
Submitted:
02 January 2025
Posted:
03 January 2025
You are already at the latest version
Abstract
Kikuchi-Fujimoto disease (KFD) is a rare condition characterized by necrotizing lymphadenitis and fever, often associated with immune dysregulation. Histologically, it features necrotic foci with abundant histiocytes and plasmacytoid dendritic cells, but notably lacks neutrophils and eosinophils. Recent evidence reveals a notable prevalence among pediatric patients, who may exhibit distinct features compared to adults.
We report the case of an 11-year-old girl presenting with persistent fever, cervical adenopathy, and a malar rash, leading to a diagnosis of KFD following lymph node biopsy, which revealed non-suppurative necrosis and histiocytic infiltration. Empirical treatment with antivirals and antibiotics was ineffective, but corticosteroid therapy achieved symptom remission.
A literature review identified 48 relevant studies involving 386 pediatric cases, with histopathological findings consistent with classical descriptions of KFD. Cutaneous involvement was reported in 11.14% of cases, ranged from maculopapular rashes to lupus-like eruptions. Notable complications included the development of systemic lupus erythematous, Sjögren syndrome, and rare instances of hemophagocytic syndrome or central nervous system involvement. Kikuchi-Fujimoto disease should be considered in the differential diagnosis of pediatric patients presenting with fever and lymphadenopathy, taking into account a higher frequency of cutaneous manifestations that in adult cases.
Keywords:
Kikuchi-Fujimoto disease
; Children
; histiocytic necrotizing lymphadenitis
; Lupus erythematosus
; Skin
1. Introduction
Kikuchi-Fujimoto disease (KFD) is a rare condition characterized by subacute necrotizing lymphadenopathy and fever[1,2]. Its etiology remains unknown, although an immune-mediated pathogenesis has been proposed[2]. This hypothesis could explain the association between KFD and systemic lupus erythematosus (SLE), which relatively frequently results in the coexistence of both conditions in the same patient[2].
Histologically, KFD is characterized by histiocytic necrosis with abundant karyorrhectic nuclear debris and a notable absence of neutrophils and eosinophils[2]. Immunohistochemistry (IHC) commonly reveals histiocytes that are myeloperoxidase-positive (MPO+) and CD68+, a predominance of T cells within the lesions, and CD123+ plasmacytoid dendritic cells surrounding the necrotic areas[1,2,3].
Although KFD was initially thought to predominantly affect young adults, recent increases in reports of pediatric cases suggest that this condition is not as uncommon in childhood as previously believed[4,5,6]. Additionally, some studies have suggested differences between pediatric and adult cases, such as a higher prevalence of cutaneous rash in children[4]. In this study, we present a case of pediatric KFD and provide a literature review to enhance the understanding of this condition in children.
2. Case Report
Clinical Presentation
We present the case of an 11-year-old female admitted to the Department of Pediatrics with a persistent fever lasting more than a month, reaching temperatures up to 39°C, and accompanied by a cervical adenopathic conglomerate. A similar episode had resulted in hospitalization the previous month, which had resolved with intravenous (IV) methylprednisolone.
During her hospital stay, she developed a rash characterized by erosive lesions and crusts located in the bilateral ciliary and malar regions, as well as on the lobes of both ears (Figure 1). The patient was clinically diagnosed with Kaposi’s varicelliform eruption, and a PCR test for herpes simplex virus was performed on the erosive lesions. Additionally, a complete blood count (CBC), autoimmunity panel, lymphocyte subpopulation analysis, and serology for multiple infectious agents were requested. An excisional biopsy of the cervical adenopathy and a punch biopsy of the skin were also conducted. Before a definitive clinical diagnosis was established, intravenous linezolid (600 mg/12 hours) and acyclovir (10 mg/kg/8 hours) were administered empirically, but without significant clinical improvement.
PCR testing for viruses in the erosive lesions was negative. The CBC revealed leucopenia (2750/ul) and a slight increase in acute phase reactants. Serology tests for cytomegalovirus (CMV), Ebstein-Barr virus (EBV), human immunodeficiency virus (HIV), Hepatitis A, B, and C, Toxoplasma, Treponema, Bartonella, Brucella, and Leishmania were all negative. However, IgM antibodies against Mycoplasma pneumoniae were identified, along with positive antinuclear antibodies (ANAs) (speckled pattern,1:160).
Although the skin biopsy demonstrated a nonspecific superficial perivascular lymphocytic infiltrate, the histological examination of the lymph node revealed findings consistent with non-suppurative necrotizing lymphadenitis with abundant histiocytes. Based on these results, a diagnosis of Kikuchi-Fujimoto disease (KFD) was made. IV methylprednisolone (40 mg/day for 5 days) was administered, leading to remission of both systemic and cutaneous symptoms. The patient was subsequently discharged on oral prednisone (30 mg/day with gradual tapering).
The patient is currently receiving hydroxychloroquine (200 mg/day) and remains under follow-up care with the pediatric dermatology department. One month after discharge, she has not experienced any recurrence of adenopathy or fever.
Histopathologic Findings
The excisional biopsy revealed a lymph node measuring 1.3 × 1 cm, with a brownish surface and a typical nodular appearance.
