
Submitted:
30 December 2024
Posted:
02 January 2025
You are already at the latest version
Abstract
Background/Objectives: There is extensive evidence that breastfeeding saves lives, improves health and provides value to the economy and societies worldwide. The Philippines and Viet Nam have progressive policies to enable breastfeeding, and breastfeeding rates in these countries have substantively improved. In the Philippines, exclusive breastfeeding under six months (EBF) increased from 35.9% (2008) to 60.1% (2021) and in Viet Nam, in just over a decade, EBF has more than doubled, from 17.0% (2010) to 45.4% (2021). We aimed to consolidate learnings from policy support to enable breastfeeding in the Philippines and Viet Nam, and synthesized insights highlighting successful implementation strategies and areas for improvement to guide future programming. Methods: This paper presents an evidence synthesis of seven research articles using mixed methods research from the Philippines and Viet Nam. Results: Since the 1960s, the Philippines and Viet Nam have notably improved policies protecting breastfeeding. Both countries have implemented legislation that is substantially aligned with the International Code of Marketing of Breast-milk Substitutes and subsequent World Health Assembly resolutions. Both countries have improved maternity leave provisions, with Viet Nam providing six months of paid leave, yet insufficient coverage to informal workers, and the Philippines providing 3.5 months paid maternity leave while expanding maternity protection coverage to informal workers. Between 2006-2021, breastfeeding rates increased in both countries alongside policy improvements yet barriers to implementation remain. Conclusions: Implementation research has documented policy progress and improved breastfeeding rates in the Philippines and Viet Nam. Our analysis offers valuable lessons applicable beyond these contexts, emphasizing the need for targeted cross-sectoral policy actions to enhance breastfeeding practices. Learnings from implementing national marketing restrictions of commercial milk formula and associated products, and maternity protection policies in these countries could inform the implementation of newly developed regional standards together with supportive policies, facilitating the harmonization of regional regulatory environments.
Keywords:
breastfeeding
; maternal
; infant
; and young child nutrition
; policy implementation
; International Code
; maternity protection
; maternal health
; care economy
; gender equality
; the Philippines
; Viet Nam
1. Introduction
There is extensive and conclusive evidence that breastfeeding saves lives, improves health, and supports economies in countries worldwide [1,2,3,4]. The actions required to improve breastfeeding rates to protect the health of women and children are recognized and established [1,2,5,6]. Yet even though progress in achieving breastfeeding goals has been made, improvements are unequal across countries and remain insufficient to meet the Global Nutrition Target that 50% of infants under six months of age be exclusively breastfed (EBF) by 2025 and the Global Breastfeeding Collective target of 70% EBF by 2030 [7,8].
Many global declarations, policy guidelines, and recommendations for protecting, promoting, and supporting breastfeeding have been made over the past 45 years [9,10,11]. Since 2017, the Global Breastfeeding Collective has prioritized seven policy actions for countries to protect and support breastfeeding [8]:
- Funding: Increase investment in programs and policies to enable breastfeeding
- The International Code of Marketing of Breast-milk Substitutes (The Code): Full implementation with legislation and effective enforcement
- Maternity protection in the workplace: Enact paid family leave and workplace policies
- Baby-Friendly Hospital Initiative (BFHI): Implement the 10 steps to successful breastfeeding in maternity facilities
- Breastfeeding counseling and training: Improve access to skilled breastfeeding counseling in health facilities
- Community support programs: Encourage networks that protect, promote, and support breastfeeding
- Monitoring systems: Track progress on policies, programs, and funding
- Infant and young child feeding support in emergencies: Invest in policies and programs to protect continued breastfeeding during emergency situations
This study focuses on implementation of marketing restrictions for commercial milk formula (CMF) and maternity protection, two priority actions that would greatly contribute to creating an enabling environment for breastfeeding. The need to protect breastfeeding from harmful marketing of CMF has been emphasized since 1939 when the first public call for penalties on such marketing was made [12,13]. The Code was first adopted by the World Health Assembly (WHA) in 1981 as a minimum standard, thereby mandating countries to implement the provisions of the Code through legal measures [9]. At present, the Code comprises this original Code along with subsequent resolutions that reinforce or give clarity to its scope and coverage or provide additional implementation guidance [14,15,16]. The process of implementing legislation should include the adoption of legal measures aligned with global provisions, as well as monitoring and enforcement of such legislation. There is still wide variation in Code adoption and implementation in countries. As of March 2024, 146 (75%) of the 194 World Health Organization (WHO) Member States had adopted legal measures implementing at least some provisions of the Code, while 48 countries still have no national Code legislation [17]. The WHO regions of Africa, the Eastern Mediterranean, and Southeast Asia have the highest percentage of countries substantially aligned with the Code. Exploitative marketing, notably the evolving marketing tactics and political economy underpinning the CMF industry, remains a concern globally and poses a barrier to breastfeeding [6,18,19].
The International Labour Organization (ILO) first defined maternity protection over 100 years ago [20]. The current Maternity Protection Convention (MPC) 183 and Recommendation 191 of 2000 define comprehensive maternity protection for working women who are pregnant, around the time of childbirth, or breastfeeding, as including health protection at the workplace, a period of maternity leave with accompanying cash and medical entitlements, job security and income protection, non-discrimination, breastfeeding or expressing breaks, and access to childcare support [21,22]. The implementation of comprehensive maternity protection requires investment from governments. Comprehensive maternity protection is a form of social security that aims to provide protection for women workers to ensure that their income and employment, together with their and their infants’ health, will not be at risk due to pregnancy, childbirth, breastfeeding, or taking maternity leave [23]. In addition to being a labor rights issue, maternity protection has started being acknowledged as a public health intervention to support breastfeeding with importance to society and for sustainable development and gender equity, including the fulfillment of women’s reproductive rights during the periods of pregnancy, childbirth, and sexed infant care work such as breastfeeding [24,25]. For example, extending paid maternity leave has positive implications for breastfeeding practices [26,27], maternal, infant, and young child health, and maternal mental health [28,29,30]. Similarly, women’s return to work is an established barrier to EBF or breastfeeding continuation [31]. Globally, women carry a disproportionate burden (more than 75%) of unpaid care work [32]. Access to comprehensive maternity protection could contribute to reducing this inequality. Despite the establishment and existence of global standards for maternity protection, as of February 2024, only 43 countries (and not a single country in Asia) have ratified the ILO MPC 183 [33], even though many countries do meet several minimum standards of the convention [34]. Even when maternity protection is legislated, access and implementation remain challenges, especially for vulnerable groups such as “non-standard” workers who usually have minimal and inconsistent access to informal support [35,36,37].
The Philippines and Viet Nam are two Southeast Asian countries and member states of the Association of Southeast Asian Nations (ASEAN) with progressive policies to enable breastfeeding. They were among the first countries to adopt the Convention on the Rights of the Child (CRC), where Article 18 describes State Parties’ obligations and parents’ responsibilities relating to child-rearing. Article 24 of the CRC describes governments’ obligations to respect, protect, and fulfill children’s rights to the highest attainable standard of health and nutritious foods, and this includes women’s rights to have skilled support to enable breastfeeding. The CRC has acknowledged that the public must be protected from improper and biased information, and therefore, implementation of the Code is necessary for governments to fulfill their obligations under the CRC [38,39,40,41]. The Philippines and Viet Nam have made progress in legislating the Code and maternity protection, the implementation of the Baby-Friendly Hospital Initiative, early essential newborn care practice standards, breastfeeding counseling as part of essential health services, and, in Viet Nam, designated Centers of Excellence for Breastfeeding [42]. Breastfeeding rates in these two countries have subsequently increased in recent years and this enabling policy environment therefore warrants further in-depth investigation and documentation. There has been concerted advocacy for supportive policies in these two countries [43,44,45,46,47,48].
Nevertheless, there has also been documented corporate political activity from the CMF industry in the Philippines, which was met with public health resistance [49]. The size of the CMF industry in the Southeast Asia region has expanded [50], and the region has been a target for increased CMF marketing and production [51,52]. Despite fundamental differences in governance structures in the Philippines and Viet Nam and growing commercial influence, policies have remained protective of breastfeeding, likely due to technical assistance and advocacy support from multiple stakeholders [47].
Despite extensive evidence on the importance of breastfeeding and established global policies to support it, there are still significant gaps in understanding the factors that hinder the effective implementation of these policies across diverse settings. Research on the specific challenges countries face in enforcing the Code and comprehensive maternity protection legislation, especially in regions with low adherence, is limited. Additionally, there is a need for more in-depth studies on the role of informal work and economic disparities in limiting access to breastfeeding support and on how targeted advocacy can create enabling environments for breastfeeding in low-resource settings. In this study, we synthesized findings from published research coordinated by the Alive & Thrive initiative and documents on policy implementation in the Philippines and Viet Nam. The aim of this evidence synthesis is to identify insights valuable for future programming, including identifying gaps requiring further action to improve breastfeeding practices in these two countries and lessons that can be learned for similar contexts.
2. Materials and Methods
2.1. Study Design
This paper presents an evidence synthesis of seven purposively selected primary research publications from the Philippines and Viet Nam, summarized in Table 1. The primary research selected for this evidence synthesis was coordinated by the Alive & Thrive initiative (A&T). Those published studies used mixed methods: in-depth interviews, cross-sectional surveys, and secondary data analysis following a published research protocol [44].
2.2. Study Setting
The Philippines is a lower-middle-income country (LMIC) that is a democratic constitutional republic with a highly decentralized government. Table 2 provides further socio-demographic indicators. Around 60% of hospitals are private, and 69.7% of households are covered by any form of health insurance [60]. The proportion of infants EBF has increased from 29.7% in 2003 to 60.1% in 2021 [61,62] (Figure 1). The Philippines has, therefore, met the Global Nutrition Target of 50% by 2025, and if this rate of increase is maintained, it will meet the target of 70% by 2030. Despite this encouraging trend, it is important to acknowledge that the Philippines has large geographic inequalities in EBF practices [63].
The Philippines was one of the first countries to ratify the CRC in 1990 [64] but has not ratified the ILO MPC 183 [33]. The Philippines was one of the first countries to legislate the Code in 1986 and has updated its implementation rules to substantially align with the Code since 2006 [17]. The CMF industry in the Philippines is dominated by two international companies, Nestle and Reckitt Benckiser (Mead Johnson), which have controlled 94% of the market share as of 2020 [49]. In 2020, the CMF market in the Philippines was the 8th largest globally, at US$832.2 million spent on CMF in total and an annual per capita expenditure on CMF of US47.6 [65]. The CMF industry in the Philippines has continued with intensive marketing strategies, including the documented use of corporate political activity [49]. Despite not yet ratifying ILO MPC 183, the country has multiple policies for maternity protection, including provisions for paid lactation breaks, establishment of breastfeeding spaces, protection against gender discrimination, and other forms of workplace breastfeeding support. It was not until 2019 that duration of paid maternity leave was extended from 8-11 weeks/60-78 days to 15 weeks/105 days [66] to align with ILO Standards. The female labor force participation rate in the Philippines is 52.9% compared to males at 76.3% [67]. These rates have been fairly stable since 1990 [68]. The rate of vulnerable employment (i.e., least likely to have formal work arrangements, social protection, and safety nets) among women has decreased from 47.5% in 1990 to 38.5% in 2022. This is lower than the average in the East Asia and Pacific region and the average among LMIC [68]. However, rates of informal employment are not routinely reported and have been recently redefined by the ILO. Some researchers have recently estimated that overall informal employment in the Philippines (men and women combined) may exceed 80% [69]. See Table 2 for more sociodemographic indicators.
