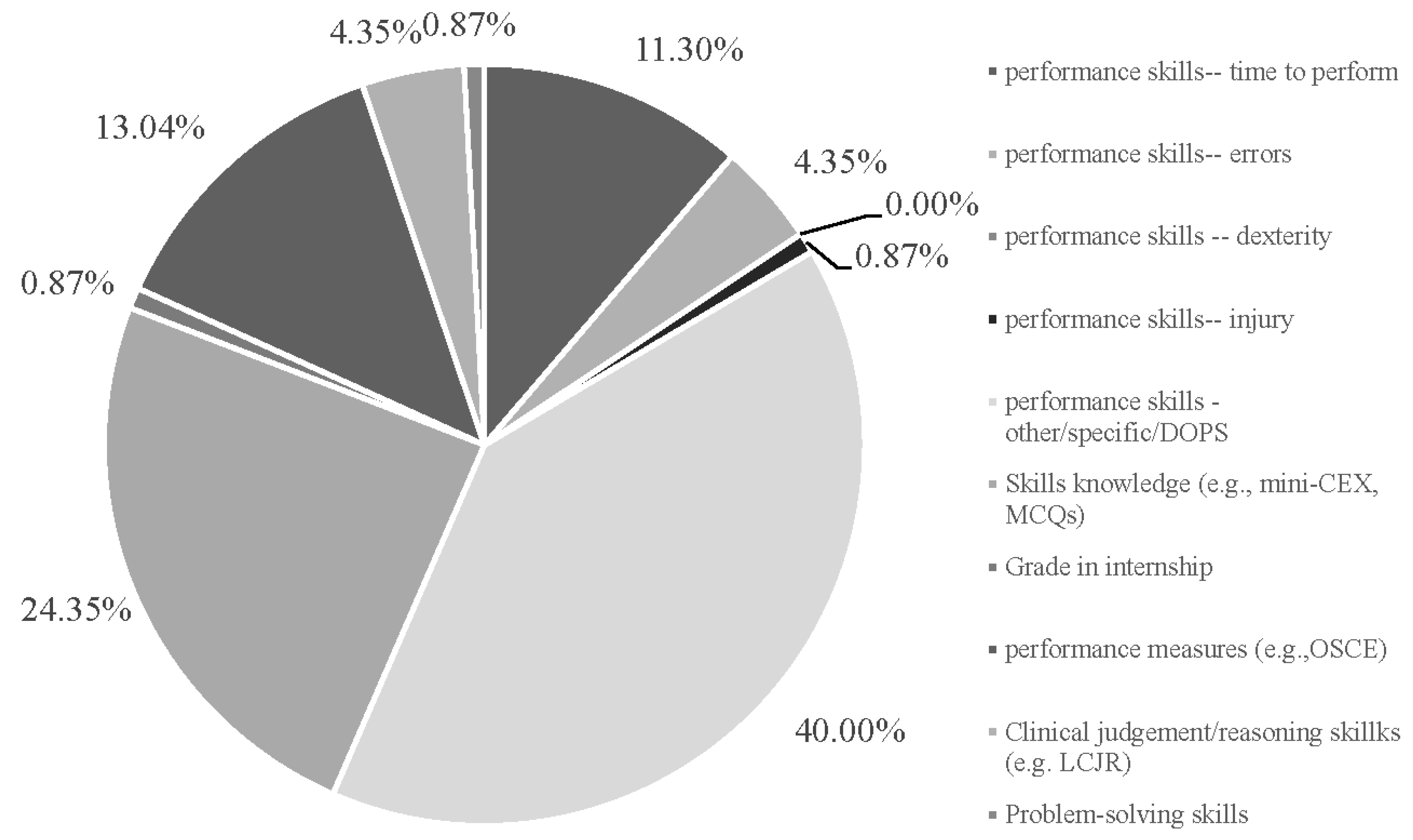
Figure 8.
Percentage of VR/AR/MR Studies by Outcome Success of Clinical Skills.
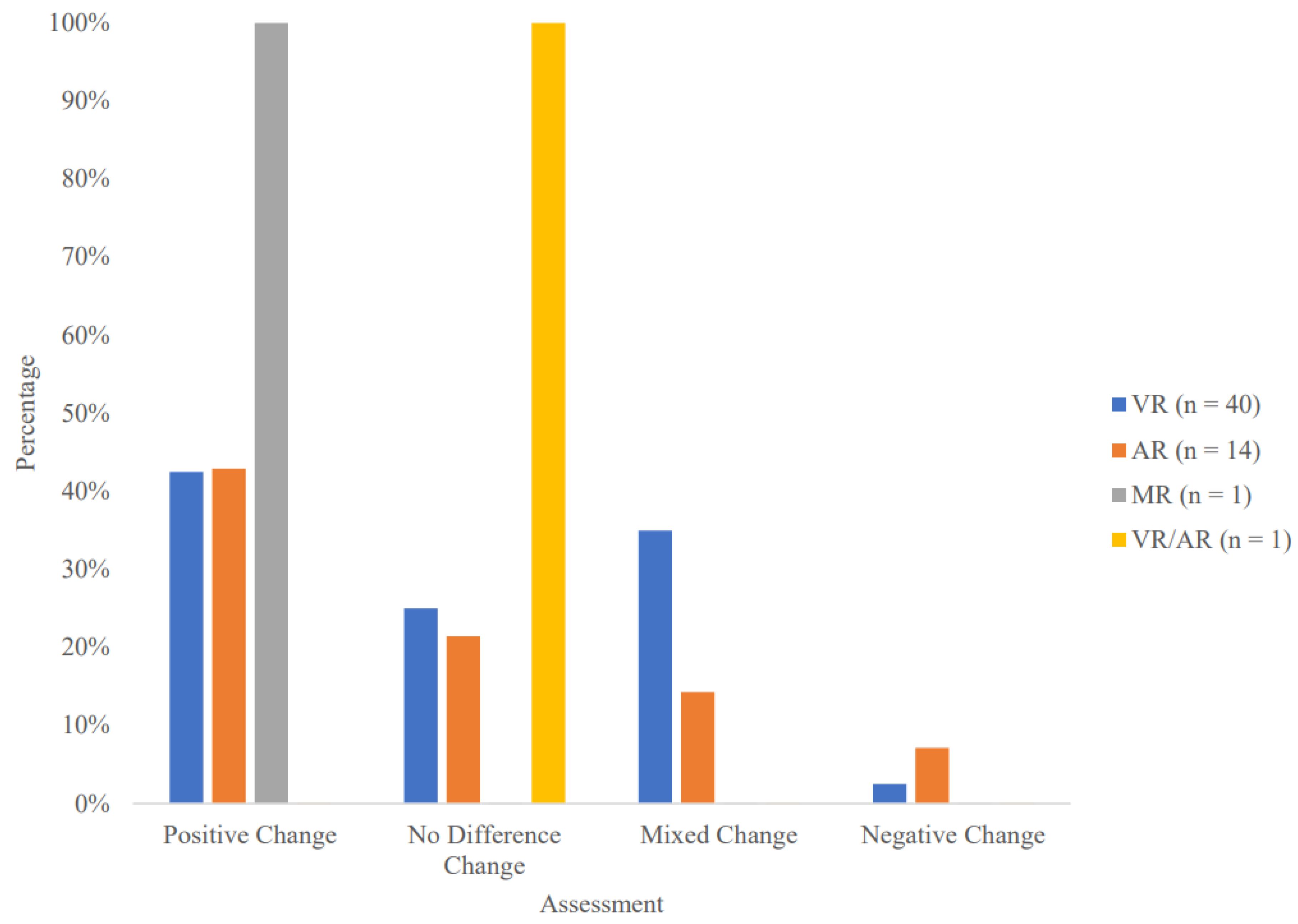

Table 1.
