
Submitted:
30 December 2024
Posted:
08 January 2025
You are already at the latest version
Abstract
Liver Sinusoidal Endothelial Cells (LSECs) play a crucial role in maintaining liver homeostasis, regulating immune responses, and regulating fibrosis in liver diseases. This review explores the unique functions of LSECs in liver pathology, particularly their roles in immune tolerance, antigen presentation, and the modulation of hepatic stellate cells (HSCs) during fibrosis. LSECs act as key regulators of immune balance in the liver by preventing excessive immune activation while also filtering antigens and interacting with immune cells, including Kupffer cells and T cells.
Metabolic dysfunction-associated steatohepatitis (MASH) is a severe form of liver disease characterized by steatosis (fatty liver), inflammation, and fibrosis in the liver. It progresses from metabolic dysfunction-associated steatotic liver disease (MASLD), commonly known as non-alcoholic fatty liver disease (NAFLD). MASH is significant because it can lead to advanced liver dysfunction, such as cirrhosis and liver cancer. The prevalence of MASH is increasing globally, particularly in the United States, and is closely linked to rising rates of obesity and type 2 diabetes. Early diagnosis and intervention are vital to prevent severe outcomes, highlighting the importance of studying LSECs in MASH liver disease. However, during chronic liver diseases such as NAFLD, alcoholic liver disease (ALD), and viral hepatitis, LSECs undergo dysfunction, leading to their capillarization, loss of fenestrations, and promotion of pro-fibrotic signaling pathways such as TGF-β.
The review also discusses the dynamic interaction between LSECs, HSCs, and other hepatic cells during the progression of liver diseases, emphasizing how changes in LSEC phenotype contribute to liver scarring and fibrosis. Furthermore, it highlights the potential of LSECs as therapeutic targets for modulating immune responses and preventing fibrosis in liver diseases. By restoring LSEC function and targeting pathways associated with their dysfunction, novel therapies could be developed to halt or reverse liver disease progression. The findings of this review reinforce the importance of LSECs in liver pathology and suggest that they hold significant promises as targets for future treatment strategies aimed at addressing chronic liver diseases.
Keywords:
LSECs
; Immune regulation
; Liver fibrosis
; MASH liver disease
; Immune tolerance
; LSEC dysfunction
; and LSEC as therapeutic targets
1. Introduction
1.1. Liver's Unique Role in Immune Regulation and the Critical Function of Liver Sinusoidal Endothelial Cells (LSECs)
The liver plays a central role in immune regulation and functions to filter blood from the gastrointestinal tract, which is rich in antigens, nutrients, and toxins. Unlike other organs, the liver has developed mechanisms to maintain immune tolerance while simultaneously preventing infections and excessive immune responses. This immunological balance is critical for preventing damage to the liver itself, which can otherwise lead to inflammation and disease[1]. Liver sinusoidal endothelial cells (LSECs), which line the hepatic sinusoids, are vital to this process. Unlike typical endothelial cells, LSECs are highly specialized in their function of filtering blood, clearing pathogens, and presenting antigens. They regulate immune responses by interacting directly with immune cells such as T cells and Kupffer cells (resident macrophages), promoting tolerance to harmless antigens while allowing an appropriate immune response to harmful pathogens[2]. LSECs are, therefore, integral to maintaining hepatic homeostasis and preventing immune-mediated damage in the liver[3].
MASH is a severe form of liver disease characterized by inflammation and fibrosis due to the accumulation of fat in the liver. It progresses from MASLD, commonly known as non-alcoholic fatty liver disease (NAFLD). MASH is particularly significant because it can lead to advanced liver conditions such as cirrhosis and liver cancer, which are life-threatening. The prevalence of MASH is increasing globally, with a notable rise in the United States. It is estimated that by 2030, around 27 million adults in the US will be living with MASH, up from 17 million in 2016[4]. This rise is closely linked to the increasing rates of obesity and type 2 diabetes, which are major risk factors for the development of MASH. The economic impact of MASH is substantial, with direct healthcare costs in the US amounting to $22.51 billion in 2021 and productivity losses estimated at $106.32 billion.
Clinically, MASH is challenging to diagnose in its early stages due to the lack of specific symptoms, which often leads to underdiagnosis and delayed treatment. The progression of MASH can result in significant liver damage, necessitating early detection and intervention to prevent severe outcomes. Understanding the prevalence, risk factors, and clinical significance of MASH is crucial for developing effective public health strategies and therapeutic interventions to manage and mitigate this growing health concern[5].
Liver Sinusoidal Endothelial Cells (LSECs) are highly specialized endothelial cells that form the unique lining of the hepatic sinusoids. Unlike the continuous endothelium found in other organs, LSECs are characterized by fenestrations—small pores in their membrane that facilitate the exchange of molecules between blood and hepatocytes. These fenestrations, along with the lack of a basement membrane, allow LSECs to filter blood efficiently, controlling the passage of lipoproteins, proteins, and immune molecules into the liver parenchyma. Positioned between the blood flow and hepatocytes, LSECs play a crucial role in the clearance of pathogens, toxins, and waste products from the blood. Through scavenger receptors, LSECs rapidly remove circulating antigens, immune complexes, and apoptotic cells, contributing to the liver’s role as a detoxification organ.
LSECs are central to maintaining immune homeostasis within the liver, in addition to their filtering function. These cells are highly active in antigen presentation, taking up antigens from the blood and presenting them to immune cells, including T cells, in a manner that typically promotes immune tolerance rather than activation. This immune-regulatory function of LSECs is crucial, given the liver’s constant exposure to dietary and bacterial antigens from the gut[6]. By promoting tolerance, LSECs prevent unnecessary immune responses that could damage the liver, making them vital to both hepatic immune surveillance and the maintenance of systemic immune balance.
Liver fibrosis, characterized by excessive deposition of extracellular matrix proteins, is a key feature of chronic liver diseases and a precursor to more severe conditions like cirrhosis and liver failure. In fibrosis, the liver's normal architecture is progressively replaced by scar tissue, leading to impaired liver function[7]. This process is largely driven by hepatic stellate cells (HSCs), which are activated in response to liver injury. LSECs play a crucial role in this process by interacting with HSCs and other immune cells. In a healthy liver, LSECs maintain a quiescent state of HSCs through the release of regulatory molecules[8]. However, during liver injury or chronic inflammation, LSECs undergo phenotypic changes that promote the activation of HSCs, leading to fibrosis.[9]. As fibrosis progresses, it compromises the liver’s regenerative capacity and can ultimately result in end-stage liver disease[10]. Understanding how LSECs contribute to both immune regulation and fibrosis development is essential for devising therapeutic strategies aimed at mitigating liver damage and improving patient outcomes[11,12].
The primary objective of this review is to examine the role of LSECs in the regulation of immune responses and the development of fibrosis in chronic liver diseases. While the liver’s immune environment has been extensively studied, there is a growing recognition of the unique contributions of LSECs to liver pathology[13]. Despite their critical roles in immune tolerance, pathogen clearance, and fibrosis modulation, LSECs have historically been underexplored compared to other hepatic cells such as hepatocytes and Kupffer cells. A deeper understanding of LSECs is crucial for developing novel therapeutic approaches that target these cells to prevent or reverse fibrosis and regulate immune responses[14]. By synthesizing recent advances in this area, this review aims to highlight the potential of LSECs as both diagnostic biomarkers and therapeutic targets in the treatment of liver diseases, addressing gaps in the current literature and guiding future research efforts[15].
This review sheds light on and explores the role of LSECs in immune regulation, detailing how these liver cells maintain immune tolerance and interact with various immune cells. It will then examine the involvement of LSECs in the development and progression of liver fibrosis, highlighting their interactions with hepatic stellate cells and other immune cells. The review will also discuss the therapeutic potential of targeting LSECs to modulate immune responses and prevent fibrosis in liver diseases. Finally, it will provide insights into emerging research areas and potential future studies on LSECs, summarizing key findings and the importance of LSECs in liver pathology.
2. Liver Sinusoidal Endothelial Cells: Structure and Function
2.1. Anatomy and Physiology of Liver Sinusoidal Endothelial Cells (LSECs)
Liver Sinusoidal Endothelial Cells (LSECs) are highly specialized endothelial cells that form the unique lining of the hepatic sinusoids, which are microvascular channels in the liver. Unlike the continuous endothelium found in other organs, LSECs are characterized by fenestrations—small pores in their membrane that facilitate the exchange of molecules between blood and hepatocytes. These fenestrations, along with the lack of a basement membrane, allow LSECs to filter blood efficiently, controlling the passage of lipoproteins, proteins, and immune molecules into the liver parenchyma[16]. Positioned between the blood flow and hepatocytes, LSECs play a crucial role in the clearance of pathogens, toxins, and waste products from the blood. Through scavenger receptors, LSECs rapidly remove circulating antigens, immune complexes, and apoptotic cells, contributing to the liver’s role as a detoxification organ[6]. Figure 1 illustrates the structure and function of LSECs in normal and injured stages.
This image illustrates the structural and functional differences in liver sinusoidal endothelial cells (LSECs) between a normal liver (A) and an injured liver (B). In the normal liver, hepatocytes are aligned with fenestrated LSECs, allowing for efficient blood flow and interaction with Kupffer cells, macrophages, and NK cells. Quiescent hepatic stellate cells (qHSC) are present in the Space of Disse. In contrast, the injured liver shows hepatocyte damage, loss of fenestration in LSECs, and the activation of hepatic stellate cells (aHSC) into myofibroblasts, leading to extracellular matrix (ECM) deposition and collagen accumulation. This results in the activation of Kupffer cells, macrophages, and the presence of lymphocytes, NKT cells, and neutrophils, indicating an inflammatory response. The image highlights the critical role of LSECs in maintaining liver function and the pathological changes that occur during liver injury.