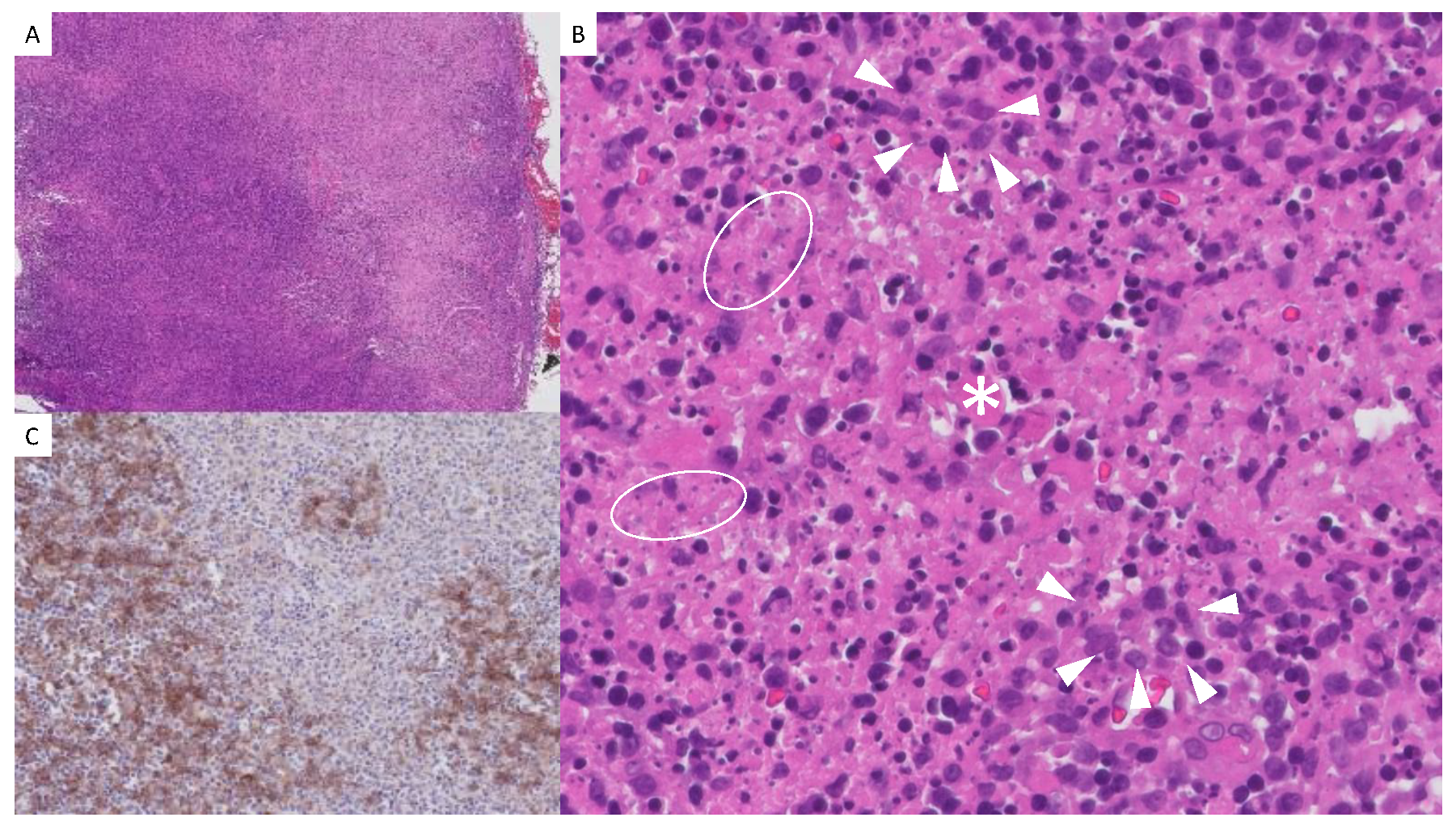
Microscopically, the lymph node exhibited a distorted architecture, with residual lymphoid follicles observed in the cortex and expansion of the paracortical area. Well-defined paracortical foci of non-suppurative necrosis with areas of karyorrhexis were identified. These foci were surrounded by an infiltrate composed of immunoblasts, plasma cells, histiocytes (Figure 2.B), abundant aggregates of CD123+ plasmacytoid dendritic cells (Figure 2.C), and lymphocytes predominantly expressing T-cell markers (CD3, CD2, CD5, CD7, CD4, and CD8). Sparse and occasionally scattered TdT-positive elements were also observed. No polymorphonuclear cells, eosinophils, or well-formed granulomas were identified.
Immunohistochemical markers assessed included CD20, Pax-5, CD79a, CD3, CD23, Bcl-6, Bcl-2, CD10, TdT, CD99, MUM-1, CD138, CD68, S100, CD1a, CD30, CD15, CD4, CD8, CD2, CD5, CD7, Ki-67, and CD123. Immunohistochemical staining for CMV was negative. The in-situ hybridization study for the detection of EBV RNA was also negative. PAS, Giemsa, Grocott, and Warthin-Starry stains, along with immunohistochemical staining for spirochetes, did not detect microorganisms in the examined sections.
The punch biopsy of the skin from the right ciliary area consisted of a 5-mm-thick sample with a typical surface and included subcutaneous cellular tissue. Microscopically, a mild superficial chronic perivascular dermatitis was observed, without adnexal tropism, interface changes, basement membrane thickening, or interstitial mucin deposition. Fungal spores were identified in the stratum corneum. An additional punch biopsy sample was submitted fresh for immunofluorescence study, which yielded negative results. The immunofluorescence panel included IgA, IgG, IgM, and C3.
3. Literature Review
A bibliographic search was conducted in the Medline database through PubMed, using the following search strategy: "Kikuchi-Fujimoto disease" OR "Kikuchi's disease" OR "Necrotizing histiocytic lymphadenitis" AND (pediatric OR childhood OR children). A total of 225 results were identified. After reviewing title and abstract, 60 studies were selected. Three studies were excluded because they were reviews, two studies were excluded due to lack of access, and seven studies were excluded because they were not relevant to the research topic upon full-text review.
A total of 48 studies were included in the final analysis (See Table 1): 11 were retrospective observational studies, and 37 were case reports involving one or two cases. The studies included 386 patients (209 males, 163 females, and 14 of unspecified gender). The overall weighted mean age was 12.67 years.
Cutaneous Manifestations
Skin manifestations were observed in approximately 11.14% of the sample. Generalized maculopapular rashes were reported in at least 40 patients[7,8,9,10,11,12,13,14], other findings included plantar annular erythema and chilblain lupus-like rashes[15], and non-pruritic generalized rash, sparing the nasolabial folds[16]. Oral ulcers where reported in 13 patients [13,17]. The only case of malar rash concomitant with KFD developed lupus during follow-up[18].
Histopathology
Most studies reported common histologic findings from excisional lymph node biopsy specimens, including cortical/paracortical necrosis, karyorrhexis, the presence of histiocytes (CD68+), plasmacytoid dendritic cells (CD123+), T-cell activation, and the absence of neutrophils, eosinophils, and granulomas (see Table 1). Lin et al. described the three histologic phenotypes of KFD: proliferative, necrotizing, and xanthomatous[19]. Camacho et al. identified organized granulomas in a lymph node specimen[20]. Skin punch biopsy was performed in only one case, revealing histologic findings of lymphohistiocytic infiltrates, predominantly perivascular, without necrosis of the adjacent vascular wall[7].
Treatment
A significant number of cases were self-limiting and did not require specific treatment[6,8,10,11,12,19,20,21,22,23,24,25,26,27,28,29]. In severe cases, or those associated with hemophagocytic syndrome, the most frequently administered treatments were prednisone[9,11,12,16,18,19,25,30,31,32], and IV methylprednisolone sometimes combined with IV immunoglobulin[9,14,33,34,35,36,37,38,39]. Hydroxychloroquine was commonly used in cases associated with SLE or lupus-like rashes[12,13,15,16,18,19].
Complications
A total of 10 cases of SLE were documented[5,6,10,13,14,15,16,18,37], with only two occurring concomitantly with KFD[13,37]. Additionally, four patients developed Sjögren syndrome[14,15]. Among the reported complications, central nervous system involvement[14,23,39,40] and hemophagocytic syndrome[9,14,33,41] were particularly noteworthy.

Table 1.