Empirical Articles (56) Included in the Systematic Review.
| Authors | Date | Type of I- XR | Population studied/ Setting | Number of participants | Control Group | Basic Experimental design/ Description | Results | DVs | Outcome Evidence for I-XR | Study Evidence for I-XR |
|---|---|---|---|---|---|---|---|---|---|---|
| Aebersold et al | 2018 | AR | nursing - tube placement | 69 nursing students | 1 (Combined) | Nursing students were tested on their ability to place a nasogastric tube. They were randomly assigned to either usual training (which included both video and didactic content) or an iPad anatomy-augmented virtual simulation training module. | The AR group was able to more accurately and successfully place the NGT, p = 0.011. CONTROL: n = 34, M = 15.39 (SD = 1.01). EXPERIMENAL: n = 35) , M = 15.96 (SD = 0.75). |
1 (performance skills - specific) | + Performance skills | Positive |
| Andersen et al. | 2021 | VR + Electronic* | Medical - catheter placement | 19 medical students | 1 (Did nothing additional) | Students were split into two different training groups: immersive virtual reality versus the control group. Both groups viewed videos showing ultrasound-guided peripheral venous cannulation placement. The control group was given no further training. | The immersive VR group was significantly more successful at peripheral venous cannulation placement in comparison to the control group, p ≤ 0.001. CONTROL: n = 9, M = 22.2% placement [0.11, 0.41]. EXPERIMENTAL: n = 10, M = 73.3% placement [0.56, 0.86] . |
1 (performance skills - specific) | + Performance skills | Positive |
| Andersen et al. | 2022 | VR | medical - Ultrasound skills | 104 medical students | 1 (Teacher) | Medical students were divided into two groups to learn Point-of-care ultrasound (POCUS) skills: a self-directed immersive virtual reality (IVR) group versus an instructor-led learning group. US skills were then assessed according to an OSAUS test. | There were no significant differences between the self-directed IVR and instructor-led groups in terms of OSAUS scoring or any other subgroup objectives. Overall effect, p = 0.36. EXPERIMENTAL: n = 51, M = 10.3 [9.0, 11.5]. CONTROL: n = 53, M = 11.0 [9.8, 12.2]. |
1 (performance measures - OSCE) | X No difference performance measures | No Difference |
| Arents et al | 2021 | VR | medical - Obstetrics training | 89 medical students | 1 (Print) | Two weeks prior to medical students' OB/Gyn internship, students underwent teaching on gentle Caesarean Sections (gash) and general obstetric knowledge. Students were divided into either a control group that underwent conventional study, or an experimental group who watched 360-degree videos using VR. After the internship, the authors analyzed the grade received for the internship, as well as administered both open-ended and multiple-choice question tests. | No significant difference in internship grade between groups, p = .66 (adjusted 0.68). EXPERIMENTAL: n = 53, M = 7.75 CONTROL: n = 48, M = 7.83 Mean difference CI [-0.33, 0.16]. No significant difference on multiple-choice testing (skills knowledge) between the groups, p = 0.91 (adjusted 0.68). EXPERIMENTAL: n = 53, M = 6.63. CONTROL: n = 48, M = 6.67 Mean difference CI [-0.61, 0.55]. |
2 (Grade internship) (Skills knowledge based on MCQs) | X No difference Grade internship X No difference Skills knowledge |
No Difference |
| Azimi et al. | 2018 | AR | nursing - IV placement & Chest compression | 20 nursing students | 1 (Practice) | Students underwent either standard training or training with AR via a head-mounted display for learning needle chest decompression and IV-line placement skills. The students’ skills were measured with a post-assessment both immediately after training and 3 weeks later. | Results are assessed with respect to control immediately after. The AR head-mounted group displayed better needle chest decompression skills. No p value or M, SD reported. No significant difference in IV placement performance was found between groups. No p value or M or SD reported. EXPERIMENTAL: n = 10 CONTROL: n = 10 |
2 (performance skills - specific chest) (performance skills- other IV) | + Performance skills X No difference performance skills |
Mixed Positive |
| Banaszek et al. | 2017 | VR | Medical - surgery | 40 medical students | 2 (Practice) (Did nothing) | Medical students underwent five weeks of independent training sessions in one of three groups: a high-fidelity virtual reality arthroscopic simulator, a bench-top arthroscopic simulator, or an untrained group (control). To measure post-test skill acquisition, students performed a diagnostic arthroscopy on both simulators and were tested in a simulated intraoperative environment using a cadaveric knee. A more difficult surprise skills transfer test was also administered. Students were evaluated using the Global Rating Scale (GRS) and a timer to determine efficiency. | Results are not reported for cross-over group post training. Both the high-fidelity VR simulator and bench-top arthroscopic simulator groups showed significant improvement in arthroscopic skills compared to the control, p < 0.05 for both. The VR simulation group showed the greatest improvement in performance in the diagnostic arthroscopy crossover tests using the GRS), p < 0.001. CONTROL: n = not reported, MD = 0.75 (SD only reflected in error bars). EXPERIMENTAL VR: n = not reported, MD = 12.6 (SD only reflected in error bars). VR group showed the fastest improvement simulated cadaveric setup with timer, p < .001. CONTROL: n = not reported, MD = 9.1 (SD only reflected in error bars). EXPERIMENTAL VR: n = not reported, MD = 17.3 (SD only reflected in error bars). |
2 (performance measures GRS) (performance skills -time) | + Performance measures + Performance skills |
Positive |
| Bayram & Caliskan | 2019 | VR | nursing -tracheostomy care | 172 nursing students | 1 (Combined) | Nursing students were divided into control and VR groups for tracheostomy care and skill knowledge. Both groups completed a theoretical class, labs, and small group study. The experimental group was provided a game-based virtual reality phone application. Skills knowledge was assessed using the FEMA IS-346 exam, and performance skills were assessed using the Decontamination Checklist for performance. | Results for the less immersive VR are not reported. Only the immersive experimental group is compared to the control group. Both groups increased their skills performance after training, but did not differ from one another, p = 0.443. CONTROL: n = 58, M = 13.48 (SD = 0.30). EXPERIMENTAL: n = 59, M = 14.24 (SD = 0.29). Both groups increased their skills knowledge after training, but did not differ from one another, p = 1.00. CONTROL: n = 58, M = 16.07 (SD = 0.30). EXPERIMENTAL: n = 59, M = 16.25 (SD = 0.29). |
2 (performance skills - specific suctioning) (skills knowledge) | X No difference performance skills X No difference skills knowledge |
No Difference |
| Blumstein et al | 2020 | VR | medical - surgery | 20 medical students | 1 (Print) | Medical students were randomized into either standard guide (SG) or virtual reality (VR) learning groups to learn intramedullary nailing (IMN) of the tibia. Students then performed a simulated tibia IMN procedure immediately following their training and were evaluated by an attending surgeon using a procedure-specific checklist and 5-point global assessment scale. Students returned 2 weeks later for repeat training and testing. | The VR groups showed significantly higher global assessment scores, p < 0.001. CONTROL: n = 10, M = 7.5, SD = not reported. EXPERIMENTAL: n = 10, M = 17.5, SD = not reported. The VR also completed a higher percentage of steps correctly according to the procedure-specific checklist, p < 0.002. CONTROL: n = 10, M =25 , SD = not reported. EXPERIMENTAL: n = 10, M = 63, SD = not reported. |
2 (performance skills - specific) (performance measures) | + Performance skills + Performance measures |
Positive |
| Bogomolova et al | 2020 | AR | BIO medical students -anatomy | 58 (bio)medical students | 2 (Print) (Practice) | Students were divided into three groups: (1) stereoscopic 3D Augmented-Reality (AR) group, (2) monoscopic 3D desktop model group, or (3) 2D anatomical atlas group. Students were told what the learning goals consisted of and were given instructions for the session. Visual-spatial abilities were measured before the learning session began. Post-session learning was measured using a 30-question knowledge test that tested factual, functional, and spatial organization of anatomical structures. | All groups performed equally well on the knowledge test, p = 1.00. Results are between the AR and atlas control. CONTROL: n = 18, M = 50.9 (SD = 13.8). EXPERIMENTAL: n = 20, M = 47.8 (SD = 9.8). |