In addition to their filtering function, LSECs are central to maintaining immune homeostasis within the liver. These cells are highly active in antigen presentation, taking up antigens from the blood and presenting them to immune cells, including T cells, in a manner that typically promotes immune tolerance rather than activation[17]. This immune-regulatory function of LSECs is crucial, given the liver's constant exposure to dietary and bacterial antigens from the gut. By promoting tolerance, LSECs prevent unnecessary immune responses that could damage the liver, making them vital to both hepatic immune surveillance and the maintenance of systemic immune balance[18].
2.2. Interaction of LSECs with Other Hepatic Cells: Kupffer Cells, Hepatic Stellate Cells (HSCs), and Hepatocytes
LSECs do not function in isolation; their interaction with other hepatic cells is central to liver health and disease. One of the most essential cellular partners of LSECs is Kupffer cells, the resident macrophages of the liver. Kupffer cells are located within the liver sinusoids and are involved in immune surveillance and phagocytosis. LSECs and Kupffer cells collaborate in maintaining immune tolerance; for instance, LSECs uptake and present antigens to Kupffer cells, which then help suppress excessive immune responses. Kupffer cells also respond to inflammatory signals from LSECs, orchestrating broader immune responses when necessary, such as during infections or liver injury[19,20].
LSECs also play a key role in the activation and regulation of hepatic stellate cells (HSCs), the primary cells responsible for liver fibrosis. Under normal conditions, LSECs help maintain HSCs in a quiescent state by releasing soluble factors like nitric oxide, which suppress HSC activation0[21]. However, in the context of liver injury or chronic inflammation, LSECs undergo changes that promote HSC activation. Activated HSCs transform into myofibroblasts, which produce collagen and extracellular matrix proteins, leading to fibrosis. Dysfunctional LSECs, often characterized by a loss of fenestration (capillarization) and an altered secretion profile, are key contributors to the progression of fibrosis. This crosstalk between LSECs and HSCs is a critical factor in liver disease progression, especially in chronic liver conditions like non-alcoholic fatty liver disease (NAFLD) and alcoholic liver disease (ALD)[22].
LSECs also interact with hepatocytes, the primary functional cells of the liver. Hepatocytes depend on LSECs for the efficient delivery of nutrients and signaling molecules. The fenestrations in LSECs allow the transfer of essential molecules such as lipoproteins and hormones to hepatocytes, while hepatocytes, in return, help maintain LSEC function by releasing regulatory factors[23]. During liver injury, the interaction between LSECs and hepatocytes becomes particularly important, as LSECs respond to hepatocyte damage by initiating immune responses and modulating fibrosis through their interaction with HSCs[24]. In conditions like cirrhosis, these interactions become dysregulated, contributing to liver dysfunction and disease progression[25].
LSECs are central to several critical liver functions and processes. Their interactions with Kupffer cells, HSCs, and hepatocytes not only regulate immune responses but also maintain overall liver homeostasis. Understanding these interactions is crucial for identifying new therapeutic approaches aimed at treating liver diseases by targeting the LSEC-mediated pathways.
3. LSECs in Immune Regulation
Liver sinusoidal endothelial cells (LSECs) are specialized endothelial cells lining the hepatic sinusoids. Unlike typical endothelial cells, LSECs are characterized by fenestrations and a lack of basal membrane, allowing them to act as key regulators of hepatic microcirculation and immune surveillance. LSECs play a crucial role in modulating the immune response by presenting antigens and promoting immune tolerance in the liver's unique immune environment, which is constantly exposed to gut-derived antigens and circulating pathogens. This delicate balance ensures that the liver can prevent inappropriate immune activation while still mounting effective immune responses when necessary[26].
3.1. Antigen Presentation and Immune Tolerance
LSECs are involved in the presentation of antigens to immune cells, especially T cells, a process critical for maintaining immune tolerance. Unlike professional antigen-presenting cells (APCs), such as dendritic cells, LSECs have a unique capability to induce tolerance rather than immune activation. They do this by presenting antigens via major histocompatibility complex (MHC) class I and class II molecules to naive T cells, leading to the induction of CD8⁺ T cell tolerance through mechanisms like clonal deletion and anergy[27].
Moreover, LSECs express low levels of costimulatory molecules, such as CD80 and CD86, which are essential for full T cell activation. This deficiency in costimulation skews T cell responses towards tolerance rather than effector functions. Additionally, LSECs secrete immunomodulatory molecules like interleukin-10 (IL-10) and transforming growth factor-beta (TGF-β), which further support the development of regulatory T cells (Tregs) and dampen pro-inflammatory T cell responses[26].
3.2. LSECs and Immune Cell Communication
LSECs communicate with various immune cells, including T cells, macrophages, and Kupffer cells, to regulate immune responses and prevent excessive immune activation.
3.2.1. Interaction with T Cells
LSECs present antigens to T cells in the context of both MHC class I and II molecules. However, due to their low expression of co-stimulatory molecules, they preferentially promote T cell tolerance rather than activation. The cross-presentation of exogenous antigens by LSECs to CD8⁺ T cells in the absence of adequate costimulation leads to T cell apoptosis or the generation of a non-responsive (anergic) state, preventing cytotoxic T lymphocyte (CTL) activation and subsequent tissue damage[28].
3.2.2. Interaction with Macrophages and Kupffer Cells
Kupffer cells, the liver-resident macrophages, play a crucial role in maintaining immune homeostasis in the liver. LSECs closely interact with Kupffer cells and other liver macrophages to modulate immune responses. Through the release of anti-inflammatory cytokines, LSECs help maintain the tolerogenic microenvironment of the liver. In turn, Kupffer cells provide feedback to LSECs by producing signaling molecules like IL-10 and TGF-β, which further enhance the immunosuppressive functions of LSECs[29].
The crosstalk between LSECs and Kupffer cells is essential for preventing excessive immune activation in the liver. Dysregulation of this communication can lead to increased inflammation, as Kupffer cells can switch to a pro-inflammatory phenotype under certain conditions, such as chronic liver disease or infections.
3.3. LSECs in Inflammatory Liver Diseases
Recent studies have highlighted the role of LSECs in the pathogenesis of inflammatory liver diseases, such as Metabolic dysfunction-associated steatohepatitis (MASH), liver fibrosis, and cirrhosis. Dysregulation of LSEC function is associated with increased inflammation and immune activation, contributing to the progression of these conditions. The recent study highlights spatial distribution of LSEC which play a crucial role in liver zonation, particularly in midlobular zone 2, which is essential for understanding fibrosis in MASH liver[30].
3.3.1. Critical Role of LSECs in MASH
In MASH, LSECs undergo morphological changes, including loss of fenestrations (defenestration) and capillarization. These changes impair their ability to regulate immune tolerance, leading to increased infiltration of pro-inflammatory immune cells such as CD8⁺ T cells and macrophages. The resulting inflammation exacerbates liver damage, promoting fibrosis and the progression of MASH to cirrhosis[24].
3.3.2. Liver Fibrosis and Cirrhosis
During liver fibrosis, LSECs lose their fenestrated structure and start behaving more like typical vascular endothelial cells. This process, known as capillarization, reduces their ability to clear antigens and maintain immune tolerance. The dysfunction of LSECs contributes to a pro-inflammatory environment in the liver, with enhanced recruitment of immune cells like monocytes and neutrophils. Over time, this chronic inflammation leads to excessive deposition of extracellular matrix (ECM) by activated hepatic stellate cells, driving fibrosis and eventually cirrhosis[31].
LSECs are critical for maintaining immune tolerance in the liver through antigen presentation, communication with immune cells, and the release of anti-inflammatory cytokines. However, dysregulation of LSEC function can disrupt this balance, leading to chronic inflammation and the progression of liver diseases such as MASH and cirrhosis. Understanding the mechanisms by which LSECs regulate immune responses and how their dysfunction contributes to liver pathology may provide new therapeutic opportunities for inflammatory liver diseases.
4. LSECs in Liver Fibrosis
4.1. LSECs' Influence on Hepatic Stellate Cell Activation and Collagen Deposition Leading to Fibrosis
Liver sinusoidal endothelial cells (LSECs) play a critical role in the regulation of hepatic stellate cells (HSCs), which are the primary cells responsible for collagen deposition and fibrosis in the liver. Under healthy conditions, LSECs help maintain HSCs in a quiescent, non-fibrogenic state by producing soluble factors such as nitric oxide (NO)[32]. NO helps to keep HSCs inactive and prevents the excessive production of extracellular matrix (ECM) proteins, including collagen. However, in the context of chronic liver injury—whether due to viral hepatitis, alcohol abuse, or metabolic disorders like non-alcoholic fatty liver disease (NAFLD)—LSECs undergo functional changes that lead to the activation of HSCs[33].
When LSECs become dysfunctional, they lose their ability to produce sufficient NO and other anti-fibrotic signals. As a result, HSCs are activated, transforming into myofibroblasts—cells responsible for secreting large amounts of collagen and other ECM proteins. This excessive collagen deposition disrupts the liver's normal architecture, leading to scarring and contributing to fibrosis progression[34]. Additionally, capillarization of LSECs, where they lose their fenestrations, exacerbates fibrosis by restricting nutrient and oxygen supply to hepatocytes, thereby promoting liver damage and inflammation[35].
