Submitted:
10 January 2025
Posted:
10 January 2025
You are already at the latest version
Abstract
Exercise therapy is an effective means of relieving neck pain. However, the effectiveness of various exercise therapy interventions is currently inconsistent. Therefore, this study aims to use network meta-analysis to investigate the effectiveness of exercise therapy in treating non-specific neck pain (NSNP) and the differences between different exercise interventions, providing insights into the application of exercise therapy in NSNP management. Randomized controlled trials (RCTs) of NSNP exercise therapy were collected by searching the databases of CNKI, Wanfang, Vipshop, Web of Science, Pubmed, Elsevier, and EBSCO. Stata software was used to assess the quality of the literature, and Stata software was used for network meta-analysis. The results showed that 1919 studies were jointly included, and 30 papers were remaining after screening.The results of the study showed that Ba duan jin, Pilates, Resistance, Stretch, Stability, Yoga, Qi gong, Endurance, and Tai chi, all 9 exercise modalities, could reduce the level of pain in patients with NSNP, of which Stretch, Stability, Resistance, Pilates, and Ba duan jin improvement had significant differences, and Stability training was the best modality to significantly improve neck pain in NSNP patients (Surface area under the cumulative ranking curve (SUCRA) = 74.5). Pilates, Resistance, Stretch, Stability, Yoga, Qi gong, and Tai chi. All 7 exercise modalities can improve neck dysfunction in patients with NSNP, Yoga, Stretch and Resistance had significant improvement, the best modality was Yoga (SUCRA=84.4). Ba duan jin, Resistance, Stretch, Qi gong, and Tai chi. these 5 exercise modalities can all improve the quality of life of NSNP patients, among which Ba duan jin has effectiveness, and the best modality to improve neck dysfunction in NSNP patients is Ba duan jin (SUCRA=91.1).Exercise therapy is an effective rehabilitation treatment for NSNP, with significant effects in relieving NP, improving neck dysfunction, and enhancing quality of life. Among them, stability training had the best effect in relieving NP, yoga training had the best effect on neck dysfunction, and Ba duan jin had the best effect on life quality improvement.
Keywords:
non-specific neck pain
; exercise therapy
; network meta-analysis
1. Introduction
Neck pain (NP), abbreviated as neck pain, refers to pain located in the anatomical region of the neck from the upper neckline to the region of the spinous process of the first thoracic vertebra[1].Non-specific neck pain (NSNP), also known as mechanical neck pain, is a type of neck pain that refers to pain in the anatomical region of the cervical spine (excluding the shoulder) caused by a variety of factors, with or without radiating arm pain, with no or mild to severe interference with activities of daily living, and with no specific pathologic manifestations, characteristic signs and symptoms[2]. With the accelerated pace of society and changes in the living and working environments, more and more people suffer from NSNP. At the onset of NSNP, patients may experience soft tissue pain in the neck muscles or accompanying dysfunction in neck movement, which has a certain adverse impact on the normal life and work of the patients[3]. Patients with NSNP have tense superficial neck muscles, while the deep neck muscles are less activated and relatively weak, which is the common muscle recruitment pattern[4]. Epidemiologic surveys have shown that the 1-year prevalence in adult workers is estimated to be between 30% and 50%[5]. The occurrence of NSNP reduces an individual's quality of life and economic productivity and places an economic burden on society. Considering the tremendous burden that neck pain places on individuals, healthcare systems, and industries around the world, it is critical to explore strategies to reduce the prevalence of neck pain[6].
In order to reduce the social burden caused by NSNP, several international guidelines on the treatment of NSNP have been published in recent years, for example, in the United States, Australia, Denmark and the Netherlands[7,8,9,10]. The guidelines all suggest the important role of exercise therapy for treatment and rehabilitation. At the same time, the promotion of physical activity appears to be a positive strategy for alleviating the prevalence of musculoskeletal disorders, including neck pain[11]. A large amount of literature shows that exercise therapy has good efficacy in treating the disease of chronic non-specific neck pain. For example, progressive shoulder and neck exercises can improve the strength of the deep and superficial neck muscles of patients with chronic neck pain, increase muscle function, strengthen the muscles of the shoulder and neck, and reduce the probability of chronic neck pain[12,13]. Cervical and shoulder resistance exercise can relieve neck pain and improve cervical joint mobility, and cervical and shoulder resistance exercise has certain advantages in improving the endurance of neck flexors and the strength of shoulder abductors, and Pilates exercise can reduce pain, lower the cervical disability index, alleviate symptoms of depression, and improve the quality of life, and at the same time, the exercise can significantly enhance the thickness of the semispinalis muscle[14]. Most patients with chronic neck pain have decreased activity of the deep cervical muscle groups and increased activity of the superficial cervical flexor muscles, while the patients' flexor endurance was significantly higher than that of the conventional group after being treated with stabilizing exercises. Stability exercises can increase the endurance of the deep neck flexors and decrease the activity of the superficial neck flexors in patients with chronic neck pain, which is beneficial for the treatment of chronic neck pain[15]. Although there have been many randomized controlled trials (RCTs) that have analyzed the effectiveness of exercise therapy in the treatment of NSNP and studies comparing the differences between several therapies, they do not reflect the effectiveness of all exercise intervention programs. It is therefore difficult to draw conclusions about the reliability of the effectiveness of different exercise intervention programs, and therefore guiding scientific and systematic recommendations are lacking.
The primary aim of this systematic review was to specifically examine the improvement of participation in exercises designed to explore movement on the level of neck pain, level of neck dysfunction, and quality of life in adult patients with NSNP. The second aim was to explore the efficacy of different exercise modalities on patients with NSNP and to discover exercise modalities with better results. We anticipate that these findings will inform clinicians who wish to advise their patients regarding participation in fitness or exercise and the potential benefits for neck pain.
2. Methods
Network meta-analysis is performed according to the preferred reporting items in the System Review and Meta-analysis (PRISMA) guide[16]. (PROSPERO: CRD42021285647).
2.1. Literature Search Strategy
The studies search was performed for the related research studies, mainly from the following databases: PubMed, Cochrane Library, Web of Science, EBSCO, CNKI. The search keywords we used were (exercise therapy OR remedial exercise OR rehabilitation exercise) AND (neck pain OR cervicalgia OR cervicodynia OR neckache OR cervical pain) AND (RCT OR random OR random controlled trial). The network meta-analysis is limited to March 2024, and only includes randomized controlled trials.
2.2. Inclusion and Exclusion Criteria
Criteria for inclusion:(1) experimental studies using exercise therapy to intervene in NSNP; (2) RCTs; (3) no significant differences in basic indicators of the included patients before the intervention; (4) outcome indicators containing neck pain level (visual analogue scale, VAS; numerical pain scale, NPS; neck pain questionnaire, NPQ), neck disability index (NDI; neck pain and disability scale, NPDS), and quality of life (SF-12, SF-36); and (5) relevant data before and after the intervention could be obtained. Criteria for exclusion:(1) observational studies; (2) non-human subjects; (3) history of trauma or surgery to the neck; (4) subjects containing symptoms other than NP; and (5) inability to extract outcome indicators.
2.3. Data Extraction
Two authors independently screened the abstracts and full-text articles of the selected works, extracting and cross-verifying the data. In instances of disagreement, a third party was consulted to mediate and reach a consensus. During the studies screening process, the initial step involved reading the titles and abstracts, followed by a thorough examination of the full texts to determine the studies to be excluded.
2.4. Quality Assessment
The quality of the included studies was evaluated. Then two authors assessed the quality of the included studies. Any disagreement was discussed with a third reviewer. The two authors/It is important to use the Cochrane Handbook for Systematic Interventions to assess the quality of studies. It includes the evaluation of randomization methods, concealment of distribution, blindness of patients and physicians, outcome evaluation, data integrity, selective reporting, and other biased sources.
