Submitted:
30 December 2024
Posted:
31 December 2024
You are already at the latest version
Abstract
Pediatric tuberculosis (TB) is still challenged by several diagnostic bottlenecks, imposing a high TB burden in low- and middle-income countries (LMICs). Diagnostic turn-around time (TAT) and ease of operation to suit resource-limited settings are critical aspects that determine early treatment and influence morbidity and mortality. Based on TAT and ease of operation, this article reviews the evolving landscape of TB diagnostics, from traditional methods like microscopy and culture to cutting-edge molecular techniques and biomarker-based approaches. We examined the benefits of efficient rapid results against potential trade-offs in accuracy and clinical utility. The review highlights emerging molecular methods and artificial intelligence-based detection methods, which offer promising improvements in both speed and sensitivity. The review also addresses the challenges of implementing these technologies in resource-limited settings, where most pediatric TB cases occur. Gaps in the existing diagnostic methods, diagnostic algorithms and operational costs were also reviewed. Development of optimal diagnostic strategies that balance speed, performance, cost and feasibility in diverse healthcare settings can provide valuable insights for clinicians, researchers, and policymakers.
Keywords:
Diagnosis
; Mycobacterium
; TB
; CRISPR
; children
; artificial intelligence
Introduction
Pediatric tuberculosis (TB) remains a significant global health challenge, with diagnosis often complicated by non-specific symptoms and difficulties in obtaining quality specimens [1]. According to the World Health Organization (WHO), an estimated 1.2 million children and young adolescents (<15 years) fell ill with TB in 2023 with 226,000 deaths globally [2]. Mortality is highest in children under five, with 76% of HIV-negative TB deaths occurring in this age group. Undiagnosed and undertreated cases suffer the highest mortality (96%). HIV co-infection significantly increases mortality risk [3,4]. The COVID-19 pandemic has impacted TB notifications, potentially affecting mortality rates. Underdiagnosis remains a major challenge, with only 49% of estimated pediatric TB cases diagnosed and reported in 2022 [4,5]. WHO has emphasized the need for rapid, accurate diagnostic tools for childhood TB, recognizing that early diagnosis and treatment initiation are crucial for improving outcomes [5].
Recent years have seen significant advancements in diagnostic technologies aimed at reducing turnaround time (TAT) while maintaining or improving accuracy. For instance, the Xpert MTB/RIF Ultra assay, which provides results in about 90 minutes, has shown improved sensitivity compared to its predecessor in pediatric populations [6,7]. Similarly, newer technologies like the Cepheid MTB-HR, a blood-based test utilizing a three-gene mRNA transcriptomic signature, aim to provide rapid results from easily obtainable samples [1,6]. However, the quest for faster diagnostics raises important questions about the balance between speed, accuracy and ease of operation in pediatric TB diagnosis. While rapid tests can facilitate quicker treatment initiation, they must be evaluated in the context of their overall clinical utility, including sensitivity, specificity, and applicability in resource-limited settings where the majority of TB cases occur [8,9].
This review will provide an up-to-date overview of available diagnostic tools for pediatric TB, exploring their TAT, performance, and application. We will discuss traditional methods, such as microscopy and culture, as well as newer molecular techniques and emerging biomarker-based approaches. Additionally, we reviewed how these diagnostic methods perform in different clinical scenarios and patient subgroups, such as HIV-infected children or those with extrapulmonary TB [8]. By critically assessing the premise that 'faster is better' in pediatric TB diagnostics, we seek to provide a nuanced understanding of the current landscape and future directions in this crucial area of global health. This review will also highlight gaps in current knowledge and areas where further research is needed to improve the diagnosis of TB in children.
Challenges in Pediatric TB Sampling
The diagnosis of TB (TB) in children presents unique challenges due to the age-dependent nature of the disease spectrum and the difficulties in obtaining suitable diagnostic samples. Younger children often exhibit non-specific signs and symptoms of paucibacillary intrathoracic or disseminated infection, making it challenging to differentiate TB from other common childhood illnesses [9]. The symptoms such as fever, cough, and weight loss are not exclusive to TB, complicating the diagnostic process [10]. Moreover, children typically have a lower bacterial load compared to adults, making it harder to detect Mycobacterium tuberculosis (Mtb) in sputum samples [1,10].
Various sample collection methods for pediatric TB diagnosis each present their own set of challenges. Expectorated or induced sputum samples, while offering high sensitivity and specificity for Xpert assays, are limited to older children with productive coughs and require specialized equipment and trained personnel [9,11]. Experimental methods like oral swabs and bioaerosols show promise but currently lack optimal diagnostic accuracy or suitable pediatric prototypes [10,11].
The WHO has endorsed stool samples for use with the Xpert MTB/RIF Ultra test, which is particularly beneficial for younger children who struggle to produce sputum [12,13]. The ease of stool collection in children makes it possible to diagnose TB at primary healthcare levels, potentially reducing the need for referrals, although stool processing for sophisticated tests requires some training [14,15]. In some studies, stool-based Xpert testing has shown considerable specificity (98-99%) [14,16]. Stool samples may also be helpful in detecting extrapulmonary TB, which are often missed by smear microscopy [17]. However, stool samples have a range of challenges. The sensitivity of stool-based Xpert testing varies widely (50% to 67%) across studies, with very low sensitivity (2-6%) in clinically diagnosed TB cases compared to culture on respiratory samples [14,15]. Potential for heterogeneity in results of stool-based Xpert testing may occur due to bacterial load, differences in processing methods or patient populations. [18]These disadvantages limit stool testing as a standalone diagnostic route but rather it is recommended as an additional specimen rather than a replacement for other diagnostic methods, especially in cases where respiratory samples can be obtained [17,18].
Gastric and nasopharyngeal aspirates are also being increasingly used, showing promising results despite potential lower sensitivity compared to sputum. However, both sampling types are invasive procedures demanding specific expertise and equipment [19,20]. Blood-based biomarkers in TB diagnosis offer a potential breakthrough, with studies investigating specific cytokines and chemokines [21].
While promising, these alternative methods still face challenges in sensitivity and require further validation in pediatric populations. Nevertheless, they represent important steps towards more child-friendly TB diagnostic approaches. The complexity of sample collection, combined with the non-specific presentation of pediatric TB, underscores the need for innovative diagnostic approaches tailored to the unique needs of pediatric population [9,10].
Existing Diagnostic Methods and Gaps
Traditional Diagnostic Methods for Pediatric TB
Microscopy remains the oldest and most widely available diagnostic tool for TB, offering rapid results within minutes to hours [22]. However, its utility in pediatric TB is severely limited due to its low sensitivity, ranging from 10-15% in children [23]. This poor performance is primarily attributed to the paucibacillary nature of pediatric TB, where children often have a low bacterial load in their specimens. A systematic review found that the pooled sensitivity of smear microscopy in children was only 22% (95% CI: 17-28%) compared to culture [13]. Recent advancements, such as LED fluorescence microscopy, have improved sensitivity, with one study reporting an increase from 52% to 73% compared to conventional light microscopy [24]. However, the fundamental limitation persists; low sensitivity makes microscopy an unreliable standalone test for diagnosing TB in children. Empirical TB diagnosis is a common practice in resource-limited settings, based on clinical signs and symptoms without laboratory confirmation. However, the sensitivity of empirical TB diagnosis widely varies from 16% to 44.4% across different studies [25]
Culture-based techniques remain the gold standard for TB diagnosis, offering definitive results and the ability to perform drug susceptibility testing. However, the lengthy turnaround time of 2-8 weeks makes it impractical for rapid diagnosis and timely treatment initiation, which is crucial in pediatric cases. A meta-analysis by Detjen et al. found that the pooled sensitivity of culture in children was 62% (95% CI: 51-73%) compared to a clinical reference standard [26]. Recent innovations like the Microscopic Observation Drug Susceptibility (MODS) assay have reduced the time to 7-10 days, with one study reporting a sensitivity of 87.5% in pediatric samples [27]. However, this is still too long for optimal clinical management. The critical limitation of culture-based methods in pediatric TB lies in the difficulty of obtaining quality specimens in children's samples.
The Tuberculin Skin Test (TST) has been a cornerstone of TB screening for decades, with a turnaround time of 48-72 hours [28]. The tuberculin skin test involves intradermal injection of purified protein derivative (PPD) to elicit a delayed-type hypersensitivity reaction, which is measured by the size of induration after 48-72 hours. However, its utility is hampered by limited specificity, particularly in BCG-vaccinated populations and those exposed to non-tuberculous mycobacteria. A recent meta-analysis reported a pooled sensitivity of 66% (95% CI: 55-76%) and specificity of 75% (95% CI: 65-84%) in children, highlighting its limitations [29]. The TST's critical shortcoming is its inability to differentiate between active TB and latent infection, a distinction crucial for clinical decision-making in pediatric cases. A study found that TST had a positive predictive value of only 4% for progression to active TB in children [30].