4.2. Signaling Pathways Involved in LSEC-Mediated Fibrosis and Endothelial Dysfunction
Several signaling pathways are involved in LSEC-mediated fibrosis and endothelial dysfunction. One of the most crucial pathways is the transforming growth factor-beta (TGF-β) signaling pathway. TGF-β is a potent pro-fibrotic cytokine that plays a major role in the activation of HSCs. Dysfunctional LSECs can produce increased levels of TGF-β, which directly stimulates HSC activation and collagen production. Furthermore, LSECs themselves become more susceptible to the effects of TGF-β, which contributes to their capillarization and loss of normal function[36].
Another significant pathway is the vascular endothelial growth factor (VEGF) signaling pathway. Under normal conditions, VEGF maintains the fenestrated structure of LSECs and supports their survival. In chronic liver disease, reduced VEGF signaling leads to capillarization of LSECs, contributing to fibrosis. Capillarized LSECs exhibit characteristics similar to vascular endothelial cells, further promoting inflammation and fibrosis by interacting with immune cells and HSCs in a pathological manner[37].
Oxidative stress is also a significant factor in LSEC-mediated fibrosis. In conditions such as alcoholic liver disease or fatty liver disease, increased oxidative stress leads to the production of reactive oxygen species (ROS), which damage LSECs and contribute to their dysfunction. This, in turn, leads to the activation of pro-fibrotic signaling pathways such as platelet-derived growth factor (PDGF), which further stimulates HSC activation and collagen production[38].
4.3. Changes in LSEC Phenotype Exacerbate Fibrosis and Liver Scarring
Studies show that changes in LSEC phenotype, such as capillarization and loss of anti-fibrotic signaling, significantly exacerbate fibrosis and liver scarring. LSECs from fibrotic livers exhibited increased expression of TGF-β and decreased expression of NO-producing enzymes. These changes were correlated with heightened HSC activation and collagen deposition, indicating a direct role of LSEC dysfunction in fibrosis progression[39]. By restoring NO levels in LSECs, it helped mitigate fibrosis by inhibiting HSC activation.
Similarly, other studies emphasized that Capillarized LSECs were less effective at filtering blood and regulating immune cell recruitment. The loss of fenestrations in LSECs led to the enhanced recruitment of inflammatory macrophages, which further stimulated HSC activation and promoted liver scarring. Targeting LSEC capillarization was proposed as a potential therapeutic strategy to prevent fibrosis[40].
These findings underscore the critical role of LSECs in the progression of liver fibrosis and suggest that therapeutic approaches aimed at restoring LSEC function could be effective in reducing fibrosis and preventing liver disease progression.
5. LSECs in Liver Disease Progression
5.1. LSECs' Contribution to the Progression of Chronic Liver Diseases (NAFLD, ALD, and Viral Hepatitis)
Liver Sinusoidal Endothelial Cells (LSECs) are pivotal players in the progression of chronic liver diseases such as non-alcoholic fatty liver disease (NAFLD), alcoholic liver disease (ALD), and viral hepatitis. In these diseases, LSECs undergo functional and structural changes that compromise their ability to maintain liver homeostasis, leading to inflammation, fibrosis, and eventually cirrhosis.
In NAFLD, a disease characterized by the accumulation of fat in the liver, LSECs contribute to disease progression by becoming dysfunctional as fat accumulation increases. As NAFLD progresses to non-alcoholic steatohepatitis (NASH), LSECs experience capillarization, where they lose their fenestrations and take on characteristics like vascular endothelial cells[23]. This loss of fenestration impairs the ability of LSECs to filter blood properly, leading to reduced clearance of lipids and toxins. Dysfunctional LSECs also produce inflammatory cytokines like tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), which amplify local inflammation and exacerbate liver injury[41]. These inflammatory signals further promote the activation of hepatic stellate cells (HSCs), leading to increased collagen deposition and fibrosis[42].
In ALD, chronic exposure to alcohol induces oxidative stress and damages LSECs[43]. Alcohol metabolism generates reactive oxygen species (ROS), which lead to endothelial dysfunction. LSECs in ALD become Capillarized and lose their ability to regulate immune tolerance, resulting in excessive immune activation. This immune dysregulation promotes inflammation, hepatocyte death, and fibrosis. Additionally, LSECs in ALD show an increase in the expression of vascular endothelial growth factor (VEGF), a response to hypoxic conditions created by alcohol-induced liver damage[16]. This shift exacerbates angiogenesis and fibrosis, further contributing to the progression of liver disease.
In viral hepatitis (such as hepatitis B and C), LSECs play a crucial role in modulating immune responses. LSECs interact with viral antigens and present them to immune cells, but in the context of chronic infection, this immune interaction becomes dysregulated. Chronic hepatitis leads to sustained inflammation, and LSECs lose their immune-regulatory capacity[44]. In these conditions, LSECs contribute to fibrosis by increasing the expression of pro-fibrotic factors like TGF-β, which activates HSCs. The continuous inflammatory environment created by viral infection drives LSECs to promote both inflammation and fibrogenesis, which accelerates the progression of liver disease to cirrhosis.
5.2. Interplay Between LSECs and Other Liver Cells During Liver Disease Progression
The progression of liver disease, from early inflammation to advanced fibrosis and cirrhosis, involves a dynamic interplay between LSECs and other liver cells, including hepatocytes, hepatic stellate cells (HSCs), and immune cells like Kupffer cells. This cellular crosstalk is critical in determining the outcome of liver injury and the rate at which chronic liver diseases progress[14].
In the early stages of liver disease, such as in NAFLD or viral hepatitis, LSECs play a protective role by maintaining immune tolerance and preventing excessive immune activation. LSECs filter antigens from the bloodstream and communicate with Kupffer cells, the liver’s resident macrophages, to modulate immune responses. However, as liver injury persists, LSECs lose their protective role. Inflammatory signals from damaged hepatocytes and infiltrating immune cells, such as macrophages and neutrophils, trigger LSECs to release pro-inflammatory and pro-fibrotic factors[45].
As inflammation becomes chronic, LSECs begin to interact with hepatic stellate cells (HSCs) in a more pathological manner. Normally, LSECs release anti-fibrotic signals such as nitric oxide (NO), which keeps HSCs in a quiescent state. However, during liver injury, LSECs reduce NO production and increase the release of TGF-β and PDGF. These signals activate HSCs, causing them to differentiate into myofibroblasts, which produce collagen and other extracellular matrix proteins that lead to fibrosis. This activation of HSCs is a hallmark of the fibrotic response in chronic liver diseases[32].
In advanced fibrosis and cirrhosis, the liver architecture becomes severely disrupted. LSECs undergo capillarization, losing their fenestrations and their ability to regulate blood flow and filtration. The capillarized LSECs promote further fibrosis by supporting angiogenesis, which is mediated by VEGF. This abnormal blood vessel formation creates a hypoxic environment that perpetuates liver scarring and dysfunction. At this stage, the interplay between LSECs, HSCs, and immune cells becomes a vicious cycle, with continuous collagen deposition, inflammation, and liver remodeling. Cirrhotic livers also show increased interaction between LSECs and macrophages recruited from the bloodstream, which produce additional pro-inflammatory and pro-fibrotic signals, accelerating liver failure[31].
LSECs are central to both the initiation and progression of liver diseases. From maintaining immune homeostasis in the early stages to contributing to fibrosis and cirrhosis in later stages, LSECs play a dual role in both protecting and damaging the liver, depending on the context of disease and progression. Understanding the mechanisms behind LSEC dysfunction and their interactions with other liver cells offers potential therapeutic targets to halt or reverse liver disease progression.
6. Stages of MASH Liver and Therapeutic Strategies
6.1. Hepatic Steatosis (Fatty Liver)
Hepatic steatosis, or fatty liver, is the initial stage of MASH, characterized by the accumulation of excess fat within hepatocytes. This stage is often asymptomatic and can be reversible with lifestyle modifications such as diet and exercise. During this stage, Liver Sinusoidal Endothelial Cells (LSECs) maintain their fenestrated structure, allowing efficient exchange of nutrients and waste products between the blood and hepatocytes[46]. Therapeutic strategies at this stage focus on lifestyle interventions and metabolic regulation to prevent progression to more severe stages.
6.2. Hepatic Fibrosis
Persistent inflammation and liver cell injury result in fibrosis, where scar tissue forms and disrupts the normal liver architecture. LSECs undergo significant capillarization, contributing to the progression of fibrosis by promoting the activation of hepatic stellate cells (HSCs) and the deposition of extracellular matrix (ECM). Therapeutic strategies at this stage focus on anti-fibrotic agents that target the ECM-LSEC interaction and mechano-transduction pathways, aiming to reverse fibrosis and restore normal liver function.
6.3. Cirrhosis
Advanced fibrosis leads to cirrhosis, characterized by extensive scarring that replaces healthy liver tissue. Cirrhosis severely impairs liver function and can lead to liver failure. LSECs are extensively Capillarized, further exacerbating liver dysfunction and contributing to portal hypertension and impaired blood flow. Therapeutic strategies at this stage are more challenging and focus on managing symptoms, reducing portal hypertension, and improving liver regeneration. Potential therapies include agents that enhance endothelial function and reduce fibrosis[47].
6.4. Hepatocellular Carcinoma (HCC)
In some cases, cirrhosis can progress to hepatocellular carcinoma (HCC), a type of liver cancer. LSECs may contribute to the tumor microenvironment by promoting angiogenesis and providing a supportive niche for cancer cells. Therapeutic strategies at this stage focus on targeting the tumor vasculature and inhibiting angiogenesis, potentially using anti-angiogenic agents and immune modulators[48].