2.5. Statistical Analysis
STATA (Version 17.0) command'mvmeta' was used to perform a multivariate network meta-analysis within a frequentist framework. The therapeutic effect of each study on NAFLD was calculated by standard mean deviation (SMD) and standard deviation (SD). For studies that provide only median and quartile ranges, we derive SMD and SD to overcome the heterogeneity between research interventions and results[17,18]. The I2 statistics are used to measure heterogeneity, which is considered high heterogeneity when it exceeds 50%. Consistency means that the treatment effect estimated by direct comparison is consistent with that estimated by indirect comparison. Statistical indicators include pain level, neck dysfunction, quality of life. Subsequently, interventions were ranked using the surface under the cumulative ranking curve (SUCRA). SUCRA is considered to be a more accurate estimate of the cumulative ranking probability. Simultaneously, SUCRA reported the overall probability based on the ranking of all interventions, that is, a given intervention is one of the best treatments[19,20].
3. Result
3.1. Literature Selection
A total of 1919 studies were assembled in various Chinese and English databases through subject term search, and 1,801 studies were remaining after de-weighting using EndNoteX9, 166 studies were obtained through the initial screening of titles and abstracts; 30 studies were finally included by reading the full text to exclude incomplete data studies, and duplicate publications, and the process of studies screening is shown in Figure 1.
3.2. Characteristics of the Included Studies
30 studies were included in this study, totaling 2,291 subjects[21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50]. 9 exercise modalities were included in the 30 papers in this study, including: Ba duan jin, Pilates, Resistance, Stretch, Stability, Yoga, Qi gong, Endurance, and Tai chi. The length of the single exercise intervention included in the study ranged from 10-90 min; the frequency of the exercise intervention ranged from 1-7 times per week; and the intervention period ranged from 3-24 weeks. (Table 1)
3.3. Result of Assessment
According to the Cochrane Handbook for Systematic Reviews of Interventions, the quality of the included studies was evaluated using the quality assessment method specific to randomized controlled trials (RCTs). The Cochrane Risk of Bias Assessment Tool highlighted the risks of various biases across 30 studies(Figure 2 and Figure 3). The highest risks were identified in relation to performance bias due to lack of blinding and detection bias in outcome evaluation when assessing new concepts. Conversely, other biases, such as attrition bias, reporting bias, and biases related to random sequence generation, were assessed to be of low risk.
3.4. Network Meta-Analysis
This study included various types of exercise therapy: Ba duan jin, Pilates, Resistance, Stretch, Stability, Yoga, Qi gong, Endurance, and Tai chi. The effects of 9 different exercises on pain levels, neck dysfunction and in patients with non-specific neck pain were analyzed. Figure 3 shows the network meta-analysis of the effects of different exercise interventions on efficacy. The size of the node is related to the number of participants in the exercise interventions, and the thickness of the lines between different nodes is related to the number of studies compared. In the network analysis, SUCRA is considered to be a more accurate estimate of the cumulative ranking probability. It can use different ranking methods, maximum or minimum, according to the different benefits of sports. (Figure 4, Figure 5 and Figure 6).
3.4.1. Pain Level
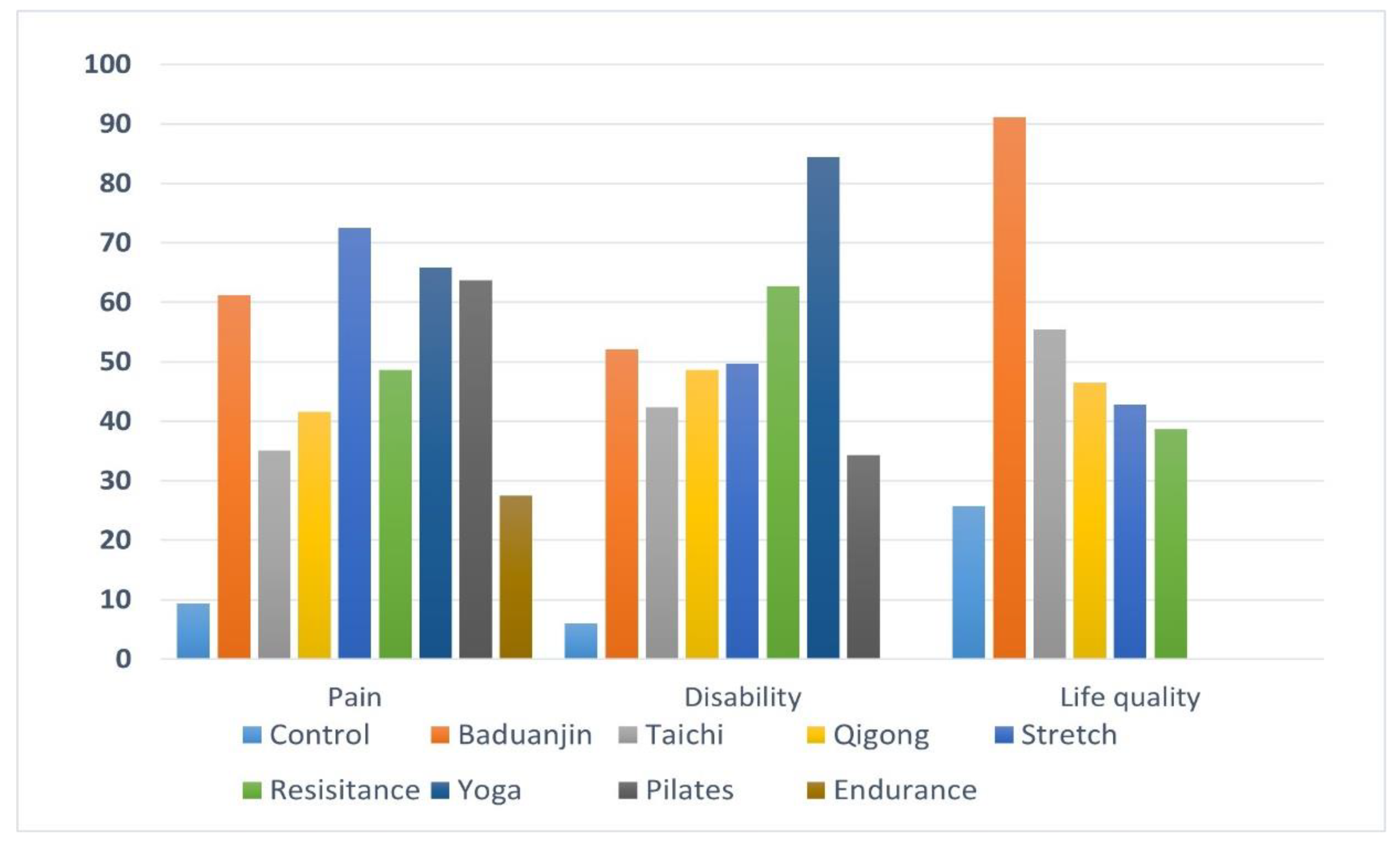
In terms of neck pain reduction, all 9 different exercise modalities reduced the level of neck pain in patients with non-specific neck pain compared to the control group. Ba duan jin( -1.79 [-3.55,-0.02]), Pilates (-1.84 [-3.35,-0.34]), Resistance (-1.38 [-2.28,-0.49]), Stretch (-2.18 [-4.02,-0.35]), Stability (-2.15 [-3.55,-0.76]), Yoga (-2.03 [-4.47,0.42]), Qi gong (-1.12 [-2.99,0.76]), Endurance (-0.55 [-2.67,1.57]), and Tai chi (-0.74 [-3.74,2.26]). Among them, Stretch, Stability, Resistance, Pilates, and Ba duan jin had a significant effect on neck pain relief (p<0.05). Inconsistency results showed p=0.9815>0.05, indicating consistency of results. Calculations by SUCRA show that Stability training (SUCRA= 74.5) provides the best benefits. Stretch (SUCRA= 72.5), Yoga (SUCRA= 65.9), Pilates (SUCRA= 63.7), Ba duan jin (SUCRA= 61.2), Resistance (SUCRA= 48.6), Qigong (SUCRA= 41.6), Tai chi (SUCRA= 35), Endurance (SUCRA= 27.5), Control (SUCRA= 9.4) (Figure 7).