1 (skills knowledge) | X No difference skills knowledge | No Difference |
| Bork et al. | 2019 | AR | medical - anatomy | 749 medical students | 2 (Print) (Practice) | Medical students were divided into one of three groups: (1) the control group using radiology atlases, (2) a virtual dissection table, or (3) AR Magic Mirror. A pre and post-test was taken about anatomy questions. | Pre-post not evaluated for final assessment. Both the AR Magic Mirror group and the Theory (control) group showed significantly increased post-test scores but did not differ from one another. No p value for comparison between change in improvement given. Results are from the post scores between the AR and the theory from print control group. CONTROL: n = 24, M = 50.60, (SD = 12.53). EXPERIMENTAL: n = 24, M = 48.00 (SD = 13.07). |
1 (skills knowledge) | X No difference skills knowledge | No Difference |
| Brinkmann et al. | 2017 | VR | med medical - surgery | 36 medical students | 1 (Practice) | Medical students underwent a 5-day laparoscopic basic skills training course using either a box-trainer or virtual reality (VR) training curriculum. Skills were measured by students' performance of an ex-situ laparoscopic cholecystectomy on a pig liver using RT and errors. The performance was evaluated by the Global Operative Assessment of Laparoscopic Skills (GOALS) score. | Both groups showed significant improvement in their acquisition of laparoscopic basic skills, and the two groups did not differ in improvement on the peg transfer, p = 0.311. CONTROL: n = 18, M = 53 (SD = 21.3). EXPERIMENTAL: n = 18 , M = 44.4 (SD = 14.9). The two groups also did not differ on their pattern cutting, p = 0.088. CONTROL: n = 18, M = 31.6 (SD = 17.3). EXPERIMENTAL: n = 18 , M = 42.6 (SD = 16.9). The two groups did not differ on loop placement, p = 0.174. CONTROL: n = 18, M = 46.3 (SD = 54). EXPERIMENTAL: n = 18 , M = 53.1 (SD = 32.5). The two groups did not differ on their knot tying, p = 0.174. CONTROL: n = 18, M = 37.2 (SD = 11.9). EXPERIMENTAL: n = 18, M = 42.6 (SD = 16.4). The GOALS scores on four of the five items were significantly higher in the box-trained group compared to the VR-trained group (individual comparisons in Table 5 of original publication). |
5 (performance skills – other peg) (performance skills – other cutting) (performance skills - other loop) (performance skills – other knot) (performance measures- GOALS) |
X No difference performance skills X No difference performance skills X No difference performance skills X No difference performance skills - Performance measures |
Mixed Negative |
| Bube et al. | 2020 | VR | medical- cystoscopy | 32 medical students | 1 (Teacher) | Two groups of medical students completed endoscopic procedure training. The control group underwent traditional lecture-based training whereas the experimental group used VR and other self-directed simulation training methods. Three weeks after the training, participants performed cystoscopies on two patients, and performance was measured using a global rating scale (GRS). | No significant difference in performance between the two groups was found after training, p = 0.63. CONTROL: n = 12, M = 14.3. EXPERIMENTAL: n = 13, M = 13.6. CI of the difference only reported: [-2.4, 3.9]. |
1 (performance measures - GRS) | X No difference performance measures | No Difference |
| Butt et al. | 2018 | VR | nursing - catheter | 20 nursing students | 1 (Combined) | Nursing students were assigned to either a control group (traditional learning with a task trainer) or an experimental group (VR software/game) to learn catheter insertion skills. Skills were assessed approximately two weeks after completion of the training session. | VR group completed more procedures than traditional group, p < 0.001. CONTROL: n = 10, M = 1.8 (SD = 0.42). EXPERIMENTAL: n = 10, M = 3.0 (SD = 1.3). Pass rates at two weeks were identical, no p value given. |
2 (performance skills – other number of procedures completed) (performance skills – other specific pass rates) | + Performance skills X No difference performance skills |
Mixed Positive |
| Cevallos et al. | 2022 | VR | medical - surgery | 20 medical students and orthopedic residents | 1 (Combined) | Medical students and orthopedic residents were randomized into either standard guide (SG) or virtual reality (VR) learning groups to learn pinning of a slipped capital femoral epiphysis (SCFE), a pediatric orthopedic surgery procedure. All participants watched a technique video, and the VR group completed additional training on the Osso VR surgical trainer. Participants then were asked to achieve "ideal placement," and performed a SCFE guidewire placement on Sawbones model 1161. Evaluation was based on time, number of pins "in-and-outs", articular surface penetration, angle between the pin and physis, distance from pin tip to subchondral bone, and distance from center-center point of the epiphysis. | The VR group showed superiority across multiple domains but where not statistically different from the control in the following: time to final pine placement, p = 0.26. CONTROL: n = 10, M = 706 (SD shown in figure). EXPERIMENTAL: n = 10, M = 573 (SD shown in figure). VR performed better compared to control for pin in and out p = 0.28. CONTROL: n = 10, M = 1.7 (SD shown in figure). EXPERIMENTAL: n = 10, M = 0.5 (SD shown in figure). VR group performed fewer surface penetrations, p = 0.36. CONTROL: n = 10, M = 0.4 (SD shown in figure). EXPERIMENTAL: n = 10, M = 0.2 (SD shown in figure). VR group had smaller distance pin to tip to subchondral bone, p = 0.42. CONTROL: n = 10, M = 5.8 (SD = 3.36). EXPERIMENTAL: n = 10, M = 7.2 (SD = 6.5). VR group had lower angle deviation between the pin and physis, p < 0.05. CONTROL: n = 10, M = 4.9 (SD = 3.0). EXPERIMENTAL: n = 10, M = 2.5 (SD = 1.42). |
5 (performance skills - time) (performance skills – other specific pin in and outs) (performance skills - errors) (performance skills – other specific pin tip to bone) (performance skills – other specific angle) |
X No difference performance skills X No differenceperformance skills X No difference performance skills X No difference performance skills + Performance skills |
Mixed Positive |
| Chao et al | 2021 | VR | nursing - tube placement | 45 nursing students | 1 (Electronic) | Nursing students were randomly assigned into two groups to learn nasogastric (NG) tube feeding: (1) immersive 3D interactive video program group or (2) regular demonstration video. Students completed a pre- and post-intervention questionnaire, which included a nasogastric tube feeding quiz (NGFQ) to study NG tube feeding knowledge. Students were assessed after intervention and 1 mo. Later. | Knowledge scores on NG tube feeding improved significantly in both groups; however, there was no significant difference in the knowledge scores after treatment, p = 0.77 CONTROL: n = 23, M = 11.7 (SD =1.86). EXPERIMENTAL: n = 22, M = 11.9 (SD = 2.04). |
1 (skills knowledge) | X No difference skill knowledge | No Difference |
| Chao et al | 2022 | VR | Medical - intake skills | 64 medical students | 1 (Electronic) | Students were randomized into two groups and received either a 10-minute immersive 360-degree virtual reality or a 2D virtual reality instructional video on history taking and physical examination skills. Within 60 minutes of watching the video, students performed a focused history and physical on a patient. The Direct Observation of Procedural Skills (DOPS) was used to measure physical exam skills, and the Mini-CEX was used to measure general history and physical exam skills. | The average DOPS-total score was significantly higher in the VR video group compared to the 2D video group, p = .01. CONTROL: n = 32, M = 85.8 (SD = 3.2). EXPERIMENTAL: n = 32, M = 88.4 (SD = 4.0). No significant differences in the average Mini-CEX scores were found between the groups, p = 0.75. CONTROL: n = 32, M = 39.8 (SD = 5.2). EXPERIMENTAL: n = 32, M = 40.1 (SD = 4.1). |
2 (performance skills - other/DOPS) (skills knowledge - mini-CEX) | + Performance skills X No difference skills knowledge |
Mixed Positive |
| Chen & Liou | 2023 | AR | Nursing students – first aid | 95 nursing students | 1) Practice | Nursing students were divided into two groups for pediatric first-aid training. The control group performed simulation using a traditional Resusci Annie whereas the experimental group used an interactive Resusci Anne that was overlaid AR. Pre and post tests were given to evaluate participant knowledge and skills. Knowledge was assessed using a 20-question test. Skill level was assessed using a graded evaluation checklist. |
