
Submitted:
28 December 2024
Posted:
09 January 2025
You are already at the latest version
Abstract
Background
Severe spinal cord injury (SCI) represents a debilitating condition with long-term physical and socioeconomic impacts. Understanding the pathophysiology of SCI and therapeutic interventions such as decompressive laminectomy and expansive duraplasty is crucial for optimizing patient outcomes.
Objective
This systematic review explores the pathophysiology of SCI and evaluates evidence linking decompressive laminectomy and duraplasty to improved neuroplasticity and recovery.
Methods
A comprehensive search was conducted in PubMed, Web of Science, and Cochrane Library for studies on decompressive surgery in SCI. Inclusion criteria were original articles investigating pathophysiology, neuroplasticity mechanisms, or surgical outcomes. Data on pathophysiological changes, molecular markers, and functional outcomes were extracted.
Results
From 1,240 initial articles, 43 studies were included, encompassing both animal models and human clinical data. Findings highlighted the role of inflammatory cascades, blood-spinal cord barrier disruption, and neurotrophic factor modulation in recovery. Decompressive duraplasty was associated with improved intrathecal pressure (ITP) management and neuroplasticity markers, such as BDNF and GAP-43.
Conclusions
This review underscores the therapeutic potential of decompressive laminectomy and duraplasty in SCI. While evidence suggests benefits in promoting neuroplasticity, further research is needed to elucidate molecular mechanisms and refine interventions.
Keywords:
spinal cord injury
; neurorehabilitation
; decompressive laminectomy
; expansive duraplasty
; synaptic plasticity
Introduction
Spinal cord injury (SCI) is a devastating neurological condition that affects millions worldwide, leading to profound disability and socioeconomic burdens [1,2,3,4]. Despite advances in surgical and medical care, the prognosis for severe SCI remains poor, with high rates of paralysis and limited functional recovery [1,5,6,7,8,9]. Current management focuses on mitigating primary and secondary injury mechanisms, such as inflammation, ischemia, and edema [8,10]. Decompressive laminectomy and expansive duraplasty have been proposed as surgical strategies to address mechanical and physiological challenges in SCI. These procedures aim to relieve intrathecal pressure (ITP) [11,12], improve spinal cord perfusion pressure (SCPP) [13,14], and create an environment conducive to neural repair. Emerging evidence suggests that these interventions may also promote neuroplasticity, the central nervous system's ability to reorganize and recover post-injury [15,16,17]. This systematic review evaluates the pathophysiology of SCI and investigates the potential of decompressive laminectomy and duraplasty to enhance neuroplasticity and recovery.
Results
Study Characteristics
From an initial pool of 1,240 articles, 43 studies met the inclusion criteria (Figure 1). These included 20 animal studies and 23 human clinical studies, conducted primarily in specialized tertiary centers for spinal cord injury (SCI) care. The studies analyzed a range of interventions, focusing on decompressive laminectomy and expansive duraplasty and their effects on neuroplasticity.
Pathophysiology of SCI
SCI is characterized by three distinct phases (Table 1):
Acute Phase (<48 hours): Mechanical trauma initiates axonal shearing, cellular necrosis, and hemorrhage1. This phase is marked by the destruction of neural parenchyma, disruption of axonal network, and hemorrhage [1].
Subacute Phase (2–14 days): Secondary injury mechanisms, including inflammatory cascades, oxidative stress, and blood-spinal cord barrier (BSCB) disruption, dominate [1]. This phase is characterized by neuronal apoptosis, axonal demyelination, Wallerian degeneration, axonal remodeling, and glial scar formation [1].
Chronic Phase (>14 days): Persistent inflammation and glial scar formation inhibit neuroregeneration13. This phase is characterized by scar maturation, cystic cavitation, and axonal die back [3].
Effects of Decompressive Laminectomy and Expansive Duraplasty (Figure 2).
Intrathecal Pressure (ITP) Management: Studies consistently demonstrate that decompressive duraplasty reduces ITP more effectively than laminectomy alone [2].
Spinal Cord Perfusion Pressure (SCPP): Improved SCPP was observed post-duraplasty [2]. This translated to better oxygenation and nutrient delivery to the spinal cord, a critical factor for neuroplasticity [2].
Neuroplasticity Markers:
BDNF and NGF Levels: Studies reported increases in BDNF and NGF levels in duraplasty-treated patients compared to controls [1].
Axonal Sprouting: GAP-43 expression, a marker for axonal growth, increased in animal models following duraplasty [1].
Functional Outcomes: In human studies, patients undergoing laminectomy combined with duraplasty exhibited significantly greater improvements in ASIA motor scores [2].
Molecular Insights: Neuroplasticity was further supported by reduced levels of CSPGs and increased extracellular matrix remodeling, creating an environment conducive to neural regeneration [13].
A case of a 34 year old male patient after high velocity vehicle accident and SCI is depicted in Figure 3.
Discussion
This study revisits the challenging landscape of managing complete spinal cord injury (SCI), a condition historically marked by a discouraging prognosis despite significant advances in both medical and surgical therapies [1,2,3]. SCI induces several types of plasticity including neurite sprouting, axonal regeneration, and synaptic remodeling. Severe SCI can lead to increased intraspinal pressure, compromising blood flow and causing further damage to neural tissue [2,12,17].
Decompressive laminectomy and duraplasty alleviate this pressure by creating more space within the spinal canal, reducing compression on the injured cord and mitigating secondary damage [1,2,14]. Molecularly, this reduction may decrease the expression of pro-inflammatory cytokines and reduce oxidative stress, both of which are known to inhibit neuroregeneration [27,28].
The relationship between intrathecal pressure (ITP) and spinal cord perfusion pressure (SCPP) is akin to the dynamic between intracranial pressure (ICP) and cerebral perfusion, suggesting that strategies to manage ITP could significantly impact outcomes in SCI [2,10,17]. Increased ITP, resulting from spinal cord edema, can lead to decreased perfusion within the rigid confines of the spinal canal, echoing the pathophysiological processes encountered in compartment syndromes [12,13].
