
Submitted:
26 December 2024
Posted:
27 December 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The impact of SARS-CoV-2 viral infection during pregnancy on the fetus can be direct, transmitted through the placenta, and indirect - creating unfavorable conditions for the development of the fetus because of inflammation, micro-thrombosis, and hypercoagulation. The Aim: Our study aimed to determine the types and frequency of pathohistological changes in placental tissue in SARS-CoV-2-positive pregnant women and to examine the possible role of oxidative stress in the prognosis of the delivery and its maternal and fetal complications. Methods: This prospective clinical study included 50 pregnant women divided into two groups, SARS-CoV-2 positive (COVID-19 group) and SARS-CoV-2 negative (Control group), from whose we collected demographic, clinical, obstetric, biochemical, and pathologic data. Data about the newborn characteristics were also collected: anamnestic, clinical, and biochemical data. Results: The values of the superoxide anion radical and index of lipid peroxidation were significantly different in mothers concerning the presence of the SARS-CoV-2 infection, while the levels of the nitric oxide, index of lipid peroxidation, reduced glutathione, and superoxide dismutase were significantly different in the newborns depending on the SARS-CoV-2 infection. Newborn characteristics were similar between groups except for concentrations of IgM antibody. The incidence of pathohistological changes of the FVM type in the COVID-19 group of pregnant women was 46%, while in the control group. Conclusions: This study confirmed the significant impact of the SARS-CoV-2 viral infection on maternal and fetal biochemical parameters and oxidative stress-mediated placental dysfunction. Future studies should be performed with more participants and follow-up neonatal development.
Keywords:
COVID 19
; pregnancy
; Placental pathological lesions
; neonatal oxidative stress
; SARS-COV-2 fetal transmission
1. Introduction
WHO data show that the number of patients with COVID-19 from the beginning of the pandemic to August 2024 exceeds 776 million with more than 6.95 million deaths. [1,2]
Even after the WHO declared the end of the pandemic on May 11, 2023, COVID-19 remains one of the biggest challenges facing the health system and world economy because of its rapid spreading and unpredictable course.
SARS-COV-2 is the pathogen responsible for the onset of COVID-19, belonging to the group of beta-type Coronaviridae. [3,4] Based on structure, it is an enveloped RNA virus that shares a genetic sequence with some SARS viruses identified in bats and pangolins, indicating a zoogenic origin. [5] SARS-COV2 components are RNA and four structural proteins: spike (S) protein, nucleocapsid (N) protein, envelope (E) protein, and membrane (M) protein with a specific role in the pathogenesis of the disease. [6]
SARS CoV-2 is transmitted from infected individuals or asymptomatic carriers through droplet infection or contact with contaminated surfaces. [1,4] When the virus encounters a potential host, it first binds to ACE2 receptors with the S protein, resulting in the fusion of the virus's and cells' membranes. [7,8,9] These receptors are found on tissue cells of the kidney, endothelium, heart, macrophage, and pneumocyte cells, but predominantly in type 2 alveolar epithelial cells, making them highly sensitive to the virus's effects. [10,11,12]
In addition to the ACE2 receptor, Type 2 Transmembrane Serine Protease (TMPRSS2) also plays a key role. This protease leads to the cleavage of the S protein and a change in shape that facilitates the fusion of the virus's and the host's membranes and allows the virus's RNA to penetrate the host cell and begin replication. [1]
The RNA of the virus is a template for the multiplication of viral RNA and proteins that are further released infecting new cells. The release of the virus into the bloodstream leads to an inflammatory reaction mediated by the release of cytokines and the consequent activation of the coagulation system. [10,13] Activation of monocytes as part of the acute phase response leads to damage to the endothelium, which is crucial for activating the procoagulant system within the body and forming immune-thrombosis. In addition to this mechanism, intrahospital venous thromboembolism is also responsible for the occurrence of complications in COVID-19 patients. [16,20–24] VTE occurs because of activation of Virkoch's thryas: activation of the endothelium, prothrombotic state, and reduced mobility of patients that is characteristic of pregnancy. [10,14,15,16,17,18]
Based on the severity of symptoms, COVID-19 can be asymptomatic, mild, moderate, severe, and critical. [19] The viral load, inflammation, and the state of the immune system also influence the severity of the clinical course. [1] Factors such as age, gender, associated diseases, and obesity are related to the severity of the disease and increased mortality. [20] The physiological changes that accompany pregnancy could theoretically contribute to the development of more severe forms of COVID-19 in this group of patients. [21] Data from the US Centers for Disease Control and Prevention show that pregnant women have the same risk of death, but an increased risk of developing complications that require hospitalization and admission to the ICU compared to patients who are not pregnant. [10]
The immune system changes along with the development of the fetus to provide the necessary immunotolerance and adequate protection for the mother. These changes are dynamic and follow the gestational age to enable the smooth development of the fetus, so in the first trimester pro-inflammatory mechanisms dominate, the second trimester is characterized by anti-inflammatory, and in the third, pro-inflammatory mechanisms again prevail. [22] During pregnancy, the Th1-induced immune response decreases in favor of the TH2 response, leading to increased production of anti-inflammatory cytokines (IL4, IL10). Activation of the immune response and interleukin-initiated cytokine storms are a key factor in developing severe forms of the disease, and it is assumed that patients infected in the first and third trimesters are at a higher risk of serious complications. [23,24]
Pregnancy is a hypercoagulable condition characterized by elevated levels of prothrombotic factors such as factors VII, VIII, X, XII, von Willebrand factor, and fibrinogen, as well as decreased protein S and altered fibrinolysis, especially in the peripartum period. [10,25] Given that these physiological changes in pregnant women have a fourfold risk of developing serious thromboembolic complications compared to the general population, SARS-COV2 infection can lead to serious thromboembolic complications. [26,27]
Direct cytotoxicity of the virus and endothelial injury led to inflammatory changes in the complex functioning of the pregnant woman's immune system. This system constantly changes to satisfy the demands of the growing embryo, and thus the time of infection can be of great importance for the prognosis of the course of the disease, maternal immune response, release from the virus, and perinatal outcome. [28]
The impact of viral infection on the fetus can be direct, transmitted through the placenta, and indirect - creating unfavorable conditions for the development of the fetus because of inflammation, micro-thrombosis, and hypercoagulation.
There are three modes of transmission of the virus to the fetus/neonate: direct/intrauterine transmission, intrapartum and postpartum transmission.
Oxidative stress is one of the key factors in the pathogenesis of COVID-19 infection. [29,30,31] Oxidative stress is an impaired homeostasis in the body between oxidants and antioxidants, which leads to further disruption of the redox system and damage to molecules. Free radicals are highly reactive molecules with an excess of one or more electrons that easily interact with other molecules and lead to disruptions in the physiologically tuned system of a healthy organism. Excessive production of free radicals: reactive oxygen species (ROS), reactive nitrogen species (RNS), and reactive chlorine species (CRS) lead to direct peroxidation of membranes, structural proteins, enzymes, and nucleic acids, and can be neutralized under physiological conditions by interaction with enzymatic and non-enzymatic antioxidants. In addition to endogenous (enzymatic and non-enzymatic antioxidants), there is also a group of exogenous (natural or synthetic antioxidants) that also have a role in binding unpaired electrons of free radicals and stabilizing them, and their cumulative effect is defined as total antioxidant capacity (TAS). [32,33,34,35]
During scientific attempts to determine the level of oxidative stress in the body, a whole panel of biochemical markers of OS were created, which, based on their origin, were divided into:
Molecules that interact with free radicals, such as:
Products of lipid peroxidation: malondialdehyde, acrolein, isoprostanes),
Protein oxidation products: (carbonyl protein, tyrosine group),
DNA oxidation products (8-hydroxy-2deoxyguanosine),
Protein stress reactions, new biomarkers (microRNAs)
Molecules that belong to the antioxidant protection system, such as
Enzymes (myeloperoxidase),
Glutathione level
Pregnancy itself represents a state of increased oxidative stress due to the intense metabolic and immunological alterations necessary for the complex process of growth and development of conception products. The main source of ROS in pregnancy is the placenta, where these molecules are key factors in the complex system responsible for intercellular signaling, transcription, adaptive homeostasis, apoptosis, and host defense through phagocytosis [39,40,41,42]. Viral infections affect the excitation of oxidative stress of the host through numerous mechanisms such as excessive cytokine production, activation of the complement system, release of lipid mediators, and lipid peroxidation during the interaction of the body's defense cells with viral pathogens. [43,44]
In addition to its nutritional, excretory, oxygenation, and hormonal function, the placenta has an important protective role and is the main barrier to bacterial and viral infections in the fetus. This role predisposes the placenta to pathological changes under the direct influence of the SARS-COV2 virus and the consequences of systemic disease and coagulation changes. Examining the changes in the placenta provides us with a unique opportunity to uncover the mechanisms by which the virus affects pregnancy and fetus. MVM encompasses a spectrum of macroscopic and microscopic changes in the placenta. These changes are the result of ischemic (hypoxic) damage and oxidative stress. [45] Macroscopic changes are placental hypoplasia (weight <10th percentile), narrowed umbilical cord (diameter less than 0.8 cm at term), infarction, and retroplacental hemorrhage. [46,47,48] Microscopic lesions of the placenta include: distal villi hypoplasia and accelerated villi maturation, [49,50,51]
(FVM) Fetal vascular malperfusions are specific lesions of the placenta that arise from the obstruction of fetal blood flow. They can originate from the umbilical cord (hyperkoyling of the umbilical cord), from hypercoagulability, hypoxia, and inflammation-mediated endothelial damage (acute chorioamnionitis with chorionic vasculitis or funisitis and chronic villitis). [48,52,53,54,55]
Chronic villitis can be a consequence of viral infections, but in most cases, the etiology has not been identified. According to the Amsterdam criterion, FVM is represented by the following findings: thrombosis, segmental avascular villi, villous stromal-vascular karyorexa, vascular intramural fibrin deposition, blood vessel obliteration/fibromuscular sclerosis and vascular ectasia. [48]
Previous observational studies dealing with the problem of MVM have shown that these changes were asymptomatic, but the cumulative effect was reflected in placental hypoperfusion leading to adverse perinatal outcome and fetal complications and is associated with preeclampsia and intrauterine growth retardation (IUGR). [56,57,58,59]. IUGR is a fetus that does not reach its genetic potential during intrauterine growth and development and is present in as many as 15% of pregnancies. [60]
FVM lesions are associated with abnormalities of the neonatal central nervous system, IUGR, intrauterine fetal death, and stillbirth.[55,61,62,63].
Some studies have proposed that the determination of different types of OS biomarkers from the umbilical cord, placenta, and maternal blood could have implications in the prediction of placental pathology and clinical symptomatology. [64,65]
Besides oxidative stress damage, a potential pregnancy hazard is the transmission of the virus to the fetus. There are a few possible maternal/fetal (neonatal) infection methods. Fetal infection can occur in utero by direct transplacental transmission. The other possible way is intrapartum infection (neonatal contact with cervical or vaginal secretions or blood), and the third way is after birth via breastfeeding or direct maternal-neonatal contact. [61]. Investigating routes of possible fetal or neonatal transmission should provide sufficient information for future decisions considering the obstetric way of delivery, neonatal care, isolation of neonates, or safety of breastfeeding. [66]
We hypothesized that:
- There is a statistically significant difference in the frequency of pathohistological changes in placental tissue in patients with confirmed SARS-COV2 infection during pregnancy compared to the control group.