3.4.2. Neck Dysfunction
In terms of enhancing quality of life, all seven different exercise modalities reduced the level of neck dysfunction in patients with non-specific neck pain compared to the control group. Pilates (-0.72 [-1.86,0.42]), Resistance (-1.32 [-2.05,-0.59]), Stretch (-1.06 [-2.17,0.04]), Stability (-1.59 [-2.79,-0.38]), Yoga (-2.00 [-3.36,-0.37]), Qi gong (-1.02 [-2.30,0.27]), and Tai chi (-0.86 [-2.92,1.21]).Among them, Yoga, Stretch and Resistance had a significant effect on neck dysfunction relief (p<0.05). Inconsistency results showed p=0.4043>0.05, indicating consistency of results. Calculations by SUCRA show that Yoga (SUCRA= 84.4) provides the best benefits. Stability (SUCRA= 72.1), Resistance (SUCRA= 62.7), Stretch (SUCRA= 49.7), Qi gong (SUCRA= 48.6), Tai chi (SUCRA= 42.3), Pilates (SUCRA= 34.3), Control (SUCRA= 6) (Figure 7).
3.4.3. Life Quality
In terms of life quality enhancement, all five different exercise modalities enhanced the level of quality of life in patients with non-specific neck pain compared to the control group. Ba duan jin(1.60 [0.57,2.63]), Resistance (0.21 [-0.94,1.35]), Stretch (0.33 [-0.94,1.35]), Qi gong (0.37 [-0.94,1.35]), and Tai chi (0.64 [-1.36,2.63]). Among them, Ba duan jin had a significant effect on life quality enhancement (p<0.05). Inconsistency results showed p=0.9976>0.05, indicating consistency of results. Calculations by SUCRA show that Ba duan jin (SUCRA= 91.1), provides the best benefits. Tai chi (SUCRA= 55.4), Qigong (SUCRA= 46.4), Stretch (SUCRA= 42.8), Resistance (SUCRA= 38.6), Control (SUCRA= 25.7) (Figure 7).
4. Discussion
NSNP, as a chronic pain with no clear etiologic source, should follow a multimodal treatment principle in which exercise therapy plays a crucial role [36]. The aim of this study was to systematically review the RTCs related to different exercise interventions for NSNP, analyze the changes in neck pain, neck dysfunction, and quality of life of patients after the intervention of different exercise regimens, and explore the effects of different exercise regimens in intervening NSNP. From a general point of view, exercise therapy is effective in improving neck pain, neck dysfunction and quality of life in patients with NSNP, but there are some effect differences between exercise intervention programs of different modalities.
4.1. Pain Improvement
Symptoms of neck pain are basically similar to those of cervical spondylosis, and are characterized by localized pain, discomfort, and limitation of movement in the neck. There are many causes of neck pain, including degenerative diseases of the cervical spine, developmental cervical spinal stenosis, etc., which cause neck muscle injury, cervical spine stability disorder, nerve root compression, and vertebral artery stimulation, etc., and can easily lead to the occurrence of cervical spondylosis. Neck pain can impact motor control, leading to co-contraction of agonist muscles, increased activity of superficial flexor and extensor muscles, delayed onset of neck muscle activation, and weakness in the deep muscles[51,52]. In recent years, stability training has become a popular form of fitness activity and has begun to be widely used in rehabilitation programs and sports medicine[53]. The results of this study found that Ba duan jin is one of the best ways to enhance the quality of life of NSNP patients. Stability training controls the balance and stability of the body through fixed or slow dynamic body posture control and activates the core, deeper smaller muscle groups, therefore, through stability training or movement control training, deep neck muscle strength and endurance can be exercised, which may have a potential therapeutic effect on NSNP. Wu found through systematic review and Meta-analysis that stability training has a significant role in the treatment of NP disorders with certain effects[54]. The clinical guidelines of the American Physical Therapy Association state that exercise is part of the therapeutic intervention for NSNP[7], and advocate active exercise aimed at strengthening neck muscle strength or endurance, in addition to movement exercises related to neck muscle stretching, coordination, and control. Similarly in the Chinese expert consensus on exercise therapy for the treatment of NP, neck muscle strength training, stability training, and yoga are also included as strongly recommended exercise treatments for NP treatment[55]. Therefore, stability training can be considered a preferred approach for exercise intervention.
4.2. Neck Dysfunction
Chronic injuries caused by neck injuries, incorrect posture, etc., cause strain and laxity of neck muscles and ligaments, and produce chronic pathological changes in the neck, all of which can cause neck dysfunction. Yoga is a mind-body training program that integrates strength, flexibility, coordination, stability, and cardiorespiratory function, which has positive therapeutic effects on chronic musculoskeletal disorders[56]. Relevant scholars at home and abroad have also proved that yoga has good effects in treating NSNP through the method of systematic review and Meta-analysis. The results of this study also further proved that the effectiveness of yoga in improving neck dysfunction is best. Yoga originally means "integration" and is a philosophical idea. Nowadays, yoga for sports is also an exercise method that keeps the practitioner physically and mentally healthy through the combination of asana, breathing and meditation. The results of this study found that yoga is one of the best ways to improve neck dysfunction in NSNP patients. Yoga helps identify and modify habitual posture patterns, thereby correcting poor body posture and muscle tension in daily life[57]. Consequently, patients with chronic neck pain report an enhanced awareness of posture in their daily activities after practicing yoga[58]. Additionally, yoga has been shown to improve proprioception and range of motion in the neck for those with chronic neck pain. Furthermore, potential nonspecific factors may include environmental and attentional effects, participants' responses to meaning and beliefs, and social influences generated by group interventions.
4.3. Life Quality
In the studies dealing with life quality enhancement for people with NSNP, the majority of exercise interventions are physical and mental training. Ba Duan Jin is a traditional Chinese method of physical and mental training, which is profound and has a long history, is an important part of Chinese culture, and in recent years has been widely recognized around the world. Traditional Chinese physical and mental training is a low-cost form of exercise that involves the musculoskeletal involvement of the whole body through changes in body posture and control of movement speed, which can enhance the qualities of strength, agility, balance and flexibility, strengthen the function of the motor nervous system, improve cardiorespiratory endurance, and have the effects of health care, body nourishment, and treatment of diseases[59]. The results of this study found that Ba duan jin is one of the best ways to enhance the quality of life of NSNP patients. Ba duan jin is believed to invigorate and nourish qi, relax muscles, strengthen the body, promote blood circulation, remove blood stasis, enhance metabolism, and harmonize internal organs. It is said to regulate cardiac function and respiration, unblock meridians to alleviate cardiac pressure, maintain calmness, and balance mental state[60]. The results of this study found that Ba duan jin is effective in alleviating neck pain and improving neck dysfunction. Additionally, the improvement in quality of life highlights Ba duan jin's holistic approach, embodying the traditional Chinese practice's dual focus on physical fitness and mental well-being.
Some of the outcome indicators included in the literature were not comprehensive enough, especially the literature containing quality of life evaluation indicators was insufficient. According to the elements of exercise prescription development, in addition to exercise modality, exercise intensity, exercise duration, exercise frequency, and exercise cycle are included, but due to the limitations of the amount of literature, these factors could not be considered comprehensively.
5. Conclusion
Exercise therapy is an effective rehabilitation treatment for NSNP, with significant effects in relieving neck pain, improving neck dysfunction, and enhancing quality of life. Among them, stability training had the best effect in relieving neck pain, yoga training had the best effect on neck dysfunction, and Ba duan jin had the best effect on life quality improvement. Therefore, in the future exercise prescription design, physical therapy programs can be better designed for NSNP patients based on these findings.
There is no conflict of interest among all authors.
