Submitted:
09 January 2025
Posted:
09 January 2025
You are already at the latest version
Abstract
Renal masses are uncommon during pregnancy, they represent the most frequently encountered urological cancer in pregnant patients and require careful surgical planning. The introduction of robotic surgical systems aims to address these challenges by simplifying intra-corporeal suturing and reducing technical complexity. Robot-assisted laparoscopic renal surgery offers potential benefits over both open surgery and conventional laparoscopy, providing greater precision and reduced invasiveness, particularly in tumor excision and suturing. Although urological tumors during pregnancy are rare, early detection significantly improves outcomes by enabling intervention before the tumor advances and while the uterus remains relatively small. The decision regarding the timing and necessity of surgery in pregnant patients requires a careful assessment of maternal health, fetal development, and the progression of the disease. Risks for adverse pregnancy outcomes should be explained, and the patient’s decision about pregnancy termination should be considered. Radical nephrectomy or nephron-sparing surgery are essential treatments for management of renal tumors. Effective management demands close collaboration between a multidisciplinary team and the patient to ensure individualized care. The aim of this review was to evaluate the renal tumors during pregnancy in terms of epidemiology, risk factors, diagnosis and the safety of a Robot-assisted laparoscopic approach in the management of these tumors.
Keywords:
Pregnancy
; Renal Tumor
; Robotic surgery
; Management
; Renal cell carcinoma
; Laparoscopic surgery
1. Introduction
Robotic surgery during pregnancy is becoming increasingly prevalent due to the advantages of minimally invasive procedures [1]. Although renal cell tumors are uncommon during pregnancy, they represent the most frequently encountered urological cancer in pregnant patients and require careful surgical planning [1,2]. For localized renal tumors, partial nephrectomy (PN) is often recommended to preserve renal function. This approach is particularly suitable for patients with exophytic renal masses measuring less than 4 cm [3]. Laparoscopic partial nephrectomy (LPN) is gaining recognition as a minimally invasive and effective treatment [4]. However, the procedure presents challenges, such as the prolonged time required for tumor excision, hemostasis, and suturing, even for skilled surgeons [5]. The introduction of robotic surgical systems, such as the da Vinci platform, aims to address these challenges by simplifying intracorporeal suturing and reducing technical complexity [6]. Robot-assisted laparoscopic partial nephrectomy (RLPN) offers potential benefits over both open surgery and conventional laparoscopy, providing greater precision and reduced invasiveness, particularly in tumor excision and suturing [7]. Although urological tumors during pregnancy are rare, early detection significantly improves outcomes by enabling intervention before the tumor advances and while the uterus remains relatively small [8]. The aim of this review was to evaluate the renal tumors during pregnancy in terms of epidemiology, risk factors, diagnosis and the safety of a Robot-assisted laparoscopic approach in the management of this tumors.
2. Study Design and Selection Criteria
On 1 December 2024, a search of medical databases was performed to find articles which included the following key words: “pregnancy”, “obstetric”, “robotic”, “surgery”, “robot”, “robot-assisted”, “minimally procedures”, "da vinci" or “davinci”, “renal tumor”, “kidney tumor”, “management”, “renal cancer” and “renal cell carcinoma”, “Therapy”. MEDLINE, Web of Science, PubMed and Google Scholar were used to search for eligible articles published in literature. The search yielded 146 articles. Eligibility of the studies was independently reviewed by two authors (L.D. and V.S.). Studies were included that addressed non-obstetric transabdominal robotic surgery occurring during pregnancy. The main aim of the present narrative review was to identify the robotic surgery in the management of renal tumors. Therefore, studies including robotic partial nephrectomy or radical nephrectomy for renal masses were selected for this review. The reference lists of all included studies were examined to help identify studies not captured by the initial search. A total of 5 case studies were included in the final literature review (Figure 1).
3. Epidemiology and Etiology
The diagnosis of cancer during pregnancy is a rare event, with an estimated incidence of 1 in every 1,000 pregnancies [9]. Among the most frequently diagnosed gestational cancers are breast cancer, lymphoma, and cervical cancer [10]. Malignant ovarian tumors are less common, comprising approximately 5% of ovarian masses identified during pregnancy [10]. Renal masses detected during pregnancy are also uncommon, with only around 100 cases documented in the literature to date. Of these, approximately 50% are malignant, potentially influenced by hormonal and paracrine effects. Among benign renal masses, angiomyolipomas account for 23%, while oncocytomas are observed in 3-7% of cases [11]. However, the role of pregnancy-related hormonal changes in promoting the formation of malignant kidney cells remains uncertain. Urinary tract cancers during pregnancy are rare, with renal cell carcinoma (RCC) being the most frequently diagnosed urological malignancy. RCC accounts for about 3% of all cancers in the general population, and despite the trend of delayed childbirth, its incidence during pregnancy remains low [3]. The routine use of ultrasonography in antenatal care may contribute to the increased incidental detection of gestational RCC [12]. Fetal metastasis has primarily been reported in cases involving placental metastases, such as melanoma and lung cancer, and is associated with a poor prognosis [13]. Based on an analysis of gestational RCC cases reported since 2004, the median age at diagnosis is 33 years, with patients ranging from 20 to 52 years old [14]. RCC during pregnancy is most commonly diagnosed in the second trimester [12]. Several factors contribute to the development of renal tumors. Non-modifiable risk factors include age and male sex, while modifiable factors encompass obesity, smoking, and hypertension [14,15]. Obesity, in particular, has a strong association with RCC. In the VITAL study by Macleod et al. [16], individuals with a body mass index (BMI) of 35 kg/m² or higher exhibited a 71% greater risk of RCC compared to those with a BMI below 25 kg/m² . A meta-analysis of 14 studies further revealed a 7% increase in RCC risk for each unit increase in BMI [17]. This connection may stem from obesity-driven processes, such as increased cell proliferation, angiogenesis, and survival, influenced by elevated levels of gonadal steroids, adipokines, and insulin-like growth factors [1]. Hormonal and reproductive factors during pregnancy may also contribute to RCC development [18]. The gestational period is characterized by heightened levels of estrogen and progesterone, both of which have receptors present on normal and malignant renal cells [19]. Parity has been associated with RCC risk in cohort studies, though the exact mechanisms remain unclear. Hypertension is another independent risk factor for renal tumors, affecting about 18% of pregnant individuals diagnosed with the disease [20]. Studies, including the VITAL study, have identified hypertension as significantly increasing RCC risk (HR 1.70; 95% CI, 1.30-2.22) [16]. The combined presence of obesity, hypertension, and type 2 diabetes further amplifies RCC risk, with women exhibiting all three conditions facing a fourfold higher likelihood of developing the disease compared to those without comorbidities [16,21].
