
Submitted:
27 December 2024
Posted:
30 December 2024
You are already at the latest version
Abstract
Background: Several studies have reported alarming rates of mental health issues and sleep problems among nurses even in the post-pandemic era. Objectives: To investigate the prevalence of stress, anxiety, depression, burnout and insomnia among nurses in Greece one year after the end of the pandemic and to construct a mediation model evaluating the impact of stress on insomnia, the chain mediating roles of depression and burnout, as well as the moderating role of anxiety in the model. Methods: This cross-sectional study was conducted online in July 2024 and included 380 hospital nurses who completed the Depression Anxiety Stress Scale (DASS-21), the Copenhagen Burnout Inventory (CBI) and the Athens Insomnia Scale (AIS). Results: The prevalence rates of stress, anxiety, depression, burnout and insomnia were 33.9%, 33.3%, 35%, 46.8% and 56.1%, respectively. Multiple regression analysis indicated that the Depression subscale of the DASS-21 explained 40.6% of the variance in AIS, while an additional 7.6% was explained by CBI and another 1.3% rate by the Stress subscale of the DASS-21. Mediation analysis revealed that stress affected insomnia both directly and indirectly through the chain mediating roles of depression and burnout. Anxiety moderated the chain mediation path by enhancing the negative impact of stress on depression. Conclusions: The proposed moderated chain mediation model introduces certain factors influencing insomnia and explains how changes in any one of these factors effectuate changes in the other factors, offering insights for individualized interventions.
Keywords:
stress
; anxiety
; depression
; burnout
; insomnia
; nurses
1. Introduction
The COVID-19 pandemic lasted almost three years, from 30 January 2020 when the World Health Organization (WHO) designated the outbreak as a Public Health Emergency of International Concern (PHEIC) [1] and labeled it a pandemic on 11 March 2020 [2], until 5 May 2023 when the WHO announced its official conclusion [3]. The onset of the pandemic completely overwhelmed the health systems in most countries. Major deficiencies of ventilators, intensive care beds, personal protective equipment and significant shortages of health workers exposed the flawed health policies implemented in previous years. Notably, the pandemic had a profound social, economic and psychological impact on populations worldwide, fundamentally changing daily life and affecting public health, far beyond the direct impact of the virus itself [4,5]. Psychological distress prevailed during the pandemic [6], with reports showing increased rates of insomnia, anxiety, depression, stress and burnout among health care workers, particularly nurses [7]. Prolonged and close interaction with patients combined with increased exposure to their emotional distress possibly explains the particular vulnerability of nurses [8].
Sleep disturbances among nurses during the pandemic have understandably drawn plenty of attention from researchers, as they can contribute to physical and mental health problems and are associated with an increased risk of workplace errors; burnout and job change [9,10,11,12]. Insomnia, shift work causing circadian rhythms disruption and insufficient sleep are common among nurses, especially hospital nurses who almost exclusively engage in shift work [13,14]. During the pandemic nurses were constantly faced with stressful situations while navigating through complicated procedures of care and treatment. Chronic exposure to increased amounts of stress often causes insomnia [15], whereas good quality sleep protects against the negative impact of stress. Studies during the pandemic reported that insomnia in nurses was associated with stress, anxiety, depression and burnout [16,17,18,19,20]. Results from these studies suggested that insomnia may have a negative effect on depression and anxiety and lead to burnout in nurses [21].
According to the 11th revision of the International Classification of Diseases (ICD-11), the code QD85 is attributed to burnout syndrome which is considered to result from ongoing work-related stress that has not been effectively addressed and resolved [22]. The main component of this syndrome is the feeling of exhaustion experienced by professionals in the occupational context, which is significantly related to job dissatisfaction [23,24]. Healthcare professionals were among the first individuals in the workforce in whom burnout syndrome was investigated [25]. All studies over the past few decades consistently reported high levels of burnout in nursing staff [26,27,28,29,30] and simultaneously evidenced constantly high associations of burnout with depression and anxiety [31,32].
The significant correlation between burnout and depression was established from the first publications examining the nature of burnout [33]. This association has prompted several scholars to argue that burnout is likely to be a form of depression [34,35]. However, typical symptoms of depression such as low self-esteem, feelings of guilt, hopelessness and suicidal tendencies are not typical symptoms of burnout. On the other hand, in burnout extended removal from work on vacation has beneficial effects, whereas a depressive episode necessitates psychotherapeutic intervention and/or medication. Research suggests that depression is a significant factor influencing burnout levels of nursing staff [36,37] and previous literature converges on the view that burnout likely acts as a predisposing factor increasing the risk of depression [38,39,40].
Stress is implicated in the etiology of depression and people who report chronic stress are more likely to be diagnosed with a depressive disorder [41,42]. By definition burnout is understood as the outcome of prolonged unresolved occupational stress [43]. Employment conditions and workload predict anxiety and perceived stress among employees and lack of administrative support is the most important factor responsible for the increase in anxiety [44]. According to research, anxiety and depression are important factors affecting burnout of nurses [32]. Moreover, scholars have investigated the correlation between insomnia and workplace stressors [45]. Consequently, nurses who work in stressful and demanding settings are at increased risk for insomnia, anxiety, depression and burnout [46].
Numerous studies have documented the prevalence of these aforementioned mental health issues among nurses [47,48] but few have focused on their interrelations [49,50] and examined their mediating effects in one model [21,46,51,52,53,54,55,56]. Also, past and current studies after the official conclusion of the pandemic reveal that these psychological effects could persist for a long time [57,58,59,60,61,62,63,64]. Therefore, in this study we aim to assess the levels and explore the interrelations among stress, anxiety, depression, burnout and insomnia in nurses working in Greek hospitals one year after the end of the pandemic. We are not aware of previous research investigating the chain mediating effects of depression and burnout as well as the moderating role of anxiety in the linkage between stress and insomnia. To address this objective we formulated the following hypotheses:
Hypothesis 1: Stress is positively associated with and predicts insomnia.
Hypothesis 2: Depression mediates the effect of stress on insomnia.
Hypothesis 3: Burnout mediates the effect of stress on insomnia.
Hypothesis 4: Stress impacts insomnia through a chain mediation effect of depression and burnout.
Hypothesis 5: Anxiety moderates the relationship between stress and depression. The higher the anxiety is, the stronger the positive association between stress and depression will be, and the stronger the chain mediation effect of depression and burnout in the relationship between stress and insomnia.
2. Materials and Methods
2.1. Research Design
To address the above objectives we conducted a cross-sectional study using a homogeneous convenience sampling method [65]. Recruited participants were nurses working in Greek hospitals with a minimum of one year of professional experience. The data were collected via Google Forms and the online questionnaire was shared electronically through the email addresses retrieved from scientific and professional registries of Greek nurses. The invitation email delivered to participants included an anonymous link that provided access to the Google Forms online research platform. Consenting participants declared that they agree to participate voluntarily by marking the “I agree” option as stated on the first page of the online questionnaire, which was considered informed consent. The sample for this study included nurses who consented to take part and subsequently filled out the other sections of the online questionnaire.
2.2. Study Participants
The study was conducted in July 2024. To determine the sample size, given that the target population was 27,103 individuals, and with a confidence level of 95%, a confidence interval of 5%, and an assumption of a 50% response rate, a minimum sample size of 379 participants was required [66]. A total of 500 invitations were emailed, with 380 responses received (response rate: 76%).
2.3. Ethical Considerations
This study was conducted following ethical principles outlined in the General Data Protection Regulation (GDPR - 2016/679) of the European Union, the World Medical Association Declaration of Helsinki (1975, revised 2008), and the guidelines of the International Committee of Medical Journal Editors. The study protocol was approved by the Ethics Committee of Clinical Research of the General Hospital for Thoracic Diseases of Athens “SOTIRIA” (Approval Number: 20649/16-05-2023).
2.4. Measurement Tools
After giving their consent and prior to answering the questionnaires, respondents were asked to provide demographic and professional data, including their gender, age, and years of work experience. Then, they were prompt to fill out the following set of questionnaires:
2.4.1. Depression Anxiety Stress Scale (DASS-21)
The Depression Anxiety Stress Scale-21 (DASS-21) [67] is a measurement tool which comprises three self report subscales intended to evaluate stress, anxiety and depression. Seven statements on a four-point Likert scale make up each subscale ranging from 0 (did not apply to me at all) to 3 (applied to me very much or most of the time). Scores must be multiplied by 2 to determine the final score. Elevated scores reflect the increasing experience of stress, anxiety and depression. The depression subscale evaluates dysphoria, anhedonia, inertia, hopelessness, feelings of sadness loss of interest or pleasure, self-deprecation and worthlessness (e.g., “I couldn’t seem to experience any positive feeling at all”). The anxiety subscale evaluates skeletal muscle effects, situational anxiety, autonomic arousal, and the subjective sensation of anxious affect (e.g., “I felt I was close to panic”). The stress subscale estimates chronic non specific arousal levels such as restlessness, nervousness, excitability, agitation, irritability, overreaction and impatience (e.g., “I felt that I was using a lot of nervous energy”). Different cut-off values exist for the conventional severity levels for each subscale; i.e., scores above 9 are indicative for depressive symptoms, above 7 for anxiety, and above 14 for stress. The total score is an indicator of general psychological distress. The DASS-21 is a screening tool designed to identify areas of concern and not a diagnostic instrument for assigning patients to specific diagnostic categories proposed in classification systems. The DASS-21 is acknowledged for its robust psychometric properties [68]. In this research the Greek version of the scale was used [69] and for the present sample, Cronbach’s alpha values of the depression, anxiety, and stress subscales were 0.912, 0.902, and 0.914, respectively.
2.4.2. Copenhagen Burnout Inventory (CBI)
The Copenhagen Burnout Inventory (CBI) is the most common instrument for burnout assessment [70], consisting of 19 questions and evaluating the concept of burnout in three subdimensions: the first six questions reflect personal burnout; the next seven questions evaluate work-related burnout; and the last six questions appraise patient-related burnout. The personal burnout subscale measures the level of perceived physical and psychological burnout (e.g., “How often do you feel weak and/or vulnerable to illness?”). Responses options are rated on a five-point Likert ranging from “always” to “never/almost never”. The perceived physical and psychological burnout related to work is evaluated by the work-related burnout subscale (e.g., “Do you feel every hour at work is exhausting?”). For this subscale response options, rated on a five-point Likert, range from “to a very high degree” through “to a very low degree” for the first three questions and from “always” to “never/almost never” for the last four questions. The patient-related burnout subscale assesses perceived physical and psychological burnout from interaction with patients (e.g., “Do you feel frustrated working with patients?”). For this subscale response options, rated on a five-point Likert, range from “to a very high degree” through “to a very low degree” for the first four questions and from “always” to “never/almost never” for the last two questions. The answers are converted into scores of 100, 75, 50, 25, 0. All burnout subscales have scores between 0 and 100, with greater scores indicating increased degrees of occupational burnout. In this study, the Greek version of the CBI was used, which is a valid scale, possessing robust psychometric properties [71]. The Cronbach’s alpha coefficient for the entire scale in this study was α = 0.933. A total score of ≥50 [72,73,74,75,76,77,78] indicates professional burnout.
