
Submitted:
02 January 2025
Posted:
03 January 2025
You are already at the latest version
Abstract
This study aims to identify cardiovascular risk factors among 91 patients with multiple sclerosis in Bucharest, Romania, using data from medical records and a self-administered questionnaire. The research focuses on smoking status, body mass index, blood sugar, cholesterol, triglycerides, blood pressure and renal function. The average age of the patients was 42.90 ± 10.60 years and 74.73% were female. The average BMI was 23.89 kg/m2 ± 4.74 kg/m2 (lower than in general population), with 41.76% of patients having a BMI outside normal limits. The majority were former smokers (35.87%), followed by non-smokers (28.26%) and the fewest were smokers with more than 20 cigarettes/day (7.61%). The average total cholesterol was 198.48 ± 38.56 mg/dl, triglycerides were 114.22 mg/dL ± 76.2281 mg/ dl, and blood glucose was 97.54 ± 36.58 mg/dl. 25.27% of the patients had fasting blood glucose > 126 mg/dl, but only 5 patients were diagnosed with DM. The average blood pressure was 137,5165 ± 19,5047 mmHg, with only 11 patients diagnosed with HTA. The study found an average cardiovascular risk of 6,6133% ± 7,1412%, with higher values among males, rural patients, those with secondary-progressive MS, and those with a disease progression >10 years (after age adjustment). The study underscores the importance of identifying and combating cardiovascular risk factors in patients with multiple sclerosis.
Keywords:
multiple sclerosis
; cardiovascular risk
; smoking
; dyslipidemia
; glycemia
; arterial hypertension
; renal function
; EDSS
1. Introduction
Multiple sclerosis (MS) represents a significant public health concern, being the primary cause of non-traumatic neurological disability among young adults both in Romania and globally, with an estimated 2.8 million individuals affected [1]. MS is a severe, chronic and progressive disease that affects the central nervous system (CNS), with predominantly cerebral lesion [2], and the manifestations of the disease have been described since the mid-19th century. The disease involves both motor and sensory manifestations, as well as cognitive impairments that worsen over time. Despite the identification of numerous potential causes and risk factors (Figure 1), the etiology of the inflammatory and degenerative processes remains elusive to this day, considered to be the result of the interaction of various environmental and genetic factors that affect the immune system [3].
The course of a patient with MS is inconstant and challenging to anticipate [3]. Both relapses and remissions are difficult to predict [4]. The diagnosis is established by associating clinical features (signs and symptoms) with the presence of lesions on paraclinical investigations, respecting the dissemination in time and space according to the McDonald diagnostic criteria [4,5] and by excluding other pathologies.
Cardiovascular diseases (CVDs) account for approximately one-third of global mortality, a significant portion of which is avoidable and occurs prematurely. CVDs, mainly ischemic heart disease (IHD) and stroke, are the foremost contributors to global illness, thereby exacerbating the disabilities experienced by individuals with MS [7]. The distress endured by patients leads to elevated disability-adjusted life years (DALYs), a reduced quality of life, and frequently substantial medical costs. The effects on patients also encompass societal and economic consequences. Absences or diminished efficacy at work result in reduced output, imposing a burden of lost productive time. This problem extends beyond paid employment; declines in productivity also impact unpaid labor, obstructing tasks such as cleaning, childcare, and volunteering, all of which are vital for a functional community [8].
Treatment options for MS have expanded significantly since the introduction of interferons, with the development of various disease-modifying therapies (DMTs) that target different mechanisms of the disease [9]. These include monoclonal antibodies such as natalizumab and ocrelizumab, oral agents like fingolimod, dimethyl fumarate, and teriflunomide, and newer infusion therapies such as alemtuzumab. These DMTs aim to reduce relapses, slow disability progression, and limit new disease activity visible on MRI [10]. Research continues to advance, with numerous drugs in development focusing on more targeted and effective approaches, including those that promote remyelination and neuroprotection. DMTs play a crucial role in altering the natural course of MS, improving long-term outcomes, and preserving quality of life.
Disease-modifying therapies (DMTs) for MS are associated with a wide range of side effects, varying by drug type. Common adverse effects include injection site reactions (e.g., with glatiramer acetate), gastrointestinal symptoms, flushing, and hair thinning (e.g., with dimethyl fumarate and teriflunomide)[11]. Monoclonal antibodies like alemtuzumab can cause infusion-related reactions, an increased risk of infections, and autoimmune complications. Rare but severe side effects include immune thrombocytopenic purpura [12], hepatitis, cardiovascular complications, and malignancies in some cases (e.g., with cladribine)[13]. While these treatments can be highly effective, their risks necessitate careful monitoring and individualized therapy plans to ensure safety and optimize outcomes.
Patients diagnosed with MS had a 3.5-fold greater risk of death from any cause and a 1.5-fold higher risk of death from cardiovascular disease [14]. As regards the prevalence of cardiovascular risk factors (hypertension, diabetes mellitus, smoking, dyslipidemia, etc.) in patients with MS compared to the general population, the data in the literature are inconsistent, with no clear consensus [7,8,9,10,11,12,13].
Genetic studies have revealed an association between the genetic burden in MS and an increased risk of cardiovascular diseases, such as coronary artery disease, heart failure, myocardial infarction, and ischemic stroke [22].
Patients with MS may also present with other comorbid conditions. Given that cardiovascular and cerebrovascular diseases rank among the leading causes of morbidity and mortality worldwide, the risk of developing these conditions remains elevated even in patients with MS [23]. Optimal care for these patients must consider the identification and management of comorbidities. Therefore, the presence of cardiovascular risk factors associated with MS increases the cumulative risk of disability by exacerbating vascular risk [24]. This underscores the importance of both disease-modifying treatment for MS and primary prevention of cardiovascular events. The medium- and long-term progression of MS is associated with a decline in general health, physical and emotional functional deficits, and disease-specific cognitive deterioration, exacerbated by physiological aging, leading to a significant decrease in quality of life [25].
The early initiation of effective disease-modifying therapy, aimed at reducing inflammation in the initial years following onset, can decrease the risk of cerebrovascular events. However, it is unclear to what extent these therapies directly influence cardiovascular risk, as some medications have side effects such as hypertension or hyperglycemia [3,26].
The management of patients with MS is complex and requires a multidisciplinary approach throughout the course of the disease. Although a causal relationship between MS and cardiovascular risk is not fully elucidated, periodic screening for risk factors is essential for preventing cardiovascular and cerebrovascular events, considering the increased risk with aging and possibly with the duration of disease-modifying treatments.
Thus, this study aims to identify and analyze the prevalence of existing cardiovascular risk factors among patients with MS and to establish the relationship between cardiovascular risk and the course of this disease. Identifying and addressing the impact of these factors on the course of patients with MS provides significant advantages for both the healthcare system and the patients. It enables personalized treatment and care. A multidisciplinary approach is essential to cover all aspects of treatment: disease modification, symptom management and recovery, thereby contributing to the improvement of patients' quality of life.
2. Materials and Methods
Type of Study
This study has the characteristics of a descriptive, observational, retrospective, cross-sectional study. The research aims to identify cardiovascular risk factors and to analyze their prevalence among 91 selected patients with MS hospitalized in the Neurology Department of the Central Military Emergency University Hospital in Bucharest between September 2022 and September 2023.
Study Population
Patients were selected according to the criteria in Table 1.
