Submitted:
03 January 2025
Posted:
06 January 2025
You are already at the latest version
Abstract
(1) Background: Wearable sensors have emerged as a promising technology in the management of Parkinson's Disease (PD). These sensors can provide continuous and real-time monitoring of various motor and non-motor symptoms of PD, allowing for early detection and intervention. In this abstract, i review current research on the application of wearable sensors in PD, focusing on gait, tremor, bradykinesia, and dyskinesia monitoring. (2) Methods: This is a literature research spanning the 2000-2024 period including the following keywords: “wearable sensors”; “Parkinson’s Disease”; “Inertial sensors” , accelerometers’’, ‘’gyroscopes’’, ‘’magnetometers” , “Smartphones” , “Smart homes”. (3) Results: Despite favorable outcomes from the early development of inertial sensors like gyroscopes and accelerometers in smartphones, application of DB is still restricted because there are no standards, harmonization, or consensus for both clinical and analytical validation. As a result, several clinical trials have been created to compare the effectiveness of DB with conventional evaluation methods in order to track the course of the disease and enhance quality of life and results. (4) Conclusions: Wearable sensors hold great promise in the management of PD and are likely to play a significant role in future healthcare systems.
Keywords:
wearable sensors
; Parkinson’s disease
; inertial sensors
; smartphones
; smart homes
1. Introduction
Parkinson's Disease (PD) is a complex neurodegenerative disorder that presents with a wide range of motor (tremors, bradykinesia, postural instability) and non-motor symptoms, including autonomic disorders, behavioral and cognitive deficits [1]. In late stage, levodopa-related motor complications include: a) off effects, where the duration of the drug's beneficial effect decreases with each dose; b) delayed ON/noON fluctuations, where the time between taking levodopa and the clinical effect is either delayed or nonexistent; and c) random ON-OFF fluctuations [2]. Traditional methods of assessing PD symptoms rely on subjective clinical evaluations (e.g. diaries, questionnaires), which can be prone to bias and variability [3,4].
However, the emergence of wearable sensor technology has revolutionized the monitoring and management of PD by enabling objective, continuous, and remote assessment of key motor symptoms. Wearable sensors are small, lightweight devices that can be worn on the body to capture various physiological parameters, such as movement, tremor, gait, balance, cognitive and sleep patterns [5,6]. These sensors utilize a range of supporting networking technologies, including accelerometers, gyroscopes, magnetometers, and electromyography, to collect data on motor and non-motor symptoms in PD patients [7]. While some methods have suggested using many sensors on various body parts, more contemporary methods often utilize sensors on the foot, wrist, fingers, cellphones with wrist adapters, or devices that resemble watches [7,8,9,10,11]. Additionally, these methods have been combined with threshold approaches, automatic classification algorithms, and deep learning techniques [7-11} to offer inexpensive and non-invasive remote surveillance systems. The data collected by wearable sensors can be analyzed in real-time or stored for later review, providing valuable insights into disease progression, treatment efficacy, and quality of life through developments in machine learning [7,8] (Figure 1.).
Previous reviews focused on wearable technologies [9] such as smartphone apps [10], inertial sensors using maschine learning models to predict motor / non- motor symptoms of PD [7,11]. This narrative review aims to provide a more comprehensive overview of the current applications, benefits, challenges, and future directions of wearable sensors in the management of PD.
2. Materials and Methods
I reviewed articles published during the 2000–2024 period, focusing on wearable sensors in PD patients. I searched PUBMED, SCOPUS and EMBASE from 2000–2024 using the following terms: “Parkinson’s disease”, “Wearable sensors”, ‘’PDMonitor®’’, ‘’PKG®system’’, ‘’STAT-ONTM’’, ‘’ KinesiaONETM ‘’, ‘’FeetMe® Monitor’’, ‘’DynaPort7TM’’, ‘’Mobility Lab™’’, ‘’accelerometers’’, ‘’gyroscopes’’, ‘’magnetometers”, “Smartphones”, “Smart homes’’ using Boolean operators. Including criteria were original research papers, reviews, and meta-analyses that have been published in peer-reviewed publications in English language. The snowballing procedure was carried out to screen the references of each selected article for potential extra papers to cover the current key evidence following by a full-text evaluation of pertinent research. For the narrative synthesis, my initial categorization was based on the benefits of wearable sensors in the management of PD, followed by a discussion of limitations and potential future directions.
3. Results
3.1. Wearable, Inertial Sensors and FDA-Approved Devices
Small electrical devices called inertial sensors, sometimes referred to as motion sensors, monitor acceleration, angular velocity, and sometimes the intensity of magnetic fields. An object's orientation and motion in three dimensions are determined using these measurements. Accelerometers, gyroscopes, and magnetometers are examples of inertial sensors that are frequently used to record a variety of motion-related data.Wearable motion sensors have shown promise in the everyday life monitoring of PD patients due to their compact size, low weight, and low energy requirements [12,13,14]. Table 1 summarizes research on wearable PD sensor.
By detecting unexpected fluctuations in acceleration, accelerometer sensors enable the monitoring of posture and movement. Gyroscopes, on the other hand, detect rotational movements and angular velocity. Magnetometers evaluate heading and orientation tracking by measuring orientation and recording alterations in the magnetic field. The wrist accounts for 18.2% of all accelerometer, gyroscope, and magnetometer attachments, with the lower leg (13.6%), waist (12.1%), upper leg (9.1%), and foot (6.1%) following in order of frequency [15]. When used together, these tools provide unbiased information on changes in posture and motor function. The most widely used sensors are a magnetometer, gyroscope, and tri-axial accelerometer. An inertial measurement unit (IMU), or three-dimensional construct with linear and angular velocity, is produced when they are integrated into a single device [16,17,18]. Small devices enable extended free walking outside labs for assessing PD motor symptoms, particularly due to the Hawthorne observation effect, which suggests that free-living activities with varying complexities and distractions may reduce attention.
Inertial sensors can differentiate PD from healthy controls based on movement patterns, enabling machine learning algorithms to identify specific features. They can also monitor PD progression, capture changes in movement patterns, and provide insights into the disease course [16,17,18,19,20,21,22,23,24]. Longitudinal data can inform treatment decisions and assess efficacy, such as tremor severity and gait disturbances.
Inertial sensors have been used in observational studies to advance digital progression biomarkers for PD such as the Personalized Parkinson Project [25], the Cincinnati Cohort Biomarker Program (CCBP) [26], the Wearable Assessment in The Clinic and at Home in PD (WATCH-PD) [27,28], the Oxford Parkinson Disease Centre (OPDC) discovery cohort [29] and the ALAMEDA study [30]. These devices objectively measure the efficacy of new interventions by capturing changes in motor symptoms over trials. By documenting variations in motor symptoms during the trial, these tools are used to objectively assess the effectiveness of novel therapies, such as medicine, physical therapy, and deep brain stimulation. Inertial sensors can better assess the efficacy of novel treatments and provide insightful information about reactions to therapy by delivering continual and quantitative data. Inertial sensors are frequently employed in clinical trials to evaluate main objectives pertaining to the degree of motor symptom severity and functional improvement. For instance, gyroscopes record improvements in gait metrics, whereas accelerometers detect changes in the intensity of tremor [25,26,27,28]. Experts can ascertain whether the therapy significantly affects motor symptoms and functional capacities by examining this data. Inertial sensors may offer secondary outcome measurements in addition to primary endpoints. These gadgets can provide a thorough understanding of a person's motor function and general mobility by recording information on movement pattern, activity level, and postural change. The effect of the treatment on routine tasks and quality of life—two crucial secondary goals in PD research—can be evaluated using this data. With everything taken together, inertial sensors are essential to the planning and implementation of PD clinical trials because they offer precise and quantitative assessments of functional skills and motor symptoms [25,26,27,28,29,30]. The accuracy and dependability of trial results could be increased by this technique, which would eventually result in the creation of more potent therapies.
NICE recommends wearable devices like PDMonitor, PKG, STAT-ON, Kinesia360, and KinesiaU for remote monitoring of PD to inform treatment, as they belong to Class I or IIa medical devices [31] (Table 2).
The chronology of the above FDA-cleared wearable devices for PD is shown in Figure 2.