- Vertical transmission of SARS CoV-2 from mother to fetus is possible.
- There is a statistically significant increase in maternal and umbilical cord blood biomarkers of oxidative stress in patients infected with SARS CoV-2 during pregnancy compared to the control group.
- There is a significantly elevated level of oxidative stress markers in patients with more pronounced pathohistological changes in placental tissue.
- There is a statistically significant difference in the neonatal outcome of newborns of mothers with COVID-19 compared to the control group.
- Certain clinical parameters such as gestational age, sex of the newborn, and maternal age significantly affect the level of oxidative stress markers in the newborn.
This study aims to:
1. To determine the types and frequency of pathohistological changes in placental tissue in patients in whom SARS-COV-2 infection was confirmed during pregnancy and compare them with the control group
2. Determine from the plasma and lysate of erythrocytes of the mother's blood immediately before delivery and the blood of the newborn from the umbilical cord the values of the parameters of the antioxidant protection system, as well as pro-oxidants: lipid peroxide index measured as TBARS, nitric oxide in the form of nitrite (NO2-), superoxide anion radical (O2-) and hydrogen peroxide (H2O2), catalase (CAT), superoxide dismutase (SOD), reduced glutathione (GSH).
3. Determine the neonatal outcome: Apgar score, body weight of the newborn, admission to the intensive care unit, and length of stay in the neonatology department and ICU
2. Materials and Methods
2.1. Ethical Concerns
This study was designed as a case-series clinical study following the Good Clinical Practice and revised Helsinki Declaration. This study was approved by the Ethical Committee of Clinical Center Kragujevac number: 01/21-18. Written informed consent was obtained from all participants for research and publication before inclusion in the study.
2.2. Participants
This prospective clinical study included pregnant women who gave birth from the 24th to the 42nd week of gestation at the Ginecology Clinic at University Clinical Center Kragujevac, aged 18 to 43 years old, from Sumadia district, Republic of Serbia, followed in the period from the diagnosis of a positive SARS COV2 test to discharge from the obstetrics department after delivery and discharge of the newborn from the Department of Neonatology at University Clinical Center Kragujevac, Serbia.
2.3. Protocol of Study
Two cohorts were derived from the population of pregnant women who were delivered at the OB/GYN Clinic of the University Clinical Center in Kragujevac: women who had a positive result for SARS-COV2 (by RT-PCR method and/or rapid antigen test) during the pregnancy. The control cohort were woman who had a negative result on rapid antigen or RT-PCR SARS COV2 test on their admission day to the Obstetric Clinic for delivery, who were asymptomatic during hole pregnancy, and who had no IgG and IgM SARS COV2 antibodies detected on serological blood test. The main inclusion criteria were positive RT-PCR and/or rapid antigen tests for SARS-COV2 during the pregnancy. Exclusion criteria were positive personal history of thromboembolic diseases, thrombophilia, antiphospholipid syndrome, diabetes mellitus, systemic lupus erythematosus, hypertensive disorders in pregnancy, Rhesus factor incompatibility, ongoing anticoagulant therapy, and tobacco smoking during pregnancy.
Within the cohort of pregnant women who tested positive for the presence of SARS-COV2 during pregnancy concerning the time of gestation in which the infection occurred, three subgroups of patients will be distinguished in whom the impact of COVID-19 on placental tissue will be monitored in parallel:
1. Patients who have been diagnosed with SARS CoV2 in the first trimester of pregnancy (from pregnancy to the end of week 13 of gestation)
2. Patients who have been diagnosed with SARS CoV2 in the second trimester of pregnancy (from 14 to the end of week 27 of gestation)
3. Patients diagnosed with SARS CoV2 in the third trimester of pregnancy (28 to 42 weeks of gestation)
2.4. Sampling and Collecting Data
We have reviewed the electronic medical record for each subject and recorded demographic, clinical, obstetric, laboratory, and pathologic data. At that time, none of the patients in either group were vaccinated against COVID-19. Blood samples were collected from those two groups following delivery, namely: maternal peripheric blood and the umbilical cord blood for oxidative stress biomarkers test, placental tissue (a section of the entire thickness of the placenta with the membranes and one section of the umbilical cord for pathohistological analysis, fixed for 48 hours in a formalin solution to eliminate the infectivity).
2.5. Determination of Oxidative Stress Markers
We have collected venous blood from each participant, maternal peripheric blood, and umbilical cord blood for oxidative stress biomarkers testing in the next 3 minutes following delivery. Oxidative stress biomarkers were assessed spectrophotometrically from plasma samples (Shimadzu UV 1800, Japan), the index of lipid peroxidation, determined as thiobarbituric acid-reactive substances (TBARS), nitrites (NO2-), levels of superoxide anion radical (O2-) and hydrogen peroxide (H2O2).
2.5.1. Determination of TBARS
The plasma sample was incubated with 1% thiobarbituric acid in 0.05 NaOH for 15 minutes at 100 °C and measured as TBARS at 530 nm. As a control, distilled water was used as a blind probe. [67]
2.5.2. Nitrite Determination (NO2-)
Rapidly breaking down nitric oxide (NO) produces stable nitrite/nitrate compounds which were determined spectrophotometrically at 543 nm using Griess’s reagent according to Green`s method. Sodium nitrite was used as the reference standard to calculate the nitrite levels. [68]
2.5.3. Superoxide Anion Radical Determination (O2-)
Using the assay mixture that contains nitroblue tetrazolium, superoxide anion radical quantities were determined. The measurement was carried out at 530 nm on the wavelength. The blank control was performed using distilled water. [69]
2.5.4. Hydrogen Peroxide Determination (H2O2)
Horseradish peroxidase was utilized to accelerate the oxidation of phenol red by H2O2, which was used as a basis for the H2O2 measurement. 800 µl of freshly created phenol red solution was used to precipitate 200 µl of perfusate, and 10 µl of freshly made (1:20) horseradish peroxidase was added next. As the blank probe distilled water was utilized. At 610 nm, the level of H2O2 was detected.[70]
2.5.5. Catalase Activity Determination (CAT)
The analysis of catalase activity is carried out based on the Aebi method [71] .
First, we diluted the hemolysate with distilled water in a ratio of 1:7. 100 μl of the hemolysate sample was then mixed with an equal volume of ethanol along with 50μl of CAT buffer and 1000μl of 10 mM H2O2. The catalase activity was then determined spectrophotometrically at 230nm wavelength. [71]
2.5.6. Superoxide Dismutase Activity Determination (SOD)
The activity of superoxide dismutase is carried out by the Beutler method. In Eppendorf, we first mixed [72] 100μl of hemolysate with 1 ml of carbonate buffer, then processed the sample into a vortex and finally added 100μl of adrenaline. Spectrophotometry was performed at a wavelength of 470nm. [72,73]
2.5.7. Reduced Glutathione Concentration Determination (GSH)
The concentration of reduced glutathione (GSH) is determined by the Beutler method. This analysis is based on the oxidation reaction of GSH with GSH with 5,5-dithio-bis-6,2-nitrobenzoic acid. Spectrophotometric measurements were made at a wavelength of 412 nm. [72]
2.6. Pathohistological Analysis of Placental Tissue
Samples were also collected according to the recommendations of the Amsterdam Consensus [51]. Six samples were taken: first a sample of the amniotic sheath from the rupture site to the edge of the placenta; a sample of the cross-section of the umbilical cord, one from the fetal and the other about 5 cm from the uterine insertion; 3 more sections of the full-thickness placental disc cut with a scalpel, covering the uterine and fetal sides, taken from the central two-thirds of the surface of the placenta and one from the insertion site.
Tissue processing: dehydration, rinsing, and impregnation is carried out by a tissue processor and then molded into paraffin blocks. Then, using a rotating microtome (Leica RM2135), we cut the tissue into samples 5 μm thick, at room temperature, which were then immersed in a water bath at a temperature of 400 C. The cross-sections processed in this way were applied to the subject glasses (Superfrost-OT Plus microscope slides) for microscopy.
2.6.1. Staining Hematoxylin-Eosin Technique
To de-paraffin the tissues, it was necessary to first subject the glasses to heating to + 56 ⁰ С and then to spontaneous cooling. After that, we immerse them in xylol consecutively twice for 5 minutes each. Once we have deparaffinated the tissues, we proceed to rehydrate the tissues by immersing the glasses in solutions with decreasing concentrations of ethyl alcohol and then evaporating them with distilled water. The next step was staining with Mayer solution (Sigma Aldric, USA) for 10 minutes, after rinsing with distilled water and staining with an alcohol solution of eosin (Sigma Aldric, USA) for the next 2 minutes. A dehydration process was then carried out, which involved submerging the glass with increasing concentrations of ethyl alcohol and then illuminating it with two xylol solutions, each for 5 minutes. [74] The tiles prepared in this way are protected by cover glass after treatment with a medium covering and dried at room temperature. The analysis was carried out independently by two experienced pathologists on an Olympus BX51 light microscope, Japan. In the case of inconsistent results, the attitude of the third pathologist was decisive.
2.7. Statistical Analysis
All data are presented in the form of tables and graphs. Statistical analysis was done using the descriptive (mean, standard deviations and errors, and analytical tests, frequency, range) and analytical tests (Student T-test, Chi-square test). The statistical threshold was set at 0.05. All analysis was done in SPSS version 26 for Apple. Inc.
3. Results
3.1. Basic Demographic and Anamnestic Data of Study Group
This study included 50 pregnant women divided into two groups, SARS-CoV-2 positive (COVID-19 group) and SARS-CoV-2 negative (control group). In the first group, the mean age was 30,61±4,72, and in the negative groups, the mean age was 31,41±4,65. The mean gestational week at delivery was 39,19±0,98 in SARS-CoV-2 positive women, and 39,42±1,26 in the group SARS-CoV-2 negative. Based on the severity of symptoms 41.38% of patients had mild symptoms, and 58.62% had moderate symptoms.
3.2. Characteristics of the Newborns at Delivery According to the Presence of SARS-CoV-2 Infection in Mothers
Table 1 presents the mean values of the newborn characteristics at delivery. Most of them were similar in both groups, except for the concentrations of IgM antibody, where we found that newborns from COVID group mothers had significantly higher levels of these inflammatory markers in comparison with the SARS-CoV-2 negative group. (Table 1)
3.3. Analysis of the Oxidative Stress Levels According to the Presence of SARS-CoV-2 Infection
According to the presence of the SARS-CoV-2 infection, the mean values of redox status parameters are presented in the form of Figure 1a–d and Figure 2a–c. The values of the superoxide anion radical and index of lipid peroxidation were significantly different in mothers concerning the presence of the SARS-CoV-2 infection, while the levels of the nitric oxide, index of lipid peroxidation, reduced glutathione, and superoxide dismutase were significantly different in the newborns depending on the SARS-CoV-2 infection (Figure 1 and Figure 2, Table 2). Other parameters were not significantly changed (Figure 1 and Figure 2, Table 2).