7. LSECs as Therapeutic Target
7.1. Therapeutic approaches targeting LSECs to prevent or reverse liver fibrosis and modulate immune responses.
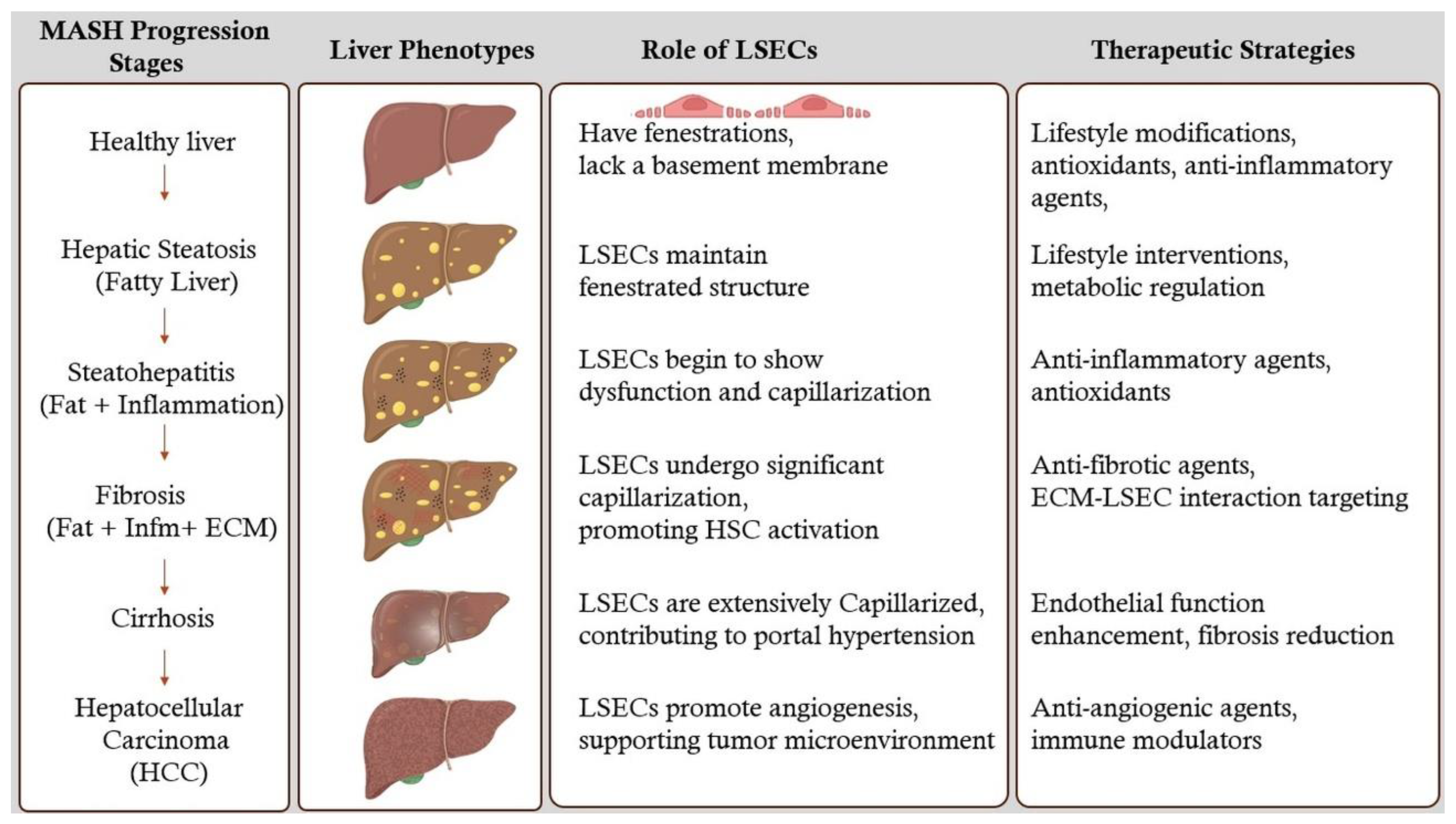
LSECs are specialized endothelial cells lining the sinusoids of the liver. They play a pivotal role in maintaining hepatic homeostasis, regulating immune responses, and modulating extracellular matrix (ECM) dynamics. Dysfunction or capillarization of LSECs is a hallmark of liver fibrosis, a progressive condition characterized by excessive deposition of ECM components leading to impaired liver function. Consequently, targeting LSECs has emerged as a promising therapeutic strategy to prevent or reverse liver fibrosis and modulate immune responses[16]. Figure 2 illustrates the MASH liver progression stages, role of LSECs and therapeutic strategies for designing. This section reviews the potential therapeutic approaches targeting LSECs and discusses current and emerging treatments aimed at enhancing LSEC function or inhibiting the fibrotic cascade.
This figure illustrates the progression stages of Metabolic metabolic-associated steatohepatitis (MASH) with associated liver phenotypes and the role of Liver Sinusoidal Endothelial Cells (LSECs). It highlights the importance of understanding LSECs in these stages to design and develop therapeutic strategies for identifying drug targets. The stages include Healthy Liver, Hepatic Steatosis (Fatty Liver), Steatohepatitis (Fat + Inflammation), Fibrosis (Fat + Inflammation + ECM), Cirrhosis, and Hepatocellular Carcinoma (HCC). Each stage is accompanied by visual representations of liver phenotypes, descriptions of LSECs' roles, and suggested therapeutic strategies, emphasizing the critical role of LSECs in disease progression and potential drug targets.
7.1.1. Potential Therapeutic Approaches Targeting LSECs
a. Restoration of LSEC Phenotype and Function
Under healthy conditions, LSECs exhibit fenestrations that facilitate the exchange of substrates between the blood and hepatocytes. In liver fibrosis, LSECs undergo capillarization—loss of fenestrations and formation of a basement membrane—leading to impaired liver function and promotion of fibrogenesis. Therapeutic strategies aimed at restoring the fenestrated phenotype and functional integrity of LSECs are thus essential.
- Vasoactive Agents: Agents such as vascular endothelial growth factor (VEGF) and nitric oxide (NO) donors can promote the maintenance of LSEC fenestrations and prevent capillarization. Enhancing VEGF signaling has been shown to sustain LSEC differentiation and function[16].
- Shear Stress Modulators: LSECs respond to shear stress induced by blood flow. Modulating shear stress through mechanical or pharmacological means can influence LSEC phenotype and prevent fibrosis progression[49].
b. Inhibition of Pro-fibrotic Signaling Pathways
LSECs interact closely with hepatic stellate cells (HSCs), the primary fibrogenic cells in the liver. Dysfunctional LSECs release factors that activate HSCs, promoting fibrosis. Targeting the signaling pathways involved in LSEC-mediated HSC activation is a viable therapeutic approach.
- TGF-β Signaling Inhibitors: Transforming growth factor-beta (TGF-β) is a key cytokine involved in HSC activation. Inhibiting TGF-β signaling in LSECs can reduce their pro-fibrotic influence on HSCs[50].
- Notch Pathway Modulators: The Notch signaling pathway in LSECs influences vascular remodeling and fibrogenesis. Modulating Notch signaling may attenuate fibrotic responses[51].
c. Modulation of Immune Responses
LSECs are integral to hepatic immune surveillance and tolerance. In liver fibrosis, LSEC dysfunction contributes to an aberrant immune environment. Therapeutic strategies that restore proper immune modulation by LSECs can mitigate fibrosis and inflammation.
- Immune Checkpoint Modulators: Targeting immune checkpoints such as PD-L1 on LSECs can regulate T cell responses, reducing chronic inflammation and fibrogenesis[52].
- Cytokine Therapy: Administering anti-inflammatory cytokines or inhibitors of pro-inflammatory cytokines can rebalance the immune milieu toward fibrosis resolution[53].
7.1.2. Current and Emerging Treatments Targeting LSECs
a. Pharmacological Agents Enhancing LSEC Function
Several drugs are currently under investigation or in use that aim to improve LSEC function, thereby preventing or reversing liver fibrosis.
- Statins: Beyond their lipid-lowering effects, statins have been shown to improve endothelial function. In LSECs, statins can enhance nitric oxide production, maintain fenestrations, and inhibit HSC activation. Clinical studies have suggested that statin therapy may slow fibrosis progression in chronic liver diseases[54].
- Angiogenesis Inhibitors: While angiogenesis is often associated with pathological conditions, controlled inhibition can prevent aberrant vascular remodeling in fibrosis. Agents targeting VEGF receptors may help maintain LSEC structure and function[31].
- FXR Agonists: Farnesoid X receptor (FXR) agonists, such as obeticholic acid, have hepatoprotective and anti-fibrotic effects. They modulate bile acid metabolism and exhibit anti-inflammatory properties that indirectly benefit LSEC function[55].
b. Antifibrotic Therapies Targeting the Fibrotic Cascade
Emerging treatments focus on directly inhibiting the fibrotic cascade, with LSECs being a critical target for these interventions.
- Pirfenidone and Nintedanib: Approved for idiopathic pulmonary fibrosis, these agents have shown potential in liver fibrosis by inhibiting fibrogenic pathways, including those mediated by LSECs[56].
- Galectin-3 Inhibitors: Galectin-3 is involved in fibrogenesis and inflammation. Inhibiting galectin-3 can reduce HSC activation and ECM production, with beneficial effects on LSEC function[57].
c. Regenerative and Cell-Based Therapies
Advancements in regenerative medicine offer innovative approaches to restore healthy LSEC populations and liver architecture.
- Stem Cell Therapy: Mesenchymal stem cells (MSCs) and endothelial progenitor cells (EPCs) can differentiate into functional LSECs, promoting vascular repair and reducing fibrosis[58].