2.4.3. Athens Insomnia Scale (AIS)
The Athens Insomnia Scale (AIS) is a self-report measurement tool intended to measure the severity of insomnia (how severely certain sleep difficulties have affected the responders during the past month) using diagnostic criteria set forth by the 10th Revision of the International Classification of Diseases and Related Health Problems (ICD-10). The scale comprises eight items amongst which the first five assess nocturnal sleep (sleep induction, night-time awakenings, final awakening, total sleep duration, and overall sleep quality) and the final three items are related to daytime dysfunction (well-being, functioning, and drowsiness throughout daytime). Response scores for each item range from 0 to 3 and total score spans from 0 to 24, with greater scores signifying increased severity of insomnia. A diagnostic threshold set at 6 indicates insomnia [79]. The AIS is a widely used tool for assessing insomnia. The Greek version of the AIS has demonstrated good psychometric properties [80]. In this study the Cronbach's alpha coefficient was measured at α = 0.878.
2.5. Statistical Analysis
Firstly, since self-report questionnaires were adopted to collect the data, the Harman single-factor test was employed to examine the common method bias [81]. The most significant component determined 39.686% of the variance which is lower than the criterion of 50%. Subsequently, descriptive statistical methods were applied to estimate means and standard deviations for continuous variables and to calculate the proportion of responders that scored above the cutoff values of clinically significant stress, anxiety, depression, burnout and insomnia. Furthermore, using t-tests and χ² tests, we compared the sample to the general population of nurses in Greece regarding years of professional experience, age, and gender, in order to examine the representativeness of the sample. Gender differences as to the study variables were assessed using t-tests. Correlations between all variables included in the present study were investigated using Pearson's correlation test. Linear regression analysis was utilized to determine if the correlated variables were significant predictors of insomnia. Before proceeding with the regression analysis, the prerequisite assumptions were checked, and specifically, normality by visual examination of the predicted probability plots, linearity through the visual review of scatter plot pairs, and homoscedasticity through residuals scatterplot. The independence of residuals was assessed with the Durbin-Watson test. The Variance Inflation Factor (VIF) analysis was performed to determine the absence of multicollinearity in the data. To examine the chain mediation effect of depression and burnout between stress and insomnia we conducted the serial mediation analysis using Hayes' SPSS Process Macro Model 6. The moderating role of anxiety in the chain mediation model was tested using Hayes' SPSS Process Macro Model 83. Regression coefficients reported were unstandardized, and 95% confidence intervals were assessed using 5,000 bootstrap samples [82]. Finally, analysis of simple slopes was performed to report the regulating effect at different levels of anxiety. The data analyses were conducted using SPSS software (Version 24.0). For all statistical analyses, statistical significance was set at p < 0.05 (two-tailed).
3. Results
Since the data acquired for the study were derived from self-reports, common method bias testing was required and for this purpose the Harman single factor method test was utilized. Results from the exploratory factor analysis indicated that the first common factor had an explanation rate of 39.686 percent, which was less than the critical value of 50 percent, suggesting no significant common method bias in this study.
A total of 380 nurses (74 males and 306 females) participated in the study. As to gender, age, and years of professional experience no significant differences were identified between the study sample and the total population of nurses working in Greece [66]. Overall, 56.1% of the nurses exhibited insomnia symptoms (AIS ≥ 6), 46.8% presented signs of burnout (CBI ≥ 50), while 31.1% experienced symptoms of general psychological distress (DASS-21>32) [83]. Regarding the severity levels of stress, anxiety, and depression 33.9%, 33.3% and 35% of the participants scored above the recommended normal values in DASS-21, whereas percentages of 25%, 26.8% and 23.9% were found to have moderate to extremely severe levels of stress, anxiety, and depression, respectively. Table 1 presents the mean values and standard deviations of the study variables.
Regarding gender, female nurses evidenced higher mean scores in the DASS-21 total and the stress subscale compared to male nurses (t-test p < 0.05, 29.53 ± 27.42 vs. 22.67 ± 21.88 and t-test p < 0.05, 13.47 ± 10.26 vs. 10.67 ± 8.2, Table 1). Additionally, female nurses showed higher scores in the Copenhagen Burnout Inventory (t-test p < 0.05, 49.64 ± 19.03 vs. 44.91 ± 17.93, Table 1).
AIS correlated positively with DASS-21 total and its three subscales and negatively with work experience. CBI scores were positively associated with both the AIS scores and the DASS-21 total and its subscales. The Anxiety subscale of the DASS-21 correlated negatively with age and work experience and moreover the Depression subscale showed a negative correlation with work experience. As expected, the three DASS-21 subscales positively correlated with each other (Pearson Correlations p < 0.01, Table 2).
We ensured that the prerequisites for the regression analysis were satisfied by checking in advance the necessary assumptions. Independence of residuals was tested using the Durbin-Watson test, with a value of 1.843 (Table 3), supporting the absence of autocorrelation. The VIF values of less than 4 indicated a lack of multicollinearity (Table 3). Normality was verified by visually observing the predicted probability plots. Homoscedasticity was explored through visual review of the scatter plot of standardized and predicted residual values. Linearity was confirmed by visually inspecting scatter plots of variable pairs.
We conducted a multiple regression analysis using the Stepwise method to explore which factors best explain the scores of the Athens Insomnia Scale (AIS). In the multiple regression analysis, AIS was set as the dependent variable, while age, gender, years of work experience, the Copenhagen Burnout Inventory (CBI), and the subscales of the Depression Anxiety Stress Scale (DASS-21) were set as independent variables. The analysis showed that the Depression subscale of the DASS-21 explained 40.6% of the variance in AIS, while an additional 7.6% was explained by CBI and another 1.3% rate was explained by the Stress subscale of the DASS-21 (Table 3). The other variables did not contribute significantly to the AIS variance.
Next, we explored the hypothesis that depression and burnout might act as mediators in the relationship between stress and insomnia. In this analysis, the Stress subscale of the DASS-21 was set as the predictor variable, the Depression subscale of the DASS-21 and CBI as the mediator variables and AIS as the outcome variable. Covariates included work experience and age. Hayes' SPSS Process Macro Model 6 was employed to investigate the chain mediating effect of depression and burnout in the relationship between stress and insomnia. The analysis was based on 5000 bootstrap samples. Unstandardized coefficients for the variables with standard errors are illustrated in Figure 1.
The chain mediation analysis revealed that depression and burnout serially mediate the relationship between stress and insomnia. In this context, the covariates, age, and work experience exhibited statistically significant relationships (Figure 1 & Table 4). The total indirect effect of depression and burnout on insomnia was found to be statistically significant [b=0.1932, 95% C.I. (0.1311, 0.1655)]. Furthermore, the direct effect of stress on insomnia in presence of the mediators was proved significant as well (b = 0.1073, p < 0.01). Therefore, there is partial serial mediation of depression and burnout on the relationship between stress and insomnia. This model explains 64.3% of the variance in the AIS outcome variable. In particular, the following three pathways yielded indirect effects that contributed to the total mediating effect: (a) Stress → Depression → AIS, which represents 36.3% of the total effect; (b) Stress → CBI → AIS, rendering 18.8% of the total effect; and (c) Stress → Depression → CBI→ AIS, constituting 9.18% of the total effect.
Lastly, we investigated the process by which anxiety may moderate the relationship between stress and depression. Specifically, we aimed to investigate if anxiety acting as a moderator is altering the potency of the indirect effect of the above chain mediation, by means of testing the moderating role of anxiety in the pathways of Stress → Depression → AIS and Stress → Depression → CBI → AIS. To perform this moderation analysis, we utilized the PROCESS method, model 83 (Figure 2).
In both pathways the index of moderated mediation was significant: b = 0.0009, 95% percentile CI [0.0001, 0.0019] and b = 0.0002, 95% percentile CI [0.0000, 0.0005], providing support for a moderated mediation. 0.37% change in depression can be accounted to the interaction term. The results revealed a significantly positive moderating role of anxiety on the linkage between stress and depression (b = 0.066, t = 2.3841, p = 0.0176), Table 5. This shows that at higher levels of anxiety, the impact of stress on depression is reinforced.
Furthermore, to demonstrate how anxiety moderated the association between stress and depression, a simple slope test was performed. High and low anxiety levels (plus or minus a standard deviation) were grouped to generate the simple effect analysis diagram (Fig. 3). The findings indicated that stress has a significant impact on depression in both high and low anxiety levels. Nevertheless, compared to nurses with a low level of anxiety (simple slope = 0.4366, t = 9.4585, p < 0.001), stress has a stronger predictive effect on depression in nurses with a high level of anxiety (simple slope = 0.5398, t = 9.6773, p < 0.001). Hence, the impact of stress on depression is much stronger at high anxiety levels.
4. Discussion
Results from this study evidenced a high prevalence of stress, anxiety, depression, burnout and insomnia among Greek hospital nurses, one year after the end of the pandemic. According to a meta-analysis of studies published up until March 2021, due to the pandemic, 40% of health workers experienced acute stress, 42% anxiety symptoms, 33% depressive symptoms, 37% burnout and 42% insomnia [84]. A review of studies published until 2021, on mental health outcomes among nurses working in emergency hospital settings reported a rate of 29.55% for moderate to severe symptoms of anxiety, 38.79% for depression and 40.66% for insomnia [86]. Meanwhile in Greece, in a study conducted from mid-November to mid-December 2021, 39.7% among hospital nurses exhibited depressive symptoms, 60.1% scored above the cut-off on state anxiety and 46.8% on trait anxiety [55]. Regarding burnout levels, a study performed in February 2021 indicated that 42.9% of nurses had scores suggestive of burnout [28]. Also, a study conducted in May 2020 among Greek hospital nurses reported a 49.7% prevalence of insomnia and 50.3% of stress [16], whereas in a study conducted in approximately two years after the onset of the pandemic [17] and another study conducted two months after the pandemic ended, 61.4% among Greek hospital nurses presented with symptoms of insomnia [86]. Results from studies performed in other countries among healthcare workers after the pandemic are inconclusive, either reporting alarming findings comparable to those during the pandemic [64] or presenting overall improvements in mental health and sleep problems [60]. In Greece, the psychological implications and sleep disturbances seem to persist for a longer period, even after the pandemic [57]. This difference may be attributed to the reduced perceived organizational support and the limited resources of nursing personnel in the Greek National Health System [87,88], who work hard under challenging conditions but are underpaid compared to their colleagues from the other OECD countries [89,90].
Among demographic and work-related factors influencing psychological and sleep symptoms age, gender and work experience were recorded in this study. In agreement with most other studies [91,92,93,94,95] that clearly show that female nurses are the most vulnerable subgroup among healthcare workers especially regarding the mental health impacts, female nurses in this study reported higher levels of stress and burnout and exhibited higher scores in the DASS-21 compared to their male counterparts. The female gender predominates in the nursing sector, unlike in other working environments and literature suggests that women are more likely to be at risk for psychological distress [96,97,98]. Moreover, hospital nurses are particularly prone to experiencing higher levels of stress and burnout than the other non-hospital nurses [99,100]. Also, in this study age and work experience proved to be among influencing factors for presenting psychological issues and sleep problems. Specifically age correlated negatively with anxiety and work experience was negatively associated with anxiety, depression and insomnia. Most existing literature justifies these results [101,102,103,104,105], but certain studies argued that the more experienced nurses were also the more anxious, possibly because they were assigned to more challenging work tasks [106].
This study focused on the effects of stress on insomnia and further investigated the separate and the chain mediating role of depression and burnout and verified the moderating role of anxiety in nurses working in Greek hospitals one year after the end of the pandemic. The results elucidate the underlying mechanism through which stress affects insomnia and identify significant factors influencing insomnia, thus providing guidance for targeted interventions for nurses. This section includes the major findings which are discussed in conjunction with other relevant literature.
