Submitted:
29 December 2024
Posted:
30 December 2024
You are already at the latest version
Abstract
In foals, Rhodococcus equi infections are typically linked to a range of non-pulmonary conditions, with hemolytic anemia being an uncommon complication. The authors are aware of only one case report involving immune-mediated hemolytic anemia in foals infected with Rhodococcus equi, highlighting the need for further research. This report aims to describe the clinical presentation, progression, outcome, and pathological findings of 4-month-old Holstein foal with Rhodococcus equi infection concurrently with presummed immune-mediated hemolytic anemia. Due to severe sepsis and worsening clinical condition, the foal was euthanized and necropsy was performed.
Keywords:
rhodococcus equi
; foal
; hemolysis
; hemolytic anemia
; blood transfusion
1. Introduction
Non-pulmonary Rhodococcus equi infections are typically seen as intestinal and mesenteric abscesses, septic physitis and osteomyelitis, endophthalmitis, guttural pouch empyema, sinusitis, pericarditis, nephritis, non-septic uveitis, and hepatic and renal abscessation [11]. Hemolytic anemia in these cases is rare and, to the authors' knowledge, there has been only one reported case of presumed immune-mediated hemolytic anemia linked to Rhodococcus equi infection in foals [15].This case report aims to explore the clinical presentation, progression, and outcomes of a foal infected with Rhodococcus equi, which was also suspected of suffering from severe immune-mediated hemolytic anemia. Dexamethasone is often used to treat immune-mediated hemolytic anemia, although its use can be contraindicated in foals with severe bacterial infections [15]. Despite antimicrobial treatment and supportive therapy in this case, a lower dose of dexamethasone was administered, also whole blood transfusion performed. Regardless of treatment, the foal’s condition deteriorated, and it was euthanized on day 56.
2. Case History
A 4-month-old Holstein foal (weighing 130kg) presented with depression, anorexia, diarrhoea, and epiphora at the Lithuanian University of Health Sciences, Large Animal Clinic. The foal was born on a farm where Rhodococcus equi pneumonia had been previously reported, and its dam had been vaccinated for Rhodococcus equi. Upon examination, the foal had tachycardia (80 bpm), a respiratory rate of 20/min, capillary refill time (CRT) of 1 second, a temperature of 38.3°C. Icterus and haemoglobinuria were observed. During auscultation crackles were heard in the trachea, bronchovesicular sounds were increased in the cranial lung parts, no dyspnea or abdominal breathing pattern was noted. Bilateral, non-painful effusion was observed in the hocks and stifles.
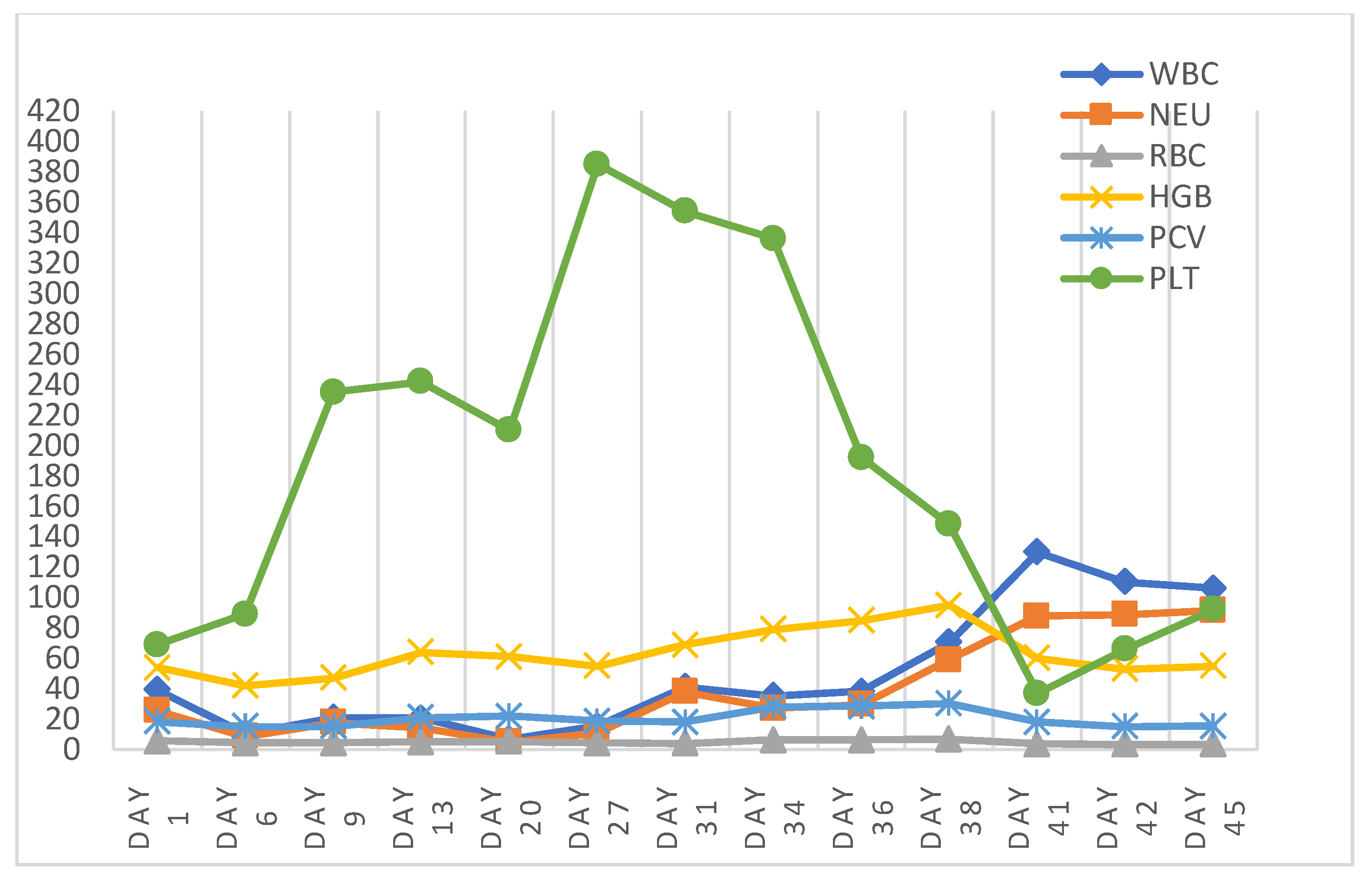
Morphological blood test was performed using the Abaxis HM5 VETSCAN Haematology analyser. Visually, after taking a blood sample, significant blood hemolysis was observed in vacutainer (Figure 7) Blood analysis showed WBC at 39.41 × 10^9/l (norm 5.4–14.3 × 10^9/l), neutrophils at 25.49 × 10^9/l (normal range 2.3–9.5 × 10^9/l), and RBC at 5.76 × 10^12/l (normal range 6.8–12.9 × 10^12/l), with haemoglobin at 54 g/l (normal range 110–190 g/l), packed cell volume (PCV) at 18.41% (normal range 32–53%), PLT (69 - 10^9/l, normal range 100-400 10^9/l), and MCV was 32 fL (normal range 37-59 fL), with MCHC was 293 g/dL (normal range 12.3-19.7 g/dL). Blood morphology hemodynamics of the whole treatment course was present at (Figure 8).
The biochemical blood test was conducted by the DiaSys respons®910VET analyzer. Serum parameters revealed hypoalbuminemia (18.5 g/l, normal range 25–42 g/l), elevated ALP (419.3 U/l, normal range 109–315 U/l), hypocalcemia (2.66 mmol/l, normal range 2.7–3.4 mmol/l), and elevated iron level (38,9 μmol/l, normal range 13-25 μmol/l). Blood gases showed hyperlactatemia (5.15 mmol/l, normal range >2 mmol/l) and hyponatremia (120 mmol/l, normal range 128–142 mmol/l). Serum amyloid A was elevated at 326 mg/l (normal range 0–20 mg/l). During blood smear analysis, poikilocytosis and microcytosis were noted. The blood smear indicated severe anemia, characterized by a notable presence of schistocytes (Figure 1-2), a limited number of prominent elliptocytes (Figure 1 and 4) and spherocytes (Figure 3), isolated echinocytes (Figure 2), and a reticulocyte count significantly below the average. Toxic nuclear granulation of segmented neutrophils was also observed in the blood smear (Figure 3-4).