4. Diagnosis and Imaging
The detection of renal masses during pregnancy often occurs incidentally during ultrasound examinations performed for unrelated reasons, such as investigating hydronephrosis caused by non-neoplastic factors (e.g., kidney stones or ureteral compression) or ascending urinary tract infections [22]. Common symptoms include pain (50%), hematuria (37%), hypertension (12%), and the classic triad of hematuria, pain, and a palpable mass (21%). Hematuria in pregnancy is typically attributed to non-neoplastic conditions like infections, stones, bladder varices, or glomerulonephritis [23]. Other symptoms, such as fever (21%), weight loss (9%), or hemorrhagic shock due to tumor bleeding (3%), are less frequent, while rare presentations include hemolytic anemia, hypercalcemia, or ruptured tumor cysts. Five cases of metastatic disease during pregnancy have been documented, with most diagnoses occurring in the second or third trimester, while first-trimester cases are less common [24]. Diagnostic imaging during pregnancy is often restricted due to the potential risks associated with ionizing radiation from conventional radiography and CT (Computed Tomography) scans, which can lead to congenital anomalies, growth restrictions, or stillbirth [26]. Ultrasound and MRI (Magnetic Resonance Imaging), which are considered safe throughout pregnancy, are the preferred imaging methods. Ultrasound is particularly effective in identifying renal masses larger than 2 cm but has limitations in detecting smaller lesions or those that do not alter kidney contours. For lesions measuring 2 cm or less, CT and ultrasound sensitivity is approximately 94% and 79%, respectively [27]. Both CT and MRI exhibit nearly 100% accuracy for diagnosing renal tumors, with CT being the preferred imaging technique. CT scans that exclude the gravid uterus result in minimal fetal radiation exposure and are generally safe during pregnancy [28]. A single CT scan through the uterus exposes the fetus to a dose of up to 25 mGy, while abdominal or pelvic CTs expose the uterus to 18–25 mGy and are reserved for emergencies [27,28]. Radiation doses exceeding 50–100 mGy within two weeks post-conception may cause fetal loss or have no effect. During organogenesis (weeks 2–8), high doses (>200 mGy) could lead to anomalies, while lower doses (>60 mGy) between weeks 8–15 might result in intellectual disabilities or microcephaly [29]. Radiation exposures of 10–20 mGy may double the lifetime risk of leukemia, and fetal thyroid or gonadal damage is a theoretical concern with certain radiation types [30]. MRI provides a reliable, though costlier, alternative to CT for evaluating renal masses in pregnancy, offering detailed information on tumor size, local extension, and potential vascular involvement. While gadolinium, a contrast agent, crosses the placental barrier, no significant fetal harm has been reported, although it could potentially induce fetal hypothyroidism [31]. Whole-body MRI is gaining recognition as a method for cancer staging, with sensitivity comparable to skeletal scintigraphy for detecting bone metastases [32]. However, its ability to detect pulmonary lesions compared to chest CT remains uncertain. The European Society of Radiology supports MRI use throughout pregnancy in all stages [28,31]. The differential diagnosis for renal masses includes inflammatory, cystic, benign, and malignant lesions beyond renal cell carcinoma. Preoperative biopsy to confirm renal mass diagnosis during pregnancy is rare, but tumor core biopsy offers high accuracy in identifying malignancy [33]. Biopsy is considered for indeterminate renal masses, suspected metastasis, or before initiating treatment, although evidence on the safety of ultrasound-guided biopsy during pregnancy is limited. Typically, definitive diagnosis relies on histopathological evaluation of surgical specimens [34,35].