Viet Nam is a lower-middle-income country that has a socialist republic with a highly centralized government. Table 2 provides further sociodemographic information. Rates of EBF under six months increased in Viet Nam from 17.0% in 2010, to 24.0% in 2014 and 45.4% in 2021 [70,71], demonstrating progress towards achieving the global nutrition targets of 50% by 2025 and 70% by 2030 [72] (Figure 1). Similarly to the Philippines, even within the context of increased national EBF rates, Viet Nam also has geographic inequalities in EBF practices [63]. Some breastfeeding indicators (early initiation of breastfeeding and bottle feeding) and the rates of cesarean sections have worsened between 2011 and 2020 [73]. Viet Nam was the first country in Asia and second in the world to ratify the CRC. The Government has adopted and amended many related policies since then to fulfill rights and the government’s obligations, including the Code and maternity protection (even though Viet Nam has not yet ratified the MPC). The Vietnamese legislation implementing the Code has been moderately aligned with global guidance since 2014 [17] and incorporates restrictions on the marketing of CMF for pregnant or breastfeeding women even though manufacturers widely disregard these. The CMF industry in Viet Nam is competitive, has experienced recent growth, and includes a variety of domestic and global manufacturers [74]. In 2018, at least 28 new formula products entered the market [75]. In 2019, Vinamilk and Nutifood made up 36% of the Vietnamese CMF market, followed by Abbott (17%), Friesland Campina (11%), Mead Johnson (9%), Nestle (8%), and others (9%) [76]. In 2020, the CMF market in Viet Nam was the 4th largest globally at US$1,421.2 million and an annual per capita expenditure of US$14.6 [65]. Viet Nam has advanced gender equality policies and was an early adopter of maternity protection, currently providing 26 weeks (six months) of paid maternity leave to women working formally. Viet Nam also has a higher female labor force participation rate (61.6% at 2021) than regional and global averages, but female labor force participation has decreased slightly since 1990 [77]. There is a high rate of informality among female workers in Viet Nam (67.2% in 2021) [78], although rates of vulnerable employment among women have decreased from 86.4% in 1991 to 57.3% in 2022 [77].
The Philippines has a higher crude birth rate than Viet Nam (21.8 per 1,000 in the Philippines compared to 15.0 per 1,000 in Viet Nam) [79]. Despite this, per capita expenditure on CMF in Viet Nam is almost double that of the Philippines (Table 2). This could be due to higher rates of exclusive and continued breastfeeding in the Philippines compared to Viet Nam and/or unnecessary supplementation with CMF in children over one year of age (in the Philippines), when they could be fed with complementary foods and regular animal milks (Table 2). Figure 1 shows that in the Philippines, EBF rates have steadily increased between 2003 and 2021 while in Viet Nam there was a decline between 2000 and 2006 with a steady increase from 2006 to 2021.
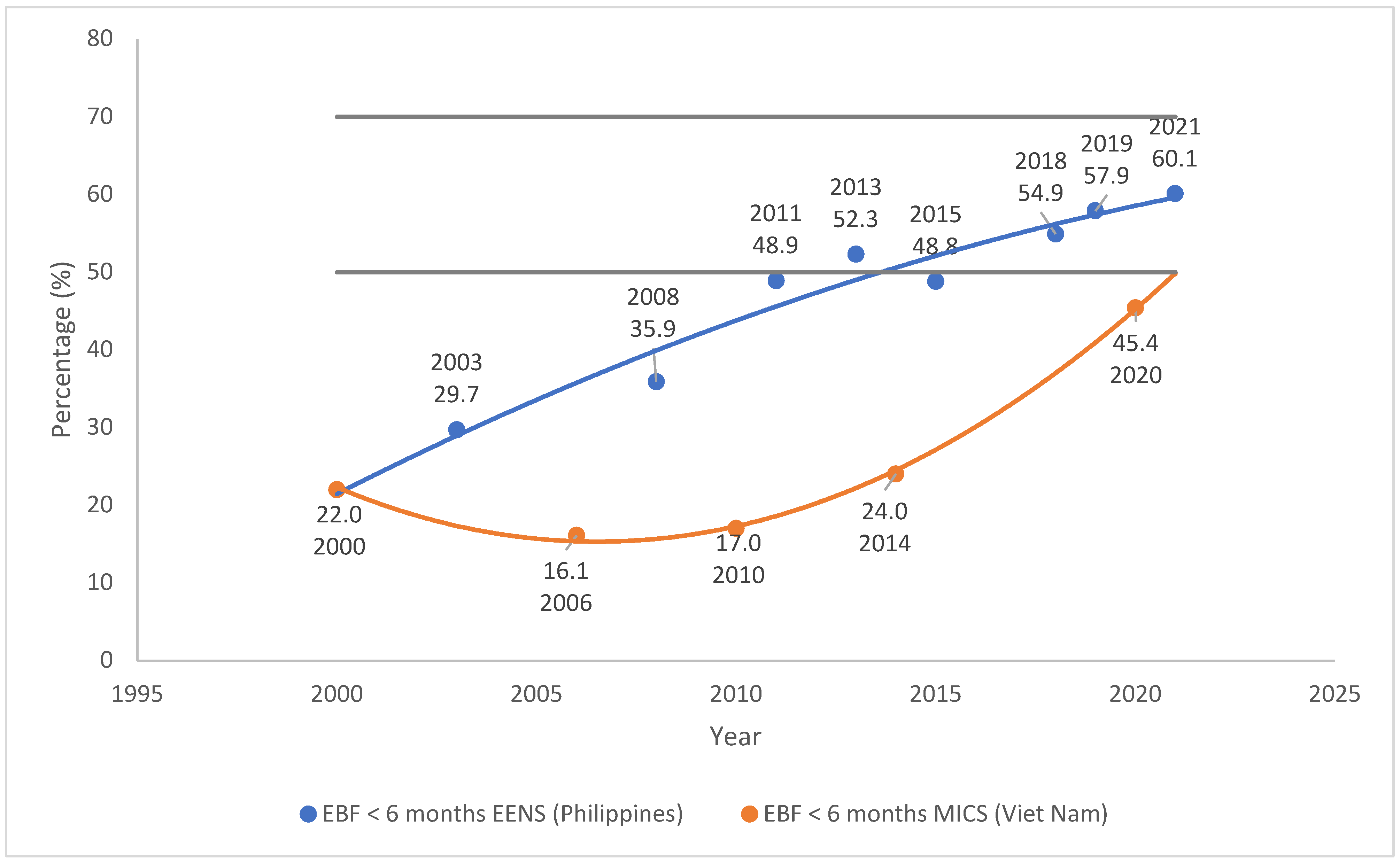

Table 2.
Sociodemographic indicators for the Philippines and Viet Nam.
| Socio-demographic indicator | Philippines | Viet Nam |
| Population | 115 559 009 [80] | 98 186 856 [81] |
| Urban: rural | 48:52 [82] | 39:61 [82] |
| Life expectancy | 69.3 years [83] | 73.6 years [83] |
| Fertility rate | 1.9 (2022) [84] | 1.9 [83] |
| Institutional birth rate | 89% (2020) from 50.5% (2010) | 96.3% |
| Crude birth rate (per 1000 people) | 21.8 (2021) [79] | 15.0 (2021) [79] |
| Public: private hospitals | 40:60 | 86:14 |
| Exclusive breastfeeding < 6 mo. | 34.0% (2008); 60.1% (2021) [62] | 17.0% (2010); 24.0% (2014); 45.4% (2021) [85] |
| Continued breastfeeding (% children 12-23 months fed breastmilk the previous day) | 57.1% (2022) [84] | 43.9% (2020) [85] |
| Immediate skin-to-skin contact | 71% [84] | 59% [86] |
| Stunting in children < 5 years | 26.7% (2021) [62] | 19.5% |
| Unemployment (2023) | 4.4% | 2.0% |
| Labor force participation rate | Men: 76.3%; Women: 52.9% [68] | Men: 74.3% Women: 61.6% [87] |
| Vulnerable employment 1 | 2022: Men: 30%; women: 38.5% [68] | 2022: Men: 46.9%; women: 57.3% [77] |
| Informal employment | 38.9% [88] | 2019: Men: 78.9 %, Women: 67.2% [78] |
| Commercial milk formula market | 2020: 8th largest globally: US$832.2 million in total US$7.6 annual per capita expenditure [65] |
2020: 4th largest globally: US$ 1,421.2 million in total US$14.6 annual per capita expenditure [65] |
“Workers in vulnerable employment are the least likely to have formal work arrangements, social protection, and safety nets to guard against economic shocks; thus, they are more likely to fall into poverty.” - https://genderdata.worldbank.org/countries/philippines.
Figure 1.
Exclusive breastfeeding under 6 months in the Philippines and Viet Nam. Abbreviations: EENS: Expanded National Nutrition Survey; MICS: Multiple Indicator Cluster Survey. Sources of data: Philippines Expanded National Nutrition Survey (ENNS) of 2019 and 2021 [61,62]; UNICEF Data Warehouse: Viet Nam Exclusive breastfeeding (0-5 months) [70].
Figure 1.
Exclusive breastfeeding under 6 months in the Philippines and Viet Nam. Abbreviations: EENS: Expanded National Nutrition Survey; MICS: Multiple Indicator Cluster Survey. Sources of data: Philippines Expanded National Nutrition Survey (ENNS) of 2019 and 2021 [61,62]; UNICEF Data Warehouse: Viet Nam Exclusive breastfeeding (0-5 months) [70].
2.3. Collating, Synthesizing, and Reporting the Results
All included studies were read, re-read, and summarized by CPK. The results from the seven included studies were extracted and synthesized using deductive content analysis to code and categorize information. The conceptual model proposed in the protocol was used as a framework to describe how breastfeeding rates increased in the context of evolving structural and environmental determinants of breastfeeding, including strengthened regulation of CMF marketing and improved maternity protection [44]. A more detailed description of the seven studies is provided in Table 1. The various syntheses that were conducted are presented in the results as boxes, tables, and figures, including milestones of main changes to legislation, lessons learned, barriers to implementing legislation, and recommendations to improve policy implementation to enable breastfeeding in the Philippines and Viet Nam.
2.4. Ethical Considerations
Since this manuscript presents a synthesis of secondary data, ethical approval was not required for this study. Appropriate ethical approvals were obtained, and ethical principles were used in the primary data collection. The original study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of FHI 360 (protocol code 1383644; approved on 16 April 2019), the Hanoi University of Public Health (protocol code 019-501/DD-YTCC; approved on 12 June 2019) and St. Cabrini Medical Center-Asian Eye Institute Ethics Review Committee (SCMC-AEI ERC) (protocol code 2020-027; approved on November 20, 2020).
3. Results
3.1. Overview of Policies to Enable Breastfeeding in the Philippines and Viet Nam
There are comprehensive and long-standing policies and legislation to protect, promote, and support breastfeeding in the Philippines and Viet Nam, many of which are consistent with global standards. Figure 2 summarizes the key policies and legislation to protect breastfeeding (i.e., key milestones for maternity protection provision and Code implementation). Box 1 and Table 3 summarize Code implementation legislation in the Philippines and Viet Nam. Table 4 and Figure 2 summarize paid maternity leave provision in the Philippines and Viet Nam, compared to global guidance.
