Submitted:
31 December 2024
Posted:
03 January 2025
You are already at the latest version
Abstract
Background. In the aftermath of perinatal loss, the physiological onset of lactation presents a complex array of emotional responses for women, including grief and despair. Effective lactation management is essential for maternal health, yet it is often inadequately ad-dressed by healthcare professionals, potentially compromising the physical and psy-chological recovery of the bereaved mother. Aim. The aim of this study is to investigate how Italian HCPs support mothers in managing lactation after a perinatal loss. Methods. This study is web-based and cross sectional. HCPs involved in perinatal bereavement care were asked to answer a survey consisting of three areas: sociodemographic information, knowledge and experience about perinatal loss and about lactation after perinatal loss. Findings. In this study, 1,227 healthcare professionals participated. A significant majority, 60.2%, had received formal training on perinatal loss care, expressing high satisfaction with an average score of 4.7 out of 5. However, less than half, at 42.5%, reported having a protocol for bereavement care in their workplace. A notable 25% of the respondents did not provide lactation information when possible. Discussions predominantly centred on pharmacological suppression of lactation in cases of stillbirth (89.5%) and neonatal death (83.8%), as well as complications associated with these events. Post-discharge follow-up was reported as lacking by 78.2% of the sample. Conclusion. The discrepancy between HCPs' training and their practice reveals a critical need for enhancing the implementation of bereavement care protocols and follow-up support, reflecting the importance of inte-grating lactation management into the perinatal loss care continuum.
Keywords:
lactation
; midwives
; bereavement
; management
1. Introduction
Perinatal death is an acknowledged global burden that affects millions of families every year [1,2]. In Italy, around 4 babies every 1000 are stillborn or die within a week from childbirth, with a great rate of variability between northern and southern regions [3]. This event has a huge impact on parents’ psychological wellbeing with several long-term consequences, such as post-traumatic stress symptoms, anxiety and depression [4]. In such a situation, mothers have to manage the initial onset of their lactation which could be very demanding and challenging to deal with [5].
In this setting, healthcare professionals (HCPs) play a pivotal role in helping mothers to manage lactation after a perinatal loss. Respectful care could actually improve the possibility that lactation itself will have a positive impact on the grieving process. Unfortunately, literature underlines how lactation care, received by mothers, is often insufficient and not tailored to their needs [5]. This aspect is usually neglected by HCPs and it often receives poor attention within guidelines for perinatal bereavement care [6]. Concerning Italy, recommendations about care around stillbirth have only recently been published [7]. However, no formal guidelines are actually available to support HCPs during clinical practice. In particular, few indications are given about lactation: prompt milk suppression or milk donation is advised, without other recommendations for HCPs.
Lactogenesis is a physiological process of pregnancy and the post-partum period which starts at 16 weeks of pregnancy. International guidelines stipulate that all bereaved mothers should be offered lactation support and written information about the available options [6,8]. Beyond its biological role, breastfeeding carries more than a nutritional significance within the dyad of mother and child. It can assume several meanings, like the expression of maternal love and of the emotional bonding with the baby; it may also represent self-empowerment and agency for women, and an invaluable essential life support for premature babies. Breastfeeding is actually linked to the new identity as a mother and, for some bereaved mothers, it may represent an emotional connection with the deceased baby [9,10]. Considering such psychological and relational implications, it shouldn’t be given for granted that mothers’ best option after perinatal loss is immediate milk suppression. Other options, such as milk donation [10] or non-pharmacological suppression, could fit more with mothers’ needs than other paths [11]. Furthermore, literature underlines several health benefits given by an extended breastfeeding, including its influence on perinatal depression [12] which has a high incidence on mothers with previous losses [13], also influencing subsequent pregnancies [14].
As previously mentioned, HCPs involved in bereavement care often overlook the topic of lactation after perinatal loss [5,10]. This may be due to a lack of knowledge about this specific issue and the commonly held belief among HCPs that pharmacological suppression of lactation is the best course of action for the well-being of all mothers [10,15]. Many HCPs are not adequately trained to provide support to parents experiencing perinatal loss [16]: the lack of formal training is more likely to increase the risk of burnout syndrome [17] and post-traumatic stress disorder (PTSD) symptoms [18]. HCPs with burnout symptoms may exhibit less empathy towards patients and provide impaired emotional support and care [19]. Specifically, the burnout dimension of emotional exhaustion can lead to an emotional disinvestment that may hamper the proper shared decision making process in bereavement care .
The LISTEN (Lactation Support afTer pEriNatal loss) study aims to investigate the knowledge, thoughts, feelings, and experiences of Italian HCPs who are specifically involved in lactation care after perinatal loss. The objective of this research is to enhance our knowledge and understanding of this topic, in order to help HCPs in assisting mothers in the difficult issue of managing lactation after a perinatal loss.
2. Materials and Methods
The LISTEN study was an anonymous web-based, mixed methods and cross sectional study hosted on the Qualtrics platform (www.qualtrics.com) provided by Florence University PeaRL laboratory and was distributed through the online channels of CiaoLapo Foundation, an Italian charity for perinatal loss support, from January to December 2023, in collaboration with several Italian hospitals. All data were collected and analysed anonymously.
Participants were considered eligible to complete the survey if they were healthcare professionals involved in bereavement care after a perinatal loss. The survey was voluntary and anonymous, no personal data were recorded, in no way it was possible to identify the single respondents. Informed consent was provided at the start of the survey once participants had read the participant information and met the eligibility criteria.
The survey consisted of questions across several key areas including: (1) Sociodemographic information; (2) knowledge and experience about perinatal loss; (3) knowledge and experience about lactation after perinatal loss.
2.1. Statistical Analysis and Data Presentation
Survey responses were downloaded and extracted from the online survey tool Qualtrics, and imported into Stata BE 18 (StataCorp) for statistical analysis. Incomplete records were excluded, and descriptive statistics were used to analyse quantitative data. Categorical data were reported as frequencies and percentages and compared using the chi-squared test, whereas continuous data were reported as mean values with standard deviations (SD) or as median [quartiles] and compared using t-test or Kruskall Wallis and Mann Witney test. All results were considered to be statistically significant at p<0.05. A mixed-method analysis was conducted on open-end questions with the help of Artificial Intelligence as described by Ravaldi et al. (2023) [20], then themes and categories were classified using MAXQDA 2018 to identify negative aspects of clinical and care management. Graphs were plotted using Tableau Desktop 2023.3 (Tableau Software, LLC) or Stata BE 18 (StataCorp).