4.1. The Influence of Stress on Insomnia
The results from both the regression and the mediation analysis indicated that stress positively predicted insomnia, thus supporting the first hypothesis. From a neurobiological perspective sleep/circadian rhythmicity and the stress response system engage the same neural networks [107]. Stress dysregulation involving the sympathetic-adrenomedullary and the hypothalamic-pituitary-adrenocortical systems may lead to insomnia. Literature suggests that stressful experience is the most common precipitating factor of insomnia [108] and work is one of the most common sources of environmental stress [109]. Occupational stress and insomnia relationship has been investigated by numerous studies and a recent meta-analysis identified the strength of this association [110]. Research indicates that nurses are a vulnerable and high-risk population for occupational stress which is a major risk factor for insomnia in nurses [111]. Notably, hospital nurses compared to community and other non-hospital nurses report higher levels of stress [112]. These stressful experiences are related to the nature of the nursing profession and therefore cannot be easily modified, but the identification of the mediating variables between stress and insomnia could offer valuable insights in order to alleviate the effect of stress on insomnia through the effective manipulation of these mediating variables.
4.2. The Mediating Role of Depression
The results from the regression analysis indicated that depression explained 40.6% of the variance in insomnia and the mediation analysis revealed that stress was positively related to depression that consequently was associated with insomnia, thus supporting the second hypothesis. In this case depression operates as a catalyst between stress and insomnia. Recent research confirms the mediating effect of depression in the association between perceived stress and sleep quality among healthcare workers [113]. The experience of stressful negative life events is implicated in the vulnerability to depression [114]. People are more prone to developing negative cognitive-emotional appraisals when they experience increased levels of stress [115]. Similarly, stressful life events may fuel rumination in some individuals, usually combined with negative emotions [116]. In the long run, failure to regulate these negative cognitions and alleviate these emotions would lead to depression [117,118]. Further, emotional hyperarousal derived from depressive emotions as a result of perceived stress, may disrupt the normal sleep cycle, leading to a spectrum of sleep issues [119,120,121].
4.3. The Mediating Role of Burnout
The mediation analysis revealed that burnout was not only an outcome of stress but also played a mediating role between stress and insomnia, thus verifying the third hypothesis. Furthermore, the regression analysis evidenced that burnout explained 7.6% of the variance in insomnia. Literature points to a bidirectional association between burnout and insomnia, suggesting that either might be a risk factor for the other [122,123]. Specifically, stress, burnout and insomnia are reciprocally related in a vicious cycle [123,124]. Dysregulation involving the sympathetic nervous system and/or the hypothalamic–pituitary–adrenal axis are observed in both burnout and insomnia [124]. A prospective study supported that burnout at baseline not only intensified insomnia symptoms over time for individuals already exhibiting these symptoms at baseline, but it was also related to the emergence of new cases at follow-up [125]. A recent longitudinal population-based cohort study indicated that burnout was the strongest among several risk factors for insomnia [126]. A possible mechanism explaining the way that burnout may cause insomnia implicates emotional exhaustion which contributes to increased sleep reactivity and in turn lead to hyperarousal before sleep and ultimately to sleep problems, like insomnia [127]. Also, a meta-analysis confirmed the relationship between burnout and sleep disorders in nurses and provided information about influencing variables, such as gender, shift work and workplace violence [128].
4.4. The Chain Mediating Role of Depression and Burnout
This study evidenced that depression and burnout play a chain mediating role between stress and insomnia, hence confirming the forth hypothesis. Studies suggest a reciprocal relationship between depression and burnout and some researchers identified burnout as a significant predictor of depressive symptoms [129,130,131,132]. Differently, other researchers supported that depression can increase the possibility of burnout [126,133] and an earlier study indicated that current depressive symptoms predicted burnout and furthermore an underlying susceptibility for depression as inferred from a personal and familial history of depression, increased the risk for burnout [134]. Also, there is a debate among researchers over the possibility that burnout and depression overlap [135,136]. In this sense, both depression and burnout can be caused by stressors in the workplace [137] and employees in occupational environments that are particularly demanding and stressful, such as healthcare settings, are prone to suffering from comorbid depression and burnout [138]. This has led some scholars to reconceptualise burnout as a form of 'occupational depression' [139]. However, a recent meta-analysis revealed that depression and burnout are different and robust constructs with no overlap between them [140]. Thus, despite being regarded as distinct nosological entities, depression and burnout syndrome have been found to be intimately linked in a number of studies [141,142]. Further, associations between sleep quality and depressive and burnout symptoms are well established [143,144]. Results from a longitudinal study confirmed that depressive and burnout symptomatology predicted impaired sleep quality, whereas impaired sleep quality did not predict burnout, but only depressive symptoms. The authors argued that work-related stressors also need to be present to elicit an increase in burnout symptoms [145].
4.5. The Moderating Role of Anxiety
Another important result from this study is that anxiety moderates the relationship between stress and depression, thus confirming the filth hypothesis. This finding suggests that the degree to which stress and depression impact insomnia varies depending on anxiety levels. Stress and anxiety are frequently comorbid and research has identified the underlying neurobiological mechanism implicated in the bidirectional association between chronic stress and anxiety disorder [146,147]. Stressful life events often precede anxiety disorders [148] and the positive association between any kind of anxiety and the severity of insomnia is apparent since shared psychopathological mechanisms, such as emotional overactivity, can be identified [149]. A study exploring the symptom level associations between insomnia, depression, and anxiety identified uncontrollable worrying and trouble relaxing as the most central symptoms [150]. The role of emotion dysregulation in insomnia has long been proposed [151] and the cognitive model of insomnia describes one of the patterns of subjective experiences of emotions characterized by increased negatively valenced pre-sleep cognitive activity [152,153]. Rumination and worry are the two components of intrusive thoughts [154] and while rumination is related to dysphoric mood and primarily focuses on the causes of this mood state, worry is associated with anxious mood and involves catastrophizing about future stressful events [155]. Another prospective study demonstrated that anxiety and depression at baseline predicted insomnia at follow-up [156]. Available evidence indicates a reciprocal relationship between anxiety and depression as to insomnia [157], but the nature of this relationship may differ across specific insomnia symptoms [158,159]. Also, another study supported that insomnia may have separate, possibly causally different, directional relationships with anxiety disorders as opposed to depression [160].
The moderated chain mediation model constructed in this study clarifies the associations among stress, anxiety, depression, burnout and insomnia, aiming to provide practical implications for prevention and intervention purposes. The hypothesized mechanisms of link between the aforementioned factors influencing insomnia should raise the possibility that some of these nurses suffering from insomnia may simultaneously display symptoms of anxiety, depression and burnout, all caused by the harmful effects of stress [126,161]. Thus, nurses who present with insomnia symptoms should also be assessed and treated for these other symptoms and certain risk factors may differentiate nurses who exhibit distinct combinations of these symptoms which unless recognized and addressed they would contribute to the chronicity of the disturbance [162]. Although the treatment of choice for chronic insomnia is cognitive–behavioral therapy [163], distinguishing among different constellations of co-occurring symptoms would lead to more focused treatment plans targeting at diverse behavioral, psychosomatic, and biological patterns [164,165].
The results from this study highlight the needs for primary prevention measures in the working environment, both at organizational and administrative level, in order to support nurses in dealing with the stressful working conditions. Early identification of risk factors such as demanding working environment, quality of the hospital, night shifts, not having a permanent job, working experience, excessive workload and inadequate rewards would enable the implementation of effective workplace interventions to prevent or reduce mental health problems among nurses. Targeted interventions such as stress management programs, mindfulness-based interventions, training in positive coping strategies to combat stress, frustration, and emotion management through self-compassion techniques and self-care programs can effectively reduce anxiety, depression, burnout and insomnia and may also prove beneficial in managing stress and prevent the occurrence and/or worsening of the above stress-related disorders among nurses [166,167,168,169].
Certain limitations should be recognized. First, the cross-sectional method of this study precluded inferences about causal associations among the variables, which could only be established with longitudinal studies. Secondly, the employed convenience sampling methodology could hinder the generalizability of the results. Third, data relied on nurses’ self-reports measurements conferring a potential self-report bias. Fourth, important limitation is the lack of information about other work-related variables namely, nurses' work department, work shifts, rotation and staff shortages. Finally, this study focused on specific stress-related risk factors influencing insomnia among nurses, with a limited number of covariates. Future studies may consider including more risk as well as protective factors to improve our understanding about their complex interrelations beyond the pandemic, for prevention and intervention purposes.
5. Conclusions
High prevalence rates of stress, anxiety, depression, burnout and insomnia were observed in hospital nurses one year after the end of the pandemic. More than one in three nurses experienced stress, anxiety and depression, almost half of them displayed signs of burnout and more than half complained about insomnia symptoms. The moderated chain mediation model constructed in this study indicates that stress exerts significant direct and indirect effects on insomnia, mediated by depression and burnout and also that anxiety moderates the relationship between stress and depression. These findings provide insights for designing interventions to reduce the adverse effects of stress and insomnia among nurses, with complementary measures focused on improving potential co-occurring symptoms of anxiety, depression and burnout.
Author Contributions
Conceptualization, A.P., C.S. and A.T.; methodology, A.P. and A.T.; software, D.M., M.I and C.S.; validation, A.P., M.I and C.S.; formal analysis, A.P., I.I. and A.T.; investigation C.S., D.M, N.S and A.T.; resources, A.P. and I.I.; data curation, C.S., S.A, M.I and A.T.; writing—original draft preparation, A.P. and A.T.; writing—review and editing, A.P., N.S. and C.S.; supervision, A.P. and A.T.; project administration, I.I. and A.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Clinical Research Ethics Committee of “Sotiria” General Hospital (Number 20649/16-05-2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, [A.T.], upon reasonable request.
Acknowledgments
We would like to thank all participants in our study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- WHO Statement (31 January 2020). "Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV)". World Health Organization. 31 January 2020. Archived from the original on 15 August 2021. Retrieved 6 February 2020.
- "WHO Director-General's opening remarks at the media briefing on COVID-19 – 11 March 2020". World Health Organization. 20 March 2020. Archived from the original on 15 August 2021. Retrieved 11 March 2020.
- "Statement on the fifteenth meeting of the International Health Regulations (2005) Emergency Committee regarding the coronavirus disease (COVID-19) pandemic". www.who.int. Archived from the original on 5 May 2023. Retrieved 5 May 2023.
- Mofijur M, Fattah IMR, Alam MA, et al. Impact of COVID-19 on the social, economic, environmental and energy domains: Lessons learnt from a global pandemic. Sustain Prod Consum. 2021 Apr;26:343-359. [CrossRef]
- Tselebis, A.; Pachi, A. Primary Mental Health Care in a New Era. Healthcare 2022, 10, 2025. [CrossRef]
- Marzo RR, Ismail Z, Nu Htay MN, et al. Psychological distress during pandemic Covid-19 among adult general population: Result across 13 countries. Clin Epidemiol Glob Health. 2021 Apr-Jun;10:100708. [CrossRef]
- Jaber, M. J., AlBashaireh, A. M., AlShatarat, M. H., et al. (2022). Stress, depression, anxiety, and burnout among healthcare workers during the COVID-19 pandemic: a cross-sectional study in a tertiary centre. The Open Nursing Journal, 16(1). [CrossRef]
- Kunz, M., Strasser, M., & Hasan, A. (2021). Impact of the coronavirus disease 2019 pandemic on healthcare workers: systematic comparison between nurses and medical doctors. Current opinion in psychiatry, 34(4), 413-419.