Figure 1.
Large number of schistocytes (arrows) and several elliptocytes (arrowhead). Hemacolor, x1000.
Figure 1.
Large number of schistocytes (arrows) and several elliptocytes (arrowhead). Hemacolor, x1000.
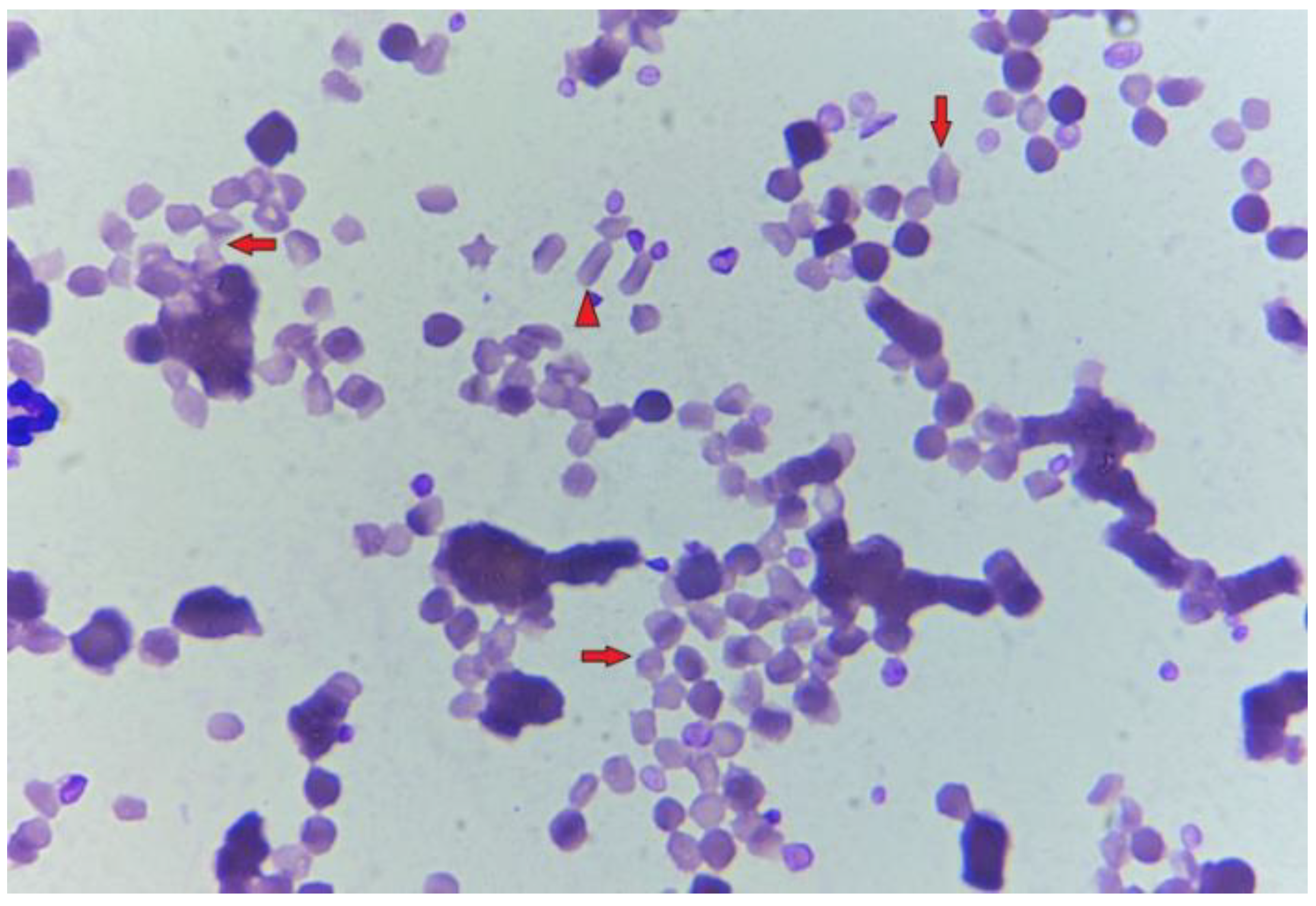
Figure 2.
A significant quantity of schistocytes (arrows) and one echinocyte visible (arrowhead). Hemacolor, x1000.
Figure 2.
A significant quantity of schistocytes (arrows) and one echinocyte visible (arrowhead). Hemacolor, x1000.
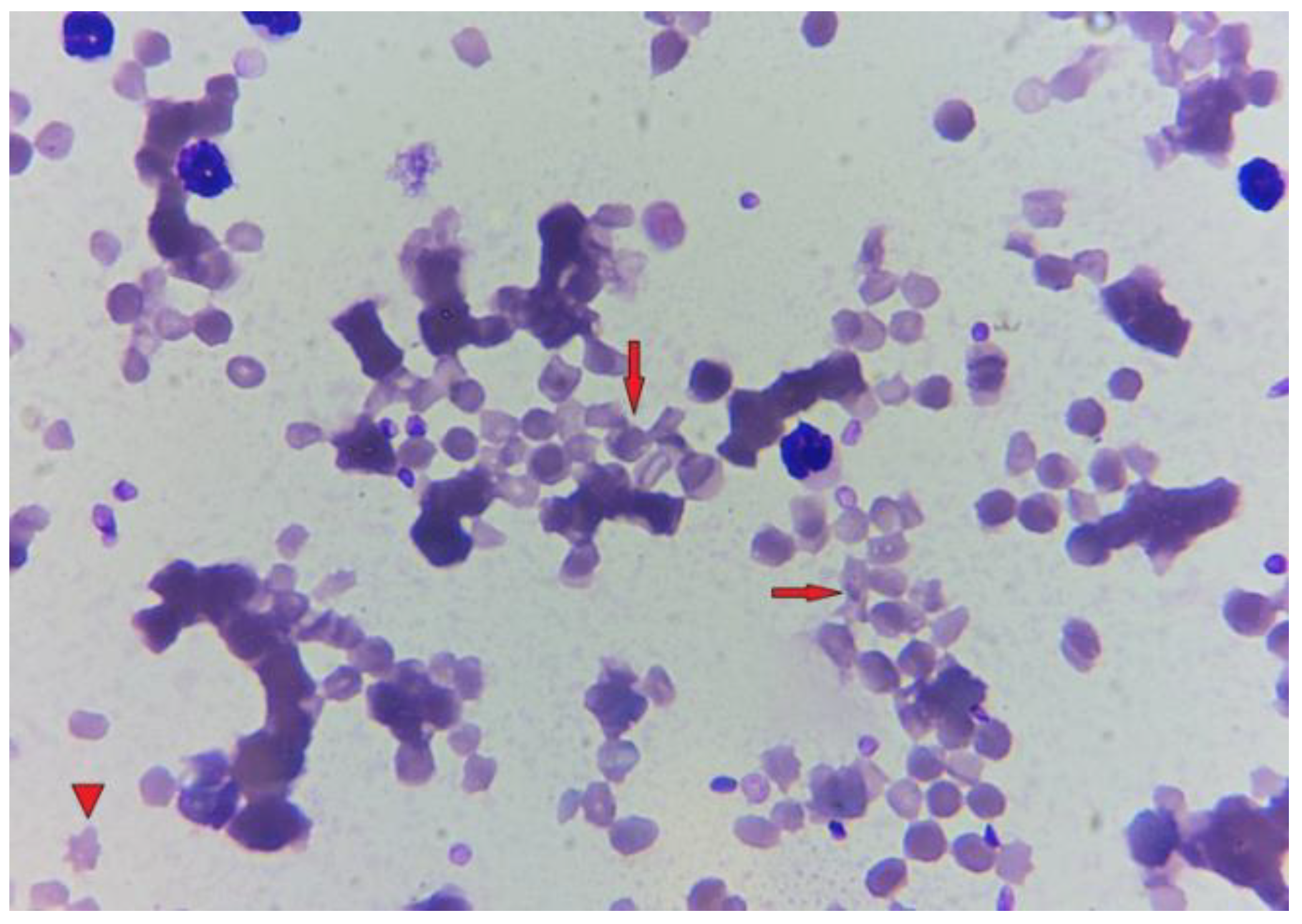
Figure 3.
Single spherocytes (red arrowheads) and segmented neutrophil with toxic nuclear granulation (black arrow). Hemacolor, x1000.