3. Results
3.1. Sample Characteristics
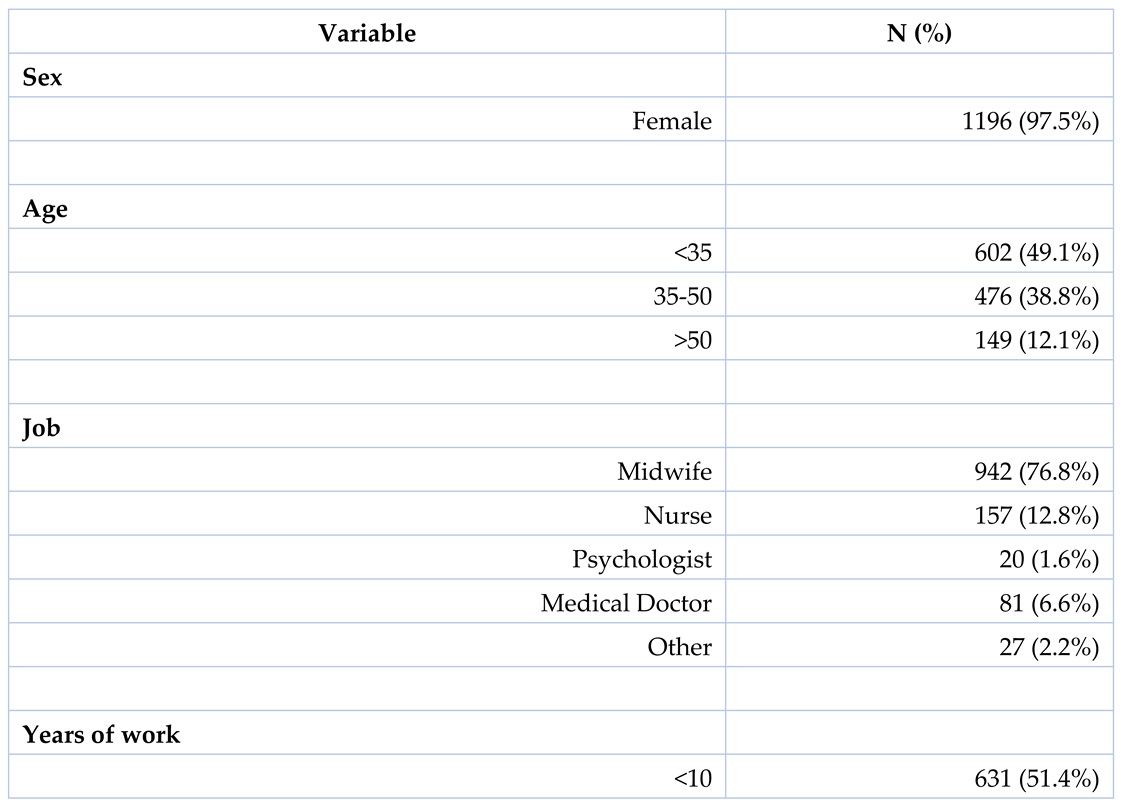
A total of 1227 HCPs participated in this study, with the majority being women (97.5%). The largest group consisted of midwives (76.8%). More than half of the participants had less than 10 years of work experience (51.4%). The majority of HCPs worked in public hospitals (80.2%), particularly in birth rooms (56.9%) and maternity wards (43.1%). Table 1 provides a detailed overview of the participants’ demographic and professional characteristics.
3.2. Perinatal Loss Management
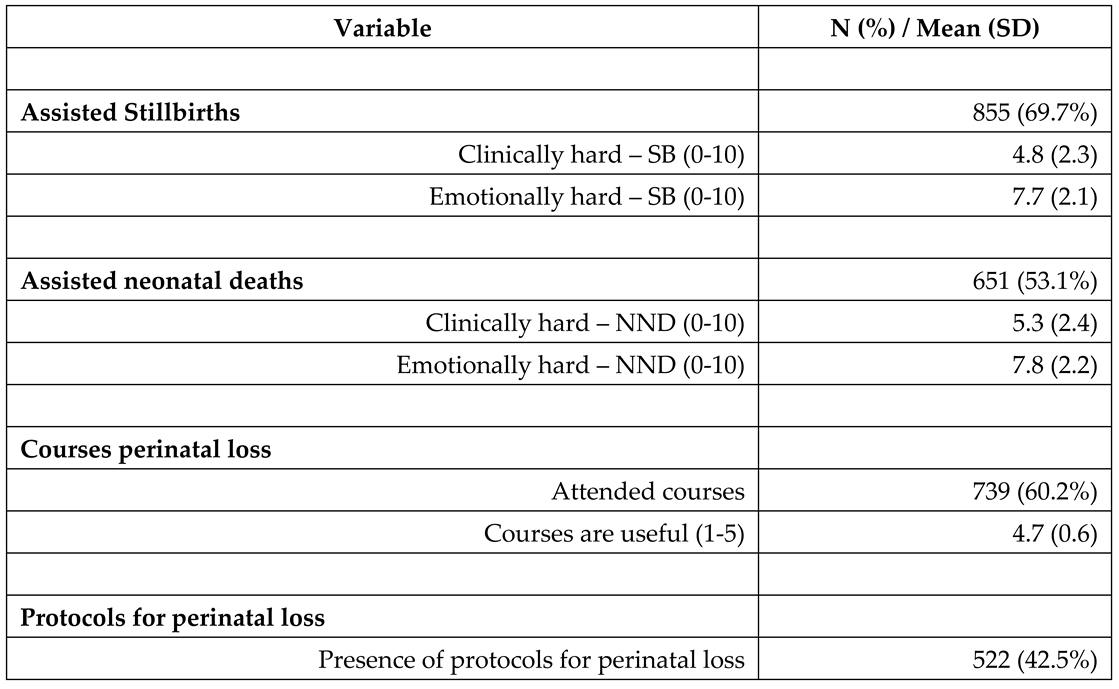
More than half of the participants reported having assisted in cases of stillbirths (69.7%) and neonatal deaths (53.1%). Additionally, 60.2% of the respondents had attended specialised formal training on perinatal loss. Based on our findings, such training was highly valued; it received an average usefulness rating of 4.7 on a Likert-type scale ranging from 1 (not useful at all) to 5 (extremely useful), as detailed in Table 2.
In our study, only 42.5% of HCPs reported the presence of a perinatal loss care protocol in their workplace and 31.5% indicated the existence of a formalised support pathway for parents’ psychological care. Regarding the implementation period of these protocols, 23.2% of the respondents reported their implementation within the last five years, 43.5% reported their establishment over five years ago, and the remaining 33.3% were unaware of the timeframe. The HCPs in our study emphasised the usefulness of having a protocol on bereavement care after a perinatal loss, assigning a high score of 4.8 on a Likert-type scale ranging from 1 (not useful at all) to 5 (extremely useful) (Table 2).
HCPs were asked to rate their difficulties in the emotional and clinical management of perinatal loss on a Likert-type scale, ranging from 0 (“not difficult at all”) to 10 (“extremely difficult”). While emotional involvement in the two cases was comparable and higher than clinical one, clinical management of neonatal death was considered more challenging than stillbirth (5.3±0.1 vs 4.9±0.1, p<0.01) (Figure 1, panel A).
We also investigated whether attending specific courses or working in settings with specific protocols had any impact on the difficulty ratings. However, our findings did not reveal a significant difference in difficulty ratings between HCPs who had received specific training or worked in settings with protocols. It is important to note that there was a slight decrease in emotional difficulty reported by HCPs with specific training in stillbirth management, although the statistical significance was only borderline (4.7±0.1 vs 5.1±0.1, p=0.05).
3.3. Information on Lactation After Perinatal Loss
We also examined HCPs training in lactation suppression techniques. Participants were asked to self-report their training on a Likert-type scale ranging from 1 (“not trained at all”) to 5 (“very trained”), with a mean score of 2.7 (SD 1.0). Additionally, they were asked to rank the degree of usefulness for various interventions in lactation management on a scale from 0 (“not useful at all”) to 10 (“very useful”). All treatments were considered moderately effective (mean 5.2 SD 3.2), with hand expressing considered slightly more effective than the others (mean 6.5 SD 2.9, p<0.01) and tight bandages considered less effective (mean 3.7 SD 3.1, p<0.01) (Figure 1, panel B).