- Imes CC, Tucker SJ, Trinkoff AM, et al. Wake-up call: Night shifts adversely affect nurse health and retention, patient and public safety, and costs. Nurs Adm Q. 2023 Oct-Dec 01;47(4):E38-E53. [CrossRef]
- Sagherian K, Cho H, Steege LM. The insomnia, fatigue, and psychological well-being of hospital nurses 18 months after the COVID-19 pandemic began: A cross-sectional study. J Clin Nurs. 2024 Jan;33(1):273-287. [CrossRef]
- Janatolmakan, M., Naghipour, A. & Khatony, A. Prevalence and factors associated with poor sleep quality among nurses in COVID-19 wards. Sci Rep 14, 16616 (2024). [CrossRef]
- Norful AA, Haghighi F, Shechter A. Assessing sleep health dimensions in frontline registered nurses during the COVID-19 pandemic: implications for psychological health and wellbeing. Sleep Adv. 2022 Dec 16;4(1):zpac046. [CrossRef]
- Tselebis, A.; Zoumakis, E.; Ilias, I. Dream Recall/Affect and the Hypothalamic–Pituitary–Adrenal Axis. Clocks & Sleep 2021, 3, 403-408. [CrossRef]
- Chung Y, Kim H, Koh DH, et al. Relationship Between Shift Intensity and Insomnia Among Hospital Nurses in Korea: A Cross-sectional Study. J Prev Med Public Health. 2021 Jan;54(1):46-54. [CrossRef]
- Kalmbach DA, Anderson JR, Drake CL. The impact of stress on sleep: Pathogenic sleep reactivity as a vulnerability to insomnia and circadian disorders. J Sleep Res. 2018 Dec;27(6):e12710. [CrossRef]
- Tselebis A, Lekka D, Sikaras C, et al. (2020) Insomnia, Perceived Stress, and Family Support among Nursing Staff during the Pandemic Crisis. Healthcare (Basel, Switzerland) 8(4), 434. [CrossRef]
- Sikaras C, Tsironi M, Zyga S, et al. (2023) Anxiety, insomnia and family support in nurses, two years after the onset of the pandemic crisis. AIMS public health 10(2), 252–267. [CrossRef]
- Peng P, Liang M, Wang Q, et al. Night shifts, insomnia, anxiety, and depression among Chinese nurses during the COVID-19 pandemic remission period: A network approach. Front Public Health. 2022 Dec 5;10:1040298. [CrossRef]
- Bennaroch K and Shochat T (2023) Psychobiological risk factors for insomnia and depressed mood among hospital female nurses working shifts. Front. Sleep 2:1206101. [CrossRef]
- Sagherian K, Steege LM, Cobb SJ, et al. Insomnia, fatigue and psychosocial well-being during COVID-19 pandemic: A cross-sectional survey of hospital nursing staff in the United States. J Clin Nurs. 2023 Aug;32(15-16):5382-5395. [CrossRef]
- Mao X, Lin X, Liu P, et al. (2023) Impact of Insomnia on Burnout Among Chinese Nurses Under the Regular COVID-19 Epidemic Prevention and Control: Parallel Mediating Effects of Anxiety and Depression. Int J Public Health 68:1605688. [CrossRef]
- "Burn-out an "occupational phenomenon": International Classification of Diseases". www.who.int. Retrieved 2023-11-09.
- Quesada-Puga C, Izquierdo-Espin FJ, Membrive-Jiménez MJ, et al. Job satisfaction and burnout syndrome among intensive-care unit nurses: A systematic review and meta-analysis. Intensive Crit Care Nurs. 2024 Jun;82:103660. [CrossRef]
- Friganović A, Selič P, Ilić B, et al. Stress and burnout syndrome and their associations with coping and job satisfaction in critical care nurses: a literature review. Psychiatr Danub. 2019 Mar;31(Suppl 1):21-31.
- Freudenberger, H. J. (1974). Staff burn-out. Journal of social issues, 30(1), 159-165.
- Kousloglou S, Mouzas O, Bonotis K, et al. Insomnia and burnout in Greek Nurses. Hippokratia. 2014 Apr;18(2):150-5. PMID: 25336879; PMCID: PMC4201402.
- Bratis D, Tselebis A, Sikaras C, et al. (2009) Alexithymia and its association with burnout, depression and family support among Greek nursing staff. Human resources for health 7, 72. [CrossRef]
- Sikaras C, Ilias I, Tselebis A, et al. Nursing staff fatigue and burnout during the COVID-19 pandemic in Greece. AIMS Public Health. 2021 Nov 23;9(1):94-105. [CrossRef]
- Membrive-Jiménez MJ, Pradas-Hernández L, Suleiman-Martos N, et al. Burnout in Nursing Managers: A Systematic Review and Meta-Analysis of Related Factors, Levels and Prevalence. Int J Environ Res Public Health. 2020 Jun 4;17(11):3983. [CrossRef]
- Monsalve-Reyes, C.S., San Luis-Costas, C., Gómez-Urquiza, J.L. et al. Burnout syndrome and its prevalence in primary care nursing: a systematic review and meta-analysis. BMC Fam Pract 19, 59 (2018). [CrossRef]
- Pachi A, Sikaras C, Ilias I, et al. (2022) Burnout, Depression and Sense of Coherence in Nurses during the Pandemic Crisis. Healthcare (Basel, Switzerland) 10(1), 134. [CrossRef]
- Stelnicki AM, Jamshidi L, Angehrn A, et al. Associations Between Burnout and Mental Disorder Symptoms Among Nurses in Canada. Can J Nurs Res. 2021 Sep;53(3):254-263. [CrossRef]
- Schonfeld, I. S., & Bianchi, R. (2016). Burnout and depression: two entities or one?. Journal of clinical psychology, 72(1), 22-37.
- Bianchi, R., Boffy, C., Hingray, C., et al. (2013). Comparative symptomatology of burnout and depression. Journal of health psychology, 18(6), 782-787.
- Iacovides A, Fountoulakis KN, Kaprinis S, et al. The relationship between job stress, burnout and clinical depression. J Affect Disord. 2003 Aug;75(3):209-21. [CrossRef]
- Noh EY, Park YH, Chai YJ, et al. Frontline Nurses’ Burnout and its Associated Factors during the COVID-19 Pandemic in South Korea. Appl Nurs Res (2022) 67:151622. [CrossRef]
- Serrão, C.; Duarte, I.; Castro, L.; et al. Burnout and Depression in Portuguese Healthcare Workers during the COVID-19 Pandemic—The Mediating Role of Psychological Resilience. Int. J. Environ. Res. Public Health 2021, 18, 636. [CrossRef]
- Kaschka WP, Korczak D, Broich K. Burnout: a fashionable diagnosis. Dtsch Arztebl Int. 2011 Nov;108(46):781-7. [CrossRef]
- Bakker AB, Schaufeli WB, Demerouti E, et al. Using Equity Theory to Examine the Difference Between Burnout and Depression. Anxiety Stress Coping. 2000;13(3):247–268.
- Hatch DJ, Potter GG, Martus P, et al. Lagged versus concurrent changes between burnout and depression symptoms and unique contributions from job demands and job resources. J Occup Health Psychol. 2019 Dec;24(6):617-628. [CrossRef]
- Mazure, C. M. (1998). Life stressors as risk factors in depression. Clinical Psychology: Science and Practice, 5(3), 291–313. https://doi .org/10.1111/j.1468-2850.1998.tb00151.x.
- Hammen, C. (2005). Stress and depression. Annual Review of Clinical Psychology, 1, 293–319. [CrossRef]
- Maslach, C., & Leiter, M. P. (2016). Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry, 15(2), 103–111. [CrossRef]
- Kamal, A.M.; Ahmed, W.S.E.; Wassif, G.O.M.; et al. Work Related Stress, Anxiety and Depression among School Teachers in general education. Qjm: Int. J. Med. 2021, 114 (Suppl. 1), hcab118.003.
- Wang MF, Shao P, Wu C, et al. The relationship between occupational stressors and insomnia in hospital nurses: The mediating role of psychological capital. Front Psychol. 2023 Feb 14;13:1070809. [CrossRef]
- Hsieh, H.-F.; Liu, Y.; Hsu, H.-T.; et al. Relations between Stress and Depressive Symptoms in Psychiatric Nurses: The Mediating Effects of Sleep Quality and Occupational Burnout. Int. J. Environ. Res. Public Health 2021, 18, 7327. [CrossRef]
- Al Maqbali M, Al Sinani M, Al-Lenjawi B. Prevalence of stress, depression, anxiety and sleep disturbance among nurses during the COVID-19 pandemic: A systematic review and meta-analysis. J Psychosom Res. 2021 Feb;141:110343. [CrossRef]
- Ge MW, Hu FH, Jia YJ, et al. Global prevalence of nursing burnout syndrome and temporal trends for the last 10 years: A meta-analysis of 94 studies covering over 30 countries. J Clin Nurs. 2023 Sep;32(17-18):5836-5854. [CrossRef]
- Tao R, Wang S, Lu Q, et al. (2024) Interconnected mental health symptoms: network analysis of depression, anxiety, stress, and burnout among psychiatric nurses in the context of the COVID-19 pandemic. Front. Psychiatry 15:1485726. [CrossRef]
- Akova, İ., Hasdemir, Ö., & Kiliç, E. (2021). Evaluation of the relationship between burnout, depression, anxiety, and stress levels of primary health-care workers (Center Anatolia). Alexandria Journal of Medicine, 57(1), 52–60. [CrossRef]
- Spányik A, Simon D, Rigó A, et al. Subjective COVID-19-related work factors predict stress, burnout, and depression among healthcare workers during the COVID-19 pandemic but not objective factors. PLoS One. 2022 Aug 12;17(8):e0270156. [CrossRef]
- Liu F, Zhao Y, Chen Y, et al. The mediation effect analysis of nurse's mental health status and burnout under COVID-19 epidemic. Front Public Health. 2023 Oct 17;11:1221501. [CrossRef]
- Gustavsson, K., Jernajczyk, W., & Wichniak, A. (2022). Insomnia Partially Mediates the Relationship of Occupational Stress with Mental Health Among Shift Working Nurses and Midwives in Polish Hospitals. Nature and Science of Sleep, 14, 1989–1999. [CrossRef]
- Song Y, Yang F, Sznajder K, et al. Sleep Quality as a Mediator in the Relationship Between Perceived Stress and Job Burnout Among Chinese Nurses: A Structural Equation Modeling Analysis. Front Psychiatry. 2020 Nov 13;11:566196. [CrossRef]
- Sikaras, C.; Zyga, S.; Tsironi, M.; et al. The Mediating Role of Depression and of State Anxiety on the Relationship between Trait Anxiety and Fatigue in Nurses during the Pandemic Crisis. Healthcare 2023, 11, 367. [CrossRef]
- Huang W, Wen X, Li Y, et al. Association of perceived stress and sleep quality among medical students: the mediating role of anxiety and depression symptoms during COVID-19. Front Psychiatry. 2024 Jan 18;15:1272486. [CrossRef]
- Pachi A, Panagiotou A, Soultanis N, et al. Resilience, Anger, and Insomnia in Nurses after the End of the Pandemic Crisis. Epidemiologia (Basel). 2024 Oct 10;5(4):643-657. [CrossRef]
- Powell MA, Oyesanya TO, Scott SD, et al. Beyond Burnout: Nurses’ Perspectives on Chronic Suffering During and After the COVID-19 Pandemic. Global Qualitative Nursing Research. 2024;11. [CrossRef]
- Grasmann L, Morawa E, Adler W, et al. Depression and anxiety among nurses during the COVID-19 pandemic: Longitudinal results over 2 years from the multicentre VOICE-EgePan study. J Clin Nurs. 2024 Mar 22. [CrossRef]
- Ding W, Wang MZ, Zeng XW, et al. Mental health and insomnia problems in healthcare workers after the COVID-19 pandemic: A multicenter cross-sectional study. World J Psychiatry. 2024 May 19;14(5):704-714. [CrossRef]
- Liu D, Zhou Y, Tao X, et al. Mental health symptoms and associated factors among primary healthcare workers in China during the post-pandemic era. Front Public Health. 2024 May 14;12:1374667. [CrossRef]
- Galanis P, Moisoglou I, Katsiroumpa A, et al. (2023) Increased Job Burnout and Reduced Job Satisfaction for Nurses Compared to Other Healthcare Workers after the COVID-19 Pandemic. Nursing Reports (Pavia, Italy) 13(3), 1090–1100. [CrossRef]
- Xiao J, Liu L, Peng Y, et al. Anxiety, depression, and insomnia among nurses during the full liberalization of COVID-19: a multicenter cross-sectional analysis of the high-income region in China. Front Public Health. 2023;11:1179755.
