
Submitted:
23 December 2024
Posted:
24 December 2024
You are already at the latest version
Abstract
Remifentanil is routinely administered in human neurosurgery whilst its use in non-human primates is not described. Here we described a new remifentanil-propofol total intravenous anesthesia (TIVA) for macaque neurosurgery and we compared it retrospectively to fentanyl-propofol anesthesia. Twelve anesthesias were performed (F=6; R=6). After premedication, anesthesia was induced with 3 mcg/kg fentanyl (F) or 3 mcg/kg remifentanil (R) intravenously (IV) and maintained through propofol and fentanyl [0.17 ± 0.01 mcg/kg/min after induction and 0.13 ± 0.01 mcg/kg/min during maintenance] or remifentanil [0.1 ± 0.02 mcg/kg/min after induction and 0.16 ± 0.05 mcg/kg/min during maintenance] constant-rate-infusion (CRI), respectively. Tracheal intubation in R was characterized by apnea, absence of laryngeal reaction, and cough compared to F. The mean propofol rate administered in F [0.3 ± 0.1 at start to 0.2± 0.1 mg/kg/min for maintenance] was significantly higher than in R [0.17 ± 0.1 at start to 0.16 ± 0.01 mg/kg/min for maintenance].The cardiovascular and respiratory parameters did not differ significantly between the two groups. Extubation time was shorter in R compared to F [8 (6– 10) and 18 (14– 22) minutes respectively]. Finally, the new remifentanil-propofol TIVA proved to be a beneficial refinement for macaque neurosurgery, providing smoother intubation, cardiovascular stability, lower propofol requirements and faster recovery.
Keywords:
macaques
; neurosurgery
; fentanyl
; remifentanil
; anesthesia
1. Introduction
Non-human primates (NHPs), in particular Macaca mulatta and fascicularis, are frequently used in translational medicine for their anatomical and physiological proximity to humans. For neurosurgery in both humans and animals, total (TIVA) or partial intravenous anesthesia (PIVA) might be preferred to inhalation anesthesia, for its minor interference with the cerebral autoregulation mechanisms [1]. Also in macaques, isoflurane or sevoflurane anesthesia might lead to dose-dependent hypotension and impairment of cerebral autoregulation [2], increasing peri-anesthetic morbidity [3]. Further advantages of TIVA anesthesia in humans consists of the lower incidence of postoperative nausea and vomiting (PONV) [4]. Moreover, TIVA improves the safety for the operator bypassing halogenates toxicity and reducing the environmental pollution [5]. A combination of propofol and fentanyl is a commonly used TIVA protocol for NHPs [6,7] for a variety of experimental procedures. In the authors’ experience, induction with fentanyl-propofol do not provide ideal intubation conditions – namely absence of cough reflex and apnea time. Furthermore, during maintenance, MAP values would lower under 60 mmHg, so that vasopressors are required. In human neurosurgery, remifentanil maintains hemodynamic stability, decreasing cardiovascular hyperdynamic status that in patients with increased intracranial pressure (ICP) can cause severe cardiac and/or cerebral complications during extubating phase [8]. Moreover, remifentanil in people decreases movements during craniotomy in lack of muscle relaxants [9]. Finally, regarding pain management, this opioid has, in comparison to fentanyl, a faster onset and metabolization, leading consequently to a more rapid recovery.
Thence, we hypothesized that a propofol - remifentanil TIVA would allow for a more manageable, qualitative, hemodynamically stable and safer anesthesia for macaques undergoing neurosurgery.
2. Materials and Methods
This is a retrospective comparative clinical trial. All experimental procedures related to the anesthesia in this study were approved by the cantonal veterinary authorities, following Swiss Animal Welfare Act of 16 December 2005 (Animal Welfare Law – TSchG), Animal Protection Ordinance of 23 April 2008 (Tierschutzverordung – TSchV) and the 3Rs principles.
2.1. Animals
The anesthetic records of macaques undergoing neurosurgical procedures between 2022 and 2023 were collected and reviewed (see Table 1).
Macaques were socially housed in compatible groups of the same sex (from 2 to 6 animals per room) according to the Swiss Welfare Act and Swiss Ordinance on animal experimentation, in a research facility approved by the cantonal authorities.
Physical examination, complete blood count and biochemical parameters were carried out before surgery.
2.2. Anesthetics and Surgery
All anesthesias were performed by or under the supervision of a specialized veterinary anesthesiologist and asenior human anesthesiologist.
Animals were weighted the day before surgery and were fasted overnight before the anesthesia. On surgery day, premedication was done with ketamine 10 mg/kg (Narketan 100mg/ml, Vetoquinol, Ismaning, Germany) and midazolam 0.3 mg/kg (Dormicum 5 mg/ml, Roche, Basel, Switzerland) intramuscularly (IM), whilst NHPs were restrained in the chair. Animals in Group F also received methadone 0.2 mg/kg (Methadon 10 mg/ml, Streuli Pharma AG, Uznach, Switzerland) IM.
During the surgical preparation of the macaques, flow-by oxygen (4 to 6 L/min) was administered by high flow nasal cannula (Sentri™ pediatric, Intersurgical, Wokingham, UK) and temperature loss was prevented with a heating blanket (Mistral-Air® MA1200, The Surgical Company, Amersfoort, The Netherlands), which was also used during surgery. Vascular access was gained through 24 to 18 G size catheters and depending on the length of anesthesia, only 1 or both saphenous veins were cannulated.
On the operating table, all animals were pre-oxygenated by face mask (ClearLite™, Intersurgical, Wokingham, UK) with 100 % O2 (6 L/min) and heart rate (HR) through electrocardiogram, non-invasive systolic (SAP), mean (MAP) and diastolic arterial pressure (DAP), RR and end-tidal carbon dioxide (ETCO2), SpO2, rectal temperature (T), tidal volume (TV) and peak inspiratory pressure (PIP) (Aisys CS2, Anandic Medical System AG, Feuerthalen, Switzerland) were monitored every 5 minutes. The urethra was catheterized (Mila Foley 5 Fr x 30 cm, 12 in, Provet AG, Lyssach, Switzerland), and urine output measured. Cefazoline (Kefzol 1g, Teva Pharma AG, Basel, Switzerland) 20 mg/kg was given IV and repeated every 6 hours. Eye drops (Lacryvisc SE 0.5 g, Alcon, Zug, Switzerland) were repeatedly applied.
As soon as the monitoring was fully functional and SpO2 was above 96%, 0.1 mg/kg/min IV propofol constant rate infusion (CRI) was started and 5 minutes later anesthesia was co-induced with a bolus of 3 mcg/kg fentanyl (Fentanyl Sintetica 0.5 mg/10ml, Sintetica SA, Mendrisio, Switzerland) IV or a bolus of 3 mcg/kg remifentanil (Ultiva®, Aspen Pharma Schweiz GmbH, Baar, Switzerland) in groups F and R respectively. Intubation was performed with the animal in sternal decubitus, and its head everted, and the larynx was sprayed with lidocaine (Xylocaine spray 10%, Aspen Pharma Schweiz GmbH, Baar, Switzerland). The tracheas were intubated with a cuffed endotracheal (ET) tube (Endotube, 2 – 4 mm cuffed with murphy eye, Covetrus, Lyssach, Switzerland), depending on their size, and connected to a circular rebreathing system (Flextube™ pediatric breathing system, Intersurgical, Wokingham, UK) or a F circuit (QTube™, Anandic Medical System AG, Feuerthalen, Switzerland).
The following criteria were considered for scoring intubation: jaw relaxation, position of the arytenoids, need for suction and first-pass success [10]. In case of failure of ET intubation at the first attempt, an adjunctive bolus of propofol (0.5 mg/kg) was administered IV.
Volume-controlled ventilation (VCV) (Aespire 7100, GE HealthCare, Illinois, USA) was started TV= 6 mL/kg, 20-22 breaths per minute, ratio 1:2 ratio and pressure limit 20 cmH2O and adjusted later to patient necessities. Flow was reduced to 0,5 L/min and air was added to achieve a FiO2 of 0.6.