Literature review. ANAs: Antinuclear Antibodies; CNS: Central Nervous System; CMV: Cytomegalovirus; COVID-19: Coronavirus Disease 2019; EBV: Epstein-Barr Virus; IV: Intravenous; IVIG: Intravenous Immunoglobulin; MTX: Methotrexate; NA: Not Available; SLE: Systemic Lupus Erythematosus; SS: Sjögren Syndrome.
Table 1.
Literature review. ANAs: Antinuclear Antibodies; CNS: Central Nervous System; CMV: Cytomegalovirus; COVID-19: Coronavirus Disease 2019; EBV: Epstein-Barr Virus; IV: Intravenous; IVIG: Intravenous Immunoglobulin; MTX: Methotrexate; NA: Not Available; SLE: Systemic Lupus Erythematosus; SS: Sjögren Syndrome.
| Study (date) |
N; sex; age. | Sample |
Histopathology | Cutaneous manifestations | Possible Trigger | Treatment | Associated complications |
|---|---|---|---|---|---|---|---|
| Heldenberg et al [21] 1996 |
1; male; 10. |
Lymph node excisional biopsy Lymph node excisional biopsy Lymph node excisional biopsy |
Cortical or paracortical necrosis. Karyorrhexis. Histiocytes (CD68+), plasmacytoid dendritic cells (CD123+), T-cell activation. Absence of neutrophils, eosinophils and granulomas Cortical or paracortical necrosis. Karyorrhexis. Histiocytes (CD68+), plasmacytoid dendritic cells (CD123+), T-cell activation. Absence of neutrophils, eosinophils and granulomas Cortical or paracortical necrosis. Karyorrhexis. Histiocytes (CD68+), plasmacytoid dendritic cells (CD123+), T-cell activation. Absence of neutrophils, eosinophils and granulomas |
No | No | No specific therapy |
No |
| Gonzálvez-Piñera et al.[8] 2000 |
1;female;7 | Generalized maculopapular rash | No | No specific therapy | No | ||
| Emir et al.[42] 2001 |
1;female;14 | No | No | No specific therapy | No |
||
| Kim et al.[9] 2003 |
1;female;13 | Generalized maculopapular rash | EBV | IVIG IV methylprednisolone |
Hemophagocytic syndrome | ||
| Chiang et al.[22] 2004 |
1;male;8 | No | No | No specific therapy | No | ||
| Chuang et al.[10] 2005 |
64; 35 males; 29 females; Mean age 16. |
Generalized maculopapular rash (4/64) | CMV (2/64) |
No specific therapy | Developed SLE (1/64) | ||
| Lin et al.[6] 2005 |
23; 15 males; 8 females; Mean age 12.8 |
NA | NA | No specific therapy | Developed SLE (1/23) | ||
| Park et al.[30] 2007 |
16; 8 males; 8 females. Mean age 10.6 | No | EBV (2) ANA (1) | Oral prednisone (6/16) | No | ||
| Zou et al.[11] 2009 |
36; 23 males, 13 females; mean age 10.1 | Generalized maculopapular rash (5/36) | EBV (3/36) HSV (2/36) ANA (3/36) |
No specific therapy | No | ||
| Gómez et al.[31] 2010. |
1; female;10 | No | No | Oral prednisone | No | ||
| Lee et al.[5] 2012 |
9; 8 males;1 female Mean age 11.3 | Generalized maculopapular rash (2/9) | No ANA (1/9) |
High-dose corticosteroids, IVIG, plasmapheresis | Developed SLE (1/9) | ||
| Tchidjou et al.[43] 2004 |
1; male; 11 | No | No | IV methylprednisolone | |||
| Gonçalves et al.[40] 2014 |
1; male;9 | No | No | IV Dexamethasone | CNS involvement | ||
| Martins et al.[18] 2014 |
1;female;12 | malar rash | ANAs | Oral prednisone Hidroxychloroquine |
Developed SLE | ||
| Ojeda et al.[32] 2015 |
1:female;9 | No | ANAs | Oral Prednisone | No | ||
| Rossetti et al.[44] 2015 |
1;male;11 | No | No | Corticosterois | Upper airway obstruction | ||
| Altinel et al.[35] 2018 |
1;male;12 | No | Salmonella | IVIG | Auto-immune thyroiditis and papilloedema. | ||
| Chowdhury et al.[39] 2019 |
1;female;14 | No | No | IV methylprednisolone | CNS involvement | ||
| Handa et al.[45] 2016 |
1;male;15 | No | No | Oral corticosteroids | No | ||
| Lelii et al.[23] 2018 |
2;male;12;female;16 | No | CMV (1/2) ANA (1/2) |
No specific Therapy (1/2) Oral prednisone and cyclosporine (1/2) |
CNS involvement in 1 patient | ||
| Singh et al.[24] 2019 |
1;male;11 | No | No | No specific Therapy |
No | ||
| Quadir et al.[25] 2020 |
2; females;12 and 16 (dizygotic twins) |
Generalized maculopapular rash (2/2) |
Mycoplasma (1/2) | No specific Therapy (1/2) Oral prednisone (1/2) |
Developed alopecia areata (1/2) |
||
| Guleria et al.[37] 2020 |
6; 4 males; 2 females; Mean age 10.8 |
No | NA | Oral prednisolone (2/6) | Concomitant SLE (1/6) | ||
| Arslan et al.[46] 2020 |
1;female;12 | No | No | Oral prednisone | Optic Neuritis | ||
| Kim et al.[26] 2020 |
1;female;7 | No | Parvovirus B19 | No specific Therapy |
Severe neutropenia | ||
| Al Mosawi et al.[12] 2020 |
11; 6 males;5females; Mean age 10 | Generalized maculopapular rash (4/11) | No | Hidroxychloroquine (7/11) Corticosteroids (1/11) No specific Therapy (3/11) |
No | ||
| Cannon et al.[27] 2020 |
1;female;11 | No | No | No specific Therapy |
No | ||
| Hua et al.[38] 2021 |
1;male;14 | No | No | IV methylprednisolone |
Appendectomy (mimicked appendicitis) | ||
| Yang et al.[14] 2021 |
13; 9 males, 4 females. | Generalized maculopapular rash in 10 patients |
ANAs in 4 patients |
IVIG + Methylprednisolone: (6/13) Methylprednisolone + Cyclosporine A: (1/13) Cyclosporine A + Dexamethasone + Etoposide: (1/13) Methylprednisolone + Cyclosporine A + Cyclophosphamide: (1/13) Ruxolitinib + Methylprednisolone: (1/13) Methylprednisolone + Dexamethasone: (1/13) Symptomatic treatment: (3/13) Intrathecal Injection + Methotrexate: (1/13) IV Immunoglobulin: (1/13) |
Hemophagocytic syndrome (13/13) CNS involvement (8/13) Developed SLE (1/13) Developed SS (2/13) |
||
| Danai et al.[13] 2021 |
1;female;10 | Generalized maculopapular rash and oral ulcers | ANAs | Prednisone Hidroxychloroquine Methotrexate |
Concomitant SLE | ||
| Öztürk et al. [47] 2021 | 1;male;5 | No | COVID-19 | No specific Therapy |
No | ||
| Chisholm et al.[28] 2022 |
14;NA;NA | NA | NA | NA | NA | ||
| Takahashi et al.[15] 2023 |
2; female,13; male;11 Brothers |
Plantar annular erythema and chilblain lupus-like rashes. | No (later met the criteria for SLE) | Corticosteroid+ Hydroxychloroquine (1/2) Hydroxychloroquine (1/2) |