References
- Nyirö, L.; Peterson, C.K.; Humphreys, B.K. Exploring the definition of "acute" neck pain: a prospective cohort observational study comparing the outcomes of chiropractic patients with 0-2 weeks, 2-4 weeks and 4-12 weeks of symptoms. Chiropractic & Manual Therapies 2017, 25. [Google Scholar] [CrossRef]
- Lohman, E.B.; Pacheco, G.R.; Gharibvandi, L.; Daher, N.; Devore, K.; Bains, G.; AlAmeri, M.; Berk, L.S. The immediate effects of cervical spine manipulation on pain and biochemical markers in females with acute non-specific mechanical neck pain: a randomized clinical trial. Journal of Manual & Manipulative Therapy 2019, 27, 186–196. [Google Scholar] [CrossRef]
- Cerezo-Téllez, E.; Torres-Lacomba, M.; Mayoral-del-Moral, O.; Pacheco-da-Costa, S.; Prieto-Merino, D.; Sánchez-Sánchez, B. Health related quality of life improvement in chronic non-specific neck pain: secondary analysis from a single blinded, randomized clinical trial. Health and quality of life outcomes 2018, 16. [Google Scholar] [CrossRef] [PubMed]
- Tsang, S.M.H.; Szeto, G.P.Y.; Xie, Y.F.; Lee, R.Y.W. Association of electromyographic activation patterns with pain and functional disability in people with chronic neck pain. European Journal of Applied Physiology 2018, 118, 1481–1492. [Google Scholar] [CrossRef]
- Haldeman, S.; Carroll, L.; Cassidy, J.D. Findings From The Bone and Joint Decade 2000 to 2010 Task Force on Neck Pain and Its Associated Disorders. Journal of occupational and environmental medicine 2010, 52, 424–427. [Google Scholar] [CrossRef]
- Hoy, D.G.; Protani, M.; De, R.; Buchbinder, R. The epidemiology of neck pain. Best Practice & Research in Clinical Rheumatology 2010, 24, 783–792. [Google Scholar] [CrossRef]
- Blanpied, P.R.; Gross, A.R.; Elliott, J.M.; Devaney, L.L.; Clewley, D.; Walton, D.M.; Sparks, C.; Robertson, E.K. Neck Pain: Revision 2017. Journal of Orthopaedic & Sports Physical Therapy 2017, 47, A1–A83. [Google Scholar] [CrossRef]
- Kjaer, P.; Kongsted, A.; Hartvigsen, J.; Isenberg-Jørgensen, A.; Schiøttz-Christensen, B.; Søborg, B.; Krog, C.; Møller, C.M.; Halling, C.M.B.; Lauridsen, H.H. National clinical guidelines for non-surgical treatment of patients with recent onset neck pain or cervical radiculopathy. European Spine Journal 2017, 26, 2242–2257. [Google Scholar] [CrossRef]
- Bier, J.D.; Scholten-Peeters, W.G.M.; Staal, J.B.; Pool, J.; van Tulder, M.W.; Beekman, E.; Knoop, J.; Meerhoff, G.; Verhagen, A.P. Clinical Practice Guideline for Physical Therapy Assessment and Treatment in Patients With Nonspecific Neck Pain. Physical therapy 2017, 98, 162–171. [Google Scholar] [CrossRef]
- Bobos, P.; MacDermid, J.C. Appraisal of Clinical Practice Guideline: Management of neck pain. J Physiother 2018, 64, 127. [Google Scholar] [CrossRef]
- Alzahrani, H.; Mackey, M.; Stamatakis, E.; Zadro, J.R.; Shirley, D. The association between physical activity and low back pain: a systematic review and meta-analysis of observational studies (vol 9, pg 8244, 2019). Scientific reports 2020, 10. [Google Scholar] [CrossRef]
- Lin, I.H.; Chang, K.H.; Liou, T.H.; Tsou, C.M.; Huang, Y.C. Progressive shoulder-neck exercise on cervical muscle functions in middle-aged and senior patients with chronic neck pain. European Journal of Physical and Rehabilitation Medicine 2018, 54, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Caputo, G.M.; Di Bari, M.; Naranjo Orellana, J. Group-based exercise at workplace: short-term effects of neck and shoulder resistance training in video display unit workers with work-related chronic neck pain-a pilot randomized trial. Clinical rheumatology 2017, 36, 2325–2333. [Google Scholar] [CrossRef] [PubMed]
- Dunleavy, K.; Kava, K.; Goldberg, A.; Malek, M.H.; Talley, S.A.; Tutag-Lehr, V.; Hildreth, J. Comparative effectiveness of Pilates and yoga group exercise interventions for chronic mechanical neck pain: quasi-randomised parallel controlled study. Physiotherapy 2016, 102, 236–242. [Google Scholar] [CrossRef]
- Ghaderi, F.; Jafarabadi, M.A.; Javanshir, K. The clinical and EMG assessment of the effects of stabilization exercise on nonspecific chronic neck pain: A randomized controlled trial. Journal of Back and Musculoskeletal Rehabilitation 2017, 30, 211–219. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Annals of internal medicine 2015, 162, 777–784. [Google Scholar] [CrossRef]
- Bennett, M.M.; Crowe, B.J.; Price, K.L.; Stamey, J.D.; Seaman, J.W., Jr. Comparison of Bayesian and frequentist meta-analytical approaches for analyzing time to event data. J Biopharm Stat 2013, 23, 129–145. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 2014, 14, 135. [Google Scholar] [CrossRef]
- Mbuagbaw, L.; Rochwerg, B.; Jaeschke, R.; Heels-Andsell, D.; Alhazzani, W.; Thabane, L.; Guyatt, G.H. Approaches to interpreting and choosing the best treatments in network meta-analyses. Syst Rev 2017, 6, 79. [Google Scholar] [CrossRef]
- Shim, S.; Yoon, B.H.; Shin, I.S.; Bae, J.M. Network meta-analysis: application and practice using Stata. Epidemiol Health 2017, 39, e2017047. [Google Scholar] [CrossRef]
- Shi, Z. Study on Fitness Qigong Baduanjin Improving the Quality of Life of Patients with Chronic Neck Pain. Contemporary Sports Technology 2023, 13, 37–40. [Google Scholar] [CrossRef]
- Zhao, M. Research on the Effects of Pilates-based Exercises for Chronic Nonspecific Neck Pain. Bulletin of Sport Science & Technology 2020, 28, 167–168. [Google Scholar] [CrossRef]
- Cai, Y.; Liu, A.; Yao, Z.; Li, J.; Wang, Y. The impact of Baduanjin on the quality of life of middle-aged and elderly people with chronic neck pain. Chinese Journal of Gerontology 2018, 38, 2934–2936. [Google Scholar]
- Wang, J. The effects of regular Qigong-Ba Duan Jin practice on promoting the health in patients with chronic neck pain. 硕士, Beijing University of Chinese Medicine, 2013.