- Gene Therapy: Delivery of genes encoding protective factors such as VEGF or anti-fibrotic proteins to LSECs can enhance their regenerative capacity and inhibit fibrogenic signaling[32].
d. Nanotechnology and Targeted Drug Delivery
Nanocarriers can be designed to deliver therapeutic agents specifically to LSECs, enhancing drug efficacy and minimizing off-target effects.
- LSEC-Targeted Nanoparticles: Utilizing ligands that bind to receptors uniquely expressed on LSECs, such as mannose receptors, allows for precise delivery of antifibrotic drugs or siRNA molecules to these cells[59].
- Controlled Release Systems: Nanotechnology-enabled systems can provide sustained release of therapeutic agents, ensuring prolonged LSEC modulation and fibrosis inhibition.
e. Biomolecular Inhibitors and Small Molecules
Discovery of novel biomolecules and small molecules that specifically modulate LSEC function is a burgeoning field.
- MicroRNA Modulators: MicroRNAs (miRNAs) regulate gene expression in LSECs. Therapeutics that mimic or inhibit specific miRNAs can alter LSEC behavior to favor antifibrotic outcomes[60].
- Small Molecule Inhibitors: Identifying small molecules that inhibit pro-fibrotic enzymes or signaling molecules in LSECs can provide targeted antifibrotic effects[61].
7.1.3. Clinical Implications and Future Directions
The therapeutic targeting of LSECs holds significant promise for the treatment of liver fibrosis. Current treatments, while beneficial, often exhibit limited efficacy or adverse effects. Emerging therapies, particularly those leveraging regenerative medicine and nanotechnology, offer novel mechanisms to precisely modulate LSEC function and the hepatic microenvironment[62]. Future research should focus on:
- Biomarker Development: Identifying reliable biomarkers for LSEC dysfunction can aid in patient stratification and monitoring therapeutic responses[63].
- Combination Therapies: Combining LSEC-targeted therapies with other antifibrotic agents may produce synergistic effects, enhancing overall treatment efficacy[64].
- Personalized Medicine: Tailoring therapies based on individual patient profiles and specific LSEC pathophysiology could optimize treatment outcomes.
- Clinical Trials: Rigorous clinical testing of emerging therapies is essential to establish safety, efficacy, and optimal dosing strategies for patients with liver fibrosis[65].
LSECs are critical players in the pathogenesis and resolution of liver fibrosis. Therapeutic strategies that target LSECs to restore their normal function, inhibit pro-fibrotic signaling, and modulate immune responses represent a promising avenue for combating liver fibrosis. Ongoing research and clinical advancements will likely expand the repertoire of effective LSEC-targeted therapies, ultimately improving outcomes for patients with chronic liver diseases. A study performed on developing biomarkers discusses the use of an automated machine learning (AutoML) diagnostic support system as a computational biomarker for detecting drug-induced liver injury (DILI) patterns in liver pathology. It highlights the effectiveness of the developed assay in accurately classifying necrotic injury patterns with high precision, providing a valuable tool for early detection and assessment of liver toxicity in drug development[66].
8. Current Challenges and Future Directions:
8.1. Gaps in the Current Understanding of LSECs in Liver Disease.
Despite significant advancements in understanding the role of Liver Sinusoidal Endothelial Cells (LSECs) in liver disease, there are still notable gaps that hinder the development of effective treatments targeting these cells. One of the primary challenges lies in the complexity of studying LSECs in the context of liver disease, particularly due to the limitations of in-vivo models[33]. Current experimental models, such as rodent models, do not fully capture the human liver’s unique environment and cellular interactions, leading to difficulties in translating preclinical findings into clinical applications. For instance, rodent LSECs differ in some key physiological aspects from human LSECs, particularly in their immune regulatory functions, making it challenging to model immune tolerance and disease progression accurately. Moreover, most existing models do not adequately replicate chronic liver conditions, such as non-alcoholic fatty liver disease (NAFLD) and cirrhosis, where long-term interactions between LSECs and other liver cells are crucial to disease progression.
Additionally, clinical studies investigating the specific roles of LSECs in liver disease are still limited. Most research on LSECs has been conducted in preclinical settings, and the number of human trials focused on LSECs as a therapeutic target remains small. While it is clear that LSECs contribute significantly to liver fibrosis and immune regulation, clinical studies that explore LSECs’ direct involvement in human liver diseases are still lacking. The heterogeneity of LSECs in different stages of liver disease, including the transition from a healthy to a diseased state, is not fully understood. Further clinical research is necessary to elucidate how changes in LSEC phenotype and function contribute to disease outcomes and to identify potential biomarkers that can predict fibrosis progression or liver dysfunction.
8.2. Future Research Directions: Role of LSECs in Liver Regeneration and Transplantation
Looking forward, future research should aim to better understand LSECs' potential roles in liver regeneration and liver transplantation, two areas where their immune regulatory functions and interactions with other hepatic cells may offer new therapeutic avenues. LSECs have shown promise in promoting liver regeneration due to their ability to maintain immune tolerance and modulate inflammation. Research has suggested that LSECs contribute to hepatocyte proliferation by secreting growth factors such as VEGF and hepatocyte growth factor (HGF). However, the mechanisms by which LSECs promote liver regeneration, especially in a chronically damaged liver, remain poorly understood. Future studies should focus on elucidating these mechanisms and exploring how LSECs can be manipulated to enhance liver regeneration following injury or surgical resection. Investigating LSECs’ regenerative potential could lead to novel strategies to treat liver diseases that currently require liver transplantation.
In the context of liver transplantation, LSECs play a critical role in maintaining immune tolerance and preventing graft rejection. One promising research direction is exploring how to enhance the immunomodulatory functions of LSECs to prevent or mitigate immune rejection in liver transplant patients. The ability of LSECs to induce regulatory T cells (Tregs) and suppress effector T cells make them an attractive target for therapies aimed at reducing the need for long-term immunosuppression in transplant recipients. Gene editing technologies, such as CRISPR-Cas9, could be utilized to modify LSECs in ways that enhance their ability to promote tolerance and protect against rejection. Furthermore, LSECs could be used in bioengineered liver grafts or as part of cell-based therapies to support graft survival and function.
Another critical area for future research is the development of organoids or liver-on-chip systems that incorporate functional LSECs to better model human liver diseases in vitro. These advanced models would allow for more accurate studies of LSECs’ interactions with other liver cells, providing insights into the dynamic processes involved in liver regeneration and disease progression. In particular, organoid models could be used to test how LSECs respond to drugs or regenerative therapies, speeding up the development of new treatments for chronic liver diseases.
In summary, while significant progress has been made in understanding LSECs, there remain considerable gaps, particularly in modeling and clinical research. Future studies should focus on developing more accurate models, investigating LSECs' role in liver regeneration and transplantation, and exploring their therapeutic potential. By addressing these challenges, we can unlock new pathways to treat and potentially reverse liver diseases, improving patient outcomes.
9. Discussion
9.1. LSEC Dysfunction in Liver Disease
Liver Sinusoidal Endothelial Cells (LSECs) play a pivotal role in maintaining liver homeostasis, and their dysfunction is a central theme in the progression of liver diseases. In conditions such as Metabolic Dysfunction-Associated Steatohepatitis (MASH), LSECs lose their fenestrations and undergo capillarization, leading to impaired filtration and immune regulation. This dysfunction contributes to the activation of hepatic stellate cells (HSCs) and the subsequent development of fibrosis. The loss of LSEC function exacerbates inflammation and promotes a pro-fibrotic environment, highlighting their critical role in liver pathology.
9.2. Unifying Hypothesis of LSEC-Mediated Pathology in MASH
Integrating findings across various sections of this review, we propose a unifying hypothesis that LSEC dysfunction is a key driver of MASH progression. The capillarization and loss of fenestrations in LSECs lead to reduced antigen clearance and impaired immune tolerance. This dysfunction triggers a cascade of events, including increased inflammation, HSC activation, and extracellular matrix deposition, ultimately resulting in fibrosis and cirrhosis. Understanding the mechanisms underlying LSEC dysfunction provides a comprehensive framework for developing targeted therapies to mitigate liver disease progression.
9.3. Emerging Research Areas
Emerging research areas such as organoids and computational modeling offer promising avenues for studying LSEC function. Organoids, which are three-dimensional cell culture systems that mimic the architecture and function of organs, can provide valuable insights into LSEC behavior in a controlled environment[67]. Computational modeling, on the other hand, allows for the simulation of complex biological processes, enabling researchers to predict the effects of LSEC dysfunction and identify potential therapeutic targets[68]. These innovative approaches hold the potential to advance our understanding of LSEC-mediated pathology and inform the development of novel treatments.
10. Limitations and Challenges
10.1. Challenges in Studying LSECs
Studying LSECs presents several challenges, including the limitations of in vivo and in vitro models. In vivo models, such as rodent models, often fail to fully replicate the human liver's unique environment and cellular interactions[69]. This discrepancy makes it difficult to translate preclinical findings into clinical applications. In vitro models, while useful for studying specific aspects of LSEC function, lack the complexity of the in vivo environment, limiting their ability to capture the full spectrum of LSEC behavior.
10.2. Translational Challenges
Translating findings from rodent models to human diseases is particularly challenging due to physiological differences between species. Rodent LSECs differ from human LSECs in key aspects, such as immune regulatory functions, making it difficult to model immune tolerance and disease progression accurately. Additionally, most existing models do not adequately replicate chronic liver conditions, such as NAFLD and cirrhosis, where long-term interactions between LSECs and other liver cells are crucial to disease progression. Addressing these challenges requires the development of more sophisticated models that better mimic human liver pathology.