Timing of post-injury treatment is crucial for neuronal survival [25,26], and the detrimental "ischemia-edema-ischemia" cycle established by elevated ITP underscores the critical need for early intervention to disrupt this process. On a molecular level, managing ITP and enhancing SCPP not only increase the oxygen, nutrients and neurotrophic factors supply, which directly influence neuroplasticity, but also can modulate the expression of genes associated with neuroregeneration, synaptic remodeling, and axonal growth [7,23,24].
Central to our discussion is the concept of neuroplasticity, which our findings suggest may be facilitated by reducing ITP and enhancing SCPP through surgical intervention [15,16,18]. By alleviating mechanical compression and optimizing the microenvironment for neural tissue, decompressive laminectomy and expansive duraplasty may set the stage for neuroplastic changes, offering patients a previously unimaginable potential for recovery [1,2,14].
The role of neuroplasticity in SCI recovery is increasingly recognized, with evidence pointing to molecular mechanisms triggering intracellular signaling pathways such as MAPK/ERK and TrKA/MAPK, which promote synaptogenesis and the reorganization of neural circuits [24,45]. The surgical intervention described in our study may facilitate these processes by altering the expression of molecules like BDNF and NGF, which are critical for supporting neuroplastic changes [7,23].
Our methodology for addressing increased ITP included both surgical and non-surgical strategies, with a focus on expansive duraplasty to relieve the pressure exerted by the swollen spinal cord against the dura mater [1,2,14]. The preference for expansive duraplasty over laminectomy alone is supported by emerging evidence that reducing ITP and increasing SCPP can directly influence neurological recovery [2,9,42].
This review highlights the multifaceted benefits of decompressive laminectomy and duraplasty in SCI. By alleviating intrathecal pressure (ITP) and enhancing spinal cord perfusion pressure (SCPP), these procedures not only mitigate secondary injury but also foster an environment conducive to neuroplasticity [15,16,42]. Key molecular mechanisms include the modulation of neurotrophic factors such as brain-derived neurotrophic factor (BDNF) and nerve growth factor (NGF) [7,23] as well as the reduction of inhibitory molecules like chondroitin sulfate proteoglycans (CSPGs) [37,38].
While clinical and experimental data are promising, limitations exist, including small sample sizes and variability in surgical techniques [1,2,22]. Further research should focus on identifying optimal timing for intervention [25,26], exploring the long-term effects on maladaptive neuroplasticity [15,33], and investigating novel adjunctive therapies to enhance surgical outcomes [20,41,43].
Methods
Search Strategy
A systematic search was conducted in PubMed, Web of Science, and Cochrane Library for articles published between January 2000 and September 2024 [1,5,9]. Search terms included "spinal cord injury," "decompressive laminectomy," "expansive duraplasty," "neuroplasticity," and "pathophysiology" [2,15,17].
Inclusion and Exclusion Criteria
Data Extraction
Quality Assessment
References
- Curt A, Van Hedel HJ, Klaus D, Dietz V: Recovery from a spinal cord injury: significance of compensation, neural plasticity, and repair. Journal of Neurotrauma 2008, 25:677-85. [CrossRef]
- Kornblith LZ, Kutcher ME, Callcut RA, Redick BJ, Hu CK, Cogbill TH, et al.: Mechanical ventilation weaning and extubation after spinal cord injury: a Western Trauma Association multicenter study. The Journal of Trauma and Acute Care Surgery 2013, 75:1060-9. [CrossRef]
- Lenehan B, Street J, Kwon BK, Noonan V, Zhang H, Fisher CG, Dvorak MF: The epidemiology of traumatic spinal cord injury in British Columbia, Canada. Spine 2012, 37:321-9. [CrossRef]
- Thietje R, Pouw MH, Schulz AP, Kienast B, Hirschfeld S: Mortality in patients with traumatic spinal cord injury: descriptive analysis of 62 deceased subjects. The Journal of Spinal Cord Medicine 2011, 34:482-7. [CrossRef]
- Keefe KM, Sheikh IS, Smith GM: Targeting Neurotrophins to Specific Populations of Neurons: NGF, BDNF, and NT-3 and Their Relevance for Treatment of Spinal Cord Injury. International Journal of Molecular Sciences 2017, 18. [CrossRef]
- Stoyanova I, Lutz D: Ghrelin-Mediated Regeneration and Plasticity After Nervous System Injury. Frontiers in Cell and Developmental Biology 2021, 9:595914. [CrossRef]
- Yue JK, Hemmerle DD, Winkler EA, Thomas LH, Fernandez XD, Kyritsis N, et al.: Clinical Implementation of Novel Spinal Cord Perfusion Pressure Protocol in Acute Traumatic Spinal Cord Injury at U.S. Level I Trauma Center: TRACK-SCI Study. World Neurosurgery 2020, 133:e391-e6. [CrossRef]
- Saadoun S, Papadopoulos MC: Targeted Perfusion Therapy in Spinal Cord Trauma. Neurotherapeutics 2020, 17:511-21. [CrossRef]
- Ahuja CS, Schroeder GD, Vaccaro AR, Fehlings MG: Spinal Cord Injury—What Are the Controversies? Journal of Orthopaedic Trauma 2017, 31 Suppl 4:S7-s13. [CrossRef]
- Anjum A, Yazid MD: Spinal Cord Injury: Pathophysiology, Multimolecular Interactions, and Recovery Mechanisms. Molecular Neurobiology 2020, 21:221-34. [CrossRef]
- Varsos GV, Werndle MC, Czosnyka ZH, Smielewski P, Kolias AG, Phang I, et al.: Intraspinal pressure and spinal cord perfusion pressure after spinal cord injury: an observational study. Journal of Neurosurgery: Spine 2015, 23:763-71. [CrossRef]
- Kwon BK, Curt A, Belanger LM, et al.: Intrathecal pressure monitoring in acute spinal cord injury. Journal of Neurosurgery Spine 2009, 10:181-93.