5. Robotic Management
Urological tumors during pregnancy are uncommon, but early diagnosis can significantly improve outcomes by allowing interventions before tumor progression and when the uterus is smaller [36]. Around 132 cases of renal masses have been documented in literature, including 93 cases of RCC. Loughlin et al. reviewed the management of solid renal masses in pregnancy, advising radical surgery during the first trimester or after 28 weeks of gestation in the second trimester [37]. For masses diagnosed in the third trimester, surgical timing depends on lung maturity, but for those near term, surgery can be postponed until after delivery. Some experts suggest immediate nephrectomy regardless of pregnancy stage, prioritizing maternal health [14,38,39]. Surgical intervention during the second trimester is generally considered safer, as the risk of spontaneous abortion or congenital abnormalities is higher in the first trimester, while preterm labor is more likely in the third [35,40]. Laparoscopic techniques have transformed minimally invasive surgery, with robotic approaches emerging as a cutting-edge option [3]. Robotic surgery, suitable even during pregnancy, offers advantages like enhanced visualization and precision, particularly when operating alongside a gravid uterus [41]. Our review highlights the limited application of robotic surgery for renal masses in pregnant patients, with only five documented cases [1,42-45] in the last two decades (Table 1). Initial abdominal access can be safely achieved using techniques such as open (Hasson), Veress needle, or optical trocar, adjusted based on uterine size. If the uterine fundus surpasses the umbilicus, upper abdominal access is preferred. In the transperitoneal robot-assisted technique, three robotic ports are aligned para-rectally, with a 12mm Air Seal port below the umbilicus (Figure 2). CO2 insufflation is typically maintained at 8–12 mmHg, although higher pressures may pose risks to uterine blood flow and fetal health [42-45]. For retroperitoneal approaches, an incision below the 12th rib provides access, with a balloon dissector creating space for port placement. Retroperitoneal techniques involve less uterine irritation, while transperitoneal approaches offer a broader surgical field and better visibility of landmarks [43]. Robotic partial nephrectomy (RPN) is advantageous over laparoscopic methods due to lower conversion rates to radical nephrectomy, better preservation of kidney function, shorter hospital stays, and reduced ischemia times. To date, only four cases of RPN in pregnant patients have been reported. Most occurred during the second trimester with transperitoneal access and controlled CO2 pressure. A retroperitoneal approach was used in a third-trimester case to accommodate an enlarged uterus (Figure 2). The right-side supine position must be managed cautiously in late pregnancy to prevent compression of the inferior vena cava [43]. Minimizing CO2 insufflation and maintaining intraperitoneal pressure below 12 mmHg can reduce complications. Retroperitoneal approaches further lower risks, offering early control of the renal hilum and reduced bowel manipulation [44,46].
6. Treatment Plan and Outcomes
Managing renal masses during pregnancy is a complex and demanding topic. There is no universal agreement on the optimal timing for interventions or the positioning of the patient during procedures [47]. Any solid renal tumor identified during pregnancy should be presumed to be RCC until proven otherwise [3]. To confirm or exclude this diagnosis, a nephrectomy—either partial or radical—may be required. Rajeev et al. described a case involving a renal mass during pregnancy, where a preoperative fine-needle biopsy suggested an oncocytic renal neoplasm [1]. However, definitive histological analysis later identified it as chromophobe renal cell carcinoma. Following thorough counseling, the patient underwent robotic radical nephrectomy at 13 weeks of gestation [1,37]. This highlights the importance of recognizing that negative biopsy results do not definitively rule out malignancy. Laparoscopic radical nephrectomy and nephron-sparing surgeries are now commonly utilized to treat renal tumors during pregnancy [1,3]. However, there is ongoing debate regarding the most appropriate treatment strategy. Surgical interventions during pregnancy require careful monitoring of maternal hemodynamics to ensure adequate utero-placental blood flow and to minimize the risk of preterm labor [49]. Not all renal tumors discovered during pregnancy demand immediate surgical intervention [50,51]. Decisions regarding treatment should consider the health of both the mother and fetus, the aggressiveness of the tumor, and, most importantly, the preferences of the pregnant individual [52,53]. When surgery becomes necessary, the timing is crucial. For localized renal tumors (stage I or II), the general recommendation is to avoid surgical procedures during the first trimester [54,55]. Interventions are typically safer in the second trimester or after fetal lung development is complete. For advanced tumors (stage III or IV), pregnancy termination may be advised to prioritize treatment for the renal tumor. Radical nephrectomy and nephron-sparing surgeries remain critical options for RCC management [56]. The National Comprehensive Cancer Network guidelines suggest that stage I renal masses (T1a) are best managed with partial nephrectomy. For T1b tumors, partial nephrectomy has demonstrated comparable outcomes to radical surgery [57]. Radical nephrectomy is the standard treatment for stages II and III, while partial nephrectomy may be considered in cases of locally advanced tumors if technically feasible [55,57]. Reports indicate that some stage T1 and nearly all stage T2 renal tumors in pregnant patients have been treated with radical nephrectomy to reduce operative duration and minimize perioperative risks [38,40]. Studies have shown the feasibility of laparoscopic nephrectomy during pregnancy, with no significant complications [58]. Similarly, robotic surgeries have been successfully performed without notable adverse effects. Current evidence suggests no significant increase in the risk of preterm labor or perioperative complications for either mother or child [42-45].
Treatment of Metastatic Renal Tumors
Current strategies for managing metastatic renal tumors prioritize combination therapies involving immune checkpoint inhibitors. The standard treatment across all risk groups includes combinations such as pembrolizumab plus axitinib and nivolumab plus ipilimumab. When immune checkpoint inhibitors are unavailable or contraindicated, VEGFR-TKIs can serve as alternative options [59,60]. The safety profile of these treatments during pregnancy is not well-established. Limited research exists, and the available data primarily come from animal studies [61,62]. According to the United States Food and Drug Administration, these medications are classified as Category D, indicating potential risks to the fetus and advising against their use during pregnancy [63]. Consequently, systemic treatment is not advised for pregnant patients with RCC who have undergone radical tumor resection and do not exhibit metastasis. However, for patients with distant metastases, systemic therapy may be considered after pregnancy termination [64].
