
Submitted:
05 January 2025
Posted:
06 January 2025
You are already at the latest version
Abstract
Neisseria gonorrhoeae (NG) is the second most prevalent bacterial sexually transmitted infection worldwide with antimicrobial resistance for expanded-spectrum drugs.
NG antimicrobial resistance (AMR) patterns and sequence types (ST) were analyzed in Israel for the first time between 2016 and 2022. The study examined 1,205 NG isolates collected by the Israeli National NG Reference Center from various healthcare organizations. Antimicrobial susceptibility testing (AST) was performed for seven antibiotics, and molecular characterization was conducted using NG Multi-Antigen Sequence Typing (NG-MAST) on selected isolates. Key findings include:
High resistance rates were observed for ciprofloxacin (54.4%), azithromycin, tetracycline, and benzylpenicillin.
All isolates remained susceptible to ceftriaxone and spectinomycin.
8.6% of isolates were classified as multi-drug resistant (MDR) and 3% as extensively drug resistant (XDR).
72 different NG-MAST sequence types were identified, with ST292, ST4269, and ST5441 being the most common.
Some sequence types showed associations with MDR and XDR phenotypes.
This study provides valuable insights into NG AMR trends and genetic diversity in Israel, highlighting the importance of ongoing surveillance for guiding treatment strategies and public health interventions
Keywords:
gonorrhea
; antimicrobial resistance
; surveillance
; NG-MAST
; sexually transmitted diseases
1. Introduction
Neisseria gonorrhoeae (NG) is the second most prevalent bacterial sexually transmitted infection (STI) worldwide. It has developed antimicrobial resistance (AMR) to all previous first-line drugs, such as penicillin, tetracycline, and fluoroquinolones [1,2], leaving the expanded-spectrum cephalosporins: ceftriaxone and cefixime as the only antibiotics recommended for treatment of gonococcal infections [3,6].
The evolution of AMR in NG has emerged as a critical global health challenge over the past decade. This gram-negative pathogen has demonstrated an exceptional ability to develop resistance to multiple classes of antibiotics, severely limiting treatment options and raising concerns about potentially untreatable gonorrhea infections [5].
One of the most alarming trends has been the increasing resistance to extended-spectrum cephalosporins (ESCs), particularly ceftriaxone, which has long been considered the last line of defense against gonorrhea [4].
In New Zealand, surveillance reports from 2018 to 2022 have tracked the proportion of gonococcal isolates with reduced susceptibility to ceftriaxone [9]. This data provides valuable insights into the evolution of AMR patterns over time and across different demographic groups.
Many nations observed a steady rise in azithromycin resistance, compromising its effectiveness as part of dual therapy regimens [10].
Ciprofloxacin resistance remained high globally, with rates exceeding 50% in numerous countries [10].
The emergence of MDR and XDR strains is particularly concerning [11]. These strains often carry multiple resistance determinants, severely limiting treatment options and posing a significant challenge to public health efforts.
The COVID-19 pandemic led to decreased testing capacity for NG cultures in many countries, affecting surveillance efforts [12].
There was notable inter-study variability and frequently small sample sizes in AMR studies, particularly in Africa, making appropriate inter-study and inter-country comparisons difficult [12].
These trends underscore the urgent need for continued global surveillance, development of new treatment options, and implementation of effective strategies to combat the growing threat of AMR in NG.
The sequence types (ST) of NG play a significant role in determining the patterns of AMR observed in different regions. NG ST defines on molecular analysis based on por and tbpB genes alleles NG multi-antigen sequence type's method (NG-MAST) [11,14].
The most common ST of NG associated with antimicrobial resistance include:
- 1.
- Globally Prevalent Resistant Sequence Types: ST1901 that is frequently associated with decreased susceptibility or resistance to extended-spectrum cephalosporins, particularly ceftriaxone [15,16]. ST1901 has been identified in multiple countries across different continents, indicating its global spread [17].
ST7363 linked to decreased susceptibility to ceftriaxone and resistance to multiple other antibiotics, ST-7363 has emerged as a concerning strain, especially in Asian countries [7,12]. ST1407 that is associated with multidrug resistance, including resistance to cephalosporins and azithromycin[7,14].
- 2.
- Emerging Resistant Sequence Types: ST13871 associated with high-level azithromycin resistance, ST-13871 has been reported in multiple European countries and the United States [7,13]. ST14422 that Identified as a prevalent sequence type in some regions, ST14422 has been associated with resistance to multiple antibiotics, including tetracycline and ciprofloxacin [13,15]. ST11210 that has been linked to decreased susceptibility to extended-spectrum cephalosporins and resistance to fluoroquinolones in some studies [7,15] .
The Israeli National NG Reference Center (INNGRC) of the Ministry of Health (MOH) collect all positive NG isolates from all Israeli healthcare organization (IHO). It's important that Nucleic Acids Amplification Tests (NAAT) for diagnostic of NG in urine, replaces the traditional methods of microbiological cultures, resulting in fewer NG isolates.
The aim of this study was to describe and analyze the phenotypic AMR patterns and trends of NG isolates collected in Israel, between 2016 and 2022, in conjunction with their NG-MAST.
Our study discribeed for the first time ST and antimicrobial resistance of NG in Israel. Our results may contribute to the understanding of global spread of specific ST as well as better treatment and infection containment in Israel.
2. Materials and Methods
2.1. Study Population and Sample Collection
Clinical isolates of NG were collected by the INNGRC, from all IHO: health maintenance organization (HMO), hospitals' laboratories (HL) and STI walk-in clinic (SL). In total, 1205 samples were collected, analyzed, and stored between 2016 and 2022.
2.2. Bacterial Grow and Testing
Isolates were cultured on NYC Medium [19] and incubated for 24 h at 35°C in a 5% CO2 atmosphere.
NG isolates were identified by colony morphology, Gram staining, oxidase, catalase, nitrate tests and Matrix-Assisted Laser Desorption-Ionization Time-Of-Flight Mass Spectrometry (MALDI-TOF MS, Bruker) [20]. All the isolates were stored at -80°C on Protect Micro-organism Preservation Beads in Cryovial of Technical Service Consultants Ltd 21[97]. The ATCC NG strain 49226 was used as an internal control for all test methods [22].
2.3. Antimicrobial Susceptibility Testing (AST)
Panel of 7 antimicrobials: Benzylpenicillin (BEN), ceftriaxone (CTR), cefixime (CIX), azithromycin (AZI), ciprofloxacin (CIP), tetracycline (TET), and spectinomycin (SPE) were tested by using of gradient strip E-test (bioMérieux Marcy-l’E´toile, France) [23], Minimum Inhibitory Concentrations (MIC) (mg/L) were interpreted according to the European Committee on Antimicrobial Susceptibility Testing clinical breakpoints (EUCAST) [24] for sensitivity (S), intermediate (I), and resistance (R).
MDR/XDR of NG susceptibility was defined accordingly: 1. Decreased susceptibility to the cephalosporins or resistance to azithromycin, along with resistance to at least two other antimicrobials was defined as MDR-NG, 2. Decreased susceptibility to a cephalosporin plus resistance to azithromycin as well as resistance to at least two other antimicrobials was defined XDR-NG [25].
All isolates were suspended on Mueller Hinton Broth and cultured on GC Medium Base Agar [16].
2.4. Molecular Characterization Using NG-MAST Genotyping
Sixty-seven isolates from 2017 were characterized by the NG Multi-Antigen Sequence Typing (NG-MAST) system as described [13]. The allele numbers of por and tbpB, and the sequence types (ST's) were assigned using publicly accessible database on the NG-MAST website (available at: https://pubmlst.org/).