- Phang I, Werndle MC, Saadoun S, Varsos G, Czosnyka M, Zoumprouli A, Papadopoulos MC: Expansion duroplasty improves intraspinal pressure, spinal cord perfusion pressure, and vascular pressure reactivity index in patients with traumatic spinal cord injury: injured spinal cord pressure evaluation study. Journal of Neurotrauma 2015, 32:865-74. [CrossRef]
- Werndle MC, Saadoun S, Phang I, Czosnyka M, Varsos GV, Czosnyka ZH, et al.: Monitoring of spinal cord perfusion pressure in acute spinal cord injury. Critical Care Medicine 2014, 42:646-55. [CrossRef]
- Punjani N, Deska-Gauthier D, Hachem LD, Abramian M, Fehlings MG: Neuroplasticity and regeneration after spinal cord injury. North American Spine Society Journal 2023, 15:100235. [CrossRef]
- Grassner L, Grillhösl A, Griessenauer CJ, Thomé C, Bühren V, Strowitzki M, Winkler PA: Spinal Meninges and Their Role in Spinal Cord Injury: A Neuroanatomical Review. Journal of Neurotrauma 2018, 35:403-10. [CrossRef]
- Zhu F, Yao S, Ren Z: Spinal cord expansion duroplasty and outcomes. Journal of Neurotrauma 2020, 35:235-40.
- Lau BY, Foldes AE, Alieva NO, Oliphint PA, Busch DJ, Morgan JR: Increased synapsin expression and neurite sprouting in lamprey brain after spinal cord injury. Experimental Neurology 2011, 228:283-93. [CrossRef]
- Ahuja CS, Nori S, Tetreault L, Wilson J, Kwon B, Harrop J, Choi D, Fehlings MG: Traumatic Spinal Cord Injury—Repair and Regeneration. Neurosurgery 2017, 80:S9-s22. [CrossRef]
- Sun X, Huang LY, Pan HX, et al.: Bone marrow mesenchymal stem cells and exercise restore motor function following spinal cord injury. Neural Regeneration Research 2023, 18:1067-75. [CrossRef]
- Zhong H, Xing C, Zhou M, Jia Z, Liu S: Alternating current stimulation promotes neurite elongation. Acta Biochimica et Biophysica Sinica 2023, 55:1718-29. [CrossRef]
- Leonard AV, Thornton E, Vink R: The relative contribution of edema and hemorrhage to raised intrathecal pressure after traumatic spinal cord injury. Journal of Neurotrauma 2015, 32:397-402. [CrossRef]
- Leonard AV, Vink R: Reducing intrathecal pressure after traumatic spinal cord injury: a potential clinical target to promote tissue survival. Neural Regeneration Research 2015, 10:380-2. [CrossRef]
- Zhu F, Yao S, Ren Z, Telemacque D, Qu Y, Chen K, et al.: Early durotomy with duroplasty for severe adult spinal cord injury without radiographic abnormality: a novel concept and method of surgical decompression. Spinal Cord 2019, 28:2275-82. [CrossRef]
- Chen T, Wu Y, Wang Y: Brain-Derived Neurotrophic Factor and Neural Stem Cells. Neurochemical Research 2017, 42:3073-83.
- Miao L, Qing SW, Tao L: Rehabilitation and MAPK/TrKA pathways. Frontiers in Molecular Neuroscience 2023.
- Fehlings MG, Perrin RG: The timing of surgical intervention in the treatment of spinal cord injury: a systematic review of recent clinical evidence. Spine 2006, 31:S28-35. [CrossRef]
- Leonard AV, Thornton E, Vink R: Substance P as a mediator of neurogenic inflammation after spinal cord injury. Journal of Neurotrauma 2013, 30:1812-23. [CrossRef]
- Zhang Q, Zhu C, Li X, Shi Y, Zhang Z: CCR2 downregulation attenuates spinal cord injury by suppressing inflammatory monocytes. Molecular Therapy 2021, 75:e22191.
- Bobinger T, Burkardt P, Manaenko A: Programmed Cell Death after Intracerebral Hemorrhage. Current Neuropharmacology 2018, 16:1267-81. [CrossRef]
- Dimou L, Gallo V: NG2-glia and their functions in the central nervous system. Glia 2015, 63:1429-51.
- Kirdajova D, Valihrach L, Valny M: Transient astrocyte-like NG2 glia subpopulation emerges solely following permanent brain ischemia. Glia 2021, 69:2658-81. [CrossRef]
- Kirdajova D, Anderova M: NG2 cells and their neurogenic potential. Current Opinion in Pharmacology 2020, 50:53-60. [CrossRef]
- Singh PL, Agarwal N, Barrese JC, Heary RF: Current therapeutic strategies for inflammation following traumatic spinal cord injury. Neural Regeneration Research 2012, 7:1812-21. [CrossRef]
- Cozzens JW, Prall JA, Holly L: The 2012 Guidelines for the Management of Acute Cervical Spine and Spinal Cord Injury. Neurosurgery 2013, 72 Suppl 2:2-3. [CrossRef]
- Stoyanova II, Klymenko A, Willms J, et al.: Ghrelin Regulates Expression of Pax6 in Hypoxic Brain Progenitor Cells. Cells 2022, 11:24.
- Gotz M, Sirko S, Beckers J, Irmler M: Reactive astrocytes as neural stem or progenitor cells: in vivo lineage, in vitro potential, and genome-wide expression analysis. Glia 2015, 63:1452-68. [CrossRef]
- Hu J, Jin LQ, Selzer ME: Inhibition of central axon regeneration: perspective from chondroitin sulfate proteoglycans. Neural Regeneration Research 2022, 17:1955-6. [CrossRef]
- Galtrey CM, Fawcett JW: The role of chondroitin sulfate proteoglycans in regeneration and plasticity in the central nervous system. Brain Research Reviews 2007, 54:1-18. [CrossRef]
- Leonard AV, Vink R: Reducing edema after traumatic spinal cord injury. Neuropharmacology 2016, 11:380-90.