3.2. Implementation of Code Legislation in the Philippines and Viet Nam
The Philippines and Vietnam have implemented legislation that aligns with the Code for over 20 years. The Philippines, an early adopter in 1986, is substantially aligned with the Code [57,89]. The establishment of an Inter-Agency Committee (IAC) overseeing all advertising and promotional materials within the scope of the Philippine Milk Code [57] has been described as the best-functioning part of the monitoring and enforcement system in the Philippines [90]. In Viet Nam, Decree 100 was moderately aligned with the Code in 2014, but since 2020, legislation has been substantially aligned. Viet Nam is one of the only countries with some, albeit limited, restrictions on the marketing of CMF for pregnant women (CMF-PW). Real-time policy evaluations from 2015 to 2017 in Viet Nam identified opportunities used to strengthen national Code legislation. These include integrating Code provisions into existing laws, namely the Advertisement Law. This allowed a more simplified process by already having a legal basis for developing subsequent sub-laws and preventing the need to create new enforcement mechanisms from the start [53]. Another opportunity was the leveraging of advocacy efforts to maintain stringent advertising bans. In mid-2016, when companies opened the vote and were advocating for the advertising ban to be lowered to 12 months (from 24 months), one champion acted quickly to counter this, making a compelling case to voting members of Parliament by framing the extension of the advertisement ban to 24 months as a clear and unambiguous child rights and people-centered approach. This was successful in ensuring that the scope of the advertising ban was maintained and demonstrated the need for constant vigilance against industry tactics [53]. During implementation, letters were sent to companies describing forthcoming legislative changes and their obligations [53] and Viet Nam prioritized training workshops, dissemination of compliance results, and media monitoring, leading to successful enforcement [53]. In Viet Nam, “street-level bureaucrats,” described as public sector workers detecting and reporting violations of legislation, were reported as playing an important role in Code implementation, and it would be strategic to ensure they are adequately trained [47]. The achievements in Viet Nam have served as a model for progress in other countries in the region.
Reported Code violations and implementation of legislation in Viet Nam show inconsistent compliance. Data from 2020 indicates a reduction in the promotion of CMF by health workers in health facilities, correlating with high compliance scores on the latest Code Status report [54,89]. Hospital and health leaders demonstrate a good understanding of the Code, supported by policies prohibiting company representatives from promoting substitutes at facilities. The Ministry of Health (MoH) oversees the monitoring of Decree 100 through various agencies, including the Viet Nam Food Administration (VFA) and health inspection bodies. Code implementation in health facilities is integrated into routine assessments as one of 83 criteria of the National Hospital Standards and Accreditation for both public and private hospitals, with self-assessments followed by verification from MoH and provincial health departments [54,90]. Outside the health system, the VFA conducts periodic inspections of food safety and labeling, while promotional activities at the point-of-sale are monitored by the Ministry of Commerce's Inspectors [90]. The Philippines and Viet Nam are two of the 37 countries that have explicitly included provisions regulating the promotion of breastmilk substitutes on digital platforms in their current national legislative frameworks.
3.3. Implementation of Maternity Protection Legislation in the Philippines and Viet Nam
Both countries meet the minimum requirements of the ILO MPC 183 for the length of maternity leave provided. It is appropriate that in both countries, maternity leave cash payments are 100% of previous earnings and paid breastfeeding breaks are provided [34]. Maternity protection entitlements in the Philippines have recently been improved to align more closely with international standards [59] with the Expanded Maternity Leave Law (EMLL) increasing paid maternity leave to 15 weeks in 2019, in line with the ILO MPC 183 but not the ILO MP Recommendation 191 (18 weeks) nor WHO EBF recommendation (26 weeks) (Figure 2). There is mixed source funding for cash payments, from social security and employers, since 2019. The Labor Code of the Philippines and EMLL prohibit discrimination against employing women [66,91]. Medical entitlements for mothers are provided through the Philippine Health Insurance Corporation (PhilHealth), a government-managed social health insurance program. There are comprehensive policies to mandate workplace breastfeeding support [59], for example, the Expanded Breastfeeding Promotion Act of 2009 mandates [92]:
- establishment of lactation rooms
- implementation of lactation breaks in workplaces
- workplaces are required to create a breastfeeding policy
- workplaces are required to comply with the Philippine Milk Code
- compliance with the Act is required to issue/renew business permits
- workplaces can apply for renewable exemptions in establishing lactation rooms if exemptible criteria are met
-
workplaces can apply for the Mother-Baby-Friendly Workplace Certification (valid for two years) by complying with this Act and fulfilling additional requirements set by the Department of Health.
- ∘
- Review and assessment of applications is assigned to local government units
- ∘
- Onsite inspection and approval of certification is conducted by DoH Centres for Health Development
The implementation of these lactation support policies was reported to vary according to workplace and type of work. Some employers reported having additional policies such as flexible working arrangements, free transport, additional cash assistance, free medical check-ups, and/or free childcare [59].
Viet Nam has advanced maternity protection policies, providing six months of maternity leave paid at 100% of previous earnings to women employed formally, with high uptake and moderate awareness of maternity protection entitlements among formally employed women [56]. More than 90% (91.7%) of formally employed women contribute to the public social insurance fund, the Viet Nam Social Security (VSS), coordinated by the Ministry of Labour, Invalids and Social Affairs [56].
3.4. Barriers to Implementation of Legislation to Enable Breastfeeding in the Philippines and Viet Nam
Even after more than two decades of national legislation implementing the Code in the Philippines and Viet Nam, there are still implementation gaps in both countries, relating to adoption, enactment, monitoring and enforcement of legislation (Table 5).
3.4.1. Barriers to Implementing Code Legislation in the Philippines
Although the Philippines has long-standing comprehensive legislation aligned with the Code, recent evidence indicates ongoing CMF marketing and violations [57]. This may be due to structural gaps in legislation allowing promotion to the general public and insufficient labeling provisions [57,89]. Inadequate restrictions on industry-funded research and the sponsorship of health professionals and academics result in conflicts of interest (COI) [90]. Even though the Philippines scores 10/10 for monitoring and enforcement on the global Code Status Report, weak monitoring and inadequate enforcement of the Philippine Milk Code have been recently documented from interviews with health workers and policymakers [57]. The DoH has the primary responsibility for implementing the Philippines Milk Code. Still, it has not established the monitoring teams mandated in the 2006 Rules and Implementing Regulations (IRR) and does not conduct regular inspections [90]. Ambiguity surrounding monitoring responsibilities further hampers enforcement [57], and sanctions for Code violations are too weak. These all contribute to large implementation gaps, facilitating inappropriate marketing and reducing the effectiveness of national legislation [57]. Despite this, some Filipino health workers and from the public viewed the regulations as overly strict, especially the prohibition on product donations during emergencies [57].
3.4.2. Barriers to Implementing Code Legislation in Viet Nam
In Viet Nam, the Ministry of Health (MoH) conducts routine monitoring of certain aspects of Code implementation through hospital accreditation, but significant limitations exist. The Code is mentioned in only one of 83 quality standards, making it easily overlooked. Accreditation relies on self-assessment or pre-notified MoH inspections, allowing facilities and manufacturers to prepare, resulting in few Code violations being identified. Data on health inspections are unavailable, and enforcement is limited by human resource constraints and pro-industry tendencies [54,90]. There is no specified agency to monitor digital marketing, which CMF manufacturers exploit [90]. Recent evidence in Viet Nam shows continued promotion of CMF in health facilities (through company representatives), shops and pharmacies, at home (e.g., delivery of formula samples), and through digital channels [54]. While increased awareness among health workers and hospital leaders has reduced access for CMF company representatives, some contact persists [54]. Research conducted by the WHO and UNICEF between 2019-2021 reported that CMF companies frequently contact health professionals in public and private settings, with some private hospitals accepting payments to promote certain brands. In Viet Nam, 19% of women reported seeing promotional booths in health settings, often offering free samples in exchange for contact details, followed by calls and promotions. Research by Alive & Thrive confirmed invasive tactics like collecting personal information through photographs or health records and approaching pregnant women and mothers directly [54]. Some CMF manufacturers purposefully recruit former hospital staff as representatives who may dress in company uniforms, misleading mothers into thinking they are health workers [54].
Companies exploit gaps in legislation to target pregnant women for CMF-PW promotion, using prohibited tactics (e.g., acquiring contact information during pregnancy, providing free samples of CMF-PW in facilities, and advertising free samples on social media) [54]. Misleading claims about CMF-PW, including those about brain development and the inclusion of "novel" ingredients, are widespread [55]. In Viet Nam, industry-sponsored research has influenced national nutrition guidelines for pregnant and lactating women, with MoH endorsement, likely influencing health workers. The industry also sponsors health professionals' attendance at events and provides financial support to health centers, creating conflicts of interest and leading to product promotion by health professionals [55].
3.4.3. Barriers to Implementing Maternity Protection Legislation in the Philippines
Maternity protection policies in the Philippines are mostly aligned with ILO standards since 2019, but the 15-week paid maternity leave falls short of the WHO’s recommended six months (26 weeks) for EBF. Access to maternity entitlements in the Philippines is limited, especially for informally employed women not covered by the Social Security System (SSS), which only reaches 54% of workers nationally [59]. Lactation support at workplaces varies, with some employers (e.g., in Greater Manila) providing lactation rooms, while others offer minimal support or refer women to external facilities [59]. Local government units (LGUs) were encouraged to establish lactation support for informal workers and form partnerships with the private sector, but this is not widespread. Despite awareness of lactation policies, few mothers use available facilities due to perceived inconvenience and challenges such as lack of equipment, workload, inadequate breaks, and unsuitable environments, particularly in the informal sector [59]. Women who work in output-based jobs face the difficult choice between breastfeeding and income generation [59]. Some employers exploit short-term contracts to avoid maternity entitlements, while others lack awareness of their responsibilities, leading to inadequate support for breastfeeding [57] and relying on mothers' initiatives rather than employers actively sharing information [59]. The absence of systematic monitoring and enforcement, unclear roles for government agencies, and limited workplace inspections further hinder effective implementation [59]. Voluntary mechanisms like the Mother-Baby Workplace Certification lack sufficient uptake. Additionally, the disconnect between maternity protection and breastfeeding promotion, along with unsupportive social norms, limits workplace support for breastfeeding [59].
3.4.4. Barriers to Implementing Maternity Protection Legislation in Viet Nam
Gaps in implementing maternity protection legislation in Viet Nam include limited awareness among mothers of legal entitlements, delays in accessing cash entitlements, and workplace discrimination based on pregnancy and childbirth [56]. Awareness among formally employed women is higher for paid maternity leave (78.7% of pregnant women and mothers) and breastfeeding breaks (62.3%) compared to antenatal care leave (only 35%) and other rights like health protection, job security, and non-discrimination. Some women mistakenly perceived maternity protection as employer-provided benefits rather than legal entitlements financed through social insurance [56]. While most women (over 90%) acknowledge the mental health and social benefits of maternity leave, fewer perceive its income benefits (59.5%), career advancement (46.4%), or advantages to employers [56]. Many mothers on maternity leave do not receive the cash entitlements they need during this crucial time, with only 69.3% of mothers with infants 0-5 months and 86.3% of women with infants 6-11 months receiving timely payments [56]. Reasons for these delays include late employer submissions, lack of bank accounts, and delayed evidence of childbirth [56]. Some women (4.9%-6.5%) reported returning to work early due to insufficient or absent cash payments. Recent research in Viet Nam among formally employed women highlights discriminatory hiring and employment practices, with 16% of women asked to confirm they were not pregnant and 33.6% questioned about marital or pregnancy plans. Some were even pressured not to conceive within the first two years of employment and or to resign upon becoming pregnant. Many reported inappropriate working conditions for pregnant women or mothers of infants, with three-quarters experiencing issues like prolonged sitting or standing and 15% experiencing unfair treatment at work [56].
Viet Nam's extended paid maternity leave policy has had unintended negative consequences on women's labor force participation. In certain demographics, the policy change was linked to a reduced likelihood of women having formal labor contracts [58]. Analysis of Labor Force Surveys from 2015-2018 revealed that despite the implementation of extended leave, there was no increase in the likelihood of women holding paid or formal jobs three to five years after childbirth [58].