In all cases, anesthesia was titrated clinically to effect to maintain a stable anesthetic plane characterized by autonomic stability, with HR and MAP ranging between 100 -130 min-1 and 60-80 mmHg respectively, muscle relaxation evaluated by looking at the tonicity of the hand, palpebral reflex and lack of purposeful movements. Physical access to the NHP under the surgical drapes was very limited. Fentanyl was titrated at 0.08 – 0.16 mcg/kg/min, remifentanil at 0.05 – 0.5 mcg/kg/min and propofol 0.1-0.6 mg/kg/min. To maintain adequate anesthetic depth, sevoflurane in oxygen and air was delivered in addition to the described anaesthetic protocol was added or boli of 1 mg/kg propofol IV were given in both groups to maintain proper level of hypnosis as deemed necessary clinically. Intraoperative rescue analgesia was provided with fentanyl 1 mcg/kg or remifentanil 1 to 3 mcg/kg, when MAP and HR increased suddenly more than 20% compared to the values recorded at the beginning of the surgery, as indicators of intraoperative nociception.
For the aim of the rurgeries, all animals were positioned in a stereotaxic frame. A 4-points scalp block with 2 mg/kg bupivacaine 0.25% (Bupivacain Sintetica 2.5 mg/ml, Sintetica SA, Mendrisio, Switzerland) was performed for 1 craniotomy, and 5 chamber implantations. For 2 animals undergoing laminectomies, bupivacaine was infiltrated SC at the incision site.
Macaques received 6 mL/kg/h NaCl 0.9% and 10 mL/kg/h heated ringer lactate IV. Hypotension was defined as a MAP lower than 60 mmHg, and in this case IV dopamine (Dopamin sintetica 50mg/5ml, Sintetica S.A., Mendrisio, Switzerland) 1-6 mcg/kg/min was administered.
For three surgeries of group R where the MAP values were not displayed on the anesthesia monitor or recorded, they were calculated post-hoc with the formula MAP=DAP+1/3(SAP-DAP).
For immediate post-operative analgesia, 30 minutes before the end of the procedure, animals received IV or SC 4 mg/kg carprofen (Rimadyl® 50 mg/ml, Zoetis, Schweiz GmbH, Delémont, Switzerland), group F received 0.03 mg/kg IV buprenorphine (Bupaq® 0.3 mg/ml, Richter Pharma AG, Wels, Switzerland) and group R had 0.2 mg/kg IV methadone.
To prevent PONV, maropitant 1 mg/kg (Prevomax, Dr.E.Graeub AG, Bern, Switzerland) was injected IV.
Once the operation ended, TIVA was discontinued, and animals removed from the stereotax. Monitoring of HR, RR, BP and SpO2 remained continuous whilst ventilatory support was gradually decreased, allowing animals to regain spontaneous breathing. Oxygen was provided until the animals were extubated and if they could not maintain a SpO2 above 95% while spontaneously breathing on air alone. Extubation took place when animals got cough reflex back; time from discontinuation of anesthesia until extubation was recorded (recovery time). Animals were consequently placed in a padded ICU cage covered by the heating blanket and checked until full recovery. When sitting and coordinated, they were brought back to their animal room in the facility, where they would spend the first post-operative night in an intermediate cage. Feed and water were provided, and they were in direct sight, auditive and tactile contact with the roommates.
Postoperative pain was evaluated in the following 7 days 3 times a day through a self-developed 3 point scoresheet. Buprenorphine 0.03 mg/kg IM or morphine 0,2 mg/kg IM were administered to treat moderate or severe pain respectively. Weight was also monitored before surgeries and daily thereafter.
3.1. Statical Analyses
The statistical evaluation was performed by using a computer software (Stata/SE 17.0, StataCorp, TX, USA). Data were evaluated for normality of distribution using Shapiro – Wilk test. Normally distributed data were compared between the 2 groups by using Student’s T-test and reported as mean ± standard deviation (SD). Not normally distributed data were compared with a Mann Whitney U test and reported as median and interquartile range (IQR). Quantity of both fluids was summed for each group and their mean extrapolated. Nominal data (number of animals receiving additional boli of propofol or opioids and the incidence of complications) were compared by using a Chi-squared test. A p value < 0.05 was considered statistically significant.
The outliers were calculated by using Microsoft Excel Software (version 16.78).
4. Results
A total of 16 anesthetic procedures in 10 animals were performed between 2022 and 2023. Two terminal procedures with remifentanil were then excluded, and 2 anesthesias, 1 with fentanyl and 1 with remifentanil, were ruled out because the mean duration of 572 minutes, was considerably longer than the others, based on an outlier calculation. Therefore, 12 anesthetic procedures involving 7 macaques (4 M. mulatta and 3 M. fascicularis) were included for this study: 4 anesthesia with fentanyl/propofol TIVA, 2 with fentanyl/propofol/0.4 (Minimun alveolar concentration) MACsevo PIVA and 6 anesthesia with remifentanil/propofol TIVA. Number of procedures, anesthetics and animals are presented in Table 1.

Table 1.
Detailed demographic data and procedures of the 7 Macaques included in the study.
| ID | Species | Weight (kg) | Gender | Age (years) | Procedure | TIVA/PIVA | Anesthesia’s duration (min) |
|---|---|---|---|---|---|---|---|
| Animal 1 | Macaca mulatta | 9 | F | 6 | spinal cord injury | propofol – fentanyl | 350 |
| tracer injection and bilateral craniotomy | propofol – fentanyl-0.4MACsevo | 195 | |||||
| Animal 2 | Macaca mulatta | 7.5 | F | 8 | ECoG implantation | propofol - remifentanil | 220 |
| Animal 3 | Macaca mulatta | 7 | M | 8 | headpost implantation | propofol - fentanyl | 295 |
| chamber implantation | propofol - remifentanil | 260 | |||||
| Animal 4 | Macaca mulatta | 8.2 | M | 8 | headpost implantation | propofol – fentanyl-0.4MACsevo | 390 |
| chamber implantation | propofol - remifentanil | 295 | |||||
| Animal 5 | Macaca fascicularis | 7 | F | 6 | stroke | propofol - fentanyl | 220 |
| RB-induced stroke | propofol - remifentanil | 130 | |||||
| Stroke + ANCE biopsy + Mapping and Imaging | propofol - remifentanil | 220 | |||||
| Animal 6 | Macaca fascicularis | 3.5 | F | 6 | headpost implantation | propofol - remifentanil | 145 |
| Animal 7 | Macaca fascicularis | 4.2 | F | 5 | headpost implantation | propofol - fentanyl | 95 |
F: female; M: male. ECoG: Electrocorticography; RB: Rose Bengalee; ANCE: adult neural cell ecosystem.
Animal 3 was anesthetized once with fentanyl-propofol TIVA and once with remifentanil-propofol TIVA. Animal number 4 was anesthetized once with fentanyl-propofol PIVA (with 0.4MACsevo). Animal number 5 was anesthetized once with fentanyl-propofol and twice with remifentanil-propofol TIVA. For the animals receiving both treatments, a washout period of at least 2 weeks occurred between each anesthesia.
The mean age of the animals was 6.5 ± 1.2 years in group F and 7.1 ± 1.1 years in group R. The median weight of the animals was 7.6 (7 – 8.8) kg in group F and 7 kg (7 – 7.5) kg in group R. The age and the weight of the animals (see Table 2) did not differ significantly between the 2 groups.
All animals were assigned to an ASA (American Society of Anesthesiologist) physical status classification II. A moderate to deep sedation and loss of consciousness in both groups was reached after a median time of 8.5 (4 – 12) minutes from injection, independently of the use of methadone in the premedication mix. The mean anesthesia duration was 257.5 ± 108.8 minutes in group F and 211.7 ± 64.1 minutes in group R and did not differ significantly between the 2 groups.
4.1. Group F:
For induction, propofol 0.3 ± 0.1 mg/kg/min CRI was started IV, followed by 3 mcg/kg fentanyl bolus and then CRI commenced with mean rate of 0.17 mcg/kg/min IV.