The AR intervention group showed significantly higher post-test knowledge, p < 0.001. CONTROL: n = 49, M = 18.08, (SD =1.6). EXPERIMENTAL: n = 46, M = 18.78, (SD = 1.1). The AR group also showed improved skill in first aid level scoring compared to the control group post-test, p < 0.001. CONTROL: n = 49, M = 29.71, (SD = 1.5). EXPERIMENTAL: n = 46, M = 32.52, (SD = 1.3) . |
2 (skills knowledge) (performance measures – other specific first aid) |
+ Skills knowledge + Performance measures |
Positive |
| Ekstrand et al | 2018 | VR + Print* | medical - neuroanatomy | 64 medical students | 1 (did nothing additional) | Medical students were assigned into either a control group who underwent paper-based neuroanatomy learning, or an experimental group who underwent neuroanatomy learning with VR. Pre and post-intervention tests were given, including a post-test immediately after the study completion and one 5-9 days later. | Both groups showed significant improvement between pre- and post-test scores, but no significant differences on the neuroanatomy test between the groups on either of the post-test results, p = 0.5. Means and SDs are not reported: T-statistic reported for control (n = 33) vs. VR (n = 31) post-training, t(62)= -0.38. | 1 (skills knowledge) | X No difference skills knowledge | No Difference |
| Fu et al | 2020 | VR | medical - suturing | 14 medical students | 1 (Practice) | Students were assigned to one of two training groups: (1) the VBLaST-SS (virtual simulator) training group or (2) the FLS training group. Students then watched a video that taught the intracorporal suturing task they were going to be practicing. Students then performed the task on both systems to measure baseline performance. Students then practiced once a day, five days a week, for three weeks. Performance scoring was based on the original FLS scoring system. | Both training modalities showed significant performance improvement, but there were no significant differences in the group x time interaction, p = 0.20. Learning curves for both learning modalities were also similar. Means and SD only shown in figure. | 1 (performance skills – specific FLS) | X No difference performance skills | No Difference |
| Haerling et al. | 2018 | VR | Nursing - case evaluation for COPD | 81 nursing students | 1 (Practice) | This study placed students in two groups, those using mannequin-based simulations and those using VR simulations. Participants completed a standardized patient encounter of a complex case involving a patient with COPD. Pre and post-intervention knowledge assessments were also performed using the LCJR and the C-SEI. | Students in both groups showed significant improvement in post-test knowledge assessment. Scores between the groups were not significantly different in the post-test knowledge assessment, p = 0.48. CONTROL: n = 14, M= 79.82 (SD = 17.63). EXPERIMENTAL: n = 14, M = 82.16 (SD = 11.76). There was no statistical difference post-intervention for either group for the LCJR, p = 0.374. CONTROL: n = 14, M = 82.69 (SD = 13.65). EXPERIMENTAL: n= 14, M = 78.18 (SD = 12.71). There was also no statistical difference post-intervention on the C-SEI between groups. CONTROL: n = 14, M = 84.62 (SD = 14.91). EXPERIMENTAL: n = 14, M = 81.93 (SD = 16.41). |
3 (skills knowledge) (clinical reasoning – LCJR) (clinical reasoning – C-SEI) |
X No difference skills knowledge X No difference clinical reasoning X No difference clinical reasoning |
No Difference |
| Han et al. | 2021 | VR + SP | medical - neurological | 95 medical students | 1 (did nothing additional) | Medical students were divided into two groups: a standardized patient (SP) group that was provided neurological findings using conventional methods (verbal description, pictures, videos) versus a SP with Virtual Reality-based Neurological Examination Teaching Tool (VRNET) group. A researcher measured student performance using the Neurologic Physical Exam (NPE) score. | The SP + VR group had significantly higher NPE scores compared to the SP group, p = 0.043. CONTROL: n = 39, M = 3.40 (SD = 1.01). EXPERIMENTAL n = 59, M = 3.81 (SD = 0.92). |
1 (skills knowledge - NPE score) | + Skills knowledge | Positive |
| Henssen et al. | 2019 | AR | medical & Biomedical- neuroanatomy | 31 medical and biomedical students | 1 (Print) | Students were assigned to one of two groups for learning neuroanatomy. The control group underwent learning with cross-sections of the brain whereas the experimental group underwent AR learning. | Results are assessed with respect to control. The control group showed improved post-test scoring compared to the AR, p = 0.035. Results for adapted test scores after training are reported next. CONTROL: n = 16, M =60.6 (SD = 12.4). EXPERIMENTAL: n = 15, M = 50.0 (SD = 10.2). |
1 (skills knowledge) | - Skills knowledge | Negative |
| Hu et al. | 2020 | VR + workshop in ultrasound* | medical - Ultrasound skills | 101 medical students | 1 (Print) | Medical students took place in an ultrasonography (US) training program. They were divided into either the virtual reality (VR) intervention group, or the control group. Both groups participated in an ultrasound workshop; however, the intervention group used a self-directed VR-enhanced anatomy review and used VR to complete additional review sessions during the US hands-on practice. After the US workshop was completed, participant competency was measured using a standardized practical US test, which focused on the identification of various anatomical structures, and a 10-Q MCQ on anatomy. | Participants in the intervention group showed significantly higher scores on US task performance overall, p < 0.01. Results below are for mean rank. No variability given. CONTROL: n = 54, MR = 38.52. EXPERIMENTAL: n = 47, MR = 65.34. The VR group also showed significantly better scores on the knowledge test, p < .05. CONTROL: n = 54, median = 2 (IQR = 3). EXPERIMENTAL: n = 47, Median = 3 (IQR = 3). |
2 (skills knowledge) (performance skills - other practical US) |
+ Skills knowledge + Performance skills |
Positive |
| Issleib et al. | 2021 | VR | medical - CPR | 160 medical students | 1 (Practice) | Medical students were randomized into an intervention or control group. The intervention group completed a the BLS course in virtual reality, whereas the control group underwent standard BLS training. At the end of training, all students performed a 3-minute practical test using the Leardal Mannequin to record no flow time on the task. | The control group had significantly shorter no flow time compared to the VR, p < 0.0001. CONTROL: n = 104, M = 82.03 (SD = not reported). EXPERIMENTAL: n = 56, M = 92.96 (SD = not reported). |
1 (performance skills - specific no flow time) | - Performance skills |
Negative |
| Jaskiewicz et al. | 2020 | VR + Practice* | medical - CPR | 91 medical students | 1 (Teacher) | Both the control and experimental groups completed a 3-hour BLS course including background training and practice on a CPR mannequin. Students then participated in either a tadeonal teaching or VR scenario where hands-only CPR was completed. The quality of the chest compressions (rate and depth) was then tested and analyzed. | There were no significant differences in chest rate compression performance between the control and virtual reality groups, p = 0.48. CONTROL: n = 45, Median = 114 (IQR 108-122). EXPERIMENTAL: n = 45, Median = 115 (IQR 108-122). There was also no significant difference on chest rate depth between groups, p > 0.05. CONTROL: n = 45, Median = 48 (IQR = 44-55). EXPERIMENAL: n = 45, Median = 49 (IQR = 43-53). Finally, there was a significant increase in the percentage of chest compression relaxation for the control group compared to the VR group, p < 0.01. CONTROL: n = 45, Median = 97 (IQR = 85-100). EXPERIMENTAL: n = 45, Median = 69 (IQR = 26-98). |
3 (performance skills - specific rate) (performance skills - specific depth) (performance skills – specific relaxation) |
X No difference performance skills X No difference performance skills -Performance skills |
Mixed Negative |
| Jung & Park | 2022 | VR | Nursing students – chemport insertion surgery | 60 nursing students | 1 (Print) | Nursing students were divided into two groups to learn chemoport insertion surgery. The control group's learning consisted of instruction by an operating nursing instructor, learning via a handout, and time for self-study. The experimental group used VR. Pre and post-test knowledge was assessed using a 10-point questionnaire about key knowledge of insertion. |
The VR group showed significantly higher post-test knowledge scores compared to the control group after training, p = 0.001. CONTROL: n = 30, M = 4.80 (SD = 1.65). EXPERIMETNAL: n = 30, M = 6.97 (SD = 1.35). |