Interferon-gamma release assays (IGRAs) are blood tests that measure ex vivo T-lymphocyte release of interferon-γ after stimulation by Mtb-specific antigens. IGRAs offer improved specificity over TST, with results available in 24-48 hours. A meta-analysis found that IGRAs had a pooled sensitivity of 67% (95% CI: 62-73%) and specificity of 98% (95% CI: 97-99%) in children [29]. However, like TST, IGRAs cannot distinguish between active and latent TB, limiting their diagnostic value. Furthermore, they require specialized laboratory equipment and trained personnel to perform blood collection, processing, and result interpretation, making them less operationally simple for resource-limited settings. Their performance too is suboptimal in young children and immunocompromised patients, who are often at highest risk for severe TB disease. A recent study found that IGRA performance was particularly poor in children under 5 years, with indeterminate results in up to 40% of cases [31]. Recent advancements, such as the T-cell activation marker-TB assay, show promise in differentiating active from latent TB, with one study reporting a sensitivity of 83.3% and specificity of 96.8% in children [30]. However, these newer approaches require further validation in diverse pediatric populations.
Molecular Diagnostic Techniques for Pediatric TB
Xpert MTB/RIF is a widely used cartridge-based nucleic acid amplification test (NAAT) for TB diagnosis [32]. It can simultaneously detect TB and rifampicin resistance within approximately 2 hours. The assay has a limit of detection of 131 CFU/ml in sputum and detected as few as 10 CFU/ml per sputum sample in 35% of samples with a much longer TAT [33]. The test's sensitivity for TB detection ranges from 89% to 98% in smear-positive samples and 67% to 75% in smear-negative, culture-positive samples [34]. While Xpert MTB/RIF offers rapid results and requires simple operative expertise, it needs stable electricity and temperature control, which can be challenging in resource-limited settings. It is also limited to detecting resistance to only rifampicin. Additionally, its high equipment cost (~$11000-$70000 based on module type and accessories, excluding maintenance costs) and relatively high cost per test (>$20) as compared to smear microscopy limit its widespread use in some contexts [35,36,37]. The Xpert MTB/RIF Ultra assay improves upon its predecessor, the Xpert MTB/RIF, by utilizing two multicopy targets (IS6110 and IS1081) and a larger PCR chamber, resulting in enhanced sensitivity and a lower limit of detection (15.6 CFU/mL) compared to 131 CFU/mL for the original test [38]. The World Health Organization recommends Xpert Ultra as the initial diagnostic test for pulmonary TB in children, as it outperforms traditional methods like smear microscopy and culture, especially in cases with low bacterial loads [39]. However, despite its advantages, Xpert Ultra has faced criticism regarding its specificity, which can decrease as sensitivity increases, leading to potential false positives [38,40].
TrueNAT, a chip-based NAAT for TB detection, provides results in 30-60 minutes [41]. It involves three main steps such as sample preparation using a pre-treatment pack, automated DNA extraction using the Trueprep AUTO device, and PCR amplification/detection using Truenat chips and the Truelab Real Time micro-PCR Analyzer [1,5]. Recent studies have shown promising results, with one multicenter evaluation in Cameroon demonstrating a sensitivity of 91% (95% CI: 86-94%) and specificity of 96% (95% CI: 94-97%) compared to culture [34]. However, the performance of TrueNAT can be affected by various factors, including sample quality and operator skill. A study in India found that the rate of invalid MTB results was 5.2% and the rate of indeterminate rifampicin resistance results was 15.3% [35]. While TrueNAT offers quick turnaround times, more data is needed on its performance in diverse settings, particularly for detecting extensively drug-resistant TB.
Line Probe Assay (LPA) can detect TB and resistance to multiple drugs within 1-2 days. It has shown high sensitivity and specificity for detecting rifampicin and isoniazid resistance, especially for smear-positive samples in various studies [42,43]. It uses PCR and reverse hybridization techniques to identify specific DNA sequences on nitrocellulose strips [44]. However, LPA requires sophisticated laboratory infrastructure and skilled technicians. Its inability to be used directly on clinical samples limits its applicability in some settings, particularly at the point of care.
Loop-mediated Isothermal Amplification (LAMP) is a nucleic acid amplification technique that uses 4-6 specially designed primers and a strand-displacing DNA polymerase to amplify target DNA sequences at a constant temperature (60-65°C). For TB detection it has a turnaround time of about 1 hour [45]. A systematic review and meta-analysis found that LAMP had a pooled sensitivity of 89.6% (95% CI: 85.6-92.6%) and specificity of 94.0% (95% CI: 91.0-96.1%) for pulmonary TB diagnosis [46]. While LAMP offers rapid results owing to its simplicity (to perform and interpret), its lower sensitivity compared to Xpert MTB/RIF and inability to detect drug resistance limit its utility in comprehensive TB management [43,46].
The Lipoarabinomannan (LAM) Antigen Test is a lateral flow immunochromatographic assay that detects mycobacterial LAM in urine samples, providing results within 25-30 minutes. The test is operationally simple, requiring only a small amount of unprocessed urine and visual interpretation of results, making it suitable for point-of-care use in resource-limited settings [47]. It is particularly useful for diagnosing TB in HIV-positive patients with low CD4 counts. A meta-analysis found that the pooled sensitivity of LAM in HIV-positive individuals was 42% (95% CI: 31-55%), increasing to 56% (95% CI: 41-70%) in those with CD4 counts ≤100 cells/μl [48,49]. However, its lower sensitivity in HIV-negative individuals limits its broader applicability.
Next-Generation Sequencing (NGS), for TB diagnosis, particularly targeted NGS (tNGS), is a high-throughput DNA sequencing technology that allows for rapid and comprehensive detection of mutations associated with drug resistance in Mtb. It involves DNA extraction, library preparation, sequencing, and bioinformatic analysis to identify resistance-conferring mutations across multiple genes simultaneously. With a TAT of 2-3 days, NGS offers higher comprehension in terms of resistance profiling compared to phenotypic drug susceptibility testing, however, its implementation in routine TB diagnostics faces challenges such as the need for specialized equipment, complex sample preparation, sophisticated bioinformatics analysis, and higher costs per sample ($75-200 for NGS). However, efforts are ongoing to simplify workflows and reduce turnaround times, making it increasingly feasible for implementation in reference laboratories in high-burden settings [50,51,52].
The TAM-TB (T cell Activation Marker-TB) assay is a novel immunodiagnostic test for TB that measures the expression of activation markers (CD38, HLA-DR, Ki67) and a maturation marker (CD27) on Mtb-specific CD4 T-cells using flow cytometry[53]. Requiring only minimum fresh blood, it shows promise for diagnosing extrapulmonary TB and in pediatric cases, with results available within 24 hours. [54]. The assay can distinguish between active and latent TB infection and potentially monitor treatment response [53,54]. However, it requires specialized equipment and trained personnel, limiting its current use as a point-of-care test. While promising, further validation in larger cohorts and diverse populations is needed before widespread clinical implementation [53].