Data Collection
The data used in this study were collected by analyzing the observation forms of the patients in the hospital's archive, previously obtained through anamnesis, clinical examination and paraclinical investigations. Among them, we used in this study the following data: age, sex, background, form of MS and age of onset of the disease; Body Mass Index (BMI); Pathological and hereditary personal history; Smoking; Alcohol consumption; Treatment; Glycaemia; Lipid profile (Cholesterol, HDL, LDL, triglycerides). We also collected data by means of a self-administered questionnaire designed to obtain the information necessary to identify possible cardiovascular risk factors. The questionnaire was distributed both online and in physical format. The processing of patient data was done in accordance with international regulations, legislation and ethical rules. Consent to access patients' medical data was obtained by application to the hospital ethics committee (approval number: CR 6344, obtained on July 1st 2023). We used the SCORE algorithm to estimate cardiovascular (CV) risk over a 10-year period. This tool has been developed by the European Society of Cardiology (ESC) and is used to estimate the risk of coronary atherosclerosis and major cardiovascular events such as heart attacks and strokes [27].
Statistical Analysis
The collected data were stored and subsequently processed and statistically analyzed using Microsoft Office Excel 2021. Both categorical (binary, nominal, ordinal) and quantitative (discrete and continuous) variables were used. Descriptive analysis (frequencies, ranges, minimum and maximum values) and indicators of central tendency (mean) were used to process the quantitative variables, calculating errors and standard deviations. In order to determine the statistical significance of the processed data, we calculated the predictive p-value using the Student-T test for quantitative variables. A p-value < 0.05 is considered statistically significant.
3. Results
Of the 108 patients who met the inclusion criteria for the study, 17 of them were eliminated due to exclusion criteria: 3 for criteria 1, 2 for criteria 2, 11 for criteria 3 and 1 for criteria 4 (Table 1).
3.1. Baseline Characteristics
Among the 91 patients included in the study, 68 (74.73%) were female, reflecting the gender distribution of MS cases in the general population [28]. The mean age of the cohort was 42.90 ± 10.60 years. The largest subgroup of patients was aged 30-45 years, comprising 40 individuals (43.96%), followed by those over 45 years with 39 individuals (42.86%), and the smallest subgroup, consisting of 12 individuals (13.19%), was under 30 years. The mean age at disease onset was 33.86 ± 9.81 years. The mean duration of disease progression within the study group was 9.14 ± 5.86 years, with a range from 8 months to 28 years.
Most of the patients, 65 (71.43%), resided in urban areas, while the remaining 26 (28.57%) were from rural areas, yielding an urban-to-rural ratio of 3:1. This may be due to a lack of attendance and limited access to health services for people in rural areas. Also, another factor may be the migration of young people to urban areas with the ageing of the rural population, the average age of urban people being 42.33 years compared to 45.20 years for rural areas.
Regarding the characteristics of the disease, the relapsing-remitting form of MS was the most prevalent, accounting for 84.62% of cases. This was followed by the secondary-progressive form, which constituted 10.99% of cases, and the primary-progressive form, which was the least common at 4.40% (Table 2).
We assessed the degree of disability in patients using the Expanded Disability Status Scale (EDSS), with a mean score of 2.60 ± 1.82. To streamline reporting and utilize disability levels as a marker of disease severity, we classified patients with an EDSS score of <2.5 as having a mild form of the disease, while those with a score ≥2.5 were categorized as having a more severe form.
3.2. Lifestyle Risk Factors
For a better analysis of the data obtained about smoking, we divided the patients into 5 categories: non-smokers, ex-smokers, passive smokers (non-smoker but exposed to cigarette smoke regularly) and current smokers with ≥ or < 20 cigarettes per day. Most of the patients were former smokers (33, 35.87%), followed by non-smokers (26, 28.26%) and the fewest were smokers with more than 20 cigarettes/day (7, 7.61%).
Regarding alcohol consumption, the results are encouraging: 40% of patients reported never drinking alcohol, while another 40% stated they consume alcohol monthly or less frequently.
To get an overview of the psychological status of the patients, using the questionnaire they self-assessed their level of stress in the last 6 months, the frequency of anxiety and depression episodes. About one third of the patients (31.86%) considered themselves to be stressed for more than 3 out of 6 months or even permanently, 34 of the patients (37.36%) said they were sometimes or rarely stressed, and the rest (30.77%) were not stressed (Figure 2 (a)). Symptoms that suggest panic attacks were experienced by 29.67% of patients, 66.66% of whom reported having panic attacks on a weekly basis (Figure 2 (b)). Feelings of sadness, depression, hopelessness, loneliness or loss of interest in social interaction were present in almost half (43.95%) of the patients in the group, with a third (32.50%) of them reporting their presence weekly or more often (Figure 2 (c)).
Given that body weight is a significant cardiovascular risk factor, we assessed each patient's body mass index (BMI) and abdominal circumference. The mean BMI was 23.89 ± 4.74 kg/m², while the mean abdominal circumference was 83.51 ± 17.71 cm. More than half of the patients (53, 58.24%) had a BMI within the normal range. However, 6 patients (6.59%) were classified as underweight, 25 (27.47%) as overweight, 5 (5.49%) as having grade II obesity, and 2 (2.20%) as having grade III obesity.
The mean BMI of participants was analyzed based on age group and sex. The lowest mean BMI (22.94 ± 4.03 kg/m²) was observed in the 30-45 age group, while similar mean BMIs were recorded for patients under 30 (24.55 ± 3.25 kg/m²) and those over 45 (24.65 ± 5.64 kg/m²). A statistically significant difference (p < 0.05) emerged when stratifying by sex, with females having a lower mean BMI compared to males (23.41 ± 4.61 kg/m² vs. 25.31 ± 4.91 kg/m², respectively).
According to the questionnaire, patients self-rated their level of physical activity in one of 4 possible categories: sedentary, light, moderate and vigorous. About 13% of patients were identified as sedentary, while the majority (55%) reported engaging in light physical activity. Approximately 26% of participants indicated a moderate level of physical activity, and only 6% fell into the intense activity category. We then averaged the EDSS score for each category. The sedentary patients had the highest mean EDSS score (4.9545), and those with intense physical activity had a mean EDSS score of 1.500. Physical activity level was not correlated with patients' BMI, with all groups having a mean BMI within normal limits (Table 3). It was evident that the degree of disability served as a restrictive factor for the level of activity, but no correlation between the BMI and the level of physical activity was observed.
Medical History
For analyzing personal pathological history, we used both data from the observation sheets and data provided by the patients through the questionnaire. We selected only personal pathological antecedents relevant to cardiovascular risk: diagnosed cardiovascular disease (hypertension), diagnosed atherosclerosis, acute myocardial infarction in the past, stroke in the past, angina in the last 3 months and diabetes mellitus (Figure 3).
On clinical examination, including a single blood pressure measurement, the mean blood pressure values were 137.52 ± 19.50 mmHg for systolic blood pressure (sBP) and 84.67 ± 22.88 mmHg for diastolic blood pressure (dBP). Although only 11 patients had a formal diagnosis of hypertension, 44 (48.35%) exhibited systolic BP ≥ 140 mmHg or diastolic BP ≥ 90 mmHg, and 30 (32.97%) had borderline high BP. Notably, when comparing these findings with data from the literature, the percentage of MS patients diagnosed with hypertension is similar to reported figures [21,29], but the percentage of those with elevated blood pressure values is significantly higher, closely mirroring the prevalence of hypertension in the general adult population in Romania [30]. It is important to acknowledge potential limitations related to blood pressure values, such as the influence of white-coat hypertension, which could affect the accuracy of single-point measurements in certain individuals.
Stratifying by age group, the mean sBP and dBP values were calculated. Patients aged 30-45 years had the lowest values (sBP = 132.83 mmHg, dBP = 82.68 mmHg), whereas those over 45 years had the highest values, with means exceeding the maximum accepted normal values (sBP = 143.13 mmHg, dBP = 86.69 mmHg). This slightly concave shape of the mean blood pressure curve (Figure 4) may be attributed to greater awareness of cardiovascular risk among patients aged 30-45 years and the initiation of antihypertensive treatment within this group.
Blood Tests
We selected only the blood analyses available for all patients and calculated the mean values for each, using as biological reference intervals the values of the laboratory of the hospital where the analyses were worked (Table 4).