3.5. Recommendations to Improve the Implementation of Policies to Enable Breastfeeding in the Philippines and Viet Nam
The papers reviewed and synthesized provided comprehensive recommendations, summarized in Table 6. Both countries should implement social and behavior change communication strategies to raise awareness of Code legislation and promote breastfeeding. Improved breastfeeding counseling, community and health system support, and continuous training for health professionals are essential. Effective monitoring, political commitment, and enforcement are crucial to protect breastfeeding (Table 6). To improve maternity protection in the Philippines and Viet Nam, paid maternity leave should be extended to six months in the Philippines. It should be more accessible for the informal sector in both countries by reducing contribution requirements and expanding coverage. Strengthening communication about entitlements, promoting supportive work environments, and improving awareness of social security programs are crucial. Strengthened policy enforcement, inter-agency monitoring, and public or social insurance funding for paid leave are needed. Government-workplace partnerships should support breastfeeding programs.
4. Discussion
Since the 1960s, the Philippines and Viet Nam have made significant improvements to breastfeeding policies and between 2006-2021, breastfeeding rates have increased in both countries. The Philippines and Viet Nam have largely aligned their legislation with the Code and WHA resolutions, with the Philippines among the first to legislate the Code. Both countries have improved maternity protection, with Viet Nam being an early adopter of adequate paid maternity leave. Viet Nam currently provides six months of paid maternity leave to formal workers but has yet to extend this entitlement to informal sector women, who comprise at least 60% of the female labor force. The Philippines meets global minimum requirements for paid maternity leave and is working to extend coverage to informal workers. This positive policy environment has likely played an important role in contributing to increased EBF rates in both countries over the past two decades. However, gaps remain in regulatory frameworks that serve to protect breastfeeding. Some laws still lack clarity, and the full implementation and impact of recent legislation are still emerging. Recent studies indicate that while progress has been made, there is still room for better alignment between national nutrition strategies and global standards in Southeast Asia [94,95]. Additionally, the lack of policy coherence and disjointed links with efforts to address individual barriers through social and behavior change communication continue to limit policy impact and effectiveness.
4.1. National Code Legislation in the Philippines and Viet Nam
The CMF market has grown in the Asia-Pacific region, where sales nearly doubled, from US$18.7 billion in 2010 to US$36.4 billion in 2020, and by 2020, 68% of global CMF sales were from Asia-Pacific [65]. Given the size and power of the CMF industry in the region, regulation (in the form of national Code and maternity protection legislation) becomes a necessary strategy to counteract this dominance and ensure a fairer playing field for public health. Gaps in the content of Code legislation in the Philippines and Viet Nam are clear. Both countries need to determine actions to fully implement the recent WHO guidance on regulatory measures to restrict digital marketing of breastmilk substitutes [96]. The CMF industry’s “marketing playbook” has been well described and documented [18], including the use of cross-promotion and product range extension beyond common CMF products. For example, recent research from Viet Nam reported that 19.5% of mothers had given colostrum milk powder to infants under six months [97]. Policymakers should ensure these strategies are acknowledged when strengthening national Code legislation. Deciding on the most appropriate mechanism to improve Code legislation is complex, with risks and benefits. However, the actors involved should ensure that industry lobbying does not weaken existing legislation. There are examples of successful resistance to corporate political activity from both the Philippines and Viet Nam [45,49] and governments need to recognize evolving tactics to indirectly weaken national Code legislation, such as lobbying around corporate social responsibility [98].
Despite strong Code legislation in both countries, barriers remain. Representatives of CMF companies still have a presence in health facilities in Viet Nam [54,75], while Code violations persist in the Philippines [57,99,100]. This demonstrates how manufacturers exploit any gaps in national legislation for marketing purposes. The Code and subsequent WHA resolutions should be viewed as minimum standards, which countries should adopt in full, aiming to score 100/100 on Code Status Reports, together with robust monitoring and enforcement. This is essential in the context of pervasive marketing. The Philippines and Vietnam experience challenges similar to those faced by many countries in monitoring and enforcing Code legislation. The NetCode Ongoing Monitoring System Protocol should be institutionalized in all countries, with strong civil society involvement [93]. Monitoring and enforcement should align with new WHO digital marketing recommendations, potentially leveraging artificial intelligence (AI) tools to support monitoring activities with support from civil society organizations to enhance sustainability. In the Philippines a citizen reporting platform was developed that encouraged crowd-based monitoring [101,102,103,104]. Unfortunately, challenges arose in maintaining enforcement actions against violators of the Philippines Milk Code [90], and these efforts were not sustained beyond 2019. In Viet Nam, the Virtual Violations Detector (VIVID) was launched in October 2022 and developed through a partnership between Alive & Thrive and the Vietnamese government. VIVID is an automated online program using AI and supervised machine learning to detect violations of Code-relevant national legislation on digital platforms [105,106,107]. This tool has successfully detected large numbers of online Code violations [108] and demonstrates the potential for sustainable government-led monitoring strategies to ensure legislation enforcement on digital platforms.
4.2. Maternity Protection Legislation in the Philippines and Viet Nam
In the Philippines, limited awareness of legal entitlements among workers and employers, together with employers’ perceived disadvantages of maternity protection policies [59], highlight the need for improved social and behavior change communication. These interventions are crucial to raising awareness of the importance of these policies for enabling breastfeeding and advancing policy coherence. Also, challenges persist in accessing maternity protection entitlements in the Philippines, despite their availability. Similar issues regarding accessing cash payments during maternity leave were observed in South Africa [35,109]. Complex administrative processes and bottlenecks hinder women, particularly informal workers, from fully realizing their entitlements. The ILO has recently recommended removing administrative barriers to accessing social insurance, especially among informal workers [110]. Governments should consider implementing measures such as Centers of Excellence for Breastfeeding and context-specific toolkits to support breastfeeding in the workplace, as Viet Nam [111,112] and the Philippines have done [113].
The conflicting findings in Viet Nam reveal potentially negative implications for women, that improved paid maternity leave policies don’t necessarily increase the likelihood of women having a paid, formal job 3-5 years after giving birth [58], demonstrating unintended consequences of policy incoherence. Reasons for limitations on women’s labor force participation despite policy reforms include maternity leave pay being less than previous earnings, late payment of maternity entitlements, and inaccessible, unaffordable childcare for children under two years [58]. A contrasting positive implication of improved maternity protection policy in Viet Nam, is that longer paid maternity leave is associated with increased formal employment and less unpaid work among women [114]. Therefore, it is important that other policies incorporate provisions that protect and promote women and children’s rights. Integrating other international labor conventions can help strengthen and improve maternity protection policies [47]. Women working informally or in rural areas still have limited access to maternity protection in Viet Nam [47], prompting advocacy for policy expansion [115]. Viet Nam’s Social Insurance Law is currently being amended to provide a one-time maternity allowance to informal sector employees who contributed to the voluntary insurance scheme, but the proposed amount is minimal (US$90). The allowance should be increased to at least the level of the urban poverty line [36] to ensure that mothers and babies do not enter into poverty due to childbirth and entitlements should be expanded to all informal workers, with adequate budgetary support [115]. The cost for providing adequate maternity allowances is less than the health consequences for mothers and children when paid maternity leave and breastfeeding support are unavailable or inaccessible [115]. A key lesson from Viet Nam’s maternity protection policy is that inclusive maternity protection for formal and informal workers should not be separate advocacy exercises, and all working women should be eligible for maternity protection, regardless of their place or sector of work.
International conventions do not yet stipulate paternity leave. The Philippines and Viet Nam provide four and five days of paid paternity leave, respectively [116]. Without appropriate paternity leave provisions, women continue to bear the disproportionate load of unpaid domestic and care work. These unequal gender norms perpetuate gender inequality.
A recent systematic literature review reported that over 80% of studies described the impact of returning to work on breastfeeding duration and CMF initiation as key aspects of women’s experiences when returning to work following maternity leave [31]. Work-related factors that facilitate breastfeeding continuation upon return to work include workplace breastfeeding support policies, lactation room facilities, breaks for expressing breastmilk, breastfeeding support groups, on-site childcare [31], and paid maternity leave. This review recommended more research on women’s lived experiences when returning to work after maternity leave and especially the impact on maternal mental and physical health.
The Philippines and Viet Nam governments should ratify ILO MPC 183 to ensure accountability for providing maternity protection entitlements. ILO conventions are not universally ratified, and in LMIC, this may be influenced by the economic costs of ratification [117]. Countries should be encouraged to implement maternity protection policies that go beyond ILO minimum requirements. Global organizations have started to recommend six months of paid maternity leave at 100% pay to all women, regardless of income, employment, or immigration status [25].
The policy change processes in Viet Nam, which started in 2009, have led to improved infant and young child feeding (IYCF) policies [46] and increased breastfeeding rates. This process has been supported by an initiative through efforts from Alive & Thrive, UNICEF, and partners in seven Southeast Asian countries, including Viet Nam using the Collective Impact framework [46]. This has expanded to other countries in the region and involves establishing partnerships, building evidence, developing messages and materials, and fostering consensus [46]. The process has been evaluated and challenges encountered during expansion, partly attributed to the complex nature of the initiative, provide insights into potential obstacles in harmonizing regulatory environments across the region. A key lesson was the need for flexibility and innovation at the regional level to provide backbone support to adapt when expanding to diverse country structures [46]. Interviews with policy stakeholders in Viet Nam emphasize the importance of broader policies promoting women and children’s rights for implementing national Code and maternity protection legislation [47]. Strong government relationships and coordination with non-governmental and international organizations facilitated policy revisions. However, effective implementation requires support from national and local governments.
4.3. Cross-Sectoral Nature of Breastfeeding Policy Implementation
In both the Philippines and Viet Nam, cross-cutting barriers have been documented to impact the implementation of policies related to the Code and maternity protection. In the Philippines, individual barriers influencing breastfeeding policy implementation include knowledge and skills gaps among mothers, fathers, and health workers; infant feeding misconceptions among mothers and community members; and low confidence among mothers partly due to insufficient support from household members [57]. A structural barrier described in the Philippines is inconsistent breastfeeding promotion at a societal level, including in communities, workplaces, and households [57], with many women describing the return to work as a reason for using CMF despite awareness of the immune protection conferred by breastfeeding. In Viet Nam, gaps in health system practices interrupt breastfeeding policy implementation. Almost 90% of women in Viet Nam bring CMF with them or purchase CMF at the facility when they give birth, presumably because they are worried about breastmilk supply in the first few days [54,73]. This corresponds to high CMF use, with 79.3% of mothers providing CMF in the first three days [73]. Unsurprising, this corresponds to a low prevalence of early initiation of breastfeeding (EIBF) and EBF in the first three days (EBF3D). It seems that social norms (in and outside the health facility) encourage CMF feeding and low self-efficacy towards breastfeeding, and these norms have spread widely across geographical regions and socioeconomic groups. Additional health systems practices delaying breastfeeding in the first days include medical procedures (high rates of cesarean sections and episiotomies), lack of skin-to-skin care (SSC), limited breastfeeding counseling, and widespread availability of CMF (either by mothers bringing it with them, purchasing at facilities or receiving samples) [73]. The availability and marketing of CMF-PW in Viet Nam has also likely contributed to the high use of CMF-PW by pregnant women [54,55,73]. Cross-promotion of CMF-PW creates the norm that using CMF-PW during pregnancy should progress using the same brand of CMF once the baby is born.