In our research on lactation information provided to mothers, all professionals agreed on the importance of educating women about managing lactation following a perinatal loss. This was reflected in a high average rating (mean 4.7, SD 0.6, range 1-5). However, we founded that approximately 25% of professionals, despite having the opportunity, did not provide this information to parents (Table 3). Additionally, around 10% were unsure of what information to convey, and a similar proportion (9.6% following stillbirth and 8.4% after neonatal death, totaling 78 healthcare professionals) did not consider providing lactation guidance as part of their professional responsibilities. When considering their roles, we observed that those who viewed lactation counselling as outside their professional domain were more likely to be medical doctors (13.6% of them considered it not their duty to provide information on lactation) or psychologists (10.0%), and less likely to be nurses (7.6%) or midwives (5.6%; p<0.05).
We also examined the significance of clear communication and the appropriate timing for discussing lactation with healthcare professionals dealing with stillbirth. Our respondents were asked to specify the most suitable time and the majority of them (64.7%) believed that the optimal approach was to share this information within 24 hours of childbirth. Additionally, 10.4% of HCPs chose to provide these details immediately after birth, while 7.8% offered lactation management information only upon the mother’s explicit request (Table 3).
Regarding the nature of information typically provided by respondents, pharmacological suppression of lactation was a common topic, mentioned by 89.5% of participants in the context of stillbirth and 83.8% in cases of neonatal death. Additionally, complications like mastitis or leaking milk were frequently addressed, with 62.9% of respondents discussing these after stillbirth and 62.1% following neonatal death. General information about lactation was also commonly shared (as illustrated in Figure 2, panel A and B). However, the topic of milk donation was less frequently discussed, with only 21.8% of respondents providing information on this subject after stillbirth and 25.4% after neonatal death.
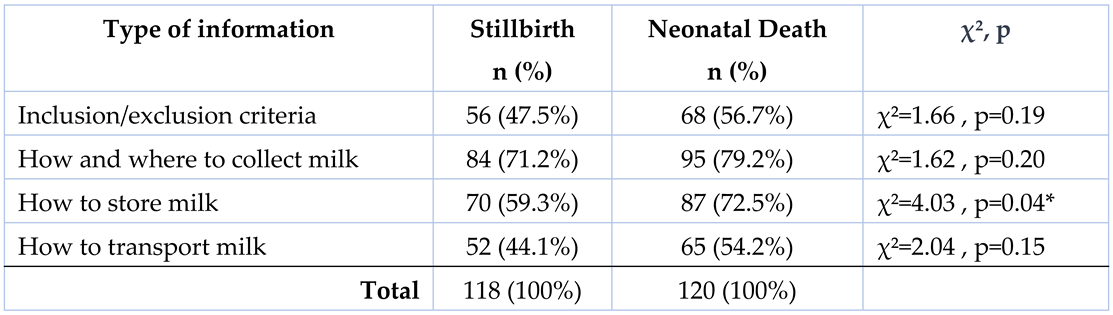
Table 4 shows that HCPs tended to give more information on milk donation to parents after neonatal death than after stillbirth, in particular regarding milk conservation (p<0.05).
Generally, written information on lactation management was lacking in discharge materials. Only 15.8% of healthcare professionals provided information through leaflets, although they were deemed to be quite useful (mean 3.9, SD 0.9 on a scale of 1-5).
Figure 2 (panel C) displays a map with stars marking the locations of human milk banks (HMBs) across Italy. Regions shaded in blue represent the highest percentage of healthcare professionals who provided information about milk management, while those in red represent the lowest percentage (percentages were calculated exclusively from respondents who had the opportunity to offer such information). The findings reveal an absence of a significant correlation (Rsq=0.01; p=0.87) between the presence of a local HMB and the likelihood of healthcare professionals providing information on this topic.
3.4. Follow Up and Outpatient Services
Regarding follow-up programs, 267 healthcare professionals (21.8%) indicated that their facility offered a formal care pathway to support women post-discharge. Among these, 99 (37.1%) reported that women commonly brought up lactation management concerns during follow-up visits. The most frequently mentioned issues were emotional difficulties (35.6%), breast engorgement (16.9%), challenges with pharmacological lactation suppression (14.2%), non-pharmacological lactation suppression (6.7%), and mastitis (4.1%). Additionally, a mere 28.1% of healthcare professionals reported the existence of dedicated outpatients service in their local community aimed at assisting parents with lactation concerns following a perinatal loss.
3.5. Open-Ended Questions
The majority of healthcare professionals, accounting for 76.2%, contributed to open-ended questions, sharing insights into the most challenging facets of bereavement care concerning stillbirth and neonatal death. We identified several principal themes through the frequency of their mention (m) and assigned a normalised score (s) on a scale from 0 to 10:
- Communication (m 66 / s 8.6): emerged as a fundamental aspect, underscoring the vital role of effective, empathetic communication in navigating the delicate circumstances surrounding perinatal loss. Its high frequency and score indicated its paramount importance in providing sensitive and supportive care.
- Finding the right words (m 60 / s 7.4): this theme, with its significant score, highlighted the profound challenge healthcare professionals faced in articulating comfort and empathy. It reflected the intricacy of verbalising support in a way that acknowledged the immense grief while offering solace.
- Empathy (m 39 / s 5.9): A critical component, illustrating the need for healthcare providers to connect emotionally and understand the depth of the parents’ loss, while maintaining professional boundaries.
- Pain (m 30 / s 4.5): Captured both the physical anguish of the mother and the emotional suffering of all involved. This theme’s notable presence in the responses underscored the pervasive impact of grief and loss in these scenarios.
- Helplessness/Impotence (m 25 / s 3.8): Reflected a sense of powerlessness often felt by professionals in the face of such profound loss, impacting their sense of efficacy and contributing to emotional strain.
- Bureaucracy (m 13 / s 2.3): Particularly highlighted in stillbirths, this theme points to the complexities and challenges of navigating administrative procedures during emotionally charged times, adding another layer of difficulty to the care process.
- Not crying (m 9 / s 2.7): More pronounced in stillbirths, it signifies the struggle of healthcare professionals to manage their own emotional responses in a professional setting, illustrating the personal impact of these events.
- Silence (m 8 / s 1.7): Unique to stillbirths, this theme encompassed the literal absence of the newborn’s sounds and the broader societal reticence surrounding stillbirths. It may symbolise the profound depth of loss and the emotional complexities entwined in providing care.
4. Discussion
It is widely known that perinatal loss has a huge impact on parents’ psychological wellbeing [21]. In the last twenty years, literature has deepened the knowledge about the emotional burden of HCPs who are at the forefront of perinatal bereavement care [17,18,22,23,24]. Frustration, impotence, guilt and sense of personal failure are among the most common emotions experienced by HCPs [22,23,24]. Our results confirmed this emotional difficulty to face bereavement care during both prenatal and neonatal period:
“I didn’t feel up to the task of caring for the couples in such a very delicate and intimate moment for them”.A young midwife
Emotional issues could have hampered HCPs’ attitude for training on bereavement care. A sense of personal failures, as described above, could play a key role in developing burnout syndrome which is linked to a decrease in professionalism and personal job investment [25]. HCPs’ strain in dealing with their own emotions should be acknowledged, due to the essential part played by their emotional experience in caring for parents after a loss. Professional knowledge and care cannot be separated from such aspects. In a study conducted by McCreight (2005) [24] semi-structured in-depth interviews, with a narrative frame, were carried out with nurses: during the interviews, the emotional impact on nurses of perinatal loss strongly emerged, allowing nurses to consider their emotions a resource in their clinical practice. Scheduled debriefing appointments with staff, based on a narrative approach, could be used to improve HCPs’ self understanding. Considering the high emotional impact on staff that care for grieving parents, this strategy could make emotional experience functional to clinical practice itself and not a barrier. Furthermore, our data have shown emotional difficulty was lower in HCPs with a specific training in perinatal loss bereavement care, while assisting stillbirth. Although the statistical significance of the result was borderline, previous researchers point out the positive correlation between specific training and HCPs’ psychological wellbeing [17,18]. In this sense, training could be considered a protective factor.