Although only 5 patients in the group had a formal diagnosis of diabetes mellitus (DM), an additional 5 patients exhibited blood glucose levels ≥126 mg/dL, suggesting possible undiagnosed DM. The percentage of patients with DM in this study was lower than that reported in a similar cohort (35.5%)[16]. When compared to the prevalence of DM type 2 in Romania, the results are comparable in terms of the percentage of diagnosed diabetics (8.4%-11.6%)[31].
The mean total cholesterol value among the patients was 198.48 ± 38.56 mg/dL, which is close to the upper limit of normal. According to reference values, 51 patients (56.04%) had normal cholesterol levels, 27 patients (29.67%) were at moderate cardiovascular risk (200-239 mg/dL), and 13 patients (14.29%) were at high risk (values > 240 mg/dL).
The mean LDL-cholesterol value was 120.80 ± 36.67 mg/dL. Approximately one-third of the patients had normal values, while those at low risk (100-129 mg/dL) were nearly equal in number to those at moderate risk (130-159 mg/dL). Only 7 individuals had values above 160 mg/dL, indicating high risk.
The mean HDL-cholesterol value was 56.66 ± 14.93 mg/dL, with most patients having normal values. According to reference values, 21 women (30.88%) had HDL-C values <50 mg/dL, and 3 men (13.04%) had HDL-C values <40 mg/dL, placing them at major cardiovascular risk. Regarding triglyceride levels, an increase in the mean value was observed in direct proportion to the age of the patients. Patients under 30 years of age had the lowest mean value (82.39 ± 21.56 mg/dL), while those over 45 years of age had a mean value of 140.10 ± 95.79 mg/dL. When dividing the group by sex and age, an approximately linear increase in mean triglyceride values was observed in men, whereas a sharp increase in triglycerides occurred among women after the age of 45 years (Figure 5).
In our analysis of inflammatory markers, we focused exclusively on the erythrocyte sedimentation rate (ESR), as it was the only marker consistently available in the patients' blood tests. The mean value of ESR was 13,4407±10,9580 mm/s. Notably, patients with the secondary progressive form of MS exhibited the highest mean value of the erythrocyte sedimentation rate (ESR) at 21,0000 mm/s, in comparison to 12,8065 mm/s for the relapsing-remitting form and 6,7500 mm/s for the primary progressive form.
Recognizing the myriad factors that contribute to the decline in renal function of MS patients—including age, comorbidities such as hypertension or diabetes, and the adverse effects of treatments—presents a challenge in isolating the impact of each individual factor. We analyzed the serum creatinine and urea values, which had means of 0.7369 mg/dl and 34.8428 mg/dl, respectively. No significant difference was observed between the age groups. Patients with systolic blood pressure exceeding 130 mmHg demonstrated higher mean creatinine and urea levels, though the difference was not statistically significant (p-value > 0.05).
SCORE Algorithm
The Romanian population was categorized as being at high CV risk. Thus, depending on age, sex, smoking/non-smoking status, non-HDL cholesterol and systolic blood pressure values, we calculated the SCORE value. The mean value of the cardiovascular risk obtained was 5.9670% ± 6.8774% (MIN=0%, MAX=31%). Mean cardiovascular risk in men (6.4782 ± 8.8824%) was higher than in women (4.7941 ± 6.1244%).
A significant difference was observed in terms of the patients' background, with people from rural area having a cardiovascular risk of 7.9629% compared to urban people with a much lower mean 5.1250%.
We analyzed the influence of the presence of dyslipidemia on the SCORE value. Indeed, the non-HDL-cholesterol value is part of the algorithm for calculating the score, but we looked at the influence of the accumulation of lipid metabolism disorders on cardiovascular risk. We therefore calculated the risk for each group of patients: no dyslipidemia, only hypercholesterolemia, only hypertriglyceridemia or both. Patients with both hypertriglyceridemia and hypercholesterolemia had the greatest cardiovascular risk (Table 5).
We divided patients again, this time according to EDSS score as we presented at the beginning of this study. We averaged the cardiovascular risk for each group of patients. The results showed that patients with a lower degree of disability, had a SCORE value approximately half that of those with more severe disability, and the difference was statistically significant (p < 0.05).
Figure 6.
Mean SCORE for each form of multiple sclerosis.
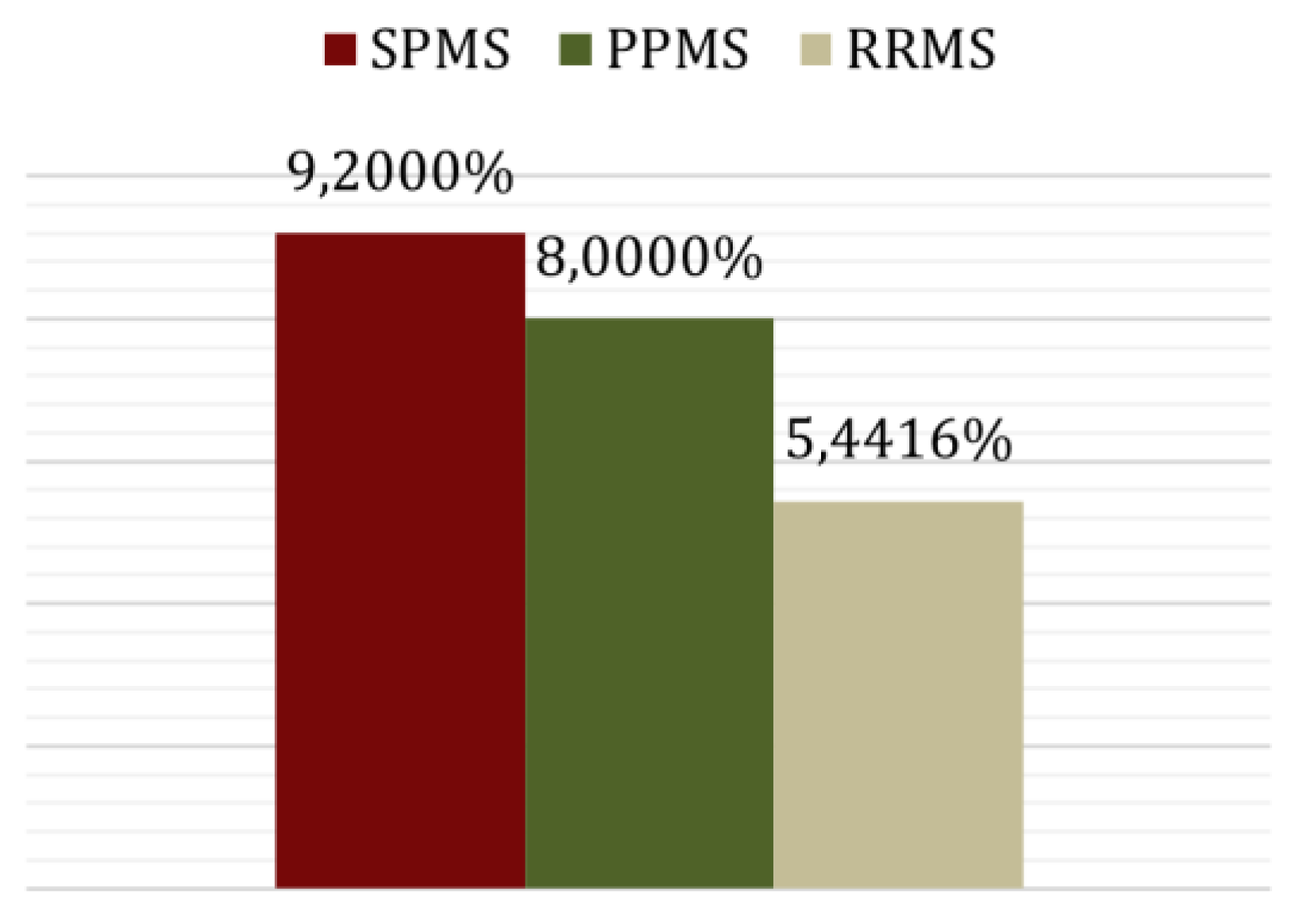
Patients with relapsing-remitting MS had the lowest risk, 5.441%, and those with secondary-progressive MS (SPMS) reached a value of 9.2000% being only one per cent higher than those with primary-progressive MS (PPMS) (Figure 5). Disease progression in SPMS and PPMS involves a steady increase in disability, potentially contributing to higher cardiovascular risk. Chronic inflammation, which is more sustained in SPMS and PPMS, can lead to cardiovascular issues. Patients with progressive forms of MS might have more limitations in physical activity, leading to a sedentary lifestyle and higher cardiovascular risk. Additionally, comorbidities such as hypertension or diabetes might be more prevalent in patients with progressive MS, further elevating their cardiovascular risk. Lastly, the effects of long-term treatments for MS could also play a role in increasing cardiovascular risk in these patients.