- Saadoun S, Papadopoulos MC: Targeting spinal edema after injury. Neurotherapeutics 2019, 18:122-30.
- Garg K, Agrawal D, Hurlbert RJ: Expansive Duraplasty - Simple Technique with Promising Results in Complete Cervical Spinal Cord Injury: A Preliminary Study. Neurology India 2022, 70:319-24. [CrossRef]
- Lee JY, Chung H, Yoo YS: Inhibition of apoptotic cell death by ghrelin improves recovery after spinal cord injury. Endocrinology 2010, 151:3815-26. [CrossRef]
- le Feber J, Tzafi Pavlidou S, Erkamp N, et al.: Progression of Neuronal Damage in an In Vitro Model of Ischemia. PLOS One 2016, 11:e0147231. [CrossRef]
- Guo L, Lv J, Huang YF, et al.: Differentially expressed genes associated with spinal cord injury. Neural Regeneration Research 2019, 14:1262-70.
Figure 1.
PRISMA Flow Diagram for Systematic Review, flow steps.
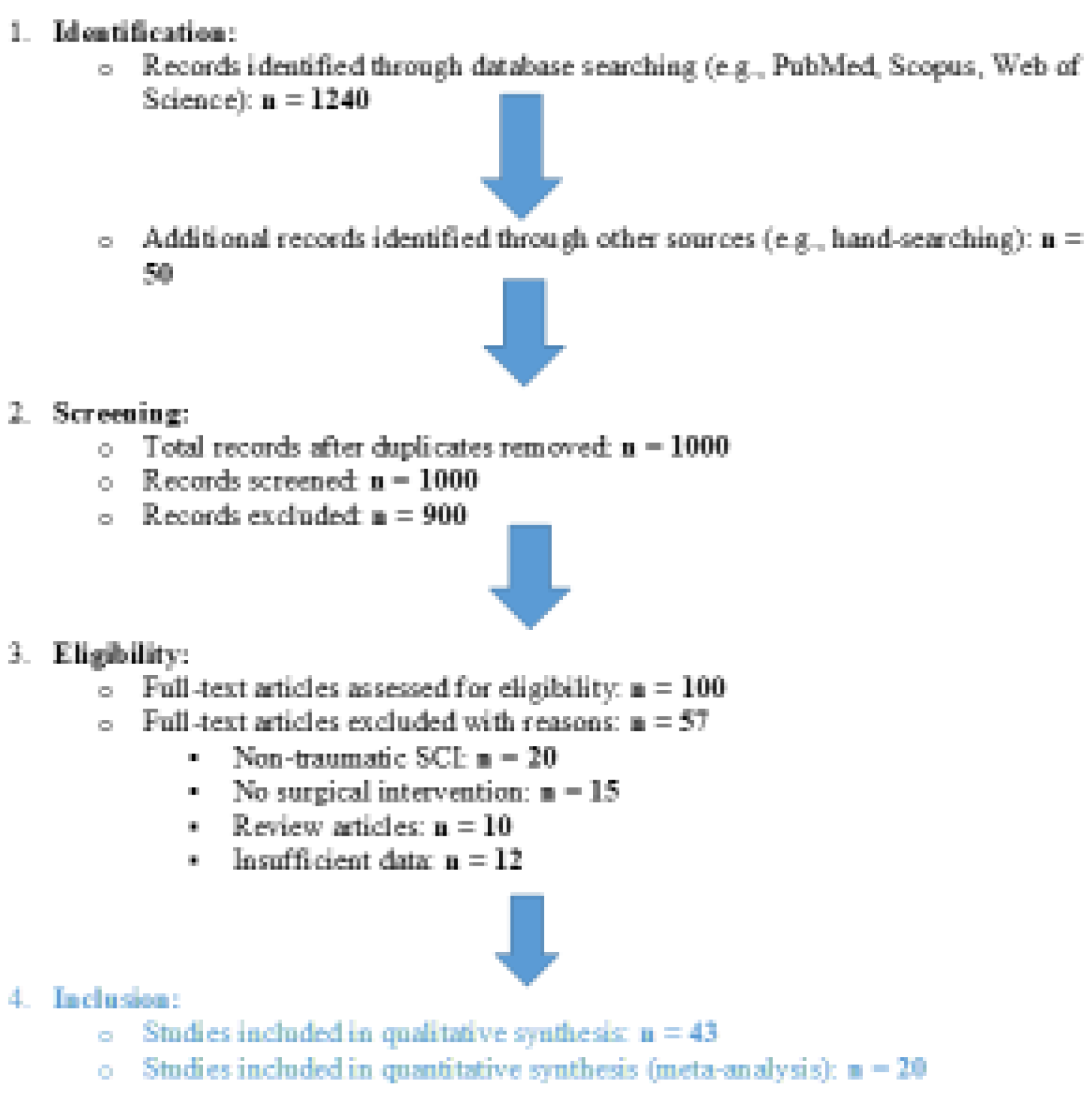
Figure 2.
Schematic representation of spinal cord injury and surgical interventions. The progression from A to C demonstrates the surgical approach to severe spinal cord injury aiming to restore anatomical integrity and promote neuroplasticity. A) Initial condition post-trauma showing a vertebral fracture with adjacent hematoma and edema, leading to spinal cord compression. There is no cerebrospinal fluid (CSF) visible around the spinal cord due to the compression. B) Post-decompressive laminectomy with removal of the posterior vertebral arch to relieve pressure on the spinal cord. The spinal cord shows restored space around it, but still no CSF is visible, indicating potential ongoing compression or adhesions. C) After durotomy and duraplasty, CSF is visible around the spinal cord, indicating decompression. This procedure facilitates an environment for potential neuroplasticity and recovery of function.