- Hernandez-Lucas, P.; Leirós-Rodríguez, R.; Lopez-Barreiro, J.; García-Soidán, J.L. Effects of back school-based intervention on non-specific neck pain in adults: a randomized controlled trial. BMC Sports Sci Med Rehabil 2023, 15, 60. [Google Scholar] [CrossRef]
- Sahiner Picak, G.; Yesilyaprak, S.S. Effects of clinical pilates exercises in patients with chronic nonspecific neck pain: a randomized clinical trial. Irish journal of medical science 2022. [Google Scholar] [CrossRef]
- Javdaneh, N.; Saeterbakken, A.H.; Shams, A.; Barati, A.H.T.a.d.n.c.o.i. Pain Neuroscience Education Combined with Therapeutic Exercises Provides Added Benefit in the Treatment of Chronic Neck Pain. International journal of environmental research and public health 2021, 18. [Google Scholar] [CrossRef]
- Bernal-Utrera, C.; Anarte-Lazo, E.; Gonzalez-Gerez, J.J.; Saavedra-Hernandez, M.; De-La-Barrera-Aranda, E.; Serrera-Figallo, M.A.; Gonzalez-Martin, M.; Rodriguez-Blanco, C. Effect of Combined Manual Therapy and Therapeutic Exercise Protocols on the Postural Stability of Patients with Non-Specific Chronic Neck Pain. A Secondary Analysis of Randomized Controlled Trial. J Clin Med 2021, 11. [Google Scholar] [CrossRef]
- avdaneh, N.; Molayei, F.; Kamranifraz, N. Effect of adding motor imagery training to neck stabilization exercises on pain, disability and kinesiophobia in patients with chronic neck pain. Complementary therapies in clinical practice 2021, 42, 101263. [Google Scholar] [CrossRef]
- de Araujo Cazotti, L.; Jones, A.; Roger-Silva, D.; Ribeiro, L.H.C.; Natour, J. Effectiveness of the Pilates Method in the Treatment of Chronic Mechanical Neck Pain: A Randomized Controlled Trial. Arch Phys Med Rehabil 2018, 99, 1740–1746. [Google Scholar] [CrossRef]
- Dunleavy, K.; Kava, K.; Goldberg, A.; Malek, M.H.; Talley, S.A.; Tutag-Lehr, V.; Hildreth, J. Comparative effectiveness of Pilates and yoga group exercise interventions for chronic mechanical neck pain: quasi-randomised parallel controlled study. Physiotherapy 2016, 102, 236–242. [Google Scholar] [CrossRef]
- von Trott, P.; Wiedemann, A.M.; Lüdtke, R.; Reishauer, A.; Willich, S.N.; Witt, C.M. Qigong and exercise therapy for elderly patients with chronic neck pain (QIBANE): a randomized controlled study. J Pain 2009, 10, 501–508. [Google Scholar] [CrossRef]
- Helewa, A.; Goldsmith, C.H.; Smythe, H.A.; Lee, P.; Obright, K.; Stitt, L. Effect of therapeutic exercise and sleeping neck support on patients with chronic neck pain: A randomized clinical trial. Journal of Rheumatology 2007, 34, 151–158. [Google Scholar] [PubMed]
- Khosrokiani, Z.; Letafatkar, A.; Sokhanguei, Y. Long-term effect of direction-movement control training on female patients with chronic neck pain. Journal of bodywork and movement therapies 2018, 22, 217–224. [Google Scholar] [CrossRef]
- Li, X.; Lin, C.; Liu, C.; Ke, S.; Wan, Q.; Luo, H.; Huang, Z.; Xin, W.; Ma, C.; Wu, S. Comparison of the effectiveness of resistance training in women with chronic computer-related neck pain: a randomized controlled study. Int Arch Occup Environ Health 2017, 90, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Rendant, D.; Pach, D.; Lüdtke, R.; Reisshauer, A.; Mietzner, A.; Willich, S.N.; Witt, C.M. Qigong versus exercise versus no therapy for patients with chronic neck pain: a randomized controlled trial. Spine 2011, 36, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Viljanen, M.; Malmivaara, A.; Uitti, J.; Rinne, M.; Palmroos, P.; Laippala, P. Effectiveness of dynamic muscle training, relaxation training, or ordinary activity for chronic neck pain: randomised controlled trial. BMJ (Clinical research ed.) 2003, 327, 475. [Google Scholar] [CrossRef] [PubMed]
- Beer, A.; Treleaven, J.; Jull, G. Can a functional postural exercise improve performance in the cranio-cervical flexion test?--a preliminary study. Man Ther 2012, 17, 219–224. [Google Scholar] [CrossRef]
- Ma, C.; Szeto, G.P.; Yan, T.; Wu, S.; Lin, C.; Li, L. Comparing biofeedback with active exercise and passive treatment for the management of work-related neck and shoulder pain: a randomized controlled trial. Arch Phys Med Rehabil 2011, 92, 849–858. [Google Scholar] [CrossRef]
- Andersen, L.L.; Kjaer, M.; Søgaard, K.; Hansen, L.; Kryger, A.I.; Sjøgaard, G. Effect of two contrasting types of physical exercise on chronic neck muscle pain. Arthritis and rheumatism 2008, 59, 84–91. [Google Scholar] [CrossRef]
- Ahlgren, C.; Waling, K.; Kadi, F.; Djupsjöbacka, M.; Thornell, L.E.; Sundelin, G. Effects on physical performance and pain from three dynamic training programs for women with work-related trapezius myalgia. J Rehabil Med 2001, 33, 162–169. [Google Scholar] [CrossRef]
- Wang, J.-Y.; Guo, H.; Tang, L.; Meng, J.; Hu, L.-y. Case-control study on regular Ba Duan Jin practice for patients with chronic neck pain. International Journal of Nursing Sciences 2014, 1, 360–366. [Google Scholar] [CrossRef]
- Lauche, R.; Stumpe, C.; Fehr, J.; Cramer, H.; Cheng, Y.W.; Wayne, P.M.; Rampp, T.; Langhorst, J.; Dobos, G. The Effects of Tai Chi and Neck Exercises in the Treatment of Chronic Nonspecific Neck Pain: A Randomized Controlled Trial. The journal of pain 2016, 17, 1013–1027. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.; Bronfort, G.; Schulz, C.; Maiers, M.; Bracha, Y.; Svendsen, K.; Grimm, R.; Garvey, T.; Transfeldt, E. Supervised Exercise With and Without Spinal Manipulation Performs Similarly and Better Than Home Exercise for Chronic Neck Pain. Spine 2012, 37, 903–914. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, T.G.; Pecos-Martin, D.; Girbés, E.L.; Plaza-Manzano, G.; Caldentey, R.R.; Melús, R.M.; Mariscal, D.B.; Falla, D. Comparison of Cranio-Cervical Flexion Training Versus Cervical Proprioception Training in Patients with Chronic Neck Pain: A Randomized Controlled Clinical Trial. Journal of Rehabilitation Medicine 2016, 48, 48–55. [Google Scholar] [CrossRef]
- Lansinger, B.; Larsson, E.; Liselott, C.P.; Carlsson, J.Y. Qigong and exercise therapy in patients with long-term neck pain. Spine 2007, 32, 2415–2422. [Google Scholar] [CrossRef]
- Luo, Y.; Fan, Y.; Ma, T.; Wang, L.; Wu, H. The intervention of neck resistance training in different postures for chronic nonspecific neck pain. Chinese Journal of Rehabilitation Medicine 2024, 39, 693–698. [Google Scholar]
- Akodu, A.K.; Nwanne, C.A.; Fapojuwo, O.A. Efficacy of neck stabilization and Pilates exercises on pain, sleep disturbance and kinesiophobia in patients with non-specific chronic neck pain: A randomized controlled trial. Journal of bodywork and movement therapies 2021, 26, 411–419. [Google Scholar] [CrossRef]
- Kaka, B.; Ogwumike, O.O.; Adeniyi, A.F.; Maharaj, S.S.; Ogunlade, S.O.; Bello, B. Effectiveness of neck stabilisation and dynamic exercises on pain intensity, depression and anxiety among patients with non-specific neck pain: a randomised controlled trial. Scandinavian journal of pain 2018, 18, 321–331. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Hohmann, C.; Lüdtke, R.; Haller, H.; Michalsen, A.; Langhorst, J.; Dobos, G. Randomized-controlled Trial Comparing Yoga and Home-based Exercise for Chronic Neck Pain. Clinical Journal of Pain 2013, 29, 216–223. [Google Scholar] [CrossRef]
- Falla, D.; Jull, G.; Hodges, P.W. Feedforward activity of the cervical flexor muscles during voluntary arm movements is delayed in chronic neck pain. Exp Brain Res 2004, 157, 43–48. [Google Scholar] [CrossRef]
- Ylinen, J.; Salo, P.; Nykänen, M.; Kautiainen, H.; Häkkinen, A. Decreased isometric neck strength in women with chronic neck pain and the repeatability of neck strength measurements. Arch Phys Med Rehabil 2004, 85, 1303–1308. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.R.; Lambert, M.I.; Hunter, A.M. Contemporary perspectives of core stability training for dynamic athletic performance: a survey of athletes, coaches, sports science and sports medicine practitioners. Sports medicine-open 2018, 4, 32. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Yuan, H.; Geng, D.; Zhang, L.; Zhang, C. The impact of a stabilization exercise on neck pain: a systematic review and meta-analysis. Journal of Neurological Surgery Part A: Central European Neurosurgery 2020, 81, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wang, y.; Zhang, Z.; Zhu, Y.; Chen, P. Exercise therapy for neck pain:Consensus from Chinese Experts. Journal of Shanghai University of Sport 2020, 44, 59–69. [Google Scholar] [CrossRef]
- Denham-Jones, L.; Gaskell, L.; Spence, N.; Pigott, T. A systematic review of the effectiveness of Pilates on pain, disability, physical function, and quality of life in older adults with chronic musculoskeletal conditions. Musculoskeletal care 2022, 20, 10–30. [Google Scholar] [CrossRef]
- Cramer, H.; Klose, P.; Brinkhaus, B.; Michalsen, A.; Dobos, G. Effects of yoga on chronic neck pain: a systematic review and meta-analysis. Clin Rehabil 2017, 31, 1457–1465. [Google Scholar] [CrossRef]
- Tul, Y.; Unruh, A.; Dick, B.D. Yoga for chronic pain management: a qualitative exploration. Scandinavian journal of caring sciences 2011, 25, 435–443. [Google Scholar] [CrossRef]
- Bai, Z.; Guan, Z.; Fan, Y.; Liu, C.; Yang, K.; Ma, B.; Wu, B. The effects of qigong for adults with chronic pain: systematic review and meta-analysis. The American journal of Chinese medicine 2015, 43, 1525–1539. [Google Scholar] [CrossRef]
- Li, J.; Yu, F.; Huang, N.; Lu, J.; Xu, W.; Liu, N. Effect of Baduanjin exercise on patients with chronic heart failure: protocol for a systematic review and meta-analysis. BMJ open 2019, 9, e028771. [Google Scholar] [CrossRef]
Figure 1.