The PDMonitor® is a Class IIa medical device designed to monitor patients with PD. It consists of five IMU sensing devices placed on wrists, shins, and waist (1) a SmartBox used to collect, process and upload data to the Cloud; (2) Five sensing/monitoring devices each with internal data storage (up to 7 days) that can transfer data when docked into the SmartBox; and (3) accessories for attaching the devices to the patient. The system was used to assess 65 PD patients in-hospital and at home for at least 7 hours/day [32]. The device calculated the probability of the patient being OFF based on gait, tremor, FoG, and bradykinesia.
The PKG®system, first FDA-cleared in 2014, is a medical device for PD patients. It captures motor symptoms, monitors medication administration, detects device removal, and monitors movement during sleep. The watch, attached to the wrist, collects data 6-10 days and has a rechargeable battery and accelerometer. The data is translated into bradykinesia and dyskinesia scores, which generate a graphical report. The device also measures motor complications, including fluctuations and dyskinesia scores. The device has shown high sensitivity and specificity in identifying tremors and distinguishing between fluctuators and non-fluctuators vs the gold-standards, ie, the AIMS score (dyskinesia) and UPDRS-III (bradykinesia) [33,34].
The STAT-ONTM is a wearable sensor that uses real-time machine learning algorithms to measure inertial signals. It weighs 86g and consists of two ultralow triaxial nano-accelerometers and two microcontrollers using Bluetooth Low Energy wireless technology. The sensor records gait, step length, FoG, falls, and trunk or neck dyskinesia. Despite its high sensitivity and specificity, it has been compared to patient self-reporting. The device has been successful in identifying trunk dyskinesia, FoG, and falls, with high sensitivity>93% and specificity75–98%[35]. The sensor is user-friendly and allows for input of events like medication use.
The KinesiaONETM is a Class I medical device that evaluates motor signs of PD using an iPad mini loaded with KinesiaONE software, an electronic diary, a wearable sensor, and a charge pad [33]. The mobile application uses TETRAS and UPDRS to help users through activities, and the sensor captures angular velocity and linear acceleration. Severity scores are determined by algorithms when the data is uploaded to a secure cloud repository. Two wireless motion sensors are used by the Kinesia360TM gadget to measure body position, steps taken throughout routine tasks, bradykinesia, dyskinesia, and tremor. Numerous investigations have demonstrated the device's dependability, with good sensitivity and specificity [36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53].
The most recent iteration of the DynaPort Hybrid technology, the DynaPort7TM, evaluates movement by integrating gyroscopes and acceleration sensors. Among other things, it gauges gait rhythmicity, steps, and walking patterns. The DynaPort7 has been proven to accurately identify misstep occurrences in a huge cohort of senior adults who do not have dementia or Parkinson's disease [54]. According to in-hospital evaluations, MDS-UPDRS part III was substantially correlated with seven mobility parameters [55]. The DynaPort gadget is acceptable and pleasant.
The FeetMe® Monitor is a real-time monitoring device that measures gait parameters and plantar pressure in the insole. The insole is equipped with a single Inertial Measurement Unit (IMU) that comprises a three-dimensional accelerometer and a three-dimensional gyroscope, enabling the detection of movement across six axes. It measures key gait cycle events and other factors stride length, stride duration, stance duration, swing duration, step duration, single support duration. The device is attached to an insole and has been proven effective in PD patients [56,57,58,59,60].
The Mobility Lab™ device uses wearable inertial sensors to monitor gait and balance in patients with PD. It includes six wireless sensors, software for user and patient guidance, and automated analysis. The system can detect subtle parkinsonian gait in early PD, evaluate parkinsonian gait/posture response to levodopa, and evaluate global gait and balance impairment. It also detects FoG episodes with high agreement with clinical raters, making it a valuable tool for gait and postural analysis in hospitalized patients[61].
3.2. Acoustic, Optical and Electrical and Electrochemical Sensors
Acoustic sensors can analyze speech patterns to assess vocal function and speech intelligibility in PD. They can also quantify gait parameters, such as step length and velocity. Wan et al. [62] used data from early disease patients' persistent vowel phonations to determine the severity of the disease. Deng et al. [63] showed in another investigation that PD may be effectively identified using voice, gait/rest, and tapping data. It's interesting to note that sustained vowels increased these data's discriminative power [64]. Clinicians can assess the effectiveness of speech treatment, monitor the course of the condition, and improve communication techniques in Parkinson's disease by tracking voice characteristics over time. Optical sensors can detect gait parameters and finger tapping in PD, enabling healthcare professionals to monitor treatment strategies and adjust accordingly. EMG sensors can assess muscle activity and movement patterns in PD, identifying muscle groups affected by the disease and guiding personalized rehabilitation strategies. Advances in electroencephalographic (EEG) technology have enabled the use of these sensors to monitor motor symptoms in PD, such as impulse control disorders and heart electrical activity. These technologies can help healthcare providers assess cardiac function and intervene early to mitigate adverse events.
An electrochemical biosensor is defined as "a self-contained integrated device able to provide specific quantitative or semi-quantitative analytical information, by using a biological recognition element (i.e., biochemical receptor), retained in direct spatial contact with an electrochemical transduction element" by the International Union of Pure and Applied Chemistry (IUPAC) [65]. One study, for instance, showed how to use a wearable electrochemical aptasensor for circulating blood α-synuclein oligomers, which has good sensitivity and specificity [66]. Rapid quantification and real-time monitoring are still challenges, despite the fact that the severity of motor symptoms is correlated with the plasma levodopa concentration [67]. These encouraging investigations unquestionably call for more investigation and advancement in along with possible use in different biofluids, including as urine, tears, and saliva.
3.3. Smartphones
Smartphones' extensive use, versatility, and multitasking make them potentially essential tools for identifying common symptoms of PD [68]. To investigate fine-motor deficits in early PD, for instance, Iakovakis et al. [69] employed natural smartphone touchscreen typing. A remote study with 253 individuals who contributed 252,000 typing sessions through the iPrognosis mobile app (Apple Computer Inc., Cupertino, CA, USA) and a dataset of 36,000 typing sessions from 39 subjects were used to validate this methodology. The findings were noteworthy and showed a close relationship with MDS-UPDRS part III. likewise, digital assessments and traditional clinical scales, such as the MDS-UPDRS, Symbol Digit Modalities Test, and Montreal Cognitive Assessment, demonstrated a good connection in the 12-month WATCH-PD multicenter longitudinal trial conducted with cellphones [26].
3.4. Smart Domotics
The word "domotics" is derived from the Latin "domus," implying "house," and "tics," which refers to computer science, robotics, and telematics. In addition to providing overall convenience, safety, and autonomy, domotics and smart homes can be a rich source of real-time data for ongoing monitoring and management in PD[70]. Combining wearable technology with stationary equipment, such as video and temperature, pressure, and movement sensors, may have benefits in thoroughly describing patterns of motion in the home [71]. Furthermore, smart mattresses, automated electrical equipment, and voice-activated lights provide real advantages to those with incapacitating illnesses [71]. Devices for virtual reality and leisure time could be employed in home physiotherapy to help people with PD with their balance and walk. For instance, a recent study conducted at home with a Nintendo® Wii console and wireless controller found that constant visual input made it easier to focus and execute movements [72].
4. Discussion
There are several key benefits of using wearable sensors in the management of PD. Firstly, wearable sensors enable continuous and objective monitoring of motor/non-motor symptoms, offering a more accurate assessment of disease progression compared to traditional episodic evaluations [7,8,9,10,11,12,13,15,18,30,32,33,52,53,55]. Ultimately, wearables are suitable for measuring autonomic status in real time, such as with ingestible respiratory function devices and cuffless blood pressure monitors. Inter-rater variability, symptom swings in and out of clinic, and sensitivity, infrequent rating scales and questionnaires are some of the shortcomings these solutions address with relation to discrepancies [9]. This real-time data can help clinicians personalize treatment plans, adjust medication dosages, and optimize therapeutic interventions to improve patient outcomes in and out of the clinical setting [25,28,73].One example of wearable technology is a non-invasive vibrotactile glove that uses implanted mechanical triggers to stimulate PD patients' fingertips and reduce motor symptoms including tremor and gait [73]. Additionally, wearable sensors can detect subtle changes in motor symptoms that may not be apparent during clinic visits, providing early indicators of disease progression or treatment response [39,40,42,43,45,46]. Physiology-driven inputs from wearable technology can be utilized to guide customized PD treatments like deep brain stimulation (DBS). More precisely, PD patients' shank velocity from IMUs can be utilized as a kinematic control variable for directing dynamic STN-DBS intervention in real-time to ameliorate freezingand gait dysfunction [74]. Furthermore, wearable sensors enable remote monitoring and telemedicine, allowing patients to receive care from the comfort of their homes and reducing the burden of frequent hospital visits [9].