After induction, no apnea was observed and adequate jaw relaxation was achieved. First-pass success rate was 100% but moderate to severe cough was observed in all macaques and the arytenoids were moving while introducing the ET tube. Suction was necessary for 2 animals out of 6. During maintenance, average propofol CRI rate was decreased to 0.2 ± 0.05 mg/kg/min and average fentanyl was 0.13 ± 0.01 mcg/kg/min. In 2 animals (animals 1 and 4, see Table 1), aiming to stabilizing the anesthetic plane, low dose sevoflurane was added at an average of 0.8% (± 0.3 %) ETsevo (corresponding to 0.4 MACsevo) [11]. During 1 (out of 6) anesthetic procedure only 1 additional bolus of fentanyl was administered to improve intraoperative pain management. During 3 (out of 6) anesthetic procedures additional boli of propofol were administered with a median of 2 (1-2) boli. Fentanyl CRI had a stable decreasing administered dosage tapering off when the most painful stage of the procedure was over, and suturing was started. Hypotension (MAP < 60 mmHg) occurred in 5 anesthesias and, in 4 out of 5 mean 2.9 ± 2.3 mcg/kg/min dopamine was administered IV (Table 3).
Total NaCl 0.9% and Ringer lactate administered were 14.7 ± 4.4ml/kg/h.
4.2. Group R:
For induction, propofol CRI was commenced at 0.17 ± 0.1 mg/kg/min followed by 3 mcg/kg remifentanil bolus and CRI commenced at mean 0.1 ± 0.02 mcg/kg/min. The quality of intubation in all animals was excellent, with 100%,first-pass success rate, apneic time, adequate jaw relaxation, still arytenoids and no signs of laryngospasm or cough, making the visibility of the larynx optimal without need of suction. Propofol was decreased up to 0.16 ± 0.03 mg/kg/min for maintenance. During 3 (out of 6) anesthetic procedures additional boli of propofol were administered with a median of 0.5 (0-1) boli.
Remifentanil rate was increased to 0.2 mcg/kg/min at skin incision and, when intense surgical stimulation was taking place, a 1-3 mcg/kg bolus was administered via the pump. The mean rate of remifentanil used during anesthesia was 0.16 ± 0.05 mcg/kg/min.
During 4 (out of 6) anesthetic procedures a median of 4 (3-4) additional boli of remifentanil were administered to improve intraoperative pain management.
Overall, the mean fluids rate was 13.9 ± 6.3 ml/kg/h.
No episodes of bradycardia or hypotension were detected, and therefore no vasoactive support was given to 5 out of 6 animals (Table 3). Animal 4 experienced arrhythmias during rose Bengale induced cortical photothrombotic stroke, and its HR in 25 minutes decreased from 120 to 90 to 65 beats/min. Concurrently the oscillometric device failed detecting the blood pressure and the metatarsal pulse was no more assessable, therefore hypotension was suspected. Ephedrine 0.1 mg/kg was administered, fluids increased to 27 ml/kg for 15 minutes and atropine 0.01 mg/kg was also administered IV to contrast bradycardia.
The mean dose of fluids administered intraoperatively did not differ significantly between the 2 groups.
Anesthesia with remifentanil had a more dynamic course of action and remifentanil was titrated during anesthesia depending on patient’s requirements (Figure 1 and Figure A1).
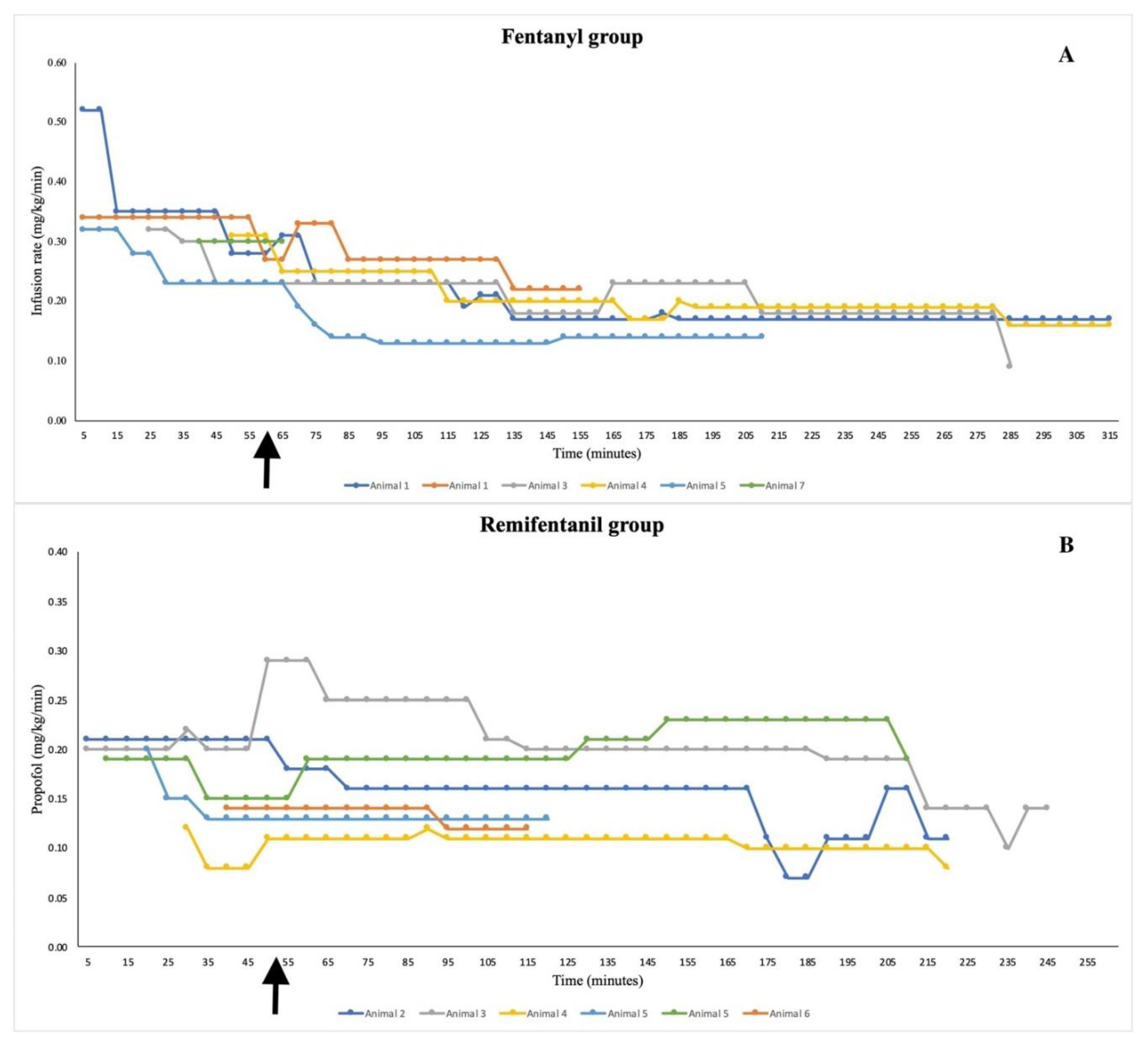
Overall, the rate of propofol administered in group F was significantly higher than in group R during both induction and maintenance phase (p= 0.008 and p=0.02 respectively) (Figure 2 and Figure A2).
The number of animals receiving additional boli of propofol or the median number of boli did not differ significantly between the 2 groups. Intraoperatively, the cardiovascular and respiratory parameters did not differ significantly between the 2 groups (Table 2). However, the incidence of hypotension was significantly higher in group F (Table 3).
Intraoperatively, the macroscopic appearance of the dura and the brain were normal and none of the animals developed cerebral edema.
Recoveries were significantly faster (p<0.001) from discontinuation of the CRI in group R – with 8 (6– 10) minutes – compared to group F, with 18 (14– 22) minutes (Figure 3). All the recoveries were uneventful in both groups and no morbidity nor signs of distress and neurologic impairment were recorded. No animals developed PONV.
5. Discussion
This is the first description of a remifentanil-based TIVA for macaques undergoing neurosurgery demonstrating its favourable clinical quality, hemodynamic stability, decreased incidence of cardiovascular complications and practicability by allowing a rapid modulation of the anaesthetic plan based on patient’s needs compared to fentanyl-propofol TIVA.
Remifentanil is a selective μ-opioid agonist, with potency similar to fentanyl [12] but with faster analgesic efficacy and shorter elimination half – life, thanks to its pharmacokinetic profile. In fact, unlike fentanyl, remifentanil is hydrolysed by plasmatic esterases, and therefore its duration of effect is independent from liver or kidney function [13].
