
Submitted:
07 January 2025
Posted:
08 January 2025
You are already at the latest version
Abstract
Background/Objectives: Neonatal hypoxic-ischemic encephalopathy (HIE) due to perinatal complications remains an important pathology with a significant burden for neonates, families, and the healthcare system. Resuscitation and simulation team training are key elements in increasing patient safety. In this retrospective cohort study, we evaluated whether regular constant trainings of all personnel working in the delivery rooms in South Tyrol increased the outcome of neonates with HIE. Methods: We retrospectively analyzed three groups of neonates with moderate to severe HIE who required therapeutic hypothermia. The first group included infants before the systematic introduction of trainings and compared it to the second group after three years of regular trainings. A third group after the SARS-CoV-2 pandemics was compared in order to evaluate retention of skills and the long-term effect of our training program. Results: Over the three study periods mortality decreased from 41.2% to 0% and 14.3% respectively. There was also a significant reduction of patients with subclincal seizures detected only in EEG from 47.1% in the first period to 43.7% and 14.3% in the second and third study period respectively. Clinical manifest seizures decreased significantly from 47.1% to 37.5% and 10.7%, as well as severe brain lesions in ultrasound (US) and MRI.
Conclusions: Constant and regular simulation training for all birth attendants significantly decreases mortality and improves the outcome in neonates with moderate to severe HIE. This positive effect seems to last even after a one-year period where training sessions could not be performed due to the Covid pandemics.
Keywords:
simulation
; team training
; perinatal asphyxia
; hypoxic ischemic encephalopathy
1. Introduction
Hypoxic-ischemic encephalopathy (HIE) occurs in approximately 1.5 per 1000 live births in developed countries and is caused by a lack of oxygen and blood perfusion in the brain during the perinatal period [1,2].
Therapeutic hypothermia for 72 hours to a core temperature of 33.5°C is a standard therapy to reduce mortality and long-term neurological consequences [3,4,5].
Despite this neuroprotective treatment, mortality and lifelong morbidity, such as infantile cerebral palsy, cognitive delay, epilepsy, learning and behavioral difficulties remain high [1,6,7] with approximately 40-50% of newborns who have undergone hypothermic treatment presenting neurological difficulties in their further development [8,9,10].
Hypoxia and ischemia occur either before birth (20%), during birth (30%), before and during birth (35%) and only in a few cases after birth (10%) [11]. Such episodes are considered perinatal and neonatal emergencies, which always involve a multidisciplinary team. High-fidelity simulation training for obstetric emergencies can improve the skills of healthcare staff by practicing regularly emergency events without posing patients at risk [12]. It is proven that neonatal resuscitation and simulation trainings can significantly reduce the incidence of HIE and improve short term outcomes [13,14].
Since 2013, the Patient Safety Center in our institution offers neonatal resuscitation and simulation team trainings for all the staff working in delivery rooms in all hospitals in our region of South Tyrol. The purpose of this study is to examine the effects of these trainings on the outcomes of newborns with HIE.
2. Materials and Methods
This was a retrospective study of babies born during the period between October 2009 and December 2012, between January 2016 and December 2019 and between January 2021 and March 2024. All neonates with a diagnosis of HIE who were treated with therapeutic hypothermia during these periods were included. Five newborns were excluded due to underling genetic pathologies or conditions. Included patients were divided into three cohorts (Figure 1):
- -
- Pre-training: October 2009 - December 2012, N=17
- -
- Post-training: January 2016 - December 2019, N=16
- -
- Post-SARS-CoV-2: January 2021 - March 2024, N=28
Patients in the three years between the first two cohorts (2013-2015) were excluded since this time was necessary to assure that almost all healthcare staff attended resuscitation and simulation training. We excluded those patients born during the SARS-Cov-2 pandemic (Dec 2019–Dec 2020), since no courses could be organized during this period. The third cohort included patients with HIE born after the Covid pandemic, in order to evaluate skills retention and the related long-term effects of our training program. The timeline of the single periods and the number of included patients is shown in Figure 1.