Despite the numerous benefits of wearable sensors, there are also several challenges and limitations to consider. One of the main challenges is the integration of sensor data into clinical practice, as clinicians may not have the resources or expertise to interpret and utilize the complex data generated by wearable sensors. In addition, issues related to data privacy, security, and regulatory compliance must be carefully addressed to ensure the ethical use of sensor data in healthcare settings. Furthermore, wearable sensors may not be suitable for all PD patients, particularly those with cognitive impairments or mobility issues that prevent them from wearing or using the devices effectively. Notably, decreased score on these smartphone cognitive tests was associated with a lower score on the traditional cognitive assessment [9]. Finally, there is a need for standardization of sensor technologies, data analytics, and outcome measures to facilitate the adoption of wearable sensors in routine clinical practice.
The future of wearable sensors in the management of PD holds great promise for advancing precision medicine and personalized care. With the continued development of artificial intelligence and machine learning algorithms, wearable sensors have the potential to predict disease progression, optimize treatment regimens, and identify novel biomarkers for early diagnosis and intervention [75,76,77,78,79].Data enhancement and domain adjustment might enhance the generalizability of models in the healthy-to-PD transition scenario, and deep neural network models based on healthy data may be able to effectively identify actions carried out by PD patients [76].However, the recent PD deep learning models are inadequate against optimal dataset management problems, effective time series data analysis problems, real-time sensor handling problems, data regularization issues, and home-based PD monitoring solutions [76,77]. To resolve these issues, pant body sensor networks are the driving force behind the novel deep clustering model's autonomous health monitoring and analysis paradigm, which enables quick and efficient decision-making [78]. Additionally, the integration of wearable sensors with smart devices and mobile applications can enhance patient engagement, self-management, and adherence to treatment plans. A current study using IMUs combined with convolutional neural network modeling to measure FOG in PD individuals evaluated sensor sites that optimized patient adherence for individualized at-home motor symptom tracking [79]. Collaborative efforts among researchers, clinicians, industry partners, and regulatory agencies will be essential to drive innovation and adoption of wearable sensors in PD care.
5. Conclusions
Wearable sensors represent a powerful and innovative tool for monitoring and managing motor symptoms in PD. By providing objective, continuous, and remote assessment of key motor symptoms, wearable sensors offer numerous benefits for clinicians, patients, and caregivers. However, the widespread adoption of wearable sensors in clinical practice will require addressing challenges related to data interpretation, privacy, compliance, and standardization. Moving forward, collaborative efforts and interdisciplinary approaches will be essential to leverage the full potential of wearable sensors in improving outcomes and quality of life for PD patients. Future prospects for wearable sensors in PD include the development of more advanced and user-friendly devices, integration with other technologies such as artificial intelligence and telemedicine, and validation in large-scale clinical trials. These advancements could revolutionize the management of PD by enabling early diagnosis, personalized treatment plans, and improved quality of life.
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Bougea, A.; Angelopoulou, E. Non-Motor Disorders in Parkinson Disease and Other Parkinsonian Syndromes. Medicina (Kaunas). 2024, 11, 60–309. [Google Scholar] [CrossRef] [PubMed]
- Hauser, R.A.; McDermott, M.P.; Messing, S. Factors associated with the development of motor fluctuations and dyskinesias in Parkinson disease. Arch. Neurol. 2006, 63, 1756–1760. [Google Scholar] [CrossRef] [PubMed]
- Antonini, A.; Stoessl, A.J.; Kleinman, L.S.; et al. Developing consensus among movement disorder specialists on clinical indicators for identification and management of advanced Parkinson's disease: a multi-country Delphi-panel approach. Curr. Med. Res.Opin. 2018, 34, 2063–2073. [Google Scholar] [CrossRef] [PubMed]
- Löhle, M.; Bremer, A.; Gandor, F.; Timpka, J.; Odin, P.; Ebersbach, G.; Storch, A. Validation of the PD home diary for assessment of motor fluctuations in advanced Parkinson's disease. NPJ Parkinsons Dis. 2022, 2, 8–69. [Google Scholar] [CrossRef]
- Lukšys, D.; Jonaitis, G.; Griškevičius, J. Quantitative Analysis of Parkinsonian Tremor in a Clinical Setting Using Inertial Measurement Units. Parkinsons Dis. 2018, 2018, 1683831. [Google Scholar] [CrossRef]
- Alvarez, F.; Popa, M.; Solachidis, V.; Hernandez-Penaloza, G.; Belmonte-Hernandez, A.; Asteriadis, S.; Vretos, N.; Quintana, M.; Theodoridis, T.; Dotti, D.; Daras, P. Behavior analysis through multimodal sensing for care of Parkinson’s and Alzheimer’s patients. IEEE Multimed, 2018, 25, 14–25. [Google Scholar] [CrossRef]
- Giannakopoulou, K.M.; Roussaki, I.; Demestichas, K. Internet of Things Technologies and Machine Learning Methods for Parkinson's Disease Diagnosis, Monitoring and Management: A Systematic Review. Sensors 2022, 22, 1799. [Google Scholar] [CrossRef]
- Mahoney, D.F.; Purtilo, R.B.; Webbe, F.M.; Alwan, M.; Bharucha, A.J.; Adlam, T.D.; Jimison, H.B.; Turner, B.; Becker, S.A. In-home monitoring of persons with dementia: Ethical guidelines for technology research and development. Alzheimers Dement 2007, 3, 217–226. [Google Scholar] [CrossRef]
- Kehnemouyi, Y.M.; Coleman, T.P.; Tass, P.A. Emerging wearable technologies for multisystem monitoring and treatment of Parkinson’s disease: a narrative review. Front. Netw. Physiol. 2024, 4, 1354211. [Google Scholar] [CrossRef]