Two hunderd and twelve isolates from years 2018 and 2022 were charscterized by whole genome sequencing (WGS). DNA Paired-end libraries were prepared using the Illumina Nextera XT DNA Library Preparation Kit according to Illumina protocols [26]. For sequencing, we utilized the Illumina MiSeq platform using a MiSeq Reagent Kit v2 (500-cycles) (catalogue MS-102-2003) or a MiSeq Reagent Kit v3 (600-cycle), (catalogue MS-102-3003).
Raw short reads were quality analyzed with FastQC v0.11.9 [27] and then trimmed with Trimmomatic v0.39 [28] using the parameters "SLIDINGWINDOW: 4:15 MINLEN: 50". De novo assembly of the short reads was performed using the SPAdes v3.13.1 [29] assembler. NG-MAST [14] STs were assigned to each isolate using the MLST [https://github.com/tseemann/mlst] tool.
3. Results
3.1. Demographic Characteristics of the Study Group
A total of 1205 samples were collected and analyzed throughout the study period. All isolates underwent both phenotypic and molecular testing and were identified as NG based on characteristic colony growth on selective agar media, microscopy of Gram-negative diplococci, biochemical activity tests, and MALDI-TOF MS. The basic demographic information is summarized in Table 1 "Gender distribution".
Among the 1205 examined samples, 82.9% of the isolates were from males, 9.7% from females, and 7.4% were from unknown gender. The median age of all patients was 33 years for males, and 30 years for females for the entire testing period. The gender and age distribution trends for the patients from all IHO are illustrated in Figure 1. "Gender and age distribution of a patients from IHO".
Figure 2 “Comparing of the reported cases and received positive inoculates" compares the number of NG positive inoculates collected at the INNGRC with the overall number of NG positive cases reported to the MOHs Department of Epidemiology.
The number of reported cases was four times higher than the number of NG isolates identified.
3.2. Antimicrobial Susceptibility Testing (AST)
A panel of seven antibiotics—Cefixime (CIX), Azithromycin (AZI), Tetracycline (TET), Benzylpenicillin (BEN), Spectinomycin (SPE), Ciprofloxacin (CIP), and Ceftriaxone (CTR)—was employed for AST on all NG isolates collected in the INNGRC.
The antimicrobial resistance profile of the 1205 isolates is summarized in Table 2 "NG isolates phenotypic antimicrobial resistance profile".
Notably, 54.4% of the isolates exhibited phenotypic resistance to CIP, 41.3% to AZI, 8.7% to CIX, 27.6% to TET, 15.9% to BEN, while no resistance was observed for SPE and CTR.
Figure 3 “Trends of antimicrobial resistance of NG tested in Israel, 2016-2022 (%)” presents the antimicrobial resistance profile for each antibiotic individually.
There was no observed resistance to CTR and SPE, and from 82% up to 99% of the samples were sensitive to CIX. For certain antibiotics such as BEN, AZI, CIP, and TET, three levels of susceptibility were noted: resistant (R), sensitive (S), and intermediate resistance (I). The intermediate resistance level was predominant for BEN (60% - 90%) and TET (40% - 60%), while fluctuations in R/S/I levels for other drugs did not show clear trends. Analysis of the combined effect of various antibiotics indicated that 104 isolates were classified as NG-MDR (8.6%) and 36 isolates as NG-XDR (3%). The distribution of NG MDR/XDR inoculates is illustrated in Figure 4 " NG MDR/XDR distribution in Israel: 2016-2022", showing a low level of NG-MDR isolates (5%) with no NG-XDR detected in the last two years of the study (2021-2022).
3.3. Molecular Characterization by NG-MAST Genotyping
Seventy-two different NG-MAST sequence types were identified among the 279 sequenced isolates collected during the years 2017-2018 and 2022. Only at 2017 the NG-MAST for all samples were identified according to two alleles the number (por and tbpB), and at 2018 and 2022 the NG-MAST was obtained from the WGS data. The full WGS data of NG inoculates in Israel will appear in a separate article. Of these, 36 were represented by a single isolate, 11 by double isolates, and 4 by triple isolates. Twenty-one clusters contained more than four NG isolates. Notably, 8 (11.3%) of the STs had not been previously reported in other countries. The interruption of NG-MAST characterization from 2019 to 2021 was due to all molecular testing resources being redirected to COVID-19 diagnosis and characterization.
All sequence type clusters comprising at least four identical STs are presented in Table 3 "Distribution of NG-MAST sequence types in Neisseria gonorrhoeae isolates in Israel 2017-2018, 2022".
The most common NG-MAST types and their corresponding antimicrobial resistance results are summarized in Table 4.
The most frequently observed STs in Israel included: ST19665 (n=31), ST11461 (n=25), ST292 (n=16), ST4269 (n=16), ST5441 (n=13), ST14994 (n=10), and ST2318 (n=9).
4. Discussion
Our study provides a first overview of the antimicrobial resistance profiles of NG isolates collected over a seven-year period from 2016 to 2022 in Israel. This research also presents the first basic genetic characterization of NG isolates using the NG-MAST method in Israel.
Previous studies have examined various aspects of STIs in Israel, including several publications that have discussed gonococcal antibiotic sensitivity [27,28,29,30] . One such study [31] specifically examined the antibiotic susceptibility patterns of NG isolates obtained from two major healthcare providers in Israel, the HMO and SL. This research focused on evaluating the antimicrobial resistance profiles of NG isolates and provided valuable insights into the changing trends of gonococcal resistance in the region.
The current study aims to expand upon the existing knowledge by conducting a more comprehensive analysis of NG antimicrobial resistance over a longer time frame and incorporating the genetic characterization of the isolates. This multifaceted approach will contribute to a deeper understanding of the epidemiology and evolution of NG strains in Israel, which is crucial for informing targeted public health interventions and guiding the development of effective treatment strategies to combat the growing threat of gonococcal infections.
The NG AMR Monitoring system in Israel provides valuable insights into the epidemiology of gonococcal infections within the country. As depicted in Figure 1, the proportion of male samples (84.2%) was considerably higher than female samples across all IHOs. This observed trend may be attributable to the fact that in many cases, gonococcal infections in females often present asymptomatically [34,35]. This phenomenon likely explains the significant difference and dominance of male samples represented in all types of Israeli IHOs, with a median overall Male-to-Female (MtF) ratio of 12.3:1.
The proportion of females tested in Israel was notably lower (8.4% compared to 15.5%), while their median age was considerably higher (33 years versus 25 years) than the corresponding figures reported in the European study on gonococcal antimicrobial susceptibility surveillance conducted from 2009 to 2017 [2].
Israel has not conducted regular STI surveys that include NG testing across genders. The observed difference in median female age could potentially be linked to Israel's universal military conscription and the tendency for extensive travel post army service.
The age distribution of isolates showed a concentration in sexually active demographics: 76% were from individuals aged 21-40, and 15% from those aged 41-60. Previous Israeli studies have indicated that a portion of patients in these age groups may engage with sex workers [36].
Gonorrhea is a notifiable disease in Israel, requiring mandatory reporting to health authorities [30]. The incidence of reported gonorrhea cases to the MOH's epidemiology department (Figure 2) was found to be four times higher than the number of NG isolates obtained at the INNGRC. This discrepancy is largely due to the prevalence of molecular diagnostic methods for gonorrhea [37], which are primarily used for NG detection in urine samples and allows to obtain reliable results quickly without the need to culture the bacteria.
