
Submitted:
10 January 2025
Posted:
10 January 2025
You are already at the latest version
Abstract
Introduction: Inappropriate antibiotic use is a big driver of bacterial antimicrobial resistance, and an increasing problem worldwide. Antibiotic use has sometimes been found to be more frequent by patients without malaria than patients with malaria. However, much uncertainty still exists, especially in places with varying malaria prevalence. In this study, the residuals of commonly used antibiotics in Tanzania were measured in samples collected from subjects living in three regions with different malaria epidemiology. Methods: A cross sectional household survey was conducted in 2015 to assess antimalarial medicine use in a population of 6000 individuals in three regions. Antibiotics residuals were measured in dried blood spots of a subset of people using broad-range tandem mass spectrometry technology. Risk factors for presence of antibiotic residuals were evaluated, including household healthcare seeking behaviors, malaria testing and other potential variables. Results: The overall prevalence of residual antibiotics in blood in the studied population was 14.4% (438/3036) with 95% CI of 11.4 – 15.8%. Stratifying by malaria transmission intensity, the antibiotic prevalence was 17.2% (95% CI: 12.9 - 17.2%) in Mwanza (low), 14.6% (95% CI: 10.6-15.0 %) in Mbeya (moderate), and 11.2% (95% CI: 7.9–11.6%) in Mtwara (high). Trimethoprim was the medication most often detected (6.1%) followed by sulfamethoxazole (4.4%), and penicillin V (0.001%).
Keywords:
Antimicrobial resistance (AMR)
; Community survey
; Dried Blood Spot (DBS)
; Drug pressure
; Residual antibiotics
; Tanzania
1. Introduction
Tanzania has made notable strides in controlling malaria, with Malaria Indicator Survey reports showing a significant decline in prevalence among children under five years, from 15% in 2015 to 7.9% in 2022 (Ministry of Health (MoH) [Tanzania Mainland], 2023). This progress is largely attributed to a combination of vector control strategies (Matindo et al., 2022), preventive therapies (Makenga et al., 2023), and improved diagnostics, notably the use of malaria rapid diagnostic tests (mRDTs) (Goodman et al., 2024). However, research has shown that the use of mRDTs has led to increased antibiotic prescriptions for negative results due to insufficient guidance on non-malaria fevers and lack of diagnostic support for distinguishing viral and bacterial infections (Hopkins et al., 2017) (Van de Maat et al., 2021, Mbwasi et al., 2020, Mabilika et al., 2022). As malaria rates continue to decline, especially in low-endemicity regions, the challenge of managing non-malarial fevers without over-relying on antibiotics is critical in preventing antimicrobial resistance (AMR). In 2019, deaths from AMR worldwide surpassed those from both HIV/AIDS and malaria combined, highlighting AMR’s escalating impact on global health (Murray et al., 2022). This crisis threatens to undermine decades of medical progress, making routine surgeries, cancer treatments, and even common infections far more dangerous (Ahmed et al., 2024). The World Health Organization (WHO) has identified AMR as one of the top ten global health threats, calling for immediate action to combat the spread of resistant bacteria (Organization, 2014). Such actions include monitoring antibiotic use in regions with different disease burdens, such as areas with varying levels of malaria endemicity, and strengthening antibiotic stewardship to ensure responsible use of antimicrobials (Rautman et al., 2024, Browne et al., 2021). In Tanzania, addressing the factors driving antibiotic misuse is crucial in both high and low malaria-endemic regions to prevent the acceleration of AMR.
This research builds on the earlier Antimalarial Concentration study, which sought to determine the prevalence and factors linked to residual antimalarial drugs in blood samples of the population (Gallay et al., 2018b). In that study, the prevalence of residual antimalarials was 20.8%. The current follow-up study aimed to examine the same blood samples for the presence of residual antibiotics. The primary objective is to evaluate the prevalence of residual antibiotics in community blood samples and identify the risk factors associated with exposure. Additionally, this study seeks to explore how antibiotic exposure prevalence differs across low, moderate, and high malaria endemicity regions in Tanzania.
2. Material and Methods
2.1. Study Design, Setting and Population
A household cross-sectional survey, including interviews and dried blood spot (DBS) sample collection, was conducted after the rainy season. Laboratory analysis of the blood samples was performed to quantify residual antibiotics, which were then examined alongside individual and household-level variables collected during the survey. The survey was conducted between May and August 2015 across three Tanzanian regions with differing levels of malaria endemicity: Mtwara (20%) and Mwanza (15%) representing moderate to high endemicity, and the Mbeya-Songwe region, with less than 1% prevalence, classified as low endemicity (Ministry of Health, 2016). Mtwara and Mwanza are characterized by tropical climates, whereas Mbeya-Songwe has a temperate climate. In each region, both urban and rural councils were included in the survey.
2.2. Sample Size, Study Sampling and Data Collection
As a secondary analysis, random selection of 3,036 DBS samples from the main study (Gallay et al., 2018b) were conducted from a pool of 6,391 samples. The selection of 3,036 samples was made to achieve sufficient statistical power to detect a prevalence of 10% or higher of antibiotics found in the DBS, thus ensuring the reliability and accuracy of the study's findings (with a power of 80% and a confidence level of 95%), considering an estimated intracluster correlation coefficient of 0.0229. These calculations were performed using the epi.ssclus2estb function within the epiR package in R software (version 4.2.1).