Figure 3.
Single spherocytes (red arrowheads) and segmented neutrophil with toxic nuclear granulation (black arrow). Hemacolor, x1000.
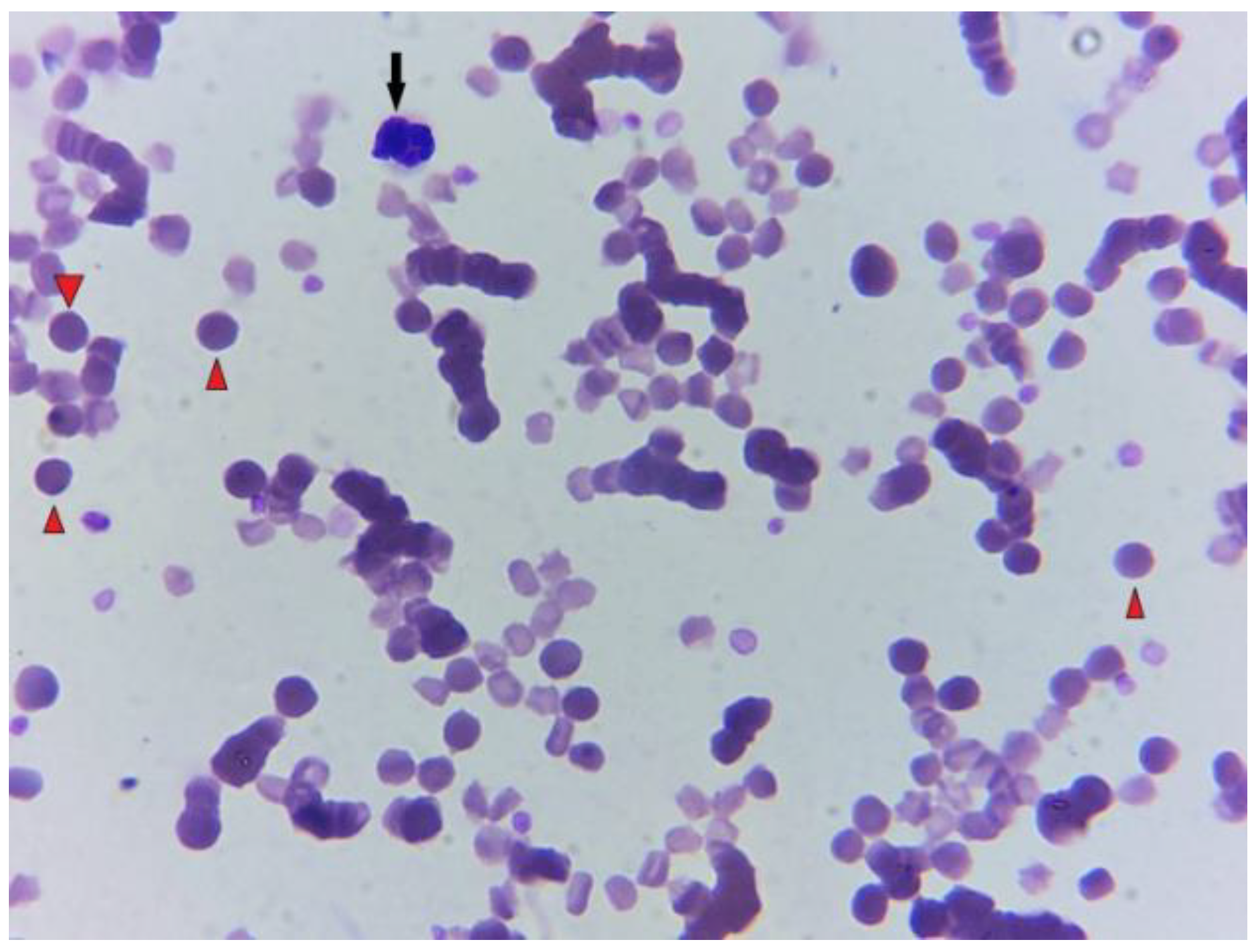
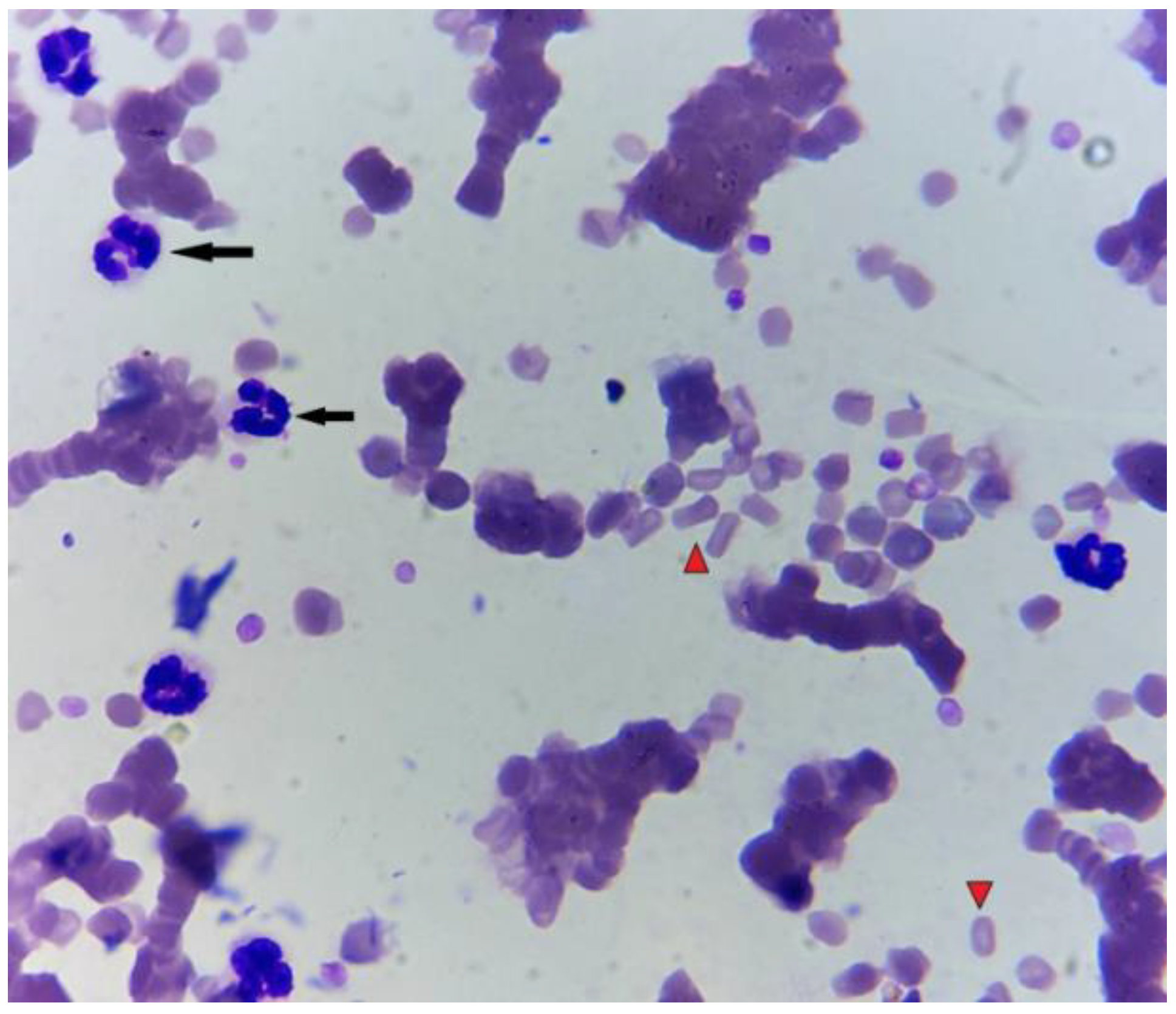
Figure 4.
Several segmented neutrophils with toxic nuclear granulation (black arrows) and elliptocytes (red arrowheads). Hemacolor, x1000.
Figure 4.
Several segmented neutrophils with toxic nuclear granulation (black arrows) and elliptocytes (red arrowheads). Hemacolor, x1000.