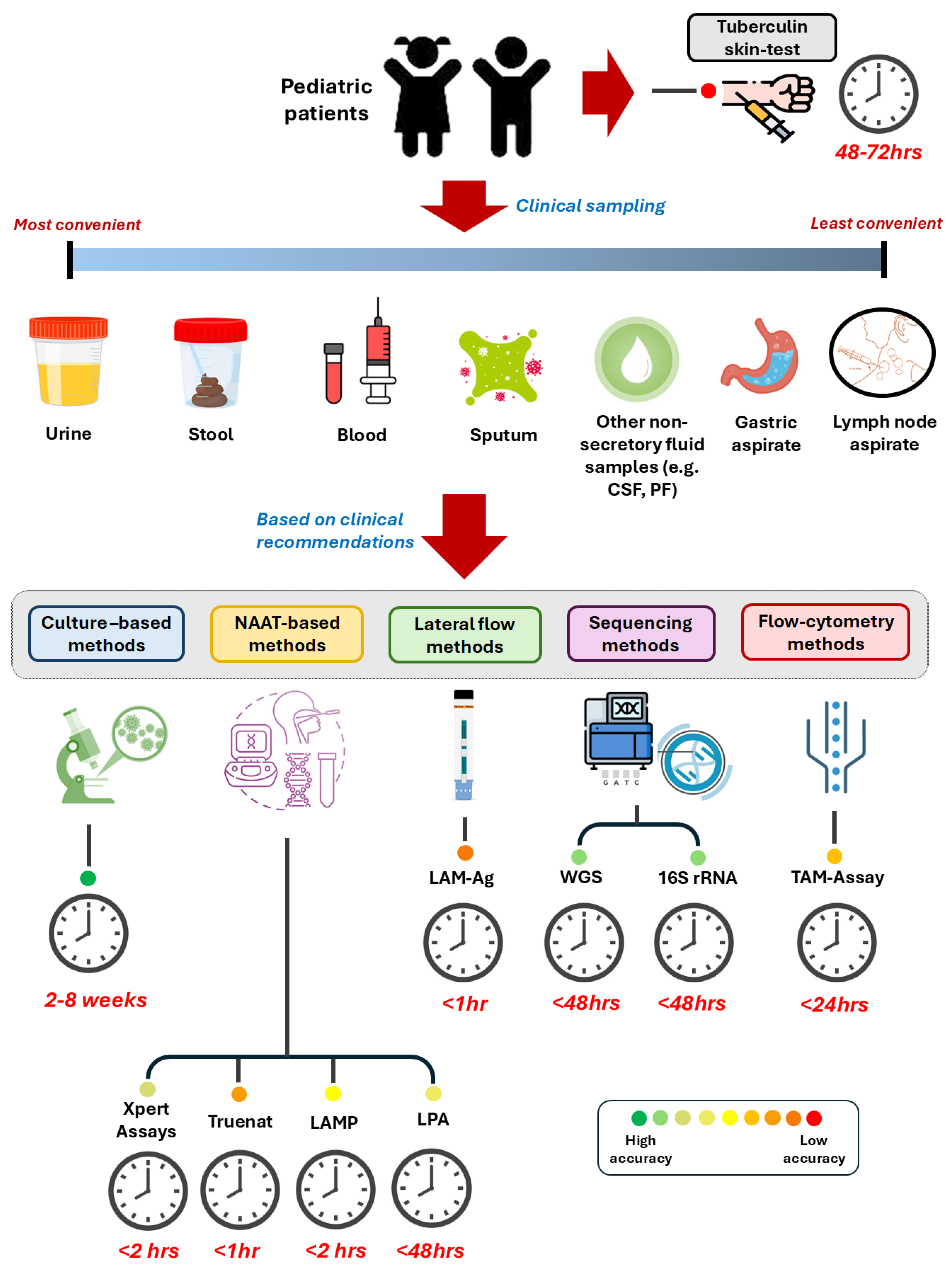
The combination of centralized laboratory-based testing and decentralized point-of-care testing is increasingly recognized as an effective approach to TB diagnosis [55]. This strategy can help balance the need for rapid results with comprehensive drug resistance profiling. For example, using Xpert MTB/RIF or TrueNAT at the point of care for initial diagnosis, followed by more comprehensive testing like LPA or NGS at reference laboratories for drug resistance profiling, could improve overall TB care cascades [56]. The ongoing development and refinement of these diagnostic tools continue to play a crucial role in the global fight against TB (Table 1). An overview of the recommended diagnostic methods is given in. Figure 1 based on speed, ease of operation and accuracy.
Emerging Approaches in Pediatric TB Diagnosis
The landscape of TB (TB) diagnostics is rapidly evolving, with several innovative approaches showing promise for improved detection, particularly in challenging populations such as children [61]. An overview of recent developments and proof-of-concept studies are summarized.
The Cepheid MTB-HR (Host Response) assay represents a significant advancement in TB diagnosis, utilizing a blood-based host response signature. With a turnaround time of approximately 90 minutes and the ability to use easily obtainable fingerstick blood samples, it shows promise for pediatric TB diagnosis [62]. A recent multicenter study conducted across South Africa, Uganda, and Vietnam demonstrated encouraging results in children, achieving a sensitivity of 83% and specificity of 84% for TB detection [63]. However, further validation in diverse pediatric populations is needed to establish its place in diagnostic algorithms, especially in high-burden, low-resource settings.
CRISPR-based detection methods are at the forefront of innovative TB diagnostics. These techniques offer results within 1-2 hours and show promise for ultrasensitive detection of TB DNA [64]. A recent study by Zhang et al. developed a CRISPR/Cas12a-based assay combined with recombinase-aided amplification (RAA) that could detect Mtb with a limit of detection as low as 3.13 CFU/mL [65]. This method, termed TB-CRISPR, demonstrated a sensitivity of 88.3% and specificity of 94.0% when compared to BACTEC 960 culture, with a total detection time of less than 1.5 hours [64,65,66]. A CRISPR/Cas13a assay showed a low limit of detection of one target sequence copy/μL and provided superior sensitivity (97.4%) compared to acid-fast bacilli (48.5%) and mycobacterial culture (71.6%) assays in clinical samples. The turnaround time for this assay was not explicitly stated but is likely within the 1–2-hour range typical of CRISPR-based methods [66,67]. A novel application of CRISPR technology involves the detection of circulating cell-free TB DNA (Mtb-cfDNA) in serum. A study demonstrated high sensitivity (100%) and specificity (94%) in detecting microbiologically and clinically confirmed TB cases in a predominantly HIV-negative adult cohort. Importantly, this method also showed promise in pediatric populations, with 83% sensitivity and 95% specificity in a cohort of children, including all cases of extrapulmonary TB [67].
A report by MacLean et al. identified a 3-protein biosignature (C-reactive protein, transthyretin, and complement factor H) that could differentiate TB from other diseases with 86% sensitivity and 84% specificity [21]. This approach, which uses a blood test, has a potential turnaround time of a few hours and could be particularly valuable for children who often struggle to produce sputum samples. Metabolomic approaches are also showing promise. A recent study by Manyelo et al. identified a 7-marker serum metabolomic biosignature that showed 80% sensitivity and 89% specificity for TB diagnosis in children [68]. While these biomarker-based approaches are still in the discovery or early validation phases, they offer the potential for rapid, non-sputum-based diagnostics with turnaround times potentially as short as a few hours once fully developed [69]. While these innovative approaches show great promise, particularly for challenging diagnostic scenarios like pediatric and extrapulmonary TB, they are still in various stages of development, validation or at the proof-of-concept stage. Further large-scale studies in diverse populations are needed to establish their accessibility, clinical utility and cost-effectiveness before they can be widely implemented in TB diagnostic procedures [70].
Portable chest X-ray (CXR) systems combined with computer-aided detection (CAD) software can improve access to screening in remote areas. CXR has higher sensitivity and specificity than symptom screening alone and can potentially reduce the number and costs of follow-on diagnostic tests [71,72]. Recent advances in machine learning and AI-based methods have significantly improved TB (TB) diagnosis, particularly through the analysis of medical imaging and molecular data [73]. Some of the popular tools have been given in Table 2. Deep learning models, especially convolutional neural networks (CNNs) such as ResNet, VGG, and AlexNet, have demonstrated high accuracy in detecting TB from chest X-rays, with some studies reporting area under the receiver operating characteristic curve (Area Under Curve) values of 0.99 or higher [74]. For instance, a ResNet-based AI system achieved 96.73% accuracy in TB detection from chest X-rays, outperforming other models. These AI systems have shown comparable or even superior performance to radiologists in TB detection tasks [75,76]. Additionally, AI-based radiographic extent analysis, such as the one developed using OpenCV for visualization, has emerged as a significant predictor of treatment success and culture conversion in pulmonary TB. Beyond image analysis, machine learning approaches like support vector machines (SVMs) and random forests have been applied to genetic data for rapid detection of drug-resistant TB strains. Tools like Xpert MTB/RIF assay, combined with AI analysis of its cycle threshold (Ct) values, offer promising avenues for improving TB diagnosis and treatment monitoring [76,77]. While these AI methods show great potential in enhancing TB care efficiency and accuracy, challenges remain in model generalization across diverse populations and clinical settings [78].
Balancing Speed, Accuracy and Cost of Diagnosis
Recent studies have highlighted the critical role of cheap and rapid diagnosis in improving patient outcomes and reducing disease transmission. Shorter TATs could lead to earlier treatment initiation, potentially reducing morbidity and mortality associated with TB in children [9]. Diagnostic cost is one of the most critical factors that limits the implementation of rapid and sophisticated tests. A recent analysis of moderate complexity automated nucleic acid amplification tests (MC-NAATs) for TB diagnosis revealed that the base-case per-test cost was $18.52 (range: $13.79 - $40.70) for lower throughput (LT) tests and $15.37 (range: $9.61 - $37.40) for higher throughput (HT) tests [82]. These costs were most sensitive to the number of testing days per week, equipment costs, and TB-specific workloads. Generally, HT NAATs were more cost-effective at all testing volume levels, but LT tests could be cheaper at lower testing volumes (less than 2,000 per year) if the durability of the testing system was markedly better or equipment costs were lower [82].