Developed SLE Developed SS (2/2) |
||
| Sevrin et al.[48] 2023 |
1;male,12 |
No | COVID-19 vaccination | Corticosterois |
No | ||
| Choi Sujin et al.[17] 2023 |
114;62 males;52 females; Mean age 12 | Oral ulcer (12/114) Generalized rash (11/114) |
NA | Corticosteroids (46/114) | No | ||
| Zhou et al[49] 2024 |
1;male;4 | No | No | Oral prednisone | CASPR2 antibody-associated encephalitis | ||
| Lu et al.[50] 2024 |
1;male;13 | No | No |
Corticosterois Rituximab |
occlusive retinal vasculitis with near total central retinal artery occlusion | ||
| Bao et al.[36] 2024 |
1;male;13 | No | No | IVIG, Oral Prednisone |
Optic Neuritis |
||
| Harrison et al.[16] 2024 |
1;female;16 | Generalized rash, sparing the nasolabial folds. | No (later met the criteria for SLE) | Hydroxychloroquine, prednisone, and mycophenolate mofetil |
Developed SLE |
||
| Camacho-Badilla et al.[20] 2005 |
1;male;10 | Lymph node excisional biopsy | Granulomas characterized by central necrosis with abundant karyorrhexis, surrounded by histiocytes, lymphocytes and giant multinucleated cells, without neutrophils. | No | No | No specific therapy |
No |
| Burns et al.[29] 2020 |
1;female;16 | FNAC | Necrotizing lymphadenitis | No | EBV, CMV | No specific Therapy |
No |
| Sierra et al.[7] 1999 |
1;male;14. | 1. Lymph node excisional biopsy 2. Cutenaous biopsy |
1. Histiocytic necrotizing lymphadenitis (see previous) 2. Lymphohistiocytic infiltrates, predominantly perivascular, without any necrosis of the adjacent vascular wall |
Generalized maculopapular rash | No | IV Methylprednisolone | Multisystemic involvement Adverse reaction to drugs |
| Chen et al.[33] 2000 |
1;female;13 | 1. Lymph node excisional biopsy 2.Bone marrow aspirate |
1. Histiocytic necrotizing lymphadenitis (see previous) 2.hemophagocytic histiocytes |
No | EBV | IVIG IV methylprednisolone oral dexamethasone |
hemophagocytic syndrome |
| Jun-Fen et al.[34] 2007. |
1; female;7 | 1. Lymph node excisional biopsy 2.Bone marrow aspirate |
1. Histiocytic necrotizing lymphadenitis (see previous) 2. Specific changes of idiopathic thrombocytopenic purpura |
No | No | IVIG IV methylprednisolone Oral dexamethasone |
Idiopathic thrombocytopenic purpura and Mobitz type II atrioventricular block |
| Sykes et al.[41] 2016 |
1;female;26 | 1. Lymph node excisional biopsy 2.Bone marrow aspirate |
1. Cortical or paracortical necrosis with various histiocytes, plasmacytoid monocytes and a variable number of lymphoid cells with caryorrhectic nuclear fragments and absence of neutrophils 2. hemophagocytic histiocytes |
No | No | High-dose corticosteroids, IVIG, and plasmapheresis | Hemophagocytic syndrome |
| Das et al.[51] 2019 |
1;male;NA | 1. Lymph node excisional biopsy 2.Bone marrow aspirate |
1. Cortical or paracortical necrosis with various histiocytes, plasmacytoid monocytes and a variable number of lymphoid cells with caryorrhectic nuclear fragments and absence of neutrophils 2. Reticulo-endothelial activity |
Generalized maculopapular rash | Brucella | Rifampicin and gentamicin, doxycycline, trimethoprim-sulfamethoxazole. Oral prednisolone |
Doxycycline-Induced Intracranial Hypertension |
| Lin et al.[19] 2019 |
40;20 males;20 females;Mean age 13.9 | Lymph node excisional biopsy | 14 patients with proliferative type containing karyorrhectic nuclear fragments, eosinophilic apoptotic debris and various histiocytes 23 patients with necrotizing type showing the existence of coagulative necrosis 1 patient wit xanthomatous type showing foamy histiocytes. 2 patients with NA histopathology. |
Generalized maculopapular rash (2/40) | ANAs (1/40) EBV (1/40) |
Oral prednisone (5/40) Hidroxychloroquine (5/40) No specific Therapy in the rest. |
No |
| Abdu et al.[52] 2022 |
1;female,10 |
1. Lymph node excisionalbiopsy 2. Bone marrow biopsy |
1. Necrotizing his- tiocytic lymphadenitis, 2. Normocellular bone marrow with reactive lymphocytosis and hemophagocytosis |
No | Acute otitis media |
Corticosterois |
No |
4. Discussion
The currently available literature supports the notion that KFD is not an uncommon condition in childhood. Our case can be considered epidemiologically typical, as it occurs in a female under 30 years of age. While earlier studies suggested a female predominance, more recent research indicates that the incidence of KFD is similar between males and females [1,53]. Based on our review of pediatric cases, a higher proportion of males has been reported. This male predominance in pediatric cases has also been described in other series not included in this review [4].
Cutaneous manifestations associated with KFD have been described as more frequent in children, with an incidence of approximately 10% [4], consistent with the findings in our review. These manifestations typically present as a maculopapular rash, predominantly on the face and the upper trunk. However, a wide range of dermatoses has been documented, including urticarial, morbilliform, rubella-like, lupus-like, or drug-eruption-like rashes; facial erythema; generalized erythema; papules, plaques, and nodules; leukocytoclastic vasculitis; erythema multiforme; papulopustules; and even eyelid edema [54,55,56]. The histopathology of cutaneous lesions in KFD is similarly diverse. Specific findings associated with extranodal KFD include an infiltrate composed of lymphocytes, histiocytes, plasmacytoid monocytes, and nuclear debris, notably in the absence of neutrophils [55]. Occasionally, the histology resembles the cutaneous features of SLE, showing interface changes with vacuolar degeneration of basal cells and mild perivascular infiltrates of lymphocytes and histiocytes in skin biopsies[54,57]. It has been suggested that interface changes observed in skin biopsies may predict an increased risk of developing SLE[58].