- Reichmann, H.; Klingelhoefer, L.; Bendig, J. The use of wearables for the diagnosis and treatment of Parkinson's disease. J Neural Transm (Vienna). 2023, 130, 783–791. [Google Scholar] [CrossRef]
- Franco, A.; Russo, M.; Amboni, M.; Ponsiglione, A.M.; Di Filippo, F.; Romano, M.; Amato, F.; Ricciardi, C. The Role of Deep Learning and Gait Analysis in Parkinson's Disease: A Systematic Review. Sensors (Basel). 2024, 24, 5957. [Google Scholar] [CrossRef] [PubMed]
- Ancillao, A.; Tedesco, S.; Barton, J.; O'Flynn, B. Indirect Measurement of Ground Reaction Forces and Moments by Means of Wearable Inertial Sensors: A Systematic Review. Sensors 2018, 18, 2564. [Google Scholar] [CrossRef] [PubMed]
- Mazzetta, I.; Zampogna, A.; Suppa, A.; Gumiero, A.; Pessione, M.; Irrera, F. Wearable Sensors System for an Improved Analysis of Freezing of Gait in Parkinson's Disease Using Electromyography and Inertial Signals. Sensors 2019, 19, 948. [Google Scholar] [CrossRef] [PubMed]
- Anand, V.; Bilal, E.; Ho, B. .; Rice, J.J. Towards motor evaluation of Parkinson's Disease Patients using wearable inertial sensors. AMIA Annu Symp Proc. 2021, 2020, 203–212. [Google Scholar]
- Klingelhoefer, L.; Rizos, A.; Sauerbier, A.; McGregor, S.; Martinez-Martin, P.; Reichmann, H.; Horne, M.; Chaudhuri, K.R. Night-time sleep in Parkinson’s disease – the potential use of Parkinson’s KinetiGraph: A prospective comparative study. Eur J Neurol 2016, 23, 1275–1288. [Google Scholar] [CrossRef]
- Howell, M.J.; Arneson, P.A.; Schenck, C.H. A novel therapy for REM sleep behavior disorder (RBD). J Clin Sleep Med 2011, 7, 639–644. [Google Scholar] [CrossRef]
- Riggare, S.; Scott, Duncan, T. ; Hvitfeldt, H.; H¨agglund, M. “You have to know why you’re doing this”: A mixed methods study of the benefits and burdens of self-tracking in Parkinson’s disease. BMC Med Inform Decis Mak 2019, 19, 1–16. [Google Scholar] [CrossRef]
- Maetzler, W.; Domingos, J.; Srulijes, K.; Ferreira, J.J.; Bloem, BR. Quantitative wearable sensors for objective assessment of Parkinson's disease. Mov Disord. 2013, 28, 1628–1637. [Google Scholar] [CrossRef]
- Godinho, C.; Domingos, J.; Cunha, G.; Santos, A.T.; Fernandes, R.M.; Abreu, D.; Gonçalves, N.; Matthew, H.; Isaacs, T.; Duffen, J.; Al-Jawad, A.; Larsen, F.; Serrano, A.; Weber, P.; Thoms, A.; Sollinger, S.; Graessner, H.; Maetzler, W.; Ferreira, J.J. A systematic review of the characteristics and validity of monitoring technologies to assess Parkinson's disease. J Neuroeng Rehabil. 2016, 13, 24. [Google Scholar] [CrossRef]
- Rovini, E.; Maremmani, C.; Cavallo, F. Automated Systems Based on Wearable Sensors for the Management of Parkinson's Disease at Home: A Systematic Review. Telemed. J. E Health. 2019, 25, 167–183. [Google Scholar] [CrossRef]
- Thorp, J.E.; Adamczyk, P.G.; Ploeg, H.L.; Pickett, K.A. Monitoring Motor Symptoms During Activities of Daily Living in Individuals With Parkinson's Disease. Front Neurol. 2018, 9, 1036. [Google Scholar] [CrossRef] [PubMed]
- Del Din, S.; Godfrey, A.; Mazzà, C.; Lord, S.; Rochester, L. Free-living monitoring of Parkinson's disease: Lessons from the field. Mov Disord. 2016, 31, 1293–1313. [Google Scholar] [CrossRef] [PubMed]
- Rovini, E.; Maremmani, C.; Cavallo, F. How Wearable Sensors Can Support Parkinson's Disease Diagnosis and Treatment: A Systematic Review. Front Neurosci. 2017, 11, 555. [Google Scholar] [CrossRef] [PubMed]
- Morgan, C.; Rolinski, M.; McNaney, R.; Jones, B.; Rochester, L.; Maetzler, W.; Craddock, I.; Whone, A.L. Systematic Review Looking at the Use of Technology to Measure Free-Living Symptom and Activity Outcomes in Parkinson's Disease in the Home or a Home-like Environment. J Parkinsons Dis. 2020, 10, 429–454. [Google Scholar] [CrossRef]
- Bloem, B.R.; Marks, W.J.; Silva de Lima, A.L.; Kuijf, M.L.; van Laar, T.; Jacobs, B.P.F.; Verbeek, M.M.; Helmich, R.C.; van de Warrenburg, B.P.; Evers, L.J.W.; intHout, J.; van de Zande, T.; Snyder, T.M.; Kapur, R.; Meinders, M.J. The Personalized Parkinson Project: examining disease progression through broad biomarkers in early Parkinson's disease. BMC Neurol. 2019, 19, 160. [Google Scholar] [CrossRef]
- Sturchio, A.; Marsili, L.; Vizcarra, J.A.; Dwivedi, A.K.; Kauffman, M.A.; Duker, A.P.; Lu, P.; Pauciulo, M.W.; Wissel, B.D.; Hill, E.J.; Stecher, B.; Keeling, E.G.; Vagal, A.S.; Wang, L.; Haslam, D.B.; Robson, M.J.; Tanner, C.M.; Hagey, D.W.; El Andaloussi, S.; Ezzat, K.; Fleming, R.M.T.; Lu, L.J.; Little, M.A.; Espay, A.J. Phenotype-Agnostic Molecular Subtyping of Neurodegenerative Disorders: The Cincinnati Cohort Biomarker Program (CCBP). Front Aging Neurosci. 2020, 12, 553635. [Google Scholar] [CrossRef]
- Adams, J.L.; Kangarloo, T.; Tracey, B.; O'Donnell, P.; Volfson, D.; Latzman, R.D.; Zach, N.; Alexander, R.; Bergethon, P.; Cosman, J.; Anderson, D.; Best, A.; Severson, J.; Kostrzebski, M.A.; Auinger, P.; Wilmot, P.; Pohlson, Y.; Waddell, E.; Jensen-Roberts, S.; Gong, Y.; Kilambi, K.P.; Herrero, T.R.; Ray Dorsey, E.; Parkinson Study Group Watch-PD Study Investigators and Collaborators. Using a smartwatch and smartphone to assess early Parkinson's disease in the WATCH-PD study. NPJ Parkinsons Dis. 2023, 9, 64. [Google Scholar] [CrossRef]
- Adams, J.L. WATCH-PD: Wearable assessments in the clinic and home in Parkinson’s disease: Study design and update. Mov.Disord. 2020, 35, S1–S702. [Google Scholar]
- Lawton, M.; Baig, F.; Rolinski, M.; Ruffman, C.; Nithi, K.; May, M.T.; Ben-Shlomo, Y.; Hu, M.T. Parkinson's Disease Subtypes in the Oxford Parkinson Disease Centre (OPDC) Discovery Cohort. J Parkinsons Dis. 2015, 5, 269–279. [Google Scholar] [CrossRef]
- Sorici, A.; Băjenaru, L.; Mocanu, I.G.; Florea, A.M.; Tsakanikas, P.; Ribigan, A.C.; Pedullà, L.; Bougea, A. Monitoring and Predicting Health Status in Neurological Patients: The ALAMEDA Data Collection Protocol. Healthcare 2023, 11, 2656. [Google Scholar] [CrossRef]
- NICE. NICE Recommends NHS Collects Real-World Evidence on Devices that Monitor People with Parkinson’s Disease. 2023. Available online: https://www.nice.org.uk/guidance/ dg51 (accessed on 5 December 2024).