2.1. Neonatal Resuscitation and Simulation Team Training
Between 2013 and 2019, and again from 2021 onwards approximately 20 neonatal resuscitation and simulation team trainings for neonatal and obstetric emergencies were organized annually at the Patient Safety Center in Bolzano. Participation in the courses was on voluntary basis, but every member of staff working in this area was expected to take part at least once a year. The target groups were doctors in pediatrics, gynecology and obstetrics, neonatology, anesthesia, as well as midwives and nurses.
2.2. Patients and Outcomes
All neonates born in any hospital of our region and who met criteria for therapeutic hypothermia were admitted to our Neonatal Intensive Care Unit (NICU) in our Center and underwent hypothermic treatment within 6 hours from the hypoxic ischemic event.
Criteria for the active cooling according to the Guidelines of the Italian Society of Neonatology (SIN) were gestational age >35 weeks, birth weight >1800gms, pH of ≤ 7.0 or base excess ≥ -12mmol/L in a sample of umbilical cord blood or arterial analysis within the first hour of life, an Apgar score <5 at ten minutes or need for positive pressure ventilation at 10 minutes.
Included patients were coded with a consecutive number (pseudonymized), demographic, clinical, laboratory and diagnostic data were analyzed. All birth-related data, such as place of birth (inborn or outborn), birth weight, gender, gestational age, pH-value and base excess (BE) collected within the first 60 minutes of life were documented and analyzed. Severity of HIE was evaluated based on the Sarnat and Sarnat score [18,19].
Main outcomes were mortality within 30 days of life, clinical and electrophysiological seizures recorded on video and EEG (performed for at least 30 minutes before hypothermic treatment, during cooling and after the rewarming phase), as well as brain ultrasound and MRI findings. These were classified according to the Barkovich score: 0=normal findings,1= abnormal signal in basal ganglia or thalamus, 2= Isolated damage in the cortex, 3=damage in the cortex and basal ganglia or 4=damage in the entire cortex and basal ganglia [20].
Additional data included the need for mechanical ventilation and inotropic agents, creatinine levels and coagulation times and the occurrence of thrombocytopenia or bradycardia during hypothermic treatment.
2.3. Statistical Analysis
Categorical variables were expressed as numbers and percentages, while continuous variables were reported as means with standard deviation (SD) or medians with interquartile range (IQR), depending on their distribution. Univariate comparisons between the three groups were conducted using ANOVA or Kruskal-Wallis test for continuous variables, depending on the normality of the data. For categorical variables, the Chi-square test was used. For comparison of outcomes between two groups, Student's t-test, Kruskal-Wallis test, Mann-Whitney test or Chi-square test were used, depending on the type of variable considered.
In addition, Kaplan-Meier survival curves were generated to compare 30-day mortality among the three groups, and comparisons between both two and three groups were made using the log-rank test. All statistical analyses were performed using STATA software version 16.1. A p-value < 0.05 was considered statistically significant.
3. Results
A total of N = 61 patients were enrolled during the study period. Of these, 27.9% (17/61) were part of the pre-training group, 26.2% (16/61) were part of the post-training group, and 45.9% (28/61) were part of the post-SARS-CoV-2 group. Characteristics of the infants in the three cohorts are presented in Table 1. The groups differed only by BE value < 60 minutes, showing that severity of acidosis decreased progressively over the three phases of the study.
During the three study periods mortality at 30 days decreased from 41.2% in the pre-training group to 0% in the post-training and 14.3% in the post - SARS - CoV - 2 group.
HIE scores were progressively less severe in the three study groups and normalities at head ultrasounds and at MRI of the brain increased significantly.
The incidence of subclinical seizures recorded only by EEG decreased from 47.1% in the pre-intervention to 43.7% in the post-intervention cohort and to 10.7% in the post-COVID - 19 patients. Clinical seizures decreased from 47.1% during the first period to 37.5% and 10.7% in the second and third period accordingly.