In recent years, there has been a shift towards molecular diagnostic tests for NG detection, driven by their availability, sensitivity, specificity, reliability, cost-effectiveness, and rapid turnaround time. This trend has resulted in a decrease in the number of NG isolates obtained through traditional microbiological cultures. However, live cultures remain crucial for phenotypic AST, cluster identification, and other genome-based analyses [38], highlighting their continued importance in comprehensive NG surveillance and research.
The World Health Organization (WHO) has set an ambitious global target of reducing gonorrhea incidence by 90% [39], a goal mirrored in Israel's national STI program for 2025 [27]. However, our data reveal no significant decrease in reported gonorrhea cases in Israel between 2016 and 2022, contrary to these objectives similar to many other countries in Europe [40]. Several factors may contribute to this persistent trend:
- Continuous importation of the pathogen through international travel
- Evolving sexual behaviors and practices
- Decreased condom use, potentially influenced by the increased adoption of HIV Pre-Exposure Prophylaxis (PrEP)
- Expanded availability of anonymous testing facilities
- Establishment of dedicated sexual health clinics within HMOs, focusing on STI testing and treatment
These factors collectively create a complex landscape for gonorrhea control, highlighting the challenges in achieving the targeted reduction in incidence. The interplay between improved detection methods, changing risk behaviors, and increased testing accessibility may partially explain the sustained number of reported cases, underscoring the need for multifaceted intervention strategies.
Israel is not considered an endemic country for NG. This non-endemic status has important implications for interpreting the AMR trends observed in our study. While our isolate susceptibility test results reveal clear AMR patterns, these may not represent long-term endemic trends typically seen in countries with sustained local transmission. Instead, they likely reflect a combination of imported strains and limited local spread.
This interpretation is supported by several factors:
- Genetic diversity: our NG-MAST results revealed a high diversity of sequence types, including several found in other countries, suggesting frequent importation [42].
- Fluctuations in AMR patterns: The variability in resistance profiles over time aligns more closely with changing patterns of imported strains rather than stable endemic transmission [43].
Despite these considerations, it's important to note that the AMR trends we've identified in our study shown considerable harmony with findings from analogous research in different parts of the world [44,45,46]. This global concordance suggests that while Israel may not be endemic for NG, it is part of the global network of NG transmission and AMR development.
This interpretation underscores the importance of continued surveillance and the need to consider both local and global factors in understanding and addressing NG AMR in Israel. Further research, including detailed travel history of cases and more extensive molecular typing, would be valuable in confirming and quantifying the extent of imported versus locally transmitted strains.
Similar to the outcomes of European AMR monitoring [47], our study did not detect any resistance to CTR and SPE, which are utilized in Israel for the treatment of NG. These results carry important implications for treatment choices and highlight the necessity for thorough resistance profiling to inform clinical practices.
Our research has indicated a notable rise in resistance to CIP among NG isolates in Israel. The average resistance rate for CIP was found to be 54.4% ± 13.4%, which is more than double the rate of 26.1% recorded in a previous study conducted between 2002 and 2007. This increase is consistent with elevated resistance levels reported worldwide [48,49,50,51]. Resistance to other antibiotics has also approximately doubled compared to earlier studies, as presented in Table 2. The increase in AMR is probably associated with the widespread usage of antibiotics, which has diminished their effectiveness as first-line treatments.
The findings of our study underscore the necessity of monitoring intermediate (I) resistance alongside resistant (R) and susceptible (S) levels. For example, we noted an unexpected decline in BEN resistance from 32% in 2016 to 12% in 2020, along with a reduction in susceptibility (from 3.5% to 1.4%). This trend can be attributed to a significant rise in intermediate resistance, which increased from 62% to 86%. Similar resistance patterns were documented in a study from Northern Spain [52], where BEN resistance rates were R=1.3%, I=81.7%, and S=17.0%, with TET also exhibiting high intermediate resistance (I=43.1%). These insights can assist clinicians in determining the appropriateness of specific antibiotics for either mono or combination therapy [53].
Our study revealed a decreasing trend in XDR and MDR levels from 2016 to 2022. In 2016, 23.4% of isolates were classified as MDR-NG, while 9.9% were XDR-NG. By the years 2021-2022, only MDR-NG strains were detected at rates of 3.4% and 4.2%, respectively, with no XDR-NG strains identified. For context, a comparable number of XDR-NG strains were reported in Canada at the same period [22,54]. Cases of resistance to ceftriaxone and azithromycin have been documented globally, including in the United Kingdom, Australia [55], and France involving two heterosexual patients, one of whom had traveled to Cambodia [56].
Israel is not endemic for NG, as most cases are likely imported by tourists. In comparison, XDR-NG infections in France were linked to patients returning from Cambodia [44]. The impact of the COVID-19 pandemic on tourism could account for the absence of extensively drug-resistant strains and the relatively low prevalence (<5%) of multidrug-resistant strains in 2021-2022.
This research provides the first overview of the sequence type (ST) epidemiology of NG in Israel. We identified significant genetic diversity among a total of 279 isolates. This diversity likely reflects the non-endemic status of gonorrhea in Israel and the impact of international travel and tourism on the strains importation. Several STs prevalent in Israel (ST4269, ST5441, ST2318, ST2997, ST11547, ST16169) were underrepresented in the latest Euro-GASP surveys [2,47].
The study revealed 27 NG-MAST in Israel, previously documented in European surveys conducted between 2009-2010 and 2013. While certain STs were prevalent across various EU countries, not all were detected in Israel. Notably, several clusters common in Israel, including ST2318, ST5441, and ST2992, were also reported in a survey from Spain [2,39,42,54,57].
The most common Israeli clones—ST4269, ST5441, ST2318, ST2997, ST11547, and ST16169—were underrepresented in the most recent Euro-GASP [2,47,53,58]. ST4269, classified as an extensively drug-resistant (XDR) or multidrug-resistant (MDR) cluster, was not identified in Israel in 2022. While internationally disseminated XDR-NG strains ST1407 and ST16406 were absent from Israel, other XDR/MDR-NG clusters like ST4269 and ST2318 were discovered in 2017-2018 and 2017+2022, respectively.
Six of the most prevalent STs in European countries were also detected in Israel (ST21, ST292, ST2992, ST5624 and ST5793) [53,59]. Out of the 21 most prevalent Israeli ST clusters (≥4 isolates), four STs (ST5441, 2992, 5624, 292) were strains circulating in Europe.
Diversity in AMR levels was observed within the same clusters. For instance, two isolates of ST1993, primarily circulating in Belarus and the EU, exhibited sensitivity to all tested antimicrobial agents, whereas ST19972 demonstrated resistance to azithromycin in 50% of cases.
The open and sex-tolerant nature of Israeli society and international travel habits may facilitate the introduction of NG strains. Recent literature has discussed international sexual networks [36]. The scarcity of global data on molecular genotyping for NG may account for the significant number of STs identified solely in Israel, although the existence of local NG variants cannot be discounted.
The WHO recommend to perform ongoing AMR surveillance. Reports on AMR should function as an early warning mechanism for potential community resistance. In cases of suspected AMR, a systematic investigation should be initiated in conjunction with national reference laboratories or WHO regional/international networks.
Currently, Israel lacks a national strategy for AMR NG monitoring, in contrast to established programs such as WHO's GASP, EuroGASP, GASP-Canada, US GISP [50,60,61], AGSP, or UK GRASP. The implementation of an annual GASP/GISP-like program could be vital for overseeing Israel's national STI landscape and for the timely detection of NG superbugs.