The full implementation of breastfeeding-supportive policies can contribute to a broader gender transformative agenda in both the Philippines and Viet Nam. This would include strategies such as increasing fathers’ involvement and support, societal shifts that encourage breastfeeding as the norm, improved individual counseling and group support programs, universal implementation of the BFHI/Mother-Baby-Friendly Initiative, and further support for vulnerable parents [73]. It is important that the economic contribution of unpaid care work, predominantly by women and including breastfeeding, is adequately recognized. The recently developed Mothers’ Milk Tool can be used to aid advocacy to acknowledge the economic and societal contributions of breastfeeding women, including in ensuring food security [3,4]. Given the vulnerability of both countries to climate change and natural hazards, breastfeeding advocacy should be integrated into climate and disaster response planning. The Green Feeding Tool demonstrates how investing in breastfeeding has the potential to mitigate the greenhouse gas impacts of CMF and highlights the importance of acknowledging breastfeeding in first-food systems advocacy [118]. Further research is needed to explore the alignment between health and labor-related policies to enable breastfeeding (such as the Code and maternity protection) with other social policies, such as childcare. However, scale-up of nutrition-sensitive policies that enable breastfeeding (such as national Code implementation and maternity protection) is essential to address structural barriers in a broad range of disciplines, including maternal, infant, and young child health and nutrition, gender equity in the labor sector, women’s rights, and even with implications for climate. Another important consideration for future policy is the geographic disparities in breastfeeding practices documented in the Philippines and Viet Nam, which are projected to increase in the Philippines [63], indicating the need for geographic targeting of interventions.
ASEAN is a political and economic group of 10 countries in Southeast Asia including the Philippines and Viet Nam, representing over 600 million people. The ASEAN Health Cluster has recently published minimum standards to facilitate a more harmonized regulatory environment in the region (for the Protection, Promotion and Support of Breastfeeding and Complementary Feeding, including Code implementation and Guidelines on Actions to Protect Children from the Harmful Impact of Marketing of Food and Non-alcoholic Beverages) [119,120]. The learnings from the Philippines and Viet Nam are important for the rollout of these standards for member states. Similar minimum standards for maternity protection could be developed to ensure regional policy coherence, leveraging member states’ commitments to ASEAN, as described in “The ASEAN Leaders Declaration on Ending All Forms of Malnutrition” of 2017 [121].
4.4. Feasibility of Recommendations
In this manuscript, we summarize key recommendations from previous studies. The feasibility of implementing these recommendations on the Code and maternity protection depends on several factors. Addressing legal gaps and enhancing regulations restricting CMF promotion requires strong political will and comprehensive legislative frameworks. Both countries need to invest in social and behavior change communication strategies to raise awareness and promote breastfeeding, which involves significant resources and coordination among various stakeholders. Improving breastfeeding counseling and support necessitates training health professionals and engaging communities, which can be challenging but is essential for long-term success.
Increasing paid maternity leave and expanding coverage to the informal sector are ambitious but necessary steps for maternity protection. In the Philippines, institutionalizing maternity cash transfers for the informal sector and reducing contribution requirements are feasible with legislative support and adequate funding. In Viet Nam, expanding entitlements to a large portion of the labor force not currently covered by social insurance requires substantial policy changes and financial investment. Strengthening communication about maternity entitlements and ensuring supportive work environments are critical but require cultural shifts and employer buy-in. Effective monitoring and enforcement of policies, supported by inter-agency teams and integrated government monitoring, are crucial for ensuring compliance and protecting workers’ rights.
Although the recommendations are ambitious, they outline the next steps required for policy advocacy and program implementation. For example, in Viet Nam in the past, successful advocacy for six months of paid maternity leave (2012) was motivated by children’s rights and the need for EBF for children under six months. Further successful workplace lactation support, which mandates 60-minute paid breastfeeding breaks and lactation rooms in companies with over 1,000 female employees (2021), was based on the argument that children need to continue breastfeeding until 24 months. These entitlements were considered not feasible at the time they were proposed but were indeed approved and implemented. While many recommendations require financial commitments, the cost of inaction is far greater than the investment needs, as illustrated by the cost of not breastfeeding estimates for both countries [3]. Strategies to enhance the financial feasibility of these recommendations could include supporting these countries to improve responsive public financial management, renewing financial commitments, and exploring innovative financing to support recommended actions [122]. There is an opportunity to deliver more for the resources available by improving the efficiency of spending. Untapped opportunities include leveraging universal health coverage financing and adaptive social protection and assistance programs, repurposing of subsidies, and accessing climate funds with ongoing efforts for breastfeeding investments to be recognized as carbon offsets [123].
4.5. Strengths and Limitations
This paper has been able to draw on extensive in-depth primary research using mixed methods conducted in the Philippines and Viet Nam. The primary research adapted existing questionnaires based on global standards. Much of the primary research was cross-sectional in nature and cannot be used to conclude causal relationships, yet trends and associations have been described. We acknowledge that the selection of studies was purposeful and not systematic. Still, since the synthesis was reviewed by authors involved in the primary data collection and familiar with the landscape, we anticipate that key literature has been included. We acknowledge that bias may exist due to the potential subjective nature of qualitative analysis but have attempted to reduce this through reflexivity and by checking interpretations with researchers involved in some of the primary data collection on which the synthesis is based.
5. Conclusions
The Philippines and Viet Nam have progressive policies to enable breastfeeding, associated with substantial increases in breastfeeding rates in recent years. Comprehensive implementation research has documented policy progress, remaining barriers, and improvement in breastfeeding rates in these two countries. Challenges identified and lessons learned from successful policy advances in breastfeeding support in these two countries could serve as valuable insights when advocating for improved policy to enable breastfeeding in other countries in the region and other LMICs. Learnings from the implementation of national marketing restrictions of CMF and associated products and maternity protection policy in the Philippines and Viet Nam can inform the implementation of newly developed regional standards together with supportive or related policies, facilitating the harmonization of regulatory environments in the region.
Author Contributions
Conceptualization and methodology, P.Z., R.M and C.P.K.; formal analysis, C.P.K.; writing—original draft preparation, C.P.K.; writing—review and editing, J.D.S., D.V., P.Z., T.T.N., R.M., C.C. and J.C.; visualization, C.P.K. and T.T.N.; supervision, R.M..; project administration, P.Z.; funding acquisition, R.M. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported in part by the Bill & Melinda Gates Foundation (Grant Number INV-042392) and the Government of Ireland, to cover staff time spent working with previously collected data or information. The views and opinions set out in this article represent those of the authors, and do not necessarily represent the position of the donors. Under the grant conditions of the Foundation, a Creative Commons Attribution 4.0 Generic License has already been assigned to the Author Accepted Manuscript version that might arise from this submission.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data generated or analyzed during this study are included in this article and / or appropriately cited to publicly accessible resources.
Acknowledgments
The authors thank Tina Sanghvi and Diana Tetterton from the Alive & Thrive initiative at FHI 360 Global Nutrition for their comments and suggestions to improve this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
AI: Artificial intelligence; ASEAN: Association of Southeast Asian Nations; BFHI: Baby-friendly Hospital Initiative; CMF : Commercial milk formula; CMF-PW : Commercial milk formula for pregnant women; DOST-FNRI Department of Science and Technology – Food and Nutrition Research Institute; EBF: Exclusive breastfeeding under six months; EMLL: Expanded Maternity Leave Law; ILO: International Labour Organization; IYCF: Infant and Young Child Feeding; LMIC: Low-and-middle-income countries; MBFHI: Mother-Baby Friendly Hospital Initiative; MOH: Ministry of Health; MPC: Maternity Protection Convention; NDHS: National Demographic and Health Survey; PhilHealth: Philippine Health Insurance Corporation (PhilHealth) ; SSS: Social Security System; WHA: World Health Assembly; WHO: World Health Organization.
References
- Victora CG, Bahl R, Barros AJD, França GVA, Horton S, Krasevec J, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387:475–90. [CrossRef]
- Rollins NC, Bhandari N, Hajeebhoy N, Horton S, Lutter CK, Martines JC, et al. Why invest, and what it will take to improve breastfeeding practices? Lancet. 2016;387:491–504. [CrossRef]
- Walters DD, Phan LTH, Mathisen R. The cost of not breastfeeding: global results from a new tool. Health Policy Plan. 2019;34:407–17. [CrossRef]
- Smith JP, Iellamo A, Nguyen TT, Mathisen R. The volume and monetary value of human milk produced by the world’s breastfeeding mothers: Results from a new tool. Front Public Heal. 2023;11. [CrossRef]
- Hernández-Cordero S, Pérez-Escamilla R. What will it take to increase breastfeeding? Matern Child Nutr. 2022;18:1–5.
- Pérez-Escamilla R, Tomori C, Hernández-Cordero S, Baker P, Barros AJD, Bégin F, et al. Breastfeeding: crucially important, but increasingly challenged in a market-driven world. Lancet. 2023;401:472–85. [CrossRef]
- World Health Organization (WHO). Global Nutrition Targets 2025 Policy Brief Series. Geneva; 2014.
- WHO-UNICEF. Global Breastfeeding Scorecard 2023. Geneva & New York; 2023.
- World Health Organization (WHO). International Code of Marketing of Breast-milk Substitutes. Geneva; 1981.
- WHO & UNICEF. Innocenti Declaration on the Protection, Promotion and Support of Breastfeeding. New York; 1990.
- WHO & UNICEF. Global Strategy for Infant and Young Child Feeding. Geneva; 2003.
- Alive & Thrive, IBFAN. Protecting Breastfeeding Throughout History: The Evolution of the International Code of Marketing of Breastmilk Substitutes. 2021.
- Baumslag N. Cicely Delphine Williams: Doctor of the World’s Children. J Hum Lact. 2005;21:6–7. [CrossRef]
- World Health Organization (WHO). Code and subsequent resolutions. Nutrition and Food Safety. 2024. https://www.who.int/teams/nutrition-and-food-safety/food-and-nutrition-actions-in-health-systems/code-and-subsequent-resolutions. Accessed 18 Nov 2024.
- United Nations Children’s Fund (UNICEF). What I Should Know About “the Code”: A guide to implementation, compliance and identifying violations. New York; 2023.
- International Code Documentation Centre (ICDC). International Code of Marketing of Breastmilk Substitutes and relevant WHA resolutions. Penang; 2022.
- WHO UNICEF and IBFAN. Marketing of breast-milk substitutes: National implementation of the International Code, status report 2024. Geneva; 2024.
- Rollins N, Piwoz E, Baker P, Kingston G, Mabaso KM, McCoy D, et al. Marketing of commercial milk formula: a system to capture parents, communities, science, and policy. Lancet. 2023;401:486–502. [CrossRef]
- Baker P, Smith JP, Garde A, Grummer-Strawn LM, Wood B, Sen G, et al. The political economy of infant and young child feeding: confronting corporate power, overcoming structural barriers, and accelerating progress. Lancet. 2023;401:503–24. [CrossRef]
- International Labour Organization (ILO). C003 - Maternity Protection Convention, 1919 (No. 3). 1919. https://www.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO::P12100_INSTRUMENT_ID:312148. Accessed 4 Oct 2023.
- International Labour Organization (ILO). Maternity Protection Convention (No. 183). 2000. https://normlex.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO::P12100_ILO_CODE:C183. Accessed 18 Nov 2024.
- International Labour Organization (ILO). R191 - Maternity Protection Recommendation, 2000 (No. 191). 2000. https://www.ilo.org/dyn/normlex/de/f?p=1000:12100:0::NO::P12100_INSTRUMENT_ID,P12100_LANG_CODE:312529,en:NO. Accessed 23 Nov 2020.
- International Labour Organization (ILO). International Labour Standards on Maternity protection. Labour standards. 2024. https://www.ilo.org/global/standards/subjects-covered-by-international-labour-standards/maternity-protection/lang--en/index.htm. Accessed 22 Feb 2024.