- Antonini, A.; Reichmann, H.; Gentile, G.; Garon, M.; Tedesco, C.; Frank, A.; Falkenburger, B.; Konitsiotis, S.; Tsamis, K.; Rigas,G. ; Kostikis, N.; Ntanis, A.; Pattichis, C. Toward objective monitoring of Parkinson's disease motor symptoms using a wearable device: wearability and performance evaluation of PDMonitor®. Front Neurol. 2023, 14, 1080752. [Google Scholar] [CrossRef] [PubMed]
- Horne, MK.; McGregor, S.; Bergquist, F. An objective fluctuation score for Parkinson's disease. PLoS One. 2015, 10, e0124522. [Google Scholar] [CrossRef] [PubMed]
- Pahwa, R.; Isaacson, SH.; Torres-Russotto, D.; Nahab, FB.; Lynch, PM.; Kotschet, KE. Role of the Personal KinetiGraph in the routine clinical assessment of Parkinson's disease: recommendations from an expert panel. Expert Rev Neurother. 2018, 18, 669–680. [Google Scholar] [CrossRef] [PubMed]
- Samà, A.; Pérez-López, C.; Rodríguez-Martín, D.; Català, A.; Moreno-Aróstegui, JM.; Cabestany, J.; de Mingo, E.; Rodríguez-Molinero, A. Estimating bradykinesia severity in Parkinson's disease by analysing gait through a waist-worn sensor. Comput Biol Med. 2017, 84, 114–123. [Google Scholar] [CrossRef]
- Giuffrida, JP.; Riley, DE.; Maddux, BN.; Heldman, D.A. Clinically deployable Kinesia technology for automated tremor assessment. Mov Disord. 2009, 24, 723–730. [Google Scholar] [CrossRef]
- Mera, T.O.; Heldman, D.A.; Espay, A.J.; Payne, M.; Giuffrida, J.P. Feasibility of home-based automated Parkinson's disease motor assessment. J Neurosci Methods. 2012, 203, 152–156. [Google Scholar] [CrossRef]
- Hadley, A.J.; Riley, D.E.; Heldman, D.A. Real-World Evidence for a Smartwatch-Based Parkinson's Motor Assessment App for Patients Undergoing Therapy Changes. Digit Biomark. 2021, 5, 206–215. [Google Scholar] [CrossRef]
- Pulliam, C.L.; Heldman, D.A.; Brokaw, E.B.; Mera, T.O.; Mari, Z.K.; Burack, M.A. Continuous Assessment of Levodopa Response in Parkinson's Disease Using Wearable Motion Sensors. IEEE Trans Biomed Eng. 2018, 65, 159–164. [Google Scholar] [CrossRef]
- Isaacson, S.H.; Boroojerdi, B.; Waln, O.; McGraw, M.; Kreitzman, DL.; Klos, K.; Revilla, F.J.; Heldman, D.; Phillips, M.; Terricabras, D.; Markowitz, M.; Woltering, F.; Carson, S.; Truong, D. Effect of using a wearable device on clinical decision-making and motor symptoms in patients with Parkinson's disease starting transdermal rotigotine patch: A pilot study. Parkinsonism Relat Disord. 2019, 64, 132–137. [Google Scholar] [CrossRef]
- Hoffman, J.D.; McNames, J. Objective measure of upper extremity motor impairment in Parkinson's disease with inertial sensors. Annu Int Conf IEEE Eng Med Biol Soc. 2011, 2011, 4378–4381. [Google Scholar]
- Espay, A.J.; Giuffrida, J.P.; Chen, R.; Payne, M.; Mazzella, F.; Dunn, E.; Vaughan, J.E.; Duker, A.P.; Sahay, A.; Kim, S.J.; Revilla, F.J.; Heldman, D.A. Differential response of speed, amplitude, and rhythm to dopaminergic medications in Parkinson's disease. Mov Disord. 2011, 26, 2504–2508. [Google Scholar] [CrossRef] [PubMed]
- Mera, T.; Vitek, J.L.; Alberts, J.L.; Giuffrida, J.P. Kinematic optimization of deep brain stimulation across multiple motor symptoms in Parkinson's disease. J Neurosci Methods. 2011, 198, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Heldman, D.A.; Filipkowski, D.E.; Riley, D.E. , Whitney, C.M.; Walter, B.L.; Gunzler, S.A.; Giuffrida, J.P.; Mera, T.O. Automated motion sensor quantification of gait and lower extremity bradykinesia. Annu Int Conf IEEE Eng Med Biol Soc. 2012, 2012, 1956–1959. [Google Scholar] [PubMed]
- Mera, T.O.; Filipkowski, D.E.; Riley, D.E.; Whitney, C.M.; Walter, B.L.; Gunzler, S.A.; Giuffrida, J.P. Quantitative analysis of gait and balance response to deep brain stimulation in Parkinson's disease. Gait Posture. 2013, 38, 109–114. [Google Scholar] [CrossRef]
- Mera, T.O.; Burack, M.A.; Giuffrida, J.P. Objective motion sensor assessment highly correlated with scores of global levodopa-induced dyskinesia in Parkinson's disease. J Parkinsons Dis. 2013, 3, 399–407. [Google Scholar] [CrossRef]
- Heldman, D.A.; Espay, A.J.; LeWitt, P.A.; Giuffrida, J.P. Clinician versus machine: reliability and responsiveness of motor endpoints in Parkinson's disease. Parkinsonism Relat Disord. 2014, 20, 590–595. [Google Scholar] [CrossRef]
- Pulliam, C.L.; Burack, M.A.; Heldman, D.A.; Giuffrida, J.P.; Mera, T.O. Motion sensor dyskinesia assessment during activities of daily living. J Parkinsons Dis. 2014, 4, 609–615. [Google Scholar] [CrossRef]
- Pulliam, C.L.; Heldman, D.A.; Orcutt, T.H.; Mera, T.O.; Giuffrida, J.P.; Vitek, J.L. Motion sensor strategies for automated optimization of deep brain stimulation in Parkinson's disease. Parkinsonism Relat Disord. 2015, 21, 378–382. [Google Scholar] [CrossRef]
- Heldman, D.A.; Giuffrida, J.P.; Cubo, E. Wearable Sensors for Advanced Therapy Referral in Parkinson's Disease. J Parkinsons Dis. 2016, 6, 631–638. [Google Scholar] [CrossRef]
- Heldman, D.A.; Urrea-Mendoza, E.; Lovera, L.C.; Schmerler, D.A.; Garcia, X.; Mohammad, M.E.; McFarlane, M.C.U.; Giuffrida, J.P.; Espay, A.J.; Fernandez, H.H. App-Based Bradykinesia Tasks for Clinic and Home Assessment in Parkinson's Disease: Reliability and Responsiveness. J Parkinsons Dis. 2017, 7, 741–747. [Google Scholar] [CrossRef]
- Heldman, D.A.; Harris, D.A.; Felong, T.; Andrzejewski, K.L.; Dorsey, E.R.; Giuffrida, J.P.; Goldberg, B.; Burack, M.A. Telehealth Management of Parkinson's Disease Using Wearable Sensors: An Exploratory Study. Digit Biomark. 2017, 1, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Sturchio, A.; Dwivedi, A.K.; Marsili, L.; Hadley, A.; Sobrero, G.; Heldman, D.; Maule, S.; Lopiano, L.; Comi, C.; Versino, M.; Espay, A.J.; Merola, A. Kinematic but not clinical measures predict falls in Parkinson-related orthostatic hypotension. J Neurol. 2021, 268, 1006–1015. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.S.; Leurgans, S.E.; Weiss, A.; Vanderhors, V.; Mirelman, A.; Dawe, R.; Barnes, L.L.; Wilson, R.S.; Hausdorff, J.M.; Bennett, D.A. Associations between quantitative mobility measures derived from components of conventional mobility testing and Parkinsonian gait in older adults. PLoS One. 2014, 9, e86262. [Google Scholar] [CrossRef] [PubMed]
- Hill, E.J.; Mangleburg, C.G.; Alfradique-Dunham, I.; Ripperger, B.; Stillwell, A.; Saade, H.; Rao, S.; Fagbongbe, O.; von Coelln, R.; Tarakad, A.; Hunter, C.; Dawe, R.J.; Jankovic, J.; Shulman, L.M.; Buchman, A.S.; Shulman, J.M. Quantitative mobility measures complement the MDS-UPDRS for characterization of Parkinson's disease heterogeneity. Parkinsonism Relat Disord. 2021, 84, 105–111. [Google Scholar] [CrossRef]
- Jacobs, D.; Farid, L.; Ferré, S.; Herraez, K.; Gracies, J.M.; Hutin, E. Evaluation of the Validity and Reliability of Connected Insoles to Measure Gait Parameters in Healthy Adults. Sensors 2021, 21, 6543. [Google Scholar] [CrossRef]