The study selected one urban and two rural councils from each region, and within each council, three wards were randomly chosen proportionally to their population size. In each urban ward, four streets were randomly selected, while in each rural ward, two villages as well as two sub-villages per village we selected. From each street or sub-village, 20 households were randomly selected and up to six participants were randomly selected in each sampled household until a sample of 60 individuals per sub-village/street was reached, resulting in 240 individuals sampled per ward. Within each household, all individuals were given the opportunity to participate, excluding those with severe illnesses requiring immediate referral and infants under three months of age. Interviews were conducted with a questionnaire in Swahili, starting with the head of household. The questions included information on the time to the closest health facility and the closest pharmacy or drug retailer. Randomly selected members were then asked about demographic information, history of fever in the previous two weeks, health-seeking behavior, as well as history of anti-malarial use in the previous months. Blood samples were collected from all participants using filter paper. To reach the sample size for the current sub-study, random sampling proportional to the number of samples collected in each region was employed, ensuring equal distribution across all study areas from the main study's 6,391 DBS samples. Further details on the sampling and data collection are provided elsewhere (Gallay et al., 2018a).
2.3. Laboratory Procedures
Capillary blood was collected on-site from all participants for direct mRDTs analysis (ParaHIT-f test, Span diagnostic Ltd, Surat, India, detecting HRP-2 antigens) and 4 drops were applied on filter paper cards (FTA DMPK-B cards, Whatman, GE Healthcare) for subsequent quantification of antimalarials and antibiotics in the laboratory. The DBS samples were dried at room temperature for at least two hours before being placed in a re-sealable plastic bag with desiccant and stored in a -10°C freezer at the end of the day at the study site. Samples were then transferred to a -80°C freezer at the Ifakara Health Institute within one month of collection and finally to the University Hospital of Lausanne, Switzerland, for analysis. The concentrations of seven antimalarials and two active metabolites were analyzed in the DBS samples using a liquid chromatography coupled with tandem mass spectrometry (LC-MS/MS) method specifically adapted for DBS samples (Gallay et al., 2018c). The method was further adapted and validated for the analysis of 15 common antibiotics and demonstrated good performance in terms of sensitivity, trueness and precision. All analytes were stable when stored for 24 hours at room temperature and at 37°C. Stability was also observed when replicating the study's storage and transportation conditions. The antibiotics quantified included amoxicillin, ampicillin, cloxacillin, penicillin G, penicillin V, ceftriaxone, cephalexin, trimethoprim, sulfamethoxazole, azithromycin, erythromycin, doxycycline, ciprofloxacin, metronidazole and chloramphenicol.
2.4. Statistical Analysis
Questionnaires were designed using Open Data Kit and data was stored on the ODK Aggregate data repository at the end of each survey day. Data cleaning and analysis were conducted using R (version 4.2.1). All analysis variables were summarized using common summary statistics appropriate to the variable type (Table 1). A univariable and multivariable mixed effects logistic regression model (lme4 package) was used to identify factors associated with the presence of antibiotics in the blood, and odds ratio (OR), its 95% confidence interval (CI) and p-value reported. Ward was included as a random effect in all analyses to account for clustering of observations. Statistical significance was determined by a p-value ≤ 0.05.
3. Results
3.1. Population Characteristics in the Household Surveys
The analysis included 3036 individuals, with 2030 individuals (66.9%) residing in rural and 1003 (33.1%) in urban settings. The median age of the study subjects was 17 years, ranging from 3 months to 100 years. Females accounted for 55.1% of the participants, while the predominant age group (39%) was 25 years and above. Approximately half (57.6%) of the participants lived less than one hour from government health facilities and 16.3% reported having experienced fever in the past two weeks. Among the subjects surveyed, 16.9% tested positive for malaria rapid diagnostic tests (mRDT) (Table 2).
3.2. Prevalence of Antibiotics in the Blood of the Surveyed Population
The overall prevalence of residual antibiotics in the DBS of the studied population was 14.4%. Among these, the most prevalent antibiotic was trimethoprim, with a prevalence of 5.9%, followed by sulfamethoxazole (4.5%), and metronidazole (2.4%) (Figure 1). The proportions of individuals with antibiotics found in their blood were as follows: 8.7% had 1 antibiotic, 4.7% had 2 antibiotics, 1.0% had 3 antibiotics, and 0.1% had 4 antibiotics. The overall prevalence of detected antibiotics in blood varied across regions: in Mwanza, it reached 17.2%, while in Mbeya, it was 14.6%, and in Mtwara, at 11.2%.
The analysis of the studied regions shows varying proportions of individuals with antibiotics, antimalarials, or both in their blood (Figure 2). Antimalarial detection rates were highest in Mwanza (22.4%), followed by Mtwara (15.2%) and Mbeya (9.6%). These detection rates correspond to malaria prevalence of 20.5% in Mwanza, 24.3% in Mtwara, and 4.6% in Mbeya, based on mRDT results obtained during the survey period. Figure 1: Antibiotics Detected in DBS across study regions, Tanzania, 2015.