- Zhou, Y., Gao, W., Li, H. et al. Network analysis of resilience, anxiety and depression in clinical nurses. BMC Psychiatry 24, 719 (2024). [CrossRef]
- Jager, J.; Putnick, D.L.; Bornstein, M.H. More than Just Convenient: The Scientific Merits of Homogeneous Convenience Samples. Monogr. Soc. Res. Child Dev. 2017, 82, 13–30.
- Tziallas D, Goutzias E, Konstantinidou E, et al. (2018) Quantitative and qualitative assessment of nurse staffing indicators across NHS public hospitals in Greece. Hell J Nurs 57:420–449.
- Lovibond, S.H.; Lovibond, P.F. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343.
- Cowles, B., Medvedev, O.N. (2022). Depression, Anxiety and Stress Scales (DASS). In: Medvedev, O.N., Krägeloh, C.U., Siegert, R.J., Singh, N.N. (eds) Handbook of Assessment in Mindfulness Research. Springer, Cham. [CrossRef]
- Pezirkianidis, C., Karakasidou, E., Lakioti, A., et al. (2018). Psychometric Properties of the Depression, Anxiety, Stress Scales-21 (DASS-21) in a Greek Sample. Psychology, 9, 2933-2950. [CrossRef]
- Kristensen TS, Borritz M, Villadsen E, et al. (2005) The Copenhagen Burnout Inventory: a new tool for the assessment of burnout. Work Stress 19(3), 192–207. [CrossRef]
- Papaefstathiou E, Tsounis A, Malliarou M, et al. (2019) Translation and validation of the Copenhagen Burnout Inventory amongst Greek doctors. Health psychology research 7(1), 7678. [CrossRef]
- Henriksen L, Lukasse M (2016) Burnout among Norwegian midwives and the contribution of personal and work-related factors: A cross-sectional study. Sexual & reproductive healthcare: official journal of the Swedish Association of Midwives 9, 42–47. [CrossRef]
- Madsen IE, Lange T, Borritz M, et al. (2015) Burnout as a risk factor for antidepressant treatment - a repeated measures time-to-event analysis of 2936 Danish human service workers. Journal of psychiatric research 65, 47–52. [CrossRef]
- Hovland IS, Skogstad L, Diep LM, et al. (2024) Burnout among intensive care nurses, physicians and leaders during the COVID-19 pandemic: A national longitudinal study. Acta anaesthesiologica Scandinavica 10.1111/aas.14504. Advance online publication. [CrossRef]
- Benson S, Sammour T, Neuhaus SJ, et al. (2009) Burnout in Australasian Younger Fellows. ANZ journal of surgery 79(9), 590–597. [CrossRef]
- Chou LP, Li CY, Hu SC (2014) Job stress and burnout in hospital employees: comparisons of different medical professions in a regional hospital in Taiwan. BMJ open 4(2), e004185. [CrossRef]
- Kwan KYH, Chan LWY, Cheng PW, et al. Burnout and well-being in young doctors in Hong Kong: a territory-wide cross-sectional survey. Hong Kong Med J. 2021 Oct;27(5):330-337. [CrossRef]
- Creedy DK, Sidebotham M, Gamble J, et al. (2017) Prevalence of burnout, depression, anxiety and stress in Australian midwives: a cross-sectional survey. BMC pregnancy and childbirth 17(1), 13. [CrossRef]
- Soldatos CR, Dikeos DG, Paparrigopoulos TJ (2003) The diagnostic validity of the Athens Insomnia Scale. Journal of psychosomatic research 55(3), 263–267. [CrossRef]
- Soldatos CR, Dikeos DG, Paparrigopoulos TJ (2000). Athens Insomnia Scale: validation of an instrument based on ICD-10 criteria. Journal of psychosomatic research 48(6), 555–560. [CrossRef]
- Podsakoff PM, MacKenzie SB, Lee J-Y, et al. Common method biases in behavioral research: A critical review of the literature and recom mended remedies. J Appl Psychol. 2003;88:879–903.
- Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. New York: The Guilford Press; 2013.
- Henry, J. D., & Crawford, J. R. (2005). The short-form version of the Depression Anxiety Stress Scales (DASS-21): construct validity and normative data in a large non-clinical sample. The British Journal of Clinical Psychology, 44(2), 227–239. [CrossRef]
- Aymerich C, Pedruzo B, Pérez JL, et al (2022). COVID-19 pandemic effects on health worker’s mental health: Systematic review and meta-analysis. European Psychiatry, 65(1), e10, 1–8 . [CrossRef]
- García-Vivar C, Rodríguez-Matesanz I, San Martín-Rodríguez Let al. Analysis of mental health effects among nurses working during the COVID-19 pandemic: A systematic review. J Psychiatr Ment Health Nurs. 2023 Jun;30(3):326-340. [CrossRef]
- Pachi A, Tselebis A, Sikaras C, et al. (2023) Nightmare distress, insomnia and resilience of nursing staff in the post-pandemic era. AIMS public health 11(1), 36–57. [CrossRef]
- Moisoglou I, Katsiroumpa A, Malliarou M, et al. (2024) Social Support and Resilience Are Protective Factors against COVID-19 Pandemic Burnout and Job Burnout among Nurses in the Post-COVID-19 Era. Healthcare (Basel, Switzerland) 12(7), 710. [CrossRef]
- Abdulmohdi N (2024) The relationships between nurses' resilience, burnout, perceived organisational support and social support during the second wave of the COVID-19 pandemic: A quantitative cross-sectional survey. Nursing open 11(1), e2036. [CrossRef]
- Health at a Glance: Europe 2020 STATE OF HEALTH IN THE EU CYCLE. Available online: https://ec.europa.eu/health/system/files/2020-12/2020_healthatglance_rep_en_0.pdf (accessed on 19 August 2024).
- Health at a Glance 2023: OECD Indicators. Available online: https://www.oecd.org/en/publications/health-at-a-glance-2023_7a7afb35-en.html (accessed on 19 August 2024).
- Zhang WR, Wang K, Yin L, et al. Mental Health and Psychosocial Problems of Medical Health Workers during the COVID-19 Epidemic in China. Psychother Psychosom. 2020;89(4):242-250. [CrossRef]
- Mo, Y., Deng, L., Zhang, L. et al. (2020). Work stress among Chinese nurses to support Wuhan in fighting against COVID-19 epidemic. Journal of Nursing Management, 28 (5), 1002–1009.
- El Ghaziri, M., Dugan, A. G., Zhang, Y., et al. (2019). Sex and gender role differences in occupational exposures and work outcomes among registered nurses in correctional settings. Annals of Work Exposures and Health, 63 (5), 568–582.
- Woo, T., Ho, R., Tang, A. et al. (2020). Global prevalence of burnout symptoms among nurses: A systematic review and meta-analysis. Journal of Psychiatric Research, 123, 9–20.
- Hur G, Cinar N, Suzan OK. Impact of COVID-19 pandemic on nurses' burnout and related factors: A rapid systematic review. Arch Psychiatr Nurs. 2022 Dec; 41:248-263;. [CrossRef]
- Alyami, H.; Krägeloh, C.U.; Medvedev, O.N.; et al. Investigating Predictors of Psychological Distress for Healthcare Workers in a Major Saudi COVID-19 Center. Int. J. Environ. Res. Public Health 2022, 19, 4459. [CrossRef]
- Chueh K-H, Chen K-R, Lin Y-H. Psychological Distress and Sleep Disturbance Among Female Nurses: Anxiety or Depression? Journal of Transcultural Nursing. 2021;32(1):14-20. [CrossRef]
- Simães, C., Rui Gomes, A. (2019). Psychological Distress on Nurses: The Role of Personal and Professional Characteristics. In: Arezes, P., et al. Occupational and Environmental Safety and Health. Studies in Systems, Decision and Control, vol 202. Springer, Cham. [CrossRef]
- Dor A, Mashiach Eizenberg M, Halperin O. Hospital nurses in comparison to community nurses: motivation, empathy, and the mediating role of burnout. Can J Nurs Res. 2019;51(2):72–83. [CrossRef]
- Muhamad Robat R, Mohd Fauzi MF, Mat Saruan NA, et al. Why so stressed? A comparative study on stressors and stress between hospital and non-hospital nurses. BMC Nurs. 2021;20(1):2. [CrossRef]
- Seo EH, Lee JH, MacDougall A, et al. Anxiety Symptoms and Associated Psychological and Job-Related Factors Among Hospital Nurses. Psychiatry Investig. 2024 Jan;21(1):100-108. [CrossRef]
- Tokac U , Razon S. Nursing professionals' mental well- being and workplace impairment during the COVID- 19 crisis: A Network analysis . J Nurs Manag. 2021; 29:1653 –1659 . [CrossRef]
- Roberts NJ, McAloney-Kocaman K, Lippiett K, et al. Levels of resilience, anxiety and depression in nurses working in respiratory clinical areas during the COVID pandemic. Respir Med. (2021) 176:106219. [CrossRef]
- Jiang H, Huang N, Jiang X, et al. Factors related to job burnout among older nurses in Guizhou province, China. PeerJ. (2021) 9:e12333. [CrossRef]
- Mattila E, Kaunonen M, Helminen M, et al. Finnish nurses’ anxiety levels in the early stages of the COVID-19 pandemic and 18 months later: A cross-sectional survey. Nordic Journal of Nursing Research. 2024;44. [CrossRef]
- Middleton R, Loveday C, Hobbs C, et al. The COVID-19 pandemic - A focus on nurse managers' mental health, coping behaviours and organisational commitment. Collegian. 2021 Dec;28(6):703-708. [CrossRef]
- Buckley T, Schatzberg A. On the interactions of the Hypothalamic-Pituitary-Adrenal (HPA) axis and sleep: normal HPA axis activity and circadian rhythm, exemplary sleep disorders. J Clin Endocrinol Metab. 2005;90(5):3106–3114. [CrossRef]
- Drake CL, Roth T. Predisposition in the evolution of insomnia: evidence, potential mechanisms, and future directions. Sleep Med Clin. 2006;1(3):333–349.