In humans, its recommended dosage for multimodal anaesthesia in both adult and paediatric patients ranges from 0.05 to 0.5 mcg/kg/min [14,15,16], with an estimated half-life of 8 minutes [17] and is reportedly very similar in different species: 0.4 mcg/kg/min remifentanil was used for cats undergoing ovariohysterectomy, with good level of anesthesia [18] whereas, in healthy adult female dogs 0.25 – 0.5 mcg/kg/min during surgery was considered effective [19]. Also, in rabbits undergoing a tracheomalacia model (personal communication of the senior anesthesiologists) the remifentanil (0.2-0.4 mcg/kg/min) -propofol TIVA dosing correlated to the quantity required in humans. We could prove that the rate of remifentanil required to provide effective multimodal anesthesia in NHPs was within the interval described for human patients. The dosage of remifentanil was continuously titrated based on individual sympathetic and cardiovascular reactions, aiming to rapidly achieve adequate anesthetic depth and analgesia. On contrary, the pharmacokinetic of fentanyl with its longer onset time and half-life, did not allow for such a fine tuning. Therefore, the remifentanil protocol proved to be a more dynamic and customized anesthesia. The rates of fentanyl used here are within published ranges for macaques of 0.16 to 0.42 mcg/kg/min [20]. The only study on remifentanil administration in Macaques describes higher dosages (0.58 mcg/kg/min) compared with those reported in our article [21]. However, only the sedative effects were investigated, leaving out remifentanyl cardiovascular and respiratory drug effects.
The average cardiovascular values were within desired physiological range for anesthetized macaques [22,23] and did not differ significantly in both treatment groups. This differs from human literature findings [24], where HR in remifentanil-based TIVA was significantly lower than with fentanyl. We can’t exclude that the inclusion of a larger population would highlight significant differences between the two treatments.
A clinically relevant achievement with the presented remifentanil TIVA is the physiologically stable maintenance of blood pressure without administration of dopamine or other vasopressors. On the contrary, in group F, 4 out of 5 animals needed support with dopamine. In fact, fentanyl itself, at incremental doses in Rhesus Monkeys, might induce a significant decrease in MAP which is plasma concentration dependent [6]. Moreover, the addition of inhalant anesthesia in 2 animals in group F might have been a confounding factor even if it is unlikely that 0.4 MAC sevoflurane contributed to hypotension for those animals receiving PIVA [25]. An important difference between the two groups consists in the addition of methadone for premedication in group F. Since this is a retrospective study, the lack of standardization of the premedication protocol is a limit of the study. In group R, only one animal experienced hypotension associated with bradycardia, but this was likely secondary to the intracranial manipulation and not related to the anesthetic itself.
As in humans [26] a lower quantity of propofol was administered to the macaques during the remifentanil-TIVA, presumably due to the synergism with propofol contributing to hypnosis. This sparing effect of remifentanil over propofol had already been describe also in Macaques, in which the administration of remifentanil 0.58 mcg/kg/min lead to a decrease of 61% of the sedative dose of propofol in comparison to a sedation regimen obtained without the opioid [21]. Both anesthetic regimens described here used lower rates of propofol compared with rates previously described for NHPs [27], being within 0.16 and 0.6 mg/kg/min [27,28] likely due to the multimodal anesthesia implemented, with the systematic addition of loco-regional anesthesia. Reducing the propofol rate might have played a role to the complete absence of hypotension during anesthesia with remifentanil. [26]
Nonetheless, decreasing the rate of propofol might increase the risk of intraoperative awareness and spontaneous movements, which mandates a tight monitoring of anesthetic depth. To improve anesthetic depth monitoring during maintenance, Bisprectral index (BIS) monitor is currently used in humans [29,30,31,32] and laboratory animals [33]; however, this [33] remains to be developed in NHPs both for the technical feasibility and the correlation with the anesthetic depth within different anesthetic protocols.
In humans, orotracheal intubation – especially if eliciting cough reflex – might induce an increase in HR and blood pressure due to catecholamine release [34,35], to be avoided in patients affected by cardiovascular disease or at risk of developing intracranial hypertension. Remifentanil was more effective than fentanyl to control the hemodynamic response to ET intubation in humans [24,36]. Similarly, in all macaques of this study, ET intubation with remifentanil was smooth, not eliciting cough reflexes and providing a transient apnea which was not associated with hypoxemic events [37,38]. In the authors experience, NHPs are – when compared with other veterinary species – more prone to develop hypoxia during intubation, and consequent bradycardia due to vagally mediated reflex response [39]. With the aim of preventing complications, it is of practical importance that the animals are pre-oxygenated with high flow oxygen by face mask and SpO2 and ECG monitored during induction. In fact, delivering passive oxygenation before induction might significantly reduce but not prevent the incidence of desaturation [40,41]. In humans, the addition of a neuromuscular blocking agent (NMBA) to remifentanil improved intubation conditions [42]. The results of the present study highlighted that the induction with remifentanil better suppressed airways response and allowed for a safer apneic time during intubation compared to fentanyl, even without the addition of a NMBA. The administration of the latter was contraindicated in these models as an intraoperative monitoring of the motor pathways was required.
The conditioning over the mechanical ventilation was more easily achieved in those animals’ receiving remifentanil if compared with those in which fentanyl was infused. In mechanically ventilated patients in intensive care setting, remifentanil reduced time of weaning from mechanical ventilation and extubation in comparison to other opioids [43,44]. Time to weaning from mechanical ventilation was unfortunately note recorded systematically, but remifentanil contributed also to a faster extubation time for all animals compared to fentanyl [43,44]. The reduced rate of propofol in the R group and the effective maintenance of normothermia contributed to the fast and optimal recovery, without tremors nor shivering. The quality of recovery was not scored systematically in the present study. However, it was uneventful in all the animals included. Maropitant, given at the end of every anesthesia, might contribute to reduce PONV and improve post-operative analgesia and is recommended as an elective antiemetic for NHPs undergoing neurosurgeries [45].
As per limitations of our retrospective study, we worked with a relatively small group of animals undergoing only neurosurgery, so the suitability of remifentanil – propofol TIVA for macaques involved in other procedures should be explored. Moreover, since our retrospective study followed planned experimental procedures, it was not possible to decide over the surgical procedures, including types of manipulation and duration. On the other hand, it is important to take advantage of the number of animals and situations present in the research facility where we practice, so to always be keen on refining animal care following available literatures and colleague experience. Moreover, considering that animals in both protocols were all young healthy adults, further precautions might be taken with higher risk patient population, such as older, juvenile and pregnant macaques.
Another limit of the study concerns its retrospective design. A prospective study allows the limitation of confounding factors and a higher standardization; however, this type of investigation allows reducing the number of animals used and provides a refinement to the recently anaesthetized animals with the treatment that is superior.
6. Conclusions
This retrospective assessment proved that remifentanil-propofol anesthesia improved the quality of endotracheal intubation, maintained stable hemodynamic, without administration of dopamine and excellent surgical conditions. Moreover, lower doses of propofol were infused and granted a rapid offset and recovery, resulting in a refined anesthesia compared to traditional fentanyl-propofol TIVA in macaques undergoing neurosurgery.
Author Contributions
Conceptualization, A.B.; methodology, A.B.; formal analysis, M.V.N., C.L., A. B.; investigation, M.V.N., C.C., C.L., A.W., F.L., M.C.S., A.B.; resources, M.C.S., A.B.; data curation, M.V.N., C.C., C.L., A.W., F.L.. A.B.; writing—original draft preparation, M.V.N., C.L.; writing—review and editing, C.C., A.B.; visualization, A.W., F.L., M.C.S.; supervision, A.B.; project administration, A.B., M.C.S. All authors have read and agreed to the published version of the manuscript.
Funding
MCS is supported by SNF grants 310030_204544 and 31NE30_203974 (ERAnet).
Institutional Review Board Statement
This was a retrospective review of anesthesias for experimental neurosurgical procedures, which were included in different licenses all approved by the cantonal veterinary authority of Fribourg, Switzerland (2020_07_FR, 2020-21E-FR, 2020-26E-FR, 2023-18-FR).
Data Availability Statement
The data that support the findings of this study are available upon request from the corresponding author.
Acknowledgments
This study was supported by the collaboration of: Stéphanie Lacour, Grégoire Courtine – principal investigators, Joceline Bloch - neurosurgeon, Samy Rima, Marcus Haag, Alix Trouillet, Charles Lachtoumane - scientists, Andrina Zbinden – animal welfare officer, Nina Trimmel – clinical veterinarian, Cécile Dousse, Aurelie Chanthany – animal caretakers.