3.4. The Histopathologic Lesions in the Placenta Concerning the Presence of SARS-COV2 Infection and the Timing of Infection
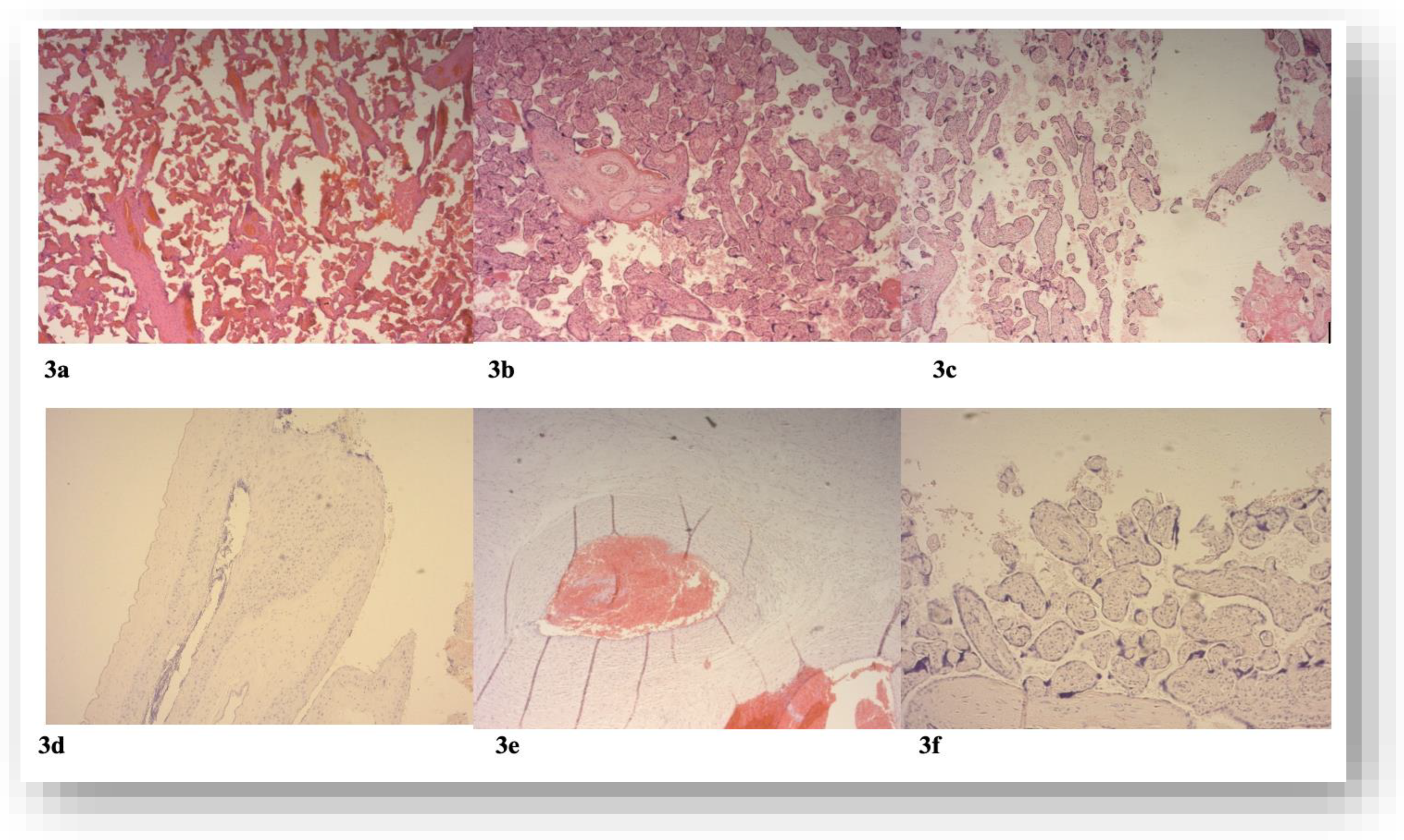
The incidence of pathohistological changes of the FVM type in the COVID-19 group of pregnant women was 46%, while in the control group, they were represented in 18% of placentas, and the incidence of MVM in the COVID group was 32%, and in the experimental group 18%. According to the moment of infection in the first trimester, pathohistological changes were registered in only 3% of patients infected in the first trimester, while they were more prevalent when the infection occurred during the second and third trimesters, in 44.4% and 47% of patients of Covid group. Inflammatory lesions in placental tissue were detected in 14.81% of placentas in the COVID group and only 4.5% of subjects in the control group. 70% of all placental lesions were detected in a group of patients with moderate/severe presentation of COVID-19. Table 3 presents the main morphometrical Placental characteristics of mothers regarding the presence of COVID-19. The results are presented as the frequency of the observed entity in percentage (%) (Table 3).
Figure 3.
The representative pathohistological findings in placental tissue samples among the study population; 3a distal villous hypoplasia-long villi with wide intervillous space; 3b the vascular ectasia-enlarged luminal diameter of the chorionic vessel; 3c Chorioamnionitis-numerous polymorphonuclear leukocytes infiltrate edematous fetal membranes; 3d-Distal villous hypoplasia; 3e-Avascular villus-lose of vessels with preservation of trophoblast; 3f-Villus vessel thrombosis-organized intraluminal Thrombus; Magnification 100x.
Figure 3.
The representative pathohistological findings in placental tissue samples among the study population; 3a distal villous hypoplasia-long villi with wide intervillous space; 3b the vascular ectasia-enlarged luminal diameter of the chorionic vessel; 3c Chorioamnionitis-numerous polymorphonuclear leukocytes infiltrate edematous fetal membranes; 3d-Distal villous hypoplasia; 3e-Avascular villus-lose of vessels with preservation of trophoblast; 3f-Villus vessel thrombosis-organized intraluminal Thrombus; Magnification 100x.
3.5. Neonatal Outcome
In the COVID-19 group, 62% of newborns were girls, 38% were boys, and in the control group, 41% were girls and 59% were boys.
The mode of delivery was vaginal birth in 68%, and C-section in 32% in the COVID-19 group, and vaginal birth in 45%, and C-section in 55% in the control group. Newborns of mothers from the Covid group had a similar mid-length of hospitalization- 4.37±1.1 days, as newborns from the control group with a mid-length of hospitalization of 4.22±2.72 days.
The length of newborn stay in neonatal ICU was 3.51±1.08 days in the COVID group and 2.22±1.39 days in the Control group.
Newborns from COVID-positive mothers were tested with nasopharyngeal swabs for RT-PCR SARS-COV2 test in the first 24 hours post-delivery. Only one positive result was registered in newborns.). 42,8% of newborns from COVID group mothers had positive SARS-COV-2 IgM antibody results, in the control group there were no positive SARS-COV-2 IgM antibody results.
4. Discussion
This prospective clinical study aimed to analyze the differences between basic, clinical, anamnestic, and biochemical data among pregnant women who were affected by COVID-19 or not. The special purpose of this research lies in the evaluation of the effects of the SARS-CoV-2 infection on fetal and newborn characteristics. Based on previous findings and literature data, for the first time, this study will evaluate the pathohistological changes in placental tissue among COVID-19 women who gave birth.
In the COVID group predominant mode of delivery was vaginal birth, except in a group of pregnant women with active COVID infection during delivery. Although the C-section birth rate was high (32%) it was significantly lower than previous studies showed. [75,76,77]. The leading indications for C-section in the COVID group were previous delivery completed by C-section, fetal distress during labor, and malpresentation, similar to the control group. Our study showed that there was no statistically significant increase in the number of cesarean sections in patients with COVID-19 during pregnancy. Studies dealing with this issue had contradictory results, some have shown an increased risk of operative termination of labor in COVID-19 patients [78,79,80], while others have shown that the mode of delivery does not depend on COVID-19 infection in pregnancy. [81]
No significant differences in neonatal outcomes were found between COVID-19 and the control group regarding birth weight, length, and head circumference. The hospitalization length for newborns was similar in both groups, with similar neonatal ICU hospitalization length 3.51±1.08 days in the COVID group and 2.22±1.39 days in the Control group.
All patients with active COVID newborns were tested with a SARS-COV-2 RT PCR test, only one was positive. Our study found that 42.8% of newborns from the COVID group mothers had positive IgM antibody findings. Initial studies focused on direct transmission showed that there was no convincing evidence of this mode of infection, however, at the end of the pandemic, worldwide pandemic meta-analyses showed that about 8.8% of newborns of COVID-19 positive mothers at birth had a positive SARS-COV2 PCR or serological test obtained after taking a nasopharyngeal swab. [82,83] The method of determining direct transmission to the fetus is also a subject of scientific doubt. In adults, the respiratory tract is the primary site of infection and the highest concentration of the virus, and the analysis of samples is performed through a nasopharyngeal or oropharyngeal swab, in the newborn, in addition to this method, is proposed to do the serological determination of the concentration of specific IgM antibodies to SARS-COV2, concerning the unknown site of primary infection. [84,85] IgM antibodies as part of the immune response to a specific viral infection, unlike IgG antibodies, cannot cross the placental barrier and can be useful in determining potential direct transmission to the fetus, but the weakness of this method is the existence of a cross-reaction and a false positive result, and the PCR test of the nasopharyngeal/oropharyngeal mucosa is the gold standard for determining the presence of SARS-COV2 infection in the newborns. [86] Studies focused on direct transmission have also used RNA Scope and In situ hybridization in scinciciotrophoblast cells, but the main problem with interpreting the results is the inconsistency of the results of the available tests. The sensitivity of the RT-PCR test is highest from the bronchial lavage sample (93%), and significantly lower from the nasopharyngeal swab and feces (63% and 29%, respectively), but as invasive, this method is not suitable for testing pregnant women and newborns. [87]
During this interaction of virus and host, studies have shown an increase in the activity of myeloperoxidase, NADPH synthetase, and inducible NO synthetase as well as changes in the levels of enzymatic and non-enzymatic antioxidants such as superoxide dismutase (SOD), glutathione peroxidase and catalase, and vitamin C, vitamin E, carotenoids, and glutathione flavonoids. [88,89,90,91,92] If the overproduction of ROS exceeds the antioxidant capacity of the placenta, tissue damage may occur. [43,93]
Placental ischemia, resulting from SARS-COV-2 infection, or systemic hypoxia and inflammation, leads to a disturbance in the balance of ROS and antioxidant protection and the onset of oxidative stress. OS is responsible for damage to proteins, lipids, and DNA. The placenta has mechanisms to counteract oxidative stress to reduce tissue damage, such as the production of NO, a potent vasodilator and antioxidant [65]. In addition to NO, CO, and H2S also play a significant gasotransmitter and vasodilator role [94].