- Lukan J, Bolliger L, Pauwels NS, et al. Work environment risk factors causing day-to-day stress in occupational settings: a systematic review. BMC Public Health. 2022 Feb 5;22(1):240. [CrossRef]
- Yang B, Wang Y, Cui F, et al. Association between insomnia and job stress: a meta-analysis. Sleep Breath. 2018;22(4):1221–1231. [CrossRef]
- Cao Q, Wu H, Tang X, et al. Effect of occupational stress and resilience on insomnia among nurses during COVID- 19 in China: a structural equation modelling analysis. BMJ Open 2024;14:e080058. [CrossRef]
- Hjörleifsdóttir E, Sigurðardóttir Þ, Óskarsson GK, et al. Stress, burnout and coping among nurses working on acute medical wards and in the community: A quantitative study. Scand J Caring Sci. 2024 Sep;38(3):636-647. [CrossRef]
- Luo Y, Fei S, Gong B, et al. Understanding the Mediating Role of Anxiety and Depression on the Relationship Between Perceived Stress and Sleep Quality Among Health Care Workers in the COVID-19 Response. Nat Sci Sleep. 2021 Oct 5;13:1747-1758. [CrossRef]
- Łosiak W, Blaut A, Kłosowska J, et al. Stressful Life Events, Cognitive Biases, and Symptoms of Depression in Young Adults. Front Psychol. 2019 Sep 20;10:2165. [CrossRef]
- Palamarchuk IS, Vaillancourt T. Mental Resilience and Coping With Stress: A Comprehensive, Multi-level Model of Cognitive Processing, Decision Making, and Behavior. Front Behav Neurosci. 2021 Aug 6;15:719674. [CrossRef]
- Espie CA. Insomnia: conceptual issues in the development, persistence and treatment of sleep disorders in adults. Annu Rev Psychol 2002;53:215–43.
- Yalvaç EBK, Gaynor K. Emotional dysregulation in adults: The influence of rumination and negative secondary appraisals of emotion. J Affect Disord. 2021 Mar 1;282:656-661. [CrossRef]
- Chahar Mahali, S., Beshai, S., Feeney, J.R. et al. Associations of negative cognitions, emotional regulation, and depression symptoms across four continents: International support for the cognitive model of depression. BMC Psychiatry 20, 18 (2020). [CrossRef]
- Fernández-Mendoza J, Vela-Bueno A, Vgontzas AN, et al. Cognitive-emotional hyperarousal as a premorbid characteristic of individuals vulnerable to insomnia. Psychosom Med. 2010 May;72(4):397-403. [CrossRef]
- Palagini L, Moretto U, Dell'Osso L, et al. Sleep-related cognitive processes, arousal, and emotion dysregulation in insomnia disorder: the role of insomnia-specific rumination. Sleep Med. 2017 Feb;30:97-104. [CrossRef]
- Xie M, Huang Y, Cai W, et al. Neurobiological Underpinnings of Hyperarousal in Depression: A Comprehensive Review. Brain Sci. 2024 Jan 4;14(1):50. [CrossRef]
- Sikaras, C.; Pachi*, A.; Alikanioti, S.; et al. Occupational Burnout and Insomnia in Relation to Psychological Resilience Among Nurses in Greece in the Post-Pandemic Era. Preprints 2024, 2024120458. [CrossRef]
- Kwee, C., Dos Santos, L. The Relationships Between Sleep Disorders, Burnout, Stress and Coping Strategies of Health Professionals During the COVID-19 Pandemic: a Literature Review. Curr Sleep Medicine Rep 9, 274–280 (2023). [CrossRef]
- Toker, S., & Melamed, S. (2017). Stress, recovery, sleep, and burnout. In C. L. Cooper & J. C. Quick (Eds.), The handbook of stress and health: A guide to research and practice (pp. 168–185). Wiley Blackwell. [CrossRef]
- Armon G, Shirom A, Shapira I, et al. On the nature of burnout-insomnia relationships: a prospective study of employed adults. J Psychosom Res. 2008 Jul;65(1):5-12. [CrossRef]
- Höglund P, Hakelind C, Nordin M, et al. Risk factors for insomnia and burnout: A longitudinal population-based cohort study. Stress Health. 2023 Oct;39(4):798-812. [CrossRef]
- Sørengaard TA, Saksvik-Lehouillier I. Associations between burnout symptoms and sleep among workers during the COVID-19 pandemic. Sleep Med. 2022 Feb;90:199-203. [CrossRef]
- Membrive-Jiménez MJ, Gómez-Urquiza JL, Suleiman-Martos N, et al. Relation between Burnout and Sleep Problems in Nurses: A Systematic Review with Meta-Analysis. Healthcare (Basel). 2022 May 21;10(5):954. [CrossRef]
- Zhang Y, Wu C, Ma J, et al. Relationship between depression and burnout among nurses in Intensive Care units at the late stage of COVID-19: a network analysis. BMC Nurs. 2024 Apr 1;23(1):224. [CrossRef]
- Chen C, Meier ST. Burnout and depression in nurses: A systematic review and meta-analysis. Int J Nurs Stud. 2021 Dec;124:104099. Epub 2021 Oct 1. Erratum in: Int J Nurs Stud. 2022 Mar;127:104180. doi:10.1016/j.ijnurstu.2022.104180. [CrossRef]
- Mbanga C, Makebe H, Tim D, et al. Burnout as a predictor of depression: a cross-sectional study of the sociodemographic and clinical predictors of depression amongst nurses in Cameroon. BMC Nurs. 2019 Nov 1;18:50. [CrossRef]
- Hakanen JJ, Schaufeli WB. Do burnout and work engagement predict depressive symptoms and life satisfaction? A three-wave seven-year prospective study. J Affect Disord. 2012 Dec 10;141(2-3):415-24. Epub 2012 Mar 24. [CrossRef]
- Papathanasiou IV. Work-related Mental Consequences: Implications of Burnout on Mental Health Status Among Health Care Providers. Acta Inform Med. 2015 Feb;23(1):22-8. [CrossRef]
- Nyklícek I, Pop VJ. Past and familial depression predict current symptoms of professional burnout. J Affect Disord. 2005 Sep;88(1):63-8. [CrossRef]
- Bianchi, R.; Schonfeld, I.S.; Laurent, E. Burnout–depression overlap: A review. Clin. Psychol. Rev. 2015, 36, 28–41.
- Verkuilen J, Bianchi R, Schonfeld IS, et al. Burnout-Depression Overlap: Exploratory Structural Equation Modeling Bifactor Analysis and Network Analysis. Assessment. 2021 Sep;28(6):1583-1600. [CrossRef]
- Bianchi, R., Brisson, R., 2019. Burnout and depression: causal attributions and construct overlap. J. Health Psychol. 24 (11), 1574–1580. [CrossRef]
- Wurm W, Vogel K, Holl A, et al. Depression-Burnout Overlap in Physicians. PLoS One. 2016 Mar 1;11(3):e0149913. [CrossRef]
- Schonfeld IS, Bianchi R. From Burnout to Occupational Depression: Recent Developments in Research on Job-Related Distress and Occupational Health. Front Public Health. 2021 Dec 10;9:796401. [CrossRef]
- Koutsimani, P.; Montgomery, A.; Georganta, K. The Relationship Between Burnout, Depression, and Anxiety: A Systematic Review and Meta-Analysis. Front. Psychol. 2019, 10, 284.
- Bianchi, R., Schonfeld, I.S., Laurent, E. (2018). Burnout Syndrome and Depression. In: Kim, YK. (eds) Understanding Depression. Springer, Singapore. [CrossRef]
- Zisook, S., Doshi, A.P., Fergerson, B.D., et al. (2023). Differentiating Burnout from Depression. In: Davidson, J.E., Richardson, M. (eds) Workplace Wellness: From Resiliency to Suicide Prevention and Grief Management. Springer, Cham. [CrossRef]
- Rothe N, Schulze J, Kirschbaum C, et al. Sleep disturbances in major depressive and burnout syndrome: A longitudinal analysis. Psychiatry Res. 2020 Feb 18;286:112868. [CrossRef]
- Yupanqui-Lorenzo, D.E., Caycho-Rodríguez, T., Baños-Chaparro, J. et al. Mapping of the network connection between sleep quality symptoms, depression, generalized anxiety, and burnout in the general population of Peru and El Salvador. Psicol. Refl. Crít. 37, 27 (2024). [CrossRef]
- Rothe N, Schulze J, Kirschbaum C, et al. Sleep disturbances in major depressive and burnout syndrome: A longitudinal analysis. Psychiatry Res. 2020 Feb 18;286:112868. [CrossRef]
- Herbison CE, Allen K, Robinson M, et al. The impact of life stress on adult depression and anxiety is dependent on gender and timing of exposure. Dev Psychopathol. 2017;29 (4):1443–1454. [CrossRef]
- Lowery-Gionta EG, Crowley NA, Bukalo O, et al. Chronic stress dysregulates amygdalar output to the prefrontal cortex. Neuropharmacology. 2018;139:68–75. [CrossRef]
- Li S, Li L, Zhu X, et al. Comparison of characteristics of anxiety sensitivity across career stages and its relationship with nursing stress among female nurses in Hunan, China. BMJ Open 2016;6: e010829. [CrossRef]
- Baglioni C, Spiegelhalder K, Lombardo C, et al. Sleep and emotions: a focus on insomnia. Sleep Med Rev. 2010 Aug;14(4):227-38. [CrossRef]
- Bard HA, O'Driscoll C, Miller CB, et al. Insomnia, depression, and anxiety symptoms interact and individually impact functioning: A network and relative importance analysis in the context of insomnia. Sleep Med. 2023 Jan;101:505-514. [CrossRef]
- Kirwan M, Pickett SM, Jarrett NL. Emotion regulation as a moderator between anxiety symptoms and insomnia symptom severity. Psychiatry Res. 2017 Aug;254:40-47. [CrossRef]
- Bélanger L, Morin CM, Gendron L, et al. Presleep cognitive activity and thought control strategies in insomnia. J Cogn Psychother 2005;19:19–28.
- Van Egeren L, Hayness SN, Franzen M, et al. Presleep cognitions and attributions in sleep onset insomnia. J Behav Med 1983;6(2):217–32.
- Carney CE, Edinger JD, Meyer B, et al. Symptom-focused rumination and sleep disturbance. Behav Sleep Med. 2006;4(4):228-41. [CrossRef]
- Watts FN, Coyle K, East MP. The contribution of worry to insomnia. Brit J Clin Psychol 1994;33:211–20.
- Jansson-Fröjmark M, Lindblom K. A bidirectional relationship between anxiety and depression, and insomnia? A prospective study in the general population. J Psychosom Res. 2008 Apr;64(4):443-9. [CrossRef]
- Alvaro PK, Roberts RM, Harris JK. A Systematic Review Assessing Bidirectionality between Sleep Disturbances, Anxiety, and Depression. Sleep. 2013 Jul 1;36(7):1059-1068. [CrossRef]
- Hartz AJ, Daly JM, Kohatsu ND, et al. Risk factors for insomnia in a rural population. Ann Epidemiol. 2007 Dec;17(12):940-7. Epub 2007 Oct 15. [CrossRef]
- Ohayon MM. Prevalence and correlates of nonrestorative sleep complaints. Arch Intern Med. 2005 Jan 10;165(1):35-41. [CrossRef] [PubMed]
- Johnson EO, Roth T, Breslau N. The association of insomnia with anxiety disorders and depression: exploration of the direction of risk. J Psychiatr Res. 2006 Dec;40(8):700-8. [CrossRef]
- Dolsen EA, Asarnow LD, Harvey AG. Insomnia as a transdiagnostic process in psychiatric disorders. Curr Psychiatry Rep. 2014 Sep;16(9):471. [CrossRef]
- Scott, B. A., & Judge, T. A. (2006). Insomnia, Emotions, and Job Satisfaction: A Multilevel Study. Journal of Management, 32(5),622–645. [CrossRef]
- Trauer, J. M., Qian, M. Y., Doyle, J. S., et al. (2015). Cognitive behavioral therapy for chronic insomnia: A systematic review and meta- analysis. Annals of Internal Medicine, 163(3), 191–204. [CrossRef]
- Sforza M, Galbiati A, Zucconi M, et al. Depressive and stress symptoms in insomnia patients predict group cognitive-behavioral therapy for insomnia long-term effectiveness: A data-driven analysis. J Affect Disord. 2021 Jun 15;289:117-124. [CrossRef]
- Mirchandaney R, Barete R, Asarnow LD. Moderators of Cognitive Behavioral Treatment for Insomnia on Depression and Anxiety Outcomes. Curr Psychiatry Rep. 2022 Feb;24(2):121-128. [CrossRef]
- Alkhawaldeh JM, Soh KL, Mukhtar F, et al. Stress management training program for stress reduction and coping improvement in public health nurses: A randomized controlled trial. J Adv Nurs. 2020 Nov;76(11):3123-3135. [CrossRef]
- Sulosaari V, Unal E, Cinar FI. The effectiveness of mindfulness-based interventions on the psychological well-being of nurses: A systematic review. Appl Nurs Res. 2022 Apr;64:151565. [CrossRef]
- Conversano C, Ciacchini R, Orrù G, et al. Mindfulness, Compassion, and Self-Compassion Among Health Care Professionals: What's New? A Systematic Review. Front Psychol. 2020 Jul 31;11:1683. [CrossRef]
- Williams SG, Fruh S, Barinas JL, et al. Self-Care in Nurses. J Radiol Nurs. 2022 Mar;41(1):22-27. [CrossRef]
Figure 1.