Conflicts of Interest
Conflict of interests do not apply for the authors of this article.
Appendix A
Figure A1.
Individual Fentanyl (A) and remifentanil (B) infusion rates (mcg/kg/min). The Animal ID refers to Table 1. The arrow indicates the shift from the induction phase to the maintenance phase of anesthesia.
Figure A1.
Individual Fentanyl (A) and remifentanil (B) infusion rates (mcg/kg/min). The Animal ID refers to Table 1. The arrow indicates the shift from the induction phase to the maintenance phase of anesthesia.
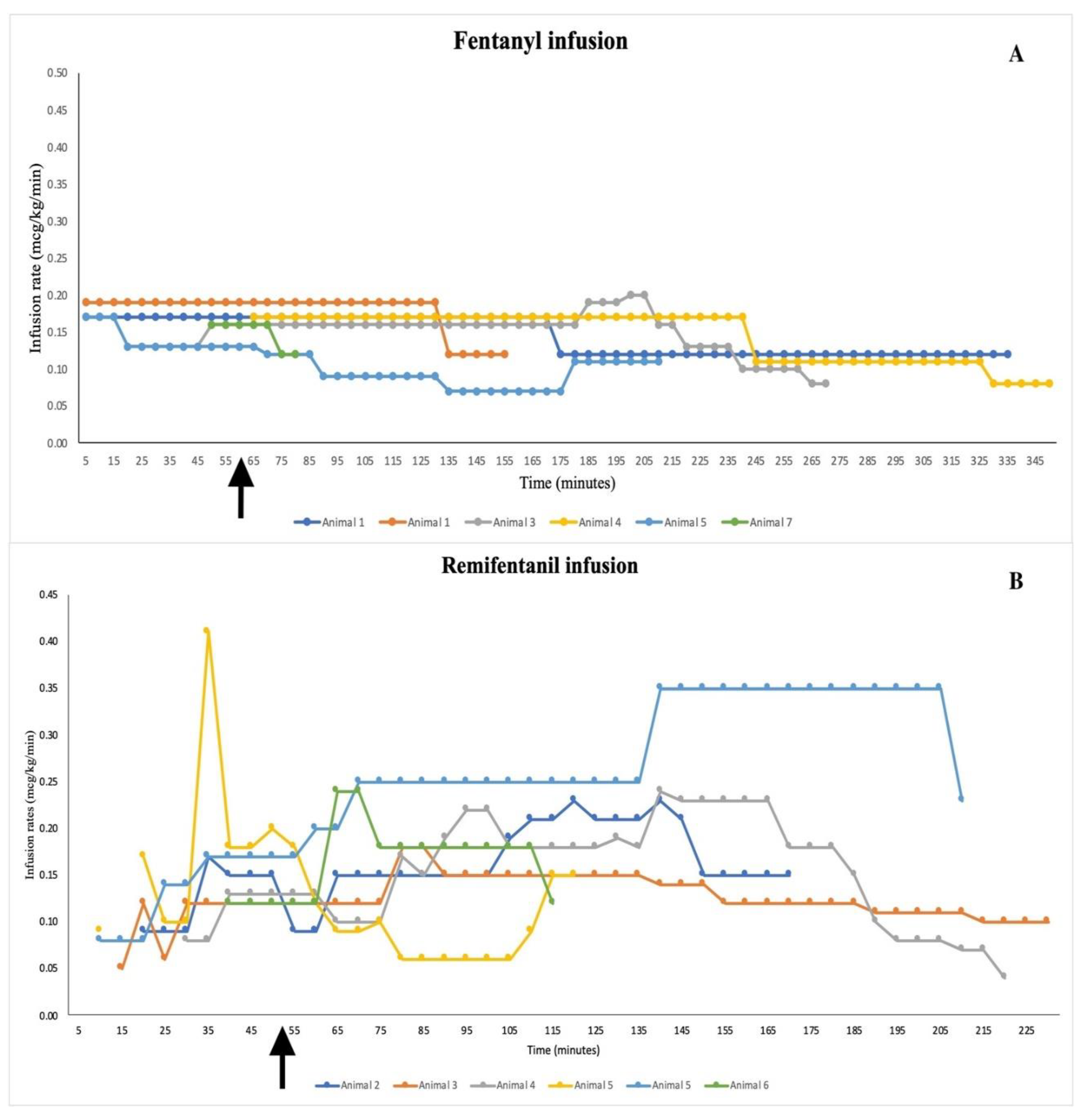
Figure A2.
Individual Propofol infusion rate (mg/kg/min) in fentanyl (A) and remifentanil (B) based TIVA/PIVA. The Animal ID refers to Table 1. The arrow indicates the shift from the induction phase to the maintenance phase of anesthesia.
Figure A2.
Individual Propofol infusion rate (mg/kg/min) in fentanyl (A) and remifentanil (B) based TIVA/PIVA. The Animal ID refers to Table 1. The arrow indicates the shift from the induction phase to the maintenance phase of anesthesia.
References
- Kaisti, K.K.; Metsähonkala, L.; Teräs, M.; Oikonen, V.; Aalto, S.; Jääskeläinen, S.; Hinkka, S.; Scheinin, H. Effects of Surgical Levels of Propofol and Sevoflurane Anesthesia on Cerebral Blood Flow in Healthy Subjects Studied with Positron Emission Tomography. Anesthesiology 2002, 96, 1358–1370. [CrossRef]
- Matta, B.F.; Heath, K.J.; Tipping, K.; Summors, A.C. Direct Cerebral Vasodilatory Effects of Sevoflurane and Isoflurane. Anesthesiology 1999, 91, 677–677. [CrossRef]
- Enlund, M.; Andersson, J.; Hartvig, P.; Valtysson, J.; Wiklund, L. Cerebral Normoxia in the Rhesus Monkey during Isoflurane- or Propofol- Induced Hypotension and Hypocapnia, despite Disparate Blood-Flow Patterns. A Positron Emission Tomography Study. Acta Anaesthesiol Scand 1997, 41, 1002–1010. [CrossRef]
- Yoo, Y.C.; Bai, S.J.; Lee, K.Y.; Shin, S.; Choi, E.K.; Lee, J.W. Total Intravenous Anesthesia with Propofol Reduces Postoperative Nausea and Vomiting in Patients Undergoing Robot-Assisted Laparoscopic Radical Prostatectomy: A Prospective Randomized Trial. Yonsei Med J 2012, 53, 1197–1202. [CrossRef]
- Varughese, S.; Ahmed, R. Environmental and Occupational Considerations of Anesthesia: A Narrative Review and Update. Anesth Analg 2021, 133, 826–835. [CrossRef]
- Nussmeier, N.A.; Benthuysen, J.L.; Steffey, E.P.; Anderson, J.H.; Carstens, E.E.; Eisele, J.H.; Stanley, T.H. Cardiovascular, Respiratory, and Analgesic Effects of Fentanyl in Unanesthetized Rhesus Monkeys. Anesth Analg 1991, 72, 221–226. [CrossRef]
- Liu, J. V.; Hirano, Y.; Nascimento, G.C.; Stefanovic, B.; Leopold, D.A.; Silva, A.C. FMRI in the Awake Marmoset: Somatosensory-Evoked Responses, Functional Connectivity, and Comparison with Propofol Anesthesia. Neuroimage 2013, 78, 186–195. [CrossRef]
- Hosseinzadeh, H.; Eydi, M.; Ghaffarlou, M.; Ghabili, K.; Golzari, S.E.; Bazzazi, A.M. Administration of Remifentanil in Establishing a More Stable Post-Anesthesia Cardiovascular Status in Neurosurgical Procedures. J Cardiovasc Thorac Res 2012, 4, 21–24. [CrossRef]
- Maurtua, M.A.; Deogaonkar, A.; Bakri, M.H.; Mascha, E.; Na, J.; Foss, J.; Sessler, D.I.; Lotto, M.; Ebrahim, Z.; Schubert, A. Dosing of Remifentanil to Prevent Movement During Craniotomy in the Absence of Neuromuscular Blockade. J Neurosurg Anesthesiol 2008, 20, 221–225. [CrossRef]
- Sakles, J.C.; Chiu, S.; Mosier, J.; Walker, C.; Stolz, U. The Importance of First Pass Success When Performing Orotracheal Intubation in the Emergency Department. Academic Emergency Medicine 2013, 20, 71–78. [CrossRef]
- Soma, L.R.; Tierney, W.J.; Hogan, G.K.; Satoh, N. The Effects of Multiple Administrations of Sevoflurane to Cynomolgus Monkeys: Clinical Pathologic, Hematologic, and Pathologic Study; 1995.