Given the wide range of years of disease progression within the study group, we categorized patients into two groups: those with less than 10 years of disease progression and those with more than 10 years. To ensure accurate statistical analysis, we excluded patients under 40 years of age, as their SCORE is 0%. We then tested the influence of current age using a t-test and there was no significant difference in terms of age between the groups that could affect cardiovascular risk (p > 0.05). Consequently, we proceeded with the statistical analysis of the estimated cardiovascular risk for the two categories. The results indicated, with statistical significance (p < 0.05), that individuals with a disease duration longer than 10 years had a higher cardiovascular risk.
4. Discussion
The significant predominance of females among individuals with MS is a notable aspect of the disease This gender disparity has significant implications, particularly in terms of cardiovascular risk. Women are subject to hormonal fluctuations due to menstruation, pregnancy, menopause, hormone replacement therapies, and pregnancy-related pathologies, all of which can elevate the risk of major cardiovascular diseases [32].
The elevated number of non-smokers and ex-smokers compared to current smokers among the study participants may be attributed to the strong recommendation to cease smoking upon diagnosis of MS. However, these figures are not significantly different from those observed in the general population of Romania according to the data from Eurostat in 2019[33].
When comparing our findings with those of a study that used the Depression, Anxiety, and Stress Scale-21 (DASS-21) to assess MS patients, the results show similar levels of stress and anxiety. However, our study group exhibited lower levels of depression [34]. A possible explanation for this discrepancy could be the patients' perception of quality of life. According to a Eurostat report published in October 2023, Romania ranks third in Europe for quality of life, with a score of 7.7[35].
The BMI values observed align with literature data, showing that the average BMI is lower in MS patients compared to the general population of the same age and sex. This difference can be attributed to muscle atrophy and the increased metabolic rate commonly seen in individuals with MS [16,36,37].
Notably, there appears to be a higher proportion of MS patients who have not yet been diagnosed with hypertension and diabetes mellitus [17,18,19]. The prevalence of elevated LDL-C appears to be lower among MS patients compared to the general population [38].The literature shows wide variability in the prevalence of low HDL-cholesterol values, making it difficult to determine whether the results obtained are consistent with existing data. Due to all patients in our study being part of the national multiple sclerosis treatment program with disease-modifying therapies (DMTs), we were unable to analyze the impact of DMTs on the lipid profiles of the patients. The existing literature on this topic is limited. However, one study evaluating real-life data from six different DMTs (Interferon-beta, Glatiramer acetate, Teriflunomide, Dimethyl fumarate, Fingolimod and Ocrelizumab) concluded that these therapies had no effect on serum lipid levels [39].
Patients with MS show a blood triglyceride concentration pattern similar to that of the general population, with a sharp increase observed in females during the postmenopausal period [32], highlighting the need for careful monitoring and assessment.
The elevated ESR levels observed in patients with secondary progressive MS may suggest the presence of inflammatory "flare-ups" and increased disease activity, as supported by the literature [40]. To draw more definitive conclusions, a comprehensive study that includes additional inflammatory markers (such as C-reactive protein and homocysteine), along with MRI imaging to confirm disease activity and assessments to rule out other potential causes of inflammation and elevated ESR (including infections and secondary effects of medication), is warranted.
The SCORE algorithm was updated in 2021 to the SCORE2 version which calculates the risk of mortality as well as morbidity and contains 4 population categories: low, moderate, high and very high, and the total cholesterol values were replaced by non-HDL cholesterol values. In the new algorithm, Romania moves from the category of high-risk countries to that of very high risk, with a value approximately double the estimated risk for each person, and the difference between the risk value for women and men decreases considerably [27]. Since SCORE2 was published in October 2021 and the studies conducted using this new score are very few, even more so if we refer only to those done in Romania, we decided to use the old algorithm in this study, in order to compare the results with the data from the literature. Nonetheless, the exponential increase in cardiovascular risk for each patient remains a significant concern, underscoring the need for a thorough understanding of its severity.
Approximately 6 out of 100 patients with MS are at risk of developing cardiovascular disease in the next 10 years, double comparing to the general population in Romania.
The higher cardiovascular risk among urban patients may be due to the fact that the majority of young patients under 40 years of age live predominantly in urban areas. The combination of hypertriglyceridemia and hypercholesterolemia elevates the risk of cardiovascular disease more than a single lipid disorder, potentially by exacerbating other cardiovascular risk factors like high blood pressure.
Comparing the results about the characteristics of MS and the cardiovascular risk, the results are consistent with those obtained in a study that calculated cardiovascular risk using the Framingham score in patients with MS [41].
5. Conclusions
Patients with multiple sclerosis have a higher cardiovascular risk compared to the general population. The prevalence of type II diabetes mellitus among these patients is similar to that of the general population in Romania. Elevated cholesterol levels in MS patients are associated with a higher degree of disability. The pattern of blood triglyceride concentration evolution in these patients mirrors that of the general population. Additionally, patients with MS and a higher degree of disability face an increased cardiovascular risk. Those with secondary-progressive MS also exhibit a higher cardiovascular risk. A prolonged duration of MS (> 10 years) correlates with an elevated cardiovascular risk. The relationship between cardiovascular risk and the progression of MS is complex and necessitates extensive research. However, the primary focus of this study is to emphasize the importance of early identification and mitigation of cardiovascular risk factors, alongside advocating for a multidisciplinary therapeutic approach in managing patients with MS.
Author Contributions
F.C.P. and E.A.A.; methodology, F.C.P.; software, A.A.B.; validation, F.C.P., E.A.A., and A.P.; formal analysis, M.M.Ț. and C.A.S.; investigation, E.A.A., A.P., and D.A.; resources, S.B. and A.E.M.; data curation, A.A.B. and O.V.; writing—original draft preparation, A.P. and E.A.A.; writing—review and editing, F.C.P. and S.B.; visualization, M.M.Ț.; supervision, A.E.M.; project administration, E.A.A.; funding acquisition, A.E.M. and O.V.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Central Military Emergency University Hospital (approval number: CR 6344, obtained on July 1st 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- WHO Endorses Landmark Public Health Decisions on Essential Medicines for Multiple Sclerosis Available online: https://www.who.int/news/item/26-07-2023-who-endorses-landmark-public-health-decisions-on-essential-medicines-for-multiple-sclerosis.