1 (skills knowledge) | + Skills knowledge | Positive |
| Kane et al. | 2022 | VR | med students- obstetrics | 69 medical students | 1 (Electronic) | Medical students were placed into one of two groups to help them learn and conceptualize fetal lie and presentation. The interventional group was immersed in a virtual reality learning environment (VRLE) to explore fetal lie, and the control group used traditional 2D images. After their sessions, clinical exam skills were tested using an obstetric abdominal model. Knowledge was assessed by students' ability to determine fetal lie and presentation on this model. Time taken to complete the test was also measured. | No significant differences were found between the two groups in terms of knowledge assessment, although the authors note that there was a noticeable trend of higher success rates in the intervention group in the VR group compared to the control group) for combined lie and presentation scores, p = not reported. CONTROL: n =34, M = 70.0 (SD = not reported). EXPERIMENTAL : n = 33), M = 56% (SD = not reported). However, time to complete the task was significantly less in the intervention group compared to the control group, p = 0.012. CONTROL: n = 34, M = 38 (SD = 10.83). EXPERIMENTAL: n = 33, M = 45 (SD = 12.95). |
2 (performance skills - time) (performance skills -specific success) | X No Difference performance skills + Positive performance skills |
Mixed Positive |
| Kowalewski et al | 2019 | VR | medical - surgery | 100 medical students | 1 (Did nothing) | Medical students were divided into three groups to complete laparoscopic training: (1) the control group, which received no training, (2) the "alone" group, and (3) the dyad group. Intervention groups completed box and VR training, after which performance was measured with a cadaveric porcine laparoscopic cholecystectomy (LC), and the objective structured assessment of technical skills (OSATS) was used. Global operative assessment of laparoscopic skills (GOALS), time to completed LC, and VR performances were also measured. | Results are reported for improvement between the VR and control group only. The VR group and the control group did not differ on the OSATS, p = 0.548. CONTROL: n = 20, M = 37.1 (SD = 7.4). EXPERIMENTAL: n = 40, M = 40.2 (SD = 9.8). The two groups did not differ on the GOALS either, p = 0.998. CONTROL: n = 20, M = 10.1 (SD = 3.0). EXPERIMENTAL: n = 40, M = 10.6 (SD = 3.0). The VR groups were faster than the control group in completion time, p < 0.001. CONTROL: n = 20, M = 13.5 [11.8, 17.5]. EXPERIMENTAL: n = 40, M = 10.2 [7.9, 11.3]. The VR group also had fewer movements, p = 0.002. CONTROL: n = 20, M = 871 [637, 1105]. EXPERIMENTAL: n = 40, M = 683 [468, 898]. The VR group also had a shorter path length, p = 0.004. CONTROL: n = 20, M = 1640 [1174, 2106]. EXPERIMENTAL: n = 40, M = 1316 [948, 1684]. |
5 (performance measures -OSATS) (performance measures - GOALS) (performance skills - time) (performance skills- other specific path) (performance skills- other specific length) | X No difference performance measures X No difference performance measures + Performance skills + Performance skills + Performance skills |
Mixed Positive |
| Küçük et al | 2016 | AR | medical -anatomy | 70 medical students | 1 (Print) | Medical students were placed into a control group, which used traditional teaching methods (textbook) or an experimental group, which used mobile augmented reality (mAR) technology (MagicBook) to learn neuroanatomy. Post-intervention knowledge was measured using an Academic Achievement Test (AAT), a 30-question multiple-choice test. | The experimental mAR group showed significantly superior performance on the AAT test, p < 0.05. CONTROL: n = 34, M = 68.34 (SD = 12.83). EXPERIMENTAL: n = 36, M = 78.14 (SD = 16.19). |
1 (performance measures - AAT) | + Performance measures | Positive |
| Lau et al | 2023 | VR | Nursing students | 34 nursingstudents | 1) Nothing (pre-post) | Nursing students participated in pre-test and post-test knowledge questionnaires regarding both subcutaneous insulin injection and intravenous therapy. After completing the pre-test, participants underwent learning using immersive VR before completing the post-test questionnaire. | There was a significant improvement in knowledge test scores (IV and subcutaneous injection) after training, p = 0.075. Only z-scores were reported with ranks. No M or SDs are reported pre vs. post. |
1 (skills knowledge) | + Skills knowledge | Positive |
| Lemke et al | 2020 | AR | medical - suturing | 44 medical students | 2 (Teacher) (Combined) | Students were randomized into one of three intervention groups to learn suturing skills: (1) faculty-led, (2) peer tutor-led, or (3) holography-augmented intervention arms (Suture Tutor). Outcomes measured include: the number of simple interrupted sutures that were placed to achieve proficiency, the total number of full-length sutures used, and time to achieve proficiency. | Results are reported among three groups. No significant differences among the intervention groups in the number of full-length sutures used, p = .376. Means and SD are reported for Teacher control vs. AR CONTROL: N = 16, M = 80.0 (SD = 47.2). EXPERIMENTAL: n = 14, M = 107.4 (SD = 61.3). No significant differences among the intervention groups in the number of simple interrupted sutures placed, p = 0.735. CONTROL: n = 16, M = 9.3 (SD = 5.3). EXPERIMETNAL: n = 14, M = 11.0 (SD = 6.0). No significant differences among the intervention groups in the time to achieve proficiency, p = 0.390. CONTROL: n = 16, M = 158.1 (SD = 89.2). EXPERIMETNAL: n = 14, M = 205.0 (SD = 113.2). |
3 (performance skills – other specific # placed) (performance skills – other specific interruptions) (performance skills – other specific # used) |
X No difference performance skills X No difference performance skills X No difference performance skills |
No Difference |
| Logishetty et al. | 2019 | AR | Medical - surgery | 24 medical students | 1 (Practice) | This study simulated total hip arthroplasty (THA) and placed students in one of two groups to determine what training is more effective at improving the accuracy of acetabular component positioning: (1) augmented reality (AR) training (with live holographic orientation feedback) or (2) hands-on training with a hip arthroplasty surgeon. Students participated in one baseline assessment, training session, and reassessment a week for four weeks and were recorded on the target angle (inclination – anteversion). | AR intervention group showed smaller average errors than the control practice with surgeon group after training, p < 0.0001. CONTROL: n = 12, M = 6 (SD = 4). EXPERIMENTAL: n = 12, M = 1 (SD = 1). In the final session, both groups showed improvement on the target angle, but there was no significant difference in performance between groups, p = 0.281. Means and SD are reported as differences from pre. CONTROL: n = 12 , MD = -8.4 [-7.0, -9.8]. EXPERIMENTAL: n = 12, MD = -7.8 [-5.5, -10.2]. |
2 (performance skills - errors) (performance skills – other specific target angle) | + Performance skills X No difference Performance skills |
Mixed Positive |
| Maresky et al. | 2018 | VR immersive + VR simulation* | medical - anatomy | 42 medical students | 1 (Print) | Before learning cardiac anatomy, medical students underwent a VR simulation of the subject. Students then were separated into either a control group that continued independent anatomy study, or an experimental group that underwent an immersive VR experience. Pre and post-test scores were obtained, which measured both conventional and visual-spatial (VS) cardiac anatomy questions. | Students in the immersive VR intervention group scored significantly higher overall after the intervention, p < 0.001. Mean differences between control (n = 14) and experimental group (n = 28) are only reported: MD = 24.8 (SD = 3.89). This included both subsections of VS and conventional content. |
1 (skills knowledge) | + Skills knowledge | Positive |
| Moll- Khosrawi et al. | 2022 | VR | medical - BLS | 88 medical students | 1 (Electronic) | Medical students were placed into one of two groups to compare a control group that received web-based basic life support (BLS) training to an intervention group that underwent additional individual virtual reality (VR) training. The quality of BLS skills was assessed after training with a no-flow-time indicator. Overall BLS performance was also assessed using an adapted observational checklist, graded by experts. | The VR intervention group showed significantly lower no-flow-time compared to the control, p = 0.009. CONTROL: n = 42, M = 11.05 (SD = 10.765). EXPERIMENTAL: n = 46, M = 6.46 (SD = 3.49). The VR group also showed significantly superior overall (lower penalty point) for their BLS performance in comparison to the control group, p < 0.001. CONTROL: n = 42, M = 29.19 (SD = 16.31). EXPERIMENTAL: n = 46, M = 13.75 (SD = 9.66). |