Our case presented malar erosive lesions typically affecting the ears, resembling those described in other case reports involving both pediatric and adult patients[59,60]. Histologically, no evidence of extranodal KFD or cutaneous lupus was identified; instead, the biopsy revealed a superficial perivascular lymphocytic infiltrate. The limited findings in the skin biopsy may be attributed to the supraciliary location of the sample, chosen to minimize the aesthetic impact of scarring in an area where the erosive component was minimal. Nevertheless, non-specific perivascular dermatitis is a common finding in skin biopsies of patients with KFD [7,61]. Lupus-like rash appears to predict a higher risk of developing SLE. This, combined with the presence of ANAs in the patient's analysis, prompted the initiation of hydroxychloroquine therapy and the establishment of close follow-up.
Fine needle aspiration of the lymph node does not seem to provide a sufficient sample for diagnosis[2], although it was the technique used in one of the cases in our review[29]. In general, excisional biopsy of a lymph node is recommended for the diagnosis of KFD. The histopathologic findings of the lymph node biopsy, both in the case presented and in most of the pediatric cases reviewed, are consistently similar: cortical or paracortical necrosis, karyorrhexis, histiocytes (MPO+, CD68+), plasmacytoid dendritic cells (CD123+), and T-cell activation. Notably, there is an absence of neutrophils, eosinophils, and granulomas. Histopathologically, three chronologically related stages of KFD have been described[1,2]. Initially, the proliferative stage is characterized by follicular hyperplasia and lymphohistiocytic infiltrates[1,2]. During the necrotizing stage, karyorrhexis and necrosis artifacts become evident, while the lymph node architecture remains intact[1,2]. Finally, in the xanthomatous stage, foamy histiocytes are observed as the necrotic areas regress[1,2]. Based on these stages, it can be inferred that most pediatric cases presented findings consistent with the proliferative and necrotizing phases, although this distinction was not explicitly made by the authors. Only Lin et al. classified their findings according to these phenotypes, reporting 14 patients with the proliferative type, 23 with the necrotizing type, and 1 with the xanthomatous type[19]. In summary, the histologic findings of lymph node biopsies in pediatric KFD are similar to those observed in adults.
An acute M. pneumoniae infection may have triggered the clinical presentation in our patient. Other pediatric and adult cases have also identified this infectious agent as a potential trigger[25,62,63]. Additional agents including Yersinia, Toxoplasma, EBV, human herpes virus 6 and 8, human T-lymphotropic virus type 1, and parvovirus B19 have been implicated as possible causes, though these associations remain unconfirmed [1,2]. However, the majority of reviewed cases were idiopathic.
KFD is typically a self-limiting condition unless complications arise [1,2]. Antibiotics are frequently administered prior to a definitive diagnosis, as occurred in our case [1,2]. The use of IV immunoglobulin and methylprednisolone appears justified in severe cases, such as those involving CNS complications or hemophagocytic syndrome [9,14,33,34,35,36,37,38,39]. Similarly, hydroxychloroquine has been employed in cases with concomitant SLE or those at high risk of developing it [1,12,13,15,16,18]. Nonetheless, clinical trial data remain insufficient to fully validate these therapeutic approaches.
The present case provides results consistent with an extensive literature review of reported cases. However, some articles lacked detailed descriptions of histological findings, limiting the ability to identify KFD subtypes. The absence of follow-up in certain studies may have led to an underestimation of immune-mediated diseases associated with KFD. Additionally, a lack of specific dermatological examinations in some cases has diminished the value of findings related to cutaneous manifestations.
In conclusion, KFD should be considered in the differential diagnosis of persistent fever and lymphadenopathy in pediatric patients, as cutaneous manifestations are common, often presenting as maculopapular rashes. An excisional biopsy of a lymph node is essential for a definitive diagnosis, though a skin biopsy can provide valuable diagnostic information and help identify patients at risk of developing SLE.
Sources of funding
No funding was provided for this work.
Ethics statement
The participants in this manuscript have given informed consent for publication of the details of their cases.
Data Availability
Data supporting the conclusions of this study are available upon request from the corresponding author.
Conflicts of Interest
None of the authors have any conflicts of interest in relation to this work.
References
- Perry AM, Choi SM. Kikuchi-Fujimoto Disease: A Review. Arch Pathol Lab Med. 2018 Nov;142(11):1341–6. [CrossRef]
- Masab M, Surmachevska N, Farooq H. Kikuchi-Fujimoto Disease. In Treasure Island (FL); 2024.
- Cuglievan B, Miranda RN. Kikuchi-Fujimoto disease. Blood. 2017 Feb;129(7):917.
- Kim TY, Ha K-S, Kim Y, Lee J, Lee K, Lee J. Characteristics of Kikuchi-Fujimoto disease in children compared with adults. Eur J Pediatr. 2014 Jan;173(1):111–6. [CrossRef]
- Lee BC, Patel R. Kikuchi-Fujimoto disease: a 15-year analysis at a children’s hospital in the United States. Clin Pediatr (Phila). 2013 Jan;52(1):92–5.
- Lin H-C, Su C-Y, Huang S-C. Kikuchi’s disease in Asian children. Pediatrics. 2005 Jan;115(1):e92-6. [CrossRef]
- Sierra ML, Vegas E, Blanco-González JE, GonzálezA, Martínez P, Calero MA. Kikuchi’s disease with multisystemic involvement and adverse reaction to drugs. Pediatrics. 1999 Aug;104(2):e24. [CrossRef]
- Gonzálvez Piñera J, Ruiz Cano R, García Rodríguez MR, Fernández Córdoba MS, Crusat Braña S, Sango Lamban M. [Necrotizing histiocytic lymphadenitis (Kikuchi-Fujimoto disease) in a 7-year-old girl]. Cir Pediatr. 2000 Jul;13(3):126–8.