- Lunardini, F.; Malavolti, M.; Pedrocchi, A.L.G.; Borghese, N.A.; Ferrante, S. A mobile app to transparently distinguish single- from dual-task walking for the ecological monitoring of age-related changes in daily-life gait. Gait Posture. 2021, 86, 27–32. [Google Scholar] [CrossRef]
- Farid, L.; Jacobs, D.; Do Santos, J.; Simon, O.; Gracies, J.M.; Hutin, E. FeetMe® Monitor-connected insoles are a valid and reliable alternative for the evaluation of gait speed after stroke. Top Stroke Rehabil. 2021, 28, 127–134. [Google Scholar] [CrossRef]
- Granja Domínguez, A.; Romero Sevilla, R.; Alemán, A.; Durán, C.; Hochsprung, A.; Navarro, G.; Páramo, C.; Venegas, A.; Lladonosa, A.; Ayuso, G.I. Study for the validation of the FeetMe® integrated sensor insole system compared to GAITRite® system to assess gait characteristics in patients with multiple sclerosis. PLoS One. 2023, 18, e0272596. [Google Scholar] [CrossRef]
- Parati, M.; Gallotta, M.; Muletti, M.; Pirola, A.; Bellafà, A.; De Maria, B.; Ferrante, S. Validation of Pressure-Sensing Insoles in Patients with Parkinson's Disease during Overground Walking in Single and Cognitive Dual-Task Conditions. Sensors 2022, 22, 6392. [Google Scholar] [CrossRef]
- Curtze, C.; Nutt, J.G.; Carlson-Kuhta, P.; Mancini, M.; Horak, F.B. Levodopa Is a Double-Edged Sword for Balance and Gait in People With Parkinson's Disease. Mov Disord. 2015, 30, 1361–1370. [Google Scholar] [CrossRef]
- Wan, S.; Liang, Y.; Zhang, Y.; Guizani, M. Deep Multi-Layer Perceptron Classifier for Behavior Analysis to Estimate Parkinson’s Disease Severity Using Smartphones. IEEE Access. 2018, 6, 36825–36833. [Google Scholar] [CrossRef]
- Deng, K.; Li, Y.; Zhang, H.; Wang, J.; Albin, R.L.; Guan, Y. Heterogeneous digital biomarker integration out-performs patient self-reports in predicting Parkinson's disease. Comm. Biol. 2022, 5, 58. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.P.; Liang, H.Y.; Chen, Y.S.; Lu, C.H.; Wu, Y.R.; Chang, Y.Y.; Lin, W.C. Objective assessment of impulse control disorder in patients with Parkinson's disease using a low-cost LEGO-like EEG headset: a feasibility study. J Neuroeng Rehabil. 2021, 18, 109. [Google Scholar] [CrossRef] [PubMed]
- Thévenot, D.R.; Toth, K.; Durst, R.A.; Wilson, G.S. Electrochemical biosensors: recommended definitions and classification. Biosens Bioelectron. 2001, 16, 121–131. [Google Scholar] [CrossRef]
- Jang, S.J.; Lee, C.S.; Kim, T.H. α-Synuclein Oligomer Detection with Aptamer Switch on Reduced Graphene Oxide Electrode. Nanomaterials 2020, 10, 832. [Google Scholar] [CrossRef]
- Lipsmeier, F.; Taylor, K.I.; Kilchenmann, T.; Wolf, D.; Scotland, A.; Schjodt-Eriksen, J.; Cheng, W.Y.; Fernandez-Garcia, I.; Siebourg-Polster, J.; Jin, L.; Soto, J.; Verselis, L.; Boess, F.; Koller, M.; Grundman, M.; Monsch, A.U.; Postuma, R.B.; Ghosh, A.; Kremer, T.; Czech, C.; Gossens, C.; Lindemann, M. Evaluation of smartphone-based testing to generate exploratory outcome measures in a phase 1 Parkinson's disease clinical trial. Mov Disord. 2018, 33, 1287–1297. [Google Scholar] [CrossRef]
- Powers, R.; Etezadi-Amoli, M.; Arnold, E.M.; Kianian, S.; Mance, I.; Gibiansky, M.; Trietsch, D.; Alvarado, A.S.; Kretlow, J.D.; Herrington, T.M.; Brillman, S.; Huang, N.; Lin, P.T.; Pham, H.A.; Ullal, A.V. Smartwatch inertial sensors continuously monitor real-world motor fluctuations in Parkinson's disease. Sci Transl Med. 2021, 13, eabd7865. [Google Scholar] [CrossRef]
- Iakovakis, D.; Hadjidimitriou, S.; Charisis, V.; Bostantjopoulou, S.; Katsarou, Z.; Klingelhoefer, L.; Reichmann, H.; Dias, S.B.; Diniz, J.A.; Trivedi, D.; Chaudhuri, K.R.; Hadjileontiadis, L.J. Motor Impairment Estimates via Touchscreen Typing Dynamics Toward Parkinson's Disease Detection From Data Harvested In-the-Wild. Front. ICT 2018, 5, 28. [Google Scholar]
- Simonet, C.; Noyce, A.J. Domotics, Smart Homes, and Parkinson's Disease. J Parkinsons Dis. 2021, 11, S55–S63. [Google Scholar] [CrossRef]
- Silva de Lima, A.L.; Smits, T.; Darweesh, S.K.L.; Valenti, G.; Milosevic, M.; Pijl, M.; Baldus, H.; de Vries, N.M.; Meinders, M.J.; Bloem, B.R. Home-based monitoring of falls using wearable sensors in Parkinson's disease. Mov Disord. 2020, 35, 109–115. [Google Scholar] [CrossRef]
- Di Biagio, L. , M., Cingolani, D., Buzzatti, L., Capecci, M., Ceravolo, M.G. Virtual reality: A new rehabilitative approach in neurological disorders. In Ambient Assisted Living; Longhi, S., Siciliano, P., Germani, M., Monteriu, A., Eds.; Springer International Publishing: Switzerland, 2014; pp. 167–176. [Google Scholar]
- Pfeifer, K.J.; Kromer, J.A.; Cook, A.J.; Hornbeck, T.; Lim, E.A.; Mortimer, B.J.P.; Fogarty, A.S.; Han, S.S.; Dhall, R.; Halpern, C.H.; Tass, P.A. Coordinated Reset Vibrotactile Stimulation Induces Sustained Cumulative Benefits in Parkinson's Disease. Front Physiol. 2021, 12, 624317. [Google Scholar] [CrossRef] [PubMed]
- Melbourne, J.A. , Kehnemouyi, Y.M., O'Day, J.J., Wilkins, K.B., Gala, A.S., Petrucci, M.N., Lambert, E.F.; Dorris, H.J.; Diep, C.; Herron, J.A.; Bronte-Stewart, H.M. Kinematic adaptive deep brain stimulation for gait impairment and freezing of gait in Parkinson's disease. Brain Stimul. 2023, 16, 1099–1101. [Google Scholar] [CrossRef] [PubMed]
- Davidashvilly, S.; Cardei, M.; Hssayeni, M.; Chi, C.; Ghoraani, B. Deep neural networks for wearable sensor-based activity recognition in Parkinson's disease: investigating generalizability and model complexity. Biomed Eng Online. 2024, 23, 17. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Zhang, D.; Yao, L.; Guo, B.; Yu, Z.; Liu, Y. Deep learning for sensor-based human activity recognition: Overview challenges and opportunities. ACM Comput. Surv. 2022, 54, 1–40. [Google Scholar] [CrossRef]
- Nagasubramanian, G.; Sankayya, M. ; Multi-variate vocal data analysis for detection of Parkinson disease using deep learning. Neural Comput. Appl. 2021, 33, 4849–4864. [Google Scholar] [CrossRef]
- Soundararajan, R.; Prabu, A.V.; Routray, S.; Malla, P.P.; RAY, A.K.; Palai, G.; Faragallah, O.S.; BAZ, M.; Abualnaja, M.M.; . Eid, M.M.A.; Rashed, A.N.Z. Deeply Trained Real-Time Body Sensor Networks for Analyzing the Symptoms of Parkinson’s Disease. IEEE Access 2022, 10, 63403–63421. [Google Scholar] [CrossRef]
- O'Day, J.; Lee, M.; Seagers, K.; Hoffman, S.; Jih-Schiff, A.; Kidziński, Ł.; Delp, S.; Bronte-Stewart, H. Assessing inertial measurement unit locations for freezing of gait detection and patient preference. J Neuroeng Rehabil. 2022, 19, 20. [Google Scholar] [CrossRef]
Figure 1.
An overview of the sensors for PD, their data collection and analysis by health professionnels.
Figure 1.
An overview of the sensors for PD, their data collection and analysis by health professionnels.