Study flow diagram.
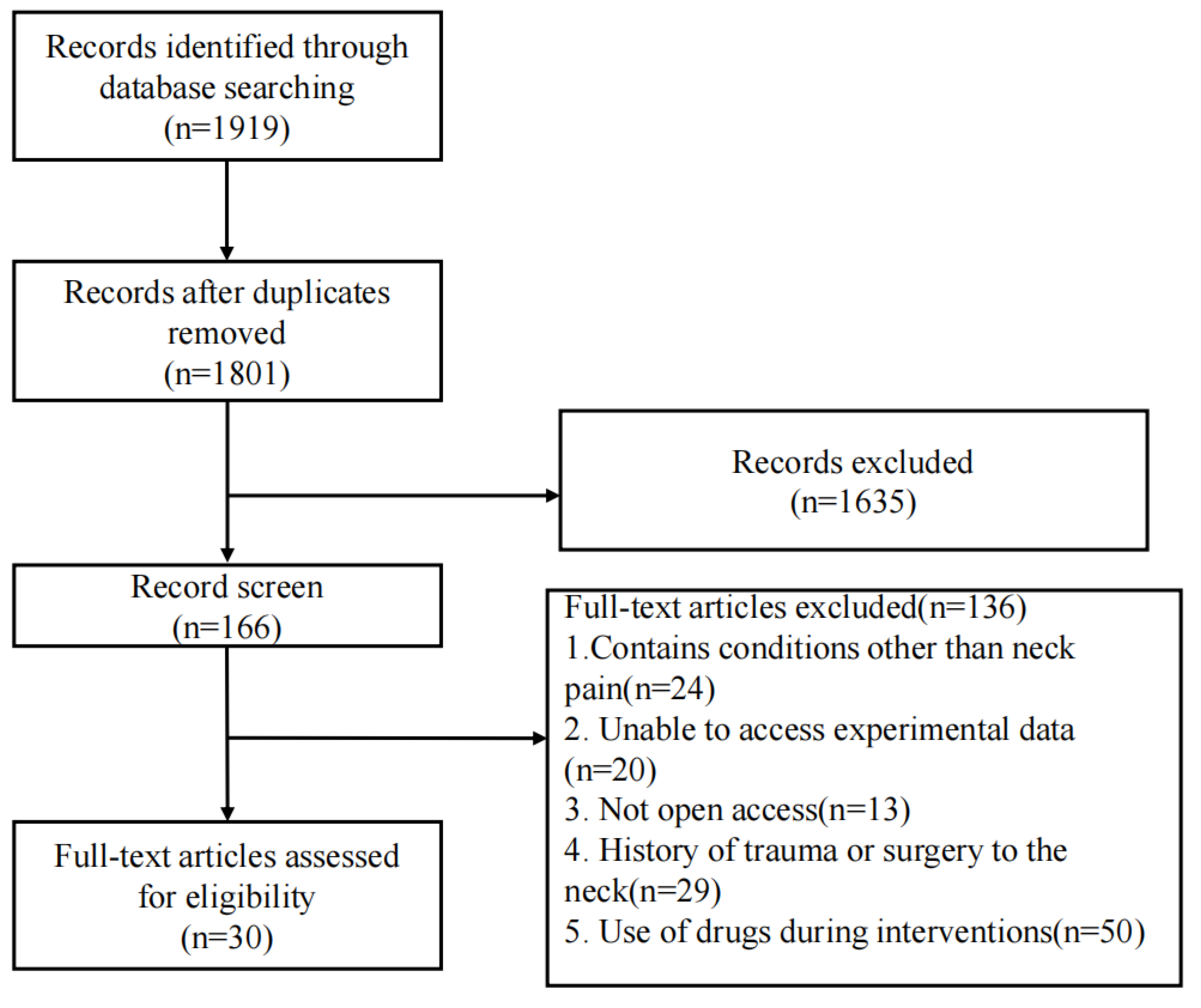
Figure 2.
Schematic of Cochrane bias risk assessment.
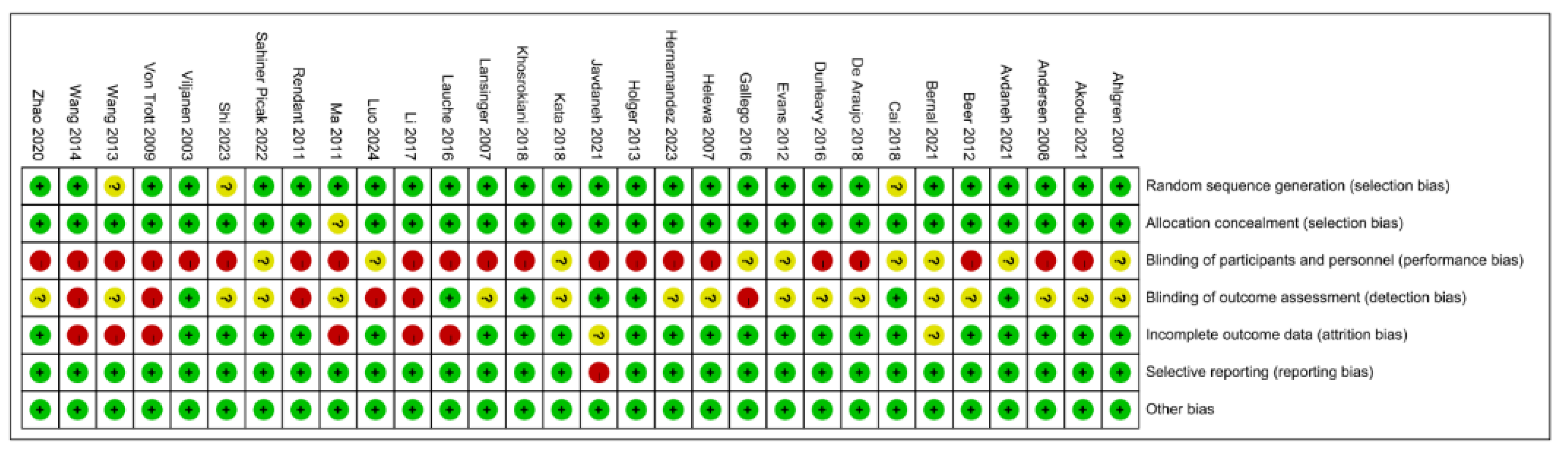
Figure 3.