- Kim YM, Lee YJ, Nam SO, Park SE, Kim JY, Lee EY. Hemophagocytic syndrome associated with Kikuchi’s disease. J Korean Med Sci. 2003 Aug;18(4):592–4. [CrossRef]
- Chuang C-H, Yan D-C, Chiu C-H, Huang Y-C, Lin P-Y, Chen C-J, et al. Clinical and laboratory manifestations of Kikuchi’s disease in children and differences between patients with and without prolonged fever. Pediatr Infect Dis J. 2005 Jun;24(6):551–4. [CrossRef]
- Zou CC, Zhao ZY, Liang L. Childhood Kikuchi-Fujimoto disease. Indian J Pediatr. 2009 Sep;76(9):959–62. [CrossRef]
- Al Mosawi Z, Ebrahim B, Baik S, Madan W, Aljufairi E. Kikuchi-Fujimoto Disease: Eleven Pediatric Cases and Literature Review. Arch Rheumatol. 2020 Jun;35(2):303–7. [CrossRef]
- Danai MM, Kaye SP, Gong R, McKnight H. A Rare Pediatric Case of Persistent Kikuchi-Fujimoto Disease and Underlying Systemic Lupus Erythematosus. J Clin Rheumatol Pract reports Rheum Musculoskelet Dis. 2021 Apr;27(3):e111–2. [CrossRef]
- Yang Y, Lian H, Ma H, Zhao Y, Zhang Q, Zhang L, et al. Hemophagocytic Lymphohistiocytosis Associated with Histiocytic Necrotizing Lymphadenitis: A Clinical Study of 13 Children and Literature Review. J Pediatr. 2021 Feb;229:267-274.e3. [CrossRef]
- Takahashi K, Okura Y, Shimomura M, Taniguchi K, Nawate M, Takahashi Y, et al. Development of Sjögren’s syndrome following Kikuchi-Fujimoto disease - A sibling case. Pediatr Int. 2023;65(1):e15524.
- Harrison J, Sukumaran S, Vijayan V. Systemic Lupus Erythematosus Lymphadenopathy Presenting as Kikuchi-Fujimoto Disease in an Adolescent. Vol. 15, Cureus. United States; 2023. p. e35304. [CrossRef]
- Choi S, Choi HS, Ryu YJ, Kim JY, Paik JH, Ahn S, et al. Characterization of Kikuchi-Fujimoto Disease in Children and Risk Factors Associated with Its Course. J Pediatr. 2023 Sep;260:113515. [CrossRef]
- Martins SS, Buscatti IM, Freire PS, Cavalcante EG, Sallum AM, Campos LMA, et al. [Kikuchi-Fujimoto disease prior to childhood-systemic lupus erythematosus diagnosis]. Rev Bras Reumatol. 2014;54(5):400–3. [CrossRef]
- Lin Y-C, Huang H-H, Nong B-R, Liu P-Y, Chen Y-Y, Huang Y-F, et al. Pediatric Kikuchi-Fujimoto disease: A clinicopathologic study and the therapeutic effects of hydroxychloroquine. J Microbiol Immunol Infect. 2019 Jun;52(3):395–401. [CrossRef]
- Camacho-Badilla K, Cañas-Coto A, Soriano-Fallas A, Carranza-Portocarrero A, Avila-Agüero ML. [Kikuchi-Fujimoto disease in pediatric population: a case report and a review of literature]. Gac Med Mex. 2005;141(1):53–6.
- Heldenberg D, Amar M, Ben-Arie Y, Iuchtman M. Axillary involvement in pediatric Kikuchi’s disease. Eur J Pediatr Surg Off J Austrian Assoc Pediatr Surg. [et al] = Zeitschrift fur Kinderchirurgie. 1996 Feb;6(1):32–4.
- Chiang Y-C, Chen RMY, Chao P-Z, Yang T-H, Lee F-P. Pediatric Kikuchi-Fujimoto disease masquerading as a submandibular gland tumor. Int J Pediatr Otorhinolaryngol. 2004 Jul;68(7):971–4. [CrossRef]
- Lelii M, Senatore L, Amodeo I, Pinzani R, Torretta S, Fiori S, et al. Kikuchi-Fujimoto disease in children: two case reports and a review of the literature. Ital J Pediatr. 2018 Jul;44(1):83. [CrossRef]
- Singh JM, Shermetaro CB. Kikuchi-Fujimoto Disease in Michigan: A Rare Case Report and Review of the Literature. Clin Med insights Ear, nose throat. 2019;12:1179550619828680. [CrossRef]
- Quadir A, Peacock K, Hsu P, Singh-Grewal D, Alexander S. A familial case of Kikuchi-Fujimoto disease in dizygotic twins. Pediatr Rheumatol Online J. 2020 Aug;18(1):62. [CrossRef]
- Kim L, Tatarina-Numlan O, Yin YD, John M, Sundaram R. A Case of Kikuchi-Fujimoto Disease in a 7-Year-Old African American Patient: A Case Report and Review of Literature. Am J Case Rep. 2020 Aug;21:e922784. [CrossRef]
- Cannon L, Wang E, Becker M. Diagnosis of Kikuchi-Fujimoto disease in an 11-year-old girl with fever and sickle cell disease. BMJ Case Rep. 2020 Aug;13(8). [CrossRef]
- Chisholm KM, Bohling SD, Tsuchiya KD, Paulson VA. A Malignant Mimicker: Features of Kikuchi-Fujimoto Disease in the Pediatric Population. Pediatr Dev Pathol Off J Soc Pediatr Pathol Paediatr Pathol Soc. 2022;25(5):538–47. [CrossRef]
- Burns J, Pathania S, Griesser R, Norelli J, Gilgeours K, Tugetman J, et al. Evaluation of a unilateral neck mass in a 16-year-old female: Kikuchi-Fujimoto disease with superimposed bacterial lymphadenitis. Vol. 8, SAGE open medical case reports. England; 2020. p. 2050313X20962640. [CrossRef]
- Park HS, Sung MJ, Park SE, Lim YT. Kikuchi-Fujimoto disease of 16 children in a single center of Korea. Pediatr allergy Immunol Off Publ Eur Soc Pediatr Allergy Immunol. 2007 Mar;18(2):174–8. [CrossRef]
- Gómez C, Eraso RM, Aguirre CA, Pérez MDP. [Kikuchi-Fujimoto disease: pediatric case presentation]. Biomedica. 2010;30(4):465–72.
- Ojeda Lewis E, Vásquez Paz H. Kikuchi-Fujimoto disease: pediatric case report. Medwave. 2015 Sep;15(8):e6270.
- Chen JS, Chang KC, Cheng CN, Tsai WH, Su IJ. Childhood hemophagocytic syndrome associated with Kikuchi’s disease. Vol. 85, Haematologica. Italy; 2000. p. 998–1000.
- Jun-Fen F, Chun-Lin W, Li L, Dayan C, Guan-Ping D, Fang H. Kikuchi-Fujimoto disease manifesting as recurrent thrombocytopenia and Mobitz type II atrioventricular block in a 7-year-old girl: a case report and analysis of 138 Chinese childhood Kikuchi-Fujimoto cases with 10 years of follow-up in 97 patients. Acta Paediatr. 2007 Dec;96(12):1844–7. [CrossRef]
- Altinel Açoğlu E, Sari E, Şahin G, Oğuz MM, Akçaboy M, Zorlu P, et al. Kikuchi-Fujimoto disease triggered by Salmonella enteritidis in a child with concurrent auto-immune thyroiditis and papilloedema. Paediatr Int Child Health. 2018 Nov;38(4):298–301.