Our study showed significantly increased TBARS levels in mothers of the COVID-19 group (p=0,002) compared with mothers of the control group, probably result of lipid damage caused by the SARS-COV-2 virus. Levels of O2- are significantly higher in our study in control group, which could be a consequence of the mode of delivery. SC was more frequent mode of delivery in the control group 55%, and 32% in the COVID group. Also leading indication for C-section in the control group was fetal nonreassuring status and previous C-section. Levels of NO were significantly lower in newborns of the COVID-19 group in our study, indicating that the placenta of COVID mothers could not sufficiently counterbalance the produktion of ROS after SARS-COV-2 infection. Increased levelas of SOD in COVID-19 group newborns suggested that placentas developed an oxidative damage defense system. The method of delivery could significantly affect the elevated level of biomarkers OS in the newborn, where these values are significantly increased in prolonged vaginal delivery and emergency cesarean section, as well as in stimulated oxytocin delivery. [32,95,96,97] The effect of the oxidative stress of the mother on the oxidative stress of the fetus depends on the antioxidant capacity of the newborn, which is determined genetically, depending on the sex of the fetus, the maturity of the fetus, and the age of the mother.[32]
Determination of individual biomarkers of OS cannot predict the level of pathological changes within the placenta and potential fetal/neonatal complications. Pregnancy and placental growth and development are accompanied by numerous changes due to the balance of the ROS and the antioxidant protection system, which is also involved in the complex mechanisms of cell signaling. The development of the placenta begins with the insertion of a fertilized blastocyst and the primary mode of transport through the placenta is diffusion conditions of low partial pressure of O2, which is necessary for normal growth and development of the embryo and the prevention of the formation of ROS.[98] As pregnancy progresses from the periphery of the placenta to the center, there is a gradual opening of the occluding blood vessels and a gradual increase in the partial pressure of oxygen within the intervillous space due to the continuous flow of oxygenated blood. This process takes place at the end of the first trimester and is responsible for the shift in the partial pressure of oxygen in the intervillous space. [99] When there is a disturbance at any level of placentation, the result is a sudden increase in oxygen pressure within the intervillous space and the consequent formation of ROS. [100]A gradual increase in O2 pressure allows the placenta to adapt to the new conditions of ROS formation by developing an antioxidant protection system (primarily by producing GPx and CAT). [101] To counteract the effect of ROS (O2 -, NO, H2O2, ONOO-) in the cells of the cytotrophoblast and stroma, a protection system is developed that includes the enzymes MnSOD, CuSOD, ZnSOD, however, when the level of ROS production exceeds the antioxidative capacity of the placenta, protein, lipids, and DNA damage occurs with consecutive cell damage and death. [101,102].
The determination of individual biomarkers of oxidative stress in placental pathology has no scientific or clinical significance, but a comparative examination at birth showed a positive correlation between elevated values of OS biomarkers in the mother's blood and blood from the umbilical cord of the newborn.[103] Studies focused on the effect of oxidative stress on placental tissue depending on the timing of infection in pregnancy have shown that changes within the scinciotroblast dominate the first trimester compared to the cytotrophoblast. This is reflected in a decrease in the surface area of microvilli and a decrease in mitochondria, with a very low amount of antioxidants detected. [104] A factor responsible for the onset of oxidative stress during the second and third trimesters is the intermittent flow of maternal blood within the villus, which produces ischemic reperfusion damage[105]
Some studies have detected the frequent presence of pathohistological changes by type of maternal vascular malperfusions (MVM), while others have reported changes by type of fetal vascular malperfusions (FVM), diagnosed according to the Amsterdam criterion based on the side of the placenta on which they occurred. [62,77,106,107,108] In addition to vascular changes, some studies have also proven the presence of inflammatory histopathological changes within the placentas of patients infected with COVID. [109]. Several studies have examined macroscopic and microscopic histopathological changes within the placental tissue in patients infected during pregnancy, but the results are incoherent [110,111,112,113,114,115,116]. Some studies even demonstrated no specific placental pathological findings in COVID patients regardless of the timing or severity of the disease. [117,118] The weaknesses of these studies are represented by the small number of samples, the inconsistency in the classification of histopathological changes, confounding factors such as chronic diseases in pregnancy and lifestyle habits that can have a significant impact on the result, as well as the choice of the control group.
Our study showed that placental pathology findings differ significantly between COVID-19 and the control group. We found FVM in 46% of the placentas of patients in the COVID group and 18% placentas of patients in the control group. MVM lesions were present in 32% of the placentas of the COVID group and in 18% of patients in the control group. Previous studies showed unequivocal results of placental findings, some demonstrated FVM in 30% and the other only 8% of placentas examined.[107,119] The most frequent findings in placental pathology of COVID patients in our study were: the obliteration of blood vessels, avascular villi, retroplacental hemorrhage, and accelerated villus maturation. Other study's most frequent pathophysiological findings were fibrin deposition, micro classification, thrombus, avascular villi, infraction, and villous edema. [120]
Given that the growth and development of the placenta is a dynamic process controlled by genetics and immunology, the moment when COVID-19 infection occurs during pregnancy can be an important factor in histopathological changes and maternal and fetal outcomes. Some studies showed that the timing of infection is crucial for developing pathophysiological placental lesions [62]
Our study's limitations include the small number of participants and the fact that it was unblinded for pathologists, so there is potential bias.
5. Conclusions
Based on the previous observation, in the summary we can conclude the following issues:
1. The types and frequency of pathohistological changes in placental tissue in patients in whom SARS-CoV-2 infection was confirmed during pregnancy differs from the control group. FVM is found to be the most frequent placental lesion in the COVID-19 group;
2. Plasma and lysate of erythrocytes of the mother's blood immediately before delivery and the blood of the newborn from the umbilical cord the values of the parameters of the antioxidant protection system, as well as pro-oxidants: lipid peroxide index measured as TBARS, nitric oxide in the form of nitrite (NO2-), superoxide anion radical (O2-) superoxide dismutase (SOD), reduced glutathione (GSH) significantly deferred between COVID-19 and control group;
3. Neonatal outcome: Apgar score, body weight of the newborn, admission to the intensive care unit, and length of stay in the neonatology department and ICU did not differ significantly between newborns from mothers of COVID-19 and the control group. COVID-19 patients do not have higher obstetrics potential for C-section delivery.
COVID-19 pregnancies exhibited an increase in histopathological abnormalities of the placenta, namely inflammatory changes of unknown etiology, as well as disturbed redox status of the mothers and newborns. Future studies investigating this specific influence of SARS-CoV-2 on placental tissue and newborn outcomes are needed, with more participants, with longer follow-ups for newborns, following neonatal and child development.
Author Contributions
Conceptualization, M.B.I and A.D.; methodology, N.J.; software, B.P and I.I; validation, G.B., N.A. and J.J.J; formal analysis, A.Z.; investigation, K.M., S.M.;M.S and J.S resources, N.A; data curation, D.R.; writing—original draft preparation, M.B.I; writing—review and editing, T.N.T; visualization, T.N.T; supervision, A.N.; project administration, N.J.; funding acquisition, A.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Faculty of Medical Sciences, Junior Project, grant number 13/21.
Institutional Review Board Statement
This study was designed as a case-series clinical study following the Good Clinical Practice and revised Helsinki Declaration. This study was approved by the Ethical Committee of Clinical Center Kragujevac number: 01/21-18.
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
All data are available upon the request to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| COVID-19 | Coronavirus disease 2019. |
| ICU | Intensive care unit |
| SARS-COV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| FVM | Fetal Vascular Malperfusion |
| MVM | Maternal Vascular Malperfusion |
| TMPRESS2 | Transmembrane serin proteases 2 |
| VTR | Venous Thrombosis |
| ROS | Reactive Oxygen Species |
| RNS | Reactive Nitric Species |
| CRS | Chlorine Reactive Species |
| TAS | Total Antioxidative Status |
| CAT | Catalase |
| GPX | Glutathione peroxidase |
| SOD | Superoxide dismutase |
| IUGR | Intrauterine Grow Restriction |
| TBARS | Thiobarbituric acid Reactive Substances |
| GSH | Glutathione |
| RT-PCR | Reverse Transcription Polymerase Chain Reaction |
References
- Zhu, Y.; Sharma, L.; Chang, D. Pathophysiology and clinical management of coronavirus disease (COVID-19): a mini-review. Front Immunol. 2023, 14. [Google Scholar] [CrossRef] [PubMed]
- Number of COVID-19 cases reported to WHO (cumulative total) World. 2024.