Chain Mediation effect of Depression and Burnout in the relationship between Stress and Insomnia.
Figure 1.
Chain Mediation effect of Depression and Burnout in the relationship between Stress and Insomnia.
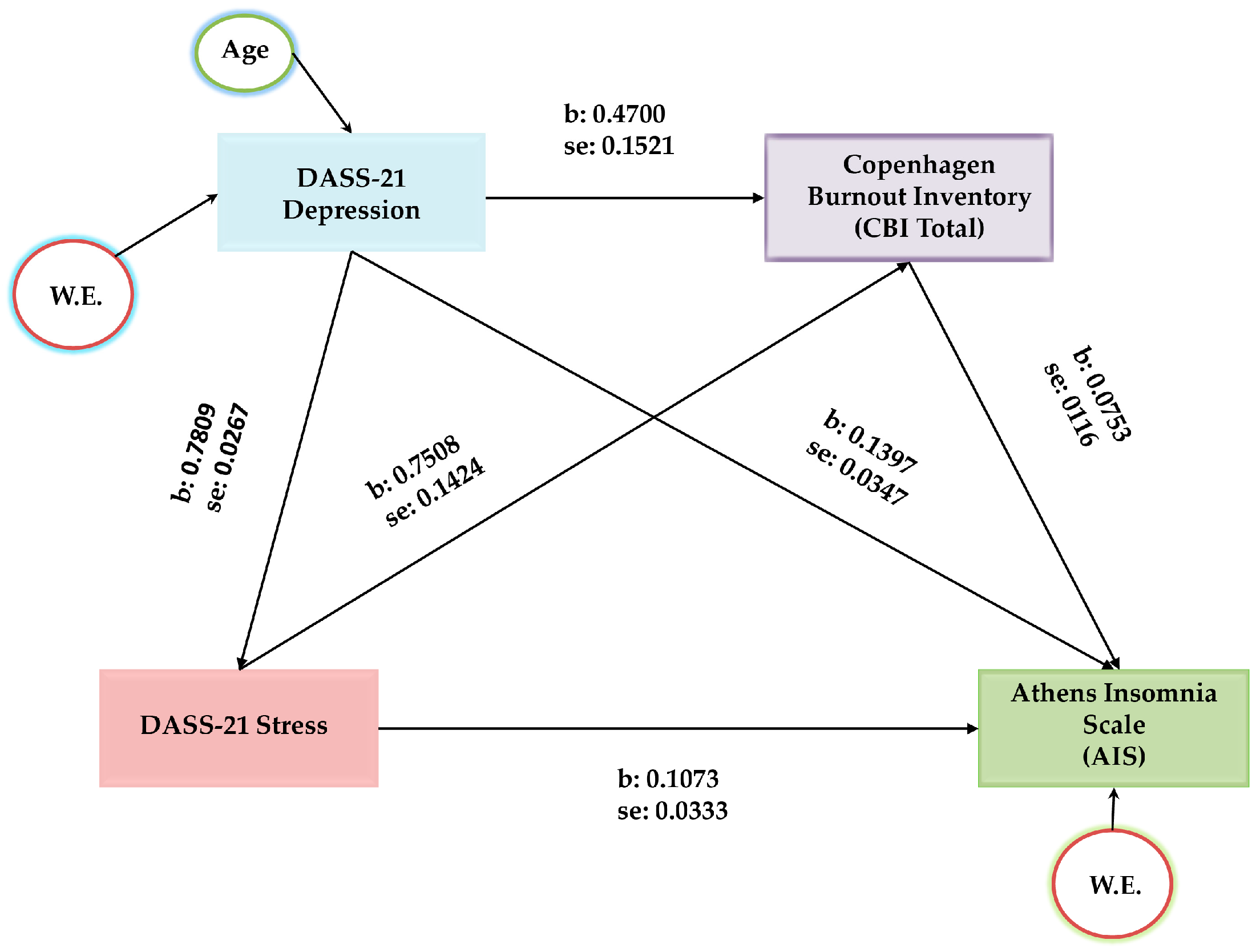
Figure 2.
The moderated chain mediation model in this study: Stress impacts insomnia through a chain mediation effect of depression and burnout and anxiety moderates the relationship between stress and depression in the first and third paths of the chain mediation.
Figure 2.
The moderated chain mediation model in this study: Stress impacts insomnia through a chain mediation effect of depression and burnout and anxiety moderates the relationship between stress and depression in the first and third paths of the chain mediation.
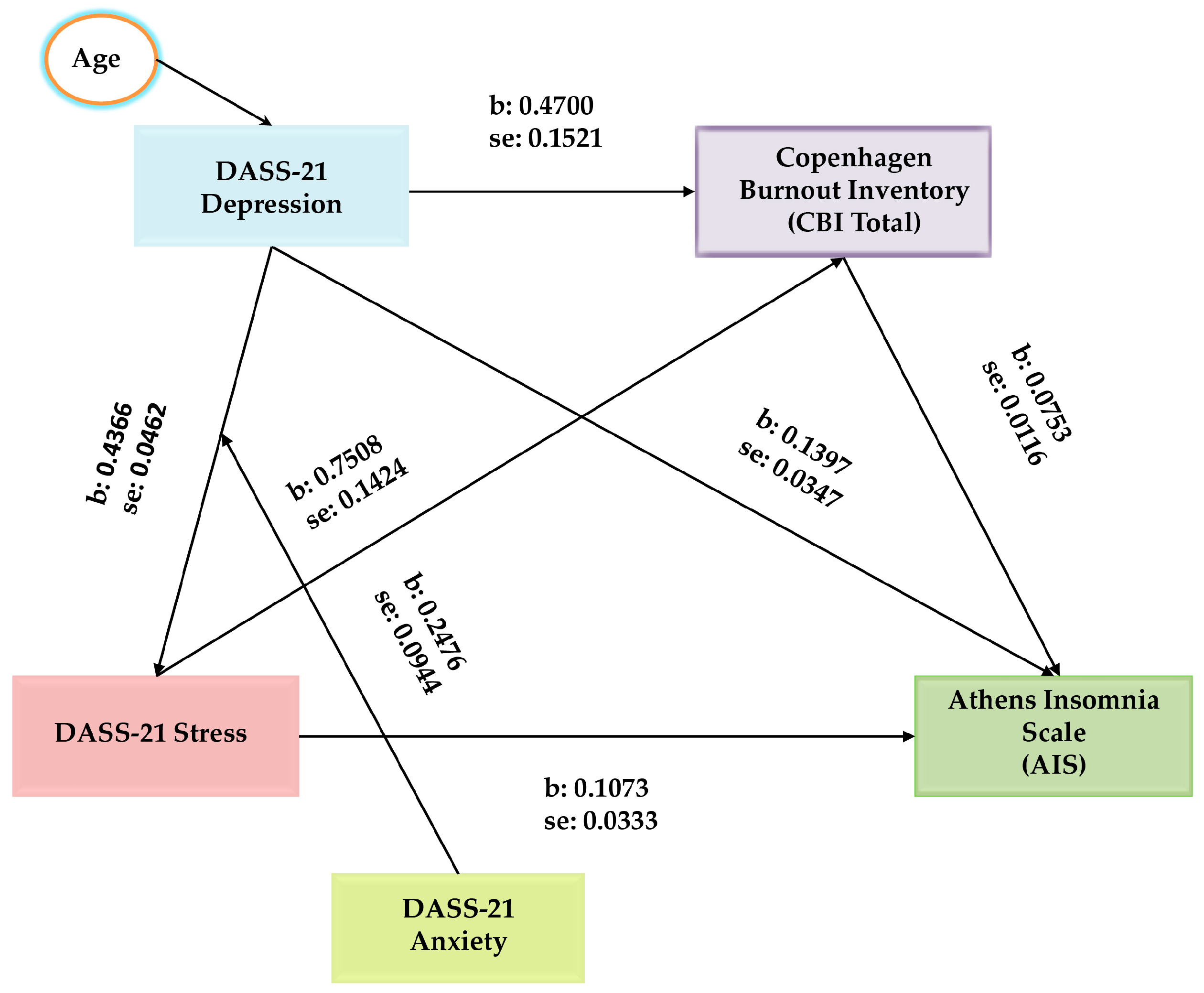
Figure 3.
Simple slopes indicating the interaction of the moderation analysis.