Brain ultrasound (US) showed a significant increase in normal findings and a reduction in moderate and severe lesions. Echographic diagnoses were supported by MRI results, which showed a significant decrease of moderate and severe brain lesions according to Barkovich score [20].

Table 2.
Mortality and neurologic outcome.
| Pre-training | Post-training | Post-SARS CoV-2 | p | |
|---|---|---|---|---|
| Death < 30 days, n (%) | 7 (41.2) | 0 (0.0) | 4 (14.3) | 0.007 |
| HIE score, n (%) Moderate Severe |
6 (35.3) 11 (64.7) |
8 (50.0) 8 (50.0) |
21 (75.0) 7 (25.0) |
0.093 |
| EEG seizures, n (%) | 8 (47.1) | 7 (43.7) | 4 (14.3) | 0.032 |
| Clinical seizures, n (%) | 8 (47.1) | 6 (37.5) | 3 (10.7) | 0.019 |
| Brain US, n (%) Normal Hyperechogenic areas Status marmoratus |
5 (29.4) 11 (64.7) 1 (5.9) |
5 (31.2) 11 (68.8) 0 (0.0) |
20 (71.4) 6 (21.4) 2 (7.1) |
0.011 |
| MRI, n (%)* 0 1 2 3 |
3 (30.0) 4 (40.0) 2 (20.0) 1 (10.0) |
5 (31.2) 2 (12.5) 7 (43.7) 2 (12.5) |
20 (80.0) 2 (8.0) 1 (4.0) 2 (8.0) |
0.005 |
HIE: hypoxic ischemic encephalopathy; EEG: electroencephalogram; US: ultrasound, MRI: magnetic resonance tomography; *this result was obtained in n=55/61 infants, there were no infants with 4th grade lesions.
Comparison between groups for mortality at thirty days was performed using Kaplan-Meier as shown in Figure 2. Survival between the three groups shows a statistically significant difference with a Log-rank test reporting a p=0.005. If we compare the pre-intervention group with the post-intervention group the Log-rank test reports a p=0.004, while if we compare the post-intervention group with the post-SARS-CoV-2 group the Log-rank test reports a p=0.119.
Short term morbidity and initial interventions are presented in Table 3. The groups varied statistically significantly for the requirement of inotropic support, the incidence of mechanical ventilation, creatinine level and incidence of thrombocytopenia. Prolonged coagulation times were equal in the 3 groups (p=0.218). Incidence of bradycardia increased significantly across the three different study periods (<0.001).
4. Discussion
HIE after perinatal asphyxia is an important burden for infants and families due to the elevated associated mortality and morbidity [10]. Even though the mortality of fetuses, newborns and mothers has been greatly reduced in recent decades, further reduction remains an important goal in perinatal care [21].
In this retrospective cohort study, we evaluated the possible effects of neonatal resuscitation courses combined with simulation team-training in obstetrics and neonatology for all doctors, midwives and nurses working in the delivery rooms of all hospitals in our region.
Introduction and evaluation of such a training program involving all personnel was possible because the region is comparatively small covering approximately 5000 neonates per year. In addition, all hospitals are part of the same organization with our NICU being the perinatal center where all neonates at risk for HIE are cared for.
High rates of morbidity and mortality are preventable and multidisciplinary team training could contribute to achieve this goal [22]. Resuscitation and simulation team trainings are considered as potential quality improvement (QI) opportunities in neonates with HIE [23]. One previous study reported that simulation training of healthcare staff in neonatal resuscitation led to a reduction in neonatal mortality, but also suggested the need of further studies to investigate a reduction in morbidity including HIE and neurodevelopmental impairment [12]. Trainings of obstetric emergencies reportedly decreased HIE, but did not include medium-term clinical outcomes [13]. Our results show a significant reduction in mortality in the first month of life combined with a decrease of important morbidities like the incidence of moderate and severe HIE, a reduction of seizures as well as more stable respiratory and cardiocirculatory conditions.