2 (performance skills – other specific flow time) (performance measures - checklist) | + Performance skills + Performance measures |
Positive |
| Moro et al | 2017 | AR /VR | medical- anatomy | 59 medical and health science students | 1 (Electronic) | Medical students completed a lesson on skull anatomy using one of three learning modalities: (1) virtual reality (VR), (2) augmented reality (AR), or (3) tablet-based (TB). After their 10-minute anatomy lesson using their respective learning modality, students completed a 20-question multiple-choice anatomy test to measure their knowledge. | No significant differences in the anatomy test scores were found between the three groups; AR and VR intervention did not show superior knowledge acquisition in comparison to table-based skull anatomy learning after intervention, p = 0.874. Means are for VR group and control group only. Standard deviations are depicted only in figure. CONTROL: n = 22, M = 61. EXPERIMETNAL: n = 20 , M = 59. |
1 (skills knowledge) | X No difference skills knowledge | No Difference |
| Nagayo et al | 2022 | AR | medical - surgery | 38 medical students | 1 (Electronic) | Medical students were randomized into one of two groups for self-training suturing learning: (1) the augmented reality (AR) training group or (2) the instructional video group. Both groups watched an instructional video on subcuticular interrupted suturing and took a pretest. They then practiced the suture 10 times using their assigned learning modality, before completing a post-test. Pre- and post-tests were performed on a skin pad and were graded using global rating and task-specific subscales. | Both groups showed significant improvement between pretest and posttest scores in both global rating and task-specific subscales on suturing performance; however, no significant difference in performance was found between the AR and instruction video training groups using the global rating, p = 0.38. CONTROL: n =19 , M = 15.11 (SD = 2.84). EXPERIMENTAL: n = 19, M 15.03 (SD = 1.94). |
1 (performance skills – other specific suturing performance) | + Performance skills | Positive |
| Neumann et al | 2019 | VR | medical - surgery | 51 medical students | 1 (Electronic) | Medical students were randomized into two groups for cystoscopy (UC) and transurethral bladder tumor resection (TURBT) training. The control group watched video tutorials by an expert. After completion of the training, students performed a VR-UC and VR-TURBT performance task and 12 measures of performance were recorded. | Both groups improved on three variables after training, including significantly lower average procedure length, lower resectoscope movement, and accidental bladder injury, but there was only one significant difference in the improved performances for the VR compared to the control (procedure time, p = 0.04). All Means and SD listed in Table 2. | 12 (performance skills – other specific x 9) (performance skills - injury) (performance skills - time x 2) | X No difference performance skills (for 11 of the 12 variables) + Performance skills |
No Difference |
| Nielsen et al. | 2021 | VR | medical - Ultrasound skills | 20 medical students | 1 (Electronic) | Medical students were randomized into either a virtual reality (VR) or e-learning group for ultrasound education and training. Performance was scored using the OSAUS. | The VR group showed significantly higher scoring on the OSAUS compared to the e-learning group after intervention, p ≤ 0.001. CONTROL: n = 9, M = 125.7 (SD = 16.2). EXPERIMENTAL: n = 11, M = 142.6 (SD = 11.8) . |
1 (performance measures - OSAUS) | + Performance measures | Positive |
| Noll et al | 2017 | AR | medical - dermatology | 44 medical students | 1 (Print) | Medical students were randomized into one of two groups for learning dermatological knowledge. Group A's training involved the use of a mobile Augmented Reality (mAR) application, whereas Group B's training involved textbook-based learning. Baseline and post-test knowledge were assessed using a 10-question single choice (SC) test, which was repeated after 14 days to assess longer-term retention. | The initial SC post-test showed significant knowledge gain in both groups, but the VR group showed a marginally significant memory for correct answers after two weeks, compared to the control group, p = 0.10. CONTROL: n = 22, M = 0.33 (SD = 1.62). EXPERIMENTAL: n = 22, M = 1.14 (SD = 1.30). |
1 (skills knowledge) | + (marginal) Skills knowledge | Positive |
| Orland et al. | 2020 | VR+ | Medical - surgery | 25 medical students | 1 (Print) | Medical students were randomized into one of three groups for learning intramedullary tibial nail insertion: (1) the technique guide only control group, (2) the virtual reality (VR) only group, or (3) the VR plus technique guide group. The experimental groups participated in three separate VR simulations, 3-4 days apart. After 10-14 days of preparation, students performed an intramedullary tibial nail insertion simulation into a bone-model tibia. Completion and accuracy were assessed. | Overall assessments are made with comparisons to both VR groups compared to control group. Both experimental groups that involved VR training showed higher completion rates, p = .01 Both groups also had fewer incorrect steps, p = .02, in comparison to the control group. Means and SD below are for VR+ and control group only. ERRORS CONTROL: n = 8, M = 5.7 (SD = 0.2). EXPERIMENTAL: n = 9, M = 3.1 (SD = 0.1). COMPLETION TIME CONTROL: n = 8, M = 24 (SD = 4). EXPERIMENTAL: n = 9, M = 18 (SD = 8). |
2 (performance skills - errors) (performance skills - time) | + Performance skills + Performance skills |
Positive |
| Plotzky et al. | 2023 | VR 'high' | Nursing students- endotracheal suctioning skills | 131 nursing students | 2 (low VR) + Electronic | Nursing students were split into one of three groups for learning of endotracheal suctioning skills. The control group's intervention was a video tutorial. The intervention groups consisted of a VR low group and a VR high group. The VR 'low' group's intervention consisted of basic VR technology, including head tracking and controller-based controls. The VR 'high' group's intervention consisted of more advanced VR technology, including head and hand tracking, allowing users to interact with their actual hands, and as well as supplementing with real-world video clips. Participants were assessed using a knowledge test and a skill demonstration test on a manikin using an objective structured clinical examination (OSCE). The knowledge test was given immediately after intervention and 3 weeks later. |
Each of three groups showed a significant increase in knowledge acquisition, however, there was no significant difference among them for skills knowledge, p = 0.730. Means and SDs are for the VR+ vs. control group after intervention. CONTROL: n = 43, M = 7.16 (SD = 2.29). EXPERIMENTAL: n =47, M= 7.06 (SD = 1.42). There was a significant difference among groups on the OSCE after intervention, p < 0.001. Means and SDs are for the VR+ vs. control group after intervention. CONTROL: n = 43, M = 11.95 (SD = 1.65). EXPERIMENTAL: n = 47, M= 9.41 (SD = 2.70). |
2 (skills knowledge) (performance measures –OSCE) | X No difference skills knowledge - Performance measures |
Mixed Negative |
| Price et al. | 2018 | VR | nursing - triage skills | 67 nursing students | 1 (Practice) | This study compared the use of VR to clinical simulation to determine the efficiency in executing the START (Simple Triage and Rapid Treatment) triage. | There were no significant differences between the VR and clinical simulation group in the percentage of victims that were correctly triaged, p = 0.612 CONTROL: n = 35, M = 88.3 (SD = 9.65). EXPERIMENTAL: n =32, M = 87.2 (SD = 7.2). |
1 (performance skills - specific triage variables) | + Performance skills | Positive |
| Ros et al. | 2020 | VR + Print | medical -surgery | 176 medical students | 1 (Did nothing additional) | All students were given a technical note detailing an external ventricular drainage (neurosurgical) technique. Students were randomized into two groups, one of which received no additional training, and one which used immersive virtual reality (VR) as supplemental teaching. Knowledge was assessed with a multiple-choice test immediately after training and six months after. | VR training showed significantly superior knowledge gain, after both initial assessment and at the six-month mark, p = 0.01. Means and SD are reported after the initial training. CONTROL: n = 88, M = 4.59, (SD = 1.4). EXPERIMENTAL: n = 85, M = 5.17 (SD = 1.29). |