In high multidrug-resistant TB (MDR-TB) settings, such as Moldova, the average diagnostic cost per patient suspected of TB, including diagnosis of TB and TB drug resistance, was estimated at $82 [83]. This study provided empirical estimates for various diagnostic tests, including sputum smear microscopy (SSM), Löwenstein-Jensen (LJ) solid culture, BACTEC MGIT, Xpert MTB/RIF, and line probe assays (LPAs). The per-test costs ranged from $8.15 for SSM to $30.75 for Xpert MTB/RIF [83].
A cost and affordability analysis of TB-LAMP and Xpert MTB/RIF assays in Vietnam and Malawi demonstrated that the weighted average per-test cost of nationwide implementation was between $14.37–$15.85 for TB-LAMP and $20.06–$26.86 for Xpert [84]. This study highlighted that both NAATs would account for a significant portion of or exceed the national TB program budget if complete nationwide roll-out to peripheral laboratories were considered.
The balance between speed and accuracy in different settings remains another crucial consideration. The trade-offs between rapid results and diagnostic accuracy continue to be a subject of intense debate. While faster results can lead to quicker treatment initiation, the potential for false-positive or false-negative results must be carefully considered. A report explored the clinical implications of false-positive results from rapid molecular tests, highlighting the risks of unnecessary treatment and the psychological impact on patients and families [85]. Conversely, false-negative results can lead to delayed diagnosis and treatment, potentially resulting in disease progression and continued transmission. A recent meta-analysis demonstrated that the optimal diagnostic strategy varies depending on the local TB prevalence, available resources, and healthcare infrastructure [33]. In high-burden, resource-limited settings, rapid point-of-care tests with moderate sensitivity may be preferred over highly accurate but lengthy laboratory-based methods. Conversely, in low-burden settings with more resources, a combination of rapid screening tests followed by confirmatory molecular assays might be more appropriate [86]. Therefore, future research should focus on developing innovative, cost-effective diagnostic strategies that balance speed, accuracy, ease of use and accessibility to improve TB detection and patient outcomes across various resource settings.
Future Directions
Sample collection and implementation of state-of-the art diagnostic tools in resource limited settings are the major challenges owing to infrastructure, cost, and specialized skills required [13,86]. Active case finding (ACF) has shown potential for increasing early detection of TB cases in underserved communities. Effective RDTs for TB detection along with capacity-building for healthcare workers would facilitate ACF implementation in LMICs [87]. In addition, creating centralized "hubs" that perform advanced diagnostics like whole genome sequencing for each country or region can help overcome infrastructure and cost barriers. This approach requires developing efficient sample transport systems [88]. For economic accessibility of the diagnostic tools, negotiating with manufacturers and exploring bulk purchasing options can help reduce costs. Building bioinformatics and laboratory capacity besides investing in training programs can develop local expertise to expedite the process [13,86].
Home-based TB diagnosis is emerging as a promising approach to improve case detection and reduce barriers to TB evaluation. A proof-of-concept study in Eastern Cape, South Africa, found in-home testing using GeneXpert Edge highly acceptable, with 98% consent rate and 96% result delivery. It significantly increased testing rates (47% vs 13%) and reduced result turnaround time (0 vs 16.5 days median) compared to clinic-based testing [89]. However, a Uganda study using SMS-facilitated evaluation showed implementation challenges [90]. Recent high-impact literature on pediatric TB (TB) diagnosis and management has led to several key recommendations for clinicians, researchers, and policymakers to improve pediatric TB conditions worldwide[1,91]. Policymakers play a vital role in improving pediatric TB conditions. Updating clinical guidelines to incorporate new evidence-based diagnostic algorithms and novel diagnostic tools is essential. Investing in health system strengthening, including improved infrastructure, supply chains, and training programs, is necessary to support the implementation of new diagnostic tools. Promoting integrated care approaches by encouraging the integration of TB services with other child health programs can improve case detection and treatment initiation. Supporting research and development through resource allocation for pediatric-specific TB diagnostics and treatments is crucial. Finally, addressing social determinants by implementing policies to tackle poverty, malnutrition, and other social factors that contribute to TB vulnerability in children is of utmost importance.
Conclusions
Implementing fast, simple, and accurate TB diagnostic tools in resource-limited settings of LMICs requires a multifaceted approach that combines technological innovations, capacity building, and health system strengthening. By adopting these strategies and continually evaluating their effectiveness, endemic regions, especially LMICs, can work towards improving TB diagnosis and moving closer to achieving global TB elimination goals.
Author Contributions
Conceptualization, S.B. and S.C., Writing, data curations, S.B., Supervision, Review and Editing, S.C. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Institute of Allergy and Infectious Disease under JHU TRAC NIH/NIAID fund P30AI18436. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Data Availability Statement
The data presented in this study are available in the manuscript.
Declaration of Interest: The authors have no conflict of interest
References
- Basile, F.W.; Nabeta, P.; Ruhwald, M.; Song, R. Pediatric Tuberculosis Diagnostics: Present and Future. J Pediatric Infect Dis Soc 2022, 11, S85–S93. [CrossRef]
- World Health organization https://www.who.int/teams/global-tuberculosis-programme/data. Geneva 2024,.
- Geneva: World Health Organization Diagnosis of Tuberculosis and Detection of Drug-Resistance: Rapid Communication.
- World Health Organization WHO TB Knowledge Sharing Platform.
- World Health organization Global Tuberculosis Report 2022.
- Olbrich, L.; Nliwasa, M.; Sabi, I.; Ntinginya, N.E.; Khosa, C.; Banze, D.; Corbett, E.L.; Semphere, R.; Verghese, V.P.; Michael, J.S.; et al. Rapid and Accurate Diagnosis of Pediatric Tuberculosis Disease: A Diagnostic Accuracy Study for Pediatric Tuberculosis. Pediatric Infectious Disease Journal 2023, 42, 353–360. [CrossRef]