- Bao S, Huang H, Jin Y, Ding F, Yang Z, Xu X, et al. Optic Neuritis in a Pediatric Patient with Kikuchi-Fujimoto Disease: A Case Report and Review of the Literature. Vol. 17, Journal of inflammation research. New Zealand; 2024. p. 2889–95. [CrossRef]
- Guleria S, Gupta A, Pilania RK, Pandiarajan V, Rawat A, Saikia UN, et al. Kikuchi-Fujimoto Disease: An Under Recognized Cause of Fever with Lymphadenopathy. Vol. 87, Indian journal of pediatrics. India; 2020. p. 85. [CrossRef]
- Hua C-Z, Chen Y-K, Chen S-Z, Gu W-Z, Shu Q. Histiocytic Necrotizing Lymphadenitis Mimicking Acute Appendicitis in a Child: A Case Report. Vol. 9, Frontiers in pediatrics. Switzerland; 2021. p. 682738. [CrossRef]
- Chowdhury SR. Extra-nodal Kikuchi Disease and Kikuchi Encephalitis. Vol. 56, Indian pediatrics. India; 2019. p. 881–2.
- Gonçalves LF, Debelenko L V, Bhambhani KJ, Scheid A, Altinok D. Histiocytic necrotizing lymphadenitis (Kikuchi-Fujimoto disease) with CNS involvement in a child. Pediatr Radiol. 2014 Feb;44(2):234–8. [CrossRef]
- Sykes JA, Badizadegan K, Gordon P, Sokol D, Escoto M, Ten I, et al. Simultaneous Acquired Self-limited Hemophagocytic Lymphohistiocytosis and Kikuchi Necrotizing Lymphadenitis in a 16-Year-Old Teenage Girl: A Case Report and Review of the Literature. Pediatr Emerg Care. 2016 Nov;32(11):792–8.
- Emir S, Gögüş S, Güler E, Büyükpamukçu M. Kikuchi-Fujimoto disease (histiocytic necrotizing lymphadenitis) confused with lymphoma in a child. Med Pediatr Oncol. 2001 Dec;37(6):546–8. [CrossRef]
- Tchidjou HK, Macchiaiolo M, Ariganello P, Carducci FC, De Vito R, De Benedetti F, et al. Kikuchi-Fujimoto disease in patient with systemic phacomatosis pigmentovascularis. Blood Coagul fibrinolysis an Int J Haemost Thromb. 2014 Oct;25(7):783–5. [CrossRef]
- Rossetti E, Appierto L, Bianchi R, Picardo S. Kikuchi-Fujimoto disease and life-threatening upper airway obstruction. Vol. 25, Paediatric anaesthesia. France; 2015. p. 864–5.
- Handa A, Nozaki T, Hosoya Y, Sakoda A, Suzuki K. Multiple migratory recurrence of Kikuchi-Fujimoto disease. Pediatr Int. 2016 Dec;58(12):1360–2. [CrossRef]
- Arslan A, Kraus CL, Izbudak I. Optic Neuritis as an Isolated Presentation of Kikuchi–Fujimoto Disease in a Pediatric Patient. Vol. 37, Balkan medical journal. Turkey; 2020. p. 172–3. [CrossRef]
- Öztürk N, Kılıç İ, Göçün PU, Kaya Z. Kikuchi-Fujimoto disease in a child who had a high suspicion of COVID-19 infection. J Hematop. 2022 Sep;15(3):197–8. [CrossRef]
- Sevrin F, Beaujot J, Jaillard A, Fayard C, Forestier A, Defachelles A-S. Kikuchi-Fujimoto disease following SARS-CoV-2 vaccination in a patient with previous history of rhabdomyosarcoma. Pediatric blood & cancer. United States; 2023. p. e30345.
- Zhou Y, Shu S. Histiocytic necrotizing lymphadenitis with autoimmune encephalitis in a child: a case report. Transl Pediatr. 2024 Oct;13(10):1892–8. [CrossRef]
- Lu ES, Hoyek S, Yuan M, El Khatib BA, Gonzalez E, Rothermel H, et al. Occlusive Retinal Vasculitis in a Pediatric Patient With Kikuchi-Fujimoto Disease and Sickle Cell Trait. Ophthalmic Surg Lasers Imaging Retina. 2024 Apr;55(4):235–9. [CrossRef]
- Das A, Bhave SJ, Pal B, Arun I, Goel G, Bhattacharya S, et al. Brucellosis Complicated by Kikuchi-Fujimoto Disease and Doxycycline-Induced Intracranial Hypertension. Vol. 86, Indian journal of pediatrics. India; 2019. p. 1063–4. [CrossRef]
- Abdu A, Pajkrt D, Bijker EM. Kikuchi Disease in Children: Case Report and Review of the Literature. Pediatr Infect Dis J. 2022 Mar;41(3):199–204.
- Seo J-H, Lee JS, Lee E-J, Lee J-H, Kim JP, Woo SH, et al. Comparison of clinical features and EBV expression in histiocytic necrotizing lymphadenitis of children and adults. Int J Pediatr Otorhinolaryngol. 2014 May;78(5):748–52. [CrossRef]
- Yen H-R, Lin P-Y, Chuang W-Y, Chang M-L, Chiu C-H. Skin manifestations of Kikuchi-Fujimoto disease: case report and review. Eur J Pediatr. 2004 Apr;163(4–5):210–3. [CrossRef]
- Yasukawa K, Matsumura T, Sato-Matsumura KC, Takahashi T, Fujioka Y, Kobayashi H, et al. Kikuchi’s disease and the skin: case report and review of the literature. Br J Dermatol. 2001 Apr;144(4):885–9. [CrossRef]
- Kim KJ, Jee MS, Chang SE, Choi JH, Sung KJ, Moon KC, et al. Kikuchi-Fujimoto disease with papulopustular skin manifestations. Clin Exp Dermatol. 2003 Mar;28(2):142–4. [CrossRef]
- Spies J, Foucar K, Thompson CT, LeBoit PE. The histopathology of cutaneous lesions of Kikuchi’s disease (necrotizing lymphadenitis): a report of five cases. Am J Surg Pathol. 1999 Sep;23(9):1040–7.