The prevalence of residual antibiotics varied significantly across age groups: 17.1% in children aged 0-4 years, 16.0% in adults aged 25 and older, 12.6% in young adults aged 15-24, and 11.9% in children aged 5-14. Individuals living within one hour of a government healthcare facility had a prevalence of 15.3%. In contrast, those residing near non-government health facilities showed a prevalence of 17.8% for the same distance category. Additionally, the prevalence among individuals with a negative malaria test was notably higher at 15.2%, compared to 9.6% for those with a positive test result. Statistically significant differences among these groups are highlighted in Table 3.
3.3. Factors Associated with the Presence of Antibiotics
Several factors were associated with higher odds of having residual antibiotics in blood samples. Females were more likely to have antibiotics in their blood compared to males (OR = 1.30, 95% CI: 1.05–1.61). Individuals who tested negative for malaria had higher odds of residual antibiotics compared to those who tested positive (OR = 1.46, 95% CI: 1.04–2.06). Additionally, individuals with antimalarial drugs in their blood were more likely to have antibiotics detected than those without antimalarial drugs (OR = 1.37, 95% CI: 1.06–1.77). Conversely, certain demographic and travel-related factors were associated with lower odds of residual antibiotics. Individuals aged 5-14 years demonstrated 44% lower odds (OR = 0.66, 95% CI: 0.48-0.91) and 15-24 years 43% lower odds (OR = 0.67, 95% CI: 0.46-0.98) of having antibiotics in their blood as compared to children aged 0-4 years. Additionally, individuals who had a travel time to non-governmental healthcare facilities of more than 1 hour had lower odds (OR = 0.61, 95% CI: 0.42-0.88). No significant associations were found for the other variables (Table 2).
4. Discussion
This study investigates the prevalence and predictors of antibiotics detected in the DBS among Tanzanian population across regions with varying malaria transmission rates. Using a highly sensitive LC-MS/MS laboratory method, the study accurately quantified residual antibiotics. In the surveyed regions, 14% of participants had detectable residual antibiotics, with trimethoprim and sulfamethoxazole being the most prevalent, aligning with findings from previous research (Lotto et al., 2024). Several factors were associated with higher odds of residual antibiotics in blood samples, including being female, testing negative for malaria, and having antimalarial in the bloodstream.
Healthcare providers might be prescribing both medications to address potential dual infections, driven by the need for timely intervention in areas with elevated malaria prevalence (Kanan et al., 2023). This is evident in a study by (Makanjuola and Taylor-Robinson, 2020) which showed that Individuals with detectable antimalarial drugs in their blood were more likely to also have antibiotics present, indicating concurrent medication use, a practice common in malaria-endemic regions with limited diagnostic facilities. Similarly, another study highlighted the frequent co-prescription of antibiotics with antimalarial drugs, indicating a need to address irrational prescribing practices (Ampadu et al., 2019). Moreover, a study by (D'Acremont et al., 2011b, D'Acremont et al., 2011a) reported a significant increase in antibiotic prescriptions, rising from 49% before the introduction of mRDTs to 72% after their implementation (RR = 1.47, 95% CI 1.37–1.59). Understanding the differential diagnosis of fever in patients who test negative with mRDTs is essential for designing targeted interventions that encourage appropriate antibiotic use and reduce unnecessary exposure within the population.
A study conducted in the Mwanza region in Nyamagana, Ilemela, and Sengerema districts, as well as in other regions, revealed several factors contributing to poor dispensing practices, including pressure from customers, profit-making orientation of drug dispensers, and customers' economic circumstances (Ndaki et al., 2023, Ndaki et al., 2021). A study also identified a widespread willingness to dispense antibiotics without a prescription in community pharmacies and accredited drug-dispensing outlets in the area (Ndaki et al., 2022). These findings emphasize the importance of addressing the level of informal sector accurate diagnosis and careful drug use to combat inappropriate dispensing practices and antibiotic reliance in the region.
Women exhibited a higher prevalence of residual antibiotics (16.1%) compared to men (12.4%), a finding that aligns with a meta-analysis conducted in nine high-income countries (Schröder et al., 2016). A similar pattern was observed in Bangladesh, where women were more likely to receive antibiotic prescriptions than men (OR = 4.04, 95% CI 1.55, 10.55) (Rousham et al., 2023). This discrepancy can be attributed to the fact that women are more prone to infections such as urinary or gynecological conditions, which often result in higher antibiotic prescriptions (Abou Heidar et al., 2019).
The current study builds on these findings by providing insights into antibiotic exposure across different age groups. Individuals aged 10-14 and 15-24, as well as those who reported no illness in the previous two weeks, had lower odds of having residual antibiotics in their blood. This may be due to the lower morbidity rates from infectious diseases in individuals aged 10-24 compared to younger children under five (Masquelier et al., 2018) (Patton et al., 2016).
This study possesses several scientific strengths. Firstly, it employed LC-MS/MS technology, which allowed for the precise measurement of antibiotic concentrations in blood samples. Additionally, the inclusion of a representative sample of the general population enabled a comprehensive assessment of antibiotic exposure across diverse demographic groups. Through capturing not only prescribed antibiotics from healthcare settings but also those obtained through self-medication, the study provides a more accurate estimate of overall antibiotic exposure. Furthermore, the analysis of a broad range of commonly used antibiotics strengthens the validity of the findings, offering valuable insights into the multiple pathways of antibiotic exposure in the population.