- Gebre, M.; Cameron, L.H.; Tadesse, G.; Woldeamanuel, Y.; Wassie, L. Variable Diagnostic Performance of Stool Xpert in Pediatric Tuberculosis: A Systematic Review and Meta-Analysis. Open Forum Infect Dis 2021, 8. [CrossRef]
- Togun, T.O.; Kampmann, B. Diagnostics for Childhood Tuberculosis: A Marathon Rather than a Sprint. Lancet Infect Dis 2024, 24, 110–112. [CrossRef]
- Wobudeya, E.; Bonnet, M.; Walters, E.G.; Nabeta, P.; Song, R.; Murithi, W.; Mchembere, W.; Dim, B.; Taguebue, J.-V.; Orne-Gliemann, J.; et al. Diagnostic Advances in Childhood Tuberculosis—Improving Specimen Collection and Yield of Microbiological Diagnosis for Intrathoracic Tuberculosis. Pathogens 2022, 11, 389. [CrossRef]
- Mesman, A.W.; Soto, M.; Coit, J.; Calderon, R.; Aliaga, J.; Pollock, N.R.; Mendoza, M.; Mestanza, F.M.; Mendoza, C.J.; Murray, M.B.; et al. Detection of Mycobacterium Tuberculosis in Pediatric Stool Samples Using TruTip Technology. BMC Infect Dis 2019, 19, 563. [CrossRef]
- Walters, E.; Demers, A.-M.; van der Zalm, M.M.; Whitelaw, A.; Palmer, M.; Bosch, C.; Draper, H.R.; Gie, R.P.; Hesseling, A.C. Stool Culture for Diagnosis of Pulmonary Tuberculosis in Children. J Clin Microbiol 2017, 55, 3355–3365. [CrossRef]
- Mafirakureva, N.; Klinkenberg, E.; Spruijt, I.; Levy, J.; Shaweno, D.; de Haas, P.; Kaswandani, N.; Bedru, A.; Triasih, R.; Gebremichael, M.; et al. Xpert Ultra Stool Testing to Diagnose Tuberculosis in Children in Ethiopia and Indonesia: A Model-Based Cost-Effectiveness Analysis. BMJ Open 2022, 12, e058388. [CrossRef]
- Gunasekera, K.S.; Vonasek, B.; Oliwa, J.; Triasih, R.; Lancioni, C.; Graham, S.M.; Seddon, J.A.; Marais, B.J. Diagnostic Challenges in Childhood Pulmonary Tuberculosis—Optimizing the Clinical Approach. Pathogens 2022, 11, 382. [CrossRef]
- Walters, E.; van der Zalm, M.M.; Palmer, M.; Bosch, C.; Demers, A.-M.; Draper, H.; Goussard, P.; Schaaf, H.S.; Friedrich, S.O.; Whitelaw, A.; et al. Xpert MTB/RIF on Stool Is Useful for the Rapid Diagnosis of Tuberculosis in Young Children With Severe Pulmonary Disease. Pediatric Infectious Disease Journal 2017, 36, 837–843. [CrossRef]
- Mafirakureva, N.; Klinkenberg, E.; Spruijt, I.; Levy, J.; Shaweno, D.; de Haas, P.; Kaswandani, N.; Bedru, A.; Triasih, R.; Gebremichael, M.; et al. Xpert Ultra Stool Testing to Diagnose Tuberculosis in Children in Ethiopia and Indonesia: A Model-Based Cost-Effectiveness Analysis. BMJ Open 2022, 12, e058388. [CrossRef]
- Segala, F.V.; Papagni, R.; Cotugno, S.; De Vita, E.; Susini, M.C.; Filippi, V.; Tulone, O.; Facci, E.; Lattanzio, R.; Marotta, C.; et al. Stool Xpert MTB/RIF as a Possible Diagnostic Alternative to Sputum in Africa: A Systematic Review and Meta-Analysis. Front Public Health 2023, 11. [CrossRef]
- Datta, S.; Gonzales-Huerta, L.E.; Evans, C.A. The Potential for Testing Stool to Reduce Tuberculosis Missed Diagnoses and Misdiagnoses. Am J Trop Med Hyg 2018, 99, 243–245. [CrossRef]
- Jayagandan, S.; Singh, J.; Mudliar, S.R.; Shankar, P.; Maurya, A.K.; Malhotra, A.G.; Malik, S.; Purwar, S.; Singh, S. Evaluation of Xpert MTB/RIF Assay on Stool Samples for the Diagnosis of Pulmonary Tuberculosis among the Pediatric Population. J Lab Physicians 2023, 15, 329–335. [CrossRef]
- Baghaei, P.; Tabarsi, P.; Farnia, P.; Radaei, A.; Kazempour, M.; Faghani, Y.; Mirsaeidi, M.; Novin, A.; Chitsaz, E.; Mansouri, D.; et al. Utility of Gastric Lavage for Diagnosis of Tuberculosis in Patients Who Are Unable to Expectorate Sputum. J Glob Infect Dis 2011, 3, 339. [CrossRef]
- Khambati, N.; Song, R.; MacLean, E.L.-H.; Kohli, M.; Olbrich, L.; Bijker, E.M. The Diagnostic Yield of Nasopharyngeal Aspirate for Pediatric Pulmonary Tuberculosis: A Systematic Review and Meta-Analysis. BMC Global and Public Health 2023, 1, 18. [CrossRef]
- MacLean, E.; Broger, T.; Yerlikaya, S.; Fernandez-Carballo, B.L.; Pai, M.; Denkinger, C.M. A Systematic Review of Biomarkers to Detect Active Tuberculosis. Nat Microbiol 2019, 4, 748–758. [CrossRef]
- Huang, Y.; Ai, L.; Wang, X.; Sun, Z.; Wang, F. Review and Updates on the Diagnosis of Tuberculosis. J Clin Med 2022, 11, 5826. [CrossRef]
- Brent, A.J.; Mugo, D.; Musyimi, R.; Mutiso, A.; Morpeth, S.C.; Levin, M.; Scott, J.A.G. Bacteriological Diagnosis of Childhood TB: A Prospective Observational Study. Sci Rep 2017, 7, 11808. [CrossRef]
- Song, R.; Click, E.S.; McCarthy, K.D.; Heilig, C.M.; Mchembere, W.; Smith, J.P.; Fajans, M.; Musau, S.K.; Okeyo, E.; Okumu, A.; et al. Sensitive and Feasible Specimen Collection and Testing Strategies for Diagnosing Tuberculosis in Young Children. JAMA Pediatr 2021, 175, e206069. [CrossRef]
- Abdullahi, O.; Moses, N.; Sanga, D.; Annie, W. The Effect of Empirical and Laboratory-Confirmed Tuberculosis on Treatment Outcomes. Sci Rep 2021, 11, 14854. [CrossRef]
- Detjen, A.K.; DiNardo, A.R.; Leyden, J.; Steingart, K.R.; Menzies, D.; Schiller, I.; Dendukuri, N.; Mandalakas, A.M. Xpert MTB/RIF Assay for the Diagnosis of Pulmonary Tuberculosis in Children: A Systematic Review and Meta-Analysis. Lancet Respir Med 2015, 3, 451–461. [CrossRef]
- Agarwal, A.; Katoch, C.D.S.; Kumar, M.; Dhole, T.N.; Sharma, Y.K. Evaluation of Microscopic Observation Drug Susceptibility (MODS) Assay as a Rapid, Sensitive and Inexpensive Test for Detection of Tuberculosis and Multidrug Resistant Tuberculosis. Med J Armed Forces India 2019, 75, 58–64. [CrossRef]
- Hamada, Y.; Kontsevaya, I.; Surkova, E.; Wang, T.T.; Liu, V.; Ziganshina, L.E.; Rangaka, M.X.; Denkinger, C.; Abubakar, I. WHO Consolidated Guidelines on Tuberculosis Module 3: Diagnosis. Tests for TB Infection Web Annex B Safety of Mycobacterium Tuberculosis Antigen-Based Skin Tests: A Systematic Review and Meta-Analysis; 2021; ISBN 9789240056602.
- Mastrolia, M.V.; Sollai, S.; Totaro, C.; Putignano, P.; de Martino, M.; Galli, L.; Chiappini, E. Utility of Tuberculin Skin Test and IGRA for Tuberculosis Screening in Internationally Adopted Children: Retrospective Analysis from a Single Center in Florence, Italy. Travel Med Infect Dis 2019, 28, 64–67. [CrossRef]
- Machingaidze, S.; Wiysonge, C.S.; Gonzalez-Angulo, Y.; Hatherill, M.; Moyo, S.; Hanekom, W.; Mahomed, H. The Utility of an Interferon Gamma Release Assay for Diagnosis of Latent Tuberculosis Infection and Disease in Children. Pediatric Infectious Disease Journal 2011, 30, 694–700. [CrossRef]
- Pai, M.; Dewan, P.K.; Swaminathan, S. Transforming Tuberculosis Diagnosis. Nat Microbiol 2023, 8, 756–759. [CrossRef]
- Nurwidya, F.; Handayani, D.; Burhan, E.; Yunus, F. Molecular Diagnosis of Tuberculosis. Chonnam Med J 2018, 54, 1–9. [CrossRef]
- Kohli, M.; Schiller, I.; Dendukuri, N.; Yao, M.; Dheda, K.; Denkinger, C.M.; Schumacher, S.G.; Steingart, K.R. Xpert MTB/RIF Ultra and Xpert MTB/RIF Assays for Extrapulmonary Tuberculosis and Rifampicin Resistance in Adults. Cochrane Database of Systematic Reviews 2021, 2021. [CrossRef]