More than half of respondents pointed up the absence of a formal protocol around perinatal bereavement care in their workplace. This is a crucial point, as highlighted in the CLASS study [26]: adherence to international standards is linked to a greater satisfaction of care and, more importantly, to lower grief and post-traumatic stress symptoms in bereaved parents. The stigma around perinatal death [27], the lack of formal training around this topic [16,28,29], and the fact that Italian recommendations on stillbirth management were only recently published [7], could explain the embarrassing delay of our country in adopting national bereavement care pathways. However, the respondents were aware and agreed to the pivotal role of having a protocol and a formal training to guarantee respectful and tailored care:
“Staff training is essential and [care] should not be left to chance or rely on personal empathy in difficult situations such as the puerperium period or the management of lactation of a woman who suffered a perinatal loss.”A nurse
Vocational training for HCPs usually gives priority to academic knowledge overshadowing the relational and communication skills [30]. Considering this issue and the HCPs’ needs, hospitals decision makers should offer a formal training about perinatal bereavement care including specific aspects such as the management of lactation after a loss.
Getting to the heart of the LISTEN study, HCPs in our sample deemed themselves to have a very poor training about lactation suppression techniques. This situation could explain that a quarter of the sample didn’t give any information about lactation management after a perinatal loss as well as those that didn’t know what to say to parents about this topic or thought that it wasn’t on their duties. Furthermore, this lack of knowledge could clarify why some non-pharmacological interventions to suppress lactation were considered useful, at least to some degree, even if they are known to be harmful. For instance, it has been demonstrated, for many years, that breast binding, ice packs, or analgesics could cause breast engorgement and pain [31,32]. It’s essential to underline that if women are uninformed about their options an informed choice and shared decision making process can’t be guaranteed. Although the Italian recommendations about stillbirth are recent and they report poor information about lactation management, international guidelines agree on the significant role played by this aspect within bereavement care [8,11,33,34]. The Perinatal Society of Australia and New Zealand [8] underlines that giving information about lactation is a critical point due to the emotional value carried by breastfeeding [35]. Moreover, some women could not be aware that milk production starts even when a baby is stillborn. This unexpected event required very sensitive care from HCPs.
Concerning information about suppression, every woman should have the possibility to decide the best way of action with her HCPs. Non-pharmacological options [11,33,34] should be offered as well as milk donation. This last option was taken a few times into account by our sample, although literature shows the undoubted benefits for some women who choose this option [36]. Our data underlines that HCPs were more likely to give information about milk donation after a neonatal death than a stillbirth. This result could be explained by the fact that mothers with a baby hospitalised in a neonatal intensive care unit usually have already started to pump milk. It could be possible that in such a situation HCPs feel more comfortable to talk about this topic than after a stillbirth. As mentioned before, the grief process is very individual and unique: for this reason, HCPs should promote a shared decision making approach on milk management [11,15,37] with the aim to empower women during their grieving process. This aspect was well explain by a midwife of our sample who usually give information about milk donation:
“I believe it is right that a couple has to know every option. Grieving parents could decide to transform what they have into a gift for other families.”A midwife
An interesting fact is that HCPs usually give more information about lactation suppression or management after a stillbirth than after a neonatal death. This data could be explained by two factors. On the one hand, the absence of a dedicated midwife who supports mothers in the neonatal intensive care unit (NICU) during the hospitalisation of their baby and after the death. On the other hand, the poor support given to mothers to manage lactation in NICU by nurses. This latter hypothesis is confirmed by literature which shows the lack of effective lactation support in this context [38].
Additionally, Italy is known for having a significant number of HMBs, which is the highest in Europe [39], indicating a strong commitment to neonatal care. However, our research suggested that there is a discrepancy between the presence of HMBs and the level of information provided to parents who have experienced the loss of a child. This finding implies that the main barriers may be related to cultural issues and a lack of knowledge about this topic, rather than a shortage of services. It is known that there are noticeable differences in the quality of services between different regions in Italy: southern regions tend to have lower quality services compared to the central and northern regions [26]. These differences could be attributed to cultural factors within the healthcare community. However, it is worth noting that Sardinia, which is typically similar to the southern regions in terms of healthcare performance, stands out by providing high levels of lactation information despite the absence of HMBs. This exception indicates the need for a cultural shift in healthcare practices to improve bereavement care throughout Italy.
As mentioned before, another issue about lactation management is the possible complications which can appear after both pharmacological and non-pharmacological suppression [6]. This aspect was witnessed by our sample who encountered complications, such as breast engorgement, during follow-up visits. For this reason, women should be informed face to face about this possibility by HCPs and written information should be given [8,11,33,34]. Generic information about this topic could be distressing for grieving mothers, so tailored written materials should be created [8]. Moreover, such information should include pros and cons of every strategy of lactation suppression and, when possible, what to do in case of complications [6]. Receiving proper and specific information is a key aspect of bereavement care [8,40] which allows mothers to make an informed decision without being forced toward a decision taken by others. Furthermore, an informed decision could prevent physical and emotional complications linked to milk management.
Concerning the more appropriate timing for informing mothers about their options of lactation management, guidelines of the Ireland Health Service Executive encourage giving such information right after the diagnosis to facilitate informed decision making [11]. In addition, a lactation specialist consultation is advisable [8]. Our respondents usually give such information within 24 hours from childbirth and a little, but not insignificance, part of them talked about this topic only if a mother specifically asks about it. Moreover, a period of time of 24 hours (from childbirth to discharge) gives HCPs an excessive margin of discretion in deciding the most appropriate moment to inform mothers. In this sense, informing mothers about their options right after the diagnosis allows them to have as much time as possible to make a decision, considering that drugs for suppression should be taken within 24 hours from childbirth [11].
Qualitative analysis on HCPs words offered valuable insights into the nuanced challenges faced in the context of stillbirths and neonatal deaths, confirming the quantitative data shown above. Difficulties in communication and providing comfort highlighted the delicate role of offering solace in the midst of profound grief. Additionally, “navigating bureaucracy” emerged as a significant challenge, emphasising the administrative hurdles added to the emotional burden. Managing personal emotions was another critical aspect: impotence was the main feelings expressed by HCPs which could impair the care provided to parents. These quotes and themes collectively underscore the multifaceted nature of the challenges in perinatal care. They illuminate the need for targeted training and support for healthcare professionals, not only in clinical skills but also in emotional intelligence, communication, and administrative competencies. This holistic approach is vital in ensuring that healthcare providers are equipped to handle these complex situations with sensitivity, empathy, and effectiveness.