This study has several limitations. Key variables such as socioeconomic status, education level, and marital status, which have been shown to affect antibiotic exposure in previous studies (Sun et al., 2022, Guo et al., 2022, Iskandar et al., 2021) were not collected in this study. Additionally, the findings are specific to the studied regions and may not be generalizable to other settings or populations. Prevalence rates of antibiotic detection and associated risk factors can differ across geographic locations and demographic groups, necessitating caution when extrapolating these results to other contexts.
In conclusion, this study identifies a complex relationship between antibiotics and malaria endemicity settings. While the prevalence of residual antibiotics does not directly align with malaria transmission rates, the findings suggest that healthcare provider practices, particularly the co-prescription of antibiotics and antimalarials, play a significant role. The higher odds of antibiotic detection among malaria-negative individuals also point to the need for improved diagnostic capacity to reduce unnecessary antibiotic use. These insights are important for designing targeted interventions that balance effective malaria management with the judicious use of antibiotics, ultimately mitigating the risk of antimicrobial resistance in malaria-endemic regions.
Author Contributions
B.G. conceptualized the project and acquired the funding. J.G., M.Z. developed the study protocol and data collection plan. J.G., M.Z. collected the data and performed data quality assurance. T.L., B.T. and L.A.D. conducted the laboratory analyses. T.L. and A.K. conducted the statistical analysis and drafted the manuscript. B.G., J.G. provided critical review of the manuscript.
Funding
The Swiss National Science Foundation (SNSF) under grant number 320030_149597 funded this study.
Data Availability Statement
All data generated or analyzed during this study are available from the corresponding author upon reasonable request.
Acknowledgements
The authors sincerely thank all the research participants and the government entities in Tanzania for their support and assistance in facilitating access to the study sites. We are also deeply grateful to the field staff for their dedication to data collection and to the laboratory team at Lausanne University Hospital for their great work in analyzing the samples. Furthermore, we extend our appreciation to Dr. Rainer Tan for his invaluable feedback and thoughtful comments on our manuscript.
Conflicts of Interest
The authors declare no competing interests.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and approved by the following ethical committees: the Ifakara Health Institute (IHI/IRB/No: 20-2020), the National Institute for Medical Research in Tanzania (NIMR/HQ/R.8a/Vol. IX/3463), and the Ethikkommission Nordwest- und Zentralschweiz in Switzerland (AO_2020-00050). Written informed consent was obtained in Swahili from all adult participants. An adult guardian aged 18 years or older provided written informed consent. Additionally, children aged 12 years and older were required to provide written assent. For individuals unable to read or write, an impartial witness was present to provide additional verification and signed the consent forms.
References
- Abou Heidar, N. F., Degheili, J. A., Yacoubian, A. A. & Khauli, R. B. Management of urinary tract infection in women: A practical approach for everyday practice. Urology annals, 2019, 11, 339.
- Ahmed, S. K., Hussein, S., Qurbani, K., Ibrahim, R. H., Fareeq, A., Mahmood, K. A. & Mohamed, M. G. Antimicrobial resistance: Impacts, challenges, and future prospects. Journal of Medicine, Surgery, and Public Health, 2024, 2, 100081.
- Ampadu, H. H. , Asante, K. P., Bosomprah, S., Akakpo, S., Hugo, P., Gardarsdottir, H., Leufkens, H. G. M., Kajungu, D. & Dodoo, A. N. O. Prescribing patterns and compliance with World Health Organization recommendations for the management of severe malaria: a modified cohort event monitoring study in public health facilities in Ghana and Uganda. Malaria Journal, 2019, 18, 36. [Google Scholar] [PubMed]
- Browne, A. J., Chipeta, M. G., Haines-Woodhouse, G., Kumaran, E. P. A., Hamadani, B. H. K., Zaraa, S., Henry, N. J., Deshpande, A., Reiner, R. C., JR., Day, N. P. J., et al. Global antibiotic consumption and usage in humans, 2000–18: a spatial modelling study. The Lancet Planetary Health 2021, 5, e893–e904.
- D'acremont, V., Kahama-Maro, J., Swai, N., Mtasiwa, D., Genton, B. & Lengeler, C. Reduction of anti-malarial consumption after rapid diagnostic tests implementation in Dar es Salaam: a before-after and cluster randomized controlled study. Malar J, 2011, 10, 107.
- D'acremont, V., Kahama-Maro, J., Swai, N., Mtasiwa, D., Genton, B. & Lengeler, C. Reduction of anti-malarial consumption after rapid diagnostic tests implementation in Dar es Salaam: a before-after and cluster randomized controlled study. Malaria Journal, 2011, 10, 1-16.
- Gallay, J., Mosha, D., Lutahakana, E., Mazuguni, F., Zuakulu, M., Decosterd, L. A., GENTON, B. & Pothin, E. Appropriateness of malaria diagnosis and treatment for fever episodes according to patient history and anti-malarial blood measurement: a cross-sectional survey from Tanzania. Malaria journal, 2018, 17, 1-13.
- Gallay, J., Pothin, E., Mosha, D., Lutahakana, E., Mazuguni, F., Zuakulu, M., Decosterd, L. A. & Genton, B. Predictors of residual antimalarial drugs in the blood in community surveys in Tanzania. PloS one, 2018, 13, e0202745.