- Macáková, K.; Pšenková, P.; Šupčíková, N.; Vlková, B.; Celec, P.; Záhumenský, J. Effect of SARS-CoV-2 Infection and COVID-19 Vaccination on Oxidative Status of Human Placenta: A Preliminary Study. Antioxidants 2023, 12, 1403. [Google Scholar] [CrossRef] [PubMed]
- CDCWeekly, C. Protocol for Prevention and Control of COVID-19 (Edition 6). China CDC Wkly. 2020, 2, 321–6. [Google Scholar] [CrossRef]
- Asselah, T.; Durantel, D.; Pasmant, E.; Lau, G.; Schinazi, R.F. COVID-19: Discovery, diagnostics and drug development. J Hepatol. 2021, 74, 168–84. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Nomura, N.; Muramoto, Y.; Ekimoto, T.; Uemura, T.; Liu, K.; et al. Structure of SARS-CoV-2 membrane protein essential for virus assembly. Nat Commun 2022, 13, 4399. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280e8. [Google Scholar] [CrossRef]
- Wrapp, D.; Wang, N.; Corbett, K.S.; Goldsmith, J.A.; Hsieh, C.L.; Abiona, O.; et al. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science 2020, 367, 1260–3. [Google Scholar] [CrossRef]
- Yan, R.; Zhang, Y.; Li, Y.; Xia, L.; Guo, Y.; Zhou, Q. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science 2020, 367, 1444–8. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, R.; Malhamé, I.; Teshler, L.; Acharya, G.; Hunt, B.J.; McLintock, C. A critical review of the pathophysiology of thrombotic complications and clinical practice recommendations for thromboprophylaxis in pregnant patients with COVID-19. Acta Obstet Gynecol Scand 2020, 99, 1110–20. Available online: https://obgyn.onlinelibrary.wiley.com/doi/abs/10.1111/aogs.13962. [CrossRef] [PubMed]
- Sardu, C.; Gambardella, J.; Morelli, M.B.; Wang, X.; Marfella, R.; Santulli, G. Hypertension, Thrombosis, Kidney Failure, and Diabetes: Is COVID-19 an Endothelial Disease? A Comprehensive Evaluation of Clinical and Basic Evidence. J Clin Med. 2020, 9, 1417. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Zhao, Z.; Wang, Y.; Zhou, Y.; Ma, Y.; Zuo, W. Single-cell RNA expression profiling of ACE2, the putative receptor of Wuhan 2019-nCov. bioRxiv 2020. [Google Scholar] [CrossRef]
- Xiong, T.Y.; Redwood, S.; Prendergast, B.; Chen, M. Coronaviruses and the cardiovascular system: acute and long-term implications. Eur Heart J. 2020, 41, 1798–800. [Google Scholar] [CrossRef] [PubMed]
- Middeldorp, S.; Coppens, M.; van Haaps, T.F.; Foppen, M.; Vlaar, A.P.; Müller, M.C.A.; et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. Journal of Thrombosis and Haemostasis 2020, 18, 1995–2002. [Google Scholar] [CrossRef] [PubMed]
- Ranucci, M.; Ballotta, A.; Di Dedda, U.; Baryshnikova, E.; Dei Poli, M.; Resta, M.; et al. The procoagulant pattern of patients with COVID-19 acute respiratory distress syndrome. Journal of Thrombosis and Haemostasis 2020, 18, 1747–51. [Google Scholar] [CrossRef] [PubMed]
- Barrett, C.D.; Moore, H.B.; Yaffe, M.B.; Moore, E.E. ISTH interim guidance on recognition and management of coagulopathy in COVID-19: A comment. Journal of Thrombosis and Haemostasis 2020, 18, 2060–3. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Kruip, M.J.H.A.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.A.M.P.J.; Kant, K.M.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020, 191, 145–7. [Google Scholar] [CrossRef]
- Llitjos, J.; Leclerc, M.; Chochois, C.; Monsallier, J.; Ramakers, M.; Auvray, M.; et al. High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. Journal of Thrombosis and Haemostasis 2020, 18, 1743–6. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.F.W.; To, K.K.W.; Tse, H.; Jin, D.Y.; Yuen, K.Y. Interspecies transmission and emergence of novel viruses: lessons from bats and birds. Trends Microbiol. 2013, 21, 544–55. [Google Scholar] [CrossRef] [PubMed]
- Zu, Z.Y.; Jiang MDi Xu, P.P.; Chen, W.; Ni, Q.Q.; Lu, G.M.; et al. Coronavirus Disease 2019 (COVID-19): A Perspective from China. Radiology 2020, 296, E15–25. [Google Scholar] [CrossRef] [PubMed]
- Bende, M.; Gredmark, T. Nasal Stuffiness During Pregnancy. Laryngoscope 1999, 109, 1108–10. [Google Scholar] [CrossRef] [PubMed]
- Mor, G.; Cardenas, I.; Abrahams, V.; Guller, S. Inflammation and pregnancy: the role of the immune system at the implantation site. Ann N Y Acad Sci. 2011, 1221, 80–7. [Google Scholar] [CrossRef]
- Liu, H.; Wang, L.L.; Zhao, S.J.; Kwak-Kim, J.; Mor, G.; Liao, A.H. Why are pregnant women susceptible to COVID-19? An immunological viewpoint. J Reprod Immunol. 2020, 139, 103122. [Google Scholar] [CrossRef]
- Falahi, S.; Abdoli, A.; Kenarkoohi, A. Maternal COVID-19 infection and the fetus: Immunological and neurological perspectives. New Microbes New Infect. 2023, 53, 101135. [Google Scholar] [CrossRef] [PubMed]
- Thornton, P.; Douglas, J. Coagulation in pregnancy. Best Pract Res Clin Obstet Gynaecol. 2010, 24, 339–52. [Google Scholar] [CrossRef] [PubMed]
- Varlas, V.N.; Borș, R.G.; Plotogea, M.; Iordache, M.; Mehedințu, C.; Cîrstoiu, M.M. Thromboprophylaxis in Pregnant Women with COVID-19: An Unsolved Issue. Int J Environ Res Public Health 2023, 20, 1949. [Google Scholar] [CrossRef]
- Frantzeskaki, F.; Armaganidis, A.; Orfanos, S.E. Immunothrombosis in Acute Respiratory Distress Syndrome: Cross Talks between Inflammation and Coagulation. Respiration 2017, 93, 212–25. [Google Scholar] [CrossRef] [PubMed]
- Narang, K.; Enninga, E.A.L.; Gunaratne, M.D.S.K.; Ibirogba, E.R.; Trad, A.T.A.; Elrefaei, A.; et al. SARS-CoV-2 Infection and COVID-19 During Pregnancy: A Multidisciplinary Review. Mayo Clin Proc. 2020, 95, 1750–65. [Google Scholar] [CrossRef] [PubMed]
- Sies, H.; Berndt, C.; Jones, D.P. Oxidative Stress. Annu Rev Biochem. 2017, 86, 715–48. [Google Scholar] [CrossRef] [PubMed]
- Sies, H. Oxidative stress: a concept in redox biology and medicine. Redox Biol. 2015, 4, 180–3. [Google Scholar] [CrossRef]
- Sies, H. Oxidative Stress: Concept and Some Practical Aspects. Antioxidants 2020, 9, 852. [Google Scholar] [CrossRef] [PubMed]
- Chitra, M.; Mathangi, D.C.; Priscilla, J. Oxidative stress during spontaneous vaginal delivery: comparison between maternal and neonatal oxidative status. International Journal of Medical Research and Review 2016, 4, 60–6. [Google Scholar]
- Marín, R.; Abad, C.; Rojas, D.; Chiarello, D.I.; Alejandro, T.G. Biomarkers of oxidative stress and reproductive complications. Adv Clin Chem. 2023, 113, 157–233. [Google Scholar]
- Simon-szabo, Z.; Fogarasi, E.; Nemes-Nagy, E.; Denes, L.; Croitoru, M.; Szabo, B. Oxidative stress and peripartum outcomes (Review). Exp Ther Med. 2021, 22, 771. [Google Scholar] [CrossRef] [PubMed]
- Ghiselli, A.; Serafini, M.; Natella, F.; Scaccini, C. Total antioxidant capacity as a tool to assess redox status: critical view and experimental data. Free Radic Biol Med. 2000, 29, 1106–14. [Google Scholar] [CrossRef]
- Perrone, S.; Laschi, E.; Buonocore, G. Biomarkers of oxidative stress in the fetus and in the newborn. Free Radic Biol Med. 2019, 142, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Fogarasi, E.; Croitoru, M.D.; Fülöp, I.; Muntean, D.L. Is the Oxidative Stress Really a Disease? Acta Med Marisiensis 2016, 62, 112–20. [Google Scholar] [CrossRef]
- Ibrahim, A.; Khoo, M.I.; Ismail, E.H.E.; Hussain, N.H.N.; Zin, A.A.M.; Noordin, L.; et al. Oxidative stress biomarkers in pregnancy: a systematic review. Reproductive Biology and Endocrinology 2024, 22, 93. [Google Scholar] [CrossRef] [PubMed]
- Davies, K.J.A. Adaptive homeostasis. Mol Aspects Med. 2016, 49, 1–7. [Google Scholar] [CrossRef]
- Burton, G.J.; Jauniaux, E. Oxidative stress. Best Pract Res Clin Obstet Gynaecol. 2011, 25, 287–99. [Google Scholar] [CrossRef]
- Valenzuela, F.J.; Vera, J.; Venegas, C.; Pino, F.; Lagunas, C. Circadian System and Melatonin Hormone: Risk Factors for Complications during Pregnancy. Obstet Gynecol Int. 2015, 2015, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.; Sun, X.; Dey, S.K. Mechanisms of implantation: strategies for successful pregnancy. Nat Med. 2012, 18, 1754–67. [Google Scholar] [CrossRef] [PubMed]
- Marín, R.; Pujol, F.H.; Rojas, D.; Sobrevia, L. SARS- CoV-2 infection and oxidative stress in early-onset preeclampsia. Biochim Biophys Acta Mol Basis Dis. 2022, 1868, 166321. [Google Scholar] [CrossRef]
- Peterhans, E. Sendai virus stimulates chemiluminescence in mouse spleen cells. Biochem Biophys Res Commun. 1979, 91, 383–92. [Google Scholar] [CrossRef] [PubMed]
- Roberts, D.J.; Post, M.D. The placenta in pre-eclampsia and intrauterine growth restriction. J Clin Pathol. 2008, 61, 1254–60. [Google Scholar] [CrossRef]
- Khong, T.Y.; Mooney, E.E.; Ariel, I.; Balmus, N.C.M.; Boyd, T.K.; Brundler, M.A.; et al. Sampling and Definitions of Placental Lesions: Amsterdam Placental Workshop Group Consensus Statement. Arch Pathol Lab Med. 2016, 140, 698–713. [Google Scholar] [CrossRef] [PubMed]
- Ernst, L.M. Maternal vascular malperfusion of the placental bed. APMIS 2018, 126, 551–60. [Google Scholar] [CrossRef]
- Sharps, M.C.; Hayes, D.J.L.; Lee, S.; Zou, Z.; Brady, C.A.; Almoghrabi, Y.; et al. A structured review of placental morphology and histopathological lesions associated with SARS-CoV-2 infection. Placenta 2020, 101, 13–29. [Google Scholar] [CrossRef]
- Ernst, L.M. Maternal vascular malperfusion of the placental bed. APMIS 2018, 126, 551–60. [Google Scholar] [CrossRef] [PubMed]
- Sharps, M.C.; Hayes, D.J.L.; Lee, S.; Zou, Z.; Brady, C.A.; Almoghrabi, Y.; et al. A structured review of placental morphology and histopathological lesions associated with SARS-CoV-2 infection. Placenta 2020, 101, 13–29. [Google Scholar] [CrossRef]
- Khong, T.Y.; Mooney, E.E.; Ariel, I.; Balmus, N.C.M.; Boyd, T.K.; Brundler, M.A.; et al. Sampling and Definitions of Placental Lesions: Amsterdam Placental Workshop Group Consensus Statement. Arch Pathol Lab Med. 2016, 140, 698–713. [Google Scholar] [CrossRef]
- Lista, G.; Castoldi, F.; Compagnoni, G.; Maggioni, C.; Cornélissen, G.; Halberg, F. Neonatal and maternal concentrations of hydroxil radical and total antioxidant system: protective role of placenta against fetal oxidative stress. Neuro Endocrinol Lett. 2010, 31, 319–24. [Google Scholar]
- Chisholm, K.M.; Heerema-McKenney, A. Fetal Thrombotic Vasculopathy. American Journal of Surgical Pathology 2015, 39, 274–80. [Google Scholar] [CrossRef] [PubMed]
- Redline, R.W. Clinical and pathological umbilical cord abnormalities in fetal thrombotic vasculopathy. Hum Pathol. 2004, 35, 1494–8. [Google Scholar] [CrossRef] [PubMed]
- Redline, R.W.; Ariel, I.; Baergen, R.N.; deSa, D.J.; Kraus, F.T.; Roberts, D.J.; et al. Fetal Vascular Obstructive Lesions: Nosology and Reproducibility of Placental Reaction Patterns. Pediatric and Developmental Pathology 2004, 7, 443–52. [Google Scholar] [CrossRef] [PubMed]
- Arts, N.; Schiffer, V.; Severens-Rijvers, C.; Bons, J.; Spaanderman, M.; Al-Nasiry, S. Cumulative effect of maternal vascular malperfusion types in the placenta on adverse pregnancy outcomes. Placenta 2022, 129, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Wright, E.; Audette, M.C.; Ye, X.Y.; Keating, S.; Hoffman, B.; Lye, S.J.; et al. Maternal Vascular Malperfusion and Adverse Perinatal Outcomes in Low-Risk Nulliparous Women. Obstetrics & Gynecology 2017, 130, 1112–20. [Google Scholar]
- Parks, W.T.; Catov, J.M. The Placenta as a Window to Maternal Vascular Health. Obstet Gynecol Clin North Am. 2020, 47, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Zur, R.L.; Kingdom, J.C.; Parks, W.T.; Hobson, S.R. The Placental Basis of Fetal Growth Restriction. Obstet Gynecol Clin North Am. 2020, 47, 81–98. [Google Scholar] [CrossRef] [PubMed]
- Gordijn, S.J.; Beune, I.M.; Thilaganathan, B.; Papageorghiou, A.; Baschat, A.A.; Baker, P.N.; et al. Consensus definition of fetal growth restriction: a Delphi procedure. Ultrasound in Obstetrics & Gynecology 2016, 48, 333–9. [Google Scholar]
- Caparros-Gonzalez, R.A.; Pérez-Morente, M.A.; Hueso-Montoro, C.; Álvarez-Serrano, M.A.; de la Torre-Luque, A. Congenital, Intrapartum and Postnatal Maternal-Fetal-Neonatal SARS-CoV-2 Infections: A Narrative Review. Nutrients 2020, 12, 3570. [Google Scholar] [CrossRef] [PubMed]
- Glynn, S.M.; Yang, Y.J.; Thomas, C.; Friedlander, R.L.; Cagino, K.A.; Matthews, K.C.; et al. SARS-CoV-2 and Placental Pathology. American Journal of Surgical Pathology 2022, 46, 51–7. [Google Scholar] [CrossRef] [PubMed]
- Heider, A. Fetal Vascular Malperfusion. Arch Pathol Lab Med. 2017, 141, 1484–9. [Google Scholar] [CrossRef] [PubMed]
- Rolfo, A.; Cosma, S.; Nuzzo, A.M.; Salio, C.; Moretti, L.; Sassoè-Pognetto, M.; et al. Increased Placental Anti-Oxidant Response in Asymptomatic and Symptomatic COVID-19 Third-Trimester Pregnancies. Biomedicines 2022, 10, 634. [Google Scholar] [CrossRef]
- Schoots, M.H.; Gordijn, S.J.; Scherjon, S.A.; van Goor, H.; Hillebrands, J.L. Oxidative stress in placental pathology. Placenta 2018, 69, 153–61. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.A.; Thomas, K.M. Characterizing COVID-19 maternal-fetal transmission and placental infection using comprehensive molecular pathology. EBioMedicine 2020, 60, 102983. [Google Scholar] [CrossRef]
- Ohkawa, H.; Ohishi, N.; Yagi, K. Assay for lipid peroxides in animal tissues by thiobarbituric acid reaction. Anal Biochem. 1979, 95, 351–8. [Google Scholar] [CrossRef] [PubMed]
- Green, L.C.; Wagner, D.A.; Glogowski, J.; Skipper, P.L.; Wishnok, J.S.; Tannenbaum, S.R. Analysis of nitrate, nitrite, and [15N]nitrate in biological fluids. Anal Biochem. 1982, 126, 131–8. [Google Scholar] [CrossRef]
- Handbook Methods For Oxygen Radical Research; CRC Press, 2018.