- Scott, L.J.; Perry, C.M. Remifentanil: A Review of Its Use during the Induction and Maintenance of General Anaesthesia. Drugs 2005, 65, 1793–1823. [CrossRef]
- Lauzuers, H.; Camu, F.; Vanlersberghe, C. Opioid What Advantages Does It Offer in Analgesia and Anaesthesia?
- Burkle, H.; Dunbar, S.; Van Aken, H. Remifentanil. Anesth Analg 1996, 83, 646–651. [CrossRef]
- Hall, A.P.; Thompson, J.P.; Leslie, N.A.; Fox, A.J.; Kumar, N.; Rowbotham, D.J. Comparison of Different Doses of Remifentanil on the Cardiovascular Response to Laryngoscopy and Tracheal Intubation. Br J Anaesth 2000, 84, 100–102. [CrossRef]
- Sneyd, J.R.; Camu, F.; Doenicke, A.; Mann, C.; Holgersen, O.; Helmers, J.H.J.H.; Appelgren, L.; Noronha, D.; Upadhyaya, B.K. Remifentanil and Fentanyl during Anaesthesia for Major Abdominal and Gynaecological Surgery. An Open, Comparative Study of Safety and Efficacy. Eur J Anaesthesiol 2001, 18, 605–614. [CrossRef]
- Heard, C.M.B.; Fletcher, J.E. Sedation and Analgesia. In Pediatric Critical Care; Elsevier, 2011; pp. 1654–1681.
- Machado, M.L.; Soares, J.H.N.; Kuster de Albuquerque Gress, M.A.; dos Santos e Castro, D.; Teodoro Rosa, K.; Bauer de Araujo Doria, P.; Otero Ascoli, F. Dose-Finding Study Comparing Three Treatments of Remifentanil in Cats Anesthetized with Isoflurane Undergoing Ovariohysterectomy. J Feline Med Surg 2018, 20, 164–171. [CrossRef]
- Gimenes, A.M.; De Araujo Aguiar, A.J.; Perri, S.H.V.; De Paula Nogueira, G. Effect of Intravenous Propofol and Remifentanil on Heart Rate, Blood Pressure and Nociceptive Response in Acepromazine Premedicated Dogs. Vet Anaesth Analg 2011, 38, 54–62. [CrossRef]
- Nunamaker, E.; Malinowski, C.; Godrooe, A.; Guerriero, K.; Burns, M. Anesthesia and Analgesia in Non Human Primates - Chapter 18. In Anesthesia and Analgesia in Laboratory Animals; Dyson, M.C., Jirkof, P., Lofgren, J., Nunamaker, E.A., Pang, D., Eds.; Elsevier: Cambridge, Massachusetts, USA, 2023; pp. 441–479 ISBN 9780128222157.
- Kops, M.S.; Pesic, M.; Petersen, K.U.; Schmalix, W.A.; Stöhr, T. Impact of Concurrent Remifentanil on the Sedative Effects of Remimazolam, Midazolam and Propofol in Cynomolgus Monkeys. Eur J Pharmacol 2021, 890. [CrossRef]
- Young, S.S.; Schilling, A.M.; Skeans, S.; Ritacco, G. Short Duration Anaesthesia with Medetomidine and Ketamine in Cynomolgus Monkeys. Lab Anim 1999, 33, 162–168. [CrossRef]
- Brownlee, R.D.; Kass, P.H.; Sammak, R.L. Blood Pressure Reference Intervals for Ketamine-Sedated Rhesus Macaques (Macaca Mulatta). J Am Assoc Lab Anim Sci 2020, 59, 24–29. [CrossRef]
- Ko, B.J.; Oh, J.N.; Lee, J.H.; Choi, S.R.; Lee, S.C.; Chung, C.J. Comparison of Effects of Fentanyl and Remifentanil on Hemodynamic Response to Endotracheal Intubation and Myoclonus in Elderly Patients with Etomidate Induction. Korean J Anesthesiol 2013, 64, 12–18. [CrossRef]
- Ebert, T.J.; Muzi, M.; Lopatka, C.W. Neurocirculatory Responses to Sevoflurane in Humans. Anesthesiology 1995, 88–95. [CrossRef]
- Del Gaudio, A.; Ciritella, P.; Perrotta, F.; Puopolo, M.; Lauta, E.; Mastronardi, P.; De Vivo, P. Remifentanil vs Fentanyl with a Target Controlled Propofol Infusion in Patients Undergoing Craniotomy for Supratentorial Lesions. Minerva Anestesiol 2006, 72, 309–319.
- Fowler, K.A.; Huerkamp, M.J.; Pullium, J.K.; Subramanian, T. Anesthetic Protocol: Propofol Use in Rhesus Macaques (Macaca Mulatta) during Magnetic Resonance Imaging with Stereotactic Head Frame Application. Brain Research Protocols 2001, 7, 87–93. [CrossRef]
- Benveniste, H.; Fowler, J.S.; Rooney, W.D.; Moller, D.H.; Walter Backus, W.; Warner, D.A.; Carter, P.; King, P.; Scharf, B.; Alexoff, D.A.; et al. Maternal-Fetal In Vivo Imaging: A Combined PET and MRI Study; 2003; Vol. 44;
- Gao, W. wei; He, Y. hong; Liu, L.; Yuan, Q.; Wang, Y. feng; Zhao, B. BIS Monitoring on Intraoperative Awareness: A Meta-Analysis. Curr Med Sci 2018, 38, 349–353. [CrossRef]
- Zhang, C.; Xu, L.; Ma, Y.Q.; Sun, Y.X.; Li, Y.H.; Zhang, L.; Feng, C.S.; Luo, B.; Zhao, Z.L.; Guo, J.R.; et al. Bispectral Index Monitoring Prevent Awareness during Total Intravenous Anesthesia: A Prospective, Randomized, Double-Blinded, Multi-Center Controlled Trial. Chin Med J (Engl) 2011, 124, 3664–3669. [CrossRef]
- Myles, P.S.; Leslie, K.; McNeil, J.; Forbes, A.; Chan, M.T.V. Bispectral Index Monitoring to Prevent Awareness during Anaesthesia: The B-Aware Randomised Controlled Trial. Lancet 2004, 363, 1757–1763. [CrossRef]
- Oliveira, C.R.D.; Bernardo, W.M.; Nunes, V.M. Benefit of General Anesthesia Monitored by Bispectral Index Compared with Monitoring Guided Only by Clinical Parameters. Systematic Review and Meta-Analysis. Brazilian Journal of Anesthesiology (English Edition) 2017, 67, 72–84. [CrossRef]
- Petrucci, M.; Spadavecchia, C.; Wanderer, S.; Boillat, G.; Marbacher, S.; García Casalta, L.G.; Casoni, D. Usefulness and Reliability of the Bispectral Index during Balanced Anesthesia for Neurovascular Surgery in New Zealand White Rabbits. Brain Sci 2023, 13. [CrossRef]
- Shribman, A.J.; Smith, G.; Achola, K.J. Cardiovascular and Catecholamine Responses to Laryngoscopy with and without Tracheal Intubation. Br J Anaesth 1987, 59, 295–299. [CrossRef]
- Sarkar, J.; Anand, T.; Kamra, S.K. Hemodynamic Response to Endotracheal Intubation Using C-Trach Assembly and Direct Laryngoscopy. Saudi J Anaesth 2015, 9, 343–347. [CrossRef]
- Albertin, A.; Casati, A.; Deni, F.; Danelli, G.; Comotti, L.; Grifoni, F.; Fanelli, G.; San Raffaele, I.H. Clinical Comparison of Either Small Doses of Fentanyl or Remifentanil for Blunting Cardiovascular Changes Induced by Tracheal Intubation. Minerva Anestesiol 2000, 66, 691–696.