In the end, this study showed the inadequacy of both the follow-up programs and the knowledge of our sample about these programs, when available. Again, all the major international guidelines about perinatal bereavement care agree about the pivotal role played by continuity of care [8,11,33,34]. Salgado et al. (2021) shows how continuity of care is an essential part of the “Perinatal bereavement safety thermometer” which highlights ten important aspects that actively impact on maternal psychological wellbeing and grieving process [41]. Further, couples who experience a perinatal death should be referred to a bereavement service which could appropriately take care about all the clinical and psychological issues that arose after loss. This aspect is highlighted also within the recent Italian recommendations around stillbirth care which focused on clinical and psychological support after the discharge [7].
To guarantee an informed decision and to prevent adverse outcomes, bereaved mothers should receive guidance and support from qualified HCPs [6]. Lactation management issues after a perinatal loss are actually disregarded in our country, but instead they should become a priority aspect to improve due to its medical, psychological and emotional implications for mothers [10].
4.1. Strength and Limitations
This study marks a significant advancement in examining lactation management following perinatal loss within Italy, particularly through the lens of healthcare professionals (HCPs). The LISTEN study, by integrating the emotional and knowledge-based responses of participants, offers a comprehensive insight into the intricacies of providing care in such delicate circumstances. Moreover, the substantial size of the sample and its widespread geographical coverage ensure a highly representative understanding of the national landscape, further enhancing the study’s contribution to this critical area of healthcare.
While the study offers valuable insights within the context of Italy, it also highlights the necessity for further research in diverse cultural and healthcare settings globally. The regional focus of the LISTEN study, insightful as it is, invites future research endeavours to examine how these findings might be applicable or vary in different international contexts. Additionally, acknowledging the inherent limitations typical of survey-based research, it becomes imperative for future studies to address the potential for response bias. This will contribute to a more faithful representation of actual practices and attitudes in the real world. Furthermore, a thorough investigation into various confounding factors that might affect the responses of healthcare professionals is recommended. Such an exploration would enrich our comprehension of the requirements and challenges in providing lactation support following perinatal loss, thereby enhancing care standards in this critical area.
5. Conclusions
The LISTEN study underscores HPCs’ lack of knowledge and emotional difficulties in managing lactation after a perinatal loss. Considering such issues, Italian recommendations around stillbirth care should be improved and expanded to aid HCPs during their clinical practice.
Furthermore, training courses about communication and lactation support and management should be regularly scheduled. Our data shows that it is necessary to improve HCPs’ knowledge not only about lactation management after a perinatal loss, but also about physiological issues such as suppression. This topic involves both grieving and not grieving mothers; nonetheless, lactation suppression can occur for many reasons which could be not linked to perinatal loss. Moreover, lactation support should be enhanced in NICU by improving nurses’ knowledge and ensuring midwives’ presence. In the end, a cultural shift in the healthcare community is paramount to enable mothers to make an informed choice by offering tailored information and lactation management options.
Author Contributions
CR and AV led this research including proposal write up and designed the instrument. All authors collected data, CR and AV analysed them. CR, AV and LM discussed data and wrote the manuscript. All authors read and approved the final manuscript.
Funding
The study was not funded; no researcher received grants, salary or reimbursements for the realisation of the study.
Institutional Review Board Statement
The survey was voluntary and anonymous, no personal data were recorded, in no way it was possible to identify the single respondents. Informed consent was provided at the start of the survey once participants had read the participant information and met the eligibility criteria. Data were acquired in compliance with GDPR regulation (General Data Protection Regulation, European Union 2016/679). The research proposal was approved by the Florence University Commission for Ethics (prot. 25810, 06/02/2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
CiaoLapo Foundation for Healthy Pregnancy and Perinatal Loss Support provided infrastructure for the realisation of the study (documents, questionnaires, material, software, web platforms, open access, etc.).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HCPs | Healthcare Professionals |
| NICU | Neonatal Intensive Care Unit |
| HMBs | Human Milk Banks |
| PTSD | Post-Traumatic Stress Disorder |
| GDPR | General Data Protection Regulation |
| UN IGME | United Nations Inter-agency Group for Child Mortality Estimation |
| PSANZ | Perinatal Society of Australia and New Zealand |
References
- United Nations Inter-agency Group for Child Mortality Estimation (UN IGME). A Neglected Tragedy: the global burden of stillbirths. New York: United Nations Children’s Fund, 2020.
- World Health Organization [Internet]. Newborn Mortality [cited 2023 Aug 22]. Available from: https://www.who.int/news-room/fact-sheets/detail/levels-and-trends-in-child-mortality-report-2021.
- EpiCentro [Internet]. Stillbirth, i dati 2019 [cited 2023 Aug 25]. Available from: https://www.epicentro.iss.it/materno/stillbirth-report-2020.
- Westby CL, Erlandsen AR, Nilsen SA, Visted E, Thimm JC. Depression, anxiety, PTSD, and OCD after stillbirth: a systematic review. BMC Pregnancy Childbirth 2021;21(1):782. [CrossRef]
- Noble-Carr D, Carroll K, Copland S, Waldby C. Providing Lactation Care Following Stillbirth, Neonatal and Infant Death: Learning from Bereaved Parents. Breastfeed Med Off J Acad Breastfeed Med 2023;18(4):254-64.
- Carroll K, Noble-Carr D, Sweeney L, Waldby C. The “Lactation After Infant Death (AID) Framework”: a guide for online health information provision about lactation after stillbirth and infant death. J Hum Lact 2020;36(3):480-91. [CrossRef]
- Fondazione Confalonieri Ragonese. Gestione della morte endouterina fetale (MEF). Prendersi cura della natimortalità. SIGO, AOGOI, AGUI, 2023.
- Perinatal Society of Australia and New Zealand (PSANZ). Clinical Practice Guideline for Care Around Stillbirth and Neonatal Death: Version 3.4. 2020.
- Welborn JM. The experience of expressing and donating breast milk following a perinatal loss. J Hum Lact 2012;28(4):506-10. [CrossRef]
- Waldby C, Noble-Carr D, Carroll K. Mothers, milk and mourning: the meanings of breast milk after loss of an infant. Sociol Health Illn 2023;45(1):109-27. [CrossRef]
- McDonnell A, Butler M, White J, et al. National Clinical Practice Guideline: Stillbirth – Prevention, Investigation, Management and Care. National Women and Infants Health Programme and The Institute of Obstetricians and Gynaecologists, 2023.
- Pope CJ, Mazmanian D. Breastfeeding and postpartum depression: an overview and methodological recommendations for future research. Depress Res Treat 2016;2016:4765310. [CrossRef]
- Herbert D, Young K, Pietrusińska M, MacBeth A. The mental health impact of perinatal loss: a systematic review and meta-analysis. J Affect Disord 2022;297:118–29. [CrossRef]
- Blackmore ER, Côté-Arsenault D, Tang W, et al. Previous prenatal loss as a predictor of perinatal depression and anxiety. Br J Psychiatry 2011;198(5):373-8. [CrossRef]
- Dickens J. Lactation after loss: supporting women’s decision-making following perinatal death. Br J Midwifery 2020;28(7):442–8. [CrossRef]
- Ravaldi C, Levi M, Angeli E, et al. Stillbirth and perinatal care: are professionals trained to address parents’ needs? Midwifery 2018;64:53–9.