- Paradela S, Lorenzo J, Martínez-Gómez W, Yebra-Pimentel T, Valbuena L, Fonseca E. Interface dermatitis in skin lesions of Kikuchi-Fujimoto’s disease: a histopathological marker of evolution into systemic lupus erythematosus? Lupus. 2008 Dec;17(12):1127–35. [CrossRef]
- Frankel AM, Frenkel S, Aminlari A, Chan T. Kikuchi Disease: A Case Report. J Emerg Med. 2020 Dec;59(6):927–30. [CrossRef]
- Yen A, Fearneyhough P, Raimer SS, Hudnall SD. EBV-associated Kikuchi’s histiocytic necrotizing lymphadenitis with cutaneous manifestations. J Am Acad Dermatol. 1997 Feb;36(2 Pt 2):342–6. [CrossRef]
- Kuo TT. Kikuchi’s disease (histiocytic necrotizing lymphadenitis). A clinicopathologic study of 79 cases with an analysis of histologic subtypes, immunohistology, and DNA ploidy. Am J Surg Pathol. 1995 Jul;19(7):798–809. [CrossRef]
- Yu R-B, Chen Y-J, Chang C-H, Chen Y-L, Chen J-W. Kikuchi-Fujimoto Disease Associated With Mycoplasma Pneumoniae Infection. Ear Nose Throat J. 2024 Apr;103(4):NP223–5. [CrossRef]
- Müller CSL, Vogt T, Becker SL. Kikuchi-Fujimoto Disease Triggered by Systemic Lupus Erythematosus and Mycoplasma pneumoniae Infection-A Report of a Case and a Review of the Literature. Am J Dermatopathol. 2021 Mar;43(3):202–8. [CrossRef]
Figure 1.
Cutaneous manifestations. A: Onset of the cutaneous eruption, characterized by erosive lesions on erythematoedematous plaques distributed in the centrofacial area and auricular lobes. B: Resolution of the erythematoedematous component, persistence of ulcers and crusts. C: One week after hospital discharge, progressive remission and re-epithelialization of the erosions. D: One month after hospital discharge, showing residual marks of the rash resembling varioliform scars.
Figure 1.
Cutaneous manifestations. A: Onset of the cutaneous eruption, characterized by erosive lesions on erythematoedematous plaques distributed in the centrofacial area and auricular lobes. B: Resolution of the erythematoedematous component, persistence of ulcers and crusts. C: One week after hospital discharge, progressive remission and re-epithelialization of the erosions. D: One month after hospital discharge, showing residual marks of the rash resembling varioliform scars.
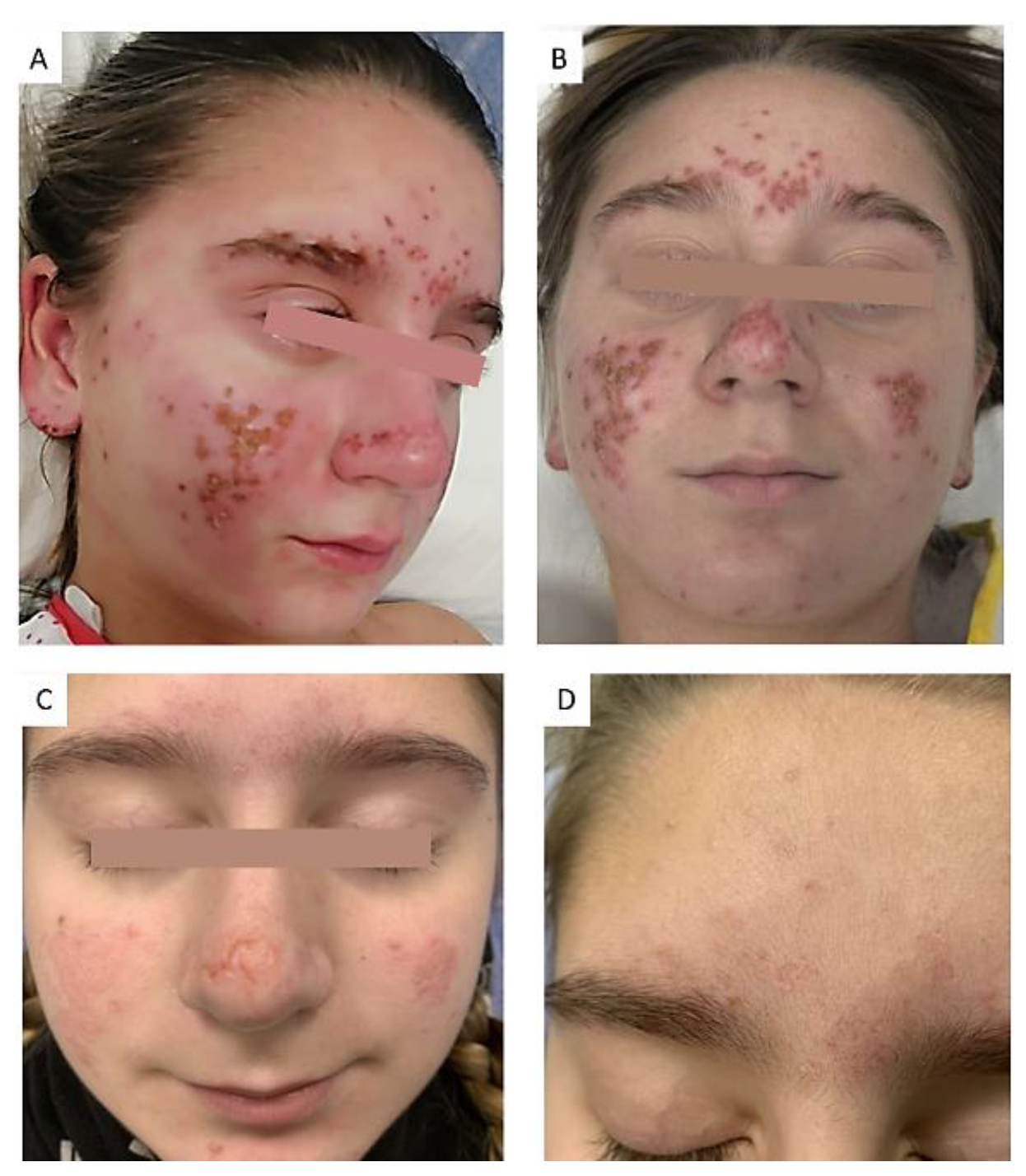
Figure 2.
Histopathology. A. Hematoxylin and eosin (H&E) stain: Normal lymphoid node population in the left half, with areas of paracortical necrosis. Extensive necrosis is observed in the right half. B. H&E: Area of central necrosis lacking polymorphonuclear cells (asterisk), flanked by an infiltrate rich in immunoblasts, plasmacytoid dendritic cells, and histiocytes (arrowheads), without forming organized granulomas. Nuclear debris (white circles) is present within the necrotic area. C. Immunohistochemistry (IHC): CD123 expression in plasmacytoid dendritic cells surrounding the areas of necrosis.
Figure 2.
Histopathology. A. Hematoxylin and eosin (H&E) stain: Normal lymphoid node population in the left half, with areas of paracortical necrosis. Extensive necrosis is observed in the right half. B. H&E: Area of central necrosis lacking polymorphonuclear cells (asterisk), flanked by an infiltrate rich in immunoblasts, plasmacytoid dendritic cells, and histiocytes (arrowheads), without forming organized granulomas. Nuclear debris (white circles) is present within the necrotic area. C. Immunohistochemistry (IHC): CD123 expression in plasmacytoid dendritic cells surrounding the areas of necrosis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