5. Study Limitations
The study has several limitations, including the fact that the isolates mainly came from men, and there were only fewer isolates from women. The study does not cover the whole country. We are not sure that all isolates were received from IHO. Another limitation is impossibility to connect behavioral and laboratory components, so the results cannot be attributed to sexual behaviors.
The study is limited by the fact that molecular diagnostic tests are becoming more common than microbiological cultures, resulting in fewer NG isolates. Furthermore, only portion of the isolates were analyzed by NG-MAST. Despite these limitations, the study provides valuable information on the antimicrobial resistance patterns and genetic diversity of gonorrhea in Israel.
Author Contributions
Conceptualization: E. Rorman, Z. Mor, I. Nissan, T. Alon and Z. Dveyrin Investigation: Z. Dveyrin, T. Alon, A. Makhon Data curation: T. Alon, Z. Dveyrin Writing—original draft preparation: Z. Dveyrin Writing—review and editing: Z. Dveyrin, A. Makhon, I. Nissan, Z. Mor and E. Rorman Supervision: Z. Dveyrin Project administration: E. Rorman.
Funding
This research received no external funding.
Data Availability Statement
“Not applicable”.
Acknowledgments
M. Rubinstein.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Unemo M, Shafer WM. Antimicrobial resistance in Neisseria gonorrhoeae in the 21st century: past, evolution, and future. Clin Microbiol Rev. 2014;Jul;27(3):587-613. [CrossRef]
- European Centre for Disease Prevention and Control. Gonococcal antimicrobial susceptibility surveillance in Europe – Results summary 2017. Published online 2019.
- Barry P.; Klausner, J. The use of cephalosporins for gonorrhea: the impending problem of resistance. Expert Opin Pharmacother, 2009, 10, 555-77. [CrossRef]
- Tapsall J. Multidrug-resistant Neisseria gonorrhoeae. CMAJ, 2009, 180(3), 268–269. [CrossRef]
- Aniskevich A, Shimanskaya I, Boiko I. Antimicrobial resistance in Neisseria gonorrhoeae isolates and gonorrhoea treatment in the Republic of Belarus, Eastern Europe, 2009–2019. BMC Infect Dis. 2021;21:520. [CrossRef]
- Ison CA, Hussey J, Sankar KN, Evans J, Alexander S. Gonorrhoea treatment failures to cefixime and azithromycin in England, 2010. Euro Surveill. 2011;16(14):19833. [CrossRef]
- Unemo M SW. Antimicrobial Resistance Expressed by Neisseria gonorrhoeae: A Major Global Public Health Problem in the 21st Century. Microbiol Spectr. 2016;4(3). [CrossRef]
- Unemo M SW. Antimicrobial resistance in Neisseria gonorrhoeae in the 21st century: past, evolution, and future. Clin Microbiol Rev. 2014;27(3)(3):587-613. [CrossRef]
- Antimicrobial resistance in Neisseria gonorrhoeae in New Zealand 2022 surveillance Report. In: Report. The Institute of Environmental Science and Research Ltd; 2023. https://www.esr.cri.nz/media/jt2f3hzt/esr-antimicrobial-resistance-in-neisseria-gonorrhoeae-surveillance-report-2022.pdf.
- Hooshiar MH, Sholeh M, Beig M, Azizian K, Kouhsari E. Global trends of antimicrobial resistance rates in Neisseria gonorrhoeae: A systematic review and meta-analysis. Front Pharmacol. 2024;15:1284665. [CrossRef]
- Schaeffer J, Lippert K, Pleininger S, et al. Association of Phylogenomic Relatedness among Neisseria gonorrhoeae Strains with Antimicrobial Resistance. 2016;Aug;28(8):1694-1698. [CrossRef]
- Kakooza F, Kiggundu R, Mboowa G, et al. Antimicrobial susceptibility surveillance and antimicrobial resistance in Neisseria gonorrhoeae in Africa from 2001 to 2020: A mini-review. Front Microbiol. 2023;14:2023.
- European Centre for Disease Prevention and Control. Molecular Typing of Neisseria Gonorrhoeae – Results from a Pilot Study 2010–2011. ECDC; 2012. [CrossRef]
- Martin IM, Ison CA, Aanensen DM, Fenton KA, Spratt BG. Rapid sequence-based identification of gonococcal transmission clusters in a large metropolitan area. J Infect Dis. 2004;189(8):1497-1505. [CrossRef]
- Hadad R, Golparian D, Velicko I, et al. First National Genomic Epidemiological Study of Neisseria gonorrhoeae Strains Spreading Across Sweden in 2016. Front Microbiol. 2022;v.12. [CrossRef]
- Agbodzi B, Duodu S, Dela H, et al. Whole genome analysis and antimicrobial resistance of Neisseria gonorrhoeae isolates from Ghana. Front Microbiol. Published online June 29, 2023. [CrossRef]
- Mitchev N, Singh R, Allam M, et al. Antimicrobial Resistance Mechanisms, Multilocus Sequence Typing, and NG-STAR Sequence Types of Diverse Neisseria gonorrhoeae Isolates in KwaZulu-Natal, South Africa. Antimicrob Agents Chemother. 2021;17;65(10):e0075921. [CrossRef]
- Yahara K, Ma KC, Mortimer TD. Emergence and evolution of antimicrobial resistance genes and mutations in Neisseria gonorrhoeae. Genome Med. 2021;13:51. [CrossRef]
- Zimbro MJ. Difco & BBL manual: manual of microbiological culture media. BD Diagnostic; 2013.
- Carroll KC. Manual of clinical microbiology. 12th ed. ASM Press; 2019.
- Protect Microorganism Preservation System Store it, preserve it, protect it. www.tscswabs.co.uk/uploads/images/PDF-Downloads/TSC_ProtectFlyerV5.pdf.
- Ng LK, Martin IE. The laboratory diagnosis of Neisseria gonorrhoeae. Can J Infect Med Microbiol. 2005;16(1):15-25. [CrossRef]
- ETEST, Antibiotic Susceptibility Testing Reagent Strips to Determine On-Scale MICs. www.biomerieux-usa.com/sites/subsidiary_us/files/prn_056750_rev_03.a_etest_brochure_final_art_2.pdf.
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version. 2022;12(0). http://www.eucast.org.
- National surveillance of antimicrobial susceptibilities of Neisseria gonorrhoeae annual summary 2019. Published online 2021. https://www.canada.ca/en/services/health/publications/drugs-health-products/national-surveillance-antimicrobial-susceptibilities-neisseria-gonorrhoeae-annual-summary-2019.html.
- Nextera® DNA Library Prep Reference Guide. https://support.illumina.com/content/dam/illumina-support/documents/documentation/chemistry_documentation/samplepreps_nextera/nexteradna/nextera-dna-library-prep-reference-guide-15027987-01.pdf.
- Andrews, S. FastQC: A Quality Control Tool for High Throughput Sequence Data [Online]. Published online 2010. http://www.bioinformatics.babraham.ac.uk/projects/fastqc/.
- Bolger AM, Lohse M, Usadel B. Trimmomatic: a flexible trimmer for Illumina sequence data. Epub 2014 Apr 1 PMID 24695404 PMCID PMC4103590. 2014;1;30(15):2114-20. [CrossRef]
- Bankevich A, Nurk S, Antipov D, et al. SPAdes: a new genome assembly algorithm and its applications to single-cell sequencing. J Comput Biol. 2012;May;19(5):455-77. [CrossRef]
- Chemtob D. A national strategic plan for reducing the burden of sexually transmitted infections in Israel by the year 2025. Isr J Health Policy Res. 2017;6:23. [CrossRef]
- M. D, Z. M, S. G, B. S, T S. Trends in Antimicrobial Susceptibility of Neisseria gonorrhoeae in Israel, 2002 to 2007, With Special Reference to Fluoroquinolone Resistance. Sex Transm Dis. 2010;37(7):451-453.