To our knowledge, this study is the first to report a significant reduction in mortality and a concomitant improvement in clinical outcome in a whole region. The improved neurologic outcome was in line with imaging on brain US and MRI. In addition, we found an improved respiratory and cardiovascular situation, with less need for invasive mechanical ventilation and less need for inotropic agents. The improved cardiovascular situation is also reflected by lower creatinine levels as markers for a better renal perfusion and a better organ function. Regarding potential side effects of hypothermic treatment, we did not see a difference in thrombocytopenia, but registered an increase in bradycardia. This is explained because we introduced analgo-sedation with Dexmedetomidine, which has a proven effect on heart rate in these neonates [24].
Unfortunately, in this study we cannot take into account specific details like personnel turnover, although we are not aware of an unexpected high turnover in the departments of obstetrics, neonatology and pediatrics during the three study periods. Another weak point of this study is the relatively limited number of infants due to the small region and the low incidence of HIE of (0.5 – 3/1000 live born neonates in HIC [2,10]. On the other hand, this is also a strength of this study, since we are well aware of all neonates requiring therapeutic hypothermia, which guarantees that we included all infants in the whole region. In addition, the personnel working in the hospitals of our region are all part of the same institution. Therefore, it is possible to define a program that guarantees neonatal resuscitation and simulation training for all health care providers working in the delivery room.
5. Conclusions
Structured and regular neonatal resuscitation and simulation team-training for all birth attendants in the field of obstetrics and neonatology leads to an improved outcome in neonates with HIE. This effect seemed to persist even over a one-year period in which trainings could not be performed.
Author Contributions
“Conceptualization, A.S. and E.C.; methodology, A.S., M.B., A.Z. J.B. and E.C.; software, A.Z., A.S.; validation, A.S. and A.Z., Y.Y.; formal analysis, A.S., A.Z.; data curation, A.S., M.B., A.Z., J.B. and E.C.; writing—original draft preparation, A.S., M.B., A.Z., E.C.; writing—review and editing, A.S., M.B., J.B., A.Z., E.C.; All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
“This research received no external funding”.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Ethics Committee of the Hospital of Bolzano (protocol code 94-2023 and 19th October 2023).”
Informed Consent Statement
“Written informed consent was obtained from all subjects involved in the study.”
Data Availability Statement
No data are shared due to privacy regulatory reasons.
Conflicts of Interest
“The authors declare no conflicts of interest.”
References
- Adstamongkonkul D, Hess DC. Ischemic conditioning and neonatal hypoxic ischemic encephalopathy: a literature review. Cond Med. 2017 Dec;1(1):9-16.
- Greco P, Nencini G, Piva I, Scioscia M, Volta CA, Spadaro S, et al. Pathophysiology of hypoxic-ischemic encephalopathy: a review of the past and a view of the future. Acta Neurol Belg. 2020;120(2):277-280. [CrossRef]
- Azzopardi DV, Strohm B, Edwards AD, Dyet L, Halliday HL, Juszczak E, Kapellou O, Levene M, Marlow N, Porter E, Thoresen M, Whitelaw A, Brocklehurst P; TOBY Study Group. Moderate hypothermia to treat perinatal asphyxial encephalopathy. N Engl J Med. 2009 Oct 1;361(14):1349-58. [CrossRef]