11. Future Directions
11.1. Advancing Biomarker Development
Advancing biomarker development for the early detection of LSEC dysfunction is a critical area of future research. Identifying reliable biomarkers can aid in patient stratification, monitor therapeutic responses, and predict disease progression. Biomarkers specific to LSEC dysfunction could enable earlier intervention and improve patient outcomes by allowing for timely and targeted treatments.
11.2. Regenerative Therapies
Exploring regenerative therapies to restore LSEC function in advanced disease stages holds significant promise. Regenerative approaches, such as stem cell therapy and gene editing, could potentially reverse LSEC dysfunction and promote liver regeneration. For instance, mesenchymal stem cells (MSCs) and endothelial progenitor cells (EPCs) have shown potential in differentiating into functional LSECs, supporting vascular repair and reducing fibrosis. Gene editing technologies, such as CRISPR-Cas9, could be utilized to enhance LSEC function and prevent disease progression.
LSECs are central to the regulation of immune responses and fibrosis in MASH liver disease. Addressing the challenges in studying LSECs and advancing research in emerging areas will be crucial for developing effective therapeutic strategies. By focusing on early detection, targeted treatments, and regenerative therapies, we can improve the management and treatment of chronic liver diseases, ultimately enhancing patient outcomes.
12. Conclusions:
In conclusion, Liver Sinusoidal Endothelial Cells (LSECs) play an essential role in regulating liver function, particularly in the context of immune responses and fibrosis in chronic liver diseases. Throughout this review, we have highlighted the unique anatomy and specialized functions of LSECs, which allow them to act as critical modulators of hepatic homeostasis. LSECs not only filter blood and remove pathogens, but also engage in immune regulation by presenting antigens and promoting immune tolerance. Their interaction with other hepatic cells, such as Kupffer cells, hepatic stellate cells (HSCs), and hepatocytes, is central to the maintenance of immune balance and prevention of excessive inflammation. However, when LSECs become dysfunctional, they contribute to the progression of liver diseases such as non-alcoholic fatty liver disease (NAFLD), alcoholic liver disease (ALD), and viral hepatitis. Dysfunctional LSECs promote hepatic stellate cell activation and collagen deposition, leading to fibrosis, and exacerbate liver scarring, contributing to disease progression.
One of the key takeaways from this review is the understanding that LSECs are not merely passive endothelial cells but active regulators of the liver’s immune environment and fibrotic response. Changes in LSEC phenotype, such as capillarization and the loss of fenestrations, lead to dysregulated immune responses and fibrogenesis. This positions LSECs as both key drivers and potential therapeutic targets in chronic liver diseases. The ability of LSECs to modulate immune responses, interact with HSCs, and influence fibrosis progression underscores their significance in liver pathology.
Moving forward, LSECs represent a promising therapeutic target for both immune modulation and fibrosis prevention in liver disease. By targeting the pathways involved in LSEC dysfunction—such as nitric oxide production, TGF-β signaling, and capillarization—it may be possible to restore their normal function and prevent the progression of fibrosis. Furthermore, enhancing the regenerative potential of LSECs or harnessing their immune-regulatory capabilities could provide new strategies for treating chronic liver diseases and improving outcomes in liver transplantation. As research continues to unravel the complex roles of LSECs, their potential in therapeutic applications will likely play a pivotal role in shaping future treatments for liver diseases.

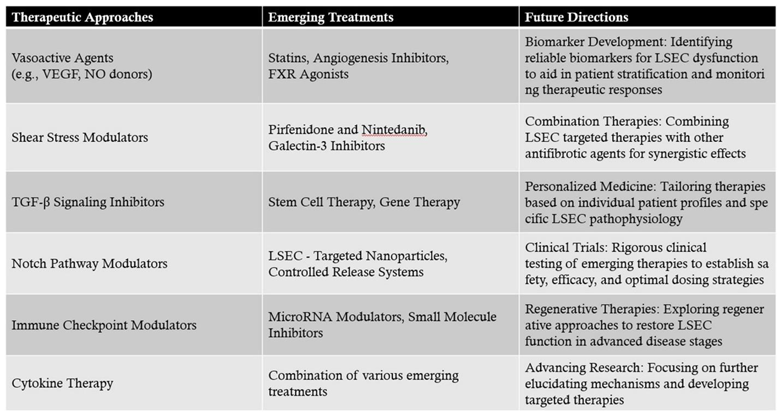
Table 1.
Summary of Therapeutic Approaches, Emerging Treatments, and Future Directions for Targeting Liver Sinusoidal Endothelial Cells (LSECs) in Liver Fibrosis and Immune Modulation.
Table 1.
Summary of Therapeutic Approaches, Emerging Treatments, and Future Directions for Targeting Liver Sinusoidal Endothelial Cells (LSECs) in Liver Fibrosis and Immune Modulation.
 |
References
- Shetty, S.; Lalor, P.F.; Adams, D.H. Liver Sinusoidal Endothelial Cells — Gatekeepers of Hepatic Immunity. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 555–567. [Google Scholar] [CrossRef]
- Knolle, P.A.; Wohlleber, D. Immunological Functions of Liver Sinusoidal Endothelial Cells. Cell. Mol. Immunol. 2016, 13, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Heymann, F.; Tacke, F. Immunology in the Liver--from Homeostasis to Disease. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 88–110. [Google Scholar] [CrossRef] [PubMed]
- Estes, C.; Razavi, H.; Loomba, R.; Younossi, Z.; Sanyal, A.J. Modeling the Epidemic of Nonalcoholic Fatty Liver Disease Demonstrates an Exponential Increase in Burden of Disease. Hepatol. Baltim. Md 2018, 67, 123–133. [Google Scholar] [CrossRef]
- Eskridge, W.; Cryer, D.R.; Schattenberg, J.M.; Gastaldelli, A.; Malhi, H.; Allen, A.M.; Noureddin, M.; Sanyal, A.J. Metabolic Dysfunction-Associated Steatotic Liver Disease and Metabolic Dysfunction-Associated Steatohepatitis: The Patient and Physician Perspective. J. Clin. Med. 2023, 12, 6216. [Google Scholar] [CrossRef]
- Bhandari, S.; Larsen, A.K.; McCourt, P.; Smedsrød, B.; Sørensen, K.K. The Scavenger Function of Liver Sinusoidal Endothelial Cells in Health and Disease. Front. Physiol. 2021, 12. [Google Scholar] [CrossRef]
- Koyama, Y.; Brenner, D.A. Liver Inflammation and Fibrosis. J. Clin. Invest. 2017, 127, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Cogliati, B.; Yashaswini, C.N.; Wang, S.; Sia, D.; Friedman, S.L. Friend or Foe? The Elusive Role of Hepatic Stellate Cells in Liver Cancer. Nat. Rev. Gastroenterol. Hepatol. 2023, 20, 647–661. [Google Scholar] [CrossRef]
- Miyao, M.; Kotani, H.; Ishida, T.; Kawai, C.; Manabe, S.; Abiru, H.; Tamaki, K. Pivotal Role of Liver Sinusoidal Endothelial Cells in NAFLD/NASH Progression. Lab. Invest. 2015, 95, 1130–1144. [Google Scholar] [CrossRef]
- DeLeve, L.D. Liver Sinusoidal Endothelial Cells and Liver Regeneration. J. Clin. Invest. 2013, 123, 1861. [Google Scholar] [CrossRef] [PubMed]
- Campana, L.; Esser, H.; Huch, M.; Forbes, S. Liver Regeneration and Inflammation: From Fundamental Science to Clinical Applications. Nat. Rev. Mol. Cell Biol. 2021, 22, 608–624. [Google Scholar] [CrossRef]