- Green M, Anis E, Gandacu D, Grotto I. The fall and rise of gonorrhoea incidence in Israel: an international phenomenon? Sex Transm Infect. 2003;79(2):116-118. [CrossRef]
- Kridin K, Ingram B, Becker D, et al. Sexually Transmitted Diseases in Northern Israel: Insights From a Large Referral Laboratory. J Low Genit Tract Dis. 2023;1;27(1):51-55.
- Walker CK, Sweet RL. Gonorrhea infection in women: prevalence, effects, screening, and management. Int J Womens Health. 2011;3:197-206. [CrossRef]
- Martín-Sánchez M. Clinical presentation of asymptomatic and symptomatic women who tested positive for genital gonorrhoea at a sexual health service in Melbourne, Australia. Epidemiol Infect. 2020;148:240. [CrossRef]
- Levi I, Mor Z, Anis E. MSM, risk behavior and HIV infection: integrative analysis of clinical, epidemiological and laboratory databases. Clin Infect Dis. 2011;51(11):1363-1370. [CrossRef]
- Meyer T, Buder S. The Laboratory Diagnosis of Neisseria gonorrhoeae: Current Testing and Future Demands. Pathogens. 2020;9:91. [CrossRef]
- Ghanem KG. Clinical manifestations and diagnosis of Neisseria gonorrhoeae infection in adults and adolescents. https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-neisseria-gonorrhoeae-infection-in-adults-and-adolescents.
- Global health sector strategy on sexually transmitted infections 2016–2021, WHO. https://iris.who.int/bitstream/handle/10665/246296/WHO-RHR-16.09-eng.pdf?sequence=1.
- Chidiac O, AlMukdad S, Harfouche M, Harding-Esch E, Abu-Raddad LJ. Epidemiology of gonorrhoea: systematic review, meta-analyses, and meta-regressions, World Health Organization European Region, 1949 to 2021. Euro Surveill. 2024;29((9):2300226). [CrossRef]
- Clifton S, Bolt H, Mohammed H, et al. Prevalence of and factors associated with MDR Neisseria gonorrhoeae in England and Wales between 2004 and 2015: analysis of annual cross-sectional surveillance surveys. J Antimicrob Chemother. 2018;73(4):923-932. [CrossRef]
- Harris SR, Cole MJ, Spiteri G, et al. Public health surveillance of multidrug-resistant clones of Neisseria gonorrhoeae in Europe: a genomic survey. Lancet Infect Dis. 2018;18(7):758-768. [CrossRef]
- Kirkcaldy RD, Weston E, Segurado AC, Hughes G. Epidemiology of gonorrhoea: a global perspective. Sex Health. 2019;16(5):401-411. [CrossRef]
- Wi T, Lahra MM, Ndowa F, et al. Antimicrobial resistance in Neisseria gonorrhoeae: Global surveillance and a call for international collaborative action. PLoS Med. 2017;17(7). [CrossRef]
- Unemo M, Lahra MM, Cole M, et al. World Health Organization Global Gonococcal Antimicrobial Surveillance Program (WHO GASP): review of new data and evidence to inform international collaborative actions and research efforts. Sex Health. 2019;16(5):412-425. [CrossRef]
- Williamson DA CM. Emerging and Reemerging Sexually Transmitted Infections. N Engl J Med. 2020;382(21):2023-2032. doi:doi:10.1056/NEJMra1907194.
- Cole. The European gonococcal antimicrobial surveillance program (Euro-GASP) appropriately reflects the antimicrobial resistance situation for Neisseria gonorrhoeae in the European Union/ European Economic Area. BMC Infect Dis. 2019;19(1040). [CrossRef]
- World Health Organization. Global action plan to control the spread and impact of antimicrobial resistance in Neisseria gonorrhoeae. Published online 2012. https://apps.who.int/iris/handle/10665/44863.
- World Health Organization. Enhanced Gonococcal Antimicrobial Surveillance Programme (EGASP): general protocol. Published online 2021. https://apps.who.int/iris/rest/bitstreams/1347568/retrieve.
- Kirkcaldy RD, Kidd S, Weinstock HS, Papp JR, Bolan GA. Trends in antimicrobial resistance in Neisseria gonorrhoeae in the USA: the Gonococcal Isolate Surveillance Project (GISP), January 2006-June 2012. Sex Transm Infect. 2013;89(4):5-10. [CrossRef]
- Lahra MM, Hogan TR, Shoushtari M, Armstrong BH. Australian Gonococcal Surveillance Programme Annual Report, 2020. Commun Intell. Published online 2018:45. [CrossRef]
- García UI. Epidemiological surveillance study of gonococcal infection in Northern Spain. Enferm Infecc Microbiol Clın. 2020;38(2):59-64. [CrossRef]
- Młynarczyk-Bonikowska, B., Majewska, A., Malejczyk, M. et al. Multiresistant Neisseria gonorrhoeae: a new threat in second decade of the XXI century. Med Microbiol Immunol. 2020;209:95-108. [CrossRef]
- Martin I, Sawatzky P, Allen V. Multidrug-resistant and extensively drug-resistant Neisseria gonorrhoeae in Canada, 2012-2016. Can Commun Rep. 2019;45(2-3):45-53. [CrossRef]
- ASSESSMENT RAPIDRISK. European Centre for Disease Prevention and Control. Extensively Drug-Resistant (XDR) Neisseria Gonorrhoeae in the United Kingdom and Australia – 7 May 2018. ECDC; 2018.
- Maubaret C, Caméléna F, Mrimèche M, et al. Two cases of extensively drug-resistant (XDR) Neisseria gonorrhoeae infection combining ceftriaxone-resistance and high-level azithromycin resistance. Euro Surveill. Published online May 2022. [CrossRef]
- Chisholm SA, Unemo M, Quaye N, et al. Molecular epidemiological typing within the European Gonococcal Antimicrobial Resistance Surveillance Programme reveals predominance of a multidrug-resistant clone. Euro Surveill. 2013;18(3). http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20358.
- European Centre for Disease Prevention and Control. Gonococcal antimicrobial susceptibility surveillance in Europe, 2011. Published online 2013. [CrossRef]
- Kandinov I, Dementieva E, Kravtsov D, et al. Molecular Typing of Neisseria gonorrhoeae Clinical Isolates in Russia, 2018-2019: A Link Between penA Alleles and NG-MAST Types. Pathogens. 2020;9(11):941. [CrossRef]
- Gonococcal Isolate Surveillance Project (GISP) and Enhanced GISP (eGISP), 2021. Published online 2021. https://www.cdc.gov/std/gisp/gisp-egisp-protocol-august-2021.pdf.
- Kirkcaldy RD, Harvey A, Papp J. Neisseria gonorrhoeae Antimicrobial Susceptibility Surveillance — The Gonococcal Isolate Surveillance Project, 27 Sites, United States, 2014. MMWR Surveill Summ. 2016;65(SS-7):1-19. [CrossRef]
Figure 1.
Gender and age distribution of patients from IHO.