- Pick, E.; Keisari, Y. A simple colorimetric method for the measurement of hydrogen peroxide produced by cells in culture. J Immunol Methods 1980, 38, 161–70. [Google Scholar] [CrossRef]
- Aebi, H. [13] Catalase in vitro. Methods in Enzymology 1984, 105, 121–126. [Google Scholar]
- Beutler, E. Red Blood Cell Metabolism, A Manual of Biochemical Methods. In Red Blood Cell Metabolism: A Manual of Biochemical Methods, 2nd ed.; Bergmeyen, H.V., Ed.; Grune and Stratton: New York, 1975; pp. 112–114. [Google Scholar]
- Beutler, E. Red Cell Metabolism: A Manual of Biochemical Methods, 3rd ed.; Beutler, E., Ed.; Grune and Stratton: New York, 1982; 105p. [Google Scholar]
- Fischer, A.H.; Jacobson, K.A.; Rose, J.; Zeller, R. Hematoxylin and Eosin Staining of Tissue and Cell Sections. Cold Spring Harb Protoc. 2008, 2008, pdb.prot4986. [Google Scholar] [CrossRef] [PubMed]
- Knight, M.; Bunch, K.; Vousden, N.; Morris, E.; Simpson, N.; Gale, C.; et al. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2 infection in UK: national population based cohort study. BMJ 2020, 369, m2107. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Li, Q.; Zheng, D.; Jiang, H.; Wei, Y.; Zou, L.; et al. Clinical Characteristics of Pregnant Women with Covid-19 in Wuhan, China. New England Journal of Medicine 2020, 382, e100. [Google Scholar] [CrossRef]
- Prabhu, M.; Cagino, K.; Matthews, K.; Friedlander, R.; Glynn, S.; Kubiak, J.; et al. Pregnancy and postpartum outcomes in a universally tested population for SARS-CoV-2 in New York City: a prospective cohort study. BJOG 2020, 127, 1548–56. [Google Scholar] [CrossRef]
- Giaxi, P.; Maniatelli, E.; Vivilaki, V. Evaluation of mode of delivery in pregnant women infected with COVID-19. Eur J Midwifery 2020, 4, 28. [Google Scholar] [CrossRef]
- Liu, H.; Liu, F.; Li, J.; Zhang, T.; Wang, D.; Lan, W. Clinical and CT imaging features of the COVID-19 pneumonia: Focus on pregnant women and children. Journal of Infection 2020, 80, e7–13. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. The Lancet 2020, 395, 809–15. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, M.; Perreand, E.; Mangione, M.; Patel, M.; Cojocaru, L.; Seung, H.; et al. Mode of Delivery in Patients with COVID-19. Am J Obstet Gynecol. 2022, 226, S582–3. [Google Scholar] [CrossRef]
- Chi, H.; Chiu, N.C.; Tai, Y.L.; Chang, H.Y.; Lin, C.H.; Sung, Y.H.; et al. Clinical features of neonates born to mothers with coronavirus disease-2019: A systematic review of 105 neonates. Journal of Microbiology, Immunology and Infection 2021, 54, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Azinheira Nobrega Cruz, N.; Stoll, D.; Casarini, D.E.; Bertagnolli, M. Role of ACE2 in pregnancy and potential implications for COVID-19 susceptibility. Clin Sci. 2021, 135, 1805–24. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.A.; Keith, M.; Pace, R.M.; Williams, J.E.; Ley, S.H.; Barbosa-Leiker, C.; et al. SARS-CoV-2 specific antibody trajectories in mothers and infants over two months following maternal infection. Front Immunol. 2022, 13, 1015002. [Google Scholar] [CrossRef] [PubMed]
- Flannery, D.D.; Gouma, S.; Dhudasia, M.B.; Mukhopadhyay, S.; Pfeifer, M.R.; Woodford, E.C.; et al. Assessment of Maternal and Neonatal Cord Blood SARS-CoV-2 Antibodies and Placental Transfer Ratios. JAMA Pediatr. 2021, 175, 594. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.A.; Morotti, D.; Beigi, B.; Moshfegh, F.; Zafaranloo, N.; Patanè, L. Confirming Vertical Fetal Infection With Coronavirus Disease 2019: Neonatal and Pathology Criteria for Early Onset and Transplacental Transmission of Severe Acute Respiratory Syndrome Coronavirus 2 From Infected Pregnant Mothers. Arch Pathol Lab Med. 2020, 144, 1451–6. [Google Scholar] [CrossRef]
- Lamouroux, A.; Attie-Bitach, T.; Martinovic, J.; Leruez-Ville, M.; Ville, Y. Evidence for and against vertical transmission for severe acute respiratory syndrome coronavirus 2. Am J Obstet Gynecol. 2020, 223, 91.e1–91e4. [Google Scholar] [CrossRef] [PubMed]
- Camini, F.C.; da Silva Caetano, C.C.; Almeida, L.T.; de Brito Magalhães, C.L. Implications of oxidative stress on viral pathogenesis. Arch Virol. 2017, 162, 907–17. [Google Scholar] [CrossRef]
- Broz, P.; Monack, D.M. Molecular mechanisms of inflammasome activation during microbial infections. Immunol Rev. 2011, 243, 174–90. [Google Scholar] [CrossRef]
- Reshi, M.L.; Su, Y.C.; Hong, J.R. RNA Viruses: ROS-Mediated Cell Death. Int J Cell Biol. 2014, 2014, 1–16. [Google Scholar] [CrossRef]
- Schwarz, K.B. Oxidative stress during viral infection: A review. Free Radic Biol Med. 1996, 21, 641–9. [Google Scholar] [CrossRef] [PubMed]
- Burdon, R.H. Superoxide and hydrogen peroxide in relation to mammalian cell proliferation. Free Radic Biol Med. 1995, 18, 775–94. [Google Scholar] [CrossRef] [PubMed]
- Rani, N.; Dhingra, R.; Arya, D.S.; Kalaivani, M.; Bhatla, N.; Kumar, R. Role of oxidative stress markers and antioxidants in the placenta of preeclamptic patients. Journal of Obstetrics and Gynaecology Research 2010, 36, 1189–94. [Google Scholar] [CrossRef] [PubMed]
- Holwerda, K.M.; Faas, M.M.; van Goor, H.; Lely, A.T. Gasotransmitters. Hypertension 2013, 62, 653–9. [Google Scholar] [CrossRef]
- Hracsko, Z.; Safar, Z.; Orvos, H.; Novak, Z.; Pal, A.; Varga, I.S. Evaluation of oxidative stress markers after vaginal delivery or Caesarean section. In Vivo 2007, 21, 703–6. [Google Scholar]
- Chiba, T.; Omori, A.; Takahashi, K.; Tanaka, K.; Kudo, K.; Manabe, M.; et al. Correlations between the detection of stress-associated hormone/oxidative stress markers in umbilical cord blood and the physical condition of the mother and neonate. Journal of Obstetrics and Gynaecology Research 2010, 36, 958–64. [Google Scholar] [CrossRef] [PubMed]
- Karaçor, T.; Sak, S.; Başaranoğlu, S.; Peker, N.; Ağaçayak, E.; Sak, M.E.; et al. Assessment of oxidative stress markers in cord blood of newborns to patients with oxytocin-induced labor. Journal of Obstetrics and Gynaecology Research 2017, 43, 860–5. [Google Scholar] [CrossRef] [PubMed]