- Gribble KD, Smith JP, Gammeltoft T, Ulep V, Van Esterik P, Craig L, et al. Breastfeeding and infant care as ‘sexed’ care work: reconsideration of the three Rs to enable women’s rights, economic empowerment, nutrition and health. Front Public Heal. 2023;11:1–16. [CrossRef]
- Bettinelli ME, Smith JP, Haider R, Sulaiman Z, Stehel E, Young M, et al. ABM Position Statement: Paid Maternity Leave—Importance to Society, Breastfeeding, and Sustainable Development. Breastfeed Med. 2024;19:141–51. [CrossRef]
- Chai Y, Nandi A, Heymann J. Does extending the duration of legislated paid maternity leave improve breastfeeding practices? Evidence from 38 low-income and middle-income countries. BMJ Glob Heal. 2018;3:e001032. [CrossRef]
- Navarro-Rosenblatt D, Garmendia M-L. Maternity Leave and Its Impact on Breastfeeding: A Review of the Literature. Breastfeed Med. 2018;13:589–97. [CrossRef]
- Nandi A, Hajizadeh M, Harper S, Koski A, Strumpf EC, Heymann J. Increased Duration of Paid Maternity Leave Lowers Infant Mortality in Low- and Middle-Income Countries: A Quasi-Experimental Study. PLOS Med. 2016;13:e1001985. [CrossRef]
- Aitken Z, Garrett CC, Hewitt B, Keogh L, Hocking JS, Kavanagh AM. The maternal health outcomes of paid maternity leave: A systematic review. Soc Sci Med. 2015;130:32–41. [CrossRef]
- Heshmati A, Honkaniemi H, Juárez SP. The effect of parental leave on parents’ mental health: a systematic review. Lancet Public Heal. 2023;8:e57–75. [CrossRef]
- Franzoi IG, Sauta MD, De Luca A, Granieri A. Returning to work after maternity leave: a systematic literature review. Arch Womens Ment Health. 2024. [CrossRef]
- Charmes J, International Labour Office (ILO). The unpaid care work and the labour market: an analysis of time use data based on the latest world compilation of time-use surveys. Geneva: ILO; 2019.
- International Labour Organization (ILO). Ratifications of C183 - Maternity Protection Convention, 2000 (No. 183). https://www.ilo.org/dyn/normlex/en/f?p=1000:11300:0::NO:11300:P11300_INSTRUMENT_ID:312328. Accessed 8 Jan 2024.
- International Labour Organization (ILO). Care at work: Investing in care leave and services for a more gender equal world of work - Executive Summary. Geneva; 2022.
- Pereira-Kotze C, Doherty T, Faber M. Maternity protection for female non-standard workers in South Africa: the case of domestic workers. BMC Pregnancy Childbirth. 2022;22:657. [CrossRef]
- Ulep VG, Zambrano P, Datu-Sanguyo J, Vilar-Compte M, Belismelis GMT, Pérez-Escamilla R, et al. The financing need for expanding paid maternity leave to support breastfeeding in the informal sector in the Philippines. Matern Child Nutr. 2021;17:1–8. [CrossRef]
- Stumbitz B, Lewis S, Kyei AA, Lyon F. Maternity protection in formal and informal economy workplaces: The case of Ghana. World Dev. 2018;110:373–84. [CrossRef]
- Committee on the Rights of the Child (CRC). General Comment 15 on the right of the child to the enjoyment of the highest attainable standard of health (art. 24). 2013.
- Committee on the Rights of the Child (CRC). The Convention on the Rights of the Child. 1989.
- Office of the United Nations High Commissioner for Human Rights (OHCHR). Joint statement by the UN Special Rapporteurs on the Right to Food, Right to Health, the Working Group on Discrimination against Women in law and in practice, and the Committee on the Rights of the Child in support of increased efforts to promote, support. 2016. https://www.ohchr.org/en/statements/2016/11/joint-statement-un-special-rapporteurs-right-food-right-health-working-group. Accessed 19 May 2024.
- Grummer-Strawn LM, Zehner E, Stahlhofer M, Lutter C, Clark D, Sterken E, et al. New World Health Organization guidance helps protect breastfeeding as a human right. Matern Child Nutr. 2017;13:e12491. [CrossRef]
- Joyce CM, Hou SS-Y, Ta BTT, Vu DH, Mathisen R, Vincent I, et al. The Association between a Novel Baby-Friendly Hospital Program and Equitable Support for Breastfeeding in Vietnam. Int J Environ Res Public Health. 2021;18:6706. [CrossRef]
- Hernández-Cordero S, Pérez-Escamilla R, Zambrano P, Michaud-Létourneau I, Lara-Mejía V, Franco-Lares B. Countries’ experiences scaling up national breastfeeding, protection, promotion and support programmes: Comparative case studies analysis. Matern Child Nutr. 2022;18:1–27. [CrossRef]
- Nguyen TT, Weissman A, Cashin J, Ha TT, Zambrano P, Mathisen R. Assessing the Effectiveness of Policies Relating to Breastfeeding Promotion, Protection, and Support in Southeast Asia: Protocol for a Mixed Methods Study. JMIR Res Protoc. 2020;9:e21286. [CrossRef]
- Michaud-Létourneau I, Gayard M, Pelletier DL. Contribution of the Alive & Thrive-UNICEF advocacy efforts to improve infant and young child feeding policies in Southeast Asia. Matern Child Nutr. 2019;15:1–14. [CrossRef]
- Michaud-Létourneau I, Gayard M, Mathisen R, Phan LTH, Weissman A, Pelletier DL. Enhancing governance and strengthening advocacy for policy change of large Collective Impact initiatives. Matern Child Nutr. 2019;15:1–12. [CrossRef]
- Payán DD, Zahid N, Glenn J, Tran HTT, Huong TTT, Moucheraud C. Implementation of two policies to extend maternity leave and further restrict marketing of breast milk substitutes in Vietnam: a qualitative study. Health Policy Plan. 2022;37:472–82. [CrossRef]
- Harris J, Frongillo EA, Nguyen PH, Kim SS, Menon P. Changes in the policy environment for infant and young child feeding in Vietnam, Bangladesh, and Ethiopia, and the role of targeted advocacy. BMC Public Health. 2017;17:492. [CrossRef]
- Baker P, Zambrano P, Mathisen R, Singh-Vergeire MR, Escober AE, Mialon M, et al. Breastfeeding, first-food systems and corporate power: a case study on the market and political practices of the transnational baby food industry and public health resistance in the Philippines. Global Health. 2021;17:125. [CrossRef]
- Baker P, Santos T, Neves PA, Machado P, Smith J, Piwoz E, et al. First-food systems transformations and the ultra-processing of infant and young child diets: The determinants, dynamics and consequences of the global rise in commercial milk formula consumption. Matern Child Nutr. 2021;17:1–18. [CrossRef]
- Chen Y. Global infant formula products market: estimations and forecasts for production and consumption. China Dairy. 2018; July:4 pp.
- Koe T. Growth 2024: Why South East Asian countries are the emerging nutrition markets to look out for this year 03-Jan-2024 By Tingmin Koe. Nutraingredients Asia. 2024.
- Michaud-Létourneau I, Gayard M, Pelletier DL. Translating the International Code of Marketing of Breast-milk Substitutes into national measures in nine countries. Matern Child Nutr. 2019;15:1–13. [CrossRef]
- Nguyen TT, Tran HTT, Cashin J, Nguyen VDC, Weissman A, Nguyen TT, et al. Implementation of the Code of Marketing of Breast-Milk Substitutes in Vietnam: Marketing Practices by the Industry and Perceptions of Caregivers and Health Workers. Nutrients. 2021;13:2884. [CrossRef]
- Nguyen TT, Cashin J, Ching C, Baker P, Tran HT, Weissman A, et al. Beliefs and Norms Associated with the Use of Ultra-Processed Commercial Milk Formulas for Pregnant Women in Vietnam. Nutrients. 2021;13:4143. [CrossRef]
- Nguyen TT, Cashin J, Tran HTT, Vu DH, Nandi A, Phan MT, et al. Awareness, Perceptions, Gaps, and Uptake of Maternity Protection among Formally Employed Women in Vietnam. Int J Environ Res Public Health. 2022;19:4772. [CrossRef]
- Samaniego JAR, Maramag CC, Castro MC, Zambrano P, Nguyen TT, Datu-Sanguyo J, et al. Implementation and Effectiveness of Policies Adopted to Enable Breastfeeding in the Philippines Are Limited by Structural and Individual Barriers. Int J Environ Res Public Health. 2022;19:10938. [CrossRef]
- Joyce CM, Nguyen TT, Pham TN, Mathisen R, Nandi A. The impact of Vietnam’s 2013 extension of paid maternity leave on women’s labour force participation. J Asian Public Policy. 2023;00:1–18. [CrossRef]
- Maramag CC, Samaniego JAR, Castro MC, Zambrano P, Nguyen TT, Cashin J, et al. Maternity protection policies and the enabling environment for breastfeeding in the Philippines: a qualitative study. Int Breastfeed J. 2023;18:60. [CrossRef]
- Philippine Statistics Authority. Special Release: 2022 National Demographic and Health Survey (NDHS) Key Indicators - Health Insurance Coverage. 2023:2–4. https://rssocar.psa.gov.ph/system/files/attachment-dir/CAR-SSR-2023-23_2022-NDHS-Insurance-Coverage.pdf. Accessed 18 Nov 2024.
- DOST-FNRI. Expanded National Nutrition Survey: 2019 Results - Nutritional Status of Filipino Infants and Young Children (0-23 months). 2019. https://www.fnri.dost.gov.ph/images/sources/eNNS2018/Infants_and_Young_Children_0-23m.pdf. Accessed 18 Nov 2024.
- DOST-FNRI. Expanded National Nutrition Survey: 2021 Survey Results. 2022;282. https://www.scribd.com/document/747228306/2021-ENNS-National-Results-Dissemination. Accessed 18 Nov 2024.
- Bhattacharjee N V., Schaeffer LE, Hay SI, Lu D, Schipp MF, Lazzar-Atwood A, et al. Mapping inequalities in exclusive breastfeeding in low- and middle-income countries, 2000–2018. Nat Hum Behav. 2021;5:1027–45. [CrossRef]
- Office of the United Nations High Commissioner for Human Rights (OHCHR). Status of ratification: Interactive Dashboard. 2024. https://indicators.ohchr.org/. Accessed 8 Apr 2024.
- Wood B, O’Sullivan D, Baker P, Nguyen T, Ulep V, McCoy D. Who Benefits from Undermining Breastfeeding? Exploring the global commercial milk formula industry’s generation and distribution of wealth and income. 2022.
- Official Gazette- Republic of the Philippines. Republic Act 11210. An Act Increasing the Maternity Leave Period to One Hundred Five (105) Days for Female Workers with an Option to Extend for an Additional Thirty (30) Days Without Pay, and Granting an Additional Fifteen (15) Days for Solo Mothers, and. Official Gazette- Republic of the Philippines. 2019;1–10. http://legacy.senate.gov.ph/republic_acts/ra 11210.pdf. Accessed 18 Nov 2024.
- Philippine Statistics Authority (PSA). Labor Force Survey Media Release. Quezon City; 2023.
- World Bank. Philippines Gender Landscape. 2024. https://genderdata.worldbank.org/en/economies/philippines. Accessed 16 Nov 2024.
- Cabegin ECA. Policy Brief: The Informal Labor Carries the Brunt of a COVID-19 – induced Economic Recession: The Need for Stronger Transition Policies to Formality. Quezon City; 2022.