- Dobson, R.; Giovannoni, G. Multiple Sclerosis - a Review. Eur J Neurol 2019, 26, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Garg, N.; Smith, T.W. An Update on Immunopathogenesis, Diagnosis, and Treatment of Multiple Sclerosis. Brain Behav 2015, 5. [Google Scholar] [CrossRef]
- Tintore, M.; Otero-Romero, S.; Río, J.; Arrambide, G.; Pujal, B.; Tur, C.; Galán, I.; Comabella, M.; Nos, C.; Arévalo, M.J.; et al. Contribution of the Symptomatic Lesion in Establishing MS Diagnosis and Prognosis. Neurology 2016, 87, 1368–1374. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of Multiple Sclerosis: 2017 Revisions of the McDonald Criteria. Lancet Neurol 2018, 17, 162–173. [Google Scholar] [CrossRef]
- McGinley, M.P.; Cohen, J.A. Evolution of the Diagnostic Criteria in Multiple Sclerosis. In Neuroimmunology; Piquet, A.L., Alvarez, E., Eds.; Springer International Publishing: Cham, 2021; pp. 75–87. ISBN 978-3-030-61882-7. [Google Scholar]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J Am Coll Cardiol 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- What Is the Socioeconomic Burden of Cardiovascular Disease? Available online: https://www.wifor.com/en/socioeconomic-burden-of-cardiovascular-disease/ (accessed on 21 December 2024).
- HISTORY OF INTERFERON TREATMENTS IN MULTIPLE SCLEROSIS – 60 YEARS OF PROGRESS – Farmacia Journal. Available online: https://farmaciajournal.com/issue-articles/history-of-interferon-treatments-in-multiple-sclerosis-60-years-of-progress/ (accessed on 22 December 2024).
- Cree, B.A.C.; Oksenberg, J.R.; Hauser, S.L. Multiple Sclerosis: Two Decades of Progress. Lancet Neurol 2022, 21, 211–214. [Google Scholar] [CrossRef]
- Zadeh, A.R.; Askari, M.; Azadani, N.N.; Ataei, A.; Ghadimi, K.; Tavoosi, N.; Falahatian, M. Mechanism and Adverse Effects of Multiple Sclerosis Drugs: A Review Article. Part 1. Int J Physiol Pathophysiol Pharmacol 2019, 11, 95. [Google Scholar]
- Plesa, C.F.; Chitimus, D.M.; Sirbu, C.A.; Țânțu, M.M.; Ghinescu, M.C.; Anghel, D.; Ionita-Radu, F. Thrombotic Thrombocytopenic Purpura in Interferon Beta-1a-Treated Patient Diagnosed with Relapsing-Remitting Multiple Sclerosis: A Case Report. Life 2022, Vol. 12, Page 80 2022, 12, 80. [Google Scholar] [CrossRef]
- Jalkh, G.; Abi Nahed, R.; Macaron, G.; Rensel, M. Safety of Newer Disease Modifying Therapies in Multiple Sclerosis. Vaccines (Basel) 2020, 9, 1–30. [Google Scholar] [CrossRef]
- Palladino, R.; Marrie, R.A.; Majeed, A.; Chataway, J. Evaluating the Risk of Macrovascular Events and Mortality Among People With Multiple Sclerosis in England. JAMA Neurol 2020, 77, 820. [Google Scholar] [CrossRef]
- Marrie, R.A.; Reider, N.; Cohen, J.; Stuve, O.; Trojano, M.; Cutter, G.; Reingold, S.; Sorensen, P.S. A Systematic Review of the Incidence and Prevalence of Cardiac, Cerebrovascular, and Peripheral Vascular Disease in Multiple Sclerosis. Multiple Sclerosis Journal 2015, 21, 318–331. [Google Scholar] [CrossRef]
- Pinhas-Hamiel, O.; Livne, M.; Harari, G.; Achiron, A. Prevalence of Overweight, Obesity and Metabolic Syndrome Components in Multiple Sclerosis Patients with Significant Disability. Eur J Neurol 2015, 22, 1275–1279. [Google Scholar] [CrossRef] [PubMed]
- Marrie, R.A.; Horwitz, R.I. Emerging Effects of Comorbidities on Multiple Sclerosis. Lancet Neurol 2010, 9, 820–828. [Google Scholar] [CrossRef] [PubMed]
- Maric, G.; Pekmezovic, T.; Tamas, O.; Veselinovic, N.; Jovanovic, A.; Lalic, K.; Mesaros, S.; Drulovic, J. Impact of Comorbidities on the Disability Progression in Multiple Sclerosis. Acta Neurol Scand 2022, 145, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Magyari, M.; Sorensen, P.S. Comorbidity in Multiple Sclerosis. Front Neurol 2020, 11, 851. [Google Scholar] [CrossRef]
- Horton, M.; Rudick, R.A.; Hara-Cleaver, C.; Marrie, R.A. Validation of a Self-Report Comorbidity Questionnaire for Multiple Sclerosis. Neuroepidemiology 2010, 35, 83–90. [Google Scholar] [CrossRef]
- Jadidi, E.; Mohammadi, M.; Moradi, T. High Risk of Cardiovascular Diseases after Diagnosis of Multiple Sclerosis. Multiple Sclerosis Journal 2013, 19, 1336–1340. [Google Scholar] [CrossRef]
- Yang, F.; Hu, T.; He, K.; Ying, J.; Cui, H. Multiple Sclerosis and the Risk of Cardiovascular Diseases: A Mendelian Randomization Study. Front Immunol 2022, 13. [Google Scholar] [CrossRef]
- Rapp, D.; Michels, S.; Schöpe, J.; Schwingshackl, L.; Tumani, H.; Senel, M. Associations between Multiple Sclerosis and Incidence of Heart Diseases: Systematic Review and Meta-Analysis of Observational Studies. Mult Scler Relat Disord 2021, 56. [Google Scholar] [CrossRef]
- Albuquerque, L. da S.; Damasceno, N.R.T.; Maia, F.N.; Carvalho, B.M. de; Maia, C.S.C.; D’Almeida, J.A.C.; Melo, M.L.P. de Cardiovascular Risk Estimated in Individuals with Multiple Sclerosis: A Case-Control Study. Mult Scler Relat Disord 2021, 54. [Google Scholar] [CrossRef]
- Jakimovski, D.; Topolski, M.; Genovese, A.V.; Weinstock - Guttman, B.; Zivadinov, R. Vascular Aspects of Multiple Sclerosis: Emphasis on Perfusion and Cardiovascular Comorbidities. Expert Rev Neurother 2019, 19, 445–458. [Google Scholar] [CrossRef] [PubMed]
- Diebold, M.; Derfuss, T. Immunological Treatment of Multiple Sclerosis. Semin Hematol 2016, 53, S54–S57. [Google Scholar] [CrossRef]
- Csenteri, O.; Jancsó, Z.; Szöllösi, G.J.; Andréka, P.; Vajer, P. Differences of Cardiovascular Risk Assessment in Clinical Practice Using SCORE and SCORE2. Open Heart 2022, 9, e002087. [Google Scholar] [CrossRef]
- Magyari, M. Gender Differences in Multiple Sclerosis Epidemiology and Treatment Response. Dan Med J 2016, 63, B5212. [Google Scholar]
- Keytsman, C.; Eijnde, B.O.; Hansen, D.; Verboven, K.; Wens, I. Elevated Cardiovascular Risk Factors in Multiple Sclerosis. Mult Scler Relat Disord 2017, 17, 220–223. [Google Scholar] [CrossRef]
- Dorobantu, M.; Tautu, O.-F.; Dimulescu, D.; Sinescu, C.; Gusbeth-Tatomir, P.; Arsenescu-Georgescu, C.; Mitu, F.; Lighezan, D.; Pop, C.; Babes, K.; et al. Perspectives on Hypertension’s Prevalence, Treatment and Control in a High Cardiovascular Risk East European Country. J Hypertens 2018, 36, 690–700. [Google Scholar] [CrossRef]
- Hâncu, A.; Roman, G.; Bala, C.; Timar, B.; Roman, D.; Păun, D.; Mechanick, J.I. Diabetes Care in Romania: A Lesson on the Central Role of Lifestyle Medicine. Am J Lifestyle Med 2023, 15598276231195572. [Google Scholar] [CrossRef]
- Norris, C.M.; Mullen, K.-A.; Foulds, H.J.A.; Jaffer, S.; Nerenberg, K.; Gulati, M.; Parast, N.; Tegg, N.; Gonsalves, C.A.; Grewal, J.; et al. CANADIAN WOMEN’S HEART HEALTH ALLIANCE ATLAS: EPIDEMIOLOGY, DIAGNOSIS, AND MANAGEMENT OF CARDIOVASCULAR DISEASE IN WOMEN Chapter 7: Sex, Gender, and the Social Determinants of Health. CJC Open 2023, S2589790X23002111. [Google Scholar] [CrossRef]
- Statistics | Eurostat. Available online: https://ec.europa.eu/eurostat/databrowser/view/hlth_ehis_sk1c/bookmark/table?lang=en&bookmarkId=440194bd-fc13-44d8-9c4c-bec758227f5e (accessed on 16 September 2024).