- Douglas-Escobar M, Weiss MD. Hypoxic-ischemic encephalopathy: a review for the clinician. JAMA Pediatr. 2015 Apr;169(4):397-403. [CrossRef]
- Abate BB, Bimerew M, Gebremichael B, Mengesha Kassie A, Kassaw M, Gebremeskel T, Bayih WA. Effects of therapeutic hypothermia on death among asphyxiated neonates with hypoxic-ischemic encephalopathy: A systematic review and meta-analysis of randomized control trials. PLoS One. 2021 Feb 25;16(2):e0247229. [CrossRef]
- Adhikari S, Rao KS. Neurodevelopmental outcome of term infants with perinatal asphyxia with hypoxic ischemic encephalopathy stage II. Brain Dev. 2017 Feb;39(2):107-111. [CrossRef]
- Mathew JL, Kaur N, Dsouza JM. Therapeutic hypothermia in neonatal hypoxic encephalopathy: a systematic review and meta-analysis. J Glob Health. 2022;12: 04030. [CrossRef]
- Lawn JE, Lee AC, Kinney M. Two million intrapartum-related stillbirths and neonatal deaths: where, why, and what can be done? Int J Gynaecol Obstet. 2009;107 (1):S5–18. OctSupplS19. [CrossRef]
- Higgins RD, Raju T, Edwards AD, Azzopardi DV, Bose CL, Clark RH, Ferriero DM, Guillet R, Gunn AJ, Hagberg H, Hirtz D, et al. Hypothermia and other treatment options for neonatal encephalopathy: an executive summary of the Eunice Kennedy Shriver NICHD workshop. J Pediatr. 2011 Nov;159(5):851-858.e1. [CrossRef]
- Lee AC, Kozuki N, Blencowe H. Intrapartum-related neonatal encephalopathy incidence and impairment at regional and global levels for 2010 with trends from 1990. Pediatr Res. 2013;74 Suppl 1(1):50–72. [CrossRef]
- McGuire W. Perinatal asphyxia. BMJ Clin Evid. 2007 Nov 7;2007:0320.
- Strozzi MM, Varrica A, Colivicchi M, Pelazzo C, Negri R, Galante A, Ianniello P, Sterpone R, Nannini P, Leo D, Mannarino F, Striani M, Montani S, Gazzolo D. High-Fidelity simulation-based program improves flow state scale in the perinatal team. Ital J Pediatr. 2021 Feb 25;47(1):42. [CrossRef]
- Draycott T, Sibanda T, Owen L, Akande V, Winter C, Reading S, et al. Does training in obstetric emergencies improve neonatal outcome? BJOG. 2006;113(2):177-82. [CrossRef]
- Duran R, Aladağ N, Vatansever U, Süt N, Acunaş B. The impact of Neonatal Resuscitation Program courses on mortality and morbidity of newborn infants with perinatal asphyxia. Brain Dev. 2008 Jan;30(1):43-6. [CrossRef]
- Perlman JM, Wyllie J, Kattwinkel J, Atkins DL, Chameides L, Goldsmith JP, Guinsburg R, Hazinski MF, Morley C, Richmond S, Simon WM, Singhal N, Szyld E, Tamura M, Velaphi S; Part 11: Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Neonatal Resuscitation Chapter Collaborators. Circulation. 2010 Oct 19;122(16 Suppl 2):S516-38. [CrossRef]
- Wyckoff MH, Aziz K, Escobedo MB, Kapadia VS, Kattwinkel J, Perlman JM, Simon WM, Weiner GM, Zaichkin JG. Part 13: Neonatal Resuscitation: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015 Nov 3;132(18 Suppl 2):S543-60. [CrossRef]
- Wyckoff MH, Wyllie J, Aziz K, de Almeida MF, Fabres J, Fawke J, Guinsburg R, Hosono S, Isayama T, Kapadia VS, Kim HS, Liley HG, McKinlay CJD, Mildenhall L, Perlman JM, Rabi Y, Roehr CC, Schmölzer GM, Szyld E, Trevisanuto D, Velaphi S, Weiner GM; Neonatal Life Support Collaborators. Neonatal Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2020 Oct 20;142(16_suppl_1):S185-S221. [CrossRef]
- Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch. Neurol. 1976;33(10):696–705. [CrossRef]
- Shankaran S, et al. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N. Engl. J. Med. 2005;353(15):1574–1584. [CrossRef]
- Barkovich AJ, Hajnal BL, Vigneron D, Sola A, Partridge JC, Allen F, Ferriero DM. Prediction of neuromotor outcome in perinatal asphyxia: evaluation of MR scoring systems. AJNR Am J Neuroradiol. 1998 Jan; 19(1): 143-9.