- Ravaldi C, Carelli E, Frontini A, et al. The BLOSSoM study: Burnout after perinatal LOSS in Midwifery. Results of a nation-wide investigation in Italy. Women Birth 2022;35(1):48–58. [CrossRef]
- Ravaldi C, Mosconi L, Mannetti L, et al. Post-traumatic stress symptoms and burnout in healthcare professionals working in neonatal intensive care units: results from the STRONG study. Front Psychiatry 2023;14:1050236. [CrossRef]
- Wilkinson H, Whittington R, Perry L, Eames C. Examining the relationship between burnout and empathy in healthcare professionals: A systematic review. Burn Res 2017;6:18–29. [CrossRef]
- Ravaldi C, Mosconi L, Bonaiuti R, Vannacci A. The emotional landscape of pregnancy and postpartum during the COVID-19 pandemic in Italy: a mixed-method analysis using artificial intelligence. J Clin Med 2023;12(19):6140. [CrossRef]
- Heazell AEP, Siassakos D, Blencowe H, et al. Stillbirths: economic and psychosocial consequences. Lancet 2016;387(10018):604-16. [CrossRef]
- Puia DM, Lewis L, Beck CT. Experiences of obstetric nurses who are present for a perinatal loss. J Obstet Gynecol Neonatal Nurs 2013;42(3):321-31. [CrossRef]
- Wallbank S, Robertson N. Predictors of staff distress in response to professionally experienced miscarriage, stillbirth and neonatal loss: a questionnaire survey. Int J Nurs Stud 2013;50(8):1090-7. [CrossRef]
- McCreight BS. Perinatal grief and emotional labour: a study of nurses’ experiences in gynae wards. Int J Nurs Stud 2005;42(4):439-48. [CrossRef]
- Taranu SM, Ilie AC, Turcu A-M, et al. Factors associated with burnout in healthcare professionals. Int J Environ Res Public Health 2022;19(22):14701. [CrossRef]
- Ravaldi C, Roper F, Mosconi L, Vannacci A. CLASS - CiaoLApo Stillbirth Support checklist: adherence to stillbirth guidelines and women’s psychological well-being. medRxiv 2023;23291084. [CrossRef]
- Pollock D, Ziaian T, Pearson E, Cooper M, Warland J. Understanding stillbirth stigma: A scoping literature review. Women Birth 2020;33(3):207-218. [CrossRef]
- Nuzum D, Meaney S, O’Donoghue K. The impact of stillbirth on consultant obstetrician gynaecologists: a qualitative study. BJOG 2014;121(8):1020-8. [CrossRef]
- Shakespeare C, Merriel A, Bakhbakhi D, et al. The RESPECT Study for consensus on global bereavement care after stillbirth. Int J Gynecol Obstet 2020;149(2):137-47. [CrossRef]
- Ministero dell’Istruzione dell’Università e della Ricerca [Internet]. Decreto Interministeriale 2 aprile 2001 - Determinazione delle classi delle lauree universitarie delle professioni sanitarie [cited 2024 Jan 23]. Available from: 2001 https://www.miur.it/0006Menu_C/0012Docume/0015Atti_M/1421CLASSE.htm.
- Spitz AM, Lee NC, Peterson HB. Treatment for lactation suppression: little progress in one hundred years. Am J Obstet Gynecol 1998;179(6 Pt 1):1485-90. [CrossRef]
- Oladapo OT, Fawole B. Treatments for suppression of lactation. Cochrane Database Syst Rev 2012;2012(9):CD005937. [CrossRef]
- Sands (Stillbirth and Neonatal Death Charity). National Bereavement Care Pathway - Neonatal Death. 2022.
- Sands (Stillbirth and Neonatal Death Society). National Bereavement Care Pathway - Stillbirth.
- McGuinness D, Coghlan B, Butler M. An exploration of the experiences of mothers as they suppress lactation following late miscarriage, stillbirth or neonatal death. Evidence Based Midwifery 2014;12(2):65-70.
- Fernández-Medina IM, Jiménez-Lasserrotte MDM, Ruíz-Fernández MD, Granero-Molina J, Fernández-Sola C, Hernández-Padilla JM. Milk Donation Following a Perinatal Loss: A Phenomenological Study. J Midwifery Womens Health 2022;67(4):463-469. [CrossRef]
- Cole M. Lactation after Perinatal, Neonatal, or Infant Loss. Clin Lact 2012;3:94–100. [CrossRef]
- Hallowell SG, Spatz DL, Hanlon AL, Rogowski JA, Lake ET. Characteristics of the NICU work environment associated with breastfeeding support. Adv Neonatal Care 2014;14(4):290-300. [CrossRef]
- Nisi GD, Moro GE, Arslanoglu S, et al. The third survey on the activity of human milk banks in Italy and the impact of the COVID-19 pandemic. Int J Nutr 2022;7(2):31–41.
- Health Service Executive Ireland. National Standards for Bereavement Care Following Pregnancy Loss and Perinatal Death. 2022.
- Salgado HO, Andreucci CB, Gomes ACR, Souza JP. The perinatal bereavement project: development and evaluation of supportive guidelines for families experiencing stillbirth and neonatal death in Southeast Brazil-a quasi-experimental before-and-after study. Reprod Health 2021;18:5. [CrossRef]
Figure 1.
Clinical and emotional management of perinatal loss (panel A) and evaluation of the usefulness of different treatments (panel B). * p<0.05.
Figure 1.
Clinical and emotional management of perinatal loss (panel A) and evaluation of the usefulness of different treatments (panel B). * p<0.05.
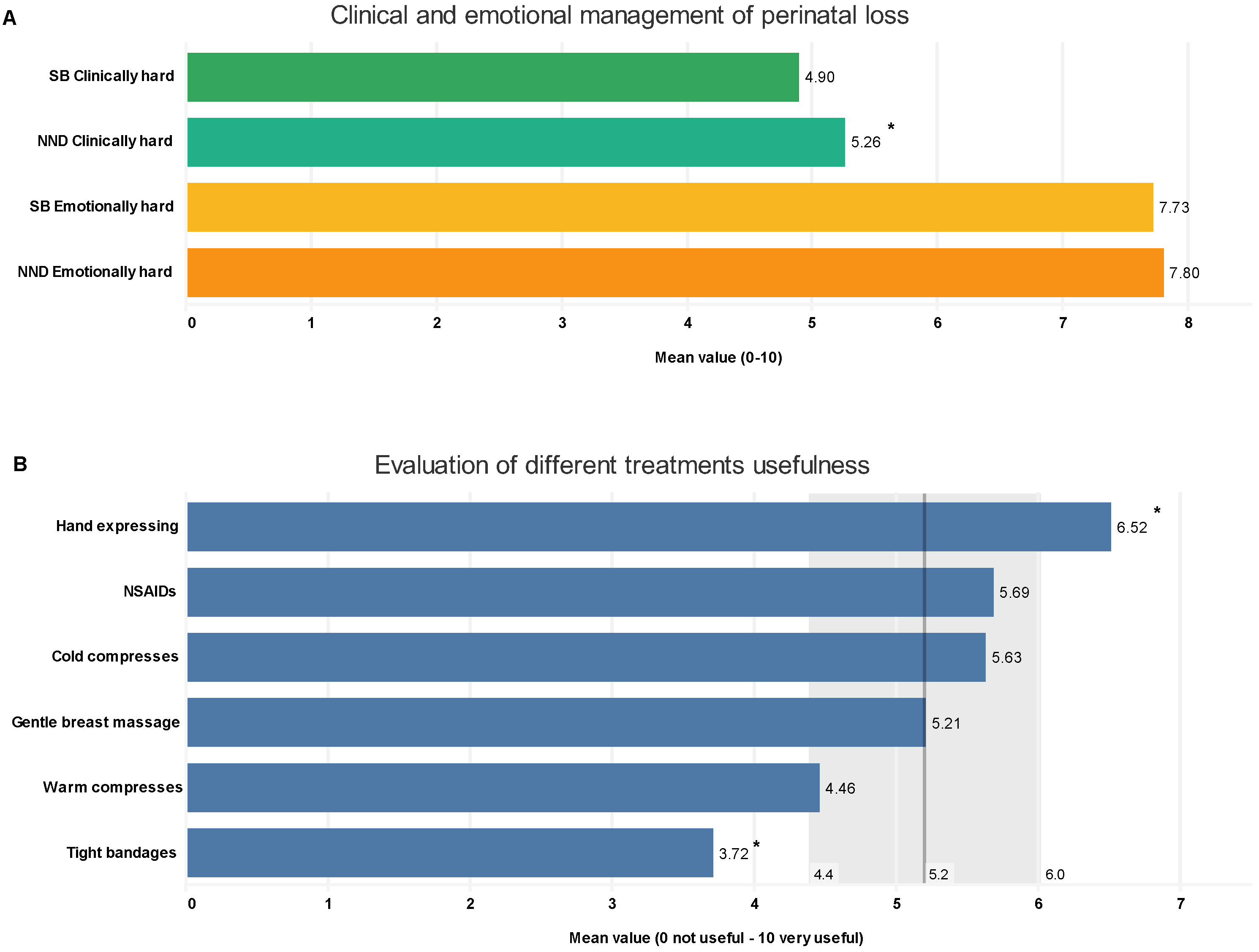
Figure 2.