Faecal examination using the modified McMaster method did not detect helminth eggs. A bronchoscopy revealed a hyperemic trachea with yellowish discharge all over trachea and bronchi (grade 2) and bifurcation edema 2/4 (according to B. Wysocka, W. Klucinski 2014). The cytological analysis of a transtracheal wash (TTW) revealed 94.5% neutrophils, 2.75% macrophages, 2.25% lymphocytes, 0.5% mast cells, and a limited quantity of bacteria was detected individually.
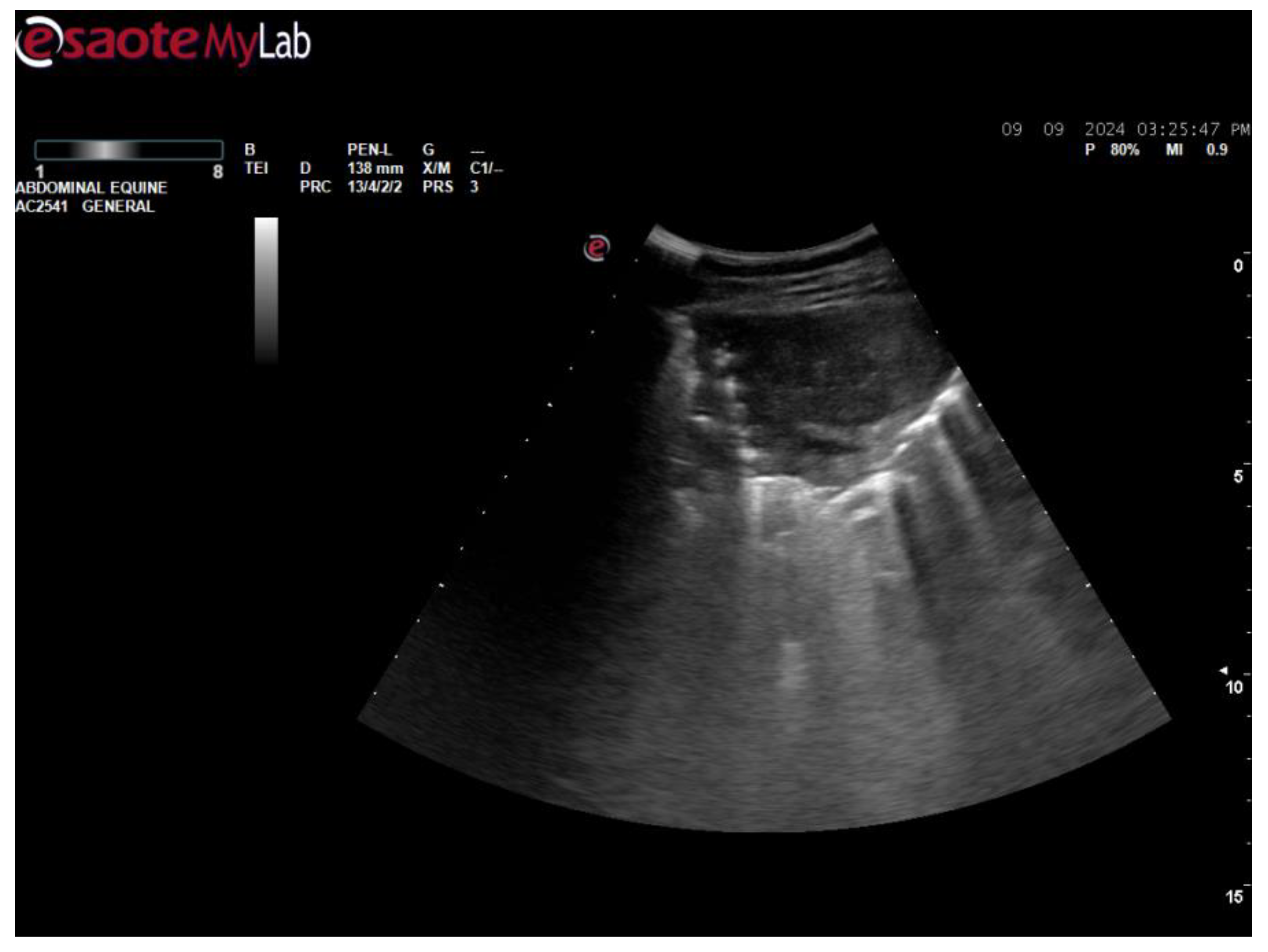
Thoracic ultrasound (EsaoteMyLab, depth 138mm, P 80%, MI 0.9) revealed a 45mm x 50mm anechoic, airless derivative in the left lung cranioventral part (Figure 5), lesion grade 5 from 10 according to Nathan M. Slovis et al. 2005 grading system). On both sides, prominent B- lines were visible almost everywhere throughout the pleura. During treatment period derivatives did not change its size and echogenity ultrasonographically.
Using percutaneus ultrasound, mixed echogenity mas (approximately 7 cm in diameter) was observed in lower abdomen with significant vascularization (video S1). Mesentery lymphadenopathy or abscesses were presumed. During treatment it was observed that mas was changing its location in the abdomen, sometimes it was not seen at all. During hospitalization, the mass tended to grow and permanently stay in the lower abdomen and increased in size (approximately 12 cm in diameter).
Figure 5.
Anechoic, airless derivative in the left lung cranioventral part.
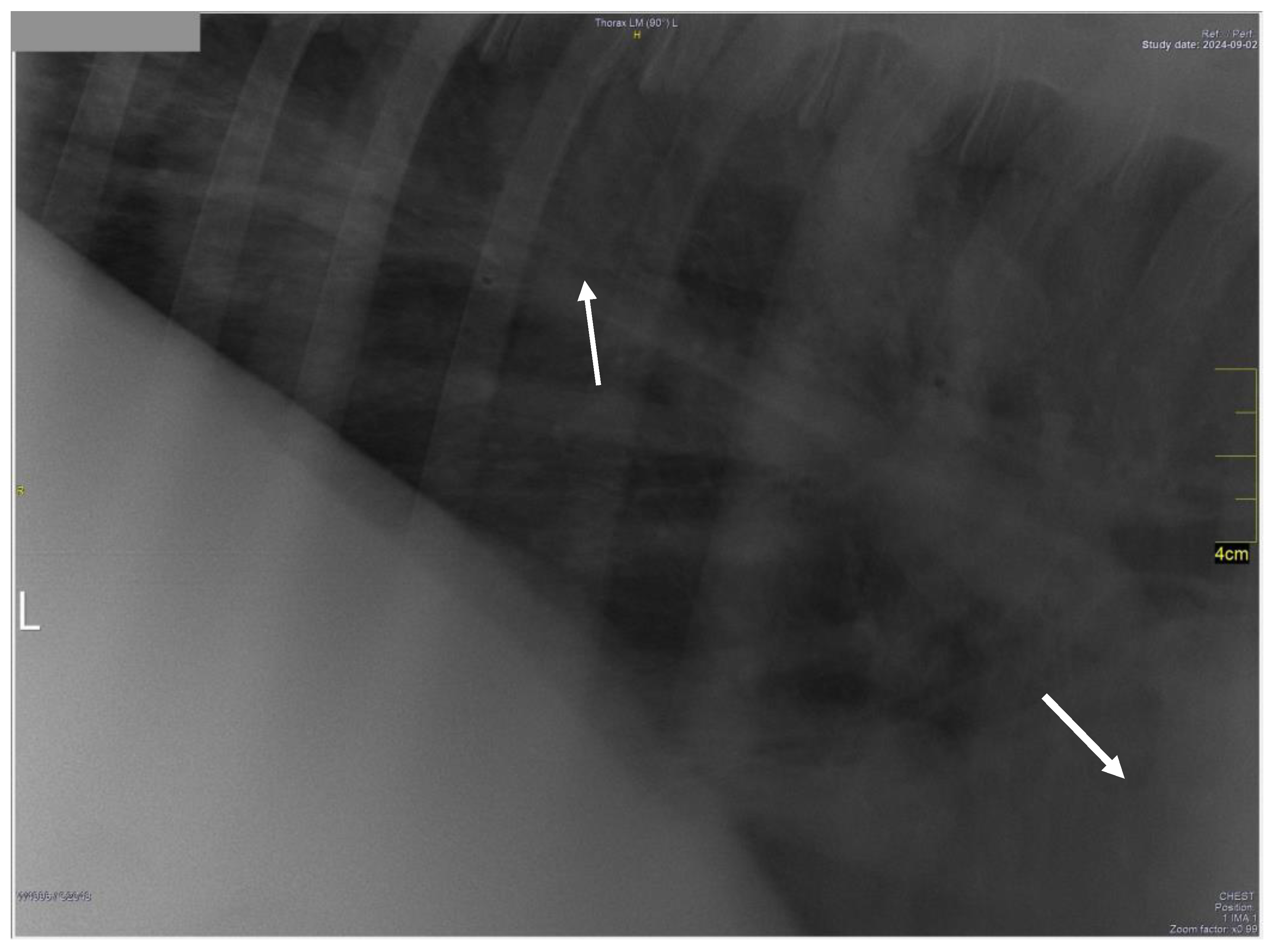
Thoracic radiographs revealed a severe patchy alveolar pattern with rounds of soft tissue opacities with areas of gas lucency (Figure 6).