- Leone, M.; Rousseau, S.; Avidan, M.; Delmas, A.; Viviand, X.; Guyot, L.; Martin, C. Target Concentrations of Remifentanil with Propofol to Blunt Coughing during Intubation, Cuff Inflation, and Tracheal Suctioning. Br J Anaesth 2004, 93, 660–663. [CrossRef]
- Muellejans, B.; López, A.; Cross, M.H.; Bonome, C.; Morrison, L.; Kirkham, A.J.T. Remifentanil versus Fentanyl for Analgesia Based Sedation to Provide Patient Comfort in the Intensive Care Unit: A Randomized, Double-Blind Controlled Trial. Crit Care 2004, 8, R1–R11. [CrossRef]
- Poliquin, P.G.; Biondi, M.; Ranadheera, C.; Hagan, M.; Bello, A.; Racine, T.; Allan, M.; Funk, D.; Hansen, G.; Hancock, B.; et al. Delivering Prolonged Intensive Care to a Non-Human Primate: A High Fidelity Animal Model of Critical Illness. Sci Rep 2017, 7. [CrossRef]
- Wimalasena, Y.; Burns, B.; Reid, C.; Ware, S.; Habig, K. Apneic Oxygenation Was Associated with Decreased Desaturation Rates during Rapid Sequence Intubation by an Australian Helicopter Emergency Medicine Service. Ann Emerg Med 2015, 65, 371–376. [CrossRef]
- Riyapan, S.; Lubin, J. Apneic Oxygenation May Not Prevent Severe Hypoxemia During Rapid Sequence Intubation: A Retrospective Helicopter Emergency Medical Service Study. Air Med J 2016, 35, 365–368. [CrossRef]
- Jiao, J.; Huang, S.; Chen, Y.; Liu, H.; Xie, Y. Comparison of Intubation Conditions and Apnea Time after Anesthesia Induction with Propofol/Remifentanil Combined with or without Small Dose of Succinylcholine. Int J Clin Exp Med 2014, 7, 393–399.
- Breen, D.; Karabinis, A.; Malbrain, M.; Morais, R.; Albrecht, S.; Jarnvig, I.-L.; Parkinson, P.; Kirkham, A.J. Open Access Decreased Duration of Mechanical Ventilation When Comparing Analgesia-Based Sedation Using Remifentanil with Standard Hypnotic-Based Sedation for up to 10 Days in Intensive Care Unit Patients: A Randomised Trial. Crit Care 2005, 9, R200–R210. [CrossRef]
- Zhu, Y.; Wang, Y.; Du, B.; Xi, X. Could Remifentanil Reduce Duration of Mechanical Ventilation in Comparison with Other Opioids for Mechanically Ventilated Patients? A Systematic Review and Meta-Analysis. Crit Care 2017, 21, 206. [CrossRef]
- Steinbach, J.R.; MacGuire, J.; Chang, S.; Dierks, E.; Roble, G.S. Assessment of Pre-Operative Maropitant Citrate Use in Macaque (Macaca Fasicularis & Macaca Mulatta) Neurosurgical Procedures. J Med Primatol 2018, 47, 178–184. [CrossRef]
Figure 1.
Remifentanil and fentanyl infusion rates (mcg/kg/min) in Macaca anaesthetized with remifentanil/propofol TIVA (n=6) or fentanyl/propofol TIVA (n=6) and undergoing neurosurgical procedures. The arrow indicates the shift from the induction phase to the maintenance phase of anaesthesia.
Figure 1.
Remifentanil and fentanyl infusion rates (mcg/kg/min) in Macaca anaesthetized with remifentanil/propofol TIVA (n=6) or fentanyl/propofol TIVA (n=6) and undergoing neurosurgical procedures. The arrow indicates the shift from the induction phase to the maintenance phase of anaesthesia.
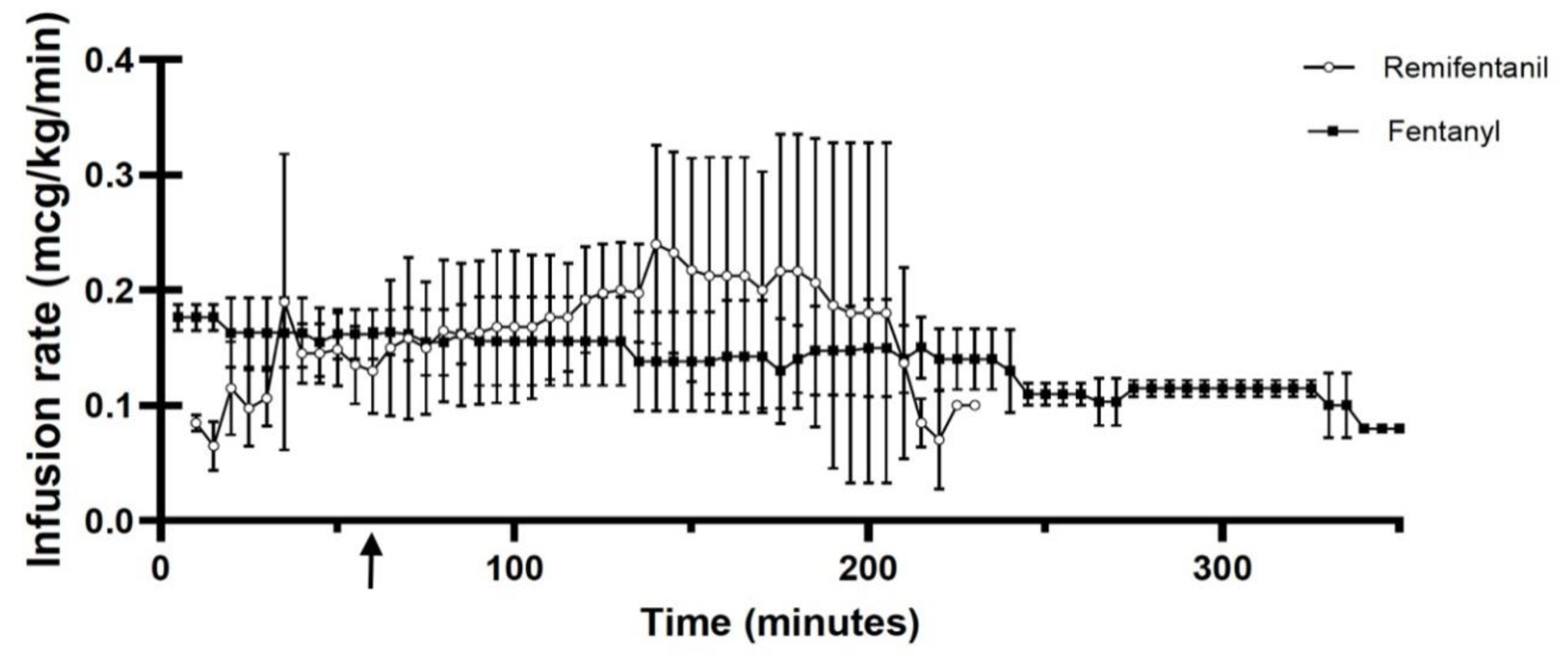
Figure 2.
Propofol infusion rate (mg/kg/min) administered for maintenance of general anaesthesia in Macaca undergoing nuerosurgeries and anaesthetized with remifentanil/propofol TIVA (n=6) or fentanyl/propofol TIVA (n=6). in remifentanil or fentanyl based TIVA/PIVA. The arrow indicates the shift from the induction phase to the maintenance phase of anesthesia.
Figure 2.
Propofol infusion rate (mg/kg/min) administered for maintenance of general anaesthesia in Macaca undergoing nuerosurgeries and anaesthetized with remifentanil/propofol TIVA (n=6) or fentanyl/propofol TIVA (n=6). in remifentanil or fentanyl based TIVA/PIVA. The arrow indicates the shift from the induction phase to the maintenance phase of anesthesia.