- Karimi, S.; Andayeshgar, B.; Khatony, A. Prevalence of Anxiety, Depression, and Stress in Patients with Multiple Sclerosis in Kermanshah-Iran: A Cross-Sectional Study. BMC Psychiatry 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Statistics | Eurostat. Available online: https://ec.europa.eu/eurostat/databrowser/view/ilc_pw01/default/table?lang=en (accessed on 16 September 2024).
- Aune, D.; Sen, A.; Prasad, M.; Norat, T.; Janszky, I.; Tonstad, S.; Romundstad, P.; Vatten, L.J. BMI and All Cause Mortality: Systematic Review and Non-Linear Dose-Response Meta-Analysis of 230 Cohort Studies with 3.74 Million Deaths among 30.3 Million Participants. BMJ 2016, i2156. [Google Scholar] [CrossRef]
- Dardiotis, E.; Tsouris, Z.; Aslanidou, P.; Aloizou, A.-M.; Sokratous, M.; Provatas, A.; Siokas, V.; Deretzi, G.; Hadjigeorgiou, G.M. Body Mass Index in Patients with Multiple Sclerosis: A Meta-Analysis. Neurol Res 2019, 41, 836–846. [Google Scholar] [CrossRef] [PubMed]
- Akbartabar Toori, M.; Kiani, F.; Sayehmiri, F.; Sayehmiri, K.; Mohsenzadeh, Y.; Ostovar, R.; Angha, P.; Mohsenzadeh, Y. Prevalence of Hypercholesterolemia, High LDL, and Low HDL in Iran: A Systematic Review and Meta-Analysis. Iran J Med Sci 2018, 43, 449–465. [Google Scholar] [CrossRef] [PubMed]
- Koca, N.; Seferoğlu, M. Effects of Disease-Modifying Therapies on Lipid Parameters in Patients with Multiple Sclerosis. Mult Scler Relat Disord 2023, 77, 104876. [Google Scholar] [CrossRef] [PubMed]
- Nazeri, M.; Bazrafshan, H.; Abolhasani Foroughi, A. Serum Inflammatory Markers in Patients with Multiple Sclerosis and Their Association with Clinical Manifestations and MRI Findings. Acta Neurol Belg 2022, 122, 1187–1193. [Google Scholar] [CrossRef]
- Petruzzo, M.; Reia, A.; Maniscalco, G.T.; Luiso, F.; Lanzillo, R.; Russo, C.V.; Carotenuto, A.; Allegorico, L.; Palladino, R.; Brescia Morra, V.; et al. The Framingham Cardiovascular Risk Score and 5-year Progression of Multiple Sclerosis. Eur J Neurol 2021, 28, 893–900. [Google Scholar] [CrossRef]
Figure 1.
Possible etiologies and risk factors that contribute to the development of multiple sclerosis.
Figure 1.
Possible etiologies and risk factors that contribute to the development of multiple sclerosis.
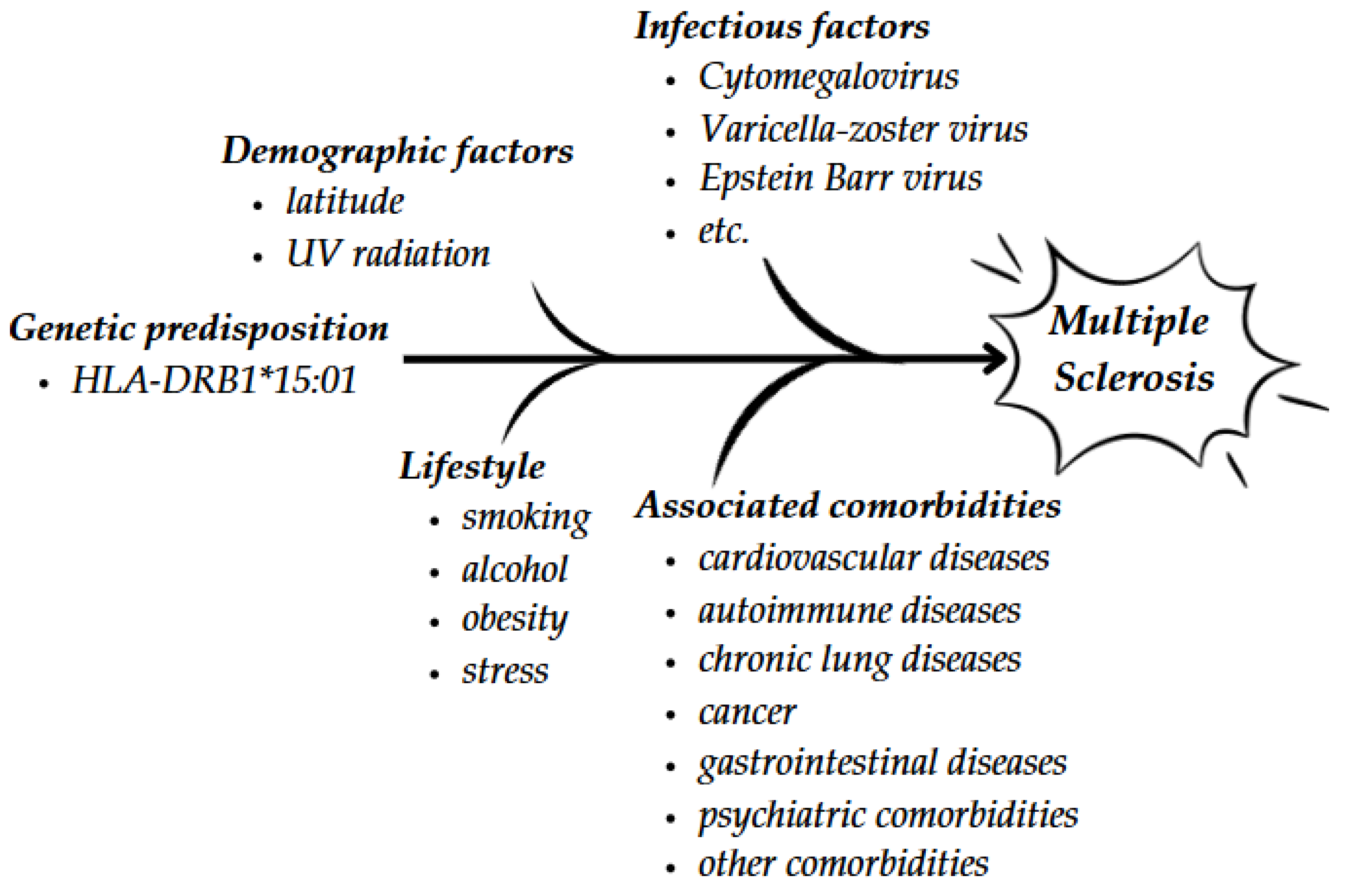
Figure 2.
(a) Level of stress; (b) Frequency of anxiety episodes (c) Frequency of depression episodes.
Figure 2.
(a) Level of stress; (b) Frequency of anxiety episodes (c) Frequency of depression episodes.