- Gallay, J., Prod’hom, S., Mercier, T., Bardinet, C., Spaggiari, D., Pothin, E., Buclin, T., Genton, B. & Decosterd, L. A. LC–MS/MS method for the simultaneous analysis of seven antimalarials and two active metabolites in dried blood spots for applications in field trials: Analytical and clinical validation. Journal of pharmaceutical and biomedical analysis, 2018, 154, 263-277.
- Goodman, C. , Tougher, S., Shang, T. J. & Visser, T. Improving malaria case management with artemisinin-based combination therapies and malaria rapid diagnostic tests in private medicine retail outlets in sub-Saharan Africa: a systematic review. Plos one, 2024, 19, e0286718. [Google Scholar] [PubMed]
- Guo, H., Hildon, Z. J.-L., Lye, D. C. B., Straughan, P. T. & Chow, A. 2022. The Associations between Poor Antibiotic and Antimicrobial Resistance Knowledge and Inappropriate Antibiotic Use in the General Population Are Modified by Age. Antibiotics, 11, 47.
- Hopkins, H. , Bruxvoort, K. J., Cairns, M. E., Chandler, C. I., Leurent, B., Ansah, E. K., Baiden, F., Baltzell, K. A., Björkman, A. & Burchett, H. E. 2017. Impact of introduction of rapid diagnostic tests for malaria on antibiotic prescribing: analysis of observational and randomised studies in public and private healthcare settings. bmj,.
- Iskandar, K. , Molinier, L., Hallit, S., Sartelli, M., Hardcastle, T. C., Haque, M., Lugova, H., Dhingra, S., Sharma, P. & Islam, S. 2021. Surveillance of antimicrobial resistance in low-and middle-income countries: a scattered picture. Antimicrobial Resistance & Infection Control,.
- Kanan, M. , Ramadan, M., Haif, H., Abdullah, B., Mubarak, J., Ahmad, W., Mari, S., Hassan, S., Eid, R. & Hasan, M. Empowering Low-and Middle-Income Countries to Combat AMR by Minimal Use of Antibiotics: A Way Forward. Antibiotics,.
- Lotto, T. , Renggli, S., Kaale, E., Masanja, H., Ternon, B., Décosterd, L. A., D'acremont, V., Genton, B. & Kulinkina, A. V. 2024. Prevalence and predictors of residual antibiotics in children’s blood in community settings in Tanzania. Clinical Microbiology and Infection.
- Mabilika, R. J. , Shirima, G. & Mpolya, E. 2022. Prevalence and Predictors of Antibiotic Prescriptions at Primary Healthcare Facilities in the Dodoma Region, Central Tanzania: A Retrospective, Cross-Sectional Study. Antibiotics,.
- Makanjuola, R. O. & Taylor-Robinson, A. W. 2020. Improving accuracy of malaria diagnosis in underserved rural and remote endemic areas of sub-Saharan Africa: a call to develop multiplexing rapid diagnostic tests. Scientifica,.
- Makenga, G. , Baraka, V., Francis, F., Nakato, S., Gesase, S., Mtove, G., Madebe, R., Kyaruzi, E., Minja, D. T. & Lusingu, J. P. 2023. Effectiveness and safety of intermittent preventive treatment with dihydroartemisinin–piperaquine or artesunate–amodiaquine for reducing malaria and related morbidities in schoolchildren in Tanzania: a randomised controlled trial. The Lancet Global Health, 2023, 11, e1277–e1289. [Google Scholar] [PubMed]
- Masquelier, B., Hug, L., Sharrow, D., You, D., Hogan, D., Hill, K., Liu, J., Pedersen, J. & Alkema, L. Global, regional, and national mortality trends in older children and young adolescents (5-14 years) from 1990 to 2016: an analysis of empirical data. Lancet Glob Health, 2018, 6, e1087-e1099.
- Matindo, A. Y. , Kalolo, A., Kengia, J. T., Kapologwe, N. A. & MUNISI, D. Z. 2022. The role of community participation in planning and executing malaria interventions: experience from implementation of biolarviciding for malaria vector control in Southern Tanzania. BioMed Research International, 2022. [Google Scholar]
- Mbwasi, R. , Mapunjo, S., Wittenauer, R., Valimba, R., Msovela, K., Werth, B. J., Khea, A. M., Nkiligi, E. A., Lusaya, E. & Stergachis, A. 2020. National consumption of antimicrobials in Tanzania: 2017–2019. Frontiers in Pharmacology,.
- Ministry of health (moh) [tanzania mainland], m. O. H. M. Z. , national bureau of statistics (nbs), office of the chief government statistician (ocgs), and icf. 2023. Tanzania Demographic and Health Survey and Malaria Indicator Survey 2022 Key Indicators Report. Dodoma, Tanzania, and Rockville, Maryland, USA: MoH, NBS, OCGS, and ICF.
- Ministry of health, c. D. , gender, elderly and children (mohcdgec) [tanzania mainland], ministry of health (moh) [zanzibar], national bureau of statistics (nbs), office of the chief government statistician (ocgs), and icf. 2016. Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) 2015-16. Dar es Salaam, Tanzania, and Rockville, Maryland, USA: MoHCDGEC, MoH, NBS, OCGS, and ICF.