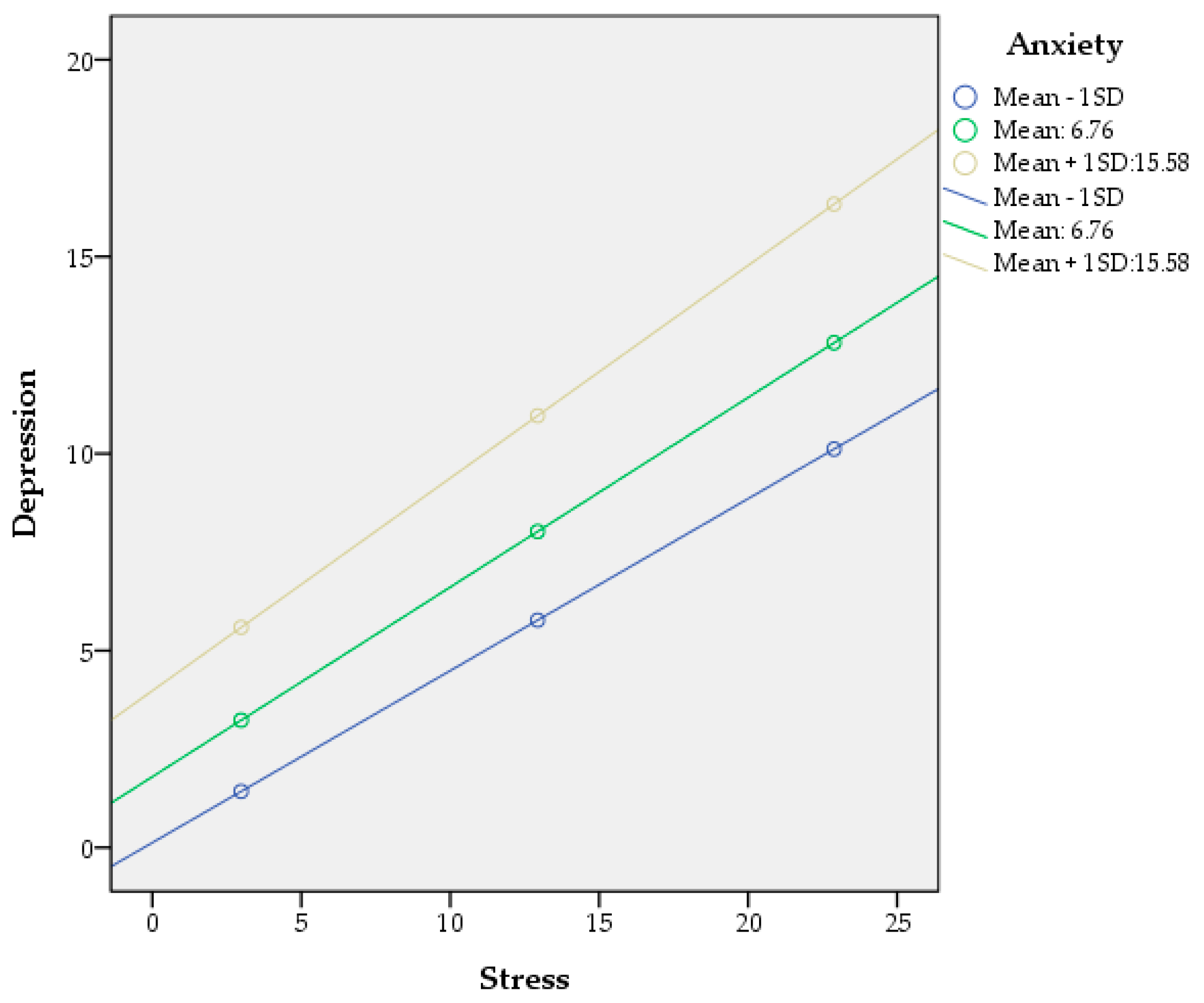

Table 1.
Descriptive statistics of participants.
| Gender | Age | Work experience (in years) |
Athens Insomnia Scale | Copenhagen Burnout Inventory | Depression Anxiety Stress Scale | ||||
| Total | Stress | Anxiety | Depression | ||||||
| Male | Mean | 47.57* | 21.89 | 6.35 | 44.91* | 22.67* | 10.67* | 5.05 | 6.94 |
| N | 74 | 74 | 74 | 74 | 74 | 74 | 74 | 74 | |
| S.D. | 10.85 | 11.92 | 4.23 | 17.93 | 21.88 | 8.2 | 7.52 | 7.99 | |
| Female | Mean | 44.58* | 19.92 | 7.31 | 49.64* | 29.53* | 13.47* | 7.17 | 8.88 |
| N | 306 | 306 | 306 | 306 | 306 | 306 | 306 | 306 | |
| S.D. | 10.41 | 11.47 | 4.92 | 19.03 | 27.42 | 10.26 | 9.06 | 9.67 | |
| Total | Mean | 45.16 | 20.30 | 7.12 | 48.72 | 28.2 | 12.93 | 6.75 | 8.5 |
| N | 380 | 380 | 380 | 380 | 380 | 380 | 380 | 380 | |
| S. D. | 10.55 | 11.57 | 4.80 | 18.89 | 26.54 | 9.95 | 8.81 | 9.39 | |
* t test p<0.05, ** t test p<0.01
Table 2.
Correlations among age, work experience, AIS, CBI and DASS-21.
| Pearson Correlation N: 380 |
Age | Work experience (in years) | AIS | CBI | DASS-21 Total | Stress | Anxiety | |
| Work experience (in years) | r | 0.894** | ||||||
| p | 0.001 | |||||||
| Athens Insomnia Scale (AIS) | r | -0.064 | -0.126* | |||||
| p | 0.214 | 0.014 | ||||||
| Copenhagen Burnout Inventory (CBI) | r | -0.031 | -0.058 | 0.587** | ||||
| p | 0.552 | 0.257 | 0.001 | |||||
| Depression Anxiety Stress Scale (DASS-21 Total) |
r | -0.072 | -0.132* | 0.662** | 0.586** | |||
| p | 0.161 | 0.010 | 0.001 | 0.001 | ||||
| Stress | r | -0.051 | -0.089 | 0.633** | 0.590** | 0.949** | ||
| p | 0.323 | 0.083 | 0.001 | 0.001 | 0.001 | |||
| Anxiety | r | -0.123* | -0.186** | 0.600** | 0.499** | 0.939** | 0.840** | |
| p | 0.016 | 0.000 | 0.001 | 0.001 | 0.001 | 0.001 | ||
| Depression | r | -0.034 | -0.104* | 0.637** | 0.563** | 0.940** | 0.835** | 0.822** |
| p | 0.508 | 0.044 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
* Pearson Correlations p < 0.05, ** Pearson Correlations p < 0.01.
Table 3.
Stepwise multiple regression.
| Dependent Variable: Athens Insomnia Scale |
R Square |
R Square Change |
Beta | t | p | VIF | Durbin-Watson |
| DASS-21 Depression | 0.406 | 0.406 | 0.290 | 4.310 | 0.001* | 3.382 | 1.843 |
| Copenhagen Burnout Inventory (CBI) | 0.483 | 0.076 | 0.296 | 6.438 | 0.001* | 1.573 | |
| DASS-21 Stress | 0.496 | 0.013 | 0.217 | 3.143 | 0.002* | 3.545 |
Notes: Beta = standardized regression coefficient; *Correlations are statistically significant at the p <0.01 level (only statistically significant variables are included).
Table 4.
Chain Mediation Analysis of Depression and Burnout on Stress/ Insomnia relationship.
| Variable | b | SE | t | p | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| LLCI | ULCI | |||||
| Stress -> Depression | 0.7809 | 0.0267 | 29.2765 | 0.0000 | 0.7284 | 0.8333 |
| Stress -> CBI | 0.7508 | 0.1424 | 5.2712 | 0.0000 | 0.4708 | 1.0309 |
| Depression-> CBI | 0.4700 | 0.1521 | 3.0906 | 0.0021 | 0.1710 | 0.7690 |
| Stress-> AIS | 0.1073 | 0.0333 | 3.2235 | 0.0014 | 0.0418 | 0.1727 |
| Depression-> AIS | 0.1397 | 0.0347 | 4.0234 | 0.0001 | 0.0714 | 0.2079 |
| CBI->AIS | 0.0753 | 0.0116 | 6.4684 | 0.0000 | 0.0524 | 0.0982 |
| (1)Stress-> Depression -> AIS | 0.1091 | 0.0290 | 3.7620 | 0.0513 | 0.1655 | |
| (2)Stress-> CBI -> AIS | 0.0565 | 0.0146 | 3.8698 | 0.0306 | 0.0885 | |
| (3)Stress-> Depression -> CBI-> AIS | 0.0276 | 0.0091 | 3.0329 | 0.0109 | 0.0464 | |
| Covariates | ||||||
| Age -> Depression | 0.1540 | 0.0560 | 2.7505 | 0.0062 | 0.0439 | 0.2641 |
| W.E. -> Depression | -0.1498 | 0.0512 | -2.9254 | 0.0036 | -0.2505 | -0.0491 |
| W.E.-> AIS | -0.0853 | 0.0369 | -2.3117 | 0.0213 | -0.1578 | -0.0127 |
| Effects | ||||||
| Direct | 0.1073 | 0.0333 | 3.2235 | 0.0014 | 0.0418 | 0.1727 |
| *Total Indirect | 0.1932 | 0.0309 | 0.1311 | 0.1655 | ||
| Total | 0.3005 | 0.0192 | 15.6336 | 0.0000 | 0.2627 | 0.3383 |
Notes: W.E., work experience (in years); Ind1: (1)Stress-> Depression -> AIS= Stress -> Depression * Depression-> AIS, Ind2: (2)Stress-> CBI -> AIS= Stress-> CBI * CBI -> AIS, Ind3: (3)Stress-> Depression -> CBI-> AIS= Stress-> Depression * Depression -> CBI * CBI-> AIS * Total Indirect = Ind1+ Ind2+ Ind3, Based on 5000 bootstrap samples.
Table 5.
Moderated chain mediation analysis of the effect of DASS-21 Anxiety on the association between the DASS-21 Stress and Athens Insomnia Scale (AIS) through DASS-21 Depression. .
Table 5.
Moderated chain mediation analysis of the effect of DASS-21 Anxiety on the association between the DASS-21 Stress and Athens Insomnia Scale (AIS) through DASS-21 Depression. .
| Direct Relationships | |||||||
|---|---|---|---|---|---|---|---|
| Variable | b | SE | t | p | 95% Confidence Interval | ||
| LLCI | ULCI | ||||||
| Stress → Depression | 0.4366 | 0.0462 | 9.4585 | 0.0000 | 0.3459 | 0.5274 | |
| Anxiety → Depression | 0.2476 | 0.0944 | 2.6214 | 0.0091 | 0.0616 | 0.4333 | |
| Stress*Anxiety → Depression | 0.0066 | 0.0028 | 2.3841 | 0.0176 | 0.0012 | 0.0121 | |
| Stress → CBI | 0.7508 | 0.1424 | 5.2712 | 0.0000 | 0.4708 | 1.0309 | |
| Depression → CBI | 0.4700 | 0.1521 | 3.0906 | 0.0021 | 0.1710 | 0.7690 | |
| Stress → AIS | 0.1073 | 0.0333 | 3.2235 | 0.0014 | 0.0418 | 0.1727 | |
| Depression → AIS | 0.1397 | 0.0347 | 4.0234 | 0.0001 | 0.0714 | 0.2079 | |
| CBI → AIS | 0.0753 | 0.0116 | 6.4684 | 0.0000 | 0.0524 | 0.0982 | |
| Covariates | |||||||
| Age → Depression | 0.1038 | 0.0516 | 2.0101 | 0.0451 | 0.0023 | 0.2053 | |
| Effects | |||||||
| Direct | 0.1073 | 0.0333 | 3.2235 | 0.0014 | 0.0418 | 0.1727 | |
| Moderated Indirect Relationships | |||||||
| Indirect 1: Stress-> Depression -> AIS | |||||||
| Anxiety (mean-1SD) | 0.0610 | 0.0173 | 3.5260 | 0.0288 | 0.0972 | ||
| Anxiety (mean) | 0.0672 | 0.0188 | 3.5744 | 0.0322 | 0.1062 | ||
| Anxiety (mean+1SD) | 0.0754 | 0.0213 | 3.5399 | 0.0359 | 0.1189 | ||
| Index of Moderated Mediation | 0.0009 | 0.0005 | 0.0001 | 0.0019 | |||
| Indirect 2: Stress-> CBI -> AIS | 0.0565 | 0.0147 | 3.8435 | 0.0309 | 0.0886 | ||
| Indirect 3: Stress-> Depression -> CBI -> AIS | |||||||
| Anxiety (mean-1SD) | 0.0155 | 0.0053 | 2.9245 | 0.0059 | 0.0266 | ||
| Anxiety (mean) | 0.0170 | 0.0058 | 2.9310 | 0.0066 | 0.0293 | ||
| Anxiety (mean+1SD) | 0.0191 | 0.0066 | 2.8939 | 0.0073 | 0.0333 | ||
| Index of Moderated Mediation | 0.0002 | 0.0001 | 0.0000 | 0.0005 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