Figure 6.
A severe patchy alveolar pattern with rounds of soft tissue opacities with areas of gas lucency (arrows).
Figure 6.
A severe patchy alveolar pattern with rounds of soft tissue opacities with areas of gas lucency (arrows).
A diagnosis of bronchopneumonia due to Rhodococcus equi was made. The foal was treated with rifampin (5 mg/kg bw, PO, q12h) and clarithromycin (7.5 mg/kg bw, PO, q12h), along with supportive therapy (vitamin C, B, and IV fluids) to correct electrolyte imbalances.
Flunixin meglumine (Vetaflumex 50mg/ml,VetAgro, Poland, dose 1.1mg/kg bw q12h) and later metamizole natrium monohydrate (Pyralgin 500mg, Biowet Pulavy, Poland, 20-50mg/kg bw q4h) were used for fever, and 2 liters of hyperimmunised plasma was administered for colloidal support. Gentamicin was added after TTW’s culture revealed Pasteurella multocida infection. Despite treatment, the foal's condition deteriorated, and it was re-admitted to the clinic because of persistent pyrexia, anorexia, depression.
Figure 7.
Blood hemolysis after taking a blood sample for blood morphology.

Figure 8.
Hemodynamics of white blood cells (WBC), neutrophils (NEU), red blood cells (RBC), hemoglobin (HGB), packed cell volume (PCV), and platelets (PLT) during hospitalization.
Figure 8.
Hemodynamics of white blood cells (WBC), neutrophils (NEU), red blood cells (RBC), hemoglobin (HGB), packed cell volume (PCV), and platelets (PLT) during hospitalization.
After re-admission, a blood test indicated a further decrease in PCV to 15%, a reduction in RBC to 3.36 × 10^12/l (normal range 6.8–12.9 × 10^12/l), stable haemoglobin at 53 g/l (normal range 110–190 g/l), and an increase in WBC to 110.19 × 10^9/l (normal range 5.4–14.3 × 10^9/l), with neutrophils at 88.79 × 10^9/l (normal range 2.3–9.5 × 10^9/l). Additionally, iron levels remained elevated for a long time (37,5μmol/l, normal 13-25 μmol/l). Antimicrobial treatment was changed to azithromycin (Summamed 500 mg, Teva, dose 10 mg/kg bw, PO, q24h) and doxycycline (DOXYFORT 500, Centrowet Sp. Zo.o., dose 10 mg/kg bw PO q12h) for 14 days. Treatment with dexamethasone i.v. was continued for 14 days (dose 0.04 mg/kg bw every two days). On consecutive days foal’s clinical condition was deteriorating frequently; anorexia, depression and small amount of anechoic- free fluid on the ride side of thorax were detected. Due to worsened clinical condition bronchoscopy was performed a second time, and TTW bacteriology sample was taken. In the pharynx, the dorsal recess, and trachea were hyperemic. Thick yellowish discharge was seen up to bifurcation. Bifurcation edema was 2/4. Foal started to show colic signs periodically. On 32nd day of hospitalization foal’s blood morphology worsened (WBC 41.15 + 10^9/l (normal range 7.29-11.68 + 10^9/l), NEU 38.11 + 10^9/l (normal range 4.8-8.20+ 10^9/l) , RBC 4.23 - 10^12/l (normal range 8.20-9.80 - 10^12/l) , HGB 69 - g/l (normal range 106-130 g/l) , PCV 18.12 %, normal range 30.34-40.18%). TTW bacteriology revealed Pseudomonas Aeruginosa (sensitive to enrofloxacin), Pseudomonas spp. (sensitive to enrofloxacin, doxycycline, ceftiofur), Staphylococcus Aureus (sensitive to ceftiofur, amikacin) and Rhodococcus spp. (sensitive to enrofloxacin, ceftiofur and amikacin) growth. High bacterial resistance was observed. Antimicrobials were changed to ceftiofur (Eficur 50mg/ml, LABORATORIOS HIPRA, S.A.,Spain, dose 10mg/kg bw IM q12h).
On day 38 WBC increased to 70.68 + 10^9/l (normal range 7.29-11.68 + 10^9/l), and PCV dropped to 12% (normal range 30.34-40.18%). Foal’s clinical condition worsened, no response for antimicrobial treatment was observed, and consistent pyrexia was seen. Due to dramatically dropped PCV, severe anemia, and septicemia blood transfusion was performed from a donor identified as compatible via cross-matching (21ml/kg bw). A slight improvement of RBC, HB, PCV was observed after the transfusion, which deteriorated after a couple of days. On day 45 of hospitalization due to worsened clinical condition (anorexia, apathy, pyrexia, shortness of breath, colic) and septicemia foal was euthanized.
3. Post-Mortem Examination
The foal’s body condition score was 3.5 (Henneke Horse Body Condition Scoring System). At necropsy, pale and jaundiced mucous membranes were noted. The inguinal lymph nodes were enlarged, and cross-sections of the hock joints revealed marked jaundice and significant synovial fluid. Subcutaneous tissues appeared pale, yellowish, and dry, and all abdominal organs were similarly pale. A small amount of exudate was found in the abdominal cavity. The mesenteric lymph nodes were enlarged and purulent (Figure 9).The spleen and kidneys were also enlarged and pale. The heart and liver contained chicken fat blood clots. The lungs had multiple small nodules, some up to 5 cm in size, with pus-like exudate present inside (Figure 10). Floatation tests showed emphysema in the lungs.
Figure 9.
Nodules in mesentery.
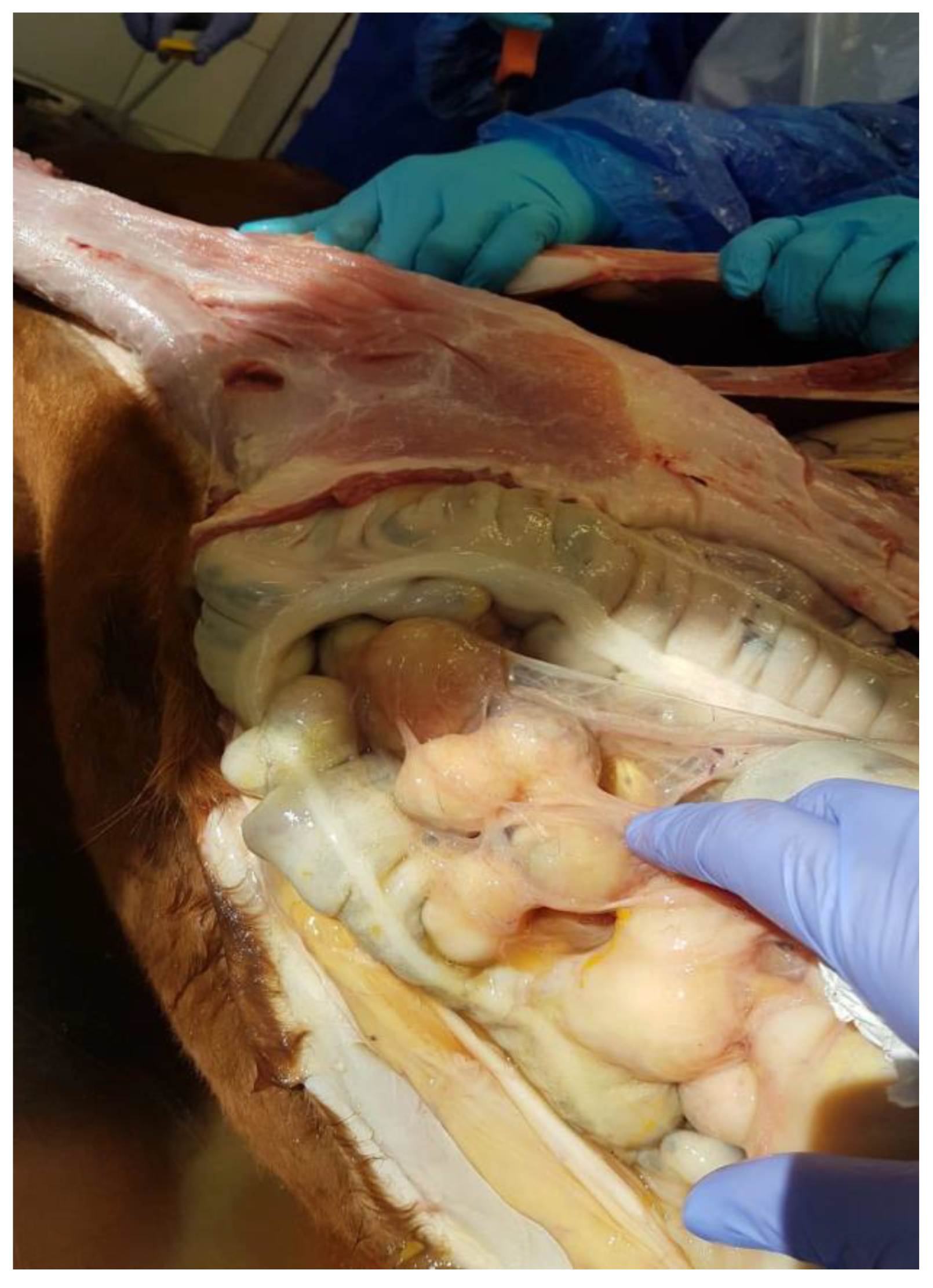
Figure 10.