- Ngangue, Y.R.; Mbuli, C.; Neh, A.; Nshom, E.; Koudjou, A.; Palmer, D.; Ndi, N.N.; Qin, Z.Z.; Creswell, J.; Mbassa, V.; et al. Diagnostic Accuracy of the Truenat MTB Plus Assay and Comparison with the Xpert MTB/RIF Assay to Detect Tuberculosis among Hospital Outpatients in Cameroon. J Clin Microbiol 2022, 60. [CrossRef]
- Gopalaswamy, R.; Kumar, N.; Vashistha, H.; Rajendran, P.; Kayesth, J.; Peravali, C.J.; Kashyap, S.; Ghosh, S.; Yumo, H.; Moore, M.; et al. Comprehensive Assessment of Invalid and Indeterminate Results in Truenat MTB-RIF Testing across Sites under the National TB Elimination Program of India. Front Public Health 2023, 11. [CrossRef]
- Opota, O.; Mazza-Stalder, J.; Greub, G.; Jaton, K. The Rapid Molecular Test Xpert MTB/RIF Ultra: Towards Improved Tuberculosis Diagnosis and Rifampicin Resistance Detection. Clinical Microbiology and Infection 2019, 25, 1370–1376. [CrossRef]
- Kaso, A.W.; Hailu, A. Costs and Cost-Effectiveness of Gene Xpert Compared to Smear Microscopy for the Diagnosis of Pulmonary Tuberculosis Using Real-World Data from Arsi Zone, Ethiopia. PLoS One 2021, 16, e0259056. [CrossRef]
- Bouzouita, I.; Ghariani, A.; Dhaou, K. Ben; Jemaeil, S.; Essaalah, L.; Bejaoui, S.; Draoui, H.; El Marzouk, N.; Mehiri, E.; Slim-Saidi, L. Usefulness of Xpert MTB/RIF Ultra for Rapid Diagnosis of Extrapulmonary Tuberculosis in Tunisia. Sci Rep 2024, 14, 2217. [CrossRef]
- Waters, R.; Laubscher, M.; Dunn, R.N.; Adikary, N.; Coussens, A.K.; Held, M. Higher Sensitivity of Xpert MTB/RIF Ultra Over Tuberculosis Culture for the Diagnosis of Spinal Tuberculosis With Open or Computed Tomography–Guided Biopsies. Open Forum Infect Dis 2024, 11. [CrossRef]
- Slail, M.J.; Booq, R.Y.; Al-Ahmad, I.H.; Alharbi, A.A.; Alharbi, S.F.; Alotaibi, M.Z.; Aljubran, A.M.; Aldossary, A.M.; Memish, Z.A.; Alyamani, E.J.; et al. Evaluation of Xpert MTB/RIF Ultra for the Diagnosis of Extrapulmonary Tuberculosis: A Retrospective Analysis in Saudi Arabia. J Epidemiol Glob Health 2023, 13, 782–793. [CrossRef]
- Lee, D.J.; Kumarasamy, N.; Resch, S.C.; Sivaramakrishnan, G.N.; Mayer, K.H.; Tripathy, S.; Paltiel, A.D.; Freedberg, K.A.; Reddy, K.P. Rapid, Point-of-Care Diagnosis of Tuberculosis with Novel Truenat Assay: Cost-Effectiveness Analysis for India’s Public Sector. PLoS One 2019, 14, e0218890. [CrossRef]
- Desikan, P.; Panwalkar, N.; Mirza, S.; Chaturvedi, A.; Ansari, K.; Varathe, R.; Chourey, M.; Kumar, P.; Pandey, M. Line Probe Assay for Detection of Mycobacterium Tuberculosis Complex: An Experience from Central India. Indian Journal of Medical Research 2017, 145, 70. [CrossRef]
- Ssengooba, W.; Katamba, A.; Sserubiri, J.; Semugenze, D.; Nyombi, A.; Byaruhanga, R.; Turyahabwe, S.; Joloba, M.L. Performance Evaluation of Truenat MTB and Truenat MTB-RIF DX Assays in Comparison to Gene XPERT MTB/RIF Ultra for the Diagnosis of Pulmonary Tuberculosis in Uganda. BMC Infect Dis 2024, 24, 190. [CrossRef]
- Nathavitharana, R.R.; Cudahy, P.G.T.; Schumacher, S.G.; Steingart, K.R.; Pai, M.; Denkinger, C.M. Accuracy of Line Probe Assays for the Diagnosis of Pulmonary and Multidrug-Resistant Tuberculosis: A Systematic Review and Meta-Analysis. European Respiratory Journal 2017, 49, 1601075. [CrossRef]
- Singh, P.; Kanade, S.; Nataraj, G. Performance of Loop-Mediated Isothermal Amplification Assay for Diagnosis of Extrapulmonary Tuberculosis and Antituberculosis Treatment Initiation. The International Journal of Mycobacteriology 2021, 10, 373–378. [CrossRef]
- Nagai, K.; Horita, N.; Yamamoto, M.; Tsukahara, T.; Nagakura, H.; Tashiro, K.; Shibata, Y.; Watanabe, H.; Nakashima, K.; Ushio, R.; et al. Diagnostic Test Accuracy of Loop-Mediated Isothermal Amplification Assay for Mycobacterium Tuberculosis: Systematic Review and Meta-Analysis. Sci Rep 2016, 6, 39090. [CrossRef]
- Bjerrum, S.; Schiller, I.; Dendukuri, N.; Kohli, M.; Nathavitharana, R.R.; Zwerling, A.A.; Denkinger, C.M.; Steingart, K.R.; Shah, M. Lateral Flow Urine Lipoarabinomannan Assay for Detecting Active Tuberculosis in People Living with HIV. Cochrane Database of Systematic Reviews 2019, 2019. [CrossRef]
- Broger, T.; Koeppel, L.; Huerga, H.; Miller, P.; Gupta-Wright, A.; Blanc, F.X.; Esmail, A.; Reeve, B.W.P.; Floridia, M.; Kerkhoff, A.D.; et al. Diagnostic Yield of Urine Lipoarabinomannan and Sputum Tuberculosis Tests in People Living with HIV: A Systematic Review and Meta-Analysis of Individual Participant Data. Lancet Glob Health 2023, 11, e903–e916. [CrossRef]
- Shah, M.; Hanrahan, C.; Wang, Z.Y.; Dendukuri, N.; Lawn, S.D.; Denkinger, C.M.; Steingart, K.R. Lateral Flow Urine Lipoarabinomannan Assay for Detecting Active Tuberculosis in HIV-Positive Adults. Cochrane Database of Systematic Reviews 2016. [CrossRef]
- Schwab, T.C.; Perrig, L.; Göller, P.C.; Guebely De la Hoz, F.F.; Lahousse, A.P.; Minder, B.; Günther, G.; Efthimiou, O.; Omar, S.V.; Egger, M.; et al. Targeted Next-Generation Sequencing to Diagnose Drug-Resistant Tuberculosis: A Systematic Review and Meta-Analysis. Lancet Infect Dis 2024, 24, 1162–1176. [CrossRef]
- Dookie, N.; Khan, A.; Padayatchi, N.; Naidoo, K. Application of Next Generation Sequencing for Diagnosis and Clinical Management of Drug-Resistant Tuberculosis: Updates on Recent Developments in the Field. Front Microbiol 2022, 13. [CrossRef]
- Iyer, A.; Ndlovu, Z.; Sharma, J.; Mansoor, H.; Bharati, M.; Kolan, S.; Morales, M.; Das, M.; Issakidis, P.; Ferlazzo, G.; et al. Operationalising Targeted Next-Generation Sequencing for Routine Diagnosis of Drug-Resistant TB. Public Health Action 2023, 13, 43–49. [CrossRef]
- Ahmed, M.I.M.; Ziegler, C.; Held, K.; Dubinski, I.; Ley-Zaporozhan, J.; Geldmacher, C.; von Both, U. The TAM-TB Assay—A Promising TB Immune-Diagnostic Test With a Potential for Treatment Monitoring. Front Pediatr 2019, 7. [CrossRef]
- Portevin, D.; Moukambi, F.; Clowes, P.; Bauer, A.; Chachage, M.; Ntinginya, N.E.; Mfinanga, E.; Said, K.; Haraka, F.; Rachow, A.; et al. Assessment of the Novel T-Cell Activation Marker–Tuberculosis Assay for Diagnosis of Active Tuberculosis in Children: A Prospective Proof-of-Concept Study. Lancet Infect Dis 2014, 14, 931–938. [CrossRef]
- Trenti, T. Synergy Between Point-of-Care Testing and Laboratory Consolidations. EJIFCC 2021, 32, 328–336.
- Hong, J.M.; Lee, H.; Menon, N. V.; Lim, C.T.; Lee, L.P.; Ong, C.W.M. Point-of-Care Diagnostic Tests for Tuberculosis Disease. Sci Transl Med 2022, 14. [CrossRef]
- Lewinsohn, D.M.; Leonard, M.K.; Lobue, P.A.; Cohn, D.L.; Daley, C.L.; Desmond, E.; Keane, J.; Lewinsohn, D.A.; Loeffler, A.M.; Mazurek, G.H.; et al. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clinical Infectious Diseases 2017, 64, e1–e33.
- Graham, S.M.; Oliwa, J.N. DIAGNOSIS AND MANAGEMENT OF TUBERCULOSIS IN CHILDREN AND ADOLESCENTS A DESK GUIDE FOR PRIMARY HEALTH CARE WORKERS Fourth Edition 2023; 2023;
- World Health Organization Guidance for National Tuberculosis Programmes on the Management of Tuberculosis in Children; World Health Organization, 2015; ISBN 9789241548748.