- Burton, G.J.; Hempstock, J.; Jauniaux, E. Oxygen, early embryonic metabolism and free radical-mediated embryopathies. Reprod Biomed Online 2003, 6, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Hempstock, J.; Greenwold, N.; Burton, G.J. Trophoblastic Oxidative Stress in Relation to Temporal and Regional Differences in Maternal Placental Blood Flow in Normal and Abnormal Early Pregnancies. Am J Pathol. 2003, 162, 115–25. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Zaidi, J.; Jurkovic, D.; Campbell, S.; Hustin, J. Pregnancy: Comparison of colour Doppler features and pathological findings in complicated early pregnancy. Human Reproduction 1994, 9, 2432–7. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Watson, A.L.; Hempstock, J.; Bao, Y.P.; Skepper, J.N.; Burton, G.J. Onset of Maternal Arterial Blood Flow and Placental Oxidative Stress: A Possible Factor in Human Early Pregnancy Failure. Am J Pathol. 2000, 157, 2111–22. [Google Scholar] [CrossRef]
- Burton, G.J.; Hempstock, J.; Jauniaux, E. Oxygen, early embryonic metabolism and free radical-mediated embryopathies. Reprod Biomed Online 2003, 6, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Fogel, I.; Pinchuk, I.; Kupferminc, M.J.; Lichtenberg, D.; Fainaru, O. Oxidative stress in the fetal circulation does not depend on mode of delivery. Am J Obstet Gynecol. 2005, 193, 241–6. [Google Scholar] [CrossRef]
- Watson, A.L.; Skepper, J.N.; Jauniaux, E.; Burton, G.J. Changes in concentration, localization and activity of catalase within the human placenta during early gestation. Placenta 1998, 19, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Hung, T.H.; Skepper, J.N.; Burton, G.J. In Vitro Ischemia-Reperfusion Injury in Term Human Placenta as a Model for Oxidative Stress in Pathological Pregnancies. Am J Pathol. 2001, 159, 1031–43. [Google Scholar] [CrossRef]
- Mulvey, J.J.; Magro, C.M.; Ma, L.X.; Nuovo, G.J.; Baergen, R.N. Analysis of complement deposition and viral RNA in placentas of COVID-19 patients. Ann Diagn Pathol. 2020, 46, 151530. [Google Scholar] [CrossRef] [PubMed]
- Patberg, E.T.; Adams, T.; Rekawek, P.; Vahanian, S.A.; Akerman, M.; Hernandez, A.; et al. Coronavirus disease 2019 infection and placental histopathology in women delivering at term. Am J Obstet Gynecol. 2021, 224, 382.e1–382e18. [Google Scholar] [CrossRef] [PubMed]
- Shanes, E.D.; Mithal, L.B.; Otero, S.; Azad, H.A.; Miller, E.S.; Goldstein, J.A. Placental Pathology in COVID-19. Am J Clin Pathol. 2020, 154, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Hsu, A.L.; Guan, M.; Johannesen, E.; Stephens, A.J.; Khaleel, N.; Kagan, N.; et al. Placental SARS-CoV-2 in a pregnant woman with mild COVID-19 disease. J Med Virol. 2021, 93, 1038–44. [Google Scholar] [CrossRef]
- Suhren, J.T.; Meinardus, A.; Hussein, K.; Schaumann, N. Meta-analysis on COVID-19-pregnancy-related placental pathologies shows no specific pattern. Placenta 2022, 117, 72–7. [Google Scholar] [CrossRef]
- Levitan, D.; London, V.; McLaren, R.A.; Mann, J.D.; Cheng, K.; Silver, M.; et al. Histologic and Immunohistochemical Evaluation of 65 Placentas From Women With Polymerase Chain Reaction–Proven Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection. Arch Pathol Lab Med. 2021, 145, 648–56. [Google Scholar] [CrossRef] [PubMed]
- Al-Rawaf, S.A.; Mousa, E.T.; Kareem, N.M. Correlation between Pregnancy Outcome and Placental Pathology in COVID-19 Pregnant Women. Infect Dis Obstet Gynecol. 2022, 2022, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, A.C.M.; Avvad-Portari, E.; Meuser-Batista, M.; Conde, T.C.; de Sá, R.A.M.; Salomao, N.; et al. Histopathological and clinical analysis of COVID-19-infected placentas. Surgical and Experimental Pathology 2024, 7, 4. [Google Scholar] [CrossRef]
- Baergen, R.N.; Heller, D.S. Placental Pathology in Covid-19 Positive Mothers: Preliminary Findings. Pediatric and Developmental Pathology 2020, 23, 177–80. [Google Scholar] [CrossRef]
- Hosier, H.; Farhadian, S.F.; Morotti, R.A.; Deshmukh, U.; Lu-Culligan, A.; Campbell, K.H.; et al. SARS–CoV-2 infection of the placenta. Journal of Clinical Investigation 2020, 130, 4947–53. [Google Scholar] [CrossRef] [PubMed]
- Smithgall, M.C.; Liu-Jarin, X.; Hamele-Bena, D.; Cimic, A.; Mourad, M.; Debelenko, L.; et al. Third-trimester placentas of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-positive women: histomorphology, including viral immunohistochemistry and in-situ hybridization. Histopathology 2020, 77, 994–9. [Google Scholar] [CrossRef] [PubMed]
- Corbetta-Rastelli, C.M.; Altendahl, M.; Gasper, C.; Goldstein, J.D.; Afshar, Y.; Gaw, S.L. Analysis of placental pathology after COVID-19 by timing and severity of infection. Am J Obstet Gynecol MFM 2023, 5, 100981. [Google Scholar] [CrossRef] [PubMed]
- Schaumann, N.; Suhren, J.T. An Update on COVID-19-Associated Placental Pathologies. Z Geburtshilfe Neonatol. 2024, 228, 42–8. [Google Scholar] [CrossRef] [PubMed]
- Gulersen, M.; Prasannan, L.; Tam Tam, H.; Metz, C.N.; Rochelson, B.; Meirowitz, N.; et al. Histopathologic evaluation of placentas after diagnosis of maternal severe acute respiratory syndrome coronavirus 2 infection. Am J Obstet Gynecol MFM 2020, 2, 100211. [Google Scholar] [CrossRef]
- Belay, G. Article Review on Histopathologic Features of Placenta and Adverse Outcome in Pregnant Women with COVID-19 Positive. Pathology and Laboratory Medicine 2023, 7, 4–11. [Google Scholar] [CrossRef]
Figure 1.
a. The mean concentration of the plasma superoxide anion radical (O2-). Results are presented as mean plus standard deviations. Statistical analysis was done using the Student T test. b The mean concentration of the plasma hydrogen peroxide (H2O2-). Results are presented as mean plus standard deviations. Statistical analysis was done using the Student T test. c. The mean concentration of the plasma nitric oxide (NO-). Results are presented as mean plus standard deviations. Statistical analysis was done using Student T test. d. The mean concentration of the plasma index of lipid peroxidation (TBARS). Results are presented as mean plus standard deviations. Statistical analysis was done using the Student T test.
Figure 1.
a. The mean concentration of the plasma superoxide anion radical (O2-). Results are presented as mean plus standard deviations. Statistical analysis was done using the Student T test. b The mean concentration of the plasma hydrogen peroxide (H2O2-). Results are presented as mean plus standard deviations. Statistical analysis was done using the Student T test. c. The mean concentration of the plasma nitric oxide (NO-). Results are presented as mean plus standard deviations. Statistical analysis was done using Student T test. d. The mean concentration of the plasma index of lipid peroxidation (TBARS). Results are presented as mean plus standard deviations. Statistical analysis was done using the Student T test.
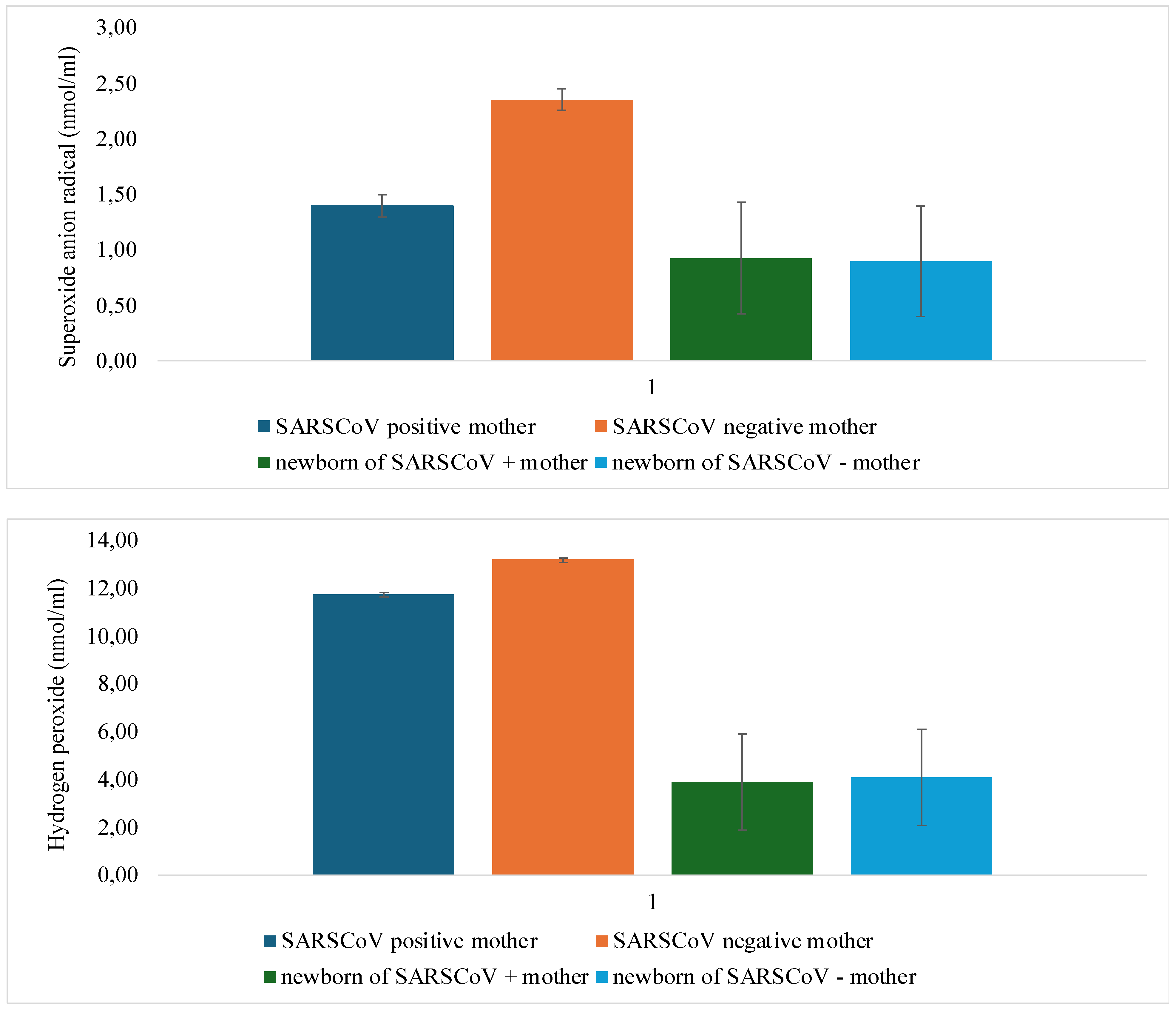
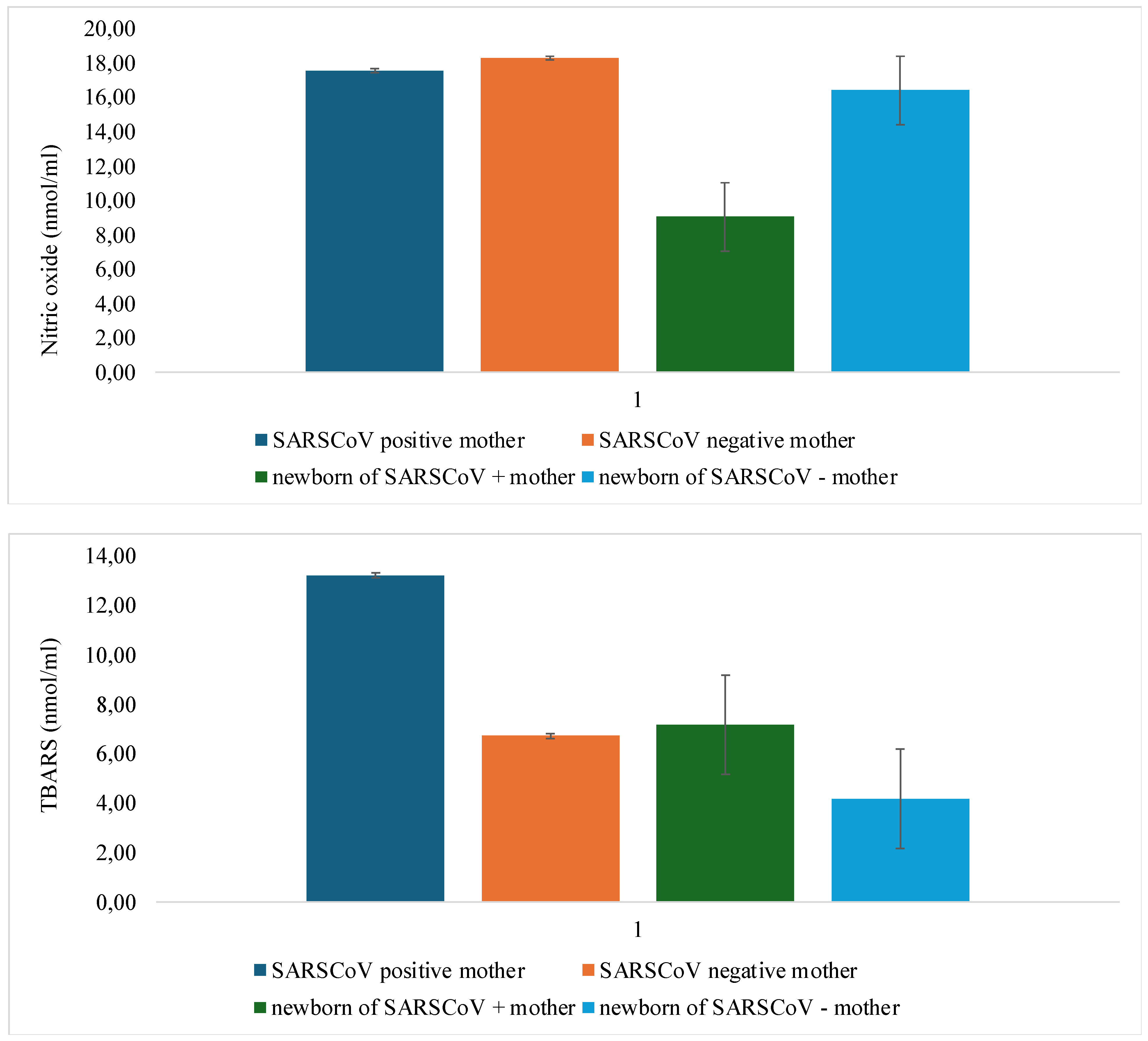
Figure 2.