- Molloy EJ, El-Dib M, Juul SE, Benders M, Gonzalez F, Bearer C, Wu YW, Robertson NJ, Hurley T, Branagan A, Michael Cotten C, Tan S, Laptook A, Austin T, Mohammad K, Rogers E, Luyt K, Bonifacio S, Soul JS, Gunn AJ; Newborn Brain Society Guidelines and Publications Committee. Neuroprotective therapies in the NICU in term infants: present and future. Pediatr Res. 2023 Jun;93(7):1819-1827. [CrossRef]
- Afifi J, Shivananda S, Wintermark P, Wood S, Brain P, Mohammad K. Quality improvement and outcomes for neonates with hypoxic-ischemic encephalopathy: obstetrics and neonatal perspectives. Semin Perinatol. 2024 Apr;48(3):151904. [CrossRef]
- Sadler LC, Farquhar CM, Masson VL, Battin MR. Contributory factors and potentially avoidable neonatal encephalopathy associated with perinatal asphyxia. Am J Obstet Gynecol. 2016;214(6):747:e1-8. [CrossRef]
- Elliott M, Burnsed J, Heinan K, Letzkus L, Andris R, Fairchild K, Zanelli S. Effect of dexmedetomidine on heart rate in neonates with hypoxic ischemic encephalopathy undergoing therapeutic hypothermia. J Neonatal Perinatal Med. 2022;15(1):47-54. [CrossRef]
Figure 1.
timeline of interventions and evaluation periods.

Figure 2.
Kaplan Meyer curves showing mortality during the first 30 days of life in the three groups.
Figure 2.
Kaplan Meyer curves showing mortality during the first 30 days of life in the three groups.
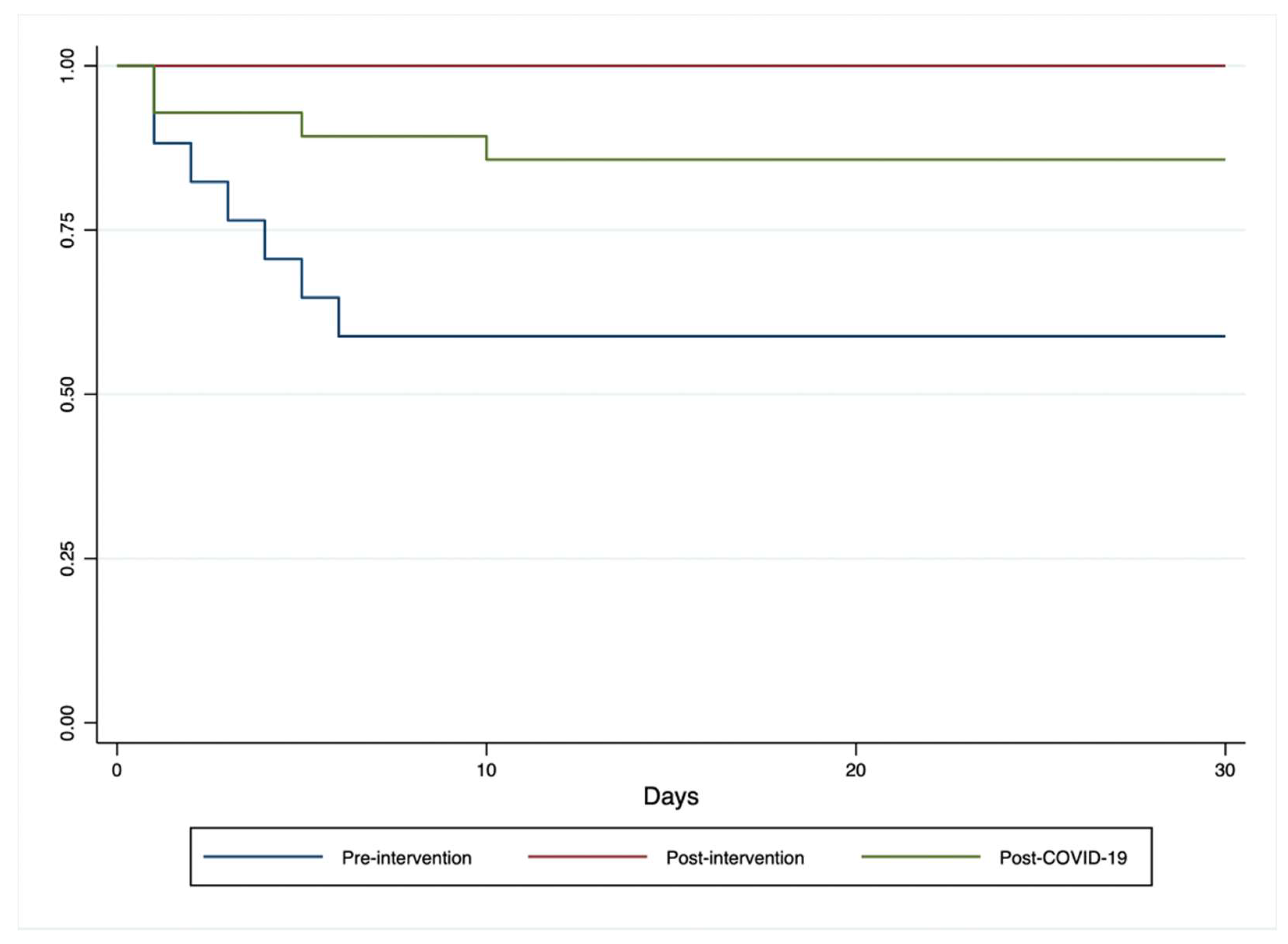
Table 1.
Characteristics of included infants.