7. Future Directions and Conclusions
Although rare, renal masses identified during pregnancy can be malignant. In cases of renal cell carcinoma during pregnancy, timely diagnosis and appropriate management are vital for optimizing maternal and fetal outcomes. While no specific guidelines for managing renal tumors in pregnant patients currently exist, clinicians can rely on established protocols for kidney tumor treatment in non-pregnant individuals and surgical guidelines tailored to pregnancy. Emerging evidence indicates that routine ultrasonographic screening facilitates the early detection of renal cancer during pregnancy, enabling timely intervention. Radical nephrectomy has demonstrated a high curative potential and can be performed safely during pregnancy with favorable maternal and fetal outcomes comparable to those in non-pregnant patients with renal cancer. Advances in robotic surgery have contributed to reduced blood loss, quicker postoperative recovery, and operation times that align with safety standards for pregnant patients. The decision regarding the timing and necessity of surgery in pregnant patients requires a careful assessment of maternal health, fetal development, and the progression of the disease. In cases of extensive metastatic disease, termination of the pregnancy may be considered. Effective management demands close collaboration between a multidisciplinary team and the patient to ensure individualized care.
Author Contributions
Conceptualization, L.D. and V.S.; methodology, L.D. and V.S.; software, V.S.; validation, V.S. and L.D.; formal analysis, V.S.; investigation, L.D.; resources, L.D.; data curation, V.S.; writing—original draft preparation, L.D.; writing—review and editing, V.S.; visualization, V.S.; supervision, L.D.. All authors have read and agreed to the published version of the manuscript.
Funding
No funding.
Institutional Review Board Statement
We note that this study adhered to the tenets of the Declaration of Helsinki. This is a retrospective study of medical records, and our data were fully anonymized.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The author declares no conflict of interest.
References
- Rajeev, S.; Brendan, B. Robot-assisted radical nephrectomy for renal-cell carcinoma during twin pregnancy. Urol Nephrol Open Access J. 2023, 11, 111–113. [Google Scholar]
- Xu, H.; Tan, S. Diagnosis and treatment of renal cell carcinoma during pregnancy. Cancer Manag Res. 2021, 13, 9423–9428. [Google Scholar] [CrossRef] [PubMed]
- Dell’Atti, L.; Borghi, C.; Galosi, AB. Laparoscopic approach in management of renal cell carcinoma during pregnancy: state of the art. Clin Genitourin Cancer 2019, 17, e822–830. [Google Scholar] [CrossRef]
- Palanivelu, C.; Rangarajan, M.; Senthilkumaran, S.; et al. Safety and efficacy of laparoscopic surgery in pregnancy: experience of a single institution. J Laparoendosc Adv Surg Tech A. 2017, 17, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Ruiz Guerrero, E.; Claro, A.V.O.; Ledo Cepero, M.J.; Soto Delgado, M.; Álvarez-Ossorio Fernández, J.L. Robotic versus Laparoscopic Partial Nephrectomy in the New Era: Systematic Review. Cancers (Basel) 2023, 15, 1793. [Google Scholar] [CrossRef] [PubMed]
- Gettman, M.T.; Blute, M.L.; Chow, G.K.; Neururer, R.; Bartsch, G.; Peschel, R. Robotic-assisted laparoscopic partial nephrectomy: Technique and initial clinical ex-perience with daVinci robotic system. Urology 2004, 64, 914–918. [Google Scholar] [CrossRef] [PubMed]
- Haseebuddin, M.; Benway, B.M.; Cabello, J.M.; Bhayani, S.B. Robot- assisted partial nephrectomy: Evaluation of learning curve for an experienced renal surgeon. J. Endourol. 2010, 24, 57–61. [Google Scholar] [CrossRef]
- Wolters, V.; Heimovaara, J.; Maggen, C.; et al. Management of pregnancy in women with cancer. Int J. Gynecol Cancer 2021, 31, 314–322. [Google Scholar] [CrossRef]
- Kalampokas, E.; Vlahos, N.; Kalampokas, T.; Gurumurthy, M. Common Malignancies During Pregnancy: A Comprehensive Review. Cancer Diagn Progn. 2021, 1, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Milosevic, B.; Likic Ladjevic, I.; Dotlic, J.; et al. Cancer during pregnancy: Twenty-two years of experience from a tertiary referral center. Acta Obstet Gynecol Scand. 2024, 103, 716–728. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Li, X.; Peng, L.; Gou, X.; Fan, J. An update on recent developments in rupture of renal angiomyolipoma. Medicine (Baltimore). 2018, 97, e0497. [Google Scholar] [CrossRef]
- Chu, J.S.; Wang, Z.J. Protocol optimization for renal mass detection and characterization. Radiol Clin North Am. 2020, 58, 851–873. [Google Scholar] [CrossRef] [PubMed]