a. The mean activity of the hemolysate reduced glutathione (GSH). Results are presented as mean plus standard deviations. Statistical analysis was done using the Student T test. b. The mean activity of the hemolysate superoxide dismutase (SOD). Results are presented as mean plus standard deviations. Statistical analysis was done using the Student T test. c. The mean activity of the hemolysate catalase (CAT). Results are presented as mean plus standard deviations. Statistical analysis was done using the Student T test.
Figure 2.
a. The mean activity of the hemolysate reduced glutathione (GSH). Results are presented as mean plus standard deviations. Statistical analysis was done using the Student T test. b. The mean activity of the hemolysate superoxide dismutase (SOD). Results are presented as mean plus standard deviations. Statistical analysis was done using the Student T test. c. The mean activity of the hemolysate catalase (CAT). Results are presented as mean plus standard deviations. Statistical analysis was done using the Student T test.
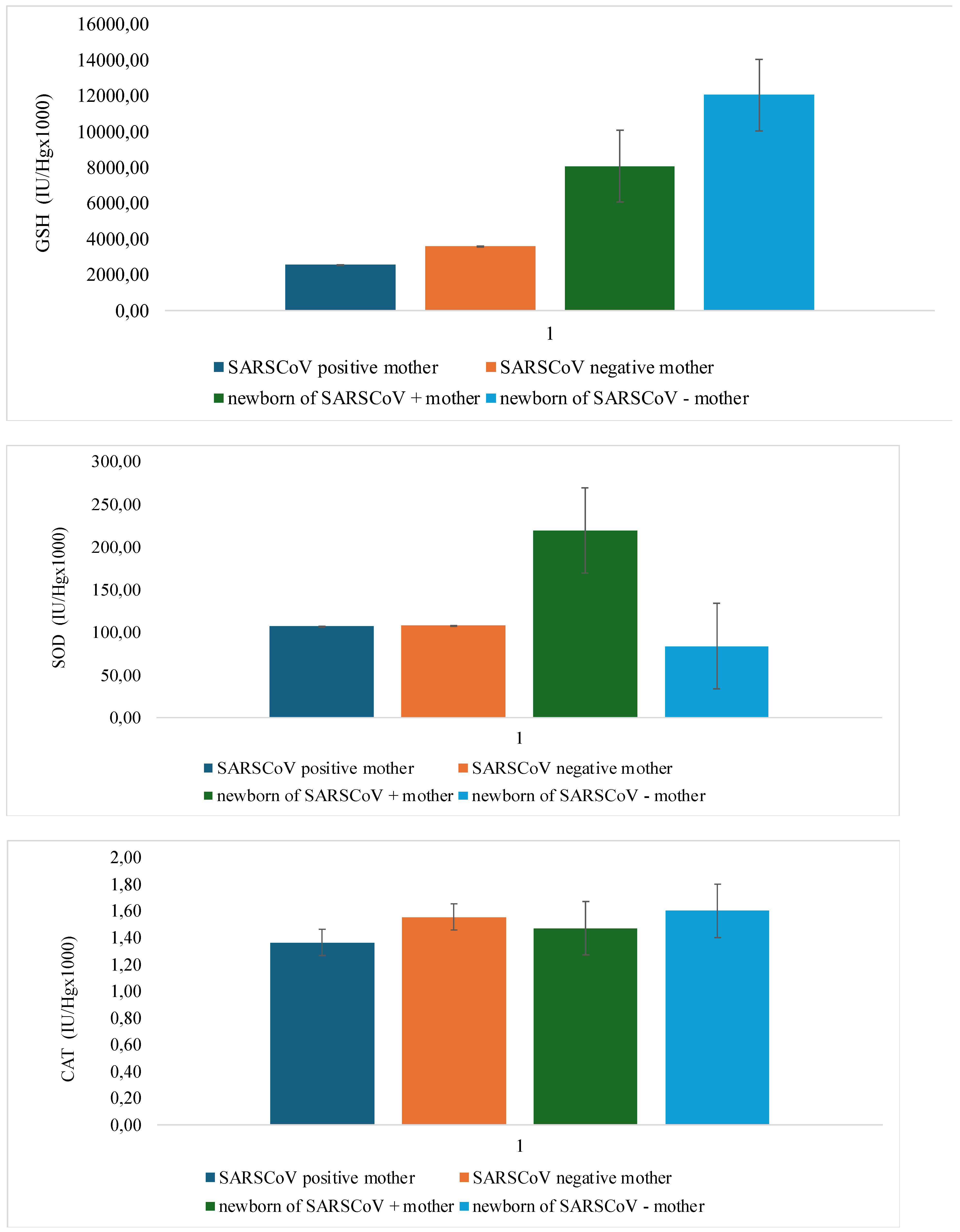

Table 1.
The mean values of the parameters related to the newborn at delivery according to the presence of SARS-CoV-2 infection. Results are presented as mean plus standard deviations. Statistical analysis was done using the Student T test.
Table 1.
The mean values of the parameters related to the newborn at delivery according to the presence of SARS-CoV-2 infection. Results are presented as mean plus standard deviations. Statistical analysis was done using the Student T test.
| Parameters | Gestational week at delivery | APGAR Score 1’ | APGAR Score 5’ | Baby Body Weight (g) | Baby Body length (cm) | Head circumference (cm) | IgM antibody (g/L) | Placenta weight (g) | |
| SARS-CoV-2+ | Mean | 39.19 | 8.96 | 9.10 | 3359.17 | 48.75 | 34.38 | 3.42 | 608.26 |
| SD | 0.98 | 0.62 | 0.62 | 491.69 | 2.25 | 1.58 | 3.25 | 129.81 | |
| SARS-CoV-2- | Mean | 39.42 | 9.23 | 9.19 | 3534.09 | 50.27 | 35.23 | 0.30 | 577.37 |
| SD | 1.26 | 0.61 | 0.60 | 404.35 | 2.12 | 1.38 | 0.27 | 143.37 | |
| P value | p=0.676 | p=0.556 | p=0.780 | p=0.465 | p=0.681 | p=0.899 | p=0.000* | p=0.322 | |
A symbol asterisk (*) represents the p values less than 0.05.
Table 2.
Data of the statistical analysis using the Student T test in comparison with two groups of concentrations of pro-oxidative markers antioxidative enzymes.
Table 2.
Data of the statistical analysis using the Student T test in comparison with two groups of concentrations of pro-oxidative markers antioxidative enzymes.
| Comparison | Mothers | Newborns |
|---|---|---|
| SARS-CoV2+ vs. SARS CoV2 - | SARS-CoV2+ vs. SARS CoV2 - | |
| O2- | p=0.002* | p=0.113 |
| H2O2 | p=0.012 | p=0.043 |
| NO- | p=0.509 | p=0.003* |
| TBARS | p=0.001* | p=0.004* |
| GSH | p=0.322 | p=0.001* |
| SOD | p=0.488 | p=0.002* |
| CAT | p=0.566 | p=0.623 |
Table 3.
Morphometrical Placental characteristics of mothers regarding the presence of COVID-19. Results are presented as frequency of the observed entity in percentage (%).
Table 3.
Morphometrical Placental characteristics of mothers regarding the presence of COVID-19. Results are presented as frequency of the observed entity in percentage (%).
| Placental characteristics | Thrombosis | Avascular villi | Deposits of fibrines | Villous stromal vascular karyorrhexis | Obliteration of blood vessels | Vascular ectasia | Delayed villous maturation | placental infarction | retroplacental hemorrhage | Hypoplasia of distal villus | Accelerated villous maturation | Decidual arteriopathy | inflammatory changes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| COVID-19 participants | + [6/28] [21.4%] |
++ [9/28] [32.1%] |
+ [1/28] [3.57%] |
- [0/28] [0%] |
+++ [12/28] [42.8%] |
++ [8/28] [28.5%] |
- [0/28] [0%] |
+ [3/28] [10.7%] |
++ [7/28] [25%] |
+ [2/28 [7.14%] |
++ [8/28] [28.5%] |
- [0/28] [0%] |
+ [4/28] [14.3%] |
| Non-COVID-19 participants | + [1/22] [4.54%] |
+ [1/22] [4.54%] |
- [0/22] [0%] |
- [0/22] [0%] |
+ [1/22] [4.54%] |
- [0/22] [0%] |
+ [1/22] [4.54%] |
- [0/22] [0%] |
- [0/22] [0%] |
- [0/22] [0%] |
++ [4/22] [18.1%] |
- [0/22] [0%] |
- [0/22] [0%] |
+ = presence of entity in 10%. ++ = presence of entity in 25%. +++ = presence of an entity in 40% and more.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