Schematic of Cochrane bias risk assessment.
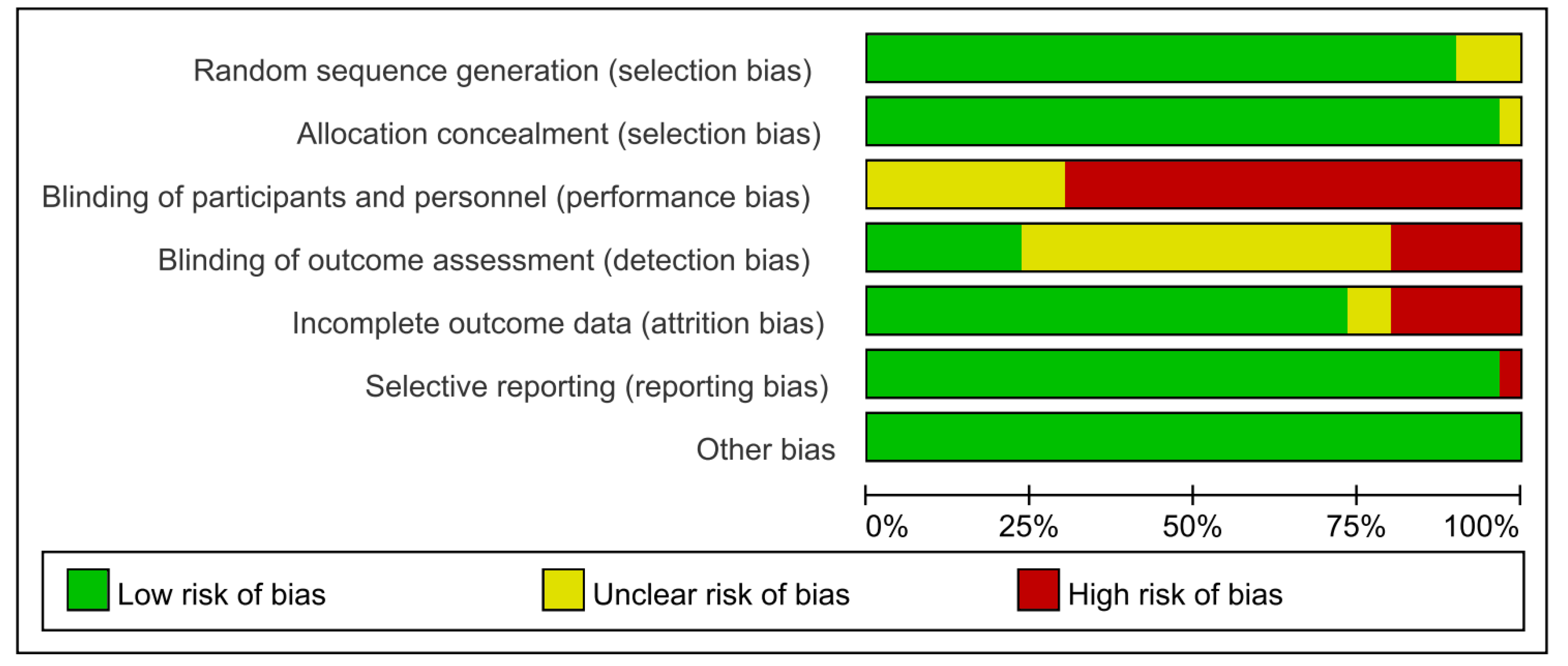
Figure 4.
The effect of different exercise methods on neck pain in NSNP patients.
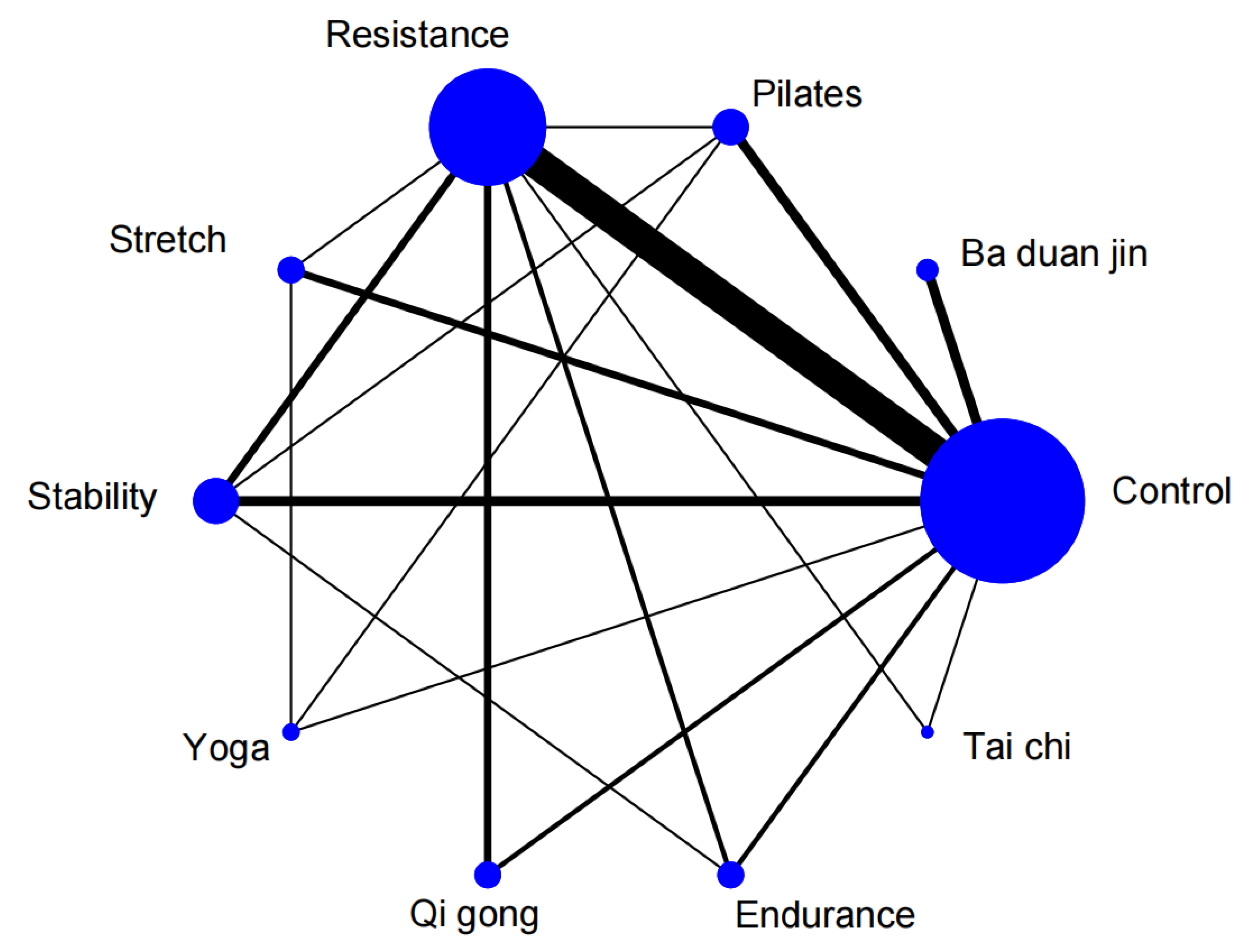
Figure 5.