1 (skills knowledge) | + Skills knowledge | Positive |
| Ros et al. | 2021 | VR | Medical- lumbar puncture | 89 medical students | 1 (Teacher) | Medical students were randomized into one of two groups to complete training in how to perform a lumbar puncture. The control group participated in traditional lecture learning whereas Group 2 participated in immersive VR 3D video filmed from first-person point of view (IVRA-FPV). After training, students performed a simulated lumbar puncture on a mannequin to analyze their applied learning skillset. An oral examination was also included as an assessment. | The group that participated in the traditional lecture showed significantly superior scoring n oral examination, p < 0.001. CONTROL: n = 45, M = 4.06, SE = 0.12. EXPERIMENTAL: n = 44, M = 4.97, SE = 0.10. The VR group took more time to perform the simulated lumbar puncture compared to the control, p < 0.01. CONTROL: n = 55, M = 73, SE = not reported. EXPERIMENTAL: n = 36, M = 50, SE = not reported. The VR group also had reduced errors compared to the control, p < 0.01. Means are reported as latency of errors. CONTROL: n = 44, M = 153.26, SE = 11.19. EXPERIMENTAL: n = 43, M = 227.50, SE = 34.34. |
3 (skills knowledge) (performance skills - time) (performance skills - errors) | - Skills knowledge + Performance skills + Performance skills |
Mixed Positive |
| Schoeb et al | 2020 | MR + Practice | medical - catheter placement | 164 medical students | 1 (Did nothing additional) | Medical students were randomized into one of two groups to undergo bladder catheter placement learning. One group underwent learning with an instructor, while the other group received mixed reality (MR) training using a Microsoft HoloLens. Both groups were able to participate in hands-on training before undergoing a standardized objective structured clinical examination (OSCE) for performance assessment. | The MR intervention group showed significantly superior bladder catheter placement simulation in comparison to the control group, p = 0.000. CONTROL: n = 107, M = 19.96, (SD = 2.42). EXPERIMENTAL: n = 57, M = 21.49, (SD = 2.27) |
1 (performance measures - OSCE) | + Performance measures |
Positive |
| Shao et al. | 2020 | VR | Medical - anatomy | 30 medical students | 1 (Combined) | Students were divided into either a traditional teaching group, or a virtual reality (VR) teaching group for teaching skull base tumors and skull anatomy. The traditional teaching group used literature-based learning, problem-based teaching, and case-based teaching, whereas the VR groups used real case images and Hololens (VR) glasses. After completion of their intervention. | VR group had higher total scoring on the basic knowledge assessment compared to the traditional control group, p < 0.001. CONTROL: n =15, M = 63.6 (SD = 3.81). EXPERIMENTAL: n =15, M = 77.07 (SD = 4.00). |
1 (skills knowledge) | + Skills knowledge | Positive |
| Smith et al. | 2018 | VR immersive or VR computer | nursing - decontamination skills | 172 nursing students | 1 (Print) | Nursing students were divided into 3 groups for decontamination skills training. The control group used a traditional written instructions learning method, whereas the experimental groups underwent immersive VR or computer-based VR training. Post-learning competency was measured using a Decontamination checklist in which students performed skills on a mannequin. Cognitive test scores, performance scores, and time to complete skills were measured immediately post-training and 6 months later. | Results are reported for the immediate follow-up post intervention. There were no significant differences among groups for the cognitive scores, p = 0.568. Means and SD are shown both VR groups combined and the traditional control group only. CONTROL: n = 43, M = 19 [8, 23]. EXPERIMENTAL: n = 43, M = 19 [13, 23]. There was no difference among the groups for time to completion on the OSCE, p = 0.723. Means and SD are shown both VR groups combined and the traditional control group only. CONTROL: n = 43, M = 260 [180, 360] EXPERIMENTAL: n = 43, M = 260 [180, 360]. The computer/mouse VR groups showed superior performance measures compared to the control group on the immediate post-test, p = 0.017. Means and SD are shown both VR groups combined and the traditional control group only. CONTROL: n = 43, M = 54 [46, 57]. EXPERIMENTAL: n = 43, M = 55 [46, 57]. |
3 (skills knowledge) (performance skills - time) (performance skills -other specific decontainment mannikin) | X No difference skills knowledge X No difference performance skills - Performance skills |
Mixed Negative |
| Stepan et al. | 2017 | VR | medical - neuroanatomy | 66 medical students | 1 (Electronic) | Medical students were assigned to either a control (online textbook) or an experimental (3D imaging VR interactive model) group for the learning of neuroanatomy. | Students completed preintervention, postintervention, and retention tests for assessment of knowledge. No significant differences in anatomy knowledge assessments were found between the control and VR groups, p = 0.87. CONTROL: n= 33, M = 0.76 (SD = 0.14) EXPERIMENTAL: n = 33, M = 75 (SD = 0.16) |
1 (skills knowledge) | X No difference skills knowledge | No difference |
| Sultan et al. | 2019 | VR | Medical - tube placement | 169 medical students | 1 (Practice) | Medical students were split into two groups to participate in a learning workshop regarding communication and collaboration. The workshop was a half-day, once a week, for 6 months. VR group received VR instruction, whereas the control group received conventional learning (simulated patients, lectures). Post-intervention assessment included an MCQs score and an Objective Structured Clinical Examinations (OSCE) score. | The VR intervention groups showed significantly higher MCQs compared to the control group after training, p < 0.001. CONTROL: n = 112, M = 15.9, (SD = 2.9). EXPERIMENTAL: n = 57, M = 17.4, (SD = 2.1) . The VR group also showed improved OSCE after training compared to the conventional learning group, p < 0.001. CONTROL: n = 112, M = 9.8, (SD = 4.2). EXPERIMENTAL: n =57, M = 12.9, (SD = 4.1). |
2 (skills knowledge) (performance measures-OSCE) | + Skills knowledge + Performance measures |
Positive |
| Watari et al. | 2020 | VR | medical students - basic clinical knowledge | 210 medical students | 1 Nothing (pre-post) | Medical students participated in a lecture that used Virtual Patient Simulations (VPSs). Pre- and post-test 20 item multiple-choice questionnaires were taken and involved both knowledge and clinical reasoning items. | Students showed a significant increase in post-test scoring on both knowledge, p = 0.003. EXPERIMENTALpre: n = 169, M = 4.78, [4.55, 5.01].EXPERIMENTALpost: n = 169, 5.12, [4.90, 5.43]. Students also had increased clinical reasoning after training, p < 0.001. EXPERIMENTALpre: n = 169 , M = 5.3, [4.98, 5.58]EXPERIMENTALpost: n =169, M = 7.81, [7.57, 8.05]. |
2 (skills knowledge) (clinical reasoning) |
+ Skills knowledge + Clinical reasoning |
Positive |
| Wolf et al | 2021 | AR | Medical - surgery | 21 medical students | 1 (Print) | Medical students were recruited for training in extracorporeal membrane oxygenation (ECMO) cannulation. They were split into two groups: (1) conventional training instructions for the first procedure, and AR instructions for the second; (2) reverse order (AR instructions for the first procedure). Participants performed the two ECMO cannulation procedures on a simulator. Training times and a detailed error protocol were used for assessment. | AR group showed minimally higher training times compared to the control group, no p values given. Means and SD in figures only. AR group had significantly less errors when performing the second (more complex) simulation procedure, no p values given. Means and SD in figures only. |
2 (performance skills - error) (performance skills – time) |
+ Performance skills -Performance skills |
Mixed |
| Yang & Oh | 2022 | VR | nursing - infant respiration | 83 nursing students | 2 (Teacher) (Practice) | Nursing students were separated into three groups to undergo neonatal resuscitation training. These groups included: a virtual reality group, high-fidelity simulation group, and a control (online lectures only) group. Pre and post-test scores were analyzed on neonatal resuscitation knowledge, problem-solving ability, and clinical reasoning ability. | Knowledge scores increased for all groups post-intervention, but the VR and simulation group showed significantly higher knowledge after intervention compared to the control group, p = 0.004. Means and SDs are reported for the VR and control groups only. CONTROL: n = 26, M =11.85, (SD = 5.43). EXPERIMENTAL: n = 29, M = 18.00, (SD = 2.55). The VR group showed significantly improved problem-solving ability scores in comparison to both the simulation and control groups, p = 0.038. CONTROL: n = 26, M = 106.24, (SD = 24.52). EXPERIMENTAL: n = 29, M = 122.72, (SD = 15.68). Clinical reasoning ability showed significant improved performance, but the none of the groups differed statistically, p = 0.123. CONTROL: n = 26, M = 53.69, (SD = 12.02). EXPERIMENTAL: n = 29, M = 59.66, (SD = 9.44). |