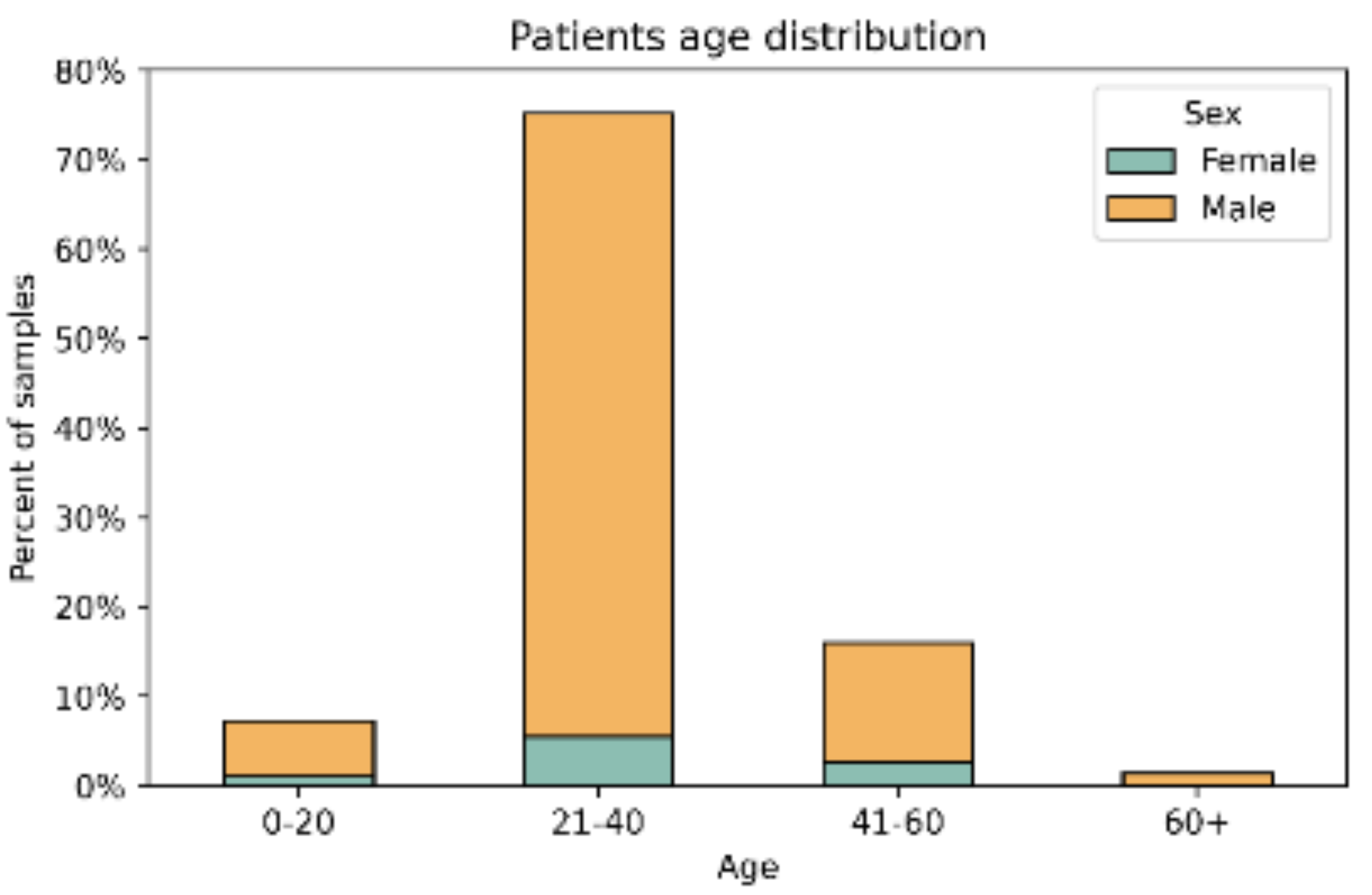
Figure 2.
“Comparing of the reported cases and received positive inoculates.
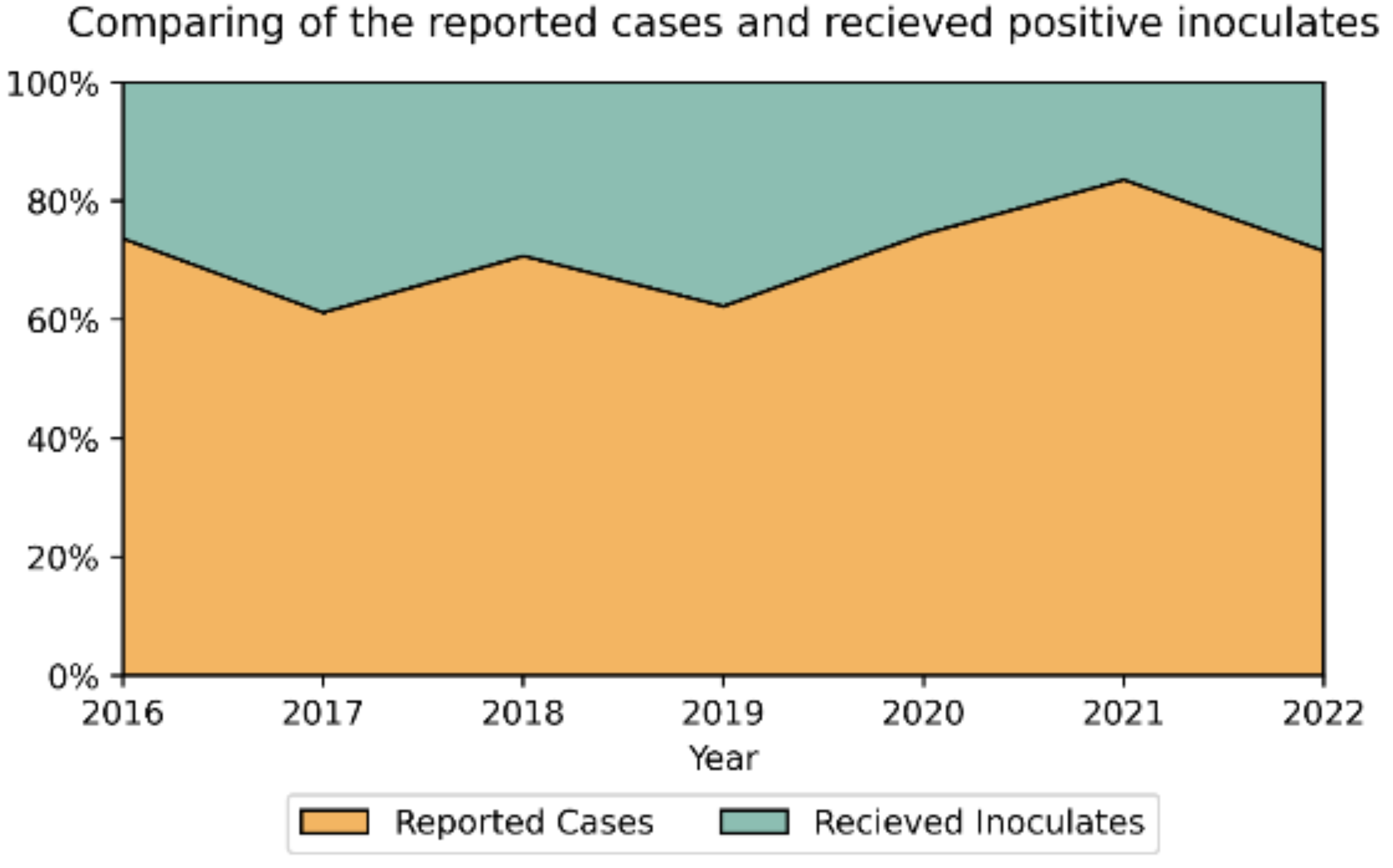
Figure 3.