| Pre-training | Post-training | Post-SARS-CoV-2 | p | |
|---|---|---|---|---|
| Patients, n (%) | 17 (27.9) | 16 (26.2) | 28 (45.9) | |
| Male, n (%) Female, n (%) |
10 (58.8) 7 (41.2) |
8 (50.0) 8 (50.0) |
13 (46.4) 15 (53.6) |
0.720 |
| Inborn Outborn |
5 (29.4) 12 (70.6) |
8 (50.0) 8 (50.0) |
8 (28.6) 20 (71.4) |
0.311 |
| Birth weight (gms), mean (SD) | 3354 (512) | 3119 (696) | 3188 (505) | 0.306 |
| GA+, mean (SD) | 39.4 (1.6) | 38.5 (2.4) | 39.1 (1.7) | 0.382 |
| Term n (%) Preterm# n (%) |
16 (94.1) 1 (5.9) |
14 (87.5) 2 (12.5) |
25 (89.3) 3 (10.7) |
0.798 |
| pH*, mean (SD) | 6.8 (0.2) | 6.8 (0.2) | 6.9 (0.2) | 0.106 |
| BE*, mean (SD) | 22.5 (7.2) | 19.0 (6.2) | 15.3 (5.9) | 0.003 |
+GA: gestational age; # defined as infants born between 35-37 weeks of gestational age; *ph and base excess reflect the lowest value during the first hour of life.
Table 3.
Short term morbidity and interventions.
| Pre-training | Post-training | Post-SARS-Cov-2 | p | |
|---|---|---|---|---|
| Need for mechanical ventilation, n (%) | 17 (100.0) | 11 (68.7) | 14 (50.0) | 0.002 |
| Need for inotropic agents, n (%) | 13 (76.5) | 5 (31.2) | 14 (50.0) | 0.032 |
| Creatinine > 1.2mg/dl, n (%) | 9 (56.2) | 2 (12.5) | 3 (11.5) | 0.002 |
| Prolonged coagulation, n (%) | 7 (43.7) | 8 (53.3) | 7 (26.9) | 0.218 |
| Bradycardia, n (%) | 4 (23.5) | 9 (56.2) | 24 (85.7) | < 0.001 |
| Trombocytopenia, n (%) | 8 (47.1) | 5 (31.2) | 3 (10.7) | 0.023 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