3 (skills knowledge – other specific resuscitation) (problem solving) (clinical reasoning) |
+ Skills knowledge + Problem solving X No difference clinical reasoning |
Mixed Positive |
| Yeo et al. | 2018 | AR + Ultrasound | medical- lumbar puncture and facet joint injection | 36 medical students | 1 (Practice) | Medical students were randomized into either a control group (ultrasound use only), or an experimental group that involved training with ultrasound and AR using Perk Tutor software. Training involved learning lumbar puncture and facet joint injection skills on five different tasks for two tasks, a simpler and hard one (ultrasound-guided facet joint injection). | Results are reported for the harder task, only. The AR group had more successful injections p = 0.04. CONTROL: n = 10, M = 37.5, SD = not reported. EXPERIMETNAL: n = 10, M = 62.5, SD = not reported. AR was also better than control post-training for total time, p < 0.001. CONTROL: n = 10, M = 103, (SD = 13). EXPERIMETNAL: n = 10, M = 47, (SD =3). AR was also better than control post-training for time inside the phantom body, p < 0.01. CONTROL: n = 10, M = 31, (SD = 5). EXPERIMETNAL: n = 10, M = 14, (SD = 2). AR was also better than control post-training for path distance inside the phantom body, p < 0.01. CONTROL: n = 10, M = 266, (SD = 76). EXPERIMETNAL: n = 182, M = 47, (SD =36). AR was also better than control post-training for potential tissue damage, p = 0.03. CONTROL: n = 10, M = 3217, (SD = 1173). EXPERIMETNAL: n = 10, M = 2376, (SD = 673). |
5 (performance skills - time) (performance skills – other specific time inside) (performance skills - other specific path) (performance skills – other specific damage) (performance skills - other specific success) | + Performance skills – + Performance skills + Performance skills + Performance skills + Performance skills |
Positive |
| Yu et al | 2022 | VR + Practice (BOX)* | Medical - surgery | 51 medical students | 1 Nothing (pre-post) | Medical students completed four pre and post experiments with a box trainer based laparoscopic surgery simulators (VRLS). Students were assessed by expert surgeons using the Global operative assessment of laparoscopic skills (GOALS) standards on performance and time on two tasks, fundamental task (FT) and the color resection task (CRT) | Post-test assessments showed a significantly faster task completion post training on both tasks, p < 0.01. Means and SDs are shown pre and post for one task (FT). EXPERIMENTALpre: n = 51, M =21.95, SD = not reported. EXPERIMETNALpost: n = 51, M = 14.04, SD = not reported. Post-training also had improved performance on the GOALS (heart rate) for both tasks, p < 0.05. Means and SDs are shown pre and post for one task (FT). EXPERIMENTALpre: n = 51, M = 94.96, (SD = 11.14). EXPERIMENTALpost: n = 51, M = 92.71, (SD = 11.67). |
2 (performance measures -GOALS) (performance skills - time) |
+ Performance skills + Performance measures - |
Positive |
| Zackoff et al. | 2020 | VR + Teacher + Practice | Med students- infant respiratory distress | 168 medical students | 1 (Teacher) | Medical students completed standard respiratory distress training using traditional didactic material, as well as a mannequin simulation. A randomized group of students also completed an additional 30-minute training using immersive virtual reality with various infant simulations (no distress, respiratory distress, and impending respiratory failure). After training, all students completed a free-response test regarding various video questions including mental status, breathing, breadth sounds, and vital signs for three different cases, no distress, respiratory distress, and respiratory failure. In addition, the need for escalation of care was assessed in each case. | Students who underwent additional VR intervention showed significantly superior status interpretation across all assessed dimensions and all cases, p < 0.01. Means and SDs for one case are shown (no distress). CONTROL: n = 90, M = 104 (SD = 61.2). EXPERIMENTAL: n = 78, M = 124 (SD = 80). The additional VR status groups also had a higher recognition for the need for increased care, p = 0.0004. Means and SDs for one case are shown (respiratory failure). CONTROL: n = 90, M = 41, (SD = 45.6). EXPERIMENTAL: n = 78, M = 56, (SD = 72.7). |
2 (skills knowledge- respiratory) (skills knowledge - level of care) | + Skills knowledge + Skills knowledge |
Positive |
| Zhou et al. | 2022 | AR | Nursing - stroke | 36 nursing students | 1 (Practice) | Nursing students were divided into two groups: a mannequin-based simulation only (control) or a mannequin-based simulation with AR. They were assessed for clinical judgment with the LCJR. | The AR group spent less time than the control group in the critical phase of the stroke simulation, p < 0.05. CONTROL: n = 18, M = 99.57, (SD = 79.00). EXPERIMENTAL: n = 18, M = 46.61, (SD = 27.92). AR outperformed the control group on the LCJR for one of three sections (noticing), p < 0.05. Means and SDs are only shown in figure. |
2 (performance skills - time) (clinical reasoning - LCJR) | + Performance skills + Clinical Reasoning |
Positive |
1.Note: Means (M) or Medians, and standard deviations (SD) or Interquartile Ranges (IQRs) are reported when available. Confidence intervals are reported in place of SD where available and appear in [ ].
Table 2.
Learning Theories Noted and Calculated MERSQI/NOS-E and QUADAS scores.
| Author, Date | Learning Theory Mentioned | MERSQI + NOS-E score (max 24) | QUADAS score (max 11) |
|---|---|---|---|
| Aebersold et al., 2018 | Situated learning theory | 22 | 10 |
| Andersen et al., 2021 | No | 21.5 | 11 |
| Andersen et al., 2022 | No | 21.5 | 9 |
| Arents et al., 2021 | Cognitive load | 15.5 | 6 |
| Azimi et al., 2018 | No | 12.5 | 4 |
| Banaszek et al., 2017 | No | 21 | 10 |
| Bayram & Caliskan, 2019 | NLN/Jeffries Simulation Theory | 17.5 | 7 |
| Blumstein et al., 2020 | No | 21 | 8 |
| Bogomolova et al., 2020 | Constructive Alignment Theory & Blooms | 21 | 8 |
| Bork et al., 2019 | No | 13.5 | 7 |
| Brinkmann et al., 2017 | No | 17.5 | 8 |
| Bube et al., 2020 | Directed self-regulated learning (DSRL) theory; Simulation-based mastery learning | 19 | 8 |
| Butt et al., 2018 | Deliberate practice theory | 19.5 | 9 |
| Cevallos et al., 2022 | No | 20 | 8 |
| Chao et al., 2021 | No | 17.5 | 8 |
| Chao et al., 2023 | Cognitive load theory | 21.5 | 8 |
| Chen & Liou, 2023 | No | 19 | 7 |
| Ekstrand et al., 2018 | No | 16.5 | 9 |
| Fu et al., 2020 | No | 16.5 | 9 |
| Haerling, 2018 | NLN/Jeffries Simulation Theory | 16.5 | 9 |
| Han et al., 2021 | No | 16 | 7 |
| Henssen et al., 2019 | Cognitive load theory; Blooms | 14.5 | 8 |
| Hu et al., 2020 | No | 19 | 7 |
| Issleib et al., 2021 | No | 20 | 3 |
| Jaskiewicz et al., 2020 | No | 15 | 3 |
| Jung & Park, 2023 | No | 16.5 | 9 |
| Kane et al., 2022 | No | 21 | 5 |
| Kowalewski et al., 2019 | No | 21 | 7 |
| Küçük et al., 2016 | Cognitive load theory | 18.5 | 9 |
| Lau et al., 2023 | No | 14 | 10 |
| Lemke et al., 2020 | No | 18.5 | 10 |
| Logishetty et al., 2018 | No | 20.5 | 9 |
| Maresky et al., 2018 | No | 17 | 3 |
| Moll- Khosrawi et al., 2022 | No | 20 | 8 |
| Moro et al., 2017 | Cognitive load theory | 17.5 | 3 |
| Nagayo et al., 2022 | No | 21 | 6 |
| Neumann et al., 2019 | No | 21 | 4 |
| Nielsen et al., 2021 | No | 19.5 | 8 |
| Noll et al., 2017 | No | 20.5 | 9 |
| Orland et al., 2020 | No | 21 | 4 |
| Plotzky et al., 2023 | No | 21 | 8 |
| Price et al., 2018 | No | 17 | 2 |
| Ros et al., 2020 | No | 17.5 | 3 |
| Ros et al., 2021 | Kolb | 20.5 | 4 |
| Schoeb et al., 2020 | No | 20.5 | 10 |
| Shao et al., 2020 | No | 19.5 | 3 |
| Smith et al., 2018 | No | 19 | 9 |
| Stepan et al., 2017 | No | 20.5 | 7 |
| Sultan et al., 2019 | Experiential learning theory | 19.5 | 8 |
| Watari et al., 2020 | No | 16 | 7 |
| Wolf et al,. 2021 | No | 15.5 | 7 |
| Yang & Oh, 2022 | No | 19 | 7 |
| Yeo et al., 2018 | No | 19 | 6 |
| Yu et al,. 2022 | Cognitive load theory | 18 | 6 |
| Zackoff et al., 2020 | No | 17.5 | 9 |
| Zhou et al., 2022 | No | 19 | 9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