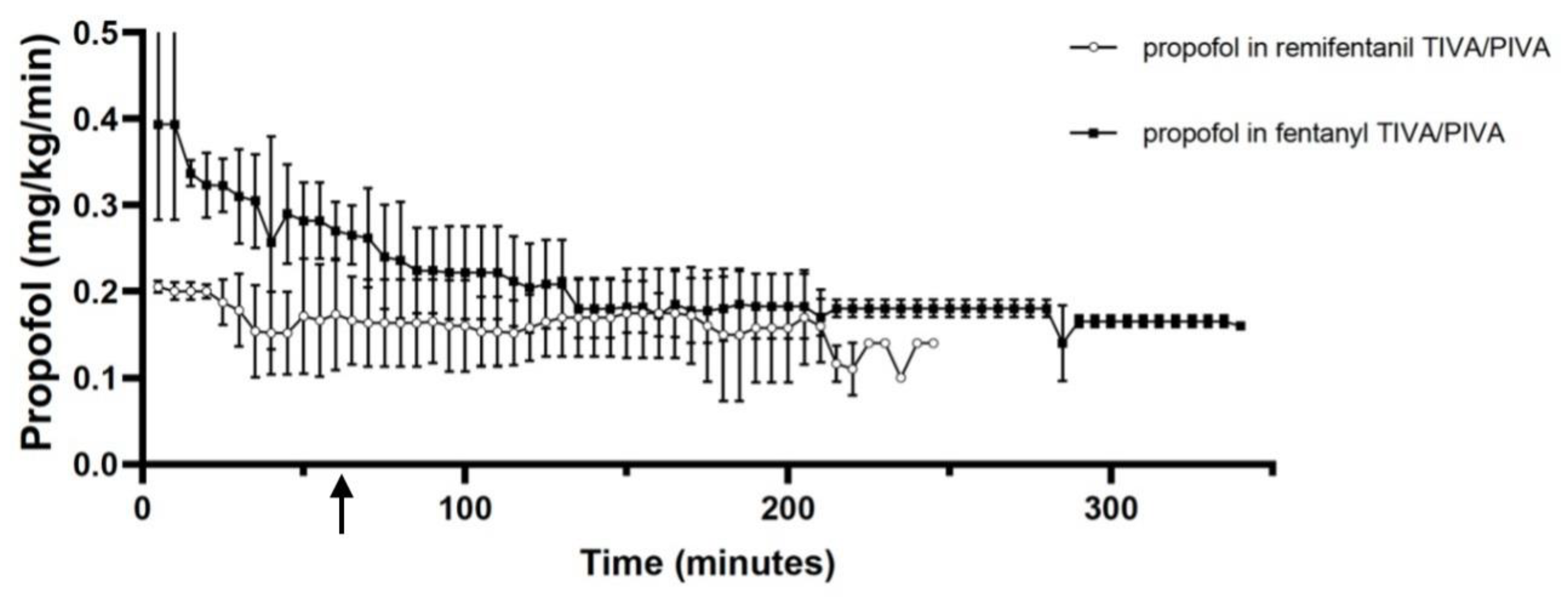
Figure 3.
Box and whiskers plots representing the recovery time in Macaca in Macaca anaesthetized with (F) fentanyl /propofol (n=6) or (R) remifentanil /propofol (n=6) TIVA/PIVA infusion intraoperatively. p<0.05 statistically significant.
Figure 3.
Box and whiskers plots representing the recovery time in Macaca in Macaca anaesthetized with (F) fentanyl /propofol (n=6) or (R) remifentanil /propofol (n=6) TIVA/PIVA infusion intraoperatively. p<0.05 statistically significant.
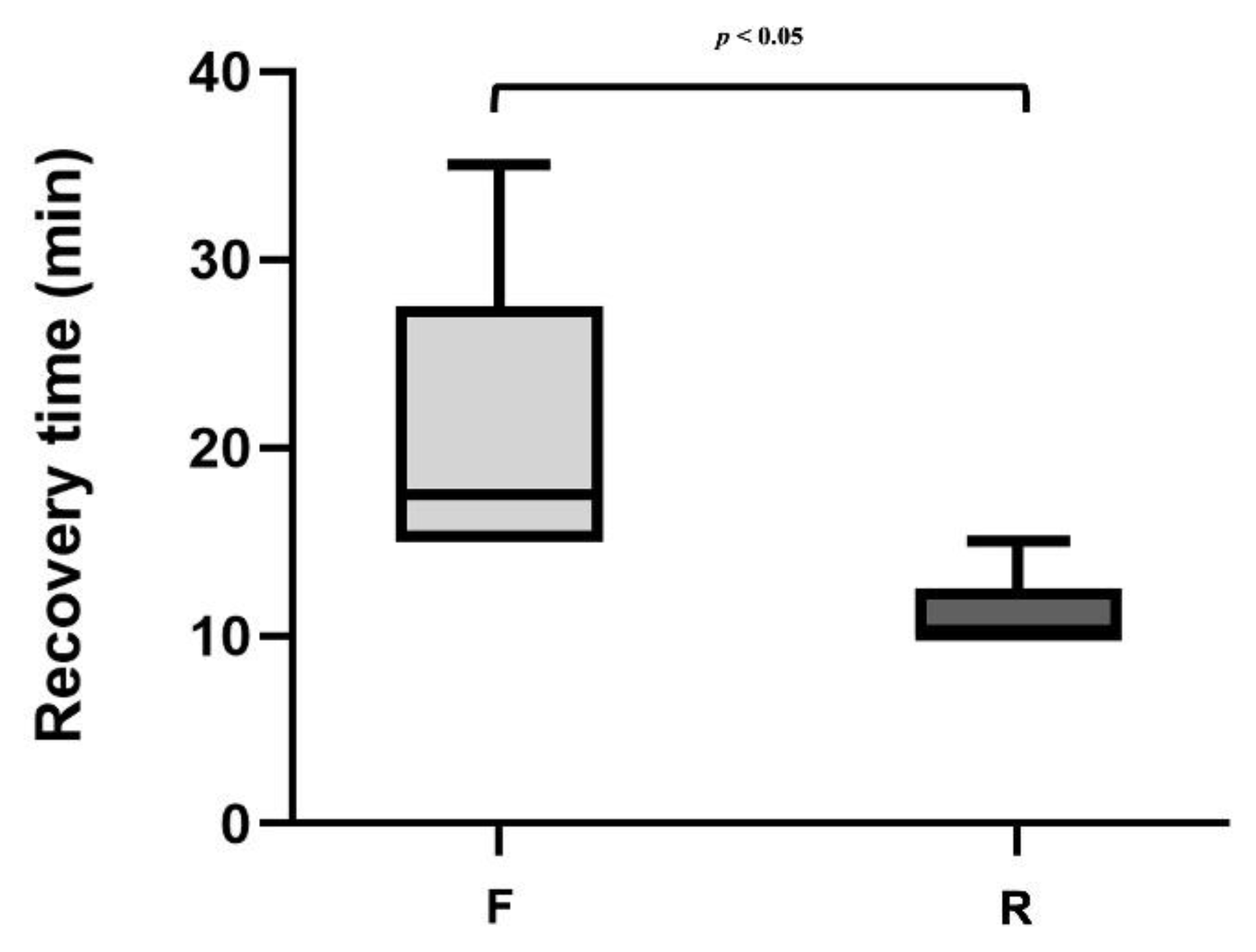
Table 2.
Comparison of variables in fentanyl versus remifentanil TIVA/PIVA.
| Variables | Fentanyl TIVA/PIVA | Remifentanil TIVA |
|---|---|---|
| HR (beats/min) | 118 ± 26 | 102 ± 11 |
| RR (breaths/min) | 22 ± 5 | 21 ± 4 |
| SAP (mmHg) | 104 ± 14 | 93 ± 8 |
| MAP (mmHg) | 67 ± 2 | 70 ± 8 |
| DAP (mmHg) | 51 ± 20 | 54 ± 10 |
| ETCO2 (mmHg) | 46 ± 5 | 38 ± 8 |
| SpO2 (%) | 96 ± 2 | 96 ± 1 |
| TV (ml/kg) | 7 ± 2 | 9 ± 1 |
| PIP (cm H2O) | 13 ± 2 | 15 ± 2 |
| T (°C) | 37 ± 1 | 37 ± 1 |
Table 3.
Incidence (number of animals out of total) of hepisodes of bradycardia and hypotension in Macaques receving fentnayl-propofol (group F) or remifentanil-propofol (group R) TIVA.
Table 3.
Incidence (number of animals out of total) of hepisodes of bradycardia and hypotension in Macaques receving fentnayl-propofol (group F) or remifentanil-propofol (group R) TIVA.
| Complication | Group F | Group R |
|---|---|---|
| Hypotension | 5/6 | 1/6 |
| Bradycardia | 0/6 | 1/6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