- Murray, C. J. , Ikuta, K. S., Sharara, F., Swetschinski, L., Aguilar, G. R., Gray, A., Han, C., Bisignano, C., Rao, P. & Wool, E. 2022. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The Lancet, 2022, 399, 629–655. [Google Scholar]
- Ndaki, P. M. , Mushi, M. F., Mwanga, J. R., Konje, E. T., Mugassa, S., Manyiri, M. W., Mwita, S. M., Ntinginya, N. E., Mmbaga, B. T., Keenan, K., et al. 2022. Non-prescribed antibiotic dispensing practices for symptoms of urinary tract infection in community pharmacies and accredited drug dispensing outlets in Tanzania: a simulated clients approach. BMC Primary Care, 2022, 23, 287. [Google Scholar]
- Ndaki, P. M. , Mushi, M. F., Mwanga, J. R., Konje, E. T., Ntinginya, N. E., Mmbaga, B. T., Keenan, K., Sabiiti, W., Kesby, M., Benitez-Paez, F., et al. 2021. Dispensing Antibiotics without Prescription at Community Pharmacies and Accredited Drug Dispensing Outlets in Tanzania: A Cross-Sectional Study. Antibiotics (Basel),.
- Ndaki, P. M. , Mwanga, J. R., Mushi, M. F., Konje, E. T., Fredricks, K. J., Kesby, M., Sandeman, A., Mugassa, S., Manyiri, M. W., Loza, O., et al. Practices and motives behind antibiotics provision in drug outlets in Tanzania: A qualitative study. PLoS One, 2023, 18, e0290638. [Google Scholar] [CrossRef] [PubMed]
- Organization, W. H. 2014. Antimicrobial resistance: global report on surveillance, World Health Organization.
- Patton, G. C. , Sawyer, S. M., Santelli, J. S., Ross, D. A., Afifi, R., Allen, N. B., Arora, M., Azzopardi, P., Baldwin, W., Bonell, C., et al. Our future: a Lancet commission on adolescent health and wellbeing. Lancet, 2016, 387, 2423–2478. [Google Scholar] [CrossRef] [PubMed]
- Rautman, L. H., Eibach, D., Boateng, F. O., Akenten, C. W., Hanson, H., Maiga-Ascofaré, O., May, J. & Krumkamp, R. Modeling pediatric antibiotic use in an area of declining malaria prevalence. Scientific Reports, 2024, 14, 16431.
- Rousham, E. K., Nahar, P., Uddin, M. R., Islam, M. A., Nizame, F. A., Khisa, N., Akter, S. S., Munim, M. S., Rahman, M. & Unicomb, L. Gender and urban-rural influences on antibiotic purchasing and prescription use in retail drug shops: a one health study. BMC Public Health, 2023, 23, 229.
- Schröder, W., Sommer, H., Gladstone, B. P., Foschi, F., Hellman, J., Evengard, B. & Tacconelli, E. 2016. Gender differences in antibiotic prescribing in the community: a systematic review and meta-analysis. J Antimicrob Chemother, 71, 1800-6.
- Sun, R., Yao, T., Zhou, X., Harbarth, S. & Lin, L. Non-biomedical factors affecting antibiotic use in the community: a mixed-methods systematic review and meta-analysis. Clin Microbiol Infect, 2022, 28, 345-354.
- Van de Maat, J., de Santis, O., Luwanda, L., Tan, R. & Keitel, K. Primary Care Case Management of Febrile Children: Insights From the ePOCT Routine Care Cohort in Dar es Salaam, Tanzania. Frontiers in pediatrics, 2021, 9, 626386.
Figure 1.
Antibiotics Detected in DBS across study regions, Tanzania, 2015.

Figure 2.
Distribution of antibiotics and antimalarials detected in blood samples across studied regions.
Figure 2.
Distribution of antibiotics and antimalarials detected in blood samples across studied regions.