Trends of antimicrobial resistance of NG tested in Israel, 2016-2022 (%).
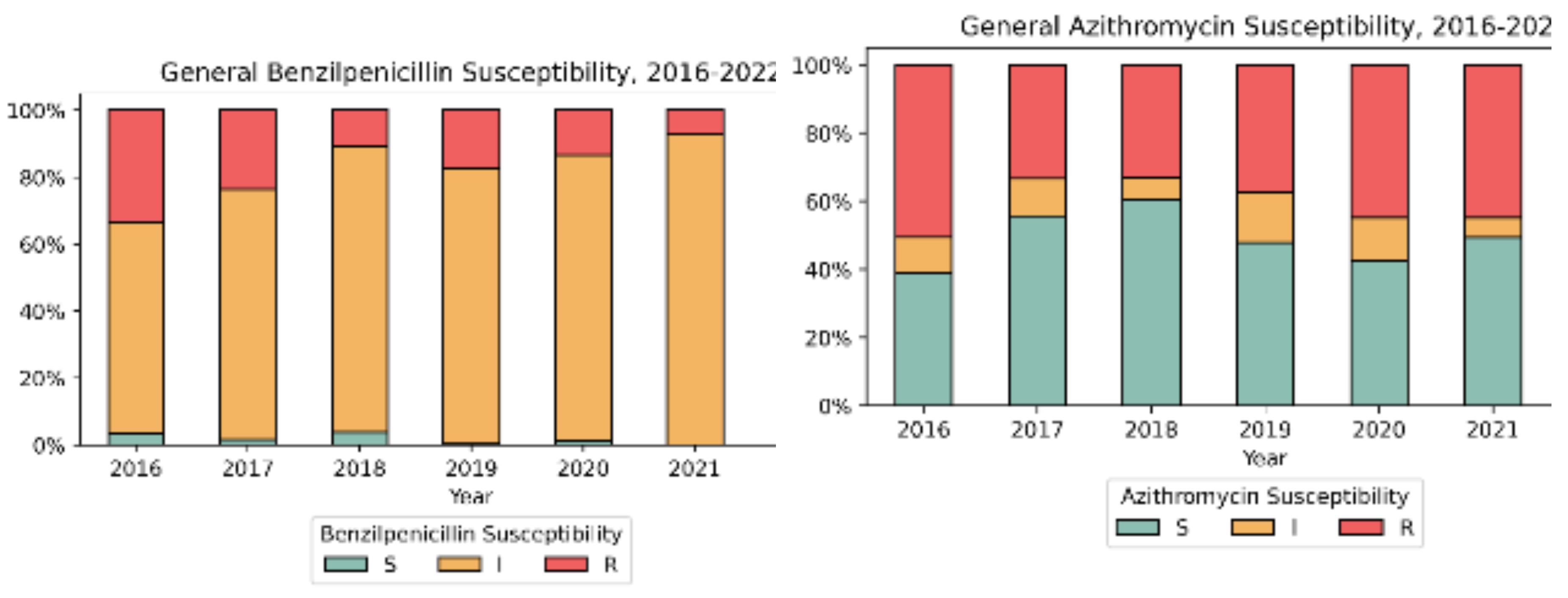

Figure 4.
NG MDR/XDR distribution in Israel: 2016-2022.
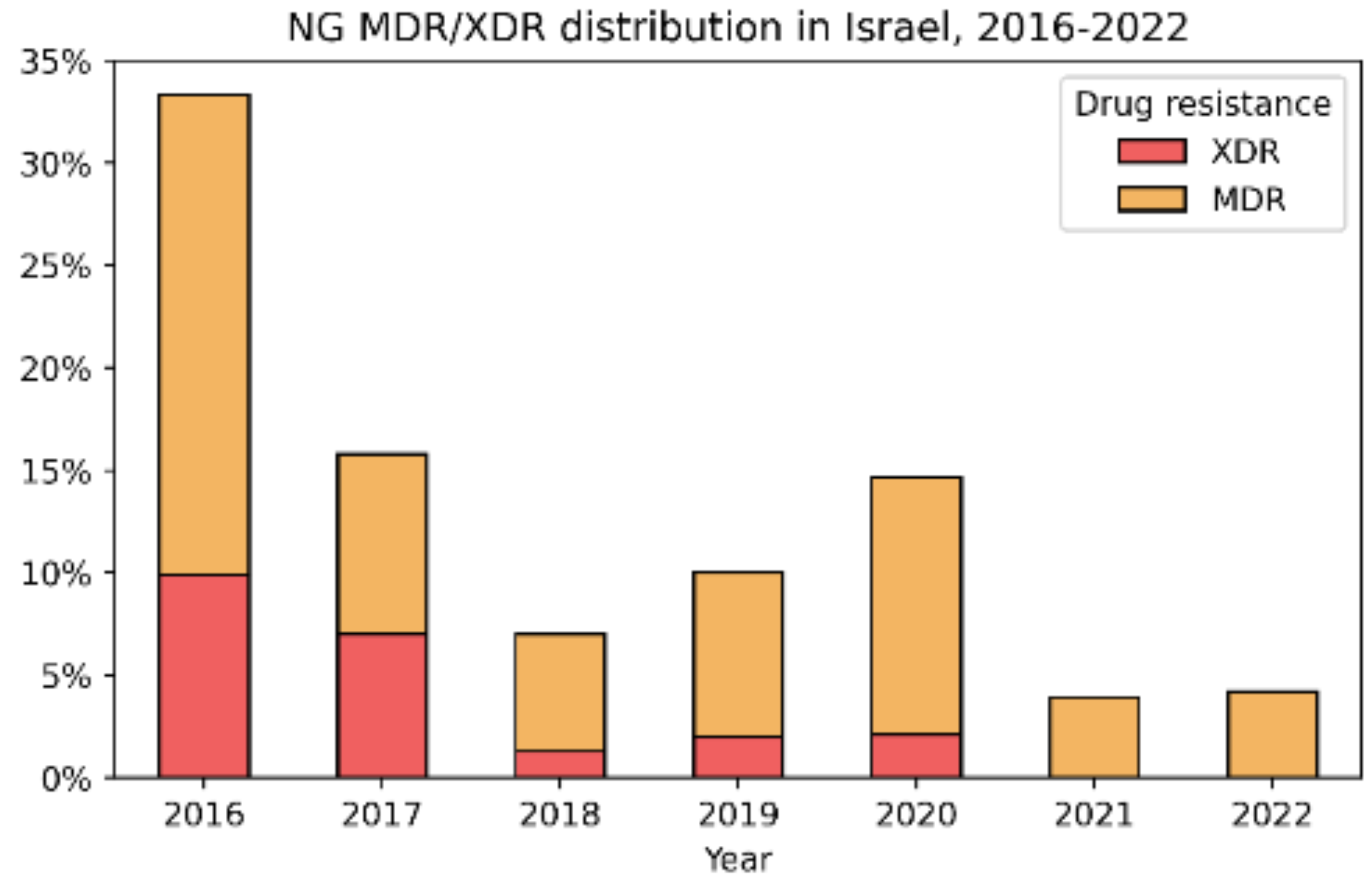

Table 1.
Gender distribution.
| Year | Number of isolates | Ratio male-to-female | Median Age Female/ Male |
|---|---|---|---|
| 2016 | 111 | 14.7 | 27/29 |
| 2017 | 228 | 6.8 | 31/30 |
| 2018 | 157 | 5.8 | 31/29 |
| 2019 | 200 | 14.6 | 41/31 |
| 2020 | 143 | 16.1 | 46/29 |
| 2021 | 152 | 8.9 | 33/28.5 |
| 2022 | 214 | 15.3 | 30/32 |
| All years | 1205 | 10* | 33*/30* |
| 12.3** | 32/30** |
* -average result. **- median result.