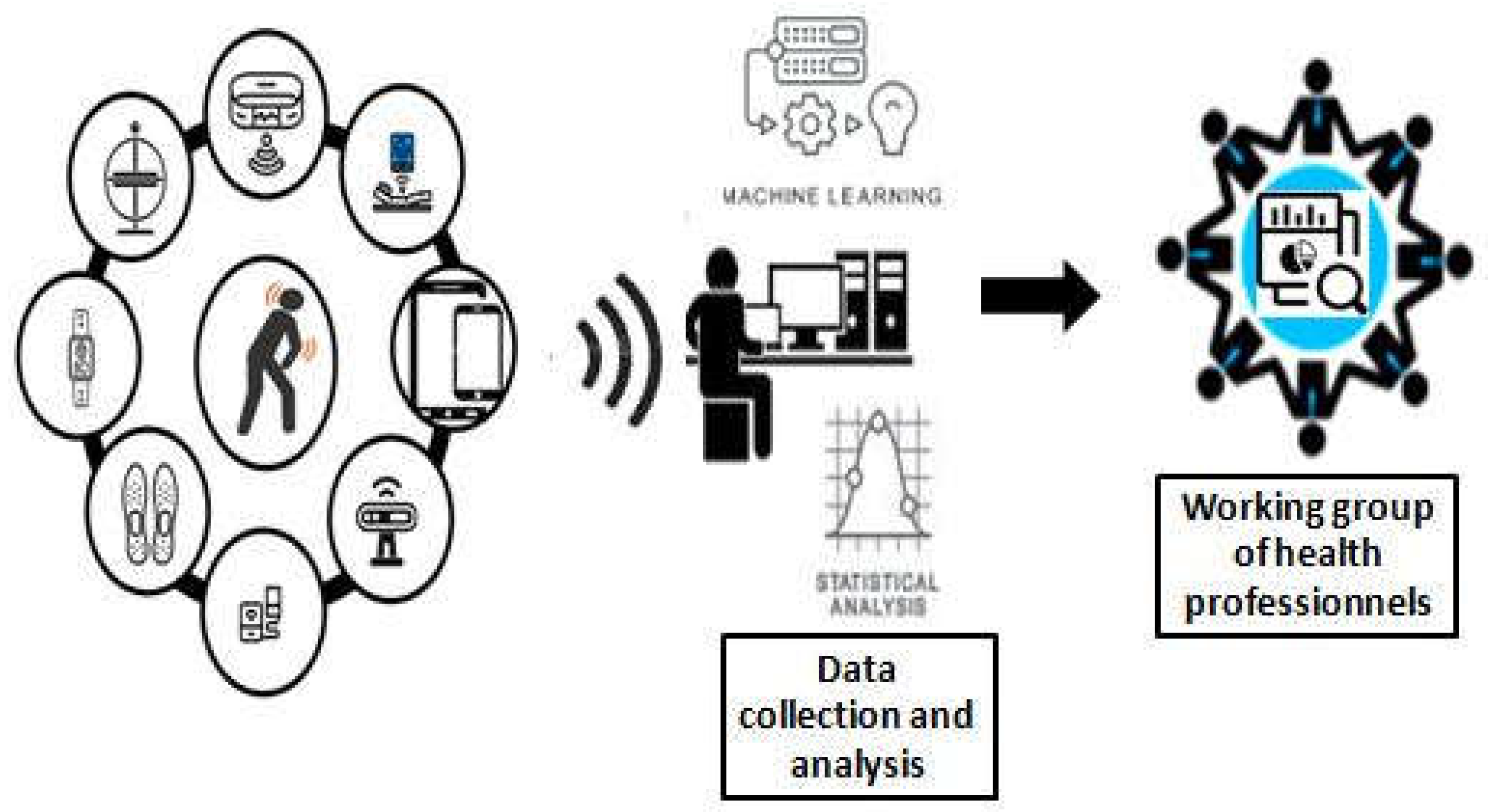
Figure 2.
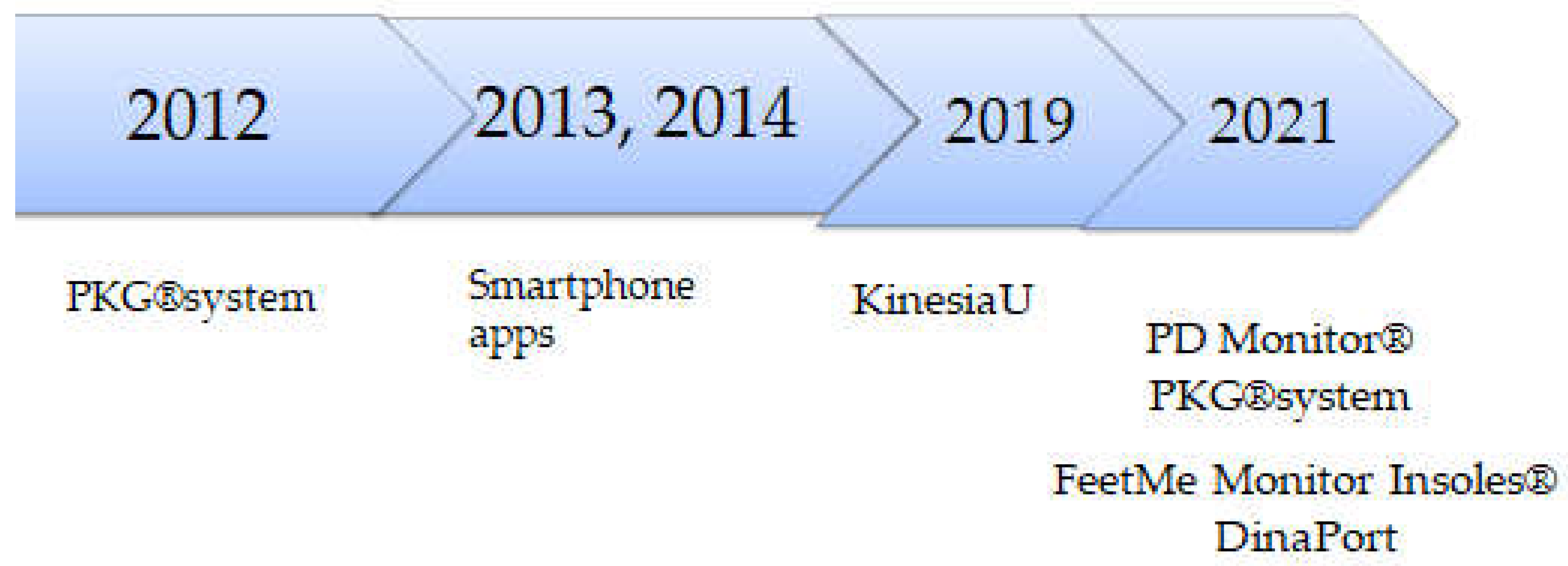

Table 1.
Selected studies of wearable sensors for PD.