- UNICEF. UNICEF Data Warehouse: Viet Nam indicator - exclusive breastfeeding. 2023. https://data.unicef.org/resources/data_explorer/unicef_f/?ag=UNICEF&df=GLOBAL_DATAFLOW&ver=1.0&dq=VNM.NT_BF_EXBF.&startPeriod=1970&endPeriod=2023. Accessed 5 Oct 2023.
- UNICEF. Viet Nam SDGCW (Sustainable Development Goal Indicators on Children and Women) Survey 2020-2021: Infant and Young Child Feeding. 2021;5–6.
- WHO & UNICEF. The extension of the 2025 Maternal, Infant and Young Child nutrition targets to 2030: Discussion paper. 2019.
- Nguyen TT, Cashin J, Tran HT, Hoang TA, Mathisen R, Weissman A, et al. Birth and newborn care policies and practices limit breastfeeding at maternity facilities in Vietnam. Front Nutr. 2022;9:1–15. [CrossRef]
- Interesse G. Vietnam’s Baby Formula Market: Key Considerations for Foreign Brands and Exporters. Vietnam Briefing. 2023. https://www.vietnam-briefing.com/news/vietnams-baby-formula-market-key-considerations-for-foreign-brands-and-exporters.html/. Accessed 11 Jan 2024.
- WHO & UNICEF. How the marketing of formula milk influences our decisions on infant feeding. Geneva; 2022.
- YCP Solidiance. Vietnam Market Study on Formula Milk. 2020; October. https://www.gov.br/empresas-e-negocios/pt-br/invest-export-brasil/exportar/conheca-os-mercados/pesquisas-de-mercado/estudo-de-mercado.pdf/formulamilkhanoiengl.pdf. Accessed 16 Nov 2024.
- World Bank. Viet Nam Gender Landscape. 2024. https://genderdata.worldbank.org/en/economies/vietnam. Accessed 16 Nov 2024.
- Barcucci V, Cole W, Rosina G. Research brief: Gender and the Labor Market in Vietnam. Hanoi, Viet Nam; 2021.
- The World Bank Group. Birth rate, crude (per 1,000 people). 2022. https://data.worldbank.org/indicator/SP.DYN.CBRT.IN?locations=VN. Accessed 31 May 2024.
- World Bank. Population total - Philippines. 2022. https://data.worldbank.org/indicator/SP.POP.TOTL?locations=PH. Accessed 23 Feb 2024.
- World Bank. Population, total - Viet Nam. 2022. https://data.worldbank.org/indicator/SP.POP.TOTL?locations=VN. Accessed 23 Feb 2024.
- World Bank. Rural population (% of total population). 2023. https://data.worldbank.org/indicator/SP.RUR.TOTL.ZS. Accessed 18 Nov 2024.
- World Bank. Health Nutrition and Population Statistics. 2021. https://databank.worldbank.org/source/health-nutrition-and-population-statistics. Accessed 4 Mar 2024.
- Philippine Statistics Authority (PSA), ICF. Philippine National Demographic and Health Survey (NDHS): Final Report. Quezon City, Philippines and Rockville, Maryland, USA; 2023.
- General Statistics Office, UNICEF. Survey Measuring Viet Nam Sustainable Development Goal Indicators on Children and Women 2020-2021, Survey Findings Report. Ha Noi, Viet Nam; 2021.
- WHO Western Pacific Region, UNICEF. Action Plan for Healthy Newborn Infants in the Western Pacific Region (2014-2020): Second biennial progress report (2016–2017). 2018.
- General Statistics Office (GSO) [Viet Nam]. Report on Labour Force Survey 2021. Ha Noi, Viet Nam; 2022.
- Philippines Statistics Authority. Philippines Labor Force Survey December 2023. 2023. https://psa.gov.ph/statistics/labor-force-survey/node/1684062347. Accessed 15 Mar 2024.
- WHO, UNICEF, IBFAN. Marketing of breast-milk substitutes: national implementation of the international Code, status report 2022. Geneva; 2022.
- UNICEF East Asia & Pacific Region. Strengthening Implementation of the Breast-milk Substitutes Code in Southeast Asia: Putting Child Nutrition First. 2021.
- Department of Labor and Employment (DOLE) [Philippines]. Renumbering of the Labor Code of the Philippines, as Amended. Manila, Philippines and Calverton, Maryland USA; 2015.
- Official Gazette- Republic of the Philippines. Expanded Breastfeeding Promotion Act of 2009. Metro Manila; 2010.
- WHO & UNICEF. NetCode toolkit. Monitoring the marketing of breast-milk substitute: protocol for ongoing monitoring systems. 2017.
- Nguyen TT, Darnell A, Weissman A, Cashin J, Withers M, Mathisen R, et al. National nutrition strategies that focus on maternal, infant, and young child nutrition in Southeast Asia do not consistently align with regional and international recommendations. Matern Child Nutr. 2020;16:1–13. [CrossRef]
- Nguyen TT, Huynh NL, Huynh PN, Zambrano P, Withers M, Cashin J, et al. Bridging the evidence-to-action gap: enhancing alignment of national nutrition strategies in Cambodia, Laos, and Vietnam with global and regional recommendations. Front Nutr. 2024;10 January:1–11. [CrossRef]
- World Health Organization (WHO). Guidance on regulatory measures aimed at restricting digital marketing of breast-milk substitutes. Geneva; 2023.
- Giang HTN, Duy DTT, Vuong NL, Ngoc NTT, Pham TT, Duc NTM, et al. Prevalence of exclusive breastfeeding for the first six months of an infant’s life and associated factors in a low–middle income country. Int Breastfeed J. 2023;18:47. [CrossRef]
- Republic of the Philippines House of Representatives. Bill encouraging corporate social responsibility passed in the House. Press and Public Affairs Bureau. 2023. https://www.congress.gov.ph/press/details.php?pressid=12521. Accessed 19 Mar 2024.
- Capili DIS, Datu-Sanguyo J, Mogol-Sales CS, Zambrano P, Nguyen TT, Cashin J, et al. Cross-sectional multimedia audit reveals a multinational commercial milk formula industry circumventing the Philippine Milk Code with misinformation, manipulation, and cross-promotion campaigns. Front Nutr. 2023;10:1–13. [CrossRef]
- Brewer BK, Salgado R V, Alexander E, Lo A, Bhatia R. National Assessment on the Compliance with the Code and the National Measures: Philippines Report. Rockville, Maryland; 2021.
- Reinsma K, Ballesteros AJC, Bucu RAA, Dizon TS, Jumalon NJU, Ramirez LC, et al. Mother-Baby Friendly Philippines: Using Citizen Reporting to Improve Compliance to the International Code of Marketing of Breastmilk Substitutes. Glob Heal Sci Pract. 2022;10:e2100071. [CrossRef]
- Perez R. You Can Now File Your SSS Maternity Notification, Report Milk Code Violations Via Apps. 2020. https://www.smartparenting.com.ph/life/news/sss-mobile-app-and-mother-baby-friendly-app-a00041-20190706#. Accessed 19 Feb 2024.
- Philippines Department of Health. Mother-Baby Friendly Philippines. https://mbfp.doh.gov.ph/.
- World Vision Development Foundation. Mother-Baby Friendly PH App. 2019. https://apps.apple.com/us/app/mbf-ph/id1260502250.
- FHI Solutions. VIVID: Virtual Violations Detector. 2022. https://www.fhisolutions.org/innovation/vivid-virtual-violations-detector/. Accessed 18 Jan 2024.
- Alive & Thrive. News: In a first, innovative tool reveals findings on Code violations, showing potential to disrupt digital marketing of commercial milk formula. 2023. https://www.aliveandthrive.org/en/news/in-a-first-innovative-tool-reveals-findings-on-code-violations-showing-potential-to-disrupt-digital. Accessed 23 Feb 2024.
- Alive & Thrive, Hekate. VIVID: Virtual Violations Detector. 2024. https://code.corporateaccountabilitytool.org/vietnam. Accessed 23 Feb 2024.
- Backholer K, Nguyen L, Vu D, Ching C, Baker P, Mathisen R. Violations of Vietnamese laws related to the online marketing of breastmilk substitutes: Detections using a virtual violations detector. Matern Child Nutr. 2025;21(1):e13680. [CrossRef]
- Pereira-Kotze C, Malherbe K, Faber M, Doherty T, Cooper D. Legislation and Policies for the Right to Maternity Protection in South Africa: A Fragmented State of Affairs. J Hum Lact. 2022;089033442211080.
- International Labour Organization (ILO). Making the right to social security a reality for domestic workers: A global review of policy trends, statistics and extension strategies. Geneva: ILO; 2022.
- Alive & Thrive. Centers of Excellence for Breastfeeding Model in Viet Nam. 2023.
- Alive & Thrive. Toolkit to support breastfeeding women in the workplace: For reference in Viet Nam. Hanoi, Viet Nam; 2023.
- International Labour Organization (ILO). Healthy Beginnings for a Better Society: Breastfeeding in the Workplace is Possible - A Toolkit. Makati City; 2015.
- Vu K, Glewwe P. Maternity benefits mandate and women’s choice of work in Vietnam. World Dev. 2022;158:105964. [CrossRef]
- Alive & Thrive, Scaling Up Nutrition. Report on Maternity Protection Policy Expansion for female workers in non-formal sector. 2023.
- International Labour Organization (ILO). Care at work: Investing in care leave and services for a more gender equal world of work. Geneva; 2022.
- Boockmann B. The Ratification of ILO Conventions: A Failure Time Analysis. Mannheim; 2000.
- Smith JP, Borg B, Iellamo A, Nguyen TT, Mathisen R. Innovative financing for a gender-equitable first-food system to mitigate greenhouse gas impacts of commercial milk formula: investing in breastfeeding as a carbon offset. Front Sustain Food Syst. 2023;7:1–9. [CrossRef]
- ASEAN, UNICEF, Alive & Thrive. Guidelines and Minimum Standards for the Protection, Promotion and Support of Breastfeeding and Complementary Feeding. Jakarta; 2022.
- ASEAN, UNICEF. Minimum standards and guidelines on actions to protect children from the harmful impact of marketing of food and non-alcoholic beverages in the ASEAN region. Jakarta; 2023.
- ASEAN. ASEAN Leaders’ Declaration on Ending All Forms of Malnutrition. 2017.
- Skekar M, Okamura KS, D’Alimonte M, Dell’Aria C. Financing the Global Nutrition Targets: Progress to Date. In: Skekar M, Okamura KS, Vilar-Compte M, Dell’Aria C, editors. Investment Framework for Nutrition 2024. Washington, DC: World Bank Group; 2024. p. 231–67.
- Smith J, Baker P, Mathisen R, Long A, Rollins N, Waring M. A proposal to recognize investment in breastfeeding as a carbon offset. Bull World Health Organ. 2024;102:336–43. [CrossRef]
Figure 2.
Timeline of paid maternity leave provisions in the Philippines and Viet Nam from 1947 to present.
Figure 2.
Timeline of paid maternity leave provisions in the Philippines and Viet Nam from 1947 to present.