- Khazzaka, A.; Rassy, E. , Sleiman, Z. ; Boussios, S.; Pavlidis, N. Systematic review of fetal and placental metastases among pregnant patients with cancer. Cancer Treat Rev. 2022, 104, 102356. [Google Scholar]
- Caglayan, A.; Rabbani, RD.; Sanchez, E.; et al. Gestational Renal Cell Cancer- An Update. Anticancer Res. 2023, 43, 3871–3880. [Google Scholar] [CrossRef] [PubMed]
- Lambe, M.; Lindblad, P.; Wuu, J.; Remler, R.; Hsieh, C.C. Pregnancy and risk of renal cell cancer: a population-based study in Sweden. Br J Cancer, 2002, 86, 1425–1429. [Google Scholar] [CrossRef] [PubMed]
- Macleod, L.C.; Hotaling, J.M.; Wright, J.L.; et al. Risk factors for renal cell carcinoma in the VITAL study. J Urol. 2013, 190, 1657–1661. [Google Scholar] [CrossRef] [PubMed]
- Bergström, A.; Hsieh, C.C.; Lindblad, P.; Lu, C.M.; Cook, N.R.; Wolk, A. Obesity and renal cell cancer – a quantitative review. Br J Cancer 2001, 85, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Schouten, L.J.; Van De Pol, J.; Kviatkovsky, M.J. , Van Den Brandt, P. A. Reproductive and external hormonal factors and the risk of renal cell cancer in the Netherlands Cohort Study. Cancer Epidemiol. 2022, 79, 102171. [Google Scholar] [PubMed]
- Aurilio, G.; Piva, F.; Santoni, M.; et al. The role of obesity in renal cell carcinoma patients: clinical pathological implications. Int J Mol Sci. 2019, 20, 5683. [Google Scholar] [CrossRef]
- Padala, S.A.; Barsouk, A.; Thandra, K.C.; et al. Epidemiology of renal cell carcinoma. World J Oncol. 2020, 11, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Deckers, I.A.; Van Den Brandt, P.A.; Van Engeland, M.; et al. Polymorphisms in genes of the renin-angiotensin-aldosterone system and renal cell cancer risk: Interplay with hypertension and intakes of sodium, potassium and fluid. Int J Cancer 2015, 136, 1104–1116. [Google Scholar] [CrossRef]
- Yilmaz, E.; Oguz, F.; Tuncay, G.; et al. Renal cell carcinoma diagnosed during pregnancy: a case report and literature review. J Int Med Res. 2018, 46, 3422–3426. [Google Scholar] [CrossRef] [PubMed]
- Bettez, M.; Carmel, M. , Temmar, R. et al. Fatal fast-growing renal cell carcinoma during pregnancy. J Obstet Gynaecol Can. 2011, 33, 258–261. [Google Scholar]
- Casella, R.; Ferrier, C.; Giudici, G.; et al. Surgical management of renal cell carcinoma during the second trimester of pregnancy. Urol Int. 2006, 76, 180–181. [Google Scholar] [CrossRef] [PubMed]
- Bourgioti C, Konidari M, Gourtsoyianni S, Moulopoulos LA. Imaging during pregnancy: What the radiologist needs to know. Diagn Interv Imaging. 2021, 102, 593–603.
- Tremblay, E.; Thérasse, E.; Thomassin-Naggara, I.; Trop, I. Quality initiatives: guidelines for use of medical imaging during pregnancy and lactation. Radiographics 2012, 32, 897–911. [Google Scholar] [CrossRef] [PubMed]
- Gjelsteen, A.C.; Ching, B.H.; Meyermann, M.W.; et al. CT, MRI, PET, PET/CT, and ultrasound in the evaluation of obstetric and gynecologic patients. Surg Clin North Am. 2008, 88, 361–390. [Google Scholar] [CrossRef]
- Chen, J.; Lee, R.J.; Tsodikov, A.; Smith, L.; Gaffney, D.K. Does radiotherapy around the time of pregnancy for Hodgkin's disease modify the risk of breast cancer? Int J Radiat Oncol Biol Phys. 2004, 58, 1474–1479. [Google Scholar] [CrossRef]
- Goldberg-Stein, S.; Liu, B.; Hahn, P.F.; Lee, S.I. Body CT during pregnancy: utilization trends, examination indications, and fetal radiation doses. AJR Am J Roentgenol. 2011, 196, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Kelaranta, A.; Mäkelä, T.; Kaasalainen, T.; Kortesniemi, M. Fetal radiation dose in three common CT examinations during pregnancy: Monte Carlo study. Phys Med. 2017, 43, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Angel, E.; Wellnitz, C.V.; Goodsitt, M.M.; et al. Radiation dose to the fetus for pregnant patients undergoing multidetector CT imaging: Monte Carlo simulations estimating fetal dose for a range of gestational age and patient size. Radiology 2008, 249, 220–227. [Google Scholar] [CrossRef]
- Han, S.N.; Amant, F.; Michielsen, K.; et al. Feasibility of whole-body diffusion-weighted MRI for detection of primary tumour, nodal and distant metastases in women with cancer during pregnancy: a pilot study. Eur Radiol. 2018, 28, 1862–1874. [Google Scholar] [CrossRef]
- Khochikar, M.V. Management of urological cancers during pregnancy. Nat Rev Urol. 2010, 7, 195–205. [Google Scholar] [CrossRef]
- Moguel González, B.; Garcia Nava, M.; Orozco Guillén, O.A.; et al. Kidney biopsy during pregnancy: a difficult decision. A case series reporting on 20 patients from Mexico. J Nephrol. 2022, 35, 2293–2300. [Google Scholar]