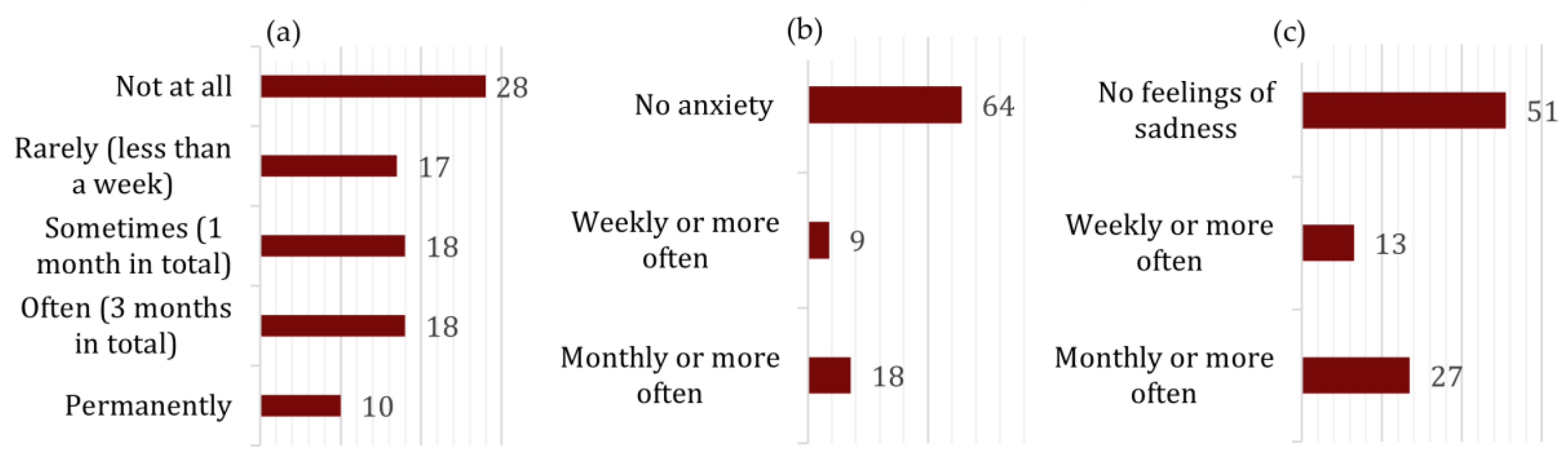
Figure 3.
Medical history.*AMI= acute myocardial infarction.
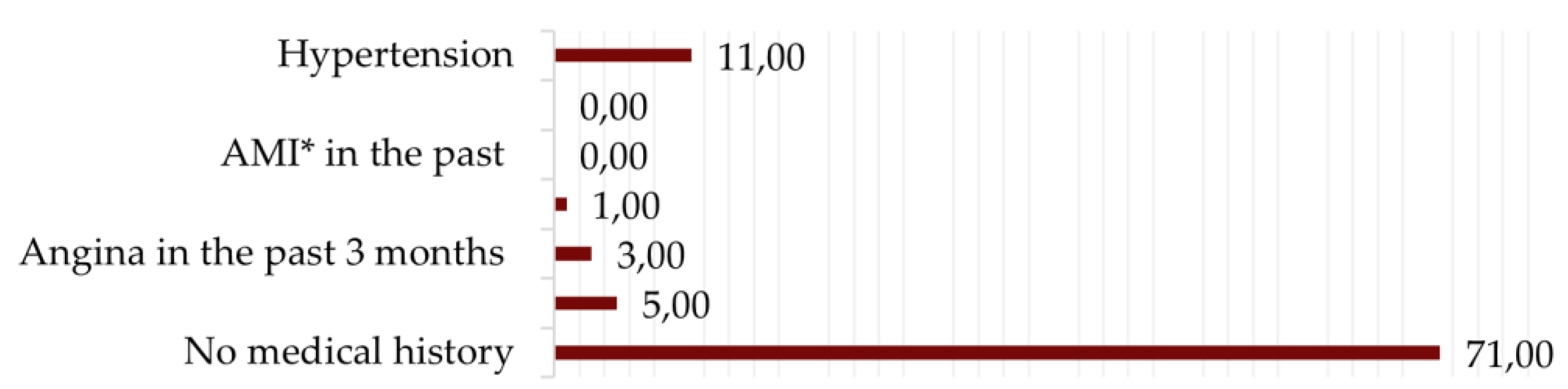
Figure 4.
Mean systolic and diastolic blood pressure stratified by age group.
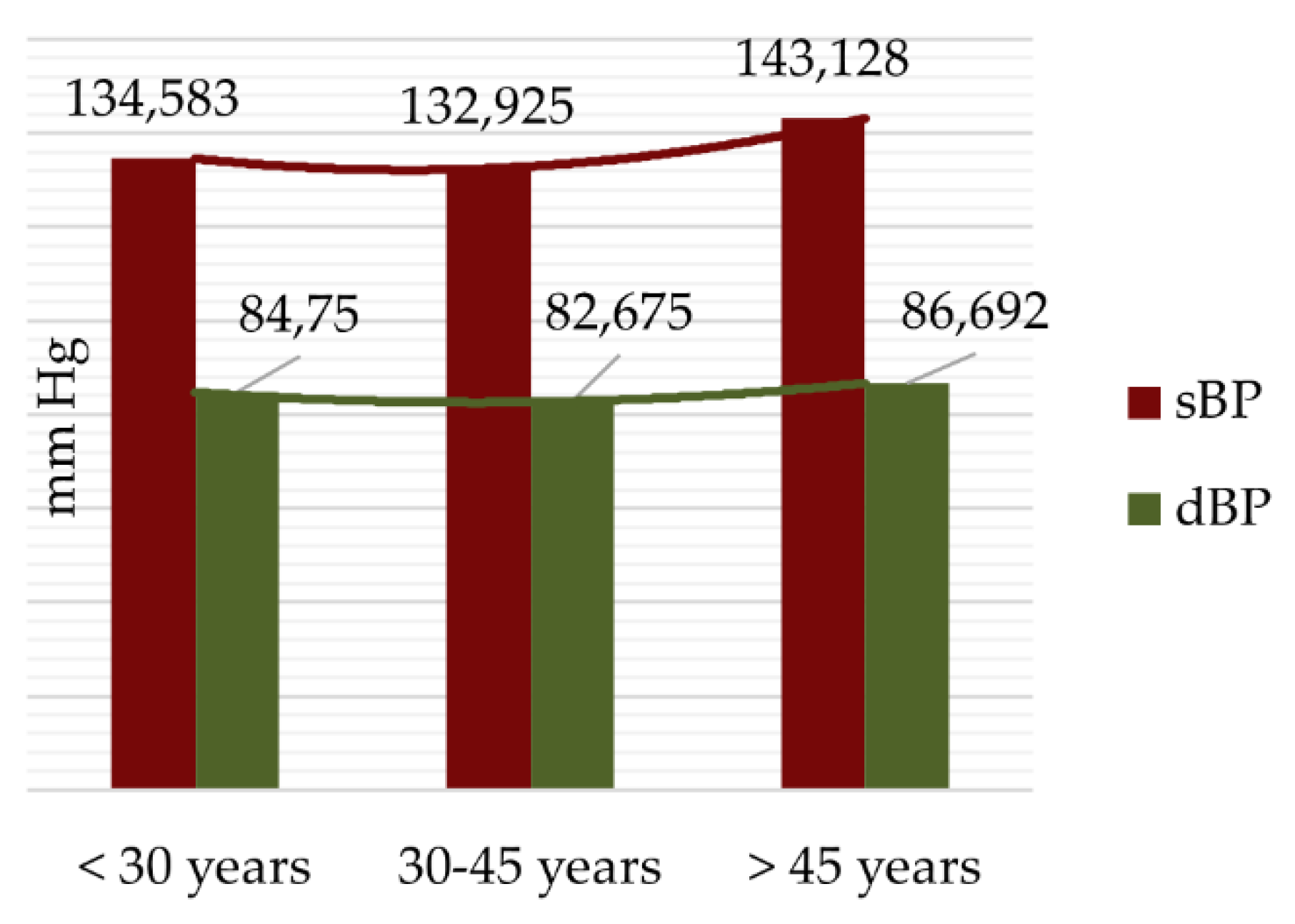
Figure 5.