Nodule in the lung.

4. Discussion
Rhodococcus equi pneumonia primarily affects foals aged 1–6 months and causes significant economic losses in the equine breeding industry [8]. Immune complex deposition can cause polysynovitis which contribute to the development of uveitis, anemia or thrombocytopenia in infected foals [14].While pneumonia is the most common manifestation, R. equi in horses ,infections can also present with other extra-pulmonary conditions distant to the respiratory tract such as polysynovitis, abdominal abscesses and uveitis. Extrapulmonary findings are often associated with more severe cases and worse prognosis [29]. Anemia, fever of unknown origin is reported in human medicine with Rhodococcus equi infection in an immunocompetent patient [33]. Immune-mediated hemolytic anemia (IMHA) associated with R. equi is rare, with only one previous case reported in foals [15]. Rhodococcus equi is generally thought to be non-haemolytic although some earlier investigations reported minor haemolytic activity. A case of a haemolytic R. equi isolate from a swine lymph node with granulomatous lesions is reported [23].
Immune-mediated hemolytic anemia (IMHA) is a rare condition in horses. In adult horses IMHA is mostly associated with chronic bacterial (for example clostridium induced) or viral infection, lymphoma or drug administration [18], idiopatic immune- mediated hemolysis [6]. Secondary IMHA is often triggered by infections or medications that provoke antibody production against red blood cell (RBC) antigens. In cases of secondary IMHA, antibodies are formed against substances, that abnormally coat the red cells [32]. The predominant antibody intent in equine IMHA is IgG. Blood hemolysis for the equids can be intravascular or extravascular. Intravascular hemolysis is less common and characterised by hemoglobinemia and hemoglobinuria. Generally, hemolysis occurs extravasculary, while monocytic-phagocytic system removes immunoglobulin- coated RBC’s by spleen [32,40]. At present case, weakness, tachycardia, depression, icterus and hemoglobinuria suggested intravascular hemolysis [7]. Unique feature of R.Equi is synergistic hemolysis, which occurs when R. equi are cultured on sheep blood agar are cross-streaked with other bacteria, including Staphylococcus aureus, Listeria monocytogenes, and Corynebacterium pseudotuberculosis [26].
Preliminary IMHA diagnosis begins with reduced PCV with normal (or increased) total protein (TPP) concentration [4]. In the current case, reduced PCV and decreased TPP concentration occurred. Icterus, hemoglobinemia, hemoglobinuria is supportive of diagnosis of intravascular IMHA, as seen at present case. Further evidence that this case may be haemolytic anaemia comes from the continued detection of low haemoglobin levels and low MCT. In this case the increased number of inflammatory cells suggests that the haemolytic anaemia could have been initiated by an infection, during which inflammatory cells mistakenly target and eliminate their own erythrocytes. The analysis of the smear indicates a diagnosis of haemolytic anaemia, as it reveals significant alterations in the shape and structure of erythrocytes, including schistocytes, elliptocytes, spherocytes, and other abnormally shaped erythrocytes present in the blood. In chronic disease-related anaemia, erythrocytes typically remain unchanged in shape and size, resulting in normocytic - normochromic anaemia, with haemoglobin levels generally unaffected [17].This type of anaemia typically results from inhibited erythropoiesis, leading to a decreased number of erythrocytes. In hemolytic anemia, the iron concentration in the serum is elevated due to the destruction of red blood cells, as iron from the red blood cells enters the plasma, as it was observed at present case. Justification of IMHA may be supported by direct agglutination or Coomb’s test [32] .However, false negative results can occur, as in previous case report [15], Coomb’s test was also false negative. Test sensitivity reported in dogs are 37-89% [22,38].
Reported IMHA causes are the use of beta-lactam and potentiated sulphonamide antimicrobials [37].In horses, commonly implicated with IMHA antimicrobials are penicillin and trimethoprim [32].In human medicine, rifampin and erythromycin (which were used in the current case) were also reported as possible drugs caused by IMHA in humans. Furthermore, the occurrence is extremely rare [21,25]. Drugs related to IMHA were considered unlikely in this case, because foal already arrived in the clinic highly anemic, before using any of IMHA-related drugs.
Blood loss anemia was ruled out in this case. In blood smear, a limited quantity of reticulocytes was observed, suggesting that the anemia was challenging to regenerate. Horses release reticulocytes from bone marrow very rarely. Typically, hemolytic anemias induce a greater reticulocyte response than blood-loss anemias. Previous studies have documented that horses do not have reticulocytes in peripheral blood in blood-loss anemia [34]. Typically, anemia caused of chronic disease is mild to moderate, slowly progressive and clinically insignificant. Thus, in this case anemia was severe and considered most likely hemolytic.
Corticosteroids are a golden standard in IMHA treatment. They inhibit sequestration and phagocytosis of RBC and decrease antibody production against RBC [18,20]. However, corticosteroid use for IMHA treatment is still debatable among equine practitioners. For horses with severe bacterial infection, corticosteroid use can interfere with the immune response to clearing the infection. Corticosteroids decrease oxygen radicals and lysosomal enzyme release from PMNs also disturbs intracellular bacteria phagocytosis [18,30] .It’s doubtful improvement in hemogram. Permanent or worsening anemia and poor response to antimicrobial treatment will force equine practitioners to strongly consideration of corticosteroid use. Usually, 0.04-0.06 mg/kg bw q24h dexamethasone dosage is used [16,18]. However, there are no clear guidelines in equine medicine for dexamethasone use to prevent further cell destruction. In the present case imminently anemia using corticosteroids was deemed to take precedence over the long-term goal of bacterial cure, bearing in mind the lack of response to antimicrobial treatment, persistent pyrexia, anorexia, and hemolysis. In the current case, the initial dose of 0.1mg/kg bw [24] of dexamethasone was used, with the following dose of 0.04 mg/kg bw q24h ,later q48h. A relatively low corticosteroid dose was used.
In order to reduce endotoxemia and septicemia and provide colloidal support plasma was applied in the current case [36]. On day 38 when PCV dropped to 13%, a whole blood transfusion was performed. A slight improvement of RBC, HB, PCV (Figure 8) was observed after the transfusion, which deteriorated after a couple of days. The purpose of whole blood transfusion is to restore oxygen delivery to the tissues [13]. According to [12] PCV as low as 10-12% is considered too low and blood transfusion is recommended, because adequate oxygen delivery to tissues is not provided. Usually, horses become tachycardic, tachypneic, and depressive while adequate oxygen delivery is not provided. Transfused blood cells have a relatively short half-life and antibody production against transfused cells occurs rapidly [16,34] .In the current case, only one blood transfusion was performed. Despite a slight clinical and hematological increasement, the foal condition deteriorated, and septicemia occurred lately, so it was decided to perform euthanasia.