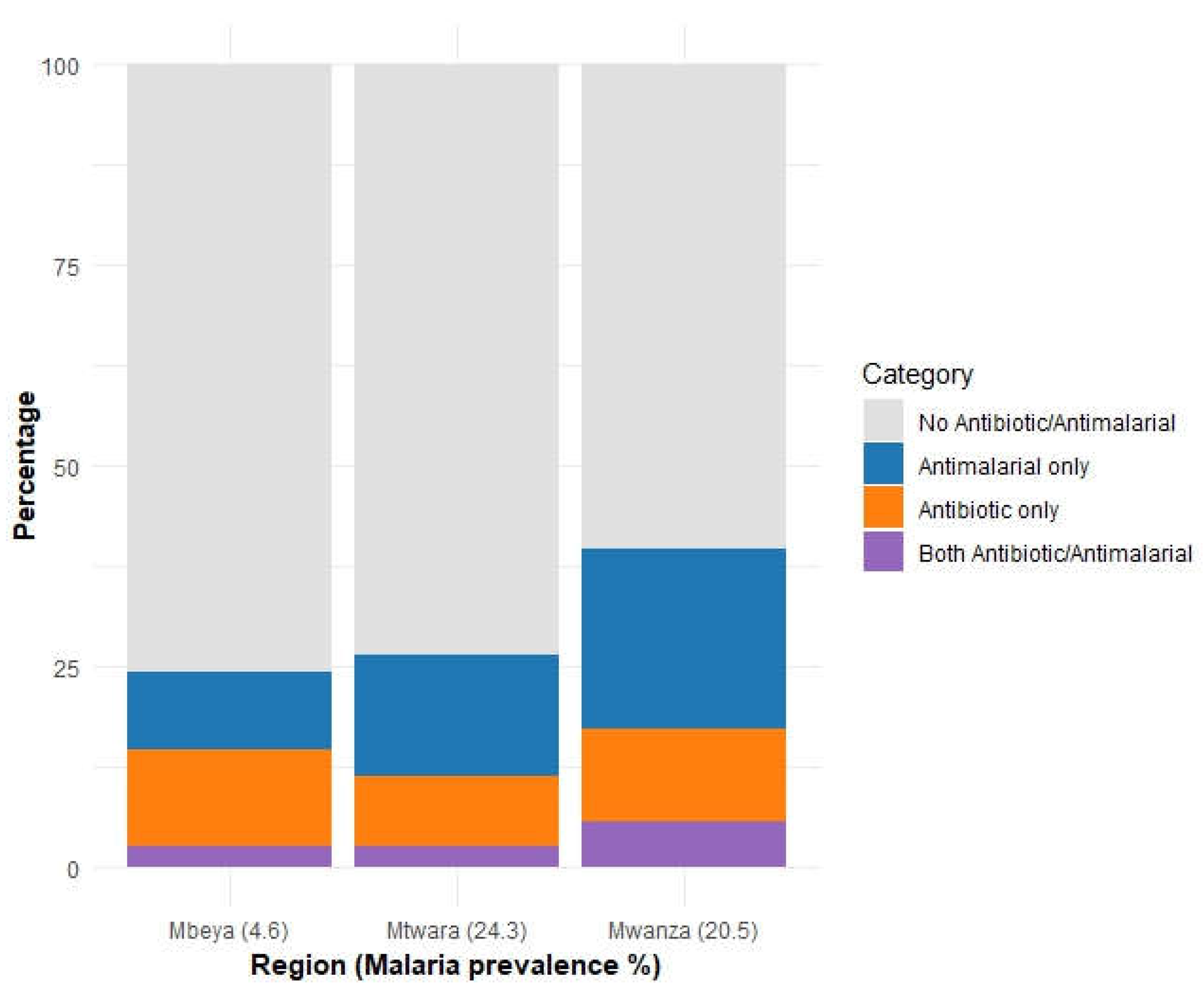

Table 1.
Summary of the variables used.
| Variable | Type | Definition |
| Outcome | ||
| Antibiotics in blood | Binary | Presence of any antibiotic(s) in the blood equal or above the limits of quantification |
| Participant information | ||
| Age (years) | Ordinal | Participant’s age, categorized as 0-4, 5-14, 15 – 24 and 25+ |
| Sex | Categorical | Categorized as male or female |
| Time to nearest government health care facilities | Ordinal | Time required to reach nearby government health facility, categorized as < 15 min, 15 min < 1hour, >=1, unknown |
| Time to nearest nongovernment hospital | Categorical | Time required to reach nearby nongovernment health facility, categorized as < 15 min, 15 min < 1hour, >=1, unknown |
| Time to nearest medical shop | Categorical | Time required to reach nearby medical shop, categorized as < 15 min, 15 min < 1hour, >=1, unknown |
| mRDT results on site | Categorical | Rapid malaria diagnostic test taken during the survey categorized as Positive, negative, not valid, missing |
| History of fever in the past 14 days | Categorical | Self-reported fever in past 14 days prior to the survey, categorized as yes, no, doesn’t know |
| Sought care for this fever | Categorical | Whether care was sought in case of fever, categorized as yes, no, doesn’t know |
| Time taken to travel to the provider | Categorical | Time required to reach health care provider, categorized as < 15 min, 15 min < 1hour, >=1, unknown |
| Malaria blood test performed | Categorical | Malaria diagnostic test performed when seeking care, categorized as? |
| Malaria test results | Categorical | Reported result of the malaria diagnostic test performed when seeking care, categorized as positive, negative & not valid |
Table 2.
Demographic information.
| Variable | Frequency | Percentage |
| Total Participants | 3036 | 100 |
| Sex | ||
| Male | 1359 | 44.80 |
| Female | 1674 | 55.10 |
| Missing | 3 | 0.10 |
| Age (Years) | ||
| 0-4 | 531 | 17.50 |
| 5 – 14 | 839 | 27.60 |
| 15-24 | 428 | 14.10 |
| 25+ | 1185 | 39.00 |
| Time to Government Health Facility | ||
| < 15 minutes | 811 | 26.70 |
| 15 minutes to < 1 hour | 1748 | 57.60 |
| 1 hour or more | 386 | 12.70 |
| Missing | 3 | 0.10 |
| Time to Non-Government Health Facility | ||
| < 15 minutes | 474 | 15.60 |
| 15 minutes to < 1 hour | 1041 | 34.30 |
| 1 hour or more | 431 | 14.20 |
| Missing | 3 | 0.10 |
| Time to Medicine Shops | ||
| < 15 minutes | 1353 | 44.60 |
| < 1 hour | 1262 | 41.60 |
| ≥ 1 hour | 418 | 8.50 |
| Missing | 3 | 0.10 |
| mRDT Result | ||
| Positive | 512 | 16.90 |
| Negative | 2500 | 82.20 |
| Missing | 24 | 2 |
| Had Fever in the Previous 2 Weeks | ||
| Yes | 494 | 16.30 |
| No | 2539 | 83.50 |
| Missing | 3 | 0.10 |
| Had Antimalarial in Blood | ||
| Yes | 599 | 19.7 |
| No | 2435 | 80.2 |
| Missing | 3 | 0.1 |
| Regions | ||
| Mbeya | 933 | 30.80 |
| Mtwara | 1000 | 32.90 |
| Mwanza | 1100 | 36.20 |
| Missing | 3 | 0.10 |
Table 3.