Table 2.
NG isolates phenotypic antimicrobial resistance profile.
| No | Year | Number o fisolates |
Resistance* | ||||||
|---|---|---|---|---|---|---|---|---|---|
| CIX | AZI | TET | BEN | SPE | CIP | CTR | |||
| 1 | 2016 | 111 | 20 (18.0%) | 56 (50.5%) | 50 (46.3%) | 37 (33.3%) | 0 | 79 (71.2%) | 0 |
| 2 | 2017 | 228 | 38 (16.7%) | 76 (33.3%) | 58 (25.4%) | 54 (23.7%) | 0 | 105 (46.1%) | 0 |
| 3 | 2018 | 157 | 18 (11.5%) | 52 (33.1%) | 36 (22.9%) | 17 (10.8%) | 0 | 62 (39.5%) | 0 |
| 4 | 2019 | 200 | 14 (7.0%) | 75 (37.5%) | 56 (28.0%) | 35 (17.5%) | 0 | 109 (54.5%) | 0 |
| 5 | 2020 | 143 | 11 (7.7%) | 64 (44.8%) | 43 (30.1%) | 19 (13.3%) | 0 | 105 (73.4%) | 0 |
| 2021 | 152 | 2 (1.3%) | 68 (44.7%) | 36 (23.7%) | 11 (7.2%) | 0 | 85 (55.9%) | 0 | |
| 2022 | 214 | 2 (0.9%) | 106 (49.5%) | 53 (24.8%) | 18 (8.4%) | 0 | 111 (51.9%) | 0 | |
|
Total (Ave%±SD) |
1205 | 105 (8.7% ± 6.3) | 497 (41.2% ± 7.1) | 332 (27.6% ± 8.7) | 191 (15.9% ± 9.6) | 0 | 656 (54.4% ± 13.4) | 0 | |
Abbreviations: Cefixime= CIX, Azithromycin=AZI, Tetracycline=TET, Benzylpenicillin=BEN, Spectinomycin=SPE, Ciprofloxacin=CIP, Ceftriaxone=CTR. The data is number of isolates, with % where relevant. *Resistance breakpoints determined by EUCAST.
Table 3.
Distribution of NG-MAST sequence types in Neisseria gonorrhoeae isolates in Israel 2017-2018, 2022 * represented only by at least 4 isolates.
Table 3.
Distribution of NG-MAST sequence types in Neisseria gonorrhoeae isolates in Israel 2017-2018, 2022 * represented only by at least 4 isolates.
| Year | Number of isolates |
Number of NG-MAST | Most common NG-MAST ST (number of isolate)* |
|---|---|---|---|
| 2017 | 78 | 72 | ST4269 (13), ST2318 (7), ST2997 (7), ST5441 (6), ST5049 (5), ST292 (4), ST5624 (4) |
| 2018 | 77 | 72 | ST292 (12), ST5441 (6), ST16169 (6), ST2992 (5), ST11547 (5), ST11461 (4) |
| 2022 | 124 | 72 | ST19665 (31), ST11461 (25), 14994 (10), 19762 (10), 17972 (8), 14764 (5) |
| Total | 279 | 72 | ST19665 (31), ST11461 (30), ST4269 (16), ST292 (16), ST14994 (14), ST5441 (13), ST19762 (10), ST2318 (9), ST17972 (8), ST2992 (7), ST11547 (7), ST2997 (7), ST16169 (6), ST5049 (5), ST9208 (5), ST14764 (5), ST3935 (4), ST14760 (4), ST14051 (4), ST5624 (4), ST12302 (4) |
Table 4.
Distribution of most prevalent STs antimicrobial pattern.
| NG-MAST | n* | MDR,% | XDR,% | CIP** | BEN** | TET** | AZI** | CIX** |
|---|---|---|---|---|---|---|---|---|
| 19665 | 31 | 0 | 0 | S(96.8%) R(3.2%) |
I | S(3.2%) I(93.5%) R(3.2%) |
S(9.7%) R(90.3%) |
S(96.8%) R(3.2%) |
| 11461 | 30 | 0 | 0 | S(83.3%) R(16.7%) |
I | S(3.3%) I(13.3%) R(83.3%) |
S(86.7%) R(13.3%) |
S |
| 292 | 16 | 0 | 0 | S | I | S(25.0%) I(75.0%) |
S(87.5%) I(6.2%) R(6.2%) |
S |
| 4269 | 16 | 29.4 | 64.7 | R | I(17.6%) R(82.4%) |
I(5.9%) R(94.1%) |
I(5.9%) R(94.1%) |
S(29.4%) R(70.6%) |
| 14994 | 14 | 0 | 0 | R | I(92.9%) R(7.1%) |
S(50.0%) I(50.0%) |
S(85.7%) I(7.1%) R(7.1%) |
S |
| 5441 | 13 | 0 | 0 | S | S(7.7%) I(92.3%) |
S | S(30.8%) I(30.8%) R(38.5%) |
S |
| 19762 | 10 | 10 | 0 | R | I | S(10.0%) I(80.0%) R(10.0%) |
S(20.0%) R(80.0%) |
S |
| 2318 | 9 | 45.5 | 9.1 | S(9.1%) R(90.9%) |
I(81.8%) R(18.2%) |
I(18.2%) R(81.8%) |
S(27.3%) R(72.7%) |
S(90.9%) R(9.1%) |
| 17972 | 8 | 12.5 | 0 | R | I | I(87.5%) R(12.5%) |
S(25.0%) R(75.0%) |
S |
| 2997 | 7 | 0 | 0 | S | I | I(71.4%) R(28.6%) |
I(14.3%) R(85.7%) |
S |
| 2992 | 7 | 0 | 0 | S(85.7%) I(14.3%) |
I | S(14.3%) I(85.7%) |
I(28.6%) R(71.4%) |
S |
| 11547 | 7 | 14.3 | 0 | R | I(85.7%) R(14.3%) |
S(28.6%) I(71.4%) |
S(71.4%) I(14.3%) R(14.3%) |
S(14.3%) R(85.7%) |
| 16169 | 6 | 0 | 0 | R | I | S(33.3%) I(66.7%) |
S(66.7%) R(33.3%) |
S |
| 9208 | 5 | 0 | 0 | S | I | S(40.0%) I(60.0%) |
S(40.0%) I(20.0%) R(40.0%) |
S |
| 5049 | 5 | 0 | 0 | S | I | I(80.0%) R(20.0%) |
R | S |
| 14764 | 5 | 0 | 0 | R | I | I | R | S |
| 14760 | 4 | 0 | 0 | S | S(25.0%) I(50.0%) R(25.0%) |
S(50.0%) I(50.0%) |
S | S |
| 12302 | 4 | 50 | 0 | I(25.0%) R(75.0%) |
I | I(50.0%) R(50.0%) |
R | S |
| 14051 | 4 | 50 | 0 | R | I | I(25.0%) R(75.0%) |
S(50.0%) R(50.0%) |
S |
| 5624 | 4 | 50 | 0 | R | I(50.0%) R(50.0%) |
I | R | S |
| 3935 | 4 | 0 | 0 | S | I | I | R | S |
*represented by n = 4 isolates. **Abbreviations: Ciprofloxacin=CIP, Tetracycline=TET, Azithromycin=AZI, Benzylpenicillin=BEN, Cefixime= CIX.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