The effect of different exercise methods on in dysfunction NSNP patients.
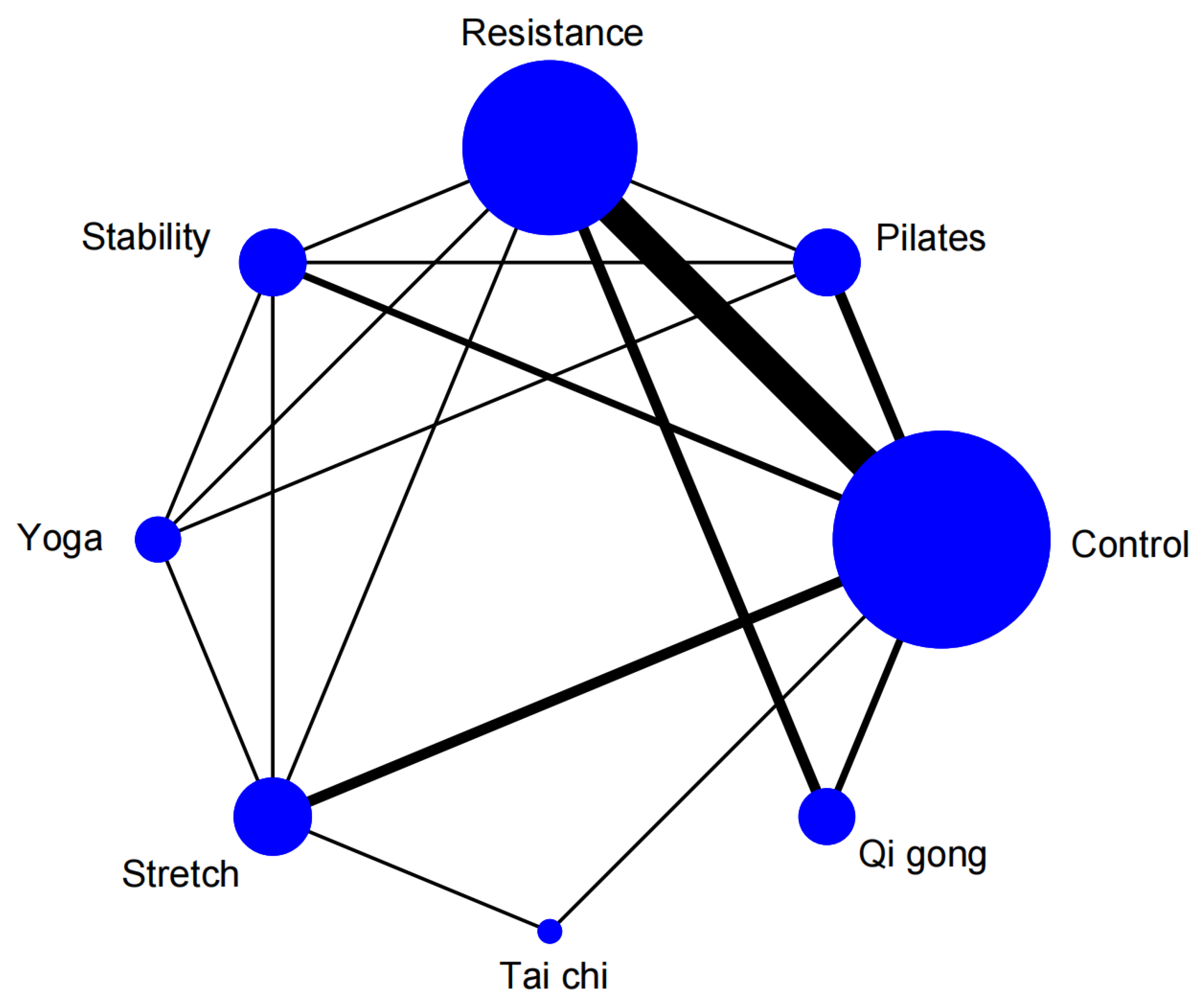
Figure 6.
The effect of different exercise methods on in life quality NSNP patients.
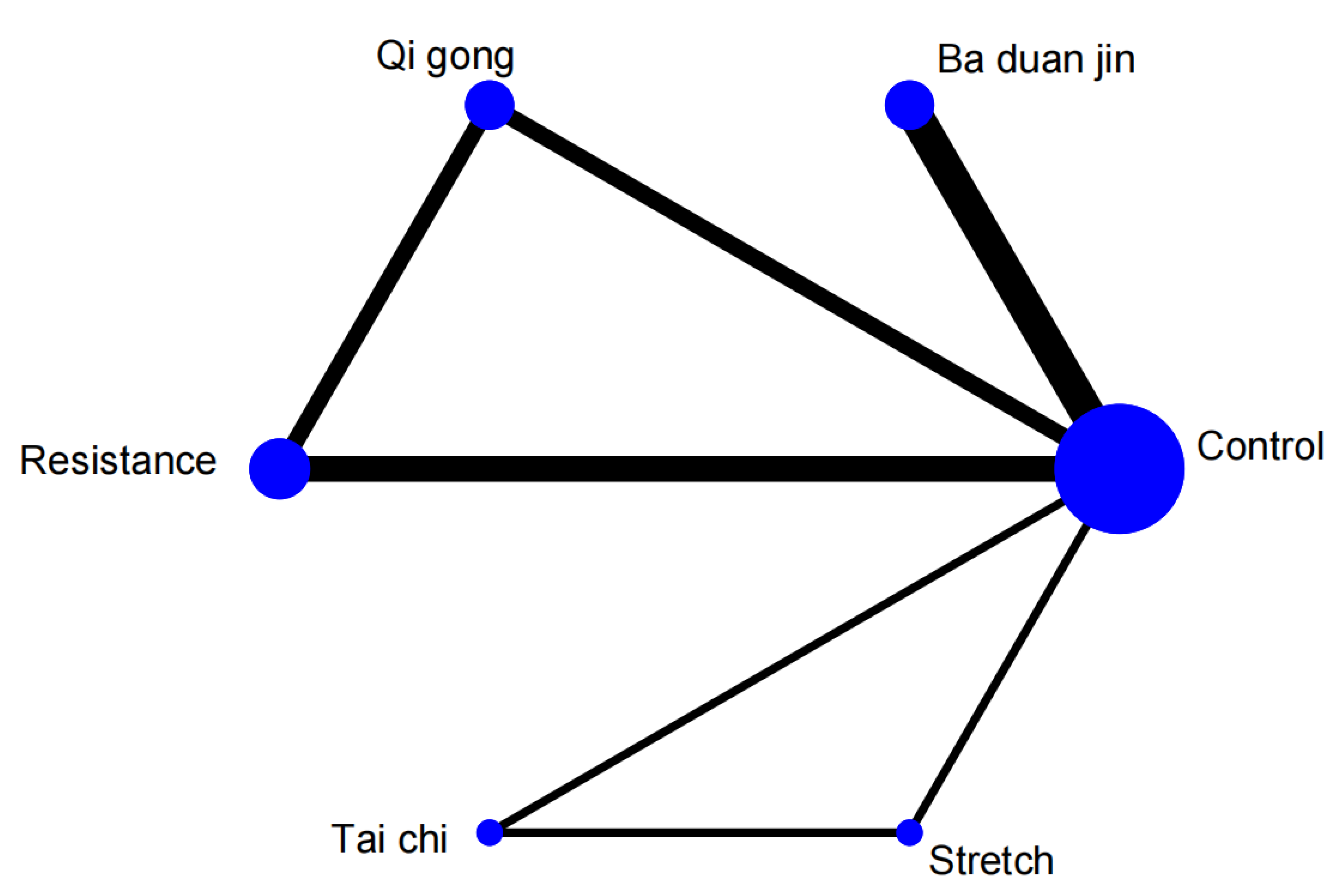
Figure 7.
Efficacy of different exercise modalities.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