Figure 2.
Schematic representation of spinal cord injury and surgical interventions. The progression from A to C demonstrates the surgical approach to severe spinal cord injury aiming to restore anatomical integrity and promote neuroplasticity. A) Initial condition post-trauma showing a vertebral fracture with adjacent hematoma and edema, leading to spinal cord compression. There is no cerebrospinal fluid (CSF) visible around the spinal cord due to the compression. B) Post-decompressive laminectomy with removal of the posterior vertebral arch to relieve pressure on the spinal cord. The spinal cord shows restored space around it, but still no CSF is visible, indicating potential ongoing compression or adhesions. C) After durotomy and duraplasty, CSF is visible around the spinal cord, indicating decompression. This procedure facilitates an environment for potential neuroplasticity and recovery of function.
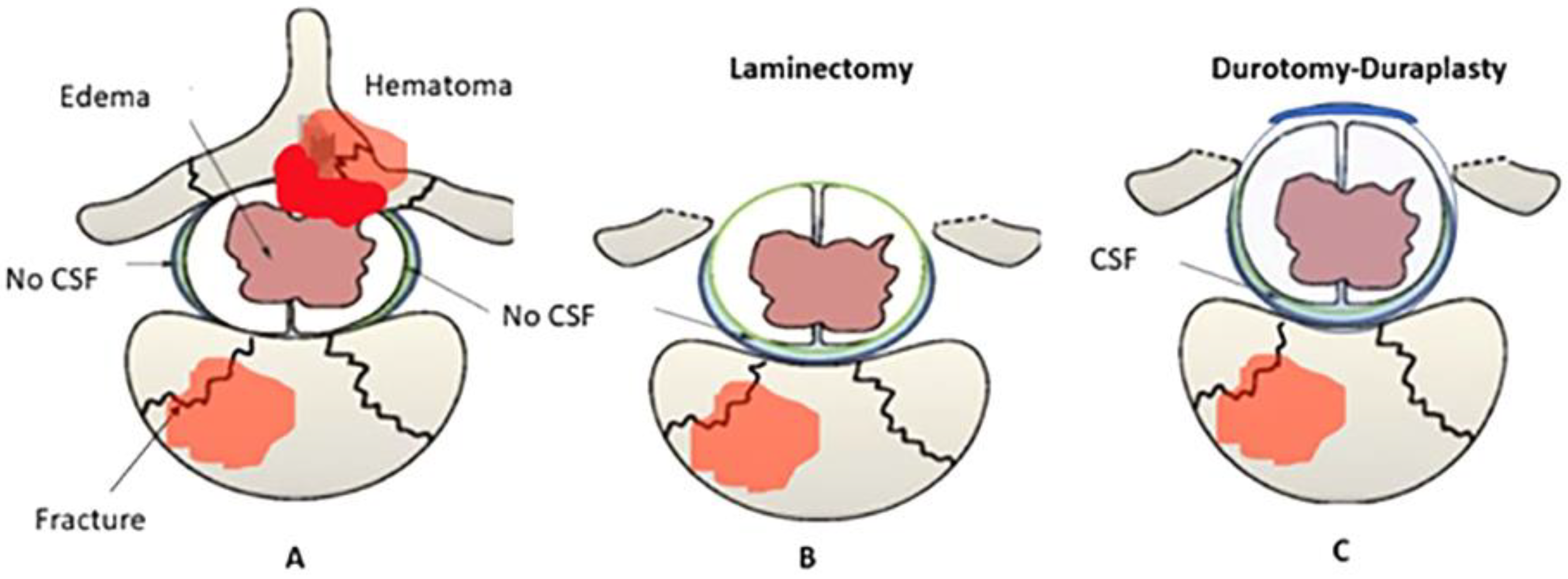
Figure 3.
Case showing preoperative imaging, surgical interventions and postoperative and imaging in severe spinal cord injury management. A) This panel demonstrates multiple unstable cervical and thoracic fractures, highlighting the severe structural compromise and the necessity for surgical intervention. B) Damage to the posterior osteoligamentary structures as a result of injury is depicted, underscoring the extent of trauma and the resultant instability requiring stabilization. C) A severe edema and catastrophic spinal cord contusion at levels C4-5 is shown, illustrating the urgency and complexity of the neurosurgical challenge. D) The surgical field post-decompressive laminectomy is displayed, revealing the direct aftermath of removing the laminae to relieve pressure on the spinal cord. E) The effective decompression post-surgery is evident, showcasing the alleviation of pressure and the potential for improved neurological function. F) Laminectomy at levels C4-5-6 is shown, which is a surgical procedure to remove a portion of the lamina. G) Cervicothoracic stabilization is displayed, indicating the surgical measures taken to secure the spinal integrity following decompression. H) Duraplasty expansion is illustrated, which is used to provide additional space for the spinal cord and nerves by expanding the dural sac.
Figure 3.
Case showing preoperative imaging, surgical interventions and postoperative and imaging in severe spinal cord injury management. A) This panel demonstrates multiple unstable cervical and thoracic fractures, highlighting the severe structural compromise and the necessity for surgical intervention. B) Damage to the posterior osteoligamentary structures as a result of injury is depicted, underscoring the extent of trauma and the resultant instability requiring stabilization. C) A severe edema and catastrophic spinal cord contusion at levels C4-5 is shown, illustrating the urgency and complexity of the neurosurgical challenge. D) The surgical field post-decompressive laminectomy is displayed, revealing the direct aftermath of removing the laminae to relieve pressure on the spinal cord. E) The effective decompression post-surgery is evident, showcasing the alleviation of pressure and the potential for improved neurological function. F) Laminectomy at levels C4-5-6 is shown, which is a surgical procedure to remove a portion of the lamina. G) Cervicothoracic stabilization is displayed, indicating the surgical measures taken to secure the spinal integrity following decompression. H) Duraplasty expansion is illustrated, which is used to provide additional space for the spinal cord and nerves by expanding the dural sac.