Factors Associated with Residual Antibiotics in Blood Samples among Participants.
| Variables |
Total participants N (%) |
Participants with antibiotic in the blood | ||||
| N (%) | Univariable analysis | Multivariable analysis | ||||
| ORs | p-value | OR (95% CI) | p-value | |||
| Total | 3036 | 438 (14.4) | ||||
| Sex | ||||||
| Male | 1359 (44.8) | 168 (12.4) | Ref | 1 | ||
| Female | 1674 (55.1) | 269 (16.1) | 1.33 (1.08 - 1.64) | 0.008 | 1.30 (1.05 –1.61) | 0.017 |
| Missing | 3 (0.1) | 1 (33.3) | ||||
| Age (Years) | ||||||
| 0-4 | 531 (17.5) | 91 (17.1) | Ref | -- | ||
| 5-14 | 839 (27.6) | 100 (11.9) | 0.64 (0.47-0.88) | 0.006 | 0.66 (0.48-0.91) | 0.011 |
| 15 - 24 | 428 (14.1) | 54 (12.6) | 0.65 (0.45-0.94) | 0.022 | 0.67 (0.46-0.98) | 0.039 |
| 25+ | 1185 (39.0) | 190 (16.0) | 0.94 (0.71 -1.25) | 0.682 | 0.93 (0.70-1.23) | 0.598 |
| Time to Government Health Facility | ||||||
| < 15 minutes | 811 (26.7) | 115 (14.2) | Ref | -- | -- | -- |
| 15 minutes to < 1 hour | 1748 (57.6) | 268 (15.3) | 1.13 (0.88 – 1.46) | 0.329 | 1.15 (0.87 – 1.51) | 0.322 |
| 1 hour or more | 386 (12.7) | 54 (11.4) | 0.75 (0.49 – 1.13) | 0.171 | 0.91 (0.59 – 1.39) | 0.659 |
| Missing | 3 (2) | 1 (33.3) | ||||
| Non-Government HF time | ||||||
| < 15 minutes | 474 (15.6) | 92 (19.4) | Ref | -- | -- | -- |
| 15 minutes to <1 hour | 1041 (34.3) | 185 (17.8) | 1.01 (0.74 – 1.37) | 0.967 | 1.03 (0.74-1.44) | 0.869 |
| 1 hour or more | 431 (14.2) | 160 (10.5) | 0.60 (0.40 – 0.92) | 0.018 | 0.61 (0.42-0.88) | 0.024 |
| Missing | 3 (2) | 1 (33.3) | ||||
| Time to medicine shops | ||||||
| < 15 minutes | 1353 (44.6) | 218 (16.1) | Ref | -- | -- | -- |
| <1 hour | 1262 (41.6) | 177 (14.0) | 0.98 (0.77 – 1.25) | 0.891 | 0.95 (0.73 – 1.24) | 0.721 |
| >=1 hour | 418 (8.5) | 42 (10.0) | 0.69 (0.44 – 1.10) | 0.118 | 0.89 (0.59 – 1.36) | 0.600 |
| Missing | 3 (2) | 1 (33.3) | ||||
| mRDT result | ||||||
| Positive | 512 (16.9) | 49 (9.6) | Ref | -- | -- | -- |
| Negative | 2500 (82.2) | 381 (15.2) | 1.57 (1.13 – 2.18) | 0.007 | 1.46 (1.04 – 2.06) | 0.029 |
| Missing | 24 (2) | 8 (33.3) | ||||
| Had fever in the previous 2 weeks | ||||||
| Yes | 494 (16.3) | 86 (17.4) | Ref | -- | -- | -- |
| No | 2539 (83.5) | 351 (13.8) | 0.75 (0.57 – 0.98) | 0.034 | 0.78 (0.59 – 1.03) | 0.083 |
| Missing | 3 (2) | 1 (33.3) | ||||
| Had antimalarial in blood | ||||||
| Yes | 599 (19.7) | 111 (18.5) | 1.48 (1.16-1.89) | 0.002 | 1.37 (1.06 – 1.77) | 0.014 |
| No | 2435 (80.2) | 327 (13.4) | -- | -- | -- | -- |
| Missing | 3 (0.1) | 0 | ||||
| Regions | ||||||
| Mbeya | 933 (30.8) | 136 (14.6) | -- | -- | -- | |
| Mtwara | 1000 (32.9) | 112 (11.2) | 0.79 (0.51 – 1.22) | 0.291 | 0.87 (0.58 – 1.28) | 0.476 |
| Mwanza | 1100 (36.2) | 189 (17.2) | 1.30 (0.85 – 1.98) | 0.222 | 1.17 (0.81 – 1.70) | 0.397 |
| Missing | 3 (0.1) | 1 (33.3) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