- Ghorbani, H. ; Mottaghi,M.; Soltani, S. Renal Tumors in Pregnancy: A Case Report Focusing on the Timing of the Surgery and Patient Positioning. Case Rep Obstet Gynecol. 2022, 1143478. [Google Scholar]
- Guerre, M.; Boehnlein, C.; Sohaey, R.; Seideman, C.A. Imaging of Prenatal and Neonatal Intra-abdominal Genitourinary Tumors: a Review of the Literature. Curr Urol Rep. 2022, 23, 39–46. [Google Scholar] [CrossRef]
- Loughlin, K. The management of urological malignancies during pregnancy. Br J Urol. 1995, 76, 639–644. [Google Scholar] [CrossRef]
- Akpayak, I.; Shuiabu, S.; Ofoha, C.; Dakum, N.; Ramyil, V. Renal cell carcinoma in pregnancy: Still a management challenge. Afr J Urol. 2015, 21, 167–170. [Google Scholar] [CrossRef]
- Bettez, M.; Carmel, M.; Temmar, R.; et al. Fatal fast-growing renal cell carcinoma during pregnancy. J Obstet Gynaecol Can. 2011, 33, 258–261. [Google Scholar] [CrossRef]
- Wiles, R.; Hankinson, B.; Benbow, E.; Sharp, A. Making decisions about radiological imaging in pregnancy. BMJ. 2022, 377, e070486. [Google Scholar] [CrossRef]
- Capella, C.E.; Godovchik, J.; Chandrasekar, T.; Al-Kouatly, H.B. Nonobstetrical Robotic-Assisted Laparoscopic Surgery in Pregnancy: A Systematic Literature Review. Urology. 2021, 151, 58–66. [Google Scholar] [CrossRef]
- Park, S.Y.; Ham, WS.; Jung, H.J.; et al. Robot-assisted laparoscopic partial nephrectomy during pregnancy. J Robot Surg. 2008, 2, 193. [Google Scholar] [CrossRef]
- Ramirez, D.; Maurice, M.J.; Seager, C.; Haber, G.P. Robotic Partial Nephrectomy during Pregnancy: Case Report and Special Considerations. Urology 2016, 92, 1–5. [Google Scholar] [CrossRef]
- Völler, M.; Mahmud, W.; Vallo, S.; Grabbert, M.; John, P.; Khoder, W.Y. A 27-Year-Old Primigravida with a Right Renal Cell Carcinoma Removed at 30 Weeks of Gestation by Robot-Assisted Retroperitoneoscopic Partial Nephrectomy. Am J Case Rep. 2021, 22, e927164. [Google Scholar] [CrossRef]
- Tsutsui, K.; Miki, A.; Wakita, T.; et al. A case of robot-assisted laparoscopic partial nephrectomy during pregnancy. IJU Case Rep. 2023, 6, 458–460. [Google Scholar] [CrossRef]
- Dong, J.; Zhao, Y.; Xu, W. Case report: Retroperitoneal laparoscopic partial nephrectomy for T2 renal cell carcinoma during pregnancy. Front Oncol. 2020, 10, 552228. [Google Scholar] [CrossRef]
- Zhao, Y.; Yang, Z.; Xu, W.; Ji, Z.; Dong, J. Management of renal tumors during pregnancy: case reports. BMC Nephrol. 2021, 22, 127. [Google Scholar] [CrossRef]
- Kumar, S.S.; Collings, A.T.; Wunker, C.; et al. SAGES guidelines for the use of laparoscopy during pregnancy. Surg Endosc. 2024, 38, 2947–2963. [Google Scholar] [CrossRef]
- Ye, P.; Zhao, N.; Shu, J.; Shen, H.; et al. Laparoscopy versus open surgery for adnexal masses in pregnancy: a meta-analytic review. Arch Gynecol Obstet. 2019, 299, 625–634. [Google Scholar] [CrossRef]
- Lee, D.; Abraham, N. Laparoscopic radical nephrectomy during pregnancy: case report and review of the literature. J Endourol. 2008, 22, 517–518. [Google Scholar] [CrossRef]
- Berczi C, Flasko T. Renal Tumor in Pregnancy: A Case Report and Review of the Literature. Urol Int. 2017, 99, 367–369.
- Amant, F.; Berveiller, P.; Boere, I.A.; et al. Gynecologic cancers in pregnancy: guidelines based on a third international consensus meeting. Ann Oncol. 2019, 30, 1601–1612. [Google Scholar] [CrossRef]
- Wolters, V.; Heimovaara, J.; Maggen, C.; et al. Management of pregnancy in women with cancer. Int J Gynecol Cancer. 2021, 31, 314–322. [Google Scholar] [CrossRef]
- Ohyama, T.; Shimbo, M.; Endo, F.; et al. Renal cell carcinoma treatment during pregnancy: Histopathological findings suggestive of rapid tumor growth. IJU Case Rep. 2019, 2, 265–268. [Google Scholar] [CrossRef]
- Dey, S.; Pakrasi, R.; Saha, D.; Datta, S. Rapidly progressive growth of Renal Clear Cell Carcinoma and Gastrointestinal Stromal Tumor during the 3rd trimester of pregnancy: A clinical and diagnostic dilemma. Urol Case Rep. 2021, 40, 101891. [Google Scholar] [CrossRef]
- Zambrana, F.; Barbancho, C.; Huelves, M.; et al. Successful Pregnancy and Cancer Outcomes With Ipilimumab and Nivolumab for Metastatic Renal Cell Carcinoma: Case Report and Review of the Literature. J Immunother. 2023, 46, 27–28. [Google Scholar] [CrossRef]
- Campbell, S.C.; Uzzo, R.G.; Karam, J.A.; et al. Renal Mass and Localized Renal Cancer: Evaluation, Management, and Follow-up: AUA Guideline: Part II. J Urol. 2021, 206, 209–218. [Google Scholar] [CrossRef]
- Dai K, Jiang W, Chen S, Luo S, Ding S, Wang D. Case report: Going through pregnancy safely after twice partial nephrectomy for bilateral kidneys with HLRCC-associated RCC. Front Oncol. 2022, 12, 932996.