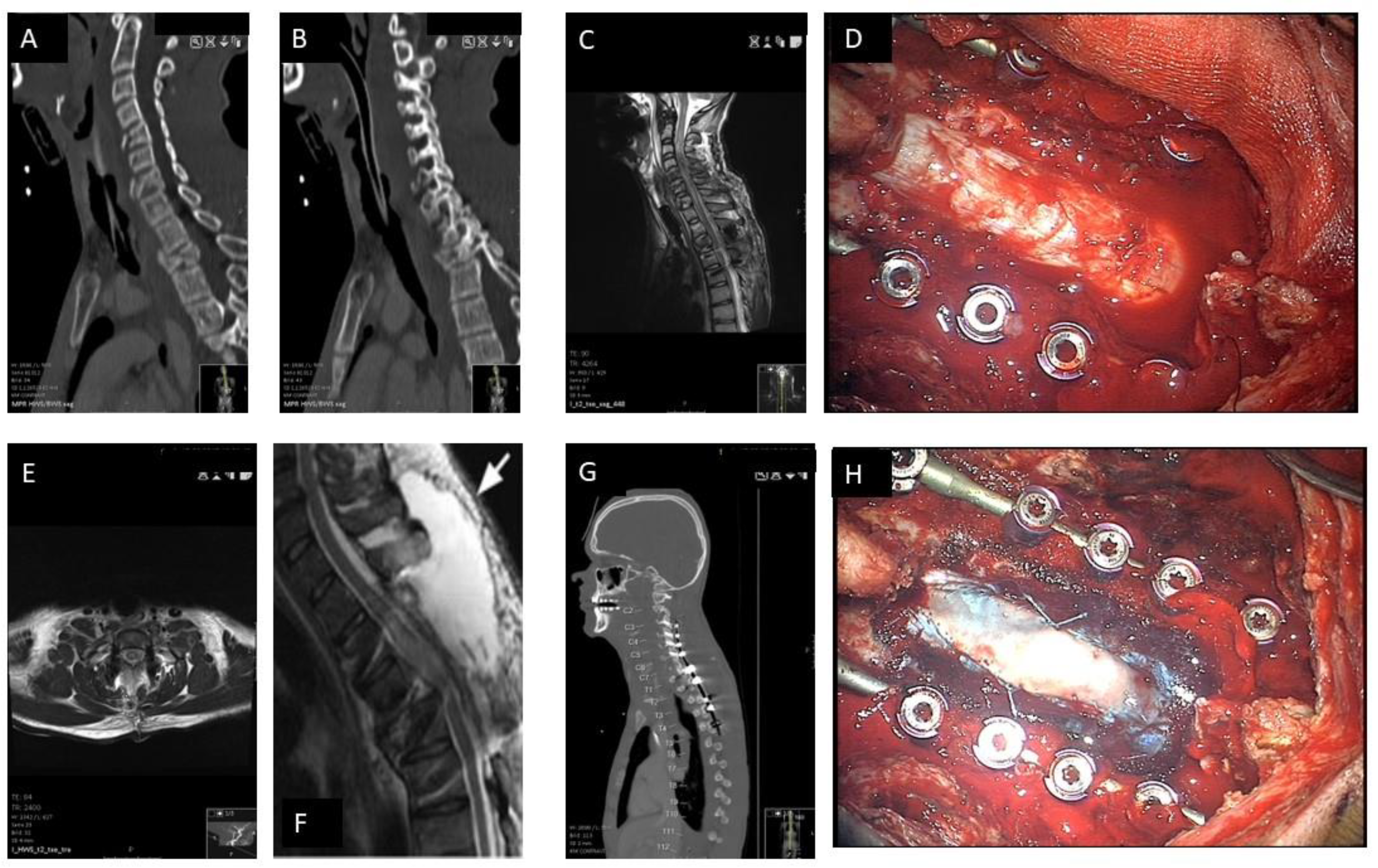

Table 1.
Timeline of Spinal Cord Injury and Neuroplasticity events under pathophysiological aspects: There are three stages after spinal cord injury: an acute phase (<48 hours) directly after the trauma, with an early immune response and limited neuroplasticity. A Subacute Phase (2-14 days) with early plasticity and glial scar formation. An intermediate and chronic phase (>14 days and over six months) with chronic inflammation events and adaptive and maladaptive plasticity attempts.
Table 1.
Timeline of Spinal Cord Injury and Neuroplasticity events under pathophysiological aspects: There are three stages after spinal cord injury: an acute phase (<48 hours) directly after the trauma, with an early immune response and limited neuroplasticity. A Subacute Phase (2-14 days) with early plasticity and glial scar formation. An intermediate and chronic phase (>14 days and over six months) with chronic inflammation events and adaptive and maladaptive plasticity attempts.