- World Health Organization WHO Consolidated Guidelines on Tuberculosis Module 5: Management of Tuberculosis in Children and Adolescents; 2022;
- Yerlikaya, S.; Broger, T.; Isaacs, C.; Bell, D.; Holtgrewe, L.; Gupta-Wright, A.; Nahid, P.; Cattamanchi, A.; Denkinger, C.M. Blazing the Trail for Innovative Tuberculosis Diagnostics. Infection 2024, 52, 29–42. [CrossRef]
- Wu, X.; Tan, G.; Ma, J.; Yang, J.; Guo, Y.; Lu, H.; Ke, H.; Li, M.; Tang, Y.-W.; Sha, W.; et al. Assessment of the Cepheid 3-Gene Host Response Fingerstick Blood Test (MTB-HR) on Rapid Diagnosis of Tuberculosis. Emerg Microbes Infect 2023, 12. [CrossRef]
- Sutherland, J.S.; van der Spuy, G.; Gindeh, A.; Thuong, N.T.T.; Namuganga, A.; Owolabi, O.; Mayanja-Kizza, H.; Nsereko, M.; Thwaites, G.; Winter, J.; et al. Diagnostic Accuracy of the Cepheid 3-Gene Host Response Fingerstick Blood Test in a Prospective, Multi-Site Study: Interim Results. Clinical Infectious Diseases 2022, 74, 2136–2141. [CrossRef]
- Qi, Y.; Li, K.; Li, Y.; Guo, D.; Xu, J.; Li, Y.; Gong, W. CRISPR-Based Diagnostics: A Potential Tool to Address the Diagnostic Challenges of Tuberculosis. Pathogens 2022, 11, 1211. [CrossRef]
- Zhang, X.; He, X.; Zhang, Y.; Chen, L.; Pan, Z.; Huang, Y.; Li, H. A New Method for the Detection of Mycobacterium Tuberculosis Based on the CRISPR/Cas System. BMC Infect Dis 2023, 23, 680. [CrossRef]
- Ren, W.; Zhou, Y.; Li, H.; Shang, Y.; Zhang, X.; Yuan, J.; Li, S.; Li, C.; Pang, Y. Development and Clinical Evaluation of a CRISPR/Cas13a-Based Diagnostic Test to Detect Mycobacterium Tuberculosis in Clinical Specimens. Front Microbiol 2023, 14. [CrossRef]
- Huang, Z.; LaCourse, S.M.; Kay, A.W.; Stern, J.; Escudero, J.N.; Youngquist, B.M.; Zheng, W.; Vambe, D.; Dlamini, M.; Mtetwa, G.; et al. CRISPR Detection of Circulating Cell-Free Mycobacterium Tuberculosis DNA in Adults and Children, Including Children with HIV: A Molecular Diagnostics Study. Lancet Microbe 2022, 3, e482–e492. [CrossRef]
- Manyelo, C.M.; Solomons, R.S.; Snyders, C.I.; Mutavhatsindi, H.; Manngo, P.M.; Stanley, K.; Walzl, G.; Chegou, N.N. Potential of Host Serum Protein Biomarkers in the Diagnosis of Tuberculous Meningitis in Children. Front Pediatr 2019, 7. [CrossRef]
- Nathavitharana, R.R.; Garcia-Basteiro, A.L.; Ruhwald, M.; Cobelens, F.; Theron, G. Reimagining the Status Quo: How Close Are We to Rapid Sputum-Free Tuberculosis Diagnostics for All? EBioMedicine 2022, 78, 103939. [CrossRef]
- Walzl, G.; McNerney, R.; du Plessis, N.; Bates, M.; McHugh, T.D.; Chegou, N.N.; Zumla, A. Tuberculosis: Advances and Challenges in Development of New Diagnostics and Biomarkers. Lancet Infect Dis 2018, 18, e199–e210. [CrossRef]
- World Health Organization WHO on tuberculosis (Module 2: Screening); 2021;
- Kazemzadeh, S.; Kiraly, A.P.; Nabulsi, Z.; Sanjase, N.; Maimbolwa, M.; Shuma, B.; Jamshy, S.; Chen, C.; Agharwal, A.; T. Lau, C.; et al. Prospective Multi-Site Validation of AI to Detect Tuberculosis and Chest X-Ray Abnormalities. NEJM AI 2024, 1. [CrossRef]
- Nijiati, M.; Ma, J.; Hu, C.; Tuersun, A.; Abulizi, A.; Kelimu, A.; Zhang, D.; Li, G.; Zou, X. Artificial Intelligence Assisting the Early Detection of Active Pulmonary Tuberculosis From Chest X-Rays: A Population-Based Study. Front Mol Biosci 2022, 9. [CrossRef]
- Kaur, G.; Sharma, N.; Chauhan, R.; Thapliyal, S.; Gupta, R. Tuberculosis Classification Using EfficientNet B3 Deep Learning Architecture. In Proceedings of the 2023 Global Conference on Information Technologies and Communications (GCITC); IEEE, December 1 2023; pp. 1–6.
- Kaviani, P.; Digumarthy, S.R.; Bizzo, B.C.; Reddy, B.; Tadepalli, M.; Putha, P.; Jagirdar, A.; Ebrahimian, S.; Kalra, M.K.; Dreyer, K.J. Performance of a Chest Radiography AI Algorithm for Detection of Missed or Mislabeled Findings: A Multicenter Study. Diagnostics 2022, 12, 2086. [CrossRef]
- Qin, Z.Z.; Ahmed, S.; Sarker, M.S.; Paul, K.; Adel, A.S.S.; Naheyan, T.; Barrett, R.; Banu, S.; Creswell, J. Tuberculosis Detection from Chest X-Rays for Triaging in a High Tuberculosis-Burden Setting: An Evaluation of Five Artificial Intelligence Algorithms. Lancet Digit Health 2021, 3, e543–e554. [CrossRef]
- Kim, H.-J.; Kwak, N.; Yoon, S.H.; Park, N.; Kim, Y.R.; Lee, J.H.; Lee, J.Y.; Park, Y.; Kang, Y.A.; Kim, S.; et al. Artificial Intelligence-Based Radiographic Extent Analysis to Predict Tuberculosis Treatment Outcomes: A Multicenter Cohort Study. Sci Rep 2024, 14, 13162. [CrossRef]
- David, P.M.; Onno, J.; Keshavjee, S.; Ahmad Khan, F. Conditions Required for the Artificial-Intelligence-Based Computer-Aided Detection of Tuberculosis to Attain Its Global Health Potential. Lancet Digit Health 2022, 4, e702–e704.
- Murphy, K.; Habib, S.S.; Zaidi, S.M.A.; Khowaja, S.; Khan, A.; Melendez, J.; Scholten, E.T.; Amad, F.; Schalekamp, S.; Verhagen, M.; et al. Computer Aided Detection of Tuberculosis on Chest Radiographs: An Evaluation of the CAD4TB v6 System. Sci Rep 2020, 10, 5492. [CrossRef]
- Biewer, A.; Tzelios, C.; Tintaya, K.; Roman, B.; Hurwitz, S.; Yuen, C.M.; Mitnick, C.D.; Nardell, E.; Lecca, L.; Tierney, D.B.; et al. Accuracy of Digital Chest X-Ray Analysis with Artificial Intelligence Software as a Triage and Screening Tool in Hospitalized Patients Being Evaluated for Tuberculosis in Lima, Peru. medRxiv 2023. [CrossRef]
- Kazemzadeh, S.; Yu, J.; Jamshy, S.; Pilgrim, R.; Nabulsi, Z.; Chen, C.; Beladia, N.; Lau, C.; McKinney, S.M.; Hughes, T.; et al. Deep Learning Detection of Active Pulmonary Tuberculosis at Chest Radiography Matched the Clinical Performance of Radiologists. Radiology 2023, 306, 124–137. [CrossRef]
- Malhotra, A.; Thompson, R.; De Vos, M.; David, A.; Schumacher, S.; Sohn, H. Determining Cost and Placement Decisions for Moderate Complexity NAATs for Tuberculosis Drug Susceptibility Testing. PLoS One 2023, 18, e0290496. [CrossRef]
- Cates, L.; Crudu, V.; Codreanu, A.; Ciobanu, N.; Fosburgh, H.; Cohen, T.; Menzies, N.A. Laboratory Costs of Diagnosing TB in a High Multidrug-Resistant TB Setting. The International Journal of Tuberculosis and Lung Disease 2021, 25, 228–230. [CrossRef]
- Sohn, H.; Puri, L.; Nguyen, N.A.T.; Van’t Hoog, A.H.; Nguyen, V.A.T.; Nliwasa, M.; Nabeta, P. Cost and Affordability Analysis of TB-LAMP and Xpert MTB/RIF Assays as Routine Diagnostic Tests in Peripheral Laboratories in Malawi and Vietnam. Journal of Global Health Science 2019, 1. [CrossRef]
- Theron, G.; Venter, R.; Smith, L.; Esmail, A.; Randall, P.; Sood, V.; Oelfese, S.; Calligaro, G.; Warren, R.; Dheda, K. False-Positive Xpert MTB/RIF Results in Retested Patients with Previous Tuberculosis: Frequency, Profile, and Prospective Clinical Outcomes. J Clin Microbiol 2018, 56. [CrossRef]
- Thomas, T.A. Challenges in Diagnosing Childhood Tuberculosis HHS Public Access; 2016; Vol. 25;.