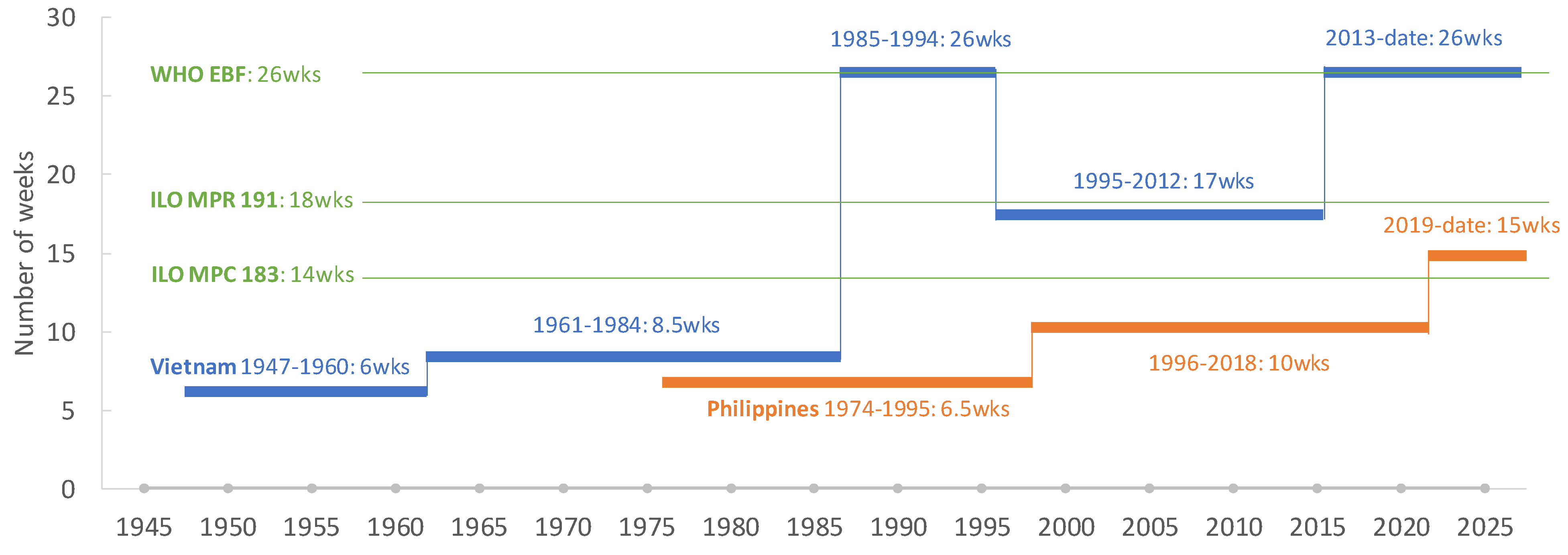
Table 1.
Published research assessing the effectiveness of policies relating to breastfeeding protection, promotion, and support in the Philippines and Viet Nam.
Table 1.
Published research assessing the effectiveness of policies relating to breastfeeding protection, promotion, and support in the Philippines and Viet Nam.
| Title, author, year | Country, year of data collection | Study design | Study sample, data collection techniques and data used | Aim | Policy type investigated |
| Translating the International Code of Marketing of Breast-milk Substitutes into national measures in nine countries [53] | Viet Nam, May 2015 to March 2017. | Real-time evaluation | Participant observation 16 key informant meetings 3 in-depth interviews (IDIs) Reflective practice; Desk review |
To document the extent to which policy objectives were (or were not) achieved in 9 countries (including Viet Nam) and to identify the key drivers of policy changes. | Breastfeeding protection: the Code |
| Implementation of the Code of Marketing of Breast-milk Substitutes in Vietnam: marketing practices by the industry and perceptions of caregivers and health workers [54] | Viet Nam, May to July 2020. | Mixed methods, cross-sectional | Quantitative survey of 268 pregnant women and 726 mothers of infants aged 0–11 months. Qualitative IDIs with 70 participants, incl. subsets of interviewed women (n = 39), policymakers, media executives, and health workers (n = 31). |
To examine the enactment and implementation of the Code of Marketing of Breast-Milk Substitutes (the Code) in Viet Nam, focusing on marketing practices by the baby food industry and perceptions of caregivers, health workers, and policymakers. | Breastfeeding protection: the Code |
| Beliefs and norms associated with the use of ultra-processed commercial milk formulas for pregnant women in Vietnam [55] | Viet Nam, May to July 2020. | Post-hoc analysis of quantitative survey data | Quantitative interviews with 268 pregnant women in their second and third trimesters from two provinces and one municipality representing diverse communities in Vietnam. | To examine the association between the use of commercial milk formula for pregnant women and related beliefs and norms among pregnant women in Vietnam. | Breastfeeding protection: the Code |
| Awareness, perceptions, gaps, and uptake of maternity protection among formally employed women in Vietnam [56] | Viet Nam, May to July 2020. | Mixed methods, cross-sectional | Quantitative interviews with 494 formally employed female workers (107 pregnant and 387 mothers of infants). IDIs with a subset of women (n = 39). |
To examine the uptake of Vietnam’s maternity protection policy in terms of entitlements and awareness, perceptions, and gaps in implementation through the lens of formally employed women. | Maternity protection |
| Implementation and effectiveness of policies adopted to enable breastfeeding in the Philippines are limited by structural and individual barriers [57] | The Philippines, December 2020 to March 2021. | Mixed methods, cross-sectional | Desk review of policies and documents IDIs with 100 caregivers, employees, employers, health workers, and policymakers in the Greater Manila Area. |
This study assesses the adequacy and potential impact of breastfeeding policies, as well as the perceptions of stakeholders of their effectiveness and how to address implementation barriers. | Breastfeeding protection promotion and support, including the Code and maternity protection |
| The impact of Vietnam’s 2013 extension of paid maternity leave on women’s labour force participation [58] |
Viet Nam, 2015-2018 (data from Labor Force Surveys) | Regression discontinuity (RD) design | RD to evaluate the impact of paid maternity leave on the probability of women holding a job and formal labour contract 3-5 years after giving birth. | To evaluate whether the expansion of Vietnam’s paid maternity leave policy was associated with improved long-term labor outcomes for Vietnamese women | Maternity protection |
| Maternity protection policies and the enabling environment for breastfeeding in the Philippines: a qualitative study [59] | The Philippines, December 2020 to April 2021 | Mixed methods, cross-sectional | Desk review of policies, guidelines, and related documents on maternity protection. IDIs with 87 mothers and partners, employers, and authorities from government and non-government organizations in the Greater Manila Area. |
This study reviewed the content and implementation of maternity protection policies in the Philippines, assessed their role in enabling recommended breastfeeding practices, and identified bottlenecks to successful implementation. | Maternity protection |
Table 3.
Implementation status of the Code in the Philippines and Viet Nam: Scores allocated per provision.
Table 3.
Implementation status of the Code in the Philippines and Viet Nam: Scores allocated per provision.
| Provision | Philippines | Viet Nam | Highest scores |
| Scope | 20 | 16 | 20 |
| Monitoring and enforcement | 10 | 10 | 10 |
| Informational / educational materials | 9 | 5 | 10 |
| Promotion to general public | 10 | 20 | 20 |
| Promotion in health facilities | 10 | 10 | 10 |
| Engagement with health workers and systems | 14 | 10 | 15 |
| Labeling | 12 | 8 | 15 |
| Total | 85 | 79 | 100 |
Source: WHO, UNICEF, and IBFAN. 2024. Marketing of Breast-milk Substitutes: National Implementation of the International Code, Status Report 2024. https://www.who.int/publications/i/item/9789240094482.
Table 4.
Summary of maternity protection provisions in legislation in the Philippines and Viet Nam.
| ILO Maternity Protection Convention 183 | ILO Maternity Protection Recommendation 183 | Philippines | Viet Nam | |
|---|---|---|---|---|
| Paid maternity leave | ||||
| Duration of maternity leave in national legislation | Mandates minimum maternity leave of 14 weeks. | Recommends increasing maternity leave to 18 weeks. | 15 weeks (105 days), option to extend an additional 30 days | 26 weeks (6 months) |
| Amount of maternity leave cash payments (% of previous earnings) |
Adequate to keep mother and child healthy, out of poverty, especially women in informal economy; >67% of previous earnings. | Recommends increasing maternity leave cash payments to 100%, when possible. | 100% for 15 weeks (105 days) | 100% |
| Source of funding maternity leave cash payments | Employers should not be individually liable for direct costs of maternity leave. Cash benefits shall be provided through compulsory social insurance, public funds or non-contributory social assistance to women who do not qualify for benefits out of social insurance; especially for informal economy or self-employed workers. | Social insurance and employer | Social insurance only | |
| Maternity leave cash payments for self-employed workers | Yes, but only for workers who are actively paying members of the Social Security System | No | ||
| Source of funding | 7 days (4 paid), employer | 5 days, social insurance | ||
| Breastfeeding (nursing) breaks | ||||
| Entitlement to paid nursing breaks | Women should be provided with the right to one or more daily breaks, or daily reduction of work hours to breastfeed. The period during which this is allowed, the number, duration of breaks and procedures for reducing daily work hours shall be determined by national law. | Frequency and length of nursing breaks should be adapted to needs. It should be possible to combine time allotted for daily nursing breaks to allow reduced work hours at beginning/ end of the workday. Where practical, provision should be made for establishing hygienic nursing facilities at or near the workplace. | Paid | Paid |
| Number of daily nursing breaks | Not limited | Not specified | ||
| Total daily nursing break duration | 40 minutes | 60 minutes | ||
| Period when nursing breaks are allowed by law | Not specified | Until child is 12 months | ||
| Statutory provisions for working nursing facilities | All workers | Mandatory at workplaces ≥ 1,000 female employees | ||
Table 5.
Key barriers to implementing legislation to enable breastfeeding in the Philippines and Viet Nam.
Table 5.
Key barriers to implementing legislation to enable breastfeeding in the Philippines and Viet Nam.
| The Philippines | Viet Nam |
|---|---|
| 1. Barriers to implementing Code legislation | |
| Structural gaps in legislation. Ambiguity surrounding monitoring responsibilities and irregular inspections. Weak sanctions limit enforcement. Some consider existing legislation to be too strict. |
Gaps in legislation: insufficient scope, inadequate regulation of information and education materials, engagement with health workers and systems, and labeling. Conflicting advertising regulations exist regarding functional food, supplemented food, food for special medical purposes for children under 24 months, and breastmilk substitutes. Legislative gaps mean company representatives still access health facilities and obtain contact information from pregnant women and new mothers. Gaps in scope allow rampant cross-promotion, especially of CMF-PW with CMF for infants. Routine monitoring is limited, relies on self-assessment, and data is unavailable. Limited enforcement due to human resource constraints and pro-industry tendencies. Gaps are illustrated by continued violations. |
| 2. Barriers to implementing maternity protection | |
| Informal sector workers are not reached by maternity protection entitlements. Length of paid maternity leave less than WHO recommendation of EBF to six months. Implementation of workplace lactation support policies varies according to workplace and type of work. Employers recognize the value of maternity protection but perceive disadvantages to policies with some not supporting workplace lactation. Sense of acceptance that breastfeeding will stop when women return to work. No systematic enforcement and monitoring. |
Low knowledge among all mothers of the full set of maternity protection entitlements. Perceived barriers to using entitlements. Disparities in knowledge and uptake by occupation and sector. Limited access to cash entitlements while on maternity leave and low maternity allowance do not protect mothers and infants from poverty due to low contribution to social security fund before maternity leave. Discrimination is based on pregnancy and childbirth. Unintended negative consequences on labor force participation. |
CMF-PW: Commercial milk formula for pregnant women.
Table 6.
Summary of recommendations to improve implementation of policies to enable breastfeeding.
| Recommendations to improve implementation of Code legislation in the Philippines and Viet Nam |
|
| Recommendations to improve implementation of maternity protection legislation in the Philippines and Viet Nam |
|
Box 1.
Summary of legislation implementing the Code in the Philippines and Viet Nam
| Philippines (“Substantially aligned” with the Code) |
|
| Viet Nam (“Substantially aligned” with the Code) |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