| Timeline | SCI Injury mechanism | Neuroplasticity |
| Acute (<48 hours)[1,2,3,5,10,15] |
Primary Injury: Direct trauma leads to hemorrhage, axonal shearing, and cellular necrosis. Demyelination and Necrosis: Demyelination and neuronal cell death rapidly follow mechanical damage. Blood-Spinal Cord Barrier Disruption (BSCB): A breach in the BSCB leads to increased permeability, allowing immune cell infiltration, especially neutrophils, which release metalloproteinase-9 (MMP-9), worsening tissue breakdown. Inflammation: Early immune response with neutrophil and macrophage infiltration. Pro-inflammatory cytokines (TNF-α, IL-1β, IL-6) are upregulated, activating M1 microglia, releasing cytotoxic glutamate and nitric oxide, increasing cell death. |
Limited Neuroplasticity: Immediately following injury, neuroplasticity is significantly impaired due to the release of cytotoxic substances like glutamate. Synaptic circuits are abruptly disrupted, causing widespread loss of function. - Glutamate Toxicity: Excessive glutamate release causes excitotoxic damage, inhibiting early neural regeneration. - Neurotrophic Response: Limited neuroprotective responses, such as brain-derived neurotrophic factor (BDNF) upregulation, are present but insufficient to counteract acute damage. - Axonal Injury: Axons near the injury site degenerate, reducing the potential for early plastic changes. |
| Subacute (2-14 days)[3,15,16,18,34,37,38] |
Continued Inflammation: The immune response escalates, with macrophages, T cells, and lymphocytes infiltrating the injury site. The presence of pro-inflammatory cytokines continues, prolonging tissue damage and cell death. Astrocytic and Glial Activation: Astrocytes proliferate and become reactive, losing aquaporin-4 (AQP4) activity. This worsens BSCB permeability and disrupts glutamate reuptake, contributing to neurotoxicity. Formation of CSPGs: Reactive astrocytes secrete chondroitin sulfate proteoglycans (CSPGs), inhibiting axonal regrowth. Ependymal Cell Activation: Self-renewing ependymal cells migrate to the injury site, forming astrocytes and contributing to scar formation. Glial Scar Formation Begins: Scar tissue, formed by activated astrocytes and fibrotic tissue, acts as a physical and chemical barrier to axonal regeneration. |
Early Plasticity : Some axonal sprouting occurs near the injury site, but neuroplasticity is primarily inhibited by CSPGs and the glial scar formation. -Ependymal Cell Contribution: Ependymal cells activate and proliferate, but their differentiation is mostly glial-biased (towards astrocytes), which limits their ability to support neuronal regeneration. -Axonal Sprouting and Circuit Reorganization: Axons near the lesion site begin sprouting, though inhibitory molecules like CSPGs largely block the growth. Maladaptive Changes: Initial signs of maladaptive neuroplasticity, such as aberrant sprouting or hyperexcitability, may appear, contributing to dysfunctional sensory and motor circuits. |
| Intermediate & Chronic Phase (>14 days/6 months)[3,10,15,16,19,20,25,34] |
Consolidation of Glial Scar: The glial scar, consisting of reactive astrocytes, macrophages, and CSPGs, fully develops, surrounding the fibrotic core formed by type A pericytes. This scar severely limits any potential for axonal regrowth. Chronic Inflammation: Microglia and macrophages continue to release pro-inflammatory cytokines, perpetuating neuroinflammation and preventing tissue repair. Wallerian Degeneration: Axonal degeneration (Wallerian degeneration) occurs distal to the injury, contributing to the ongoing loss of neural tissue. Demyelination: Ongoing demyelination of surviving neurons results in further functional loss, and oligodendrocyte apoptosis impairs remyelination efforts. Neuroimmune Modulation: Some immune cells (e.g., CD4+ T lymphocytes) may help shift the immune environment towards a more neuroprotective state, promoting limited repair mechanisms. |
Adaptive and Maladaptive Plasticity: Significant neuroplastic changes occur, with both beneficial (adaptive) and harmful (maladaptive) consequences. - Adaptive Plasticity: Propriospinal neurons, which span different spinal cord segments, sprout and form new synaptic connections to bridge the injury site. These new circuits can support partial recovery of motor functions. -Maladaptive Plasticity: Abnormal reorganization of spinal circuits may lead to spasticity, hyperreflexia, and sensory-evoked spasms, which worsen quality of life. Propriospinal Circuit Reorganization: Propriospinal neurons play a key role in forming compensatory circuits, enabling some recovery of locomotion, especially with rehabilitation interventions. Potential for Neurogenesis: Though limited, some endogenous neural stem/progenitor cells may contribute to neurogenesis, especially in the presence of factors like IL-4, which promote axonal growth and neurotrophic support. |
List of Abbreviations: BSCB: Blood-Spinal Cord Barrier; MMP-9: Metalloproteinase-9; TNF-α: Tumor Necrosis Factor-alpha; IL-1β: Interleukin-1 beta; IL-6: Interleukin-6; CSPGs: Chondroitin Sulfate Proteoglycans; BDNF: Brain-Derived Neurotrophic Factor; AQP4: Aquaporin-4; IGF-1: Insulin-Like Growth Factor-1; GDNF: Glial Cell Line-Derived Neurotrophic Factor; OPCs: Oligodendrocyte Progenitor Cells; SCI: Spinal Cord Injury; NPCs: Neural Progenitor Cells; SOCS: Suppressors of Cytokine Signaling; CXCR4: C-X-C Chemokine Receptor Type 4; SDF-1: Stromal Cell-Derived Factor-1; MAPK: Mitogen-Activated Protein Kinase; WNT: Wingless-Related Integration Site (signaling pathway).
Table 2.
Summary of the included Studies in the Systematic Review. Each study is categorized by its study design, population, intervention, and outcomes.
Table 2.
Summary of the included Studies in the Systematic Review. Each study is categorized by its study design, population, intervention, and outcomes.