Age- and sex-specific triglyceride curves.
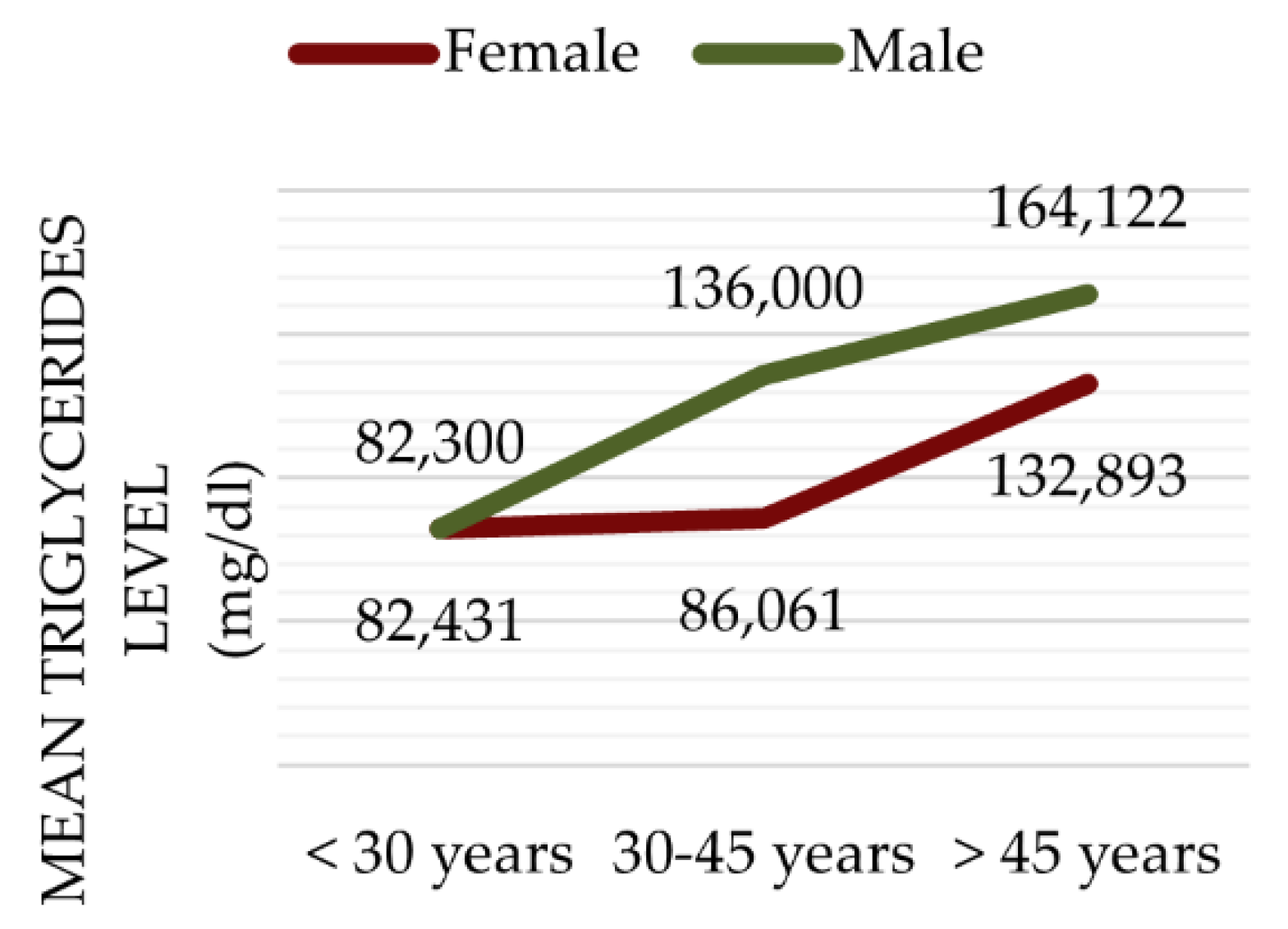

Table 1.
Inclusion and exclusion criteria for defining study population. * As the prevalence of cardiovascular risk factors may be increased in elderly patients.
Table 1.
Inclusion and exclusion criteria for defining study population. * As the prevalence of cardiovascular risk factors may be increased in elderly patients.
| Inclusion criteria |
| Patients diagnosed with multiple sclerosis |
| Patients under treatment through the National Health Program for MS between September 2022 and September 2023 |
| Patients whose paraclinical investigations are in the hospital record |
| Exclusion criteria |
| Patients who had serious concomitant diseases (cancer, hepatitis, etc.) or treatments (e.g., chemotherapy) that could interfere with cardiovascular risk (3) |
| Patients who refused to answer the questionnaire (2) |
| Women aged ≥ 60 years and men aged ≥ 55 years* (11) |
| Patients with Clinically isolated syndrome (CIS) (1) |
Table 2.
The distribution of patients according to the type of MS.
| MS-type | Number (percentage) of patients | Average years of disease progression |
|---|---|---|
| Relapsing-remitting MS | 77 (84.62%) | 8.72 |
| Secondary-progressive MS | 10 (10.99%) | 13.44 |
| Primary-progressive MS | 4 (4.40%) | 4.08 |
Table 3.
Average age, EDSS and BMI for different groups according to their level of activity.
| Level of Physical Activity | Average Age (years) | Average EDSS Score | Average BMI (kg/m²) |
|---|---|---|---|
| Sedentary (minimal activity, mostly sitting/watching TV) | 45.23 | 4.9545 | 21.5350 |
| Light Activity (slow walking, household chores) | 46.22 | 2.6300 | 24.9327 |
| Moderate Activity (walking more than 30 minutes daily, cycling, dancing) | 37.75 | 1.5625 | 23.1498 |
| Intense Activity (regular sports: jogging, cycling, yoga, etc.) | 33.89 | 1.5000 | 22.6430 |
Table 4.
The mean value of selected medical analyses from patients' observation sheets and.
| Blood Test | Mean | Standard deviation | Biological reference intervals |
|---|---|---|---|
|
Glycemia (mg/dl) |
97,5948 | 36,5822 | 74,00 - 100,00 |
|
Total Cholesterol (mg/dl) |
198,4817 | 38,5618 | <200 - normal 200 - 239 – moderate risk >240 – high risk |
|
LDL-cholesterol (mg/dl) |
120,8003 | 36,6784 | <100 -normal 100 - 129 – low risk 130 - 159 – moderate risk >160 – high risk |
|
HDL-cholesterol (mg/dl) |
56,6636 | 14,9341 | 10 - 40 (male)/ 50 (female) high risk 41/51 - 90 normal |
|
ESR (Erythrocytesedimentation rate) (mm/1h) |
13,4407 | 10,9580 | 0,00 - 20,00 |
|
Creatinine (mg/dl) |
0,7369 | 0,1711 | 0,51-0,95 |
|
Urea (mg/dl) |
29,3637 | 8,5922 | 17,00-43,00 |
Table 5.
Mean SCORE according to the association of hypercholesterolemia and hypertriglyceridemia among patients.
Table 5.
Mean SCORE according to the association of hypercholesterolemia and hypertriglyceridemia among patients.
| Mean SCORE (%) | ||
| Cholesterol <200 mg/dl | Cholesterol ≥ 200 mg/dl | |
| Triglycerides <150 mg/dl | 5,4523 | 5,62068 |
| Triglycerides ≥150 mg/dl | 4,1111 | 10,3636 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