Type of information provided by respondents regarding lactation after perinatal loss in case of stillbirth (panel A) and neonatal death (panel B). Panel C illustrates the geographical distribution of respondents: white circles represent the locations of responders, with size indicating number; regions shaded in blue denote a higher percentage, and those in red a lower percentage of professionals providing lactation information. Black stars highlight the locations of human milk banks.
Figure 2.
Type of information provided by respondents regarding lactation after perinatal loss in case of stillbirth (panel A) and neonatal death (panel B). Panel C illustrates the geographical distribution of respondents: white circles represent the locations of responders, with size indicating number; regions shaded in blue denote a higher percentage, and those in red a lower percentage of professionals providing lactation information. Black stars highlight the locations of human milk banks.
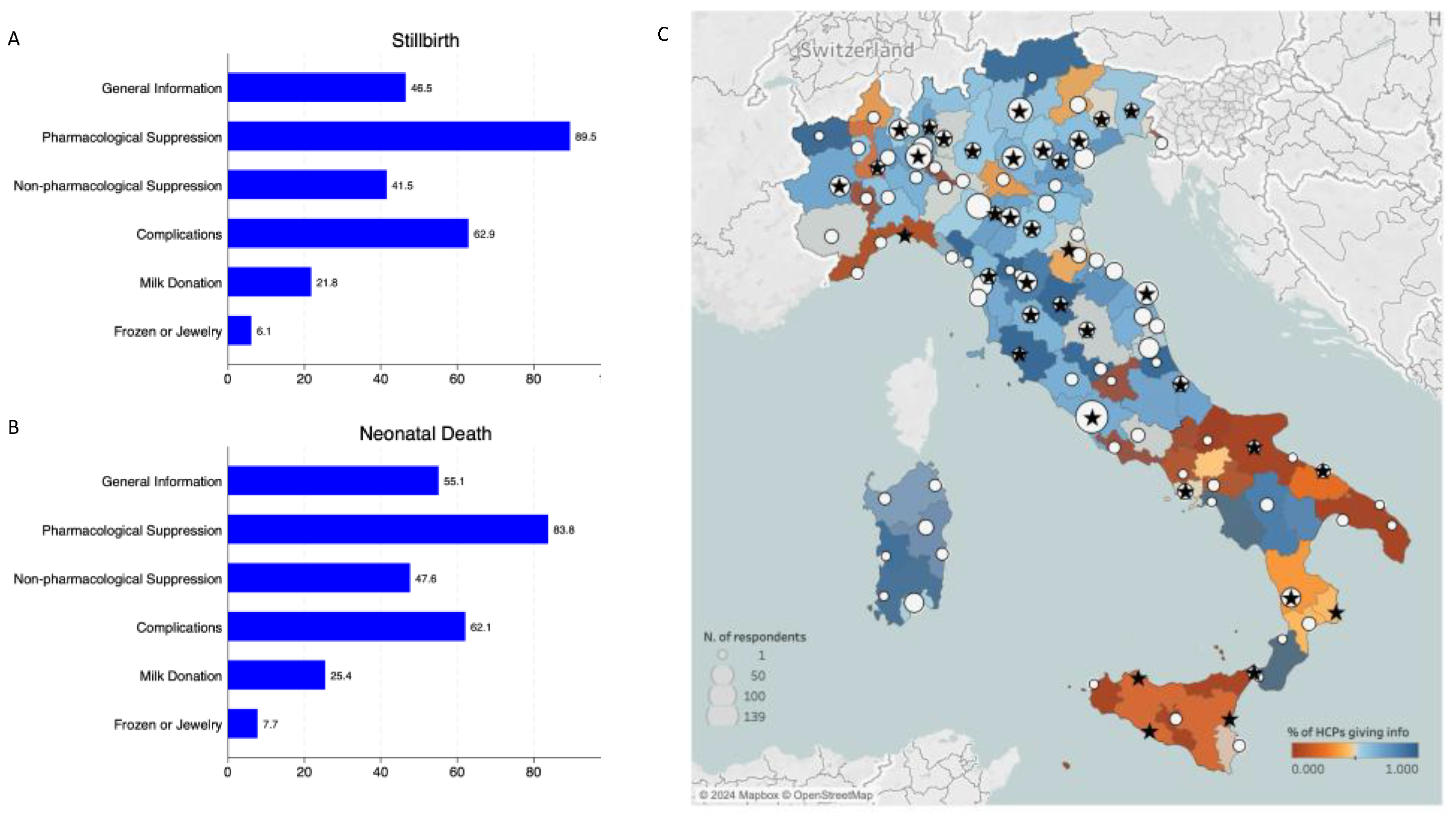

Table 1.
Main characteristics of the sample. Other jobs: healthcare assistants, lactation consultants. Other settings: outpatient clinic, emergency room, paediatrics, screening services, psychiatric and psychological services.
Table 1.