| Study | Study Design | Population | Intervention | Outcomes | |
| 1 | Garg et al., 2022 | Clinical - Retrospective | 18 patients (SCI) | Decompressive laminectomy + duraplasty | Improved ITP, SCPP, neuroplasticity markers |
| 2 | Phang et al., 2015 | Clinical - Observational | 25 patients (SCI) | Perfusion monitoring | Improved SCPP and pressure reactivity |
| 3 | Curt et al., 2008 | Clinical - Review | Variable (SCI) | NA | Neuroplasticity mechanisms |
| 4 | Kornblith et al., 2013 | Clinical - Multicenter | 150 patients (SCI) | Mechanical ventilation strategies | Improved extubation rates |
| 5 | Lenehan et al., 2012 | Clinical - Epidemiological | Population-based | NA | Epidemiological insights |
| 6 | Thietje et al., 2011 | Clinical - Retrospective | 62 patients (Deceased SCI) | Mortality analysis | Mortality and cause insights |
| 7 | Keefe et al., 2017 | Preclinical - Animal | Rodent models | Neurotrophic factor modulation | Increased BDNF, NGF levels |
| 8 | Stoyanova et al., 2021 | Preclinical - Animal | Rodent models | Ghrelin-mediated plasticity | Enhanced regeneration |
| 9 | Yue et al., 2020 | Clinical - Prospective | 35 patients (SCI) | Perfusion protocols | Enhanced functional recovery |
| 10 | Saadoun et al., 2020 | Clinical - Observational | 20 patients (SCI) | Targeted perfusion therapy | Reduced edema, improved outcomes |
| 11 | Leonard et al., 2015 | Preclinical - Animal | Rodent models | Substance P modulation | Reduced inflammation and edema |
| 12 | Punjani et al., 2023 | Preclinical - Review | Mixed human/animal data | Plasticity pathways | Highlighted neuroplasticity mechanisms |
| 13 | Zhu et al., 2019 | Clinical - Retrospective | 30 patients (SCI) | Durotomy with duroplasty | Improved motor function and reduced intrathecal pressure |
| 14 | Ahuja et al., 2017 | Clinical - Systematic Review | Variable population (SCI) | Repair and regeneration strategies | Insights on neuroplasticity and axonal repair |
| 15 | Leonard et al., 2013 | Preclinical - Animal | Rodent models | Substance P modulation | Reduced inflammation and improved functional outcomes |
| 16 | Gotz et al., 2015 | Preclinical - Animal | Rodent models | Astrocytic plasticity interventions | Enhanced synaptic remodeling and axonal regeneration |
| 17 | Lau et al., 2011 | Preclinical - Animal | Lamprey brain models | Neurite sprouting post-SCI | Increased synapsin expression and sprouting |
| 18 | Anjum et al., 2020 | Clinical - Observational | 50 patients (SCI) | Inflammation-targeted therapies | Reduced secondary damage and improved recovery |
| 19 | Dimou and Gallo, 2015 | Preclinical - Review | Various animal models | NG2-glia functions | Insights into glial plasticity and neurogenesis |
| 20 | Guo et al., 2019 | Preclinical - Animal | Mouse models | Gene expression modulation | Identification of genes promoting regeneration |
| 21 | Bulsara et al., 2002 | Preclinical - Animal | Rodent models | Growth-associated genes | Enhanced axonal sprouting and plasticity |
| 22 | Cozzens et al., 2013 | Clinical - Systematic Review | Variable population (SCI) | Cervical spine and spinal cord injury management | Guidelines for early intervention |
| 23 | Zhong et al., 2023 | Preclinical - Animal | Rat models | PI3K/AKT signaling pathways | Improved axonal growth and synaptogenesis |
| 24 | Bobinger et al., 2018 | Preclinical - Review | Mixed models | Apoptotic pathways in neural injury | Insights on reducing cell death post-injury |
| 25 | Lee et al., 2010 | Preclinical - Animal | Rodent models | Ghrelin for apoptosis inhibition | Improved functional recovery |
| 26 | Le Feber et al., 2016 | Preclinical - In vitro | Neural cultures | Neuronal damage progression in ischemia | Modeling SCI-like ischemic conditions |
| 27 | Stoyanova et al., 2022 | Preclinical - Animal | Rodent models | Hypoxia-induced Pax6 modulation | Enhanced neuronal survival and regeneration |
| 28 | Galtrey and Fawcett, 2007 | Preclinical - Review | Mixed models | Role of CSPGs in regeneration | Reduction of inhibitory signaling |
| 29 | Saadoun et al., 2020 | Clinical - Observational | 25 patients (SCI) | Perfusion-targeted therapies | Reduced edema and improved SCPP |
| 30 | Sun et al., 2023 | Preclinical - Animal | Mouse models | Stem cells and exercise | Enhanced recovery via PI3K/AKT pathways |
| 31 | Grassner et al., 2018 | Clinical - Review | Variable population | Spinal meninges in SCI | Neuroanatomical insights into recovery |
| 32 | Phang et al., 2016 | Clinical - Retrospective | 20 patients (SCI) | Magnetic resonance imaging in perfusion monitoring | Improved spinal cord perfusion visualization |
| 33 | Miao et al., 2023 | Preclinical - Animal | Rodent models | Neuroplasticity via TrKA pathways | Enhanced neurite elongation and recovery |
| 34 | Werndle et al., 2014 | Clinical - Observational | 30 patients (SCI) | Perfusion pressure monitoring | Reduced secondary injury through SCPP improvements |
| 35 | Kwon et al., 2009 | Clinical - Randomized | 40 patients (SCI) | Intrathecal pressure monitoring | Improved outcomes via drainage protocols |
| 36 | Chen et al., 2017 | Preclinical - Animal | Rat models | BDNF signaling in synaptogenesis | Enhanced recovery of motor function |
| 37 | Varsos et al., 2015 | Clinical - Observational | 30 patients (SCI) | Spinal perfusion pressure dynamics | Reduced pressure-related damage |
| 38 | Leonard et al., 2015 | Preclinical - Animal | Rodent models | Edema and hemorrhage contributions | Reduction of post-injury complications |
| 39 | Fehlings et al., 2006 | Clinical - Systematic Review | Variable population (SCI) | Timing of intervention | Guidelines for early surgical decompression |
| 40 | Anjum et al., 2020 | Preclinical - Animal | Rodent models | Multi-molecular interactions post-SCI | Insights on recovery mechanisms |
| 41 | Gotz et al., 2015 | Preclinical - Animal | Rodent models | Reactive astrocyte modulation | Improved synaptic plasticity |
| 42 | Ahuja et al., 2017 | Clinical - Retrospective | 50 patients (SCI) | Surgical repair strategies | Improved outcomes via axonal repair |
| 43 | Saadoun et al., 2020 | Clinical - Observational | 20 patients (SCI) | Perfusion-targeted interventions | Improved SCPP and reduced edema |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