- Wang, X.-K.; Peng, Z.-G. Targeting Liver Sinusoidal Endothelial Cells: An Attractive Therapeutic Strategy to Control Inflammation in Nonalcoholic Fatty Liver Disease. Front. Pharmacol. 2021, 12, 655557. [Google Scholar] [CrossRef] [PubMed]
- Poisson, J.; Lemoinne, S.; Boulanger, C.; Durand, F.; Moreau, R.; Valla, D.; Rautou, P.-E. Liver Sinusoidal Endothelial Cells: Physiology and Role in Liver Diseases. J. Hepatol. 2017, 66, 212–227. [Google Scholar] [CrossRef] [PubMed]
- Du, W.; Wang, L. The Crosstalk Between Liver Sinusoidal Endothelial Cells and Hepatic Microenvironment in NASH Related Liver Fibrosis. Front. Immunol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Furuta, K.; Guo, Q.; Hirsova, P.; Ibrahim, S.H. Emerging Roles of Liver Sinusoidal Endothelial Cells in Nonalcoholic Steatohepatitis. Biology 2020, 9, 395. [Google Scholar] [CrossRef]
- McConnell, M.J.; Kostallari, E.; Ibrahim, S.H.; Iwakiri, Y. The Evolving Role of Liver Sinusoidal Endothelial Cells in Liver Health and Disease. Hepatol. Baltim. Md 2023, 78, 649. [Google Scholar] [CrossRef]
- Mehrfeld, C.; Zenner, S.; Kornek, M.; Lukacs-Kornek, V. The Contribution of Non-Professional Antigen-Presenting Cells to Immunity and Tolerance in the Liver. Front. Immunol. 2018, 9. [Google Scholar] [CrossRef]
- Wilkinson, A.L.; Qurashi, M.; Shetty, S. The Role of Sinusoidal Endothelial Cells in the Axis of Inflammation and Cancer Within the Liver. Front. Physiol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Tacke, F.; Zimmermann, H.W. Macrophage Heterogeneity in Liver Injury and Fibrosis. J. Hepatol. 2014, 60, 1090–1096. [Google Scholar] [CrossRef] [PubMed]
- Parthasarathy, G.; Malhi, H. Macrophage Heterogeneity in NASH: More Than Just Nomenclature. Hepatol. Baltim. Md 2021, 74, 515. [Google Scholar] [CrossRef] [PubMed]
- DeLeve, L.D. Liver Sinusoidal Endothelial Cells in Hepatic Fibrosis. Hepatol. Baltim. Md 2015, 61, 1740–1746. [Google Scholar] [CrossRef]
- Li, H. Intercellular Crosstalk of Liver Sinusoidal Endothelial Cells in Liver Fibrosis, Cirrhosis and Hepatocellular Carcinoma. Dig. Liver Dis. 2022, 54, 598–613. [Google Scholar] [CrossRef]
- Szafranska, K.; Kruse, L.D.; Holte, C.F.; McCourt, P.; Zapotoczny, B. The wHole Story About Fenestrations in LSEC. Front. Physiol. 2021, 12, 735573. [Google Scholar] [CrossRef]
- He, Q.; He, W.; Dong, H.; Guo, Y.; Yuan, G.; Shi, X.; Wang, D.; Lu, F. Role of Liver Sinusoidal Endothelial Cell in Metabolic Dysfunction-Associated Fatty Liver Disease. Cell Commun. Signal. 2024, 22, 346. [Google Scholar] [CrossRef] [PubMed]
- Hasa, E.; Hartmann, P.; Schnabl, B. Liver Cirrhosis and Immune Dysfunction. Int. Immunol. 2022, 34, 455. [Google Scholar] [CrossRef] [PubMed]
- Horst, A.K.; Neumann, K.; Diehl, L.; Tiegs, G. Modulation of Liver Tolerance by Conventional and Nonconventional Antigen-Presenting Cells and Regulatory Immune Cells. Cell. Mol. Immunol. 2016, 13, 277–292. [Google Scholar] [CrossRef]
- Limmer, A.; Ohl, J.; Kurts, C.; Ljunggren, H.-G.; Reiss, Y.; Groettrup, M.; Momburg, F.; Arnold, B.; Knolle, P.A. Efficient Presentation of Exogenous Antigen by Liver Endothelial Cells to CD8+ T Cells Results in Antigen-Specific T-Cell Tolerance. Nat. Med. 2000, 6, 1348–1354. [Google Scholar] [CrossRef]
- Jenne, C.N.; Kubes, P. Immune Surveillance by the Liver. Nat. Immunol. 2013, 14, 996–1006. [Google Scholar] [CrossRef]
- Seki, E.; Schwabe, R.F. Hepatic Inflammation and Fibrosis: Functional Links and Key Pathways. Hepatol. Baltim. Md 2015, 61, 1066–1079. [Google Scholar] [CrossRef] [PubMed]
- Puri, M. Spatial Computational Hepatic Molecular Biomarker Reveals LSEC Role in Midlobular Liver Zonation Fibrosis in DILI and NASH Liver Injury. Int. J. Transl. Med. 2024, 4, 208–223. [Google Scholar] [CrossRef]
- Ni, Y.; Li, J.-M.; Liu, M.-K.; Zhang, T.-T.; Wang, D.-P.; Zhou, W.-H.; Hu, L.-Z.; Lv, W.-L. Pathological Process of Liver Sinusoidal Endothelial Cells in Liver Diseases. World J. Gastroenterol. 2017, 23, 7666. [Google Scholar] [CrossRef]
- Qu, J.; Wang, L.; Li, Y.; Li, X. Liver Sinusoidal Endothelial Cell: An Important yet Often Overlooked Player in the Liver Fibrosis. Clin. Mol. Hepatol. 2024, 30, 303. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Zuo, B.; He, Y. Liver Sinusoidal Endothelial Cells as Potential Drivers of Liver Fibrosis (Review). Mol. Med. Rep. 2024, 29, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; Seki, E. The Liver Fibrosis Niche: Novel Insights into the Interplay between Fibrosis-Composing Mesenchymal Cells, Immune Cells, Endothelial Cells, and Extracellular Matrix. Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 2020, 143, 111556. [Google Scholar] [CrossRef]
- Ruan, B.; Duan, J.-L.; Xu, H.; Tao, K.-S.; Han, H.; Dou, G.-R.; Wang, L. Capillarized Liver Sinusoidal Endothelial Cells Undergo Partial Endothelial-Mesenchymal Transition to Actively Deposit Sinusoidal ECM in Liver Fibrosis. Front. Cell Dev. Biol. 2021, 9, 671081. [Google Scholar] [CrossRef] [PubMed]
- Akkız, H.; Gieseler, R.K.; Canbay, A. Liver Fibrosis: From Basic Science towards Clinical Progress, Focusing on the Central Role of Hepatic Stellate Cells. Int. J. Mol. Sci. 2024, 25, 7873. [Google Scholar] [CrossRef] [PubMed]
- Elpek, G.Ö. Angiogenesis and Liver Fibrosis. World J. Hepatol. 2015, 7, 377. [Google Scholar] [CrossRef]
- Allameh, A.; Niayesh-Mehr, R.; Aliarab, A.; Sebastiani, G.; Pantopoulos, K. Oxidative Stress in Liver Pathophysiology and Disease. Antioxidants 2023, 12, 1653. [Google Scholar] [CrossRef] [PubMed]
- Pei, Q.; Yi, Q.; Tang, L. Liver Fibrosis Resolution: From Molecular Mechanisms to Therapeutic Opportunities. Int. J. Mol. Sci. 2023, 24, 9671. [Google Scholar] [CrossRef] [PubMed]
- DeLeve, L.D.; Maretti-Mira, A.C. Liver Sinusoidal Endothelial Cell: An Update. Semin. Liver Dis. 2017, 37, 377. [Google Scholar] [CrossRef]
- Wan, Y.; Li, X.; Slevin, E.; Harrison, K.; Li, T.; Zhang, Y.; Klaunig, J.E.; Wu, C.; Shetty, A.K.; Dong, X.C.; et al. Endothelial Dysfunction in Pathological Processes of Chronic Liver Disease during Aging. FASEB J. 2022, 36, e22125. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.-Y.; Yuan, W.-G.; He, P.; Lei, J.-H.; Wang, C.-X. Liver Fibrosis and Hepatic Stellate Cells: Etiology, Pathological Hallmarks and Therapeutic Targets. World J. Gastroenterol. 2016, 22, 10512–10522. [Google Scholar] [CrossRef]
- Hong, X.; Huang, S.; Jiang, H.; Ma, Q.; Qiu, J.; Luo, Q.; Cao, C.; Xu, Y.; Chen, F.; Chen, Y.; et al. Alcohol-Related Liver Disease (ALD): Current Perspectives on Pathogenesis, Therapeutic Strategies, and Animal Models. Front. Pharmacol. 2024, 15, 1432480. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.W.; Harmon, C.; O’Farrelly, C. Liver Immunology and Its Role in Inflammation and Homeostasis. Cell. Mol. Immunol. 2016, 13, 267–276. [Google Scholar] [CrossRef]