Post-mortem examination revealed spleen and kidney enlargement, jaundice in mucus membranes. All internal organs were anemic. Generalized icterus, splenomegaly, enlarged kidneys is characteristic feature of hemolytic anemia [7]. Severely enlarged and purulent mesenteric lymph nodes of foals with R.Equi infection are limitedly described in literature [10,28]. As in [15] case report, a large masses of mixed echogenicity, presumed to be enlarged lymph nodes or abscesses were seen in mesentery, performing percutaneous ultrasound of foal’s abdomen. Mesenteric lymphadenopathy is commonly found on postmortem examination in horses with infectious, inflammatory, or neoplastic disease but has been rarely reported as an ultrasound finding. Autoimmune hemolytic anemia (AIHA) has been associated with lymphoproliferative disorders in human medicine [5]. Mesenteric lymph nodes are not often visualized by ultrasound because of their location deep within the abdomen [3]. Ultrasonographically, lymph nodes are hypoechoic to the perinodal tissue, ovoid with smooth well-delineated margins and show an homogeneous echotexture[1,19,27,31]. It is reported, that lymph nodes can have characteristic blood perfusion, which is seen using Color Doppler ultrasound imaging [2,35]. It helps to distinguish mesenteric lymphadenopathy from abscessation. Our case report provides valuable information about ultrasonography imaging of mesenteric lymphadenopathy in foal (video S1).
During the past decade, Rhodococcus equi treatment has become more and more challenging because of multidrug resistance (MDR) which results as lack of positive response to antimicrobial treatment in vivo [9]. Many equine breeding facilities use thoracic ultrasonographic screening and antimicrobial treatment of subclinically affected foals [11]. Vaccination is a promising approach to prevent disease, but most R.equi vaccine candidates tested to date have not been sufficiently effective. In the present case, foals dam was vaccinated against R. Equi, however R.Equi infection affects foal significantly. Doxycycline use in place of macrolides and rifampicin suggests potential for reduction of resistance in some in vitro studies [8,39,40]. At present case MDR was observed not only for R. Equi but also to secondary bacterial infections detected during culture: P. Aeruginosa, Pseudomonas spp., Staphylococcus aureus.
Diagnosis of hemolytic anemia in this case was made based on strong clinical evidence, changes in blood morphology and biochemistry, blood smear analysis, positive response to dexamethasone therapy and post-mortem changes but could have been supported by further diagnostic testing.
This article provides valuable information about clinical course, progression and outcome of presumed immune- mediated hemolytic anemia in foal with Rhodococcus equi infection,especially about postmortem examination, which is not reported in Imogen C. John et. Al article, because both foals survived.
5. Conclusion
Although immune-mediated hemolytic anemia is a rare complication of Rhodococcus equi infections in foals, it is important to consider this diagnosis in cases of severe anemia . The case described highlights the need for further investigation into the clinical progression, treatment strategies, and prognosis of foals affected by R. equi infection and concurrent immune-mediated hemolytic anemia. Further studies will help develop optimal treatment plans and improve the outcomes for foals diagnosed with these rare, but significant extra-pulmonary disorders, associated with R.Equi infection.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, Video S1: mixed echogenity mas in lower abdomen, using percutaneus ultrasound.
Author Contributions
R.T-S.: writing original draft; I.M.- Writing - review & editing ,R.G.- Writing - review & editing, B.P.- Writing - review & editing, J.H.- Writing - review & editing and data curation, M.U.D.- Writing - review & editing and data curation, A.U.- Writing - review & editing and data curation
Funding
This research received no external funding.
Institutional Review Board Statement
Given that blood and other biological samples were collected for routine diagnostic purposes and solely for the animal’s benefit, and the owner had signed a consent form that authorized the use of their data and excess specimens for research purposes, formal approval from the University’s Ethical Committee was not required.
Informed Consent Statement
Not applicable
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Petra Agthe, Abby R. Caine, Barbara Posch, and Michael E. Herrtage. 2009. ULTRASONOGRAPHIC APPEARANCE OF JEJUNAL LYMPH NODES IN DOGS WITHOUT CLINICAL SIGNS OF GASTROINTESTINAL DISEASE. Vet Radiology Ultrasound 50, 2 (March 2009), 195–200. https://doi.org/10.1111/j.1740-8261.2009.01516.x. [CrossRef]
- Felix Amereller, Christian Lottspeich, Grete Buchholz, and Karl Dichtl. 2020. A horse and a zebra: an atypical clinical picture including Guillain-Barré syndrome, recurrent fever and mesenteric lymphadenopathy caused by two concomitant infections. Infection 48, 3 (June 2020), 471–475. https://doi.org/10.1007/s15010-020-01397-5. [CrossRef]
- Betsy Vaughan, DVM*; Mary Beth Whitcomb, DVM, MBA, ECVDI (LA Assoc); and Nicola Pusterla, DVM, PhD, Diplomate ACVIM. 2013. Ultrasonographic Findings in 42 Horses With Cecal Lymphadenopathy. Vol. 59, AAEP PROCEEDINGS (2013), 238. Retrieved from https://www.cabidigitallibrary.org/doi/pdf/10.5555/20143210449.
- D. E. Brown, D. J. Meyer, W. E. Wingfield, and R. M. Walton. 1994. Echinocytosis Associated with Rattlesnake Envenomation in Dogs. Vet Pathol 31, 6 (November 1994), 654–657. https://doi.org/10.1177/030098589403100604. [CrossRef]
- Nicholas B. Burley, Paul S. Dy, Suraj Hande, Shreyas Kalantri, Chirayu Mohindroo, and Kenneth Miller. 2021. Autoimmune Hemolytic Anemia as Presenting Symptom of Hodgkin Lymphoma. Case Rep Hematol 2021, (2021), 5580823. https://doi.org/10.1155/2021/5580823. [CrossRef]
- H. J. Cottle and K. J. Hughes. 2010. Haemolytic anaemia in a pony associated with a perivascular abscess caused by Clostridium perfringens. Equine Veterinary Education 22, 1 (January 2010), 13–19. https://doi.org/10.2746/095777309X474. [CrossRef]
- T. J. Divers, L. W. George, and J. W. George. 1982. Hemolytic anemia in horses after the ingestion of red maple leaves. J Am Vet Med Assoc 180, 3 (February 1982), 300–302.
- Erdal Erol, Carrie L. Shaffer, and Brian V. Lubbers. 2022. Synergistic combinations of clarithromycin with doxycycline or minocycline reduce the emergence of antimicrobial resistance in Rhodococcus equi. Equine Veterinary Journal 54, 4 (July 2022), 799–806. https://doi.org/10.1111/evj.13508. [CrossRef]
- S. Giguère, N.D. Cohen, M. Keith Chaffin, N.M. Slovis, M.K. Hondalus, S.A. Hines, and J.F. Prescott. 2011. Diagnosis, Treatment, Control, and Prevention of Infections Caused by R hodococcus equi in Foals. Veterinary Internal Medicne 25, 6 (November 2011), 1209–1220. https://doi.org/10.1111/j.1939-1676.2011.00835.x. [CrossRef]
- Steeve Giguère and Gregory D. Roberts. 2012. ASSOCIATION BETWEEN RADIOGRAPHIC PATTERN AND OUTCOME IN FOALS WITH PNEUMONIA CAUSED BY R hodococcus equi. Vet Radiology Ultrasound 53, 6 (November 2012), 601–604. https://doi.org/10.1111/j.1740-8261.2012.01964.x. [CrossRef]
- Courtney Higgins and Laura Huber. 2023. Rhodococcus Equi: Challenges to Treat Infections and to Mitigate Antimicrobial Resistance. Journal of Equine Veterinary Science 127, (August 2023), 104845. https://doi.org/10.1016/j.jevs.2023.104845. [CrossRef]
- Anna Hollis and Kevin Corley. 2007. Practical guide to fluid therapy in neonatal foals. In Practice 29, 3 (March 2007), 130–137. https://doi.org/10.1136/inpract.29.3.130. [CrossRef]
- Samuel D. Hurcombe, Margaret C. Mudge, and Kenneth W. Hinchcliff. 2007. Clinical and clinicopathologic variables in adult horses receiving blood transfusions: 31 cases (1999–2005). javma 231, 2 (July 2007), 267–274. https://doi.org/10.2460/javma.231.2.267. [CrossRef]
- Rabyia Javed, A. K. Taku, R. K. Sharma, and Gulzaar Ahmed Badroo. 2017. Molecular characterization of Rhodococcus equi isolates in equines. Vet World 10, 1 (January 2017), 6–10. https://doi.org/10.14202/vetworld.2017.6-10. [CrossRef]
- Imogen C. Johns, Anne Desrochers, Kathryn L. Wotman, and Raymond W. Sweeney. 2011. Presumed immune-mediated hemolytic anemia in two foals with Rhodococcus equi infection. J Vet Emergen Crit Care 21, 3 (June 2011), 273–278. https://doi.org/10.1111/j.1476-4431.2011.00633.x. [CrossRef]
- F. A. Kallfelz, R. H. Whitlock, and R. D. Schultz. 1978. Survival of 59Fe-labeled erythrocytes in cross-transfused equine blood. Am J Vet Res 39, 4 (April 1978), 617–620.