Main characteristics of the sample. Other jobs: healthcare assistants, lactation consultants. Other settings: outpatient clinic, emergency room, paediatrics, screening services, psychiatric and psychological services.
 |
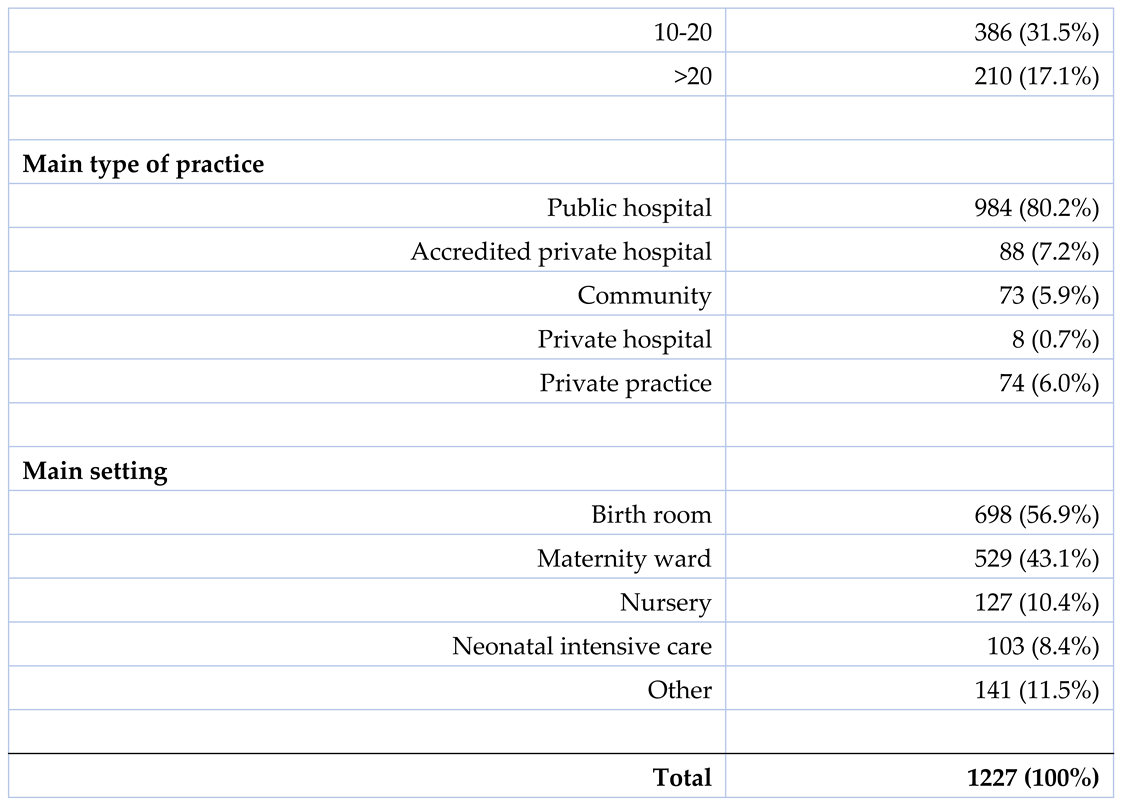 |
Table 2.
Professional experience on perinatal loss.
 |
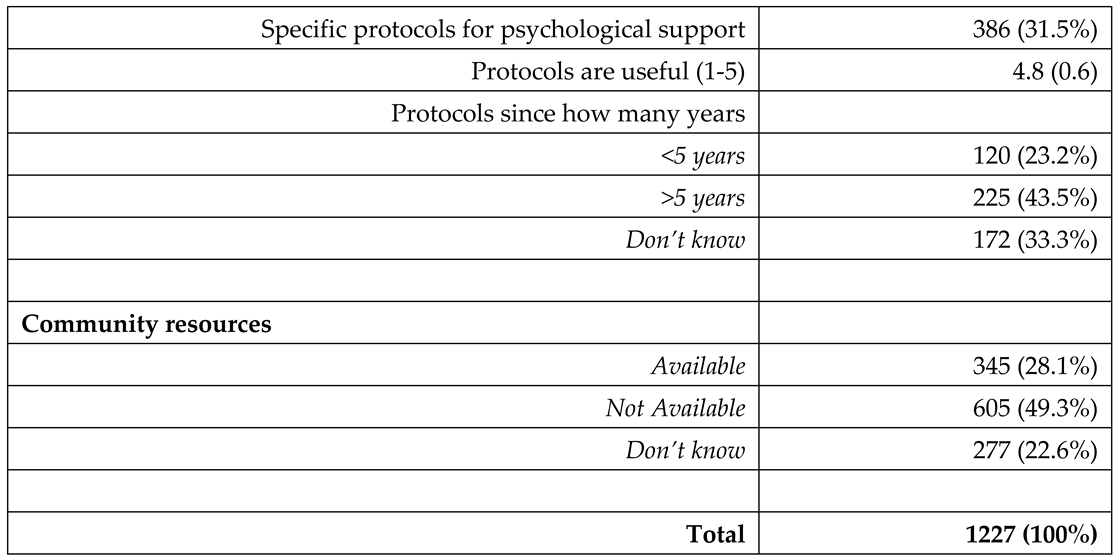 |
Table 3.
Personal experience on lactation information on perinatal loss (analysis restricted to those HCPs who had the actual opportunity of giving such information).
Table 3.
Personal experience on lactation information on perinatal loss (analysis restricted to those HCPs who had the actual opportunity of giving such information).
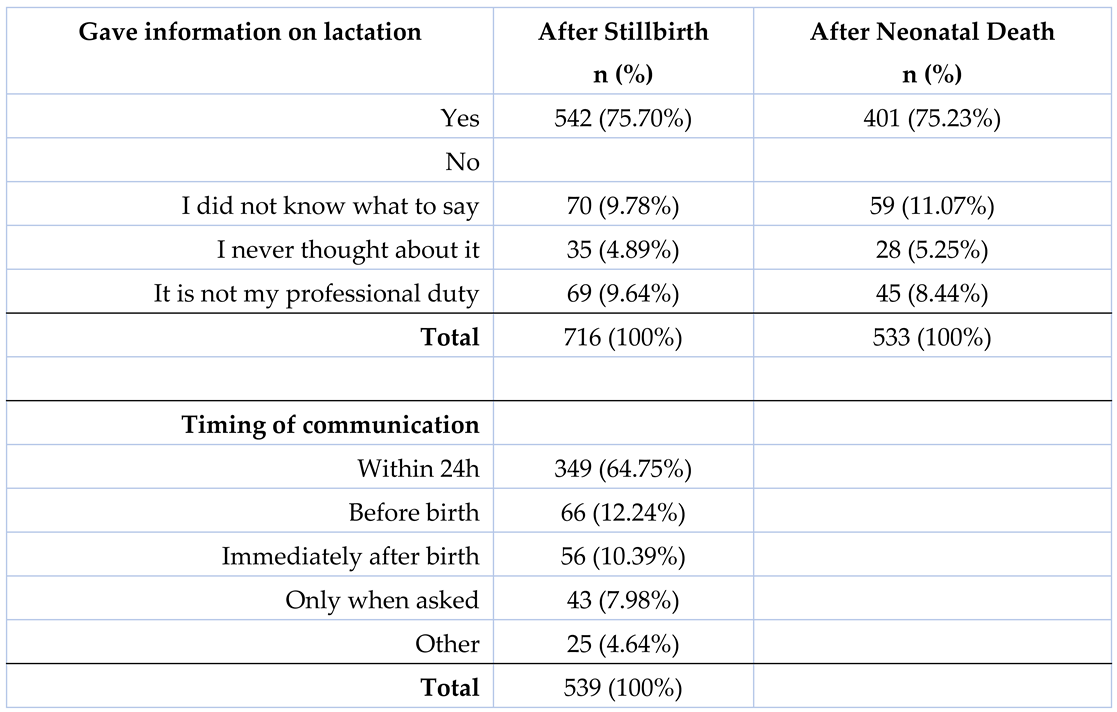 |
Table 4.
Type of information on milk donation, given after perinatal loss (analysis restricted to those HCPs who had actually given information on milk donation). *p<0.05.
Table 4.
Type of information on milk donation, given after perinatal loss (analysis restricted to those HCPs who had actually given information on milk donation). *p<0.05.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