- Sanz-García, C.; Fernández-Iglesias, A.; Gracia-Sancho, J.; Arráez-Aybar, L.A.; Nevzorova, Y.A.; Cubero, F.J. The Space of Disse: The Liver Hub in Health and Disease. Livers 2021, 1, 3–26. [Google Scholar] [CrossRef]
- Iwakiri, Y. Unlocking the Role of Liver Sinusoidal Endothelial Cells: Key Players in Liver Fibrosis: Editorial on “Liver Sinusoidal Endothelial Cell: An Important yet Often Overlooked Player in the Liver Fibrosis. ” Clin. Mol. Hepatol. 2024, 30, 673–676. [Google Scholar] [CrossRef]
- Czyzynska-Cichon, I.; Kotlinowski, J.; Blacharczyk, O.; Giergiel, M.; Szymanowski, K.; Metwally, S.; Wojnar-Lason, K.; Dobosz, E.; Koziel, J.; Lekka, M.; et al. Early and Late Phases of Liver Sinusoidal Endothelial Cell (LSEC) Defenestration in Mouse Model of Systemic Inflammation. Cell. Mol. Biol. Lett. 2024, 29, 139. [Google Scholar] [CrossRef] [PubMed]
- Nagy, D.; Maude, H.; Birdsey, G.M.; Randi, A.M.; Cebola, I. RISING STARS: Liver Sinusoidal Endothelial Transcription Factors in Metabolic Homeostasis and Disease. J. Mol. Endocrinol. 2023, 71. [Google Scholar] [CrossRef] [PubMed]
- Soydemir, S.; Comella, O.; Abdelmottaleb, D.; Pritchett, J. Does Mechanocrine Signaling by Liver Sinusoidal Endothelial Cells Offer New Opportunities for the Development of Anti-Fibrotics? Front. Med. 2020, 6, 312. [Google Scholar] [CrossRef] [PubMed]
- Dewidar, B.; Meyer, C.; Dooley, S.; Meindl-Beinker, N. TGF-β in Hepatic Stellate Cell Activation and Liver Fibrogenesis—Updated 2019. Cells 2019, 8, 1419. [Google Scholar] [CrossRef]
- Geisler, F.; Strazzabosco, M. Emerging Roles of Notch Signaling in Liver Disease. Hepatol. Baltim. Md 2015, 61, 382–392. [Google Scholar] [CrossRef] [PubMed]
- Lurje, I.; Hammerich, L.; Tacke, F. Dendritic Cell and T Cell Crosstalk in Liver Fibrogenesis and Hepatocarcinogenesis: Implications for Prevention and Therapy of Liver Cancer. Int. J. Mol. Sci. 2020, 21, 7378. [Google Scholar] [CrossRef] [PubMed]
- Bignold, R.; Johnson, J.R. Effects of Cytokine Signaling Inhibition on Inflammation-Driven Tissue Remodeling. Curr. Res. Pharmacol. Drug Discov. 2021, 2, 100023. [Google Scholar] [CrossRef]
- Bravo, M.; Raurell, I.; Hide, D.; Fernández-Iglesias, A.; Gil, M.; Barberá, A.; Salcedo, M.T.; Augustin, S.; Genescà, J.; Martell, M. Restoration of Liver Sinusoidal Cell Phenotypes by Statins Improves Portal Hypertension and Histology in Rats with NASH. Sci. Rep. 2019, 9, 20183. [Google Scholar] [CrossRef]
- Duan, S.; Li, X.; Fan, G.; Liu, R. Targeting Bile Acid Signaling for the Treatment of Liver Diseases: From Bench to Bed. Biomed. Pharmacother. 2022, 152, 113154. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Bayliss, G.; Zhuang, S. Application of Nintedanib and Other Potential Anti-Fibrotic Agents in Fibrotic Diseases. Clin. Sci. Lond. Engl. 1979 2019, 133, 1309–1320. [Google Scholar] [CrossRef] [PubMed]
- Henderson, N.C.; Mackinnon, A.C.; Farnworth, S.L.; Poirier, F.; Russo, F.P.; Iredale, J.P.; Haslett, C.; Simpson, K.J.; Sethi, T. Galectin-3 Regulates Myofibroblast Activation and Hepatic Fibrosis. Proc. Natl. Acad. Sci. 2006, 103, 5060–5065. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Mao, Y.; Xie, Y.; Wei, J.; Yao, J. Stem Cells for Treatment of Liver Fibrosis/Cirrhosis: Clinical Progress and Therapeutic Potential. Stem Cell Res. Ther. 2022, 13, 356. [Google Scholar] [CrossRef]
- Carambia, A.; Gottwick, C.; Schwinge, D.; Stein, S.; Digigow, R.; Şeleci, M.; Mungalpara, D.; Heine, M.; Schuran, F.A.; Corban, C.; et al. Nanoparticle-Mediated Targeting of Autoantigen Peptide to Cross-Presenting Liver Sinusoidal Endothelial Cells Protects from CD8 T-Cell-Driven Autoimmune Cholangitis. Immunology 2021, 162, 452–463. [Google Scholar] [CrossRef]
- Jouve, M.; Carpentier, R.; Kraiem, S.; Legrand, N.; Sobolewski, C. MiRNAs in Alcohol-Related Liver Diseases and Hepatocellular Carcinoma: A Step toward New Therapeutic Approaches? Cancers 2023, 15, 5557. [Google Scholar] [CrossRef]
- Jangra, A.; Kothari, A.; Sarma, P.; Medhi, B.; Omar, B.J.; Kaushal, K. Recent Advancements in Antifibrotic Therapies for Regression of Liver Fibrosis. Cells 2022, 11, 1500. [Google Scholar] [CrossRef]
- Tian, S.-P.; Ge, J.-Y.; Song, Y.-M.; Yu, X.-Q.; Chen, W.-H.; Chen, Y.-Y.; Ye, D.; Zheng, Y.-W. A Novel Efficient Strategy to Generate Liver Sinusoidal Endothelial Cells from Human Pluripotent Stem Cells. Sci. Rep. 2024, 14, 13831. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Ribera, M.; Gibert-Ramos, A.; Abad-Jordà, L.; Magaz, M.; Téllez, L.; Paule, L.; Castillo, E.; Pastó, R.; de Souza Basso, B.; Olivas, P.; et al. Increased Sinusoidal Pressure Impairs Liver Endothelial Mechanosensing, Uncovering Novel Biomarkers of Portal Hypertension. JHEP Rep. 2023, 5, 100722. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Wang, L.; Wang, M.; Zhou, S.; Lu, Y.; Cui, H.; Racanelli, A.C.; Zhang, L.; Ye, T.; Ding, B.; et al. Targeting Fibrosis: Mechanisms and Clinical Trials. Signal Transduct. Target. Ther. 2022, 7, 1–21. [Google Scholar] [CrossRef]
- Trautwein, C.; Friedman, S.L.; Schuppan, D.; Pinzani, M. Hepatic Fibrosis: Concept to Treatment. J. Hepatol. 2015, 62, S15–S24. [Google Scholar] [CrossRef] [PubMed]
- Puri, M. Automated Machine Learning Diagnostic Support System as a Computational Biomarker for Detecting Drug-Induced Liver Injury Patterns in Whole Slide Liver Pathology Images. Assay Drug Dev. Technol. 2020, 18, 1–10. [Google Scholar] [CrossRef]
- Nwokoye, P.N.; Abilez, O.J. Bioengineering Methods for Vascularizing Organoids. Cell Rep. Methods 2024, 4, 100779. [Google Scholar] [CrossRef]
- Gayathiri, E.; Prakash, P.; Kumaravel, P.; Jayaprakash, J.; Ragunathan, M.G.; Sankar, S.; Pandiaraj, S.; Thirumalaivasan, N.; Thiruvengadam, M.; Govindasamy, R. Computational Approaches for Modeling and Structural Design of Biological Systems: A Comprehensive Review. Prog. Biophys. Mol. Biol. 2023, 185, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Kaur, S.; Kidambi, S.; Ortega-Ribera, M.; Thuy, L.T.T.; Nieto, N.; Cogger, V.C.; Xie, W.-F.; Tacke, F.; Gracia-Sancho, J. In Vitro Models for the Study of Liver Biology and Diseases: Advances and Limitations. Cell. Mol. Gastroenterol. Hepatol. 2022, 15, 559–571. [Google Scholar] [CrossRef]
Figure 1.
Structural and Functional Changes in Liver LSECs in Normal and Injured Liver.
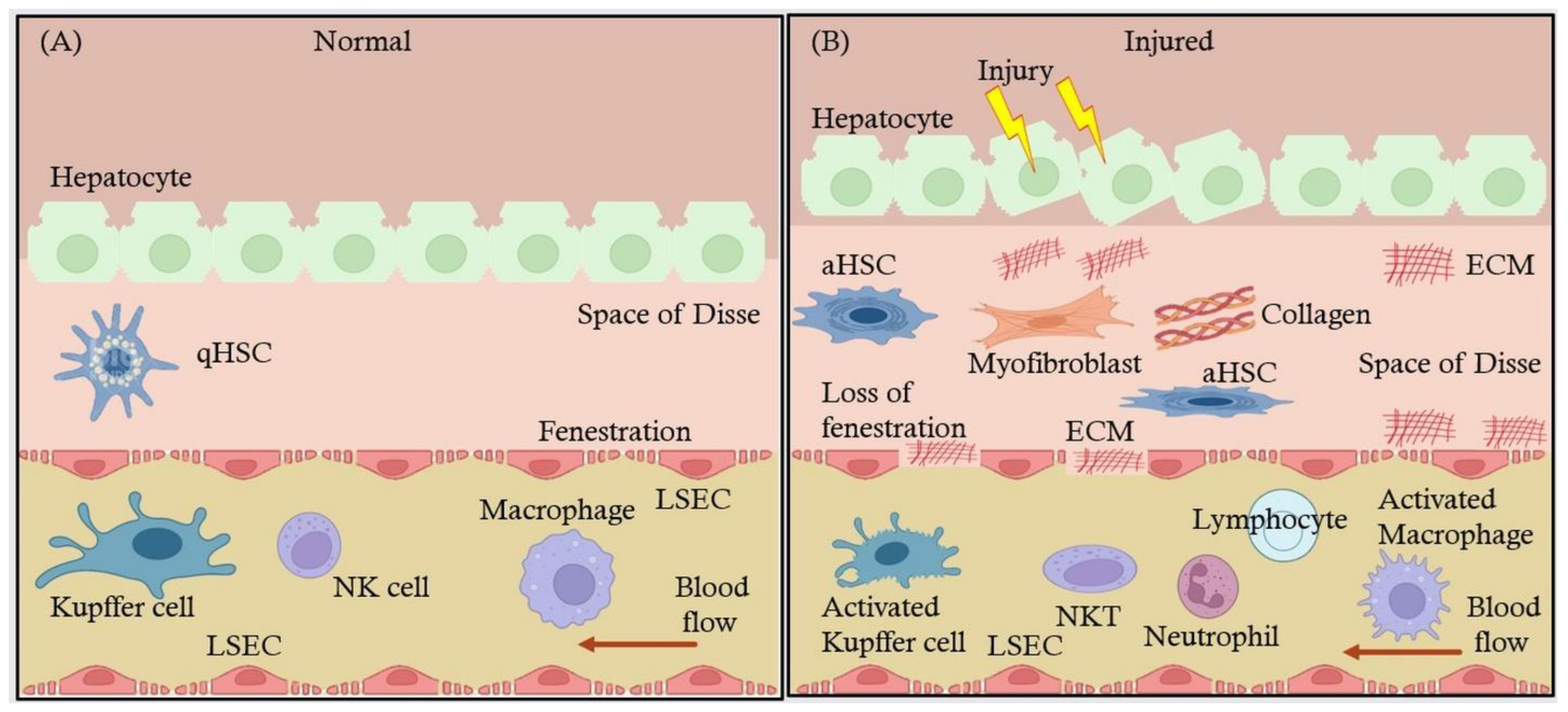
Figure 2.
MASH Liver Progression Stages and the Role of LSECs in Therapeutic Strategies.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