- Anazoeze Jude Madu and Maduka Donatus Ughasoro. 2017. Anaemia of Chronic Disease: An In-Depth Review. Med Princ Pract 26, 1 (2017), 1–9. https://doi.org/10.1159/000452104. [CrossRef]
- T. S. Mair, F. G. Taylor, and M. H. Hillyer. 1990. Autoimmune haemolytic anaemia in eight horses. Vet Rec 126, 3 (January 1990), 51–53.
- Monique N. Mayer, Joshua A. Lawson, and Tawni I. Silver. 2010. SONOGRAPHIC CHARACTERISTICS OF PRESUMPTIVELY NORMAL CANINE MEDIAL ILIAC AND SUPERFICIAL INGUINAL LYMPH NODES: Sonographic Features of Normal Lymph Nodes. Veterinary Radiology & Ultrasound 51, 6 (November 2010), 638–641. https://doi.org/10.1111/j.1740-8261.2010.01710.x. [CrossRef]
- Sheila McCullough. 2003. Immune-mediated hemolytic anemia: understanding the nemesis. Veterinary Clinics of North America: Small Animal Practice 33, 6 (November 2003), 1295–1315. https://doi.org/10.1016/j.cvsm.2003.08.003. [CrossRef]
- Sandra J. Nance, Stephan Ladisch, Timothy L. Williamson, and George Garratty. 1988. Erythromycin-Induced Immune Hemolytic Anemia. Vox Sanguinis 55, 4 (November 1988), 233–236. https://doi.org/10.1111/j.1423-0410.1988.tb04703.x. [CrossRef]
- Jed A. Overmann, Leslie C. Sharkey, Doug J. Weiss, and Dori L. Borjesson. 2007. Performance of 2 microtiter canine Coombs’ tests. Veterinary Clinical Pathol 36, 2 (June 2007), 179–183. https://doi.org/10.1111/j.1939-165X.2007.tb00205.x. [CrossRef]
- M. Pate, T. Pirš, I. Zdovc, B. Krt, and M. Ocepek. 2004. Haemolytic Rhodococcus equi Isolated from a Swine Lymph Node with Granulomatous Lesions. Journal of Veterinary Medicine, Series B 51, 5 (June 2004), 249–250. https://doi.org/10.1111/j.1439-0450.2004.00758.x. [CrossRef]
- S. F. Peek. 2010. Immune-mediated haemolytic anaemia in adult horses: Do we need to transfuse, immunosuppress or just treat the primary problem? Equine Veterinary Education 22, 1 (January 2010), 20–22. https://doi.org/10.2746/095777309X475. [CrossRef]
- A. Pereira, C. Sanz, F. Cervantes, and R. Castillo. 1991. Immune hemolytic anemia and renal failure associated with rifampicin-dependent antibodies with anti-I specificity. Ann Hematol 63, 1 (July 1991), 56–58. https://doi.org/10.1007/BF01714964. [CrossRef]
- J F Prescott. 1991. Rhodococcus equi: an animal and human pathogen. Clin Microbiol Rev 4, 1 (January 1991), 20–34. https://doi.org/10.1128/CMR.4.1.20. [CrossRef]
- Charles R. Pugh. 1994. ULTRASONOGRAPHIC EXAMINATION OF ABDOMINAL LYMPH NODES IN THE DOG. Vet Radiology Ultrasound 35, 2 (March 1994), 110–115. https://doi.org/10.1111/j.1740-8261.1994.tb00197.x. [CrossRef]
- Alicja Rakowska, Agnieszka Marciniak-Karcz, Andrzej Bereznowski, Anna Cywińska, Monika Żychska, and Lucjan Witkowski. 2022. Less Typical Courses of Rhodococcus equi Infections in Foals. Veterinary Sciences 9, 11 (October 2022), 605. https://doi.org/10.3390/vetsci9110605. [CrossRef]
- S. M. Reuss. 2022. Rhodococcus equi , extrapulmonary disorders and lack of response to therapy. Equine Veterinary Education 34, 8 (August 2022), 399–400. https://doi.org/10.1111/eve.13583. [CrossRef]
- S. Schmaldienst and W. H. Horl. 1996. Bacterial infections during immunosuppression - immunosuppressive agents interfere not only with immune response, but also with polymorphonuclear cell function. Nephrol Dial Transplant 11, 7 (July 1996), 1243–1245.
- Elke Schreurs, Kathelijn Vermote, Virginie Barberet, Sylvie Daminet, Heike Rudorf, and Jimmy H. Saunders. 2008. ULTRASONOGRAPHIC ANATOMY OF ABDOMINAL LYMPH NODES IN THE NORMAL CAT. Vet Radiology Ultrasound 49, 1 (January 2008), 68–72. https://doi.org/10.1111/j.1740-8261.2007.00320.x. [CrossRef]
- Debra C. Sellon. 2004. Disorders of the Hematopoietic System. In Equine Internal Medicine. Elsevier, 721–768. https://doi.org/10.1016/B0-72-169777-1/50014-7. [CrossRef]
- E. Sigler, A. Miskin, M. Shtlarid, and A. Berrebi. 1998. Fever of unknown origin and anemia with Rhodococcus equi infection in an immunocompetent patient. Am J Med 104, 5 (May 1998), 510.
- Joseph E. Smith, Molly Dever, Jana Smith, and Richard M. DeBowes. 1992. Post-Transfusion Survival of50 Cr-Labeled Erythrocytes in Neonatal Foals. Veterinary Internal Medicne 6, 3 (May 1992), 183–185. https://doi.org/10.1111/j.1939-1676.1992.tb00334.x. [CrossRef]
- H J Steinkamp, M Mueffelmann, J C Böck, T Thiel, P Kenzel, and R Felix. 1998. Differential diagnosis of lymph node lesions: a semiquantitative approach with colour Doppler ultrasound. The British Journal of Radiology 71, 848 (August 1998), 828–833. https://doi.org/10.1259/bjr.71.848.9828794. [CrossRef]
- Brett Tennent-Brown. 2011. Plasma Therapy in Foals and Adult Horses. (2011).
- Helen L Thomas and Michael A Livesey. 1998. Immune-mediated hemolytic anemia associated with trimethoprim-sulphamethoxazole administration in a horse. 39, (1998).
- K. Jane Wardrop. 2005. The Coombs’ test in veterinary medicine: past, present, future. Veterinary Clinical Pathol 34, 4 (December 2005), 325–334. https://doi.org/10.1111/j.1939-165X.2005.tb00057.x. [CrossRef]
- Maria Wetzig, Monica Venner, and Steeve Giguère. 2020. Efficacy of the combination of doxycycline and azithromycin for the treatment of foals with mild to moderate bronchopneumonia. Equine Veterinary Journal 52, 4 (July 2020), 613–619. https://doi.org/10.1111/evj.13211. [CrossRef]
- Melinda J. Wilkerson, Elizabeth Davis, Wilma Shuman, Kenneth Harkin, Judy Cox, and Bonnie Rush. 2000. Isotype-Specific Antibodies in Horses and Dogs with Immune-Mediated Hemolytic Anemia. J Vet Int Med 14, 2 (2000), 190. https://doi.org/10.1892/0891-6640(2000)014<0190:IAIHAD>2.3.CO;2. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