| Authors (publication year ) | DB type | Sample | Assessment tools, ML algorithms/motor parameters | Main results |
| Hoffman et al. (2011) | triaxial gyroscopes and adaptive filters | 11 PD pts | UPDRS/ angular velocity signal | The angular velocity signal was less predictable than those collected from age, weight and height-matched controls |
| Heldman et al. (2012) | heel-worn motion sensor | 22 non-DBS pts with PD20 DBS pts with PD | MDS-UPDRS | kinematic data and clinician scores and produced outputs highly correlated to clinician scores with an average correlation coefficient of 0.86 |
| Mera et al. (2013) | KinetiSense wrist-worn motion sensor | 15 pts with PD | mAIMSPDYS-26 | Prediction of the Levodopa-induced peak-dose dyskinesia severity |
| Weiss et al. (2014) | body-fixed sensor (3D accelerometer) on lower back | 107 PD pts | Walking quantity (e.g., steps per 3-days) and quality (e.g., frequency-derived measures of gait variability) | Successful detection of the transition from non-faller to faller, whereas traditional metrics did not. |
| Ossig et al. (2016) | PKG | 24 PD pts | UPDRSIII motor scorepatient diariesBDI | moderate-to-high concordance of quantitative motor status by PKG and patient diaries |
| Pérez-López et al. (2016) | single belt-worn accelerometer |
1st database:92 PD pts (validation cohort) 2nd database:10 PD pts |
Indoors walking test Outdoors walking test FoG provocation test Dyskinesia test False Positive Test |
95% specificity and 39% sensitivity detecting mild d 95% specificity and 93% sensitivity for severe and mild trunk dyskinesias |
| Samà et al. (2017) | waist-worn triaxial accelerometer | 12 PD pts | UPDRS | >90% accuracy for detection of bradykinesia |
| Bayés et al. (2018) | REMPARK System: sensor +smartphone | 41 pts with moderate to severe idiopathic PD | UPDRSIII motor scorepatient diaries | 97% sensitivity in detecting OFF states and 88% specificity (i.e., accuracy in detecting ON states). |
| Lee et al. (2018) | Shoe-type IMU sensor | 17 PD pts | MDS-UPDRS MMSE/ linear accelerations, cadence, left step length, right step length, left step time, and right step time |
excellent agreement between motor parameters and the shoe-type IMU and motion capture systems |
| Pulliam et al. (2018) | wrist and ankle motion sensors recorded by video | 13 PD prs | UPDRS-III | Algorithm scores for tremor, bradykinesia, and dyskinesia agreed with clinician ratings of video recordings (ROC area > 0.8) |
| Wan et al. (2018) | smartphone accelerometer | 42 pts of early-stage PD | UPDRS ML classification algorithms |
Among all MLs, DMLP captured the best the accelerometer data from the smartphone |
| Buongiorno et al. (2019) | Microsoft Kinect v2 sensor | 16 PD pts |
MDS-UPDRS ANN SVM |
AAN:89.4% accuracy for 9 PD features and 95.0% of accuracy of 6 features in rating PD severity SVM: 87.1% accuracy for 2 PD features |
| Isaacson et al. (2019) | Kinesia 360: wrist and ankle sensors | 39 PD pts | UPDRS Kinesia 360-derived motor scores by time for the EG PDQ-39 PAM-13 |
continuous, objective, motor symptom monitoring as an adjunct to standard care enhances clinical decision-making |
| Mazzetta et al. (2019) | wearable system | Pts with P moderate PD |
real-time FOG detection using gyro and sEMG MDS-UPDRS 7-m TUG test FOG questionnaire |
timely detection of the FOG episode and, for the first time, the automatic distinction of the FOG –fall risk related phenotypes |
| Weiss et al. (2019) | Body fixed sensor | 96 participants with PD • One-off session | MoCA | Timed up-and-go strategies were not related to cognitive function |
| Xiong et al. (2020) | vocal vectors autoencoders | 188 PD pts with and without vocal disorders | 6 Supervised ML algorithms | Efficacy of the Adaptive Grey Wolf Optimization Algorithm in distinguishing the affected and healthy samples of PD |
| Hadley et al. (2021) | smartphone-based KinesiaUTM | 16 PD pts | electronic diary | successfully captured temporal trends in symptom scores following application of new therapy on hourly, daily, and weekly timescales |
| van Kersbergen et al. (2021) | Microsoft Kinect V2 sensor | 19 PD pts |
Camera-derived dataMDS-UPDRS |
significant differences between patients and controls for step length and average walking speed |
| Parati et al. (2022) |
FeetMe® insoles GaitRite®electronic pressure-sensitive walkway |
25 mild-to-moderatePD pts | UPDRS-part III Spatiotemporal gait parameters |
moderate to excellent correlations and good agreement between the two systems |
| Safarpour et al. (2022) | 3 inertial sensors | 31 mild to moderate PD pts |
MDS-UPDRS PIGD |
Prediction of MDS-UPDRS rigidity and PIGD scores by walking bouts, gait speed, and postural sway |
| Adams et al. (2023] | Smartphone smartwatch |
82 pts with early, untreated PD |
MDS-UPDRS Trail Making Test Part A MoCA Symbol Digital Visuospatial Working Memory |
moderate to very strong correlations of gait parameters with sensors measures |
| Antonini et al. (2023) | PDMonitor® | 65 PD pts | UPDRS Part III AIMS |
high accuracy in the detection of motor symptoms and the correlation between their severity |
| Keogh et al. (2023) | McRoberts Dynaport MM + waist worn device | 20 PD pts | Interviews CRS Rabinovich questionnaire |
The device was considered both comfortable and accetable |
| Bailo et al.( 2024) | G-Walk sensor by a semi-elastic belt | 22pts with mild PD | MDS-UPDRS II +III MoCA 6MWT TUG Leg Asymmetry Index Rigidity index Tremor index BMI PIGD |
positive correlations between gait variability and motor parameters |
AIMS: Abnormal Involuntary Movement Scale, ANN: Artificial Neural Networks, BDI: Beck’s Depression Inventory, BMI:Body Mass Index, CRS: comfort rating scale, DB: digital biomarker, DBS: deep brain stimulation, FOG: Freezing of Gait, mAIMS: modified Abnormal Involuntary Movement Scale, ML: machine learning, MMSE: Mini-mental state examination, MoCA:Montreal Cognitive Assessment, MDS-UPDRS Movement Disorder Society-Unified Parkinson’s Disease Rating Scale, 6MWT : 6-Minute Walk Test, PAM-13: 13-Item Patient Activation Measure, PD: Parkinson's disease, PDQ-39: 39-Item Parkinson's Disease Questionnaire, PDYS-26: e 26-item Parkinson’s Disease Dyskinesia Scale, PIGD: Postural Instability Gait Difficulty, PKG: Parkinson's kinetigraph, pts: patients, SVM: Support Vector Machine, TUG: Timed Up and Go.
Table 2.
Overview of commercial wearable sensors for PD monitoring.
| Wearable sensors Commercial name |
Study numbers, PD population (size, age, HY, disease duration)*, | Clinical/laboratoryTools assessments | Main outcomes | Medical class/FDA authorization (yes or no) |
| PD Monitor® | Two studies (sample size: 61–65 patients) Age range: NA; | Patients’ diaries AIMS scale UPDRS FoG index postural instability score gait impairment score |
Strong associations with video-recorded UPDRS and AIMS for bradykinesia and dyskinesia, very high for Off-time (accuracy: 99% resting tremor, 96% FoG) | CE mark class IIa /no |
| PKG® | 26 studies, large sample size (max sample size: 3288 patients) Age range: 30–80 yrs; Disease duration range: de novo (2 months) —23 years; HY: 1–4 (but disease data are not reported in all studies) | Patients’ diaries AIMS UPDRS |
Moderate correlation with bradykinesia, high correlation for dyskinesia, and tremor.97.1% sensitivity differentiating fluctuators vs non-fluctuators. | CE mark class Iia /no |
| STAT-ON® | 9 studies (12–75) Age range: 59–83; disease duration: 5–18 yrs; HY: 1–4 | Patients’ diaries UPDRS | 3 studies with good accuracy for On/Off fluctuations detection if compared to patients diaries, 2 studies (12–75 patients) with moderate/high correlation vs. UPDRS-III and gait, respectively; one study with moderate correlation with trunk/leg dyskinesia; one study (39 patients) with fair agreement for dyskinesia and FoG but low agreement for motor fluctuations if compared to UPDRS IV |
CE mark Class Iia /no |
| Kinesia360® | 10 studies (13–60 patients) Age range: 46–85 yrs; disease duration: 2–31 yrs; HY: 1–4 | Patients’ diaries UPDRS TETRAS |
high correlation for resting/postural tremor, dyskinesia and bradykinesia vs. physician-based video recordings | CE mark, Class I/yes |
| DinaPort | 3 studies (40–176 patients) Age range: 41–81; disease duration: 1–14 yrs; HY: 1–4 | MDS-UPDRS | MDS-UPDRS correlates with several gait parameters and misstep with history of falls | CE mark Class II in US and Classv I in EU/ yes |
| FeetMe Monitor Insoles® | one study (25 patients) Age (mean): 69 yrs; disease duration: 4 yrs; HY:2 | GaitRite® gait parameters |
high correlation for gait parameters between pressure-sensing insoles and the electronic walkway | CE-marked class Im /no |
| APDM® | 30 studies (max sample size: 198 PD patients) Age range: 52–78 yrs; disease duration: 1–19 yrs; HY: 1–4 | gold-standard laboratory metrics (GaitRite Mat,Optical MoCap, Force Plate) clinical scales (UPDRS-III, PIGD score) |
Moderate correlation with physicians’- base scales (UPDRS-III, PIGD score) High correlation with FoG episodes longer than 2–5 and >5 s Able to differentiate fallers vs. non fallers | Class II / yes |
AIMS : Abnormal Involuntary Movement Scale, HY: Hoehn and Yah, Medical class: Im device with low risk (m for measure); IIa = with low to medium risk, installed on the body during 30 min up to 60 days. FDA:Food and Drug Administration, FoG freezing of gait, MDS-UPDRS: Movement Disorder Society- Unified Parkinson's Disease Rating Scale , PIGD postural instability and gait disorders, * if an information on clinical features is not reported in the table, it is not reported in the literature, QUEST Quebec User Evaluation of Satisfaction with assistive Technology questionnaire, TETRAS:Essential Tremor Rating Scale, yrs years.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