- Xu, H.; Tan, S. Diagnosis and Treatment of Renal Cell Carcinoma During Pregnancy. Cancer Manag Res. 2021, 13, 9423–9428. [Google Scholar] [CrossRef]
- Goebell, P.J.; Ivanyi, P.; Bedke, J.; et al. Consensus paper: current state of first- and second-line therapy in advanced clear-cell renal cell carcinoma. Future Oncol. 2020, 16, 2307–2328. [Google Scholar] [CrossRef]
- Yazigi, A.; Lecointe-Artzner, E.; Cesne, A.L.; et al. Pregnancy in Women with Metastatic Sarcomas. Oncologist. 2020, 25, e2010–e2012. [Google Scholar] [CrossRef]
- Khaled, H.; Lahloubi, N.A.; Rashad, N. Review on renal cell carcinoma and pregnancy: a challenging situation. J Adv Res. 2016, 7, 575–580. [Google Scholar] [CrossRef]
- Chys, B.; Dumont, S.; Van Calsteren, K.; et al. Renal neoplasm during pregnancy: a single center experience. Clin Genitourin Cancer. 2018, 16, e501–e507. [Google Scholar] [CrossRef] [PubMed]
- Boere, I.; Lok, C.; Vandenbroucke, T.; et al. Cancer in pregnancy: safety and efficacy of systemic therapies. Curr Opin Oncol. 2017, 29, 328–334. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Study flow chart.
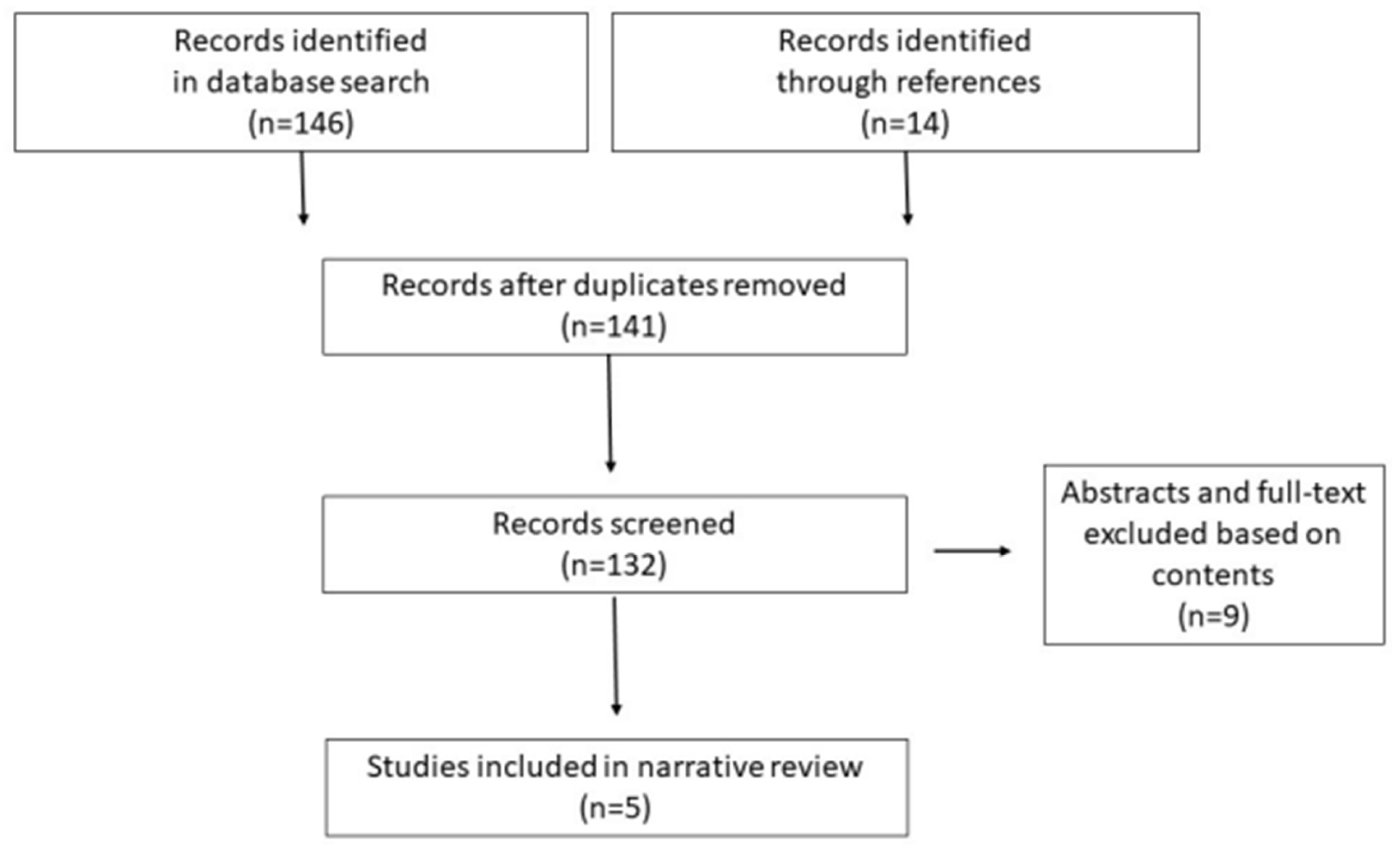
Figure 2.