- Sohn, H.; Sweeney, S.; Mudzengi, D.; Creswell, J.; Menzies, N.A.; Fox, G.J.; MacPherson, P.; Dowdy, D.W. Determining the Value of TB Active Case-Finding: Current Evidence and Methodological Considerations. The International Journal of Tuberculosis and Lung Disease 2021, 25, 171–181. [CrossRef]
- Weyer, K.; Mirzayev, F.; Migliori, G.B.; Van Gemert, W.; D’Ambrosio, L.; Zignol, M.; Floyd, K.; Centis, R.; Cirillo, D.M.; Tortoli, E.; et al. Rapid Molecular TB Diagnosis: Evidence, Policy Making and Global Implementation of Xpert MTB/RIF. European Respiratory Journal 2013, 42, 252–271. [CrossRef]
- Medina-Marino, A.; Bezuidenhout, D.; Bezuidenhout, C.; Facente, S.N.; Fourie, B.; Shin, S.S.; Penn-Nicholson, A.; Theron, G. In-Home TB Testing Using GeneXpert Edge Is Acceptable, Feasible, and Improves the Proportion of Symptomatic Household Contacts Tested for TB: A Proof-of-Concept Study. Open Forum Infect Dis 2024, 11. [CrossRef]
- Meyer, A.J.; Babirye, D.; Armstrong-Hough, M.; Mark, D.; Ayakaka, I.; Katamba, A.; Haberer, J.E.; Davis, J.L. Text Messages Sent to Household Tuberculosis Contacts in Kampala, Uganda: Process Evaluation. JMIR Mhealth Uhealth 2018, 6, e10239. [CrossRef]
- Maphalle, L.N.F.; Michniak-Kohn, B.B.; Ogunrombi, M.O.; Adeleke, O.A. Pediatric Tuberculosis Management: A Global Challenge or Breakthrough? Children 2022, 9, 1120. [CrossRef]
Figure 1.
Overview of recommended pediatric TB diagnostic samples and tests based on the types, turn-around time and accuracy.
Figure 1.
Overview of recommended pediatric TB diagnostic samples and tests based on the types, turn-around time and accuracy.

| Test | Technology | Time taken | Age | Symptoms and medical history | Target Population | Sample | Accuracy | Technical Simplicity | Recommendations | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pediatric | Adolescents | Adults | |||||||||
| ±Xpert MTB/ RIF and/ or Xpert Ultra | qPCR | <2 h | >15 years | Signs and symptoms of pulmonary TB | - | √ | √ | Sputum | High | Moderately simple; requires moderate training | Initial Diagnosis Strongly recommended |
| <15 years | Signs and symptoms of pulmonary TB | √ | Sputum, gastric aspirate, nasopharyngeal aspirate and stool | Moderate to Low | Strongly recommended | ||||||
| >15 years | Signs and symptoms of pulmonary TB and without a prior history of TB (≤5 years) or with a remote history of TB treatment (>5 years since end of treatment) | - | √ | √ | Sputum | High | Initial Diagnosis Strongly recommended |
||||
| >15 years | Signs and symptoms of pulmonary TB and with a prior history of TB and an end of treatment <5 years | - | √ | √ | Sputum | High | Initial Diagnosis Strongly recommended |
||||
| All | Signs and symptoms of TB meningitis | √ | √ | √ | Cerebrospinal fluid (CSF) | Moderate to Low | Strongly recommended | ||||
| All | Signs and symptoms of extrapulmonary TB | √ | √ | √ | Lymph node aspirate, lymph node biopsy, pleural fluid, peritoneal fluid, pericardial fluid, synovial fluid or urine specimens | Moderate to Low (Strong for rifampicin resistance) | Conditionally recommended (strongly recommended for Xpert MTB/RIF) | ||||
| All | Signs and symptoms of disseminated TB (HIV-positive) | √ | √ | √ | Blood | Moderate to Low | Conditionally recommended | ||||
| >15 years | General population who had either signs or symptoms of TB or chest radiograph with lung abnormalities or both | √ | √ | Blood | Moderate to Low | Conditionally recommended | |||||
| ±Truenat MTB, MTB plus, (Under development: MTB-Ultima, MTB-INH, MTB-BDQ, MTB TB-COVID-19) | Micro RT-PCR | <1 h | All | With signs and symptoms of pulmonary TB | √ | √ | √ | Sputum | Moderate | Moderately simple; requires moderate training | Conditionally recommended |
| ±Truenat MTB-RIF Dx | All | With signs and symptoms of pulmonary TB and a Truenat MTB or MTB Plus positive result | √ | √ | √ | Sputum | Low | Moderately simple; requires moderate training | Conditionally recommended | ||
| ±Moderate complexity automated nucleic acid amplification tests (NAATs) | High-throughput molecular PCR | 6-8 h | All | Signs and symptoms of pulmonary TB | √ | √ | √ | Respiratory samples | Moderate | Requires highly trained facility/ manpower | Conditionally recommended (also for isoniazid and rifampicin resistance) |
| ±Loopamp MTBC assay | Loop-mediated isothermal amplification | <2h | >15 years | Signs and symptoms consistent with TB | √ | √ | √ | Sputum | Low | Simple with moderate training | Conditionally recommended |
| >15 years | Necessary further testing of sputum smear-negative specimens | √ | √ | √ | Sputum | Low | Simple with moderate training | Conditionally recommended | |||
| ±LAM Ag assay | Lateral flow urine lipo-arabino-mannan assay | <1 h | All | In inpatient settings→HIV-positive adults and children with signs and symptoms of TB, CD4 cell count of less than 200 cells/mm3 | √ | √ | √ | Urine | Moderate to Low | Simple with minimal instructions | Conditionally recommended |
| All | In outpatient settings→HIV-positive adults and children with signs and symptoms of TB, CD4 cell count of less than 100 cells/mm3 | √ | √ | √ | Urine | Low | Conditionally recommended | ||||
| ±First-line line-probe assay (LPAs) | Multiplex PCR+ DNA strip reverse hybridization assay | < 48 h | All | Sputum smear-positive specimen or a cultured isolate of Mtb complex (MTBC) | √ | √ | √ | Sputum | Moderate | Requires highly trained facility/ manpower | Conditionally recommended (rifampicin/ isoniazid resistance) |
| Second-line line-probe assays (SL-LPAs)* | Multiplex PCR+ DNA strip reverse hybridization assay | < 48 h | All | Confirmed MDR/RR-TB | √ | √ | √ | Sputum | Moderate to low | Requires highly trained facility/ manpower | Conditionally recommended (Fluoroquinolone resistance detection) |
| ±High complexity reverse hybridization-based NAATs | Multiplex PCR+ DNA strip reverse hybridization assay (targeting the entire pncA gene) | Variable (<24 hrs) | All | Bacteriologically confirmed TB | √ | √ | √ | TB culture isolates | Low | Requires highly trained facility/ manpower | Conditionally recommended (Specialized for pyrazinamide resistance) |
| Next-generation sequencing | Whole genome/ targeted sequencing | < 48 h | All | NA | √ | √ | √ | Sputum, TB culture isolates | High | Requires highly trained facility/ manpower | NA |
| TAM TB assay* | Flow cytometry / TB specific biomarkers CD38/ CD27 | <24 h | All | NA | √ | √ | √ | Blood | Moderate to High | Requires highly trained facility/ manpower | NA |
*Not available commercially; ±WHO recommended.
Table 2.
Some machine learning/AI-based tools designed to escalate TB diagnosis.
| Tool | Accuracy | Input | Key Feature | References |
|---|---|---|---|---|
| CAD4TB (version 7) | 94% sensitivity and 84% specificity | Chest X-rays | Includes modules for registration, symptom screening, X-ray imaging, and integration with GeneXpert systems | [79] |
| EfficientNetB3 | high performance (highest Area Under Curve 0.999) | chest X-rays | A convolutional neural network structure that can accurately detect mislabeled and missed findings | [74]. |
| qSpot-TB | 96% sensitivity | chest X-ray analysis | Received FDA breakthrough device designation | [75] |
| InferRead DR (version 2) | 90% sensitivity and 70.4% specificity | chest X-ray analysis | Screening time is <1 min, no subsequent validation suggested | [76] |
| Lunit INSIGHT | ~89% sensitivity | chest X-ray analysis | Clinical evaluations worldwide show promise in conspicuity among other tools | [76] |
| JF CXR-1 | 94% sensitivity | chest X-rays | Clinical evaluations worldwide show promise working under limited resource | [76] |
| qXR | ~91% sensitivity | chest X-rays | Received FDA/CE clearances | [80] |
| Google Health AI system | Yet to be determined | chest X-rays | A deep learning-based system capable of personalized health management | [81] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