Robotic Ports Position (black triangle: robotic-8mm trocar; white star: 12mm trocar assistant; white circle: robotic-8mm trocar camera position) in Pregnancy during: 1st Trimester (a); 2nd Trimester (b); 3rd Trimester (c).
Figure 2.
Robotic Ports Position (black triangle: robotic-8mm trocar; white star: 12mm trocar assistant; white circle: robotic-8mm trocar camera position) in Pregnancy during: 1st Trimester (a); 2nd Trimester (b); 3rd Trimester (c).
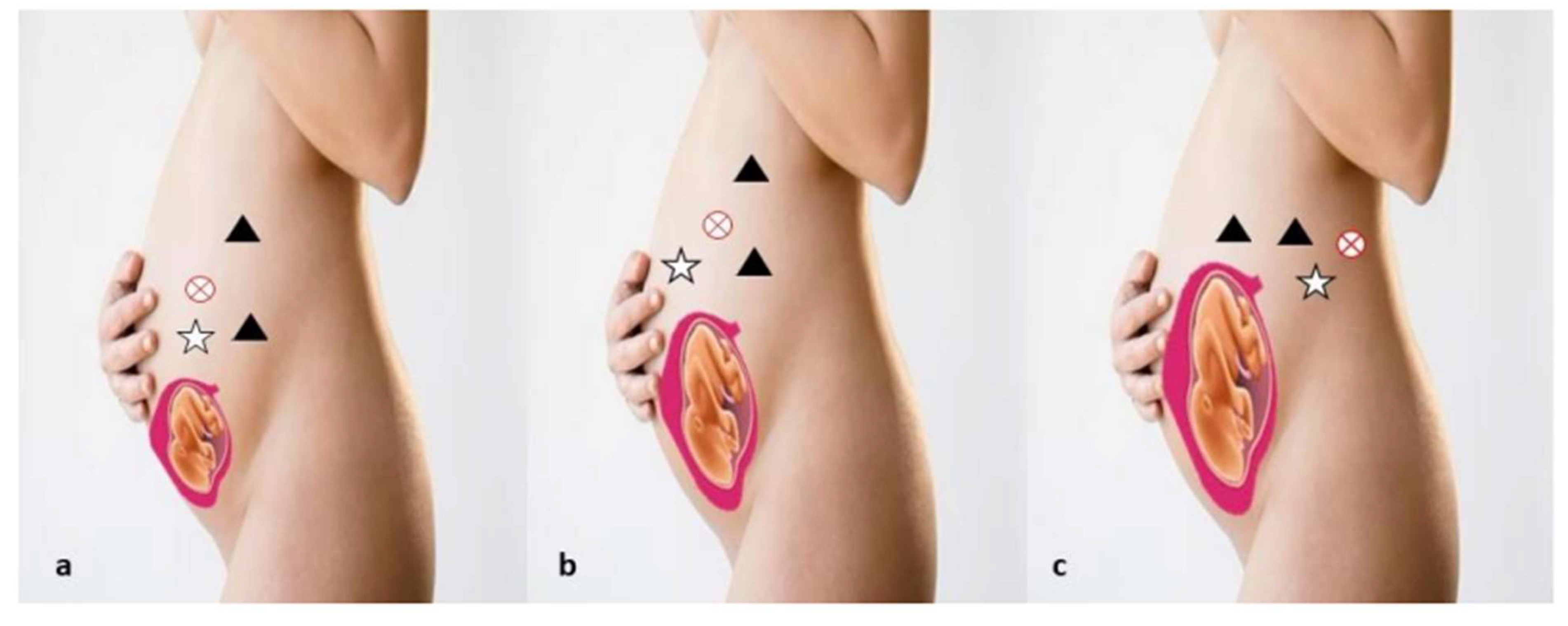

Table 1.
Management in patients affected by RCC during pregnancy and treated with Robotic surgery.
| Study |
Park SY et al.42 |
Ramirez D et al. 43 |
Völler M et al.44 |
Tsutsui K et al.48 |
Rajeev S =et al.1 |
| Patients, n. | 1 | 1 | 1 | 1 | 1 |
| Age, y | 36 | 35 | 27 | 36 | 23 |
| Age of gestation at diagnosis | 14 th w | 20 th w | 30 th w | 15 th w | 8 th w |
| Staging Imaging | MRI | MRI | MRI | CT | CT |
| Kidney Side | Left | Right | Right | Left | Left |
| Kidney Localization | Middle portion | Upper pole | Lower pole | Upper pole | Lower pole |
| Renal biopsy | No | No | No | No | Yes |
| Pathologic stage | T1a | T1b | T1b | T1a | T2a |
| Treatment | PN | PN | PN | PN | RN |
| Surgical approach | T | T | R | T | T |
| Histologic findings | RCC | RCC | CRCC | RCC | CRCC |
W= week; CT= Computed Tomography; MRI= Magnetic Resonance Imaging; CPN= partial nephrectomy; RN= radical nephrectomy; T= transperiteonal; R= retroperitoneal; RCC= renal cell carcinoma; CRCC= chromophobe renal cell carcinoma.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



